 Jordi Adamuz1,2,3
Jordi Adamuz1,2,3 Julia González-Vaca2,3*Maribel González-Samartino1,2,3María-Magdalena López-Jiménez1,2,3Andrea Urbina1,2,3Oliver Polushkina-Merchanskaya3
Julia González-Vaca2,3*Maribel González-Samartino1,2,3María-Magdalena López-Jiménez1,2,3Andrea Urbina1,2,3Oliver Polushkina-Merchanskaya3 Sergio Alonso-Fernández2,3
Sergio Alonso-Fernández2,3 Silvia Esteban-Sepúlveda2,3Sergio Barrientos-Trigo4Maria-Eulàlia Juvé-Udina3,5
Silvia Esteban-Sepúlveda2,3Sergio Barrientos-Trigo4Maria-Eulàlia Juvé-Udina3,5- 1Nursing Knowledge Management and Information Systems Department, Bellvitge University Hospital, L’Hospitalet de Llobregat, Barcelona, Spain
- 2Faculty of Nursing, University of Barcelona, L’Hospitalet de Llobregat, Barcelona, Spain
- 3Bellvitge Institute of Biomedical Research (IDIBELL), L’Hospitalet de Llobregat, Barcelona, Spain
- 4Nursing Department, University of Seville, Seville, Spain
- 5Nursing Management Team, Catalan Institute of Health, Barcelona, Spain
Background: Many elderly people required hospitalization during the pandemic period, but broader care complexity factors have not been studied in this population. This study aimed to identify the care complexity factors according to age in older people hospitalized with COVID-19.
Methods: A multicenter cross-sectional study was conducted from 1 March 2020 to 31 March 2022 at eight public hospitals in Spain. All older patients hospitalized with COVID-19 were classified in the following groups: young-old (65–74 years), middle-old (75–84 years), and oldest-old (≥85 years). The main variable was care complexity individual factors (CCIFs), which included 27 CCIFs classified in four domains: comorbidity/complications, psycho-emotional, mental-cognitive, and sociocultural. Multinomial logistic regressions were performed to identify the association of each CCIFs with age group.
Results: A total of 5,658 admissions were included. Of these, 46.3% were young-old (65–74 years), 34.8% middle-old (75–84 years) and 18.8% oldest-old (≥85 years). The analysis shows that middle-old (75–84 years) patients were associated with chronic disease, position impairment, urinary or fecal incontinence, anatomical and functional disorders, vascular fragility, involuntary movements, fear or anxiety and mental status impairments. Extreme weight, communication disorders, aggressive behavior, agitation and perception reality disorders were additional factors associated with the oldest-old (≥85 years) inpatients with COVID-19. The median number of CCIFs was higher in the oldest-old than in the other age groups (four in young-old [65–74 years]; six in middle-old [75–84 years]; seven in oldest-old [≥85 years] [OR:2.9; 95%CI:2.8–3.1; p < 0.001]).
Conclusion: The oldest groups of patients (≥75 years) admitted with COVID-19 had more CCIFs than the young-old group. CCIFs should be included in patient assessment in order to identify care needs in older hospitalized patients.
Highlights
Many older adults required hospitalization during the pandemic period, however CCIFs have not been studied in this population.
We found that the oldest groups of patients (≥75 years) admitted with COVID-19 had more CCIFs than the young-old group.
This study strengthens the argument for considering broader patient assessment to identify care complexity needs.
Introduction
The COVID-19 pandemic disproportionately affected individuals over 65 years old. According to data from Spain, more than 60% of COVID-19 patients hospitalized during the first months of the pandemic were aged over 65 years, and this demographic group accounted for approximately 85% of deaths from the disease (Instituto Nacional de Estadística. Instituto Nacional de Estadística INE, 2024).
Prior studies focusing on older people hospitalized with COVID-19 focused on identified risk factors and frailty indicators associated with unfavorable outcomes (Wiemers et al., 2024; Wei et al., 2020; Szklarzewska et al., 2023; Alsahab et al., 2021; Smits et al., 2022) however, broader care complexity factors have not been studied in this population. Understanding care complexity individual factors (CCIFs) is crucial for developing more effective and personalized management strategies for older adults with COVID-19. CCIFs are a set of patient characteristics related to different health dimensions that may complicate care delivery and contribute to adverse events (Juvé-Udina et al., 2010). Previous studies have shown the association of CCIFs with unfavorable outcomes in hospitalized patients in general and in those admitted for COVID-19 (Jiménez-Martínez et al., 2024; Adamuz et al., 2018; Adamuz et al., 2021). Therefore, prior identification of CCIFs could help to identify patients with a higher risk of complications (Adamuz et al., 2020). The use of assessment tools considering these factors could improve care planning accuracy and optimize resource allocation. This approach could inform public health policies aimed at strengthening the health system’s capacity to respond to future health emergencies and the needs of the aging population (De Foo et al., 2023). However, few studies have provided data about CCIFs in the vulnerable elderly population hospitalized with COVID-19.
The aim of this study was to identify CCIFs according to the age of older adults hospitalized with COVID-19.
Methods
Study population
A multicenter cross-sectional study was conducted from 1 March 2020 to 31 March 2022 at eight public health hospitals in Spain: three high-tech hospital (tertiary metropolitan facilities), three urban university centers and two community hospitals. All patients with a medical diagnosis of COVID-19 infection admitted to a ward or step-down unit from 1 March 2020 to 31 March 2022 with a completed hospital minimum data set report were included. Patients directly admitted and discharged from intensive care units (ICU) were excluded.
This study was evaluated and approved by the institutional review board. Ethical and data protection protocols related to anonymity and data confidentiality (access to records, data encryption and archiving of information) were complied with throughout the study.
Data source
All data were collected from the electronic health record system, the hospital minimum data set and the clinical data warehouse. A unique identification number was used to link the data sets from these sources.
Variables
Consistent with the literature, older adults were categorized as young-old (65–74 years), middle-old (75–84 years), and oldest-old (≥85 years) (Neugarten, 1974; Johfre and Saperstein, 2023). The main variable was care complexity individual factors (CCIFs) (Juvé-Udina et al., 2010). CCIFs are a group of patient characteristics related to different health dimensions that may complicate care delivery and contribute to adverse outcomes. They are classified into four domains: (i) comorbidity/complications, (ii) psycho-emotional, (iii) mental-cognitive sociocultural, and iv) sociocultural. Patients were considered to have CCIFs if they presented at least one related defined characteristic according to previous inquiries. CCIFs were collected from the nursing assessment e-charts as structured data based on the Architecture, Terminology, Interface, Knowledge (ATIC) terminology (Juvé-Udina and Adamuz, 2023; Juvé-Udina, 2013). In this study we included the following CCIFs. The comorbidity/complications domain contained: (i) major chronic disease, (ii) hemodynamic instability (intensive control of vital signs or state of shock), (iii) high risk of haemorrhage (coagulation disorders, thrombocytopenia, anticoagulant therapy), (iv) communication disorders (aphasia, dysphasia, dysarthria, laryngectomy, tracheostomy), (v) urinary or faecal incontinence, (vi) vascular fragility (capillary fragility, tortuous veins), (vii) position impairment, (viii) involuntary movements (continuous involuntary movements), (ix) extreme weight (low weight, obesity), (x) dehydration (skin turgor), (xi) oedema, (xii) uncontrolled pain (verbal numerical rating scale above three points), (xiii) transmissible infections (isolation measures), (xiv) immunosuppression and (xv) anatomical and functional disorders (amputation, deformities, joint stiffness). The psycho-emotional domain comprised: (i) aggressive behaviour, (ii) fear/anxiety and (iii) impaired adaptation (disruptive behaviour, hopelessness or surrender). The mental-cognitive domain included: (i) agitation, (ii) mental status impairments (confusion, disorientation, stupor, transient loss of consciousness), (iii) impaired cognitive functions (intellectual disability, amnesia) and (iv) perception of reality disorders (delirium, hallucinations, disconnection from reality). Finally, the sociocultural domain included: (i) language barriers, (ii) social exclusion (extreme poverty), (iii) belief conflict (spiritual distress), and (iv) lack of caregiver support.
We also collected information regarding the demographic and clinical characteristics of the patients, sex, underlying disease, continuity of care (discharged to another facility), length of hospital stay, and admission to ICU during hospitalization. Facilities were classified into two categories: high-tech hospitals or other. High-tech hospitals were defined as referral university centres that provide tertiary care for either open-heart surgery or major organ transplants.
Statistical analysis
Descriptive analysis of data was performed to describe the patients’ demographic and clinical characteristics. For categorical variables, a comparative analysis for detecting significant differences between each age group was carried out using the Fisher’s exact test. For continuous variables the Mann-Whitney U test was used. Univariate multinomial logistic regressions of each CCIFs were performed to detect which ones were potentially associated with the different age groups (Table 2). The young-old (65–74) group was used as the reference category. The findings obtained were corroborated after adjusting for potential confounders: sex and hospital type (high-tech hospital) (Supplementary Material). The median-based CCIF categories shown in Table 2 were included solely for descriptive purposes and were not used in any regression models. The results of the logistic-regressions analyses were reported as odds ratios (OR) and 95% confidence intervals (CI). P values less than 0.05 were considered statistically significant. All reported p values are two-tailed. Statistical analysis was performed using the SPSS software package version 25.0 (SPSS, Chicago, IL).
Results
A total of 5,658 older adult admissions were included. Of these, 46.3% (n = 2,622) were young-old (65–74 years), 34.8% (n = 1,971) middle-old (75–84 years) and 18.8% (n = 1,065) oldest-old (≥85 years) inpatients with COVID-19.
The baseline characteristics among patients hospitalized with COVID-19 according to the age category of older adults are presented in Table 1. Female sex and being discharged to another facility were more common in the oldest-old (≥85 years) than the other groups. Almost 91% of patients in the oldest-old group (≥85 years) presented underlying disease, mainly arterial hypertension or chronic heart failure (56.4%), diabetes or chronic kidney disease (47.9%) and chronic respiratory disease (19.2%) (p < 0.05). Conversely, length of stay (8 vs 9 days), admission to step-down unit (3.1% vs 12.6%) and transfer to ICU (6.3% vs 34.6%) were less common in the oldest-old (≥85 years) than in the young-old group (65–74 years) (p < 0.001).
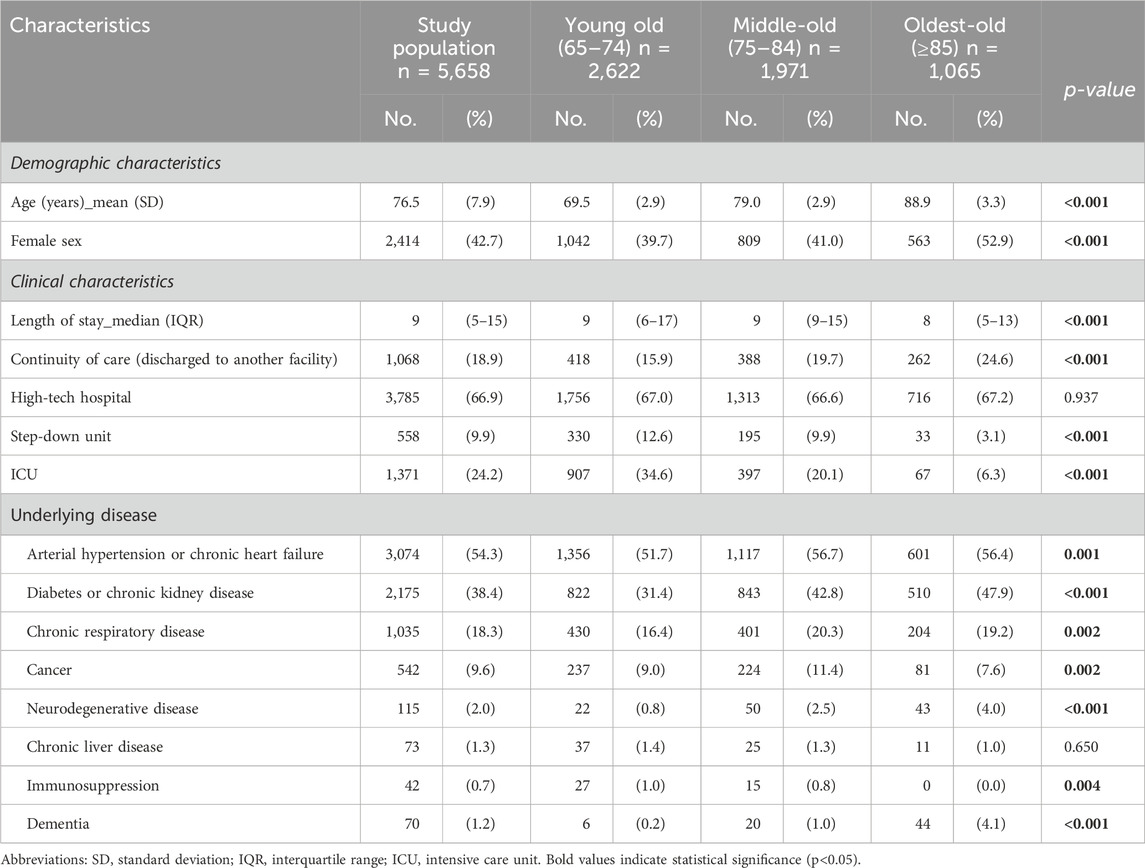
Table 1. Baseline characteristics among patients hospitalized with COVID-19 according to the age category of older adults.
Regarding CCIFs, we observed that lack of caregiver support, hemodynamic instability, chronic disease, transmissible infection, mental status impairments, and fear or anxiety were the most common CCIFs presented. The multinomial analysis showed that middle-old (75–84 years) patients were associated with chronic disease, position impairment, urinary or fecal incontinence, anatomical and functional disorders, vascular fragility, involuntary movements, fear or anxiety and mental status impairments. Extreme weight, communication disorders, aggressive behavior, agitation and perception reality disorders were additional factors associated with the oldest-old (≥85 years) inpatients with COVID-19. The median number of CCIFs was higher in the oldest-old than in the other age groups (four in young-old [65–74 years]; six in middle-old [75–84 years]; seven in oldest-old [≥85 years] [OR:2.9; 95%CI:2.8–3.1; p < 0.001]) (Table 2). Similar results we obtained after adjusting for potential confounders (Supplementary Material).
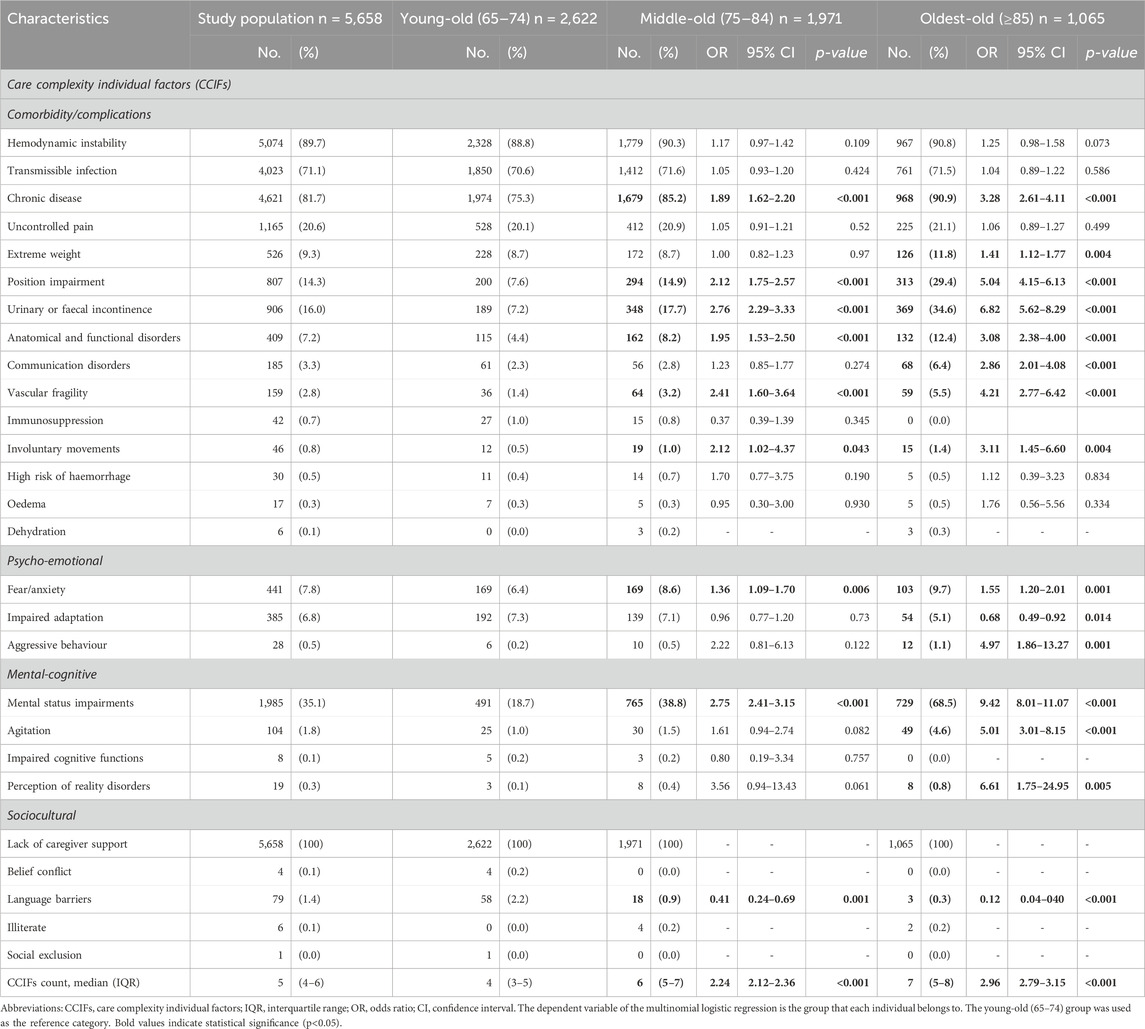
Table 2. Association of CCIFs among patients hospitalized with COVID-19 according to the age category of older adults.
Discussion
This study shows that the oldest groups of patients (≥75 years) admitted with COVID-19 had more CCIFs than the young-old group (65–74 years). Moreover, several CCIFs related to comorbidity/complications, psycho-emotional, mental-cognitive, and sociocultural domains were associated with the older patient groups.
The proportions of the subgroups of older adults described in this study are very similar to those found in the overall Spanish population (Instituto Nacional de Estadística. Instituto Nacional de Estadística INE, 2024). Furthermore, the number of CCIFs was higher in the study population compared with previous studies of admitted COVID-patients, being highest among the oldest-old patients (Seven CCIFs in patients ≥85 years old vs Four CCIFs in patients ≥18 years old) (Adamuz et al., 2021). Chronic disease, position impairment, urinary or fecal incontinence, anatomical and functional disorders, involuntary movements, vascular fragility, extreme weight, communication disorders, fear or anxiety, aggressive behavior, mental status impairments, agitation and perception reality disorders were the CCIFs associated with the middle (75–84 years), and oldest-old groups (≥85 years). As described in other studies, older and very old hospitalized individuals exhibit a higher prevalence of comorbidities and physical deterioration (Szklarzewska et al., 2023; Casas-Rojo et al., 2020) such as incontinence or position impairments. Moreover, the presence of cognitive impairment or dementia has been associated with an increase in care management complexity, due to difficulties in communication and adapting to the hospital environment (Veronese et al., 2022; Covino et al., 2020; Tondo et al., 2021). Additionally, social isolation and emotional stress, which were exacerbated during the pandemic, negatively affected the wellbeing of older patients, potentially complicating the recovery process and increasing the demand for psychosocial support (McNabney et al., 2022; Hwang et al., 2020). Finally, ICUs were often overwhelmed, and prioritization decisions for admission to these units generated ethical controversies (Hostiuc et al., 2021). In our study, the oldest-old group (≥85 years) was the least admitted to the ICU. Mortality, readmission and post-discharge functional status were not collected in this study, but we considered that this should be one of the future lines of research.
This research included a large sample size hospitalized with COVID-19 with the aim of identifying CCIFs associated with older adults. Notwithstanding, this study excluded patients directly admitted to and discharged from the ICU because CCIFs were not included in their electronic health records, and we relied on compliance in completing the healthcare history. The CCIFs included in this study, like other tools such as the Comprehensive Geriatric Assessment (CGA), provide a holistic patient assessment that involves biological, functional, psycho-affective, and social domains (Veronese et al., 2022). The CCIFs and CGA provide tools that allow healthcare staff to identify patients with a high risk of complications, and therefore prior identification of complexity factors can help to implement strategies to improve health outcomes and quality of life for older adults (Zurlo and Zuliani, 2018). The broader health assessment should be implemented in care models (McNabney et al., 2022) in order to help quantify the care burden and to estimate safe staffing for older patients. This would help establish age-friendly health systems and encourage geroscience (Inouye, 2021). Future studies should evaluate the incremental value of CCIFs relative to established tools—such as frailty indices and the CGA—since our analysis did not compare their respective discriminative performance; moreover, because CCIFs can be automatically extracted from routine nursing electronic health records, whereas frailty scales and CGA usually require times-consuming bedside assessments, they could therefore facilitate wider use and implementation compared with other tools.
Limitation
It is important to point out certain limitations of this research:
- Data quality is supported by standard nursing documentation protocols; nevertheless, certain elements—particularly sociocultural factors—may have under-recorded, and no specific data-quality audits were conducted for this study, which we acknowledge as a limitation. Missingness for the four sociocultural CCIFs ranged from 0.1% to 3%, indicating possible under-recording, consistent with findings from previous studies in non-COVID populations (Adamuz et al., 2020).
- This analysis did not adjust for other potential confounders—including vaccination status, pandemic wave, baseline disease severity, and received treatments—which may have influenced the observed associations.
- Future longitudinal research should capture post-discharge functional end-points—such as objective mobility or activities-of-daily-living measures—to determine whether a high CCIF burden, particularly in patients with chronic conditions like arterial hypertension or ischemic heart disease, translates into poorer functional recovery after COVID-19 hospitalization (Borchev et al., 2024).
Conclusion
The oldest groups of patients (≥75 years) admitted with COVID-19 had more CCIFs than the young-old group. Moreover, several CCIFs related to comorbidity/complications, psycho-emotional, mental-cognitive, and sociocultural domains were associated with the older patient groups. CCIFs should be included in patient assessment in order to identify care complexity individual needs in older hospitalized patients.
Data availability statement
The datasets presented in this article are not readily available because Datasets are property of the Catalan Institute of Health; therefore, any data sharing will require that institution’s prior approval. Data may be available from the corresponding author upon reasonable request and with permission from the Catalan Institute of Health. Requests to access the datasets should be directed toamFkYW11ekBiZWxsdml0Z2Vob3NwaXRhbC5jYXQ=.
Ethics statement
The studies involving humans were approved by this study was approved by the Clinical Research Ethics Committee of Bellvitge University Hospital (reference 293/20). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because Informed consent was waived due to the study’s retrospective design. Ethical and data protection protocols related to anonymity and data confidentiality (access to records, data encryption and archiving of information) were complied with throughout the study. The manuscript presents research on animals that do not require ethical approval for their study.
Author contributions
JA: Conceptualization, Formal Analysis, Funding acquisition, Investigation, Methodology, Resources, Validation, Writing – original draft. JG-V: Conceptualization, Formal Analysis, Methodology, Writing – original draft. MG-S: Data curation, Formal Analysis, Writing – original draft. M-ML-J: Data curation, Writing – original draft. AU: Data curation, Writing – review and editing. OP-M: Formal Analysis, Software, Writing – original draft. SA-F: Data curation, Resources, Writing – original draft. SE-S: Writing – review and editing. SB-T: Conceptualization, Data curation, Writing – review and editing. M-EJ-U: Conceptualization, Project administration, Supervision, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Colegio Oficial de Enfermeras y Enfermeros de Barcelona (grant PR-542/2022 and PR494/2021), and the Spain’s Ministerio de Ciencia e Innovación, Instituto de Salud Carlos III, co-financed by the European Regional Development Fund ‘FEDER' (grant PI21/01267), and by the Departament de Recerca i Universitats de la Generalitat de Catalunya and AGAUR (grant 2021 SGR 00929).
Acknowledgments
We thank the CERCA Programme/Generalitat de Catalunya for institutional support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fragi.2025.1524849/full#supplementary-material
References
Adamuz, J., González-Samartino, M., Jiménez-Martínez, E., Tapia-Pérez, M., López-Jiménez, M., Ruiz-Martínez, M., et al. (2018). Care complexity individual factors associated with hospital readmission: a retrospective cohort study. J. Nurs. Scholarsh. 50, 411–421. doi:10.1111/jnu.12393
Adamuz, J., González-Samartino, M., Jiménez-Martínez, E., Tapia-Pérez, M., López-Jiménez, M. M., Rodríguez-Fernández, H., et al. (2021). Risk of acute deterioration and care complexity individual factors associated with health outcomes in hospitalised patients with COVID-19: a multicentre cohort study. BMJ Open 11, e041726. doi:10.1136/bmjopen-2020-041726
Adamuz, J., Juve-Udina, M. E., Gonzalez-Samartino, M., Jiménez-Martínez, E., Tapia-Pérez, M., López-Jiménez, M. M., et al. (2020). Care complexity individual factors associated with adverse events and in-hospital mortality. PLoS One 15, e0236370. doi:10.1371/journal.pone.0236370
Alsahab, M., Beishon, L., and Brown, B. (2021). Age and frailty are independently associated with increased COVID-19 mortality and increased care needs in survivors: results of an international multi-centre study. Age Ageing 50, 617–630. doi:10.1093/ageing/afab026
Borchev, K., Shirshova, E., Solodovnik, A., and Bondarev, D. (2024). Functional recovery in older inpatients with hypertension and ischemic heart disease post-COVID-19. Adv. Gerontol. 37, 122–129. doi:10.34922/AE.2024.37.1-2.016
Casas-Rojo, J. M., Antón-Santos, J. M., and Millán-Núñez-Cortés, J. (2020). Características clínicas de los pacientes hospitalizados con COVID-19 en España: resultados del Registro SEMI-COVID-19. Rev. Clin. Esp. 220, 480–494. doi:10.1016/j.rce.2020.07.003
Covino, M., De Matteis, G., Santoro, M., Sabia, L., Simeoni, B., Candelli, M., et al. (2020). Clinical characteristics and prognostic factors in COVID-19 patients aged ≥80 years. Geriatr. Gerontol. Int. 20, 704–708. doi:10.1111/ggi.13960
De Foo, C., Verma, M., Tan, S. Y., Hamer, J., van der Mark, N., Pholpark, A., et al. (2023). Health financing policies during the COVID-19 pandemic and implications for universal health care: a case study of 15 countries. Lancet Glob. Health 11, e1964–e1977. doi:10.1016/S2214-109X(23)00448-5
Hostiuc, S., Negoi, I., Maria-Isailă, O., Diaconescu, I., Hostiuc, M., and Drima, E. (2021). Age in the time of COVID-19: an ethical analysis. Aging Dis. 12, 7–13. doi:10.14336/AD.2020.0929
Hwang, T.-J., Rabheru, K., Peisah, C., Reichman, W., and Ikeda, M. (2020). Loneliness and social isolation during the COVID-19 pandemic. Int. Psychogeriatr. 32, 1217–1220. doi:10.1017/S1041610220000988
Inouye, S. K. (2021). Creating an anti-ageist healthcare system to improve care for our current and future selves. Nat. Aging 1, 150–152. doi:10.1038/s43587-020-00004-4
Instituto Nacional de Estadística. Instituto Nacional de Estadística (INE) (2024). Demography and population. Available online at: www.ine.es.
Jiménez-Martínez, E., Adamuz, J., González-Samartino, M., Muñoz-Carmona, M. A., Hornero, A., Martos-Martínez, M. P., et al. (2024). Peripheral intravenous catheter failure, nurse staffing levels and care complexity individual factors: a retrospective multicentre cohort study. PLoS One 19, e0303152. doi:10.1371/journal.pone.0303152
Johfre, S., and Saperstein, A. (2023). The social construction of age: concepts and measurement. Annu. Rev. Sociol. 49, 339–358. doi:10.1146/annurev-soc-031021-121020
Juvé-Udina, M. E. (2013). What patients’ problems do nurses e-chart? Longitudinal study to evaluate the usability of an interface terminology. Int. J. Nurs. Stud. 50, 1698–1710. doi:10.1016/j.ijnurstu.2013.04.008
Juvé-Udina, M.-E., and Adamuz, J. (2023). “Nursing Knowledge tools and strategies to improve patient outcomes and the work environment,” in Mentoring in nursing through narrative stories across the world (Springer International Publishing), 211–222.
Juvé-Udina, M. E., Matud, C., Farrero, S., Jiménez, H., Rodríguez, E., and Martínez, M. (2010). Intensity of nursing care: workloads or individual complexity? Metas Enfermería 13, 6–14. Available online at: https://diposit.ub.edu/dspace/bitstream/2445/33804/1/606874.pdf.
McNabney, M. K., Green, A. R., Burke, M., Le, S. T., Butler, D., Chun, A. K., et al. (2022). Complexities of care: common components of models of care in geriatrics. J. Am. Geriatr. Soc. 70, 1960–1972. doi:10.1111/jgs.17811
Neugarten, B. L. (1974). Age groups in American society and the rise of the young-old. Ann. Am. Acad. Pol. Soc. Sci. 415, 187–198. doi:10.1177/000271627441500114
Smits, R. A. L., Trompet, S., van der Linden, C. M. J., van der Bol, J. M., Jansen, S. W. M., Polinder-Bos, H. A., et al. (2022). Characteristics and outcomes of older patients hospitalised for COVID-19 in the first and second wave of the pandemic in The Netherlands: the COVID-OLD study. Age Ageing 51, afac048. doi:10.1093/ageing/afac048
Szklarzewska, S., Vande Walle, J., De Breucker, S., and Schoevaerdts, D. (2023). A comparison of clinical characteristics between old and oldest-old patients hospitalised for SARS-COV2. Acta Clin. Belg 78, 192–199. doi:10.1080/17843286.2022.2102115
Tondo, G., Sarasso, B., Serra, P., Tesser, F., and Comi, C. (2021). The impact of the COVID-19 pandemic on the cognition of people with dementia. Int. J. Environ. Res. Public Health 18, 4285. doi:10.3390/ijerph18084285
Veronese, N., Custodero, C., Demurtas, J., Smith, L., Barbagallo, M., Maggi, S., et al. (2022). Comprehensive geriatric assessment in older people: an umbrella review of health outcomes. Age Ageing 51, afac104. doi:10.1093/ageing/afac104
Wei, C., Liu, Y., Liu, Y., Zhang, K., Su, D., Zhong, M., et al. (2020). Clinical characteristics and manifestations in older patients with COVID-19. BMC Geriatr. 20, 395. doi:10.1186/s12877-020-01811-5
Wiemers, E. E., Lin, I.-F., Wiersma Strauss, A., Chin, J., Hotz, V. J., and Seltzer, J. A. (2024). Age differences in experiences of pandemic-related health and economic challenges among adults aged 55 and older. Gerontologist 64, gnae023. doi:10.1093/geront/gnae023
Keywords: care complexity, patient assessment, older adults, hospitalization, COVID-19
Citation: Adamuz J, González-Vaca J, González-Samartino M, López-Jiménez M-M, Urbina A, Polushkina-Merchanskaya O, Alonso-Fernández S, Esteban-Sepúlveda S, Barrientos-Trigo S and Juvé-Udina M-E (2025) Association between care complexity individual factors and older inpatients with COVID-19: a cross-sectional study. Front. Aging 6:1524849. doi: 10.3389/fragi.2025.1524849
Received: 08 November 2024; Accepted: 23 July 2025;
Published: 05 August 2025.
Edited by:
Emiliana Giacomello, University of Trieste, ItalyReviewed by:
Dmitriy Bondarev, University of Jyväskylä, FinlandEliete Maria Silva, State University of Campinas, Brazil
Copyright © 2025 Adamuz, González-Vaca, González-Samartino, López-Jiménez, Urbina, Polushkina-Merchanskaya, Alonso-Fernández, Esteban-Sepúlveda, Barrientos-Trigo and Juvé-Udina. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julia González-Vaca, anVsaWFnb256YWxlenZhY2FAdWIuZWR1