 Max Sannemalm1*
Max Sannemalm1* Nathalie Lybert1
Nathalie Lybert1 Lisa Gunnarsson2
Lisa Gunnarsson2 Per Andrén3Martin Kraepelien1
Per Andrén3Martin Kraepelien1 Maria Bragesjö1Robin Fondberg2
Maria Bragesjö1Robin Fondberg2 Volen Z. Ivanov1
Volen Z. Ivanov1 David Mataix-Cols1,3
David Mataix-Cols1,3 Lorena Fernández de la Cruz1
Lorena Fernández de la Cruz1 Erik Andersson4Christian Rück1
Erik Andersson4Christian Rück1 Ekaterina Ivanova1
Ekaterina Ivanova1
- 1Centre for Psychiatry Research, Department of Clinical Neuroscience, Karolinska Institutet & Stockholm Health Care Services, Region Stockholm, Stockholm, Sweden
- 2Department of Psychiatry, University of Oxford, Oxford, United Kingdom
- 3Department of Clinical Sciences, Lund, Lund University, Lund, Sweden
- 4Division of Psychology, Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden
Introduction: Tourette syndrome (TS) and chronic motor or vocal tic disorder (CTD) are neurodevelopmental disorders associated with functional impairment and reduced quality of life. Behavioral therapy (BT) is an effective treatment, but lack of experienced practitioners makes it hard for patients to receive appropriate help. One approach to bridge the gap between demand and availability is to offer the treatment remotely over the internet with minimal support from a therapist.
Methods: This single-blind randomized controlled superiority trial including 110 participants will compare internet-delivered BT (I-BT) primarily consisting of exposure and response prevention (ERP) to a control condition consisting of internet-delivered general psychological support. The primary aim of the trial is to evaluate whether ERP-based I-BT is superior to the control condition in reducing TS/CTD symptoms. The primary outcome measure is the Yale Global Tic Severity Scale - Total Tic Severity score administered by blinded raters at primary endpoint 11 weeks after the treatment start. Secondary endpoints occur at week 23 and 14 months after the treatment start, and the secondary outcomes include tic-related impairment, rates of responders, self-rated tic severity, symptoms of depression, quality of life and cost-effectiveness. Data on dropout rates and adverse events is also collected.
Discussion: This is the first randomized controlled trial to evaluate therapist-guided ERP-based I-BT for adults with TS/CTD. The study has been approved by the Swedish Ethical Review Authority (EPM 2023-06541-01). The hypotheses were pre-registered before the start of the data collection. Results from all analyses will be reported according to the Consolidated Standards of Reporting Trials statement for non-pharmacological trials (CONSORT) and Consolidated Health Economic Evaluation Reporting Standards (CHEERS). The participants in the control condition will have the opportunity to receive I-BT after the data from the first follow-up is collected. The study will be published in open access and the results will be shared with service user organizations. At the moment of submission, the study has recruited 87 out of 110 planned participants and the recruitment is expected to be completed in February 2025.
Trial registration: Open Science Framework: https://osf.io/cq97b/ (uploaded 31/01/2024); Clinicaltrials.gov: NCT06271083 (submitted 14/02/2024).
1 Introduction
Tourette syndrome (TS) and chronic motor or vocal tic disorder (CTD) are neurodevelopmental conditions that originate and typically peak in childhood (1), but about 20% of patients seem to present with the symptoms beyond their teenage years (2, 3). TS is characterized by both motor and vocal tics for at least one year, while CTD involves either motor or vocal tics also lasting at least one year (1). Both conditions are associated with reduced quality of life, lower educational attainment, risk of other psychiatric and somatic conditions, and increased mortality rates (3–10).
The most common pharmacological treatment for TS/CTD is antipsychotic medication, which is associated with substantial side effects (11). Behavior therapy (BT) is a non-pharmacological treatment option aimed at teaching individuals to better manage their tics (12). BT is an effective treatment (13–16), but is not always available due to a lack of experienced practitioners.
One approach to increase treatment availability is to offer BT online instead of in-person (17). Internet-delivered BT (I-BT) includes the same treatment content but is delivered through a secure online platform. Patients work with self-help materials and assignments and communicate with a therapist via the platform. Research shows that self-help-based I-BT can be provided to adults with TS/CTD (18). Therapist-supported I-BT using exposure and response prevention (ERP) techniques has been successfully provided to children and adolescents in two large randomized controlled trials (19, 20) with one trial showing significant reductions in tic severity compared to an active control group (19), and the second trial showing significant reductions in both groups with no between-group effect (20). Our research group recently conducted a feasibility trial of internet-delivered ERP for adults (n = 31) with TS/CTD (21). The treatment was deemed both feasible and safe. Additionally, preliminary efficacy results showed a significant within-group tic severity reduction, with an effect size of Cohen's d = 0.49.
The primary aim of the study is to investigate whether guided internet-delivered ERP-based BT is superior to an active control condition consisting of guided internet-delivered general psychological support in reducing TS/CTD symptoms. We hypothesize that, compared to the control group, participants in the treatment group will show greater reduction in tic severity, as measured with Yale Global Tic Severity Scale - Total Tic Severity subscale (YGTSS-TTS) (22) at the primary endpoint (post treatment or week 11 after treatment start).
The secondary aim at the primary endpoint (week 11 after the start of the treatment) is to compare the two arms regarding:
(1) Tic-related impairment
(2) Rates of responders
(3) Self-rated tic severity
(4) Symptoms of depression
(5) Quality of life
(6) Cost-effectiveness
The third aim is to evaluate long-term maintenance of gains. We hypothesize that the intervention condition will be superior to the control condition at week 23 after the treatment start (better response, less severe symptoms, higher quality of life) regarding all outcome measures and that the results will be maintained in the intervention group at the 14-month follow-up. The fourth aim is to evaluate the cost-effectiveness of the intervention from the healthcare organization payer perspective, the healthcare system perspective, and the societal perspective.
2 Methods and analysis
2.1 Trial design
A parallel group randomized (1:1) controlled superiority trial (RCT) will be carried out at Karolinska Institutet in Stockholm, Sweden. The study will be conducted in Swedish and will include a total of 110 adult participants with TS/CTD. The study will be conducted according to the Declaration of Helsinki and relevant parts of ICH E6 Good Clinical Practice (GCP). The Consolidated Standards of Reporting Trials (CONSORT) flow chart for the trial is shown in Figure 1. Both the outcome measures and the treatment will be administered via a secure online treatment platform (BASS4) requiring two-step authentication, run by the Karolinska Institutet eHealth Core Facility. Prior to the start of recruitment, the trial was approved by the Swedish Ethical Review Authority (EPM 2023-06541-01) and pre-registered at Open Science Framework, osf.io (https://osf.io/cq97b/). The trial was registered at ClinicalTrials.gov (NCT06271083) at the very start of recruitment. Potential protocol modifications will be described in detail on osf.io, ClinicalTrials.gov, and, if required, amendments will be submitted to the Swedish Ethical Review Authority.
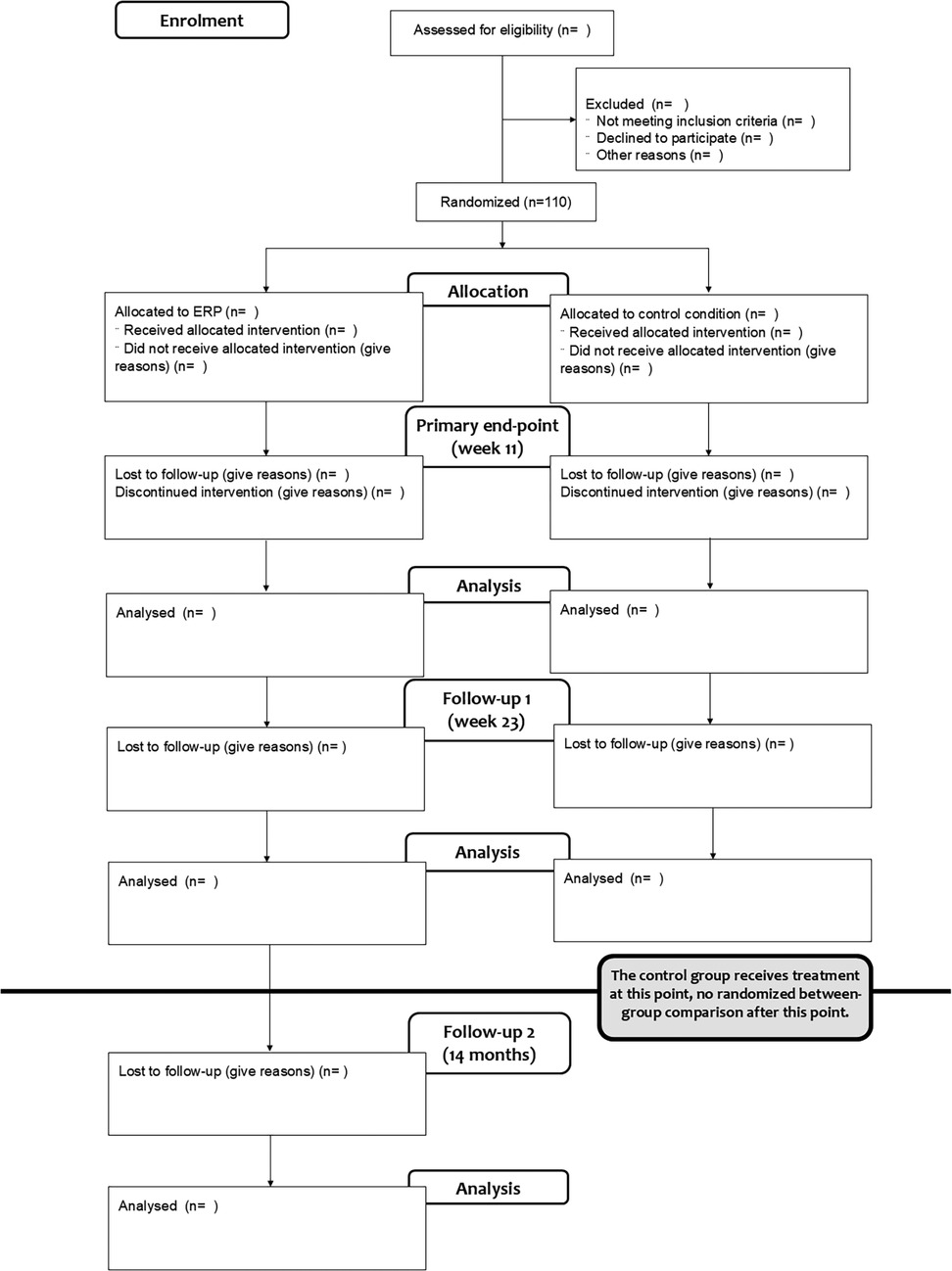
Figure 1. CONSORT flow chart over the trial recruitment and treatment process.
2.2 Participants
Eligibility criteria for the participants are listed in Table 1. The participants will be recruited nationally by means of advertisement in social and regular media (online and printed copies) and by spreading information via psychiatric and neurological clinics and service user organizations across Sweden. The advertisements will guide the prospective participants to the study website (ticsstudien.se) where more detailed information about the study will be provided and the visitor will be encouraged to proceed to the treatment platform for registration. During the registration procedure, the prospective participants will be provided necessary practical information about the project. Thereafter, if they are still interested in participating, they will provide digital consent for study participation, identify themselves with two-step authentication by receiving a text message to their phone number and e-mail address, create an account at the treatment platform, and fill out a preliminary screening form focused on the nature and severity of their tics, the eligibility criteria, and sociodemographic information. Potentially eligible participants will undergo a psychiatric assessment via video-conferencing software or telephone to check the eligibility criteria, collect clinician-administered measurements, and assess psychiatric comorbidities. Eligible participants will be included in the trial, randomized, and enrolled within two weeks after the assessment of pre-treatment tic severity with the YGTSS (if more than two weeks pass from the date of pre-treatment YGTSS to the start of the treatment, the pre-treatment YGTSS will be re-administered).
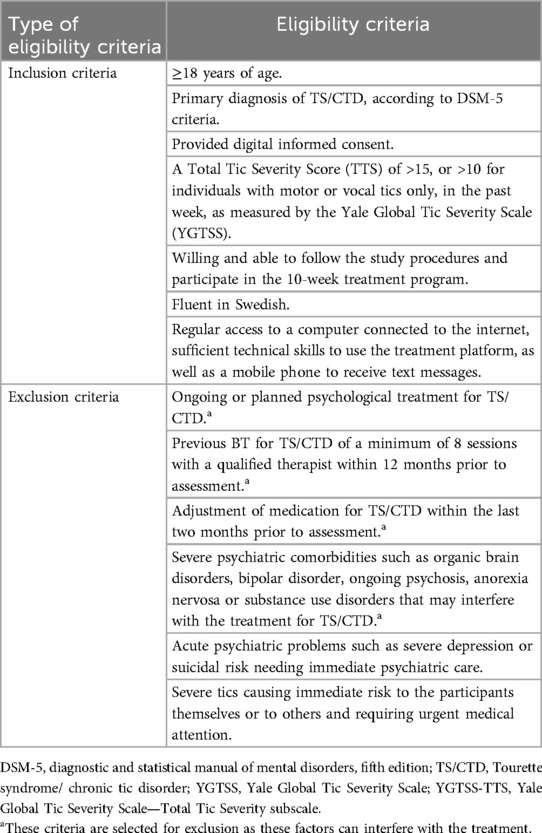
Table 1. Overview of eligibility criteria.
2.3 Interventions
2.3.1 Intervention condition: internet-delivered exposure with response prevention
The active intervention will contain eight chapters with homework assignments after each chapter, as well as working sheets for the participants to register and monitor their activity during the treatment. The participants will work with their treatment for 10 weeks, communicating with their therapists via asynchronous written messages in the platform. On the first day of the treatment, the participants in both intervention and control conditions will be greeted by their therapist via a message sent on the treatment platform. The therapists will introduce themselves, inform the participants about the outline of the treatment, and encourage them to start working with the treatment content immediately. The first two chapters of the treatment will be available to the participants from the start. The participants will be encouraged to work with one treatment chapter per week and the following chapter will be opened by the therapist when the previous week's homework is reviewed. The therapist's role will be to encourage the participants’ activity in the treatment and follow up on inactivity, problem solve and follow up on potential safety issues when necessary.
During the treatment, participants will receive information about tics and ERP, the central component of the intervention (see Table 2 for an overview of the ERP condition). Continuously throughout the treatment, participants will work with exposing themselves to situations that trigger their premonitory urges and practice suppressing their tics. They will learn different strategies to provoke their premonitory urges to make suppression of their tics more challenging and gradually increase the time they can suppress the tics. A central tool in the treatment will be the Ticstimer, a worksheet where participants will continuously record their ERP practice and the time they manage to suppress tics. The participants will be encouraged to work with the Ticstimer daily. Additionally, the treatment will include an introduction to habit reversal training (HRT) which is another BT-strategy, to give the participants and therapists a broader range of tools and make the treatment more suitable for regular psychiatric settings where clinicians appreciate being able to offer a range of evidence-based techniques. The treatment will include one scheduled phone call around the time the participant received the rationale for the ERP and is about to start their practice, to maximize the chance for the first practice to align with the rationale.
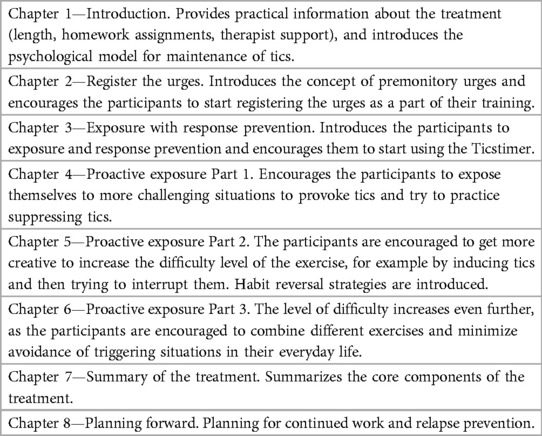
Table 2. Overview of the active condition.
2.3.2 Control condition: internet-delivered general psychological support
Participants who are randomized to the control group will receive access to brief psychoeducational content about TS/CTD in the platform in combination with general psychological support from a therapist. The materials will be divided in two chapters. Chapter 1 will cover the topics of what tics are, and the different ways stress can influence the symptoms. Chapter 2 will focus on supporting stress management and healthy lifestyle habits related to food, sleep, and physical activity. No active BT components (i.e., ERP, HRT, applied relaxation) are provided to the participants in the control group. The therapists will welcome the participants to the treatment, encourage them to engage in the treatment content and to reach out to the therapist if they have any questions. Thereafter, the therapists will only reply to the participants’ messages without taking any contact initiative themselves (unless there is an indication of severe deterioration or severe depressive symptoms or suicidal ideation requiring medical attention). The aim of the control condition is to control for basic therapist attention, relevant disorder-specific content, and the passage of time. The participants in the control group who wish to have additional help will have an opportunity to receive I-BT after the data from the first long-term follow-up (week 23 after the start of the treatment) are collected.
2.3.3 Therapists
The therapists will answer participants’ messages within 24 h on weekdays. The therapists will be licensed psychologists and psychologists or psychology students under supervision and with basic training in cognitive behavior therapy. All therapists will be treating participants in both conditions. The therapists will receive a half-day training in the program followed by supervision sessions every two weeks throughout the duration of the trial with an experienced therapist.
2.4 Outcomes
If not specified otherwise, the outcome measures will be collected at pre-treatment, at week 11 counting from the start of the treatment (post-treatment, primary endpoint), week 23 (3 months after the end of the treatment), and 14 months after the treatment start (12 months after the end of the treatment) (Table 3).
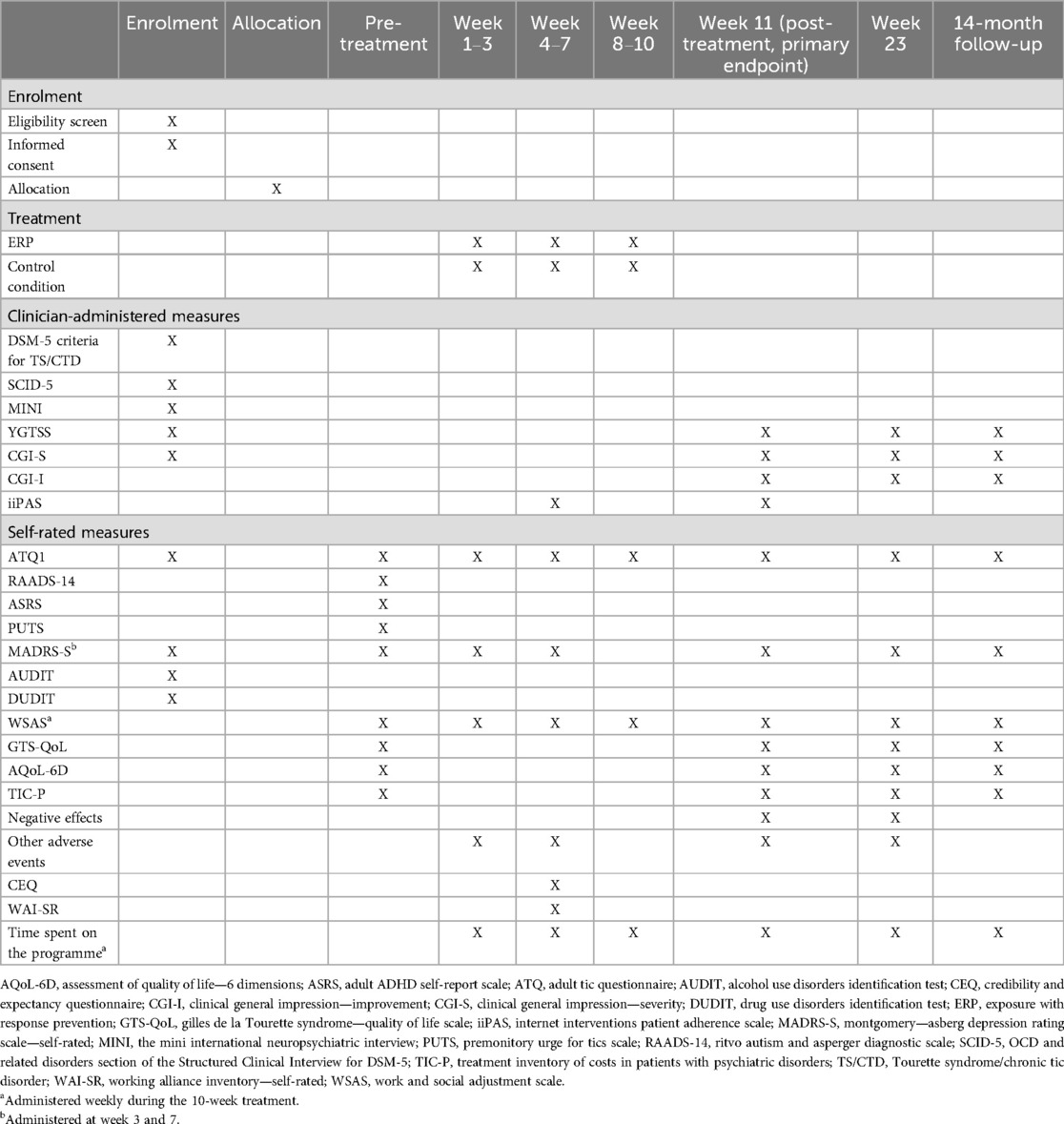
Table 3. Overview of the recruitment, treatment, and assessment points and measures.
The primary outcome measure will be the YGTSS-TTS (22), administered by a clinician blinded to the randomization condition. The raters will be psychiatrists or psychiatry residents, clinical psychologists, psychologists under training or psychology students receiving supervision. The raters will receive training in administering the YGTSS and participate in at least two test ratings with subsequent supervision before they are allowed to conduct assessments in the trial. Co-ratings will be arranged every 6 months for the active raters during the data collection period. Data on inter-rater reliability will be reported.
Secondary clinician-rated outcome measures will be the YGTSS-Impairment, as well as the Clinical Global Impression—Severity and Improvement (CGI-S and CGI-I, the latter not administered at pre-treatment) (23). The clinicians will receive training in administering the CGI that will be repeated every 6 months. Participants that are rated as “much improved” or “very much improved” on the CGI-I will be classified as treatment responders (24). If the participant keeps the responder status at subsequent follow-ups, they will be classified as long-term responders at that follow-up.
Self-rated tic-specific outcome measures will be the Adult Tic Questionnaire (ATQ) (also administered weekly) (25), the Gilles de la Tourette Syndrome—Quality of Life Scale (GTS-QoL) (26), and the Work and Social Adjustment Scale (WSAS) (27) adapted for TS/CTD by the research team. General quality of life will be measured using the Assessment of Quality of Life—6 Dimensions (AQoL-6D) (28), and these scores will be used in the health-utility analysis (see below). Symptoms of depression will be assessed using Montgomery-Asberg Depression Rating Scale—Self-report (MADRS-S) (29) (also administered at week 3 and 7). The self-reported Treatment Inventory of Costs in Patients with psychiatric disorders (TIC-P) will be administered to measure health-related costs (30).
The participants’ adherence to the treatment will be measured by their therapist using the Internet Intervention Patient Adherence Scale (iiPAS) (31) at week 6 and 11. In the ERP condition, once the Ticstimer is introduced, the participants will be asked to assess weekly how much time they have spent practicing. The participants will rate the perceived credibility of the treatments using the Credibility and Expectancy Questionnaire (CEQ) (32) at week 5. The participants will also fill out the Working Alliance Inventory—Self-Report (WAI-SR) (33) at week 5. Data on the number of sent and received messages, phone calls, and completed treatment chapters will be collected, as well as data on time spent by the therapists on supporting each participant.
The following instruments will only be administered at pre-treatment: The Mini International Neuropsychiatric Interview (M.I.N.I.) (34) and the OCD and related disorders section of the Structured Clinical Interview for DSM-5 (SCID) (35) to assess psychiatric comorbidities (clinician-administered); questions on tic symptoms following DSM-5 criteria for TS/CTD to confirm the diagnosis (clinician-administered), as well as the following self-rated measures: Premonitory Urge for Tics Scale (PUTS) (36), Alcohol Use Disorders Identification Test (AUDIT) (37), Drug Use Disorders Identification Test (DUDIT) (38), the Ritvo Autism and Asperger Diagnostic Scale (RAADS-14) (39), and the Adult ADHD Self-report Scale (ASRS) (40). Data on medication and previous psychological treatments will be collected at the baseline clinical assessment.
Negative effects will be assessed by administering a 16-item questionnaire on negative events developed by the research group at post-treatment and at week 23. Adverse events connected to worsened symptoms, suicidality, and impatient care will be measured using an additional questionnaire developed by the research group focusing specifically on whether those events have occurred, with possibility for elaboration, also administered at week 6. Spontaneously reported adverse events will be registered. Patient safety will be monitored during the recruitment procedures, by administering the MADRS and an adverse events questionnaire twice during the treatment, as well as by clinician monitoring in their contact with the participants. In case of significant deterioration, severe depressive symptoms or signs of suicidality, or in case of progression of other psychiatric disorder needing medical attention, the participant will be contacted for an additional assessment and an experienced clinician will decide on recommended future care (e. g., discontinuation of the treatment, referral to inpatient or other outpatient care).
To promote completion of follow up questionnaires, the participants will receive automatic reminders via text messages in the study platform. In case of longer measurement inactivity, study personnel will be contacting the participants via text messages or by phone.
2.5 Sample size
The within-group effect size in the feasibility trial was Cohen's d = 0.49 (21). As tic severity is known to fluctuate over time, we expect a certain amount of improvement in the control condition. However, we do not expect it to be as large as in the two previous ERP-based I-BT studies in children (19, 20), because the control group in those studies was much more potent. Furthermore, the participants in our previous adult pilot trial improved as much as the participants in a previous adult trial (18), but their pre-treatment tic severity was unexpectedly low, making the overall pre-to-post-treatment effects small. In the current trial, we expect the participants to have a more representative pre-treatment tic severity and their improvement to the primary endpoint is expected to be larger. In sum, we assume the between-group effect-size measured with Cohen's d to be around 0.5. With n = 50 participants in each group we will achieve 80% power to detect the effect of between-group Cohen's d = 0.5 (one-tailed test). A total sample size of n = 110 will allow for 10% drop-out rate.
2.6 Randomization and blinding
The participants will be starting treatment in cohorts. Every time a cohort is ready to start, the online service random.org will be used to create a randomized list of the participants included into the cohort. The list will be emailed to a person not associated with the research group with the instruction to choose the following: (1) where an imaginary line dividing the cohort into two approximately equal groups should be drawn, and (2) whether the group above the line should be marked with “I” (meaning intervention) or “K” (meaning control). The outcome assessors will be blinded to the allocation of the participants, and they will be asked to guess the allocation after each assessment. The frequency of correct guesses will be reported as a measure of blinding integrity.
2.7 Statistical methods
The significance level for all statistical tests will be α = 0.05. For all scale level measures, Cohen's d will be used as a measure of effect size. Odds ratios will be reported for categorical variables. Confidence intervals (95%) will be reported for all estimated measures.
The intention-to-treat approach to the analysis population will be applied in all cases unless specified otherwise. In case more than 10% of the data is missing, maximum likelihood imputations will be performed based on demographical data and the scores from the pretreatment assessment. The between-group differences at week 11 (primary endpoint) for the primary (YGTSS-TTS) and secondary outcome measures, an analysis of covariance (ANCOVA) with pre-score of the measure as covariate will be calculated. For ATQ and WSAS that are collected weekly, mixed effect models will be applied with random intercept and random slope. Chi squared tests will be calculated to explore the between-group differences in proportions of responders and long-term responders at all endpoints.
2.8 Health-economic evaluation
We will conduct a within-trial health economic evaluation (41) whereby outcome and cost data will be compared at week 11. It will encompass two analyses: (1) a cost-effectiveness analysis using the responder status as outcome; (2) a cost-utility analysis using the outcome quality adjusted life years (QALYs) measured using the AQOL-6D (30).
Health-related quality of life (HRQoL) will be collected using the AQOL-6D (28, 42), a multi-attribute utility instrument for use in economic evaluations. Data on resource use will be collected using an adapted version of the self-reported Treatment Inventory of Costs in Psychiatric Patients (TIC-P) questionnaire (36). Costs will be measured from three perspectives: a healthcare organization payer perspective (including intervention costs only), a healthcare system perspective (additionally including costs related to the use of medical resources, and medication), and a societal perspective (additionally including social care costs and productivity losses for the individual). Costs from each perspective will be analysed in relation to clinical efficacy (responder status; cost-effectiveness analysis) and QALYs (cost-utility analysis). Results will be presented as incremental cost-effectiveness ratios (ICER), as the ratio between the difference in costs and the difference in health outcomes ICERs will be put against values of willingness to pay for a QALY to determine cost-effectiveness.
Standard health economic evaluation techniques will be used to explore uncertainty around the cost and effect data, which will be represented on cost-effectiveness planes. The probability of cost-effectiveness according to different willingness to pay thresholds will be represented on cost effectiveness acceptability curves (43).
3 Discussion
This will be the first superiority trial to compare a therapist-guided digital I-BT programme, primarily consisting of ERP, for adults with TS/CTD to an active control group. This trial aims to provide a population that rarely has access to effective treatments with an evidence-based intervention that can be widely disseminated.
4 Ethics and dissemination
This study has been approved by the Swedish Ethical Review Authority (EPM 2023-06541-01). The benefits of the project outweigh its potential harms. The treatment is built on the same evidence-based principles shown to be safe in previous trials and in our own pilot trial (21). The participants in the control condition will have a chance to receive the treatment after the data from the first follow-up are collected. The participants’ symptoms will be closely monitored by the study personnel. At signs of deterioration or worsening of symptoms of depression or suicidal ideation, the participant will be assessed by a licensed clinical psychologist or psychiatrist. If necessary, the trial participation will be ended for these participants, and they will be referred to adequate medical services. All participant data will be collected and stored at either the encrypted treatment platform BASS4, run by the Karolinska Institutet eHealth Core Facility and requiring two-step authentication, or at the encrypted servers at Karolinska Institutet, set up specifically for storing sensitive research data and requiring a VPN-connection. There will be no external data monitoring committee in this trial. All data will be monitored in-house by study personnel. Participants always have the right to discontinue treatment at any time, without needing to provide an explanation. The research team is not allowed to modify the intervention, but the participants are not prohibited to do so, meaning their treatment will not be automatically discontinued if they engage in another treatment.
The publications within the current project will be published in Open Access journals. The statistical code for the analyses will be uploaded at osf.io (https://osf.io/cq97b/) and a detailed description of the dataset will be saved in Swedish National Database (SND).
5 Current trial status
The first participant was included in the study on the 8th of February 2024 and recruitment is expected to end in January 2025. At the time for the submission, 87 participants have been included in the study. The last follow up will preliminarily take place in July 2026. Data analysis will begin after all primary endpoint data have been collected in July 2025.
Ethics statement
The studies involving humans were approved by The Swedish Ethical Review Authority. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MS: Conceptualization, Data curation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. NL: Data curation, Methodology, Project administration, Supervision, Writing – review & editing. LG: Data curation, Project administration, Writing – review & editing. PA: Conceptualization, Methodology, Supervision, Writing – review & editing. MK: Conceptualization, Methodology, Supervision, Writing – review & editing, Software. MB: Conceptualization, Methodology, Supervision, Writing – review & editing. RF: Conceptualization, Methodology, Supervision, Writing – review & editing, Writing – original draft. VI: Conceptualization, Methodology, Supervision, Writing – review & editing, Investigation. DM-C: Conceptualization, Methodology, Supervision, Writing – review & editing. LF: Conceptualization, Methodology, Supervision, Writing – review & editing. EA: Conceptualization, Methodology, Supervision, Writing – review & editing. CR: Conceptualization, Methodology, Supervision, Writing – review & editing. EI: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The project was funded by a Karolinska Institutet Research Grant, decision number FS-2024:0017.
Acknowledgments
We thank Lina Lundström for contributing to the preparation of the materials during the initiation of the project; Sara Thisner Lindstedt, Lovisa Nilsson, Linnéa Hagström, and Nika Sigaroudi for conducting pre-treatment assessments and treatments; Jonathan Johansson for conducting blinded outcome assessments and treatments; Hedvig Tillberg for conducting treatment; Maxime Hultkvist, Hana Fotoohi, Malin Rödström, and Caroline Geiger for conducting blinded assessments.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdgth.2025.1518666/full#supplementary-material
Abbreviations
ADHD, attention deficit/hyperactivity disorder; ANCOVA, analysis of covariance; AQoL—6D, assessment of quality of life - 6 dimensions; ASRS, adult ADHD self-report scale; ATQ, adult tic questionnaire; AUDIT, alcohol use disorders identification test; BT, behavior therapy, CEQ, credibility/expectancy questionnaire; CGI, clinical global impression; CGI-I, clinical global impression—improvement; CGI-S, clinical global impression—severity; CTD, chronic tic disorder; DIDIT, drug use disorders identification test; DSM-5, diagnostic and statistical manual of mental disorders, fifth edition; ERP, exposure and response prevention; GCP, good clinical practice; GTS-QoL, Gilles de la Tourette syndrome—quality of life scale; HRQoL, health-related quality of life; HRT, habit reversal training; I-BT, internet-delivered behavior therapy; ICER, incremental cost-effectiveness ratios; IIPAS, internet intervention participant adherence scale; MADRS-S, Montgomery-Åsberg depression rating scale—self-rated; OCD, obsessive-compulsive disorder; PUTS, premonitory urge for tics scale; QALY, quality adjusted life years; RAADS, ritvo autism and asperger diagnostic scale; RCT, randomized controlled trial; TIC-P, treatment inventory of costs in patients with psychiatric disorders; TS, Tourette syndrome; WAI, working alliance inventory; WSAS, work and social adjustment scale; YGTSS, Yale global tic severity scale; YGTSS-TTS, Yale global tic severity scale—total tic severity subscale.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). Washington, DC: American Psychiatric Pub (2013). p. 1520.
2. Bloch MH, Leckman JF. Clinical course of tourette syndrome. J Psychosom Res. (2009) 67(6):497–501. doi: 10.1016/j.jpsychores.2009.09.002
3. Groth C, Mol Debes N, Rask CU, Lange T, Skov L. Course of tourette syndrome and comorbidities in a large prospective clinical study. J Am Acad Child Adolesc Psychiatry. (2017) 56(4):304–12. doi: 10.1016/j.jaac.2017.01.010
4. Bloch MH, Peterson BS, Scahill L, Otka J, Katsovich L, Zhang H, et al. Adulthood outcome of tic and obsessive-compulsive symptom severity in children with tourette syndrome. Arch Pediatr Adolesc Med. (2006) 160(1):65–9. doi: 10.1001/archpedi.160.1.65
5. Elstner K, Selai CE, Trimble MR, Robertson MM. Quality of life (QOL) of patients with Gilles de la Tourette’s syndrome: QOL patients with Gilles de la Tourette’s syndrome. Acta Psychiatr Scand. (2008) 103(1):52–9. doi: 10.1111/j.1600-0447.2001.00147.x
6. Pérez-Vigil A, de la Cruz LF, Brander G, Isomura K, Jangmo A, Kuja-Halkola R, et al. Association of tourette syndrome and chronic tic disorders with objective indicators of educational attainment: a population-based sibling comparison study. JAMA Neurol. (2018) 75:1098–105. doi: 10.1001/jamaneurol.2018.1194
7. Brander G, Isomura K, Chang Z, Kuja-Halkola R, Almqvist C, Larsson H, et al. Association of tourette syndrome and chronic tic disorder with metabolic and cardiovascular disorders. JAMA Neurol. (2019) 76:454–61. doi: 10.1001/jamaneurol.2018.4279
8. Meier SM, Dalsgaard S, Mortensen PB, Leckman JF, Plessen KJ. Mortality risk in a nationwide cohort of individuals with tic disorders and with tourette syndrome: mortality risk in TIC disorders/tourette syndrome. Mov Disord. (2017) 32(4):605–9. doi: 10.1002/mds.26939
9. Fernández De La Cruz L, Mataix-Cols D. General health and mortality in tourette syndrome and chronic tic disorder: a mini-review. Neurosci Biobehav Rev. (2020) 119:514–20. doi: 10.1016/j.neubiorev.2020.11.005
10. Fernández de la Cruz L, Rydell M, Runeson B, Brander G, Rück C, D’Onofrio BM, et al. Suicide in tourette’s and chronic tic disorders. Biol Psychiatry. (2017) 82(2):111–8. doi: 10.1016/j.biopsych.2016.08.023
11. Waldon K, Hill J, Termine C, Balottin U, Cavanna AE. Trials of pharmacological interventions for tourette syndrome: a systematic review. Behav Neurol. (2013) 26(4):265–73. doi: 10.1155/2013/626410
12. Capriotti MR, Himle MB, Woods DW. Behavioral treatments for tourette syndrome. J Obsessive Compuls Relat Disord. (2014) 3(4):415–20. doi: 10.1016/j.jocrd.2014.03.007
13. Azrin NH, Peterson AL. Treatment of tourette syndrome by habit reversal: a waiting-list control group comparison. Behav Ther. (1990) 21(3):305–18. doi: 10.1016/S0005-7894(05)80333-8
14. Wilhelm S, Deckersbach T, Coffey BJ, Bohne A, Peterson AL, Baer L. Habit reversal versus supportive psychotherapy for tourette’s disorder: a randomized controlled trial. Am J Psychiatry. (2003) 160(6):1175–7. doi: 10.1176/appi.ajp.160.6.1175
15. Wilhelm S, Peterson AL, Piacentini J, Woods DW, Deckersbach T, Sukhodolsky DG, et al. Randomized trial of behavior therapy for adults with tourette syndrome. Arch Gen Psychiatry. (2012) 69(8):795–803. doi: 10.1001/archgenpsychiatry.2011.1528
16. Deckersbach T, Rauch S, Buhlmann U, Wilhelm S. Habit reversal versus supportive psychotherapy in tourette’s disorder: a randomized controlled trial and predictors of treatment response. Behav Res Ther. (2006) 44(8):1079–90. doi: 10.1016/j.brat.2005.08.007
17. Andersson G, Titov N, Dear BF, Rozental A, Carlbring P. Internet-delivered psychological treatments: from innovation to implementation. World Psychiatry. (2019) 18(1):20–8. doi: 10.1002/wps.20610
18. Haas M, Jakubovski E, Kunert K, Fremer C, Buddensiek N, Häckl S, et al. ONLINE-TICS: internet-delivered behavioral treatment for patients with chronic tic disorders. JCM. (2022) 11(1):250. doi: 10.3390/jcm11010250
19. Hollis C, Hall CL, Jones R, Marston L, Novere ML, Hunter R, et al. Therapist-supported online remote behavioral intervention for tics in children and adolescents in England (ORBIT): a multicentre, parallel group, single-blind, randomised controlled trial. Lancet Psychiatry. (2021) 8(10):871–82. doi: 10.1016/S2215-0366(21)00235-2
20. Andrén P, Holmsved M, Ringberg H, Wachtmeister V, Isomura K, Aspvall K, et al. Therapist-supported internet-delivered exposure and response prevention for children and adolescents with tourette syndrome: a randomized clinical trial. JAMA Netw Open. (2022) 5(8):e2225614. doi: 10.1001/jamanetworkopen.2022.25614
21. Ivanova EN, Birovecz A, Andrén P, Flygare O, Mataix-Cols D, Fernández De La Cruz L, et al. Online behavior therapy based on exposure with response prevention for adults with Tourette syndrome or chronic tic disorder: a feasibility trial. OSF Preprints. (2024). doi: 10.31219/osf.io/v7anb
22. Leckman JF, Riddle MA, Hardin MT, Ort SI, Swartz KL, Stevenson J, et al. The Yale global tic severity scale: initial testing of a clinician-rated scale of tic severity. J Am Acad Child Adolesc Psychiatry. (1989) 28(4):566–73. doi: 10.1097/00004583-198907000-00015
23. Guy W. ECDEU Assessment Manual for Psychopharmacology. Rockville, MD: US Department of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration (1976).
24. Jeon S, Walkup JT, Woods DW, Peterson A, Piacentini J, Wilhelm S, et al. Detecting a clinically meaningful change in tic severity in tourette syndrome: a comparison of three methods. Contemp Clin Trials. (2013) 36(2):414–20. doi: 10.1016/j.cct.2013.08.012
25. Abramovitch A, Reese H, Woods DW, Peterson A, Deckersbach T, Piacentini J, et al. Psychometric properties of a self-report instrument for the assessment of tic severity in adults with tic disorders. Behav Ther. (2015) 46(6):786–96. doi: 10.1016/j.beth.2015.06.002
26. Cavanna AE, Schrag A, Morley D, Orth M, Robertson MM, Joyce E, et al. The Gilles de la Tourette syndrome-quality of life scale (GTS-QOL): development and validation. Neurology. (2008) 71(18):1410–6. doi: 10.1212/01.wnl.0000327890.02893.61
27. Mundt JC, Marks IM, Shear MK, Greist JM. The work and social adjustment scale: a simple measure of impairment in functioning. Br J Psychiatry. (2002) 180(5):461–4. doi: 10.1192/bjp.180.5.461
28. Richardson JR, Peacock SJ, Hawthorne G, Iezzi A, Elsworth G, Day NA. Construction of the descriptive system for the assessment of quality of life AQoL-6D utility instrument. Health Qual Life Outcomes. (2012) 10(1):38. doi: 10.1186/1477-7525-10-38
29. Svanborg P, Åsberg M. A comparison between the Beck Depression Inventory (BDI) and the self-rating version of the Montgomery Åsberg Depression Rating Scale (MADRS). J Affect Disord. (2001) 64(2–3):203–16. doi: 10.1016/S0165-0327(00)00242-1
30. Timman R, Bouwmans C, Busschbach JJV, Hakkaart-van Roijen L. Development of the treatment inventory of costs in psychiatric patients: tIC-P Mini and midi. Value Health. (2015) 18(8):994–9. doi: 10.1016/j.jval.2015.07.006
31. Lenhard F, Mitsell K, Jolstedt M, Vigerland S, Wahlund T, Nord M, et al. The internet intervention patient adherence scale for guided internet-delivered behavioral interventions: development and psychometric evaluation. J Med Internet Res. (2019) 21(10):e13602. doi: 10.2196/13602
32. Devilly GJ, Borkovec TD. Psychometric properties of the credibility/expectancy questionnaire. J Behav Ther Exp Psychiatry. (2000) 31(2):73–86. doi: 10.1016/S0005-7916(00)00012-4
33. Hatcher RL, Gillaspy JA. Development and validation of a revised short version of the working alliance inventory. Psychother Res. (2006) 16(1):12–25. doi: 10.1080/10503300500352500
34. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-international neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) 59(Suppl 20):22–33. quiz 34–57.9881538
36. Woods DW, Piacentini J, Himle MB, Chang S. Premonitory urge for tics scale (PUTS): initial psychometric results and examination of the premonitory urge phenomenon in youths with tic disorders. J Dev Behav Pediatr. (2005) 26(6):397–403. doi: 10.1097/00004703-200512000-00001
37. Lundin A, Hallgren M, Balliu N, Forsell Y. The use of alcohol use disorders identification test (AUDIT) in detecting alcohol use disorder and risk drinking in the general population: validation of AUDIT using schedules for clinical assessment in neuropsychiatry. Alcoholism Clin Exp Res. (2015) 39(1):158–65. doi: 10.1111/acer.12593
38. Hildebrand M. The psychometric properties of the drug use disorders identification test (DUDIT): a review of recent research. J Subst Abuse Treat. (2015) 53:52–9. doi: 10.1016/j.jsat.2015.01.008
39. Eriksson JM, Andersen LM, Bejerot S. RAADS-14 screen: validity of a screening tool for autism spectrum disorder in an adult psychiatric population. Mol Autism. (2013) 4(1):49. doi: 10.1186/2040-2392-4-49
40. Brevik EJ, Lundervold AJ, Haavik J, Posserud M. Validity and accuracy of the adult attention-deficit/hyperactivity disorder (ADHD) self-report scale (ASRS) and the wender utah rating scale (WURS) symptom checklists in discriminating between adults with and without ADHD. Brain Behav. (2020) 10(6):e01605. doi: 10.1002/brb3.1605
41. Drummond M. Methods for the Economic Evaluation of Health Care Programmes. 4th Eds Oxford, United Kingdom, New York, NY, USA: Oxford University Press (2015). p. 445. (Oxford medical publications).
42. Maxwell A, Özmen M, Iezzi A, Richardson J. Deriving population norms for the AQoL-6D and AQoL-8D multi-attribute utility instruments from web-based data. Qual Life Res. (2016) 25(12):3209–19. doi: 10.1007/s11136-016-1337-z
Keywords: Tourette syndrome, chronic motor or vocal tic disorder, behavioral therapy, internet-delivered behavior therapy, exposure and response prevention, randomized controlled trial, health economics
Citation: Sannemalm M, Lybert N, Gunnarsson L, Andrén P, Kraepelien M, Bragesjö M, Fondberg R, Ivanov VZ, Mataix-Cols D, Fernández de la Cruz L, Andersson E, Rück C and Ivanova E (2025) Study protocol for a parallel-group randomized controlled trial of internet-delivered behavior therapy for adults with Tourette syndrome. Front. Digit. Health 7:1518666. doi: 10.3389/fdgth.2025.1518666
Received: 28 October 2024; Accepted: 29 July 2025;
Published: 29 August 2025.
Edited by:
Renata Rizzo, University of Catania, ItalyReviewed by:
Valeria Sajin, Asklepios Klinik St.Georg, GermanyAdriana Prato, University of Messina, Italy
Copyright: © 2025 Sannemalm, Lybert, Gunnarsson, Andrén, Kraepelien, Bragesjö, Fondberg, Ivanov, Mataix-Cols, Fernández de la Cruz, Andersson, Rück and Ivanova. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Max Sannemalm, bWF4LnNhbm5lbWFsbUBraS5zZQ==