 Huailan Zhao
Huailan Zhao Siquan Zhu*
Siquan Zhu*- Department of Ophthalmology, Clinical College of Southwest Medical University, Luzhou, China
High myopia (≥ − 6.00 D) poses significant challenges to visual function and quality of life, with implantable collamer lens (ICL) V4c implantation emerging as a pivotal treatment. This mini review synthesizes evidence on visual-related quality of life (VRQoL) following ICL V4c implantation, focusing on predictability, objective/subjective visual quality, and complications. ICL V4c demonstrates long-term safety and efficacy, with safety indices (postoperative best-corrected visual acuity/preoperative best-corrected visual acuity) of 1.01–1.10 and efficacy indices (postoperative uncorrected visual acuity/preoperative best-corrected visual acuity) exceeding 0.90 over 5 years. Objective metrics, including higher-order aberrations and intraocular scattering, remain stable or improve postoperatively, while subjective outcomes show high patient satisfaction despite common but mild issues like halos (90.1% incidence) and glare (66.7% incidence). Complications such as cataract (1.7–6.8% incidence), corneal endothelial cell loss (≤5.7% over 8 years), and ICL malposition are rare and often manageable. While axial length progression in super-high myopia requires monitoring, ICL V4c remains a robust option for enhancing VRQoL in high myopia patients. Future research should prioritize large-scale, long-term studies to validate outcomes and optimize surgical protocols.
1 Introduction
Myopia, particularly high myopia (≥ − 6.00 D), poses significant challenges to visual function and quality of life, with global prevalence projected to affect 50% of the population by 2050 (1, 2). Myopia correction strategies primarily include corneal refractive surgery and intraocular refractive surgery. Intraocular approaches often involve lens-based interventions in the anterior chamber, with options including lens replacement and implantation (3). Direct lens replacement carries a higher risk of retinal detachment, limiting its clinical application. Corneal refractive surgeries, such as femtosecond laser small incision lenticule extraction (SMILE), are widely used for myopia correction, offering high safety, predictability, and stability. However, they are insufficient for treating high myopia and may cause postoperative complications like astigmatism and glare (4, 5).
The ICL V4c, an advanced posterior chamber phakic intraocular lens, features a 0.36-mm central aperture and bilateral openings, enhancing aqueous humor dynamics and reducing intraocular pressure fluctuations (6). This design minimizes optical quality impairment and cataract risk; for example, Lin et al. (7) reported no cataract formation in a 6-month follow-up of ICL V4c recipients. Constructed from biocompatible collamer material, the ICL V4c reduces complications such as anterior subcapsular cataracts and secondary glaucoma, with minimally invasive techniques further enhancing safety and tolerability.
Compared to traditional ICLs, the V4c model demonstrates superior clinical outcomes but is not without limitations. Chen et al. (8) reported postoperative glare in some patients, attributed to the lens design and surgical handling. Preoperative hydration of the lens surface is critical to maintain optical integrity during implantation, given the lens’s transparent, flexible, and compact nature, which requires meticulous handling to avoid contamination. The newer V5 model addresses these issues through preloaded implantation and an expanded optical zone, reducing glare and improving surgical efficiency (9).
In vitro studies by Pérez-Vives et al. (10) confirmed optimal optical quality with ICL V4c, while Chaitanya et al.’s (11) retrospective analysis of 67 myopic astigmatism patients (109 eyes) demonstrated significant refractive improvement: mean spherical equivalent reduced from −10.90 ± 3.7 D to −0.02 ± 0.13 D, and cylinder from −2.3 ± 1.3 D to −0.04 ± 0.2 D. Notably, 62% of eyes maintained stable best-corrected visual acuity, with only 1.8% requiring reoperation due to high vault complications.
With the proliferation of electronic devices, myopia prevalence and progression have become global public health concerns. The sixth-generation ICL V4c, a posterior chamber phakic intraocular lens with a central aperture, has emerged as a pivotal treatment for high myopia. Concurrently, the medical community’s focus has shifted toward postoperative quality of life. Visual-related quality of life (VRQoL), integrating objective metrics (e.g., higher-order aberrations, intraocular scattering) and subjective outcomes (e.g., uncorrected visual acuity), provides a comprehensive assessment of ICL V4c efficacy and safety. By bridging sociological, psychological, and clinical perspectives, VRQoL evaluations offer holistic insights into patient outcomes, guiding personalized interventions to enhance post-implantation quality of life. This review synthesizes current evidence on VRQoL after ICL V4c implantation in high myopia patients, aiming to inform clinical practice and future research.
2 Visual-related quality of life after ICL V4c implantation
In recent years, ICL V4c implantation has demonstrated prominent clinical advantages in correcting high myopia, featuring excellent efficacy, stability, and predictability, with minimal impact on postoperative VRQoL. VRQoL, a critical metric for evaluating refractive correction outcomes, is assessed through two dimensions: objective visual quality (wavefront aberrations, intraocular scattering) and subjective visual quality (uncorrected visual acuity).
2.1 Predictability and stability of ICL V4c implantation
Multiple studies confirm the long-term safety and efficacy of ICL V4c implantation, with safety indices (postoperative BCVA/preoperative BCVA) ranging from 1.01–1.10 and efficacy indices (postoperative UCVA/preoperative BCVA) exceeding 0.90 over extended follow-ups (12–14). The procedure maintains effectiveness in subgroups such as patients over 40 years old and those with shallow anterior chambers. Morkos et al. (15) further validated its utility in unilateral high myopia with anisometropic amblyopia, demonstrating stable visual acuity and refraction without long-term complications, thus positioning ICL V4c as a low-risk option that may help reduce the risk of amblyopia in selected pediatric cases.
The superior postoperative BCVA in most patients—equal to or better than preoperative values—may stem from the ICL V4c’s placement in the ciliary sulcus of the posterior chamber, which aligns with physiological optics, reduces the optical path to the retina, and enhances retinal magnification and image quality (16). However, myopic drift and axial length (AL) elongation are key factors affecting long-term efficacy. AL growth leads to myopia progression and UCVA decline, particularly in super-high myopia (≤−10.00 D), consistent with findings by Lee et al. and others (17, 18). Wang et al. observed that while efficacy indices remained above 1.00 at most time points, the 5-year index fell below 1.00, likely due to progressive myopia; higher preoperative myopia degrees correlate with greater progression risk. Chen et al. confirmed that myopia progression correlates with AL elongation rather than ICL type, underscoring V4c stability. Notable limitations include small sample sizes and short follow-up periods, necessitating longer-term data to validate durability.
2.2 Objective visual quality
2.2.1 Wavefront aberrations
Objective visual quality encompasses wavefront aberrations and intraocular scattering. Wavefront aberrometry separates low-order aberrations (myopia, hyperopia, astigmatism) from high-order aberrations (HOAs; e.g., coma, spherical aberration, trefoil). Correcting low-order aberrations often induces new HOAs, which degrade VRQoL, making HOA assessment critical for refractive surgeries (19). High myopia, associated with AL elongation and corneal curvature changes, exacerbates optical issues (20). Clinically, ICL V4c reduces HOAs more effectively than excimer laser in situ keratomileusis (LASIK) (21), likely due to minimal corneal disruption, preservation of native corneal properties, and induction of negative spherical aberration. Comparisons between ICL V4 and V4c show no significant HOA differences at 3 months (22), while He et al. (23) noted similar HOA profiles and glare/halo severity between the two models. Collectively, these findings confirm superior HOA management with ICL V4c, enhancing objective visual quality.
2.2.2 Intraocular scattering
Intraocular scattering, comprising forward and backward components, degrades VRQoL by reducing contrast through light veil formation on the retina, leading to halos, glare, reduced night vision, and contrast sensitivity (24). The Objective Scattering Index (OSI) correlates positively with scattering severity. Theoretically, ICL implantation—particularly the central hole—might increase scattering by complicating light paths, while lens rotation or residual astigmatism in toric ICL (TICL) patients could exacerbate this. Clinically, however, the stable positioning of ICL V4c in the ciliary sulcus minimizes tilt/shift, and its thin, hydrophilic collamer edges promote gradual refractive index transitions with aqueous humor, reducing scattering (25). He et al. (23) found no significant OSI changes post-ICL V4c, indicating neutral impact on intraocular scattering and preserving optical performance comparable to healthy eyes.
We have summarized the common objective visual quality indicators after ICL V4c implantation, see Table 1.
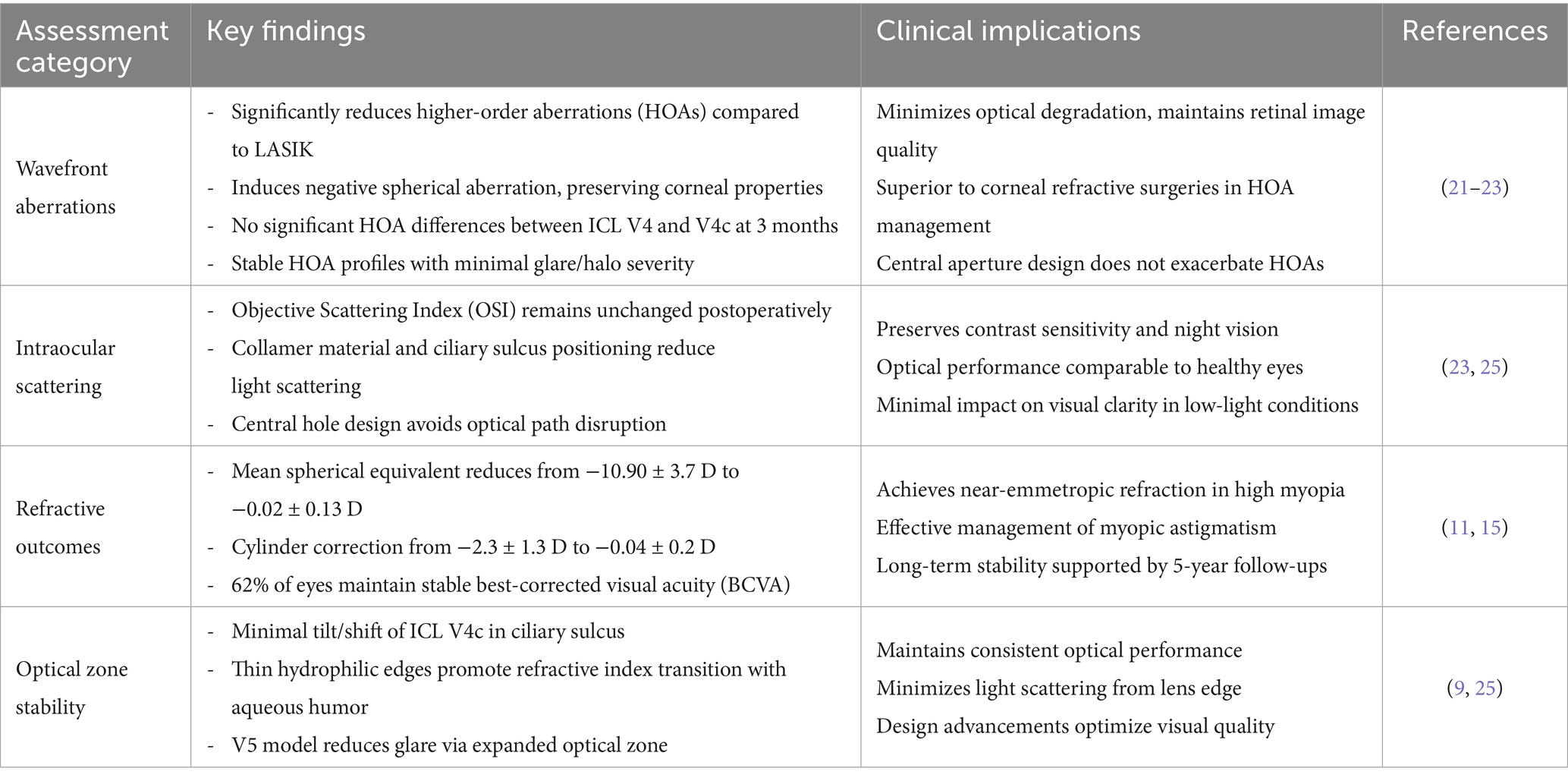
Table 1. Objective visual quality metrics after ICL V4c implantation for high myopia.
2.3 Subjective visual quality
2.3.1 Visual acuity and contrast sensitivity
Uncorrected visual acuity (UCVA) improves significantly after ICL V4c implantation, with 5-year outcomes surpassing preoperative BCVA in most cases. Younger patients (<21 years) exhibit better contrast sensitivity, likely due to healthier refractive systems and fewer retinal pathologies (26). Long-term follow-up (8 years) by Kamiya et al. (27) showed 83 and 93% of eyes achieved refraction within ±0.5 D and ±1.0 D of target values, respectively, affirming durable visual stability.
2.3.2 Visual quality questionnaires
Subjective outcomes are evaluated via validated tools like the Visual Function Questionnaire. Mohr et al. (28) reported that 90.1% of patients experienced halos, 66.7% glare, 60.0% visual fluctuations, 47.2% focusing difficulties, and 43.2% starbursts post-ICL V4c; while halos were most common, they caused only mild visual disturbance, with older patients more susceptible. This high incidence of halos may be attributed to the central aperture design of ICL V4c, which can alter light refraction patterns, especially in low-light conditions. Variations in such symptoms across studies may stem from differences in patient demographics (e.g., age-related lens transparency), surgical techniques (e.g., lens centration accuracy), and follow-up durations (e.g., symptom resolution over time). For instance, younger patients with healthier crystalline lenses might exhibit less severe scattering-related symptoms compared to older cohorts. Chen et al. (29) noted low glare severity despite high night-time glare scores, emphasizing the need to address poor night vision—a mechanism yet to be clarified. Patient satisfaction remains high: 5 years postoperatively, most reported improved self-image and confidence, with 50% attributing career advancements to ICL V4c. All patients cited enhanced daily convenience, particularly those with super-high myopia. Table 2 shows the Visual Quality Questionnaires for ICL V4c Implantation.
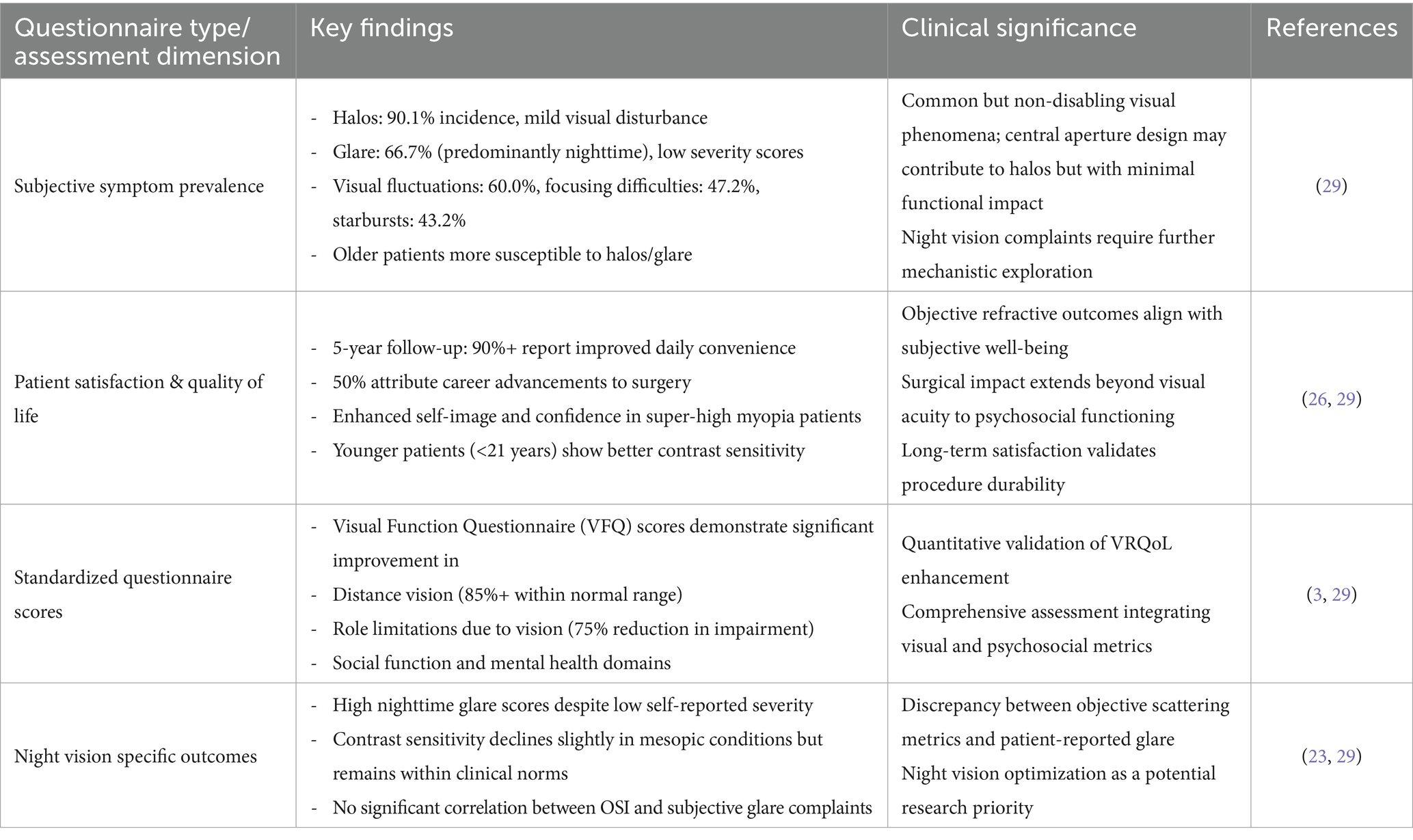
Table 2. Visual quality questionnaires after ICL V4c implantation.
2.4 Complications
Complications, including cataract, corneal endothelial cell loss, ICL V4c malposition, elevated intraocular pressure, and retinal detachment, are significant determinants of postoperative quality of life.
2.4.1 Cataract
Cataract is a common complication following ICL V4c implantation, with risk factors including preoperative myopia > − 12.0 D, age >40 years, low vault, and increased preoperative lens thickness/density. Igarashi et al. (30) reported anterior subcapsular opacification (ASO) in 8 eyes (6.8%) after ICL V4c implantation, with 7 eyes (5.9%) developing ASO immediately postoperatively, likely due to contact between the lens anterior surface and ICL V4c during irrigation/aspiration. Long-term studies show that after 5 years, 2 eyes (2.11%) experienced BCVA loss of ≥2 lines due to peripheral ASO, and 1 eye (1.05%) due to central ASO. Compared to ICL V4, ICL V4c causes less lens impact and milder opacification, suggesting the central hole may nourish the lens, though it does not prevent ASO. The primary risk factor for ASO remains lens-ICL contact. An 8-year follow-up revealed cataract formation in 3 eyes (1.7%), with preserved visual acuity even in patients with preexisting mild peripheral ASO, confirming ICL V4c’s safety for high myopia.
2.4.2 Corneal endothelial cell loss
Corneal endothelial damage after ICL V4c implantation may arise from direct contact with the corneal endothelium or postoperative inflammation, though corneal remodeling is also a proposed mechanism. Yang et al. (31) found high vault increases endothelial cell loss risk. Reported endothelial cell loss rates vary across studies: 1.6% ± 8.1% at 2.2 years, 2.68–3.87% at 5 years, 5.7% beyond 5 years, 2.60% at 7 years, and 3.6% ± 7.0% at 8 years, all within physiological loss rates. Even in patients with high vault (>1,000 μm), endothelial cell loss at 5 years was only 0.85%, demonstrating minimal long-term impact on corneal endothelium.
2.4.3 ICL V4c position abnormalities
Postoperative ICL V4c positional issues include vault abnormalities, dislocation, rotation, and flipping, with vault decreasing over time. Li et al. (32) observed mean vault decreasing from 540.83 ± 186.13 μm at 1 month to 471.42 ± 211.35 μm at 2 years, with greater reduction in eyes with shallow preoperative anterior chamber depth (ACD) or high refractive error. High vault can be managed by ICL rotation; Fernández-Vega-Cueto et al. (33) and Wei et al. (34) showed vertical rotation reduces vault without requiring lens exchange. Notably, subcapsular opacification occurred in some normal-vault eyes, while low-vault eyes showed no opacification, indicating no linear correlation between vault and cataract risk. Standardization of safe vault thresholds requires further research.
2.4.4 Elevated intraocular pressure (IOP) and glaucoma
Igarashi et al. (30) found no significant IOP elevation in 2.2-year follow-ups. Long-term studies (≥5 years) reported no pigmentary glaucoma, pupillary block, or vision-threatening complications. A 7-year study showed no IOP increase >20 mmHg or ≥5 mmHg from baseline, while Guber et al. (35) noted 13% incidence of elevated IOP over 7.3 years. The central hole design effectively prevents IOP elevation related to pupillary block or pigment dispersion.
2.4.5 Retinal detachment
High myopia itself increases risk of rhegmatogenous retinal detachment (RRD) due to early vitreous liquefaction, posterior vitreous detachment, and lattice degeneration. Xu et al. (36) did not find increased RRD risk after ICL V4c implantation, though higher early RRD incidence within 1 year may relate to intraoperative disruption of ocular stability, IOP fluctuations, or surgical inexperience. Long-term data confirm ICL V4c safety for high myopia correction.
3 Conclusion
In conclusion, ICL V4c implantation represents a safe, effective, and stable option for correcting high myopia, with robust evidence supporting its long-term efficacy and favorable VRQoL. The procedure demonstrates predictable refractive outcomes, minimal impact on objective optical parameters like higher-order aberrations and intraocular scattering, and high subjective patient satisfaction, despite common but generally mild complaints such as halos and glare. While complications such as cataract, corneal endothelial cell loss, and ICL malposition exist, their incidence remains low and often within physiological or manageable ranges, particularly with advancements in surgical technique and lens design (e.g., central aperture, expanded optical zone in V5 models). Key challenges include monitoring axial length progression in super-high myopia to mitigate refractive regression and addressing rare but significant complications like retinal detachment. Future research should prioritize large-scale, long-term studies to validate durability across diverse populations and further optimize surgical protocols, ensuring ICL V4c remains a leading choice for enhancing visual function and quality of life in high myopia patients.
Author contributions
HZ: Writing – original draft, Writing – review & editing. SZ: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sankaridurg, P, Tahhan, N, Kandel, H, Naduvilath, T, Zou, H, Frick, KD, et al. IMI impact of myopia. Invest Ophthalmol Vis Sci. (2021) 62:2. doi: 10.1167/iovs.62.5.2
2. George, AS, George, ASH, and Shahul, A. The myopia epidemic: a growing public health crisis impacting children worldwide. Partn Univers Int Res J. (2023) 2:120–38.
3. Jonker, SMR, Berendschot, TTJM, Saelens, IEY, Bauer, NJC, and Nuijts, RMMA. Phakic intraocular lenses: an overview. Indian J Ophthalmol. (2020) 68:2779–96. doi: 10.4103/ijo.IJO_2995_20
4. Zhang, H, Deng, Y, Li, Z, and Tang, J. Update of research progress on small incision lenticule extraction (SMILE) lenticule reuse. Clin Ophthalmol. (2023) 17:1423–31. doi: 10.2147/OPTH.S409014
5. Huang, G, and Melki, S: Small incision Lenticule extraction (SMILE): Myths and realities. Abingdon, United Kingdom: Taylor & Francis. (2021) 140–148.
6. Packer, M. The implantable Collamer Lens with a central port: review of the literature. Clin Ophthalmol. (2018) 12:2427–38. doi: 10.2147/OPTH.S188785
7. Lin, Q, Yang, D, and Zhou, X. Early outcomes of anterior segment parameters after implantable collamer lens V4c implantation. BMC Ophthalmol. (2022) 22:429. doi: 10.1186/s12886-022-02656-9
8. Chen, L, Sun, L, Tang, Y, Sui, W, Bian, A, Zhang, X, et al. Visual performance, safety, and patient satisfaction after binocular clear lens extraction and trifocal intraocular lens implantation in Chinese presbyopic patients. BMC Ophthalmol. (2024) 24:305. doi: 10.1186/s12886-024-03573-9
9. Thompson, V, Cummings, AB, and Wang, X. Implantable collamer lens procedure planning: a review of global approaches. Clin Ophthalmol. (2024) 15:1033–43.
10. Pérez-Vives, C, Ferrer-Blasco, T, Madrid-Costa, D, García-Lázaro, S, and Montés-Micó, R. Optical quality comparison of conventional and hole-visian implantable collamer lens at different degrees of decentering. Am J Ophthalmol. (2013) 156:69–76.e1. doi: 10.1016/j.ajo.2013.01.030
11. Chaitanya, SR, Anitha, V, Ravindran, M, Ghorpade, A, Rengappa, R, and Uduman, MS. Safety and efficacy of toric implantable collamer lens V4c model–a retrospective south Indian study. Indian J Ophthalmol. (2020) 68:3006–11. doi: 10.4103/ijo.IJO_1492_20
12. Chen, X, Li, L, Rao, J, Chen, Y-X, Gao, Y, Huang, R-X, et al. Long-term observation on safety and visual quality of implantable collamer lens V4c implantation for myopia correction: a 5-year follow-up. Int J Ophthalmol. (2023) 16:1123–9. doi: 10.18240/ijo.2023.07.18
13. Dong, J, Liu, Q, and Qin, B. One-year evaluation of rotational stability and visual outcomes following horizontal, vertical, and oblique implantation of ICL V4c. BMC Ophthalmol. (2025) 25:200. doi: 10.1186/s12886-025-03995-z
14. Wan, Q, Chen, L, He, P, Wei, R, Ma, K, Yin, H, et al. Deng Y-p: five years comparation of efficacy and safety after ICL-V4c implantation for high and super high myopia correction. Ann Med. (2025) 57:2448282. doi: 10.1080/07853890.2024.2448282
15. Morkos, FF, Fawzy, NF, El Bahrawy, M, Fathy, N, and Elkitkat, RS. Evaluation of the efficacy, safety, and stability of posterior chamber phakic intraocular lenses for correcting intractable myopic anisometropic amblyopia in a pediatric cohort. BMC Ophthalmol. (2021) 21:311. doi: 10.1186/s12886-021-02074-3
16. Wei, Q, Zhou, X, Chang, W, Jiang, R, Zhou, X, and Yu, Z. Retinal and choroidal changes following implantable Collamer Lens V4c implantation in high myopia patients—a 1-year follow-up study. Diagnostics. (2023) 13:3097.
17. Lee, JTL, Guo, X, Li, Z, Jong, M, Sankaridurg, P, and He, M. Progression and longitudinal biometric changes in highly myopic eyes. Invest Ophthalmol Vis Sci. (2020) 61:34. doi: 10.1167/iovs.61.4.34
18. Jiang, F, Wang, D, Yin, Q, He, M, and Li, Z. Longitudinal changes in axial length and spherical equivalent in children and adolescents with high myopia. Invest Ophthalmol Vis Sci. (2023) 64:6. doi: 10.1167/iovs.64.12.6
19. Zeng, J, Lan, G, Zhu, M, Sun, K, Shi, Q, Ma, G, et al. Factors associated with corneal high-order aberrations before and after femtosecond laser-assisted in situ keratomileusis. Ann Transl Med. (2021) 9:989. doi: 10.21037/atm-21-2367
20. Fan, Y, Huang, Y, and Huang, X. Association between axial length to corneal curvature radius ratio and myopia in adult patients. J Ophthalmol. (2024) 2024:4981095.
21. Chen, D, Zhao, X, Chou, Y, and Luo, Y. Comparison of visual outcomes and optical quality of femtosecond laser–assisted SMILE and visian implantable collamer lens (ICL V4c) implantation for moderate to high myopia: a meta-analysis. J Refract Surg. (2022) 38:332–8. doi: 10.3928/1081597X-20220411-01
22. Yang, Y. Analysis of stability and high order aberration of implantable collamer lens with a central hole (ICL V4c) for moderate and high myopia. Int. Eye Sci. (2019) 2019:644–8.
23. He, T, Zhu, Y, and Zhou, J. Optical quality after posterior chamber Phakic implantation of an intraocular lens with a central hole (V4c implantable Collamer lens) under different lighting conditions. BMC Ophthalmol. (2020) 20:1–6.
24. Zhang, J, Shao, J, Zheng, L, Zhao, X, and Sun, Y. Changes in ocular parameters of the crystalline lens after implantation of a collamer lens. Clin Exp Optom. (2022) 105:587–92. doi: 10.1080/08164622.2021.1958654
25. Ying, X, Li, Y, and Zhang, F. Predictive factors for postoperative visual acuity improvement with ICL-V4c for ultrahigh myopia above− 10 D. Graefes Arch Clin Exp Ophthalmol. (2022) 260:3107–14. doi: 10.1007/s00417-022-05626-5
26. Cakir, I, Sonmez, O, Pehlivanoglu, S, Cakir, GY, Yildiz, BK, Yildirim, Y, et al. Long-term results of a new posterior chamber phakic intraocular lens in patients with high myopia: 5-year results. J Cataract Refract Surg. (2023) 49:409–15. doi: 10.1097/j.jcrs.0000000000001110
27. Kamiya, K, Shimizu, K, Takahashi, M, Ando, W, Hayakawa, H, and Shoji, N. Eight-year outcomes of implantation of posterior chamber phakic intraocular lens with a central port for moderate to high ametropia. Front Med. (2021) 8:799078. doi: 10.3389/fmed.2021.799078
28. Mohr, N, Dirisamer, M, Siedlecki, J, Mayer, WJ, Schworm, B, Harrant, L, et al. Determinants of subjective quality of vision after phakic intraocular lens implantation. J Refract Surg. (2022) 38:280–7. doi: 10.3928/1081597X-20220405-01
29. Chen, X, Wang, X, Xu, Y, Cheng, M, Han, T, Niu, L, et al. Five-year outcomes of EVO implantable collamer lens implantation for the correction of high myopia and super high myopia. Eye and Vision. (2021) 8:1–8. doi: 10.1186/s40662-021-00264-0
30. Igarashi, A, Kamiya, K, Ichikawa, K, Kitazawa, Y, Kojima, T, Nakamura, T, et al. Multicenter clinical outcomes of hole implantable collamer lens implantation in middle-aged patients. Sci Rep. (2022) 12:4236. doi: 10.1038/s41598-022-08298-7
31. Yang, W, Zhao, J, Sun, L, Zhao, J, Niu, L, Wang, X, et al. Four-year observation of the changes in corneal endothelium cell density and correlated factors after implantable Collamer Lens V4c implantation. Br J Ophthalmol. (2021) 105:625–30. doi: 10.1136/bjophthalmol-2020-316144
32. Li, B, Chen, X, Cheng, M, Lei, Y, Jiang, Y, Xu, Y, et al. Long-term vault changes in different levels and factors affecting vault change after implantation of implantable Collamer Lens with a central hole. Ophthalmol Therapy. (2023) 12:251–61. doi: 10.1007/s40123-022-00606-8
33. Fernández-Vega-Cueto, L, Alfonso-Bartolozzi, B, Lisa, C, Madrid-Costa, D, and Alfonso, JF. Seven-year follow-up of posterior chamber phakic intraocular lens with central port design. Eye and Vision. (2021) 8:1–9.
34. Wei, R, Li, M, Aruma, A, Knorz, MC, Yang, D, Yu, Y, et al. Factors leading to realignment or exchange after implantable collamer lens implantation in 10 258 eyes. J Cataract Refract Surg. (2022) 48:1190–6. doi: 10.1097/j.jcrs.0000000000000950
35. Guber, I, Mouvet, V, Bergin, C, Perritaz, S, Othenin-Girard, P, and Majo, F. Clinical outcomes and cataract formation rates in eyes 10 years after posterior Phakic Lens implantation for myopia. JAMA Ophthalmol. (2016) 134:487–94. doi: 10.1001/jamaophthalmol.2016.0078
Keywords: high myopia, ICL V4c, visual-related quality of life, objective visual quality, subjective visual quality, complications
Citation: Zhao H and Zhu S (2025) Visual related quality of life after ICL V4c implantation in high myopia patients: a mini review. Front. Med. 12:1630025. doi: 10.3389/fmed.2025.1630025
Edited by:
Sebastião Cronemberger, Federal University of Minas Gerais, BrazilReviewed by:
Trakanta Wannapanich, Chulalongkorn University, ThailandCopyright © 2025 Zhao and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Siquan Zhu, cXVhbnNpemh1aGNqaEB5ZWFoLm5ldA==