 Daichi Sone
Daichi Sone Shunichiro Shinagawa
Shunichiro Shinagawa- Department of Psychiatry, Jikei University School of Medicine, Tokyo, Japan
The biological basis of neuropsychiatric symptoms (NPS) in individuals who have dementia is poorly understood, despite the significant burden on patients, caregivers, and communities. Recent neuroimaging advances have provided reliable and less-invasive methods to investigate human brains in vivo. However, compared to the significant progress that has been made in the fields of diagnostic values and cognitive symptoms in dementia, the neuroimaging findings of NPS are less consistent, particularly in terms of the affected brain regions. This discrepancy may be due to differences in neuroimaging modalities or analytical methods, the fact that NPS can change over time, and/or the subjective nature of NPS assessments. In this narrative review, we summarize the extant literature on neuroimaging findings of NPS in dementia. We also discuss both the controversies and potential solutions to overcome the current problems.
1 Introduction
The prevalence of dementia worldwide among individuals aged ≥65 years is >10%, and an even greater percentage of people are expected to develop dementia in the coming decades (Alzheimer’s Association, 2024). It is now established that dementia is no longer just a disease of cognitive dysfunction. Neuropsychiatric symptoms (NPS) in dementia, also known as behavioral psychological symptoms in dementia (BPSD), refers to a heterogeneous group of non-cognitive symptoms and behaviors that are observed in people with dementia (Cerejeira et al., 2012), and NPS can be develop from the mild cognitive impairment (MCI) stage (David et al., 2016). Approximately 90% of individuals with Alzheimer’s disease (AD) experience one or more NPS at some point over the course of their disease (Radue et al., 2019). “Neuropsychiatric symptoms” is also included in the diagnostic criteria used for other types of dementia, e.g., visual hallucination in dementia with Lewy bodies (DLB) and behavioral disinhibition in behavioral variant frontotemporal dementia (bvFTD).
The social and economic burdens of dementia are expected to increase markedly over the next few decades (GBD 2019 Dementia Forecasting Collaborators, 2022), and thus NPS is also important in terms of social issues. In fact, NPS is a significant factor in (i) the high burdens and burnout of the individuals who are caregivers for people with dementia, (ii) nursing home placements, and (iii) the greater risks of morbidity and mortality (Tampi and Jeste, 2022). Despite the negative impacts of NPS on society, the neurobiological underpinnings of NPS have not been sufficiently elucidated, and this may hinder the development of effective treatments or interventions. Neuroimaging has been utilized to diagnose and monitor various neurological disorders and to uncover the biological mechanisms that underlie brain diseases. However, neuroimaging findings of NPS are less consistent compared to significant progress in the study of cognitive symptoms in dementia. In this narrative review, we summarize the literature concerning the neuroimaging findings of NPS in dementia, and we discuss both the current controversies and potential solutions to overcome the remaining problems. Our search strategy for literature included “neuropsychiatric symptoms in dementia”, “behavioral psychological symptoms in dementia”, and “neuroimaging” in PubMed, but strict systematic criteria in line with the PRISMA guideline were not adopted because of the narrative style of our review.
2 Measurement of NPS
Several scales for NPS assessment were developed after the first application of the Behavioral Pathology in Alzheimer’s Disease Rating Scale (BEHAVE-AD) in the late 1980s (Reisberg et al., 1987). The Neuropsychiatric Inventory (NPI) is widely used; its initial version included 10 items (Cummings et al., 1994), and two items have been added (Cummings, 1997). The 12-item version of the NPI consists of the following items for evaluation: delusions, hallucinations, agitation, depression, anxiety, euphoria, apathy, disinhibition, irritability, aberrant motor behavior, night-time behavior disturbances, and appetite and eating abnormalities. Many other scales are also available, including the Behavioral Syndromes Scale for Dementia (BSSD) (Devanand et al., 1992) and the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD)’s Behavior Rating Scale for Dementia (BRSD) (Devanand et al., 1992). There are also several scales for specific symptoms, e.g., the Geriatric Depression Scale (GDS) (Yesavage et al., 1982) for depressive symptoms, the Apathy Evaluation Scale (AES) (Marin et al., 1991) for apathy symptoms, and the Aggressive Behavior Scale (ABS) (Perlman and Hirdes, 2008) for aggressive symptoms. A systematic review published in 2014 suggested that none of these single measures is superior to the others (Gitlin et al., 2014).
These assessment scales enable a quantitative evaluation of NPS, and this has made it possible to determine correlations between NPS and neuroimaging findings, thus greatly advancing neuroimaging research. Quantitative assessments of NPS depend largely on the measurement methodology, as is the case for many other psychiatric disorders and symptoms. Although NPS scales are useful for clinical and research purposes, scales can also be a significant limitation in investigations of the neurobiological mechanisms underlying NPS. At this time, researchers can only investigate what can be measured by scales, and scales are inevitably influenced by the subjectivity of the evaluators. Another consideration in the measurement of NPS is its multidimensional structure and socio-cultural context. It is suggested that even within a single NPS domain, there are various dimensional factors (Yi et al., 2024). To enhance diagnostic precision and better align observed symptoms with their underlying neural correlates, it is also important to consider the influence of the socio-cultural context on NPS, as with various other psychiatric disorders (Yi et al., 2024; Poon et al., 2025).
3 Subdomains of NPS
The issues of how NPS should be classified and whether NPS should be considered an individual syndrome or syndromes are also relevant to investigations of the neural mechanisms of and treatments for NPS. The rational classification of NPS symptoms is important for the practical use of treatment algorithms in clinical practice. For example, the European Alzheimer’s Disease Consortium (EADC) recommended classifying NPS into several distinct groups that reflect the prevalence, time course, biological associations, and psychosocial factors (Robert et al., 2005).
As certain neuropsychiatric symptoms tend to co-occur with others, many studies have employed clustering or grouping strategies, such as a principal component analysis. A systematic review made available in 2022 applied a meta-analytic method for this purpose and observed a factor structure with a good model fit for the NPI-10 (Hiu et al., 2022). Generally, delusions and hallucinations, anxiety and depression, euphoria and disinhibition, and agitation and irritability tend to be incorporated into the same category, whereas apathy can be placed in a depression category or considered an independent item (Hiu et al., 2022). Whether such a research strategy using grouping factors is truly appropriate in terms of validity remains to be established.
4 Neuroimaging findings of NPS
Another systematic review summarized 118 studies on neuroimaging correlates of NPS in 2016 (Boublay et al., 2016) and suggested that delusions and apathy and depression symptoms were particularly associated with brain alterations in individuals with AD. The review’s authors also indicated that the brain regions that are most relevant for NPS are mainly in the frontal lobes, particularly the anterior cingulate gyrus (ACG), although temporal, parietal, insula, and subcortical structures are also involved (Boublay et al., 2016). Following this review, many more studies made continuous efforts to clarify the brain regions associated with NPS, using newer methodologies and/or multi-center approaches. Table 1 summarizes the neuroimaging research concerning the neurobiological aspects of NPS (47 studies) published since 2016.
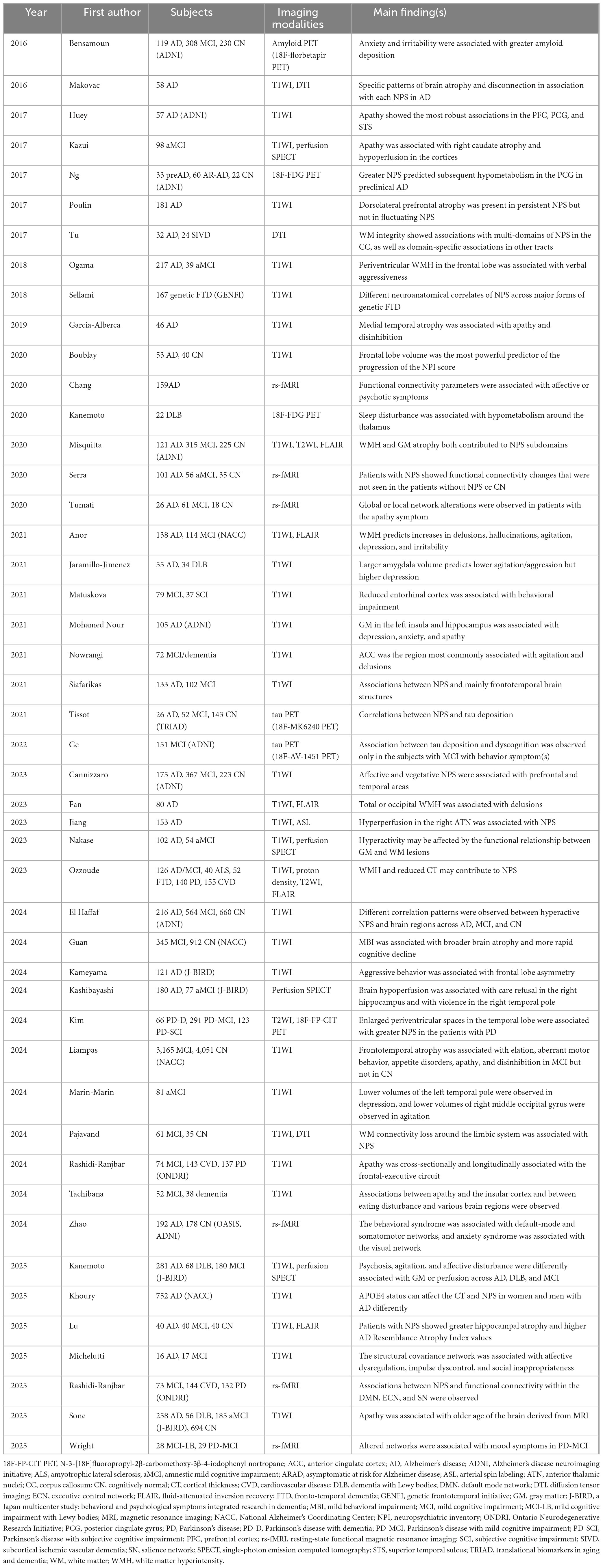
Table 1. Neuroimaging research regarding the neurobiological aspects of neuropsychiatric symptoms (NPS) published since 2016.
Brain morphometric imaging investigations using T1-weighted magnetic resonance imaging (MRI) account for the majority of these studies (Huey et al., 2017; Poulin et al., 2017; Ogama et al., 2018; Sellami et al., 2018; Garcia-Alberca et al., 2019; Boublay et al., 2020; Jaramillo-Jimenez et al., 2021; Matuskova et al., 2021; Mohamed Nour et al., 2021; Nowrangi et al., 2021; Siafarikas et al., 2021; Cannizzaro et al., 2023; El Haffaf et al., 2024; Guan et al., 2024; Kameyama et al., 2024; Liampas et al., 2024; Marin-Marin et al., 2024; Rashidi-Ranjbar et al., 2024; Tachibana et al., 2024; Khoury et al., 2025), with many reports implicating limbic structures such as the cingulate gyrus, entorhinal cortex, hippocampus, and amygdala as brain regions associated with NPS such as depression, apathy, agitation, and delusions (Huey et al., 2017; Garcia-Alberca et al., 2019; Jaramillo-Jimenez et al., 2021; Matuskova et al., 2021; Mohamed Nour et al., 2021; Nowrangi et al., 2021). Abnormalities in the prefrontal cortex (PFC) have also been reported (Huey et al., 2017; Poulin et al., 2017; Cannizzaro et al., 2023). Given the involvement of limbic structures and the PFC in emotional regulation and executive function, these findings may have some neuroscientific validity. However, there is variability across the studies regarding more detailed brain structures and symptom domains. Two recent studies reported associations between NPS and the insular cortex (Mohamed Nour et al., 2021; Tachibana et al., 2024). The role of the insular cortex in NPS may be of interest, as the insular cortex has recently received considerable attention for its involvement in a variety of functions, including somatosensory perception, emotion processing, and decision-making.
Considering that neuropathological changes in AD begin >10 years before the appearance of symptoms (Counts et al., 2017), the mechanism of NPS might not be elucidated by brain morphological changes alone. Several research groups have thus used multimodal neuroimaging (Makovac et al., 2016; Kazui et al., 2017; Misquitta et al., 2020; Anor et al., 2021; Fan et al., 2023; Jiang et al., 2023; Nakase et al., 2023; Ozzoude et al., 2023; Kim et al., 2024; Pajavand et al., 2024; Kanemoto et al., 2025; Lu et al., 2025). Assessments of white matter hyperintensity (WMH) in particular with the use of T2-weighted and fluid-attenuated inversion recovery (FLAIR) images have been continuous (Misquitta et al., 2020; Anor et al., 2021; Fan et al., 2023; Ozzoude et al., 2023), and it has been demonstrated that both WMH and gray matter loss contribute to NPS, which would justify a research approach combining multimodality images. Studies combining T1-weighted and diffusion tensor imaging (DTI) have also been attempted (Makovac et al., 2016; Pajavand et al., 2024). DTI can non-invasively assess white matter fibers in the brain and has been widely applied to elucidate the mechanisms of NPS (Tu et al., 2017; Zhou et al., 2023).
Cerebral blood flow and glucose metabolism are also important clinical and research targets that have been used to assess brain functions in dementia research (Kazui et al., 2017; Ng et al., 2017; Kanemoto et al., 2020; Jiang et al., 2023; Nakase et al., 2023; Kashibayashi et al., 2024; Kanemoto et al., 2025). Perfusion single-photon emission computed tomography (SPECT) is a relatively common modality in brain functional studies of NPS (Kazui et al., 2017; Nakase et al., 2023; Kashibayashi et al., 2024; Kanemoto et al., 2025). For example, cortical and hippocampal hypoperfusion has been associated with apathy or care refusal (Kazui et al., 2017; Kashibayashi et al., 2024), but given the heterogeneous results across studies, it may be necessary to confirm the reproducibility of some of these findings. Arterial spin labeling (ASL), which is an MRI technique used to non-invasively assess cerebral blood flow, has also been applied to NPS research (Jiang et al., 2023). 18F-Fludeoxyglucose positron emission tomography (FDG-PET), a nuclear medicine imaging modality that can measure cerebral glucose metabolism and is an essential modality in the treatment of dementia, is also used to study NPS, including in studies showing that the presence of NPS predicts hypometabolism in the posterior cingulate gyrus (PCG) and that sleep disturbances are associated with hypometabolism around the thalamus (Ng et al., 2017; Kanemoto et al., 2020).
Molecular imaging is an emerging topic in dementia research, and it has become a pivotal modality when coupled with disease-modifying therapies (van Dyck et al., 2022). This technique, which visualizes the deposition of proteins associated with neurodegeneration (e.g., amyloid and tau proteins), has also been applied to NPS research in recent years. It has generally been observed that NPS is more likely to be seen in individuals with greater depositions of tau or amyloid (Bensamoun et al., 2016; Tissot et al., 2021; Ge et al., 2022), but the number of such studies is limited.
The implementation of analyses of brain networks has been advocated in light of the complexity of the human brain with trillions of connections and interactions among the many regions of the brain. Several research groups have performed a brain network analysis concerning NPS, based on the functional connectivity derived from resting-state functional MRI (rs-fMRI) (Chang et al., 2020; Serra et al., 2020; Tumati et al., 2020; Zhao et al., 2024; Rashidi-Ranjbar et al., 2025; Wright et al., 2025). Associations between NPS and various networks (including the default-mode network) have been reported, but these need further validation. There are also a few reports about structural networks that were observed with DTI or morphological MRI (Pajavand et al., 2024; Michelutti et al., 2025). Decreased white matter networks around the limbic system and changes in the anatomical covariance networks are reported to be associated with NPS.
The use of artificial intelligence (AI), including machine learning, in the field of medicine has become a major trend in recent years, in brain imaging studies as well as many other fields. Nevertheless, few studies have used machine learning in NPS imaging research. Neuroimaging-based brain-age prediction is an advanced machine learning application that has been applied to calculate the age of individuals’ brains, and the gap between brain age and actual age is expected to be a novel biomarker for various neuropsychiatric disorders (Sone and Beheshti, 2022). A recent investigation of the relationship between brain-age and NPS indicates that apathy is associated with abnormal brain aging (Sone et al., 2025). Considering the advantages of machine learning analyses, these AI methods are expected to be applied to future NPS research.
As can be seen in Table 1, AD and amnestic MCI have been the most common targets of NPS studies. This may be due not only to the high prevalence of these two disorders but also to the availability of multicenter public databases, including the Alzheimer’s Disease Neuroimaging Initiative (ADNI). Other studies targeted FTD, cerebrovascular disease, or cognitive dysfunctions in Lewy body disease (Sellami et al., 2018; Kanemoto et al., 2020; Jaramillo-Jimenez et al., 2021; Ozzoude et al., 2023; Kim et al., 2024; Rashidi-Ranjbar et al., 2024; Kanemoto et al., 2025; Rashidi-Ranjbar et al., 2025; Sone et al., 2025; Wright et al., 2025). Other multicenter databases have also been accessed, including the National Alzheimer’s Coordinating Center (NACC) database, Translational Biomarkers in Aging and Dementia (TRIAD), the Genetic Frontotemporal Initiative (GENFI), the Ontario Neurodegenerative Research Initiative (ONDRI), and the J-BIRD (Japan multicenter study: Behavioral and psychological symptoms Integrated Research in Dementia). Some of these databases allow public access and some do not, which may lead to a high level of evidence in the future. In contrast, the targeted or reported subdomains of NPS are highly heterogeneous (Table 1), and thus a more unified research methodology is desired in this respect.
5 Integration of multimodal neuroimaging findings
Given the heterogeneity of research methods and targeted participants, it may be difficult at present to establish a unified view on the neural basis of NPS. However, focusing on studies with larger samples (N > 100), structural MRI studies consistently report abnormalities in the frontal and temporal lobes in NPS (Poulin et al., 2017; Ogama et al., 2018; Mohamed Nour et al., 2021; Siafarikas et al., 2021; Cannizzaro et al., 2023; Kameyama et al., 2024; Liampas et al., 2024). At a subdomain level, for aggression, frontal lobe abnormalities have been consistently reported (Ogama et al., 2018; Kameyama et al., 2024), whereas for depression and anxiety, atrophy of limbic structures was reported (Mohamed Nour et al., 2021; Cannizzaro et al., 2023). An FDG-PET study has shown that NPS predicts hypometabolism in the posterior cingulate gyrus (Ng et al., 2017), which may indicate that brain structure and metabolism in NPS are associated through the limbic circuit. Regarding other types of dementia than AD, there are still limited number of studies with relatively small sample size (mostly N < 100). Thus, it is not clear whether we can assume a similar neural basis of NPS in DLB or FTD to that in AD.
6 Future directions
Neuroimaging research that applies molecular imaging, multimodal imaging, multicenter or longitudinal data, network analyses, and machine learning are expected to play further significant roles in the future. More unified research methods are also important in terms of the reproducibility and generalizability of findings, and the same goes for the evaluations of NPS and its sub-domains.
The concept of mild behavioral impairment (MBI) has been proposed as a category of psychiatric and behavioral disturbance prior to the onset of typical cognitive symptoms in dementia (Ismail et al., 2016). Indeed, an increasing number of neuroimaging studies of MBI have been conducted (Matsuoka et al., 2023), and the expansion of the concepts of NPS may provide new insights into the relationship between psychiatric symptoms and neurodegeneration. Moreover, in addition to socio-cultural contextualization (Yi et al., 2024; Poon et al., 2025), it is also important to take into account the real-world functional impact of NPS on daily lives of patients and caregivers to advance precision medicine in this field (Karttunen et al., 2011; Chen et al., 2022).
In conclusion, although much imaging research has revealed aspects of the neural mechanisms of NPS, challenges remain, particularly in terms of the heterogeneity in methodologies and results. It is hoped that the further development of research methods will benefit both the individuals affected by neuropsychiatric symptoms and society.
Author contributions
DS: Conceptualization, Writing – original draft. SS: Conceptualization, Supervision, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by grants from the Japan Society for the Promotion of Science (KAKENHI) (nos. JP21K15720 and JP24K10690) and the Japan Agency for Medical Research and Development (AMED) (no. JP21dk0207056).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alzheimer’s Association (2024). 2024 Alzheimer’s disease facts and figures. Alzheimers Dement. 20, 3708–3821. doi: 10.1002/alz.13809
Anor, C. J., Dadar, M., Collins, D. L., and Tartaglia, M. C. (2021). The longitudinal assessment of neuropsychiatric symptoms in mild cognitive impairment and Alzheimer’s disease and their association with white matter hyperintensities in the national Alzheimer’s coordinating center’s uniform data set. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 6, 70–78. doi: 10.1016/j.bpsc.2020.03.006
Bensamoun, D., Guignard, R., Furst, A. J., Derreumaux, A., Manera, V., Darcourt, J., et al. (2016). Associations between neuropsychiatric symptoms and cerebral amyloid deposition in cognitively impaired elderly people. J. Alzheimers Dis. 49, 387–398. doi: 10.3233/JAD-150181
Boublay, N., Bouet, R., Dorey, J. M., Padovan, C., Makaroff, Z., Federico, D., et al. (2020). Brain volume predicts behavioral and psychological symptoms in Alzheimer’s disease. J. Alzheimers Dis. 73, 1343–1353. doi: 10.3233/JAD-190612
Boublay, N., Schott, A. M., and Krolak-Salmon, P. (2016). Neuroimaging correlates of neuropsychiatric symptoms in Alzheimer’s disease: A review of 20 years of research. Eur. J. Neurol. 23, 1500–1509. doi: 10.1111/ene.13076
Cannizzaro, A., Ronat, L., El Haffaf, L. M., Hanganu, A., and Adni. (2023). Associations between neuropsychiatric symptoms of affective and vegetative domains and brain morphology in aging people with mild cognitive impairment and Alzheimer’s disease. Int. J. Geriatr. Psychiatry 38:e5952. doi: 10.1002/gps.5952
Cerejeira, J., Lagarto, L., and Mukaetova-Ladinska, E. B. (2012). Behavioral and psychological symptoms of dementia. Front. Neurol. 3:73. doi: 10.3389/fneur.2012.00073
Chang, Y. T., Hsu, J. L., Huang, S. H., Hsu, S. W., Lee, C. C., and Chang, C. C. (2020). Functional connectome and neuropsychiatric symptom clusters of Alzheimer’s disease. J. Affect. Disord. 273, 48–54. doi: 10.1016/j.jad.2020.04.054
Chen, Y. R., Tan, C. H., Su, H. C., Chien, C. Y., Sung, P. S., Lin, T. Y., et al. (2022). Investigating the interaction between neuropsychiatry features and daily activities on social function in patients with Parkinson’s disease with mild cognitive impairment. BJPsych Open 8:e205. doi: 10.1192/bjo.2022.611
Counts, S. E., Ikonomovic, M. D., Mercado, N., Vega, I. E., and Mufson, E. J. (2017). Biomarkers for the early detection and progression of Alzheimer’s disease. Neurotherapeutics 14, 35–53. doi: 10.1007/s13311-016-0481-z
Cummings, J. L. (1997). The neuropsychiatric inventory: Assessing psychopathology in dementia patients. Neurology 48, S10–S16. doi: 10.1212/wnl.48.5_suppl_6.10s
Cummings, J. L., Mega, M., Gray, K., Rosenberg-Thompson, S., Carusi, D. A., and Gornbein, J. (1994). The neuropsychiatric inventory: Comprehensive assessment of psychopathology in dementia. Neurology 44, 2308–2314. doi: 10.1212/wnl.44.12.2308
David, N. D., Lin, F., Porsteinsson, A. P., and Alzheimer’s Disease Neuroimaging Initiative. (2016). Trajectories of neuropsychiatric symptoms and cognitive decline in mild cognitive impairment. Am. J. Geriatr. Psychiatry 24, 70–80. doi: 10.1016/j.jagp.2015.06.001
Devanand, D. P., Brockington, C. D., Moody, B. J., Brown, R. P., Mayeux, R., Endicott, J., et al. (1992). Behavioral syndromes in Alzheimer’s disease. Int. Psychogeriatr. 4, 161–184. doi: 10.1017/S104161029200125X
El Haffaf, L. M., Ronat, L., Cannizzaro, A., Hanganu, A., and Alzheimer’s Disease Neuroimaging Initiative. (2024). Associations between hyperactive neuropsychiatric symptoms and brain morphology in mild cognitive impairment and Alzheimer’s disease. J. Alzheimers Dis. 97, 841–853. doi: 10.3233/JAD-220857
Fan, W., Ma, S., Wang, Z., Han, Y., Liu, X., Gu, R., et al. (2023). Correlation between white matter hyperintensity and delusional symptoms in Alzheimer’s disease. BMC Psychiatry 23:914. doi: 10.1186/s12888-023-05420-5
Garcia-Alberca, J. M., Florido, M., Caceres, M., Sanchez-Toro, A., Lara, J. P., and Garcia-Casares, N. (2019). Medial temporal lobe atrophy is independently associated with behavioural and psychological symptoms in Alzheimer’s disease. Psychogeriatrics 19, 46–54. doi: 10.1111/psyg.12363
GBD 2019 Dementia Forecasting Collaborators (2022). Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 7, e105–e125. doi: 10.1016/S2468-2667(21)00249-8
Ge, X., Qiao, Y., Choi, J., Raman, R., Ringman, J. M., Shi, Y., et al. (2022). Enhanced association of tau pathology and cognitive impairment in mild cognitive impairment subjects with behavior symptoms. J. Alzheimers Dis. 87, 557–568. doi: 10.3233/JAD-215555
Gitlin, L. N., Marx, K. A., Stanley, I. H., Hansen, B. R., and Van Haitsma, K. S. (2014). Assessing neuropsychiatric symptoms in people with dementia: A systematic review of measures. Int. Psychogeriatr. 26, 1805–1848. doi: 10.1017/S1041610214001537
Guan, D. X., Rehman, T., Nathan, S., Durrani, R., Potvin, O., Duchesne, S., et al. (2024). Neuropsychiatric symptoms: Risk factor or disease marker? A study of structural imaging biomarkers of Alzheimer’s disease and incident cognitive decline. Hum. Brain Mapp. 45:e70016. doi: 10.1002/hbm.70016
Hiu, S. K. W., Bigirumurame, T., Kunonga, P., Bryant, A., and Pillai, M. (2022). Neuropsychiatric Inventory domains cluster into neuropsychiatric syndromes in Alzheimer’s disease: A systematic review and meta-analysis. Brain Behav. 12:e2734. doi: 10.1002/brb3.2734
Huey, E. D., Lee, S., Cheran, G., Grafman, J., Devanand, D. P., and Alzheimer’s Disease Neuroimaging Initiative. (2017). Brain regions involved in arousal and reward processing are associated with apathy in Alzheimer’s disease and frontotemporal dementia. J. Alzheimers Dis. 55, 551–558. doi: 10.3233/JAD-160107
Ismail, Z., Smith, E. E., Geda, Y., Sultzer, D., Brodaty, H., Smith, G., et al. (2016). Neuropsychiatric symptoms as early manifestations of emergent dementia: Provisional diagnostic criteria for mild behavioral impairment. Alzheimers Dement. 12, 195–202. doi: 10.1016/j.jalz.2015.05.017
Jaramillo-Jimenez, A., Giil, L. M., Tovar-Rios, D. A., Borda, M. G., Ferreira, D., Bronnick, K., et al. (2021). Association between amygdala volume and trajectories of neuropsychiatric symptoms in Alzheimer’s disease and dementia with lewy bodies. Front. Neurol. 12:679984. doi: 10.3389/fneur.2021.679984
Jiang, J., Wang, A., Liu, Y., Yao, Z., Sun, M., Jiang, T., et al. (2023). Spatiotemporal characteristics of regional brain perfusion associated with neuropsychiatric symptoms in patients with Alzheimer’s disease. J. Alzheimers Dis. 95, 981–993. doi: 10.3233/JAD-230499
Kameyama, H., Tagai, K., Takasaki, E., Kashibayashi, T., Takahashi, R., Kanemoto, H., et al. (2024). Examining frontal lobe asymmetry and its potential role in aggressive behaviors in early Alzheimer’s disease. J. Alzheimers Dis. 98, 539–547. doi: 10.3233/JAD-231306
Kanemoto, H., Kashibayashi, T., Takahashi, R., Suehiro, T., Satake, Y., Taomoto, D., et al. (2025). Neuroimaging of psychosis, agitation, and affective disturbance in Alzheimer’s disease, dementia with Lewy bodies, and mild cognitive impairment. Int. Psychogeriatr. 37:100059. doi: 10.1016/j.inpsyc.2025.100059
Kanemoto, H., Kazui, H., Adachi, H., Yoshiyama, K., Wada, T., Nomura, K. T., et al. (2020). Thalamic pulvinar metabolism, sleep disturbances, and hallucinations in dementia with Lewy bodies: Positron emission tomography and actigraphy study. Int. J. Geriatr. Psychiatry 35, 934–943. doi: 10.1002/gps.5315
Karttunen, K., Karppi, P., Hiltunen, A., Vanhanen, M., Valimaki, T., Martikainen, J., et al. (2011). Neuropsychiatric symptoms and quality of life in patients with very mild and mild Alzheimer’s disease. Int. J. Geriatr. Psychiatry 26, 473–482. doi: 10.1002/gps.2550
Kashibayashi, T., Kanemoto, H., Takahashi, R., Fujito, R., Chadani, Y., Tagai, K., et al. (2024). Neural basis of agitated behaviors in patients with amnestic mild cognitive impairment and Alzheimer’s disease. J. Alzheimers Dis. 100, 1399–1406. doi: 10.3233/JAD-240256
Kazui, H., Takahashi, R., Yamamoto, Y., Yoshiyama, K., Kanemoto, H., Suzuki, Y., et al. (2017). Neural basis of apathy in patients with amnestic mild cognitive impairment. J. Alzheimers Dis. 55, 1403–1416. doi: 10.3233/JAD-160223
Khoury, M. A., Valcic, M., Churchill, N. W., Di Battista, A., De Luca, V., Fornazzari, L. R., et al. (2025). Sex differences in cortical thickness and neuropsychiatric symptom burden based on APOE4 Homozygosity in Alzheimer’s disease. Am. J. Med. Genet. B Neuropsychiatr. Genet. 198:e33008. doi: 10.1002/ajmg.b.33008
Kim, S., Na, H. K., Sun, Y., Yoon, Y. J., Chung, S. J., Sohn, Y. H., et al. (2024). Regional burden of enlarged perivascular spaces and cognition and neuropsychiatric symptoms in drug-naive patients with Parkinson disease. Neurology 102:e209483. doi: 10.1212/WNL.0000000000209483
Liampas, I., Siokas, V., Stamati, P., Kyriakoulopoulou, P., Tsouris, Z., Zoupa, E., et al. (2024). Neuropsychiatric symptoms associated with frontotemporal atrophy in older adults without dementia. Int. J. Geriatr Psychiatry 39:e70008. doi: 10.1002/gps.70008
Lu, H., Xu, C., and Liang, J. (2025). Evaluation of AccuBrain-based MRI quantitative analysis in diagnosing Alzheimer’s disease and assessing behavioral and psychological symptoms of dementia. Aging Clin. Exp. Res. 37:126. doi: 10.1007/s40520-025-03023-6
Makovac, E., Serra, L., Spano, B., Giulietti, G., Torso, M., Cercignani, M., et al. (2016). different patterns of correlation between grey and white matter integrity account for behavioral and psychological symptoms in Alzheimer’s disease. J. Alzheimers Dis. 50, 591–604. doi: 10.3233/JAD-150612
Marin, R. S., Biedrzycki, R. C., and Firinciogullari, S. (1991). Reliability and validity of the apathy evaluation scale. Psychiatry Res. 38, 143–162. doi: 10.1016/0165-1781(91)90040-v
Marin-Marin, L., Renau-Lagranja, J., Avila, C., and Costumero, V. (2024). Depression and agitation factors are related to regional brain atrophy and faster longitudinal cognitive decline in mild cognitive impairment. J. Alzheimers Dis. 97, 1341–1351. doi: 10.3233/JAD-230929
Matsuoka, T., Imai, A., and Narumoto, J. (2023). Neuroimaging of mild behavioral impairment: A systematic review. PCN Rep. 2:e81. doi: 10.1002/pcn5.81
Matuskova, V., Ismail, Z., Nikolai, T., Markova, H., Cechova, K., Nedelska, Z., et al. (2021). Mild behavioral impairment is associated with atrophy of entorhinal cortex and hippocampus in a memory clinic cohort. Front. Aging Neurosci. 13:643271. doi: 10.3389/fnagi.2021.643271
Michelutti, M., Urso, D., Tafuri, B., Gnoni, V., Giugno, A., Zecca, C., et al. (2025). Structural covariance network patterns linked to neuropsychiatric symptoms in biologically defined Alzheimer’s disease: Insights from the mild behavioral impairment checklist. J. Alzheimers Dis. 104, 338–350. doi: 10.1177/13872877251316794
Misquitta, K., Dadar, M., Louis Collins, D., Tartaglia, M. C., and Alzheimer’s Disease Neuroimaging Initiative. (2020). White matter hyperintensities and neuropsychiatric symptoms in mild cognitive impairment and Alzheimer’s disease. Neuroimage Clin. 28:102367. doi: 10.1016/j.nicl.2020.102367
Mohamed Nour, A. E. A., Jiao, Y., Teng, G. J., and Alzheimer’s Disease Neuroimaging Initiative. (2021). Neuroanatomical associations of depression, anxiety and apathy neuropsychiatric symptoms in patients with Alzheimer’s disease. Acta Neurol. Belg. 121, 1469–1480. doi: 10.1007/s13760-020-01349-8
Nakase, T., Thyreau, B., Tatewaki, Y., Tomita, N., Takano, Y., Muranaka, M., et al. (2023). Association between gray and white matter lesions and its involvement in clinical symptoms of Alzheimer’s-type dementia. J. Clin. Med. 12:7642. doi: 10.3390/jcm12247642
Ng, K. P., Pascoal, T. A., Mathotaarachchi, S., Chung, C. O., Benedet, A. L., Shin, M., et al. (2017). Neuropsychiatric symptoms predict hypometabolism in preclinical Alzheimer disease. Neurology 88, 1814–1821. doi: 10.1212/WNL.0000000000003916
Nowrangi, M. A., Marano, C., Oishi, K., Mori, S., Sair, H. I., Outen, J., et al. (2021). The association of neuropsychiatric symptoms with regional brain volumes from patients in a tertiary multi-disciplinary memory clinic. Int. Psychogeriatr. 33, 233–244. doi: 10.1017/S1041610220000113
Ogama, N., Sakurai, T., Saji, N., Nakai, T., Niida, S., Toba, K., et al. (2018). Frontal White matter hyperintensity is associated with verbal aggressiveness in elderly women with Alzheimer disease and amnestic mild cognitive impairment. Dement. Geriatr. Cogn. Dis. Extra 8, 138–150. doi: 10.1159/000486826
Ozzoude, M., Varriano, B., Beaton, D., Ramirez, J., Adamo, S., Holmes, M. F., et al. (2023). White matter hyperintensities and smaller cortical thickness are associated with neuropsychiatric symptoms in neurodegenerative and cerebrovascular diseases. Alzheimers Res. Ther. 15:114. doi: 10.1186/s13195-023-01257-y
Pajavand, A. M., Grothe, M. J., De Schotten, M. T., Giorgi, F. S., Vergallo, A., Hampel, H., et al. (2024). Structural white matter connectivity differences independent of gray matter loss in mild cognitive impairment with neuropsychiatric symptoms: Early indicators of Alzheimer’s disease using network-based statistics. J. Alzheimers Dis. 102, 1042–1056. doi: 10.1177/13872877241288710
Perlman, C. M., and Hirdes, J. P. (2008). The aggressive behavior scale: A new scale to measure aggression based on the minimum data set. J. Am. Geriatr. Soc. 56, 2298–2303. doi: 10.1111/j.1532-5415.2008.02048.x
Poon, S. F., Tan, C. H., Hong, W. P., Chen, K. C., and Yu, R. L. (2025). Tailoring anxiety assessment for Parkinson’s disease: The Chinese Parkinson anxiety scale with cultural and situational anxiety considerations. Soc. Sci. Med. 381:118284. doi: 10.1016/j.socscimed.2025.118284
Poulin, S. P., Bergeron, D., Dickerson, B. C., and Alzheimer’s Disease Neuroimaging Initiative. (2017). Risk factors, neuroanatomical correlates, and outcome of neuropsychiatric symptoms in Alzheimer’s disease. J. Alzheimers Dis. 60, 483–493. doi: 10.3233/JAD-160767
Radue, R., Walaszek, A., and Asthana, S. (2019). Neuropsychiatric symptoms in dementia. Handb. Clin. Neurol. 167, 437–454. doi: 10.1016/B978-0-12-804766-8.00024-8
Rashidi-Ranjbar, N., Churchill, N. W., Black, S. E., Kumar, S., Tartaglia, M. C., Freedman, M., et al. (2025). A cross sectional and longitudinal assessment of neuropsychiatric symptoms and brain functional connectivity in patients with mild cognitive impairment, cerebrovascular disease and parkinson disease. Int. J. Geriatr. Psychiatry 40:e70075. doi: 10.1002/gps.70075
Rashidi-Ranjbar, N., Churchill, N. W., Black, S. E., Kumar, S., Tartaglia, M. C., Freedman, M., et al. (2024). Neuropsychiatric symptoms and brain morphology in patients with mild cognitive impairment, cerebrovascular disease and Parkinson disease: A cross sectional and longitudinal study. Int. J. Geriatr. Psychiatry 39:e6074. doi: 10.1002/gps.6074
Reisberg, B., Borenstein, J., Salob, S. P., Ferris, S. H., Franssen, E., and Georgotas, A. (1987). Behavioral symptoms in Alzheimer’s disease: Phenomenology and treatment. J. Clin. Psychiatry 48, 9–15. doi: 10.1037/t13385-000
Robert, P. H., Verhey, F. R., Byrne, E. J., Hurt, C., De Deyn, P. P., Nobili, F., et al. (2005). Grouping for behavioral and psychological symptoms in dementia: Clinical and biological aspects. Consensus paper of the European Alzheimer disease consortium. Eur. Psychiatry 20, 490–496. doi: 10.1016/j.eurpsy.2004.09.031
Sellami, L., Bocchetta, M., Masellis, M., Cash, D. M., Dick, K. M., van Swieten, J., et al. (2018). Distinct neuroanatomical correlates of neuropsychiatric symptoms in the three main forms of genetic frontotemporal dementia in the GENFI cohort. J. Alzheimers Dis. 65, 147–163. doi: 10.3233/JAD-180053
Serra, L., Bruschini, M., Di Domenico, C., Mancini, M., Bechi Gabrielli, G., Bonarota, S., et al. (2020). Behavioral psychological symptoms of dementia and functional connectivity changes: A network-based study. Neurobiol. Aging 94, 196–206. doi: 10.1016/j.neurobiolaging.2020.06.009
Siafarikas, N., Alnaes, D., Monereo-Sanchez, J., Lund, M. J., Selbaek, G., Stylianou-Korsnes, M., et al. (2021). Neuropsychiatric symptoms and brain morphology in patients with mild cognitive impairment and Alzheimer’s disease with dementia. Int. Psychogeriatr. 33, 1217–1228. doi: 10.1017/S1041610221000934
Sone, D., and Beheshti, I. (2022). Neuroimaging-based brain age estimation: A promising personalized biomarker in neuropsychiatry. J. Pers. Med. 12:1850. doi: 10.3390/jpm12111850
Sone, D., Beheshti, I., Tagai, K., Kameyama, H., Takasaki, E., Kashibayashi, T., et al. (2025). Neuropsychiatric symptoms and neuroimaging-based brain age in mild cognitive impairment and early dementia: A multicenter study. Psychiatry Clin. Neurosci. 79, 158–164. doi: 10.1111/pcn.13777
Tachibana, A., Iga, J. I., Ozaki, T., Yoshino, Y., Yamazaki, K., Ochi, S., et al. (2024). Behavioral and psychological symptoms and brain volumes in community-dwelling older persons from the Nakayama Study. Sci. Rep. 14:26097. doi: 10.1038/s41598-024-77477-5
Tampi, R. R., and Jeste, D. V. (2022). Dementia is more than memory loss: Neuropsychiatric symptoms of dementia and their nonpharmacological and pharmacological management. Am. J. Psychiatry 179, 528–543. doi: 10.1176/appi.ajp.20220508
Tissot, C., Therriault, J., Pascoal, T. A., Chamoun, M., Lussier, F. Z., Savard, M., et al. (2021). Association between regional tau pathology and neuropsychiatric symptoms in aging and dementia due to Alzheimer’s disease. Alzheimers Dement. 7:e12154. doi: 10.1002/trc2.12154
Tu, M. C., Huang, W. H., Hsu, Y. H., Lo, C. P., Deng, J. F., and Huang, C. F. (2017). Comparison of neuropsychiatric symptoms and diffusion tensor imaging correlates among patients with subcortical ischemic vascular disease and Alzheimer’s disease. BMC Neurol. 17:144. doi: 10.1186/s12883-017-0911-5
Tumati, S., Marsman, J. C., De Deyn, P. P., Martens, S., Aleman, A., and Alzheimer’s Disease Neuroimaging Initiative. (2020). Functional network topology associated with apathy in Alzheimer’s disease. J. Affect. Disord. 266, 473–481. doi: 10.1016/j.jad.2020.01.158
van Dyck, C. H., Swanson, C. J., Aisen, P., Bateman, R. J., Chen, C., Gee, M., et al. (2022). Lecanemab in early Alzheimer’s disease. N. Engl. J. Med. 388, 9–21. doi: 10.1056/NEJMoa2212948
Wright, L. M., Donaghy, P. C., Burn, D. J., Taylor, J. P., O’Brien, J. T., Yarnall, A. J., et al. (2025). Brain network connectivity underlying neuropsychiatric symptoms in prodromal Lewy body dementia. Neurobiol. Aging 151, 95–106. doi: 10.1016/j.neurobiolaging.2025.04.007
Yesavage, J. A., Brink, T. L., Rose, T. L., Lum, O., Huang, V., Adey, M., et al. (1982). Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 17, 37–49. doi: 10.1016/0022-3956(82)90033-4
Yi, H. J., Tan, C. H., Hong, W. P., and Yu, R. L. (2024). Development and validation of the geriatric apathy scale: Examining multi-dimensional apathy profiles in a neurodegenerative population with cultural considerations. Asian J. Psychiatr. 93:103924. doi: 10.1016/j.ajp.2024.103924
Zhao, K., Xie, H., Fonzo, G. A., Carlisle, N. B., Osorio, R. S., and Zhang, Y. (2024). Dementia subtypes defined through neuropsychiatric symptom-associated brain connectivity patterns. JAMA Netw. Open 7:e2420479. doi: 10.1001/jamanetworkopen.2024.20479
Zhou, Y., Wei, L., Gao, S., Wang, J., and Hu, Z. (2023). Characterization of diffusion magnetic resonance imaging revealing relationships between white matter disconnection and behavioral disturbances in mild cognitive impairment: A systematic review. Front. Neurosci. 17:1209378. doi: 10.3389/fnins.2023.1209378
Keywords: neuropsychiatric symptoms, behavioral psychological symptoms in dementia, dementia, neuroimaging, magnetic resonance imaging, positron emission tomography
Citation: Sone D and Shinagawa S (2025) Seeking the neural basis of neuropsychiatric symptoms in dementia: neuroimaging findings and controversies. Front. Aging Neurosci. 17:1633309. doi: 10.3389/fnagi.2025.1633309
Received: 22 May 2025; Accepted: 31 July 2025;
Published: 12 August 2025.
Edited by:
Quelen Iane Garlet, Federal University of Paraná, BrazilReviewed by:
Rwei-Ling Yu, National Cheng Kung University, TaiwanCopyright © 2025 Sone and Shinagawa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daichi Sone, ZC1zb25lQGppa2VpLmFjLmpw