 Ronny Klawunn
Ronny Klawunn Urs-Vito Albrecht
Urs-Vito Albrecht Deliah Katzmarzyk
Deliah Katzmarzyk Marie-Luise Dierks
Marie-Luise Dierks- 1Department for Patient Orientation and Health Education, Institute for Epidemiology, Social Medicine and Health System Research, Hannover Medical School (MHH), Hanover, Germany
- 2Department of Digital Medicine, Medical Faculty OWL, Bielefeld University, Bielefeld, Germany
Introduction: Hospitalised patients could benefit from the emergence of novel technologies for nursing care. There are numerous technical products available, but these rarely find their way into practice. Further knowledge is required about the circumstances under which technology in nursing is accepted and used. In the research project “Centre for Implementing Nursing Care Innovations”, technical innovations are implemented on a trauma surgery inpatient ward in Germany. After implementation, it was investigated: Which implemented technologies are accepted/rejected, and which factors influence the acceptance/rejection of technology for nurses?
Material and methods: A focused ethnography was used, containing two approaches: First, participant observation was conducted to examine nurses’ and patients’ interaction with technologies. Observations were fixed in a field research diary and analysed using evaluative qualitative content analysis. Second, a questionnaire was used by nurses to provide information about the use frequency and technology suitability. The results of the study were consolidated and analysed using the UTAUT model.
Results: Seven studied technologies can be summarised in four result categories: (1) A Mobilising mattress, a Special projector and a Sound pillow are accepted and used by nurses and patients, because they offer a way to provide high quality care with little additional effort. (2) A Fall prevention system is consistently used in patient care as a work obligation, but since nurses consider the system error-prone, acceptance is low. (3) An Interactive therapy ball is accepted but nurses cannot use it due to the high workload. (4) An App for nurse-patient communication and a work-equipment tracking system are not used or accepted because nurses do not see a practical benefit in the systems.
Discussion: Acceptance or rejection of a product does not necessarily equate to use or non-use of the technology. Before implementation, technology acceptance among users occurs as prejudice—when users are given time to experiment with technology, intention-to-use can stabilize into sustained use. Accepted and used technologies can serve to mask problems (such as staff shortages) and encourage problematic developments, such as the reduction of contact time at the bedside. Therefore, technology acceptance should be qualified in asking to what accepted technology contributes.
1 Background
1.1 Nursing, technology and acceptance
With the growing use of digital technologies in healthcare, new technologies become increasingly available for nursing in recent years. For this profession in particular, technology is one possible response to the challenges of an ageing population being cared for by a decreasing number of available professionals (1, 2). Technology uptake in nursing care needs to accelerate to use the potential benefits of new technologies, and enablers and barriers related to technology implementation should be investigated and understood. Potential factors are numerous, e.g., a lack of fit between technology output and user need, inappropriate design for use needs, misguided implementation efforts or institutional limitations (3, 4). These could have an impact on the use and acceptance of nursing technologies.
Behavioural intention or actual use of technology has been studied regarding the acceptance of nursing technology. However, while new technology is implemented, the user's perspective may change due to the occurrence of unintended or unanticipated consequences of technology use (5), the social and contextual influences of implementation or facilitating conditions. For instance, through getting to know a new device and getting used to its functions and abilities, a negative expected usefulness and ease of use may shift to a positive attitude and vice versa. More research is needed to learn how and why behavioural intention shifts to a sustained and accepted actual use or a disruption of use and rejection of technology.
1.2 State of research
The adoption of new technologies in nursing is related to various determinants of technology acceptance. In the case of tele-nursing and remote visual monitoring of patients, studies have indicated that while the technology may reduce the number of falls, the acceptance of technology may only be moderate (6). Similarly, in the case of mobile healthcare communication tools, it has been shown that promoting early adopters can significantly influence user's behavioural intention to use the technology (7, 8). Similarly, in the case of mobile healthcare communication tools, it has been shown that promoting early adopters can significantly influence user's behavioural intention to use the technology (9). Users tend to favour mobile tools for inter-professional or professional-patient communication when tools are easy to use and efficient (10, 11). For AI technology that improves decision-making, another study have found that technology acceptance may be high among nurses and other professionals if the technology incorporates professional expertise and evidence into decision-making (3). However, such a technology may be associated with fears of loss of autonomy and expected negative impact on clinical workflows (12).
Only some studies have investigated how and why the intention to use technology in nursing may shift towards accepting or rejecting it after implementation. One study in a critical care nursing unit has demonstrated in a pre/post comparison of technology implementation that self-concern and expectation for ease of use decreased for nurses after adapting the technology (13). However, concerns about technology's impact on practice and perceived usefulness increased at the same time (ibid.). Another study has investigated the implementation of a digital oral healthcare intervention in Norway. As users adopted the new technology, they gradually changed their mode of use from—what the authors described as—“norm-based to routine-based behaviour”, highlighting the relevance of familiarisation with technology and the corresponding shift of user behaviour (14). For tele-nursing technology, it has been shown that only the performance expectancy was significant for caregivers’ behavioural intentions. After introducing the technology, the facilitating conditions and the performance became relevant for caregivers (15).
1.3 Research project and research question
The “Centre for Implementing Nursing Care Innovations” study (Funding: German Federal Ministry of Education and Research, funding number 16SV7892K) aims to implement new technologies in a trauma surgery inpatient ward of a university hospital in Germany. After technology introduction, we investigate the modes nurses’ use technologies and how patient care and nursing processes will change during technology implementation. The research question is:
Which implemented technologies are accepted/rejected by nurses, and which factors influence the acceptance/rejection of these technologies?
We conducted an ethnographic study and evaluated and reported the results using the Unified Theory of Acceptance and Use of Technology 1-model (16). The advantage of this model, which unifies eight separate models, is the provision of various explanatory factors that can predict or explain both the intention to use technology and the actual use (17). UTAUT conceptualises acceptance and use not merely as individual user decisions but places user behaviour and intentions in the context of institutional, organisational, and social environmental factors that may be influenced by mediating factors (age, gender, experience and voluntariness of use).
The study's implementation strategy allows to investigate how behavioural intention to use technology may shift to actual acceptance or rejection. Following Greenhalgh et al., this strategy involves two approaches: (1) We cooperated with the study hospital and managerial nursing staff to create institutional conditions for a successful and sustainable introduction of new technology to facilitate change of working structures (implementation) (18). (2) To select suitable technologies, we involved nurses from the study ward in a participatory manner by consulting them about potential technology and its usefulness (dissemination) (ibid.). For this purpose, we identified areas of nursing care on the project ward that could be supported with technical solutions—these areas involved, for instance, assistance with geriatric patients, dangers related to falls or pressure ulcers, inefficient patient communication or long walking distances (19). Based on these areas of need, the research project first took a closer look at potentially useful technologies and examined their implementability. For this purpose, an internal guideline was developed that included the IT perspective, nursing science, ethical, legal and social implications and the known study literature on the technology (19, 20). Once the potential technical and organizational implementability of the technology had been confirmed, it was presented to nursing staff. In workshops, they reflected on their behavioural intention to use the technology within their daily working routine (21, 22). If nurses showed their interest in using the presented technology and therefore articulated their intention to use it, the implementation of the product followed. Afterwards, the use of technology and patterns of acceptance or rejection has been observed. All costs that are associated with the purchase and maintenance of the technology were covered by the project budget as part of the research project. In the case of maintenance and repair work, the corresponding effort was shared between employees of the project station and the research project (see Limitations).
1.4 Overview of implemented technology in the research project
During the research and implementation activities, seven technologies were implemented and researched at the project ward, the technologies can be found in Table 1.
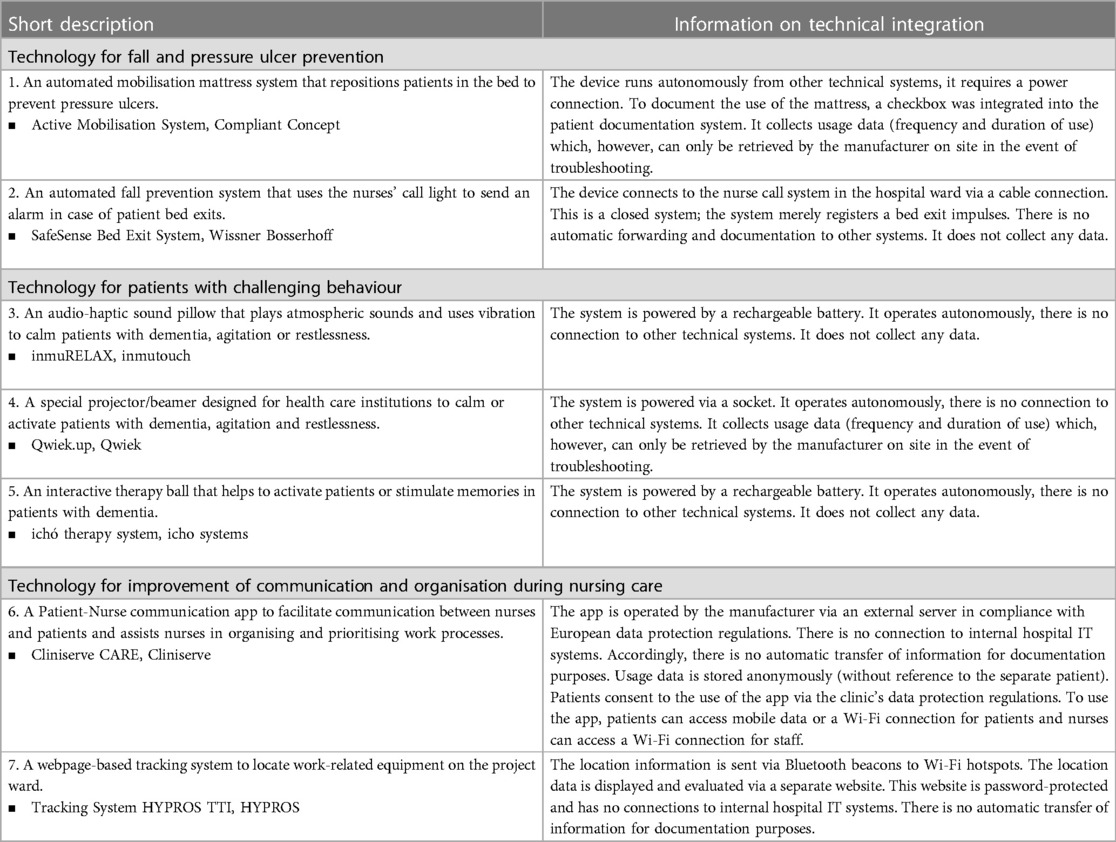
Table 1. List of implemented and studies technologies.
2 Materials and methods
2.1 Study design
The study used a focused ethnographic, multi-methods investigation with a distinct qualitative emphasis. Focused ethnography is suitable for investigating social fields with high degrees of professionalism and functional differentiation by studying the entanglements and interactions between individual actors, institutional processes, settings and technologies (23). A main goal is to investigate social and cultural processes that are implicit or difficult to articulate for those being studied (24, 25). Compared to anthropological ethnography, the focused account is characterised by short field stays and an intense data collection phase (26). The following methods were applied:
1. Participant observation of nursing workflows to explore the use of implemented technologies and
2. Questionnaire survey to explore the nurses’ perspective on the usability of the implemented products.
The steps of data collection, processing and analysis are described in the following sections, an overview of the research design can be found in Figure 1.
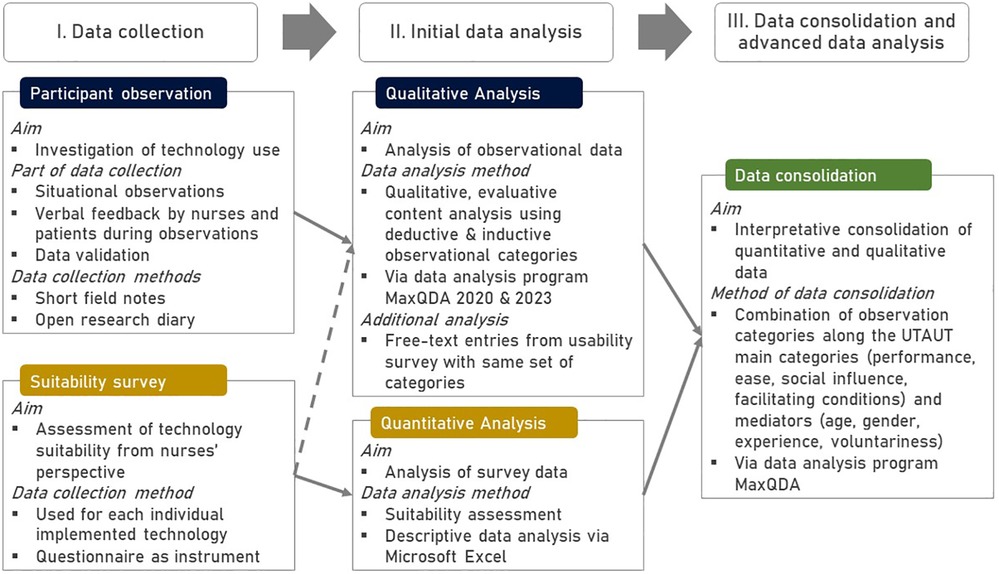
Figure 1. Research Design.
2.2 Methods 1: data collection
(a) Participant observation
The observation aimed to follow professional nurses during their workday for several hours to explore work processes and interactions with patients and other nurses with the introduced technologies. The observation was carried out by the author RK and conducted as an “observer as participant”, which means that the observer role tends to be passive, yet transparent to all participants in the field. The choice of non-functional, everyday clothing and a restrained accompaniment was intended to keep the observer passively in the background while enabling the investigation of a native perspective of the observed concerning specific “situations, activities and actions” (26).
One of the members of the research project (not the observer and no co-author) acted as a gatekeeper to gain access to the field, as he also worked as a nursing professional on the project ward. In the course of the observations, it was possible to establish personal relationships with other nursing staff who allowed access to the ward to observe shifts. In terms of recruitment, all nurses were eligible to participate whom: (1) worked as professionally trained on the project ward, (2) were currently using a technology of interest, (3) would like to be accompanied and (4) gave written consent to be observed (see Ethical Considerations section).
At the beginning, fixed time points for the observations were set. However, this pattern needed to be adjusted, e.g., because some technology was not used for an extended period and then used intensively for a short period. These required spontaneous station visits outside the fixed observation pattern until sufficient information for each technology was gathers. Another way of achieving data saturation was to present and discuss the results with the nursing staff on the ward (see section Quality Assurance).
An observation guideline (see Table 2) with specific questions was designed to help the observer during the field stay (27). These questions were developed deductively from existing models on technology implementation (28), adoption (29, 30), technology acceptance (16) and intention (31)—the guideline is shown in Table 2. The instrument was developed based on multiple theoretical starting points to integrate different perspectives on technology use. The categories were later integrated into the UTUAT model, which can also be found in Table 2 (see also 2.4, Methods III). The guiding questions were discussed by the research team and field tested before its initial use—no changes were needed afterwards.
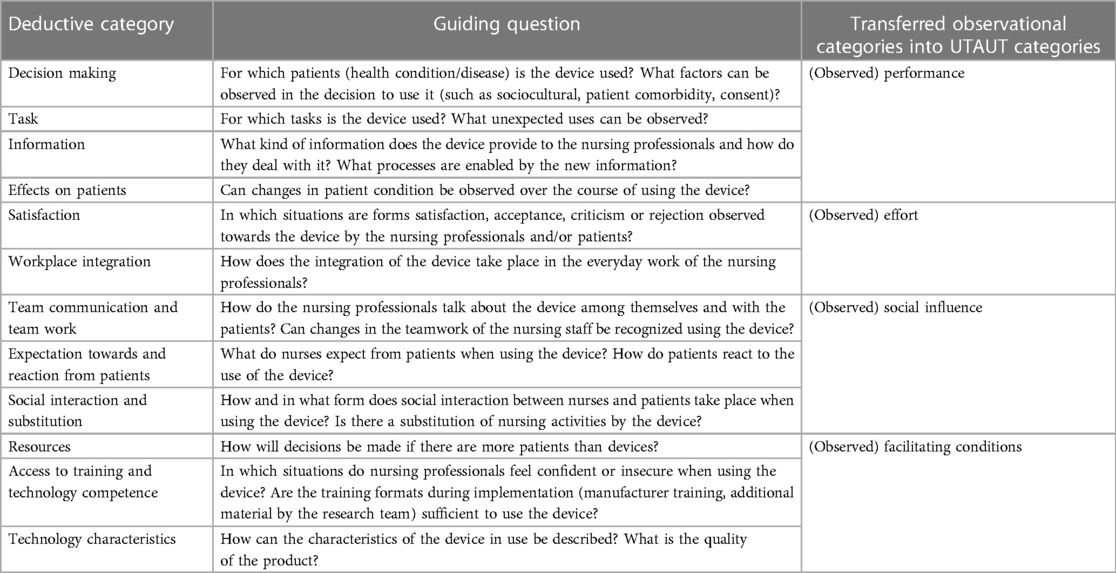
Table 2. Deductive categories and guiding questions for the observational units.
During the field stays, handwritten notes containing summaries, situation descriptions, reflections and ideas were taken. After each observational unit, the observation questions listed in Table 2 were used to structure the writing of open-ended, chronological fieldwork diary entries that reflect observed situations in detail, reproducing dialogues, and characterising people, technologies and situations (32).
(b) Questionnaire-based survey on technology suitability
A technology suitability questionnaire was used to investigate the range of opinions of the nursing professionals. This instrument was used additionally to the observations, because the observation could only incorporate the views of individual employees (who were working at the times observed), rather than obtain the diversity of opinions on a technical product. Therefore, a questionnaire was used that descriptively included the respondents’ views on the suitability of the technology for use. Since no meaningful case numbers can be obtained on the project ward, the use of the questionnaire can only be classified as a supplement and contextualization of the qualitative results from the observation. This instrument was developed and used in another research projects (22, 33). The questionnaire was provided to all nurses on the project ward for each implemented product. It contained four sections:
1. Three items on the general use of the product since its introduction (use yes/no, frequency of use and, reasons for not using the technology).
2. General questions covering usability, workflow, compatibility, functionality, product quality and patient well-being.
3. Questions specific to the technology covering power supply, alarms, screens, mobility, consumables, and reprocessing.
4. Further comments on the device to be entered in free text entries.
In the general and specific sections, the questions were answered using a five-point Likert scale from ’Strongly agree’ to “Do not agree at all”—or “not applicable”.
This is a measurement instrument for technology suitability and not an instrument from the field of technology acceptance/UTAUT research. Therefore, the findings of the suitability survey are classified under the UTAUT category of (observed) effort.
All nurses received the questionnaire for each of the implemented technologies three months after the first deployment of the given technology, either in workshops or in their mailboxes on the ward. In the case of using the individual post box, they were notified at the time of distribution and with a reminder by E-Mail. Due to the long implementation phase in the study, the number of employees on the project ward varied significantly, but on average 22 full-time staff are employed on the ward. However, this number varies, mainly due to staff shortages. As the study design was set up in such a way that only one ward was equipped with technology, the questionnaire could only be used in one setting and comparisons with other wards/settings were not planned in the study design (see also Limitations).
2.3 Methods II: initial data analysis
(a) Qualitative data analysis—evaluative qualitative content analysis
The entries from the open field research diaries and the free text entries from the technology suitability survey were analysed using evaluative qualitative content analysis (34). While applying this method, each deductive main code received a set of at least three sub codes for (1) a positive manifestation, (2) a negative manifestation and (3) a neutral or non-evaluative category (35). For example, the main code of “work integration” received the sub codes (1) “smooth integrated”, (2) “problems with integration” or (3) “other”—in this care, a forth sub code for ambivalent observations were also used.
The guiding questions in Table 2 were used to develop the main codes deductively. Only one inductive main code was added for “Expectations of new technologies”. Through this approach, a code system of main codes and sub codes (see Supplementary Data Sheet) were developed that helped to organise the data material and to perform a pre-analysis.
(b) Quantitative data analysis
In the questionnaire-based survey on technology suitability, the answers to the second and third areas (general and specific aspects of the technology) were analysed quantitatively (33). For this purpose, the scores achieved by the technology in each area were first expressed as a percentage of the maximum possible score. These two percentage results were then weighted according to the number of items in each area, and an average, general value were given. If a technology achieved up to 49%, it is considered unsuitable; if it achieved 50%–69%, it is rated as suitable to a limited extent; and if it achieved 70% or more, the technology is rated as very suitable.
2.4 Methods III: data consolidation
Quantitative results were compared with the qualitative analysis of the observation data and the free-text entries of the appropriate questionnaires. The data collection and analysis was performed parallel rather than sequentially. We merged and compared the data to identify consistencies, inconsistencies or complementarities (36). The basis for data consolidation and analysis was the UTAUT model, initially presented by Venkatesh in 2003 (16). Four main categories are presented in this model:
▪ “Performance expectancy is defined as the degree to which an individual believes that using the system will help him or her to attain gains in job performance.” (ibid.)
▪ “Effort expectancy is defined as the degree of ease associated with the use of the system.” (ibid.)
▪ “Social influence is defined as the degree to which an individual perceives that important others believe he or she should use the new system.” (ibid.)
▪ “Facilitating conditions are defined as the degree to which an individual believes that an organizational and technical infrastructure exists to support use of the system.” (ibid.)
The use of the UTAUT model in our study served two purposes. (1) To arrange and summarise the results along these categories for transparent reporting. (2) To use a mix of qualitative and quantitative findings to explore how much influence each category had on technology use, acceptance, rejection, and adaptation. Therefore, the observation categories from Table 2 were assigned to one of the four main categories, which can be found in the same table. The survey results were assigned to effort expectance based on the construct “Suitability”. In our study, the UTAUT model was used to evaluate observed user behaviour (therefore “Observed Performance” etc.), not used to predict user intention or behaviour. The four mediators’ gender, age, experience, and voluntariness of use (ibid.) will be addressed in the results section if relevant to the reporting.
2.5 Ethical considerations
The research project was approved by the Ethics Committee of the Hannover Medical School on the 6th of July, 2018, ID: 7933_Bo_K_2018 (amended 16th of July, 2020). The procedure was reviewed by the hospital's staff council and the clinic data protection officer. The data protection-compliant processing of research results (above all with the aim of protecting study participants) was carried out in accordance with the guidelines of the University Hospital, above all with the help of lockable rooms in the case of hard copies and password-protected drives in the case of digital data. Raw data was only shared with research project participants, and patient care leaders were merely given access to analysed, non-personal, summarized data as required, making re-identification implausible.
(a) Participant observation
The scheme for situationally appropriate privacy expectations was used to identify which individuals in the field should be asked for written consent to observation (37). Written informed consent was obtained from professional nurses observed during their shifts. Before giving their consent, nurses received an introduction to the study's goals and reasons. If possible, participants in the field were informed of the observer's presence, especially to patients when first entering the patient's room (38).
(b) Questionnaire-based survey on technology suitability
Nursing professionals who completed the questionnaire also filled out a written consent form. Sociodemographic data (such as years of professional experience or age) were not collected due to the small size of nursing staff to avoid re-identification.
2.6 Quality assurance
For the reporting on methodical decisions and processes in this paper, the COREQ-Checklist was used (39)—all relevant information are provided in the dedicated section of the paper or in Supplementary Image S1.
(a) Participant observation
(1) Key observational findings on the impact of technology implementation were presented, discussed and again documented in dedicated validation workshops as a form of “respondent validation” (40). (2) The research team reviewed and discussed result plausibility and implications at periodic meetings internally and in external research workshops. (3) Parts of the results have already been presented regarding individual technologies and selective research questions at conferences (41, 42). (4) The observed nurses were offered to read the diary entries after completing them; however, no participant used this offer. Coding and consolidation of the data material was performed independently by two authors (RK & DK) and then compared. Intercoder reliability was not numerically calculated.
(b) Questionnaire-based survey on technology suitability
Two independent data entries were made to ensure no errors occurred during the transfer. The main results of this survey were presented in the validation workshops to the nurses mentioned above. All results from the questionnaire survey were presented, interpreted and discussed within the interdisciplinary team of the research project.
3 Results
3.1 Participant observation
Observations began in July 2020. New technology has been explored in 23 observation units, representing 38.5 h of observation time. The author RK conducted all observations. The average time of an observation unit is two hours. These observations resulted in 132 pages of field research diary entries. Member validation workshops were protocolled. The results of these data collections are summarised in this chapter. In the course of the participant observations, fifteen nurses could be accompanied on their shift. All but one of the nurses responded positively to be observed—the person who did not wish to participate has been omitted from all observational descriptions.
Table 3 provides an overview of the observations’ results on the implemented technologies reported by UTAUT's main categories. The boxes in the table are marked with colours and indicate whether the observation results for the corresponding UTAUT category are characterised as favourable for the use of the technology (green box), adverse and unfavourable (red box), or both positive and negative and thus ambivalent (yellow box). Categories with no effect are left blank.
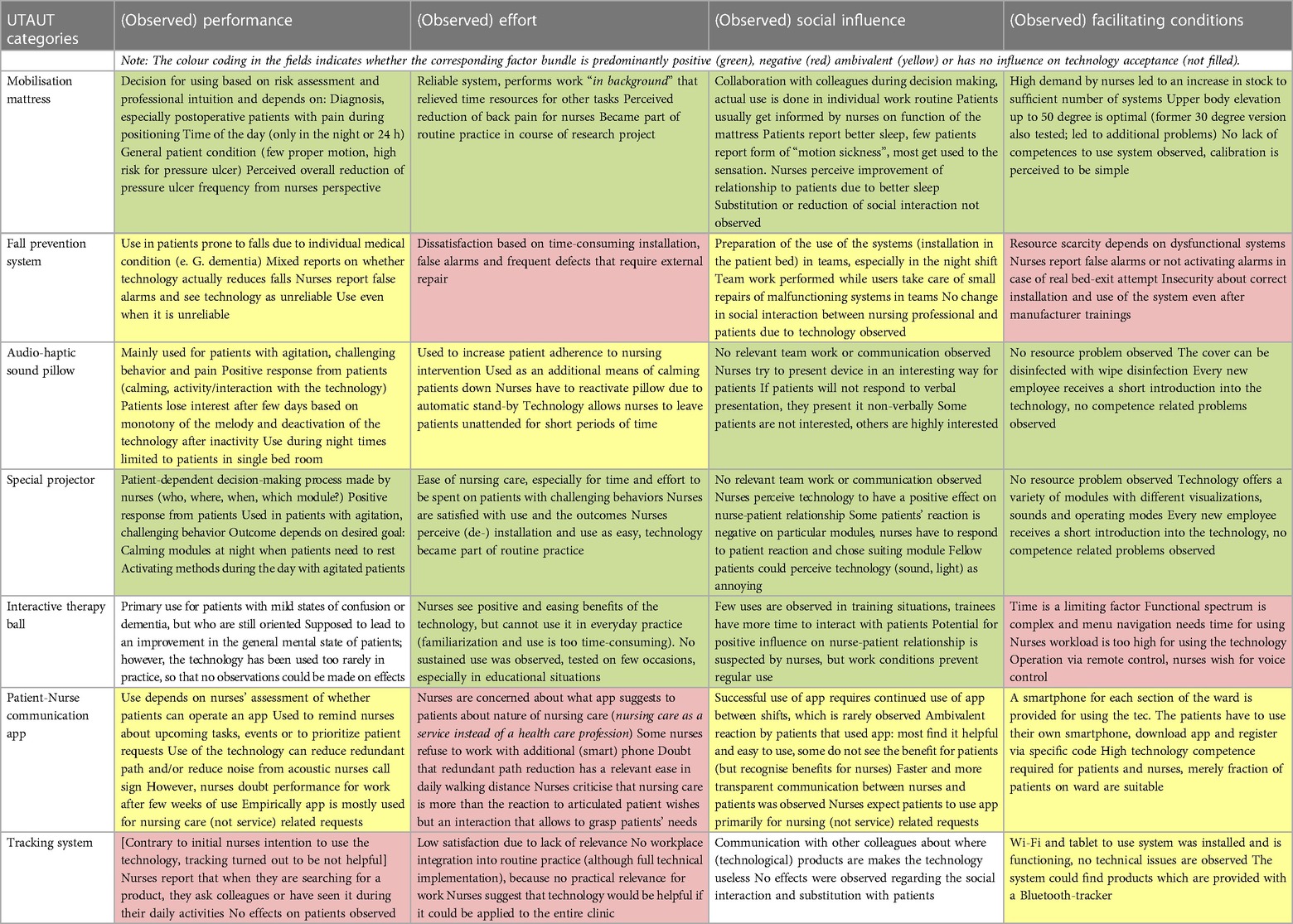
Table 3. Results of ethnographic observations analysed by UTAUT-categories.
3.1.1 (Observed) performance
The mobilisation mattress and the special projector provide a positively perceived performance from the point of view of nurses and patients. The mobilising mattress is frequently used on the project ward. The individual risk assessment for the development of pressure ulcers is not the sole deciding factor for whom, when and how the system is used:
While we walk to the next patient room, the nurse says that the mattress: “almost does not matter during the day”. She explains that many patients lying in the systems require intensive care anyway, such as patients with incontinence pads that need to be changed regularly. For these patients the mattress is advantageous at night because using the system helps position patients less frequently, and one needs to wake them up less often. […] Patients who suffer from much pain are an exception: People who have suffered trauma will experience less pain due to the system’s movement. (Field Research Diary_Mobilization mattress-BE04, p. 2)
Other nurses run the system on all patients and use the system’s pause function instead to perform interventions. The special projector is primarily used in patients with dementia or agitated behaviour in two different ways: One is to calm nervous patients and address challenging behaviour. The other way is by reactivating apathetic patients, in whom the use of the projector activates memories. According to the nurses, both ways can help improve care of these patients, making care delivery easier. The decision-making is biography-based or stems from getting to know the patients' behaviour. The special projector and the mobilisation mattress are often used together.
Technologies that have shown mixed and thus ambivalent performance in the ward are observed for the sound pillow, the fall prevention system and the communication app. The sound pillow functions according to its intended purpose, as the following situation description shows:
A mask for inhalation is placed on the patient’s face—the sound pillow lies on his chest. The nurse seems surprised and says this was not easy in the last few days because the patient kept pulling the mask off his face. The patient now seems sleepy—about 2 min pass. The patient gets quieter and finally almost falls asleep. The patient seems so calm that the nurse wants to leave him alone to return in 15 min. (Field Research Diary_inmu-BE01, p. 28)
Most patients lose interest in the technology after a few days due to its repetitive sound. Therefore, an actual benefit is limited to a time range that is shorter than the patient's hospital stay. For the communication app, situations are observed where patients send their requirements, nurses read them and can react according to the current workflow, for instance to take medication with them to the room. However, the app is rarely used since some nurses question whether the app makes a difference in everyday work. For the fall prevention system, it is observed that nurses respond immediately to a bed exit. However, the perceived performance of the system is low as users report frequent false alarms or missing alarms, resulting in low system confidence.
The nurse reports that the system was running overnight but did not activate even when the patient already stood in the room. (Field research diary_SaSe-BE01, pos. 9)
The perceived performance of the system for equipment tracking is low. The system proves to have no technical problems in practical tests, so non-use initiates from a lack of practical relevance for the users. Communication and teamwork among nursing colleagues to find equipment is easier to realise according to nurses.
The interactive therapy ball is rated as neutral regarding its perceived performance because users cannot operate the technology as intended (this will be explained in detail below).
3.1.2 (Observed) effort
Nurses perceive the mobilising mattress and the special projector as easy to use. Both systems are perceived to be reliable and supportive of work processes, saving effort on time-consuming tasks and helping cope with work process-related requirements. They are perceived as being easy to install and are considered part of daily work routines. The devices do not need to be operated constantly but can be used partly autonomously (in the background), as the following entry illustrates:
While documenting, the nurse said, “On days like today, the system is worth its weight in gold.” I asked what she meant by that. She explained that with the system, she could sit at the PC for as long to document. Repositioning the patient to prevent pressure ulcers would require her to interrupt her current activity regularly. I asked her if she was confident the system was doing a good job in the background. She confirmed this and said that it was a great relief. (Field Research Diary_Mobilization mattress-BE04, p. 3)
The nurses repeatedly emphasise that using the mattress and the projector does not mean patients are left alone for long periods and interactions between nurses and patients are not reduced. Instead, it changes the nature of the interaction by removing specific tasks perceived as unpleasant, such as positioning patients.
Positive effects and ease of use are identified with the sound pillow and the interactive therapy ball, but to a limited extent. Nurses evaluate that the sound pillow has a calming effect on patients. This calming effect, in turn, directly influences patient adherence to specific therapeutic measures and makes it easier for patients to cope with difficult emotions or pain. However, many patients lose interest in the technology after a few days of use. A patient can use the pillow without the constant supervision of a caregiver. For the therapy ball—that in contrast needs the permanent presence of a caregiver –, no sustainable use can be observed. Nurses and trainees use this device in a few instances and have positive experiences, but could not use it in everyday practice due to a lack of time. Therefore the technology's easing effect could not be realised under the given work organisation.
In the case of the communication app, the tracking and fall prevention systems, findings suggest that the devices require additional effort for little to no benefit. Nurses do not see any practical benefit for the tracking system. However, an expansion within the entire hospital could be beneficial. For the communication app, some nurses find the additional smartphone impractical in everyday practice, because they are not always within reach or their pocket are already packed with other items. While the fall prevention system is used in practice, nurses mention frequent technical problems, most of the users see the product as having little overall benefit:
The nurse currently has a patient lying in the fall prevention system. This patient has not tried to get up recently, but the system has been alarming at regular intervals. This makes the system unusable; she adds “You make an effort to set it up, and then it does not even work”. (Sound pillow_Fragment 01)
3.1.3 (Observed) social influence
Four of the introduced technologies positively influenced the interaction between nurses and patients. The three technologies for patients with challenging behaviour performed similarly in this area. Teamwork is performed merely when a nurse seeks advice from colleagues on selecting suitable patients. After that, the nurses work with the technology without further cooperation. The technologies have a positive impact on nurse-patient interactions, as the following two research notes demonstrate:
For the special projector, the nurse likes the forest-walk module. She had a patient with dementia who used this module and, while watching, tried to find out where the shots might have been taken. (Special projector_Fragment_01, pos. 13)
The nurse had a night shift, and a patient could not find rest and walked around the room for several hours. She gave him the sound pillow. After that, the patient slept soundly for hours. (Field Research Diary_Communication app _BE02, Pos. 5)
Nurses also emphasise a module that displays a night sky with shining stars that is selected for patients to fall asleep at night. Nurses say that the calming and activating use of the sound pillow and special projector enable easier interaction with these patients and fewer challenging situations and conflicts. While using the mobilizing mattress, patients find better sleep than those who have to be woken several times during the night for positioning. Nurses describe that sleep improvement also improves relationships with patients.
An ambivalent influence of technologies on the social interaction of users is found in the fall prevention system and communication app. The fall prevention system does not directly affect the relationship between nurses and patients. Although patients are repeatedly surprised that nurses quickly enter the room when they try to stand up. Repeated technical problems, malfunctioning components, or the system installation lead to negatively perceived collaboration between nurses. The mediator category voluntariness of use explains why the product is frequently used on the project station. It seems plausible that the nursing supervisor requires the system to be used for liability. This factor is part of why the device is frequently used, but the overall satisfaction is low. While the Patient-nurse communication app is used, some patients particularly emphasising the benefit of additional information, such as how long they must wait for a response. The following conversation is observed between a nurse and a patient:
A feature of the app that both consider useful is task prioritisation. Both talked about how it can make sense if you know that a request such as “close the window” occurs in one room and “severe pain” in another. Both agree that it is good to process first the pain and then the window request. (Field Research Diary_Communication app_BE01, Pos. 21)
For other patients, the app has no advantage because the waiting time does not change. In addition, nurses are cautious in selecting the appropriate patient to use the app. They are concerned about low-skilled patients who send requests by accident. Others fear that the app suggests professional nursing to the patients as a (hotel) service.
None of the technologies introduced have an overall negative impact on the users’ social relationships. Regarding the tracking system, nurses find no support for the technology because communication between colleagues is more effective. Therefore, the social factor is still a robust explanatory category for non-use of technology.
3.1.4 (Observed) facilitating conditions
For the special projector, the sound pillow and the mobilisation mattress, sufficient resources for using the technologies—like technical infrastructure—are provided. Therefore, no conflicts about too few devices are found for these technologies. All nurses receive detailed training for these devices. The mobilising mattress had a problematic feature at the beginning that deactivated the system if the patient raised the head of the bed by more than 30 degrees. This often leads to unintended deactivation by patients. After consultation with the manufacturer, the limit was elevated to 50 degrees. Since this update, nurses reporte fewer problems. The sound pillow and the special projector are easy to integrate into existing facilities. All three systems can be cleaned with the regular disinfectant on the ward and no severe technical malfunctions are reported.
For the tracking system and the communication app, the findings indicate that facilitating conditions have both positive and negative influences on the use of technology. Although nurses receive training on how the technologies work, in practice, there are regular uncertainties about use. The tracking system and the communication app run mostly without technical problems. The wi-fi coverage on the station is sufficient to provide both services most of the time. In a few instances, there have been examples of the tracking system showing the wrong location of the tracked equipment:
The nurse says there was an incorrect location in the system for an electronic rail. He says that it was indicated in a different room than it was. […].The access points are installed too close to each other […].’ (Field Research Diary_Communication app_BE02, item 31)
Nurses suspects that messages from the communication app sometimes do not get through in real-time. For patients, there are currently no input devices for the app on the ward so patients must bring their smartphones to use the app. Nurses must explain the downloading and functioning to patients if they require assistance. The nurses receive this point critically since they have no time to train patients. For this reason, nurses select patients in particular by anticipating their technical abilities and patients must be motivated to use the app.
The technical and organisational conditions are limiting factors for the therapy ball and the fall prevention system:
“I have no time for [the therapy ball]. An everyday companion would have time.” “I dealt with it once and then I knew how it worked, but now I have already forgotten about it.” (Protocol of member validation meeting, June 2023)
Hence, the device's menu navigation is seen as complicated. The nurses would like to use the therapy ball and would enjoy working with it but do not see the time for this. The fall prevention system exhibits system errors and false or outstanding alarms that hinder its use. Caregivers repeatedly report that the device's correct installation and operation is complicated, resulting in uncertainties.
3.2 Technology suitability from nurses’ perspective
The survey on technology suitability could be conducted on all technologies. The results can be found in Table 4.
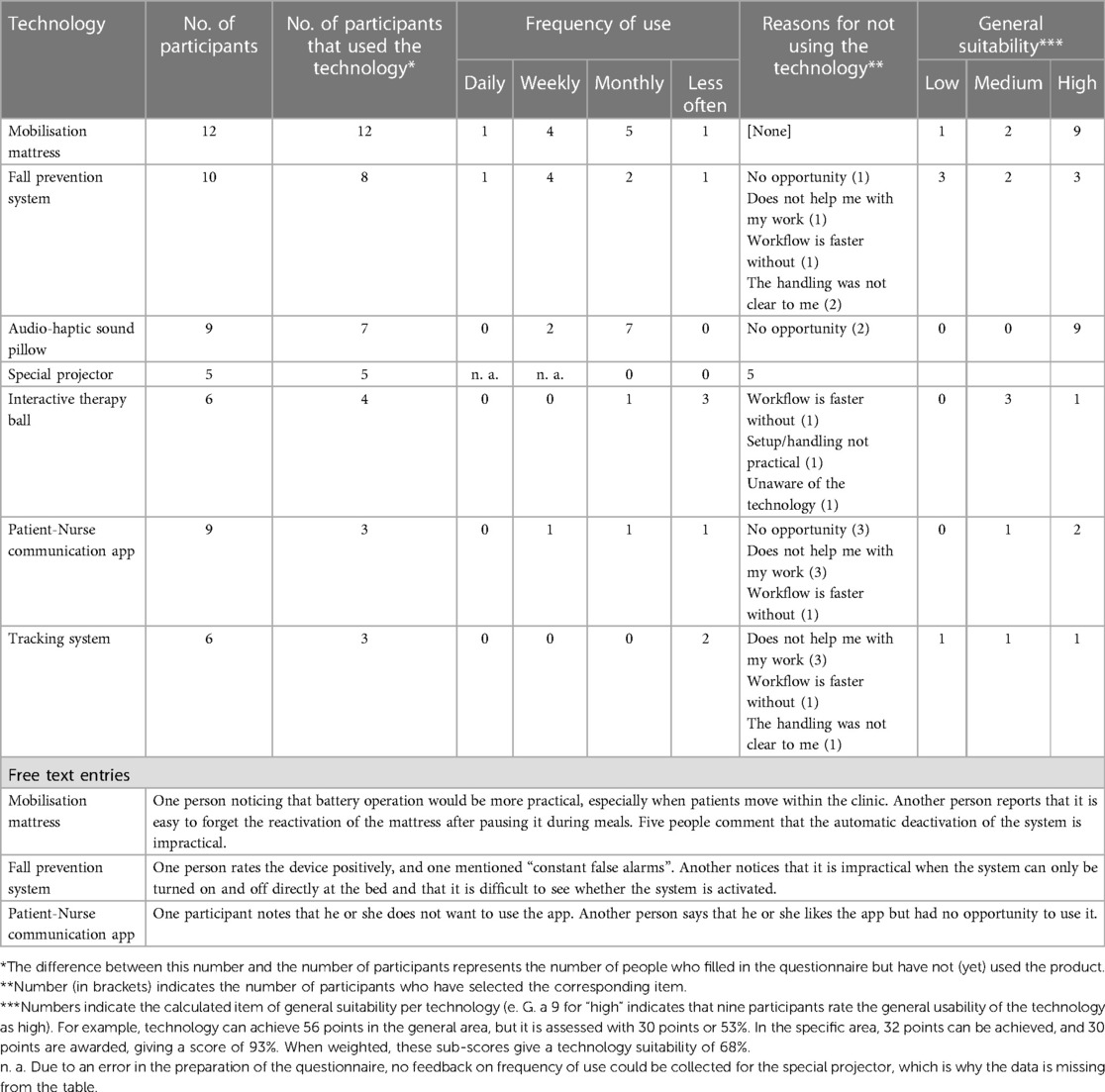
Table 4. Results of the suitability survey by nurses that used implemented technology.
The number of participants varies because the average number of nurses working on the project ward varied during the research project and not all nurses participated in the survey. Similarly, not every technology was used by all employees; in particular, temporary workers often stated that they had not used the technology due to short training periods on the ward. Other people also stated informally that they did not have time to complete the questionnaires during daily work. For these reasons, the number of participants in the surveys varied from five to twelve employees (as described above, an average of twenty-two people work on the ward at full-time employment).
The comparison between the observational results and the standardised survey shows a coherent picture. The technologies are described as easing and beneficial (mobilisation mattress and special projector) are also evaluated positively. In contrast, the ambivalent (sound pillow and therapy ball) and unfavourable technologies (fall prevention system, communication app, and tracking) receive mixed evaluations. The frequency of use is also consistent to qualitative results; The technology that stood out in the observations as accepted and used received a higher frequency in the survey, like for the mobilization mattress (used daily or multiple times a week).
3.3 Summary of results
A summary of results can be found in Table 5. The results are consistent with the observational data and the survey on technology suitability.
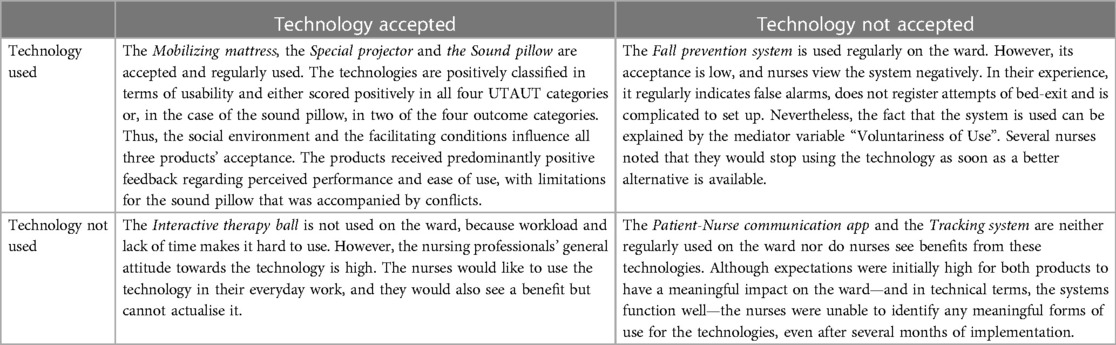
Table 5. Summary of results according to use and acceptance.
4 Discussion
4.1 How accepted and not used technology can (not so easily) be distinguished
The observation results of the study were summarised along the four main UTAUT categories and the positive, negative or ambivalent influence on technology acceptance per category per product was identified. These results can be compared with the technology suitability survey, which provides information on the assessment of nurses and the frequency of use. But how to answer which technology was used, which was not and how to distinguish the influencing factors as enabling or hindering factors?
The conclusion of whether a technology was accepted or rejected cannot be based solely on the positive, negative or ambivalent results of individual UTAUT categories, because this would confuse the phenomena to be explained (explanandum) with what it is explained by (explanans) (43). Until the outcome of the implementation process is uncertain, classifying the influential factors from the UTAUT categories in the implementation process is unattainable. At this point, frequency of use could be utilised as a proxy for general product acceptance but little data could be collected on this. In addition, a technology may be highly accepted even though it does not need to be used regularly.
To solve this problem, we use ethnographic sensibility. This term refers to a feeling or impression towards the ethnographic, i.e., the lived and experienced reality in the research field, about its “complexity, contradictions, possibilities, and grounds [for the observed] cultural group” [(44), see also (45)]. This sensitivity was gained by the observer over years of field research activity and enables knowledge about the users’ general attitude towards the technologies, which was needed to situate the results eventually.
The above presented summary of four result categories leads to the follow consequences:
(1) A predominantly positive influence of the technology in terms of the UTAUT categories (see Table 3, green fields) strongly indicates that the technology is used and accepted.
(2) Use and acceptance cannot be equated. The fall prevention technology—acceptance low, but regularly used—and the interactive therapy ball—high acceptance, but not used—shows that these outcomes do not have to exist simultaneously.
(3) The occurrence of more than one origin of negative and ambivalent influence of the technology (see Table 3, red and yellow fields) strongly indicates that the technology is not accepted or used regularly.
(4) The main categories of the UTAUT model can be a strong indicator for explaining technology acceptance. However, they should be distinct from explanatory factors because factors like perceived usefulness or ease of use occur within broader socio-technical constellations and contexts of actualised technology use (46). Explanatory power unfolds with an understanding of the use context. This context was approached in our study by using ethnographic sensitivity.
To conclude the four consequences, it takes more than adding variables to predict user acceptance towards technologies. Instead, acceptance emerges as the result of complex socio-technical arrangements in which users must convince themselves of the benefit of technology for their actions by constantly trying, failing and succeeding.
4.2 Intention to use technology must be stabilized by experimenting
Some expectations users set regarding a technology's usefulness were not met after implementation. The intention to use technology indicates a necessary curiosity that motivated the start of technology use. However, this is no guarantee that a sustainable technology acceptance will occur. Users take cautious first steps in using novel technologies when familiarity with and skill to use technology still needs to be established. In this initial, critical experimentation phase, users renegotiated attitudes toward the technologies through positive or negative experiences.
On the one hand, unanticipated adverse effects—such as frequent false alarms—could change a high expectation into scepticism or reservation (5). On the other hand, surprising or hoped-for effects that turn out to be true could result in positive attitudes among users. This was frequently observed, for instance, when nurses asked whether they could be supplied with more system mattress, sound pillows or special projectors to cover demands.
Different users face the introduction of technologies with different skills and prior experience and with varying degrees of optimism or scepticism. Age and experience as mediator variables in the UTAUT model provided a valuable orientation for our analysis. However, introducing a helpful technology can transform existing work conditions, changing how a work field and a social reality functions (47). While the different preconditions among users may provide clues to different levels of acceptance and rejection, a helpful technology can change these preconditions among users [for the case of generalised distrust among nurses towards technology, see (48)]. Thus, it is more plausible to assume that a rejected technology does not bring any actual benefit instead of assuming a primordial attitude of rejection among users who would not give valuable technologies a chance (and vice versa).
4.3 Acceptance may not be sufficient
Our results show that four technologies—the mobilising mattress, the special projector, the sound pillow and the fall prevention system—offer a way to mitigate the high demands of a professional nursing work environment that is increasingly characterised by staff shortages and a growing number of multi-morbid patients. The other three technologies—the tracking system, the communication app and the therapy call—could not meet these demands. From an acceptance perspective, this can be understood as fulfilled or unfulfilled device performance expectations.
Alternatively, these results can also be explained by the fact that the successful technologies can be operated in a background mode. A “background relation” between a technology and a user can be explained by a device that the user does not continuously operate—i.e., it works in the background—but nonetheless shapes the environment and the user's experience (49). A background technology does its work without the need for permanent operation. Solely in case of a malfunction, users are reminded about its importance and have to act in an effort to repair it—an example would be an air conditioning system. It is opposed to a technology that requires the user's constant input.
The features of the mobilising mattress, the fall prevention system, the special projector and sound pillow can be utilised without constant manipulation and nurses’ presence, which makes them handy on stressful workdays. The communication app, the tracking system and the interactive therapy ball cannot be used similarly. For the therapy ball, for instance, nurses emphasised that the permanent input needed for the system’s operation is the reason they were not using the system after all.
However, when viewed from the perspective of patients, the background characteristic is problematic. After all, this implies that patients receive parts of care by technology. For instance, in the case of the mobilising mattress, re-positioning a patient to prevent pressure ulcers is not executed by a human but by the technical system, changing the caregivers’ task from an active part of doing the reposition to the passive part or controlling the technologies output. At the same time, nursing action as interaction work consists of more components than executing a nursing care action (50). As such, it also consists of emotional and sentimental labour, in which the nurse can recognise the patient's needs through interaction and communication with them and then react based on these encounter (ibid.).
The mere adoption of tasks by technology is no evidence of less social interaction between professionals and patients—also we did not collect data on contact times. However, technology that is successful because it is usable in the background may eventually reduce opportunities for interaction. The evidence of successfully implemented technology that supports nurses in managing their increasingly demanding workday under staff shortages might indicate that technology is accepted because it enables them to continue working under problematic conditions. Implementing technology may therefore reinforces problematic developments (more missing human resources) rather than questioning it. For this reason, looking purely at acceptance as a measure of successful use of technology in care may fall short. Instead, the potential change in the levels of interaction and resonance between nurses and patients caused by technology use would be a possible outcome for qualifying technology acceptance (51).
4.4 Limitations
(1) Effects were primarily perceived by the observers and the perspective of the observed is only described from “outside” No interviews were conducted—at the time of reporting—to involve the individual perspectives. However, at least in their validity, results could be discussed and confirmed with nursing professionals.
(2) The results from the questionnaire are subject to substantial limitations since participation varies to a high degree.
(3) The study's argument is based on the assumption that, due to a participatory introduction process, only those technologies found their way onto the ward that the nurses also desired. However, it was impossible to verify whether this assumption could be applied to all nurses.
(4) The narrow patient population on the project ward influenced the selection and the use of the technologies. In the example of the communication app, little benefit for the nurses could be seen because too few patients had the skills to use an app. In this respect, the (qualitative) transferability of the results to other clinical settings is limited.
(5) Patients’ perspective is marginally represented in this paper because patients in the case of the project station are mostly passive technology users or beneficiaries and have no direct experience with the devices or cannot verbalise this, for example, due to dementia.
(6) All costs associated with the acquisition, operation, malfunction and repair of the technologies were covered by project funds. Therefore, the transfer of interpretations to other health care settings is restricted, particularly in terms of (sufficient) resources. In other health care institutions, for instance, budget restrictions could trigger negative usage effects. The German healthcare system continues to lack sustainable, cross-setting and comprehensive solutions for financing innovative technologies. The same applies to the amount of work required for maintenance, servicing and in the event of malfunctions and repairs. In non-research settings, this must be carried out by employees and can have additional, negative consequences for the use of innovative technologies.
(7) The decision to equip one ward with technology in the course of the implementation activities was designed to achieve a summative (qualitative) effect through the combination of different technology approaches. Although this decision enables the investigation of interaction of technologies in one setting, it disqualifies cross-setting comparisons of the effect of technology.
(8) The seven selected systems are not integrated into existing hospital IT-systems—either because they have their own technical infrastructure (e.g., the app for communication or the tracking system) or because they do not need to communicate with other systems. This limits the implications of the study through the selection of technologies, as it was not possible to make any statements about the usage effects of interoperable systems and their advantages and disadvantages. The decision in favour of isolated solutions was made due to closed hospital IT systems that did not allow the installation of integrated systems.
(9) A direct calculation of the frequency of technology use (e.g., how often nurses used technologies or on how many patients the technologies were used on) was not achieved. The main reason for this is that it would only have been possible to count on site, but the research team could have not been permanently on the side and the nursing staff refused to document the frequency of use due to a lack of time. For this reason, the feedback from the observation and validation workshops and the corresponding item in the written survey were used. Although these are merely indications and no hard figures, they are not of primary interest in the context of the research question, as the aim is to identify qualitative reasons for use and non-use.
(10) The influence of the mediator variable gender cannot be systematically evaluated in this study, as most employees on the ward are female. However, a direct comparison of the data with the few (three to four) male nurses does not reveal any relevant differences in use patterns or attitudes toward technology.
5 Conclusion
In the research project “Centre for Implementing Nursing Care Innovations”, we explored the implementation and use of seven technologies intended to support nursing care in a hospital-based trauma surgery ward. The question was investigated which of these technologies are used and accepted or not used and rejected and which factors are responsible for this.
A Mobilising mattress, a Sound pillow and a Special projector were accepted and used, whereas a Fall prevention system was used but technology acceptance among nurses were low do to a perceived low technology quality. A system to track work equipment and an communication app for patients and nurses were neither used nor accepted because users were not able to find a suitable use case, whereas an Interactive therapy ball was accepted among nurses but work condition prevented its application.
The following practical implications can be drawn:
▪ The finding indicates that acceptance of a technology should not be confused with the use of a technology. The technology might be used but acceptance is low, if, for instance, the use of the product is expected as a work obligation. In this case, users may find the technology not helpful and sustainable transfer of technology in routine practice is weak. Likewise, a technology may be accepted and users would like to transfer it into routine practice but circumstances hinder its use. In this case, an institution should facilitate chancing working conditions if the technology is desired.
▪ The categories of performance, effort, social influence, and facilitating conditions provide a practical analytical approach to identifying acceptance or rejection factors. However, they merely provide indications of actual usage and acceptance patterns. The analysis and thus the understanding of the context of technology application itself is necessary in order to be able to classify and qualify overall acceptance.
▪ Experimenting with technology stabilises the intention-to-use into a sustainable use of technology that is adapted to the application context. If users do not find a way to transform this intention into a helpful benefit or if negative unintended or unanticipated consequences emerge, acceptance of the technology remains low. Intention-to-use is not a solid characteristic among users. Users should be given the opportunity to experiment with a new technology to stabilize an intention to use.
▪ In the practical field of nursing, the outcome of technology acceptance should not be viewed simply as the realised use of technology but rather against the background of whether nursing tasks and goals have been achieved through the use and acceptance of technology, such as the improvement of emotional, sentimental and interactive work between nurses and patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Hannover Medical School. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
RK: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. U-VA: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. DK: Data curation, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. M-LD: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article.
The study was funded exclusively by the German Federal Ministry of Education and Research, 16SV7892K. All material costs for technologies involved were purchased using these funds.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdgth.2024.1330988/full#supplementary-material
References
1. World Health Organisation. World Report on Ageing and Health. Geneva: World Health Organization (2015). p. 246.
2. Seibert K, Domhoff D, Huter K, Krick T, Rothgang H, Wolf-Ostermann K. Application of digital technologies in nursing practice: results of a mixed methods study on nurses’ experiences, needs and perspectives. Z Evid Fortbild Qual Gesundhwes. (2020) 158:94–106. doi: 10.1016/j.zefq.2020.10.010
3. Jones EK, Banks A, Melton GB, Porta CM, Tignanelli CJ. Barriers to and facilitators for acceptance of comprehensive clinical decision support system-driven care maps for patients with thoracic trauma: interview study among health care providers and nurses. JMIR Hum Factors. (2022) 9:e29019. doi: 10.2196/29019
4. Jauk S, Kramer D, Avian A, Berghold A, Leodolter W, Schulz S. Technology acceptance of a machine learning algorithm predicting delirium in a clinical setting: a mixed-methods study. J Med Syst. (2021) 45:48. doi: 10.1007/s10916-021-01727-6
5. Zwart Fd. Unintended but not unanticipated consequences. Theor Soc. (2015) 44:283–97. doi: 10.1007/s11186-015-9247-6
6. Ergai A, Spiva L, Thurman S, Hatfield M, McCollum M, Holmes M. The effectiveness of remote video monitoring on fall prevention and nurses’ acceptance. J Nurs Care Qual. (2023) 39(1):24–30. doi: 10.1097/NCQ.0000000000000716
7. Hawksworth LT, Raja S, Drake J, Davis T, O'Brien A-M, Brady JM. Exploring nurses’ perceptions of the barriers and facilitators that influence acceptance and use of remote visual monitoring technology. J Nurs Manag. (2022) 30:3466–80. doi: 10.1111/jonm.13822
8. Offermann J, Rohowsky A, Ziefle M. Emotions of scepticism, trust, and security within the acceptance of telemedical applications. Int J Med Inform. (2023) 177:105116. doi: 10.1016/j.ijmedinf.2023.105116
9. Byrd TF 4th, Kim JS, Yeh C, Lee J, O'Leary KJ. Technology acceptance and critical mass: development of a consolidated model to explain the actual use of mobile health care communication tools. J Biomed Inform. (2021) 117:103749. doi: 10.1016/j.jbi.2021.103749
10. Marcus J, MacMillan D, Ketchie M, Clark PC. Nurses’ perceptions of technology used in language interpretation for patients with limited english proficiency. Am J Nurs. (2020) 120:48–58. doi: 10.1097/01.NAJ.0000697652.73975.37
11. Nadav J, Kaihlanen A-M, Kujala S, Laukka E, Hilama P, Koivisto J, et al. How to implement digital services in a way that they integrate into routine work: qualitative interview study among health and social care professionals. J Med Internet Res. (2021) 23:e31668. doi: 10.2196/31668
12. Lambert SI, Madi M, Sopka S, Lenes A, Stange H, Buszello C-P, et al. An integrative review on the acceptance of artificial intelligence among healthcare professionals in hospitals. NPJ Digit Med. (2023) 6:111. doi: 10.1038/s41746-023-00852-5
13. Berg GM, LoCurto J, Lippoldt D. Stages of adoption concern and technology acceptance in a critical care nursing unit. J Nurs Adm. (2017) 47:441–7. doi: 10.1097/NNA.0000000000000511
14. Lee HH, Melbye EL. Nursing home caregivers’ acceptance of, and experiences with, a new digital intervention for oral healthcare: a qualitative feasibility study. Gerodontology. (2023) 41(1):68–82. doi: 10.1111/ger.12695
15. Bagot K, Moloczij N, Arthurson L, Hair C, Hancock S, Bladin CF, et al. Nurses’ role in implementing and sustaining acute telemedicine: a mixed-methods, pre-post design using an extended technology acceptance model. J Nurs Scholarsh. (2020) 52:34–46. doi: 10.1111/jnu.12509
16. Venkatesh , Morris , Davis . User acceptance of information technology: toward a unified view. MIS Q (2003) 27:425. doi: 10.2307/30036540
17. Barchielli C, Marullo C, Bonciani M, Vainieri M. Nurses and the acceptance of innovations in technology-intensive contexts: the need for tailored management strategies. BMC Health Serv Res. (2021) 21:639. doi: 10.1186/s12913-021-06628-5
18. Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q. (2004) 82:581–629. doi: 10.1111/j.0887-378X.2004.00325.x
19. Hechtel N, Krückeberg J, Sebastião M, Klawunn R. Analysing the selection of appropriate technical solutions for nurses in a clinical setting. Stud Health Technol Inform. (2021) 281:645–8. doi: 10.3233/SHTI210250
20. Krückeberg J, Rutz M, Hagen H, Hechtel N. Die perspektive der basis—welche bereiche in der stationären pflege können von technischen innovationen profitieren? Proceedings of the Clusterconference „Zukunft der Pflege“ (2019).
21. Hechtel N, Klawunn R, Mazhari R, Schmeer R, Krückeberg J. Wie kann Pflegetechnologie bedarfsgerecht und nutzerorientiert ausgewählt werden? (2020).
22. Krückeberg J, Klawunn R, Fuge I, Mazhari R, Schmeer R, Hechtel N. How to decide upon nursing technologies—a participation-based approach. Stud Health Technol Inform. (2020) 270:1305–6. doi: 10.3233/SHTI200414
23. Greenhalgh T, Swinglehurst D. Studying technology use as social practice: the untapped potential of ethnography. BMC Med. (2011) 9:45. doi: 10.1186/1741-7015-9-45
24. Higginbottom GM, Pillay JJ, Boadu NY. Guidance on performing focused ethnographies with an emphasis on healthcare research. Qual Rep. (2013) 2013:1–16. doi: 10.46743/2160-3715/2013.1550
25. Cruz EV, Higginbottom GM. The use of focused ethnography in nursing research. Nurse Res. (2013) 20:36–43. doi: 10.7748/nr2013.03.20.4.36.e305
27. Wall S. Focused ethnography: a methodological adaptation for social research in emerging contexts. Forum Qual Sozialforschung. (2015) 16:Art. 1, p. 1–15. ISSN: 1438-5627.
28. Greenhalgh T, Abimbola S. The NASSS framework—a synthesis of multiple theories of technology implementation. Stud Health Technol Inform. (2019) 263:193–204. doi: 10.3233/SHTI190123
29. Ammenwerth E, Iller C, Mahler C. IT-adoption and the interaction of task, technology and individuals: a fit framework and a case study. BMC Med Inform Decis Mak. (2006) 6:3. doi: 10.1186/1472-6947-6-3
30. Implementation Science Team Do, Institute NC. Implementation Science at a Glance: A Guide for Cancer Control Practitioners. Washington, D.C: United States Government Printing Office (2019). p. 88.
31. Neyer FJ, Felber J, Gebhardt C. Entwicklung und validierung einer kurzskala zur erfassung von technikbereitschaft. Diagnostica. (2012) 58:87–99. doi: 10.1026/0012-1924/a000067
32. Emerson RM, Fretz RI, Shaw LL. Writing Ethnographic Fieldnotes. Chicago: The University of Chicago Press (2011). p. 289.
33. Müller L, Backhaus C. Entwicklung eines Fragebogens zur Bewertung der 775 Gebrauchstauglichkeit von Medizinprodukten im Beschaffungsprozess. In: Arbeitswissenschaft GfA, editors. Arbeit Interdisziplinär Analysieren—bewerten—gestalten Dresden: Dortmund (2019). p. 1–6.
34. Kuckartz U. Qualitative Inhaltsanalyse: Methoden, Praxis, Computerunterstützung. Weinheim, Basel: BeltzJuventa (2018). p. 240.
35. Schreier M. Ways of doing qualitative content analysis: disentangling terms and terminologies. Forum Qual Sozialforschung. (2014) 15(1):1–27. doi: 10.17169/fqs-15.1.2043
36. Green CA, Duan N, Gibbons RD, Hoagwood KE, Palinkas LA, Wisdom JP. Approaches to mixed methods dissemination and implementation research: methods, strengths, caveats, and opportunities. Adm Policy Ment Health. (2015) 42:508–23. doi: 10.1007/s10488-014-0552-6
37. Heibges M, Mörike F, Feufel MA. Wann braucht Ethnografie eine Einverständniserklärung? Praktische Antworten auf ethische Fragen zu ethnografischen Methoden in der HCI-Forschung. Hamburg: Gesellschaft für Informatik e.V (2019).
38. Huber E, Imeri S. Informed Consent in Ethnographic Research: A Common Practice Facing new Challenges. Bremen: Universität Bremen (2021). doi: 10.26092/elib/1070
39. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. (2007) 19:349–57. doi: 10.1093/intqhc/mzm042
40. Green J, Thorogood N. Analysing qualitative data. In: Green J, Thorogood N, editors. Qualitative Methods for Health Research. London: Sage Publications Ltd (2004). p. 173–200.
41. Klawunn R, Ottmann I, Schmeer R, Dierks ML. Analyse interdependenter wirkungen bei der erprobung neuer digitaler pflegetechnik im stationsalltag auf basis des resonanzkonzepts. Gesundheitswesen. (2022) 84:787. doi: 10.1055/s-0042-1753766
42. Klawunn R, Sieker D, Dierks M-L. Using resonance theory as an approach to analyse implementation processes of nursing technology. 3rd International Conference of the German Society of Nursing Science—Online (2023).
43. Erasmus A, Brunet TD, Fisher E. What is interpretability? Philos Technol. (2021) 34:833–62. doi: 10.1007/s13347-020-00435-2
44. McGranahan C. Ethnography beyond method: the importance of an ethnographic sensibility. J Soc Anthropol Cult Stud. (2018) 15:1–10. doi: 10.11157/sites-id373
45. Arteaga I, Llewellyn H. Cultivating ethnographic sensibilities in ethnographies of dying people. Ethos. (2022) 50:353–71. doi: 10.1111/etho.12357
46. Krick T, Zerth J, Klawunn R. Pflegeinnovationen in der praxis: erfahrungen und empfehlungen aus dem „cluster zukunft der pflege“, einführung und orientierung. In: Krick T, Zerth J, Rothgang H, Klawunn R, Walzer S, Kley T, editors. Pflegeinnovationen in der Praxis: Erfahrungen und Empfehlungen aus dem „Cluster Zukunft der Pflege“. Wiesbaden: Springer Fachmedien Wiesbaden (2023). p. 1–16.
47. Cresswell KM, Worth A, Sheikh A. Actor-network theory and its role in understanding the implementation of information technology developments in healthcare. BMC Med Inform Decis Mak. (2010) 10:67. doi: 10.1186/1472-6947-10-67
48. Matsuzaki H. Zum generalisierten misstrauen gegenüber der technisierung der pflege. In: Krick T, Zerth J, Rothgang H, Klawunn R, Walzer S, Kley T, editors. Pflegeinnovationen in der Praxis: Erfahrungen und Empfehlungen aus dem „Cluster Zukunft der Pflege“. Wiesbaden: Springer Fachmedien Wiesbaden (2023). p. 293–309.
49. Rosenberger R, Verbeek P-P. A field guide to postphenomenology. In: Rosenberger R, Verbeek P-P, editors. Postphenomenological Investigations: Essays on Human-Technology Relations. Lanham, Boulder, New York, London: Lexington Books (2015). p. 9–42.
50. Böhle F, Weihrich M. Das konzept der interaktionsarbeit. Z Arb Wiss. (2020) 74:9–22. doi: 10.1007/s41449-020-00190-2
Keywords: ethnography, technology acceptance, UTAUT, participant observation, nursing care, implementation, technical innovations, Germany
Citation: Klawunn R, Albrecht U-V, Katzmarzyk D and Dierks M-L (2024) Beyond technology acceptance—a focused ethnography on the implementation, acceptance and use of new nursing technology in a German hospital. Front. Digit. Health 6:1330988. doi: 10.3389/fdgth.2024.1330988
Received: 31 October 2023; Accepted: 11 April 2024;
Published: 25 April 2024.
Edited by:
Jennifer Apolinário-Hagen, Heinrich Heine University of Düsseldorf, GermanyReviewed by:
Christine Jacob, University of Applied Sciences and Arts Northwestern Switzerland, SwitzerlandBernhard Breil, Niederrhein University of Applied Sciences, Germany
© 2024 Klawunn, Albrecht, Katzmarzyk and Dierks. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ronny Klawunn a2xhd3Vubi5yb25ueUBtaC1oYW5ub3Zlci5kZQ==