 Baojian Hu
Baojian Hu Qingxia Liang2
Qingxia Liang2 Huiyi Jiang
Huiyi Jiang- 1Department of Pediatrics, Children's Medical Center, The First Hospital of Jilin University, Lequn Branch, Changchun City, Jilin Province, China
- 2Enping People's Hospital, Enping City, Guangdong Province, China
Objective: To investigate the effects of exercise doses recommended by the American College of Sports Medicine (ACSM) on motor skills, social interaction, behavioral patterns, and verbal and non-verbal communication domains in children with autism.
Methods: A systematic search was conducted across PubMed, Embase, Web of Science, and the Cochrane Library, focusing on the effects of physical activity on children with autism. Randomized controlled trials comparing exercise interventions with no intervention were included, and changes in motor skills, social interaction, behavioral patterns,and communication domains were assessed using standardized mean differences (SMD), 95% confidence intervals (CI), and p-values (p < 0.05).Interventions were categorized based on high or low adherence to exercise prescriptions developed or recommended by ACSM.Studies in which ≥70% of components met ACSM criteria were classified as having high adherence, while those with <70% were classified as having low adherence, based on thresholds established in previous literature. A fixed-effects or random-effects model was applied for meta-analysis, and subgroup comparisons were conducted.
Results: A total of 27 studies (29 exercise interventions) involving 1,012 participants were included. In the motor skills domain,the pooled standardized mean difference (SMD) was 1.35, 95% confidence interval (CI) [0.66,2.03]. Subgroup analysis revealed that the high-adherence group showed an SMD of 1.44, 95% CI [0.51,2.36], while the low-adherence group showed an SMD of 1.26, 95% CI [0.15,2.36]. For the social interaction domain,the overall SMD was −0.22, 95% CI [−0.54,0.99]. The high-adherence subgroup had an SMD of −0.41, 95% CI [−0.62,−0.21], whereas the low-adherence group had an SMD of 0.42, 95% CI [−0.50,1.33]. In the behavioral patterns domain, the overall SMD was −0.79, 95% CI [−1.26,−0.32]. Subgroup analysis indicated an SMD of −0.42, 95% CI [−0.73,−0.11] for the high-adherence group and −2.79, 95% CI [−5.63,0.06] for the low-adherence group.For the verbal and non-verbal communication domain, the overall SMD was 0.33, 95% CI [−0.31,0.97]. Subgroup SMD were 0.21,95% CI [−0.14,0.57] for the high-adherence group and 0.59, 95% CI [−1.67,2.84] for the low-adherence group.
Conclusion: Exercise interventions had a significant positive impact on motor skills and behavioral patterns in children with autism spectrum disorder (ASD). Interventions with high adherence to ACSM-recommended exercise dosages were more effective in improving motor skills, social interaction,and behavioral patterns compared to low-adherence dosages.Future evidence-based exercise prescriptions may be established for children with ASD, optimizing motor-functional outcomes.
Systematic Review Registration: PROSPERO, identifier (CRD42024565241).
1 Introduction
ASD is a common neurodevelopmental disorder characterized by language and behavioral difficulties, including impaired social interaction,repetitive behaviors,communication deficits,and restricted interests and activities that manifest in early childhood and persist into adulthood.According to the U.S. Centers for Disease Control and Prevention (CDC) report released in 2025, the prevalence of autism among 8-year-old children reached 3.2% (equivalent to 1 in 31 children). This represents a significant increase compared to the rate of 1 in 150 children reported in 2000 (1). In China,more than 10 million individuals may be affected by autism, with over 2 million children aged 0 to 14.Males are four times more likely to be diagnosed with ASD than females.
In recent years, exercise interventions have gained increasing attention as a strategy to alleviate symptoms of autism,as physical activity is beneficial to physical, psychological,and emotional health—especially in children.Several studies have demonstrated that exercise interventions can improve motor skills,s ocial interaction,behavioral patterns, and both verbal and non-verbal communication in children and adolescents with autism. For instance, Roza et al. (2) reported that Tai Chi exercises reduced stereotypical behaviors in children with autism. However, systematic research in this area remains limited and is often based on small sample sizes, with limited investigation into population-level and individualized exercise dosage. For example, Felzer-Kim et al. (3) randomized trial revealed that a 10-week FMS intervention (4 weekly sessions ×15 min) did not significantly enhance motor proficiency in children with ASD compared to controls.
This review applied clearly defined exercise standards based on the guidelines of the American College of Sports Medicine (ACSM), which offer detailed recommendations for cardiorespiratory, resistance, and flexibility training in healthy children. However, it remains unclear whether interventions adhering closely to ACSM recommendations yield greater benefits for individuals with ASD than those with lower adherence. The objective of this systematic review is to compare the effects of high versus low adherence to ACSM-recommended exercise prescriptions on outcomes in individuals with ASD.
2 Methods
2.1 Literature search strategy
2.1.1 Primary sources of literature
A comprehensive search was conducted in PubMed, Embase, Web of Science, and the Cochrane Library. The search covered all records from the inception of each database to February 1, 2025. In addition, manual searches were performed on relevant reviews and the reference lists of the included studies.
2.1.2 Search terms and strategy
The search terms included the following Medical Subject Headings (MeSH) and keywords, used across PubMed, Embase, Web of Science, and the Cochrane Library: (“Pervasive Developmental Disorders”, “autism”, “ASD/Autism Spectrum Disorder”, “Asperger”, or“PDD-NOS”) and (“Exercise”or“Exercises” or “Sports” or “Physical Activity” or “Motor Activity” or “Training” or “endurance training” or“TaiChi”or“yoga”or “Balance”or“Resistance”or “Flexibility” or“Cardiovascular”or “Aerobic”).
The complete search strategy is presented in the Supplementary Material Data Sheet 1.
2.2 Inclusion criteria
Studies were included if they met the following criteria:
(a) Participants were children diagnosed with ASD;
(b) The intervention involved any form of exercise program, including resistance training, aerobic activity, or flexibility exercises;
(c) The behavioral outcomes of the intervention were quantitatively measured and could be expressed as percentage changes reflecting relative behavioral improvements.
2.3 Exclusion criteria
Studies were excluded if they met any of the following criteria:
(a) Reports, conference proceedings, narrative reviews, or editorials;
(b) Studies that did not include a comparison between exercise and non-exercise groups;
(c) Studies involving participants with disorders related to, but distinct from ASD;
(d) Studies in which participants concurrently received specific pharmacological treatments during the exercise intervention period;
(e) Duplicate data from multiple publications based on the same study;
(f) Studies in which the control intervention involved any form of treatment unrelated to exercise.
2.4 Study selection
All retrieved references were imported into EndNote 20, and duplicates were removed. Two reviewers independently screened the titles and abstracts to exclude irrelevant studies. Full texts of potentially relevant studies were retrieved and assessed for eligibility based on the inclusion and exclusion criteria. If either reviewer deemed a study potentially eligible, the full text was reviewed. Disagreements between reviewers regarding eligibility were resolved through discussion or adjudication by a third reviewer. There were no restrictions on participants' sex, body mass index (BMI), publication date, or language.
2.5 Data extraction
Data extraction was independently performed by two reviewers. Motor skills, social interaction, behavioral patterns, and both verbal and non-verbal communication were considered primary outcomes. A pre-designed Excel spreadsheet was used to extract relevant data, including publication characteristics (author names, country, year of publication), methodological characteristics (number of groups, group design, intervention measures, sample size), participant characteristics (age, sex ratio), exercise characteristics (intervention frequency, exercise intensity, duration, number of repetitions, and sets), and outcome characteristics.
When post-intervention outcome data were not explicitly reported in the text but presented in graphical form, data were extracted using Engauge Digitizer software. For studies with multiple follow-up assessments, only data obtained immediately after the intervention were extracted.
Following data extraction, exercise interventions were evaluated in terms of dosage and adherence. The dosage of each intervention was assessed based on the American College of Sports Medicine (ACSM) guidelines for the development and maintenance of cardiorespiratory, muscular, skeletal, and neuromotor functions in healthy children (see Table 1). Two reviewers independently assessed the adherence of each intervention to ACSM recommendations, considering dimensions such as frequency, intensity, and duration. Adherence levels were categorized based on predefined criteria.
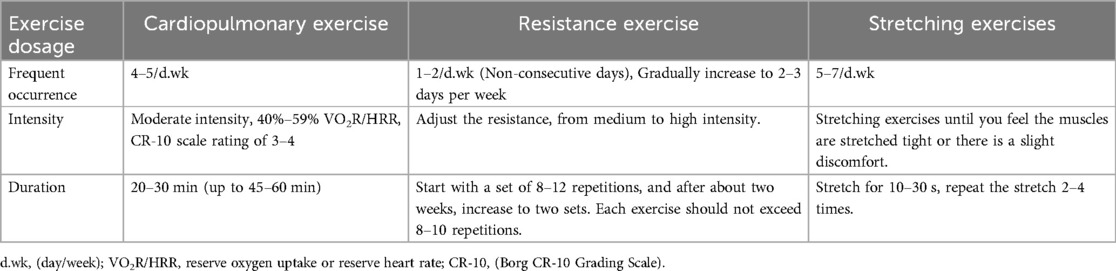
Table 1. ACSM recommendations for cardiopulmonary exercise, resistance exercise, and stretching exercise in healthy children.
Each exercise component was scored on a scale from 0 to 2. A score of 2 indicated full compliance with ACSM standards, 1 indicated uncertainty, and 0 indicated non-compliance. Discrepancies between the two reviewers were resolved through discussion with a third reviewer until consensus was reached. Based on this scoring system, the proportion of components meeting ACSM-recommended exercise dosage was calculated for each study. Studies in which ≥70% of components met ACSM criteria were classified as having high adherence, while those with <70% were classified as having low adherence, based on thresholds established in previous literature.
Results with 95% confidence intervals (CIs) that do not include zero were considered statistically more reliable. Larger absolute values of the standardized mean difference (SMD) indicate greater between-group differences and may suggest greater clinical or practical significance. However, multiple factors must be carefully considered when interpreting these results to ensure the accuracy and reliability of the conclusions.
2.6 Statistical analysis
Meta-analyses were conducted using Review Manager (RevMan) version 5.4.1 to compare the outcomes across included studies. Studies were categorized into two subgroups representing high and low adherence to ACSM guidelines. Heterogeneity within each subgroup was assessed using Higgins' I2 statistic and interpreted based on the recommendations of the Cochrane Handbook. Heterogeneity was classified as low (I2 ≤ 40%), moderate (30% < I2 ≤ 60%), substantial (50% < I2 ≤ 90%), or considerable (I2 > 75%).
A fixed-effects model was applied when I2 ≤ 50%; otherwise, a random-effects model was used. Effect sizes were reported as standardized mean differences (SMD), where larger absolute SMD values indicate more pronounced effects, accompanied by 95% confidence intervals (CIs). When substantial heterogeneity was detected, meta-regression was performed to explore potential sources of variation. Publication bias was assessed using Begg's rank correlation test and Egger's linear regression test. A p-value < 0.05 was considered statistically significant. Sensitivity analyses were conducted by sequentially removing individual studies to examine the robustness of the results.
2.7 Risk of bias assessment
The methodological quality of the included studies was independently assessed by two reviewers using the quality appraisal criteria recommended by the Cochrane Collaboration. All studies included in this review were randomized controlled trials (RCTs). According to the Cochrane Handbook, the revised Cochrane risk of bias tool for randomized trials (RoB 2) was employed. RoB 2 provides a structured framework for evaluating the risk of bias in individual outcomes of randomized trials.The tool evaluates several domains, including random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other potential sources of bias. Reviewers rated each study according to the Cochrane Handbook guidelines. Each domain was rated as “low risk”, “some concerns” or “high risk” of bias. An overall risk of bias judgment was made as follows: “low risk” if all domains were rated as low risk; “some concerns” if at least one domain raised concerns but none were rated as high risk; and “high risk” if one or more domains were rated as high risk.
3 Results
3.1 Study selection
A total of 12,392 records were retrieved from four databases: PubMed, Web of Science, Embase, and the Cochrane Library. After removing 2,352 duplicates, 10,040 articles remained. Following title and abstract screening, 9,876 records were excluded, leaving 164 full-text articles for eligibility assessment. Of these, 137 articles were excluded due to reasons such as non-randomized study design or lack of relevant outcome data. Ultimately, 27 studies were included in this review. Two of these studies [Ansari et al. (4); Li et al. (5)] contained two eligible exercise interventions, yielding a total of 29 included comparisons.
The included studies were published between 2010 and 2024 and involved authors such as: Ansari et al. (4), Li et al. (5), Manizheh (6), Jin (7), Piedad et al. (8), Mahrokh et al. (9), Felzer-Kim and Hauck (3), Amir et al. (10), Xingda et al. (11), Ketcheson et al. (12), Yumi et al. (13), Li (14), Vieira et al. (15), Pan (16, 17), Yamaner et al. (18), Zhao et al. (19), Kelong et al. (20), Koenig et al. (21), Toscano et al. (22), Wang et al. (23), Xu et al. (24), Zhou et al. (25), Sotoodeh et al. (26), Choi et al. (27), Roza et al. (2), and Ezginur et al. (28).
(See Figure 1 for the PRISMA flow diagram).
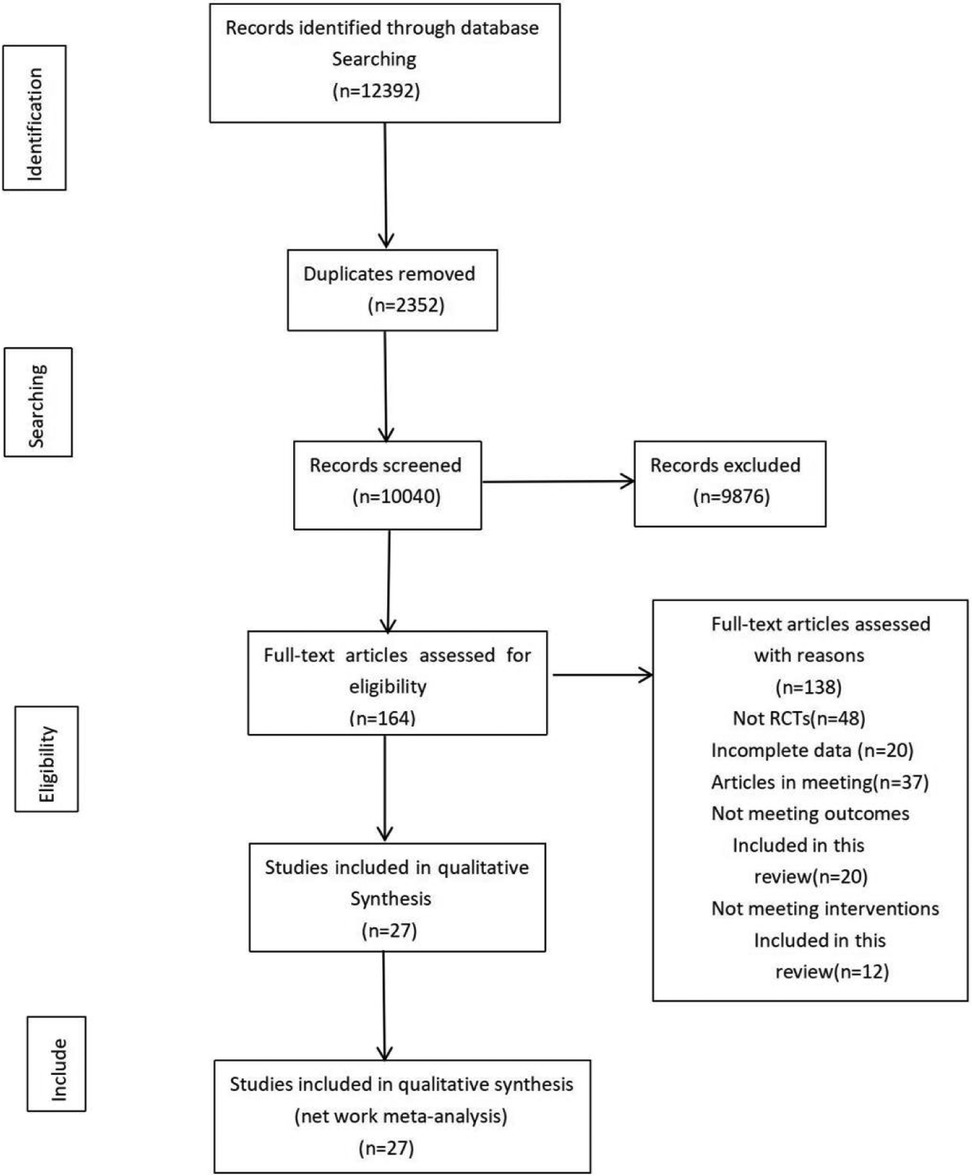
Figure 1. Literature search and screening flowchart.
3.2 Characteristics and quality assessment of included studies
3.2.1 Basic characteristics of included studies
A total of 27 randomized controlled trials were included, comprising 1,012 participants—551 in the intervention groups and 461 in the control groups. Gender distribution was explicitly reported in 22 studies, with a reported male-to-female ratio of 575:139. Four studies included only male participants. Two studies involved more than one exercise intervention group.
Among the included studies, 10 were conducted in China, 6 in Iran, 4 in the United States, 2 each in South Korea and Turkey, and 1 each in Colombia, Brazil, and Portugal. Participants were primarily recruited through schools and rehabilitation institutions (see Table 2).
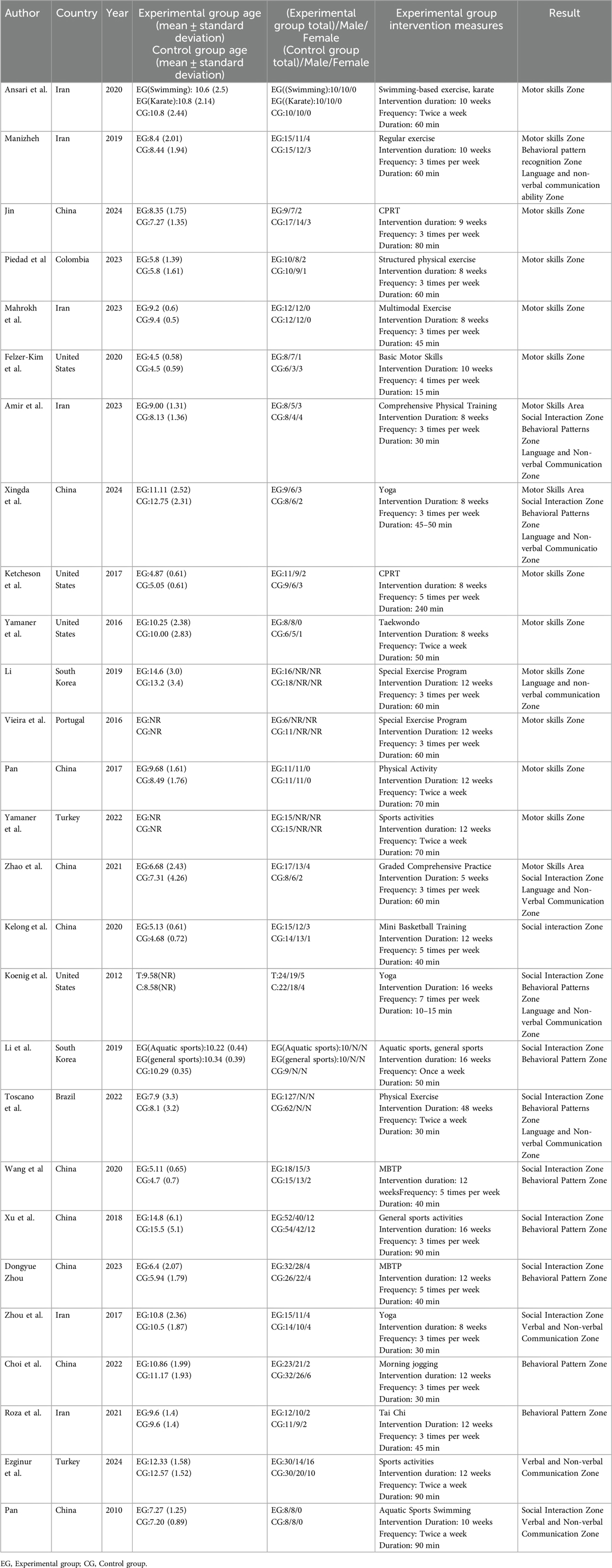
Table 2. Incorporating literature feature descriptions.
The duration of interventions ranged from 5 to 48 weeks, with exercise frequency varying between 1 and 5 days per week. All studies implemented exercise interventions, either supervised or home-based. Intervention types primarily included aerobic exercise, yoga, Tai Chi, swimming, karate, and mini-basketball.
Mean and standard deviation (SD) values were recorded for post-intervention outcomes in both intervention and control groups across the following domains: motor skills (Table 3), social interaction (Table 4), behavioral patterns (Table 5), and verbal/non-verbal communication (Table 6). After classifying the interventions, 28 studies involved cardiorespiratory exercise, 20 included resistance training, and 7 included flexibility exercises. Twenty-two studies implemented multi-modal exercise programs (Table 7).
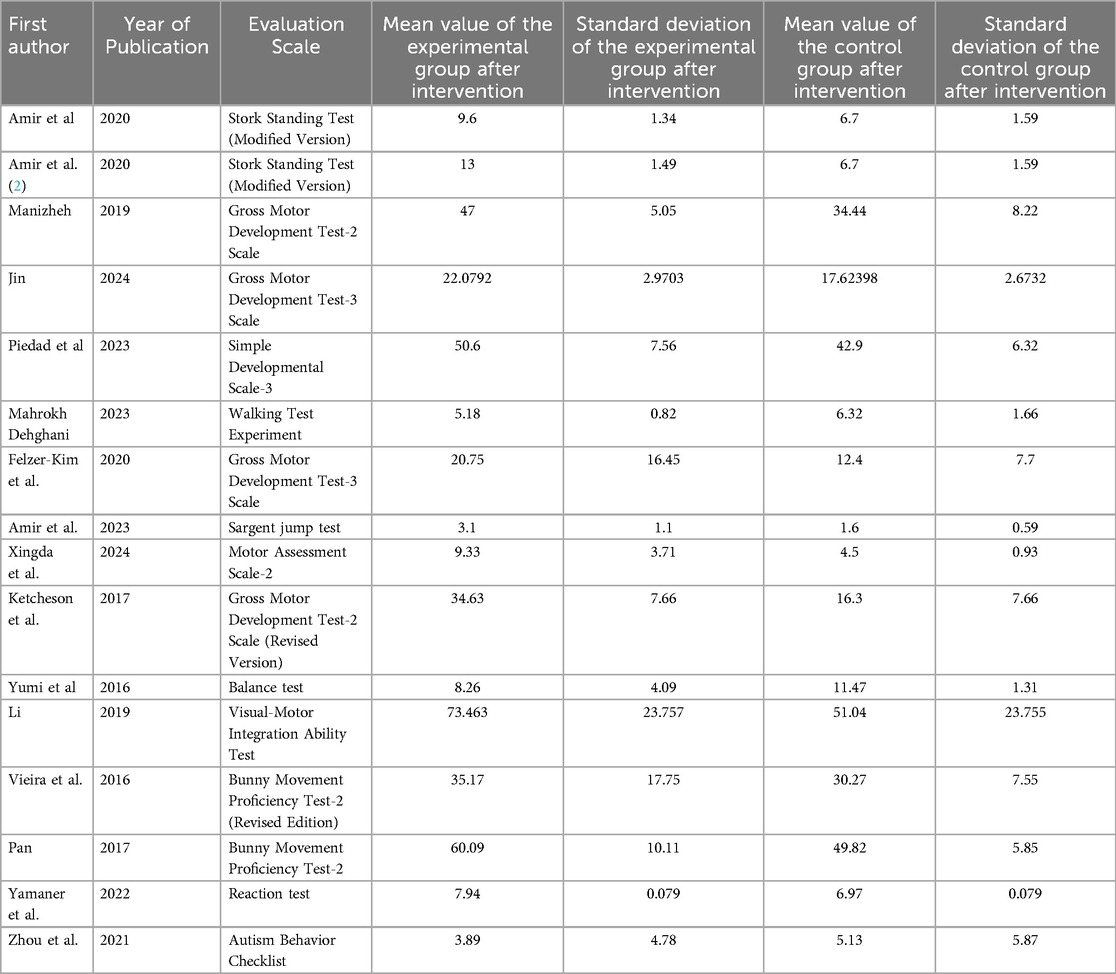
Table 3. Motor skill area group-related literature and research intervention outcomes.
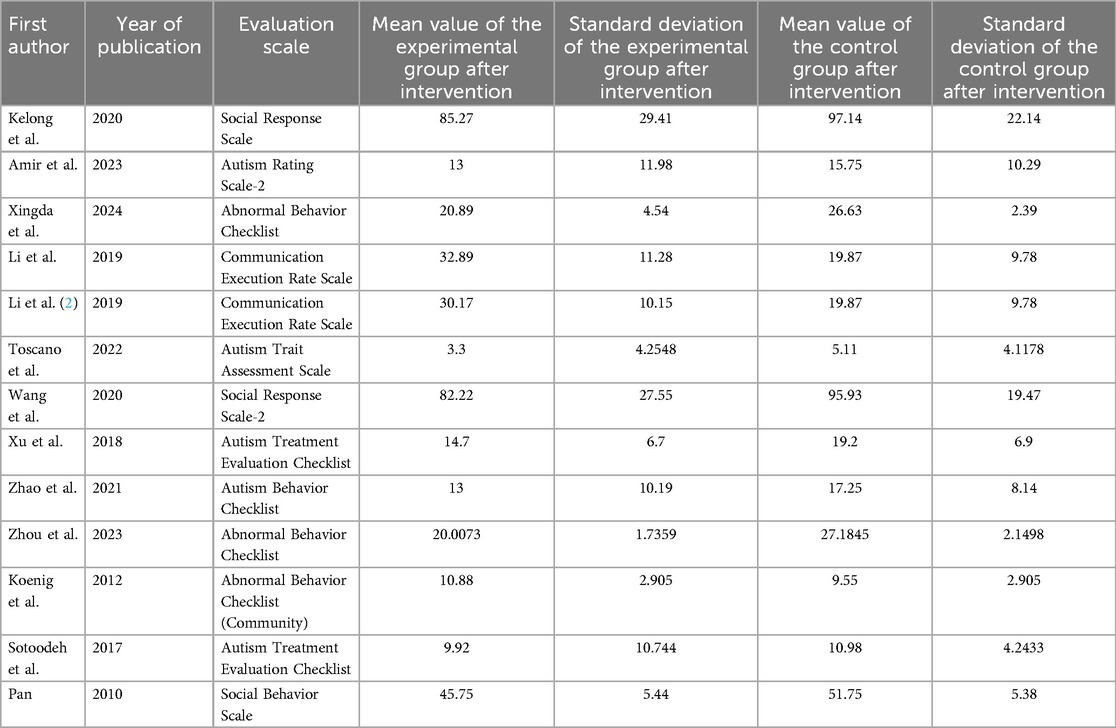
Table 4. Social interaction block-related literature and research intervention outcomes.
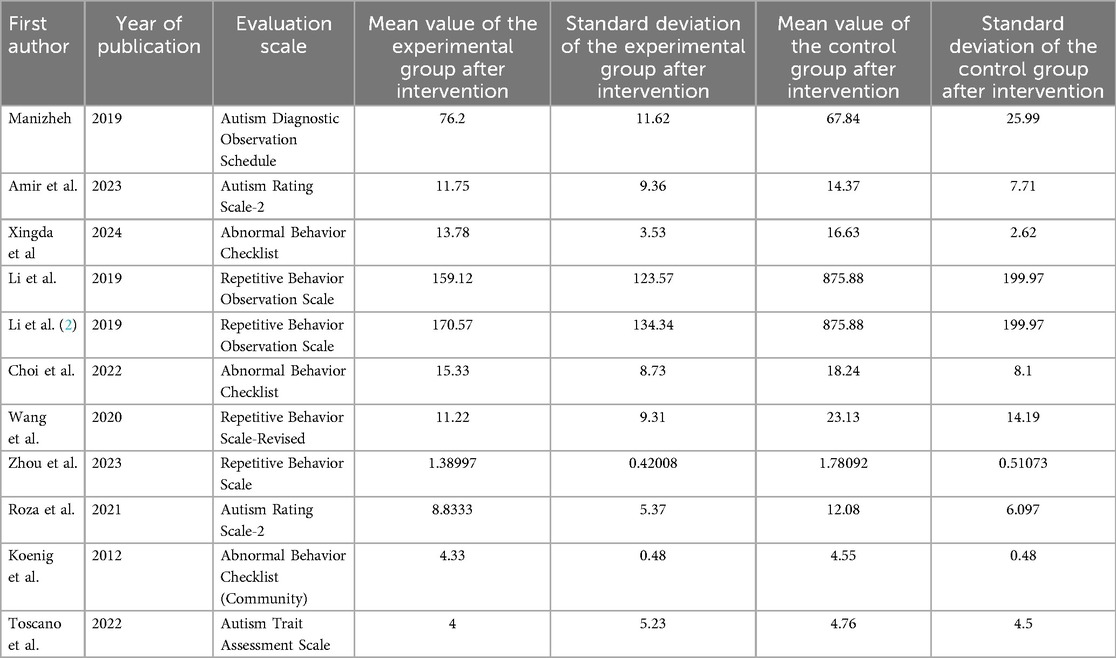
Table 5. Behavioral patterns in district groups: relevant literature and research intervention outcomes.
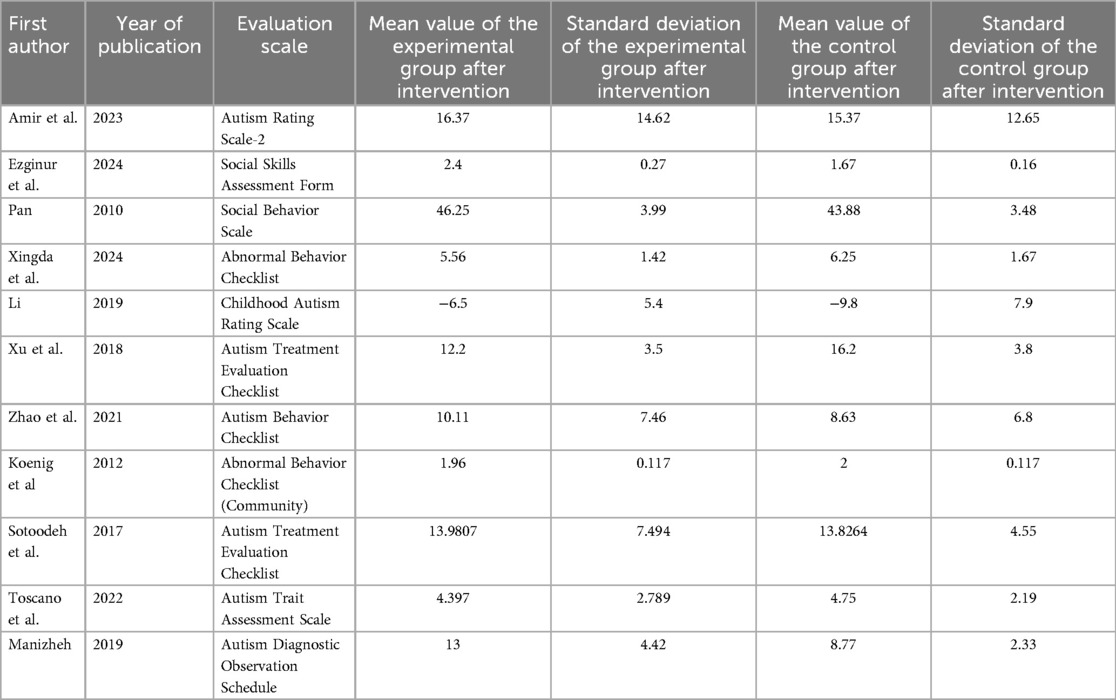
Table 6. Verbal and nonverbal communication ability group-related literature and research intervention outcomes.
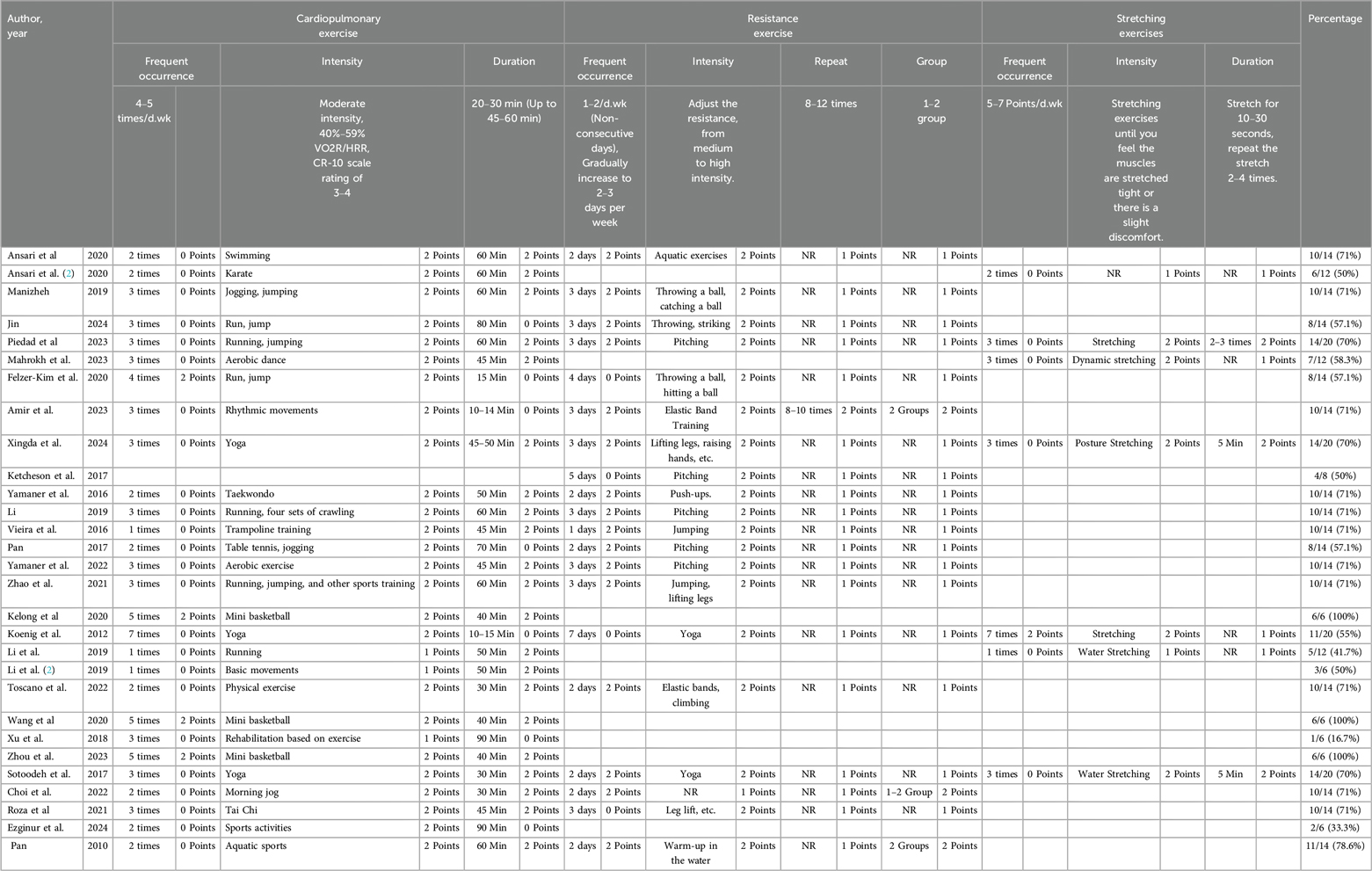
Table 7. Exercise intervention scores assessed according to the recommendations of the American college of sports medicine (ACSM).
3.2.2 Quality assessment of included studies
The methodological quality of the included studies was assessed using the risk of bias criteria recommended by the Cochrane Collaboration. All studies were judged to have a low risk of bias for random sequence generation. Among the 29 included exercise interventions, 23 were considered to have a low risk of bias for allocation concealment, while 6 studies did not report allocation methods and were rated as having an unclear risk.
Blinding of participants and personnel showed a relatively high risk of bias, as double-blinding was difficult to implement in exercise-based interventions. Outcome assessor blinding also exhibited elevated risk, as most outcomes were measured using subjective rating scales. Incomplete outcome data were observed in six cases due to missing behavioral scores, indicating a potential risk of bias.
Selective reporting was rated as low risk in 21 studies, moderate in 6 studies due to a lack of detailed explanations for participant dropout, and high in 2 studies. Additionally, two studies were identified as having other potential sources of bias (see Figure 2).
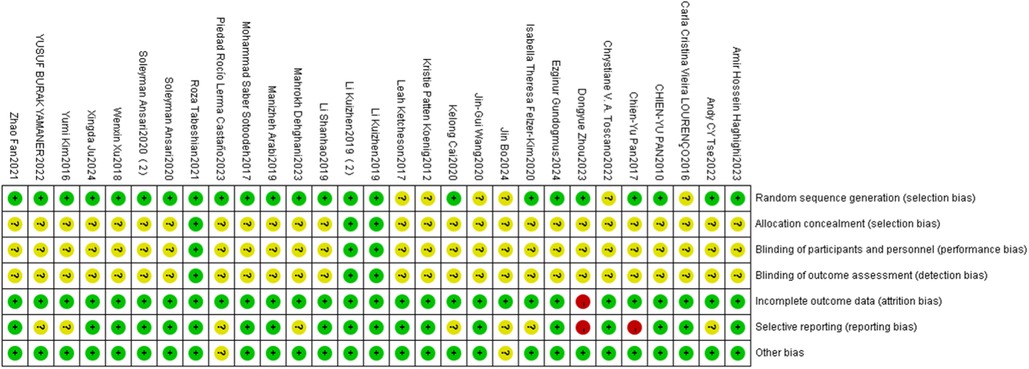
Figure 2. Risk of bias assessment for each included study.
3.3 Effects of adherence to ACSM guidelines on motor skills, social interaction, behavioral patterns, and communication domains
Among the 27 included studies (comprising 29 exercise interventions), 18 met the threshold for high adherence to ACSM guidelines (≥70%), while 11 were categorized as low adherence (<70%). Low adherence was attributed partly to discrepancies between the reported exercise dosage and the ACSM recommendations, and partly to insufficient reporting, which limited accurate evaluation of the exercise prescription.
3.3.1 Effects of adherence to ACSM guidelines on motor skills
When analyzing outcomes related to motor skills, 10 studies demonstrated high adherence to ACSM guidelines (≥70%), while 6 studies showed low adherence (<70%). Heterogeneity analysis revealed a high level of heterogeneity (I2 = 85%), prompting the use of a random-effects model for meta-analysis. The pooled standardized mean difference (SMD) for post-intervention motor skills between exercise and control groups was 1.35 (95% CI: [0.66,2.03], p < 0.001). These findings indicate a significant positive effect of exercise on motor skills in children with ASD.
Subgroup analysis yielded the following results: in the high adherence subgroup, the SMD was 1.44 (95% CI: [0.51,2.36], p = 0.002), with I2 = 86%, suggesting that high adherence to ACSM guidelines may be associated with greater improvements in motor skills. The confidence interval did not include zero, indicating statistical significance. However, the high heterogeneity indicates substantial variability across these studies.
In the low adherence subgroup, the SMD was 1.26 (95% CI: [0.15,2.36], p = 0.030), also with I2 = 86%. This result likewise suggests a positive effect of exercise on motor skills, as the confidence interval did not include zero. Nonetheless, the high heterogeneity suggests considerable differences in study design, sample characteristics, or intervention protocols, and thus the findings should be interpreted with caution.
Overall, exercise interventions with high adherence to ACSM guidelines were more strongly associated with improvements in motor skills among children with ASD compared to those with low adherence, though the substantial heterogeneity across studies warrants cautious interpretation (see Figure 3).
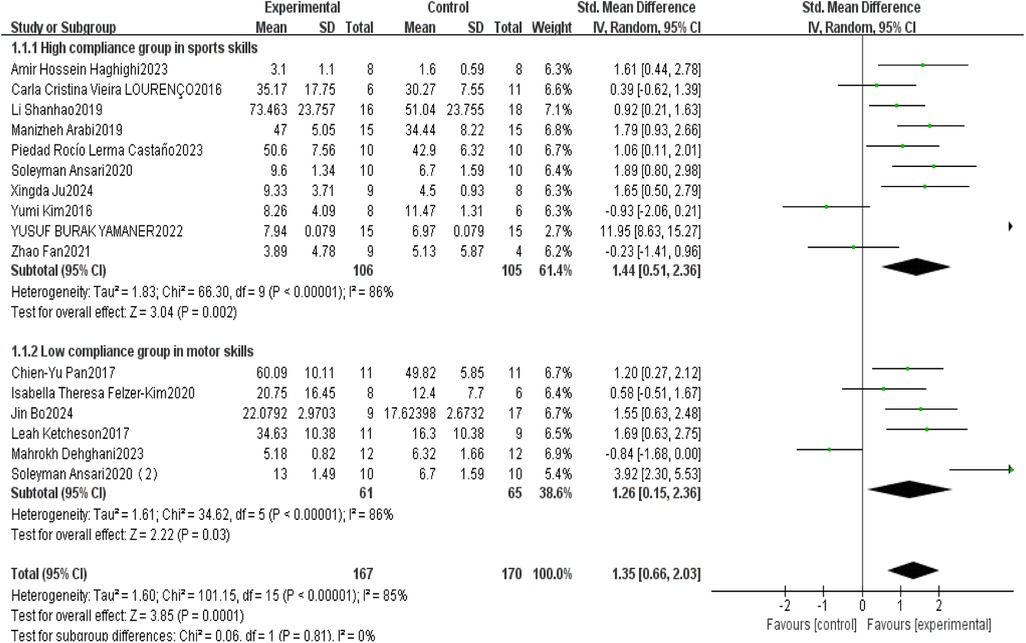
Figure 3. Forest plot of the impact of exercise intervention on motor skill domains.
Publication bias and sensitivity analyses were conducted to assess the robustness of the findings. The funnel plot (Figure 4) appeared symmetrical, suggesting no apparent publication bias. Begg's test (p = 0.105) indicated non-significant bias, whereas Egger's test (p = 0.001) revealed significant publication bias—potentially due to small-sample studies tending to report larger effect sizes, while larger studies may be underrepresented if their results were not statistically significant.
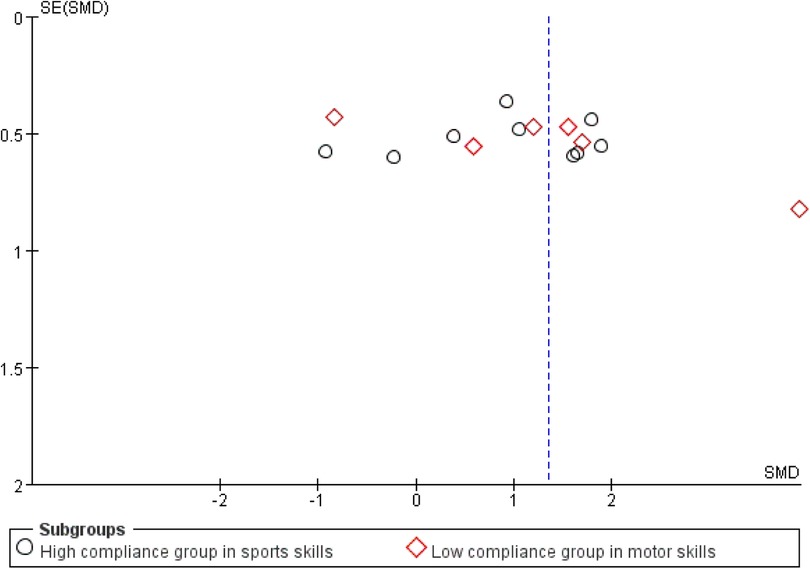
Figure 4. Funnel plot of the impact of exercise intervention on motor skill domains.
Sensitivity analysis (Figure 5) showed that excluding any single study did not materially alter the overall effect size, indicating that the results were stable and not unduly influenced by any individual study. Despite the presence of publication bias, the overall conclusions of the study remained robust.
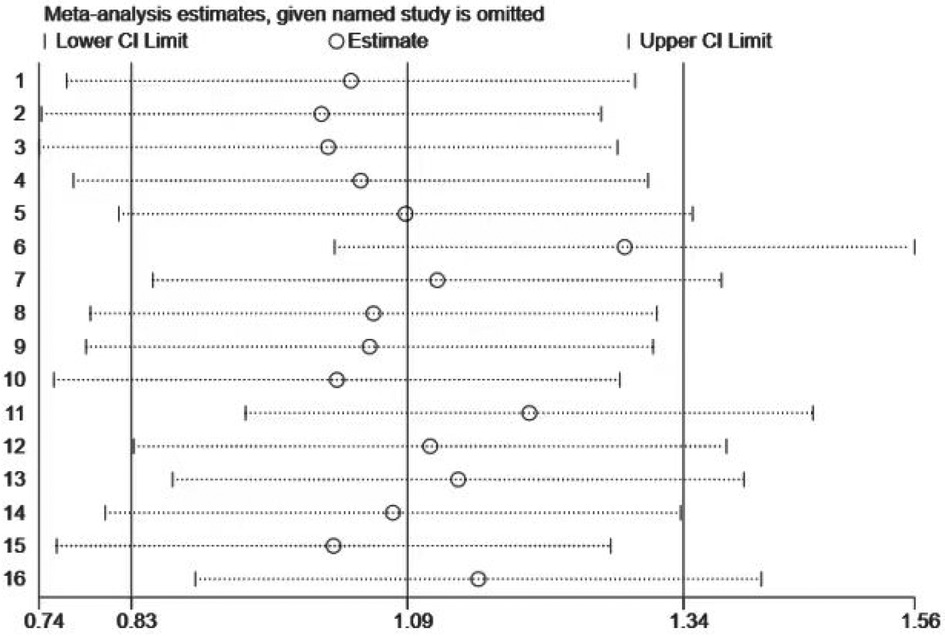
Figure 5. Sensitivity analysis of the impact of exercise intervention on motor skill domains.
3.3.2 Effects of adherence to ACSM guidelines on social interaction
This study conducted a systematic analysis of the effects of exercise interventions on social interaction in children with ASD. A total of 13 studies were included, of which 9 demonstrated high adherence to ACSM guidelines, and 4 were categorized as low adherence. Heterogeneity testing revealed I2 = 64%, indicating substantial heterogeneity (I2 > 50%); thus, a random-effects model was applied.
The standardized mean difference (SMD) in post-intervention social interaction scores between exercise and control groups was −0.22 (95% CI: [−0.54,0.99], p = 0.170), indicating a small, non-significant effect. Subgroup analyses revealed differential effects based on adherence to ACSM guidelines.
In the high adherence subgroup, the SMD was −0.41 (95% CI: [−0.62,−0.21], p < 0.001), with I2 = 0%. This suggests a statistically significant and reliable positive effect of exercise on social interaction, supported by the narrow confidence interval and absence of heterogeneity. Conversely, in the low adherence subgroup, the SMD was 0.42 (95% CI: [−0.50,1.33], p = 0.370), with high heterogeneity (I2 = 87%), indicating a non-significant effect with poor consistency across studies (Figure 6).
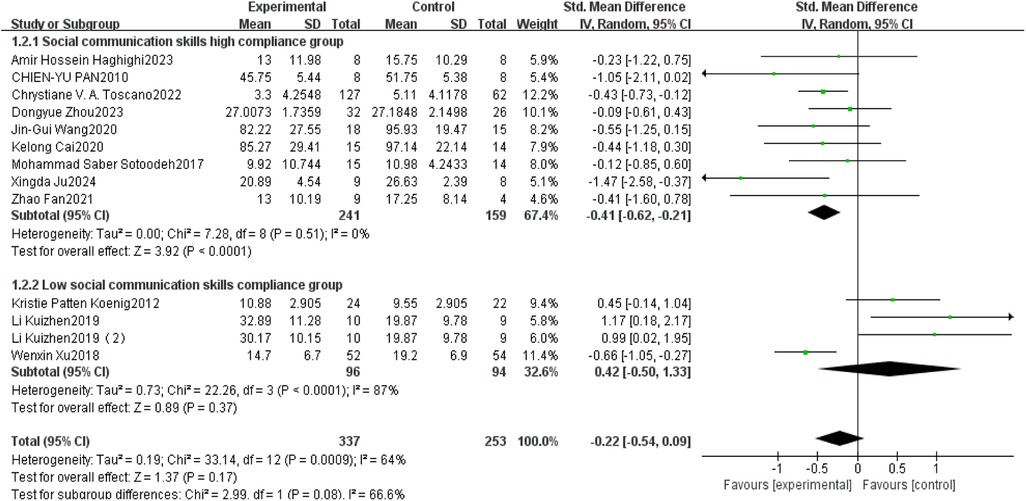
Figure 6. Forest plot of the impact of exercise intervention on the social interaction domain.
In summary, exercise interventions with high adherence to ACSM recommendations had a significant and robust effect on social interaction, whereas low adherence interventions showed no significant effect and high heterogeneity.
Publication bias and sensitivity analyses were subsequently performed to validate the robustness of the findings. Visual inspection of the funnel plot (Figure 7) revealed near symmetry, indicating no apparent publication bias. Quantitative assessment using Begg's test (p = 0.903) and Egger's test (p = 0.483) further confirmed the absence of significant publication bias. This suggests that small-study effects or other potential biases had minimal influence on the results.
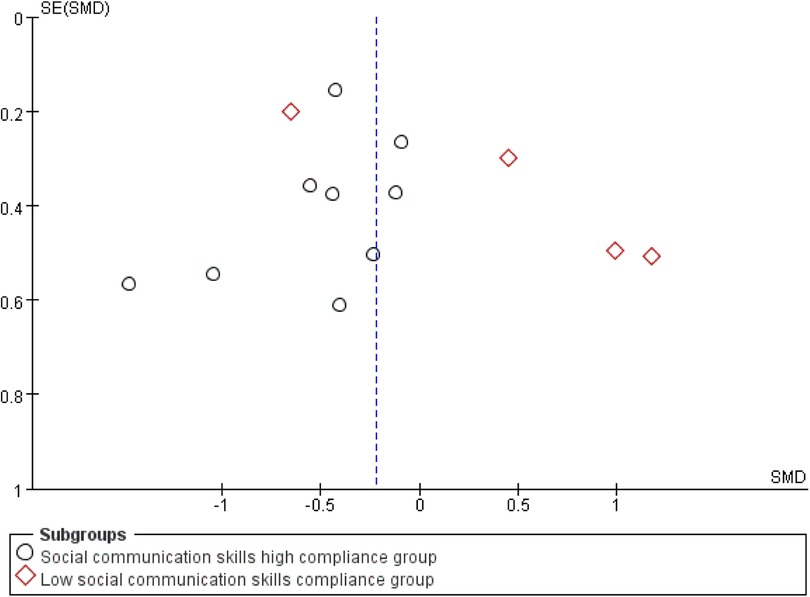
Figure 7. Funnel plot of the impact of exercise intervention on the social interaction domain.
Sensitivity analysis (Figure 8) was conducted by sequentially removing each individual study, showing that no single study materially altered the overall effect estimate. This further supports the robustness of the findings, as the overall effect estimate remained stable even when individual studies were excluded.
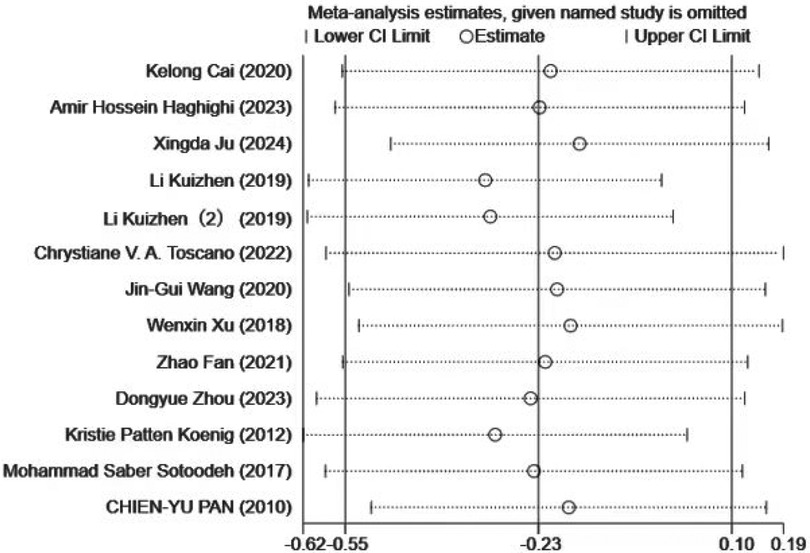
Figure 8. Sensitivity analysis of the impact of exercise intervention on social competence.
3.3.3 Effects of adherence to ACSM guidelines on behavioral patterns
This study conducted a systematic analysis of the effects of exercise interventions on behavioral patterns in children with ASD. A total of 11 studies were included, with 8 showing high adherence to ACSM guidelines and 3 categorized as low adherence. Heterogeneity testing revealed I2 = 79%, indicating substantial heterogeneity (I2 > 50%); therefore, a random-effects model was used for analysis.
The overall standardized mean difference (SMD) between the exercise and control groups for post-intervention behavioral scores was −0.79 (95% CI: [−1.26,−0.32], p = 0.001). These results indicate that exercise interventions had a significant positive effect on behavioral patterns in children with ASD, with a confidence interval that did not include zero.
Subgroup analysis further revealed the influence of adherence level on intervention outcomes. In the high adherence subgroup, the standardized mean difference (SMD) for post-intervention behavioral scores was −0.42(95% CI: [−0.73,−0.11], p = 0.008), with I2 = 47%. This indicates a statistically significant and reliable positive effect of exercise on behavioral patterns in children with ASD, supported by the narrow confidence interval and moderate heterogeneity.
In the low adherence subgroup, the SMD was −2.79 (95% CI: [−5.63,0.06], p = 0.050), with I2 = 93%. This suggests that the effect was not statistically significant, as the confidence interval included zero and the extremely high heterogeneity (I2 = 93%) reflects low consistency across studies (Figure 9).
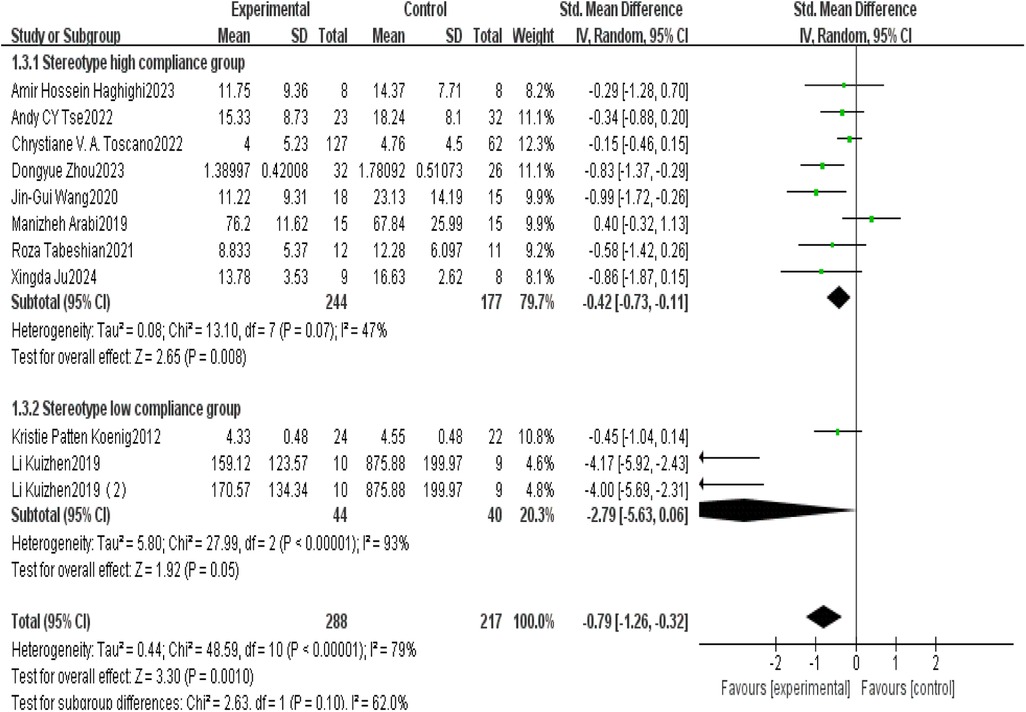
Figure 9. Forest plot of the impact of exercise intervention on behavioral pattern subdomains.
Publication bias and sensitivity analyses were subsequently conducted for this outcome domain. Visual inspection of the funnel plot (Figure 10) showed near symmetry, initially suggesting the absence of substantial publication bias. However, statistical tests indicated otherwise: Begg's test (p = 0.016) and Egger's test (p = 0.015) both indicated the presence of significant publication bias. This suggests possible selective reporting, where studies with statistically significant results are more likely to be published, while those with null findings may be underreported.
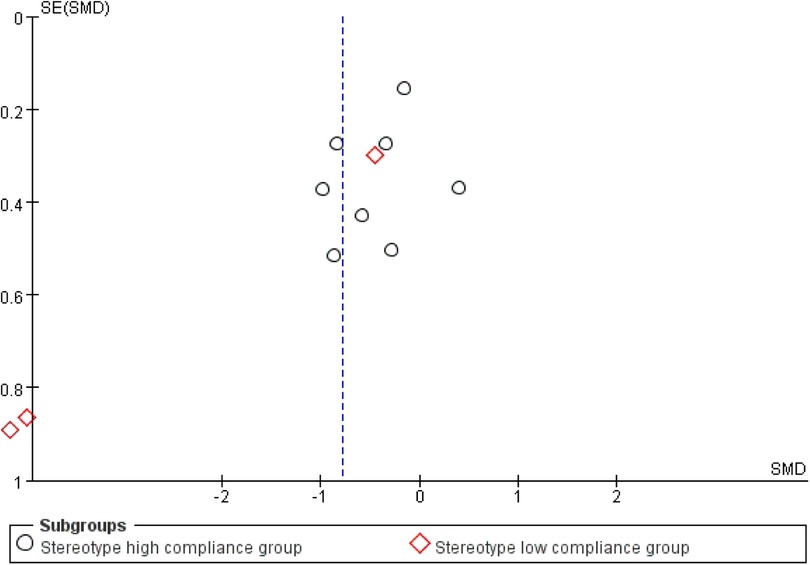
Figure 10. Funnel plot of the impact of exercise intervention on behavioral pattern domains.
Sensitivity analysis (Figure 11) was conducted by sequentially removing each included study, and the results indicated that no single study had a material impact on the overall effect estimate. This finding suggests that, despite the presence of publication bias, the overall results remain stable and are likely to reflect the true effect.
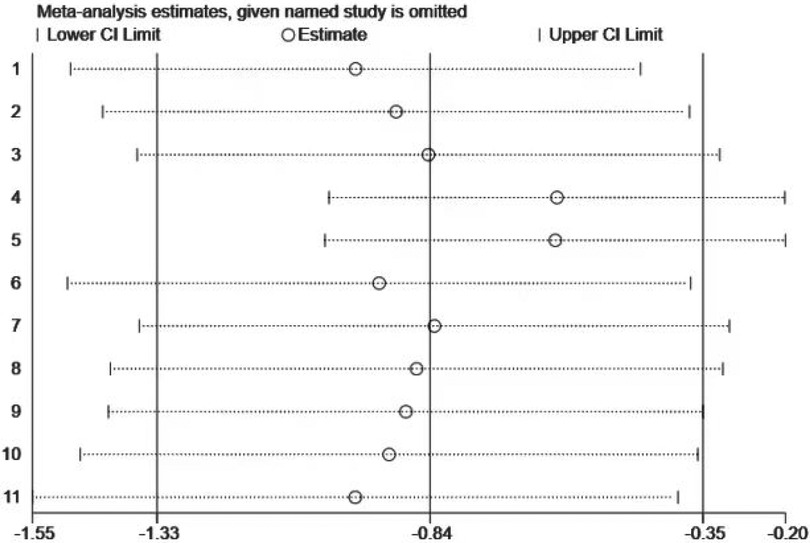
Figure 11. Sensitivity analysis of the impact of exercise intervention on behavioral pattern domains.
However, due to the presence of publication bias, these results should still be interpreted with caution, as bias may introduce some distortion in the conclusions. Future research should further investigate the underlying causes of such bias and account for its potential impact when interpreting outcomes.
3.3.4 Effects of adherence to ACSM guidelines on verbal and non-verbal communication
This study conducted a systematic analysis of language and nonverbal communication abilities in children with ASD to evaluate the effectiveness of exercise interventions. Ten studies were included, six of which demonstrated high adherence to the American College of Sports Medicine (ACSM) guidelines, while four exhibited low adherence. The heterogeneity test indicated substantial heterogeneity among studies (I2 = 91%, I2 > 50%), and therefore, a random-effects model was employed for statistical analysis. The overall analysis revealed that the difference in language and nonverbal communication scores between the exercise intervention group and the control group after completing clinical trials was not statistically significant (SMD = 0.33, 95% CI: [−0.31,0.91], p = 0.320), as the confidence interval included zero.
Further subgroup analyses indicated the influence of adherence level on intervention outcomes. In the high-adherence subgroup, the difference in language and nonverbal communication scores between the intervention and control groups was SMD = 0.21 (95% CI: [−0.14,0.57], p = 0.240), with an I2 of 45%. The confidence interval included zero, indicating no statistically significant effect. In the low-adherence subgroup, the difference was SMD = 0.59 (95% CI: [−1.67,2.84], p = 0.610), with an I2 of 98%, suggesting poor consistency among the included studies and no significant effect of the intervention.
In summary, regardless of adherence to ACSM-recommended exercise protocols, no significant effects of exercise interventions on the language and nonverbal communication abilities of children with ASD were observed. These findings suggest that exercise interventions may not be an effective strategy for improving communication in children with ASD, or that optimization of intervention protocols may be necessary to enhance their efficacy (Figure 12).
![Forest plot showing meta-analysis results of studies on language and nonverbal communication. It includes high and low compliance groups, with subgroups and total figures. Standardized mean differences are represented with confidence intervals, indicated by black diamonds. High compliance group summary: 0.21 [-0.14, 0.57]. Low compliance group summary: 0.59 [-1.67, 2.84]. Total summary: 0.33 [-0.31, 0.97]. Heterogeneity statistics are provided for each group and overall. Horizontal axis shows favor towards experimental or control groups.](https://www.frontiersin.org/files/Articles/1647280/frcha-04-1647280-HTML/image_m/frcha-04-1647280-g012.jpg)
Figure 12. Forest plot of the effects of exercise intervention on verbal and non-verbal communication.
This study further visually assessed potential publication bias using a funnel plot (Figure 13). The plot appeared approximately symmetrical on both sides, suggesting the absence of apparent publication bias. Subsequent statistical tests, including Begg's test (p = 0.102) and Egger's test (p = 0.17), revealed no significant publication bias, further supporting the robustness of the study findings.
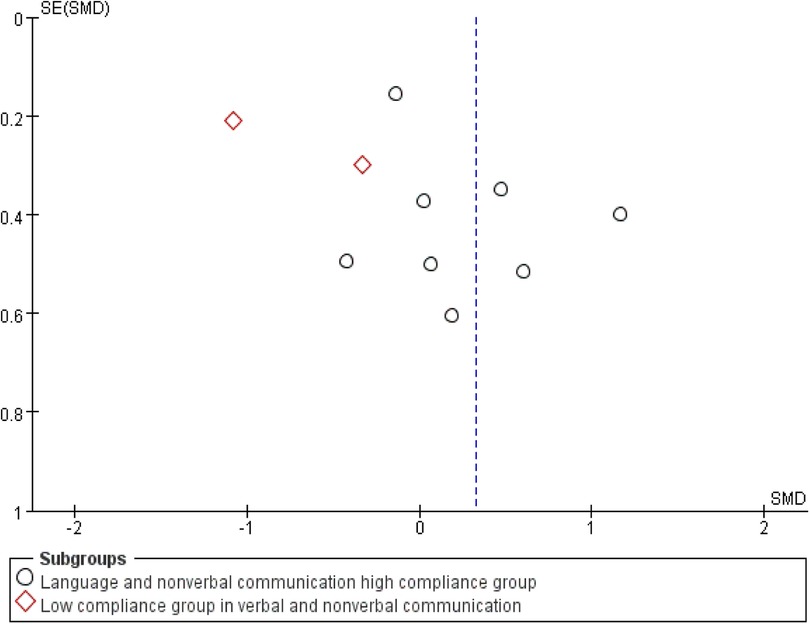
Figure 13. Funnel plot of the effects of exercise intervention on verbal and non-verbal communication.
In the sensitivity analysis (Figure 14), the sequential exclusion of each individual study indicated that no single study had a substantial impact on the overall results. This finding suggests that the results are robust, as the overall effect estimate remained stable even when individual studies were removed.
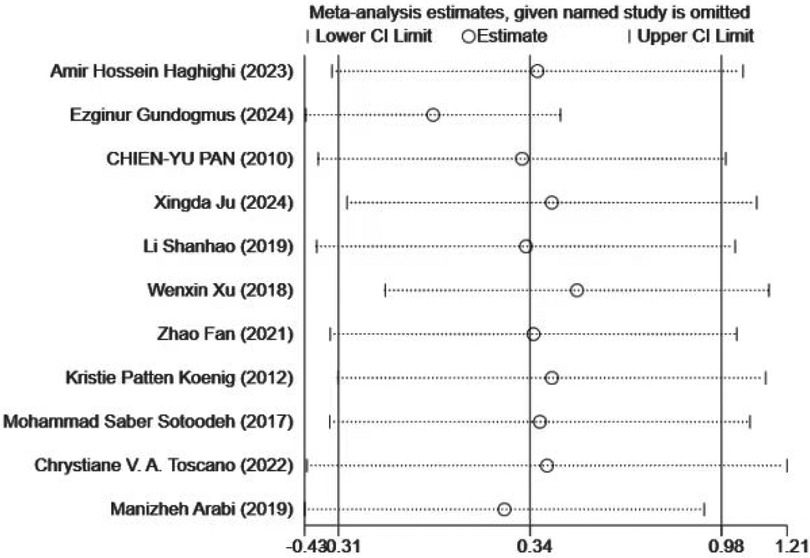
Figure 14. Sensitivity Analysis Diagram of the Impact of Exercise Intervention on Verbal and Nonverbal Communication.
3.3.5 Meta-regression analysis
Given the high level of observed heterogeneity, a meta-regression analysis was conducted to explore potential study-level characteristics that may have contributed to this variation. Participant characteristics, including health status, sex, and age, were initially considered. Studies that included participants with comorbid conditions were excluded; thus, health status was not incorporated as a factor in the meta-regression. Regarding sex, among studies that reported gender distribution, the combined male-to-female ratio was 575:139, which is consistent with the known prevalence rate of autism (approximately 3–4:1). Due to this significant sex imbalance, sex was not included as a factor in the meta-regression analysis. With respect to age, all participants were children, and age differences across studies were minimal. Furthermore, some studies did not report participant age, posing challenges to its inclusion; thus, age was excluded as a covariate.
Therefore, sample size and year of publication were included as potential sources of heterogeneity in the meta-regression analysis. The results of the meta-regression analyses across various outcome domains—including motor skills, social interaction domains, behavioral pattern domains, and language and nonverbal communication domains—revealed no statistically significant differences after adjusting for covariates such as sample size, year of publication, and overall composite factors (Table 8).

Table 8. Meta-regression analysis of the impact of different study characteristics on inter-study heterogeneity.
4 Discussion
This systematic review and meta-analysis investigated the impact of high versus low adherence to the American College of Sports Medicine (ACSM) recommendations. The analysis was based on data from 27 studies encompassing 29 exercise interventions, including 18 studies with high adherence and 11 with low adherence to the ACSM guidelines.
4.1 Positive impact of exercise interventions on children with ASD
Previous research has indicated that the effects of exercise interventions on social interaction, language, and nonverbal communication remain inconclusive. However, interventions with high adherence to the American College of Sports Medicine (ACSM) guidelines demonstrated significant improvements in social interaction, suggesting that exercise type, frequency, and intensity may play a critical role in therapeutic outcomes. Our findings further support this view, showing that a higher level of exercise dosage adherence—aligned with ACSM recommendations—was more beneficial in alleviating symptoms among children with ASD compared to interventions with lower adherence.
4.2 Adherence to exercise according to ACSM guidelines
One of the key strengths of this study is its integration of various exercise modalities, intensities, durations, and other relevant indicators employed in prior research. The study utilized adherence to the American College of Sports Medicine (ACSM) guidelines as a grouping variable to evaluate the effect of exercise dosage on symptom improvement in children with ASD. A central aspect of this study lies in the definition and operationalization of ACSM adherence, which provided a standardized framework for comparison across interventions. Based on this framework, we conducted a focused analysis specifically examining the influence of ACSM adherence across different exercise types on ASD symptomatology. The research design included analyses of aerobic exercise, resistance training, and stretching interventions.
4.3 The impact of ACSM adherence on the effectiveness of exercise interventions
In this study, we aimed to include as many types of exercise interventions as possible to assess the impact of adherence to the American College of Sports Medicine (ACSM) guidelines on intervention effectiveness. A meta-analysis with subgroup analyses based on adherence to ACSM-recommended exercise dosage revealed that interventions with high ACSM adherence were more effective than those with low adherence in improving motor skills, social interaction, and behavioral patterns in children with ASD.
For the social interaction domain, the high-adherence group showed a statistically significant effect (SMD = −0.41, 95% CI: [−0.62,−0.21]), whereas the low-adherence group did not (SMD = −0.42, 95% CI: [−0.5,1.33]). In the behavioral pattern domain, the high-adherence group also demonstrated a significant improvement (SMD = −0.35, 95% CI: [−0.55,−0.15]), while the low-adherence group did not (SMD = −2.79, 95% CI: [−5.63,0.06]). These findings suggest that high adherence to ACSM-guided exercise significantly benefits social interaction and behavioral outcomes in children with ASD.
When examining the impact of ACSM adherence on motor skills, the improvement was greater in the high-adherence group (SMD = 1.44) than in the low-adherence group (SMD = 1.26), and the narrower confidence interval in the high-adherence group indicates greater reliability of the results. In contrast, exercise interventions based on ACSM guidelines had limited effects on language and nonverbal communication, with neither subgroup demonstrating statistical significance.
In conclusion, consistent with multiple studies, adherence to ACSM-recommended exercise regimens appears to have a positive influence on various symptoms in children with ASD.
4.4 Other influencing factors
This study exhibited a degree of heterogeneity, which was addressed using sensitivity and subgroup analyses. The results remained robust following the sequential exclusion of individual studies. Similar to pharmacological treatment, exercise therapy has been explored as an alternative method for managing symptoms in children with ASD. In the process of determining optimal exercise dosage, it is essential to provide a detailed description of the intervention protocol to establish an appropriate dosage range. However, the variability across studies has increased the complexity of identifying optimal exercise modalities and dosage parameters.
Based on current evidence, we can only infer that physical activity may improve symptoms in children with ASD; no specific exercise regimen has been proven to be superior to others. Current research remains focused on comparing the effects of specific aspects of exercise interventions, and there is a lack of standardized guidelines for determining optimal exercise protocols and dosages. Although the American College of Sports Medicine (ACSM) provides general exercise recommendations, there remains controversy and uncertainty regarding their application to ASD populations. Nonetheless, our findings support the feasibility of implementing ACSM-recommended exercise prescriptions in this population.
4.5 Limitations and future directions of this study
Despite the valuable findings and contributions of this study, several limitations should be acknowledged. First, the study relied on meta-analyses of previously published research, making it inherently subject to the limitations and potential biases present in the original studies. Another limitation is the absence of standardized protocols for exercise interventions and dosage across the included studies. The variability in exercise type, intensity, duration, and frequency poses a challenge to drawing definitive conclusions regarding the optimal exercise dosage for improving symptoms in children with ASD.
Future research should focus on developing standardized intervention protocols and guidelines tailored to this population. Looking ahead, well-designed, large-scale randomized controlled trials (RCTs) with extended follow-up periods are essential. These studies should incorporate standardized exercise protocols and consider individual characteristics—such as age, sex, and comorbidities—to enable the effective personalization of exercise interventions.
5 Conclusion
Exercise interventions demonstrate positive effects on motor skills and behavioral patterns in children with ASD. In exploring optimal exercise dosage, findings indicate that interventions with high adherence to the American College of Sports Medicine (ACSM) guidelines are more effective than low-adherence interventions in improving motor skills, social interaction, and behavioral patterns in children with ASD, with particularly pronounced effects observed in the domains of social interaction and behavioral patterns.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Author contributions
BH: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – original draft. QL: Data curation, Investigation, Validation, Visualization, Writing – original draft. HJ: Funding acquisition, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors express gratitude to Enping People's Hospital for providing clinical resources and research support. We also thank Department of pediatric, Lequn district, Children's Medical Center, The First Hospital of Jilin University for academic guidance. Special appreciation to peer reviewers for their valuable insights.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frcha.2025.1647280/full#supplementary-material
References
1. Shaw KA, Williams S, Patrick ME, Valencia-Prado M, Durkin MS, Howerton EM, et al. Prevalence and early identification of autism spectrum disorder among children aged 4 and 8 years — autism and developmental disabilities monitoring network, 16 sites, United States, 2022. MMWR Surveill Summ. (2025) 74(SS-2):1–22. doi: 10.15585/mmwr.ss7402a1
2. Tabeshian R, Nezakat-Alhosseini M, Movahedi A, Zehr EP, Faramarzi S. The effect of Tai Chi Chuan training on stereotypic behavior of children with autism spectrum disorder. J Autism Dev Disord. (2022) 52(5):2180–2186. doi: 10.1007/s10803-021-05090-w
3. Felzer-Kim IT, Hauck JL. How much instructional time is necessary? Mid-intervention results of fundamental movement skills training within ABA early intervention centers. Front Integr Neurosci. (2020) 14:24. doi: 10.3389/fnint.2020.00024
4. Ansari S, Hosseinkhanzadeh AA, AdibSaber F, Shojaei M, Daneshfar A. The effects of aquatic versus kata techniques training on static and dynamic balance in children with autism spectrum disorder. J Autism Dev Disord. (2021) 51:3180–3186. doi: 10.1007/s10803-020-04785-w
5. Li K-J, Kim Y-H. The effects of aquatic exercise on communication skills and stereotypic behaviors in children with autism spectrum disorder. J Korean Soc Elem Phys Educ. (2019) 25(3):163–74.
6. Arabi M. Is visuomotor training an effective intervention for children with autism spectrum disorders? Neuropsychiatr Dis Treat. (2019):3089–3102. doi: 10.2147/NDT.S214991
7. Jin B. Transfer and retention effects of a motor program in children with autism spectrum disorders. Adapt Phys Activ Q. (2019) 41:88–106. doi: 10.1123/apaq.2022-0200
8. Castaño PRL, Suárez DPM, González ER, Robledo-Castro C, Hederich-Martínez C, Cadena HPG, et al. Effects of physical exercise on gross motor skills in children with autism spectrum disorder. J Autism Dev Disord. (2024) 54:2816–2825. doi: 10.1007/s10803-023-06031-5
9. Dehghani M, Jafarnezhadgero AA, Darvishani MA, Aali S, Granacher U. Effects of an 8-week multimodal exercise program on ground reaction forces and plantar pressure during walking in boys with autism spectrum disorder. Trials. (2023) 24(1):170. doi: 10.1186/s13063-023-07158-7
10. Haghighi AH, Broughani S, Askari R, Shahrabadi H, Souza D, Gentil P. Combined physical training strategies improve physical fitness, behavior, and social skills of autistic children. J Autism Dev Disord. (2023) 53(11):4271–4279. doi: 10.1007/s10803-022-05731-8
11. Ju X, Liu H, Xu J, Hu B, Jin Y, Lu C. Effect of yoga intervention on problem behavior and motor coordination in children with autism. Behav Sci. (2024) 14(2):116. doi: 10.3390/bs14020116
12. Ketcheson L, Hauck J, Ulrich D. The effects of an early motor skill intervention on motor skills, levels of physical activity, and socialization in young children with autism spectrum disorder: a pilot study. Autism. (2017) 21:481–492. doi: 10.1177/1362361316650611
13. Kim Y, Todd T, Fujii T, Lim J-C, Vrongistinos K, Jung T. Effects of taekwondo intervention on balance in children with autism spectrum disorder. J Exerc Rehabil. (2016) 12(4):314–317. doi: 10.12965/jer.1632634.317
14. Jin B. Effects of special physical education programs on motor skills, cognition, and behavioral changes in autistic children during the growth phase. J Korean Soc Growth Dev. (2019) 27(2):79–86.
15. Lourenço CCV, Esteves MDL, Corredeira RMN, Teixeira e Seabra AF. The efficacy of a training program on trampolines in motor proficiency of children with autism spectrum disorder. Rev Bras Educ Espec. (2016) 22(1):39–48. doi: 10.1590/S1413-65382216000100004
16. Pan CY. The efficacy of an aquatic program on physical fitness and aquatic skills in children with and without autism spectrum disorders. Res Autism Spectr Disord. (2011) 5(1):657–665. doi: 10.1016/j.rasd.2010.08.001
17. Pan C-Y, Chu C-H, Tsai C-L, Sung M-C, Huang C-Y, Ma W-Y. The impacts of physical activity intervention on physical and cognitive outcomes in children with autism spectrum disorder. Autism. (2017) 21(2):190–202. doi: 10.1177/1362361316633562
18. Yamaner YB, Demirli A, Moghanlou AE, Gökçelik E. The effect of aerobic exercises on skill behaviour of autestic children. Pak J Med Health Sci. (2022) 16(03):713. doi: 10.53350/pjmhs22163713
19. Zhao F, Lu F, Tan CH, et al. Effects of graded comprehensive motor training on children with autism spectrum disorder: A comparison between comorbidities with ADHD and non-comorbidities. Chin J Clin Psychol. (2021) 29(4):869–75.
20. Cai K, Yu Q, Herold F, Liu Z, Wang J, Zhu L, et al. Mini-basketball training program improves social communication and white matter integrity in children with autism. Brain Sci. (2020) 10(11):803. doi: 10.3390/brainsci10110803
21. Koenig KP, Buckley-Reen A, Garg S. Efficacy of the get ready to learn yoga program among children with autism spectrum disorders: a pretest–posttest control group design. Am J Occup Ther. (2012) 66(5):538–546. doi: 10.5014/ajot.2012.004390
22. Toscano CVA, Ferreira JP, Quinaud RT, Silva KMN, Carvalho HM, Gaspar JM. Exercise improves the social and behavioral skills of children and adolescent with autism spectrum disorders. Front Psychiatry. (2022) 13:102–108. doi: 10.3389/fpsyt.2022.1027799
23. Wang J-G, Cai K-L, Liu Z-M, Herold F, Zou L, Zhu L-N, et al. Effects of mini-basketball training program on executive functions and core symptoms among preschool children with autism spectrum disorders. Brain Sci. (2020) 10(5):263–268. doi: 10.3390/brainsci10050263
24. Xu W, Zhao Z, Ceng M, et al. Efectos de la intervención de un modelo de rehabilitación basado en el ejercicio sobre la soledad y las conductas saludables de adolescentes con autismo. Rev Argent Clín Psicol. (2018) 27(3):445–465.
25. Zhou D, Liu Z, Gong G, Zhang Y, Lin L, Cai K, et al. Decreased functional and structural connectivity is associated with core symptom improvement in children with autism spectrum disorder after mini-basketball training program. J Autism Dev Disord. (2024) 54:4515–4528. doi: 10.1007/s10803-023-06160-x
26. Sotoodeh MS, Arabameri E, Panahibakhsh M, Kheiroddin F, Mirdoozandeh H, Ghanizadeh A. Effectiveness of a yoga training program on the severity of autism. Complement Ther Clin Pract. (2017) 28:47–53. doi: 10.1016/j.ctcp.2017.05.001
27. Tse AC, Lee PH, Zhang J, Chan RC, Ho AW, Lai EW. Effects of exercise on sleep, melatonin level, and behavioral functioning in children with autism. Autism. (2022) 26(7):1712–1722. doi: 10.1177/13623613211062952
Keywords: autism, exercise dosage, ACSM, meta-analysis, children
Citation: Hu B, Liang Q and Jiang H (2025) Effects of exercise dosage on children with autism spectrum disorder: a systematic review and meta-analysis of randomized controlled trials. Front. Child Adolesc. Psychiatry 4:1647280. doi: 10.3389/frcha.2025.1647280
Received: 17 June 2025; Accepted: 11 August 2025;
Published: 4 September 2025.
Edited by:
Sara Calderoni, Stella Maris Foundation (IRCCS), ItalyReviewed by:
Karah Dring, Nottingham Trent University, United KingdomCarla Lourenço, University of Beira Interior, Portugal
Copyright: © 2025 Hu, Liang and Jiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huiyi Jiang, aHlqaWFuZ0BqbHUuZWR1LmNu
†Present Address: Baojian Hu,Enping People's Hospital, Enping City, Guangdong Province, China