 Elinor C. Harrison1,2
Elinor C. Harrison1,2 Allison M. Haussler2
Allison M. Haussler2 Lauren E. Tueth2
Lauren E. Tueth2 Sidney T. Baudendistel2
Sidney T. Baudendistel2 Gammon M. Earhart2,3,4*
Gammon M. Earhart2,3,4*- 1Program in Dance, Performing Arts Department, Washington University in St. Louis, St. Louis, MO, United States
- 2Program in Physical Therapy, Washington University in School of Medicine St. Louis, St. Louis, MO, United States
- 3Department of Neurology, Washington University School of Medicine in St. Louis, St. Louis, MO, United States
- 4Department of Neuroscience, Washington University School of Medicine in St. Louis, St. Louis, MO, United States
Introduction: Dance is an effective and motivating form of exercise for older women, but few studies have quantified the benefits of virtual dance classes nor, specifically, ballet. This study tested the effectiveness of virtual ballet compared to virtual wellness classes, with the goal of reaching underserved populations. It is among the first to explore the effects of virtual classical ballet on functional gait mobility, balance, and quality of life measures in older women.
Methods: Older women were recruited in two waves and randomized to two groups: a ballet class modified for older adults and a wellness-based control class. Both groups received 12 weeks of online classes, meeting twice per week for 45-min sessions. Classes were taught by a local company that offers community-based ballet classes. The same instructor led both the ballet and the wellness classes. Pre- and post-intervention assessments include gait and balance testing using wearable inertial sensors and self-report outcomes including quality of life and mood questionnaires.
Results: Forty-four older women completed the study: Ballet group (n = 21, 67.81 ± 7.3 years); Wellness group (n = 23, 69.96 ± 6.7 years). Pre- to post-intervention, both groups increased velocity on the two-minute walk test (F1,42 = 25.36, p < 0.001) and improved their time on the Timed Up and Go (F1,42 = 4.744, p = 0.035). Both groups improved balance on the Mini-BESTest (F1,42 = 38.154, p < 0.001), increased their scores on the Activities-Specific Balance Confidence Scale (F1,42 = 10.688, p < 0.001), and increased quality of life via the Short Form Health Survey (F1,42 = 7.663, p = 0.008). The ballet group improved gait variability in the backward direction (F1,42 = 14.577, p < 0.001) and reduced fall rates more than the wellness group [χ2(1) = 5.096, p = 0.024].
Discussion: Both virtual ballet and wellness classes improve select measures of gait, balance, and quality of life. The benefits seen in both groups highlight the importance of considering social interaction as a key component when developing future interventions to target mobility in older women.
1 Introduction
Falls are a major cause of disability in older adults. Every second of every day an older adult, aged 65 or older, suffers a fall in the US, leading to 30 million falls each year (CDC, 2019). Women, who are more likely than men to experience bone density loss in older age, are particularly susceptible to falls and account for 75% of all hip fractures regardless of gender (Gale et al., 2016). Even a single fall can be debilitating, leading to a fear of falling, withdrawal from activities, and reduced quality of life (Bower et al., 2016).
The two primary factors that contribute to fall risk among older adults are decline in gait and decline in balance ability (Kyrdalen et al., 2019). Gait impairment affects one third of the population over 70 years of age and represents a major cause of falls (Verghese, 2006). Gait speed, in particular, is a robust marker of overall health, as reductions in self-selected gait speed with aging can predict adverse events, future disability, healthcare utilization, and even mortality (Cesari et al., 2005). Slower walking can also lead to more variability between steps, rendering walking less stable (Kang and Dingwell, 2008). Increased gait variability in older adults is correlated to higher fall risk (Hausdorff et al., 2001). Multifactorial interventions for older adults that increase gait speed and decrease gait variability may help reduce fall rates (Gillespie et al., 2021).
Balance is a complex activity that requires coordinating multiple body systems. Effective balance involves maintaining upright posture during static conditions as well as facilitating movement during dynamic tasks, such as walking (Horak, 2006). Balance decline in aging involves reduced strength, flexibility, and sensory loss, which collectively contribute to fall risk (Kanekar and Aruin, 2014). Older adults at risk of falling, when compared to those who are not, are unable to hold static postures as long (Araujo et al., 2022), exhibit increased postural sway during standing balance tasks (Oliveira et al., 2018), and perform worse on dual cognitive-motor tasks (Verghese et al., 2002).
Dance is a multi-modal artform that provides an effective therapy for addressing gait and balance impairments in older adults as it combines multi-sensory elements including proprioceptive, visual, auditory, and motor control techniques (Earhart, 2009). In-person dance interventions for older adults frequently show benefits to functional mobility (Hwang and Braun, 2015; Britten et al., 2017). Gait improvements have been reported across a broad range of dance styles showing improvements in stride velocity (Granacher et al., 2012), walking endurance (Shigematsu et al., 2002; Hui et al., 2009), and muscle function (Cepeda et al., 2015). Balance improvements are reported in a similarly wide variety of dance styles including contemporary (Ferrufino et al., 2011; Coubard et al., 2014), jazz (Wallmann et al., 2009), ballroom (Cepeda et al., 2015), salsa (Granacher et al., 2012), tango (Hackney et al., 2007; Hackney and Earhart, 2009; Earhart, 2013; Sofianidis et al., 2017), and traditional folk dance (Eyigor et al., 2009; Sofianidis et al., 2009; Pacheco et al., 2016). Furthermore, cross-sectional studies show that older adults who dance regularly have better balance capabilities than those who do not (Verghese, 2006; Dewhurst et al., 2015).
Classical ballet interventions for older adults, however, remain underrepresented in the literature despite ample evidence to suggest that they might be useful in older populations (Hwang and Braun, 2015; Weighart and DiPasquale, 2020). Ballet trains postural stability through a mix of static and dynamic processes that may translate to gait and balance improvements. The use of a ballet barre renders training feasible and safe for older adults, while encouraging stability and upright posture during standing exercises. Ballet is highly adaptable to home studio settings, as stationary chairs readily substitute for ballet barres and much of the class period can be done in a small room with minimal shifting of the camera. Ballet classes emphasize sensorimotor integration (Tanabe et al., 2014) and teach specific visual and proprioceptive techniques that may aid postural control and body awareness (de Mello et al., 2017). Ballet combinations are cognitively challenging and require complex coordination of multiple body parts. Emphasis on movement sequencing, timing, and efficiency may help with dynamic movement tasks (Kiefer et al., 2011). Ballet may also teach strategies for complex movement tasks, such as backward or dual task walking, that frequently lead to falls (Muir-Hunter and Wittwer, 2016; Bayot et al., 2020). Focusing on full-body stabilization during ballet may challenge the body to constantly recalibrate and adjust to destabilizing forces (Weighart and DiPasquale, 2020).
Dance interventions not only address mobility issues, but also promote cognition, emotional expression, kinesthetic awareness, and social engagement (Hwang and Braun, 2015; Clifford et al., 2023). During the COVID-19 pandemic, many dance therapy classes moved online, which afforded the convenience and safety of participating from one’s own home but removed elements of social interaction and group support that are naturally structured into in-person classes (Bek et al., 2022). Kinesthetic empathy, or the ability to perceive others’ emotions through action observation, is a key component of in-person classes (Christopher and Tamplin, 2022) that may occur less spontaneously during virtual classes. While in-person classes have resumed, online classes often remain available for people who are unable to travel or need flexibility to participate from home; however, little is known about how much benefit online classes provide.
Though the main objective of the interventions was to improve functional mobility, we also assessed the synergistic interactions of mind and body reflected through complex motor dual-tasks, quality of life, and mood. In order to test the effects of ballet on gait and balance, he primary outcome measures were gait velocity and postural stability. Secondary measures were balance confidence, fall frequency, quality of life, and mood measures. We hypothesized that the ballet intervention would be more effective at improving gait and balance measures than the wellness intervention, but that both interventions would equally improve quality of life and mood.
2 Methods
The interventions consisted of a ballet class that utilized a pre-existing model of classical ballet modified for older adults, and a wellness class that served as a control intervention. The original intent of the study was to research in-person ballet classes, but due to COVID-19, the study moved entirely online well before the start of the study. The study was approved by the Washington University IRB and all participants gave written informed consent.
2.1 Participants
Older women aged 55 and above were recruited from local community centers, senior residences, and senior assistance organizations. Participants were recruited via flyers in two waves. Covariate adaptive randomization (Kang et al., 2008) counterbalancing for age was used to divide participants into two groups: a ballet class and a wellness class.
Recruitment was limited to women as they are at higher risk of frailty, hip fractures from falls, and physical inactivity than men (CDC, 2019). Additionally, women report higher anxiety and more depressive symptoms than men (Nair et al., 2021) and may therefore benefit more from interventions targeted at improving quality of life and mood.
In addition to the inclusion criteria of age and gender identity, participants needed to be able to walk independently with or without an assistive device for at least 5 min. Exclusion criteria were ballet training in the last 2 years; evidence of dementia (Mini-Mental Status Examination <24); language, visual, or hearing barriers to participation; and/or history of orthopedic or other medical problems that limit ability to participate safely in the intervention. To be included in the final analysis, participants needed to attend 70% (minimum 17 of 24) of the classes.
Sixty-five participants were recruited but 21 dropped out or had poor attendance due to extenuating factors during the pandemic including health reasons, caretaking responsibilities, and technology issues. Several people randomized to the wellness class dropped out before the classes started because they were displeased with their class placement. Attendance was taken daily; participants missed classes due to a range of conflicts such as work obligations, caretaking responsibilities, technology issues with Zoom, and vacations. Forty-four participants completed the intervention with enough classes to be included in the final analyses: ballet group (n = 21); wellness group (n = 23) (Table 1). The groups were well-matched in terms of baseline dance experience and mobility measured via gait speed. We made concerted effort to include participants from under-represented groups.; 20.45% (9/44) of the participants were non-white.
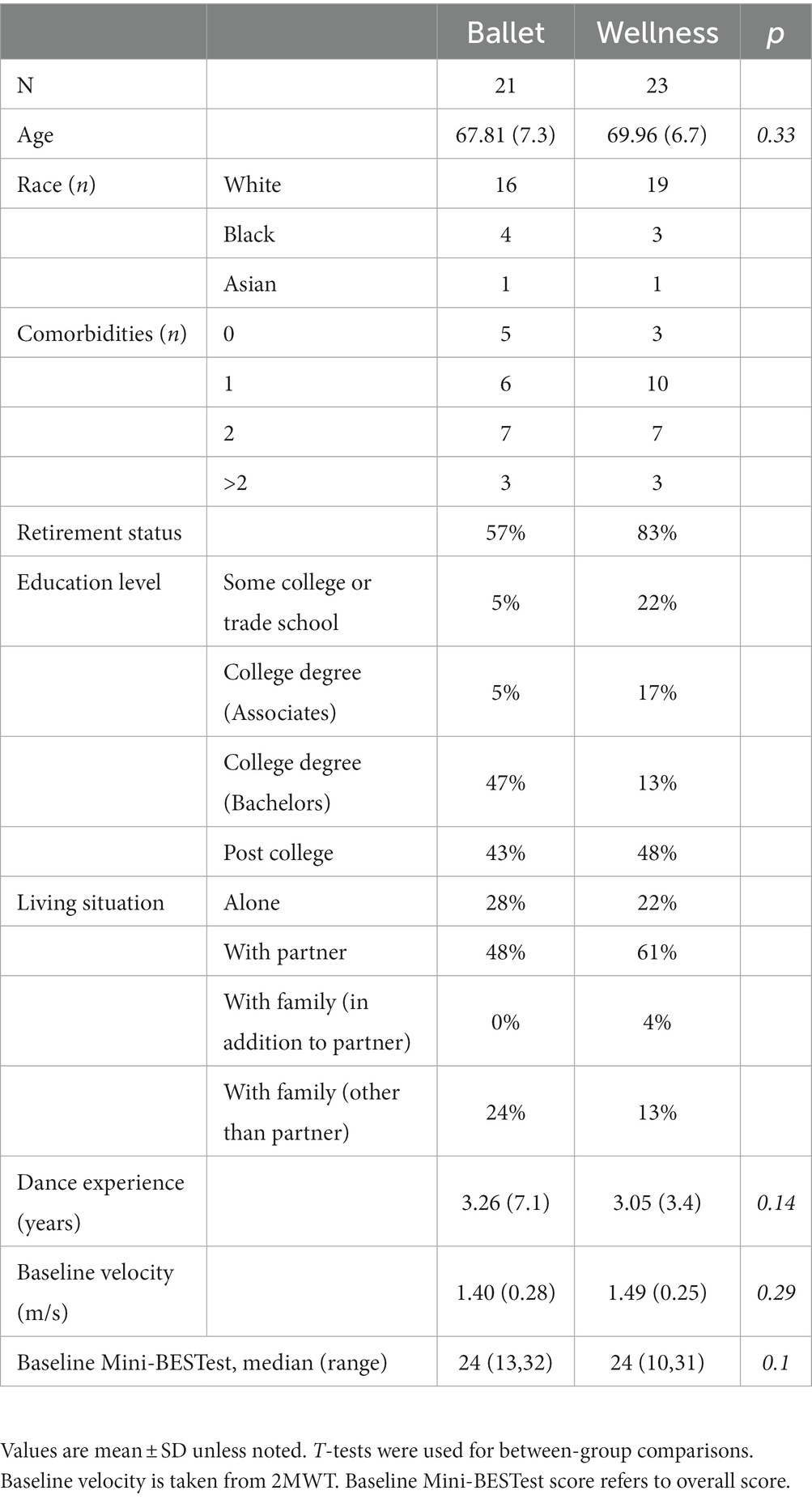
Table 1. Participant demographics.
2.2 Class structure
All classes were taught by a local organization, Vitality in Motion https://vitalityinmotion.com/, that offers high-quality, community-based ballet classes. Both groups received 12 weeks of online classes, in accordance with dosage recommendations for dance interventions (Hackney et al., 2007; Hackney and Earhart, 2009, 2010; Hwang and Braun, 2015). Both groups met two mornings per week over Zoom (Zoom Video Communications Inc., San Jose CA) for 45-min sessions, as is the standard length of Vitality in Motion classes.
The ballet classes followed conventional class formats utilizing ballet movement vocabulary and were set to classical music (Table 2). Classes were tailored to older populations and modified according to individual or group needs. Each class began with seated warm-up exercises that progressed to standing “barre work” using chairs for support. Some “center work” done in the middle of the room without the barre allowed participants to practice movement sequencing, memorization of steps, and expressive choreography while freely moving in space.
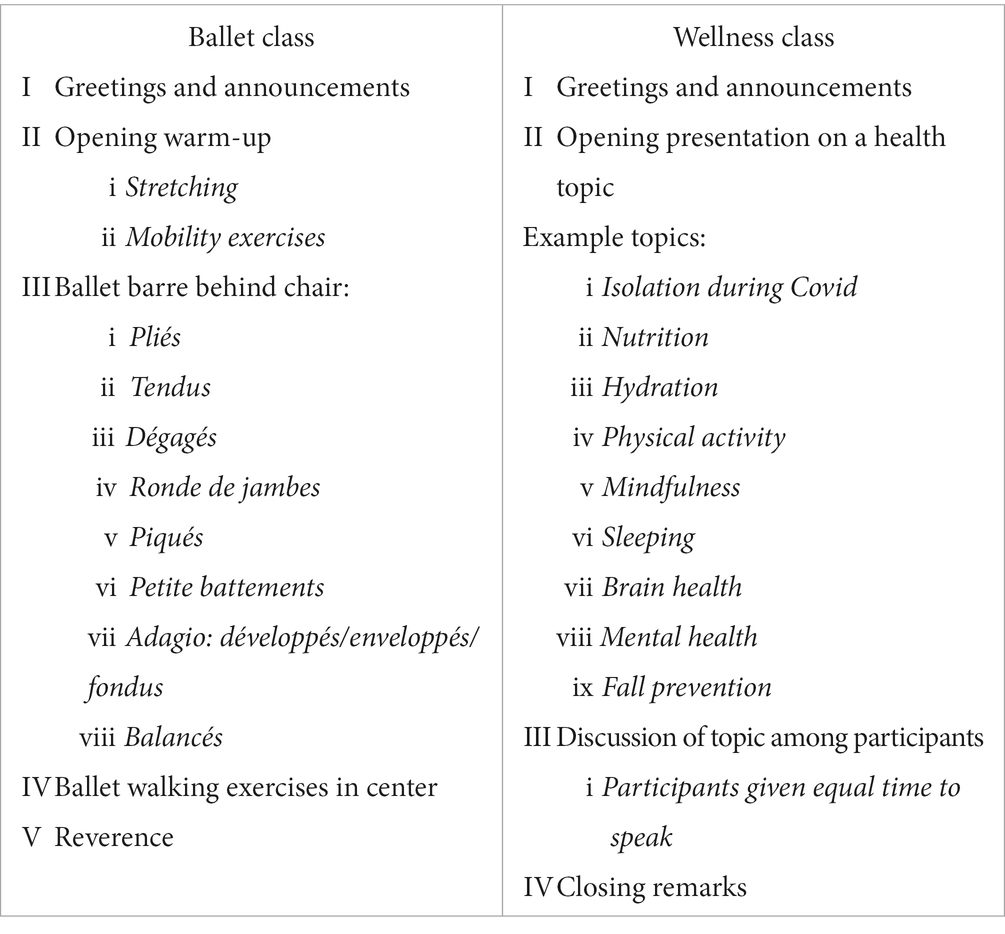
Table 2. Structure of ballet and wellness classes.
Modifications for virtual settings were intended to closely replicate the in-person class experience. Students were able to see and mimic the teacher’s movements throughout the class. There were no mirrors, but participants used their own cameras to provide visual feedback of their own performance. The online format via Zoom allowed for constant monitoring of bodies synchronizing in space, allowing for embodied interaction with others in real-time. A member of the research team was present to monitor each session and help participants with technology needs and ensure safety. To account for social interactions that typically occur during group classes, the monitor opened up the Zoom class 10 min early for participants to unmute and chat. We had no issues with Zoom during the classes. Some issues for individual participants did arise (i.e., not being able to connect to wifi, not being able to hear, not being able to find adequate space) and resulted in participants not being included in analyses.
The control intervention was selected as an active intervention that held steady variables such as class size, duration, socialization, and instructor demeanor but did not involve movement. We thought this a better comparison than utilizing a control condition that involved no intervention, which is often the default in early phase studies of movement interventions. The wellness classes (Table 2) were led by the same instructor as the ballet classes to control for any effect of the instructor’s demeanor or personality. In these education-based classes, participants discussed topics related to wellness and aging. No movements or exercises were performed during any of the wellness classes. Educational presentations were given each class by the instructor and followed with time for the participants to discuss their own experiences. This control comparator intervention was selected based on recommendations by an NIH expert panel on health-related behavioral interventions (Freedland et al., 2019).
2.3 Assessments
All participants underwent a comprehensive evaluation at two time points: pre-intervention and post-intervention. Evaluations occurred within 2 weeks of the start/end of classes. The same battery of assessments was used at both time points. Assessors were blinded to group assignment. As falls are multifactorial, commonly used assessments of gait and balance do not adequately predict fall risk in older adults in isolation (Omaña et al., 2021); therefore, multiple measures were assessed in this study.
The assessments consisted of motor and self-reported outcomes. During the motor exam, gait was captured during free walking using six wearable sensors (feet, wrists, sternum, lumbar) (APDM Mobility Lab, APDM Inc., Portland, OR). Sensors provided detailed information regarding spatiotemporal features of gait during the 2-min walk test (2MWT) and the 10-m walk test (10MWT). The 10MWT was assessed in four conditions, each performed three times: comfortable pace, fast as possible pace, dual-task (while doing a verbal cognitive task), and backward walking. Variables of interest included: stride velocity, stride length, and stride time as well as the coefficient of variation (CV) of stride velocity, stride length, and stride time.
Balance was assessed via the Mini Balance Evaluation Systems Test (Mini-BESTest), a well-validated tool that measures both static and dynamic balance, functional mobility, and gait (Marques et al., 2016). Postural sway during static balance tasks was measured via wearable sensors during single leg stance (SLS) performed twice on each leg in 30-s bouts. Balance variables were selected based on high validity and reliability and calculated within APDM software. These included duration, total sway area (computed as the area included in the acceleration per unit of time), jerk (smoothness of sway from time derivative of acceleration), mean velocity, and mean RMS (root mean square of the ACC time series). Greater static balance control is associated with higher duration (Baker et al., 2021) and lower sway area (Sohn et al., 2023), jerk (Mancini et al., 2012), mean velocity (Borysiuk et al., 2018), and mean RMS (Alsubaie, 2020). Additionally, self-reported balance confidence was measured via the Activities-Specific Balance Confidence Scale (ABC) (Schepens et al., 2010).
Sensors captured three trials of both the simple Timed Up-and-Go (TUG) and dual-task cognitive TUG (DT-TUG) in which participants subtracted backwards from 100 by threes. Dual task cost was calculated according to the following formulaw:
Questionnaires assessed quality of life [Short Form Health Survey (SF-36)] and mood [Geriatric Depression Scale (GDS)]. Self-reported fall frequency was reported at both time points and summated for the 3 months prior. Participant demographic information was also collected. Most common comorbidities reported were arthritis, high cholesterol, and hypertension.
Statistical analyses were conducted using IBM SPSS 27. We employed two-way repeated measures (RM) ANOVAs with group (ballet vs. wellness) and time (pre- vs. post-intervention) as factors to determine how the interventions impacted outcome variables. Fall rates were compared via logistic regression and the likelihood ratio was calculated via a Chi-square test. Post-hoc pairwise comparisons were used as appropriate, and Bonferroni corrections were used to correct for multiple comparisons. Statistical significance was set at p = 0.05.
3 Results
3.1 Gait results
In the 2MWT, there were main effects of time for velocity and stride length, which increased from pretest to posttest for both groups (Table 3). There was also a main effect for stride time which decreased for both groups.
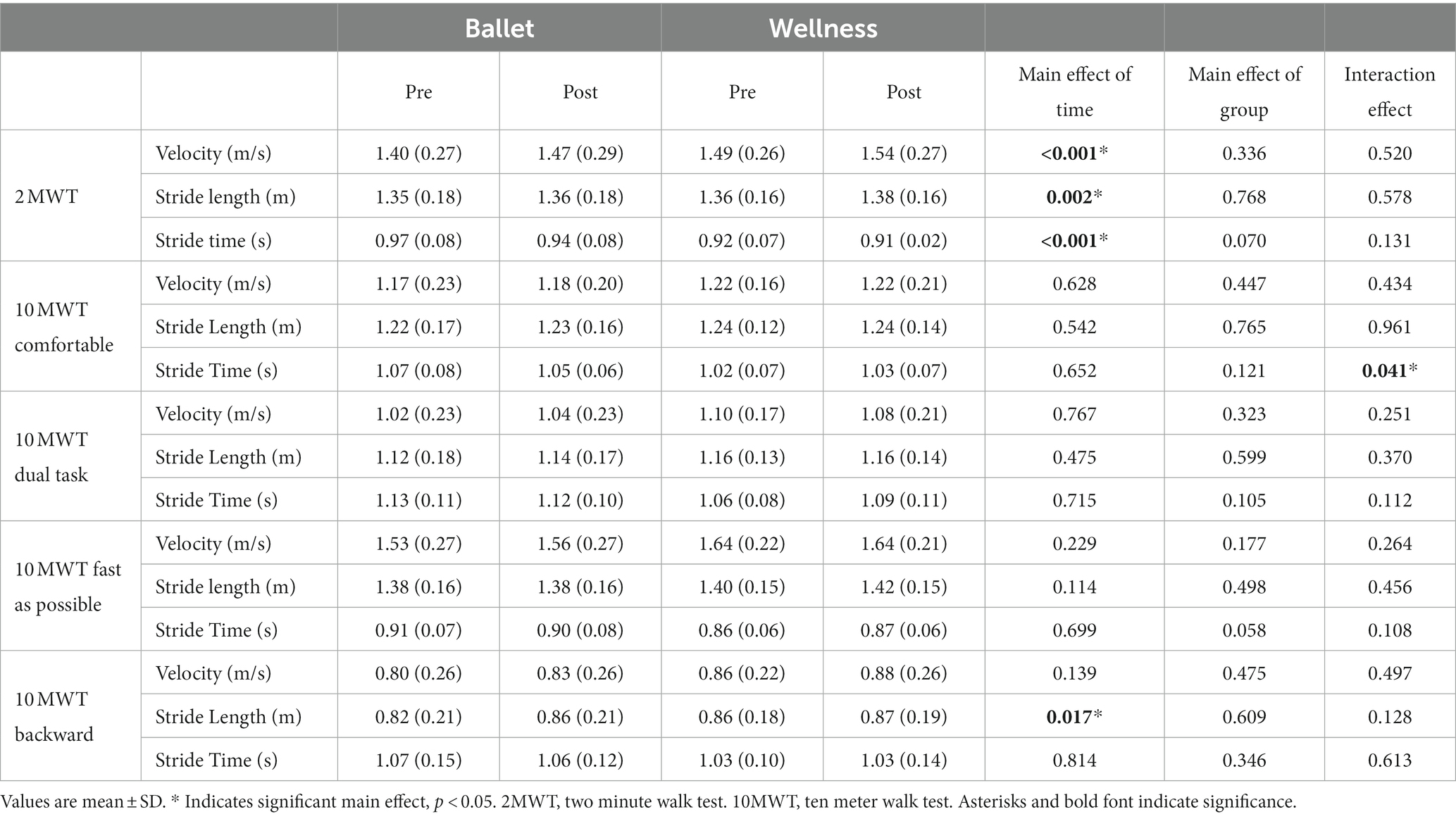
Table 3. Gait characteristics.
Among the 10MWT conditions, we observed one group x time interaction, which was for stride time in the 10MWT at a comfortable pace. Pairwise comparisons revealed that ballet participants reduced stride time (p = 0.029) whereas wellness participants increased it (p = 0.008). Additionally, for the main effect of time, stride length in the backward direction increased regardless of group.
3.2 Gait variability results
For gait variability in the 2MWT, there was a main effect of time showing an increase (i.e., worsening) in gait velocity variability (Table 4). An interaction effect showed that this was driven by the ballet group.
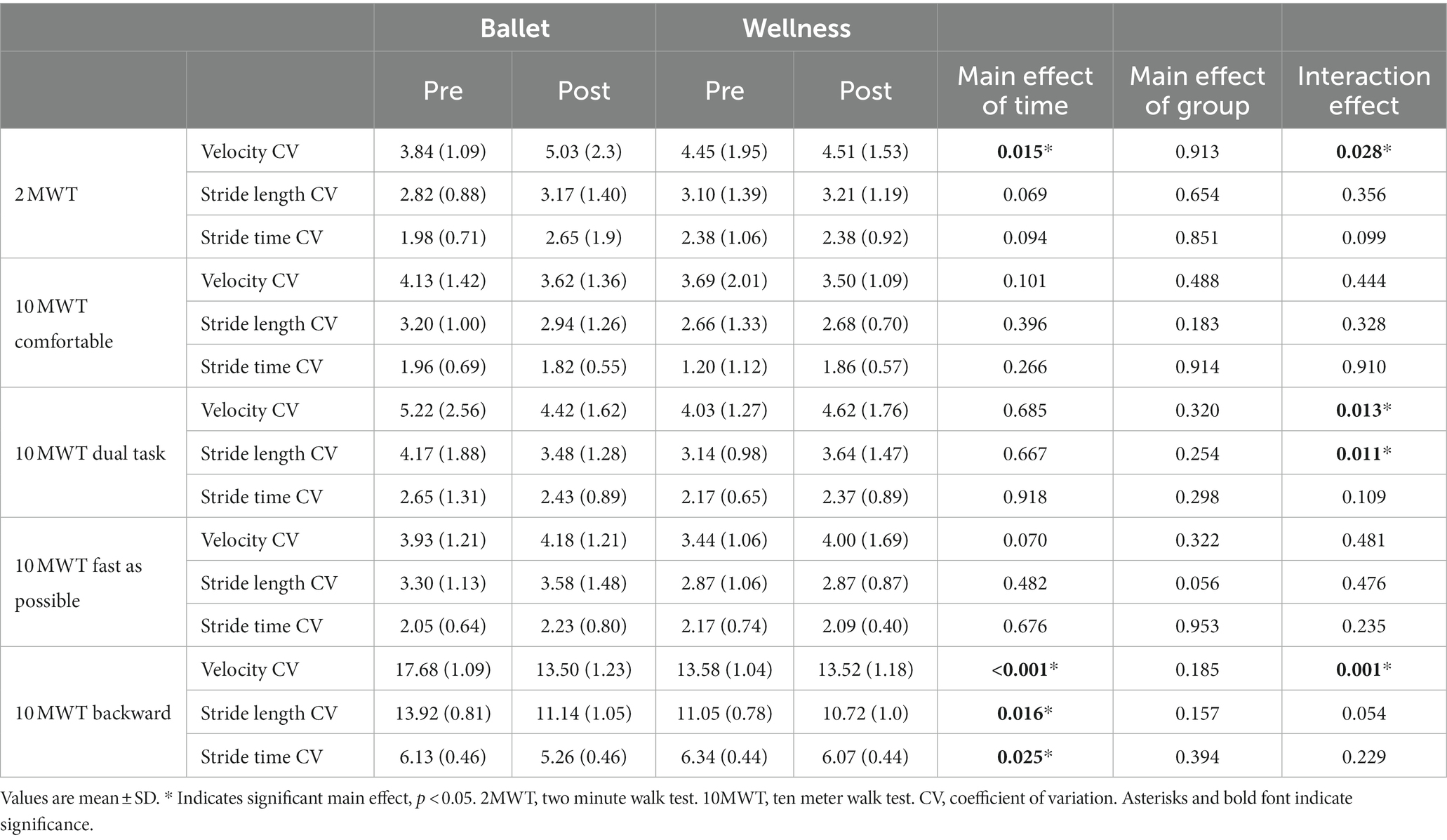
Table 4. Gait variabilities.
However, in the 10MWT, the ballet group showed the most improvement in the DT and backwards conditions. In the DT condition, there were group x time interactions for velocity CV and stride length CV revealing that ballet participants improved whereas wellness participants worsened. In the backward direction, main effects of time showed that both groups improved variability measures, including velocity CV, stride length CV, and stride time CV. There were no main effects of group, but a significant group x time interaction for velocity CV indicated that this improvement was driven by the ballet group.
3.3 Balance results
There was a main effect of time for scores on the Mini-BESTest (F1,42 = 38.15, p < 0.001) (Figure 1) and balance confidence as measured by the ABC (F1,42 = 10.69, p = 0.002). The ballet group increased Mini-BEST scores from a mean (range) of 24 (13,32) to 28 (18,32) and the wellness group increased 24 (10,31) to 28 (20,32). For balance confidence measured via the ABC, there was a main effect of time The group × time interaction trended toward significance (F2,41 = 3.86, p = 0.056) as the ballet group increased ABC scores from 86.57 (2.4) to 92.64 (1.57) while the wellness group increased from 89.99 (2.31) to 91.50 (1.50).
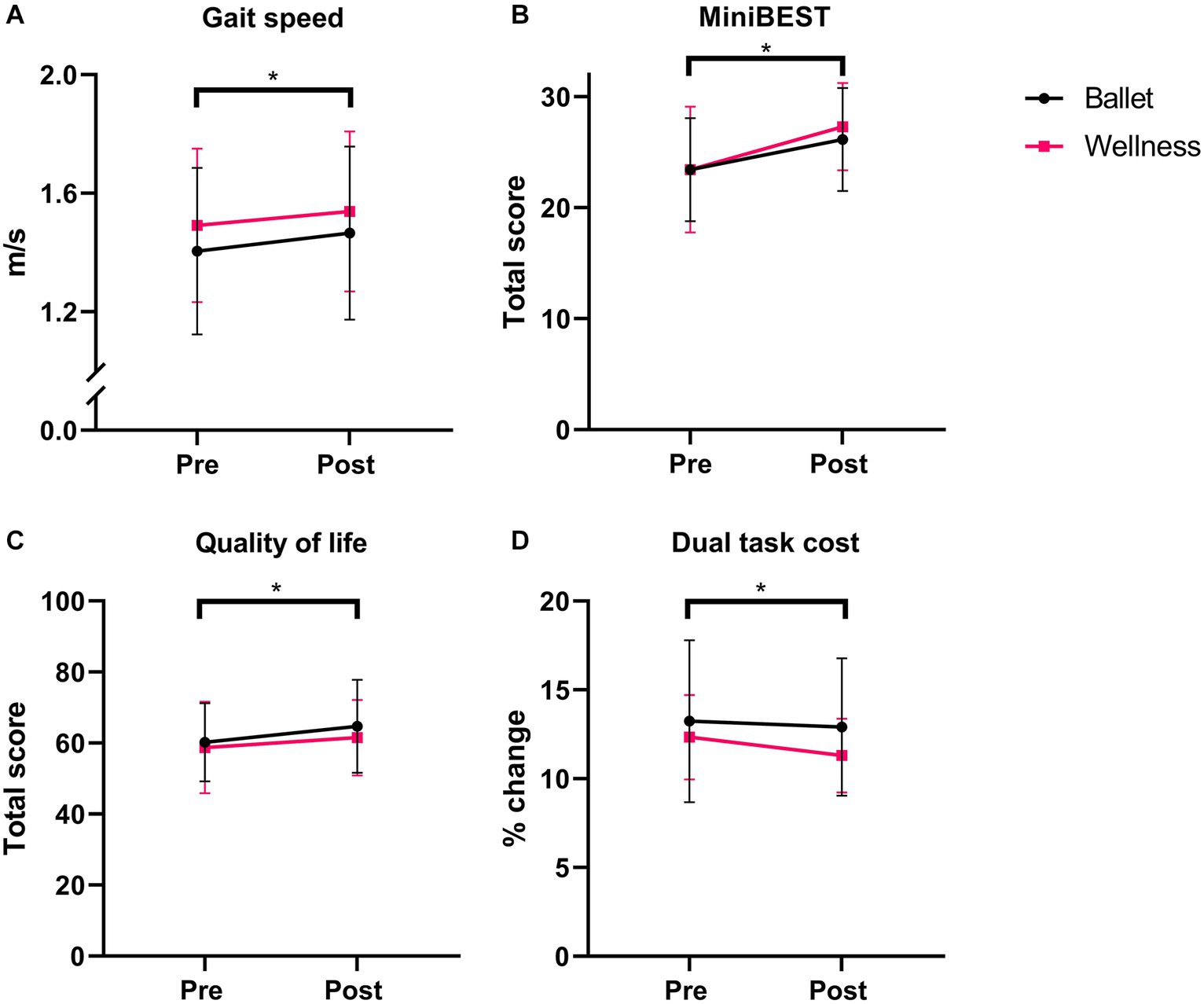
Figure 1. Key results pre- to post-intervention between groups. (A) Gait speed in 2MWT. (B) Mini-BESTest. (C) SF-36. (D) Dual Task Cost. * Indicates significance at p < 0.05.
Static balance also exhibited a main effect of time as measured by postural sway during single leg stance. From pretest to posttest, the duration that participants were able to hold a static standing posture in single leg stance (F1,42 = 12.69, p < 0.001) increased [Ballet: 12.48 s (8.45) to 15.85 s (8.53), Wellness: 14.20s (8.49) to 16.22 s (9.19)]. In single leg stance, RMS Acc (F1,42 = 5.11, p = 0.029) decreased over time, indicating more stability. There were no main effects of group.
There was no change in the TUG duration (p = 0.066), but there was a main effect of time for the DT-TUG duration (F1,42 = 4.279, p = 0.045), with the ballet group duration reducing from 14.23 s (±4.56) to 13.90s (±3.87) and the wellness group reducing from 13.33 s (±2.37) to 12.30s (±2.07). Dual task cost decreased from pretest to posttest (F1,42 = 4.744, p = 0.035) with no effect of group.
3.4 Fall rates
There was a significant effect of group on fall rates [χ2(1) = 5.096, p = 0.024], as ballet participants reduced fall rates from pretest to posttest (19 to 0%) whereas wellness participants increased fall rates (9–13%). When removing the covariate adjustment for participants’ baseline fall rates, a significant difference in posttest falls remains [χ2(1) = 4.092, p = 0.043].
3.5 Quality of life, mood, and class satisfaction
Both classes were associated with improvements in quality of life as measured by the SF-36 (F1,42 = 7.66, p = 0.008). Mood, as measured by the GDS, did not change significantly in either group (F1,42 = 3.45, p = 0.07) [Ballet: 5.29 (±0.21) to 4.95 (±0.19); Wellness: 5.17 (±0.20) to 4.96 (±0.182)].
The ballet group responded more positively in the post-intervention survey, with 71% of participants wishing to continue the classes compared to 47% of the wellness participants. Ballet participants reported that the classes improved strength, balance, and flexibility, that they were beneficial for daily activities, and that the classes made them “feel different,” “want to move again,” and inspired a “positive vibe.” Wellness participants gave feedback that they thought the classes were effective, enjoyable, and educational. Many noted a benefit of connecting with other women during a time of isolation due to COVID-19. Others noted that they became more grateful for their situations and learned to appreciate their health and communities.
4 Discussion
This study is among the first to explore the potential of virtual dance classes to benefit multiple domains of health. Our results show that both virtual ballet and wellness classes improved gait velocity, postural sway, and quality of life for older women. The ballet participants, however, improved more on complex, challenging tasks, such as dual-task walking and backward walking. Ballet classes seemed to be engaging and enjoyable, allowing people to creatively and artistically express agency and to connect kinesthetically with other women during a time of isolation. Wellness classes provided an outlet for informed knowledge-sharing while bonding with women at similar stages of life experience. The parallel improvements in quality of life and mobility highlight the importance of considering social engagement during both virtual and in-person movement therapies.
Ballet participants exhibited two notable improvements in gait variability, a known marker of fall risk, both in the most complex and attention-demanding walking paradigms: dual-task walking and backward walking. Dance is known to improve dual tasking, particularly in people with basal ganglia disorders like Parkinson disease (Kalyani et al., 2019). Ballet requires constant task-switching as people aim to remember combinations, integrate visual and auditory cues, perform complex movement patterns, and fulfill aesthetic goals. Significant reductions in variability in dual task and backward walking may reflect the potential of dance—and ballet, specifically—to train attention and focus during complex motor tasks, freeing up cognitive reserves for more successfully fulfilling the motor task. Such benefits may hold therapeutic meaning as challenging gait tasks require more cognitive reserve and frequently pose the greatest risk of falls (Verghese et al., 2002; Springer et al., 2006; Bayot et al., 2020). This explanation would support a recent study of young adult ballet dancers showing that ballet skills transfer to complex walking tasks such as walking across a narrow beam (Sawers and Ting, 2015).
In another complex motor task, the DT-TUG, which has been shown to discriminate fallers from non-fallers (Schoene et al., 2013), our participants’ (regardless of group) mean duration at baseline (13.78 s) surpasses a previously validated threshold of 13.5 s and suggests that many were within the range of fall risk (Steffen et al., 2002). The mean reduction to 13.06 s at posttest suggests that, overall, participants reduced indicators of fall risk. The improvement for both groups in dual task cost suggests that the interventions may have improved cognitive flexibility and adaptability during complex motor tasks, which could help people maintain postural control during tasks that divide attention and elicit falls (Verghese et al., 2002).
In terms of balance, improvements in the Mini-BESTest and ABC suggest global improvements in both objective and subjective stability. We expected ballet participants to improve both balance and balance confidence, confirming our hypotheses. However, wellness participants also improved in multiple domains of balance as well, which was unexpected. As the Mini-BESTest is negatively associated with fall prediction, the mean improvements for the ballet group of 2.4 and the wellness group of 3.1 are meaningful. A 1-point reduction in this test can increase the odds of a fall in the next 6 months by 14% for adults over the age of 60 and this percentage increases each decade (Magnani et al., 2020). Hence, our participants who improved their scores may have significantly reduced their risk of falls.
Static balance improved in only a few measures. Improvement in SLS duration and RMS acceleration are important as they correlate to reduced fall risk (Alqahtani et al., 2017; Omaña et al., 2021). Surprisingly, ballet participants had no better outcomes on static balance than wellness participants; however, this does confirm past findings that in-person ballet classes did not significantly alter postural stability during static poses (Weighart and DiPasquale, 2020). In previous work, this was attributed to an over-reliance on holding onto a ballet barre during class, which may not sufficiently challenge proprioceptive systems and therefore not alter performance on free-standing balance tasks (Weighart and DiPasquale, 2020). As we did not control for holding onto equipment, this may explain our similar results.
The ballet intervention successfully reduced falls while the wellness intervention did not. This corroborates past evidence that group exercise programs reduce falls whereas knowledge-based, educational interventions designed to reduce falls do not (Gillespie et al., 2021). The reduction of falls among ballet participants suggests that even small improvements in various domains of mobility and postural control may make a difference in everyday fall risk.
Both groups improved quality of life and spoke positively about the opportunity for virtual connection during a time of social isolation. As conversation time was built into the control intervention, wellness participants spent more time getting to know one another than ballet participants and may have developed bonds over shared experiences related to aging and health. Since the wellness class often showed parallel benefits to the ballet class, it is possible that the social outlet afforded during the wellness classes led to psycho-emotional benefits that translated to a global effect on motor outcomes.
Qualitatively, ballet participants reported higher class satisfaction and a stronger desire for the course to continue compared to the wellness participants. Their positive feedback emphasized the highly motivational nature of dance interventions, which may elicit deeper engagement than standard exercise (Earhart, 2009; Hwang and Braun, 2015). Participants in the ballet group also emphasized the importance of connecting creatively with other women, which highlights the interconnectedness of psycho-social–emotional wellbeing, artistic expression, and mobility (Kyrdalen et al., 2019). Lastly, they indicated that increasing mobility through engaging, expressive means gave them a sense of agency over both their physical and mental health. Such comments parallel a recent report that suggested that “the joyful, social, creative and expressive elements of dance are perhaps the precise reason for its efficacy within health contexts” (Introducing “Dance for Health”, 2020). Taken together, the success of the ballet intervention from the participants’ viewpoint further highlights the importance of considering psychosocial benefits of group movement-based interventions.
Several limitations to this study should be noted when interpreting the results. The high dropout rate reduced our sample size. The positive outcomes in the exit questionnaires could have been biased because they reflected the views of those who remained in the study. We chose the wellness class as a control intervention to provide similar social and attentional interactions but without a movement component. The control intervention did not involve movement so we cannot know how ballet classes would compare to other forms of exercise. Future studies could compare the ballet intervention to different movement-based interventions, but that was not the goal of this initial study. Lastly, some of the significant changes we saw were small and may not be clinically relevant.
5 Conclusion
This study is among the first to explore the effects of virtual ballet as a therapeutic intervention for older women. The results highlight the importance of social interaction as a key component when developing future interventions to target physical, mental, and psychosocial wellbeing in older adults, as well as the enjoyability of dance relative to other approaches. Future work should compare the effects of virtual and in-person movement classes, while accounting for the interaction between multiple domains related to brain and body health.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Washington University School of Medicine Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
EH: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AH: Investigation, Writing – review & editing. LT: Investigation, Writing – review & editing. SB: Investigation, Writing – review & editing. GE: Conceptualization, Funding acquisition, Investigation, Methodology, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This project was supported in part by an award from the Research Grants in the Arts program at the National Endowment for the Arts (NEA grant# 1880026-38-21) and by the National Institutes for Health training grant (T32-HD007434).
Acknowledgments
The authors gratefully acknowledge Vitality in Motion for class instruction, Martha Hessler for assistance with recruitment, Keith Lohse for statistical advice, and Serena Schein, Kate Bircher, and Abbie Tate for help with data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alqahtani, B. A., Ferchak, M. A., Huppert, T. J., Sejdic, E., Perera, S., Greenspan, S. L., et al. (2017). Standing balance and strength measurements in older adults living in residential care communities. Aging Clin. Exp. Res. 29, 1021–1030. doi: 10.1007/s40520-016-0693-4
Alsubaie, S. F. (2020). The postural stability measures most related to aging, physical performance, and cognitive function in healthy adults. Biomed. Res. Int. 2020:e5301534, 1–7. doi: 10.1155/2020/5301534
Araujo, C. G., de Souza e Silva, C. G., Laukkanen, J. A., Fiatarone Singh, M., Kunutsor, S. K., Myers, J., et al. (2022). Successful 10-second one-legged stance performance predicts survival in middle-aged and older individuals. Br. J. Sports Med. 56, 975–980. doi: 10.1136/bjsports-2021-105360
Baker, N., Gough, C., and Gordon, S. J. (2021). Inertial sensor reliability and validity for static and dynamic balance in healthy adults: a systematic review. Sensors 21:5167. doi: 10.3390/s21155167
Bayot, M., Dujardin, K., Dissaux, L., Tard, C., Defebvre, L., Bonnet, C. T., et al. (2020). Can dual-task paradigms predict falls better than single task? – a systematic literature review. Neurophysiol. Clin. 50, 401–440. doi: 10.1016/j.neucli.2020.10.008
Bek, J., Leventhal, D., Groves, M., Growcott, C., and Poliakoff, E. (2022). Moving online: experiences and potential benefits of digital dance for older adults and people with Parkinson’s disease. PLoS One 17:e0277645. doi: 10.1371/journal.pone.0277645
Borysiuk, Z., Konieczny, M., Kręcisz, K., Pakosz, P., and Królikowska, B. (2018). Effect of six-week intervention program on postural stability measures and muscle coactivation in senior-aged women. Clin. Interv. Aging 13, 1701–1708. doi: 10.2147/CIA.S167782
Bower, E. S., Wetherell, J. L., Petkus, A. J., Rawson, K. S., and Lenze, E. J. (2016). Fear of falling after hip fracture: prevalence, course, and relationship with one-year functional recovery. Am J Geriatr Psychiatry Off J Am Assoc Geriatr Psychiatry 24, 1228–1236. doi: 10.1016/j.jagp.2016.08.006
Britten, L., Addington, C., and Astill, S. (2017). Dancing in time: feasibility and acceptability of a contemporary dance programme to modify risk factors for falling in community dwelling older adults. BMC Geriatr. 17:83. doi: 10.1186/s12877-017-0476-6
CDC . Keep on your Feet. Centers for Disease Control and Prevention. Published December 19 (2019). Available at: https://www.cdc.gov/injury/features/older-adult-falls/index.html (Accessed April 16, 2020)
Cepeda, C. C. P., Lodovico, A., Fowler, N., and Rodacki, A. L. F. (2015). Effect of an eight-week ballroom dancing program on muscle architecture in older adults females. J. Aging Phys. Act. 23, 607–612. doi: 10.1123/japa.2014-0101
Cesari, M., Kritchevsky, S. B., Penninx, B. W., Nicklas, B. J., Simonsick, E. M., Newman, A. B., et al. (2005). Prognostic value of usual gait speed in well-functioning older people--results from the health, aging and body composition study. J. Am. Geriatr. Soc. 53, 1675–1680. doi: 10.1111/j.1532-5415.2005.53501.x
Christopher, N., and Tamplin, J. (2022). The use of Kinesthetic empathy with adults living with treatment resistant depression: a survey study. Am. J. Dance Ther. 44, 115–142. doi: 10.1007/s10465-022-09371-4
Clifford, A. M., Shanahan, J., McKee, J., Cleary, T., O’Neill, A., O’Gorman, M., et al. (2023). The effect of dance on physical health and cognition in community dwelling older adults: a systematic review and meta-analysis. Arts Health. 15, 200–228. doi: 10.1080/17533015.2022.2093929
Gillespie, L. D., Robertson, M. C., Gillespie, W. J., Sherrington, C., Gates, S., Clemson, L., et al. (2021). Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2021:CD007146. doi: 10.1002/14651858.CD007146.pub3
Coubard, O. A., Ferrufino, L., Nonaka, T., Zelada, O., Bril, B., and Dietrich, G. (2014). One month of contemporary dance modulates fractal posture in aging. Front. Aging Neurosci. 6:17. doi: 10.3389/fnagi.2014.00017
de Mello, M. C., de Sá, F. A., and Ramiro, F. L. (2017). Postural control during different unipodal positions in professional ballet dancers. J Dance Med Sci Off Publ Int Assoc Dance Med Sci. 21, 151–155. doi: 10.12678/1089-313X.21.4.151
Dewhurst, S., Peacock, L., and Bampouras, T. M. (2015). Postural stability of older female Scottish country dancers in comparison with physically active controls. J. Aging Phys. Act. 23, 128–132. doi: 10.1123/japa.2013-0050
Earhart, G. M. (2009). Dance as therapy for individuals with Parkinson disease. Eur. J. Phys. Rehabil. Med. 45, 231–238.
Earhart, G. M. (2013). Dynamic control of posture across locomotor tasks. Mov. Disord. 28, 1501–1508. doi: 10.1002/mds.25592
Eyigor, S., Karapolat, H., Durmaz, B., Ibisoglu, U., and Cakir, S. (2009). A randomized controlled trial of Turkish folklore dance on the physical performance, balance, depression and quality of life in older women. Arch. Gerontol. Geriatr. 48, 84–88. doi: 10.1016/j.archger.2007.10.008
Ferrufino, L., Bril, B., Dietrich, G., Nonaka, T., and Coubard, O. A. (2011). Practice of contemporary dance promotes stochastic postural control in aging. Front. Hum. Neurosci. 5:169. doi: 10.3389/fnhum.2011.00169
Freedland, K. E., King, A. C., Ambrosius, W. T., Mayo-Wilson, E., Mohr, D. C., Czajkowski, S. M., et al. (2019). The selection of comparators for randomized controlled trials of health-related behavioral interventions: recommendations of an NIH expert panel. J. Clin. Epidemiol. 110, 74–81. doi: 10.1016/j.jclinepi.2019.02.011
Gale, C. R., Cooper, C., and Aihie, S. A. (2016). Prevalence and risk factors for falls in older men and women: the English longitudinal study of ageing. Age Ageing 45, 789–794. doi: 10.1093/ageing/afw129
Granacher, U., Muehlbauer, T., Bridenbaugh, S. A., Wolf, M., Roth, R., Gschwind, Y., et al. (2012). Effects of a salsa dance training on balance and strength performance in older adults. Gerontology 58, 305–312. doi: 10.1159/000334814
Hackney, M. E., and Earhart, G. M. (2009). Effects of dance on movement control in Parkinson’s disease: a comparison of Argentine tango and American ballroom. J. Rehabil. Med. 41, 475–481. doi: 10.2340/16501977-0362
Hackney, M. E., and Earhart, G. M. (2010). Recommendations for implementing tango classes for persons with Parkinson disease. Am. J. Dance Ther. 32, 41–52. doi: 10.1007/s10465-010-9086-y
Hackney, M. E., Kantorovich, S., and Earhart, G. M. (2007). A study on the effects of Argentine tango as a form of partnered dance for those with Parkinson disease and the healthy elderly. Am. J. Dance Ther. 29, 109–127. doi: 10.1007/s10465-007-9039-2
Hausdorff, J. M., Rios, D. A., and Edelberg, H. K. (2001). Gait variability and fall risk in community-living older adults: a 1-year prospective study. Arch. Phys. Med. Rehabil. 82, 1050–1056. doi: 10.1053/apmr.2001.24893
Horak, F. B. (2006). Postural orientation and equilibrium: what do we need to know about neural control of balance to prevent falls? Age Ageing 35, ii7–ii11. doi: 10.1093/ageing/afl077
Hui, E., Chui, B. T., and Woo, J. (2009). Effects of dance on physical and psychological well-being in older persons. Arch. Gerontol. Geriatr. 49, e45–e50. doi: 10.1016/j.archger.2008.08.006
Hwang, P. W. N., and Braun, K. L. (2015). The effectiveness of dance interventions to improve older adults’ health: a systematic literature review. Altern. Ther. Health Med. 21, 64–70.
Introducing “Dance for Health” . International Association for Dance Medicine & science. (2020). Available at: https://www.iadms.org/blogpost/1177934/318259/Introducing-Dance-for-Health
Kalyani, H. H. N., Sullivan, K., Moyle, G., Brauer, S., Jeffrey, E. R., Roeder, L., et al. (2019). Effects of dance on gait, cognition, and dual-tasking in Parkinson’s disease: a systematic review and Meta-analysis. J. Parkinsons Dis. 9, 335–349. doi: 10.3233/JPD-181516
Kanekar, N., and Aruin, A. S. (2014). Aging and balance control in response to external perturbations: role of anticipatory and compensatory postural mechanisms. Age 36:9621. doi: 10.1007/s11357-014-9621-8
Kang, H. G., and Dingwell, J. B. (2008). Separating the effects of age and walking speed on gait variability. Gait Posture 27, 572–577. doi: 10.1016/j.gaitpost.2007.07.009
Kang, M., Ragan, B. G., and Park, J. H. (2008). Issues in outcomes research: an overview of randomization techniques for clinical trials. J. Athl. Train. 43, 215–221. doi: 10.4085/1062-6050-43.2.215
Kiefer, A. W., Riley, M. A., Shockley, K., Sitton, C. A., Hewett, T. E., Cummins-Sebree, S., et al. (2011). Multi-segmental postural coordination in professional ballet dancers. Gait Posture 34, 76–80. doi: 10.1016/j.gaitpost.2011.03.016
Kyrdalen, I. L., Thingstad, P., Sandvik, L., and Ormstad, H. (2019). Associations between gait speed and well-known fall risk factors among community-dwelling older adults. Physiother. Res. Int. 24:e1743. doi: 10.1002/pri.1743
Magnani, P. E., Genovez, M. B., Porto, J. M., Zanellato, N. F. G., Alvarenga, I. C., Freire, R. C., et al. (2020). Use of the BESTest and the Mini-BESTest for fall risk prediction in community-dwelling older adults between 60 and 102 years of age. J. Geriatr. Phys. Ther. 43, 179–184. doi: 10.1519/JPT.0000000000000236
Mancini, M., Salarian, A., Carlson-Kuhta, P., Zampieri, C., King, L., Chiari, L., et al. (2012). ISway: a sensitive, valid and reliable measure of postural control. J NeuroEngineering Rehabil. 9:59. doi: 10.1186/1743-0003-9-59
Marques, A., Almeida, S., Carvalho, J., Cruz, J., Oliveira, A., and Jácome, C. (2016). Reliability, validity, and ability to identify fall status of the balance evaluation systems test, Mini–balance evaluation systems test, and brief–balance evaluation systems test in older people living in the community. Arch. Phys. Med. Rehabil. 97, 2166–2173.e1. doi: 10.1016/j.apmr.2016.07.011
Muir-Hunter, S. W., and Wittwer, J. E. (2016). Dual-task testing to predict falls in community-dwelling older adults: a systematic review. Physiotherapy 102, 29–40. doi: 10.1016/j.physio.2015.04.011
Nair, S., Sawant, N., Thippeswamy, H., and Desai, G. (2021). Gender issues in the Care of Elderly: a narrative review. Indian J. Psychol. Med. 43, S48–S52. doi: 10.1177/02537176211021530
Oliveira, M. R., Vieira, E. R., Gil, A. W. O., Fernandes, K. B. P., Teixeira, D. C., Amorim, C. F., et al. (2018). One-legged stance sway of older adults with and without falls. PLoS One 13:e0203887. doi: 10.1371/journal.pone.0203887
Omaña, H., Bezaire, K., Brady, K., Davies, J., Louwagie, N., Power, S., et al. (2021). Functional reach test, single-leg stance test, and Tinetti performance-oriented mobility assessment for the prediction of falls in older adults: a systematic review. Phys. Ther. 101, 1–18. doi: 10.1093/ptj/pzab173
Pacheco, E., Hoyos, D. P., Watt, W. J., Lema, L., and Arango, C. M. (2016). Feasibility study: Colombian Caribbean folk dances to increase physical fitness and health-related quality of life in older women. J. Aging Phys. Act. 24, 284–289. doi: 10.1123/japa.2015-0012
Piche, E., Chorin, F., Gerus, P., Jaafar, A., Guerin, O., and Zory, R. (2023). Effects of age, sex, frailty and falls on cognitive and motor performance during dual-task walking in older adults. Exp. Gerontol. 171:112022. doi: 10.1016/j.exger.2022.112022
Sawers, A., and Ting, L. H. (2015). Beam walking can detect differences in walking balance proficiency across a range of sensorimotor abilities. Gait Posture 41, 619–623. doi: 10.1016/j.gaitpost.2015.01.007
Schepens, S., Goldberg, A., and Wallace, M. (2010). The short version of the activities-specific balance confidence (ABC) scale: its validity, reliability, and relationship to balance impairment and falls in older adults. Arch. Gerontol. Geriatr. 51, 9–12. doi: 10.1016/j.archger.2009.06.003
Schoene, D., Wu, S. M. S., Mikolaizak, A. S., Menant, J. C., Smith, S. T., Delbaere, K., et al. (2013). Discriminative ability and predictive validity of the timed up and go test in identifying older people who fall: systematic review and meta-analysis. J. Am. Geriatr. Soc. 61, 202–208. doi: 10.1111/jgs.12106
Shigematsu, R., Chang, M., Yabushita, N., Sakai, T., Nakagaichi, M., Nho, H., et al. (2002). Dance-based aerobic exercise may improve indices of falling risk in older women. Age Ageing 31, 261–266. doi: 10.1093/ageing/31.4.261
Sofianidis, G., Dimitriou, A. M., and Hatzitaki, V. (2017). A comparative study of the effects of Pilates and Latin dance on static and dynamic balance in older adults. J. Aging Phys. Act. 25, 412–419. doi: 10.1123/japa.2016-0164
Sofianidis, G., Hatzitaki, V., Douka, S., and Grouios, G. (2009). Effect of a 10-week traditional dance program on static and dynamic balance control in elderly adults. J. Aging Phys. Act. 17, 167–180. doi: 10.1123/japa.17.2.167
Sohn, J., Park, S-H., and Kim, S. Effects of DanceSport on walking balance and standing balance among the elderly - IOS press. (2023). Available at: https://content.iospress.com/articles/technology-and-health-care/thc174760
Springer, S., Giladi, N., Peretz, C., Yogev, G., Simon, E. S., and Hausdorff, J. M. (2006). Dual-tasking effects on gait variability: the role of aging, falls, and executive function. Mov Disord Off J Mov Disord Soc. 21, 950–957. doi: 10.1002/mds.20848
Steffen, T. M., Hacker, T. A., and Mollinger, L. (2002). Age- and gender-related test performance in community-dwelling elderly people: six-minute walk test, berg balance scale, timed up & go test, and gait speeds. Phys. Ther. 82, 128–137. doi: 10.1093/ptj/82.2.128
Tanabe, H., Fujii, K., and Kouzaki, M. (2014). Inter- and intra-lower limb joint coordination of non-expert classical ballet dancers during tiptoe standing. Hum. Mov. Sci. 34, 41–56. doi: 10.1016/j.humov.2013.12.003
Verghese, J. (2006). Cognitive and mobility profile of older social dancers. J. Am. Geriatr. Soc. 54, 1241–1244. doi: 10.1111/j.1532-5415.2006.00808.x
Verghese, J., Buschke, H., Viola, L., Katz, M., Hall, C., Kuslansky, G., et al. (2002). Validity of divided attention tasks in predicting falls in older individuals: a preliminary study. J. Am. Geriatr. Soc. 50, 1572–1576. doi: 10.1046/j.1532-5415.2002.50415.x
Wallmann, H. W., Gillis, C. B., Alpert, P. T., and Miller, S. K. (2009). The effect of a senior jazz dance class on static balance in healthy women over 50 years of age: a pilot study. Biol. Res. Nurs. 10, 257–266. doi: 10.1177/1099800408322600
Keywords: dance, mobility, kinesthetic empathy, dual task, socialization, ballet
Citation: Harrison EC, Haussler AM, Tueth LE, Baudendistel ST and Earhart GM (2024) Graceful gait: virtual ballet classes improve mobility and reduce falls more than wellness classes for older women. Front. Aging Neurosci. 16:1289368. doi: 10.3389/fnagi.2024.1289368
Edited by:
Aline Nogueira Haas, Federal University of Rio Grande do Sul, BrazilReviewed by:
Madeleine E. Hackney, Emory University, United StatesCarlos Cristiano Espedito Guzzo Junior, Federal University of Rio Grande do Sul, Brazil
Copyright © 2024 Harrison, Haussler, Tueth, Baudendistel and Earhart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gammon M. Earhart, ZWFyaGFydGdAd3VzdGwuZWR1