 Iryna Culpin1,2*
Iryna Culpin1,2* Rebecca M. Pearson2,3,4
Rebecca M. Pearson2,3,4 Nicky Wright3,5
Nicky Wright3,5 Alan Stein6,7
Alan Stein6,7 Marc H. Bornstein8,9,10
Marc H. Bornstein8,9,10 Henning Tiemeier11,12
Henning Tiemeier11,12 Eivor Fredriksen13Jonathan Evans2
Eivor Fredriksen13Jonathan Evans2 Tina Miller14
Tina Miller14 Esther Dermott15
Esther Dermott15 Jon Heron2,4Hannah M. Sallis2,4
Jon Heron2,4Hannah M. Sallis2,4 Gemma Hammerton2,4
Gemma Hammerton2,4
- 1Department of Child and Family Health, Florence Nightingale Faculty of Nursing, Midwifery and Palliative Care, King’s College London, London, United Kingdom
- 2Centre for Academic Mental Health, Population Health Sciences, Bristol Medical School, University of Bristol, Bristol, United Kingdom
- 3Department of Psychology, Manchester Metropolitan University, Manchester, United Kingdom
- 4Medical Research Council Integrative Epidemiology Unit at the University of Bristol, Population Health Sciences, Bristol Medical School, University of Bristol, Bristol, United Kingdom
- 5Department of Psychology, University of Leeds, Leeds, United Kingdom
- 6Department of Psychiatry, University of Oxford, Oxford, United Kingdom
- 7MRC/Wits Rural Public Health and Health Transitions Research Unit (Agincourt), School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
- 8Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, MD, United States
- 9Institute for Fiscal Studies, London, United Kingdom
- 10ECD Parenting Programmes, UNICEF, New York City, NY, United States
- 11Department of Child and Adolescent Psychiatry, Erasmus University Medical Center, Rotterdam, Netherlands
- 12Department of Social and Behavioral Science, Harvard T.H. Chan School of Public Health, Boston, MA, United States
- 13Department of Psychology, University of Oslo, Oslo, Norway
- 14School of Social Sciences, Oxford Brookes University, Oxford, United Kingdom
- 15School for Policy Studies, University of Bristol, Bristol, United Kingdom
Introduction: Paternal postnatal depression (PND) and its likely adverse impact on child development are receiving increased attention. However, research that examines processes transmitting risks of paternal PND to adverse child outcomes remains limited.
Methods: This study examines pathways from paternal PND (Edinburgh Postnatal Depression Scale; 8 months) to child emotional and behavioral development (Strengths and Difficulties Questionnaire; 7 years) through paternal parenting confidence, warmth, and father-child conflict (birth-4 years) in a UK-based birth cohort, the Avon Longitudinal Study of Parents and Children (N = 9,628). Analyses were adjusted for socioeconomic, familial, parental, and child characteristics, including maternal PND during early postnatal period.
Results: Adjusted models revealed evidence of total associations between paternal PND, child emotional symptoms, peer problems, and hyperactivity (albeit with wide 95% CIs), but not conduct problems. Indirect effects emerged from paternal PND to child emotional symptoms, hyperactivity, and peer problems through the combination of all paternal parenting factors, with no evidence of direct effects. Specificity analyses revealed indirect effects through paternal parenting confidence and father-child conflict in the associations between paternal PND and child emotional symptoms, hyperactivity, and peer problems (albeit with wide 95% CIs).
Conclusions: Targeted intervention to increase paternal parenting confidence and decrease father-child conflict may improve outcomes in children whose fathers experience postnatal depression.
Introduction
Growing evidence suggests that fathers are at increased risk of depression during their partner's pregnancy and the postnatal period (1). Meta-analyses have estimated the prevalence of paternal depression to be 9.76% during pregnancy and 8.75% during the postnatal period (2), peaking during the third trimester (9%–12%; 3) and again around 3 to 6 months postnatally (up to 26%; 4). The prevalence estimates of paternal depression in pregnancy and the postnatal period are higher than in the general adult population (3, 5), with the transition to parenthood and maternal postnatal depression (PND) increasing the risk of paternal postnatal depression (PND; 3, 4, 6). These prevalence estimates indicate that paternal depression in pregnancy and the postnatal period represent a substantial public health concern, warranting close and separate examination for their potential consequences for child development.
Increasingly, studies report consistent associations between paternal PND and increased risk of adverse child development (7), including emotional and behavioral difficulties (8, 9), peer problems (10), and hyperactivity (11). However, few studies examine processes transmitting risks from paternal PND to adverse child outcomes (7). Meta-analyses highlight genetic contributions in the inter-generational transmission of depression, with twin studies estimating its heritability at approximately 30%–40% (12). Nonetheless, depression is a complex polygenic trait influenced by many small effect genetic variants (13). Environmental mechanisms also play a role in risk transmission, including those in the immediate family environment (14, 15).
For instance, negative influences of paternal PND on child development may be transmitted through adverse effects on parenting behaviors and involvement (8, 16), including higher levels of father-child conflict, criticism, and harsh discipline and lower levels of father-child enjoyment and warmth (17). In turn, lower quality and quantity of paternal involvement (e.g., paternal non-involvement) are negatively related to emotional and behavioral child development (18, 19), thus potentially mediating the risk of depression transmission from father to child. To date, limited research has examined different dimensions of paternal involvement as potential mechanisms of risk transmission in associations between paternal PND and child development, with most studies focusing on single aspects of the father-child relationship (e.g., father-child conflict; 20) or a composite measure of paternal involvement (e.g., sum-score; 19). Conceptualizing and operationalizing father involvement as a single construct or a composite measure (unidimensional approach) may represent conceptual and methodological limitations. Conceptually, definitions of paternal involvement long ago departed from the traditional breadwinning roles and the mere time fathers and children spend together (21–23). Contemporary theories of fathering conceptualize paternal involvement as a multidimensional construct, encompassing distinct cognitive and affective/behavioral dimensions (24). The cognitive dimensions include thoughts and feelings related to parenting, such as parenting confidence (22, 25), while the affective/behavioral dimensions capture quality of father-child relationship, such as enjoyment, warmth and conflict (24–28). Paternal parenting confidence (i.e., paternal perceptions of competence in the parenting role) is a key factor in greater paternal involvement (29), playing an important role in influencing child development (30, 31). Affective/behavioral dimensions, such as enjoyment, warmth, and conflict are also important determinants of child development (25, 32, 33). Methodologically, these distinct dimensions may be differentially associated with child development. Disaggregating contributions of specific paternal cognitions and practices to child development would advance our understanding of unique paternal contributions to child outcomes, while also informing the design of targeted preventative and intervention programs (24). A systematic review of qualitative studies of father involvement during early childhood suggested that the roles of these dimensions in influencing paternal parenting behaviors and child development should be explored in future research (26).
In previous analyses, we derived several child-focused and mother-influenced dimensions of paternal involvement and examined their role in the associations between maternal PND and child development (18). Child-focused paternal involvement captured behavioral (e.g., direct involvement in caregiving), affective (e.g., enjoyment, warmth, father-child conflict, and worries about the child) and cognitive (e.g., parenting confidence and beliefs regarding caregiving) dimensions directed at the child. In contrast, mother-influenced dimensions encompassed aspects of paternal involvement with the child through the lens of maternal expectations (e.g., maternal “gatekeeping”, managing employment and parenthood), mother-father relationship (e.g., paternal beliefs regarding mother-father relationship and its impact on parenting) and indirect material care through support of the mother (e.g., paternal help with household tasks and responsibilities). Out of all child-focused dimensions (six in total) of paternal involvement, only lower levels of parental parenting confidence, enjoyment, and warmth, and higher levels of conflictual father-child relationship were strongly associated with higher risk of adverse child development in the context of maternal PND. There was no evidence for associations between any mother-influenced dimensions of paternal involvement and child development (18).
Based on these findings and stimulated by the specificity principle (34), the present study sought to estimate the extent to which associations between paternal PND at 8 months and child emotional symptoms, conduct problems, hyperactivity and peer problems at 7 years are mediated by these specific cognitive (parenting confidence) and affective/behavioral (enjoyment, warmth, and conflictual father-child relationship) dimensions of paternal involvement during the first 4 years of the child's life (Figure 2 represents our mediation model). Quantifying the magnitudes of these associations is critical for the design and implementation of targeted preventative and intervention programs aimed at improving outcomes of those children whose fathers experience PND. The clinical importance of such interventions has been highlighted by meta-analyses pointing to the modifiable nature of parenting (35), including in the context of parental depression (36). The study sample comprised participants from a large UK population-based birth-cohort study, the Avon Longitudinal Study of Parents and Children (ALSPAC). The ALSPAC cohort is a unique and rich source of longitudinal data, which enabled us to conduct confirmatory analyses to (1) model several dimensions of paternal involvement during early childhood (birth-4 years) and child development in middle childhood; (2) estimate longitudinal associations between paternal PND, paternal involvement, and child development; and (3) account for a range of socioeconomic, familial, parental, and child characteristics, including maternal PND during early postnatal period.
Methods
Study cohort
During Phase I enrolment, 14,541 pregnant women with expected dates of delivery between 1 April 1991 and 31 December 1992 were recruited into the ALSPAC cohort (Generation 0; G0). From the age of 7 years, children from eligible pregnancies, who were not originally enrolled, were encouraged to join the study (37). The total sample size for analyses in the ALSPAC cohort is therefore 15,447 pregnancies, of which 14,901 were alive at 1 year of age. G0 partners were invited by the mothers to complete questionnaires at the start of the study, but they were not formally enrolled in the study during Phase I enrolment. Data were collected from 12,113 partners (baseline number of partners who have had contact with the study), with 3,807 G0 partners currently enrolled in the study [37; ethnicity: White (97%); M age: 31 years old]. The present study sample comprised 4,898 participants with complete data on exposure, outcome, confounders, and at least one parenting item (indicators of paternal involvement) and 9,628 participants with imputed data on exposure, outcomes, and confounders (Figure 1). Demographic characteristics of the study sample are presented in the Results. Information about ALSPAC is available at https://www.bristol.ac.uk/alspac/, including a fully searchable data dictionary and variable search tool (http://www.bris.ac.uk/alspac/researchers/our-data/). Further details on the cohort profile, including G0 partners, representativeness, and phases of recruitment are described in several cohort-profile papers (37–39). Ethical approval and informed consent for the data collection were obtained from the ALSPAC Ethics and Law Committee and the Local Research Ethics Committees (http://www.bristol.ac.uk/alspac/researchers/research-ethics/). Informed consent for the use of data collected via questionnaires and clinics was obtained from participants following the recommendations of the ALSPAC Ethics and Law Committee at the time.
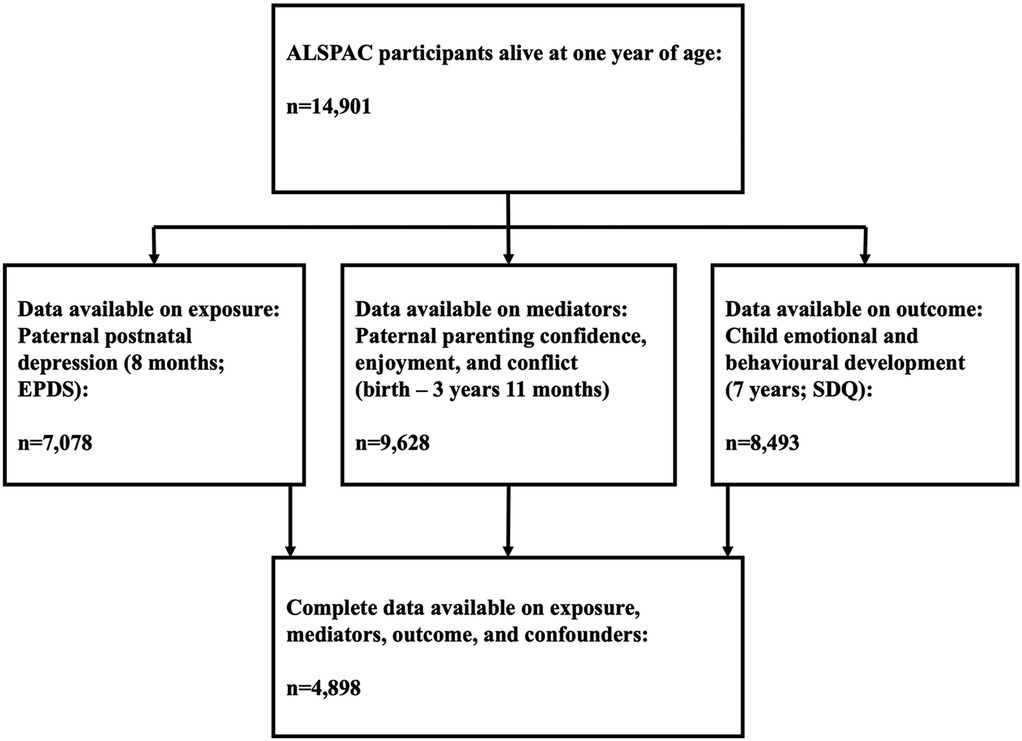
Figure 1. Flow chart depicting study derivation.
Measures
Exposure: paternal postnatal depression (PND)
Paternal depressive symptoms were measured at 8 months postnatally using the Edinburgh Postnatal Depression Scale (EPDS; 40), a 10-item self-reported questionnaire, validated and used extensively to screen for depression in men and women during the perinatal period (41). We used Confirmatory Factor Analysis (CFA) to derive a normally distributed latent trait based on the 10-EPDS ordinal response items. Similar to previous research, we dichotomized paternal depressive symptoms, derived as a continuous score, at a threshold of ≥12 (15) to examine descriptive characteristics of the study sample. Full details about the assessment of paternal depressive symptoms using the EPDS in the ALSPAC cohort, including stability across assessment points and predictive validity, are reported in Paul and Pearson (42). Throughout this manuscript, we refer to PND not as a clinical diagnosis of depression, but paternal and maternal postnatal depressive symptoms.
Outcomes: child emotional symptoms, conduct problems, hyperactivity, and peer problems
Child development was assessed using the Strengths and Difficulties Questionnaire (SDQ; 43) completed by mothers of study children at age 7 years. The SDQ consists of 25 questions with five subscales, extensively validated to demonstrate high consistency, reliability, and diagnostic predictability among children aged 4 to 16 years (44, 45), as well as good agreement with the Child Behavioral Checklist (46). We focused on four subscales capturing emotional symptoms (5 items), conduct problems (5 items), hyperactivity (5 items), and peer problems (5 items) to derive normally distributed latent traits based on 20-SDQ ordinal response items using the CFA from those subscales. We derived sum scores of the 4 subscales to examine descriptive characteristics of the study sample.
Mediators: paternal parenting confidence, enjoyment and warmth, and conflictual relationship with child
Potential parenting items were extracted from paternal self-report questionnaires completed by fathers on five occasions after the birth of the study child (8 weeks and 8 months postnatally, 1 year 9 months, 2 years 9 months, 3 years 11 months). We specifically focused on parenting items collected during the first 4 years of the child's life to capture possible early mechanisms of familial transmission of adverse developmental outcomes through paternal involvement and the quality of the father-child relationship. We drew on extensive empirical and sociological literature on paternal involvement in infancy (21, 24, 27, 28, 47, 48) to conceptualize the derivation of factors, including those capturing cognitive and affective/behavioral dimensions of paternal involvement directed at the child (i.e., child-focused; 18). In the first instance, extracted items were double-rated and independently assigned to theoretical dimensions by three researchers, followed by extensive discussions in a larger research group, including considerable input from experts in early child development and parenting (AS and MB). In the present analyses, we focused on three specific dimensions of paternal involvement as strong risk factors for adverse child development: paternal parenting confidence, enjoyment and warmth, and conflictual relationship with child. Derived factors, individual parenting items, age at assessment, and standardized factor loadings are presented in Supplementary Table S1.
Baseline confounders: socioeconomic, familial, parental, and child characteristics
We accounted for a range of possible baseline antenatal confounders including socioeconomic, familial, parental, and child characteristics in the regression models to estimate each of the exposure-outcome, exposure-mediators, and mediator-outcome pathways (Figure 2). We adjusted our analyses for child sex to account for the importance of child characteristics in child development (15) and paternal involvement (49). Paternal age, education, disadvantaged socioeconomic background, marital status, and conflict are associated with parental PND (50), less optimal parenting practices (51), and higher risk of adverse child emotions and behaviors (52). Thus, our analyses were adjusted for a range of prospectively measured potential confounding factors extracted from self-reported paternal antenatal questionnaires, including marital status (married, never married); a continuous score capturing parental conflict (higher scores representing higher levels of conflict); paternal age in years; the highest paternal educational attainment (minimal education or none/compulsory secondary level [up to age 16 years; O-Level], non-compulsory secondary level [up to age 18 years; A-Level/university level education); paternal social class (non-manual, manual); presence of financial difficulties (no financial difficulties); and type of main dwelling/accommodation (owned/mortgaged, private/council rented).

Figure 2. Structural equation mediation model estimating the direct effect of paternal postnatal depression (8 months) on child emotional and behavioral development (7 years), and the indirect (mediated) effects through paternal parenting confidence, enjoyment and warmth and conflictual relationship with child, adjusted for child sex, antenatal baseline confounders, and maternal PND. Note. Ovals represent latent variables. Individual items loading onto each specific factor comprising paternal involvement, error term covariances, and correlations between the factors are not shown to reduce figure complexity.
Existing epidemiological evidence supports associations between maternal and paternal PND (53, 54), with a substantial body of evidence documenting the adverse effect of maternal PND on child development (55). Thus, our analyses also adjusted for maternal PND measured at 8 weeks postnatally using the EPDS. To make full use of variation in maternal symptoms, individual depression items were summed to derive a continuous score (range 0–30).
Statistical analyses
Latent factor models
Individual paternal parenting items that were theoretically relevant and had standardized loadings >0.15 were assigned to the hypothesized parenting dimensions (parenting confidence, enjoyment and warmth, conflictual father-child relationship) and modeled using CFA. We used a robust Weighted Least Square (WLSMV) estimator in Mplus as recommended to model both categorical and continuous data (56). The CFA was also used to derive latent traits capturing paternal PND and child development (emotional symptoms, conduct problems, hyperactivity, and peer problems; full details in Supplementary Methods S1). The latent trait approach accounts for measurement error by only modeling shared variance across the items and separating shared from specific variance (57), while also maximizing power by modelling variables as continuous traits (58). The chi-square test of overall fit is prone to model misspecification when the sample size is large (59); thus, we gave preference to relative fit indices, the Root Mean Square Error of Approximation (RMSEA; <0.06), and Comparative Fit Index and Tucker–Lewis Index (CFI/TLI; >0.95), to evaluate the fit of the models (60). The CFA models capturing paternal parenting dimensions, paternal PND, and child development showed an adequate model fit supporting further tests of structural paths (estimates are fully described in Supplementary Methods S1).
Total, direct, and indirect effects
First, we examined descriptive characteristics of the study sample, including distribution of sociodemographic characteristics by the completeness of data. Second, we examined associations between paternal PND and child emotional symptoms, conduct problems, hyperactivity, and peer problems (total effects). Finally, we examined the extent to which the associations between paternal PND and child emotional and behavioral development are mediated (direct and indirect effects) by three dimensions of paternal involvement. We approached adjustment for confounding variables in steps. First, we estimated the unadjusted models comprising exposure, outcome, and mediators only. Second, we estimated models adjusted for baseline confounders pertaining to socioeconomic, familial, parental characteristics, and child sex (Adjusted1). Last, we adjusted analyses for maternal PND, as one of the potentially strongest confounders, to discern its effects on the model estimates (Adjusted2). Indirect effects [95% CIs] were calculated using the product-of-coefficients method and bias-corrected (BC) bootstrapping (n = 1,000 replications) to account for the non-normal distribution of the outcomes (61). Results from path analyses with continuous scores (latent traits capturing child emotional symptoms, conduct problems, hyperactivity, and peer problems), including indirect effects, are presented as standardized regression coefficients (β). We used MODEL INDIRECT (complete case analyses; n = 4,898) and MODEL CONSTRAINT (imputed analyses; n = 9,628) commands to estimate total, direct, total, and specific indirect effects with a WLSMV estimator to model continuous (exposure, mediators, and outcomes) and categorical (individual categorical items comprising latent factors) variables. All analyses were conducted using Structural Equation Modelling (SEM) in Mplus v.8.3 (62).
Missing data: multiple imputation
Similar to other population-based birth cohorts, ALSPAC is characterized by loss of data due to loss to follow-up. To examine the impact of missing data on our findings, we conducted sensitivity analyses using Multivariate Imputation by Chained Equations (MICE; 63). Imputation methods are fully described in Supplementary Methods S1. Due to relatively high rates of attrition and potential bias associated with including only complete cases in the analysis, as well as loss of precision and power (64), we report models based on the analysis with imputed data, with results of the complete case analysis fully presented in Supplementary Results S1 Tables S3–S6.
Results
Study sample characteristics
Never married fathers, those with higher levels of inter-parental conflict and financial difficulties, and those residing in rented accommodation were more likely to experience PND (Table 1). Fathers whose female partners reported higher levels of PND also reported higher PND mean scores. Children of those fathers who reported experiencing higher levels of PND had higher mean emotional symptoms, conduct problems, hyperactivity, and peer problems scores. Distribution of sociodemographic characteristics in the original ALSPAC cohort and the study complete and imputed samples are presented in Table 2. Participants comprising the complete sample were from a higher socioeconomic background, as indexed by a lower proportion of those reporting manual social class and financial difficulties and a higher proportion of those reporting residing in semi-detached/terraced accommodation and married marital status, compared to the original ALSPAC and imputed samples.
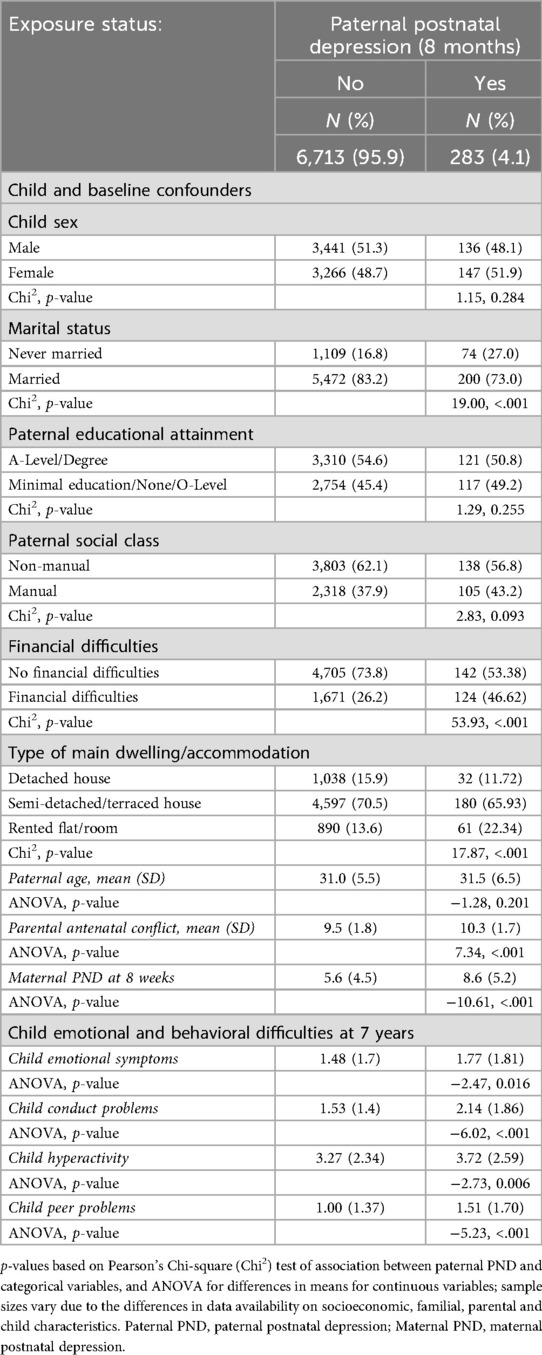
Table 1. Characteristics of the sample and child emotional and behavioral development (mean scores for emotional symptoms, conduct problems, hyperactivity, and peer problems at 7 years) by the exposure status (paternal PND at 8 months; threshold ≥12).

Table 2. Distribution of sociodemographic characteristics in the original avon longitudinal study of parents and children (ALSPAC) cohort and the study complete and imputed samples.
Paternal involvement factors: paternal parenting confidence, enjoyment and warmth, and conflictual relationship with child
Full details of the factors capturing paternal parenting confidence, enjoyment and warmth, and conflictual relationship with child are provided below. Associations between paternal involvement factors and aspects of child emotional and behavioral development are fully described in Supplementary Results S1 Table S2.
Paternal parenting confidence
11 items relating to paternal feelings of confidence in the parenting role and perceptions of the ability to engage effectively in parenting behaviors (e.g., “partner feels confident with child”, “partner unsure if doing the right thing”, “partner happy with the way he brings up child”) were extracted from paternal self-reported questionnaires administered at 8 weeks, 8 months, 1 year 9 months and 2 years 9 months. Higher factor scores represented higher levels of paternal parenting confidence.
Paternal enjoyment and warmth
27 items relating to feelings of enjoyment, affection, love and warmth toward the child (e.g., “partner enjoys child”, “partner feels very close to child”, “child gives great joy”) were extracted from paternal self-reported questionnaires administered at 8 weeks, 8 months, 1 year 9 months, 2 years 9 months and 3 years 11 months. Higher factor scores represented more paternal enjoyment, affection and warmth toward the child.
Paternal conflictual relationship with child
19 items relating to conflict, harsh disciplining and irritation with the child (e.g., “child gets on partner's nerves”, “partner dislikes mess surrounding child”, “smacking is the best way to discipline child”) were extracted from paternal self-reported questionnaires administered at 8 weeks, 8 months, 1 year 9 months and 2 years 9 months. Higher factor scores signified lower levels of conflictual parent-child relationship, irritation with the child and less harshness in paternal disciplining.
Total effects: associations between paternal PND and child development
First, we estimated the associations between paternal PND and child emotional symptoms, conduct problems, hyperactivity, and peer problems (total effects) in the unadjusted models, models adjusted for antenatal baseline socioeconomic, familial, paternal characteristics, and child sex (Adjusted1), and models further adjusted for maternal PND (Adjusted2). Paternal PND was associated with higher levels of child emotional symptoms, conduct problems, hyperactivity, and peer problems in the unadjusted and Adjusted1 models (Table 3). These associations were attenuated in Adjusted2 models (emotional symptoms: β = 0.060, 95% CI: [0.019, 0.101], p = 0.004; hyperactivity: β = 0.034, 95% CI: [−0.003, 0.071], p = 0.083; peer problems: β = 0.080, 95% CI: [0.039, 0.121], p ≤ 0.001). The attenuation effect of adjustment for maternal PND was particularly evident for child conduct problems [β = 0.032, 95% CI: (−0.009, 0.073), p = 0.135], with the evidence of total effect nearing zero. Thus, we limited examination of direct and mediated effects in mediation models to child emotional symptoms, hyperactivity, and peer problems as outcomes.

Table 3. Total associations between paternal PND and child emotional symptoms, conduct problems, hyperactivity, and peer problems in imputed sample.
Direct and indirect effects: associations between paternal PND, paternal involvement, and child development
Associations between paternal PND (exposure) and paternal parenting confidence, enjoyment and warmth, and conflictual relationship with child (mediators)
Paternal PND was strongly associated with less paternal enjoyment and warmth, more father-child conflict, and less paternal parenting confidence in the unadjusted, Adjusted1, and Adjusted2 models (paternal enjoyment and warmth: β = −0.336, 95% CI: [−0.369, −0.303], p ≤ 0.001; father-child conflict: β = −0.407, 95% CI: [−0.436, −0.378], p ≤ 0.001; paternal parenting confidence: β = −0.424, 95% CI: [−0.459, −0.389], p ≤ 0.001; see Table 4 for full results).

Table 4. Associations between paternal PND and paternal parenting confidence, enjoyment and warmth, and conflictual relationship with child in imputed sample.
Associations between paternal parenting confidence, enjoyment and warmth, conflictual relationship with child (mediators) and child emotional symptoms, hyperactivity, and peer problems (outcomes)
Higher levels of paternal parenting confidence and lower levels of father-child conflict were associated with lower levels of child emotional symptoms and hyperactivity in the unadjusted, Adjusted1, and Adjusted2 models (paternal parenting confidence to child emotional symptoms: β = −0.154, 95% CI: [−0.240, −0.068], p ≤ 0.001; paternal parenting confidence to child hyperactivity: β = −0.085, 95% CI: [−0.151, −0.018], p = 0.013; father-child conflict to child emotional symptoms: β = −0.103, 95% CI: [−0.170, −0.036], p = 0.002; father-child conflict to child hyperactivity: β = −0.125, 95% CI: [−0.183, −0.066], p ≤ 0.001; see Table 5 for full results). Higher levels of paternal parenting confidence were associated with lower risk of child peer problems in the unadjusted, Adjusted1, and Adjusted2 models, albeit with wide 95% CIs [β = −0.099, 95% CI: (−0.195, −0.003), p = 0.043]. There was no evidence for the association between father-child conflict and child peer problems in the unadjusted, Adjusted1, and Adjusted2 models.
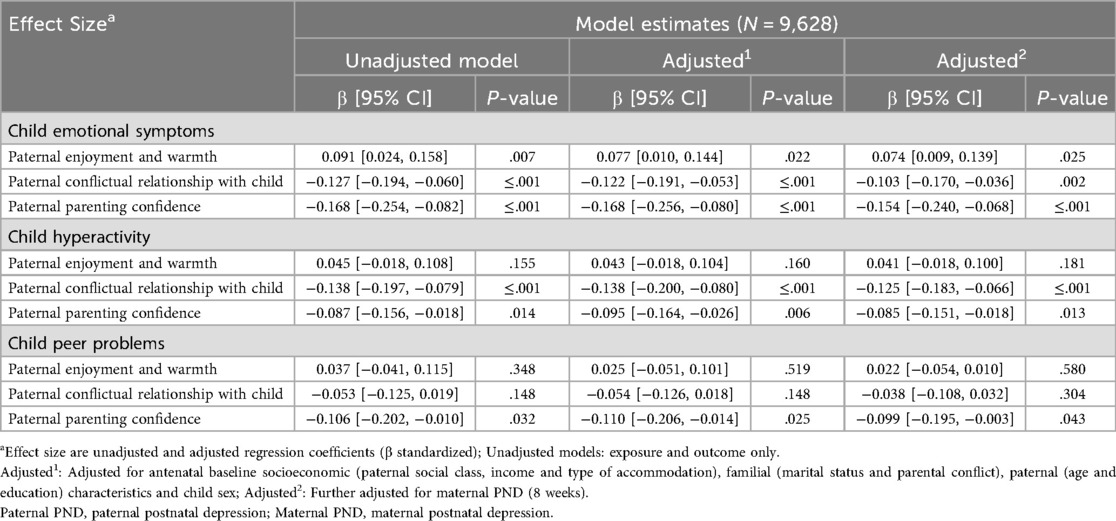
Table 5. Associations between paternal parenting confidence, enjoyment and warmth, and conflictual relationship with child and child emotional symptoms, hyperactivity, and peer problems in imputed sample.
No evidence for associations between paternal enjoyment and warmth and child hyperactivity and peer problems emerged in the unadjusted, Adjusted1, and Adjusted2 models. There was evidence of positive association between paternal enjoyment and warmth and child emotional symptoms [Adjusted2: β = 0.074, 95% CI: (0.009, 0.139), p = 0.025; Table 5], suggesting that higher levels of paternal enjoyment and warmth are associated with higher levels of adverse child emotional development. We conducted additional sensitivity analyses to examine the nature of the associations between dimensions of paternal involvement and child emotional symptoms, hyperactivity, and peer problems independent of adjustment for other paternal involvement factors in the unadjusted, Adjusted1, and Adjusted2 models (imputed analyses). The sensitivity analyses revealed that, once mutual adjustment for each of the parenting confounders was accounted for, the strength of the association between paternal enjoyment and warmth and child emotional symptoms was considerably weakened [Adjusted2: β = −0.046, 95% CI: (−0.010, 0.005), p = 0.076; Supplementary Table S7] and reversed (i.e., higher levels of paternal enjoyment and warmth associated with lower levels of adverse offspring emotional and behavioral development).
Direct and indirect effects
Strong evidence emerged for total indirect effects from paternal PND at 8 months to child emotional symptoms, hyperactivity, and peer problems at age 7 years through the combination of all dimensions of paternal involvement in the unadjusted, Adjusted1, and Adjusted2 models (emotional symptoms: β = 0.083, 95% CI:[ 0.059, 0.106], p ≤ 0.001; hyperactivity: β = 0.073, 95% CI: [0.051, 0.095], p ≤ 0.001; peer problems: β = 0.050, 95% CI: [0.023, 0.077], p ≤ 0.001; see Table 6 for full results). There was no evidence of direct effects from paternal PND to child emotional symptoms, hyperactivity, and peer problems once the indirect effects via all dimensions of paternal involvement were accounted for.
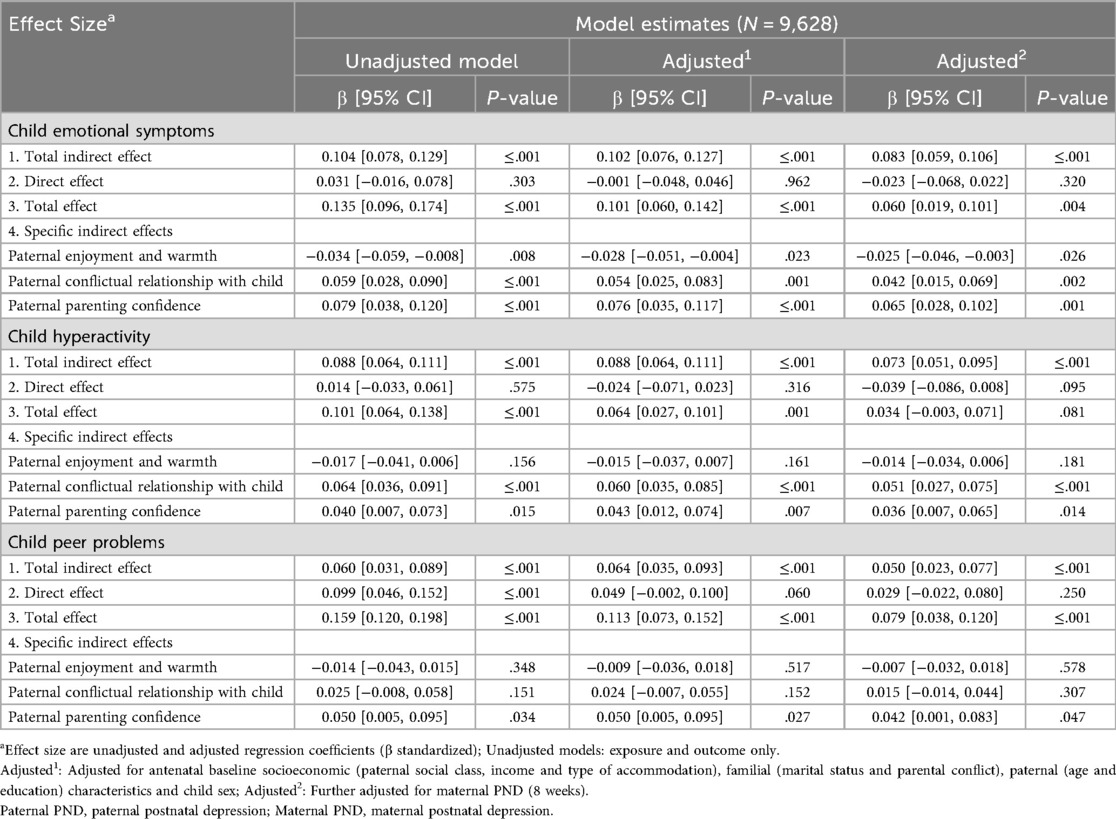
Table 6. Estimates of direct and indirect effects in imputed sample.
Evidence for specificity of indirect effects emerged depending on the child outcome. Specifically, paternal enjoyment and warmth, father-child conflict, and paternal parenting confidence mediated the association between paternal PND and child emotional symptoms in the unadjusted, Adjusted1, and Adjusted2 models (paternal enjoyment and warmth: β = −0.025, 95% CI: [−0.046, −0.003], p = 0.026; father-child conflict: β = 0.042, 95% CI: [0.015, 0.069], p = 0.002; paternal parenting confidence: β = 0.065, 95% CI: [0.028, 0.102], p = 0.001). There was evidence that father-child conflict and paternal parenting confidence mediated the association between paternal PND and child hyperactivity in the unadjusted, Adjusted1, and Adjusted2 models (father-child conflict: β = 0.051, 95% CI: [0.027, 0.075], p ≤ 0.001; paternal parenting confidence: β = 0.036, 95% CI: [0.007, 0.065], p = 0.014). There was some evidence that paternal parenting confidence mediated the association between paternal PND and child peer problems in the unadjusted, Adjusted1, and Adjusted2 models; however, the 95% CIs were wide [β = 0.042, 95% CI: (0.001, 0.083), p = 0.047]. There was no evidence for specific indirect effects through paternal enjoyment and warmth in the association between paternal PND and child hyperactivity and peer problems in unadjusted, Adjusted1, and Adjusted2 models. When the analyses were repeated using the sample with complete data, estimates of the total, direct, and indirect effects were in the same direction as they had been in the imputed data analyses, leading to the same overarching conclusions. The substantially reduced sample size, however, led to insufficient statistical power to detect some of the total and specific indirect effects in complete case analyses (estimates are fully described in Supplementary Results S1 and Tables S3–S6).
Discussion
Main findings
In this large population-based birth cohort, we used longitudinal data to estimate the extents to which associations between paternal PND at 8 months and child emotional symptoms, conduct problems, hyperactivity, and peer problems at 7 years are mediated by paternal parenting confidence, enjoyment and warmth, and conflictual father-child relationship in early childhood.
There was evidence of total associations between paternal PND and higher levels of child emotional symptoms, conduct problems, hyperactivity and peer problems, which were substantially attenuated once all child, family, socioeconomic and parental characteristics were accounted for. Attenuation was particularly evident following adjustment for maternal PND, and for child conduct problems, with the total effect nearing zero. These findings are consistent with a meta-analysis reporting weak to moderate longitudinal associations between paternal PND and child emotional and behavioral outcomes (7), including increased levels of child peer problems (65).
Evidence regarding associations between paternal PND and child externalizing behaviors, including conduct problems, is mixed. Two recent meta-analyses found small but consistent associations between paternal PND and child externalizing behaviors (8, 66), while other studies find no such effects or show weak negative associations (67, 68). Maternal PND and parental conflict may be stronger predictors of child externalizing difficulties than paternal PND (67, 69), which is reflected in our findings indicating substantial attenuation between paternal PND and child behavioral problems and hyperactivity after accounting for these factors.
One of the strengths of our study is that we examine specificity, both in risks and offspring outcomes, when considering paternal involvement in the context of paternal PND (34). Consistent with existing research, paternal PND was strongly associated with less paternal parenting confidence, less paternal enjoyment and warmth, and more father-child conflict (16). We also observed differential patterns of associations between dimensions of paternal involvement and child emotional and behavioral development, with higher levels of paternal parenting confidence being associated with lower levels of child emotional symptoms, hyperactivity, and peer problems. These findings align with the meta-analysis of the Positive Parenting Programme (Triple P), suggesting that improving parenting efficacy and confidence is the key mechanism for preventing child emotional and behavioral problems (70). Family systems interventions also emphasize the importance of providing support at the family-level to enhance parental parenting competencies, which enable parent-child interactions conducive of more optimal child development (71). Family systems framework may be particularly important in the context of parental PND, given strong associations between maternal and paternal PND (53, 54) and the adverse impacts that depression exerts on both parents' parenting (14, 16).
Positive and less conflictual father-child relationships are protective factors for less adverse child development (72). By contrast, conflictual father-child relationships are a common vulnerability that increases the risk for multiple internalizing and externalizing child disorders (73). Consistently, our findings support lower levels of child emotional symptoms in the context of less conflictual father-child relationships, which were also independently associated with lower levels of child hyperactivity. We found no evidence for the associations between paternal enjoyment and warmth and child hyperactivity and peer problems. It may be that our self-report measure did not capture key aspects of paternal enjoyment, warmth, and sensitivity that are important for child emotional and behavioral development (74). Arguably, parental self-reports of warmth and sensitivity toward the child may be biased, particularly in the context of parental depression or misinterpretation of child behavior (75). Future research may benefit from examining nuanced variations in these complex parental behaviors and their impact on child development using direct observations of father-child interactions. Conceptually, the evidence regarding associations between parental sensitivity and child behavioral development remains inconsistent, with studies reporting associations of varying magnitude (76). Further research is also needed to determine how variations among children and their circumstances influence the strength of these associations, with important research and practice implications. Theoretically and empirically, there may also be distinct causal influences of paternal warmth and enjoyment, as a proxy measure of paternal sensitivity, on emotional and behavioral dimensions of child development (77, 78), warranting investigation beyond the scope of this study.
Direct and indirect effects
Associations between paternal PND and child emotional symptoms, hyperactivity, and peer problems at age 7 years were explained by the combination of all dimensions of paternal involvement, including enjoyment and warmth, parenting confidence, and conflictual relationship with child. A previous ALSPAC-based study found that a relatively small proportion of the association between paternal PND and child emotional and behavioral development at ages 4 and 7 years was mediated by paternal non-involvement (analyzed as a sum-score), with maternal depression and parental conflict contributing to the majority of the mediation effect (19). However, measures of paternal non-involvement and child outcomes were based on maternal reports potentially underestimating the strength of the indirect effect through paternal parenting.
We found evidence for specificity of indirect effects depending on child outcome, with less paternal parenting confidence and more conflictual father-child relationship mediating the association between paternal PND, child emotional symptoms, and hyperactivity. Lower levels of paternal parenting confidence also mediated the association between paternal PND and child peer problems, although 95% CIs for the effect were wide. The likely negative impact of paternal PND on fathers' perceptions of their own competence in the parenting role may undermine their ability to be responsive to their children (79), display affectionate and supportive behavior (80), engage in high-quality interactions (81), and effective emotion regulation (82), resulting in increased levels of child emotional symptoms, hyperactivity, and peer problems (30). Father-child conflict also mediates the association between paternal PND and child emotional and behavioral development, including emotion regulation problems (20, 83). These findings suggest that paternal parenting confidence and father-child conflict may be important prevention and intervention targets to reduce adverse emotional and behavioral outcomes in children of fathers experiencing PND (30, 84).
Our findings indicated that higher levels of paternal enjoyment and warmth were associated with higher levels of adverse child emotional development. In order to substantiate these findings, we conducted further sensitivity analyses to examine associations between dimensions of paternal involvement and child emotional symptoms, hyperactivity and peer problems independent of adjustment for other paternal involvement factors. In these analyses, there was some evidence that higher levels of paternal enjoyment and warmth were associated with lower levels of adverse child development, albeit with wide 95% CIs in the fully adjusted models, suggesting that mutual adjustment for each of the parenting factors in the main mediation model may have weakened, and potentially reversed, these associations further. Therefore, the findings regarding inconsistent direction of associations between paternal enjoyment and warmth and child emotional development warrant a cautious interpretation as they may represent a potential statistical artifact resulting from the complexity of our multiple-mediator model.
Strengths and limitations
The current study has several strengths. First, ALSPAC is a unique intergenerational birth-cohort study with a large and overall representative sample of UK fathers (37). The availability of rich repeated self-reported measures of paternal parenting enabled us to model several cognitive and affective/behavioral dimensions of paternal involvement using the latent factor models across multiple time points in early childhood, capturing the longitudinal nature of paternal parenting. Nevertheless, cautious generalization of our findings to contemporary families is needed. The ALSPAC cohort, born between 1990 and 1991, reflects limited racial diversity and was largely composed of nuclear families. Parenting behaviors are known to vary across cultural contexts and may be perceived and enacted differently depending on cultural norms (85). Furthermore, family structures and gender dynamics in parenting have continued to evolve, suggesting that our findings may not fully capture the complexity of contemporary family life. Applying the latent factor approach also enabled us to model child development as four different dimensions (i.e., emotional symptoms, conduct problems, hyperactivity, and peer problems), rather than a sum score, to examine potential differential associations between paternal PND, paternal involvement, and child development in line with the specificity principle in developmental research (34).
Second, we examined possible roles of these dimensions in transmitting the risk of paternal PND on child emotional and behavioral development in mediation models adjusted for a range of socioeconomic, family, parental, and child characteristics, including parental conflict and maternal PND. There continues to be lack of studies that examine potential mediating roles of multiple dimensions of paternal involvement in the association between paternal PND and different aspects of child emotional and behavioral development (7, 19), with our study representing a potentially important corrective.
Third, although the exposure (paternal PND) and mediators (paternal involvement) were measured using paternal self-reports, the outcomes (child emotional and behavioral development) were reported by the mothers, strengthening study findings by reducing the risk of shared variance bias and inflated estimates of total associations.
Still, there are limitations to this study. We did not include additional assessments of maternal and paternal PND later in development due to moderate-to-high correlations between time-points (42) and increased risk of overadjustment bias (86). Previous ALSPAC studies (42) reported evidence of stability and predictive validity of paternal PND across assessments, indicating that fathers who experienced depression during pregnancy and the early postnatal period were also more likely to report depression at later assessments. Paternal depression at later time points is also more likely to be on a causal pathway, explaining rather than confounding, the association between paternal PND and child development (later paternal depression may be a consequence of lack of paternal involvement). However, epidemiological evidence indicates that paternal depression likely recurs across development (3, 6), thus, estimating associations between paternal depression at one time-point (8 months postnatally) and child emotional and behavioral development may represent a limitation of our conceptual approach.
Some paternal involvement items were measured concurrently with the assessment of paternal PND (8 months), providing an alternative explanation whereby lower paternal involvement is associated with higher risk of paternal PND. However, existing evidence strongly supports the adverse effect of paternal PND on paternal parenting and involvement (16), suggesting that these associations are unlikely to be in the opposite direction. Nevertheless, this possibility cannot be fully discarded and needs to be taken into account when interpreting our findings.
Even though our sample attrition is similar to that observed in other population-based studies (38, 39), it is a limitation with potential implications for internal validity. We addressed bias due to selective attrition (fathers from lower socioeconomic background and those experiencing depression were under-represented in complete case sample) by controlling for factors known to predict missingness and by imputing missing data in the exposure, outcomes and confounders. The conclusions from the imputed and complete data analyses were the same, with some evidence of stronger total and specific indirect effects in imputed analyses, suggesting that attrition may have contributed to the under- not over-estimation of effects.
Another limitation is lack of independently assessed measures of paternal involvement, which may potentially lead to overestimation of the indirect effects due to shared-method bias (e.g., fathers' depressive symptoms may negatively bias self-reports of parenting behaviors; 16). Although social desirability bias (87) may affect both self-reported and independently observed measures of parenting (88), it may be more pronounced in observational methods (16). We were unable to substantiate self-reported measures of paternal involvement with comparable domains of independently observed data as they were not collected in the ALSPAC cohort. Examination of genetic confounding that may explain associations between paternal PND and child emotional and behavioral development warrants further attention (89) but was beyond the scope of this study, while residual confounding also remains a possibility (90). Replication with a more ethnically and culturally diverse sample of fathers reflecting contemporary paternal parenting practices, as well as examination of child and parent sex effects on parental PND and parenting is also warranted.
Implications for practice
Our findings contribute to a growing body of epidemiological evidence indicating that paternal PND is a risk factor for adverse child emotional and behavioral development (7), with lower levels of paternal parenting confidence and higher levels of father-child conflict playing important roles in explaining these negative effects. Our study highlights the importance of previously articulated implications, including the needs to (1) recognize (extending screening for depression to both mothers and fathers) and treat depression in both parents when one parent experiences depression (91); (2) design intervention and prevention programs that improve both parents' relationships with the child to facilitate healthy child development (14); and (3) incorporate assessment of the family environment and functioning (e.g., parental conflict) into prevention and intervention programs to strengthen family relationships within the family unit in contradiction to the current focus on one parent (92). However, in practice, a qualitative meta-synthesis of the experiences of fathers suggests that they continue to be marginalized and neglected in the context of perinatal services delivery (93), while existing parenting programs fail to successfully engage fathers (94) even though there is evidence that paternal parenting may be positively influenced by interventions (95), including enhancing paternal sensitive parenting through prenatal video-feedback (96). Our findings may contribute to an increasing shift in thinking about addressing intergenerational transmission of emotional and behavioral risks in families through focusing on both parents' mental health, parenting, and contributions to the family environment.
Data availability statement
ALSPAC data are available through a system of managed open access. The study website contains details of all the data that is available through a fully searchable data dictionary and variable search tool data dictionary. The application steps for ALSPAC data access are highlighted below. 1. Please read the ALSPAC access policy, which describes the process of accessing the data in detail, and outlines the costs associated with doing so. 2. You may also find it useful to browse the fully searchable research proposals database, which lists all research projects that have been approved since April 2011. 3. Please submit your research proposal for consideration by the ALSPAC Executive Committee. You will receive a response within 10 working days to advise you whether your proposal has been approved. If you have any questions about accessing data, please emailYWxzcGFjLWRhdGFAYnJpc3RvbC5hYy51aw==. Requests to access the datasets should be directed toYWxzcGFjLWRhdGFAYnJpc3RvbC5hYy51aw==.
Ethics statement
Ethical approval and informed consent for the data collection were obtained from the ALSPAC Ethics and Law Committee and the Local Research Ethics Committees (http://www.bristol.ac.uk/alspac/researchers/research-ethics/). Informed consent for the use of data collected via questionnaires and clinics was obtained from participants following the recommendations of the ALSPAC Ethics and Law Committee at the time.
Author contributions
IC: Methodology, Writing – original draft, Funding acquisition, Investigation, Visualization, Formal analysis, Conceptualization, Data curation, Project administration, Supervision, Writing – review & editing. RP: Writing – review & editing, Methodology, Investigation. NW: Methodology, Writing – review & editing. AS: Writing – review & editing, Conceptualization. MB: Conceptualization, Writing – review & editing. HT: Methodology, Writing – review & editing. EF: Conceptualization, Writing – review & editing. JE: Conceptualization, Writing – review & editing. TM: Writing – review & editing, Conceptualization. ED: Writing – review & editing, Conceptualization. JH: Methodology, Writing – review & editing. HS: Methodology, Writing – review & editing. GH: Methodology, Conceptualization, Investigation, Formal analysis, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The UK Medical Research Council and Wellcome (217065/Z/19/Z) and the University of Bristol provide core support for ALSPAC. A comprehensive list of grants funding is available on the ALSPAC website (http://www.bristol.ac.uk/alspac/external/documents/grant-acknowledgements.pdf). This publication is the work of the authors and Dr Culpin will serve as guarantor for the contents of this paper. This research was funded in whole by the Wellcome Trust Research Fellowship in Humanities and Social Science (212664/Z/18/Z) awarded to Dr Culpin. For the purpose of Open Access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission. Dr Hammerton was supported by the Sir Henry Wellcome Postdoctoral Fellowship (209138/Z/17/Z). Dr Bornstein was funded by the Intramural Research Program of the NIH/NICHD, USA, and an International Research Fellowship at the Institute for Fiscal Studies, London, UK, funded by the European Research Council under the Horizon 2020 research and innovation programme (695300-HKADeC-ERC-2015-AdG). Professor Stein was supported by the NIHR Oxford Health Biomedical Research Centre. Dr Sallis is a member of the MRC Integrative Epidemiology Unit at the University of Bristol (MC_UU_00011/7), which is supported by the UK Medical Research Council Unit (MC_UU_12013/3 and MC_UU_12013/4). Dr Pearson was supported by the European Research Commission Grant (758813 MHINT). This study was also supported by the NIHR Biomedical Research Centre at the University Hospitals Bristol NHS Foundation Trust and the University of Bristol. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research.
Acknowledgments
We are extremely grateful to all the families who took part in this study, the midwives for their help in recruiting them, and the whole ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists and nurses. A preprint version of this article was published on PsyArXiv Preprints (97).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frcha.2025.1650799/full#supplementary-material
References
1. Gedzyk-Nieman SA. Postpartum and paternal postnatal depression: identification, risks, and resources. Nurs Clin. (2021) 56(3):325–43. doi: 10.1016/j.cnur.2021.04.001
2. Rao WW, Zhu XM, Zong QQ, Zhang Q, Hall BJ, Ungvari GS, et al. Prevalence of prenatal and postpartum depression in fathers: a comprehensive meta-analysis of observational surveys. J Affect Disord. (2020) 263:491–9. doi: 10.1016/j.jad.2019.10.030
3. Cameron EE, Sedov ID, Tomfohr-Madsen LM. Prevalence of paternal depression in pregnancy and the postpartum: an updated meta-analysis. J Affect Disord. (2016) 206:189–203. doi: 10.1016/j.jad.2016.07.044
4. Paulson JF, Bazemore SD. Prenatal and postpartum depression in fathers and its association with maternal depression: a meta-analysis. JAMA. (2010) 303(19):1961–9. doi: 10.1001/jama.2010.605
5. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. (2005) 62(6):593–602. doi: 10.1001/archpsyc.62.6.593
6. Goodman JH. Paternal postpartum depression, its relationship to maternal postpartum depression, and implications for family health. J Adv Nurs. (2004) 45(1):26–35. doi: 10.1046/j.1365-2648.2003.02857.x
7. Sweeney S, MacBeth A. The effects of paternal depression on child and adolescent outcomes: a systematic review. J Affect Disord. (2016) 205:44–59. doi: 10.1016/j.jad.2016.05.073
8. Cheung K, Theule J. Paternal depression and child externalizing behaviors: a meta-analysis. J Fam Psychol. (2019) 33(1):98–108. doi: 10.1037/fam0000473
9. Weitzman M, Rosenthal DG, Liu YH. Paternal depressive symptoms and child behavioral or emotional problems in the United States. Pediatrics. (2011) 128(6):1126–34. doi: 10.1542/peds.2010-3034
10. Parke RD, McDowell DJ, Kim M, Killian C, Dennis J, Flyr ML, et al. Fathers’ contributions to children’s peer relationships. In: Tamis-LeMonda CS, Cabrera N, editors. Handbook of Father Involvement: Multidisciplinary Perspectives. Mahwah, NJ: Erlbaum (2012). p. 156–82.
11. Chen LC, Chen MH, Hsu JW, Huang KL, Bai YM, Chen TJ, et al. Association of parental depression with offspring attention deficit hyperactivity disorder and autism spectrum disorder: a nationwide birth cohort study. J Affect Disord. (2020) 277:109–14. doi: 10.1016/j.jad.2020.07.059
12. Sullivan PF, Neale MC, Kendler KS. Genetic epidemiology of major depression: review and meta-analysis. Am J Psychiatry. (2000) 157(10):1552–62. doi: 10.1176/appi.ajp.157.10.1552
13. Howard DM, Adams MJ, Clarke TK, Hafferty JD, Gibson J, Shirali M, et al. Genome-wide meta-analysis of depression identifies 102 independent variants and highlights the importance of the prefrontal brain regions. Nat Neurosci. (2019) 22(3):343–52. doi: 10.1038/s41593-018-0326-7
14. Goodman SH, Rouse MH, Connell AM, Broth MR, Hall CM, Heyward D. Maternal depression and child psychopathology: a meta-analytic review. Clin Child Fam Psychol Rev. (2011) 14:1–27. doi: 10.1007/s10567-010-0080-1
15. Ramchandani P, Psychogiou L. Paternal psychiatric disorders and children’s psychosocial development. Lancet. (2009) 374(9690):646–53. doi: 10.1016/S0140-6736(09)60238-5
16. Wilson S, Durbin CE. Effects of paternal depression on fathers’ parenting behaviors: a meta-analytic review. Clin Psychol Rev. (2010) 30(2):167–80. doi: 10.1016/j.cpr.2009.10.007
17. Gulenc A, Butler E, Sarkadi A, Hiscock H. Paternal psychological distress, parenting, and child behavior: a population based, cross-sectional study. Child Care Health Dev. (2018) 44(6):892–900. doi: 10.1111/cch.12607
18. Culpin I, Hammerton G, Stein A, Bornstein MH, Tiemeier H, Cadman T, et al. Maternal postnatal depressive symptoms and offspring emotional and behavioral development at age 7 years in a UK birth cohort: the role of paternal involvement. Dev Psychol. (2023) 59(4):770–85. doi: 10.1037/dev0001482
19. Gutierrez-Galve L, Stein A, Hanington L, Heron J, Ramchandani P. Paternal depression in the postnatal period and child development: mediators and moderators. Pediatrics. (2015) 135(2):e339–47. doi: 10.1001/jamapsychiatry.2018.3667
20. Nath S, Russell G, Kuyken W, Psychogiou L, Ford T. Does father–child conflict mediate the association between fathers’ postnatal depressive symptoms and children’s adjustment problems at 7 years old? Psychol Med. (2016) 46(8):1719–33. doi: 10.1017/S0033291716000234
22. Parke RD. Father involvement. Marriage Fam Rev. (2000) 29(2–3):43–58. doi: 10.1300/J002v29n02_04
23. Parke RD, Cookston JT. Fathers and family. In: Bornstein MH, editor. Handbook of Parenting. Vol.3. Being and Becoming a Parent. 3rd ed. New York: Routlege (2019). p. 64–136.
24. Schoppe-Sullivan S, McBride B, Ho MH. Unidimensional versus multidimensional perspectives on father involvement. Fathering A J Theory Res Pract Men Fathers. (2004) 2(2):147–63. doi: 10.3149/FTH.0202.147
25. Pleck JH. Paternal involvement: revised conceptualisation and theoretical linkages with child outcomes. In: Lamb M, editor. The Role of the Father in Child Development. Hoboken, NJ: Wiley (2010). p. 58–93.
26. Diniz E, Brandao T, Verissimo M. Father involvement during early childhood: a systematic review of qualitative studies. Fam Relat. (2023) 72(5):2710–30. doi: 10.1111/fare.12858
27. Marsiglio W, Day RD, Lamb ME. Exploring fatherhood diversity: implications for conceptualizing father involvement. Marriage Fam Rev. (2000) 29(4):269–93. doi: 10.1300/J002v29n04_03
28. Palkovitz R. Expanding our focus from father involvement to father–child relationship quality. J Fam Theory Rev. (2019) 11(4):576–91. doi: 10.1111/jftr.12352
29. Trahan MH. Paternal self-efficacy and father involvement: a bi-directional relationship. Psychol Men Masc. (2018) 19(4):624. doi: 10.1037/men0000130
30. Albanese AM, Russo GR, Geller PA. The role of parental self-efficacy in parent and child well-being: a systematic review of associated outcomes. Child Care Health Dev. (2019) 45(3):333–63. doi: 10.1111/cch.12661
31. Lamb ME. How do fathers influence children’s development? Let me count the ways. In: Lamb ME, editor. The Role of the Father in Child Development. Hoboken, NJ: Wiley (2010). p. 1–26.
32. Diniz E, Brandao T, Monteiro L, Verissimo M. Father involvement during early childhood: a systematic review of the literature. J Fam Theory Rev. (2021) 13(1):77–99. doi: 10.1111/jftr.12410
33. Paquette D. Theorizing the father-child relationship: mechanisms and developmental outcomes. Hum Dev. (2004) 47(4):193–219. doi: 10.1159/000078723
34. Bornstein MH. “It’s about time!” ecological systems, transaction, and specificity as key developmental principles in children’s changing worlds. In: Parke RD, Elder GH, editors. Children in Changing Worlds: Sociocultural and Temporal Perspectives. Padstow, Cornwall: Cambridge University Press (2019). p. 277–86. doi: 10.1017/9781108264846.010
35. Jeong J, Franchett EE, Ramos de Oliveira CV, Rehmani K, Yousafzai AK. Parenting interventions to promote early child development in the first three years of life: a global systematic review and meta-analysis. PLoS Med. (2021) 18(5):e1003602. doi: 10.1371/journal.pmed.1003602
36. Cuijpers P, Weitz E, Karyotaki E, Garber J, Andersson G. The effects of psychological treatment of maternal depression on children and parental functioning: a meta-analysis. Eur Child Adolesc Psychiatry. (2015) 24:237–45. doi: 10.1007/s00787-014-0660-6
37. Northstone K, Ben Shlomo Y, Teyhan A, et al. The avon longitudinal study of parents and children ALSPAC G0 partners: a cohort profile. Wellcome Open Res. (2023) 8:37. doi: 10.12688/wellcomeopenres.18782.1
38. Boyd A, Golding J, Macleod J, Lawlor DA, Fraser A, Henderson J, et al. Cohort profile: the ‘children of the 90s’: the index offspring of the avon longitudinal study of parents and children (ALSPAC). Int J Epidemiol. (2013) 42:111–27. doi: 10.1093/ije/dys064
39. Fraser A, Macdonald-Wallis C, Tilling K, Boyd A, Golding J, Davey Smith G, et al. Cohort profile: the avon longitudinal study of parents and children: ALSPAC mothers cohort. Int J Epidemiol. (2013) 42:97–110. doi: 10.1093/ije/dys066
40. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry. (1987) 150(6):782–6. doi: 10.1192/bjp.150.6.782
41. Shafian AK, Mohamed S, Raduan NJN, Ann AYH. A systematic review and meta-analysis of studies validating Edinburgh postnatal depression scale in fathers. Heliyon. (2022) 8:e09441. doi: 10.1016/j.heliyon.2022.e09441
42. Paul E, Pearson RM. Depressive symptoms measured using the Edinburgh postnatal depression scale in mothers and partners in the ALSPAC study: a data note. Wellcome Open Res. (2020) 5:108. doi: 10.12688/wellcomeopenres.15925.2
43. Goodman RS. Strengths and difficulties questionnaire: a research note. J Child Psychol Psychiatry. (1997) 38(5):581–6. doi: 10.1111/j.1469-7610.1997.tb01545.x
44. Goodman RS. Psychometric properties of the strengths and difficulties questionnaire. J Am Acad Child Adolesc Psychiatry. (2001) 40(11):1337–45. doi: 10.1097/00004583-200111000-00015
45. Vostanis P. Strengths and difficulties questionnaire: research and clinical applications. Curr Opin Psychiatry. (2006) 19(4):367–72. doi: 10.1097/01.yco.0000228755.72366.05
46. Stone LL, Otten R, Engels RCME, Vermulst AA, Janssens JMAM. Psychometric properties of the parent and teacher versions of the strengths and difficulties questionnaire for 4-to 12-year-olds: a review. Clin Child Fam Psychol Rev. (2010) 13(3):254–74. doi: 10.1007/s10567-010-0071-2
47. Lamb ME, Lewis C. The development and significance of father–child relationships in two-parent families. In: Lamb ME, editor. The Role of the Father in Child Development. 4th ed. Hoboken, NJ: Wile (2004). p. 272–306.
48. Pleck JH. Integrating father involvement in parenting research. Parenting. (2012) 12(2-3):243–53. doi: 10.1080/15295192.2012.683365
49. Cabrera NJ, Fitzgerald HE, Bradley RH, Roggman L. The ecology of father-child relationships: an expanded model. J Fam Theory Rev. (2014) 6(4):336–54. doi: 10.1111/jftr.12054
50. Wee KY, Skouteris H, Pier C, Richardson B, Milgrom J. Correlates of ante-and postnatal depression in fathers: a systematic review. J Affect Disord. (2011) 130(3):358–77. doi: 10.1016/j.jad.2010.06.019
51. Leigh B, Milgrom J. Risk factors for antenatal depression, postnatal depression and parenting stress. BMC Psychiatry. (2008) 8(1):24. doi: 10.1186/1471-244X-8-24
52. Stein A, Pearson RM, Goodman SH, Rapa E, Rahman A, McCallum M, et al. Effects of perinatal mental disorders on the fetus and child. Lancet. (2014) 384(9956):1800–19. doi: 10.1016/S0140-6736(14)61277-0
53. Fredriksen E, Von Soest T, Smith L, Moe V. Depressive symptom contagion in the transition to parenthood: interparental processes and the role of partner-related attachment. J Abnorm Psychol. (2019) 128(5):397–403. doi: 10.1037/abn0000429
54. Thiel F, Pittelkow MM, Wittchen HU, Garthus-Niegel S. The relationship between paternal and maternal depression during the perinatal period: a systematic review and meta-analysis. Front Psychiatry. (2020) 11:563287. doi: 10.3389/fpsyt.2020.563287
55. Dachew B, Ayano G, Duko B, Lawrence B, Betts K, Alati R. Paternal depression and risk of depression among offspring: a systematic review and meta-analysis. JAMA Network Open. (2023) 6(8):e2329159. doi: 10.1001/jamanetworkopen.2023.29159
56. Muthén BO, Asparouhov T. Item response modeling in mplus: a multi-dimensional, multi-level, and multi-timepoint example. In: van der Linden WJ, Hambleton RK, editors. Handbook of Item Response Theory: Models, Statistical Tools, and Applications. Chapman & Hall/CRC Press (2013). p. 1–29.
57. Grewal R, Cote JA, Baumgartner H. Multicollinearity and measurement error in structural equation models: implications for theory testing. Mark Sci. (2004) 23(4):519–29. doi: 10.1287/mksc.1040.0070
59. Schumacker RE, Lomax RG. A Beginner’s Guide to Structural Equation Modelling. Mahwah, NJ: Erlbaum (2004).
60. Hu LT, Bentler PM. Fit indices in covariance structure modelling: sensitivity to underparameterized model misspecification. Psychol Methods. (1998) 3(4):424–53. doi: 10.1037/1082-989X.3.4.424
61. MacKinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivariate Behav Res. (2004) 39(1):99–128. doi: 10.1207/s15327906mbr3901_4
63. Royston P, White IR. Multiple imputation by chained equations (MICE): implementation in Stata. J Stat Softw. (2011) 45(4):1–20. doi: 10.18637/jss.v045.i04
64. Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. Br Med J. (2009) 338:b2393. doi: 10.1136/bmj.b2393
65. Ramchandani PG, O’Connor TG, Evans J, Heron J, Murray L, Stein A. The effects of pre-and postnatal depression in fathers: a natural experiment comparing the effects of exposure to depression on offspring. J Child Psychol Psychiatry. (2008) 49(10):1069–78. doi: 10.1111/j.1469-7610.2008.02000.x
66. Ivanova MY, Achenbach TM, Turner LV. Associations of parental depression with Children’s internalizing and externalizing problems: meta-analyses of cross-sectional and longitudinal effects. J Clin Child Adolesc Psychol. (2022) 51(6):827–49. doi: 10.1080/15374416.2022.2127104
67. Gross HE, Shaw DS, Moilanen KL, Dishion TJ, Wilson MN. Reciprocal models of child behavior and depressive symptoms in mothers and fathers in a sample of children at risk for early conduct problems. J Fam Psychol. (2008) 22(5):742. doi: 10.1037/a0013514
68. Keller PS, Mark Cummings E, Peterson KM, Davies PT. Marital conflict in the context of parental depressive symptoms: implications for the development of children’s adjustment problems. Soc Dev. (2009) 18(3):536–55. doi: 10.1111/j.1467-9507.2008.00509.x
69. Hanington L, Heron J, Stein A, Ramchandani P. Parental depression and child outcomes–is marital conflict the missing link? Child Care Health Dev. (2012) 38(4):520–9. doi: 10.1111/j.1365-2214.2011.01270.x
70. Li N, Peng J, Li Y. Effects and moderators of Triple P on the social, emotional, and behavioral problems of children: systematic review and meta-analysis. Front Psychol. (2021) 12:709851. 10.338934512467
71. Trivette CM, Dunst CJ, Hamby DW. Influences of family-systems intervention practices on parent-child interactions and child development. Topics Early Child Spec Educ. (2010) 30(1):3–19. doi: 10.1177/0271121410364250
72. Foster D, Rodrigues M, Somir I, Aziz T, Patel R, Ragunathan S, et al. Paternal positivity and child mental health: a meta-analysis. J Child Fam Stud. (2022) 31(9):2556–70. doi: 10.1007/s10826-022-02361-7
73. Burt SA, Krueger RF, McGue M, Iacono W. Parent-child conflict and the comorbidity among childhood externalizing disorders. Arch Gen Psychiatry. (2003) 60(5):505–13. doi: 10.1001/archpsyc.60.5.505
74. Lucassen N, Tiemeier H, Luijk MP, Linting M, Bakermans-Kranenburg MJ, Van IJzendoorn MH, et al. Expressed emotion during pregnancy predicts observed sensitivity of mothers and fathers in early childhood. Parenting. (2015) 15(3):158–65. doi: 10.1080/15295192.2015.1053316
75. Najman JM, Williams GM, Nikles J, Spence S, Bor W, O'Callaghan M, et al. Bias influencing maternal reports of child behavior and emotional state. Soc Psychiatry Psychiatr Epidemiol. (2001) 36:186–94. doi: 10.1007/s001270170062
76. Cooke JE, Deneault AA, Devereux C, Eirich R, Fearon RP, Madigan S. Parental sensitivity and child behavioral problems: a meta-analytic review. Child Dev. (2022) 93(5):1231–48. doi: 10.1111/cdev.13764
77. Cosgrove VE, Rhee SH, Gelhorn HL, Boeldt D, Corley RC, Ehringer MA, et al. Structure and etiology of co-occurring internalizing and externalizing disorders in adolescents. J Abnorm Child Psychol. (2011) 39(1):109–23. doi: 10.1007/s10802-010-9444-8
78. Lahey BB, Krueger RF, Rathouz PJ, Waldman ID, Zald DH. A hierarchical causal taxonomy of psychopathology across the life span. Psychol Bull. (2017) 143(2):142–86.28004947
79. Shim SY, Lim SA. Paternal self-efficacy, fathering, and children’s behavioral problems in Korea. J Child Fam Stud. (2019) 28:851–9. doi: 10.1007/s10826-018-01310-7
80. Murdock KW. An examination of parental self-efficacy among mothers and fathers. Psychol Men Masc. (2013) 14(3):314. doi: 10.1037/a0027009
81. Brown GL, Mangelsdorf SC, Neff C. Father involvement, paternal sensitivity, and father−child attachment security in the first 3 years. J Fam Psychol. (2012) 26(3):421–30. doi: 10.1037/a0027836
82. Hajal NJ, Paley B. Parental emotion and emotion regulation: a critical target of study for research and intervention to promote child emotion socialization. Dev Psychol. (2020) 56(3):403–17. doi: 10.1037/dev0000864
83. Giallo R, Cooklin A, Wade C, D’Esposito F, Nicholson JM. Fathers’ postnatal mental health and child well-being at age five: the mediating role of parenting behavior. J Fam Issues. (2014) 35(11):1543–62. doi: 10.1177/0192513X13477411
84. Van den Hoofdakker BJ, Hoekstra PJ, van der Veen-Mulders L, Sytema S, Emmelkamp PM, Minderaa RB, et al. Paternal influences on treatment outcome of behavioral parent training in children with attention-deficit/hyperactivity disorder. Eur Child Adolesc Psychiatry. (2014) 23:1071–9. doi: 10.1007/s00787-014-0557-4
85. Manuele SJ, Yap MBH, Lin SC, Pozzi E, Whittle S. Associations between paternal versus maternal parenting behaviors and child and adolescent internalizing problems: a systematic review and meta-analysis. Clin Psychol Rev. (2023) 105:102339. doi: 10.1016/j.cpr.2023.102339
86. Schisterman EF, Cole SR, Platt RW. Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology. (2009) 20(4):488–95. doi: 10.1097/EDE.0b013e3181a819a1
87. Bornstein MH, Putnick DL, Lansford JE, Pastorelli C, Skinner AT, Sorbring E, et al. Mother and father socially desirable responding in nine countries: two kinds of agreement and relations to parenting self-reports. Int J Psychol. (2015) 50(3):174–85. doi: 10.1002/ijop.12084
88. Bögels SM, van Melick M. The relationship between child-report, parent self-report, and partner report of perceived parental rearing behaviors and anxiety in children and parents. Pers Individ Dif. (2004) 37(8):1583–96. doi: 10.1016/j.paid.2004.02.014
89. Pingault JB, Rijsdijk F, Schoeler T, Choi SW, Selzam S, Krapohl E, et al. Genetic sensitivity analysis: adjusting for genetic confounding in epidemiological associations. PLoS Genet. (2021) 17(6):e1009590. doi: 10.1371/journal.pgen.1009590
90. Groenwold RH, Sterne JA, Lawlor DA, Moons KG, Hoes AW, Tilling K. Sensitivity analysis for the effects of multiple unmeasured confounders. Ann Epidemiol. (2016) 26(9):605–11. doi: 10.1016/j.annepidem.2016.07.009
91. Nazareth I. Should men be screened and treated for postnatal depression? Expert Rev Neurother. (2011) 11(1):1–3. doi: 10.1586/ern.10.183
92. Cowan PA, Cowan CP. Developmental psychopathology from family systems and family risk factors perspectives: implications for family research, practice, and policy. In: Cicchetti D, Cohen J, editors. Developmental Psychopathology. Wiley (2006). p. 530–87.
93. Taylor LB, Billings J, Morant N, Johnson S. How do women’s partners view perinatal mental health services? A qualitative meta-synthesis. Clin Psychol Psychother. (2018) 25(1):112–29. doi: 10.1002/cpp.2133
94. Panter-Brick C, Burgess A, Eggerman M, McAllister F, Pruett K, Leckman JF. Practitioner review: engaging fathers–recommendations for a game change in parenting interventions based on a systematic review of the global evidence. J Child Psychol Psychiatry. (2014) 55(11):1187–212. doi: 10.1111/jcpp.12280
95. Magill-Evans J, Harrison MJ, Rempel G, Slater L. Interventions with fathers of young children: systematic literature review. J Adv Nurs. (2006) 55(2):248–64. doi: 10.1111/j.1365-2648.2006.03896.x
96. Buisman RS, Alyousefi-van Dijk K, de Waal N, Kesarlal AR, Verhees MW, van IJzendoorn MH, et al. Fathers’ sensitive parenting enhanced by prenatal video-feedback: a randomized controlled trial using ultrasound imaging. Pediatr Res. (2023) 93(4):1024–30. doi: 10.1038/s41390-022-02183-9
97. Culpin I, Pearson RM, Wright N, Stein A, Bornstein MH, Tiemeier H, et al. Paternal postnatal depression and offspring emotional and behavioural development at age 7 years in a UK-birth cohort: the mediating roles of paternal parenting confidence, warmth, and conflict. PsyArXiv Preprints. (2024). Available online at: https://doi.org/10.31234/osf.io/rz5a7
Keywords: ALSPAC, population-based study, paternal postnatal depression, child development, father-child conflict and warmth, paternal parenting confidence
Citation: Culpin I, Pearson RM, Wright N, Stein A, Bornstein MH, Tiemeier H, Fredriksen E, Evans J, Miller T, Dermott E, Heron J, Sallis HM and Hammerton G (2025) Paternal postnatal depression and child development at age 7 years in a UK-birth cohort: the mediating roles of paternal parenting confidence, warmth, and conflict. Front. Child Adolesc. Psychiatry 4:1650799. doi: 10.3389/frcha.2025.1650799
Received: 20 June 2025; Accepted: 28 August 2025;
Published: 12 September 2025.
Edited by:
Yao Cheng, Hubei Maternal and Child Health Hospital, ChinaReviewed by:
Michaela Viragova, Kings London, United KingdomSarah Manuele, Monash University, Australia
Copyright: © 2025 Culpin, Pearson, Wright, Stein, Bornstein, Tiemeier, Fredriksen, Evans, Miller, Dermott, Heron, Sallis and Hammerton. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Iryna Culpin, aXJ5bmEuY3VscGluQGtjbC5hYy51aw==