 Ye Niu
Ye Niu Yuko Yoshimura
Yuko Yoshimura Manabu Yoshioka
Manabu Yoshioka Mitsuru Kikuchi
Mitsuru Kikuchi Hiroaki Kobayashi
Hiroaki Kobayashi- 1United Graduate School of Child Development, Osaka University, Suita, Japan
- 2Institute of Human and Social Sciences, Kanazawa University, Kanazawa, Japan
- 3Research Center for Child Mental Development, Kanazawa University, Kanazawa, Japan
- 4Affiliated School for Special Needs Education, Kanazawa University, Kanazawa, Japan
- 5Department of Psychiatry & Behavioral Science, Kanazawa University, Kanazawa, Japan
Introduction: Private speech has been shown to serve as a self-regulatory and planning tool for children during task-solving activities. While both typically developing children and those with neurodevelopmental disorders—such as attention-deficit/hyperactivity disorder and high-functioning autism spectrum disorder (ASD)—have been found to use private speech, the frequency and developmental trajectories vary across groups. However, little is known about private speech in children with intellectual disabilities.
Methods: This study examined private speech in children with intellectual disabilities (n = 20) during a selective attention task. Verbalizations were recorded and categorized based on their relevance to the task.
Results: Seventy percent of the participants used private speech during the task, and 60% produced task-relevant utterances that appeared to assist in problem-solving. Notably, children with stronger ASD characteristics exhibited more frequent use of private speech than those with milder traits.
Discussion: These findings suggest that children with intellectual disabilities engage in private speech during cognitive tasks, and that this speech may function as a tool for behavioral regulation. The increased use among those with pronounced ASD tendencies may reflect differences in cognitive or social processing, underscoring the importance of considering individual variability in educational support.
1 Introduction
Private speech, which serves as a tool for thinking with functions such as behavioral regulation and planning, has been gaining attention in the study of children's language development (Lidstone et al., 2011; Aro et al., 2015; Mulvihill et al., 2020). During early childhood, when engaging in cognitive tasks, children think about, regulate, and direct their actions through (spoken) private speech. When entering school age, a transitional period in language development from private speech to (unspoken) inner speech emerges. During this time, the incidence of private speech gradually decreases and the volume of speech becomes quieter, eventually developing into inner speech (Winsler et al., 2000; Winsler and Naglieri, 2003; Manfra and Winsler, 2006).
2 Literature review
2.1 Private speech
Private speech is a concept in developmental psychology that is particularly associated with psychologist Vygotsky's (1934/1962, 1987) work. Private speech, also known as self-directed speech, refers to the internal verbalizations employed by individuals, particularly young children, to facilitate their cognitive processes and inform their actions. Private speech, in its typical form, is audible yet not directed at other individuals and serves a cognitive function rather than one of communication (e.g., Vygotsky and Luria, 1930/1993; Luria, 1961).
According to Lev Vygotsky, private speech can be conceptualized as an intermediate form of communication that lies between external communication and internalized thought. Over time, private speech becomes silent or “inner speech,” a form of self-guided thought (Vygotsky, 1934/1962, 1987). Subsequent research has offered some empirical support for the notion that private speech is most prevalent during early childhood (ages 2–7), gradually diminishing as children progress through their developmental stages and evolve internalized thought processes (inner speech) (Kohlberg et al., 1968; Pellegrini, 1981; Duncan and Pratt, 1997). Additionally, research examining the development of private speech during the preschool and early school years has generally supported Vygotsky's theoretical predictions regarding age-related changes in its frequency and structure. Findings indicate that private speech typically follows a developmental progression, as outlined in Berk's levels of private speech, evolving from overt, task-irrelevant utterances (Level 1) to overt, task-relevant verbalizations, such as self-instructive comments (Level 2). Over time, these verbalizations become increasingly internalized, manifesting externally as whispering or inaudible muttering (Level 3), which represent transitional forms of inner speech (Berk, 1986; Berk and Garvin, 1984; Bivens and Berk, 1990).
2.2 Research on children with typical development
A substantial body of empirical evidence has emerged from studies on private speech subsequent to Vygotsky's seminal contributions. These studies have provided substantial empirical support for Vygotsky's (1934/1962) theory of the cognitive developmental function of private speech. According to this theoretical framework, private speech functions as an intermediate developmental stage, situated between externalized vocal speech and inner self-guiding verbal speech. Children use private speech as an externalized tool of thought to assist them in guiding and controlling their behaviors. With increasing cognitive maturity, private speech becomes internalized and transitions into internalized verbal thought or inner speech. Additionally, Vygotsky considered private speech vital in problem-solving when children encounter challenges in task-solving situations.
In uncovering the development of private speech during preschool and early school years, researchers have identified empirical evidence that aligns with Vygotsky's view of age-related changes in the incidence and structure of this form of speech. Researchers have identified a predictable trajectory in the development of private speech, which initially evolves from overt task-irrelevant speech to overt task-relevant speech (e.g., self-guiding comments), subsequently transitioning to external manifestations of inner speech, such as whispering and inaudible muttering (Berk and Spuhl, 1995; Winsler et al., 1997; Patrick and Abravanel, 2000; Winsler and Naglieri, 2003).
To date, research investigating the performance-related benefits of private speech has primarily explored the relationship between task performance and either the frequency or developmental trajectory of private speech toward internalization (Behrend et al., 1989; Montero and De Dios, 2006). More recent studies have extended this line of inquiry by examining the role of specific content subtypes of private speech in task performance. Evidence indicates that these subtypes may differentially affect performance outcomes depending on their functional relevance. Specifically, greater use of task-irrelevant private speech has been associated with lower accuracy during construction tasks, whereas increased use of private speech involving planning and motivational content has been linked to improved task accuracy (Mulvihill et al., 2021). Additionally, researchers have indicated that the occurrence of private speech escalates in instances when juveniles encounter obstacles in task-solving scenarios (Kohlberg et al., 1968; Zivin, 1972; Deutsch and Stein, 1972; Dickie, 1973; Berk and Garvin, 1984; Duncan and Pratt, 1997; Fernyhough and Fradley, 2005), thereby corroborating Vygotsky's perspective on the adaptive function of private speech as a mechanism for self-regulation.
2.3 Research on children with neurodevelopmental disorders
Along with studies on the private speech of typically developing children that intensified after Vygotsky (1987) first documented the importance of private speech, research on children with neurodevelopmental disorders has also progressed in recent years. Despite utilizing comparable strategies when executing cognitive tasks, in comparison to their age-mates, children diagnosed with developmental language disorders exhibit a maturational delay in the onset and gradual internalization of private speech (Sturn and Johnston, 1999; Lidstone et al., 2012). Studies on children diagnosed with attention-deficit/hyperactivity disorder (ADHD) have observed that while these children employ private speech to complete tasks akin to those performed by typically developing children, they tend to produce a higher volume of private speech. Furthermore, the transition from private to inner speech is more protracted in children with ADHD compared to their typically developing peers (Winsler et al., 1999; Corkum et al., 2008).
Furthermore, Winsler et al. (2007) indicated that children diagnosed with high-functioning autism spectrum disorder (HFASD) demonstrate patterns of internal speech that resemble those observed in children diagnosed with ADHD. However, they also noted significant individual variations among children with HFASD. In summary, children with neurodevelopmental disorders may use private speech to solve tasks, despite delayed maturation in the developmental process of private speech. However, no previous studies have focused on this topic among children with intellectual disabilities.
2.4 Children with intellectual disabilities
Intellectual disability (ID) is a disorder that manifests during the developmental period, affecting intellectual and adaptive functioning. It is characterized by challenges in acquiring cognitive skills and adaptive social and communicative behaviors (American Psychiatric Association, 2013). Both preschoolers and school-age children with ID exhibit slow progress in language and learning skills, including reading and understanding concepts involving numbers and time, compared to typically developing children. Additionally, executive functions such as strategizing and cognitive flexibility are impaired (American Psychiatric Association, 2013), resulting in difficulties in planning, shifting, and regulating inappropriate language use and non-adaptive behaviors.
Intellectual disability is categorized into four severity levels based on standardized assessments of intellectual functioning and adaptive behavior. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) outlines the following classification criteria: individuals with mild intellectual disability typically exhibit full-scale IQ scores ranging from 50 to 69; those with moderate intellectual disability fall within the IQ range of 35–49; severe intellectual disability is defined by IQ scores between 20 and 34; and profound intellectual disability is characterized by IQ scores below 20 (American Psychiatric Association, 2013). These diagnostic categories are critical for determining the level of support required and for informing appropriate educational and clinical interventions.
While traditional diagnostic frameworks have emphasized intellectual functioning as a primary indicator of intellectual disability, the DSM-5 shifts the focus to adaptive functioning as the central criterion for determining severity levels (American Psychiatric Association, 2013). According to this model, classification is based on the amount of support an individual requires across three primary domains: the conceptual domain, involving skills related to academic learning and cognitive processing; the social domain, which includes interpersonal communication, social understanding, and judgment; and the practical domain, encompassing self-care, daily living skills, and occupational performance. Adaptive functioning reflects an individual's ability to manage everyday tasks and navigate social and practical challenges, offering a more ecologically valid measure of functioning than IQ alone (Schalock et al., 2010).
IQ scores continue to be recognized as indicators of cognitive potential, yet they are relatively stable over time and less responsive to intervention. In contrast, adaptive behavior can improve with targeted support and educational interventions, making it a more dynamic and functional measure for clinical decision-making and service planning. Standardized tools such as the Vineland Adaptive Behavior Scales are commonly used to evaluate these domains in clinical and educational contexts (Sparrow et al., 2016).
Private and inner speech have been conceived as keys to uncovering the mechanisms underlying the development of children's communicative competence (Feigenbaum, 2009). According to Vygotsky (1934/1962, 1987), children primarily begin to learn how to communicate through social interactions with adults. Then, they talk aloud to themselves, rather than to others, to practice, explore, and gradually comprehend their communicative skills. When children eventually develop an understanding of conversational norms, their private speech transforms from being unconscious and unintended to conscious, purposeful, and communicatively competent (Feigenbaum, 2009). In this developmental process, language ability, particularly language acquisition, plays a critical role in the mastering of communication skills. If language ability does not develop to a certain level, children may struggle in the initial stage of interacting with adults, which could in turn affect the subsequent stages of communicative competence development.
Children with IDs often experience delays in language development. This raises the question of whether low language ability affects the development of private speech. Exploration of this possibility could offer significant value, as it would allow for the identification of potential disparities in private speech development among three distinct groups: children with IDs, typically developing children, and children with other developmental disorders. This identification of differences could provide novel insights into the domain of private speech research.
In the context of educational interventions for children diagnosed with IDs, there is a compelling need to implement teaching methodologies and specialized support that are meticulously customized to address the unique needs and characteristics of each child. For example, teachers in special support schools need evidence-based information regarding which aspects of a child's language behavior to observe to be able to respond effectively. This study aims to contribute to the body of knowledge surrounding the speech characteristics of children with IDs by providing special education teachers with actionable suggestions regarding the development of speech in this demographic, along with specific teaching methodologies and support.
In summary, research on children with typical development has demonstrated that private speech evolves in a predictable sequence from audible and externalized to more internalized, less audible, and abbreviated forms. Typically developing children utilize private speech as a means of self-regulation to assist them in overcoming challenges in tasks and regulating their behavior. Children with ADHD exhibit a speech pattern similar to that of their typically developing counterparts; however, they demonstrate a higher incidence of task-irrelevant private speech and a more protracted transition period between tasks. Research on the private speech of children with autism is quite limited, with the sole article finding that children with high-functioning autism show similar patterns of private speech to ADHD groups. To date, while discrepancies have been identified in the occurrence of private speech between children with IDs such as autism compared to their typically developing peers, no research has focused on the private speech of children with IDs. Therefore, the question regarding the characteristics of private speech among children with ID remains. To the best of our knowledge, this study is the first to examine private speech in children with IDs.
2.5 Purpose
The present study set the following research questions: (1) Do children with IDs exhibit private speech? (2) If so, what are the characteristics of their private speech?
Thus, we hypothesize:
(a) Children with IDs have private speech.
(b) The development of private speech in children with IDs shares the same pattern as that of typically developing children.
(c) Although children with IDs strategically use private speech in problem-solving tasks, there are differences in frequency and content considering their age range, intellectual abilities, language level, other coexisting disorders (e.g., ASD), and social adaptability.
3 Methods
3.1 Participants
Twenty children (seven girls) between the ages of 8 and 17 years ( = 14.1, SD = 2.4), enrolled in a special needs school in Japan, participated in this study. All participants were clinically diagnosed with ID; eight participants were diagnosed with ASD ( = 14.7, SD = 2.2), five participants (two girls) were diagnosed with Down syndrome ( = 12.9, SD = 3.3), one (female) participant was diagnosed with a language disorder, one (female) participant was diagnosed with Soto syndrome, and one (female) participant was diagnosed with ataxic cerebral palsy before they entered school. Based on the KABC-II results (for assessment profiles, see Table 1), only children with scores of 70 or below were included as participants in the study.
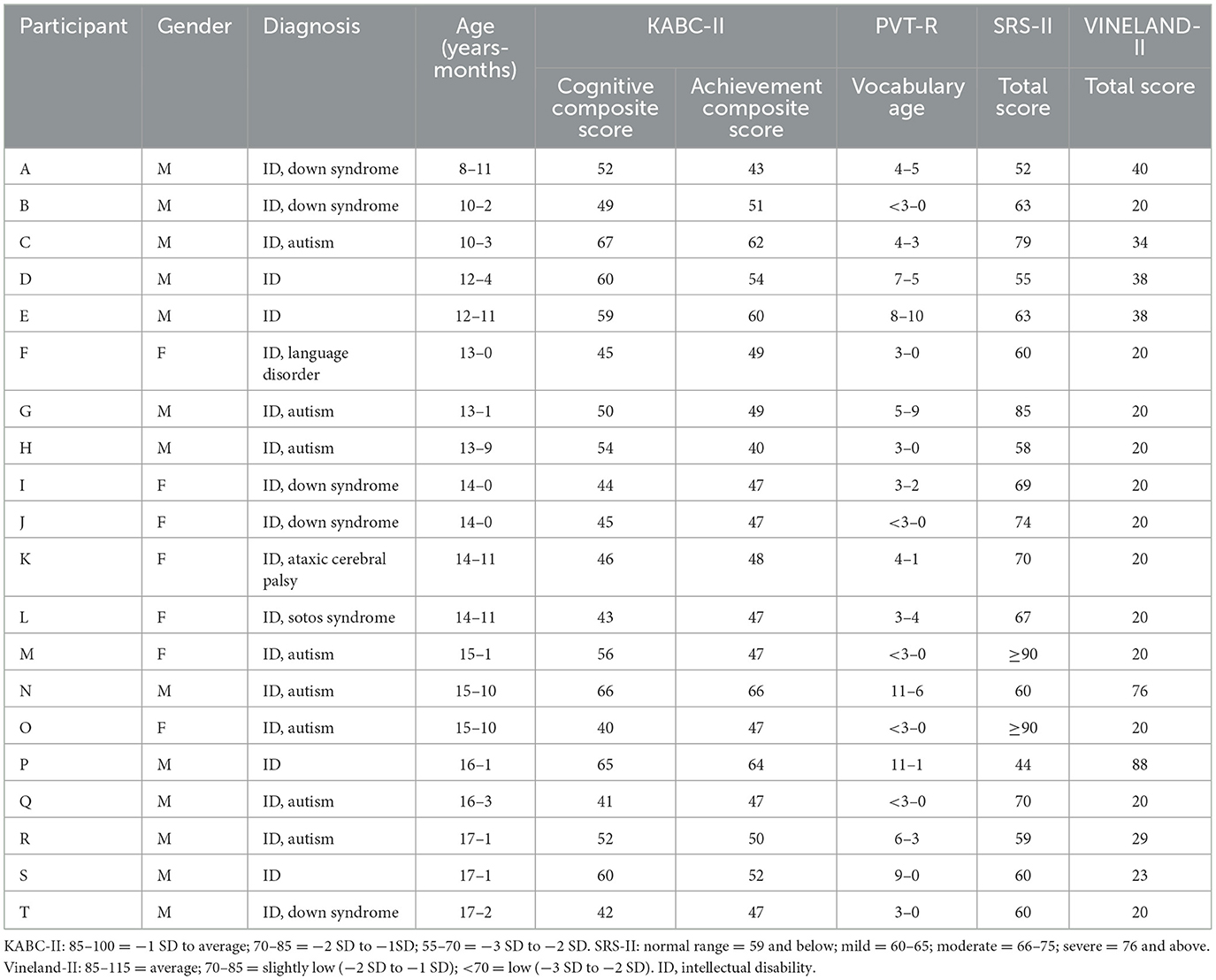
Table 1. Basis profiles and assessment results of participants.
3.2 Assessment
To assess participants' developmental conditions, a combination of standardized cognitive, language, social, and adaptive behavior measures were administered.
3.2.1 Kaufman assessment battery for children—second edition (KABC-II, Japanese version)
The KABC-II (Kaufman and Kaufman, 2018; Japanese Version KABC-II Production Committee, 2013) is a comprehensive cognitive assessment tool designed to measure problem-solving and processing abilities in children. The Japanese version includes both cognitive scales and an Achievement Scale to evaluate acquired academic skills. It is suitable for children aged 3–18.
The KABC-II demonstrates high reliability, with Cronbach's alpha coefficients ranging from 0.88 to 0.97 across various scales (Kaufman and Kaufman, 2018). The Japanese version retains comparable reliability metrics, with Cronbach's alpha coefficients ranging from 0.88 to 0.97 across various scales (Japanese Version KABC-II Production Committee, 2013). Construct validity is supported through confirmatory factor analysis, affirming a five-factor structure (Sequential, Simultaneous, Learning, Planning, and Knowledge). Standard scores are reported with a mean of 100 and a standard deviation of 15, where higher scores indicate stronger cognitive performance.
3.2.2 Picture vocabulary test—revised (PVT-R)
The PVT-R (Ueno et al., 2008) is a brief, standardized measure of receptive vocabulary development for children aged 3–12.25 years. It evaluates a child's ability to comprehend spoken words by selecting the appropriate image from multiple choices.
The PVT-R is used to assess participants' receptive vocabulary because their language age is lower than their chronological age, a typical trait of children with intellectual disabilities. It is well-suited for this population as it provides a standardized, developmentally appropriate measure of language skills, essential for evaluating their use of private speech.
The instrument has high reliability (α > 0.90) and strong test-retest reliability (r > 0.85). Its construct validity is supported by moderate to high correlations with other standardized language development assessments. While the PVT-R yields both standard scores and vocabulary age, this study adopts vocabulary age as the primary metric for evaluation.
3.2.3 Social responsiveness scale—second edition (SRS-2, Japanese version)
The SRS-2 (Kamikawa, 2017) is a norm-referenced questionnaire used to assess social impairments associated with autism spectrum disorder (ASD). It can be completed by parents or teachers and is applicable across a wide age range, from early childhood through adulthood.
The Japanese version of the SRS-2 demonstrates excellent reliability (α = 0.95) and strong test-retest reliability (r = 0.88), with construct validity supported by significant correlations with established autism diagnostic tools such as the ADOS and SCQ. The scale yields T-scores (M = 50, SD = 10), where higher scores reflect greater severity of social impairment. Severity is classified into three categories: mild (T-score 60–74), moderate (75–88), and severe (89 and above).
In the present study, 15 participants were identified as having ASD according to the SRS-2: six at the mild level, five at the moderate level, and four at the severe level.
3.2.4 Vineland adaptive behavior scales—second edition (Vineland-II, Japanese version)
The Vineland-II (Tsuji and Murakami, 2014) is used to assess adaptive functioning across domains such as communication, daily living skills, socialization, and motor skills. It is widely used in clinical and educational contexts to evaluate individuals with developmental disabilities or other adaptive concerns.
The Japanese adaptation maintains high reliability (α = 0.83–0.94) and robust inter-rater and test-retest reliability. Construct validity is demonstrated through factor analytic studies and correlations with developmental and intelligence tests. Standard scores (M = 100, SD = 15) are used, with higher scores reflecting better adaptive behavior. The scale assists in identifying both strengths and areas requiring intervention.
3.3 Procedure
3.3.1 Selective attention task
In a separate room at the school, the participants were video- and audio-recorded while performing a selective attention task. This task was developed to elicit children's private speech within an appropriate challenging range for typically developing preschoolers (Diaz, 1992; Winsler et al., 1997; Winsler, 1998; Winsler et al., 2003). Adjustments were made to accommodate the characteristics of children with IDs, including modifications in instructions, the number of tasks, and task procedures. For example, the selective task used in previous studies (Winsler et al., 2003) has two example items explained by the experimenter and 12 items for children to finish individually. However, in the current study, the experimenter provided three example items and 30 items for participants to finish by themselves. Further, instead of providing 18 answer cards for children to select from Winsler et al. (2003), the present study used three possible answer cards for each item to reduce the potential burden caused by variant stimuli for participants.
In the selective attention tasks, participants were instructed to decide first which dimension (either color or shape) was shared between two pictures on one card, then to select a new picture card with the same dimension as the other two, and finally to attach it as the third card in the set (see Figure 1). For instance, if the cards showed one “red car” and one “yellow car,” the correct answer was a “car” of any color. The correct dimension varied randomly across the 30 items with three shapes (flower, car, or cat) and three colors (red, yellow, or green).
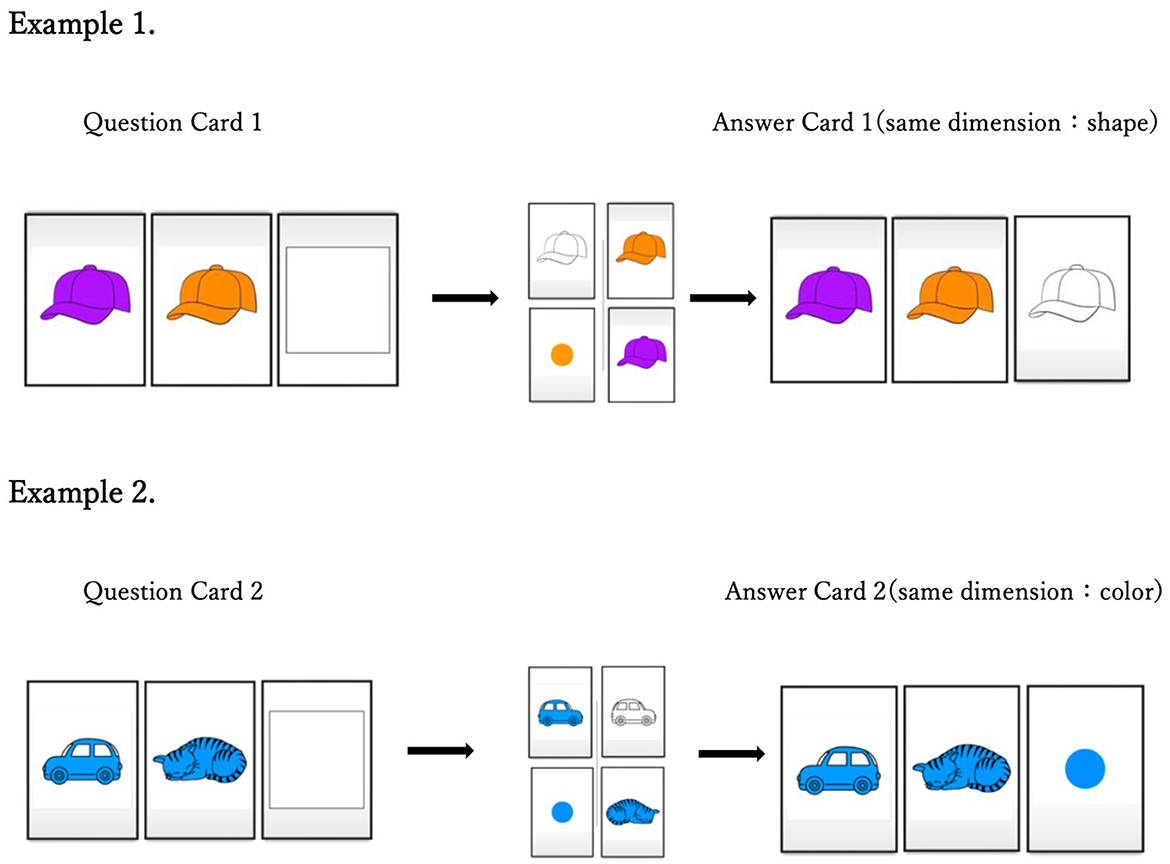
Figure 1. Instructive examples of selective attention task.
One experimenter introduced the task with three example items and asked the participants to complete three tests after each example to ensure that they understood the rules of the task. Subsequently, the participants were asked to complete the 30 items individually within 10 min. The experimenter remained silent and gave no reminders during the task unless the participant could not start or continue doing the task alone. Two video cameras mounted on a tripod were set at different corners of the room, and a digital voice recorder was placed on the table. Participants' speech was recorded by cameras and voice recorders during the task and later transcribed from videotapes and audio files by the author.
3.3.2 Ethics approval statement
The guardians of all participants were provided with a written explanation of the research overview, and written consent for participation in the study was obtained. This study was approved by the Institute of Human and Social Sciences Ethics Committee of Kanazawa University [approval number: [2021-15-4]] [20230412]. All procedures were performed in accordance with the ethical standards of the institution.
3.4 Data processing
3.4.1 Coding
The coding process was meticulously executed in two stages. Initially, each utterance was assigned to a superordinate category, namely social or private. A single utterance's categorization as “social” was based on the following criteria (Fernyhough and Russell, 1997): (1) continuous or immediate eye contact with the experimenter during or within 2 s following an utterance; and (2) the child's behavior involving the experimenter through physical contact, gaze direction, or vocalization that reflected the same topic as the experimenter's previous utterance within 2 s of one utterance. Additionally, the content of social utterances included calling the experimenter by name or a vocative or asking the experimenter questions. Utterances occurring within 2 s of a prior social utterance were also coded as social if they met the aforementioned criteria.
Private utterances were further classified into three categories according to Berk's (1986) revised coding scheme. Level 1 private speech encompasses wordplay, repetition, task-irrelevant affect expressions, and comments directed toward absent, imaginary, and non-human entities. Level 2 private speech comprises self-directed comments, descriptions of one's own activity, and task-irrelevant self-questions without answers (added to the revised edition). Level 3 private speech encompasses task-relevant external manifestations of inner speech, including inaudible muttering—that is, remarks involving clear mouthing of words that cannot be heard—and lip and tongue movement only, that is, no clear mouthing of words (for details, see Table 2).
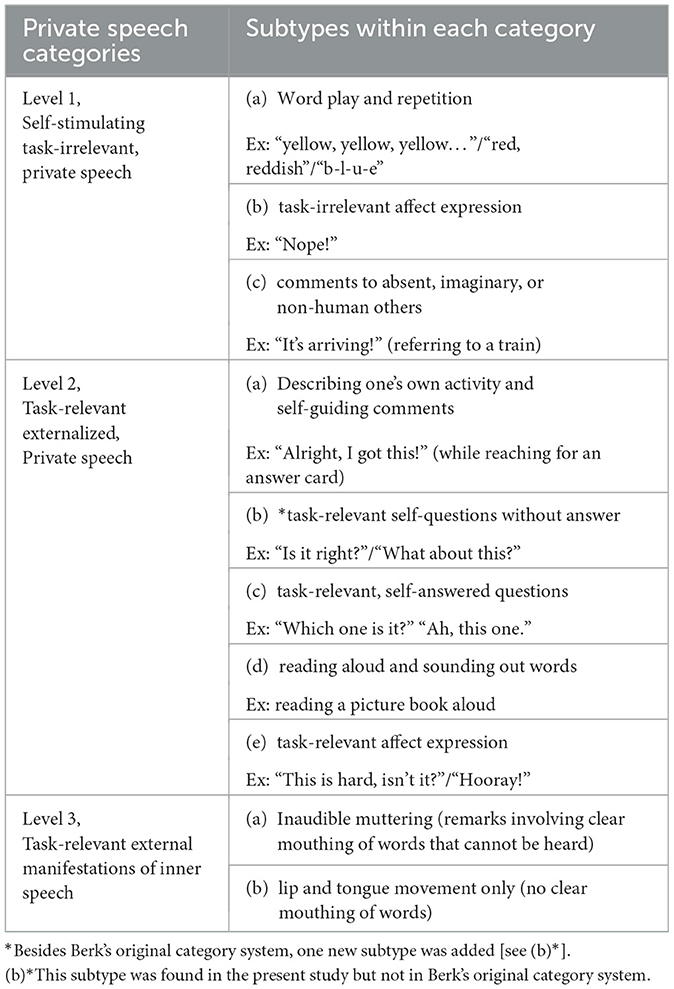
Table 2. Berk's coding system (*revised version).
Prior research (Winsler et al., 2007) has measured both social speech and private speech. Following this, the present study also assessed both forms of speech to enable potential comparisons (for details, see Tables 3a, b).
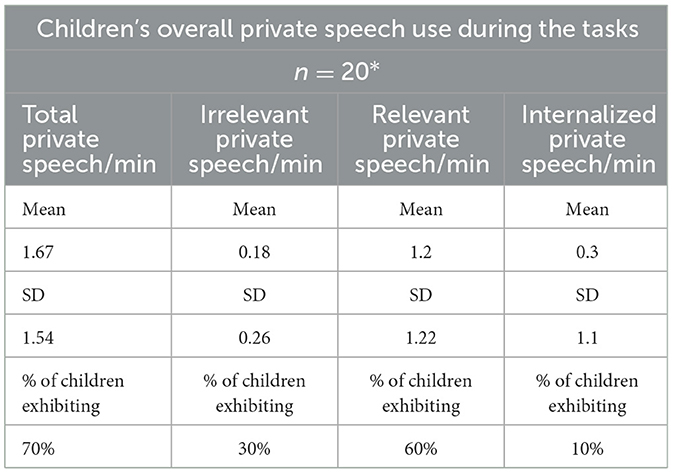
Table 3a. Children's overall private speech use during the tasks.
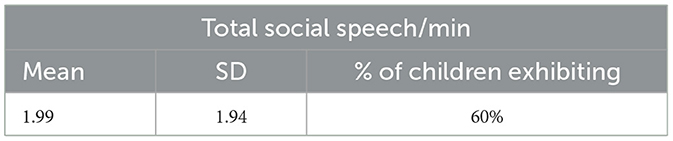
Table 3b. Children's overall social speech use during the tasks.
3.4.2 Inter-rater reliability
A subset (20%) of the transcripts was independently assessed by two graduate students studying special needs education. Cronbach's α was 0.974 for the distinction between social and private speech and 0.984 for the three-level system in Berk's coding system.
4 Results
4.1 Participant profiles
Cognitive abilities were assessed using the Kaufman Assessment Battery for Children, Second Edition (KABC-II; Kaufman and Kaufman, 2004). Results indicated that most participants demonstrated significant cognitive impairments. Specifically, 7 participants scored between −3 and −2 standard deviations below the mean, and 13 participants scored between −4 and −3 standard deviations below the normative mean.
Language abilities were evaluated using the Picture Vocabulary Test–Revised (PVT-R; Ueno et al., 1991). Performance varied substantially across the participants. Five participants demonstrated language functioning below the developmental level of a 3-year-old. Ten participants functioned at a level comparable to 3- to 6-year-old children, while 5 participants demonstrated language abilities within the developmental range of 7–11 years.
Autistic traits were assessed using the Social Responsiveness Scale, Second Edition (SRS-2). A total of 15 participants exhibited clinically significant levels of autistic traits. Of these, 4 participants scored in the severe range (T-score ≥ 76), 5 in the moderate range (T-score = 66–75), and 6 in the mild range (T-score = 60–65).
Adaptive functioning was assessed using the Vineland Adaptive Behavior Scales, Second Edition (Vineland-II). Most participants obtained scores below 70, indicating significant deficits in adaptive behavior. One participant scored in the moderately low range (ABC score = 71–85), and another scored within the average range (ABC score = 86–114).
4.2 Speech use
Participants' use of private (see Table 3a) and social speech (see Table 3b) during the task was calculated. The values for the three specific categories of private speech were examined: irrelevant, task-relevant, and partially internalized whispers/mutterings. These categories were assessed in terms of frequency per minute and proportion of total private speech. The utterance per minute measures included all participants, while the proportional measures only included participants who engaged in at least some private speech. The total private speech per minute (total private speech/min) was calculated by dividing all private speech in the task by the total task completion time. The percentage of participants exhibiting (% of children exhibiting) refers to the number of participants who exhibited such private speech.
First, it should be noted that 70% of the participants used private speech during the task. Furthermore, 67% of the participants identified as having suspended ASD according to the SRS-2 used private speech during the task (ASD = 15, = 14.1, SD = 2.2), whereas 80% of those without ASD used private speech during the task (ID = 5, = 13.2, SD = 3.7). Second, the frequencies of the three subcategories of private speech (task-irrelevant, task-relevant, and partially internalized private speech) are summarized in Table 3a. Notably, ~60% of the participants used task-relevant private speech compared to only 30% of task-irrelevant private speech users and 10% of partially internalized private speech users.
4.3 Differences between groups
To investigate differences in private speech across groups, non-parametric statistical tests were employed. Specifically, the Mann–Whitney U-test was used to compare participants with and without comorbid autistic tendencies, while the Kruskal–Wallis test was applied to assess differences across three age groups: the elementary school group (aged 8 years 11 months to 12 years 4 months), the junior high school group (aged 12 years 11 months to 14 years 11 months), and the senior high school group (aged 15 years 1 months to 17 years 2 months). Results from the Mann–Whitney U-test indicated no significant differences between participants with and without autistic tendencies in terms of total private speech per minute or any of the three private speech subcategories (see Table 4a). Similarly, the Kruskal–Wallis test revealed no significant age-related differences in total private speech per minute or in the three subcategories (see Table 4b).
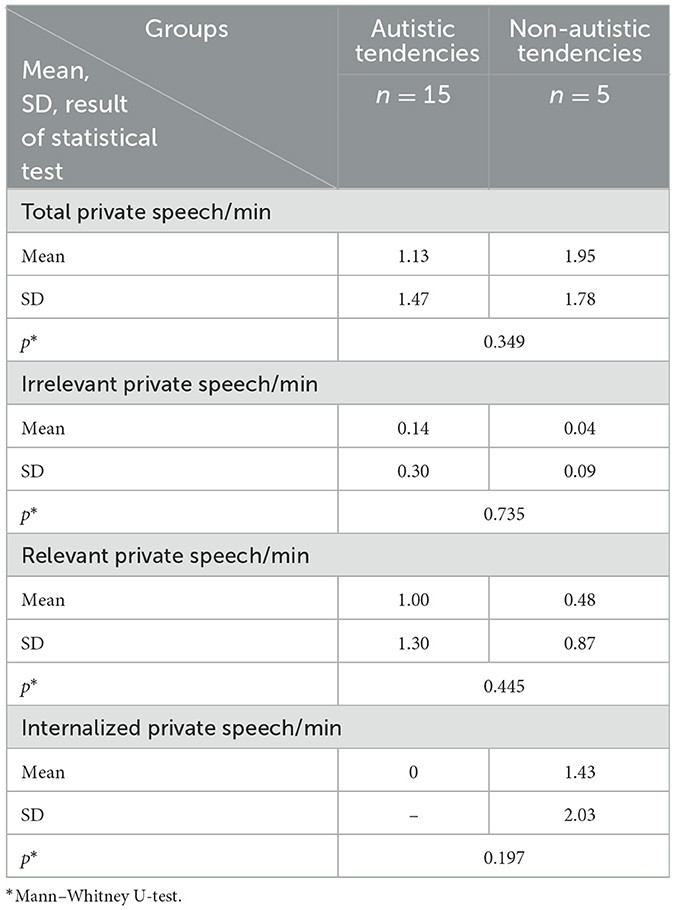
Table 4a. Autistic tendencies and non-autistic tendencies groups.
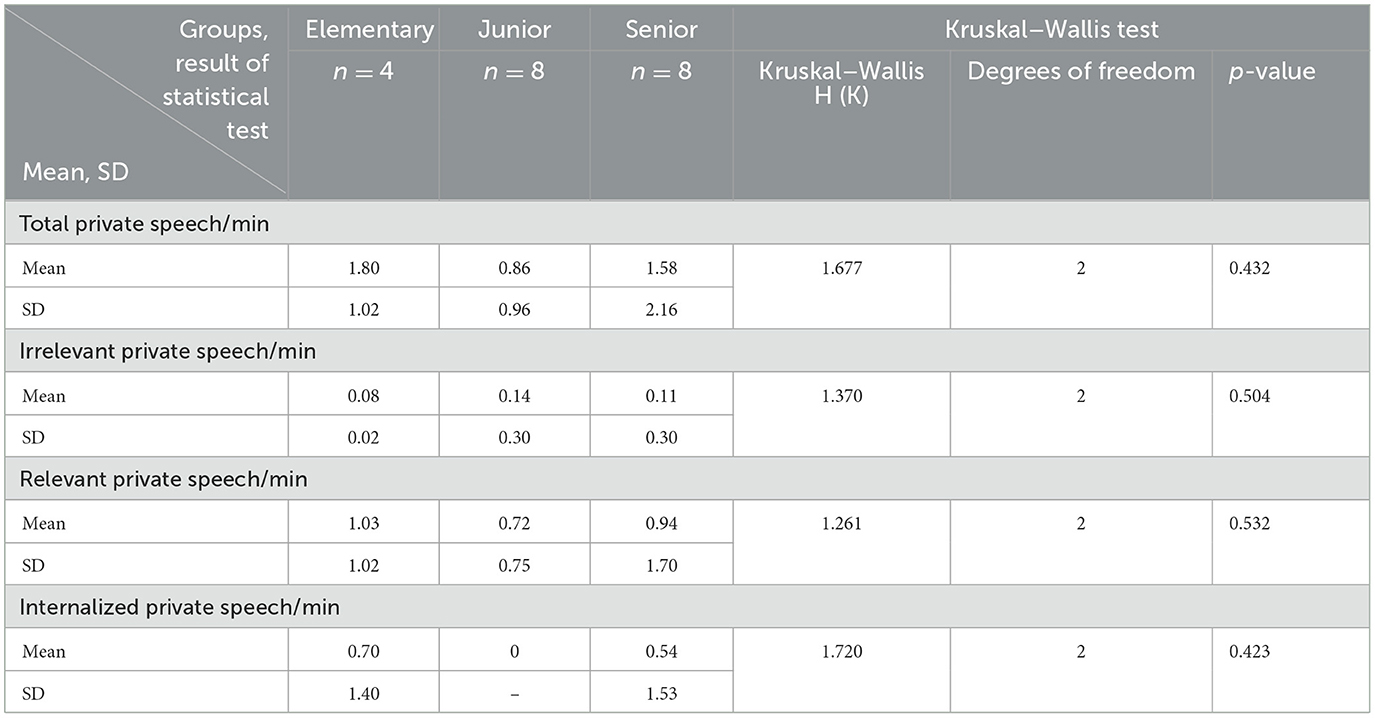
Table 4b. Three age groups: elementary (8–11 to 12–4), junior high school (12–11 to 14–11), and senior high school (15–1 to 17–2) (mean, standard deviation, and non-parametric test score).
A non-parametric analysis was conducted to investigate whether significant differences in private speech occurred across high- and low-scoring groups on various assessment measures. Results indicated that among children characterized as having autistic traits, those with more severe autism symptomatology, as measured by the SRS-2, exhibited significantly higher levels of both total and task-relevant private speech. Statistically significant group differences were observed among those classified with mild, moderate, and severe autism spectrum tendencies (p = 0.013 for both comparisons; see Table 5d). In contrast, no significant differences were observed on the PVT-R, suggesting that verbal ability did not significantly affect the use of private speech (see Table 5c). Similarly, scores on the Cognitive Composite Scale and Achievement Composite Scale of the K-ABC did not show statistically significant differences, indicating that intellectual ability was not a significant factor in private speech occurrence (see Tables 5a, b). Due to the small sample size in the Vineland-II group, non-parametric analyses were not conducted for this measure; however, descriptive statistics are reported in Table 5e.
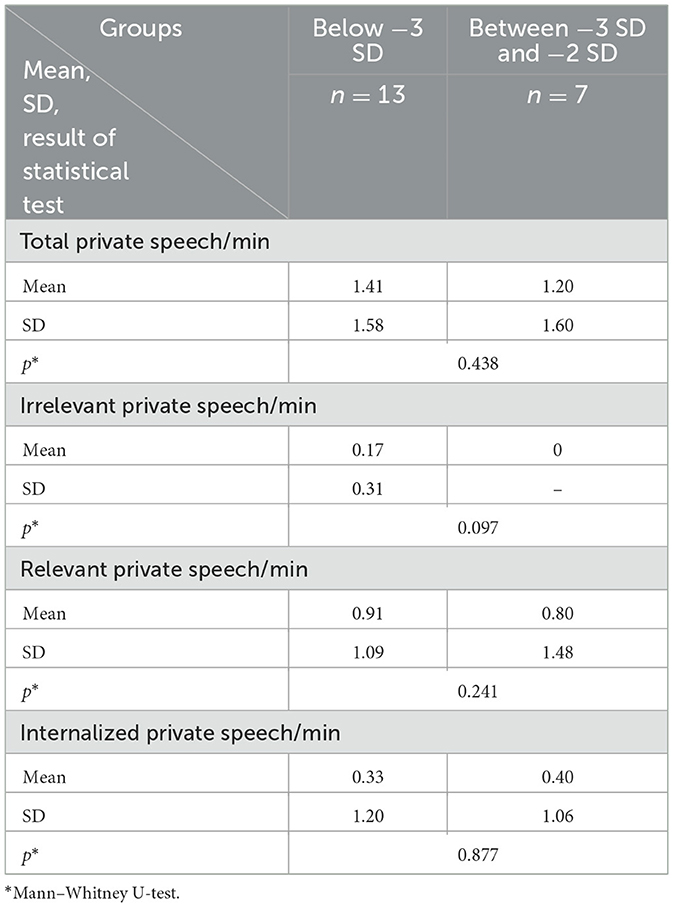
Table 5a. High- and low-scoring groups across Cognitive Composite Scale of KABC-II (mean, standard deviation, and non-parametric test score).
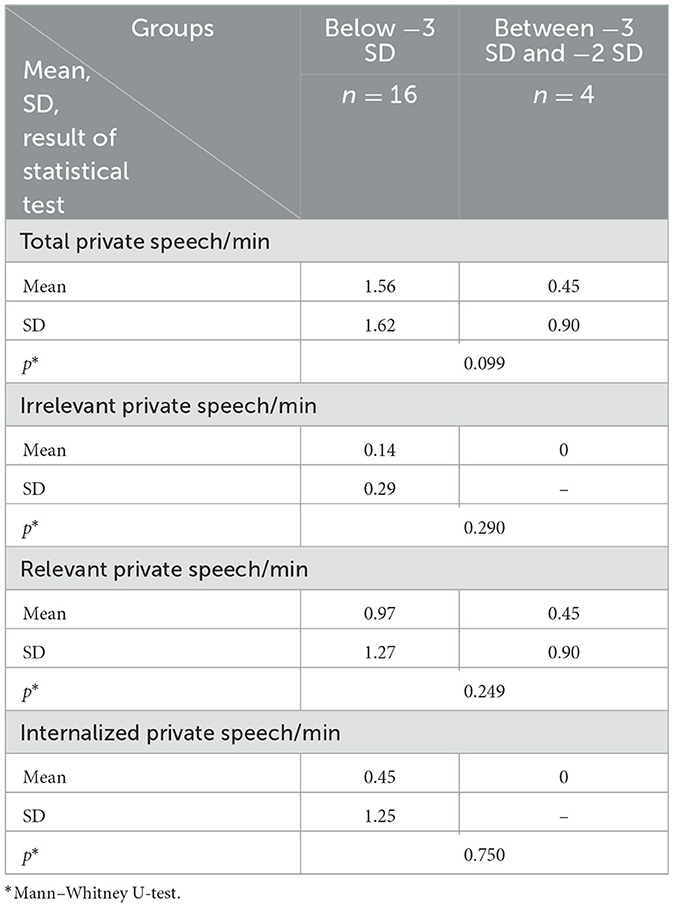
Table 5b. High- and low-scoring groups across Achievement Composite Scale of KABC-II (mean, standard deviation, and non-parametric test score).
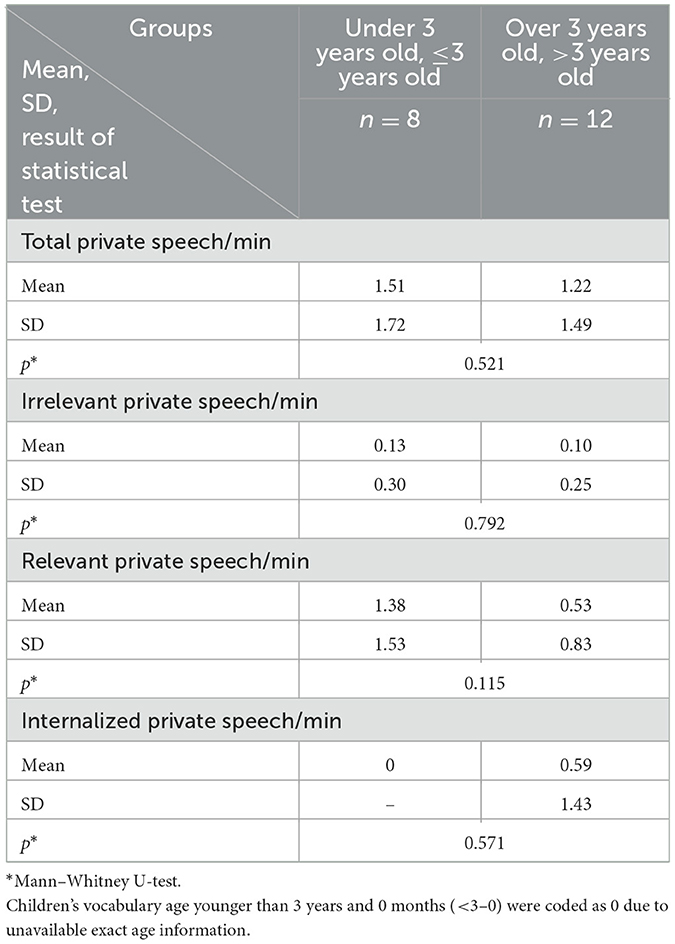
Table 5c. Low, Medium, and High-scoring groups across PVT-R (mean, standard deviation, and non-parametric test score).
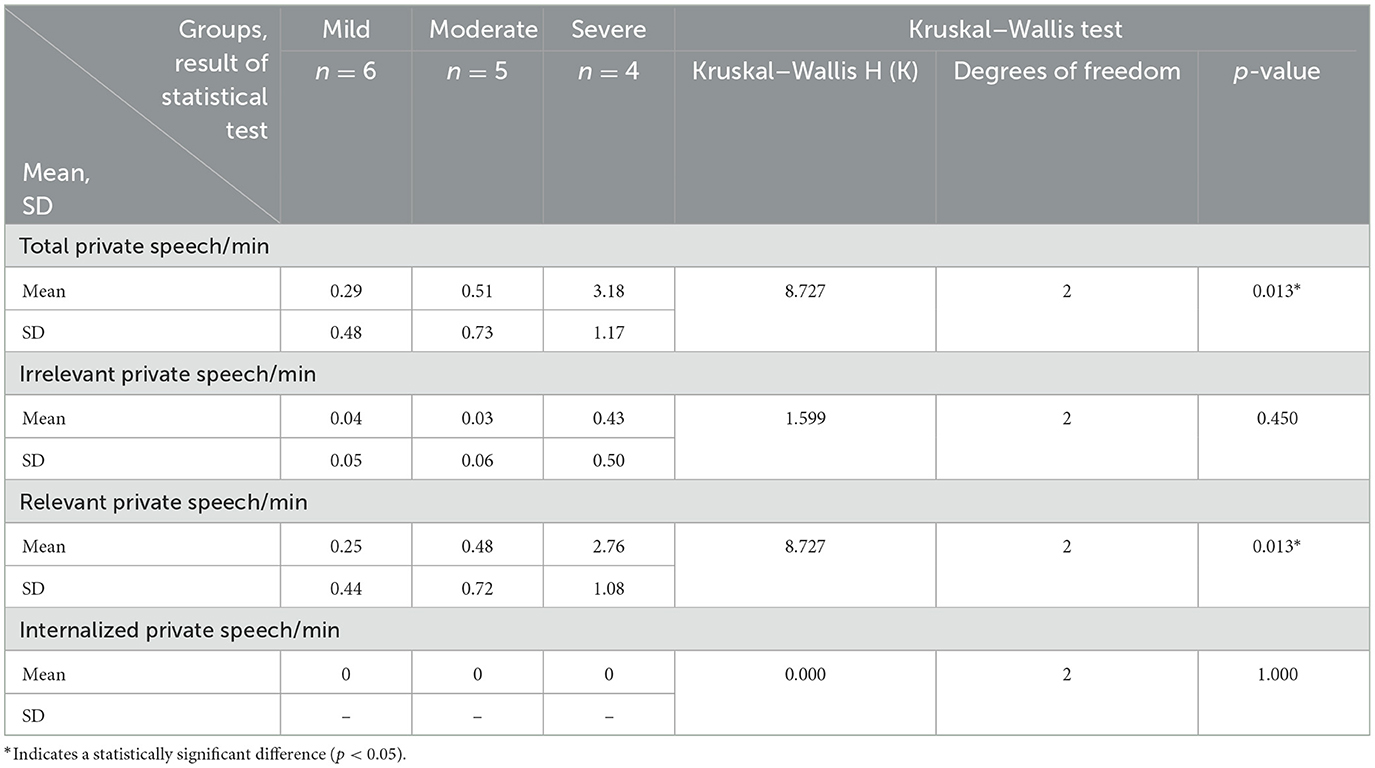
Table 5d. Mild, moderate, and severe-scoring groups across SRS-II (mean, standard deviation, and non-parametric test score).
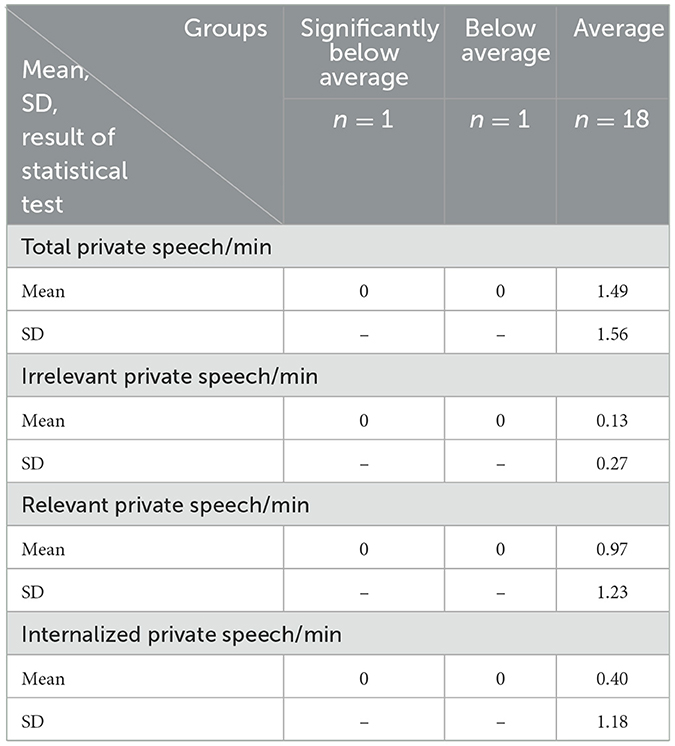
Table 5e. Significantly below average, below average, and average-scoring groups across VINELAND-II (mean, standard deviation).
4.4 Correlation factor and multiple regression analysis
Spearman's rho was calculated to test whether there were possible correlative factors, such as cognitive capacity, that influenced the output of private speech (see Table 6). SRS-II total score were found to have a positive correlation with task-relevant private speech per minute (p = 0.018), suggesting that participants with a higher tendency toward autism utilized more task-relevant private speech during the task.
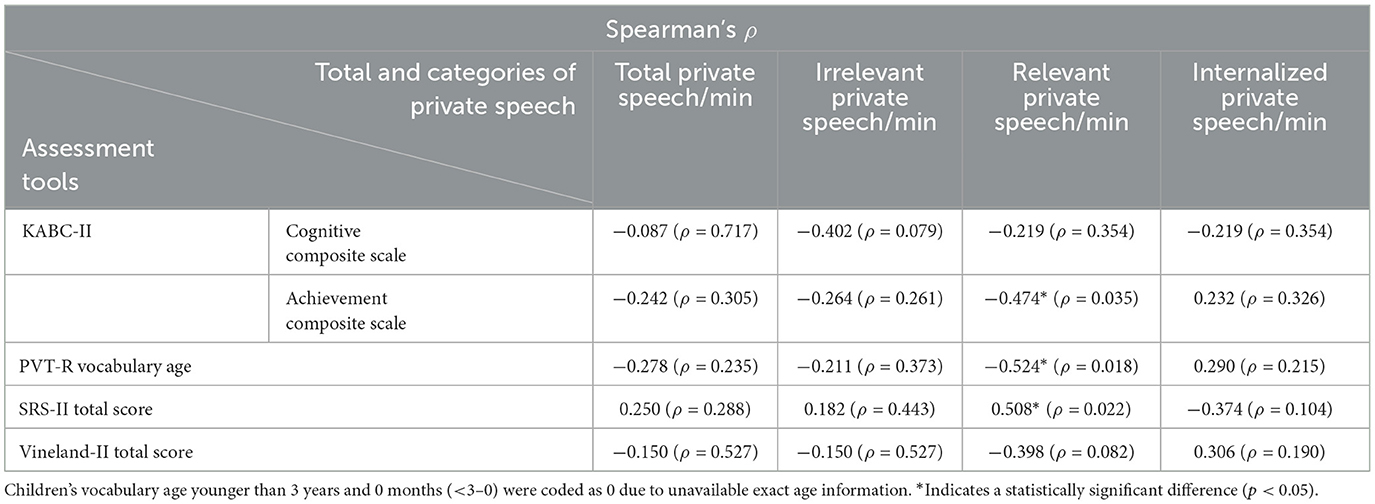
Table 6. Spearman's rank correlation coefficient on KABC-II, PVT-R, SRS-II, and Vineland-II.
Achievement Composite Scale of K-ABC, one of the key components of intellectual skills, showed a negative correlation with task-relevant private speech per minute (p = 0.035), suggesting higher acquisitive skill led to less task-relevant private speech. Furthermore, participants' PVT-R vocabulary age was negatively correlated with task-relevant private speech per minute (p = 0.022), suggesting that participants with more verb maturity used less task-relevant private speech in task-solving.
To further examine the relationship between autism spectrum tendencies (ASD) and task-relevant private speech, a multiple regression analysis was conducted using ASD, chronological age and vocabulary age (as measured by the PVT-R) as predictors. The full model was statistically significant, F(3, 16) = 7.515 p = 0.002, explaining ~60% of the variance in the use of task-relevant private speech (adjusted R2 = 0.507). ASD tendencies demonstrated a strong and statistically significant positive association with private speech (standardized β = 0.688, p = 0.003), indicating that higher levels of ASD traits were associated with increased use of self-directed speech during task performance. In contrast, neither chronological age (β = −0.217, p = 0.208) nor vocabulary age (β = −0.077, p = 0.705) were significant predictors (see Table 7). These results suggest that the observed relationship between ASD tendencies and private speech is not confounded by developmental or linguistic factors. Instead, ASD tendencies appear to independently influence the emergence or persistence of private speech in cognitive tasks, consistent with prior findings highlighting the distinct cognitive and self-regulatory strategies observed in individuals with higher autistic traits (Winsler et al., 2007; Lidstone et al., 2012). Although, conducting a multiple regression analysis with 20 participants and three predictors results in a low participant-to-predictor ratio, which compromises the reliability and stability of the findings. Additionally, the small sample size limits the ability to adequately assess and validate the assumptions underlying the regression model. Therefore, this analysis is primarily exploratory in nature and is complemented by visualizations that illustrate the relationships among variables and highlight any potential outliers (see Figures 2–4).
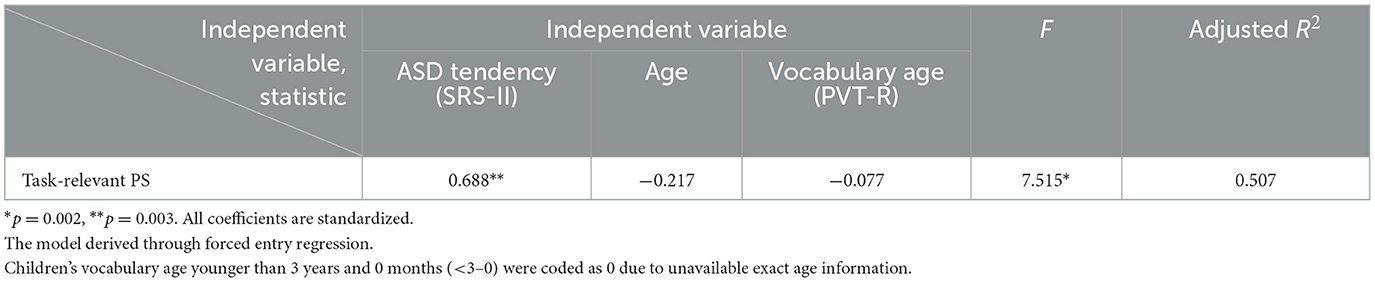
Table 7. Multiple regression analysis of task-relevant private speech.
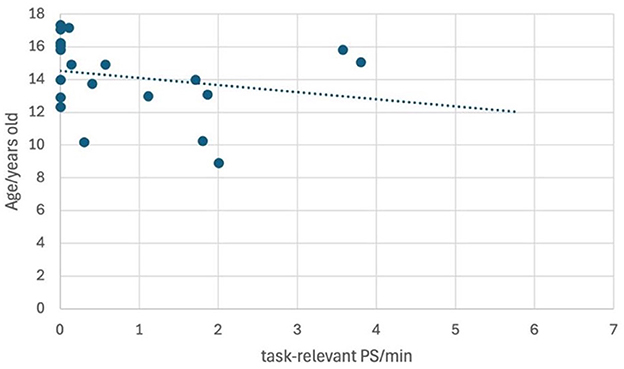
Figure 2. Scatterplot of task-relevant PS and age. Regression line for task-relevant private speech and chronological age: y = −0.4306x + 14.519.
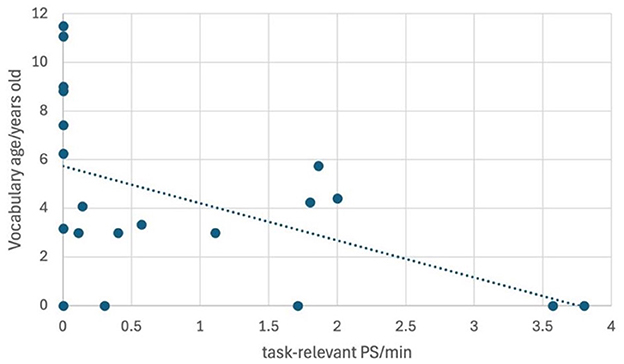
Figure 3. Scatterplot of task-relevant PS and vocabulary age (PVT-R). Children younger than 3 years and 0 months (<3–0) were coded as 0 due to unavailable exact age information. Regression line for task-relevant private speech and vocabulary age: y = −1.5233x + 5.7269.
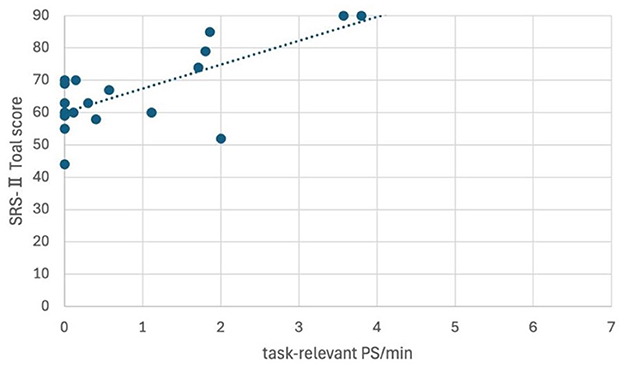
Figure 4. Scatterplot of task-relevant PS and ASD characteristics (SRS-II). Regression line for task-relevant private speech and SRS- II score: y = −0.4306x + 14.519. Children labeled with an SRS-II total score of 90 had actual scores equal to or >90.
5 Discussion
5.1 Private speech of children with IDs
This study aimed to examine whether children with intellectual disabilities (IDs) engage in private speech during task performance. Findings revealed that 70% of participants used private speech, indicating its prevalence as a self-regulatory tool within this population. Exploratory multiple regression analysis showed that neither chronological age nor vocabulary age significantly predicted private speech use, suggesting that its development may occur independently of general developmental indicators.
Moreover, intellectual functioning—as measured by the Cognitive Composite Scale and Achievement Composite Scale of the K-ABC—did not significantly affect private speech usage, as determined by the Mann–Whitney U-test. These results support the view that private speech may represent a developmentally robust self-regulatory mechanism that emerges regardless of cognitive ability. It may remain accessible to children with varying levels of intellectual functioning, underscoring its potential role in supporting learning and task engagement.
Additionally, 67% of participants identified as having ASD according to the SRS-2 used private speech during the task, a figure comparable to the 70% reported in Winsler et al.'s (2007) study of children with high-functioning ASD. This suggests that ~70% of children with ASD—regardless of the presence of an intellectual disability—engage in private speech during problem-solving tasks.
The second purpose was to uncover the characteristics of the private speech of children with ID. Participant's language development was found to negatively correlate with task-relevant private speech in the selective attention task, as well as with the Achievement Composite Scale of K-ABC. If higher verbal skills can help children better understand the task and lead them to solve it more easily, the use of private speech as a verbal tool to deal with difficulties can be relatively reduced. Further, participants with higher acquisitive skills could comprehend the essence of the task more effortlessly, so they could complete the task smoothly without or with less help from the verbal tool.
Additionally, according to Berk's categories of private speech, the level 2 task-relevant externalized private speech and task-relevant self-answered questions subtype is used by typically developing children during tasks (Kohlberg, 1968; Berk and Garvin, 1984; Berk, 1986). However, this subtype was not observed in the present study. Instead, some participants used task-relevant self-questions without providing vocalized answers. It remains unclear if this pattern constitutes a special form of private speech unique to children with IDs, as there are no previous studies for comparison. Given that private speech is for internal purposes, it is quite possible that children raised one question vocally and then did not say the answer out loud, as they already knew it in their minds. Future studies could explore the subtypes of private speech in children with IDs to determine the potential differences compared to populations.
5.2 Comparisons with research on typical developing children
Studies on the private speech of typically developing children have found that private speech peaks during the preschool years and is gradually replaced by partially internalized private speech, such as inaudible muttering, as children move to early primary school (Kohlberg et al., 1968; Berk, 1986; Winsler et al., 2003). However, for the participants with IDs in this study, the developmental process of private speech appears slower and extends across a wider age range, spanning from primary school to senior high school (from 8 to 17 years old).
From the perspective of Berk's three levels of private speech internalization, typically developing children initially use immature level 1 task-irrelevant private speech, such as word play and repetition; task-irrelevant affect expressions; and comments to absent, imaginary, or non-human entities. As they develop, children use more mature and task-relevant level 2 private speech, including describing one's own activities, task-relevant self-answered questions, self-guiding comments, reading aloud and sounding out words, and task-relevant affect expressions. Ultimately, private speech turns into level 3 partially internalized speech, consisting of inaudible muttering and silent lip and tongue movement.
For children with IDs in this study, all three types of level 1 task-irrelevant private speech were observed in the junior high school group (12–11 to 14–11 years old). For level 2 private speech, the task-relevant self-answered questions subtype was not observed. Instead, task-relevant self-answered questions without answers were noted in both the elementary (8–11 to 12–4 years old) and junior high school groups (12–11 to 14–11 years old). For level 3 partially internalized private speech, only two participants (one in elementary school and one in senior high school) produced inaudible muttering during the task. Considering the small sample size and diverse diagnostic backgrounds of participants, it is hard to draw definitive conclusions about whether children with IDs use the same subtypes of private speech as typically developing children. Nevertheless, the participants with IDs in this study indeed showed similar usage of private speech to that of typically developing children.
5.3 Comparisons with research on other developmental disorders
The current findings revealed a positive correlation between SRS-2 scores and task-related private speech during the selective attention task, suggesting that participants with intellectual disabilities (IDs) who exhibited stronger ASD tendencies engaged in more private speech than those with milder ASD characteristics. While this might initially appear to contradict existing literature, it may be better understood in the context of how individuals with ASD utilize verbal strategies for cognitive regulation. Previous research has consistently demonstrated that individuals with ASD tend to rely less on inner speech during complex cognitive tasks. For example, Williams et al. (2012) reported a reduced use of inner speech for planning among individuals with ASD, while Joseph et al. (2005) found that individuals on the spectrum did not spontaneously engage in inner speech even when processing nameable stimuli. These findings suggest that the verbal mediation of working memory is often impaired or underutilized in this population.
From a Vygotskian perspective, private speech emerges in early childhood as a tool for self-regulation and gradually internalizes into inner speech as cognitive functions mature. In typically developing children, this progression allows for increasingly efficient internal verbal mediation. However, for individuals with ASD, this developmental transition may be delayed or disrupted, leading to continued reliance on overt private speech into later developmental stages. In this context, the increased frequency of private speech observed in individuals with stronger ASD traits may reflect a compensatory mechanism, wherein private speech serves as an external scaffold to support attention and task performance due to the inefficacy of inner speech.
The implications of this interpretation are both theoretical and practical. From a theoretical standpoint, it underscores the necessity of revisiting assumptions about the normative trajectory of private-to-inner speech development, particularly in neurodiverse populations. Practically, the findings suggest that encouraging private speech in educational and therapeutic contexts may benefit children with ASD and IDs by enhancing cognitive regulation and task performance. Interventions that validate and support the use of externalized verbal strategies could serve as an effective scaffold for executive functioning. Future research should explore the integration of private speech–based strategies into individualized education plans and therapeutic protocols for children with developmental disorders.
Additionally, this study found a negative correlation between language development and task-relevant private speech. This contrasts with findings in ADHD populations, where private speech usage appears independent of verbal ability. For example, Andreou et al. (2005) noted diminished language skills in children with ADHD, yet Corkum et al. (2008) reported similar problem-solving performance to typically developing peers. In ADHD populations, private speech—particularly task-relevant and task-irrelevant external private speech—is more frequent than in typically developing children (e.g., Copeland, 1979; Zentall et al., 1983; Berk and Potts, 1991; Berk and Landau, 1993; Winsler, 1998; Kopecky et al., 2005; Corkum et al., 2008). Benedetto-Nasho (2001), for instance, found that 87% of children with ADHD used both forms of private speech during a math task, compared to only 30–40% in the control group.
In the present study, 60% of the participants produced task-relevant external private speech and 30% used task-irrelevant private speech in the problem-solving task (see Table 3a). These results suggest that children with IDs also use private speech as a regulatory tool, particularly during problem-solving. However, the relatively lower frequency of task-irrelevant speech compared to ADHD populations may reflect differing attentional profiles. Children with ADHD are more prone to distraction, potentially resulting in more off-task verbalizations. In contrast, children with IDs may demonstrate greater task persistence or task-irrelevant speech may be less detectable due to methodological limitations.
Collectively, these findings highlight the importance of understanding private speech as a dynamic and context-dependent cognitive tool, rather than as a uniform developmental marker. The patterns observed in this study underscore the need for population-specific frameworks that account for the diverse functions and developmental trajectories of private speech across neurodevelopmental conditions. Continued investigation is warranted to delineate the mechanisms underlying private speech use further and to inform the design of targeted interventions that leverage its regulatory potential in children with developmental disabilities.
5.4 Practical applications in educational settings
In special needs schools, a lack of understanding regarding children's private speech remains a concern. It is frequently observed that teachers interrupt students' private speech during class or discourage it by telling them that such behavior is inappropriate. As a result, children may refrain from using private speech spontaneously or come to perceive it negatively. Moreover, although many teachers are familiar with echolalia, private speech is often misunderstood as being synonymous with echolalia—merely meaningless repetition of sounds. Consequently, when teachers hear private speech that resembles echolalia, they may respond by asking the child to stop.
To address these issues, it is essential to distinguish clearly between echolalia and private speech and to inform teachers about the functions and significance of private speech. Children with intellectual disabilities also engage in private speech, which plays an important role in self-regulation and serves as a cognitive tool for problem-solving. By enhancing teachers' accurate understanding of both echolalia and private speech, it is expected that they will be better equipped to interpret children's verbal behavior appropriately and to provide more effective and supportive educational guidance.
5.5 Limitations
Considering the characteristics of IDs, particularly the delayed development of language acquisition, this study was conducted across a wide age range, from elementary to high school, to examine the relationship between language ability and private speech. Although the number of participants was small, valuable data were obtained. In future research, it would be beneficial to increase the number of participants and explore more potential characteristics of private speech in children with IDs.
Moreover, considering that many children with IDs have co-occurring conditions, such as ASD, this study investigated the impact of ASD tendencies on private speech. It is possible that as a coexisting factor, autistic tendencies influence the cognitive capability and receptive language ability of children, leading to different outputs of private speech in problem-solving tasks among these children compared with those who only have IDs. This study did not compare the differences between the pure ID group and the group that also had autistic tendencies. Further studies could focus on this challenging point by collecting two sample groups (pure ID group and group with both ID and ASD) and exploring whether there are different outputs of private speech during problem-solving tasks, such as selective attention tasks in the present study.
Third, future studies should consider the influence of tasks on private speech. Problem-solving tasks, such as the selective attention task used in the present study, may more easily elicit private speech, whereas other tasks (e.g., behavioral inhibition tasks) may not (Diaz, 1992; Winsler et al., 1997; Winsler, 1998; Winsler et al., 2003). Additionally, different task types may stimulate different subcategories of private speech. Corkum et al. (2008) indicated that individuals diagnosed with ADHD demonstrated distinct behavioral manifestations corresponding to varying stages of curvilinear progression from overt to internalized forms of private speech when performing problem-solving or behavioral inhibition tasks. The study's findings revealed that problem-solving tasks prompted more overt, task-irrelevant forms of internalized speech, while behavioral inhibition tasks elicited more task-relevant, partially internalized speech. Therefore, future studies should utilize two different types of tasks within the Zone of Proximal Development in children with IDs and/or ADHD/ASD to explore whether there are distinct outcomes.
Fourth, one key limitation of this study is the small sample size, which resulted in a low participant-to-predictor ratio in the multiple regression analysis (20 participants and three predictors). This compromises the reliability and stability of the regression coefficients and limits the statistical power to detect meaningful effects. Additionally, the limited sample size restricts the ability to thoroughly assess and validate the assumptions of the regression model. As such, the regression analysis should be interpreted as exploratory, and its findings are best understood in conjunction with visual representations that depict the relationships among variables and identify potential outliers.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Institute of Human and Social Sciences Ethics Committee of Kanazawa University. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
YN: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. YY: Conceptualization, Methodology, Project administration, Writing – review & editing. MY: Investigation, Writing – review & editing. MK: Funding acquisition, Writing – review & editing. HK: Conceptualization, Methodology, Project administration, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the JST Center of Innovation (COI) (grant number: JPMJCA2207).
Acknowledgments
We would like to express our gratitude to the following organizations and individuals for their invaluable support in completing this research project. First, we would like to thank the Affiliated School for Special Needs Education of Kanazawa University for providing the necessary facilities and resources to conduct our research. Second, we want to express our heartfelt thanks to all the staff at the Research Center for Child Mental Development for their cooperation and kind support throughout my research period. We would also like to extend our sincere gratitude for the support provided by the Next Generation Researcher Development Project for their financial assistance.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5™. Task force, DSM-5, 5th Edn. Arlington, VA: American Psychiatric Publishing, Incorporated. doi: 10.1176/appi.books.9780890425596
Andreou, G., Agapitou, P., and Karapetsas, A. (2005). Verbal skills in children with ADHD. Eur. J. Spec. Needs Educ. 20, 231–238. doi: 10.1080/08856250500055743
Aro, T., Poikkeus, A.-M., Laakso, M.-L., Tolvanen, A., and Ahonen, T. (2015). Associations between private speech, behavioral self-regulation, and cognitive abilities. Int. J. Behav. Dev. 39, 508–518. doi: 10.1177/0165025414556094
Behrend, D. A., Rosengren, K., and Perlmutter, M. (1989). A new look at children's private speech: the effects of age, task difficulty, and parent presence. Int. J. Behav. Dev. 12, 305–320. doi: 10.1177/016502548901200302
Benedetto-Nasho, E. A. (2001). Use of Private Speech During Math Computation in Children With Attention Deficit Hyperactivity Disorder: Methodological Challenges, Task Performance and Effects of Stimulant Medication (dissertation). University of Toronto, Toronto, ON, Canada.
Berk, L. E. (1986). Relationship of elementary school children's private speech to behavioral accompaniment to task, attention, and task performance. Dev. Psychol. 22, 671–680. doi: 10.1037/0012-1649.22.5.671
Berk, L. E., and Garvin, R. A. (1984). Development of private speech among low-income Appalachian children. Dev. Psychol. 20, 271–286. doi: 10.1037/0012-1649.20.2.271
Berk, L. E., and Landau, S. (1993). Private speech of learning disabled and normally achieving children in classroom academic and laboratory contexts. Child Dev. 64, 556–571. doi: 10.2307/1131269
Berk, L. E., and Potts, M. K. (1991). Development and functional significance of private speech among attention-deficit hyperactivity disordered and normal boys. J. Abnorm. Child Psychol. 19, 357–377. doi: 10.1007/BF00911237
Berk, L. E., and Spuhl, S. T. (1995). Maternal interaction, private speech, and task performance in preschool children. Early Childh. Res. Quart. 10, 145–169. doi: 10.1016/0885-2006(95)90001-2
Bivens, J. A., and Berk, L. E. (1990). A longitudinal study of the development of private speech in preschool children. Early Child. Res. Q. 5, 43–66. doi: 10.1016/0885-2006(90)90011-E
Copeland, A. P. (1979). Types of private speech produced by hyperactive and nonhyperactive boys. J. Abnorm. Child Psychol. 7, 169–177. doi: 10.1007/BF00918897
Corkum, P., Humphries, K., Mullane, J. C., and Theriault, F. (2008). Private speech in children with ADHD and their typically developing peers during problem-solving and inhibition tasks. Contemp. Educ. Psychol. 33, 97–115. doi: 10.1016/j.cedpsych.2006.12.003
Deutsch, R., and Stein, A. (1972). The effects of personal responsibility and task interruption on the private speech of preschoolers. Hum. Dev. 15, 310–324. doi: 10.1159/000271253
Diaz, R. M. (1992). “Methodological concerns in the study of private speech,” in [Private Speech]. From Social Interaction to Self-Regulation, eds. R. M. Diaz, and L. E. Berk (Hillsdale, NJ: Lawrence Erlbaum Associates, Incorporated), 55–81.
Dickie, J. (1973). [Private speech] The Effect of Presence of Others, Task and Interpersonal Variables (dissertation). Michigan State University, East Lansing, MI, United States.
Duncan, R. M., and Pratt, M. W. (1997). Microgenetic change in the quantity and quality of preschoolers' private speech. Int. J. Behav. Dev. 20, 367–383. doi: 10.1080/016502597385388
Feigenbaum, P. (2009). “Development of communicative competence through private and inner speech,” in Private Speech, Executive Functioning, and the Development of Verbal Self-Regulation, eds. A. Winsler, C. Fernyhough, and I. Montero (Cambridge: Cambridge University Press), 105–120. doi: 10.1017/CBO9780511581533.009
Fernyhough, C., and Fradley, E. (2005). Private speech on an executive task: relations with task difficulty and task performance. Cogn. Dev. 20, 103–120. doi: 10.1016/j.cogdev.2004.11.002
Fernyhough, C., and Russell, J. (1997). Distinguishing one's own voice from those of others: a function for private speech? Int. J. Behav. Dev. 20, 651–665. doi: 10.1080/016502597385108
Japanese Version KABC-II Production Committee. (2013). KABC-II Manual. Japanese Version. Tokyo: Maruzen Publishing Co, Ltd.
Joseph, R. M., Steele, S. D., Meyer, E., and Tager-Flusberg, H. (2005). Self-ordered pointing in children with autism: failure to use verbal mediation in the service of working memory? Neuropsychologia 43, 1400–1411. doi: 10.1016/j.neuropsychologia.2005.01.010
Kamikawa, Y. (2017). Japanese Version of the SRS-2 Social Responsiveness Scale Manual. Tokyo: Culture and Science Publishing.
Kaufman, A. S., and Kaufman, N. L. (2004). Kaufman Assessment Battery for Children, Second Edition (KABC-II). Circle Pines, MN: Pearson Assessment.
Kaufman, A. S., and Kaufman, N. L. (2018). Kaufman Assessment Battery for Children, 2nd Edn., Normative Update. Circle Pines, MN: NCS Pearson.
Kohlberg, L. (1968). Early education: a cognitive-developmental view. Child Dev. 39, 1013–1062. doi: 10.2307/1127272
Kohlberg, L., Yaeger, J., and Hjertholm, E. (1968). Private Speech: Four Studies and a Review of Theories. Child Dev. 39, 691–736. doi: 10.2307/1126979
Kopecky, H., Chang, H. T., Klorman, R., Thatcher, J. E., and Borgstedt, A. D. (2005). Performance and private speech of children with attention-deficit/hyperactivity disorder while taking the Tower of Hanoi test: effects of depth of search, diagnostic subtype, and methylphenidate. J. Abnorm. Child Psychol. 33, 625–638. doi: 10.1007/s10802-005-6742-7
Lidstone, J., Meins, E., and Fernyhough, C. (2011). Individual differences in children's private speech: consistency across tasks, timepoints, and contexts. Cogn. Dev. 26, 203–213. doi: 10.1016/j.cogdev.2011.02.002
Lidstone, J. S., Meins, E., and Fernyhough, C. (2012). Verbal mediation of cognition in children with specific language impairment. Dev. Psychopathol. 24, 651–660. doi: 10.1017/S0954579412000223
Luria, A. R. (1961). The Role of Speech in the Regulation of Normal and Abnormal Behavior. New York, NY: Liveright.
Manfra, L., and Winsler, A. (2006). Preschool children's awareness of private speech. Int. J. Behav. Dev. 30, 537–549. doi: 10.1177/0165025406072902
Montero, I., and De Dios, M. J. (2006). Vygotsky was right. An experimental approach to the relationship between private speech and task performance. Estud. Psicol. 27, 175–189. doi: 10.1174/021093906777571709
Mulvihill, A., Carroll, A., Dux, P. E., and Matthews, N. (2020). Self-directed speech and self-regulation in childhood neurodevelopmental disorders: current findings and future directions. Dev. Psychopathol. 32, 205–217. doi: 10.1017/S0954579418001670
Mulvihill, A., Matthews, N., Dux, P. E., and Carroll, A. (2021). Preschool children's private speech content and performance on executive functioning and problem-solving tasks. Cogn. Dev. 60:101116. doi: 10.1016/j.cogdev.2021.101116
Patrick, E., and Abravanel, E. (2000). The self-regulatory nature of preschool children's private speech in a naturalistic setting. Appl. Psycholinguist. 21, 45–61. doi: 10.1017/S014271640000103X
Pellegrini, A. D. (1981). The development of preschoolers' private speech. J. Pragmat. 5, 445–458. doi: 10.1016/0378-2166(81)90028-X
Schalock, R. L., Keith, K. D., Verdugo, M. A., and Gomez, L. E. (2010). “Quality of life model development and use in the field of intellectual disability,” in Quality of Life: Theory and Implementation, ed. R. Kober (New York, NY: Sage), 17–32.
Sparrow, S. S., Cicchetti, D. V., and Saulnier, C. A. (2016). Vineland Adaptive Behavior Scales, 3rd Edn. San Antonio, TX: Pearson Assessments.
Sturn, A., and Johnston, J. (1999). Thinking out loud: an exploration of problem-solving language in preschoolers with and without language impairment. Int. J. Lang. Commun. Disord. 34, 1–15. doi: 10.1080/136828299247586
Tsuji, M., and Murakami, T., (eds.). (2014). Vineland-II Adaptive Behavior Scales Manual. Japanese Version. Tokyo: Japan Culture and Science Publishing.
Ueno, K., Nagoshi, S., and Onuki, S. (1991). PVT: Picture Vocabulary Test Manual. Tokyo: Nihon Bunka Kagakusha.
Ueno, K., Nagoshi, S., and Onuki, S. (2008). PVT-R Picture Vocabulary Development Test Manual. Tokyo: Japan Society for the Promotion of Science.
Vygotsky, L. S., and Luria, A. (1930/1993). Studies on the History of Behavior. Ape, Primitive, and Child. Hillsdale, NJ: Erlbaum.
Williams, D. M., Bowler, D. M., and Jarrold, C. (2012). Inner speech is used to mediate short-term memory, but not planning, among intellectually high-functioning adults with autism spectrum disorder. Dev. Psychopathol. 24, 225–239. doi: 10.1017/S0954579411000794
Winsler, A. (1998). Parent–child interaction and private speech in boys with ADHD. Appl. Dev. Sci. 2, 17–39. doi: 10.1207/s1532480xads0201_2
Winsler, A., Abar, B., Feder, M. A., Schunn, C. D., and Rubio, D. A. (2007). Private Speech and executive functioning among high-functioning children with autistic spectrum disorders. J. Autism Dev. Disord. 37, 1617–1635. doi: 10.1007/s10803-006-0294-8
Winsler, A., De León, J. R., Wallace, B. A., Carlton, M. P., and Willson-Quayle, A. (2003). Private speech in preschool children: developmental stability and change, across-task consistency, and relations with classroom behaviour. J. Child Lang. 30, 583–608. doi: 10.1017/S0305000903005671
Winsler, A., Diaz, R. M., Atencio, D. J., McCarthy, E. M., and Adams Chabay, L. (2000). Verbal self-regulation over time in preschool children at risk for attention and behavior problems. J. Child Psychol. Psychiatry 41, 875–886. doi: 10.1111/1469-7610.00675
Winsler, A., Díaz, R. M., Espinosa, L., and Rodríguez, J. L. (1999). When learning a second language does not mean losing the first: bilingual language development in low-income, Spanish-speaking children attending bilingual preschool, Spanish. Child Dev. 70, 349–362. doi: 10.1111/1467-8624.t01-1-00026
Winsler, A., Diaz, R. M., and Montero, I. (1997). The role of private speech in the transition from collaborative to independent task performance in young children. Early Childh. Res. Quart. 12, 59–79. doi: 10.1016/S0885-2006(97)90043-0
Winsler, A., and Naglieri, J. (2003). Overt and covert verbal problem-solving strategies: developmental trends in use, awareness, and relations with task performance in children aged 5 to 17. Child Dev. 74, 659–678. doi: 10.1111/1467-8624.00561
Zentall, S. S., Gohs, D. E., and Culatta, B. (1983). Language and activity of hyperactive and comparison children during listening tasks. Except. Child. 50, 255–266. doi: 10.1177/001440298305000309
Keywords: private speech, intellectual disability, language development, autism spectrum disorder, self-regulation, school-based research
Citation: Niu Y, Yoshimura Y, Yoshioka M, Kikuchi M and Kobayashi H (2025) Private speech among children with intellectual disabilities. Front. Dev. Psychol. 3:1607706. doi: 10.3389/fdpys.2025.1607706
Received: 08 April 2025; Accepted: 19 June 2025;
Published: 16 July 2025.
Edited by:
Catherine Sandhofer, University of California, Los Angeles, United StatesReviewed by:
Niek Frans, University of Groningen, NetherlandsMargherita Siciliano, University of Campania Luigi Vanvitelli, Italy
Copyright © 2025 Niu, Yoshimura, Yoshioka, Kikuchi and Kobayashi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ye Niu, bnluaXV5ZUBnbWFpbC5jb20=