 Margalida Cardona1†
Margalida Cardona1† Pilar Andrés1,2,3*†
Pilar Andrés1,2,3*†- 1Neuropsychology and Cognition Research Group, Department of Psychology, University of the Balearic Islands, Palma de Mallorca, Spain
- 2Research Institute (IdISBa), Palma de Mallorca, Spain
- 3Research Institute on Health Sciences (IUNICS), Palma de Mallorca, Spain
Objective: Social isolation and loneliness are associated with poor health (immunity, inflammation, etc.) in ageing. The purpose of this scoping review was to investigate the link between social isolation, loneliness (as distinct constructs, in contrast to previous published work) and cognition in cognitively healthy older adults.
Method: We followed PRISMA-ScR guidelines. Our search, conducted between January 2017 and April 2021, yielded 2,673 articles, of which, twelve longitudinal studies were finally identified as meeting the inclusion criteria. Multiple cognitive functions (short-term and episodic memory, attention, and global cognitive functioning) were measured.
Results: The results showed that both social isolation and loneliness were associated with poor cognition in ageing, with depression as a possible mediator between loneliness and poor cognition. Some studies also suggested that the link between social isolation, loneliness and cognitive decline may be bidirectional.
Conclusion: We conclude that both social isolation and loneliness may have a different impact on cognition. While depression may be an important mediator between loneliness and cognitive decline, the lack of cognitive stimulation may be a greater mediator between social isolation and cognitive health.
Introduction
Attachment theory suggests that human beings are born with a psychobiological system that motivates them to seek proximity to significant others in times of need (Bowlby, 1969, 1982). According to Bowlby, the goal of this attachment behavioral system, is to maintain adequate protection and support, which is accompanied by a sense of safety and security.
The health, life and genetic legacy of members of social species are threatened when they find themselves isolated (see Cacioppo and Hawkley, 2009 for a review). During the COVID-19 lockdown, for example, we experienced social isolation, and many people suffered the consequences of loneliness. During the pandemic, the dangers of the virus were prioritized. However, social isolation and loneliness can result in both short- and long-term health effects that cannot be ignored. Holt-Lunstad et al. (2015; see Leigh-Hunt et al., 2017 for a review), for instance, showed the association of social isolation and loneliness with a significantly increased risk of death from all causes. Likewise, being disconnected posed comparable danger to smoking 15 cigarettes a day, and was more predictive of early death than the effects of air pollution or physical inactivity. Holt-Lunstad et al. (2010) also showed that people who had strong social relationships had a 50% increased likelihood of survival than those with weaker ties. Similar effects have been observed using data from the Framingham Heart Study (Fowler and Christakis, 2008; Christakis and Fowler, 2009), whereby chances of becoming happy, depressed, or obese were mirrored by similar changes in the closest friend. When friends where considered, each person was asked to name one friend, and not all of these nominations were reciprocated. Results showed that the contagion phenomenon was especially strong if the friendship was mutual (both friends nominated each other as friend) (Fowler and Christakis, 2008).
The topic of social isolation and loneliness is considered so important that, prior to the pandemic, the UK appointed a Loneliness minister and published a national strategy for tackling loneliness in 2018 and the World Health Organization declared that loneliness is a major health concern worldwide.
In a recent review, Bzdok and Dunbar (2020) summarize the evidence showing that loneliness impairs the immune system, thus reducing resistance to disease and infections. For instance, Pressman et al. (2005) found that freshmen students who reported feeling lonely had a reduced immune system response when they were given a flu vaccine compared to students who felt socially well engaged. Moreover, those students with only four to 12 close friends had significantly poorer responses than those with more friends. Thus, feeling lonely and having few friends results in a particularly poor immune defense. Sarkar et al. (2012) also found that social bonds stimulate the release of the body’s natural killer cells, one of the white blood cells of the innate immune system whose core function is to destroy harmful bacteria and viruses. Finally, Cole and collaborators have shown that loneliness is associated with higher pro-inflammatory gene expression (Cole et al., 2007), indicating an upregulation of inflammatory signaling that can be a precursor for higher systemic inflammation (Irwin and Cole, 2011; Ligthart et al., 2018) and worse health (Slavich and Cole, 2013). To conclude, the more immersed in a community—with social connections—the happier, and healthier, people are. Friends tend to act as our social support and are condition sine qua non for health quality.
A second recent systematic review by Lam et al. (2021) has also shown abnormal brain structure (gray and white matter) and/or activity in the prefrontal cortex, insula, amygdala, hippocampus, and posterior superior temporal cortex associated with loneliness. Loneliness was also related to biological markers associated with Alzheimer’s disease pathology in two cross-sectional studies using PET imaging that found a significant relationship between loneliness and higher amyloid burden and greater tau pathology in right entorhinal cortex and right fusiform gyrus, especially in APOEε4 carriers (Donovan et al., 2016; d’Oleire Uquillas et al., 2018).
Both social isolation and loneliness refer to human connection and may have a relationship with cognition, but they are not synonymous. As stated by Palmer (2019), the term “social isolation” reflects an objective reality, meaning a factual deficit in a person’s social bonds and support. On the other hand, loneliness refers to a subjective feeling of discrepancy between one’s wishes of social contacts and actual interactions.
Research on social isolation over the years has shown that both objective (social isolation) and subjective (loneliness) components must be examined when investigating their association with health and wellbeing. They are two separate constructs that have shown only modest correlations (r ∼ 0.25–0.28; Palmer, 2019; also see de Jong-Gierveld and Havens, 2004; Cornwell and Waite, 2009; Coyle and Dugan, 2012) and may have independent negative effects on older adults’ mental health (Steptoe et al., 2013; Shankar et al., 2015; Cheung et al., 2021). Also, individuals may experience loneliness without also suffering social isolation, or vice versa (Valtorta and Hanratty, 2012). This difference has been identified as social asymmetry by McHugh Power and collaborators (McHugh Power et al., 2017, 2020).
Older adults’ health and wellbeing may be specially threatened by social isolation (Victor et al., 2002; Sundström et al., 2009). For example, they experience the loss of close others through ill health and bereavement, dislocation from their relatives due to increased familial mobility and greater difficulties engaging in social activity after retirement. Also, there is evidence that attachment style becomes more avoidant with age (Webster, 1997; Magai et al., 2001), especially when compared with younger adults (Diehl et al., 1998). Knowing that cognitive functioning constitutes a major outcome of older adults’ health and wellbeing, the aim of the current review was to explore further this link between social isolation and loneliness and cognitive functioning in healthy older adults.
Previous reviews have, however, addressed this question considering only separately the link between cognition and aspects of social relationships (Kuiper et al., 2016; Kelly et al., 2017; Evans et al., 2019) and between cognition and loneliness (Cacioppo and Hawkley, 2009; Boss et al., 2015).
There is however no published work considering both constructs as separate possible causes of cognitive decline. It was therefore important to investigate within the same study the specific contributions of social isolation and loneliness to cognition in older adults. The aim of the present review was to examine for the first time, in recent longitudinal studies (last 5 years), the relationship between social isolation, loneliness, as different concepts, and cognitive changes in later life.
Methods
Search strategy
To do this, we followed Preferred Reporting Items Systematic Reviews and Meta-Analysis for scoping reviews (PRISMA-ScR) guidelines (Tricco et al., 2018), with the pursue of achieving an appropriate organization and integrity of the work.
The question we wanted to investigate was whether there is a link between social isolation, loneliness and cognitive decline among older people. In other words, do isolated and/or lonely older adults present higher rates of cognitive decline than people with rich/active social life/connections? If such relationship does exist, could it be bidirectional?
Inclusion criteria
To answer this question, the following inclusion criteria were established: studies (1) that examine the relationship between social isolation, loneliness and cognitive function, (2) using a longitudinal design, (3) including participants with a mean age ≥ 60, (4) with no diagnosis of cognitive impairment nor dementia, (5) reporting original data, (6) published in English in a peer-reviewed journal, (7) released between January 20171 and April 2021. Reviews or opinion papers were excluded.
Literature search strategy
Pubmed, Scopus, Web of Science (WOS), Medline and PsycInfo were the selected electronic databases through which the literature was searched. The search was conducted on April 2021, and it included the following terms: “social isolation,” “loneliness,” “ageing,” “older adult,” “elderly,” “cognition,” “cognitive function,” “cognitive processes,” “cognitive control,” “executive control,” “executive function,” in various combinations. For instance, in Scopus the following search was performed: (“social isolation”) AND (loneliness) AND (aging OR ageing OR “older adults” OR elderly) AND (cognition* OR “cognitive function*” OR “cognitive control” OR “cognitive processes*” OR “executive control” OR “executive function*”) AND (LIMIT-TO (PUBYEAR, 2021) OR LIMIT-TO (PUBYEAR, 2020) OR LIMIT-TO (PUBYEAR, 2019) OR LIMIT-TO (PUBYEAR, 2018) OR LIMIT-TO (PUBYEAR, 2017) AND (LIMIT-TO (LANGUAGE, “English”).
Data collection and study selection process
As shown in Figure 1, the initial search yielded 2,673 results, from which 2,262 articles were identified in Scopus, 216 in PubMed, 116 in WOS, 63 in Medline and 31 in PsycINFO. A systematic filtering process was then conducted by the two authors, and in case of uncertainty, the final decision on inclusion was made through discussion.
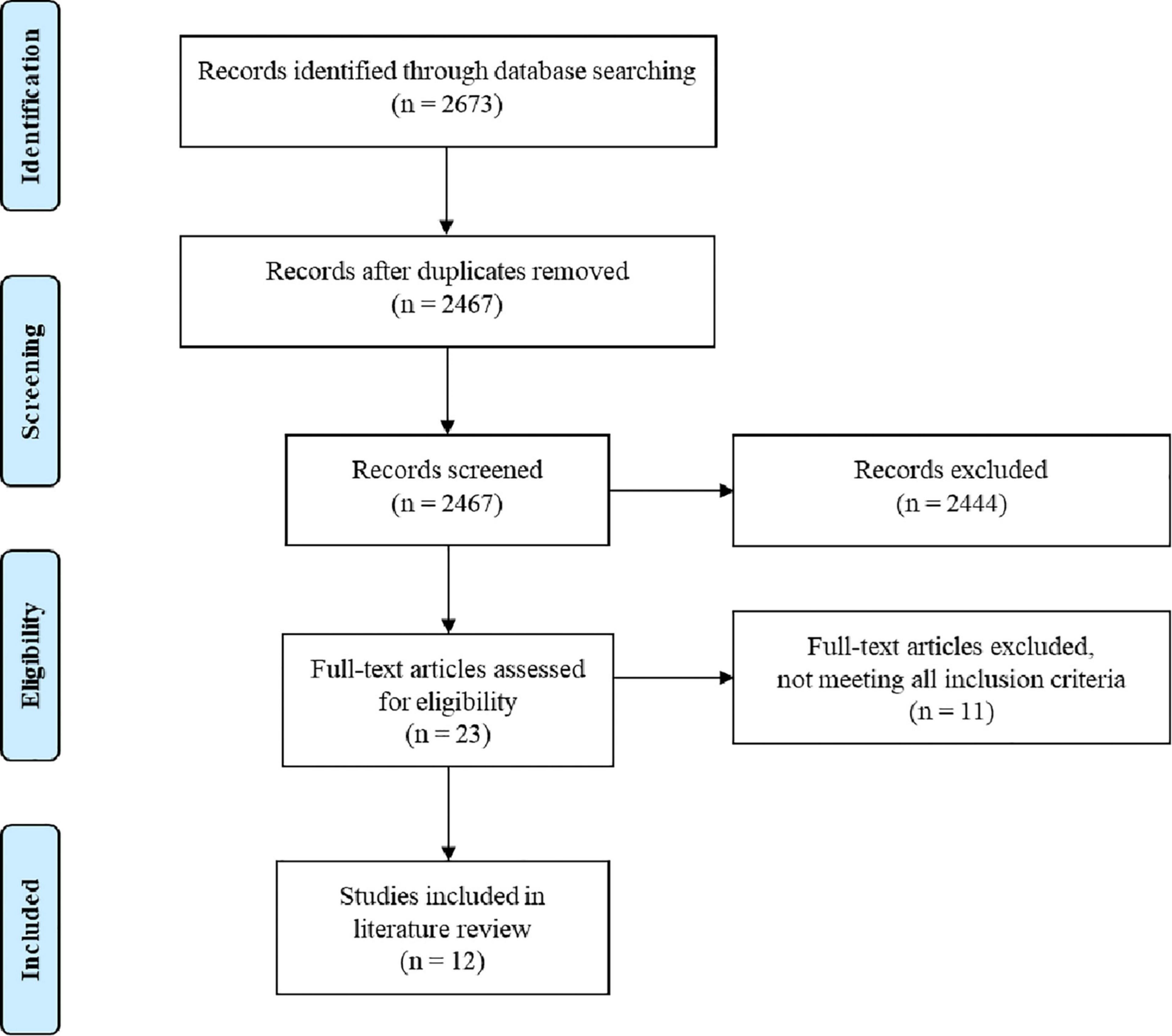
Figure 1. An overview of the study selection process.
First, 206 duplicates were removed. Titles and abstracts—and when in doubt also the methods—from the remaining 2,467 unique records were then screened, leaving 23 articles that were fully read and examined to determine eligibility for inclusion. Upon review, the final sample of this study is composed of 12 scientific publications (see Table 1). The 11 studies that were excluded for not fulfilling any of the criteria are listed in Table 2 along with the reason for exclusion.
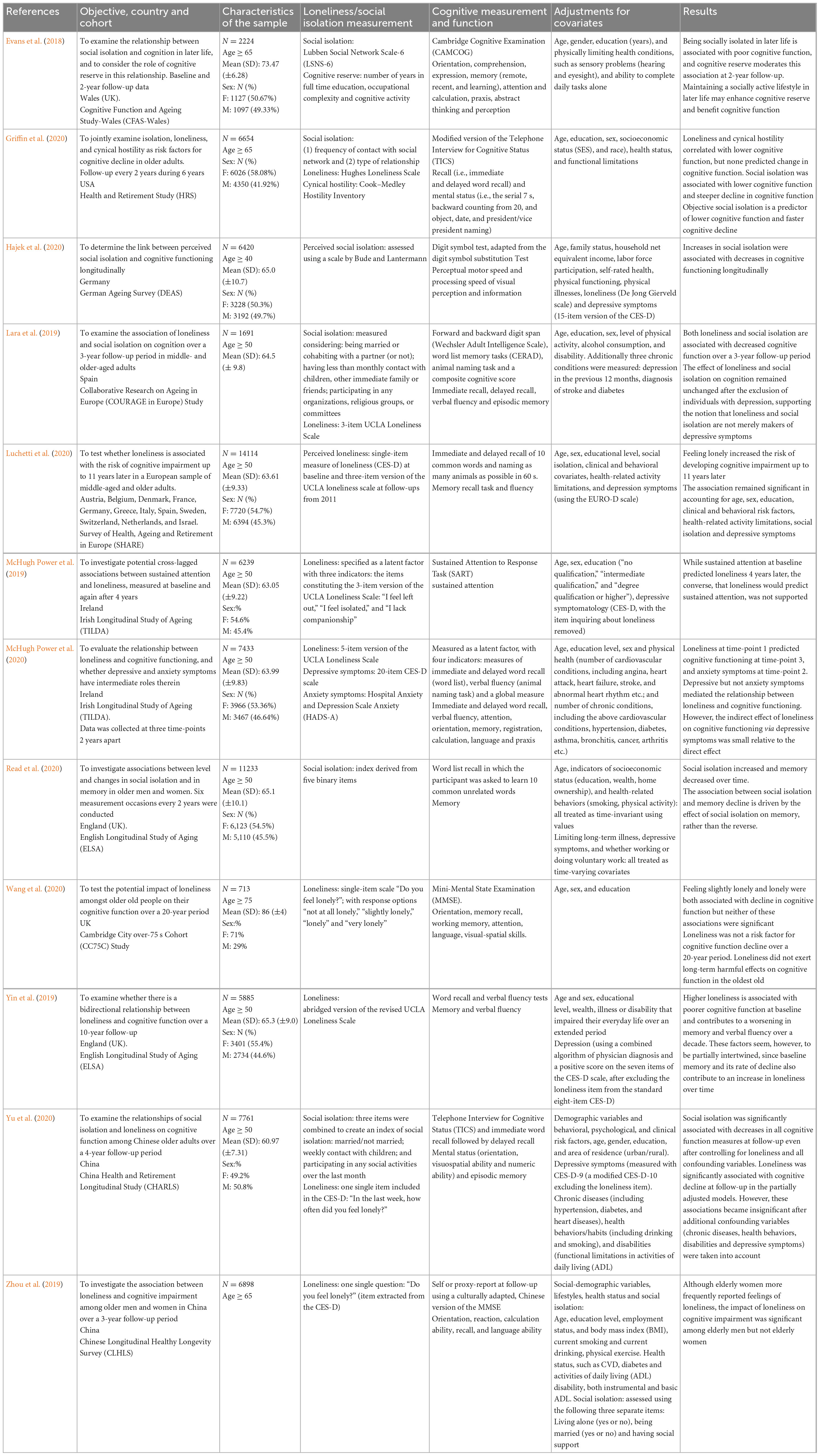
Table 1. Relationship between social isolation and/or loneliness and cognitive function in older adults.
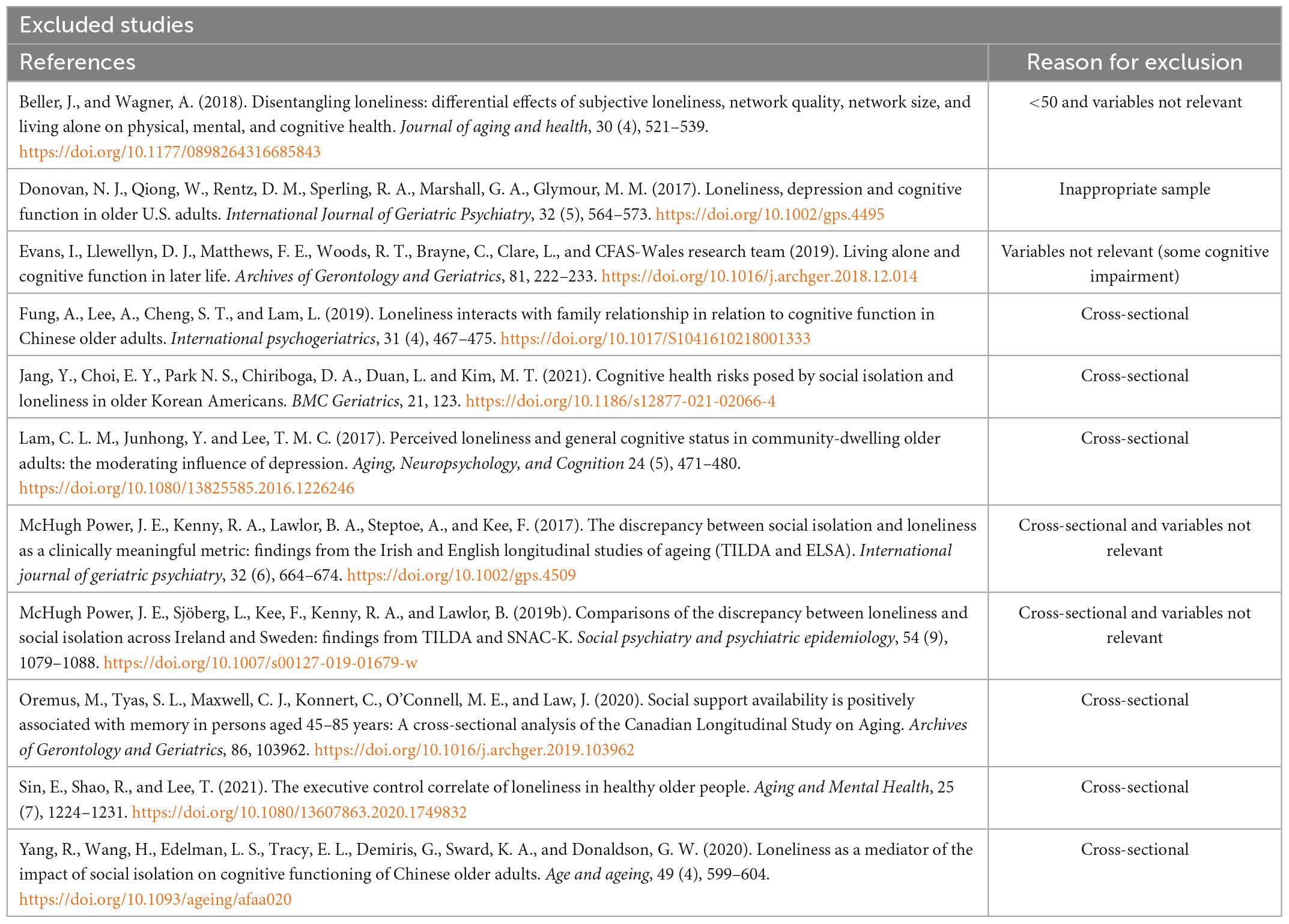
Table 2. Excluded studies with reason for exclusion.
Extracting and charting the data
The following information from each of the included studies was extracted (see Table 1): authors and year of publication, country and setting in which it was carried out, objective of the investigation, study design, characteristics of the sample, loneliness and/or social isolation measurement, cognitive domains measurement, covariates, and results obtained.
Results
Study characteristics
Design
Only longitudinal studies were included in this scoping review, as they represent the best way to investigate associations between risk factors and cognitive decline and try to establish directional relationships (e.g., Boss et al., 2015). Follow-up periods for all 12 longitudinal studies ranged from 3 (Zhou et al., 2019; Hajek et al., 2020) to 11 years (Luchetti et al., 2020). All studies reported findings from participants enrolled in large, population-based studies, being these the Survey of Health, Ageing and Retirement in Europe (SHARE; Luchetti et al., 2020), the English Longitudinal Study of Ageing (ELSA; Yin et al., 2019; Read et al., 2020), the Cognitive Function and Ageing Study-Wales (CFAS-Wales; Evans et al., 2018), the Cambridge City over-75s Cohort Study (CC75C; Wang et al., 2020), the Irish Longitudinal Study of Ageing (TILDA; McHugh Power et al., 2019, 2020), the Collaborative Research on Ageing in Europe study in Europe (COURAGE; Lara et al., 2019), the Health and Retirement Study (HRS; Griffin et al., 2020), the Chinese Longitudinal Healthy Longevity Survey (CLHLS; Zhou et al., 2019), the China Health and Retirement Longitudinal Study (CHARLS; Yu et al., 2020) and the German Ageing Survey (DEAS; Hajek et al., 2020).
Sample and location
Eight studies were conducted in Europe, including Germany (Hajek et al., 2020), Spain (Lara et al., 2019), Ireland (McHugh Power et al., 2019, 2020), and the UK (Evans et al., 2018; Yin et al., 2019; Read et al., 2020; Wang et al., 2020). Two studies were carried out in China (Zhou et al., 2019; Yu et al., 2020) and one in the USA (Griffin et al., 2020). Lastly, Luchetti et al.’s (2020) sample was formed using data from several countries—Austria, Belgium, Denmark, France, Germany, Greece, Italy, Spain, Sweden, Switzerland, Netherlands, and Israel.
In all studies samples included both genders, and the number of participants per study ranged from 713 (Wang et al., 2020) to 14,114 (Luchetti et al., 2020) for a total of 77,265 participants across all studies. All studies’ participants were independently living older adults. Most participants were described as generally healthy, although some suffered from chronic physical diseases such as hypertension, diabetes, cardiovascular conditions, arthritis as well as psychological disorders—such as depression and anxiety.
Measurement of loneliness
From the nine studies investigating loneliness, some utilized the UCLA loneliness scale (Russell, 1996; McHugh Power et al., 2020) or a three-item shortened version of it (the Hughes loneliness scale, Hughes et al., 2004; Lara et al., 2019; Griffin et al., 2020; Luchetti et al., 2020; second wave; McHugh Power et al., 2019; Yin et al., 2019). This Likert style questionnaire was designed to measure general feelings of dissatisfaction with one’s social interactions, and it includes questions such as “How often do you experience loneliness?” The other researchers used single questions. Zhou et al. (2019) and Wang et al. (2020) used yes/no format questions such as “do you feel lonely?.” Luchetti et al.’s (2020) single—item question was part of the abbreviated version of the Center for Epidemiological Studies Depression scale (CESD; Prince et al., 1999). Participants were asked: “How often have you experienced the following feelings over the last week: I felt lonely?.” Response options were: 1 = Almost all of the time; 2 = Most of the time; 3 = Some of the time; 4 = Almost none of the time. Yu et al. (2020) also used this single question from the CESD.
Measurement of social isolation
Six studies investigated social isolation. From these, Hajek et al. (2020) assessed perceived social isolation using the Bude and Lantermann’s (2006) scale, which includes 4 items. Each item ranges from 1 (strongly agree) to 4 (strongly disagree). Some other authors used indexes. For example, Lara et al. (2019) and Read et al. (2020) used an index based on the one proposed by Shankar et al. (2011), including 5 binary questions such as “did the responded live alone?,” with scores ranging from 0 to 5, and higher scores representing greater social isolation. Yu et al. (2020) combined three items to create an index of social isolation, adapted from previous research (Glei et al., 2012; Steptoe et al., 2013). One point was assigned, for example, if participants were not married or had less than weekly contact (by phone, in person, or by e-mail) with children. Scores of social isolation ranged from 0 to 3, with higher scores indicating greater isolation. Finally, Evans et al. (2018) used the Lubben Social Network scale-6 (LSNS-6, Lubben et al., 2006), a self-report standardized measure of social engagement including family and friends, constructed of three sets of questions. The three items assess the number of relatives/friends the participant sees or hears from at least once a month, could call on for help, and can speak with about private matters. Responses are collected using a six category response, in which the participant indicates the number of relatives/friends available. Response scores range from 0 (no relatives/friends) to 5 (nine or more relatives/friends). The overall scores for each six questions are summed and range from 0 to 30, with higher scores indicating lower social isolation. A score of ≤ 12 may be taken to indicate the presence of social isolation. Griffin et al. (2020) used a scale to measure frequency of three types of contact with social network (Smith et al., 2012, 2020). Participants had to rate how often they (a) met up (include both arranged and chance meetings), (b) spoke on the phone, (c) wrote to or emailed their children, other family members, and friends, respectively. Options included three or more times a week, once or twice a week, once or twice a month, every few months, once or twice a year, less than once a year, or never (Smith et al., 2013).
Measurement of cognitive function
Episodic memory was assessed in different studies via word recall (Lara et al., 2019; Luchetti et al., 2020; McHugh Power et al., 2020; Read et al., 2020; Yu et al., 2020). For example, Lara et al. (2019); Luchetti et al. (2020), and Read et al. (2020) used the 10-word list immediate and delayed verbal recall from the CERAD (Morris et al., 1989). In terms of attention, Hajek et al. (2020) used the digit symbol test adapted from the digit symbol substitution test (Wechsler, 1955). McHugh Power et al. (2019) used the Sustained Attention to Response Task (SART, Robertson et al., 1997), where a series of single digits between 1 and 9 are sequentially presented and participants are instructed to press a keyboard key as soon as possible (with response time noted) for each digit presented, except if the digit is 3. Lara et al. (2019) used the digit span from the Wechsler Adult Intelligence Scale (Wechsler, 1955). Verbal fluency was also assessed by Lara et al. (2019); Yin et al. (2019), Luchetti et al. (2020), and McHugh Power et al. (2020). Other studies assessed global cognitive function using the Mini Mental State Examination (MMSE, McHugh Power et al., 2020; Wang et al., 2020; Zhou et al., 2019). It is noteworthy that this test has been criticized and is being replaced by the Montréal Cognitive Assessment (MoCA) as it is more sensitive and specific to detect early cognitive impairment than the MMSE (Damian et al., 2011; Ciesielska et al., 2016; Pinto et al., 2019; Jia et al., 2021). Evans et al. (2018) used the Cambridge Cognitive Examination (CAMCOG), a standardized instrument used to measure orientation, language, memory, praxis, attention, abstract thinking, perception, and calculation (Roth et al., 1986). Finally, Griffin et al. (2020) used the Modified version of the telephone interview for cognitive status (TICS; de Jager et al., 2003), which includes questions of orientation, repetition, naming, and calculations.
Social isolation and cognition
Six studies from our sample examined the relationship between social isolation and cognitive functioning. Hajek et al. (2020), after examining a German sample of 6,420 people, concluded that increases in social isolation were associated with decreases in cognitive function, specifically perceptual motor speed and processing speed. Likewise, Read et al. (2020) revealed a link between social isolation and memory decline in 11,233 later-life adults in England, suggesting that the former seems to affect the latter, but not the reverse. The study by Evans et al. (2018) explored this relationship in 2,224 Welsh older adults, assessing multiple domains and showed that being socially isolated might lead to poor cognitive functioning. This research also analyzed the role that cognitive reserve could play in the relationship between social isolation and cognition in later life, showing that, although no link was found when explored cross-sectionally, at 2-year follow up, cognitive reserve seemed to moderate the association. Particularly, the association between social isolation and cognitive change was non-significant for those participants whose former main employment was considered complex (i.e., doctor or lawyer) and those whose social and economic class were higher.
Griffin et al. (2020) examined data about objective social isolation, loneliness and recall from 6654 US individuals during 6 years with follow-ups every 2 years. Concerning social isolation, their results suggest that it is a predictor of lower cognitive functioning and it accelerates cognitive decline. In the same way, after analyzing data from 7,761 Chinese adults over 50 years, Yu et al. (2020) concluded that social isolation was significantly linked to cognitive decline in all cognition measures (i.e., episodic memory, orientation and visuospatial and numeric ability) at follow-up, even after taking into account loneliness and other covariates such as chronic diseases or depression. Lara et al. (2019) evaluated 1,691 Spanish participants aged 50 or older to determine whether loneliness and/or social isolation were related to changes in cognition over a 3-year follow up period. They found that individuals with a higher isolation index tended to present lower scores in verbal fluency, forward digit span and in the composite cognitive score.
Loneliness and cognition
Nine studies from our sample investigated the association between loneliness and cognitive function. Some (Lara et al., 2019; McHugh Power et al., 2019; Luchetti et al., 2020) reported that loneliness might be a predictor of cognitive changes over time, while others (Griffin et al., 2020; Wang et al., 2020; Yu et al., 2020) did not. The study by Yin et al. (2019) suggests a bidirectional relationship between both domains and McHugh Power et al. (2019) found that attention may affect loneliness and not reversely. Finally, Zhou et al. (2019) concluded that the link between loneliness and cognitive decline over time was significant among men but not women.
Lara et al.’s (2019) study concluded that loneliness had a significant association with lower scores in immediate and delayed recall, verbal fluency, backward digit span and the composite cognitive score that evaluated overall cognition. The research by Luchetti et al. (2020) is the study with the largest sample (14,114 individuals assessed over 11 years) and culturally the most heterogeneous (comprising 12 European countries). It evaluated memory recall and verbal fluency, and the results suggest that feeling lonely increases the risk of suffering cognitive impairment regardless of all covariates controlled (i.e., social isolation, depressive symptoms).
Moreover, Yu et al. (2020) found that loneliness had a significant association with a decline in episodic memory, orientation and visuospatial and numeric ability before controlling for variables such as chronic diseases, health behaviors, disabilities, and depression. However, after controlling for them, this relationship became insignificant. In the same vein, Griffin et al. (2020) reported that, unlike social isolation, loneliness does not seem to predict changes in cognition longitudinally, although it correlated with lower cognitive function cross-sectionally. Wang et al.’s (2020) study is the only one whose sample is composed solely by individuals aged 75 or older evaluated over a 20-year period, reason why its sample (713) is the smallest. The results showed that loneliness did not seem to be a significant long-term harmful risk factor for cognitive decline among the older old.
Finally, Zhou et al. (2019) focused their efforts on analyzing whether the association between loneliness and cognitive function varied among 6,898 Chinese men and women 65 years and over. Notwithstanding older women reported feelings of loneliness more frequently, the repercussion of loneliness on cognitive decline over time was significant among older men but not women.
Is the relationship bidirectional?
A remaining question from previous reviews was whether the association between social isolation and cognition or between loneliness and cognition might be bidirectional. The fact that the reviewed studies in our scoping review were longitudinal may contribute to answer this question.
When analyzing the association between loneliness and cognitive function (memory and verbal fluency), Yin et al. (2019) observed that higher loneliness predicted poorer memory and verbal fluency at baseline and influenced such cognitive domains in a negative way after a 10-year follow up. Besides, worse baseline memory (but not verbal fluency) and its rate of decline over time seemed to contribute to an intensification of loneliness at follow-up. Additionally, higher baseline memory seemed to predict a slower change in loneliness, revealing a bidirectional relationship among loneliness and memory. In another study, McHugh Power et al. (2020) found that cognitive functioning at wave 1 predicted loneliness at wave 3 and loneliness at wave 1 predicted cognitive functioning at wave 3. Finally, McHugh Power et al. (2019) also hypothesized a bidirectional relationship between loneliness and sustained attention. Nevertheless, sustained attention at baseline predicted loneliness at 4-year follow-up, but reverse results, loneliness predicting sustained attention, were not found. This study is unique in that it is the only study in which solely cognitive function prognosticates loneliness longitudinally.
The role of depressive symptoms
Five out of the 12 reviewed studies considered the role of depression as a possible mediator between social isolation, loneliness and cognitive decline. In the study by Lara et al. (2019) depression in the previous 12 months was assessed with an adapted version of the CIDI 3.0 (Haro et al., 2006). Lara et al. (2019) concluded that the results were not affected by depression, as they remained unchanged after excluding individuals with depression. Similarly, Yin et al. (2019) reported that, albeit loneliness and depression measured using seven items of the CES-D (Radloff, 1977), seemed to be intimately linked, ultimately, they were independent and loneliness might be associated with memory decline over a decade by itself, despite of depressive symptoms.
Three studies showed however a significant link between loneliness and depression (McHugh Power et al., 2019, 2020; Yu et al., 2020). The first showed that higher levels of depressive symptomatology (measured using the validated and reliable 20-item CES-D scale, Radloff, 1977) predicted higher levels of loneliness and worse performance on sustained attention. McHugh Power et al. (2020) also observed that depressive (20-item CES-D scale), but not anxiety, symptoms mediated the relationship between loneliness and cognitive functioning. Finally, Yu et al. (2020) demonstrated that the association between loneliness (not social isolation) and cognitive decline became insignificant after depressive symptoms (measured with the 10-item CESD-10, Radloff, 1977) were taken into account.
Discussion
The aim of this scoping review was to investigate for the first time possible associations between social isolation, loneliness, as separate constructs, and cognitive function in cognitively healthy older adults. To do this, we reviewed longitudinal studies investigating social isolation, loneliness and multiple cognitive functions. Studies were carried out in three continents (Europe, Asia, and America) and included large samples with a total of 77,265 participants across studies.
Results from the selected studies revealed that social isolation, loneliness and cognition are related. The relationship between social isolation, understood as an objective manifestation of lack of social bonds and support, and cognition seems robust, with results congruently (6 out of 6 studies) showing that it is negatively associated with cognitive functions in older populations. Previous reviews assessing studies published before 2017 had shown some heterogeneity in the results, depending on variations in approaches to measuring social activity and social networks across studies (Kuiper et al., 2016; Kelly et al., 2017; Evans et al., 2019). Our scoping review on recent longitudinal studies however adds consistent evidence to the idea of a protective effect of social connection through life on cognitive functions.
The results of the recent studies looking at the effect of loneliness on cognitive function seem to be less consistent. Despite the common knowledge that “loneliness kills,” the relationship between loneliness, understood as the subjective feeling of discrepancy between one’s wishes of social contacts and actual interactions and cognition is only clearly shown in 4 out of 9 studies. While some studies identify loneliness as a predictor of cognitive function (Lara et al., 2019; Yin et al., 2019; Luchetti et al., 2020; McHugh Power et al., 2020), others do not (McHugh Power et al., 2019; Griffin et al., 2020; Wang et al., 2020; Yu et al., 2020) or show it only for men (Zhou et al., 2019). Moreover, this relationship may be, at least partially, mediated by depression (McHugh Power et al., 2019, 2020; Yu et al., 2020).
Measuring loneliness is not a simple issue. It was measured by the UCLA loneliness scale in one study (McHugh Power et al., 2020) and by a three-item shortened version of it in five studies (Lara et al., 2019; Griffin et al., 2020; Luchetti et al., 2020; second wave; McHugh Power et al., 2019; Yin et al., 2019). The other researchers used single questions (Zhou et al., 2019; Luchetti et al., 2020; Wang et al., 2020). As an example of how prevalent this approach is, from the 10 studies examining loneliness in the ageing population in Boss et al.’s (2015) meta-analysis, seven of those made use of single-item questions to measure loneliness while the remaining three used either the 3-item, short form of the Revised-UCLA Loneliness Scale (Shankar et al., 2013) or the six-item De Jong-Gierveld Loneliness Scale (Wilson et al., 2007; Schnittger et al., 2012). Also, recent research has shown that the subcomponents of loneliness scales were notably decoupled by the confinement during COVID, supporting the notion that loneliness is not a unitary, isolated construct but rather represents a cluster of different experiences of social integration and socioemotional states (Bartrés-Faz et al., 2021). It is then possible that to capture feelings of loneliness and detect associations with cognitive decline, a full scale should be used (as was the case only in the study by McHugh Power et al., 2020).
Cacioppo and Patrick (2008) define loneliness as a signal that one’s connections to others are weakening and to motivate the repair and maintenance of connections to others that are needed for our health, wellbeing and survival of our genes. This definition considers that loneliness evolved to improve survivability when socially isolated, through hypervigilance and increasing motivation to connect with others (also see Hawkley and Capitanio, 2015). Putting together the results from the current review and previous studies, the findings of depression as a mediator between loneliness and cognitive decline found in some studies (McHugh Power et al., 2019, 2020; Yu et al., 2020) would be compatible with this conception. Importantly, loneliness has been previously found to be closely associated with depressive symptoms (Cacioppo et al., 2006, 2010; Sjöberg et al., 2013). The link between depression and loneliness is clearly established by authors that conceive depression as an evolutionarily conserved mechanism to terminate separation distress (Watt and Panksepp, 2009; Panksepp and Watt, 2011; Watt, 2014; also see Slavich, 2020; social safety theory), placing social loss at the center of the neurobiological dynamics (e.g., inflammation, altered HPA axis functioning, declining neurotrophins prosocial peptides and amines) driving depression. Also, two studies excluded from this scoping review (see Table 2) demonstrated the key role played by depression as a mediator between loneliness and cognition. Donovan et al.’s (2017) study with 8,382 USA participants aged 65 or older concluded that, after 12 years, the effect of loneliness on cognitive function became marginally significant after controlling for depression, and that the latter is associated with a more rapid cognitive decline. Similarly, Lam et al. (2017) revealed that, only among the individuals who reported higher levels of depressive symptoms, loneliness was associated with poorer cognitive function.
Interestingly, this link with depressive symptoms was not observed for social isolation. In the scoping review by Courtin and Knapp (2017) on social isolation, loneliness and health in old age, 25 studies looked at the link between loneliness and depression and 3 looked at the link between social isolation and depression. The evidence reviewed clearly showed that loneliness is a strong risk factor for depression in old age, even after controlling for a number of covariates such as demographic characteristics, marital status, social isolation and psychosocial risk factors. The detrimental effect of living alone on depression was more often due to loneliness for men than for women. The evidence for a link between social isolation and depression was however weaker. This evidence suggests that the subjective experience of loneliness may be more strongly related to depression than the objective isolation per se, and that the link between social isolation and cognitive dysfunction is less mediated by depression.
Considering the studies that investigated social isolation and loneliness simultaneously, Griffin et al.’s (2020) and Yu et al.’s (2020) results also suggest that social isolation may have a more substantial impact than loneliness on cognitive decline. For instance, correlations between loneliness and cognitive function were non-significant after controlling for a wide range of demographic and psychosocial risk factors thought to influence loneliness. Consistent with our findings, recent research has suggested that social isolation is more associated with objective cognitive impairment outcomes, while loneliness is more associated with a subjective dimension of cognitive function (Jang et al., 2021; see Table 2). This is also consistent with Boss et al.’s (2015) review showing that, when social and emotional loneliness were examined, the first seemed to have a stronger correlation with global cognitive function.
These findings suggest that both social isolation and loneliness may impact cognitive health but probably in a different way, with a stronger weight on cognitive reserve for the first and on emotional wellbeing for the second. A possible explanation of the link between social isolation and cognitive decline would have to do with the “use it or lose it” perspective (Hultsch et al., 1999; Salthouse, 2006). Park and Bischof (2013) reviewed the evidence suggesting that engagement in an environment that requires cognitive effort may facilitate cognitive function in older adults. This view, linked to the notion of neuroplasticity (also see Greenwood and Parasuraman, 2010) suggests that the brain can be conceived as a muscle and that engagement in intellectual, social and physical activities stimulates the brain. If engagement in everyday activities is absent, it may result in disuse of the brain which will result in decline of cognitive functions. The seemingly stronger association between cognition and social isolation than between loneliness and cognition would go in favor of this explanation.
On the other hand, although the empirical literature regarding the underlying biological mechanisms involved in social isolation and loneliness is scarce and not fully consistent (Palmer, 2019), there is some evidence suggesting that, biologically, loneliness may trigger immune system impairment, chronic inflammation, hypertension, hyperlipidemia (Cunningham, 2013; Cacioppo et al., 2014, 2015; Hawkley and Capitanio, 2015), hypercortisolism (Boss et al., 2015) and prolonged activation of the hypothalamic–pituitary–adrenal (HPA) axis, which in turn could lead to a decrease in dendritic arborization in the prefrontal cortex (CPF) and hippocampus (Cacioppo and Hawkley, 2009). Nonetheless, many of these neurological and physiological changes are linked to ageing itself, and, hence, the mixed effects of loneliness, social isolation and ageing may be even more complex.
As for the direction of the relationship, the idea of this review came from the interest in the consequences of the isolation experienced during the COVID-19 pandemic, with the question of whether social isolation might be detrimental to cognition. In that sense, the direction of the effect may be conceived from social isolation and loneliness to cognition. However, there is evidence suggesting that the effect can also go in the opposite direction, i.e., poor cognition can lead to isolation and loneliness, known as reverse causality. It has been suggested that older adults who experience declining self-efficacy and loss of attachment relationships defensively place more emphasis on independence and self-reliance and less on interdependence (Zhang and Labouvie-Vief, 2004). Yin et al. (2019) reached such a conclusion following their result of a higher rate of memory decline predicting loneliness at follow-up and vice versa. Possible explanations for this is that poor cognition may generate feelings of insecurity. Schnittger et al. (2012), for example, showed that decreased verbal fluency was a significant predictor of social loneliness. Poor communication skills may discourage conversation, hinder meaningful relationships, and thus increase loneliness. Another recent study (Sin et al., 2021; see Table 2), also found that a dysfunction in working memory and planning might prognosticate higher perceived loneliness. McHugh Power et al. (2019) also revealed this reverse association, demonstrating that sustained attention at baseline predicted loneliness 4 years later.
Previous reviews had mentioned the difficulty to solve this question due to the great proportion of cross sectional studies (see for example, Boss et al., 2015; Courtin and Knapp, 2017). Our review minimized this risk by excluding participants with cognitive impairment of dementia and by excluding cross-sectional studies. To conclude, it is likely that the relationship between social isolation loneliness and cognitive decline may be bidirectional.
As limitations of the present study, the heterogeneity observed in measures of social isolation, loneliness and cognitive functions in the reviewed studies makes it difficult to carry out more specific analyses (e.g., meta-analysis). Also, only 12 studies fulfilled the inclusion criteria. As strengths, only powerful longitudinal studies evaluating cognitively healthy older participants were reviewed. This is the best method to explore causal relationships between the studied variables. Moreover, studies from three different continents were included, which helps generalizing the results. Finally, a key strength is that we considered both social isolation and loneliness as measures of objective and subjective isolation, respectively, which should contribute to a better understanding of differential effects of both constructs on cognitive decline in ageing.
Conclusion
After considering the 12 longitudinal studies that comprise large heterogeneous, and culturally diverse populations, we conclude that both loneliness and social isolation, common among older adults, may be associated with cognitive decline. It seems that the relationship between social isolation and cognitive decline may be stronger than the link between loneliness and cognition, possibly mediated by depression.
We also notice that both constructs are complex, with a diversity of definitions and measurements, and require more nuanced examination, with special attention to the specific nature or forms of social isolation, loneliness and their interactions in affecting mental health and cognition. Additional research is necessary to determine more precisely the causality and biological mechanisms implied in the association between social isolation, loneliness and cognitive functioning.
Data availability statement
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
Both authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
Funding
This study was supported by grant REF PSI2016-75484-R funded by MCIN/AEI/10.13039/501100011033 and “ERDF A way of making Europe,” by the “European Union”.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
- ^ The final time period within the bibliographical searches in previous reviews was January 2017 [in Kelly et al.’s (2017) study].
References
Bartrés-Faz, D., Macià, D., Cattaneo, G., Borràs, R., Tarrero, C., Solana, J., et al. (2021). The paradoxical effect of COVID-19 outbreak on loneliness. BJPsych Open 7:e30. doi: 10.1192/bjo.2020.163
Boss, L., Kang, D., and Branson, S. (2015). Loneliness and cognitive function in the older adult: A systematic review. Int. Psychogeriatr. 27, 541–553. doi: 10.1017/S1041610214002749
Bowlby, J. (1982). Attachment and loss: Retrospect and prospect. Am. J. Orthopsychiatry 52, 664–678. doi: 10.1111/j.1939-0025.1982.tb01456.x
Bude, H., and Lantermann, E. (2006). Soziale exklusion und exklusionsempfinden. KZfSS Köl. Z. Soziol. Sozialpsychol. 58, 233–252. doi: 10.1007/s11575-006-0054-1
Bzdok, D., and Dunbar, R. (2020). The neurobiology of social distance. Trends Cogn. Sci. 24, 717–733. doi: 10.1016/j.tics.2020.05.016
Cacioppo, J. T., Cacioppo, S., and Boomsma, D. I. (2014). Evolutionary mechanisms for loneliness. Cogn. Emot. 28, 3–21. doi: 10.1080/02699931.2013.837379
Cacioppo, J. T., and Hawkley, L. C. (2009). Perceived social isolation and cognition. Trends Cogn. Sci. 13, 447–454. doi: 10.1016/j.tics.2009.06.005
Cacioppo, J. T., Hawkley, L. C., and Thisted, R. A. (2010). Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago health, aging, and social relations study. Psychol. Aging 25, 453–463. doi: 10.1037/a0017216
Cacioppo, J. T., Hughes, M. E., Waite, L. J., Hawkley, L. C., and Thisted, R. A. (2006). Loneliness as a specific risk factor for depressive symptoms: Cross-sectional and longitudinal analyses. Psychol. Aging 21, 140–151. doi: 10.1037/0882-7974.21.1.140
Cacioppo, J. T., and Patrick, W. (2008). Loneliness: Human nature and the need for social connection. New York, NY: W W Norton & Co.
Cacioppo, S., Grippo, A. J., London, S., Goossens, L., and Cacioppo, J. T. (2015). Loneliness: Clinical import and interventions. Perspect. Psychol. Sci. 10, 238–249. doi: 10.1177/1745691615570616
Cheung, X., Cosco, T., and Ariyo, T. (2021). Decreasing social isolation to enhance mental health among older adults in China: A mediation analysis of aging attitude. Front. Psychol. 12:735740. doi: 10.3389/fpsyg.2021.735740
Christakis, N. A., and Fowler, J. H. (2009). Connected: The surprising power of our social networks and how they shape our lives. New York, NY: Little, Brown. doi: 10.1163/156853710X531267
Ciesielska, N., Sokołowski, R., Mazur, E., Podhorecka, M., Polak-Szabela, A., and Kędziora-Kornatowska, K. (2016). Is the Montreal Cognitive Assessment (MoCA) test better suited than the Mini-Mental State Examination (MMSE) in mild cognitive impairment (MCI) detection among people aged over 60? Meta-analysis. Psychiatr. Pol. 50, 1039–1052. doi: 10.12740/PP/45368
Cole, S. W., Hawkley, L. C., Arevalo, J. M., Sung, C., Rose, R., and Cacioppo, J. (2007). Social regulation of gene expression in human leukocytes. Genome Biol. 8:R189. doi: 10.1186/gb-2007-8-9-r189
Cornwell, E. Y., and Waite, L. J. (2009). Social disconnectedness, perceived isolation, and health among older adults. J. Health Soc. Behav. 50, 31–48. doi: 10.1177/002214650905000103
Courtin, E., and Knapp, M. (2017). Social isolation, loneliness and health in old age: A scoping review. Health Soc. Care Community 25, 799–812. doi: 10.1111/hsc.12311
Coyle, C. E., and Dugan, E. (2012). Social isolation, loneliness and health among older adults. J. Aging Health 24, 1346–1363. doi: 10.1177/0898264312460275
Cunningham, C. (2013). Microglia and neurodegeneration: The role of systemic inflammation. Glia 61, 71–90.
Damian, A. M., Jacobson, S. A., Hentz, J. G., Belden, C. M., Shill, H. A., Sabbagh, M. N., et al. (2011). The Montreal Cognitive Assessment and the mini-mental state examination as screening instruments for cognitive impairment: Item analyses and threshold scores. Dement. Geriatr. Cogn. Disord. 31, 126–131.
de Jager, C. A., Budge, M. M., and Clarke, R. (2003). Utility of TICS-M for the assessment of cognitive function in older adults. Int. J. Geriatr. Psychiatry 18, 318–324. doi: 10.1002/gps.830
de Jong-Gierveld, J., and Havens, B. (2004). Cross-national comparisons of social isolation and loneliness: Introduction and overview. Can. J. Aging 23, 109–113. doi: 10.1353/cja.2004.0021
Diehl, M. S., Elnick, A. B., Bourbeau, L. S., and Labouvie-Vief, G. (1998). Adult attachment styles: Their relations to family context and personality. J. Pers. Soc. Psychol. 74, 1656–1669. doi: 10.1037/0022-3514.74.6.1656
d’Oleire Uquillas, F., Jacobs, H. I. L., Biddle, K. D., Properzi, M., Hanseeuw, B., Schultz, A. P., et al. (2018). Regional tau pathology and loneliness in cognitively normal older adults. Transl. Psychiatry 8:282. doi: 10.1038/s41398-018-0345-x
Donovan, N. J., Okereke, O. I., Vannini, P., Amariglio, R. E., Rentz, D. M., Marshall, G. A., et al. (2016). Association of higher cortical amyloid burden with loneliness in cognitively normal older adults. JAMA Psychiatry 73, 1230–1237. doi: 10.1001/jamapsychiatry.2016.2657
Donovan, N. J., Qiong, W., Rentz, D. M., Sperling, R. A., Marshall, G. A., and Glymour, M. M. (2017). Loneliness, depression and cognitive function in older U.S. adults. Int. J. Geriatr. Psychiatry 32, 564–573. doi: 10.1002/gps.4495
Evans, I., Llewellyn, D. J., Matthews, F. E., Woods, R. T., Brayne, C., Clare, L., et al. (2018). Social isolation, cognitive reserve, and cognition in healthy older people. PLoS One 13:e0201008. doi: 10.1371/journal.pone.0201008
Evans, I., Llewellyn, D. J., Matthews, F. E., Woods, R. T., Brayne, C., Clare, L., et al. (2019). Living alone and cognitive function in later life. Arch. Gerontol. Geriatr. 81, 222–233. doi: 10.1016/j.archger.2018.12.014
Fowler, J. H., and Christakis, N. A. (2008). Dynamic spread of happiness in a large social network: Longitudinal analysis over 20 years in the Framingham Heart Study. BMJ 337:a2338. doi: 10.1136/bmj.a2338
Glei, D. A., Goldman, N., Ryff, C. D., Lin, Y.-H., and Weinstein, M. (2012). Social relationships and inflammatory markers: An analysis of Taiwan and the U.S. Soc. Sci. Med. 74, 1891–1899. doi: 10.1016/j.socscimed.2012.02.020
Greenwood, P., and Parasuraman, R. (2010). Neuronal and cognitive plasticity: A neurocognitive framework for ameliorating cognitive aging. Front. Aging Neurosci. 2:150. doi: 10.3389/fnagi.2010.00150
Griffin, S. C., Mezuk, B., Williams, A. B., Perrin, P. B., and Rybarczyk, B. D. (2020). Isolation, not loneliness or cynical hostility, predicts cognitive decline in older Americans. J. Aging Health 32, 52–60. doi: 10.1177/0898264318800587
Hajek, A., Riedel-Heller, S. G., and König, H. (2020). Perceived social isolation and cognitive functioning. Longitudinal findings based on the German Ageing Survey. Int. J. Geriatr. Psychiatry 35, 276–281. doi: 10.1002/gps.5243
Haro, J. M., Arbabzadeh-Bouchez, S., Brugha, T. S., de Girolamo, G., Guyer, M., Jin, R., et al. (2006). Concordance of the Composite International Diagnostic Interview Version 3.0 (CIDI 3.0) with standardized clinical assessments in the WHO World Mental Health Surveys. Int. J. Methods Psychiatr. Res. 15, 167–180. doi: 10.1002/mpr.196
Hawkley, L., and Capitanio, J. (2015). Perceived social isolation, evolutionary fitness and health outcomes: A lifespan approach. Philos. Trans. R. Soc. B 370:20140114. doi: 10.1098/rstb.2014.0114
Holt-Lunstad, J., Smith, T. B., Baker, M., Harris, T., and Stephenson, D. (2015). Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspect. Psychol. Sci. 10, 227–237. doi: 10.1177/1745691614568352
Holt-Lunstad, J., Smith, T. B., and Layton, J. B. (2010). Social relationships and mortality risk: A meta-analytic review. PLoS Med. 7:e1000316. doi: 10.1371/journal.pmed.1000316
Hughes, M. E., Waite, L. J., Hawkley, L. C., and Cacioppo, J. T. (2004). A short scale for measuring loneliness in large surveys: Results from two population-based studies. Res. Aging 26, 655–672. doi: 10.1177/0164027504268574
Hultsch, D. F., Hertzog, C., Small, B. J., and Dixon, R. A. (1999). Use it or lose it: Engaged lifestyle as a buffer of cognitive decline in aging? Psychol. Aging 14, 245–263. doi: 10.1037//0882-7974.14.2.245
Irwin, M. R., and Cole, S. W. (2011). Reciprocal regulation of the neural and innate immune systems. Nat. Rev. Immunol. 11, 625–632. doi: 10.1038/nri3042
Jang, Y., Choi, E. Y., Park, N. S., Chiriboga, D. A., Duan, L., and Kim, M. T. (2021). Cognitive health risks posed by social isolation and loneliness in older Korean Americans. BMC Geriatr. 21:123. doi: 10.1186/s12877-021-02066-4
Jia, X., Wang, Z., Huang, F., Su, C., Du, W., Jiang, H., et al. (2021). A comparison of the Mini-Mental State Examination (MMSE) with the Montreal Cognitive Assessment (MoCA) for mild cognitive impairment screening in Chinese middle-aged and older population: A cross-sectional study. BMC Psychiatry 21:485. doi: 10.1186/s12888-021-03495-6
Kelly, M. E., Duff, H., Kelly, S., McHugh Power, J. E., Brennan, S., Lawlor, B. A., et al. (2017). The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: A systematic review. Syst. Rev. 6:259. doi: 10.1186/s13643-017-0632-2
Kuiper, J. S., Zuidersma, M., Zuidema, S. U., Burgerhof, J. G. M., Stolk, R. P., Oude Voshaar, R. C., et al. (2016). Social relationships and cognitive decline: A systematic review and meta-analysis of longitudinal cohort studies. Int. J. Epidemiol. 45, 1169–1206. doi: 10.1093/ije/dyw089
Lam, C. L. M., Junhong, Y., and Lee, T. M. C. (2017). Perceived loneliness and general cognitive status in community-dwelling older adults: The moderating influence of depression. Aging Neuropsychol. Cogn. 24, 471–480. doi: 10.1080/13825585.2016.1226246
Lam, J., Murray, E., Yu, K., Ramsey, M., Nguyen, T., Mishra, J., et al. (2021). Neurobiology of loneliness: A systematic review. Neuropsychopharmacology 46, 873–1887. doi: 10.1038/s41386-021-01058-7
Lara, E., Caballero, F. F., Rico-Uribe, L. A., Olaya, B., Haro, J. M., Ayuso-Mateos, J. L., et al. (2019). Are loneliness and social isolation associated with cognitive decline? Int. J. Geriatr. Psychiatry 34, 1613–1622. doi: 10.1002/gps.5174
Leigh-Hunt, N., Bagguley, D., Bash, K., Turner, V., Turnbull, S., Valtorta, N., et al. (2017). An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 152, 157–171. doi: 10.1016/j.puhe.2017.07.035
Ligthart, S., Vaez, A., Võsa, U., Stathopoulou, M. G., de Vries, P. S., Prins, B. P., et al. (2018). Genome analyses of >200,000 individuals identify 58 loci for chronic inflammation and highlight pathways that link inflammation and complex disorders. Am. J. Hum. Genet. 103, 691–706. doi: 10.1016/j.ajhg.2018.09.009
Liu, D., Xi, J., Hall, B. J., Fu, M., Zhang, B., Guo, J., et al. (2020). Attitudes toward aging, social support and depression among older adults: Difference by urban and rural areas in China. J. Affect. Disord. 274, 85–92. doi: 10.1016/j.jad.2020.05.052
Lubben, J., Blozik, E., Gillmann, G., Iliffe, S., von Renteln Kruse, W., Beck, J. C., et al. (2006). Performance of an abbreviated version of the Lubben Social Network Scale among three European community-dwelling older adult populations. Gerontologist 46, 503–513. doi: 10.1093/geront/46.4.503
Luchetti, M., Terracciano, A., Aschwanden, D., Lee, J. H., Stephan, Y., and Sutin, A. R. (2020). Loneliness is associated with risk of cognitive impairment in the Survey of Health. Ageing and Retirement in Europe. Int. J. Geriatr. Psychiatry 35, 794–801. doi: 10.1002/gps.5304
Magai, C., Cohen, C., Milburn, N., Thorpe, B., McPherson, R., and Peralta, D. (2001). Attachment styles in older European American and African American adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 56B, S28–S35. doi: 10.1093/geronb/56.1.s28
McHugh Power, J. E., Hannigan, C., Carney, S., Feeney, J., Kenny, R. A., Kee, F., et al. (2019). Lonely SARTs: Loneliness and sustained attention in the Irish Longitudinal Study of Aging. Aging Neuropsychol. Cogn. 27, 197–206. doi: 10.1080/13825585.2019.1602705
McHugh Power, J. E., Kenny, R. A., Lawlor, B. A., Steptoe, A., and Kee, F. (2017). The discrepancy between social isolation and loneliness as a clinically meaningful metric: Findings from the Irish and English longitudinal studies of ageing (TILDA and ELSA). Int. J. Geriatr. Psychiatry 32, 664–674. doi: 10.1002/gps.4509
McHugh Power, J. E., Tang, J., Kenny, R. A., Lawlor, B. A., and Kee, F. (2020). Mediating the relationship between loneliness and cognitive function: The role of depressive and anxiety symptoms. Aging Ment. Health 24, 1071–1078. doi: 10.1080/13607863.2019.1599816
Morris, J., Heyman, A., and Mohs, R. (1989). The Consortium to Establish a Registry for Alzheimer’s Disease (CERAD). Part I. Clinical and neuropsychological assessment of Alzheimer’s disease. Neurology 39, 1159–1165. doi: 10.1212/wnl.39.9.1159
Palmer, B. W. (2019). The effects of loneliness and social isolation on cognitive functioning in older adults: A need for nuanced assessments. Int. Psychogeriatr. 31, 447–449. doi: 10.1017/S1041610218001849
Panksepp, J., and Watt, D. (2011). Why does depression hurt? Ancestral primary-process separation-distress (PANIC/GRIEF) and diminished brain reward (SEEKING) processes in the genesis of depressive affect. Psychiatry 74, 5–13. doi: 10.1521/psyc.2011.74.1.5
Park, D. C., and Bischof, G. N. (2013). The aging mind: Neuroplasticity in response to cognitive training. Dialogues Clin. Neurosci. 15, 109–119. doi: 10.31887/DCNS.2013.15.1/dpark
Pinto, T., Machado, L., Bulgacov, T., Rodrigues-Júnior, A., Costa, M., Ximenes, R., et al. (2019). Is the Montreal Cognitive Assessment (MoCA) screening superior to the Mini-Mental State Examination (MMSE) in the detection of mild cognitive impairment (MCI) and Alzheimer’s Disease (AD) in the elderly? Int. Psychogeriatr. 31, 491–504. doi: 10.1017/S1041610218001370
Pressman, S. D., Cohen, S., Miller, G. E., Barkin, A., Rabin, B. S., and Treanor, J. J. (2005). Loneliness, social network size, and immune response to influenza vaccination in college freshmen. Health Psychol. 24, 297–306. doi: 10.1037/0278-6133.24.3.297
Prince, M. J., Reischies, F., Beekman, A. T., Fuhrer, R., Jonker, C., Kivela, S. L., et al. (1999). Development of the EURO–D scale– a European, Union initiative to compare symptoms of depression in 14 European centres. Br. J. Psychiatry 174, 330–338. doi: 10.1192/bjp.174.4.330
Radloff, L. (1977). The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1, 385–401. doi: 10.1177/014662167700100306
Read, S., Comas-Herrera, A., and Grundy, E. (2020). Social isolation and memory decline in later-life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 75, 367–376. doi: 10.1093/geronb/gbz152
Robertson, I. H., Manly, T., Andrade, J., Baddeley, B. T., and Yiend, J. (1997). ‘Oops!’: Performance correlates of everyday attentional failures in traumatic brain injured and normal subjects. Neuropsychologia 35, 747–758. doi: 10.1016/s0028-3932(97)00015-8
Roth, M., Tym, E., Mountjoy, C. Q., Huppert, F. A., Hendrie, H., Verma, S., et al. (1986). CAMDEX. A standardised instrument for the diagnosis of mental disorder in the elderly with special reference to the early detection of dementia. Br. J. Psychiatry 149, 698–709. doi: 10.1192/bjp.149.6.698
Russell, D. (1996). UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. J. Pers. Assess. 66, 20–40. doi: 10.1207/s15327752jpa6601_2
Salthouse, T. A. (2006). Mental exercise and mental aging: Evaluating the Validity of the “Use It or Lose It” Hypothesis. Perspect. Psychol. Sci. 1, 68–87. doi: 10.1111/j.1745-6916.2006.00005.x
Sarkar, D. K., Sengupta, A., Zhang, C., Boyadjieva, N., and Murugan, S. (2012). Opiate antagonist prevents μ- and δ-opiate receptor dimerization to facilitate ability of agonist to control ethanol-altered natural killer cell functions and mammary tumor growth. J. Biol. Chem. 287, 16734–16747. doi: 10.1074/jbc.M112.347583
Schnittger, R. I., Wherton, J., Prendergast, D., and Lawlor, B. A. (2012). Risk factors and mediating pathways of loneliness and social support in community-dwelling older adults. Aging Ment. Health 16, 335–346. doi: 10.1080/13607863.2011.629092
Shankar, A., Hamer, M., McMunn, A., and Steptoe, A. (2013). Social isolation and loneliness: Relationships with cognitive function during 4 years of follow-up in the English Longitudinal Study of Ageing. Psychosom. Med. 75, 161–170. doi: 10.1097/PSY.0b013e31827f09cd
Shankar, A., McMunn, A., Banks, J., and Steptoe, A. (2011). Loneliness, social isolation, and behavioral and biological health indicators in older adults. Health Psychol. 30, 377–385. doi: 10.1037/a0022826
Shankar, A., Rafnsson, S. B., and Steptoe, A. (2015). Longitudinal associations between social connections and subjective wellbeing in the English Longitudinal Study of Ageing. Psychol. Health 30, 686–698. doi: 10.1080/08870446.2014.979823
Sin, E., Shao, R., and Lee, T. (2021). The executive control correlate of loneliness in healthy older people. Aging Ment. Health 25, 1224–1231. doi: 10.1080/13607863.2020.1749832
Sjöberg, L., Östling, S., Falk, H., Sundh, V., Waern, M., and Skoog, I. (2013). Secular changes in the relation between social factors and depression: A study of two birth cohorts of Swedish septuagenarians followed for 5 years. J. Affect. Disord. 150, 245–252. doi: 10.1016/j.jad.2013.04.002
Slavich, G. M. (2020). Social safety theory: A biologically based evolutionary perspective on life stress, health, and behavior. Annu. Rev. Clin. Psychol. 16, 265–295. doi: 10.1146/annurev-clinpsy-032816-045159
Slavich, G. M., and Cole, S. W. (2013). The emerging field of human social genomics. Clin. Psychol. Sci. 1, 331–348. doi: 10.1177/2167702613478594
Smith, E. B., Brands, R. A., Brashears, M. E., and Kleinbaum, A. M. (2020). Social networks and cognition. Annu. Rev. Sociol. 46, 159–174. doi: 10.1146/annurev-soc-121919-054736
Smith, J., Fisher, G., Ryan, L., Clarke, P., House, J., and Weir, D. (2013). Psychosocial and lifestyle questionnaire, 2006–2010: documentation report core section LB. Ann Arbor, MI: University of Michigan.
Smith, E. B., Menon, T., and Thompson, L. (2012). Status differences in the cognitive activation of social networks. Organ. Sci. 23, 67–82. doi: 10.1287/orsc.1100.0643
Steptoe, A., Shankar, A., Demakakos, P., and Wardle, J. (2013). Social isolation, loneliness, and all-cause mortality in older men and women. Proc. Natl. Acad. Sci. U.S.A. 110, 5797–5801. doi: 10.1073/pnas.1219686110
Sundström, G., Fransson, E., Malmberg, B., and Davey, A. (2009). Loneliness among older Europeans. Eur. J. Ageing 6, 267–275. doi: 10.1007/s10433-009-0134-8
Tricco, A. C., Lillie, E., Zarin, W. O., Brien, K., Colquhoun, H., Levac, D., et al. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 169, 467–473. doi: 10.7326/M18-0850
Valtorta, N., and Hanratty, B. (2012). Loneliness, isolation and the health of older adults: Do we need a new research agenda? J. R. Soc. Med. 105, 518–522. doi: 10.1258/jrsm.2012.120128
Victor, C., Scambler, S., Shah, S., Cook, D., Harris, T., Rink, E., et al. (2002). Has loneliness amongst older people increased? An investigation into variations between cohorts. Ageing Soc. 22, 585–597. doi: 10.1017/S0144686X02008784
Wang, H., Lee, C., Hunter, S., Fleming, J., Brayne, C., and CC75C Study Collaboration. (2020). Longitudinal analysis of the impact of loneliness on cognitive function over a 20-year follow-up. Aging Ment. Health 24, 1815–1821. doi: 10.1080/13607863.2019.1655704
Watt, D. F. (2014). “Depression in the elderly: Interactions with aging, stress, chronic pain, inflammation, and neurodegenerative disorders,” in Geriatric neurology, eds A. K. Nair and M. N. Sabbagh (New York, NY: Wiley), 281–301. doi: 10.1002/9781118730676.ch10
Watt, D. F., and Panksepp, J. (2009). Depression: An evolutionarily conserved mechanism to terminate separation distress? A review of aminergic, peptidergic, and neural network perspectives. Neuropsychoanalysis 11, 7–51. doi: 10.1080/15294145.2009.10773593
Webster, J. D. (1997). Attachment style and well-being in elderly adults: A preliminary investigation. Can. J. Aging 16, 101–111. doi: 10.1017/S0714980800014185
Wechsler, D. (1955). Manual for the Wechsler adult intelligence scale. New York, NY: Psychological Corporation.
Wilson, R. S., Krueger, K. R., Arnold, S. E., Schneider, J. A., Kelly, J. F., Barnes, L. L., et al. (2007). Loneliness and risk of Alzheimer’s disease. Arch. Gen. Psychiatry 64, 234–240. doi: 10.1001/archpsyc.64.2.234
Yin, J., Lassale, C., Steptoe, A., and Cadar, D. (2019). Exploring the bidirectional associations between loneliness and cognitive functioning over 10 years: The English Longitudinal Study of Ageing. Int. J. Epidemiol. 48, 1937–1948. doi: 10.1093/ije/dyz085
Yu, B., Steptoe, A., Chen, Y., and Jia, X. (2020). Social isolation, rather than loneliness, is associated with cognitive decline in older adults: The China health and retirement longitudinal study. Psychol. Med. 51, 2414–2421. doi: 10.1017/S0033291720001014
Zhang, F., and Labouvie-Vief, G. (2004). Stability and fluctuation in adult attachment style over a 6-year period. Attach. Hum. Dev. 6, 419–437. doi: 10.1080/1461673042000303127
Keywords: social isolation, loneliness, cognition, ageing, cognitive decline, depression
Citation: Cardona M and Andrés P (2023) Are social isolation and loneliness associated with cognitive decline in ageing? Front. Aging Neurosci. 15:1075563. doi: 10.3389/fnagi.2023.1075563
Received: 20 October 2022; Accepted: 23 January 2023;
Published: 23 February 2023.
Edited by:
Adrian W. Gilmore, National Institute of Mental Health (NIH), United StatesReviewed by:
Douglas F. Watt, Lesley University, United StatesRiccardo Manca, Brunel University London, United Kingdom
Copyright © 2023 Cardona and Andrés. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pilar Andrés,  cGlsYXIuYW5kcmVzQHVpYi5lcw==
cGlsYXIuYW5kcmVzQHVpYi5lcw==
†These authors have contributed equally to this work