 Alison K. Ventura*
Alison K. Ventura* Alondra RossiMolly M. RyderGabriella M. ThomasSammy EaddyKarla I. Ceja AlmontesCynthia L. Diaz
Alondra RossiMolly M. RyderGabriella M. ThomasSammy EaddyKarla I. Ceja AlmontesCynthia L. Diaz- The Healthy Kids Lab, Center for Health Research, Department of Kinesiology and Public Health, Bailey College of Science and Mathematics, California Polytechnic State University, San Luis Obispo, CA, United States
Observational studies of caregiver-infant feeding interactions are necessary for understanding early relational dynamics, infant behavior, and developmental trajectories. However, traditional in-person observation methods pose logistical and access-related barriers, particularly for families with limited resources. In this article, we provide a comprehensive guide for conducting remote observations of caregiver-infant feeding interactions using virtual home visits, with a focus on feasibility, equity, and data quality. Drawing on recent technological advances and lessons from implementation, we outline practical strategies for scheduling, participant preparation, technology setup, and researcher management of virtual visits. We also address common challenges related to video quality, audio fidelity, camera framing, internet connectivity, and environmental distractions. Recommendations include using common videoconferencing platforms (e.g., Zoom), piloting device setup, minimizing participant burden, using scripting to reduce bias, and actively managing technical limitations. When implemented thoughtfully, remote protocols can yield high-quality, ecologically valid data across diverse populations, making remote caregiver-infant feeding observations a viable alternative to in-person assessments. This article offers researchers and clinicians an adaptable framework for conducting reliable, accessible, and family-centered virtual feeding observations.
1 Introduction
Observations of caregiver-infant feeding interactions are a window into the quality of caregiver-infant relationships and the presence of risk and protective factors that may shape early development (D'Angeli et al., 2022; Pesch and Lumeng, 2017). Feeding interactions are central during early caregiving experiences because young infants feed frequently−8 to 12 times per day, or more—and most of caregivers' early experiences of caring for their infants focus on the interconnected domains of feeding, soothing, and sleep. As infants mature, their feeding frequency decreases, but their feeding experiences become more varied and dynamic as they transition from an exclusively milk-based diet to a more complex diet comprised of complementary foods and beverages (Grummer-Strawn et al., 2008). Thus, observing caregivers and infants during feeding interactions allows researchers to assess caregiver and infant behavior within contexts that are familiar, relevant, and impactful for infant development (D'Angeli et al., 2022; Gardner, 2000). In addition, there is a longstanding precedent for leveraging early feeding interactions to assess constructs relevant to broader child development, such as caregiver-child behavioral contingency and synchrony, caregiver sensitivity and responsiveness to infant cues, attachment, and markers of physical, cognitive, social and emotional growth (Ainsworth and Bell, 1969; Brown et al., 2009; Chatoor et al., 1998; Hodges et al., 2013, 2016; MacPhee and Schneider, 1996; Oxford and Findlay, 2015; Price, 1983; Toporoff and Story, 1997).
1.1 Theoretical frameworks for understanding the significance of feeding interactions
Although a primary application of direct observations of caregiver-infant feeding interactions is to obtain objective measures of caregiver feeding practices, infant eating behaviors, and the amounts and types of foods infants consume, the impact of early feeding interactions extends beyond the provision of nutrients. Feeding interactions provide numerous opportunities for socioemotional and cognitive growth fostering experiences, including early trust and relationship building, mutual regulation, sensory stimulation (e.g., affective touch, closeness), and skill development (Oxford and Findlay, 2015). Thus, the significance of early feeding interactions can be situated within foundational theories of child development, including attachment theory (Bowlby, 1977a,b, 1978), psychosocial development theory (Erikson, 1950), and cognitive development theory (Piaget, 1952), as well as learning (Bandura, 1977; Vygotsky, 1978) and ecological (Bronfenbrenner and Morris, 1998) theories that emphasize the broader social and environmental contexts within which development occurs.
Attachment theory highlights the importance of consistent, sensitive, and responsive caregiving in fostering secure attachments (Bowlby, 1977a,b, 1978). Psychosocial development theory further emphasizes the importance of establishing trust in caregivers during infancy as a foundation for healthy psychosocial development (Erikson, 1950). Feeding is among the earliest and most frequent opportunities for consistent, sensitive, and responsive caregiving; feeding routines characterized by regular access to food and affection help infants develop trust in and attachment toward their caregivers (Ainsworth and Bell, 1969). For this reason, responsive feeding is widely recommended (Perez-Escamilla et al., 2017; United States Department of Agriculture, 2020; World Health Organization et al., 2018) because it contextualizes key features of responsive caregiving – timely responses to hunger and satiation cues, contingent vocalizations, and appropriate physical support – within feeding and mealtime settings (Black and Aboud, 2011; DiSantis et al., 2011; Heller and Mobley, 2019; Hodges et al., 2013). Responsive feeding interactions support infants' abilities to self-regulate intake in response to physiological needs and promote healthy growth trajectories, but also hold the potential to promote secure attachments and healthy psychosocial development (Black and Aboud, 2011; Cormack et al., 2020; DiSantis et al., 2011; Mallan and Miller, 2019).
Early feeding interactions also provide rich opportunities for learning and cognitive development. During the sensorimotor stage of cognitive development, infants learn about the world by interacting with it using their senses and motor skills (Piaget, 1952). Feeding is a complex, multisensory experience that provides opportunities for learning about food and developing feeding skills via repeated experiences with the taste, aromas, and texture of foods; these early experiences help children develop preferences for the flavors and foods common in their families' diets (Black and Aboud, 2011; Ventura and Worobey, 2013). Caregivers can further capitalize on mealtimes as informal teaching contexts in which infants are introduced to broader concepts such as turn-taking, colors, numbers, and object names (e.g., Oxford and Findlay, 2015). The sensory experience of feeding interactions extends to caregiver-child exchanges in visual engagement, vocalizations, olfactory cues, and affective touch. These exchanges support learning and cognitive development but also promote favorable neurobiological processes, such as oxytocin release, synchronization of physiological states, and stress regulation, that, in turn, promote secure attachments and healthy psychosocial development (Duhn, 2010; La Rosa et al., 2024; Montirosso and McGlone, 2020). In these ways, feeding interactions offer a wealth of sensory and cognitive inputs that support both food-related learning and more generalized cognitive and psychosocial development—particularly when caregivers intentionally use these interactions as opportunities for exploration, teaching, and affective touch.
Moreover, the inherently social nature of early feeding interactions makes them rich contexts for sociocultural learning (Anzman-Frasca et al., 2018; Birch, 2016). Vygotsky's sociocultural theory emphasizes that cognitive development is rooted in social interaction and shaped by the cultural tools, symbols, and practices that caregivers share with children (Vygotsky, 1978). Feeding is one of the first daily routines in which infants participate in culturally embedded activities, from the specific foods offered to the rituals and timing of meals (Black and Aboud, 2011). Through shared mealtime experiences, caregivers model culturally relevant behaviors (e.g., the use of utensils, table manners, and food preparation practices) that infants begin to internalize through observation and participation (Anzman-Frasca et al., 2018; Birch, 2016). These routines also provide a natural context for guided participation, in which caregivers scaffold infants' emerging skills by adjusting the level of support they provide (e.g., holding a spoon together, naming foods, or encouraging self-feeding) thereby expanding the infant's zone of proximal development. Over time, repeated exposure to family mealtime patterns fosters not only familiarity with the tastes and textures of culturally valued foods, but also a sense of belonging within the family's social structure. In this way, feeding interactions function as an early apprenticeship in the cultural and social practices that shape identity, communication, and shared meaning.
From a socioecological perspective, feeding interactions occur within broader family, social, community, and societal contexts (Bronfenbrenner and Morris, 1998). While characteristics of the infant (e.g., temperament, clarity of cues) and caregiver (e.g., sensitivity, depression) shape feeding interactions and outcomes, dyadic interactions may also influence and be influenced by broader characteristics of the family (e.g., household size), community (e.g., availability of parent education opportunities), and broader society (e.g., cultural beliefs, family policies) (Davison and Birch, 2001). Thus, observations of feeding interactions may be one component of broader assessments of the interconnected systems that influence infant development. Taken together, feeding observations yield rich data through which researchers can quantify various aspects of caregivers‘ feeding practices and infants' eating behaviors, as well as additional components of caregiver-infant relationship building and infant physical, socioemotional, and cognitive development.
1.2 Challenges of traditional approaches to assessing feeding interactions
Caregiver-report measures are available and commonly used approaches to assess aspects of early feeding interactions, but may be biased by caregivers‘ subjectivity regarding their own or their infants' behaviors, poor recall, or under- or overestimating children's dietary intake (Corcoran and Fischer, 2013; Fisher et al., 2008; Lanigan et al., 2001). Thus, observational measures of feeding interactions are an important methodology for researchers seeking to understand how caregiver-infant interactions influence infant development.
However, observational methods are not without limitations (Gardner, 2000). Traditional face-to-face observational methods can be time-consuming and induce substantial burden on participants because they require families to travel to a researcher's laboratory or require researchers to travel to families' homes. Laboratory-based observations may be more convenient for researchers and offer more control over the observation but may not be ecologically valid. Home-based observations are more convenient for families and increase the ecological validity of the observations but may also yield lower-quality observations due to variations in factors such as lighting or space. In addition, the presence of researchers or cameras may alter the behaviors of caregivers and infants in ways that reduce the validity of the assessment, especially as infants mature and become more aware of their surroundings and responsive to novel people and objects in familiar environments.
Participation in studies that require in-person data collection, either through laboratory or home visits, may also be prohibitive for many families, which may reduce the diversity of studies that include in-person assessments and limit the generalizability of study findings (Nathe et al., 2023). For example, families of infants may feel overwhelmed with the transition to parenthood or their infant care duties, thus may feel unable to participate in studies that require travel to a research site. Families of lower socioeconomic status or living in rural locations may be less able to take time off work or secure transportation for in-person visits (Lecroy et al., 2023). Constraints of busy family schedules may also make it difficult for families to participate in assessments during traditional business hours. Many families may also feel uncomfortable with researchers visiting their home (Nathe et al., 2023). Thus, alternative methods are needed to enable behavioral observations of diverse samples that reduce burden and eliminate disparities in families' abilities to participate.
1.3 Opportunities for remote observation
Advances in the security, quality, and availability of videoconferencing and telehealth technologies provide one promising avenue for alternative methods of behavioral observation. Although use of videoconferencing and telehealth technologies has increased significantly over the past few decades, the COVID-19 pandemic was a catalyst for the widespread adoption of these technologies as an avenue to stay connected for work, school, and social needs during stay-at-home mandates and quarantines (Giansanti, 2023; Koonin et al., 2020; Shaver, 2022). The use of videoconferencing and telehealth technologies has not declined with the resolution of the pandemic and the end of stay-at-home mandates; rather, these technologies remain popular and highly utilized, thus becoming a familiar communication tool for most Americans (Anderson et al., 2021; Giansanti, 2023).
Indeed, many Americans report using videoconferencing regularly for work, school, or social connections (Igielnik, 2022). Recent data from the Pew Research Center illustrates that 97% of American adults own a cell phone and 90% own a smartphone with videoconferencing capabilities (Pew Research Center, 2024b). Additionally, U.S. Census data indicate that 95% of households own a desktop or laptop computer, and 90% have access to broadband internet (Mejía, 2024). Internet use, broadband adoption, and smartphone ownership are not limited to certain sociodemographic groups (Mejía, 2024; Pew Research Center, 2024a,b). Mobile device ownership among lower-income adults has increased significantly over the past decade, resulting in widespread adoption that is no longer dependent on socioeconomic status (Pew Research Center, 2024b). Additionally, lower-income Americans are more likely to rely on their smartphones to access the internet compared to higher-income adults (Pew Research Center, 2024b). Thus, the use of participants' personal laptops, tablets, or smartphones is now a feasible approach for remote observation, even among lower-income families, given the ubiquity of devices with videoconferencing technology and their centrality in daily life.
Previous research has employed remote observations for caregiver-child interactions (Gustafsson et al., 2021; Shin et al., 2021; Tesson et al., 2021; Zaadnoordijk et al., 2021). These studies have used remote observations to assess parent-child play, teaching interactions, and infant neurobehavioral development. Some studies have also integrated infant eye-tracking software with videoconferencing technologies to allow for virtual assessment of infant attention and habituation (Zaadnoordijk et al., 2021). Conducting visits via videoconference increased scheduling flexibility and was shown to be intuitive for most participants (Gustafsson et al., 2021). Remote methods have also facilitated the recruitment of larger and more diverse samples, reduced participant burden, and supported higher retention by lowering travel costs, minimizing physical barriers, and increasing convenience (Tesson et al., 2021). Importantly, they allow for observation in natural environments without the presence of unfamiliar research personnel or equipment, enhancing ecological validity. Despite these benefits, researchers must also consider the challenges associated with remote observations, including variability in video and audio quality, potential technology issues, and maintaining data security and privacy.
Although there is a longstanding precedent for observing caregiver-infant feeding interactions to understand both mealtime dynamics and broader aspects of the caregiver-infant relationship, there are relatively few published examples of using videoconferencing technology for this purpose. A small but growing body of research demonstrates the promise of remote observation of feeding interactions. For instance, recent research has shown that remote video-feedback interventions can effectively enhance the quality of caregiver-child feeding interactions and reduce disordered eating symptoms in children (Cimino and Cerniglia, 2024). Additionally, narrative reviews of observational tools support their adaptation to remote formats with promising validity and feasibility (D'Angeli et al., 2022). In this paper, we describe our experience adapting in-person observation protocols to videoconferencing contexts, outline the protocols we have found lead to high-quality observations, review preliminary evidence of the reliability, validity and quality of these data, discuss the strengths and limitations of this approach, and share lessons learned. The methods and insights shared within this manuscript reflect our research team's extensive experience conducting feeding observations within laboratory, home, and virtual settings and analyzing videos of these feeding observations via behavioral coding methods (Alvarez Gutierrez and Ventura, 2021; Golen and Ventura, 2015; Ventura et al., 2012, 2025; Ventura and Golen, 2015; Ventura et al., 2023; Ventura and Hernandez, 2019; Ventura et al., 2021, 2015, 2019a,b, 2024a,b; Ventura and Mennella, 2017; Ventura and Teitelbaum, 2017). Ultimately, we hope this will serve as a useful guide for researchers and clinicians who wish to incorporate remote caregiver-infant feeding observations into their research studies and practice, as well as a foundation for further research to more systematically quantify the interrater reliability, validity, accuracy, and comparability of remote caregiver-infant feeding observations to in-person observations.
2 Materials and equipment
2.1 Device considerations
Given the ubiquity of mobile device ownership (Mejía, 2024; Pew Research Center, 2024b), using participants' personal devices (e.g., smartphones, laptops, and tablets) is a feasible approach for remote observation, including for families with lower socioeconomic status. Because smartphone ownership exceeds that of laptops and tablets (Mejía, 2024; Pew Research Center, 2024b), smartphones may be the most accessible and feasible option for many participants. Most modern smartphones feature high-quality cameras and microphones, making them suitable for capturing feeding interactions.
However, smartphones can be challenging to position securely for optimal camera angles. One potential solution to this issue is to mail the participant a smartphone tripod before the observation to improve stability and camera angles. In our experience, relatively inexpensive tripods are available and work well at minimal cost to the study. Alternatively, research assistants can guide participants through phone setup before the observation to ensure high-quality video capture.
We have found laptops to be advantageous over smartphones because they naturally provide greater camera stability and flexibility in angling the camera to obtain clear views of the caregiver and infant. Participants may also find it easier to use and interact with videoconferencing software on their laptops compared to smartphones. However, a potential limitation of this approach is that families of lower socioeconomic status may not own laptops, which may limit their ability to participate.
An additional caveat to using participants' laptops or mobile devices for recording observations is considering whether the participant typically uses their laptop or mobile device for other activities (e.g., entertainment, reading, and work) during typical feeding observations. Previous research has shown that the use of technology during infant feeding is a common occurrence among some caregivers (Coyne et al., 2022; Golen and Ventura, 2015; Ventura et al., 2020; Ventura and Teitelbaum, 2017). For example, in a study of 332 mothers of infants 6 months of age and younger, 40% of mothers reported they often or always watched television while feeding their infant, 37% often or always texted or used apps on a mobile device or tablet, and 21% often or always used a computer (Ventura et al., 2020). Thus, a researcher may inadvertently alter the feeding interaction by occupying the participant's device during a feeding observation. To minimize this risk, researchers can survey participants in advance to determine typical device use during feeding (e.g., Ventura et al., 2020) and request that they use a device least likely to disrupt their usual feeding behaviors.
Despite high rates of device ownership, some families may still lack access to suitable technology or a reliable internet connection. In such cases, researchers may consider loaning low-cost tablets, potentially paired with portable hotspots, to facilitate participation. Equipment could be delivered and retrieved in person or shipped with return instructions. While this approach increases the risk of device loss or damage and requires additional logistical coordination, it may improve access for families with limited resources. Researchers should be prepared to offer technical support, which may necessitate additional staff time for setup and troubleshooting.
2.2 Videoconferencing software considerations and settings
We use Zoom Videoconferencing Software (https://zoom.us), a secure and widely adopted platform that offers end-to-end encryption, waiting room functionality, and password protection. Other secure, HIPAA-compliant videoconferencing platforms are also available and have been used in research contexts (e.g., Cisco Webex, GoToMeeting, and Doxy.me) (Lobe et al., 2020).
Each video session is hosted by a research assistant using an encrypted, password-protected computer within a private research office. Zoom offers meeting encryption by default, along with several other security features. To safeguard participant confidentiality, research assistants generate a unique Meeting ID for each visit and share it only with the designated participant. We recommend enabling the waiting room feature to control access and ensure that only the intended participant joins the session.
Regardless of the platform used, we recommend that researchers pilot-test both video and audio settings before data collection to ensure optimal quality. Capturing the nuances of caregiver speech, infant verbalizations, and subtle feeding sounds requires careful configuration of audio settings. For instance, default noise suppression features may inadvertently filter out meaningful vocalizations or sounds related to feeding in ways that may bias later video coding. Researchers should review and adjust these settings accordingly. Finally, researchers should check for platform updates and verify all security, video, and audio settings before each virtual visit to maintain quality and compliance with institutional data protection protocols.
3 Methods
3.1 Scheduling and preparing participants for the virtual home visit and remote feeding observation
Before each virtual home visit, the research team should engage participants in several preparatory steps to ensure a smooth and successful visit (Figure 1). These steps include: (1) scheduling the visit during a time when the infant typically feeds, (2) ensuring participants have the setup for an effective visit, and (3) conducting structured visit reminders before the scheduled visit.
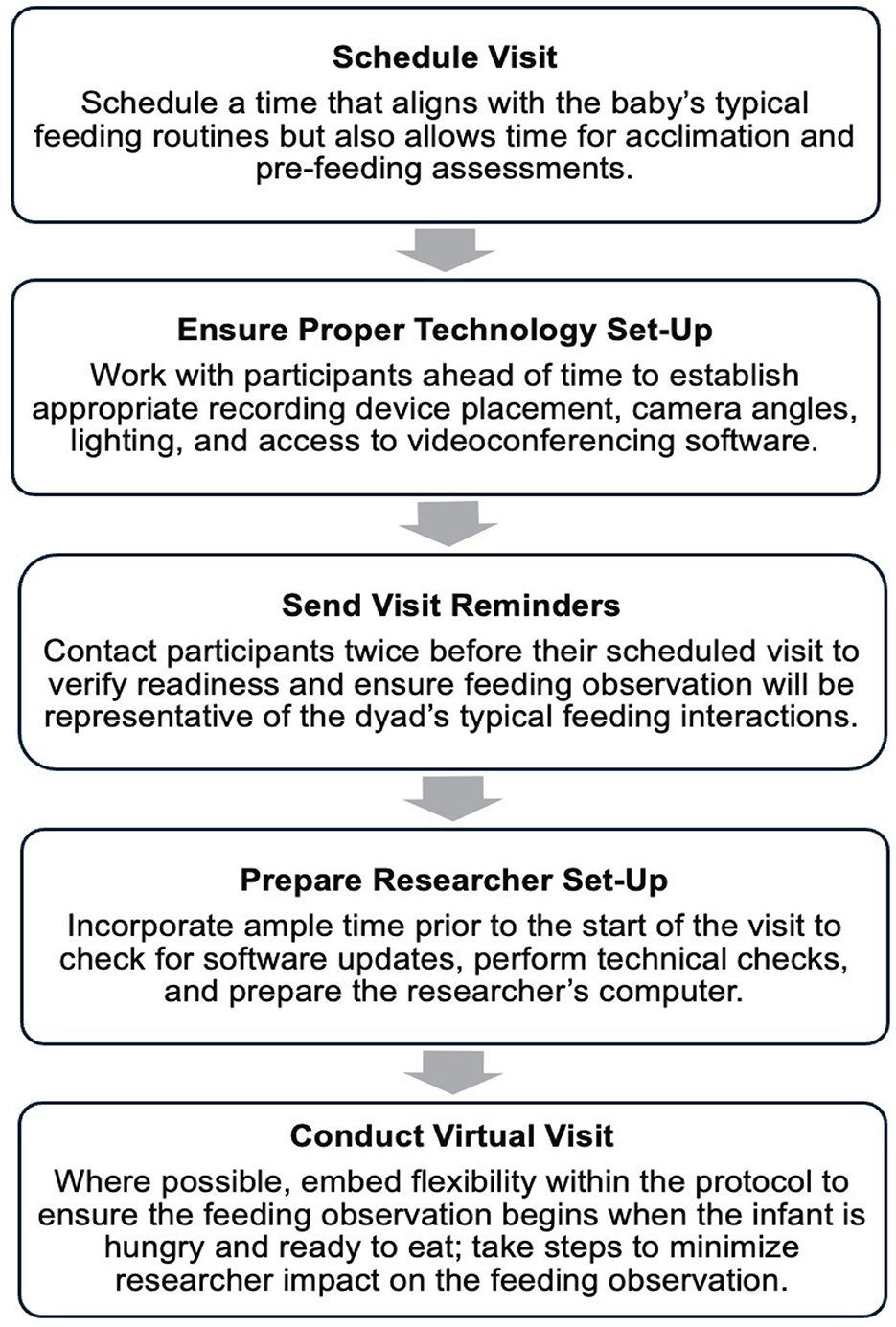
Figure 1. Recommended steps for virtual home visits and remote feeding observations.
3.1.1 Scheduling the visit
Given the variability in infants' feeding and sleeping schedules, we recommend scheduling visits by phone. This approach enables the researcher to collaborate with the caregiver in selecting a time that aligns with the infant's daily feeding patterns, thereby increasing the likelihood of capturing a typical feeding interaction.
To maximize the alignment of the scheduled observation with a typical feeding time, the researcher should ask the caregiver to describe the infant's typical feeding and sleeping schedule. To facilitate this conversation, the researcher may ask open-ended questions, such as: “Could you describe your baby's typical feeding schedule?” or “When does your baby usually sleep and feed throughout the day?” Based on the caregiver's responses, the researcher should aim to schedule the visit ~15–30 min before a typical feeding time. This window should allow enough time for the researcher to welcome the family to the visit, provide an overview of what will occur during the visit, ensure the caregiver and infant are positioned correctly for the feeding observation, and ask initial questions about the feeding before the infant is ready to eat. Attempting to complete these steps while the infant is agitated can be stressful for both the family and the research team and may compromise the quality of the observation. Thus, thoughtful scheduling of the visit is imperative so that the researcher and caregiver can prepare for the feeding observation in a calm environment, ensuring a smooth visit and collecting high-quality data.
During scheduling and follow-up reminder calls, the researcher should inform the caregiver that they can reschedule the visit if the infant's behavior or typical feeding or sleeping patterns change. Common disruptions such as illness, vaccinations, or family events may impact infant behavior. To accommodate these fluctuations, we recommend conducting at least two reminder contacts before the visit to assess for any notable changes and confirm that the originally scheduled time remains appropriate.
3.1.2 Ensuring participants have the proper setup
The researcher should work collaboratively with the caregiver to ensure they are prepared for an effective virtual home visit and remote feeding observation. First, the researcher should have the caregiver identify a suitable location in the home where feeding typically occurs and assess whether the space allows for appropriate lighting and device positioning. As illustrated in Figure 2, adequate lighting is essential for creating high-quality videos that enable video coders to see important aspects of feeding interactions, such as eye contact and facial expressions. Whenever possible, natural lighting (e.g., from a window facing the caregiver-infant dyad) should be used to improve the visibility of both the caregiver's and infant's facial expressions, eye contact, and subtle behaviors. Figure 3 illustrates the ideal angles for smartphones and laptops. While configurations may vary depending on home environments, the ultimate goal is to ensure that both the caregiver and their infant are fully visible in the camera frame.

Figure 2. The effect of better (A) vs. poorer (B) lighting on image quality.
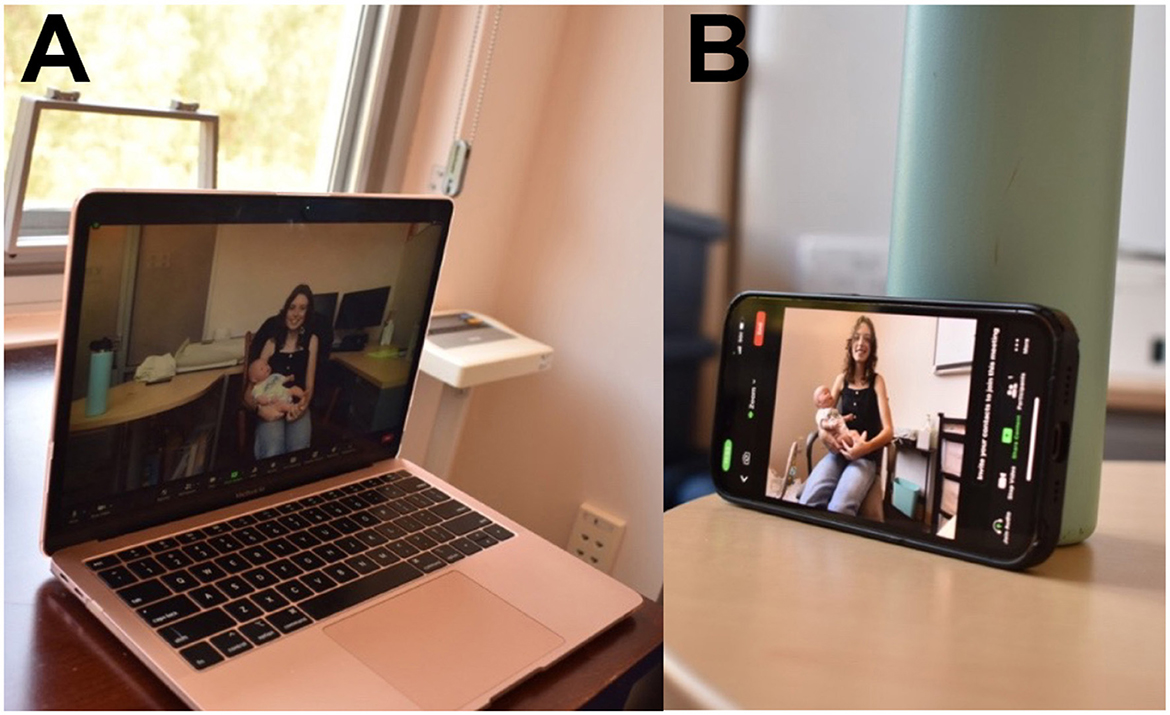
Figure 3. Recommended laptop (A) and smartphone (B) angles.
The videoconferencing software should be installed in advance of the observation. We recommend providing a written handout with detailed instructions for downloading the software, logging in, and resolving common issues. During a setup call, the researcher can guide the caregiver through these written instructions to ensure they successfully install the videoconferencing software on their mobile device or computer. The researcher can then test the software with the participant to verify it is functioning correctly and to troubleshoot any technical issues.
The researcher should consider whether additional instructions should be provided related to food preparation. If the caregiver plans to bottle-feed or give solid foods during the feeding observation, they can be instructed to prepare the bottle or solid foods before the start of the virtual visit and place food items close to where the visit will take place to facilitate a smooth transition between initiating the visit, interacting with the researcher, and starting the feeding observation.
3.1.3 Initial visit reminder (3–5 days before the visit)
Several days before the visit, the researcher should contact the caregiver to confirm the scheduled time and assess whether it still aligns with the infant's feeding routine. It is helpful to ask specific questions about the infant's health and behavior to verify that the infant has not had any experiences that may influence their behavior during the feeding observation, such as recent vaccines, illness, or teething. The researcher can also emphasize that they are interested in observing a typical feeding observation and reschedule the virtual visit if the caregiver indicates any issues or atypical infant behavior.
3.1.4 Final visit reminder (1 day before the visit)
One day before the visit, the researcher should again confirm the visit time and inquire about any last-minute changes in the infant's condition or routine. The researcher should again ask specific questions about the infant's health and behavior to verify that the infant has not had any experiences that may influence their behavior during the feeding observations. The visit should be rescheduled if any of these experiences or alterations in typical behavior are noted. The researcher should reshare the private link to the virtual meeting, review ideal lighting and camera angles, and remind the participant of instructions related to camera setup and food preparation (as discussed during the setup call). Providing structured and supportive reminders helps reduce no-shows, improves the quality of the observation, and enhances the participant experience.
3.2 Researcher setup for effective management of the virtual home visit and remote feeding observation
At least 30–60 min before the scheduled visit, the researcher should complete a series of technical and environmental checks to ensure a smooth and effective virtual visit and remote feeding observation. This preparation period allows the researcher to address any last-minute issues and maintain a professional and confidential environment.
First, the researcher should confirm that the computer and videoconferencing software are functioning correctly. This includes verifying that the video and audio recording features are enabled and working correctly. When using a laptop, the researcher should ensure the battery is fully charged and the device remains plugged in during the session to avoid disruptions. The researcher should work in a quiet, private location to minimize distractions and protect participant confidentiality. Unnecessary applications should be closed to reduce distractions, noise, or pop-up interruptions.
We also recommend that the researcher check the computer for any software or remote platform updates and perform these updates well in advance of the scheduled visit. After updating, the platform should be opened and functionality tested to ensure that the settings (e.g., audio input/output, screen layout, recording permissions) remain properly configured.
It is helpful to open and organize all necessary documents before the visit, including the protocol, scripts, visit checklists, observation guides, survey links, data collection forms, and tracking forms. As shown in Figure 4, a dual monitor setup can improve efficiency by allowing the researcher to keep the videoconferencing window open on one screen while referencing the protocol and other study materials on the other.
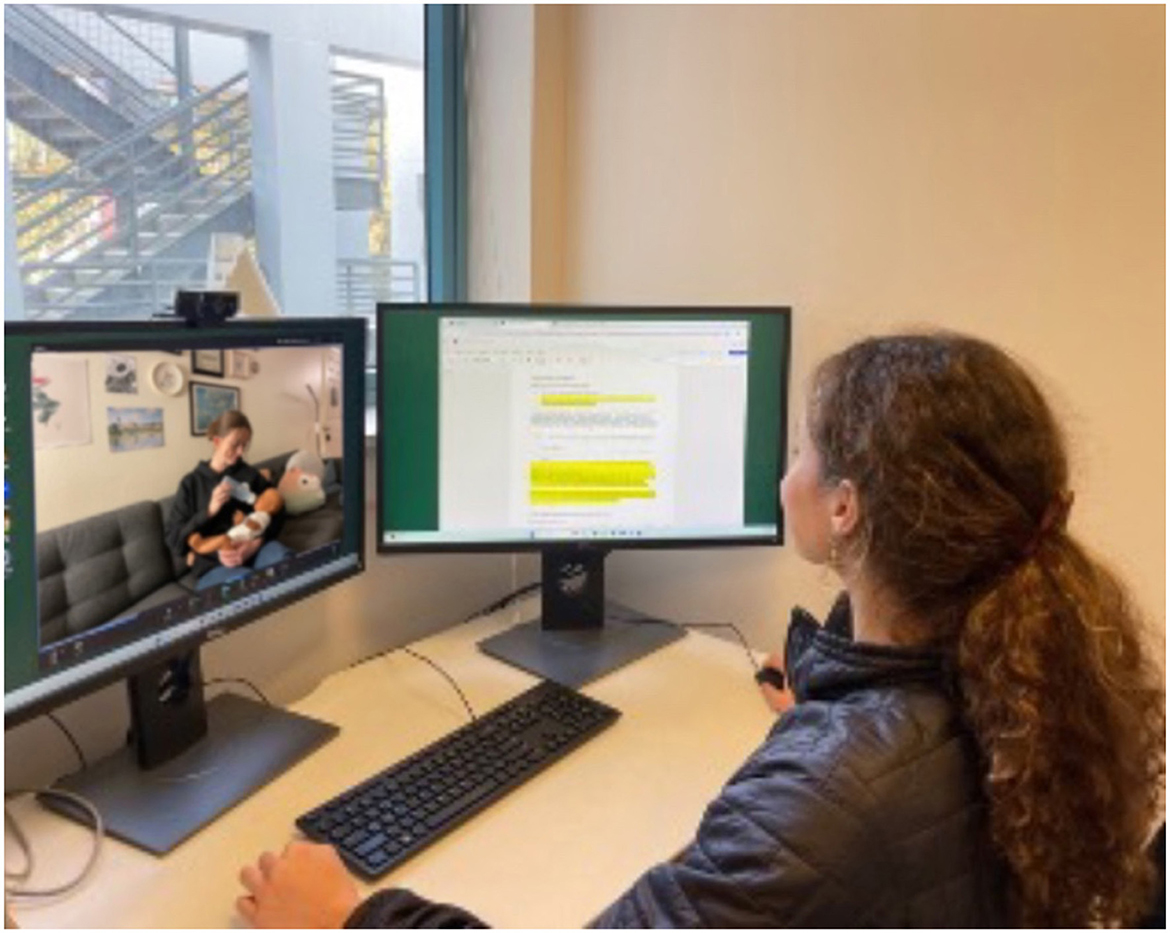
Figure 4. Researcher set-up for effective management of the virtual home visit and remote feeding observation.
3.3 Conducting the virtual home visit and remote feeding observation
Figure 5 summarizes a recommended protocol for conducting virtual home visits with remote feeding observations. When participants join the video call, the researcher should begin by welcoming them and providing an overview of what to expect. The acclimation period should be structured to allow ample time for questions and for troubleshooting any technical issues that may arise.
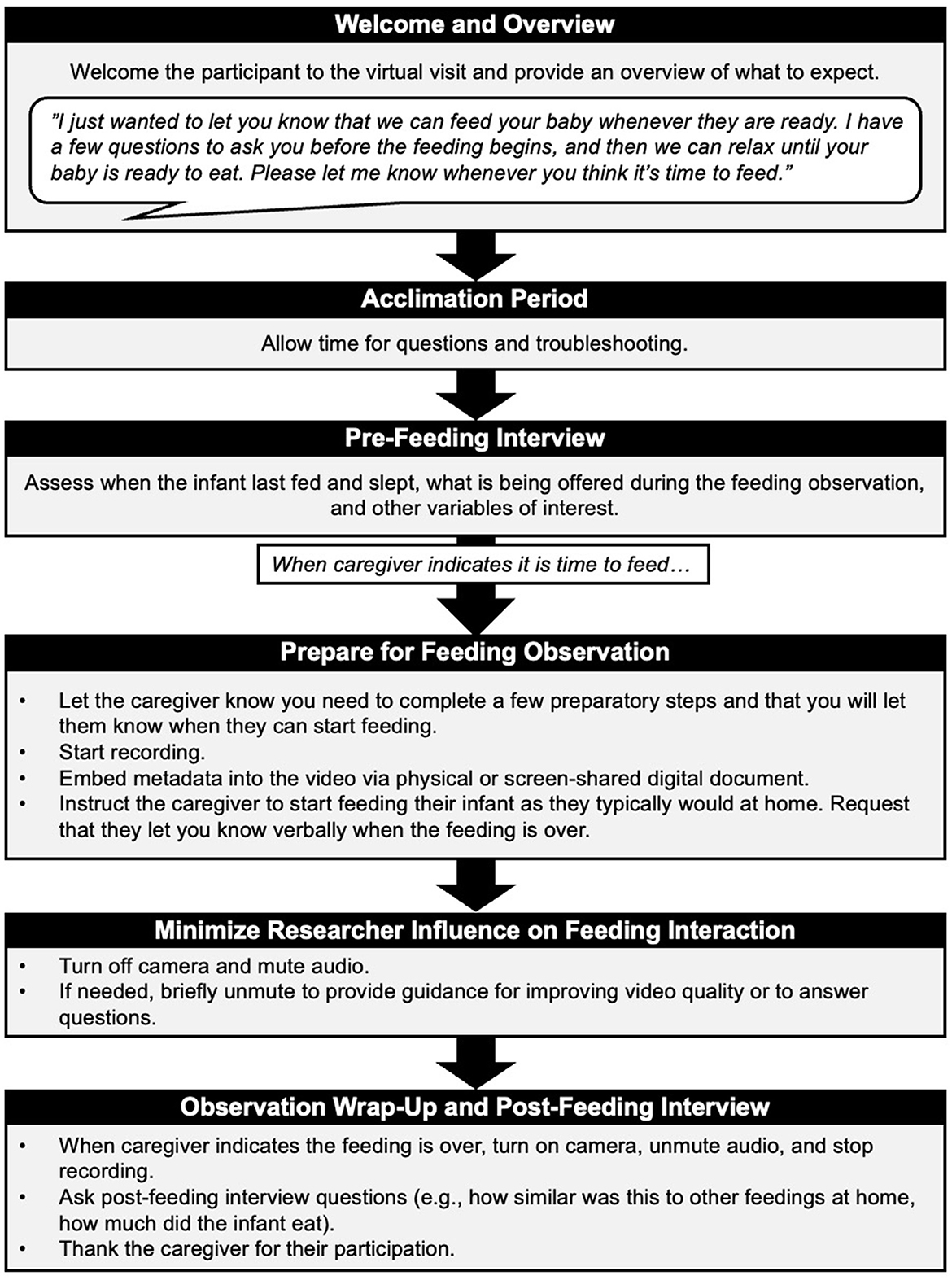
Figure 5. Process for the virtual home visit and remote feeding observation.
We recommend that researchers incorporate some flexibility into the virtual visit protocol to accommodate the unpredictability that arises from attempting to initiate feeding observations when infants are hungry and ready to eat. Some infants will be ready to feed shortly after the visit begins, while others may require more time. Regardless, researchers should ensure the caregiver does not feel pressured to start feeding prematurely. We recommend that the researcher take steps to minimize social desirability bias that may lead the participant to initiate feeding before the infant ready. To help set this tone, the researcher could instruct the caregiver as follows:
“I just wanted to let you know that you can feed your baby whenever they are ready. I have a few questions to ask you first, and then we can relax until your baby is ready to eat. Please let me know whenever you think it's time to feed.”
If the infant is not yet ready to feed, the researcher should have additional questions or tasks prepared to engage the caregiver without creating pressure to proceed prematurely. If time permits, the researcher should conduct a brief pre-feeding interview to assess when the infant last fed, the type of milk or food to be fed to the infant, and the amount being offered.
When the caregiver indicates that they and their infant are ready to start the feeding observation, they should be instructed to feed as they normally would at home. The researcher can take steps to minimize their impact on the feeding interaction and reduce participants' awareness that they are being observed by instructing the participant to feed their infant as they normally would at home and letting the participant know that they will turn off their camera and mute themselves during the feeding. We also recommend that the researcher ask the caregiver to verbally confirm when the infant is finished feeding, ensuring the researcher has a clear indication of when to end the feeding observation.
The researcher should then start recording the observation on the online platform and, before instructing the caregiver to begin the feeding, we recommend that the researcher briefly hold up a sign with the participant's ID and other visit details, or share their screen with a digital document containing this information, to embed this metadata within the video for later file tracking, data management, and quality control during behavioral coding. The researcher should then instruct the caregiver to begin the feeding, mute themselves, and turn off their camera. However, we recommend that the researcher stay near their computer to be available to the caregiver during the feeding. If the caregiver and/or infant leave the video frame at any point during the feeding observation (e.g., they shift position or the recording device moves), the researcher should be prepared to gently intervene by unmuting themselves and guiding the caregiver to reposition themself, their baby, or the recording device.
Once the caregiver has verbally indicated their baby is finished feeding, the researcher should stop the recording, unmute themselves, and turn their video camera back on. They can then ask the caregiver any follow-up questions, conduct other planned virtual assessments, and/or end the virtual home visit.
3.4 Preliminary evidence of reliability and validity
Herein, we review preliminary evidence from our previously published work for the reliability and validity of remote feeding observations from the perspective of comparability to in-person methods.
In a randomized controlled trial conducted before and during the COVID-19 pandemic, some families were assessed in person (n = 36) and others (recruited after the implementation of stay-at-home mandates) were assessed remotely (n = 40) (see Ventura et al., 2024a, for more details about the study rationale and methods). Across both groups, trained coders used the Nursing Child Assessment Parent–Child Interaction Feeding Scale (NCAFS, Oxford and Findlay, 2015) to score caregiver and infant contributions to and the overall quality of feeding interactions. Comparison of dyads assessed in-person vs. remotely revealed no differences in characteristics of mothers (e.g., age, parity, education level, race/ethnicity, marital status, family income) or infants (e.g., age, sex), or typical feeding practices (Ventura et al., 2024a). In addition, no differences were seen for inter-rater reliability and coders achieved intraclass correlations (ICC) in the good to excellent ranges for videos from both in-person and remote observations. There were no instances wherein we could not code a video due to poor video or audio quality. NCAFS total and subscale scores were comparable to published reference values (Oxford and Findlay, 2015) and did not differ between dyads assessed via in-person vs. remote observations for total scores representing the overall quality of feeding interactions (p = 0.23) or subscale scores assessing maternal sensitivity to infant cues (p = 0.06), responsiveness to infant distress (p = 0.48), socioemotional growth fostering (p = 0.37), and cognitive growth fostering (p = 0.99) or infant clarity of cues (p = 0.23) and responsiveness to the mother (p = 0.89) (Ventura et al., 2024a).
Evidence from a second, fully virtual longitudinal study of 153 mother-infant dyads further supports these findings (see McDaniel et al., Under Review1; Ventura et al., Under Review2 for more details about the study rationale and methods). Remote feeding observations were conducted when infants were 2 and 5 months old and videos were later coded using the NCAFS (Oxford and Findlay, 2015). Coders again achieved excellent agreement (98%) and while a small proportion of items (0.5%) could not be coded due to issues with video or audio quality, overall data loss was minimal. NCAFS total and subscale scores were again comparable to published reference values (Oxford and Findlay, 2015), indicating that remote feeding observations captured sufficient behavioral detail to assess relevant caregiver and infant behaviors during feeding interactions.
Taken together, these studies provide initial evidence that remote feeding observations yield reliable, codable data of similar quality to in-person assessments. At the same time, these findings should be considered preliminary. Formal validation studies are needed to more systematically test inter-rater reliability across coding approaches [i.e., microcoding vs. global coding schemes (Bakeman and Quera, 2011)], examine the accuracy of coding across device types (e.g., smartphones vs. laptops), and directly compare remote and in-person observations within the same families. Such studies are warranted for establishing the robustness and generalizability of remote feeding observation methods.
4 Anticipated results
4.1 Anticipated outcomes and characteristics of successful observations
A successful remote feeding observation yields a video recording that is of sufficient quality to allow coders to reliably score both caregiver and infant behaviors using standardized behavioral coding schemes. High-quality recordings share the following characteristics:
• Visual clarity: The caregiver-infant dyad is fully visible throughout the feeding interaction. The camera angle enables coders to observe facial expressions, eye gaze, and body posture for both the caregiver and the infant.
• Audio clarity: Verbalizations from the caregiver (e.g., speech, prompts) and vocalizations from the infant (e.g., coos, fussing) are audible, without interference from ambient noise or digital distortion.
• Minimal intrusions: There are no major distractions (e.g., background conversations, pets, or siblings) that interrupt the feeding sequence or block the camera's view for extended periods.
• Complete recording window: The recording begins before the feeding starts (e.g., includes relevant pre-feeding cues or prompts) and ends after the feeding has concluded, as verbally indicated by the caregiver.
• Naturalistic behavior: The caregiver feeds the infant as they typically would at home, without overtly altering their behaviors due to the researcher's presence or observation.
Based on our implementation experience, the majority of remote feeding sessions that follow our protocol result in recordings that meet these criteria and are suitable for frame-by-frame or global behavioral coding.
4.2 Common challenges and troubleshooting recommendations
Virtual home visits and remote feeding observations offer a flexible and inclusive alternative to in-person visits but also introduce unique challenges that can affect data quality and participant experience. Despite careful planning, researchers may encounter several challenges that can compromise data quality or participant experience. Below, we summarize the most common challenges researchers may encounter—some of which have already been mentioned above—and offer recommendations for addressing them. These challenges and recommended solutions are also summarized in the Table 1.
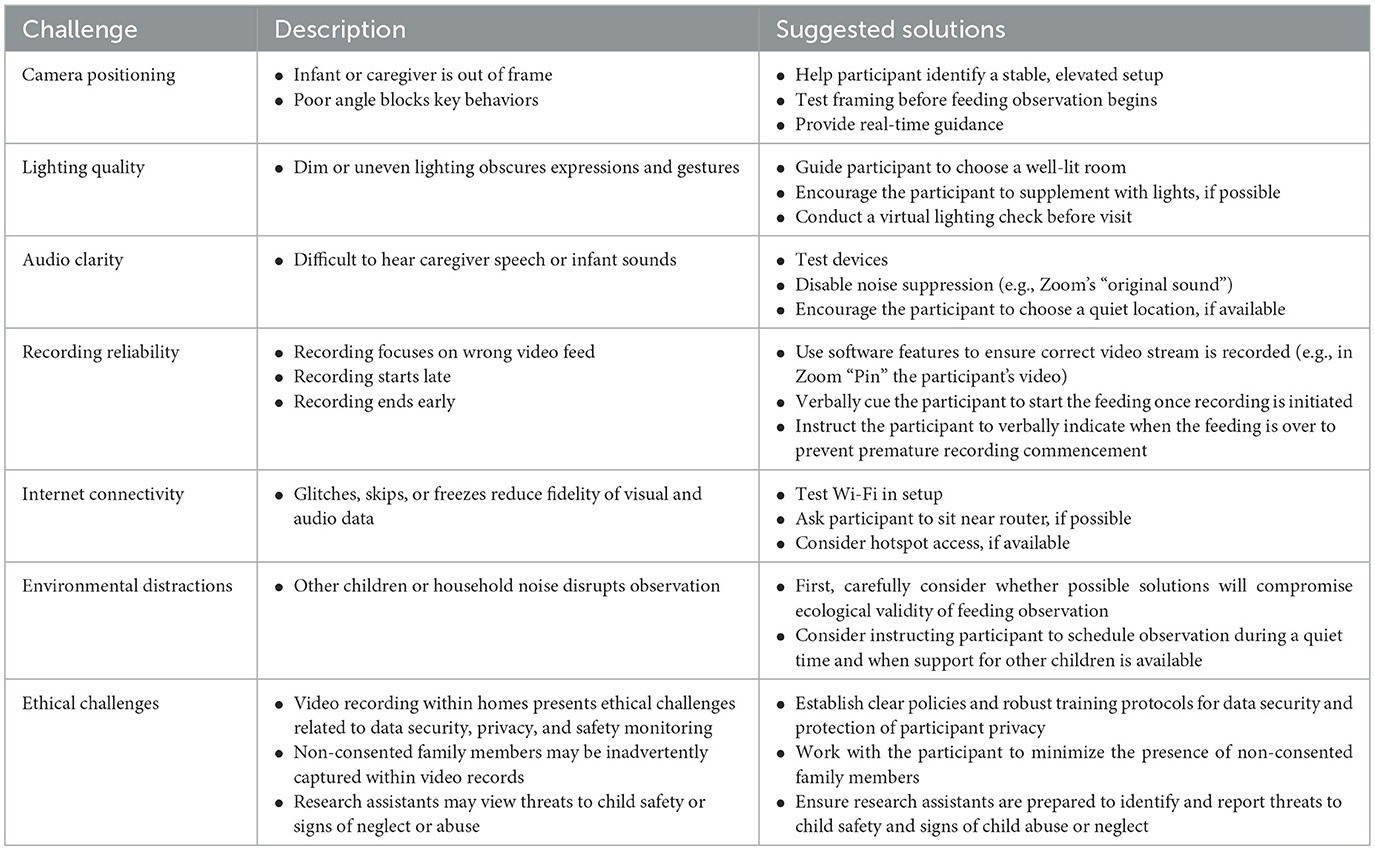
Table 1. Virtual home visit and remote feeding observation challenges and recommended solutions.
One of the most frequent challenges is maintaining a clear and consistent view of both the caregiver and the infant throughout the feeding. Because camera positioning varies across home environments, researchers often encounter issues such as the infant or caregiver facing away from the camera, the frame being too close to capture relevant body language, or the caregiver's eye gaze being obstructed. These visibility issues make it difficult to code behaviors such as facial expressions, gestures, and mutual gaze. To address this, researchers should work closely with participants to establish optimal camera placement before the start of the observation. A stable, elevated angle that captures both caregiver and infant in full view typically yields the best results. Use of a tripod or a securely propped phone can further minimize movement and disruptions during the observation.
In addition to framing, lighting conditions can significantly impact the quality of the video. Dim or uneven lighting may obscure facial cues, making fine-grained behavioral coding challenging. Whenever possible, participants should be encouraged to conduct visits in naturally well-lit rooms or to supplement with overhead or ambient lighting. A brief lighting check before the feeding can help ensure both the caregiver and infant are visible.
Audio quality is another critical component of effective remote observation. When verbalizations from the caregiver or vocalizations from the infant are inaudible or inconsistent, researchers may miss valuable information necessary for coding key behaviors. Factors such as device microphone sensitivity, background noise, and software-based noise suppression can interfere with audio clarity. If possible, researchers should test participants' audio setups in advance and consider comparing sound quality across different devices (e.g., smartphones vs. laptops). Encouraging participants to conduct the session in a quiet location and disabling automatic noise filtering features (such as Zoom's default background noise suppression) can also improve sound fidelity. In our experience with Zoom, enabling the “Original sound for musicians” setting helped preserve subtle sounds during live recording. This setting disables Zoom's built-in echo cancellation and noise reduction features that may inadvertently filter out important components of caregiver-infant interactions, such as soft vocalizations (e.g., infant coos, caregiver whispers) or feeding sounds (e.g., sucking noises).
In addition, the home environment itself can introduce distractions that affect both the recording and the feeding interaction. A chaotic environment and external sources of noise (e.g., background TV, additional family members) may disrupt the feeding observation by interfering with the recording device or demanding the caregiver's attention. Although steps can be taken to mitigate these issues (e.g., working with participants to schedule sessions during quieter times, such as when other children are napping or being cared for by another adult), researchers should carefully consider whether these steps will artificially change the feeding environment in ways that may make the feeding observation less ecologically valid. Although these features of the home environment can negatively impact video quality, they may also reflect the dyad's typical feeding context, which would be important to capture and consider during later video coding.
Recording issues may also compromise the validity of the observation. For example, software-triggered camera switching can result in the initial moments of feeding being missed or having the recording focus on the researcher's video feed instead of the participant‘s. To mitigate this, researchers should design their protocols to provide clear instructions on how to avoid these issues and ensure that the researcher captures the participants' video stream for the full duration of the feeding interaction. Prompting the caregiver to speak or make a sound at the start of the session can help ensure the platform's recording algorithm correctly prioritizes the participant's video stream.
Internet connectivity is another known barrier to high-quality video data. Glitching, freezing, or skipping frames due to bandwidth limitations can cause missed behaviors or inhibit frame-by-frame analysis. In our experience, these issues are especially problematic when trying to code rapid changes in caregiver or infant gaze and behavior. To reduce connectivity issues, researchers should assess internet stability during the setup call and suggest that participants sit near their Wi-Fi router when possible. In homes with unreliable service, mobile hotspots may offer a viable alternative.
Social desirability biases may lead caregivers to feel rushed to feed their infant when signs of hunger emerge or to encourage their infant to eat in the absence of hunger. We also find that some caregivers are anxious to feed their infants at the beginning of the virtual visit, especially if their infants are exhibiting signs of hunger (e.g., fussiness, crying). Infant fussing and crying may distract caregivers and reduce their ability to answer pre-feeding questions. Infant behaviors or caregiver anxiety around feeding may also lead caregivers to initiate feeding before the researcher has provided their pre-feeding instructions and started recording. Researchers should carefully develop their protocols and scripts to include strategies to counteract these issues. To reduce social desirability bias, we recommend scheduling ample time for the visit, incorporating an acclimation period at the beginning of the visit, and providing the caregiver with assurances that the goal of the observation is to observe typical feeding interactions. To prevent misalignment between the start of the feeding and the start of video recording, we recommend researchers provide clear instructions to participants about the sequence of events (e.g., “First I will start recording, then I will let you know when you may begin feeding…okay, you may begin feeding now”). Researchers may also want to consider keeping pre-feeding questions brief and straightforward so that a caregiver concerned about their hungry infant will not struggle to comprehend and answer the questions while their infant is fussing and crying. We have also found it helpful to incorporate sources of protocol flexibility (e.g., questionnaires that can be filled out before or after the feeding) that allow the researcher to move protocol components earlier in the visit to “fill time” when waiting for an infant to wake up or become hungry or later in the visit if an infant is ready to feed earlier than expected.
Finally, video recording within home environments presents ethical challenges related to data security, privacy, and participant safety monitoring that require careful attention. Researchers should establish clear policies regarding who has access to the recordings, how long the videos will be retained, and when and how they will be securely deleted. In addition, research assistants should be trained on these policies, as well as best practices for data security (e.g., use of password-protected computers and HIPAA compliant software, storage of videos on encrypted servers). Research assistants should also be trained on the importance of conducting virtual visits in private spaces to protect participant confidentiality. Researchers should be mindful that participants may feel increased vulnerability being recorded in their home environment and can provide reassurances that data will be used solely for research purposes and handled with sensitivity. In addition, participants should be informed of their right to pause or stop the recording at any time and to request deletion of videos if they no longer wish to participate. As mentioned above, it is also possible that other family members that are not part of the study (and thus, did not consent to be video recorded) are present during the observation and/or are captured within the video recording. Researchers can work with their institutional review boards to determine the best strategies for dealing with these issues (e.g., blurring out faces of non-consented family members, obtaining consent from these family members). Finally, as with any home-based assessment, researchers may view concerning caregiver behaviors, signs of child abuse or neglect, or concerning items in the home (e.g., drug paraphernalia, guns). Research assistants should receive training and have protocols in place to help them recognize potential safety concerns and respond promptly, in accordance with university policies and state and federal laws.
In sum, although it may not be possible to eliminate every challenge associated with virtual home visits and remote feeding observations, careful planning, pre-visit preparation, and clear communication with participants can substantially improve the quality of the data collected.
5 Discussion
Observing parent-infant feeding interactions offers a unique opportunity to understand both early relational dynamics and foundational aspects of infant development. As technology advances and the demand for more accessible research methods increases, remote feeding observations via virtual home visits have emerged as a valuable alternative to traditional in-person assessments. This manuscript has outlined key considerations, challenges, and recommendations for researchers and clinicians seeking to implement virtual observation protocols for caregiver-infant feeding interactions.
Remote observations have become increasingly feasible due to the widespread availability of smartphones, laptops, and broadband internet, even among families with lower socioeconomic status. While smartphones are the most accessible devices, factors such as device type, camera positioning, lighting, and internet connectivity can all impact the quality of remote data collection. Researchers' thoughtful attention to device setup and the implementation of strategies, such as using smartphone tripods, optimizing lighting, and providing technology handouts, can help researchers overcome many common issues that affect video quality. In addition, through careful scheduling aligned with infants' natural routines and planning of flexible protocols, researchers can reduce stress on families and increase the likelihood of capturing representative, high-quality feeding interactions.
Taken together, the guidance presented in this manuscript provides a comprehensive framework for conducting remote caregiver-infant feeding observations that are both methodologically rigorous and sensitive to the needs of participating families. By anticipating and addressing potential barriers, researchers can collect rich, ecologically valid data while expanding access to diverse populations. However, while the use of common videoconferencing platforms and widespread smartphone ownership increases the accessibility of this method, digital literacy and internet access may still pose barriers for some families. Strategies such as loaning equipment, providing mobile hotspots, and offering personalized tech support can help mitigate these barriers and expand the method's reach. Despite these limitations, virtual home visits and remote feeding observations hold the potential to be scalable, ecologically valid, and inclusive methods for studying feeding behaviors, caregiver-infant interactions, and infant development.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
AV: Supervision, Conceptualization, Writing – review & editing, Funding acquisition, Writing – original draft, Methodology, Visualization. AR: Visualization, Writing – original draft, Investigation, Writing – review & editing. MR: Visualization, Writing – review & editing, Writing – original draft, Investigation. GT: Writing – original draft, Investigation, Writing – review & editing. SE: Investigation, Writing – original draft, Writing – review & editing, Visualization. KC: Project administration, Investigation, Writing – review & editing, Writing – original draft, Methodology, Supervision. CD: Investigation, Writing – review & editing, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was generously supported by the William and Linda Frost Fund in the Cal Poly Bailey College of Science and Mathematics.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Gen AI was used in the creation of this manuscript. During the preparation of this work, generative AI tools, specifically ChatGPT and Grammarly, were used to improve grammar and readability, suggest alternative phrasing, and check for grammatical errors. After utilizing this tool/service, the author(s) reviewed and edited the content as needed and take full responsibility for the content of the publication.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^McDaniel, B. T., Ventura, A. K., Coyne, S., Wolfers, L. N., Pfafman, R., Shinde, A. S., et al. (Under Review). Handing Babies Phones: A Longitudinal Examination of Media Emotion Regulation in Early Infancy.
2. ^Ventura, A. K., Wolfers, L. N., Coyne, S. M., Pfafman, R., Uva, S., Ceja Almontes, K. I. et al. (Under Review). Objective Vs. Perceived Maternal Smartphone Use and Observed Mother-Infant Interaction Quality.
References
Ainsworth, M. D., and Bell, S. M. (1969). “Some contemporary patterns of mother-infant interaction in the feeding situation,” in Stimulation in Early Infancy, ed. A. Ambrose (Cambridge: Academic Press), 133–170.
Alvarez Gutierrez, S., and Ventura, A. K. (2021). Associations between maternal technology use, perceptions of infant temperament, and indicators of mother-to-infant attachment quality. Early Hum Dev. 154:105305. doi: 10.1016/j.earlhumdev.2021.105305
Anderson, J., Rainie, L., and Vogels, E. A. (2021). Experts say the ‘New Normal' in 2025 will be far more tech-driven, presenting new challenges. Available online at: https://www.pewresearch.org/internet/2021/02/18/experts-say-the-new-normal-in-2025-will-be-far-more-tech-driven-presenting-more-big-challenges/ (Accessed September 9, 2025).
Anzman-Frasca, S., Ventura, A. K., Ehrenberg, S., and Myers, K. P. (2018). Promoting healthy food preferences from the start: a narrative review of food preference learning from the prenatal period through early childhood. Obes. Rev. 19, 576–604. doi: 10.1111/obr.12658
Bakeman, R., and Quera, V. (2011). Sequential Analysis and Observational Methods for the Behavioral Sciences. Cambridge University Press. doi: 10.1017/CBO9781139017343
Birch, L. L. (2016). Learning to eat: behavioral and psychological aspects. Nestle Nutr Inst Workshop Ser. 85, 125–134. doi: 10.1159/000439503
Black, M. M., and Aboud, F. E. (2011). Responsive feeding is embedded in a theoretical framework of responsive parenting. J. Nutr. 141, 490–494. doi: 10.3945/jn.110.129973
Bowlby, J. (1977a). The making and breaking of affectional bonds. I. Aetiology and psychopathology in the light of attachment theory. An expanded version of the Fiftieth Maudsley Lecture, delivered before the Royal College of Psychiatrists, 19 November 1976. Br. J. Psychiatry 130, 201–210. doi: 10.1192/bjp.130.3.201
Bowlby, J. (1977b). The making and breaking of affectional bonds. II. Some principles of psychotherapy. The fiftieth Maudsley Lecture. Br. J. Psychiatry 130, 421–431. doi: 10.1192/bjp.130.5.421
Bronfenbrenner, U., and Morris, P. (1998). “The ecology of human developmental processes,” in Theoretical Models of Human Development, 5th Edn. eds. W. Damon and N. Eisenberg (Hoboken, NJ: John Wiley and Sons), 993–1028.
Brown, L. F., Thoyre, S., Pridham, K., and Schubert, C. (2009). The mother-infant feeding tool. J. Obstet. Gynecol. Neonatal. Nurs. 38, 491–503. doi: 10.1111/j.1552-6909.2009.01047.x
Chatoor, I., Getson, P., Menvielle, E., Brasseauz, C., O'Donnell, R., Rivera, Y., et al. (1998). A feeding scale for research and clinical practice to assess mother-infant interactions in the first three years of life. Infant Ment. Health J. 18, 76–91.
Cimino, S., and Cerniglia, L. (2024). Further evidence on online video-feedback intervention: enhancing parent–child interactions and reducing disordered eating in children. Int. J. Environ. Res. Public Health 2:1260. doi: 10.3390/ijerph21091260
Corcoran, K., and Fischer, J. (2013). Measures for Clinical Practice and Research (Vol. 2). Oxford: Oxford University Press.
Cormack, J., Rowell, K., and Postăvaru, G.-I. (2020). Self-determination theory as a theoretical framework for a responsive approach to child feeding. J. Nutr. Educ. Behav. 52, 646–651. doi: 10.1016/j.jneb.2020.02.005
Coyne, S. M., Shawcroft, J., Gale, M., Reich, S. M., Linder, L., McDaniel, B., et al. (2022). Digital distraction or accessible aid? Parental media use during feedings and parent-infant attachment, dysfunction, and relationship quality. Comput. Hum. Behav. 127:107051. doi: 10.1016/j.chb.2021.107051
D'Angeli, G., Mesce, M., Cerniglia, L., and Cimino, S. (2022). Observational tools using video recordings of parent-child feeding interactions: a narrative review. Children 9:1924. doi: 10.3390/children9121924
Davison, K. K., and Birch, L. L. (2001). Childhood overweight: a contextual model and recommendations for future research. Obes. Rev. 2, 159–171. doi: 10.1046/j.1467-789x.2001.00036.x
DiSantis, K. I., Hodges, E. A., Johnson, S. L., and Fisher, J. O. (2011). The role of responsive feeding in overweight during infancy and toddlerhood: a systematic review. Int. J. Obes. 35, 480–492. doi: 10.1038/ijo.2011.3
Duhn, L. (2010). The importance of touch in the development of attachment. Adv. Neonatal. Care 10, 294–300. doi: 10.1097/ANC.0b013e3181fd2263
Fisher, J. O., Butte, N. F., Mendoza, P. M., Wilson, T. A., Hodges, E. A., Reidy, K. C., et al. (2008). Overestimation of infant and toddler energy intake by 24-h recall compared with weighed food records. Am. J. Clin. Nutr. 88, 407–415. doi: 10.1093/ajcn/88.2.407
Gardner, F. (2000). Methodological issues in the direct observation of parent–child interaction: do observational findings reflect the natural behavior of participants? Clin. Child Fam. Psychol. Rev. 3, 185–198. doi: 10.1023/A:1009503409699
Giansanti, D. (2023). Ten years of telehealth and digital healthcare: Where are we? Healthcare 11:875. doi: 10.3390/healthcare11060875
Golen, R. P., and Ventura, A. K. (2015). What are mothers doing while bottle-feeding their infants? Exploring the prevalence of maternal distraction during bottle-feeding interactions. Early Hum. Dev. 91, 787–791. doi: 10.1016/j.earlhumdev.2015.09.006
Grummer-Strawn, L. M., Scanlon, K. S., and Fein, S. B. (2008). Infant feeding and feeding transitions during the first year of life. Pediatrics 122, S36–42. doi: 10.1542/peds.2008-1315D
Gustafsson, H. C., Young, A. S., Stamos, G., Wilken, S., Brito, N. H., Thomason, M. E., et al. (2021). Innovative methods for remote assessment of neurobehavioral development. Dev. Cogn. Neurosci. 52:101015. doi: 10.1016/j.dcn.2021.101015
Heller, R. L., and Mobley, A. R. (2019). Instruments assessing parental responsive feeding in children ages birth to 5 years: a systematic review. Appetite 138, 23–51. doi: 10.1016/j.appet.2019.03.006
Hodges, E. A., Johnson, S. L., Hughes, S. O., Hopkinson, J. M., Butte, N. F., and Fisher, J. O. (2013). Development of the responsiveness to child feeding cues scale. Appetite 65, 210–219. doi: 10.1016/j.appet.2013.02.010
Hodges, E. A., Wasser, H. M., Colgan, B. K., and Bentley, M. E. (2016). Development of feeding cues during infancy and toddlerhood. MCN Am. J. Matern. Child Nurs. 41, 244–251. doi: 10.1097/NMC.0000000000000251
Igielnik, R. (2022). As telework continues for many U.S. workers, no sign of widespread ‘Zoom fatigue.' Available online at: https://www.pewresearch.org/short-reads/2022/05/04/as-telework-continues-for-many-u-s-workers-no-sign-of-widespread-zoom-fatigue/(Accessed September 9, 2025).
Koonin, L. M., Hoots, B., Tsang, C. A., Leroy, Z., Farris, K., Jolly, T., et al. (2020). Trends in the use of telehealth during the emergence of the COVID-19 pandemic — United States, January–March 2020. MMWR Morb. Mortal Wkly. Rep. 69, 1595–1599. doi: 10.15585/mmwr.mm6943a3
La Rosa, V. L., Geraci, A., Iacono, A., and Commodari, E. (2024). Affective touch in preterm infant development: neurobiological mechanisms and implications for child-caregiver attachment and neonatal care. Children 11:1407. doi: 10.3390/children11111407
Lanigan, J. A., Wells, J. C., Lawson, M. S., and Lucas, A. (2001). Validation of food diary method for assessment of dietary energy and macronutrient intake in infants and children aged 6-24 months. Eur. J. Clin. Nutr. 55, 124–129. doi: 10.1038/sj.ejcn.1601128
Lecroy, M. N., Potter, L. N., Bandeen-Roche, K., Bianco, M. E., Cappola, A. R., Carter, E. B., et al. (2023). Barriers to and solutions for representative inclusion across the lifespan and in life course research: The need for structural competency highlighted by the COVID-19 pandemic. J. Clin. Trans. Sci. 7, 1–39. doi: 10.1017/cts.2022.510
Lobe, B., Morgan, D., and Hoffman, K. A. (2020). Qualitative data collection in an era of social distancing. Int. J. Qual. Met. 19:160940692093787. doi: 10.1177/1609406920937875
MacPhee, M., and Schneider, J. (1996). A clinical tool for nonorganic failure-to-thrive. J. Ped. Nurs. 11, 29–39. doi: 10.1016/S0882-5963(96)80035-2
Mallan, K., and Miller, N. (2019). Effect of parental feeding practices (i.e., responsive feeding) on children's eating behavior. Nestle Nutr. Inst. Workshop Ser. 91, 21–30. doi: 10.1159/000493675
Mejía, D. (2024). Computer and Internet Use in the United States: 2021. American Community Survey Reports, United States Census Bureau, Report Number: ACS-56.
Montirosso, R., and McGlone, F. (2020). The body comes first. Embodied reparation and the co-creation of infant bodily-self. Neurosci. Biobehav. Rev. 113, 77–87. doi: 10.1016/j.neubiorev.2020.03.003
Nathe, J. M., Oskoui, T. T., and Weiss, E. M. (2023). Parental views of facilitators and barriers to research participation: systematic review. Pediatrics 151:e2022058067. doi: 10.1542/peds.2022-058067
Oxford, M., and Findlay, D. (Eds.). (2015). Caregiver/Parent-Child Interaction: Feeding Manual (2nd ed.). NCAST Programs.
Perez-Escamilla R. Segura-Perez S. Lott M. on behalf of the RWJF HER Expert Panel on Best Practices for Promoting Healthy Nutrition Feeding Patterns, Weight Status for Infants Toddlers from Birth to 24 Months. (2017). Feeding Guidelines for Infants and Young Toddlers: A Responsive Parenting Approach. Available online at: http://healthyeatingresearch.org (Accessed September 9, 2025).
Pesch, M. H., and Lumeng, J. C. (2017). Methodological considerations for observational coding of eating and feeding behaviors in children and their families. Int. J. Behav. Nutr. Phys. Act 14:170. doi: 10.1186/s12966-017-0619-3
Pew Research Center (2024a). Internet, Broadband Fact Sheet. Available online at: https://www.pewresearch.org/internet/fact-sheet/internet-broadband/?tabItem=480dace1-fd73-4f03-ad88-eae66e1f4217 (Accessed September 9, 2025).
Pew Research Center (2024b). Mobile Fact Sheet. Available online at: https://www.pewresearch.org/internet/fact-sheet/mobile/ (Accessed September 9, 2025).
Piaget, J. (1952). The origins of intelligence in children (M. Cook, Trans.). International Universities Press. doi: 10.1037/11494-000
Price, G. M. (1983). Sensitivity in mother-infant interactions: the AMIS scale. Infant Behav. Devel. 6, 353–360. doi: 10.1016/S0163-6383(83)80043-5
Shaver, J. (2022). The state of telehealth before and after the COVID-19 pandemic. Prim. Care 49, 517–530. doi: 10.1016/j.pop.2022.04.002
Shin, E., Smith, C. L., and Howell, B. R. (2021). Advances in behavioral remote data collection in the home setting: assessing the mother-infant relationship and infant's adaptive behavior via virtual visits. Front. Psychol. 12:703822. doi: 10.3389/fpsyg.2021.703822
Tesson, S., Swinsburg, D., and Kasparian, N. A. (2021). Maintaining momentum in infant mental health research during covid-19: adapting observational assessments. J. Pediatr. Psychol. 46, 254–263. doi: 10.1093/jpepsy/jsab020
Toporoff, E. G., and Story, M. (1997). The feeding arena. Topics Clin Nutr. 12, 62–72. doi: 10.1097/00008486-199712020-00009
United States Department of Agriculture (2020). Dietary Guidelines for Americans: 2020-2025. Available online at: https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf (Accessed September 9, 2025).
Ventura, A. K., Beauchamp, G. K., and Mennella, J. A. (2012). Infant regulation of intake: the effect of free glutamate content in infant formulas. Am. J. Clin. Nutr. 95, 875–881. doi: 10.3945/ajcn.111.024919
Ventura, A. K., Drewelow, V. M., and Richardson, T. N. (2025). Does paced bottle-feeding improve the quality and outcome of bottle-feeding interactions? Early Hum. Dev. 201:106181. doi: 10.1016/j.earlhumdev.2024.106181
Ventura, A. K., and Golen, R. P. (2015). A pilot study comparing opaque, weighted bottles with conventional, clear bottles for infant feeding. Appetite 85, 178–185. doi: 10.1016/j.appet.2014.11.028
Ventura, A. K., Hart, C. N., Phelan, S., Jelalian, E., and Wing, R. R. (2023). Associations between technology use, responsive feeding, and child temperament among prior prenatal intervention participants. J. Dev. Behav. Pediatr. 44, e315–e321. doi: 10.1097/DBP.0000000000001174
Ventura, A. K., and Hernandez, A. (2019). Effects of opaque, weighted bottles on maternal sensitivity and infant intake. Matern. Child Nutr. 15:e12737. doi: 10.1111/mcn.12737
Ventura, A. K., Hupp, M., Alvarez Gutierrez, S., and Almeida, R. (2020). Development and validation of the maternal distraction questionnaire. Heliyon 6:e03276. doi: 10.1016/j.heliyon.2020.e03276
Ventura, A. K., Hupp, M., and Lavond, J. (2021). Mother-infant interactions and infant intake during breastfeeding vs. bottle-feeding expressed breast milk. Matern. Child Nutr. 17:e13185. doi: 10.1111/mcn.13185
Ventura, A. K., Inamdar, L. B., and Mennella, J. A. (2015). Consistency in infants' behavioural signalling of satiation during bottle-feeding. Pediatr. Obes. 10, 180–187. doi: 10.1111/ijpo.250
Ventura, A. K., Levy, J., and Sheeper, S. (2019a). Maternal digital media use during infant feeding and the quality of feeding interactions. Appetite 143:104415. doi: 10.1016/j.appet.2019.104415
Ventura, A. K., and Mennella, J. A. (2017). An experimental approach to study individual differences in infants' intake and satiation behaviors during bottle-feeding. Child Obes 13, 44–52. doi: 10.1089/chi.2016.0122
Ventura, A. K., Phelan, S., Alarcon, N., Quintana Diaz, A., Sklar, J. C., and Hart, C. N. (2024a). A pilot feasibility randomized controlled trial of effects of opaque bottles on maternal sensitivity, infant intake, and infant weight status. J. Acad. Nutr. Diet 124, 1149–1161 e1141. doi: 10.1016/j.jand.2024.02.005
Ventura, A. K., Ross, K. J., Miller, A. L., DeJesus, J. M., Tan, C. C., and Lumeng, J. C. (2024b). Development of the baby behaviors when satiated (BABES) behavioral coding scheme. Appetite 203:107704. doi: 10.1016/j.appet.2024.107704
Ventura, A. K., Sheeper, S., and Levy, J. (2019b). Exploring correlates of infant clarity of cues during early feeding interactions. J. Acad. Nutr. Diet 119, 1452–1461. doi: 10.1016/j.jand.2019.03.014
Ventura, A. K., and Teitelbaum, S. (2017). Maternal distraction during breast- and bottle feeding among WIC and non-WIC mothers. J. Nutr. Educ. Behav. 49, S169–S176 e161. doi: 10.1016/j.jneb.2017.04.004
Ventura, A. K., and Worobey, J. (2013). Early influences on the development of food preferences. Curr. Biol. 23, R401–408. doi: 10.1016/j.cub.2013.02.037
Vygotsky, L. S. (1978). Mind in society: The development of higher psychological processes. Harvard University Press.
World Health Organization, United Nations Children's Fund, World Bank Group. (2018). Nurturing care for early childhood development: a framework for helping children survive and thrive to transform health and human potential. Geneva: World Health Organization.
Keywords: parent-infant interaction, feeding behavior, remote observation, telehealth, virtual home visits, infant development, behavioral coding, video methods
Citation: Ventura AK, Rossi A, Ryder MM, Thomas GM, Eaddy S, Ceja Almontes KI and Diaz CL (2025) Recommendations for remote observation of caregiver-infant feeding interactions via virtual home visits. Front. Dev. Psychol. 3:1661352. doi: 10.3389/fdpys.2025.1661352
Received: 07 July 2025; Accepted: 25 August 2025;
Published: 19 September 2025.
Edited by:
Alessandra Geraci, University of Catania, ItalyReviewed by:
Arianna Bentenuto, University of Trento, ItalyValentina Lucia La Rosa, University of Catania, Italy
Copyright © 2025 Ventura, Rossi, Ryder, Thomas, Eaddy, Ceja Almontes and Diaz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alison K. Ventura, YWt2ZW50dXJAY2FscG9seS5lZHU=