 Rafael Villino-Rodríguez1,2*
Rafael Villino-Rodríguez1,2* Mirla M. Ríos-Rivera1,3
Mirla M. Ríos-Rivera1,3 Genoveva Montoya-Murillo1
Genoveva Montoya-Murillo1 Jonathan Patricio Baldera4Salomón Salazar-Londoño5María Cruz Rodríguez-Oroz1Miguel Germán Borda1,4
Jonathan Patricio Baldera4Salomón Salazar-Londoño5María Cruz Rodríguez-Oroz1Miguel Germán Borda1,4 Adolfo Jiménez-Huete1
Adolfo Jiménez-Huete1 Mario Riverol1
Mario Riverol1- 1Department of Neurology, Clínica Universidad de Navarra, Pamplona, Spain
- 2Department of Neurology, Hospital Universitario HM, Sanchinarro, Madrid, Spain
- 3School of Medicine, Universidad Autónoma de Chiriquí, David, Panama
- 4Centre for Age-Related Medicine (SESAM), Stavanger University Hospital, Stavanger, Norway
- 5Semillero de Neurociencias y Envejecimiento, Ageing Institute, Medical School, Pontificia Universidad Javeriana, Bogotá, Colombia
Background and objectives: Subjective Cognitive Decline (SCD) is recognized as an early indicator of neurodegeneration, yet factors that predict its progression to mild cognitive impairment (MCI) or dementia remains not fully understood. In this study, we aim to identify clinical and neuropsychological features associated with the progression of SCD.
Methods: 450 persons with SCD were included, consisting in 319 non progressors (SCDnp) and 131 progressors (SCDp) to MCI or dementia due to AD. The study was conducted at the Clínica Universidad de Navarra Memory Clinic between 2001 and 2017. We included data on medical interviews and neuropsychological evaluations. Differences between SCDnp and SCDp were assessed and, to evaluate the association between exposure variables and progression in time, proportional-hazards Cox models were applied. In addition to the exposure variables, the models were adjusted for age, sex, and years of education.
Results: At baseline, SCDp were older, had a higher prevalence of hypertension and hypercholesterolemia and had worst performance on tests related to processing speed, verbal fluency, visual memory, verbal memory, and executive functioning. Factors associated with progression at follow-up were lower scores in some cognitive tests: MMSE, TMT-B, and the CERAD regarding trial 1 of immediate recall, trial 2 of immediate recall, trial 3 of immediate recall and the delay recall score.
Discussion: Lower scores on global cognition, executive functioning and verbal memory tests were predictors of progression to MCI or dementia in patients with SCD. These findings underscore the importance of nuances in neuropsychological evaluation, even with a normal score, for detecting high-risk individuals for early intervention.
1 Introduction
Dementia is one of the most disabling diseases in older adults, imposing a significant societal burden due to its high frequency and costs (Scheltens et al., 2016). In the natural evolution of cognitive impairment, such as in Alzheimer’s disease (AD), patients progress through three phases: preclinical, where disease mechanisms begin without noticeable cognitive decline; prodromal, marked by mild cognitive impairment (MCI); and dementia, where cognitive impairment significantly affects daily life functioning (Jack et al., 2024). However, some individuals in the preclinical phase may experience mild cognitive symptoms, or report a complaint about their cognitive performance, while still performing normally on cognitive tests. This condition is now referred to as subjective cognitive decline (SCD), and its distinction with MCI relies on neuropsychological evaluations (Jessen et al., 2020).
SCD is a common condition in aging, affecting 25–50% of individuals aged 65 years or older (Jessen et al., 2014). It has been described that it can emerge even up to 15 years before an MCI diagnosis (Jessen et al., 2014; Molinuevo et al., 2017). Moreover, while often linked to neurodegenerative disorders, it can also result from normal aging, systemic illnesses, psychiatric conditions and non-neurodegenerative neurological disorders (Jessen et al., 2014; Reisberg et al., 2008). Thus, SCD is not always a direct indicator of preclinical AD (Jessen et al., 2014), or of another neurodegenerative disease.
Various factors can contribute to the development of SCD, with depressive symptoms being especially important (Liew, 2019). Studies suggest that having SCD and depression predicts cognitive decline and correlates with increased amyloid pathology, highlighting its potential as a longitudinal risk marker (Kleineidam et al., 2023). However, it is not always easy to determine whether SCD is solely present in the context of depression as a primary psychiatric disorder, or concomitantly as a neuropsychiatric symptom in an underlying neurodegenerative process.
Evidence also suggests that other clinical factors, such as cardiovascular risk, may be associated with the onset of SCD. However, the role of these factors in the progression to MCI or AD dementia remains unclear. While some studies indicate a possible link, the findings are often inconsistent (Dufouil et al., 2005).
Considering the relevance of neuropsychological performance and the initial clinical evaluation in SCD diagnosis, in this study we aim to investigate the factors related with progression from SCD to MCI or dementia.
2 Methods
An observational longitudinal cohort study was designed, and the STROBE checklist for cohort studies was followed. The initial sample included 1,013 patients who were evaluated at the memory clinic of Clínica Universidad de Navarra between 2001 and 2017. Of these, 945 individuals with SCD—defined as self-reported memory complaints despite normal performance on neuropsychological tests—were initially considered. The diagnosis of SCD was based on the Jessen SCD-I criteria. The SCD-plus criteria were not applied because the necessary data to fulfill those criteria, apart from age, were not available (Jessen et al., 2014). Differences between participants who were not included in the analysis due to lack of follow-up and those who completed follow-up are presented in Supplementary material.
To determine the normality of cognitive status, the scores obtained from the tests were adjusted for age, sex, and education level. This yields a cutoff point of ≥7 in scaled scores, according to the standardization for the Spanish population, based on the ‘Neuronorma’ project (Rocca et al., 2012; Lopez Miquel and Agustí, 2011; Casals-Coll et al., 2013; Peña-Casanova et al., 2009; Peña-Casanova et al., 2009; Peña-Casanova et al., 2009). Normal cognitive function was defined as performance exceeding −1.5 standard deviations (SD) from the age-, sex-, and education-adjusted normal range on all tests (Molinuevo et al., 2017; Rocca et al., 2012; Lopez Miquel and Agustí, 2011; Casals-Coll et al., 2013; Peña-Casanova et al., 2009; Peña-Casanova et al., 2009; Peña-Casanova et al., 2009).
All participants were evaluated by a behavioral neurologist. The initial assessment included a medical and history review, an interview with a family member or friend, and a general and neurological examination. All participants underwent laboratory tests (i.e., full blood count, biochemistry, vitamin B12, serum folate, glucose, lipids, syphilis serology and thyroid function), neuropsychological assessment, and brain magnetic resonance imaging (MRI). Data from patients were reviewed in a multidisciplinary consensus meeting to determine a clinical diagnosis.
The exclusion criteria for the present study were: having MCI or dementia (McKhann et al., 2011; Albert et al., 2011), significant neurological or systemic illness that could lead to cognitive impairment, present or past major psychiatric disorders (e.g., schizophrenia, major depression, and bipolar disorder), a history of alcohol or substance abuse, notable MRI abnormalities (e.g., brain tumors, large cerebral infarct, and bleeding), and a previous head trauma resulting in loss of consciousness.
Of the 945 participants with SCD, 450 were followed up at our clinic and completed one or more follow-up visits through January 2020. Follow-up was voluntary, with patients typically scheduled for annual evaluations. Each visit included an assessment by a neurologist and a comprehensive neuropsychological evaluation to determine clinical progression. Follow-up concluded when a diagnosis of MCI or dementia was made.
Among the 450 patients who were followed, 131 progressed to MCI or dementia (AD dementia = 16 patients, non-AD dementia = 1 patient [Vascular dementia]) and were classified as SCD progressors (SCDp). In contrast, 319 remained clinically stable and were classified as SCD non-progressors (SCDnp) during the follow-up (see Supplementary material). The diagnoses of MCI and AD were based on the clinical criteria established by the National Institute on Aging and the Alzheimer’s Association (NIA-AA) in 2011 (McKhann et al., 2011; Albert et al., 2011).
This study was approved by the Ethics Research Committee of the Universidad of Navarra. Written informed consent was obtained from all participants.
2.1 Measures
Demographic variables included age of SCD diagnosis, age of MCI or dementia diagnosis, sex and years of education. Based on self-report, report by a family member or by clinical records, registered medical conditions included arterial hypertension, diabetes mellitus, hypercholesterolemia, cardiovascular disease (e.g., hearth failure, acute myocardial infarction), cerebrovascular disease (including ischemic and hemorrhagic strokes) and smoking.
All subjects underwent a neuropsychological assessment to evaluate cognitive status at baseline using a comprehensive test battery that evaluated the following domains: global cognitive function [Mini-Mental State Examination (MMSE)]; depression [Geriatric Depression Scale (GDS) with 30 items]; episodic verbal memory (word list learning, recall and recognition) and episodic visual memory (figure recall) based on the [The Consortium to Establish a Registry for Alzheimer’s Disease Word List Memory Task (CERAD)]; processing speed [Trail Making Test (TMT) parts A]; executive function [Trail Making Test (TMT) part B], phonetic fluency (words with letter p), cognitive interference [The Stroop Colour and Word Test (SCWT)]; and language [animal categories and the Boston naming test (BNT)] (Rocca et al., 2012; Lopez Miquel and Agustí, 2011; Casals-Coll et al., 2013; Peña-Casanova et al., 2009; Peña-Casanova et al., 2009; Peña-Casanova et al., 2009).
Interindividual differences are supported by a standardized medical and cognitive assessment, improving reliability. As mentioned, the normality of cognitive tests was based on already stablished cutoff points for the Spanish population. All patients received the same protocolized assessment by a behavioral neurologist, and the same diagnostic criteria was applied. All the patients come from the same cohort and were evaluated at the same center.
2.2 Statistical analysis
An initial description of the cohort was produced by calculating means ± standard deviations (SD) for continuous variables and frequencies (percentages) for categorical variables. The comparative analyses between individuals with subjective cognitive decline and healthy controls are presented in Supplementary material. Differences between the subjective cognitive decline (SCD) as a progressors (SCDp) and non progressors (SCDnp) group were assessed with Student’s t-test for both means and proportions. Also, differences between the subjective cognitive decline (SCD) group and the control group were assessed with Welch’s t-test for both means and proportions, given the marked imbalance in sample size (945 vs. 68 subjects) and the likelihood of unequal variances (see Supplementary material).
To evaluate the association between the clinical and neuropsychological variables of interest and the risk of progressing from SCD to more advanced cognitive impairment, proportional-hazards Cox models were applied. The dependent variable was the time (months) elapsed from the baseline assessment to the date of clinical progression (event). In addition to the exposure variables, the models were adjusted for age, sex, and years of education. Cognitive test scores were standardized (age-adjusted z-scores) to facilitate comparability across domains, and hazard ratios were expressed per one standard deviation (1-SD) increase in the corresponding variable. The proportional-hazards assumption was verified with the global Schoenfeld residuals test, which showed no significant violations (p > 0.05). Results are reported as hazard ratios (HRs) with their corresponding 95% confidence intervals (95% CI) and p-values; Kaplan–Meier curves with 95% confidence bands and log-rank tests were constructed for selected exposure variables. For those exposure variables, the values were dichotomized based on the first quartile of their distribution in the sample, classifying participants with scores ≤ Q1 versus those with scores > Q1. A sensitivity analysis was conducted for both baseline demographic and clinical characteristics, comparing included and excluded participants to assess potential selection bias. All analyses were performed in R Studio version 4.3.1, and statistical significance was set at α = 0.05 and the Benjamini-Hochberg method was used to adjust for multiple comparisons.
3 Results
At baseline, SCDp were older and had a higher prevalence of hypertension and hypercholesterolemia. Regarding the neuropsychological analysis, SCDp had worst performance on tests related with processing speed (TMT-A), verbal fluency (animals), visual memory (figure recall), verbal memory (CERAD: immediate recall, delay recall, recognition score) and executive functioning (Stroop total and TMT-B). After adjusting the scores for age, the test related to visual memory and one of the tests assessing executive function (Stroop total) no longer reached statistical significance.
Descriptive characteristics are displayed in Table 1.
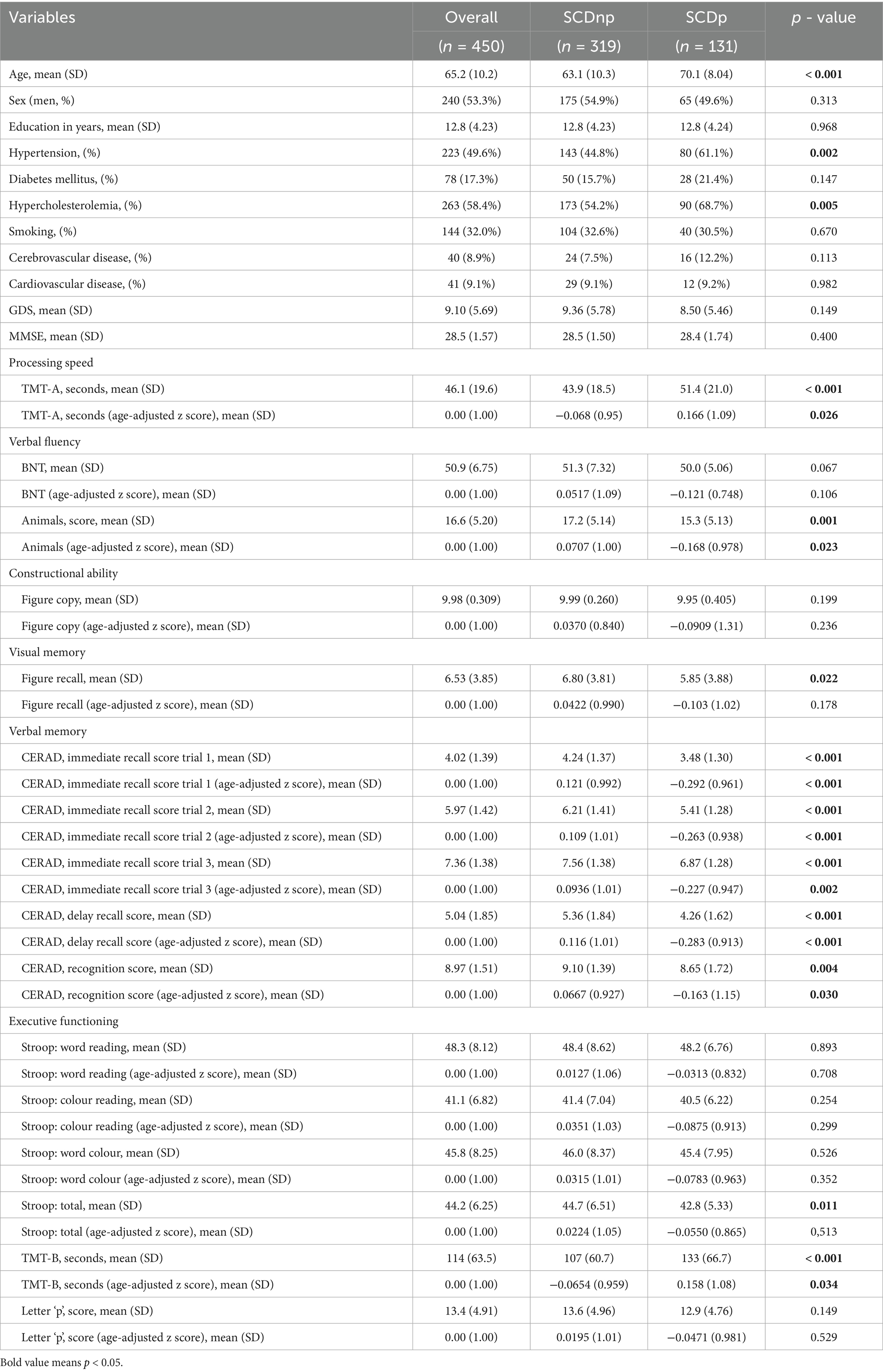
Table 1. Clinical and neuropsychological differences between groups at baseline.
The mean follow-up duration was longer in SCDp patients compared to SCDnp patients (76.33 ± 50.59 months vs. 72.68 ± 51.61 months). Table 2 shows the adjusted risk of progression to MCI or AD. Statistically significant results were found for MMSE (HR = 0.855, IC95% 0.771–0.948, p = 0.003), TMT-B (HR = 1.239, IC95% 1.051–1.462, p = 0.011), and the CERAD regarding trial 1 of immediate recall (HR = 0.580, IC95% 0.464–0.726, p < 0.001), trial 2 of immediate recall (HR = 0.623, IC95% 0.507–0.766, p < 0.001), trial 3 of immediate recall (HR = 0.644, IC95% 0.526–0.788, p < 0.001) and the delay recall score (HR = 0.657, IC95% 0.532–0.812, p < 0.001). Figure 1 shows the probability of remaining in SCD based on the performance on the CERAD delayed recall and the MMSE.
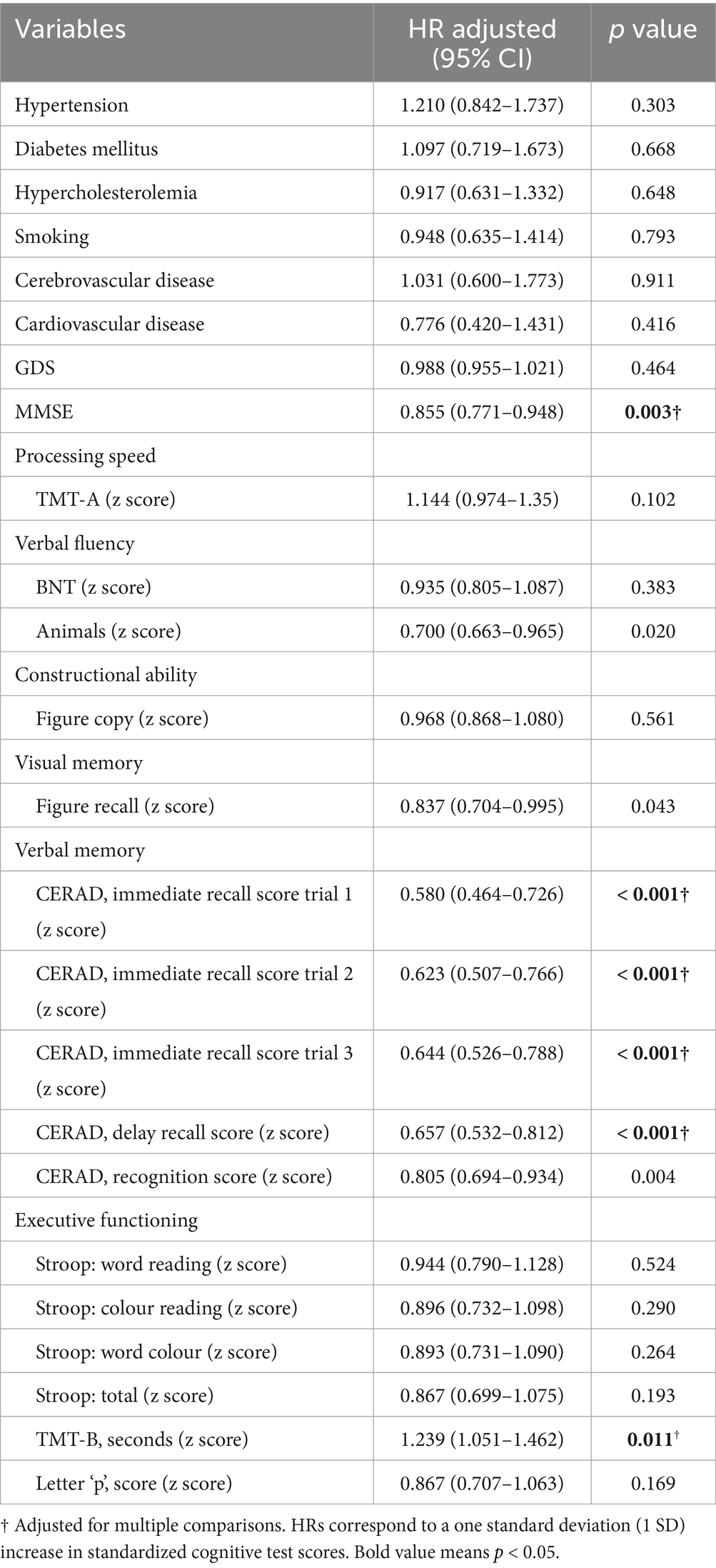
Table 2. Association between clinical and neuropsychological variables and the risk of progression.
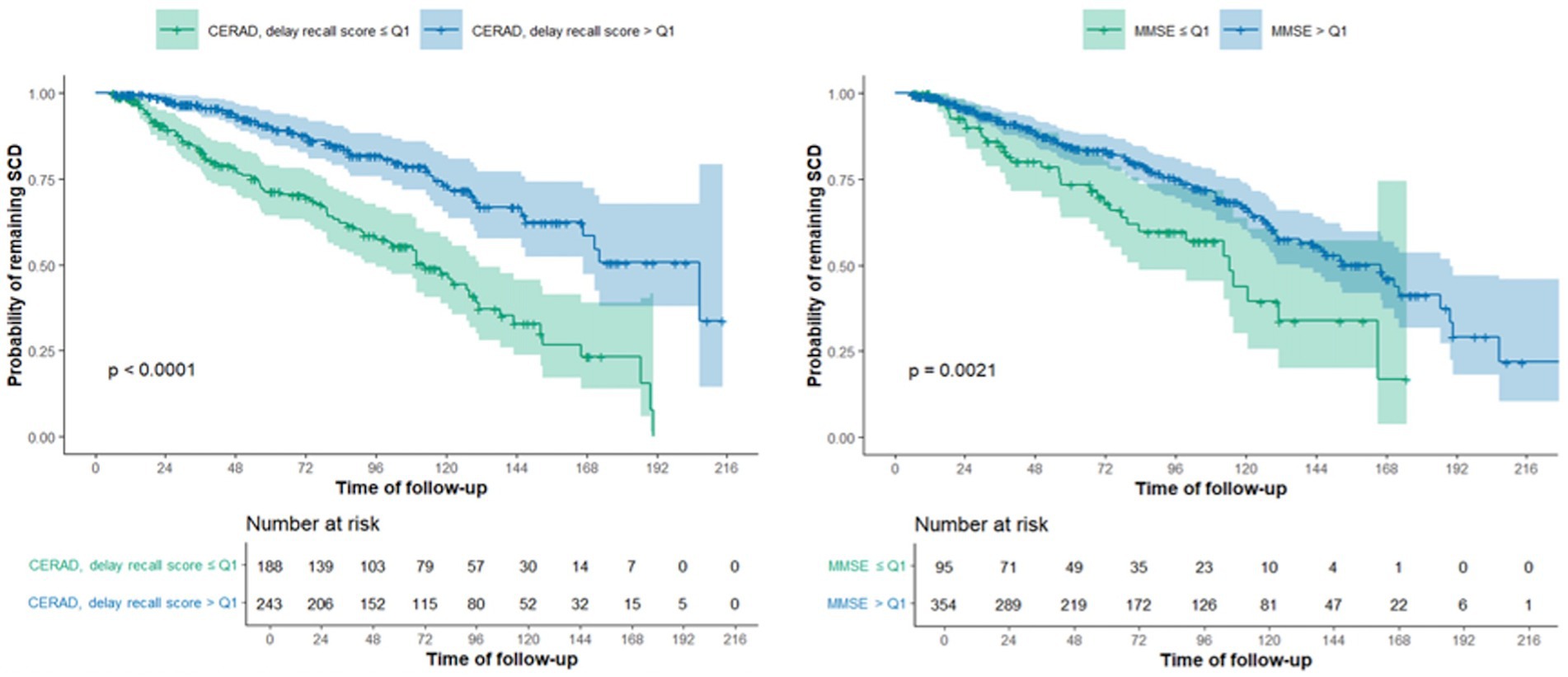
Figure 1. Kaplan–Meier curves for CERAD delayed scores and MMSE, considering the probability of remaining in SCD.
4 Discussion
In this study, we aimed to identify differences between SCDp and SCDnp, as well as variables associated with progression. At baseline, SCDp were older, had a higher prevalence of hypertension and hypercholesterolemia and had worst performance on tests regarding processing speed, verbal fluency, verbal memory, and executive functioning. Factors associated with progression at follow-up were global cognition (MMSE), executive function (TMT-B), and verbal memory test (CERAD regarding trial 1 of immediate recall, trial 2 of immediate recall, trial 3 of immediate recall and the delay recall score).
A limited number of longitudinal studies have explored the prognostic significance of neuropsychological assessments in individuals with SCD regarding their progression to MCI or dementia (Dufouil et al., 2005; Li et al., 2016; Bessi et al., 2018). Evidence suggests the superiority of memory tests, particularly those assessing delayed recall, in predicting the development of dementia in cognitively normal adults. Furthermore, tests measuring executive functions, verbal and visual memory, language, and global cognition are associated with the development of dementia (Vyhnalek et al., 2022).
According to the study carry-out by Miebach et al. (2019), memory and language were the most frequently affected domains in adults with SCD, with executive function impairment observed in less than 10% of cases. Wolfsgruber et al. (2020) supported our findings regarding neuropsychological variables related to SCD. They observed that individuals with SCD performed worse on tests of global cognition, memory, language, and executive functions. Similarly, Bäckman et al. (2005) found similar results in tests of episodic memory, executive functions, and verbal ability. However, they showed that individuals with SCD scored worse on tests of visual ability, attention, and processing speed. More recently, Jester et al. conducted a study that yielded results similar to those presented by Jester et al. (2022).
A cohort study that included both HCs and individuals with SCD found that lower scores on tests of episodic memory, naming, and semantic fluency were associated with an increased risk of progressing to MCI or AD dementia in SCD (Rowe et al., 2010). Hong et al. conducted a study with similar characteristics to determine the risk factors for SCD progression in memory clinics in South Korea (Hong et al., 2015). They performed neuropsychological assessments using the Seoul Neuropsychological Screening Battery. The most relevant risk factors for progression to MCI or AD dementia were poorer results on the MMSE and tests of verbal memory and delayed recall. Additionally, worse results on visual memory tests were associated with a risk of progression, although with less significance (Hong et al., 2015). In a prospective study by Bessi et al. (2018), the predictive role of neuropsychological assessment in the progression to AD dementia from SCD was investigated. The researchers used language and delayed recall test results to construct the Composite Memory Score. They found that lower scores on this test were a significant risk factor for progression to MCI or dementia (Bessi et al., 2018). Several other studies have also used the Composite Memory Score because it has been shown to be highly sensitive in determining the risk of progression from SCD to dementia due to AD (Crane et al., 2012). It is worth noting that this score is the sum of the results of tests of delayed recall and verbal ability.
Our results suggest that vascular risk factors such as hypertension and hypercholesterolemia, are more prevalent in the SCDp group. Both are widely recognized as a well-known risk factor for dementia and accelerates cognitive deterioration in AD through cerebrovascular damage (Ho et al., 2022; Livingston et al., 2024).
This study has limitations that need to be acknowledged. One of the most significant is its retrospective nature, as the data was not originally collected for the purpose of this research. However, this limitation is partially mitigated by the study’s substantial sample size of patients with SCD and the prolonged follow-up period, which allowed for meaningful analyses despite the retrospective design. Another limitation is the loss of subjects during follow-up and the variation in follow-up durations between groups, which could introduce bias or affect generalizability. Nevertheless, the extended tracking of patients over time enabled the correlation of clinical variables both at inclusion and during progression, enhancing the study’s relevance. Furthermore, all participants underwent a complete and standardized neuropsychological assessment, which strengthened the reliability of the cognitive profiles captured and supported the interpretation of the clinical trajectory despite the challenges noted. Finally, although Cox analyses allows for different follow up times, we must acknowledge that duration was longer in SCDp than SCDnp, providinga little more time to develop the outcome.
In future research, conducting a prospective study involving patients with SCD would be advisable, establishing their clinical and neuropsychological profiles during diagnosis and, subsequently, as they progress to MCI and eventually dementia due to AD. Moreover, as we did not include data regarding biomarkers and neuroimaging between progressors and no progressor, future work could also evaluate differences regarding biomarker positivity and structural changes in MRI, as well as functional changes, including frequency dependendent characteristics (Gong and Zuo, 2025).
5 Conclusion
Subjects at risk of progressing from SCD to MCI or dementia can be identified through neuropsychological assessments, as poorer performance in specific domains increases progression risk. These findings underscore the importance of considering nuances in neuropsychological evaluation, even if having a normal score, for detecting high-risk individuals aiming at earlier interventions.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Clinica UNIVERSIDAD DE NAVARRA. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
RV-R: Writing – original draft, Writing – review & editing. MR-R: Conceptualization, Writing – review & editing. GM-M: Methodology, Writing – original draft. JP: Formal analysis, Methodology, Writing – review & editing. SS-L: Data curation, Writing – review & editing. MR-O: Conceptualization, Investigation, Methodology, Supervision, Writing – review & editing. MB: Investigation, Methodology, Writing – original draft. AJ-H: Formal analysis, Methodology, Supervision, Validation, Writing – original draft. MR: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2025.1680762/full#supplementary-material
References
Albert, M. S., DeKosky, S. T., Dickson, D., Dubois, B., Feldman, H. H., Fox, N. C., et al. (2011). The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 7, 270–279. doi: 10.1016/j.jalz.2011.03.008
Bäckman, L., Jones, S., Berger, A. K., Laukka, E. J., and Small, B. J. (2005). Cognitive impairment in preclinical Alzheimer's disease: a meta-analysis. Neuropsychology 19, 520–531. doi: 10.1037/0894-4105.19.4.520
Bessi, V., Mazzeo, S., Padiglioni, S., Piccini, C., Nacmias, B., Sorbi, S., et al. (2018). From subjective cognitive decline to Alzheimer's disease: the predictive role of neuropsychological assessment, personality traits, and cognitive reserve. A 7-year follow-up study. J Alzheimer's Dis 63, 1523–1535. doi: 10.3233/JAD-171180
Casals-Coll, M., Sánchez-Benavides, G., Quintana, M., Manero, R. M., Rognoni, T., Calvo, L., et al. (2013). Estudios normativos españoles en población adulta joven (proyecto NEURONORMA jóvenes): normas para los test de fluencia verbal. Neurologia 28, 33–40. doi: 10.1016/j.nrl.2012.02.010
Crane, P. K., Carle, A., Gibbons, L. E., Insel, P., Mackin, R. S., Gross, A., et al. (2012). Development and assessment of a composite score for memory in the Alzheimer's disease neuroimaging initiative (ADNI). Brain Imaging Behav. 6, 502–516. doi: 10.1007/s11682-012-9186-z
Dufouil, C., Fuhrer, R., and Alpérovitch, A. (2005). Subjective cognitive complaints and cognitive decline: consequence or predictor? The epidemiology of vascular aging study. J. Am. Geriatr. Soc. 53, 616–621. doi: 10.1111/j.1532-5415.2005.53209.x
Gong, Z. Q., and Zuo, X. N. (2025). Dark brain energy: toward an integrative model of spontaneous slow oscillations. Phys Life Rev 52, 278–297. doi: 10.1016/j.plrev.2025.02.001
Ho, S., Hong, Y. J., Jeong, J. H., Park, K. H., Kim, S., Wang, M. J., et al. (2022). Study design and baseline results in a cohort study to identify predictors for the clinical progression to mild cognitive impairment or dementia from subjective cognitive decline (CoSCo) study. Dement. Neurocogn. Disord. 21, 147–161. doi: 10.12779/dnd.2022.21.4.147
Hong, Y. J., Yoon, B., Shim, Y. S., Kim, S. O., Kim, H. J., Choi, S. H., et al. (2015). Predictors of clinical progression of subjective memory impairment in elderly subjects: data from the clinical research centers for dementia of South Korea (CREDOS). Dement. Geriatr. Cogn. Disord. 40, 158–165. doi: 10.1159/000430807
Jack, C. R. Jr., Andrews, J. S., Beach, T. G., Buracchio, T., Dunn, B., Graf, A., et al. (2024). Revised criteria for diagnosis and staging of Alzheimer's disease: Alzheimer's Association workgroup. Alzheimers Dement. 20, 5143–5169. doi: 10.1002/alz.13859
Jessen, F., Amariglio, R. E., Buckley, R. F., van der Flier, W. M., Han, Y., Molinuevo, J. L., et al. (2020). The characterisation of subjective cognitive decline. Lancet Neurol. 19, 271–278. doi: 10.1016/S1474-4422(19)30368-0
Jessen, F., Amariglio, R. E., van Boxtel, M., Breteler, M., Ceccaldi, M., Chételat, G., et al. (2014). A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer's disease. Alzheimers Dement. 10, 844–852. doi: 10.1016/j.jalz.2014.01.001
Jester, D. J., Vyhnálek, M., Andel, R., Marková, H., Nikolai, T., Laczó, J., et al. (2022). Progression from subjective cognitive decline to mild cognitive impairment or dementia: the role of baseline cognitive performance. J Alzheimer's Dis 86, 1763–1774. doi: 10.3233/JAD-215291
Kleineidam, L., Wagner, M., Guski, J., Wolfsgruber, S., Miebach, L., Bickel, H., et al. (2023). Disentangling the relationship of subjective cognitive decline and depressive symptoms in the development of cognitive decline and dementia. Alzheimers Dement. 19, 2056–2068. doi: 10.1002/alz.12785
Li, J. Q., Tan, L., Wang, H. F., Tan, M. S., Xu, W., Zhao, Q. F., et al. (2016). Risk factors for predicting progression from mild cognitive impairment to Alzheimer's disease: a systematic review and meta-analysis of cohort studies. J. Neurol. Neurosurg. Psychiatry 87, 476–484. doi: 10.1136/jnnp-2014-310095
Liew, T. M. (2019). Depression, subjective cognitive decline, and the risk of neurocognitive disorders. Alzheimer's Res Ther 11:70. doi: 10.1186/s13195-019-0527-7
Livingston, G., Huntley, J., Liu, K. Y., Costafreda, S. G., Selbæk, G., Alladi, S., et al. (2024). Dementia prevention, intervention, and care: 2024 report of the lancet standing commission. Lancet 404, 572–628. doi: 10.1016/S0140-6736(24)01296-0
Lopez Miquel, J., and Agustí, G. (2011). Mini-Examen Cognoscitivo (MEC). Rev. Esp. Med. Legal 37, 122–127. doi: 10.1016/S0377-4732(11)70075-X
McKhann, G. M., Knopman, D. S., Chertkow, H., Hyman, B. T., Jack, C. R., Kawas, C. H., et al. (2011). The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 7, 263–269. doi: 10.1016/j.jalz.2011.03.005
Miebach, L., Wolfsgruber, S., Polcher, A., Peters, O., Menne, F., Luther, K., et al. (2019). Which features of subjective cognitive decline are related to amyloid pathology? Findings from the DELCODE study. Alzheimer's Res Ther 11:66. doi: 10.1186/s13195-019-0515-y
Molinuevo, J. L., Rabin, L. A., Amariglio, R., Buckley, R., Dubois, B., Ellis, K. A., et al. (2017). Implementation of subjective cognitive decline criteria in research studies. Alzheimers Dement. 13, 296–311. doi: 10.1016/j.jalz.2016.09.012
Peña-Casanova, J., Gramunt-Fombuena, N., Quiñones-Ubeda, S., Sánchez-Benavides, G., Aguilar, M., Badenes, D., et al. (2009). Spanish multicenter normative studies (NEURONORMA project): norms for the Rey-Osterrieth complex figure (copy and memory), and free and cued selective reminding test. Arch. Clin. Neuropsychol. 24, 371–393. doi: 10.1093/arclin/acp041
Peña-Casanova, J., Quiñones-Ubeda, S., Gramunt-Fombuena, N., Aguilar, M., Casas, L., Molinuevo, J. L., et al. (2009). Spanish multicenter normative studies (NEURONORMA project): norms for Boston naming test and token test. Arch. Clin. Neuropsychol. 24, 343–354. doi: 10.1093/arclin/acp039
Peña-Casanova, J., Quiñones-Ubeda, S., Quintana-Aparicio, M., Aguilar, M., Badenes, D., Molinuevo, J. L., et al. (2009). Spanish multicenter normative studies (NEURONORMA project): norms for verbal span, visuospatial span, letter and number sequencing, trail making test, and symbol digit modalities test. Arch. Clin. Neuropsychol. 24, 321–341. doi: 10.1093/arclin/acp038
Reisberg, B., Prichep, L., Mosconi, L., John, E. R., Glodzik-Sobanska, L., Boksay, I., et al. (2008). The pre-mild cognitive impairment, subjective cognitive impairment stage of Alzheimer's disease. Alzheimers Dement. 4, S98–s108. doi: 10.1016/j.jalz.2007.11.017
Rocca, W. A., Luepker, R. V., Shahar, E., Wolf, P. A., Hohol, M., and O’Connor, P. (2012). Regional north American annual meeting of the world Federation of Neurology- Research Group on Neuroepidemiology. Neuroepidemiology 38, 196–201. doi: 10.1016/j.ensci.2024.100544
Rowe, C. C., Ellis, K. A., Rimajova, M., Bourgeat, P., Pike, K. E., Jones, G., et al. (2010). Amyloid imaging results from the Australian imaging, biomarkers and lifestyle (AIBL) study of aging. Neurobiol. Aging 31, 1275–1283. doi: 10.1016/j.neurobiolaging.2010.04.007
Scheltens, P., Blennow, K., Breteler, M. M., de Strooper, B., Frisoni, G. B., Salloway, S., et al. (2016). Alzheimer's disease. Lancet 388, 505–517. doi: 10.1016/S0140-6736(15)01124-1
Vyhnalek, M., Jester, D. J., Andel, R., Horakova, H., Nikolai, T., Laczó, J., et al. (2022). Contribution of memory tests to early identification of conversion from amnestic mild cognitive impairment to dementia. J Alzheimer's Dis 88, 1397–1409. doi: 10.3233/JAD-215364
Keywords: subjective cognitive decline, Alzheimer’s disease, mild cognitive impairment, neuropsychological assessment, disease progression
Citation: Villino-Rodríguez R, Ríos-Rivera MM, Montoya-Murillo G, Patricio Baldera J, Salazar-Londoño S, Rodríguez-Oroz MC, Borda MG, Jiménez-Huete A and Riverol M (2025) Clinical and neuropsychological features associated with progression in subjective cognitive decline. Front. Aging Neurosci. 17:1680762. doi: 10.3389/fnagi.2025.1680762
Edited by:
Enzo Emanuele, 2E Science, ItalyReviewed by:
Xiu-Xia Xing, Beijing University of Technology, ChinaStephanie Cosentino, Columbia University, United States
Copyright © 2025 Villino-Rodríguez, Ríos-Rivera, Montoya-Murillo, Patricio Baldera, Salazar-Londoño, Rodríguez-Oroz, Borda, Jiménez-Huete and Riverol. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rafael Villino-Rodríguez, cnZpbGxpbm9AZ21haWwuZXM=