Abstract
Background:
The use of chatbots to address mental health conditions have become increasingly popular in recent years. However, few studies aimed to teach parenting skills through chatbots, and there are no reports on parental user experience. Aim: This study aimed to assess the user experience of a parenting chatbot micro intervention to teach how to praise children in a Spanish-speaking country.
Methods:
A sample of 89 parents were assigned to the chatbot micro intervention as part of a randomized controlled trial study. Completion rates, engagement, satisfaction, net promoter score, and acceptability were analyzed.
Results:
66.3% of the participants completed the intervention. Participants exchanged an average of 49.8 messages (SD = 1.53), provided an average satisfaction score of 4.19 (SD = .79), and reported that they would recommend the chatbot to other parents (net promoter score = 4.63/5; SD = .66). Acceptability level was high (ease of use = 4.66 [SD = .73]; comfortability = 4.76 [SD = .46]; lack of technical problems = 4.69 [SD = .59]; interactivity = 4.51 [SD = .77]; usefulness for everyday life = 4.75 [SD = .54]).
Conclusions:
Overall, users completed the intervention at a high rate, engaged with the chatbot, were satisfied, would recommend it to others, and reported a high level of acceptability. Chatbots have the potential to teach parenting skills however research on the efficacy of parenting chatbot interventions is needed.
Introduction
Behavior problems are prominent among children and adolescents (1, 2) and parenting programs have shown to be effective in reducing disruptive behaviors (3–6). However, many parents do not have access to such programs due to several barriers, such as a shortage of human therapists (7). Digital mental health interventions have become a popular method of overcoming the barriers to access and providing support for mental health. Parenting programs delivered through digital means have effectively treated behavioral problems in children and adolescents (8–12); however, the literature on chatbots for parenting skills is scarce.
Chatbots are computer-based programs that communicate with humans through text or voice conversations, are based on artificial intelligence (AI) and/or contain pre-programmed responses (13). The research on chatbots for mental health problems in adults has shown that chatbots can produce some unique effects compared to other digital interventions. Users are able to engage and bond with chatbots (14–16) and tend to humanize and perceive the chatbot as their friend (17). Users have found mental health chatbots to be helpful, informative, easy to use (13), and have reported that chatbots are more accepting and not as judgemental as humans (16). One study, in particular, found that users felt “loved” and “cared for” after using the chatbot (18). Additionally, chatbot studies reported significant improvements in depressive symptoms (19), anxiety symptoms (15), ADHD (20), and psychological distress (21). Throughout the onset of the COVID-19 pandemic, chatbots have been studied as a tool to offer psychological crisis support (22, 23).
The research on chatbots is still in its early stages, most chatbots are rule-based and follow scripts that are difficult to customize to each user (24). Some users have reported feeling frustration when the chatbot misunderstands them (25) and found it difficult to connect with them (26). Retaining and engaging users with chatbots is often challenging (14) and some people are still reluctant to use chatbots due to stigma (16, 26).
Analyzing user experience may help improve chatbots for mental health. Studies on user experience with chatbots have measured variables such as usability, satisfaction, engagement, and completion rate (27–29). Previous studies have looked at engagement by identifying the number of messages sent and characters typed by users during the conversation or over several days (30–32). Chatbots on user experience for parental interventions have undergone little research.
To our knowledge, there is one study on a parent training intervention delivered through a chatbot (33). The study examined the feasibility of delivering the beta version of a parenting chatbot micro intervention to teach parents how to praise their children. The intervention presented five skills for praising children effectively: defining the praise, being specific, avoiding combining praise with criticism, showing enthusiasm, and praising immediately. Seventy-eight percent of parents completed the intervention. On average, parents remembered 3.7 out of 5 taught skills and reported that they were likely to recommend the chatbot to other parents (7.44/10). During the micro intervention, parents sent an average of 54 messages, with a mean of 3 words per message. Overall, parents completed the intervention, were satisfied with it, and learned from the chatbot. While this suggests that parenting skills could be delivered via chatbots, some parents considered the chatbot's script impersonal or mechanical while others reported experiencing technical difficulties or they felt misunderstood by the chatbot.
This study aimed to assess the user experience of version 1.0 of the parenting chatbot micro intervention to teach how to praise children. Specifically, the study aimed to analyze the completion rate, messages sent, characters typed, degree of acceptability, satisfaction, and net promoter score.
Methods
Participants
Participants were recruited through Facebook posts and email list advertisements. A total of 170 people participated in the study. To be included in the study, participants had to reside in Argentina and have at least one child between the age of two to eleven years old.
Materials and measures
User Experience Questionnaire. Similar to previous research (34, 35), five ad hoc questions were designed to address the acceptability: ease of use, comfort, lack of technical problems, interactivity, and usefulness for everyday life. Participants rated each question using a Likert scale from 1 (“strongly disagree”) to 5 (“strongly agree”).
Satisfaction Questionnaire. A Likert scale from 1 to 5 was used, with 1 being “Totally disagree” and 5 being “Totally agree”, to assess participants' satisfaction with the question “How satisfied are you with the intervention?”.
Chatbot Parenting Micro Intervention. An intervention was designed based on an initial module of the Incredible Years parenting program (6). Its general objective is to teach parents to use positive attention and praise to stimulate positive behaviors in their children. An artificial intelligence software (TESS) designed by X2AI to provide mental health care was used. The intervention aimed to teach five skills for effective use of praise. The skills were grouped for presentation to participants under the acronym F.E.LIC.E.S. (“HAPPY” in Spanish - the original language of the intervention). The 5 skills taught were: Focus (choose specific behaviors you want to encourage), be specific, avoid combining praise with criticism, show enthusiasm when praising, and praise immediately after the good behavior. The intervention lasted approximately 15 min and was designed based on principles of conversational design, gamification, and study practices that promote interaction and learning. It included open-ended questions to encourage reflection, conversational games to distinguish between good and bad compliments, and a brief exam at the end to recover and consolidate the learning of the acquired information. Behavioral change techniques were employed, such as modeling, reinforcement, and practice. See Figures 1, 2 for samples of dialogue from the chatbot.
Figure 1
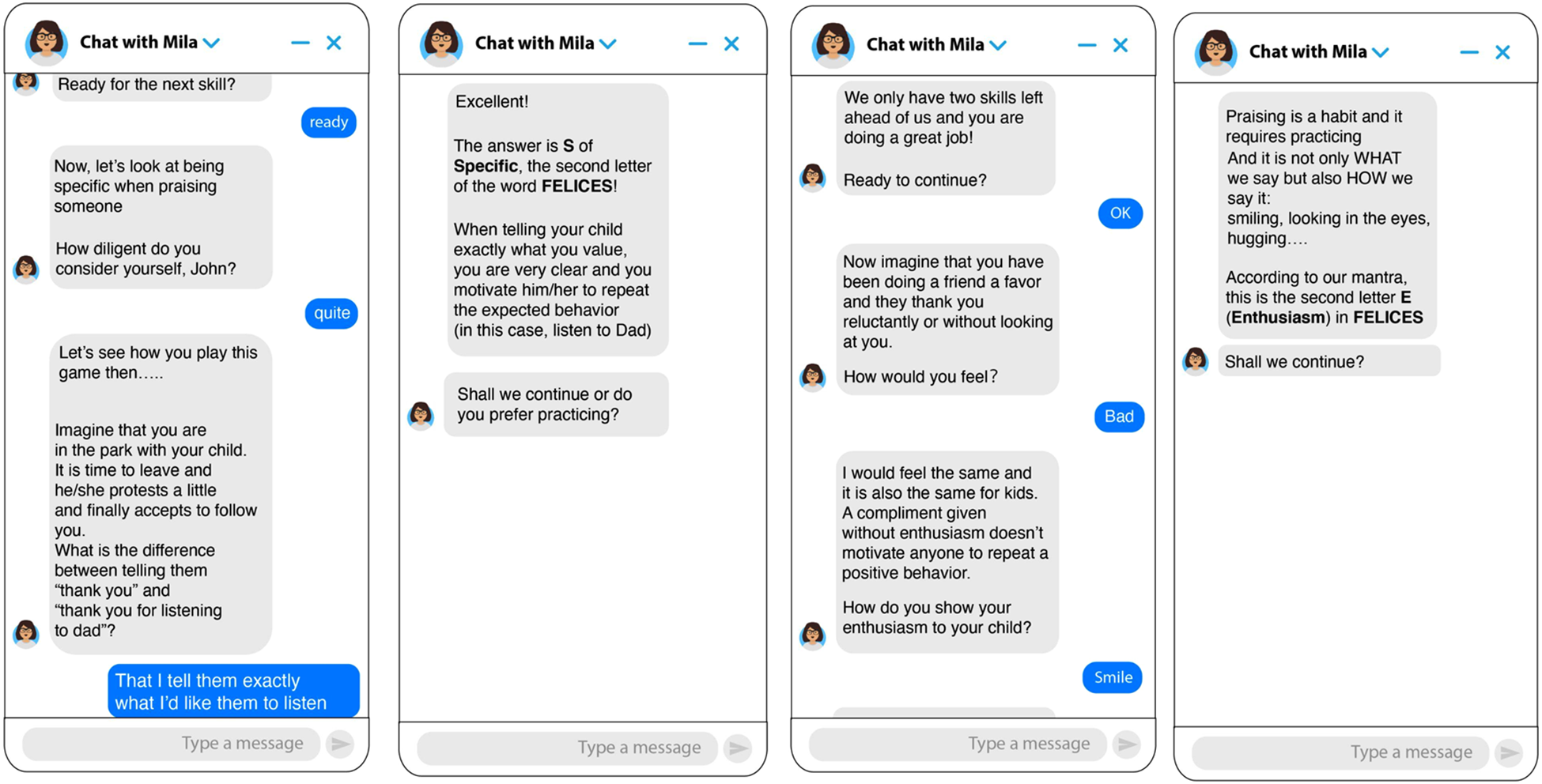
Screenshots of the chatbot for the “Specific” and “Enthusiasm” skills. Note. Images on the left show skill 1 (Specific) and images on the right show skill 4 (Enthusiasm).
Figure 2
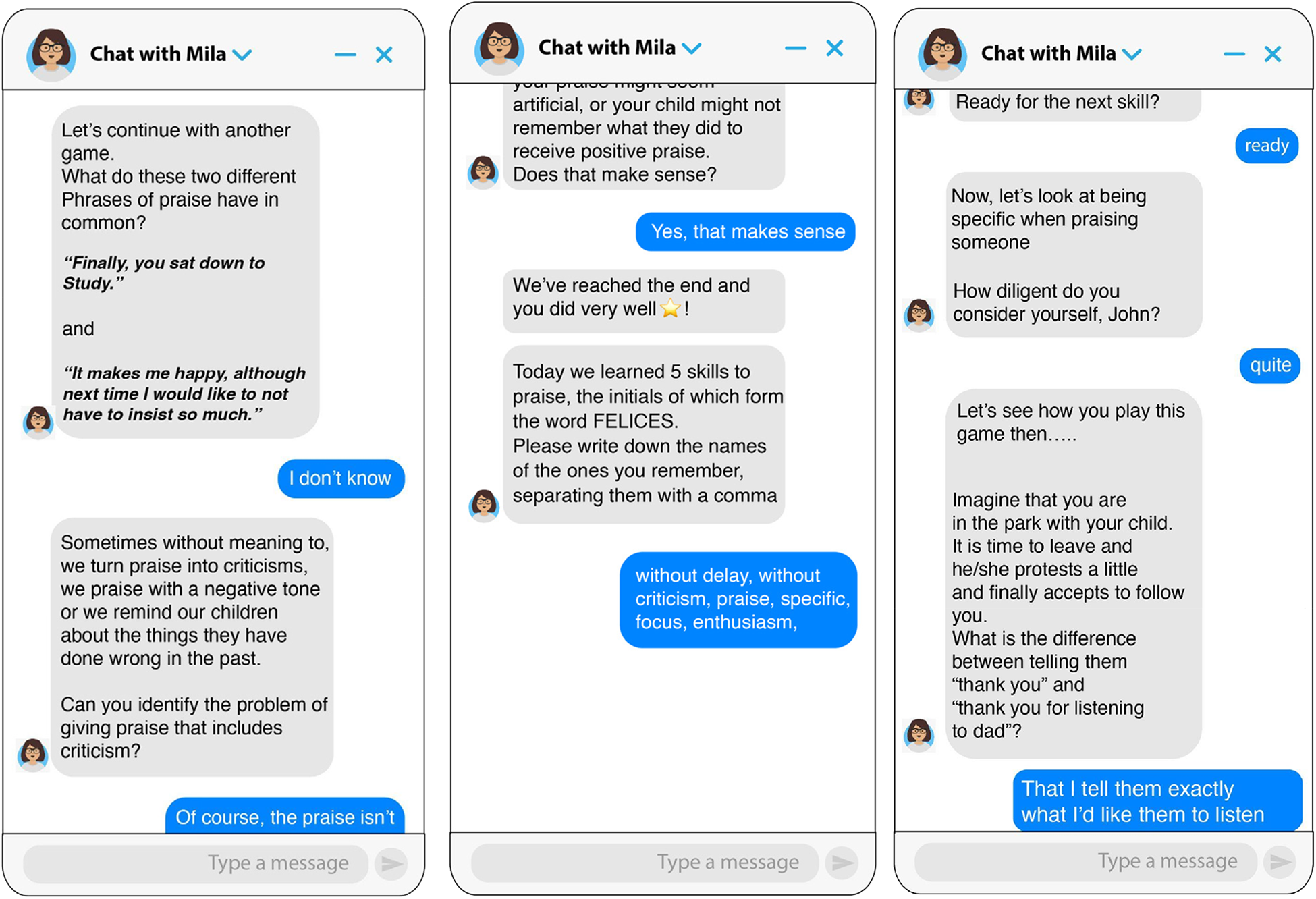
Screenshots of the chatbot for the “Avoid combining praise with criticism” skill and reviewing what was taught at the end of the intervention. Note. The image on the left shows skill 2 (Avoid combining praise with criticism) and the image on the right shows the review of what was taught at the end of the intervention.
Procedure
Participation was anonymous, voluntary, and unpaid. All participants were users of the social media on which the study was conducted (Facebook) prior to the start of the research. While using the social media during their daily life, they were presented with posts with a link to the chat feature in which to initiate the intervention, and an explanation on how to start the conversation with the chatbot. No training on how to use the chatbot was necessary as the chatbot was designed to explain the objectives, timelines and steps of the intervention during the first exchanges of the conversation. Furthermore, as participants were users of the platform, it was expected that they would have previous experience using the chat feature to engage in conversations with other people.
Once the conversation was initiated by the users, the chatbot explained the objectives and assessed the inclusion criteria. Those who met the inclusion criteria gave their consent electronically. All participants completed the baseline assessment and then were randomly assigned to an experimental group (parenting micro intervention) or control group one-day waitlist. After concluding the intervention, user experience and the level of satisfaction of the experimental group were evaluated. In line with ethical requirements in human research, all parents had access to the intervention after the study was completed. This study was approved by the Ethics Committee of the University of Buenos Aires, Argentina (CEI2120007).
Data analysis
The descriptive sociodemographics variables were analyzed for the total sample of participants who started the study (initial sample). Analysis of the current study focus on the user experience of the participants in the experimental group. The completion rate was analyzed using the frequency and percentage of participants who completed each skill. Engagement with the intervention was analyzed using the average number of messages and characters sent. For the analyses related to the user experience, the descriptive characteristics of the variables (Satisfaction, Recommendation, Ease of use, Comfort, Absence of technical problems, Interactivity, and Usefulness in everyday life) were reported.
Results
Demographics
The total sample consisted of 170 parents (Mage = 35.84; SD = 6.47). The majority of participants identified as female (n = 162, 95.3%), married (n = 119, 70%), had a university or tertiary level of education (n = 129, 75.9%), and were employed at the time of the study (n = 139, 81.7%). The average age of the parents' children was 5.69 years old (SD = 2.93), and there was relative gender homogeneity (51.2% girls and 48.8% boys). See Table 1. A total of 89 parents were randomly assigned to the experimental group and 81 to the control group. See Figure 3. There were no significant differences in demographic variables between the experimental and control group or between the intent-to-treat sample and completers. The findings presented in the following sections refer to the experimental condition only, and outcome analyses are reported elsewhere.
Figure 3
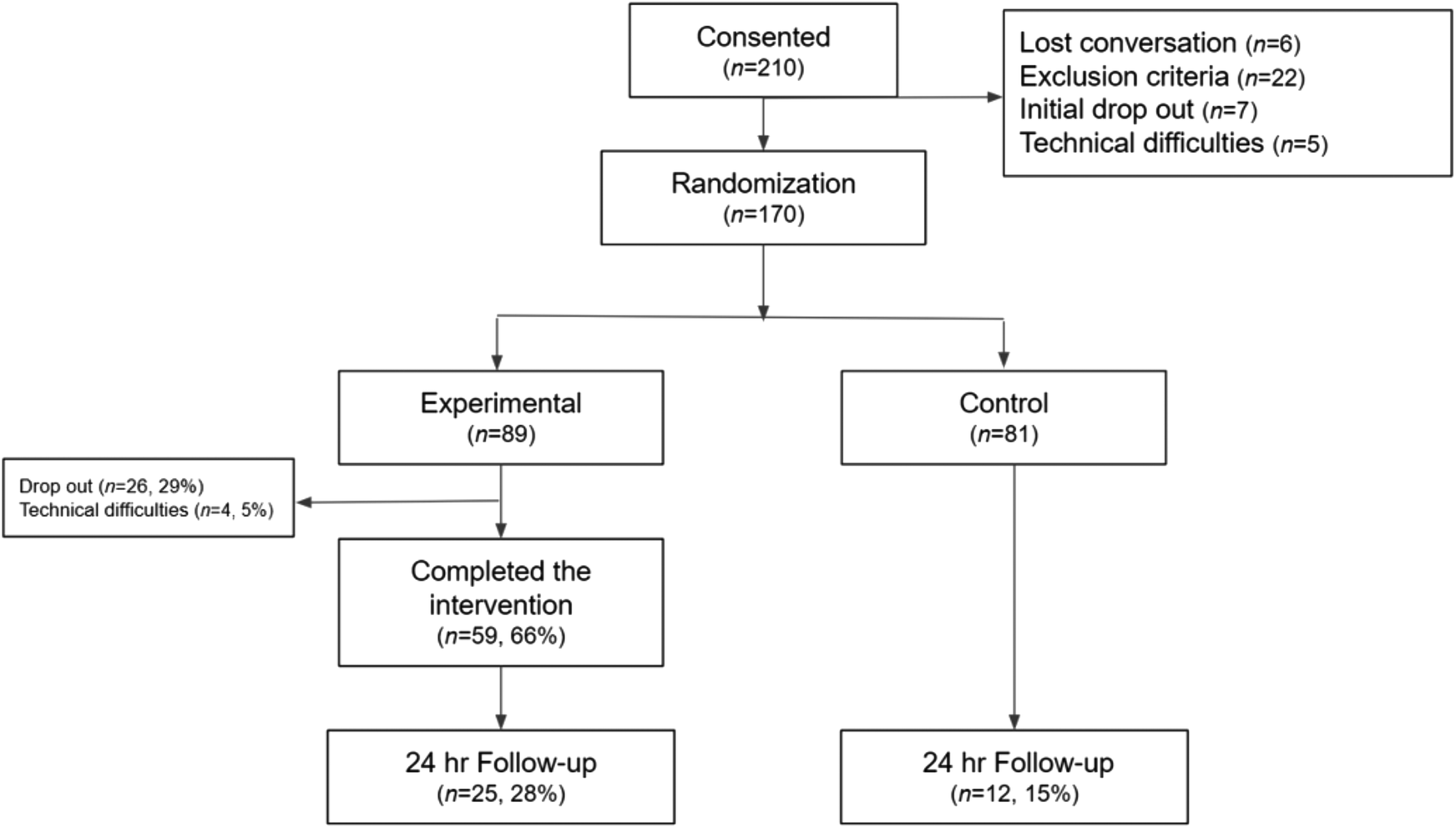
Flow of participants through the study.
Table 1
| Frequency (percentage) | ||
|---|---|---|
| Gender | Female | 162 (95.3%) |
| Male | 8 (4.7%) | |
| Education Level | Primary | 3 (1.8%) |
| Secondary | 27 (15.9%) | |
| University/technician | 129 (75.9%) | |
| Other | 11 (6.5%) | |
| Marital Status | Single | 9 (5.3%) |
| Married | 119 (70%) | |
| Divorced | 11 (6.5%) | |
| Other | 31 (18.2%) | |
| Employment Status | Employed | 82 (48.2%) |
| Self-employed | 57 (33.5%) | |
| Unemployed | 31 (18.2%) | |
| Child Gender | Female | 87 (51.2%) |
| Male | 83 (48.8%) |
Sociodemographic characteristics of baseline sample (N = 170).
Completion rates
The completion rate of the intervention in the experimental group was 66.3% (N = 59). The first skill had the lowest completion rate (82.02%), while all subsequent skills had a completion rate above 92%. See Figure 4 for a description of dropout by skill.
Figure 4
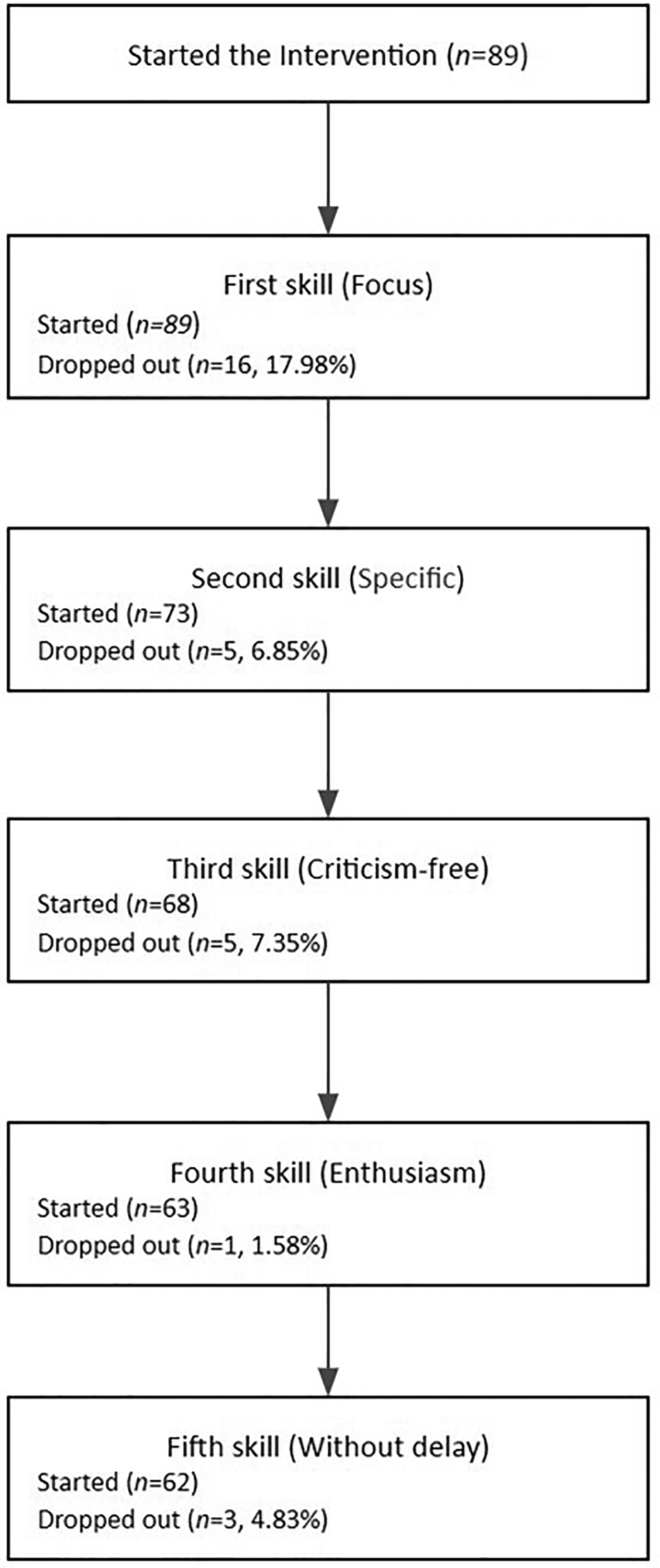
Skills completed.
Throughout the study, the platform's policy regarding hosted chatbots was modified. A restriction on the frequency with which chatbots could reach out to users after a first conversation was introduced, leading to the automatic filtering of most messages sent 24 h after the end of the intervention.
Engagement
Participants sent an average of 49.8 messages (range 20–80, SD = 1.53), an average of 660.9 characters (range 29–2398; SD = 51.68), and an average of 12.98 characters per message.
Satisfaction and net promoter score
Participants provided an average satisfaction score of 4.19 (SD = .79) and reported that they would recommend the chatbot to other parents: Net promoter score was 4.63 (SD = .66) out of 5, with 5 being the highest.
Acceptability
Parents provided a high level of acceptability (ease of use = 4.66 [SD = .73], comfort = 4.76 [SD = .46], lack of technical problems = 4.69 [SD = .59], interactivity = 4.51 [SD = .77], and usefulness for everyday life = 4.75 [SD = .54]). All dimensions measured obtained a mean greater than 4.51. The results indicated a high degree of usability and acceptability perceived by the participants who completed the intervention. See Table 2.
Table 2
| Measurements | M (SD) | Median | Range | 95% IC |
|---|---|---|---|---|
| Ease of use | 4.66 (.73) | 5 | 1–5 | [4.47, 4.85] |
| Comfort | 4.76 (.46) | 5 | 3–5 | [4.64, 4.88] |
| Absence of technical problems | 4.69 (.59) | 5 | 2–5 | [4.31, 4.71] |
| Interactivity | 4.51 (.77) | 5 | 2–5 | [4.33, 4.72] |
| Usefulness in everyday life | 4.75 (.54) | 5 | 3–5 | [4.60, 4.89] |
Descriptive statistics of the variables related to user experience (n = 59).
Note. A Likert scale from 1 to 5 was used, with 1 being “Totally disagree” and 5 “Totally agree”.
Discussion
Chatbots represent a promising intervention for delivering digital mental health. However, research on the user experience of chatbots for parent training has been scarce. This study aimed to assess the user experience of Version 1.0 of a parenting chatbot micro intervention to teach how to praise children and compare these results with those of other mental health chatbots and the beta version of the current intervention (reported in a previous pilot study - (33).
A total of 66.3% of participants completed the intervention. This rate is nearly equal to that of another single-session, web-based, self-guided parenting intervention (36) [66.4%], and comparable to brief self-guided parenting studies utilizing other technologies, such as videos (37) [45%], podcasts (38) [71.9%]), and TV series (39) [65.4%]). Congruent with most literature on online interventions, the completion rate of the current study was lower than the one reported in human-supported digital parenting interventions (40). It was also lower compared to a preventively focused 2-hour face-to-face group discussion on how to manage disruptive behaviors (41). One-session face-to-face interventions have little chance for attrition, though their scalability is lower.
Interestingly, the completion rate doubled that of another single-session parenting intervention delivered contemporaneously in Finland, during the starting stage of the pandemic (42) [32.6%]. Authors have suggested that the high dropout rate may have been due to participants having several support channels, and because the pandemic was relatively controlled in Finland (42) This suggests that digital parental interventions may be most useful in countries such as Argentina, where parents have fewer support resources, and that it was offered at a time of great need.
Compared to the pilot study (33), the completion rate was lower (78% vs. 66.3%), though the present study included more participants and had a more diverse recruitment effort (online vs. snowball recruitment), making the results more generalizable. The current completion rate is higher than the one obtained in another chatbot study conducted in Argentina (40%), although that intervention took place over a longer period of time (8 weeks) (32). Overall, the completion rate of the current study was acceptable and promising, considering that participants did not receive incentives for completion or any human support, which is associated with increased adherence (27).
Regarding attrition rates the first skill (i.e.,: Focus, choose specific behaviors you want to encourage) accounted for more than half of the total drop-outs, and the following skills had considerable lower drop out rates. This first skill demanded more interactions than the subsequent skills, suggesting that more agile modules favor adherence. It has been suggested that participants in chatbot interventions tend to drop out in the first stages because they may not perceive a need for the intervention (43) or are requested to provide too much information (44). Since the majority of participants in the current study were recruited through a Facebook post with little information, some may have only fully understood the objectives of the intervention during the first skill and considered that they did not need it. Additionally, during the first skill, the chatbot asked about parental styles (e.g., “Which words do you usually use to praise your child?”), and some participants may not have felt comfortable sharing that kind of information and decided to drop out. Since the dropout rates were low in the subsequent skills, future iterations of this intervention should test a more agile version of the script aimed at teaching parents to choose specific behaviors they want to encourage.
In terms of engagement, participants sent an average of 49.8 messages during a one-time 15-minute intervention. The number of messages is similar to what was found in the study of the beta version of the parenting micro intervention (M = 54.24) (33). Interestingly, another study on a Spanish-speaking chatbot (32) also reported a high average number of messages sent (M = 116). Overall, previous Spanish-speaking chatbot studies conducted in Argentina (32, 33) along with the current one have shown a higher engagement than what was found in a longer English-speaking chabot study (M = 17.57 messages) (45). It is possible that participants in Argentina are more open to sharing their issues with a chatbot than English-speaking users. In the US, studies with Latinx individuals show greater openness to communicating through text and mobile messaging platforms (46). It is possible that Latinx users may be well suited for chatbot interventions. Finally, previous studies have reported that the higher number of messages sent by the user was associated with higher completion rates (47), and satisfaction with the chatbot (32). Thus, the high number of messages sent by participants in the current study is a positive sign of engagement.
Participants provided a high satisfaction score and reported that they were very likely to recommend the chatbot to other parents. These results were similar to those of other mental health chatbot studies (17, 33), and indicate a good experience among participants. Another chatbot specifically designed for parents of newborns about stress, sleep, and infant feeding had lower satisfaction scores (M = 3.81), perhaps due to many parents experiencing technical problems (46%; (48)) or the specific challenges of having a newborn. It is possible that the high satisfaction level of the current chatbot was associated with the high ease of use and low rate of technical problems. Chatbots that tend to repeat questions or do not understand the user's intention have been reported as a cause of user annoyance (49) and time constraints are frequently reported by parents as barriers to therapy (7). The short duration of the intervention may have promoted greater satisfaction by adjusting to their needs and not asking only a few questions. Therefore, brief chatbot conversations may be well suited for parents struggling with their children's behaviors.
Parents who completed the intervention reported a high level of acceptability for each of the items analyzed (i.e., ease of use, comfort, absence of technical problems, interactivity, usefulness in everyday life). These acceptability levels are comparable to those obtained from other digital parenting interventions such as podcasts (38), websites (50), training television (39), and chatbots for other mental health problems (51, 52). The conversational nature of the intervention may have contributed to this high level of acceptability. Previous studies have identified that parents (53) and young adults (54) value interactive digital interventions in which they can write and talk in the same way they do with humans. Furthermore, the study was conducted during the COVID-19 pandemic, which was associated with increased levels of parental distress and child misbehavior in 2021 (55). Therefore, it is possible that in such a context, an intervention of this kind addressed relevant issues through a flexible and convenient format. More specifically, users rated the intervention's usefulness for everyday life with an average of 4.75 of 5 (95%). Since disruptive behaviors are a prominent problem among children (1), it is possible that the content offered may have aligned well with the interests of the participants in general and in the specific context of the COVID-19 pandemic.
Limitations and future directions
The chatbot designed for the present study used a rule-based model method of input processing and response generation, in which the responses available in the system are chosen based on a fixed set of predefined rules. This model is more vulnerable to user spelling and grammatical errors, and less flexible than retrieval-based and generative models, which use machine learning algorithms and deep learning techniques (56). Sörensen (57) found that error handling and the ability to understand text are crucial in chatbot user perception, which is often difficult to achieve in rule-based models. Therefore, a future iteration of this intervention using more advanced processing systems could improve the participants' experience.
The current study used a one-time micro intervention and measured engagement based on the number of interactions the participants had with the chatbot. While this is a widely used metric in chatbot research, the findings are not generalizable to a whole chatbot-based treatment with multiple sessions. Thus, the engagement with the chatbot across time is unknown. Future studies should assess users' engagement with consecutive chatbot micro-interventions for parenting and incorporate the number of sessions completed as an additional engagement metric.
Completion rates, engagement, and acceptability scores suggest that the participants' experience was positive. However, this does not imply that the intervention has proven to produce significant changes, nor evidence of clinical efficacy and safety. Therefore, results should be read with caution and further research is needed before offering the intervention to a wider public.
Finally, more than ninety percent of the sample identified as female, thus these findings may not be generalizable to fathers. Since, the involvement of both parents tends to increase the outcomes of mental health treatments in children (58), interventions that can facilitate access to both parents are needed. The chatbot nature of this intervention could encourage the involvement of both parents regardless of their gender, and future studies should aim to recruit a more representative sample of parents. Furthermore, most participants had a high level of education so the results are not generalizable to participants with a lower level of education. This limits the generalizability of the results to this population. It is possible that the recruitment materials (e.g., text and photos of Facebook posts) were not sufficiently attractive or clear to populations with lower levels of education. Future studies should be designed to capture the attention and interest of more diverse populations, either by changing the recruitment materials and/or the recruitment channels.
Conclusions
Behavior problems in childhood are highly prevalent, and there is a need to develop novel forms of parent training. Chatbot interventions could increase the accessibility of parent skills training. The results of the present study suggest that parents find a parenting chatbot micro intervention acceptable, have a positive user experience, were engaged, and were highly satisfied with the chatbot. Parents reported that they would recommend the chatbot to other parents and found it useful for everyday life. Chatbot intervention may align well with the participants' interests (especially during a time of need, such as the COVID-19 pandemic). Future studies should focus on the efficacy of the intervention by measuring if parents learn the skills, improve their parenting self-efficacy and decrease disruptive behavior in their children.
Statements
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics Committee of the University of Buenos Aires, Argentina (CEI2120007). The patients/participants provided their written informed consent to participate in this study.
Author contributions
E.B & G.E: substantial contributions to the conception or design of the work; analysis, interpretation of data for the work, drafting the work and revising it critically for important intellectual content, providing approval for publication of the content All other authors: drafting the work and revising it critically for important intellectual content. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors would like to thank the company X2AI in general, and Milagros Escordero, in particular, for their collaboration during the design and development process of the chatbot micro intervention.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1.
Kauten R Barry CT . Externalizing Behavior. In: Zeigler-Hill V, Shackelford TK, editors. Encyclopedia of Personality and Individual Differences. Cham: Springer (2020).
2.
McKee L Colletti C Rakow A Jones DJ Forehand R . Parenting and child externalizing behaviors: are the associations specific or diffuse?Aggress Violent Behav. (2008) 13(3):201–15. 10.1016/j.avb.2008.03.005
3.
De Graaf I Speetjens P Smit F De Wolff M Tavecchio L . Effectiveness of the triple P positive parenting program on parenting: a meta-analysis. Fam Relat. (2008) 57(5):553–66. 10.1111/j.1741-3729.2008.00522.x
4.
Menting AT de Castro BO Matthys W . Effectiveness of the incredible years parent training to modify disruptive and prosocial child behavior: a meta-analytic review. Clin Psychol Rev. (2013) 33(8):901–13. 10.1016/j.cpr.2013.07.006
5.
Sanders MR . Triple P-positive parenting program: towards an empirically validated multilevel parenting and family support strategy for the prevention of behavior and emotional problems in children. Clin Child Fam Psychol Rev. (1999) 2(2):71–90. 10.1023/A:1021843613840
6.
Webster-Stratton C . The incredible years: parents, teachers, and children training series. Resid Treat Child Youth. (2001) 18(3):31–45. 10.1300/J007v18n03_04
7.
McGoron L Ondersma SJ . Reviewing the need for technological and other expansions of evidence-based parent training for young children. Child Youth Serv Rev. (2015) 59:71–83. 10.1016/j.childyouth.2015.10.012
8.
Bausback KB Bunge EL . Meta-analysis of parent training programs utilizing behavior intervention technologies. Soc Sci. (2021) 10(10):367. 10.3390/socsci10100367
9.
Thongseiratch T Leijten P Melendez-Torres GJ. Online parent programs for children's Behavioral problems: a meta-analytic. Eur Child Adolesc Psychiatry. (2020) 29:1555–68. 10.1007/s00787-020-01472-0
10.
Baumel A Faber K . Evaluating triple P online: a digital parent training program for child behavior problems. Cogn Behav Pract. (2018) 25(4):538–43. 10.1016/j.cbpra.2017.10.001
11.
Spencer CM Topham GL King EL . Do online parenting programs create change?: a meta-analysis. J Fam Psychol. (2020) 34(3):364. 10.1037/fam0000605
12.
Suárez A Byrne S Rodrigo MJ . Effectiveness of a universal web-based parenting program to promote positive parenting: patterns and predictors on program satisfaction. J Child Fam Stud. (2018) 27(10):3345–57. 10.1007/s10826-018-1162-9
13.
Vaidyam AN Wisniewski H Halamka JD Kashavan MS Torous JB . Chatbots and conversational agents in mental health: a review of the psychiatric landscape. Can J Psychiatry. (2019) 64(7):456–64. 10.1177/0706743719828977
14.
Beatty C Malik T Meheli S Sinha C . Evaluating the therapeutic alliance with a free-text CBT conversational agent (wysa): a mixed-methods study. Front Digit Health. (2022) 4:847991. 10.3389/fdgth.2022.847991
15.
Fitzpatrick KK Darcy A Vierhile M . Delivering cognitive behavior therapy to young adults with symptoms of depression and anxiety using a fully automated conversational agent (woebot): a randomized controlled trial. JMIR Ment Health. (2017) 4(2):e19. 10.2196/mental.7785
16.
Skjuve M Følstad A Fostervold KI Brandtzaeg PB . My chatbot companion-a study of human-chatbot relationships. Int J Hum-Comput Stud. (2021) 149:102601. 10.1016/j.ijhcs.2021.102601
17.
Dosovitsky G Bunge EL . Bonding with bot: user feedback on a chatbot for social isolation. Front Digit Health. (2021) 3:735053. 10.3389/fdgth.2021.735053
18.
Ta V Griffith C Boatfield C Wang X Civitello M Bader H et al User experiences of social support from companion chatbots in everyday contexts: thematic analysis. J Med Internet Res. (2020) 22(3):e16235. 10.2196/16235
19.
Lim SM Shiau CWC Cheng LJ Lau Y . Chatbot-Delivered psychotherapy for adults with depressive and anxiety symptoms: a systematic review and meta-regression. Behav Ther. (2021) 53:334–47. 10.1016/j.beth.2021.09.007
20.
Jang S Kim JJ Kim SJ Hong J Kim S Kim E . Mobile app-based chatbot to deliver cognitive behavioral therapy and psychoeducation for adults with attention deficit: a development and feasibility/usability study. Int J Med Inf. (2021) 150:104440. 10.1016/j.ijmedinf.2021.104440
21.
Suganuma S Sakamoto D Shimoyama H . An embodied conversational agent for unguided internet-based cognitive behavior therapy in preventative mental health: feasibility and acceptability pilot trial. JMIR Ment Health. (2018) 5(3):e10454. 10.2196/10454
22.
Zhu Y Wang R Pu C . “I am chatbot, your virtual mental health adviser.” what drives citizens’ satisfaction and continuance intention toward mental health chatbots during the COVID-19 pandemic? An empirical study in China. Digit Health. (2022) 8:20552076221090030. 10.1177/205520762210900
23.
Noble JM Zamani A Gharaat M Merrick D Maeda N Foster AL et al Developing, implementing, and evaluating an artificial intelligence–guided mental health resource navigation chatbot for health care workers and their families during and following the COVID-19 pandemic: protocol for a cross-sectional study. JMIR Res Protoc. (2022) 11(7):e33717. 10.2196/33717
24.
Abd-Alrazaq AA Alajlani M Alalwan AA Bewick BM Gardner P Househ M . An overview of the features of chatbots in mental health: a scoping review. Int J Med Inf. (2019) 132:103978. 10.1016/j.ijmedinf.2019.103978
25.
Shumanov M Johnson L . Making conversations with chatbots more personalized. Comput Hum Behav. (2021) 117:106627. 10.1016/j.chb.2020.106627
26.
Viswanath Prakash A Das S. Would you trust a bot for healthcare advice? An empirical investigation. Proceedings of the 24th Pacific Asia Conference on Information Systems. PACIS 2020 Proceedings. (2020) p. 1–14.
27.
Boucher EM Harake NR Ward HE Stoeckl SE Vargas J Minkel J et al Artificially intelligent chatbots in digital mental health interventions: a review. Expert Rev Med Devices. (2021) 18(sup1):37–49. 10.1080/17434440.2021.2013200
28.
Cameron G Cameron D Megaw G Bond R Mulvenna M O’Neill S et al Assessing the usability of a chatbot for mental health care. In: International conference on internet science. Springer (2018) p. 121–32.
29.
Abd-Alrazaq AA Alajlani M Ali N Denecke K Bewick BM Househ M . Perceptions and opinions of patients about mental health chatbots: scoping review. J Med Internet Res. (2021) 23(1):e17828. 10.2196/17828
30.
Daley K Hungerbuehler I Cavanagh K Claro HG Swinton PA Kapps M . Preliminary evaluation of the engagement and effectiveness of a mental health chatbot. Front Digit Health. (2020) 2:576361. 10.3389/fdgth.2020.576361
31.
Gabrielli S Rizzi S Bassi G Carbone S Maimone R Marchesoni M et al Engagement and effectiveness of a healthy-coping intervention via chatbot for university students during the COVID-19 pandemic: mixed methods proof-of-concept study. JMIR MHealth UHealth. (2021) 9(5):e27965. 10.2196/27965
32.
Klos MC Escoredo M Joerin A Lemos VN Rauws M . BungeEL. Artificial intelligence–based chatbot for anxiety and depression in university students: pilot randomized controlled trial. JMIR Form Res. (2021) 5(8):e20678. 10.2196/20678
33.
Entenberg GA Areas M Roussos AJ Maglio AL Thrall J Escoredo M et al Using an artificial intelligence based chatbot to provide parent training: results from a feasibility study. Soc Sci. (2021) 10(11):426. 10.3390/socsci10110426
34.
Baños RM Etchemendy E Farfallini L García-Palacios A Quero S Botella C . EARTH Of well-being system: a pilot study of an information and communication technology-based positive psychology intervention. J Posit Psychol. (2014) 9(6):482–8. 10.1080/17439760.2014.927906
35.
Mesurado B Distefano MJ Robiolo G Richaud MC . The Hero program: development and initial validation of an intervention program to promote prosocial behavior in adolescents. J Soc Pers Relatsh. (2019) 36(8):2566–84. 10.1177/0265407518793224
36.
Sung JY Mumper E Schleider JL . Empowering anxious parents to manage child avoidance behaviors: randomized control trial of a single-session intervention for parental accommodation. JMIR Ment Health. (2021) 8(7):e29538. 10.2196/29538
37.
Dadds MR Sicouri G Piotrowska PJ Collins DAJ Hawes DJ Moul C et al Keeping parents involved: predicting attrition in a self-directed, online program for childhood conduct problems. J Clin Child Adolesc Psychol. (2019) 48(6):881–93. 10.1080/15374416.2018.1485109
38.
Morawska A Tometzki H Sanders MR . An evaluation of the efficacy of a triple P-positive parenting program podcast series. J Dev Behav Pediatr. (2014) 35(2):128–37. 10.1097/DBP.0000000000000020
39.
Sanders M Calam R Durand M Liversidge T Carmont SA . Does self-directed and web-based support for parents enhance the effects of viewing a reality television series based on the triple P – positive parenting programme?J Child Psychol Psychiatry. (2008) 49(9):924–32. 10.1111/j.1469-7610.2008.01901.x
40.
Breitenstein SM Gross D Christophersen R . Digital delivery methods of parenting training interventions: a systematic review. Worldviews Evid Based Nurs. (2014) 11(3):168–76. 10.1111/wvn.12040
41.
Dittman CK Farruggia SP Keown LJ Sanders MR . Dealing with disobedience: an evaluation of a brief parenting intervention for young children showing noncompliant behavior problems. Child Psychiatry Hum Dev. (2016) 47(1):102–12. 10.1007/s10578-015-0548-9
42.
Korpilahti-Leino T Luntamo T Ristkari T Hinkka-Yli-Salomäki S Pulkki-Råback L Waris O et al Single-Session, internet-based cognitive behavioral therapy to improve parenting skills to help children Cope with anxiety during the COVID-19 pandemic: feasibility study. J Med Internet Res. (2022) 24(4):e26438. 10.2196/26438
43.
Bendig E Erb B Meißner D Bauereiß N Baumeister H . Feasibility of a software agent providing a brief intervention for self-help to uplift psychological wellbeing (“SISU”). A single-group pretest-posttest trial investigating the potential of SISU to act as therapeutic agent. Internet Interv. (2021) 24:100377. 10.1016/j.invent.2021.100377
44.
So R Furukawa TA Matsushita S Baba T Matsuzaki T Furuno S et al Unguided chatbot-delivered cognitive behavioural intervention for problem gamblers through messaging app: a randomised controlled trial. J Gambl Stud. (2020) 36(4):1391–407. 10.1007/s10899-020-09935-4
45.
Dosovitsky G Pineda BS Jacobson NC Chang C Escoredo M Bunge EL . Artificial Intelligence Chatbot for Depression: Descriptive Study of Usage. JMIR Form Res. (2020) 4(11):e17065. 10.2196/17065
46.
Schueller SM Hunter JF Figueroa C Aguilera A . Use of digital mental health for marginalized and underserved populations. Curr Treat Options Psychiatry. (2019) 6(3):243–55. 10.1007/s40501-019-00181-z
47.
Linnet J Jensen ES Runge E Hansen MB Hertz SPT Mathiasen K et al Text based internet intervention of binge eating disorder (BED): words per message is associated with treatment adherence. Internet Interv. (2022) 28:100538. 10.1016/j.invent.2022.100538
48.
Wong J Foussat AC Ting S Acerbi E van Elburg RM Chien CM . A chatbot to engage parents of preterm and term infants on parental stress, parental sleep, and infant feeding: usability and feasibility study. JMIR Pediatr Parent. (2021) 4(4):e30169. 10.2196/30169
49.
Denecke K Abd-Alrazaq A Househ M . Artificial intelligence for chatbots in mental health: opportunities and challenges. In: HousehMBoryckiEKushnirukA, editors. Multiple perspectives on artificial intelligence in healthcare: Opportunities and challenges. Cham: Springer International Publishing (2021). p. 115–28. [cited 2022 Jul 7]. (Lecture Notes in Bioengineering). Available at:10.1007/978-3-030-67303-1_10
50.
DuPaul GJ Kern L Belk G Custer B Daffner M Hatfield A et al Face-to-face versus online behavioral parent training for young children at risk for ADHD: treatment engagement and outcomes. J Clin Child Adolesc Psychol. (2018) 47(sup1):S369–83. 10.1080/15374416.2017.1342544
51.
Gaffney H Mansell W Tai S . Conversational agents in the treatment of mental health problems: mixed-method systematic review. JMIR Ment Health. (2019) 6(10):e14166. 10.2196/14166
52.
Mehta A Niles AN Vargas JH Marafon T Couto DD Gross JJ . Acceptability and effectiveness of artificial intelligence therapy for anxiety and depression (youper): longitudinal observational study. J Med Internet Res. (2021) 23(6):e26771. 10.2196/26771
53.
Brager J Breitenstein SM Miller H Gross D . Low-income parents’ perceptions of and engagement with a digital behavioral parent training program: a mixed-methods study. J Am Psychiatr Nurses Assoc. (2021) 27(1):33–43. 10.1177/1078390319872534
54.
Koulouri T Macredie RD Olakitan D . Chatbots to support young Adults’ mental health: an exploratory study of acceptability: acceptability of mental health chatbots for young adults. ACM Trans Interact Intell Syst. (2021) 12:1–39.
55.
Sullivan AD Forehand R Acosta J Parent J Comer JS Loiselle R et al COVID-19 and the acceleration of behavioral parent training telehealth: current status and future directions. Cogn Behav Pract. (2021) 28(4):618–29. 10.1016/j.cbpra.2021.06.012
56.
Adamopoulou E Moussiades L . An overview of chatbot technology. In: MaglogiannisIIliadisLPimenidisE, editors. Artificial intelligence applications and innovations. Cham: Springer International Publishing (2020). p. 373–83. (IFIP Advances in Information and Communication Technology).
57.
Sörensen I. Expectations on chatbots among novice users during the onboarding process. (2017). p. 1–16.
58.
Clarke AT Marshall SA Mautone JA Soffer SL Jones HA Costigan TE et al Parent attendance and homework adherence predict response to a family–school intervention for children with ADHD. J Clin Child Adolesc Psychol. (2015) 44(1):58–67. 10.1080/15374416.2013.794697
Summary
Keywords
chatbot, artificial intelligence, conversational agent, parenting, user experience (UX), intervention
Citation
Entenberg GA, Dosovitsky G, Aghakhani S, Mostovoy K, Carre N, Marshall Z, Benfica D, Mizrahi S, Testerman A, Rousseau A, Lin G and Bunge EL (2023) User experience with a parenting chatbot micro intervention. Front. Digit. Health 4:989022. doi: 10.3389/fdgth.2022.989022
Received
07 July 2022
Accepted
20 December 2022
Published
11 January 2023
Volume
4 - 2022
Edited by
Stephen Schueller, University of California, United States
Reviewed by
Graciela Rojas, University of Chile, Chile Lubna Daraz, Montreal University, Canada
Updates
Copyright
© 2023 Entenberg, Dosovitsky, Aghakhani, Mostovoy, Carre, Marshall, Benfica, Mizrahi, Testerman, Rousseau, Lin and Bunge.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
* Correspondence: G. A. Entenberg guidoentenberg@etci.com.ar E. L. Bunge ebunge@paloaltou.edu
Specialty Section: This article was submitted to Human Factors and Digital Health, a section of the journal Frontiers in Digital Health
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.