 Carol A. Holland1,2*†
Carol A. Holland1,2*† Nikolett Dravecz1,2
Nikolett Dravecz1,2 Susan Broughton1,3
Susan Broughton1,3 Lynne A. Barker4
Lynne A. Barker4 Fidelia Bature5
Fidelia Bature5 Charlotte Clarke6
Charlotte Clarke6 Isaac M. Danat7
Isaac M. Danat7 Sayani Das8
Sayani Das8 Irundika H. K. Dias9Annabel Dawson10M. Dixon11
Irundika H. K. Dias9Annabel Dawson10M. Dixon11 Amanda Ellison12
Amanda Ellison12 David Façal13Roland Finch10
David Façal13Roland Finch10 Christopher J. Gaffney1,14
Christopher J. Gaffney1,14 Alan Gow15
Alan Gow15 Eirini Kelaiditi16
Eirini Kelaiditi16 Andrzej Klimczuk17
Andrzej Klimczuk17 Esperanza Navarro-Pardo18Pheobe Sharratt1,14
Esperanza Navarro-Pardo18Pheobe Sharratt1,14 Andrew Sixsmith19
Andrew Sixsmith19 Claudia K. Suemoto20
Claudia K. Suemoto20 Lalu Suprawesta21
Lalu Suprawesta21 Tamlyn Watermeyer22
Tamlyn Watermeyer22 Sally Fowler Davis23†
Sally Fowler Davis23†- 1Centre for Ageing Research (C4AR), Lancaster University, Lancaster, United Kingdom
- 2Division of Health Research, Lancaster University, Lancaster, United Kingdom
- 3Division of Biomedical and Life Sciences, Lancaster University, Lancaster, United Kingdom
- 4Sheffield Institute of Social Science, College of Social Science and Art, Sheffield Hallam University, Sheffield, United Kingdom
- 5Institute of Health Research, University of Bedfordshire, Luton, United Kingdom
- 6Wolfson Institute for Health & Wellbeing, Durham University, Durham, United Kingdom
- 7Sheffield Institute of Social Sciences, College of Social Sciences and Arts, Sheffield Hallam University, Sheffield, United Kingdom
- 8Department of Social Work, Bar-Ilan University, Ramat Gan, Israel
- 9Aston Medical School and Aston Research Centre for Health in Ageing, Aston University, Birmingham, United Kingdom
- 10Lay Contributor, Newcastle, United Kingdom
- 11Northern Health Science Alliance (NHSA), Manchester, United Kingdom
- 12Department of Psychology, Durham University, Durham, United Kingdom
- 13Department of Developmental and Educational Psychology, and Institute of Psychology, University of Santiago de Compostela, Santiago de Compostela, Spain
- 14Lancaster Medical School, Lancaster University, Lancaster, United Kingdom
- 15Department of Psychology, Heriot-Watt University, Edinburgh, United Kingdom
- 16Faculty of Sport, Technology and Health Sciences, St Mary's University Twickenham, London, United Kingdom
- 17SGH Warsaw School of Economics, Warsaw, Poland
- 18Department of Developmental and Educational Psychology, University of Valencia, Valencia, Spain
- 19Department of Gerontology, STAR Institute, Simon Fraser University, Vancouver, BC, Canada
- 20Division of Geriatrics, Universidade de São Paulo, São Paulo, Brazil
- 21Department of Health and Sport Education, Faculty of Sport Science and Public Health, Mandalika Education University, Mataram, Indonesia
- 22Department of Psychology, Northumbria University, Newcastle upon Tyne, United Kingdom
- 23School of Allied Health and Social Care, Anglia Ruskin University, Cambridge, United Kingdom
Introduction: The conjunction of physical frailty and cognitive impairment without dementia is described as Cognitive Frailty (CF). Indications that CF is potentially reversible have led to proposals that risk factors, symptoms or mechanisms of CF would be appropriate targets for interventions for prevention, delay or reversal. However, no study has brought experts together across sectors to determine targets, content or mode of interventions, and most resources on interventions are from the perspective of academic or clinical researchers only. This international Delphi consensus study brings together experts from academic and clinical research, lay people with lived experience of CF, informal carers, and professional care practitioners/clinicians.
Methods: Three rounds of Delphi study were held to discern which factors and statements were agreed upon by the whole sample and which generated different views in those with differing expertise. A scoping review and Round 1 (29 participants) were used to gather initial statements. In Round 2, 58 people responded to statements and open text items, comprising 7 lab-based researchers, 27 researchers working with people, 14 people with lived experience or informal family carers, and 10 professional carers/clinicians. Percent agreement and qualitative responses were analyzed to provide a final set of statements which were checked by 38 respondents in Round 3.
Results: Analysis of Round 2 quantitative data provided 74 statements on which there was at least 70% agreement and qualitative data produced a further 24 statements. These were combined to provide 90 statements for Round 3. There was Consensus for 89 of the statements. A few differences between the groups were observed at both stages.
Discussion and conclusion: The consensus for statements associated with CF interventions provides a useful first step in defining health promotion activities and interventions. Given the prevalence and potential disability caused by CF in older populations, the consensus statements represent expert opinion that is inter-sectoral and will inform public health policies to support implementation of evidence-based prevention and intervention plans. This study is an important step toward changing current approaches, by including all stakeholders from the outset. Outcomes can be used to feed into co-creation of interventions for cognitive frailty.
Introduction
Cognitive frailty (CF) is a condition defined as an age-related conjunction of physical frailty and cognitive impairment without dementia (Kelaiditi et al., 2013). Research on CF is growing, indicating, for example, that distinguishing the cognitive impairments and any neuropathological changes shown in CF from neurodegeneration associated with early dementia is essential (Bunce et al., 2019; Façal et al., 2019). This is important because CF is described as a state in which there is an increased risk for eventual dementia and loss of independent function, but also because it has been described as reversible, or potentially reversible (Ruan et al., 2020; Ruan et al., 2015). In the current absence of a cure for dementia, increasing prevention efforts is essential. That CF is a potentially reversible syndrome has led to the proposal that addressing risk factors, symptoms or mechanisms of either cognitive impairment or physical frailty, or importantly, the mechanisms associated with the link between the two, would be appropriate targets for intervention to prevent, delay or reverse it (see also Holland et al., 2024). Importantly, this highlights CF not just as a problem that may grow with increasing older populations, but as an important opportunity for healthy aging. However, despite the development of our understanding, CF remains poorly addressed as a target for intervention and perhaps poorly understood amongst the range of people with different kinds of expertise and experience in this area.
Physical frailty has been defined as (i) a physical phenotype (Fried et al., 2001) in which a frail state is the presence of three or more of five characteristics of physical weakness (slow gait speed, self-reported exhaustion, muscle weakness, low physical activity and unintended weight loss); and (ii) by an accumulation of deficits approach, or frailty index (Rockwood and Mitnitski, 2007). Both definitions relate to a recognized syndrome characterized as a state of increased vulnerability to adverse health outcomes when exposed to a stressor (Clegg et al., 2013). Underlying biological changes influence homeostatic mechanisms and absence of physiological resilience, including muscle wasting, metabolic deficits, cardiovascular disease, inflammatory symptoms and oxidative stress. The presence of both cognitive impairment and physical frailty may exacerbate vulnerability to adverse health outcomes, underscoring the need for integrated interventions targeting the unique mechanisms of cognitive frailty,
Cognitive Impairment No Dementia (CIND), the level of cognitive impairment at the focus of CF, has been defined in various ways, but the 2013 consensus exercise (Kelaiditi et al., 2013) suggested a Clinical Dementia Rating (CDR) of 0.5 (equivalent to “very mild” observed impairment). Other literature has emphasized an equivalence with the Mild Cognitive Impairment (MCI) range on global tests of cognition such as the Mini Mental State Exam (MMSE; Folstein et al., 1975) or Montreal Cognitive Assessment (MOCA, Nasreddine et al., 2005), or a combination of tests of specific cognitive domains such as verbal memory or executive function e.g., (see Façal et al. (2019) for a review) and others have emphasized subjective cognitive decline, particularly for a reversible level of CF (Ruan et al., 2015). Nevertheless, the key defining feature of CF, is that the cognitive impairment is in conjunction with physical frailty.
Development of interventions for physical frailty (e.g., Apostolo et al., 2018) and interventions for mild cognitive decline (e.g., Levy et al., 2022) have received significant attention. To date and to our knowledge, there are no agreed pathways for intervention for CF. Several reviews have been published examining interventions for CF, focusing on different mixes of intervention targets: physical exercise interventions (Li et al., 2022); a mixture of cognitive training, nutrition education, behavioral intervention, mind–body intervention, psychosocial support, and virtual reality but all with a component of physical activity (Tam et al., 2022); physical activity, nutrition or multidomain interventions (Zheng et al., 2022); nutrition only, with a focus on anti-oxidants (Gomez-Gomez and Zapico, 2019); and multidimensional and potentially personalized interventions (Sugimoto et al., 2022). However, no study has sought cross-disciplinary expertise to discuss the potential for interventions or brought together expertise and opinions on what might work in terms of targeted outcomes and structures of interventions. Importantly, published resources on interventions are primarily from the perspective of academic or clinical researchers, and lack the perspective of those with lived experience, e.g., informal carers and people with CF.
The objective of this study was to conduct an international Delphi consensus study bringing together experts from a range of academic and clinical research backgrounds, while also ensuring the involvement of experts by experience: lay people with lived experience of CF themselves; informal (family) carers; and professional health and social care practitioners. Hsu and Sandford (2007) defined a Delphi consensus as “a group communication process which aims to achieve a convergence of opinion on a specific real-world issue.” Delbecq et al. (1975) described the different potential objectives of a Delphi process which include: exploring or exposing underlying assumptions or information that may lead to different judgments; seeking information that may generate consensus amongst participants; and finding linkages between different judgments in a topic that spans a range of disciplines. Delphi techniques are considered to provide the lowest level of evidence for making causal inferences, i.e., subordinate to meta-analyses and intervention studies (Liu, 2022) but are appropriate particularly for consumer review in guideline development and in relation to complex issues where knowledge is uncertain (Linstone and Turoff, 2002). Importantly, the process is iterative in which a series of questionnaires can be used so that each member can contribute independently, and anonymously, and each round is a controlled feedback process of the information gained in the previous round, reducing the possibility of bias or undue influence of some experts, especially where there is a perceived power imbalance.
Methodological sources suggest that a mix of experts provides clearer face validity for any consensus achieved (e.g., Nair et al., 2011), particularly where the motivation of end users may be a key component of potential outcomes – the interventions in this case. This mix of experts was chosen to ensure that consensus on what might work in terms of scientific evidence was combined with what might work for people who may be the recipients, beneficiaries and those who may deliver the interventions.
The use of ‘experts’ is fundamental to the reliability of the outcome and rigour is associated with selection of the experts (Baker et al., 2006). Nevertheless, it was also recognized that understanding in some areas, notably biological, pharmacological, medical and neuroscience mechanisms, may be less well-developed within the range of experts included. Therefore, in addition to seeking overall consensus across the participants as in a traditional Delphi study, we also aimed to determine whether there were any significant differences between the different groups of participants.
Thus, the aims of this Delphi study were to:
i. Develop consensus among experts across disciplines and sectors, including people with lived experience, in relation to understanding of cognitive frailty and appropriate interventions for it.
ii. Examine differences in consensus between groups with different disciplinary backgrounds and lived experience.
Methods
The process included three rounds to achieve expert consensus on sub-components of interventions, as follows:
• Understanding of what CF is, whether it is preventable, could be delayed, or could be reversible;
• possible mechanisms or approaches for interventions, and target foci for interventions;
• any restrictions on for whom interventions for CF may or may not be relevant;
• screening for CF;
• factors that may affect the feasibility or likelihood of adherence to interventions, including effects of infrastructure, accessibility or personal circumstances on feasibility of interventions;
• potential targeted primary and secondary outcomes;
• factors in the design of interventions that may influence effectiveness;
• and any other design factors.
Following an initial literature search activity as part of a scoping review, (Holland et al., 2024), three Delphi rounds were held. Ethical approval was granted in advance by Lancaster University Faculty of Health and Medicine Ethical Committee (REF FHM-2022-1092-RECR-1) and updated using amendments as the survey was developed for each round (FHM-2023-1092-SA-1).
Round 1
The first round was completed as an event at an online Cognitive Frailty Interdisciplinary Network (CFIN) conference in September, 2023. Open questions based on the scoping work (Holland et al., 2024) were presented on a shared electronic notepad (“Padlet”) which participants discussed in small groups and contributed text answers within their groups. Twenty-nine experts who had mostly presented their own work in the area of cognitive frailty at the conference, including experts in psychology, neuropsychology, sociology, basic lab based biological sciences and physiology took part in the exercise, alongside two lay members of the network external advisory group (people with lived experience or with professional or informal carer expertise). All those who wanted to participate were given a participant information sheet and consent form which ensured they were aware that responses would be anonymous, but contact details would be separately retained to invite them to the second round.
Round 2
The second round consisted of an on-line survey based on responses to Round 1 distilled into a set of 127 items suitable for rating as agree/disagree, or ranking, according to the question, plus open text boxes. The items were converted into a questionnaire which was developed as an online Qualtrics questionnaire and reviewed by the chair of the advisory group. The list of items can be seen in the Supplementary Materials 1. Agree/disagree items were to be answered using a 5-point Likert scale, from strongly agree to strongly disagree. Ranked items consisted of a series of elements to be ranked in order of importance. The set of items included all contributions from Round 1 with none excluded at this stage.
To extend the participant group of experts the following actions were taken:
i. All members of CFIN who had not taken part in Round 1 were invited;
ii. Further published experts were invited;
iii. Members of the VOICE1 network of older citizens were invited specifically to increase the numbers of people with lived experience of CF themselves or experience of caring for people with CF.
Fifty-eight participants took part in Round 2, with 46 completing all questions. Partial responses were included in the analysis and numbers responding to each item are given in the analysis below. All interested individuals were provided with participant information sheets and consent forms via email. Participants were then sent the link to the questionnaire and asked to complete it online. At the end of the questionnaire, participants were asked to provide contact details so they could be involved in a further round and/or in writing or editing this report.
Analysis for Round 2
Based on a previous Delphi process in this area (Sezgin et al., 2022) and on recommendations from Nair et al. (2011) an agreement level of 70% was applied to agree/disagree questions. That is, responses rated “somewhat agree” or “strongly agree,” or, strongly disagree” or “somewhat disagree” by ≥70% of participants were accepted unless there was a sizeable opposite proportion, i.e., “strongly disagree” and “somewhat disagree” or “strongly agree” and “somewhat agree” by more than 15%. Participants who responded that any question was outside of their expertise were excluded from the percentage calculations for that item. For ranking questions, mean ranks for each item were calculated and a median overall mean rank or above was determined as demonstrating consensus. Friedman’s non-parametric test for ranked data was applied to test the null hypothesis of no difference in mean ranks across the items (that is, the hypothesis of no consensus on higher and lower ranks of items).
Following analyses of respondents as a whole, respondents were separated into groups in terms of their different types of work or association to CF based on their own descriptions of their expertise or interest in CF: laboratory-based researchers; researchers who worked directly with older people with CF or data relating to them; health and social care practitioners who worked with people with CF; and people with lived experience either as informal (usually family) carers or people self-declaring as experiencing CF themselves. Grouping participants by expertise allowed for an analysis of consensus differences based on professional or personal perspectives, providing insights into how lived experiences and disciplinary backgrounds influence cognitive frailty intervention priorities. Independent samples Kruskal-Wallis tests were used to examine whether there were any differences in the distribution of ranks for each intervention between the groups, with Bonferroni adjustments made for multiple comparisons.
Qualitative responses (open text boxes) were subjected to thematic analysis (Brady, 2015) that identified additional priorities, gaps in understanding and additional issues of importance (Shang, 2023) and put them into the format of further statements. This enabled a ‘sense check’ for the development of further statements, with qualitative outcomes synthesized with the quantitative item outcomes and formulated into a number of statements that could be incorporated into appropriate sections of Round 3 of the survey.
Round 3
All statements that had achieved consensus or had been added from the qualitative analysis were formatted into items that could be answered using the strongly agree to strongly disagree scale outlined above (that is, previously highly ranked items were re-formatted into agree-disagree statements). This was emailed to all participants from Round 2 who had agreed to be contacted again.
For the third round, the group of experts were again divided into four groups as in Round 2, but with people asked to indicate the group themselves as opposed to the researchers allocating based on participant descriptions. In addition, country, perspective (e.g., academic researcher), education, role, discipline, was also requested while still allowing the respondent to remain anonymous.
Analysis plan for Round 3
The same ≥70% agreement and ≤15% disagreement criteria for consensus were applied, excluding those who noted the question was outside their expertise. Analyses were conducted with the whole sample, as well as with respondents grouped by expertise.
Results
Initial contributions to the Padlet in Round 1 were synthesized into items for the questionnaire in Round 2.
Round 2
Participants
Fifty-eight people completed the survey in Round 2. The first question asked about their experience with CF. Several identified themselves in more than one category (e.g., having cared for a family member with CF but also experiencing it themselves; being a healthcare professional (clinician) and a researcher; being a researcher but also caring for a family member). Figure 1 shows all these self-identifications and so the total frequency is greater than the number of people. The most frequent types of experience identified were as researchers and as unpaid, or family, carers. One respondent said they had no experience or expertise of any nature with CF and were excluded from the analysis.
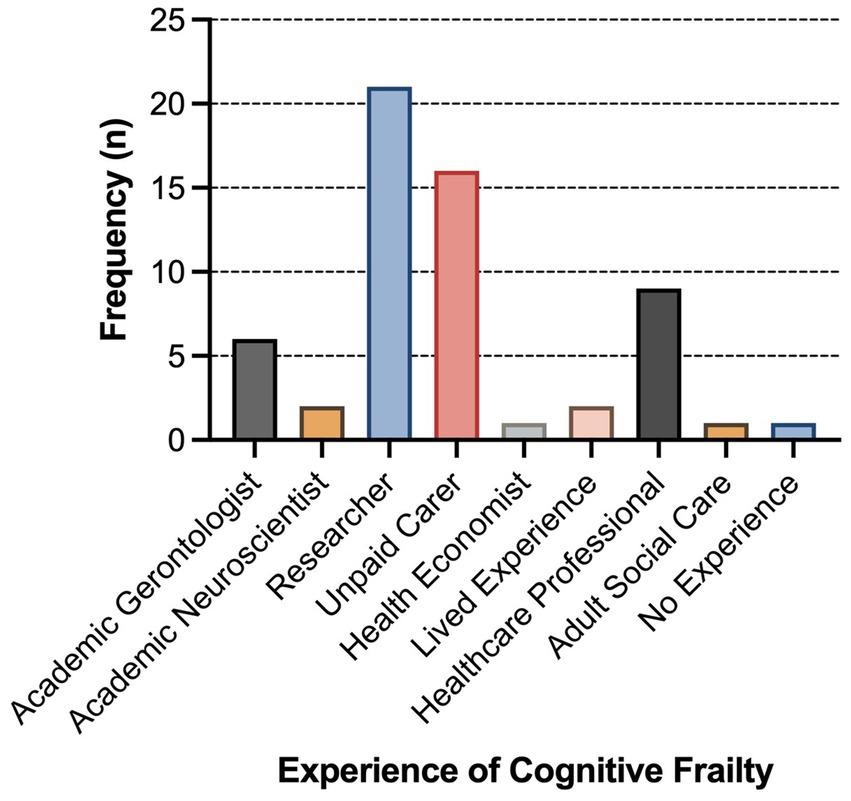
Figure 1. Frequency of categories of self-identified expertise (Figure preparation was conducted using GraphPad Prism 10 (GraphPad Software 2365 Northside Dr. Suite 560 San Diego, CA 92108)).
Overall consensus regarding the statements
Statements were examined in relation to the level of agreement observed, with 58 respondents answering most questions. Percentages are for agreement unless otherwise stated, and based on 58 respondents except where stated (missing responses or where participants did not answer a particular item because they did not perceive they had the expertise for that item). There were 7 Academic lab scientists/biologists, 27 Academics who worked with people, 14 people with lived experience and carers, and 10 professional carers (Clinicians/social care). Items where consensus was achieved according to our criteria are highlighted in bold in their respective results table. Extracted qualitative statements are appended in each table as relating to the items in relation to which they had been given.
Section 1: understanding and thinking about cognitive frailty
In the statements in Table 1, there was only clear agreement only for items 1.1 and 1.5. Participants agreed that “Many researchers and clinicians are not clear what is meant by cognitive frailty” and that “Negative attitudes toward aging are what needs changing.” For Item 1.2, “Cognitive frailty is just a part of the aging process,” there was more disagreement than agreement, but no consensus by our criteria.
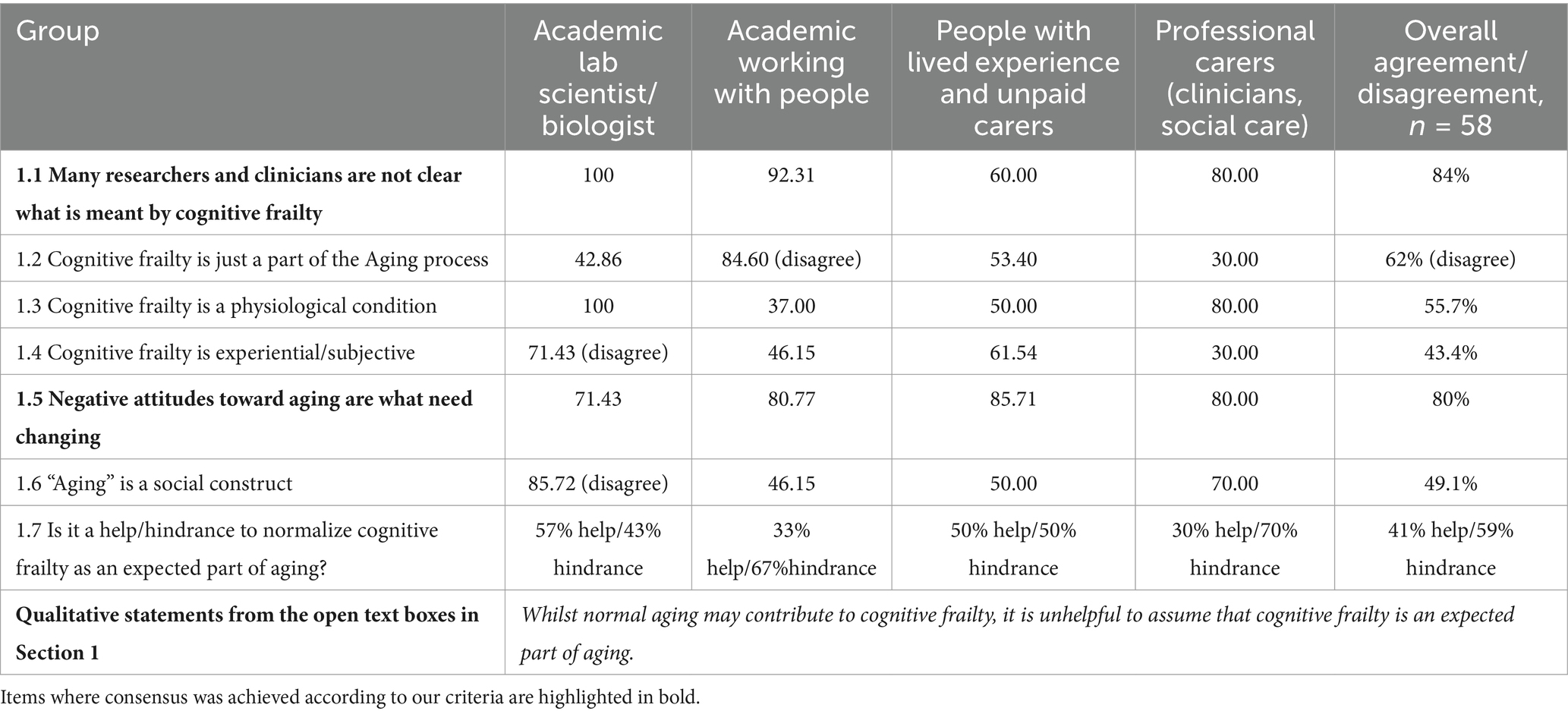
Table 1. Understanding and thinking about cognitive frailty: percentage agreement.
There was one further question in this section: “Item1.7: Is it a help or a hindrance to normalize cognitive frailty as an expected part of aging?” Of 58 responses, 58.62% responded that it was a hindrance. That is, there was no overall agreement.
Table 1 also shows the percentage agreement (or disagreement) with the statements as they varied within the different expertise groups. Although there was agreement on some issues, important differences emerged in relation to the statement on cognitive frailty being a physiological condition, with biologists and clinicians agreeing that it was, but other groups showing less consensus. Biologists also disagreed that aging was a social construct, whereas other groups, to some extent, agreed that it was. Academic researchers working with older people disagreed that CF is just part of the aging process, with other groups showing no consensus. Finally, there was a broad agreement amongst researchers working with people, and professional carers (such as clinicians) that it was a hindrance to normalize CF as an expected part of aging, while there was no consensus in other groups. This was further illustrated by the statement from the qualitative data, that Whilst normal aging may contribute to cognitive frailty, it is unhelpful to assume that cognitive frailty is an expected part of aging.
Section 2: preventability of cognitive frailty
There was clear overall consensus on all the items in Section 2, see Table 2.
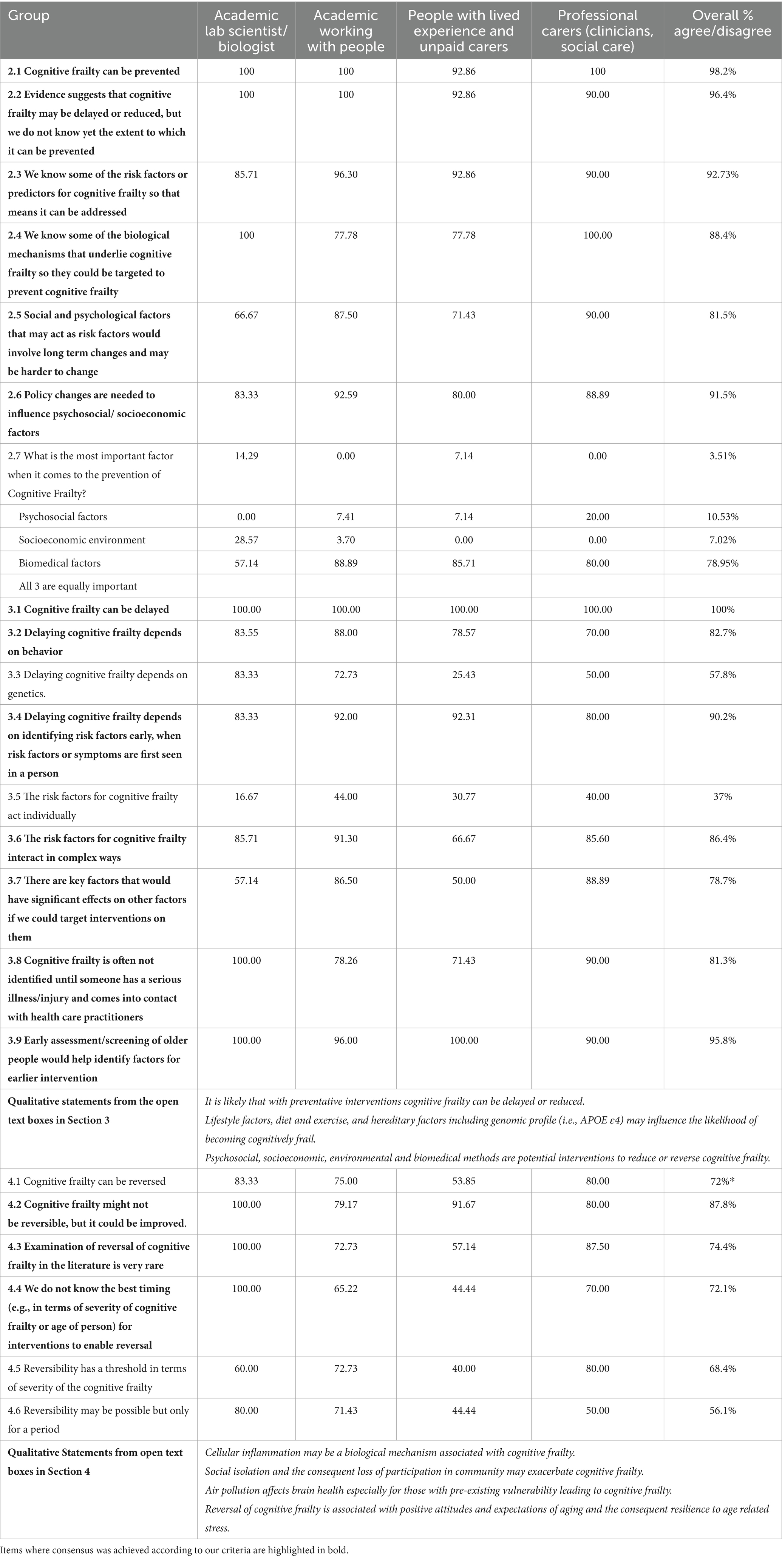
Table 2. Preventability, delay and reversibility of cognitive frailty (52–55 responses).
When these data were considered in terms of the four expertise groups, there were similar levels of agreement, except for academic laboratory scientists who did not show the required 70% consensus on items 2.5 (consensus was 66.67%) or 2.7. For 2.7, over 80% of respondents in all other groups agreed that all three factors (Psychosocial, Socioeconomic environment, Biomedical factors) were equally important in the prevention of CF, whereas only 57.14% of the laboratory scientists (biologists) endorsed that statement.
Section 3: whether cognitive frailty could be delayed
As can be seen in Table 2, all statements achieved >70% agreement except items 3.3 “Delaying cognitive frailty depends on genetics” (notably 13.46% of respondents did not feel they had the expertise to answer), and 3.5 “The risk factors for cognitive frailty act individually” where 42% of respondents disagreed with this statement and 37% agreed with it, showing differing opinions. The two kinds of academic researchers agreed that delaying CF depends on genetics (Item 3.3), whereas people with lived experience and unpaid carers, and professional carers/clinicians, showed no consensus on this topic. The qualitative statements emphasized that interventions and lifestyle factors influence the likelihood of becoming cognitively frail, but also acknowledged the role of genetic factors and suggested a range of approaches for intervention, namely psychosocial, socioeconomic, environmental and biomedical.
Section 4: whether cognitive frailty is reversible
As can be seen in Table 2, three of the six statements showed consensus. Items 4.5 “Reversibility has a threshold in terms of severity of the cognitive frailty” and 4.6 “Reversibility may be possible but only for a period” showed differing opinions. Item 4.1 “Cognitive frailty can be reversed” showed >70% agreement, but also 16% disagreement*, and so by our criteria, is not accepted as showing consensus. It is worth noting that this was an area where a number of people felt they did not have the expertise to respond to the statement, notably items 4.3 to 4.6. Of those who did not say that and so were included in the analysis, people with lived experience and carers showed the lowest consensus, notably for Item 4.1. It is also worth noting that the highest consensus was among lab-based scientists/biologists (who are among those who would be expected to have access to empirical evidence to back up this statement), and professional carers, who may see reversal of cognitive frailty in practice. The qualitative statements focused on potential mechanisms, such as cellular inflammation, social isolation and the consequent loss of participation in community, and air pollution. Finally, one comment suggested that reversal of CF is associated with positive attitudes and expectations of aging and consequent resilience to age related stress.
Section 5: intervention approaches and mechanisms
This section focused on the possible mechanisms of interventions for cognitive frailty.
There was strong agreement for all items except 5.13, where 20.4% of the respondents said the question on intervening with biological mechanisms was outside of their expertise, and 22.45% said they neither agreed nor disagreed. This suggests biological interventions are relatively unknown to participants. Even so, more people agreed than disagreed overall. Inspection of the percentage agreement for the different groups showed that only the academic laboratory-based researchers showed consensus for this item. The professional carers/clinicians group also showed no consensus for items 5.1, 5.2 and 5.16, although all other groups did. Results can be seen in Table 3. The statements extracted from the qualitative data gave suggestions for interventions or their implementation, or information on those currently being trialed, recommending sustained engagement with the target population or individual and on community facilities. A final statement emphasized the importance of addressing ageism by positive-age-belief interventions which could influence the progression of CF.
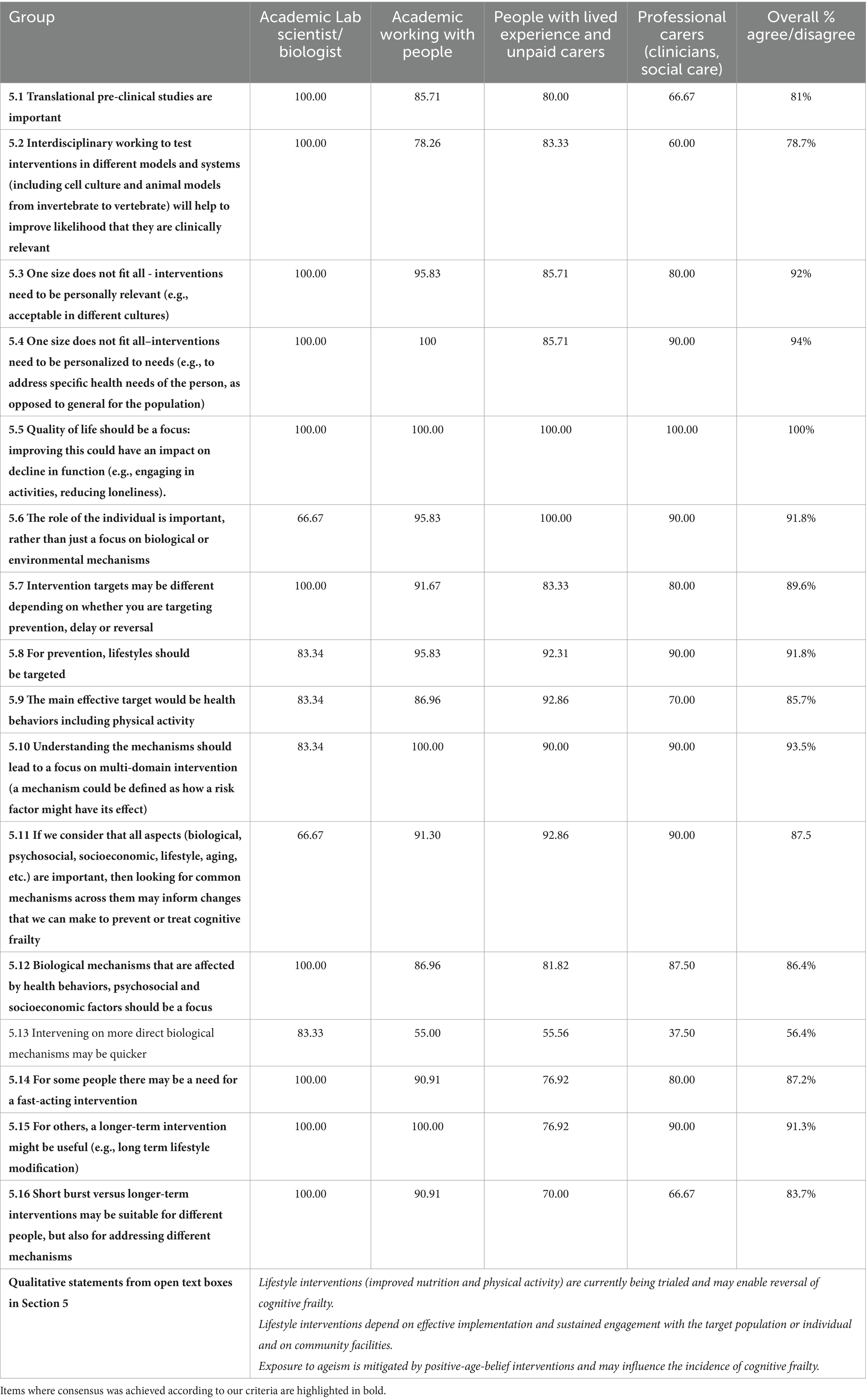
Table 3. Approaches to interventions for cognitive frailty, Section 5 (50 responded to Questions 5.1 to 5.12, and 49 answered 5.13 to 5.16).
Section 6: intervention targets
This section focused on designing interventions for cognitive frailty. Participants were asked to rank eleven proposed intervention targets with 1 being the most important and 11 the least. Forty-six people responded to this question.
Using Friedman’s non-parametric test for ranked data, there was a significant difference in the overall ranking between items [Chi-squared = 138.07 (df = 10), p < 0.001]. That is, there was agreement in the ranked order of the intervention factors across respondents, although there was still some variance. Physical activity + diet + probiotics was ranked the most important, followed by “Targeting isolation and loneliness/inclusive environments“, “Strength related exercise, not just cardiovascular,” and “Whole patient is important, e.g., caring for other morbidities such as arthritis.” Addressing menopausal effects on muscle was ranked as the least useful, as seen in Table 4.
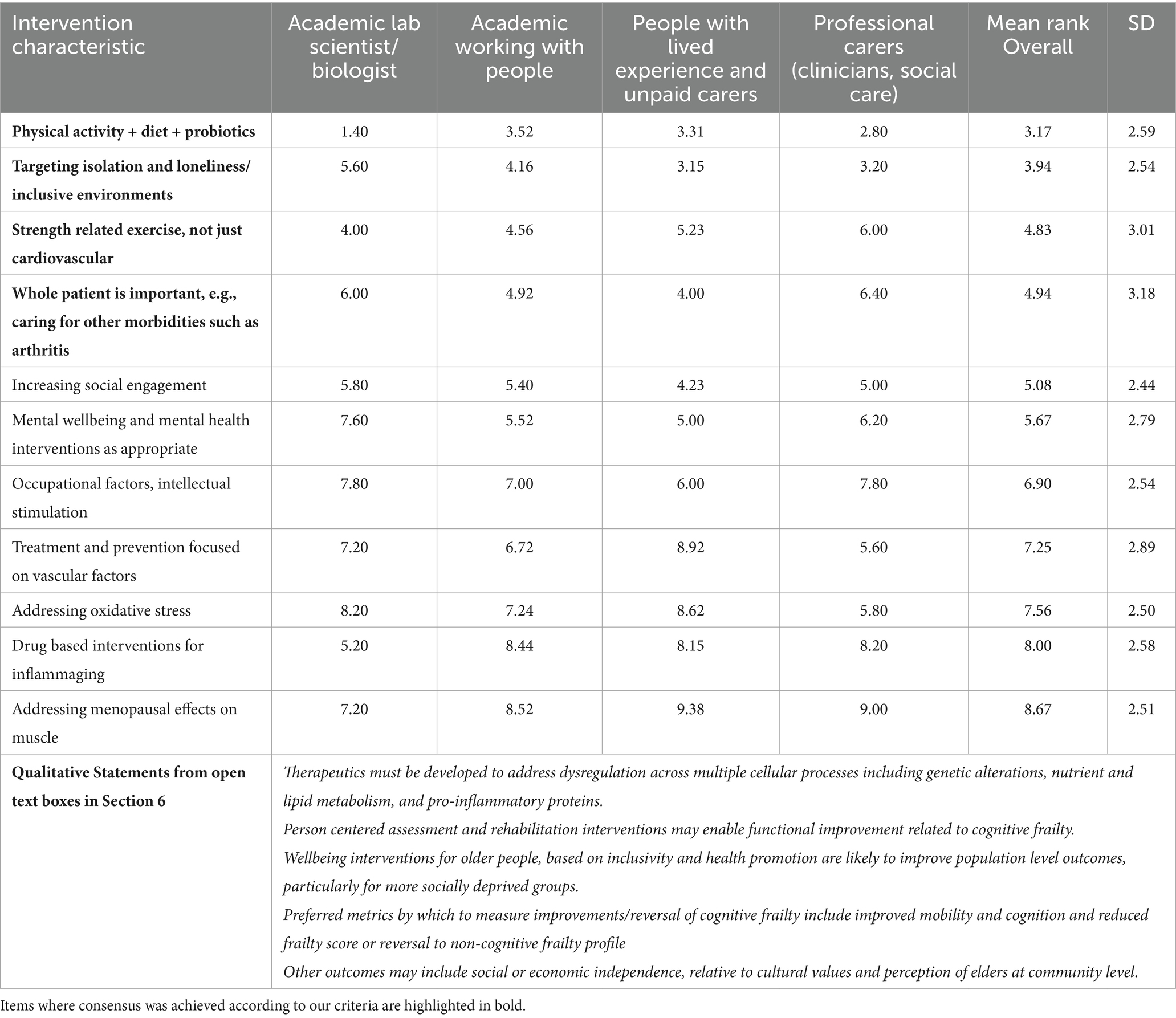
Table 4. Mean Ranking for Intervention targets in Section 6.
In terms of a decision on which statements achieved consensus as important, we used a cut-off of the rank below the median (5.08). An independent samples Kruskal-Wallis test examined whether there were any differences in the distribution of ranks for each intervention across the groups. There were no overall effects (p > 0.05). In individual pairwise comparisons, using Bonferroni adjustment for multiple comparisons, again, there were no significant differences.
The qualitative statements in this section were diverse in terms of suggested intervention targets, ranging from biomedical therapeutics to person centered assessment and rehabilitation and wellbeing interventions based on inclusivity and health, particularly for more socially deprived groups. Further statements endorsed outcomes such as improved mobility and cognition and reduced frailty score or reversal to non-cognitive frailty profile but also suggested social or economic independence, relative to cultural values and perception of elders at community level.
Section 7: possible restrictions on for whom interventions for cognitive frailty might be suitable
As seen in Table 5, only one item, 7.2 “Agency and involvement of the person is vital in agreeing on the intervention” achieved consensus. Item 7.6 “Lifestyle interventions are difficult to implement if individuals have limited social support” gained more than 70% agreement, but also 18.75% disagreement, with more disagreement in the academic lab scientist group. Only the Professional carers/clinicians showed consensus on item 7.1 referring to possible restrictions for whom interventions might be suitable, and this group joined those with lived experience in showing consensus over the difficulty of implementing lifestyle interventions if people have mobility issues.
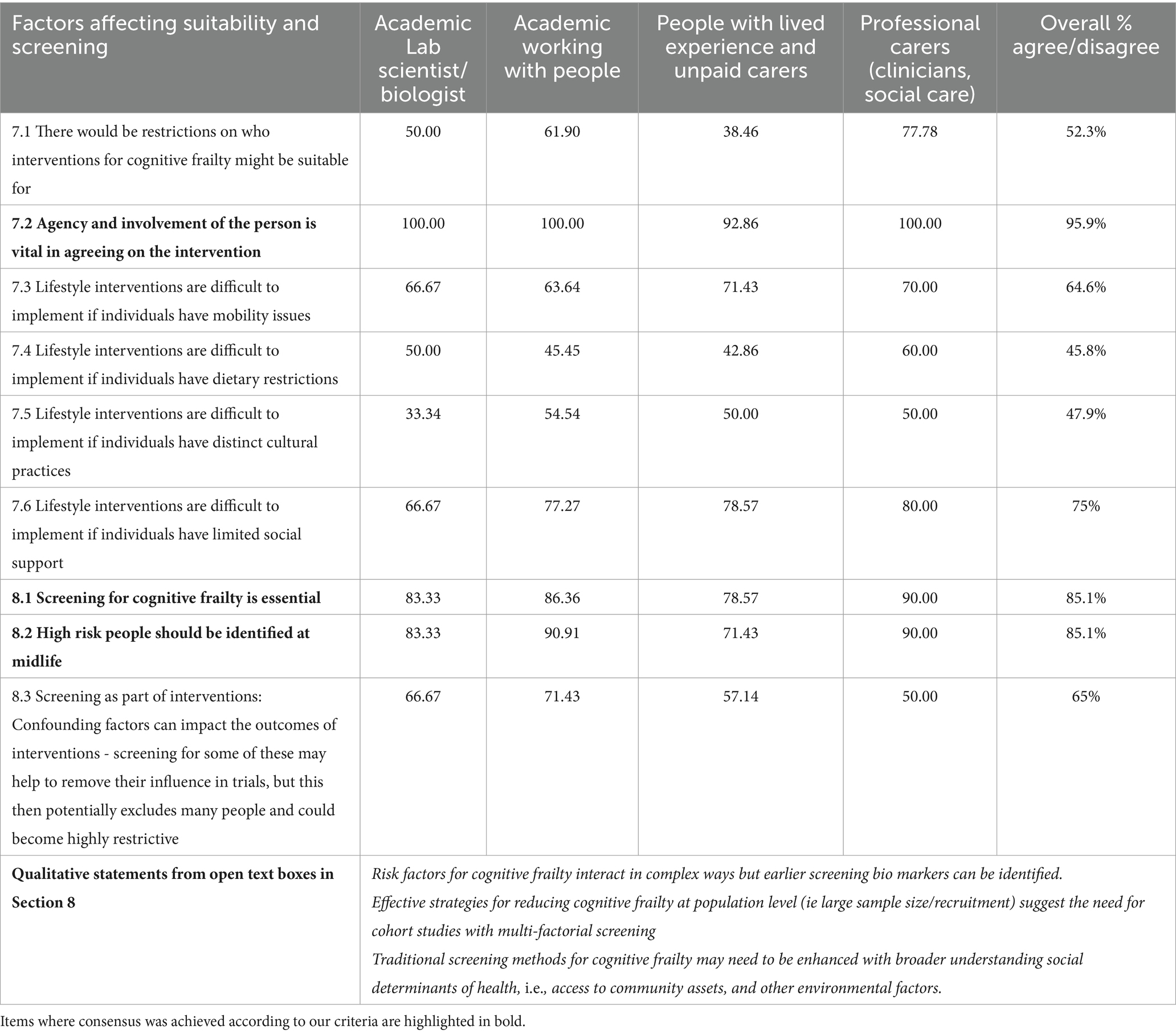
Table 5. Factors that may affect for whom interventions are suitable (Section 7), on factors related to screening (Section 8) (N = 48 for Section 7, N = 48 for Items 8.1 and 8.2 and 47 for item 8.3).
Section 8: screening for cognitive frailty
As seen in Table 5, there was consensus for the items 8.1 “Screening for cognitive frailty is essential” and 8.2 “High risk people should be identified at midlife.” For item 8.3, the more complex statement around confounding factors, 8 people responded that it was outside of their expertise and 23.4% neither agreed nor disagreed. Within the expertise groups, academics working with people did show consensus agreement. The extracted qualitative statements provide some more detail to the positive consensus on the importance of screening, in terms of suggesting that early screening biomarkers could be identified, as well as suggesting that multi-factorial screening and a broader understanding of social and environmental determinants of health should be incorporated into screening and future cohort studies.
Section 9: feasibility of interventions for cognitive frailty
Item 9.1 asked respondents to rank eight factors that may affect the feasibility or likelihood of adherence for people in relation to interventions for CF, with 1 being the most important.
The Friedman’s test showed a significant overall difference in the ranking between the items [Chi-Squared = 139.53 (df = 7), p < 0.001], confirming agreement across respondents in the ranked order of the intervention factors that may restrict or affect the feasibility or likelihood of adherence, e.g., including accessibility, affordability, acceptability, and health literacy, although there was still some variance. As illustrated in Table 6, accessibility was ranked the most important, and ethnicity as the least important. In terms of a decision on which statements were achieving consensus as important, a cut-off of a rank below the median (4.68) was used.
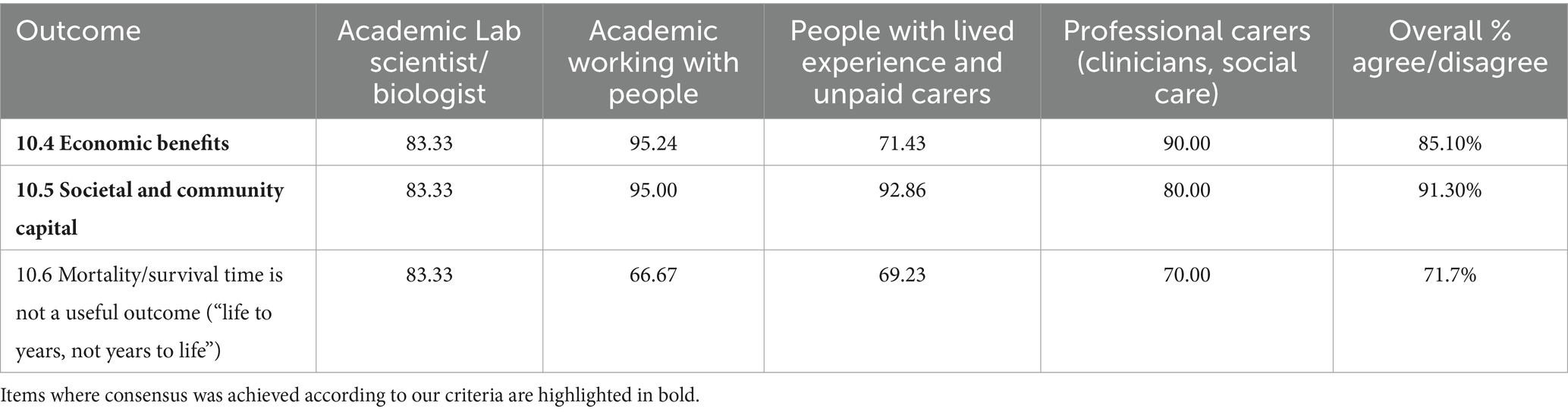
Table 6. Ranking of factors affecting feasibility of interventions (N = 48, Sections 9.1, 9.3, and 9.5).
Using the independent samples Kruskal-Wallis test, the distribution of ranks for each intervention across the groups was examined. There were no overall effects (p > 0.05). In individual pairwise comparisons between the groups, there were also no significant differences.
Question 9.3 asked participants to rank structural factors that may affect feasibility of interventions, where 1 means the most important. Forty-seven respondents completed the ranking, illustrated in Table 6:
Friedman’s test showed a significant overall difference in the ranking between the items [Chi-Squared = 45.76 (df = 8), p < 0.001]. That is, there was agreement in the ranked order of the structural factors that may restrict or affect the feasibility of involvement for respondents, although there was still some variance. Affordability or free access to classes or leisure centers was ranked as the most important, and cycle lanes, safe walking and running paths as least important. In terms of a decision on which statements achieved consensus as being important, the median cut-off was 4.60.
The extracted statements from the qualitative data (see Table 6) emphasized the need for personalized but multifactorial interventions, and the important role of co-design, scalability and transfer to different health economies.
The Kruskal-Wallis test to examine the distribution of ranks for each item across the groups found no overall effects (p > 0.05). In individual pairwise comparisons, there were no significant differences between the different groups of experts.
Item 9.5 asked participants to nine rank factors related to personal circumstances that may affect feasibility, with 1 being the most important. Friedman’s test showed a significant overall difference in the ranking between the items [Chi-Squared = 54.45 (df = 8), p < 0.001] demonstrating that there was agreement in the ranked order of the personal circumstance factors that may affect the individual feasibility of interventions, as illustrated in Table 6. Affordability was the most important personal factor, and personal energy levels seen as the least important. In terms of a decision on which statements achieved consensus as important, the median cut-off was 5.04.
The independent samples Kruskal-Wallis test showed no overall effects (p > 0.05) illustrating that the distribution of ranks for each intervention did not differ by group. In individual pairwise comparisons, again there were no significant differences between expert groups. The statements from the qualitive data (e.g., from questions 9.2 and 9.4, see Table 6) suggested that preventive strategies are likely to include environmental and inclusive community strategies, as well as focusing on personally focused strategies.
Section 10: primary and secondary outcomes of interventions for frailty
Primary outcomes
Using Friedman’s non-parametric test for ranked data, a significant overall difference in the ranking between the items was found (Chi-Squared = 23.30, df = 4, p < 0.001) demonstrating that there was agreement in the ranked order of the primary outcomes respondents considered appropriate to indicate the success of interventions for CF. Improvement in cognition was seen as the most important outcome, and an increase in physical strength as the least important (Table 7). In terms of a decision on which statements achieved consensus as important, a median cut-off of 2.98 was used.
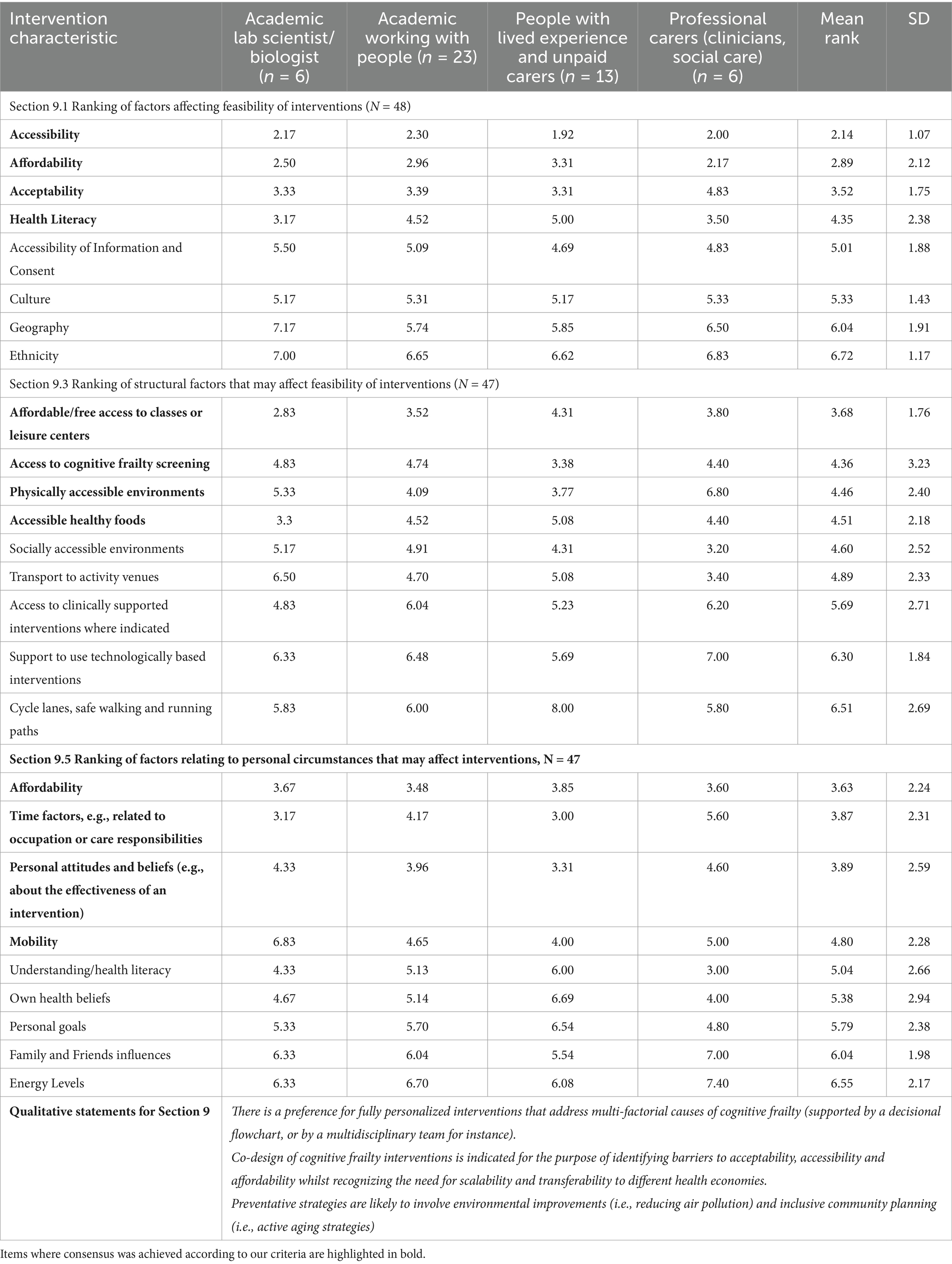
Table 7. Section 10, Ranking of primary and secondary outcomes N = 48.
The Kruskal-Wallis test examined the distribution of ranks for each outcome across the groups. There were no significant effects for any outcome except for “Revert to a non-cognitive frailty profile,” 8.29 (df = 3), p < 0.05. The individual group comparisons were not significant once the Bonferroni adjustment was applied.
Secondary outcomes
Friedman’s test showed a significant difference (Chi-Squared = 137.30, df = 9, p < 0.001) between the ranks. That is, there was agreement in the ranked order of the secondary outcomes that respondents thought would be appropriate to indicate success of interventions for cognitive frailty. “Extended or improved independence” was ranked as the most appropriate outcome, and whether “Appropriate social support was in place” as the least appropriate (Table 7). Reduced health and social care needs were also ranked as less important. In terms of a decision on which statements were achieving consensus as important, a cut-off rank below the median, 5.48, was used.
The independent samples Kruskal-Wallis test showed significant differences in the distribution of the ranks across the groups only for the outcomes of “happiness and mental health” [test statistic (df = 3) = 8.90, p < 0.05], and of “Appropriate social support is in place,” [test statistic (df = 3) = 13.09, p < 0.01]. The group of people with lived experience and carers ranked Happiness and Mental health as a more important outcome than did other groups, with the differences with the group of academic lab researchers being significant, padj < 0.05. For the outcome “Appropriate social care is in place,” the group of academics working with people judged this to be more important than did other groups, with the difference from the professional carer/clinician group being significant, padj = 0.01.
Participants were then asked what they thought were the main societal outcomes of interventions on cognitive frailty. As shown in Table 8, there was >70% agreement for Economic benefits and Social and Community Capital. Although agreement for “Mortality/survival time is not a useful outcome” was >70%, disagreement was also >15%. Specifically, academics working with people, and people with lived experience showed lower agreement with that statement.
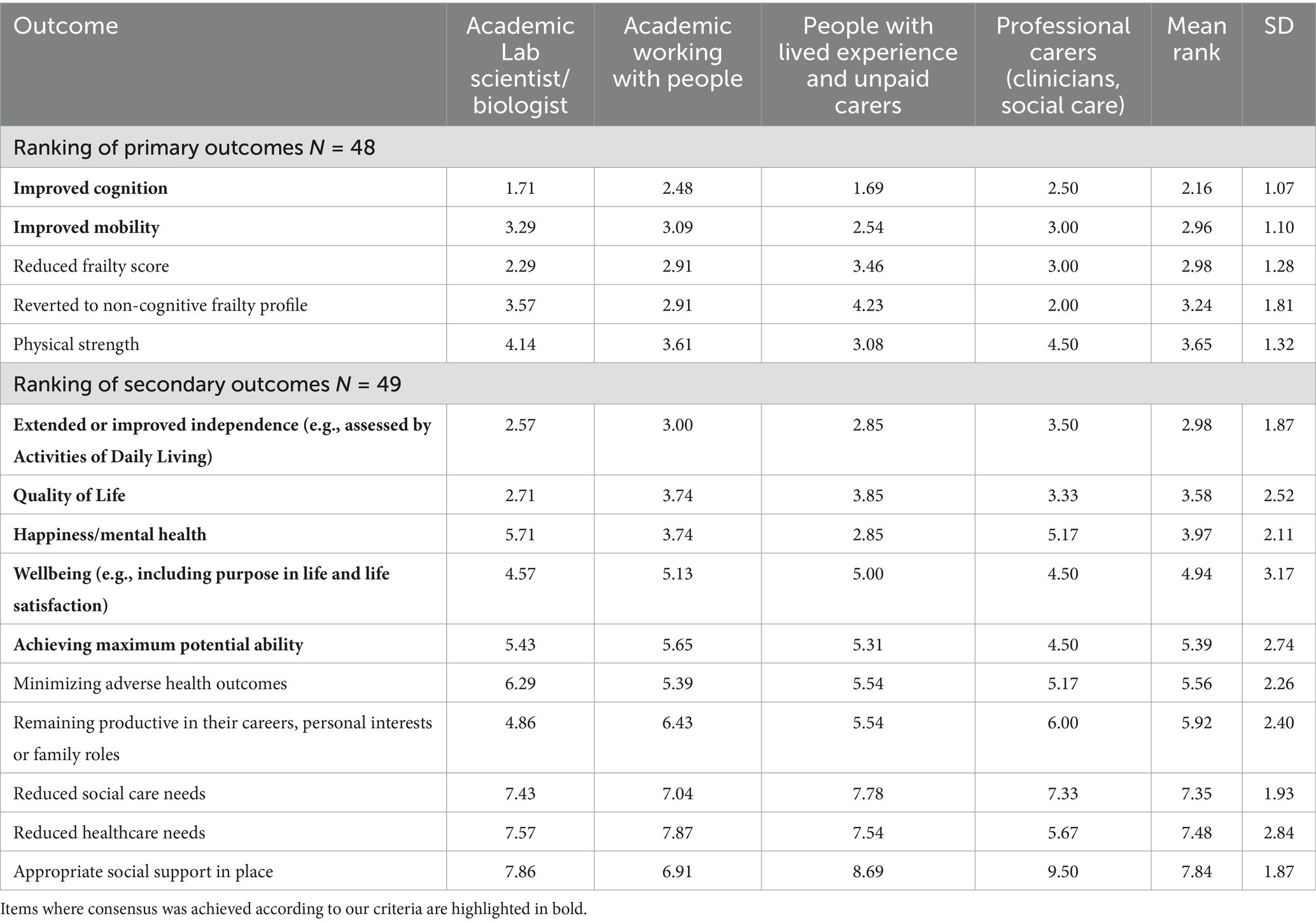
Table 8. Section 10, agreement/disagreement on potential outcomes of interventions for society (N = 48).
Section 11: effectiveness of interventions for cognitive frailty (i.e., do they work in real life?)
There was more than 70% agreement for both Questions 11.1 and 11.2, see Table 9.
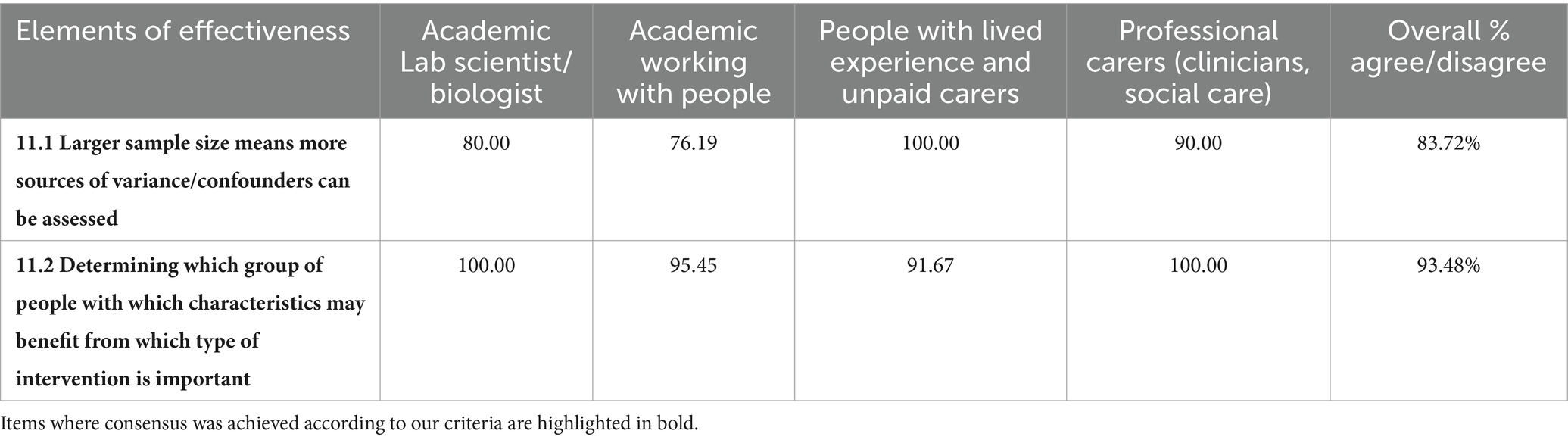
Table 9. Section 11, agreement/disagreement on elements of effectiveness of interventions N = 47.
Question 11.3 asked respondents to rank seven factors in relation to their importance in determining the effectiveness of an intervention.
Friedman’s test showed a significant difference in the ranks (Chi-Squared = 76.18, df = 6, p < 0.001). “Effectiveness in the real world” was ranked as the most important, and “ability to sustain the interventions for the amount of time they were needed” was seen as the least important. Three items tied for second rank (Table 10). As this included the median cut-off (3.41), the cut-off of a rank including and above the median was implemented.
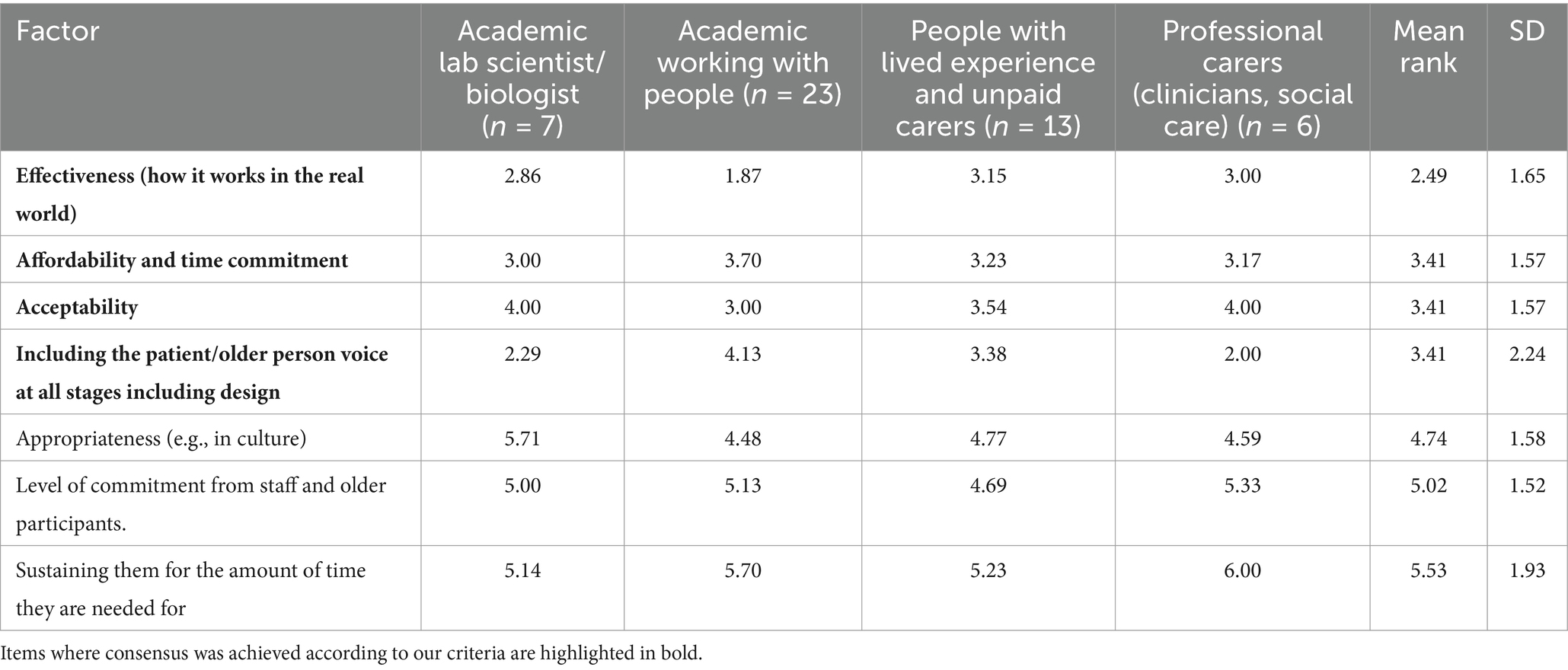
Table 10. Section 11, Ranking of factors influencing effectiveness of interventions N = 48.
The independent samples Kruskal-Wallis test showed differences in the distribution of ranks for each intervention across the groups only for the characteristics of “Effectiveness (How it works in the real world)” [Test statistic (df = 3) = 9.18, p < 0.05] and “Including the patient/older person voice at all stages including design” [Test statistic (df = 3) = 7.84, p < 0.05]. Individual group comparisons were not statistically significant in adjusted comparisons.
Section 12
This section explored intervention design strategies, beginning by asking participants to respond to a set of intervention strategies as to whether they could increase the likelihood of success. There was strong agreement for all items and little variance between expertise groups, see Table 11.
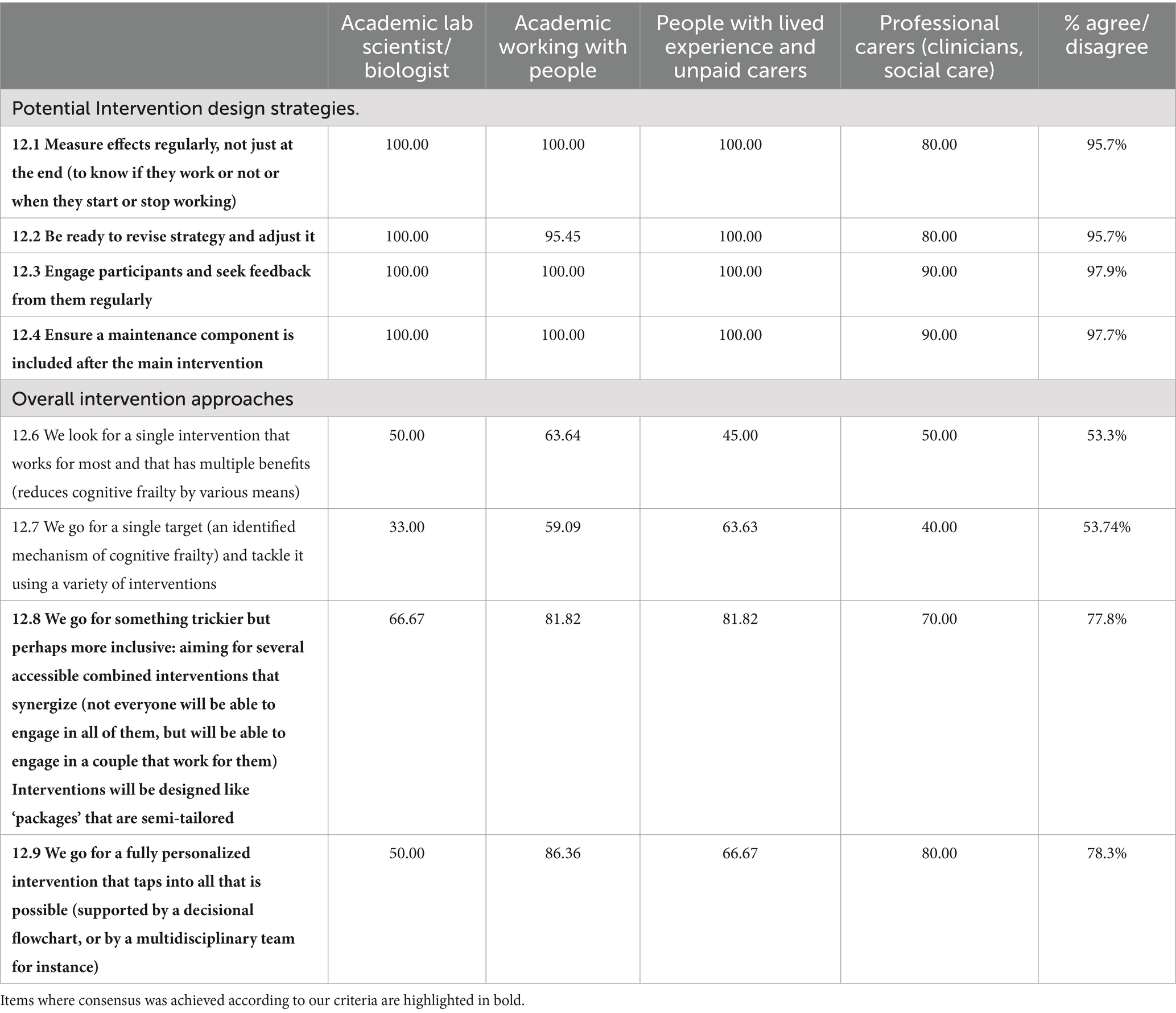
Table 11. Section 12, Percentage agreement/disagreement with potential intervention design strategies and on overall intervention approaches.
Respondents were then asked for their agreement or disagreement with overall intervention approaches, with 47 responding to this section. There was agreement of >70% on two of the intervention approaches, see Table 11.
Results of Round 3
There were 38 respondents to Round 3 with only 4 people identifying as academic Lab Scientists and 4 people as Professional carers. Percentages for these subgroups should be treated with caution. There were 21 academics working with older people and 12 people with lived experience/carers. Given high levels of consensus in these analyses, tables are only presented to illustrate where there was variability in consensus across groups or for where there was no consensus. Four respondents were classified into more than one group, hence the total of 38.
Section 1: understanding of CF
There was strong overall consensus for these statements. Our analysis of the separate expertise groups showed that there was no consensus for Items 1.1 and 1.2 for the people with lived experience and unpaid carer group, see Table 12.
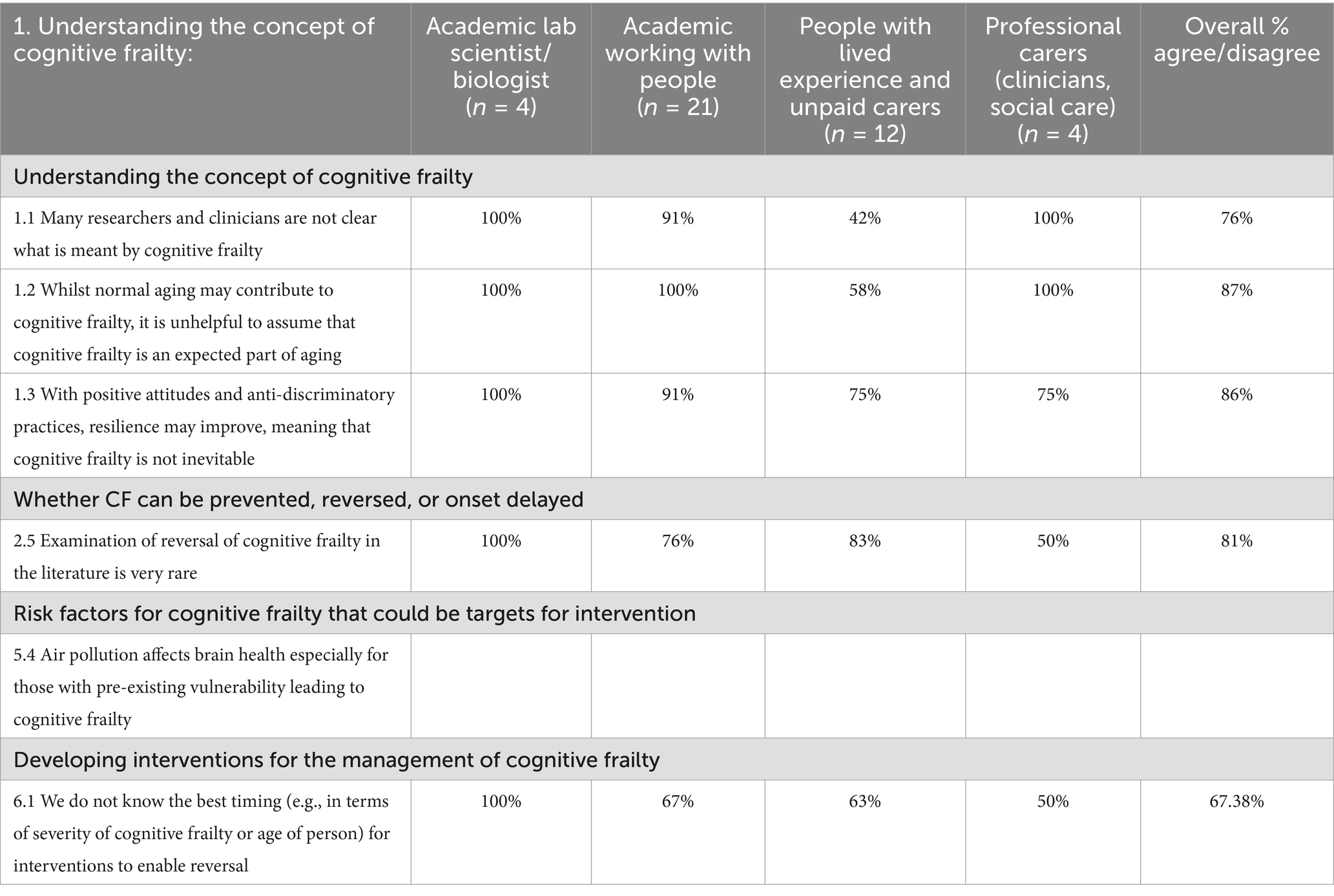
Table 12. Round 3, Sections 1, 2 and 5, percent agreement on items where there was not uniform consensus across groups, (n = 41).
Section 2: whether CF can be prevented, reversed, or onset delayed
There was clear overall consensus for every item in this section. However, there was no consensus amongst Professional carers/clinicians regarding Item 2.5 on the rarity of examinations of reversal of CF in the literature, where there was only 50% agreement, see Table 12.
There was overall consensus and also consensus within each of the groups for the following sections:
• Section 3, Screening for CF;
• Section 4. Possible mechanisms for interventions to address CF.
Section 5: acknowledged risk factors for cognitive frailty that could be targets for interventions
There was overall agreement as well as agreement within groups for all items in this section, except Item 5.4 regarding air pollution, where there was no consensus within the group of people with lived experience and carers (only 43% agreement), see Table 12.
Section 6: developing interventions for the management of cognitive frailty
All statements showed consensus except for 6.1 “We do not know the best timing (e.g., in terms of severity of cognitive frailty or age of person) for interventions to enable reversal” where there was no consensus by our 70% criterion for any subgroup except the academic lab-scientists (mean agreement was 67.38%), see Table 12.
For the remaining sections, all items achieved consensus for all statements overall and within groups. These sections are listed as follows:
• Section 7: Important targets for interventions for cognitive frailty to focus on,
• Section 8: Possible restrictions on for whom interventions for cognitive frailty might be suitable,
• Section 9: Factors that may restrict or affect the feasibility or likelihood of adhering to interventions for cognitive frailty,
• Section 10: Attention to the impact of inequalities and person variables on the feasibility of different types of interventions
• Section 11: Primary outcomes of interventions for Cognitive Frailty that we should target,
• Section 12: Secondary outcomes of interventions we should target,
• Section 13: Outcomes of interventions on cognitive frailty for society,
• Section 14: Importance in determining the effectiveness of an intervention,
• Section 15: Intervention design strategies to increase the likelihood of success,
• Section16: Further factors in intervention design.
In summary, there was consensus on 89 out of 90 statements overall, with only four items showing a subgroup without consensus. In the only item that did not show overall consensus “We do not know the best timing (e.g., in terms of severity of CF or age of person) for interventions to enable reversal,” there was also a lack of consensus with the statement for three of the four subgroups, with only academic lab scientists showing consensus agreement with the item.
Discussion
With 9% of the over 60s population estimated to be living with cognitive frailty (Qiu et al., 2022), cognitive frailty is a critical global concern associated with aging. Given the increasing number of older people globally, an increased number of people living with CF is likely, as is the associated risk of disability resulting from this co-existence of physical and cognitive impairments. CF is a potentially preventable risk state for later life consequences such as dementia and increased need for health and social care support and an important target to reduce the gap between healthy lifespan and actual lifespan, that is, healthy aging. It is also a pressing concern given the wide variation in healthcare utilization and opportunities to access and use clinical and rehabilitation services to identify and treat frailty and cognitive decline. An increased awareness of the importance of prevention and building resilience is needed to support mid-life populations to promote or maintain healthy aging in their communities.
This Delphi consensus study set out to explore and develop consensus around interventions for CF among experts across disciplines and sectors, including people with lived experience of CF, and those providing care. Views of those in carer roles, unpaid or as part of their employment, were important to include, in relation to their understanding of CF and interventions for it, recognizing sub-clinical functional effects of CF. Given that previous resources and reviews on interventions for CF had largely been from the point of view of applied health researchers or clinicians, this study represents a first attempt to obtain agreement across a broader spectrum of involved experts on critical factors for interventions. The study brought in a broader mix to include the perspectives of people who may be involved in the decisions about which interventions to operationalize with specific patients or population groups, the potential end users and those who care for them, as well as basic laboratory scientists whose perspectives may not often be considered in relation to operationalization or methods of health interventions and who are not often involved in such operationalization or design. These results emphasize the need for tailored interventions that consider both individual and structural determinants of cognitive frailty. The study’s interdisciplinary consensus approach suggests potential for broader collaboration in future frailty intervention frameworks, incorporating biological, social, and policy-driven perspectives.
Delphi studies by their design are iterative. Out of the original 127 items presented to participants in Round 2, there was consensus on 74, and although fuller consensus was achieved in the final round (Round 3), information can also be gathered from some of the items where consensus was not achieved in Round 2. Little consensus was observed in the section on understanding of the concept of CF. Notably, there was a lack of consensus on whether it was a help or a hindrance to normalize CF as an expected part of aging. For some, there is therefore a belief that CF could be a normal part of aging. While physiological changes that occur with increasing age are clearly a risk factor for CF, our own work and that of others (see Holland et al., 2024 for a review) have identified risk factors that may worsen, and in contrast, factors that reduce, the rate at which age-related biological changes occur. Examples are factors that impact on immune system aging such as stress or diet, or impacts of healthy lifestyle on cardiovascular health. Increasing understanding that some age-related conditions can be prevented, delayed or reversed is a crucial step toward countering beliefs about inevitability. That is, although reviewed evidence shows increase in likelihood of CF with increasing age, evidence also describes it as a distinct, non-universal and mainly pre-clinical condition associated with these risk factors. Nevertheless, given that the respondent group included people with lived experience, we also need to acknowledge that some people were in a situation where accepting the impacts of aging was an important part of their own coping and resilience.
There was, however, consensus on “Negative attitudes toward aging are what need changing” suggesting that experts reflected on the negative stereotypes associated with old age (including ageism) and considered that CF might be seen as a low priority for interventions. This a known problem with significant ‘self-stigma’ and wider societal stigma associating any changes in old age with commonly held beliefs that cognitive decline and frailty are inevitable conditions of older age (Preville et al., 2015). Linking to the statement on normalizing CF as a normal part of aging being seen as a hindrance, this may be because of the negative attitudes toward aging in general and the consequences this has, i.e., not prioritizing intervention for CF. Given the accurate identification by the World Health Organisation of ageism as one of the four key pillars of the Decade of Healthy Aging (World Heath Organisation, 2021), it is essential to challenge even “compassionate ageism” which incorporates stereotypical assumptions that frame mindsets, behaviors and clinical interventions, almost making frailty and cognitive decline a self-fulfilling prophecy. Providing strong evidence to support a more positive aging agenda is crucial and so emphasis on preventative interventions is critical.
The laboratory-based scientists’ level of consensus diverged from views of those with lived experience and clinicians on some topics, highlighting that the biological science associated with frailty and brain health at a mechanistic level needs to be factored into the consideration of interventions. The interaction between the potential for biological mechanisms and lifestyle, environment or policy interventions is explored further in our scoping reviews (Fowler Davis et al., 2024a; Fowler Davis et al., 2024b; Hodgson et al., 2024; Holland et al., 2024), and this Delphi study suggests that understanding and knowledge exchange across the disciplines could enhance potential theory-based design of interventions. Likewise, the high consensus associated with “Many researchers and clinicians are not clear what is meant by cognitive frailty” suggests that more needs to be done to explain and differentiate CF from purely brain related ill-health including dementias, while still accepting that people with different expertise will bring different perspectives to the mix.
Ranked items showed that respondents clearly differentiated between items such as intervention targets, factors affecting feasibility of interventions including structural factors, the impact of personal circumstances, and primary and secondary outcomes, as well as factors that may influence intervention effectiveness, such as accessibility, affordability, acceptability and addressing health literacy.
There was broad agreement on intervention design strategies. However, there was no consensus on simpler interventions–looking for a single intervention that works for most people, or a single target mechanism, and instead there was consensus on inclusive, combined and personalized interventions, e.g., that may involve a multidisciplinary team, underlining the understanding that a broad view of the factors influencing CF will link to a broad view of interventions.
Consensus shown for screening, bespoke assessment and specialist care needs to be carefully considered against the current demand for memory services. Development of early biomarkers and early screening for people at high risk were suggested strategies. Alternative methods to enable self-monitoring and self-management may be indicated, for example, with digital tools and online assessments, perhaps using Artificial Intelligence facilities.
Differences between the groups of experts were examined and a notable finding was that there were fewer differences than one might expect. However, it is important to note some of the places where there were differences; for example, in Round 3, there was no consensus among respondents with lived experience and carers in terms of items “Many researchers and clinicians are not clear what is meant by cognitive frailty” and “Whilst normal aging may contribute to CF, it is unhelpful to assume that cognitive frailty is an expected part of aging.” The lack of consensus on the latter statement can be attributed to the conflict between knowledge that certain deficits increase in likelihood with increasing age, versus knowledge that age, per se, does not cause them, rather, that a range of mechanisms that are subject to a range of risk factors and environmental influences affect the variability observed within the older population. A further difference where this group did not show consensus, but the others did, was the item referring to the impact of air pollution on brain health, especially for those with pre-existing vulnerability, leading to cognitive frailty. This is also evidenced in the literature (e.g., Power et al., 2016; Hodgson et al., 2024), but may well be an example of more recent evidence that is relatively well-known amongst researchers but not yet in the public domain.
Other differences between expert groups showed that the Lab scientists (who were all biologists), showed differential consensus on specific items in Round 2. For example, “The role of the individual is important, rather than just a focus on biological or environmental mechanisms” showed no consensus for the Lab scientists but consensus for the other groups, and “Intervening on more direct biological mechanisms may be quicker” showed consensus for the academic lab-scientists but not for any other group. Bringing together researchers and other experts who emphasize the individual person together with biologists who put more emphasis on the underlying biological mechanism in development of interventions is an important exercise as we seek to put all our expertise together to solve the challenges of aging and have impact beyond what we can at present; this is illustrated by these differences and is a strength of this approach.
The influence of people’s differing experiences was reflected well in Section 7 on “Possible restrictions on for whom interventions for cognitive frailty might be suitable.” This suggests the importance of discussing the difficulties groups experience when implementing interventions at the point of design, including acknowledging the different roles the different groups play in implementation and reception of interventions.
Finally, there was no consensus overall that CF can be reversed, with experts by experience showing the highest disagreement with this concept, although there was consensus for the other groups. Given that there is evidence (although limited as yet for reversibility in the literature; e.g., Ruan et al., 2020), this suggests that more work is needed to engage people with lived experience to promote this possibility, given that if there is little expectation of improvement once CF is present, motivation for intervention may be lower. However, further investigation is needed to understand this group’s perspective, ensuring people are distinguishing between dementia and the cognitive decline associated with CF. The consensus on the statement that few intervention studies directly address the reversibility question seems to tally with literature searches and suggests that this is an area where further research is needed. Many interventions have shown reductions in frailty and cognitive impairment (for a recent review, see Ji et al., 2025), but studies on reversibility are not absent, e.g., Huang et al. (2025) demonstrated reversal from Reversible CF (RCF) to non-cognitively frail (non-CF) and from potentially reversible CF (PRCF) status to both RCF and non-CF status in multi-domain interventions. Although statistically significant, the proportion of participants reversing was still small and further research is needed to determine why some people show reversing and others do not. A further study again using a multi-domain intervention (WE-RISE ™), found that after 12 weeks, 74% of the intervention group were no longer assessed as having cognitive frailty whereas only 10.7% of the control group were no longer cognitively frail (Murukesu et al., 2024). Further research in different populations with carefully identified RCF and PRCF groupings would undoubtedly improve the understanding of the likelihood of reversal across the expert groups. Nevertheless, there is clear evidence that reversal to a non-CF state can result from intervention.
A way forward
Although it should be emphasized that this study is based on expert consensus, rather than direct testing of interventions, many of the academic experts did refer to supporting evidence in the open text boxes. One way to consider next steps to developing interventions is suggested by Wight et al. (2016), who suggest six steps for quality intervention development (6SQuID). The first few steps align with our progress in this consensus development and the evidence syntheses that preceded it, as we have sought to (1) define and understand the problem and its causes; (2) identify which causal or contextual factors are modifiable including which have the greatest scope for change and who would benefit most; and (3) deciding on the mechanisms of change. The latter three steps of Wight et al. provide suggestions as to what is next which should be considered in further development following this consensus stage: (4) clarifying how interventions will be delivered; (5) testing and adapting the intervention; and (6) collecting sufficient evidence of effectiveness to proceed to a rigorous evaluation.
1. Define and understand the problem and its causes
The primary outcomes of any planned intervention need to address the outcomes identified via the consensus such as cognition and mobility, ensuring understanding of definitions of CF (and so inclusion in interventions). Secondarily, older adults with CF will experience a need for improved independence, quality of life and wellbeing. These broad interventions should be affordable, timely and meaningful (meet personal attitudes and beliefs. About the effectiveness of an intervention). Mobility, affordability, access to screening methods and physically accessible environments and healthy foods were all deemed significant to the cause and effects of CF.
1. Identify which causal or contextual factors are modifiable including which have the greatest scope for change and who would benefit most
There was a strong consensus that CF can be prevented, delayed or reduced, given knowledge on risk factors. Biological mechanisms could be targeted alongside social and psychological factors that involve long-term changes to lifestyle, and these may include environmental exposure. In this respect policy changes are needed to influence psychosocial/socioeconomic factors that disproportionally place some older adults at risk of CF.
Delaying CF was viewed as dependent on personal behavior but also on genetic factors. Risk factors may be individual but also interact in complex ways so require multiple interventions. Early assessment/screening of older people would help identify factors for earlier interventions, rather than only identifying a problem when the individual encounters health care practitioners.
Overall, there is a belief among some respondents that CF might not be reversible (and the best timing for interventions to enable reversal is not known, possibly because there is limited evidence for reversal in the literature), but it could be improved, although evidence on reversibility is building. Interdisciplinary working to test interventions in different models and systems (including cell culture and animal models from invertebrate to vertebrate) will help to improve likelihood that pre-clinical studies are clinically relevant.
Experts agreed that effectiveness (how it works in the real world), affordability and acceptability (for example, in terms of time commitment), were important and that interventions should be planned together with the affected person. Intervention acceptability would be based on the early measurement of effect with the option to revise and adjust interventions and to ensure that a maintenance component is included.
1. Deciding on the mechanisms of change.
Interventions need to be personally relevant (e.g., acceptable in different cultures) and personalized. Biological or environmental mechanisms may vary, and so intervention goals should target lifestyles to protect individuals from decline. Healthy behaviors including physical activity might be helpful but a focus on multi-domain intervention and common mechanisms such as psychosocial and socioeconomic factors should be emphasized. For those with urgent needs, a fast-acting personalized intervention should be considered but long-term lifestyle modification may also be suitable for different people. Physical activity with diet and probiotics, targeting isolation and loneliness, and strength-related exercise, are all important although with recognition that other morbidities such as arthritis will influence individual ability to complete those. There was consensus that agency and involvement of the person in agreement on choice of interventions was vital. There was also agreement that screening was essential, particularly that high-risk people should first be screened at midlife.
The implication of the consensus was that a multi-modal, co-produced health promotion approach will be needed, and that guidance should be used to address how to develop screening and assessment interventions alongside treatment (O'Cathain et al., 2019). This is consistent with several trials that demonstrate the effectiveness of multi-domain interventions often delivered as complex interventions for cognitive and physical frailty (Ng et al., 2015; Dedeyne et al., 2017) and for reversion of CF status (Murukesu et al., 2024).
The reversibility of CF is an extremely important differentiating factor for investment in interventions and an outcome measure suggesting treatment effectiveness will be critical for any future trial and research programs. Respondents agreed that improved cognition, improved mobility and reversal to a non-cognitive frailty profile would be the important outcomes to show effectiveness.
The dominant narrative within the section on “Approaches to interventions for cognitive frailty” suggests that most experts share values around person-centered care and assessment of wellbeing, widely agreeing upon these as critically important. However, this presents a significant challenge to researchers, given that the predicted incidence of CF may be as high as 9% of the older population (Qiu et al., 2022) and a population health approach is needed for both treatment and prevention. Although the role of person-centered or culturally specified interventions was agreed upon as necessary (“one size does not fit all”), there is a need for theory-driven, generalizable approaches that can enhance efficiency, cost-effectiveness, and scalability of existing implementation approaches (Schleider and Beidas, 2022) for CF. Scalable but contextualized interventions seem the way forward.
Limitations and strengths
Self-selection of experts is a strength of this study, particularly the inclusion of those with lived experience. However, self-selection across a range of disciplines in the CF network is a novel approach, that necessitated a disaggregation of the responses of separate groups, to examine any differences. The number of respondents in total was seen as comparable to other previous Delphi studies (e.g., Sezgin et al., 2022, had 21 experts), although the small number in some groups in Round 3 (notably laboratory scientists and professional carers/clinicians) is a limitation. The participant group was diverse in terms of geographical spread, including experts from UK, Europe, North and South America, and Asia. From our examinations of the diversity within the CF Interdisciplinary network (CFIN) in which this study was based, we know that we have good diversity of ethnicities. However, despite significant Chinese representation of CF expertise in the literature, we did not have any respondents for that country, and so this could be a limitation. Nevertheless, the approach provides broader face validity to the consensus achieved e.g., (see Nair et al., 2011). We intend that such common shared understanding can underline the roles of all these groups in development of interventions or population-level policy changes to impact the mitigation of CF and healthcare utilization, with an emphasis on prevention of disability, and associated need for care support.
Given the focus on interventions, there was no exploration of understanding of the aetiology of CF, and causes of CF were not included in the Delphi. Understanding of mechanisms will be needed to suggest how interventions would target and potentially reverse the progress of the syndrome. Nevertheless, a strength of this study is the clear consensus on lifestyle and behavioral interventions concurring with various previous reviews indicating that the syndrome is affected by personal behavior change. Our previous scoping reviews of mechanisms also suggest that behavior change may be one important factor that links underlying mechanisms to both healthy aging and also outcome CF (although there are other linking variables as well, including depression and anxiety, Holland et al., 2024) and environmental issues (Fowler Davis et al., 2024a; Fowler Davis et al., 2024b; Hodgson et al., 2024).
The lack of consensus on biologically based interventions also suggested that our experts were more interested in developing broad lifestyle intervention than a single biologically based drug therapy. None-the-less, given the dominance of pharmacological solutions and therapeutic methods, there may be existing or newer pharmacological or nutritional interventions worthy of further investigation for managing brain health, for example Vitamin D as a neuron therapeutic for reducing inflammation (Murukesu and Manucha, 2024).
We did not collect demographic information such as age and ethnicity, although we know that the CFIN network on which this study was based is relatively diverse. However, future work could usefully explore how cultural factors influence both the acceptability and effectiveness of CF interventions.
The value of the input of people with different expertise is demonstrated by this study> Although many of the proposed recommendations were based on existing evidence as well as the consensus achieved in this study, they still require validation through experimental studies.
Conclusion
The consensus achieved in this study associated with CF interventions needs to be considered as a first step in defining health promotion activities and interventions. The consensus provides a foundation for policy-guided, preventive approaches. Given the prevalence and resultant potential disability in older adult populations, the consensus statements are important and represent expert opinion that is inter-sectoral. Research in this direction will further inform public health policies to implement evidence-based research findings to the development of prevention plans (Kelaiditi et al., 2013). However, given what we know about the length of the gap between what academic researchers know and actual implementation in healthcare or policy changes (Morris et al., 2011), or adoption by patients, a new way of planning and promoting the need for prevention and intervention in this area is needed. This study takes a crucial step toward changing current siloed approaches, including all stakeholders from the outset. Interdisciplinary involvement of the broad groups identified here needs further development in future work.
Data availability statement
The anonymised data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Faculty of Health and Medicine Research Ethics Committee, Lancaster University (REF FHM-2022-1092-RECR-1 and (FHM-2023-1092-SA-1). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CH: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. ND: Conceptualization, Data curation, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing. SB: Conceptualization, Funding acquisition, Investigation, Validation, Writing – review & editing. LB: Validation, Writing – review & editing. FB: Validation, Writing – review & editing. CC: Conceptualization, Funding acquisition, Project administration, Validation, Writing – review & editing. IMD: Validation, Writing – review & editing. SD: Validation, Writing – review & editing. IHKD: Conceptualization, Funding acquisition, Validation, Writing – review & editing. AD: Conceptualization, Methodology, Validation, Writing – review & editing. MD: Conceptualization, Formal analysis, Methodology, Validation, Writing – review & editing. AE: Conceptualization, Funding acquisition, Methodology, Validation, Writing – original draft, Writing – review & editing. DF: Validation, Writing – review & editing. RF: Validation, Writing – review & editing. CG: Validation, Visualization, Writing – review & editing. AG: Conceptualization, Funding acquisition, Investigation, Methodology, Validation, Writing – review & editing. EK: Validation, Writing – review & editing. AK: Validation, Writing – review & editing. EN-P: Validation, Writing – review & editing. PS: Validation, Writing – review & editing. AS: Validation, Writing – review & editing. CS: Validation, Writing – review & editing. LS: Validation, Writing – review & editing. TW: Validation, Writing – review & editing. SF: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study is based within the Cognitive Frailty Interdisciplinary Network (CFIN), funded by the UKRI BBSRC/MRC (Grant Ref: BB/W018322/1), supporting CH, SB, SF, AG, IHKD, ND. TW is funded by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration (ARC) North East and North Cumbria. The views expressed are those of the author(s) and not necessarily those of UKRI, the BBSRC, MRC, the NIHR or the Department of Health and Social Care.
Acknowledgments
The authors would like to acknowledge the contribution of further expert respondents: Sarah Aguilar; Ilaria Bellantuono; Mark Dale; Alison Ellwood; Ian Fairclough; Ongley Fahim Hossain; Claire Jowett; Rashmi Kumar; Ira Milosevic; Catherine Pennington; Louise Phillips; Valia Rodriguez; Madiha Sajid; Peter Smith; Anne Ward; Karen Wright.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author disclaimer
The views expressed are those of the author(s) and not necessarily those of UKRI, the BBSRC or MRC, or the NIHR or the Department of Health and Social Care.
Footnotes
1. ^VOICE is a community of public, patients and carers. Embedded in the UK National Innovation Centre for Ageing at Newcastle University, it supports public and patient involvement and engagement (PPIE) in research.
References
Apostolo, J., Cooke, R., Bobrowicz-Campos, E., Santanas, S., Marcuccis, M., Canos, A., et al. (2018). Effectiveness of interventions to prevent pre-frailty and frailty progression in older adults: a systematic review. JBI Database System Rev. Implement. Rep. 16, 140–232. doi: 10.11124/JBISRIR-2017-003382
Baker, J., Lovell, K., and Harris, N. (2006). How expert are the experts? An exploration of the concept of 'expert' within Delphi panel techniques. Nurse Res. 14, 59–70. doi: 10.7748/nr2006.10.14.1.59.c6010
Brady, S. R. (2015). “The Delphi method” in Handbook of methodological approaches to community-based research: Qualitative, quantitative, and mixed methods. eds. L. A. Jason and D. S. Glenwick (New York: Oxford University Press).
Bunce, D., Batterham, P. J., and Mackinnon, A. J. (2019). Long-term associations between physical frailty and performance in specific cognitive domains. J. Gerontol. Series B Psychol. Sci. Soc. Sci. 74, 919–926. doi: 10.1093/geronb/gbx177
Clegg, A., Young, J., Iliffe, S., Rikkert, M. O., and Rockwood, K. (2013). Frailty in elderly people. Lancet 381, 752–762. doi: 10.1016/S0140-6736(12)62167-9
Dedeyne, L., Deschodt, M., Verschueren, S., Tournoy, J., and Gielen, E. (2017). Effects of multi-domain interventions in (pre)frail elderly on frailty, functional, and cognitive status: a systematic review. Clin. Interv. Aging 12, 873–896. doi: 10.2147/CIA.S130794
Delbecq, A., Ven, A., and Gustafson, D. (1975). Group techniques for program planning: A guide to nominal group and Delphi processes : University of Michigan.
Façal, D., Maseda, A., Pereiro, A. X., Gandoy-Crego, M., Lorenzo-López, L., Yanguas, J., et al. (2019). Cognitive frailty: a conceptual systematic review and an operational proposal for future research. Maturitas 121, 48–56. doi: 10.1016/j.maturitas.2018.12.006
Folstein, M. F., Folstein, S. E., and McHugh, P. R. (1975). ‘Mini-mental state’. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12, 189–198. doi: 10.1016/0022-3956(75)90026-6
Fowler Davis, S., Benkowitz, C., Holland, C., Gow, A., and Clarke, C. (2024a). A scoping review on the opportunities for social engagement and cognitive frailty in older adults. Public Health Rev. 45:1606494. doi: 10.3389/phrs.2024.1606494
Fowler Davis, S., Benkowitz, C., Nield, L., and Dayson, C. (2024b). Green spaces and the impact on cognitive frailty: a scoping review. Front. Public Health 11:1278542. doi: 10.3389/fpubh.2023.1278542
Fried, L. P., Tangen, C. M., Walston, J., Newman, A. B., Hirsch, C., Gottdiener, J., et al. (2001). Frailty in older adults: evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 56, M146–M157. doi: 10.1093/gerona/56.3.m146
Gomez-Gomez, M. E., and Zapico, S. C. (2019). Frailty, cognitive decline, neurodegenerative diseases and nutrition interventions. Int. J. Mol. Sci. 20:2842. doi: 10.3390/ijms20112842
Hodgson, J. R., Benkowitz, C., Castellani, B. C., Ellison, A., Yassaie, R., Twohig, H., et al. (2024). A scoping review of the effects of ambient air quality on cognitive frailty. Environments 11:4. doi: 10.3390/environments11010004
Holland, C., Dravecz, N., Owens, L., Benedetto, A., Dias, I., Gow, A., et al. (2024). Understanding exogenous factors and biological mechanisms for cognitive frailty: a multidisciplinary scoping review. Ageing Res. Rev. 101:102461. doi: 10.1016/j.arr.2024.102461
Hsu, C., and Sandford, B. (2007). The Delphi technique: making sense of consensus. Pract. Assess. Res. Eval. 12:10. doi: 10.7275/pdz9-th90
Huang, J. H., Wang, Q. S., Zhuo, R. M., Su, X. Y., Xu, Q. Y., Jiang, Y. H., et al. (2025). Effects of comprehensive intervention models on cognitive frailty in community-dwelling older adults: a 12-month follow-up study. Geriatr. Nurs. ; 194-202 Part B 62, 194–202. doi: 10.1016/j.gerinurse.2025.01.011
Ji, W. T., Sun, L. W., Geng, Q., and Zheng, G. H. (2025). Effect of regular exercise on cognitive frailty in the elderly: a systematic review. Exp. Aging Res., 1–27. doi: 10.1080/0361073X.2025.2485619
Kelaiditi, E., Cesari, M., Canevelli, M., Abellan van Kan, G., Ousset, P. J., Gillette-Guyonnet, S., et al. (2013). Cognitive frailty: rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J. Nutr. Health Aging 17, 726–734. doi: 10.1007/s12603-013-0367-2
Levy, S., Smith, G., De Wit, L., DeFeis, B., Ying, G., Amofa, P., et al. (2022). Behavioral interventions in mild cognitive impairment (MCI): lessons from a multicomponent program. Neurotherapeutics 19, 117–131. doi: 10.1007/s13311-022-01225-8
Li, X., Zhang, Y., Tian, Y., Cheng, Q., Gao, Y., and Gao, M. (2022). Exercise interventions for older people with cognitive frailty-a scoping review. BMC Geriatr. 22:721. doi: 10.1186/s12877-022-03370-3
Linstone, H., and Turoff, M. (2002). The Delphi Method: Techniques and Applications. United States: Addison-Wesley Publishing Company, Advanced Book Program.
Liu, J. (2022). GRADE methods in traditional medicine. Integrat. Med. Res. 11:100836. doi: 10.1016/j.imr.2022.100836
Menendez, S. G., and Manucha, W. (2024). Vitamin D as a modulator of Neuroinflammation: implications for brain health. Curr. Pharm. Des. 30, 323–332. doi: 10.2174/0113816128281314231219113942
Morris, Z. S., Wooding, S., and Grant, J. (2011). The answer is 17 years, what is the question: understanding time lags in translational research. J. R. Soc. Med. 104, 510–520. doi: 10.1258/jrsm.2011.110180
Murukesu, R. R., Shahar, S., Subramaniam, P., Rasdi, H. F. M., Nur, A. M., Singh, D. K. A., et al. (2024). The WE-RISE™ multi-domain intervention: a feasibility study for the potential reversal of cognitive frailty in Malaysian older persons of lower socioeconomic status. BMC Geriatr. 24:903. doi: 10.1186/s12877-024-05457-5
Nair, R., Aggarwal, R., and Khanna, D. (2011). Methods of formal consensus in classification/diagnostic criteria and guideline development. Semin. Arthritis Rheum. 41, 95–105. doi: 10.1016/j.semarthrit.2010.12.001
Nasreddine, Z. S., Phillips, N. A., Bédirian, V., Charbonneau, S., Whitehead, V., Collin, I., et al. (2005). The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 53, 695–699. doi: 10.1111/j.1532-5415.2005.53221.x
Ng, T. P., Feng, L., Nyunt, M. S. Z., Feng, L., Niti, M., Tan, B. Y., et al. (2015). Nutritional, physical, cognitive, and combination interventions and frailty reversal among older adults: a randomized controlled trial. Am. J. Med. 128, 1225–1236.e1. doi: 10.1016/j.amjmed.2015.06.017
O'Cathain, A., Croot, L., Duncan, E., Rousseau, N., Sworn, K., Turner, K., et al. (2019). Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open 9:e029954. doi: 10.1136/bmjopen-2019-029954
Power, M. C., Adar, S. D., Yanosky, J. D., and Weuve, J. (2016). Exposure to air pollution as a potential contributor to cognitive function, cognitive decline, brain imaging, and dementia: a systematic review of epidemiologic research. Neurotoxicology 56, 235–253. doi: 10.1016/j.neuro.2016.06.004
Preville, M., Mechakra Tahiri, S. D., Vasiliadis, H., Quesnel, L., Gontijo-Guerra, S., Lamoureux-Lamarche, C., et al. (2015). Association between perceived social stigma against mental disorders and use of health services for psychological distress symptoms in the older adult population: validity of the STIG scale. Aging Ment. Health 19, 464–474. doi: 10.1080/13607863.2014.944092
Qiu, Y., Li, G., Wang, X., Zheng, L., Wang, C., Wang, C., et al. (2022). Prevalence of cognitive frailty among community-dwelling older adults: a systematic review and meta-analysis. Int. J. Nurs. Stud. 125:104112. doi: 10.1016/j.ijnurstu.2021.104112
Rockwood, K., and Mitnitski, A. (2007). Frailty in relation to the accumulation of deficits. J. Gerontol. A Biol. Sci. Med. Sci. 62, 722–727. doi: 10.1093/gerona/62.7.722
Ruan, Q., Xiao, F., Gong, K., Zhang, W., Zhang, M., Ruan, J., et al. (2020). Prevalence of cognitive frailty phenotypes and associated factors in a community-dwelling elderly population. J. Nutr. Health Aging 24, 172–180. doi: 10.1007/s12603-019-1286-7
Ruan, Q., Yu, Z., Chen, M., Bao, Z., Li, J., and He, W. (2015). Cognitive frailty, a novel target for the prevention of elderly dependency. Ageing Res. Rev. 20, 1–10. doi: 10.1016/j.arr.2014.12.004
Schleider, J. L., and Beidas, R. S. (2022). Harnessing the single-session intervention approach to promote scalable implementation of evidence-based practices in healthcare. Front. Health Serv. 2:997406. doi: 10.3389/frhs.2022.997406
Sezgin, D., O'Donovan, M., Woo, J., Bandeen-Roche, K., Liotta, G., Fairhall, N., et al. (2022). Early identification of frailty: developing an international Delphi consensus on pre-frailty. Arch. Gerontol. Geriatr. 99:104586. doi: 10.1016/j.archger.2021.104586
Shang, Z. (2023). Use of Delphi in health sciences research: a narrative review. Medicine 102:e32829. doi: 10.1097/MD.0000000000032829
Sugimoto, T., Arai, H., and Sakurai, T. (2022). An update on cognitive frailty: its definition, impact, associated factors and underlying mechanisms, and interventions. Geriatr Gerontol Int 22, 99–109. doi: 10.1111/ggi.14322
Tam, A. C. Y., Chan, A. W. Y., Cheung, D. S. K., Ho, L. Y. W., Tang, A. S. K., Christensen, M., et al. (2022). The effects of interventions to enhance cognitive and physical functions in older people with cognitive frailty: a systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 19:19. doi: 10.1186/s11556-022-00299-9
World Heath Organisation (2021) WHO's work on the UN decade of healthy ageing (2021–2030) accessed 26/11/2–24
Wight, D., Wimbush, E., Jepson, R., and Doi, L. (2016). Six steps in quality intervention development (6SQuID). J Epidemiol Community Health, 70:520–5. doi: 10.1136/jech-2015-205952
Keywords: cognitive frailty (CF), intervention, Delphi study, expert consensus, multidisciplinary, multi-sectoral
Citation: Holland CA, Dravecz N, Broughton S, Barker LA, Bature F, Clarke C, Danat IM, Das S, Dias IHK, Dawson A, Dixon M, Ellison A, Façal D, Finch R, Gaffney CJ, Gow A, Kelaiditi E, Klimczuk A, Navarro-Pardo E, Sharratt P, Sixsmith A, Suemoto CK, Suprawesta L, Watermeyer T and Fowler Davis S (2025) Interventions for cognitive frailty: developing a Delphi consensus with multidisciplinary and multisectoral experts. Front. Aging Neurosci. 17:1541048. doi: 10.3389/fnagi.2025.1541048
Edited by:
Daniele Magistro, Nottingham Trent University, United KingdomReviewed by:
Roberto Vagnetti, University of L’Aquila, ItalySimone Varrasi, University of Catania, Italy
Copyright © 2025 Holland, Dravecz, Broughton, Barker, Bature, Clarke, Danat, Das, Dias, Dawson, Dixon, Ellison, Façal, Finch, Gaffney, Gow, Kelaiditi, Klimczuk, Navarro-Pardo, Sharratt, Sixsmith, Suemoto, Suprawesta, Watermeyer and Fowler Davis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carol A. Holland, Yy5hLmhvbGxhbmRAbGFuY2FzdGVyLmFjLnVr
†These authors share senior authorship