 Jonathan G. Perle1*
Jonathan G. Perle1* Dilip N. Chandran1
Dilip N. Chandran1 Emily Brezler2
Emily Brezler2 Michelle Coleman3Julia Deziel3Patrick Nahhas3Gabrielle McDonald4
Michelle Coleman3Julia Deziel3Patrick Nahhas3Gabrielle McDonald4 Jason F. Jent5
Jason F. Jent5
- 1Department of Behavioral Medicine and Psychiatry, Rockefeller Neuroscience Institute, West Virginia University School of Medicine, Morgantown, WV, United States
- 2Department of Internal Medicine and Pediatrics, University of Louisville School of Medicine, Louisville, KY, United States
- 3West Virginia University School of Medicine, Morgantown, WV, United States
- 4Department of Behavioral Medicine and Psychiatry, West Virginia University School of Medicine, Morgantown, WV, United States
- 5Department of Pediatrics, Leonard M. Miller School of Medicine, University of Miami, Miami, FL, United States
Introduction: With technology routinely integrated into healthcare, it is essential that practitioners obtain skills in the numerous competencies required. Unfortunately, literature to guide use remains inconsistent and fragmented. The current scoping review identified technology-enhanced practice competencies for healthcare practitioners among peer-reviewed literature.
Methods: A review of PubMed, Scopus, Web of Science, PsycInfo, Global Index Medicus, and Journal of Technology in Behavioral Science was conducted between November 2022 and March 2023.
Results: 10,583,799 articles were identified, with 109 included in the final review. Seventeen primary competencies were identified with ethics (77.1%), legality (68.8%), and data security (65.1%) among the top three.
Conclusions: Although multiple technologies across specialties were identified, limited literature comprehensively defined technology-enhanced practice competencies to guide practitioner education. To address this gap, the Intersectional Technology Education and Competency in Healthcare (iTECH) Model was created to clarify educational targets for the use of technology in healthcare practices. Model development and finding applications are discussed.
Introduction
Technology-enhanced practices, broadly defined for the current study as practices involving practitioner and patient interactions with a technology that includes some level of practitioner involvement and/or oversight for the purpose of healthcare-related information collection or intervention services (1), have been utilized in healthcare for over a century (2). Such practices are categorized as synchronous (i.e., live, interactive), asynchronous (i.e., non-live), or hybrid (i.e., combination of synchronous, asynchronous, and in-person) (3, 4). Despite use, adoption among healthcare specialties (e.g., medicine, psychology, nursing, social work, counseling, physical therapy, occupational therapy) was suggested as relatively slow (5). While universally-accepted reasons for slow adoption are not well-defined, hypothesized reasons include limited training in the technologies leading to a lack of comfort, financial barriers to implementation, and a lack of organizational infrastructure to support the ongoing use of technologies (6–9). Limited usage continued until the late 1990s and early 2000s; coinciding with technology becoming smaller, cheaper, more powerful, more readily accessible, and more interconnected (10, 11). Among all technologies, telecommunication technologies uniquely demonstrated an unexpected and unprecedented growth in integration and expansion in response to the COVID-19 pandemic (12, 13). Expansion across time, combined with both practitioner and patient satisfaction (14–16) suggested that the integration of technologies into healthcare services is not only here to stay, but warrants clarification of relevant competencies to ensure that healthcare practitioners are effectively harnessing the technologies within their practices.
A cursory review of the technology-focused competency literature suggests the large emphasis on telehealth, or the integration of telecommunication technologies with healthcare services (e.g., videoconferencing, telephone, email, messaging programs), which has frequently been heralded as the future of medical and mental health-related healthcare (17, 18). While still considered limited, telehealth literature across healthcare specialties has demonstrated attempts to standardize competencies, including consolidated discussion by the American Telemedicine Association (19–21), the American Psychological Association (22), the American Psychiatric Association (23), and the American Medical Association (24). Nevertheless, literature remains fragmented, as well as varying in focus and elaboration by resource. More specifically, competencies across discussions have included, but are not limited to: awareness of research related to technologies, methods of adapting in-person strategies for digital administration, ethics of practice, legality, data security, troubleshooting technology, interpersonal skills, and interprofessional communication (11, 25–28).
While a positive first step, the landscape of healthcare technology has rapidly evolved beyond the narrow confines of telehealth alone. Recent literature underscores the research-validated utility of a diverse array of technologies in patient care, including virtual/augmented/extended reality (VR, AR, XR) (29, 30); robotics (31), video games (32), wearable technologies (33), artificial intelligence (AI) (34), and web-based self-guided assessment and intervention packages (35). This expansion necessitates a broader conceptualization of technology-enhanced practices that extends far beyond telecommunication alone.
Unfortunately, the rapid evolution of healthcare technology outpaced current educational paradigms, creating a critical gap between innovation and practitioner competencies. This disparity threatens the ethical, legal, evidence-informed, and safe integration of novel technologies into patient care (11). Proficient use of technology in healthcare demands more than both general knowledge and applied skills; it requires a nuanced understanding of diverse applications across various settings and populations. Simply put, being an excellent practitioner and adept at general technology use does not necessarily make one readily able to successfully integrate novel technologies into healthcare practices due to the large number of unique and unknown challenges that may arise.
As guiding healthcare organizations, ethical codes, and regulatory/licensing boards continue to promote evidence-informed education for technology-enhanced practice, clarification of relevant competencies to guide integration and continuing education remains prudent. Towards this end, there remains an urgent need for evaluation of available evidence-informed recommendations that address the broad spectrum of technology-enhanced practices in healthcare to inform practitioners' judicious use of these diverse technologies and ensure their effective integration into clinical practices. This endeavor can identify relevant documentation, as well as ongoing field gaps. Unfortunately, to date, no known work has evaluated the literature for technology-enhanced practice competencies (beyond telehealth), either independently or across healthcare specialties. This study aims to address this notable gap in the literature by conducting a scoping review of technology-enhanced practice competencies among peer-reviewed literature across healthcare specialties. Utilizing a comprehensive approach, we examine synchronous, asynchronous, and hybrid practitioner-patient interactions within various technological contexts. The investigation is guided by two primary research questions: (1) Which technology types are discussed in competency frameworks across healthcare specialties, and (2) What technology-enhanced practice competencies are recommended in the literature to guide practitioner use? By synthesizing findings from peer-reviewed sources, this study seeks to provide insights into the current landscape of technology competencies in healthcare, and may inform the development of more cohesive, multiprofessional approaches to technology integration in clinical practice.
Methods
Identifying relevant studies and study selection
The review utilized the Preferred Reporting Items for Systematic Review and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) reporting standards (36) (Supplementary Figure S1), as well as published scoping review methodologies (37, 38). More specifically, as based upon the study's primary questions, a modified population, concept, and context (PCC) framework was utilized in which the population was defined more broadly as healthcare specialties rather than specific population characteristics (e.g., age, race), concept was defined broadly as technology competencies, and the context included the setting of the technology use (39, 40). PubMed, Scopus, Web of Science, PsycInfo, and Global Index Medicus were reviewed between November 2022 and March 2023 (see Supplementary Table S1 for Boolean operators). Due to a high number of competency- and training-focused works being published in the Journal of Technology in Behavioral Science, yet not all works being identified on searched databases, this journal was also specifically reviewed with the same search methodology. Rayyan, a web-based application for conducting structured literature reviews, was utilized to organize data and remove duplicates (41).
Inclusionary criteria
Following the removal of duplicates, an item was included in the final dataset if it was written in English, was a manuscript in a peer-reviewed journal, focused on technology, focused on healthcare, focused on the education of a healthcare practitioner (i.e., graduate-level training through licensed professional), and included a direct naming of a specific competency or educational target combined with at least one statement defining/detailing the competency (i.e., a manuscript stating “data security” was not included, while a manuscript saying “data security” and also detailing that this is inclusive of passwords and/or encryption standards was included). This approach was designed to eliminate papers that were merely listing topics, and thus less helpful for practitioners seeking applied knowledge for their practices. A competency was defined for the current review as a designated target of practitioner knowledge and/or applied skill for the specific technology to ensure an ethical, legal, safe, and evidence-informed service. This definition aligns with similar review literature defining the term competency or competencies (33, 42–46). As the use of technology in healthcare can be traced back to the 1800s (2), to ensure comprehensive review, no year-related criteria were applied (i.e., all manuscripts through March 2023 were eligible for inclusion).
Data cleaning and screening processes
In line with suggestions for screening very large amounts of data, a title-first approach was utilized (47). This approach has been suggested as more efficient, yet comparable to screening both titles and abstracts together. To account for Rayyan's lack of sequential Boolean operator-based screening, titles were first screened by education-, teaching-, and training-related keywords; then technology-related keywords; and finally, healthcare-related keywords for relevancy. Standardized keywords were collectively identified by the authors as relevant to the scoping review (Supplementary Table S2). Among the remaining items, abstracts were screened for additional applicability. Each potential item was reviewed by three sets of two authors, with a third author as a tie breaker, as needed. Following training by the primary author, interrater reliability kappa values for all pairs were ≥0.99, suggesting “almost perfect” levels of agreement (48). Finally, full texts of remaining items were screened and coded to identify technology-focused competencies (e.g., ethics, legality) relevant to healthcare services. Coding was completed by the two first authors to establish consensus. Prior to discussion of disagreements until consensus was reached (42), interrater reliability kappa value was 0.93 for overall agreement for inclusion/exclusion of each identified manuscript.
As further detailed in Table 1, manuscripts were coded across the variables of: paper type, publication date, author location, specialty area, whether the discussion was interdisciplinary (i.e., discussed more than one specialty), career stage, location of discussion, types of technology, and identified competencies.
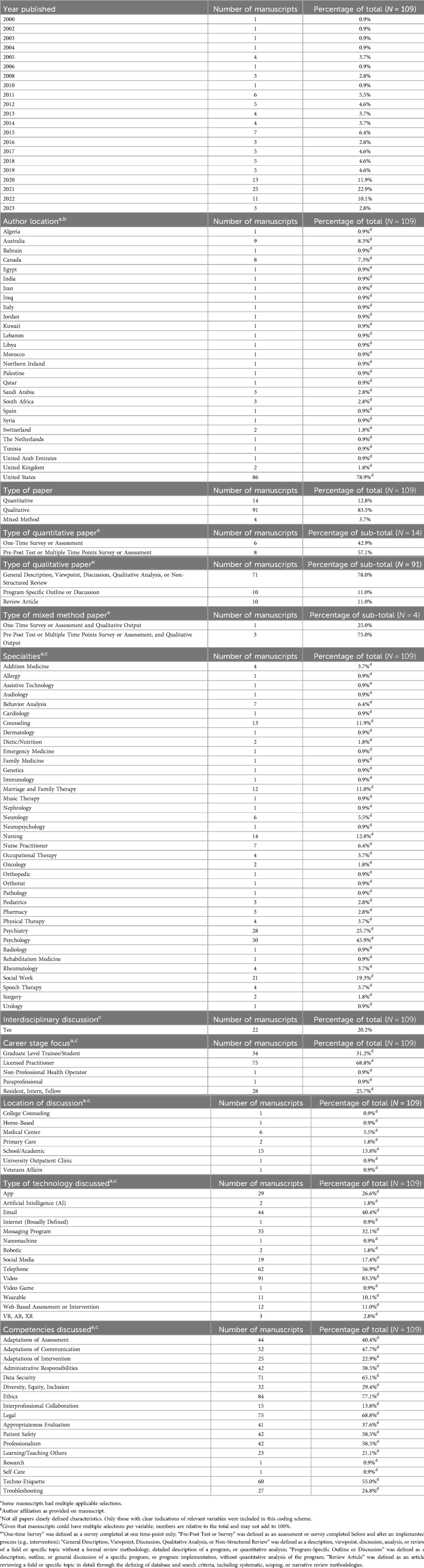
Table 1. Frequencies of coded variables Among included manuscripts (N = 109).
Results
The initial search yielded 10,583,799 records (Supplementary Figure S1). One hundred and nine met inclusionary criteria and were included in the final review (Tables 1, 2).

Table 2. Characteristics of included studies (N = 109)a.
Summary findings
Paper type
Among included manuscripts (N = 109), 14 (12.8%) were coded as quantitative, 91 (83.5%) were coded as qualitative, and 4 (3.7%) were coded as mixed method. Among the 14 quantitative manuscripts, 6 (42.9%), were coded as a general one-time survey or assessment, and 8 (57.1%) were coded as a pre-post test or multiple time points survey or assessment. Among the 91 qualitative manuscripts, 71 (78.0%) were coded as a general description, viewpoint, discussion, qualitative analysis, or nonsystematic review; 10 (11.0%) were coded as a program-specific outline or discussion; and 10 (11.0%) were coded as a review article (e.g., formal systematic, scoping, or narrative review with a database search, goals, and/or search terms). Among the 4 mixed-method manuscripts, 1 (25.0%) was coded as a one-time survey or assessment and qualitative output, while 3 (75.0%) were coded as a pre-post test or multiple time points survey or assessment and qualitative output.
Publication date
All included manuscripts (N = 109) were published between 2000 and 2023, with a substantially greater number of publications per year in or following 2020 as compared to 2019 and earlier.
Author location
Among included manuscripts (N = 109), most authors had affiliations within the United States (86, 78.9%).
Specialty area
Specialty area of manuscript discussions (N = 109) varied widely across both mental health and medical domains. Psychology- (50, 45.9%), psychiatry- (28, 25.7%), and social work-focused manuscripts (21, 19.3%) were the three most discussed types of specialty areas.
Interdisciplinary discussion
Among included manuscripts (N = 109), 22 (20.2%) included more than one specialty as a focus of discussions.
Career stage
Of the total manuscripts (N = 109), 75 (68.8%) focused discussions on licensed practitioners, 34 (31.2%) focused on graduate level students/trainees, 28 (25.7%) focused on residents, interns, or fellows, one (0.9%) focused on paraprofessionals, and one (0.9%) focused on non-professional health operators.
Location of discussion
Of the total manuscripts (N = 109), 15 (13.8%) focused on school/academic locations, 6 (5.5%) focused on medical centers, 2 (1.8%) focused on primary care clinics, and 1 (0.9% each) focused on college counseling, home-based, university outpatient clinic, and Veterans Affairs.
Types of technology
Of the total manuscripts (N = 109), video (91, 83.5%), telephone (62, 56.9%), and email (44, 40.4%) were the three most discussed types of technology.
Identified competencies
Of the total manuscripts (N = 109), ethics (84, 77.1%), legal considerations (75, 68.8%), and data security (71, 65.1%) were the three most discussed types of competencies.
Additional considerations
Many excluded manuscripts focused on: (a) applications of technology in general healthcare service without discussion of competencies or training, (b) methods of training healthcare skills through the use of technology (e.g., e-learning), (c) practitioner or patient attitudes towards technology, (d) satisfaction with technology use, and (e) programmatic descriptions of technology integration with general healthcare clinics without detailing the applied competencies. Across studies with diverse focuses, authors consistently emphasized the necessity for more extensive training in both graduate education and professional practice to foster a comprehensive understanding and appreciation of the various competencies required for effective technology-enhanced practice.
In addition to the majority of included manuscripts focusing on mental health-focused specialties, it was recognized that among manuscripts not included, several other specialties have discussed or been discussed to utilize technology-enhanced practices, such as anesthesiology. Settings among manuscript not included, yet discussed as integrating technology, were also highly variable and included: childcare center, community mental health clinic, federally-qualified healthcare center, government agency (e.g., Department of Defense), mobile unit, prison/corrections, private practice, and military.
Discussion
The current scoping review is believed to be the first to consolidate literature from across healthcare specialties to clarify competencies relevant to technology-enhanced practices. Among the 109 included manuscripts, all were published since 2000, with the majority being published during or post 2020. While the current study did not evaluate reasons for this finding, it was hypothesized that since a significant portion of the included manuscripts focused on telecommunication technologies, the increase in telehealth utilization post-COVID-19, combined with technology becoming more readily available and applied (12, 13), led to an increased recognition of the importance of competencies related to technology, thus fostering increased publication of study-relevant literature.
Related to the competencies themselves, as well as research question 1, literature discussed numerous modalities ranging from telecommunication technologies (e.g., video, telephone) to more esoteric technologies (e.g., wearable, VR/AR/XR). Findings not only suggested ongoing expansion of novel technologies into healthcare services, but also growing abilities of healthcare practitioners to harness the technologies to overcome historical barriers precluding effective healthcare. As one example, the use of wearable technologies permits ongoing physiological monitoring without relying on a patient to track their progress on paper-and-pencil forms, allowing for live and more accurate progress monitoring.
Related to research question 2, despite a multitude of articles suggesting the importance of developing competencies for the various technologies, relatively few highlighted specific competencies needed for different technologies. Fewer yet (N = 109) included a basic definition or operationalization of competencies to guide practitioners in the specifics of what to learn and how to adapt the technologies in order to effectively integrate them into their day-to-day practices. Additionally, among those detailing the competencies, the majority focused on ethical and legal considerations, as well as data security, with significant variability among the remaining competencies. Although specific reasons for why these three emerged as the most common are not currently clear, since the majority of the manuscripts included focused more on telehealth-related competencies (i.e., video, telephone) relative to other technologies (e.g., virtual reality, robotics), it was hypothesized that the marked increase in telehealth-related work following COVID-19 (12, 13) that coincided with the increased focus in ethical and legal practices emphasized by governing organizations (e.g., American Medical Association, American Psychiatric Association, American Psychological Association, National Association of Social Workers), licensing boards, and researchers, led to an increased recognition of the importance of ethics, legal, and data security specifically above and beyond any other possible competencies.
Finally, while some quantitative studies were reviewed, the majority of included publications were qualitative, and generally comprised of reviews, descriptions, viewpoints, recommendations, or program-specific overviews. As a result, it becomes clear that additional study is required to not only test often-suggested recommendations to better clarify what competencies are required as varying by technology, location, and specialty, but also how to best teach/acquire such information.
While not a primary target of the current study, some additional interesting findings were recognized. The review concluded that although a wider range of specialties than what was included in the final analysis were suggested to utilize technology in practice, discussions of competencies remain limited for many of these specialties. This becomes especially impactful for more specialized practitioners who may not seek cross-discipline journal articles to inform their practice, thus potentially missing relevant technology-related literature. For instance, although multiple manuscripts discussed the application of robotics (e.g., surgery), few manuscripts included in the final review discussed relevant competencies or means to gain such knowledge for the use of robotics in healthcare services.
Integration and clinical application – iTECH model
Upon review of the findings, it became apparent that due to fragmentation and variability, no singular discussion was applicable to all specialties or technologies, or comprehensive enough to cover the wide range of possible service variations that may present for healthcare practitioners. To address this challenge, findings were organized into domains of competency to create the Intersectional Technology Education and Competency in Healthcare (iTECH) Model: a model designed as a comprehensive, intersectional, versatile, and multiprofessional means to guide practitioner education and training to foster optimal use of technologies in healthcare-related practices. The model is not only believed to influence educational and training activities, but also foster improved patient outcomes and practitioner effectiveness through guiding practitioners to the most pertinent competencies relative for their unique healthcare service.
Creation of the model was a multi-step process involving integration of study outcomes in combination with author consensus for grouping and naming. This approach aligned with past methodologies for telehealth/technology competency scoping reviews and model creation (26). In this way, information gathered from the study characteristics outlined in Table 2 (i.e., identified competencies, technology type, setting, career state focus, specialty area) created the foundation of domains for the novel model. Authors then combined their individual and collective experiences in training, research (including knowledge of the current study's non-included review articles), and professional work related to technology-enhanced practices to supplement the core information. Through this method, a domain for the model was established when consensus was reached that the identified domain was not only directly applicable to a healthcare practitioner's technology-enhanced practice, but provided a meaningful distinction from other domains, even if one influences another (26). This method (Figure 1) yielded six broad domains: (1) primary knowledge; (2) service type; (3) modality type; (4) delivery format; (5) setting; and (6) diversity, equity, inclusion, and justice (DEIJ). A seventh domain was also identified; however, based on author review of the literature, this domain, titled “supplemental knowledge,” was believed to be informative for practitioners, but nonessential (e.g., history of technology use). Each included domain is believed to be equally important to consider for any technology-enhanced practice, and can influence the others. For example, modality type can influence the types of services that could be provided, as well as the primary knowledge considerations required for effective use of that technology. While aspirational in nature, the model can be viewed as a means to guide an ethical, legal, evidence-informed, and safe practice through the selection of relevant competencies, while removing those less relevant to one's unique role. The healthcare practitioner can then utilize relevant competencies to focus readings, trainings, consultation, or other methods of gaining knowledge on these specific targets.
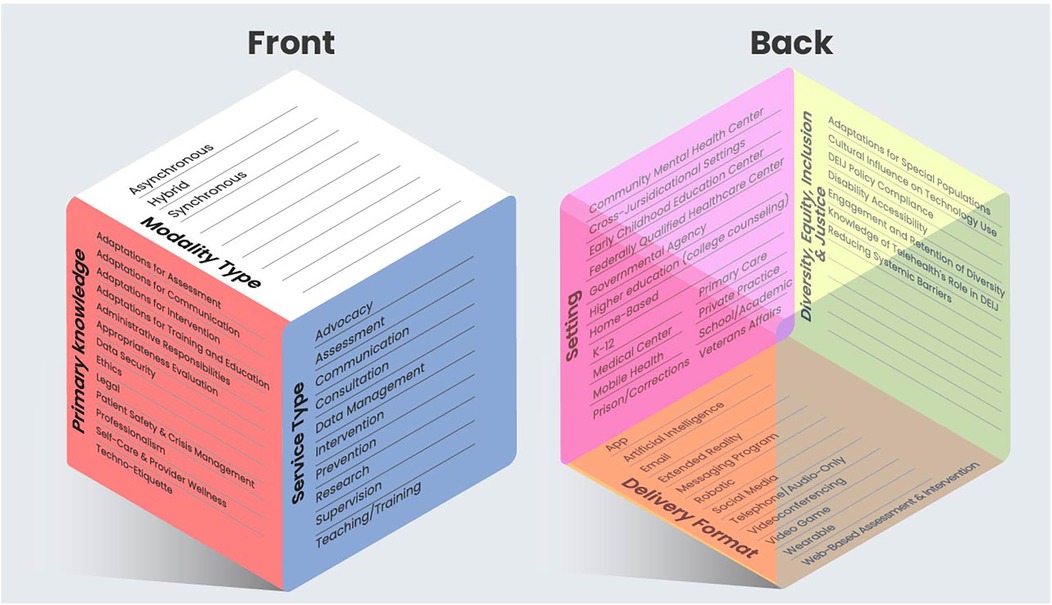
Figure 1. Intersectional technology education and competency in healthcare (iTECH) model. aModality Type = The method in which technology is applied; Service Type = How the technology is used; Primary Knowledge = The type of technology-focused information practitioners should know to ensure ethical, legal, evidence-informed, and safe technology-enhanced practices; Delivery Format = The type of technology utilized; Setting = The locations in which the technology is utilized; Diversity, Equity, Inclusion, and Justice (DEIJ) = Consideration of factors relevant to the use of, and attitudes towards, the use of technology. bThe model can be adapted and applied for emerging technologies, settings, and uses.
As an example of model application, consider a hospital-based child psychiatrist wanting to utilize an AI chatbot that tracks daily patient mood and patient-reported skill use. They may begin their application of the model by first clarifying the AI technology as their delivery format, with the service type focusing on assessment (i.e., data collection), the modality type as asynchronous, and the setting type as both a hospital (for practitioner) and home-based (for patient). The psychiatrist can use this information to educate themselves on primary knowledge relevant topics, including, but not limited to, differences between pencil-and-paper tracking vs. digital methods in terms of outcomes, data security considerations of sending and receiving patient data, and safety planning should a mood-related crisis arise. Additionally, the psychiatrist can explore setting-specific guidelines/requirements/restrictions of their organization for the use of AI. Finally, DEIJ factors, such as the role of systemic barriers and means of engagement and retention, should be considered, including the potential for financial-related data limitations (i.e., data allotment by plan) and how that can affect ongoing use of the chatbot. Additionally, biases (e.g., language) that could be introduced through the machine learning and natural language processing developmental operations of the AI chatbot should be considered (49).
Limitations
Study findings should be interpreted within the context of recognized limitations. First, similar to other scoping reviews, literature may have been missed or omitted due to database selection, language criteria, and Boolean operators not matching all relevant manuscript meta data (50). Additionally, although the sequential adding of search terminology aligned with past literature and use of Rayyan, it is recognized that this could have resulted in some relevant literature being excluded due to not meeting full search term criteria for further review. Similarly, while published research procedures were followed, a screening of title and abstract may have inadvertently removed some literature that would have been relevant, but not clearly indicated as such in the title or abstract information. While attempts were made to control for human error (e.g., multiple coders, spot checking), given the large amount of data and subjective nature of the coding, human error cannot be fully ruled-out. Nevertheless, overall reporting is believed representative of the constructs within the literature. Although a decision was made to exclude non-peer-reviewed outlets (e.g., certificate programs), some non-studied outlets may include competency-related information not accounted for in peer-reviewed literature. Additionally, the lack of grey literature imposes a publication bias. Finally, in line with other scoping review methodologies (51, 52), the study was descriptive in nature and did not include an appraisal of the quality of the literature.
Future directions
Future work related to the current study should include more databases and literature that were published following the current study's review period in order to determine any subsequent developments in technology-enhanced practice competencies. Additionally, a wider scope should be considered, including both peer-reviewed and non-peer-reviewed literature. For example, organization guidebooks (e.g., American Psychological Association, American Telemedicine Association), certificate programs, books, book chapters, and grey literature can be considered for inclusion. Future work should also seek to create universally-accepted standards for competency acquisition for technology-enhanced practices. More specifically, tighter operational definitions of a skill, testing and refinement, and proximal and distal (i.e., longitudinal) evaluation should be established. Standardization and long-term review can foster more objective measurement to evaluate successful methodologies, as well as areas for improvement. Additionally, standardization can allow for more direct evaluation of relevant outcome measures, such as cost-benefit assessments for the individual, the organization, and the patient in terms of positive outcomes and financial costs. Finally, future work should seek to further explore the iTECH model through two means. First, the model should be compared to other known models/recommendations of technology-related competency acquisition by guiding organizations, including the American Medical Association (24), the American Psychological Association (22), American Psychiatric Association (23), American Telemedicine Association (21), World Health Organization (9), and the American medical Informatics Association (53), as well as researcher-based models/recommendations [e.g., (26)]. This comparison can allow for identification of strengths and areas of improvement for the iTECH model. Second, it is essential that the model is implemented and assessed in healthcare practitioner's training curriculum to determine its influence in fostering both knowledge and hands-on competencies. This evaluation can consider usability and adaptability to different healthcare specialties and technologies. Pre- and post-education assessment can clarify trainer attitudes towards the model, trainee attitudes towards the model, and educational outcomes in terms of both evidence-informed understanding of utilized technologies and application. Once determined useful, the model can serve as a guide to create technology-enhanced practice curriculum for training programs in terms of coursework, applied hands-on work, and supervision. As the model is implemented, it is important to utilize an established framework for skill acquisition and education. One recommended method is the Kirkpatrick Model (54), as this model has been heavily cited within the literature for such purposes (55, 56). This model focuses on four levels of evaluation: reaction, learning, behavior, and results. Reactions focus on how trainees like a particular training model. Such an evaluation could include both quantitative (e.g., surveys/ratings of satisfaction) and/or qualitative (e.g., focus groups) assessments to measure trainees' perceptions of the model (54, 55). Effective learning assessment measures both program acceptance and knowledge transfer while gathering feedback to enhance future training. When trainees view a program positively, they are more likely to engage with and retain the material (54). Of important note, it is essential that evaluation objectively measures the amount of learning that takes place in addition to subjective experiences. Such evaluations can be completed through performance testing, simulations, case studies, and pre to post assessments (55). Behavior evaluates real-world behavior change with comparison of an intervention group to a control group. According to Kirkpatrick (54), this approach demands a scientific methodology using systematic before-and-after performance evaluations (examining both proximal and distal outcomes) with statistical analyses to measure behavioral changes. Finally, results evaluate system-wide or organizational impacts of the training program, such as improved evidence-informed practices, reduced costs, higher quality, increased production rates of satisfaction, varying based on specific program goals (54, 55). Graduate education presents an optimal opportunity to integrate the iTECH model with Kirkpatrick's method, enabling evaluation of technology-enhanced practices by training directors across various levels including practicum, internship, fellowship, and residency programs, depending on the healthcare specialty. Following evaluation, the iTECH model's implementation can be modified through an iterative approach to implementation. As trainee's advance through their training, milestone levels can be evaluated through the Dreyfus and Dreyfus model (57, 58), which evaluates the acquisition of expertise as a developmental process through five primary steps: novice, to advanced beginner, competent, proficient, and expert. As adapted by Hilty et al. (55), novice could be equated to a graduate student, advanced beginner to a first-year resident, competent to a senior resident, proficient to a graduating resident, and expert as a competent and licensed practitioner.
Utilizing such an educational framework, integration of the iTECH model can occur at multiple stages of one's professional development to account for the need for both didactic and hands-on experiential training (11). First, didactic information regarding relevant technologies can be provided during or following the introduction of general healthcare strategies. More specifically, the application of healthcare techniques (e.g., assessment, interventions) can be discussed in terms of both traditional and technology-enhanced methods. Such discussion can focus on general use of the technologies, relevant research, and both benefits and limitations of usage relative to non-technology methods in order to foster critical thinking of the use of the technologies (11). For example, a course describing ethical and legal healthcare can also include a discussion of jurisdictional practices and differences when implementing video or robotics (e.g., surgery) that may span different states, provinces, territories, or countries. Methods of learning about such differences, as well as how to safely account for and navigate such differences can also be outlined. Supplementing general discussions, advanced coursework can be created for either the broad integration of technology, or for specific technologies, such as a class on robotics for surgery, artificial intelligence in the use of medical research, or video for psychotherapy. While limited discussions of such coursework are available in the literature, and predominantly focus on telehealth rather than other technologies, courses and curriculums that can provide templates from which additional technology-focused work can be derived include Perle's Introduction to Telehealth for Clinical Psychologists (59), the University of Illinois College of Medicine at Peoria's robotic surgery training curriculum (60), and Greenberg and colleague's description of a pilot robotic surgery curriculum (61). Following the trainees acquisition of didactic information, hands-on experiences should be completed with classroom-based role play and simulation labs, as well as through real-world application in placements (e.g., practicum, internship, fellowship, residency). All work should be supervised with scheduled and/or live supervision, as appropriate to the site and training model. Technology-focused supervision must not only include consideration of the general healthcare practices and patient outcomes, but also numerous technology-focused considerations. For instance, supervision should include discussions of how the technologies were used, how they compared to non-technology-enhanced methods, the benefits of the integration of the technologies, limitations of the technologies, how any arising issues were addressed, how the technologies were perceived by the practitioner, how the technologies were perceived by the patient, and how the technologies interacted to change the healthcare service being provided. Training and supervision requirements can be guided by principles and standards set by governing organizations of the healthcare specialty, such as the American Psychological Association's Commission on Accreditation (62) and the Accreditation Council for Graduate Medical Education (63, 64). To monitor the impact of the novel curriculum and methodologies, graduate programs should implement both objective and subjective methods of assessment outside of the coursework and fieldwork. Assessment can include measurement of the improvement in both knowledge and hands-on technology-enhanced competencies as defined by the iTECH model and available literature, as well as aligning standards set forth by accreditation governance. Assessment can also evaluate attitude changes towards technologies, perceived ease of use of the technologies, perceived benefits and limitations of the technologies, supervisor challenges with teaching technologies, and trainee challenges with learning the technologies. Finally, distal assessment should evaluate if the training fostered ongoing use of technologies, as well as which types, into the future (11). Given rapid developments, ongoing continuing education post graduate education is essential. As a result, training institutions (e.g., universities, hospitals, licensing boards, professional organizations) must design new self-guided and professionally-led continuing education series to foster ongoing education of specific technologies for specific healthcare specialties. Such strategies can include self-education through continuing education literature, didactic presentations either live or via webinar, and hands-on training workshops. Well-rounded training and knowledge are believed necessary to foster optimal technology-enhanced healthcare services that adapt as the field continues to evolve to yield new technologies and competencies. Education is not only to ensure a practitioner's ability to effectively integrate and maintain the technologies, but also to ensure that practitioners are equipped with research-informed rationales for what technology works best for who, as well as which may be contraindicated or to be used with caution. Further, as not all individuals may equally respond to different technologies and strategies, methods of how to adapt the technologies for unique population demographics (e.g., age, education, race, language, disability, socioeconomic status, technology comfort level) and pathologies are essential.
Conclusions
The current scoping review suggested ongoing expansion of technology into healthcare practices, indicating the need for greater practitioner resources to ensure their acquisition of necessary competencies to foster ethical, legal, evidence-informed and safe practices. In doing so, practitioners can acquire necessary knowledge to be able to tailor technologies and clinical services to unique services, population demographics, and pathologies. Nevertheless, findings also indicated that few peer-reviewed manuscripts highlighted and expounded upon specific competencies needed or recommended for practice. Additionally, despite the review yielding a variety of technologies used across healthcare specialization, the review process allowed for recognition that a wider range of technologies are believed to be utilized across a larger scope of healthcare specialties than what was recognized in the final scoping review as based upon the inclusionary criteria (e.g., many studies did not expound upon competencies), necessitating the need for greater competency development and dissemination to inform practitioners. To address this gap, the iTECH Model was created to guide a practitioner's technology-enhanced practice. The model is believed to assist practitioners in identifying relevant competencies to ensure knowledge and hands-on experiences relevant to their unique practices in order to foster optimal care and patient outcomes, while reducing possible issues. Although believed helpful, the current work is viewed as a first-step. There remains a need for additional study to not only better understand literature-suggested competencies, as evolving over time, but also to explore best methods for integrating the iTECH model into graduate coursework, real-world experiences, and continuing education to enhance its utility for diverse healthcare practitioners.
Author contributions
JP: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing, Data curation, Investigation, Project administration, Resources, Software, Supervision, Validation, Visualization. DC: Data curation, Methodology, Writing – original draft, Writing – review & editing, Conceptualization, Formal analysis, Investigation, Supervision. EB: Data curation, Investigation, Writing – original draft, Writing – review & editing. MC: Data curation, Investigation, Writing – original draft, Writing – review & editing. JD: Data curation, Investigation, Writing – original draft, Writing – review & editing. PN: Data curation, Investigation, Writing – original draft, Writing – review & editing. GM: Data curation, Investigation, Writing – original draft, Writing – review & editing. JJ: Conceptualization, Formal analysis, Funding acquisition, Methodology, Visualization, Writing – original draft, Writing – review & editing, Data curation, Investigation.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors would like to thank Abigail Peskin, PhD for her feedback.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdgth.2025.1571518/full#supplementary-material
References
1. Anton MT, Jones DJ. Adoption of technology-enhanced treatments: conceptual and practical considerations. Clin Psychol Sci Pract. (2017) 24(3):223–40. doi: 10.1111/cpsp.12197
3. Chen K, Huang JJ, Torous J. Hybrid care in mental health: a framework for understanding care, research, and future opportunities. NPP Digit Psychiatry Neurosci. (2024) 2:16. doi: 10.1038/s44277-024-00016-7
4. Lagera PGD, Chan SR, Yellowlees PM. Asynchronous technologies in mental health care education. Curr Treat Options Psych. (2023) 10:59–71. doi: 10.1007/s40501-023-00286-6
6. Chen J, Amaize A, Barath D. Evaluating telehealth adoption and related barriers among hospitals located in rural and urban areas. J Rural Health. (2021) 37(4):801–11. doi: 10.1111/jrh.12534
7. England I, Stewart D, Walker S. Information technology adoption in health care: when organisations and technology collide. Aust Health Rev. (2000) 23(3):176–85. doi: 10.1071/AH000176
8. Poon EG, Jha AK, Christino M, Honour MM, Fernandopulle R, Middleton B, et al. Assessing the level of healthcare information technology adoption in the United States: a snapshot. BMC Med Inform Decis Mak. (2006) 6(1):1–9. doi: 10.1186/1472-6947-6-1
9. World Health Organization. WHO guideline: Recommendations on digital interventions for health system strengthening (2019). Available at: https://iris.who.int/bitstream/handle/10665/311941/9789241550505-eng.pdf?sequence=31 (Accessed March 07, 2025).
10. Bashshur RL, Reardon TG, Shannon GW. Telemedicine: a new health care delivery system. Annu Rev Public Health. (2000) 21(1):613–37. doi: 10.1146/annurev.publhealth.21.1.613
11. Perle JG. Training psychology students for telehealth: a model for doctoral-level education. J Technol Behav Sci. (2021) 6:456–9. doi: 10.1007/s41347-021-00212-8
12. Perle JG. Mental health providers’ telehealth education prior to and following implementation: a COVID-19 rapid response survey. Prof Psychol Res Pract. (2022) 53(2):143–50. doi: 10.1037/pro0000450
13. Shachar C, Engel J, Elwyn G. Implications for telehealth in a postpandemic future: regulatory and privacy issues. J Am Med Assoc. (2020) 323(23):2375–6. doi: 10.1001/jama.2020.7943
14. Gentry MT, Puspitasari AJ, McKean AJ, Williams MD, Breitinger S, Geske JR, et al. Clinician satisfaction with rapid adoption and implementation of telehealth services during the COVID-19 pandemic. Telemed J e-Health. (2021) 27(12):1385–92. doi: 10.1089/tmj.2020.0575
15. Harting MT, Wheeler A, Ponsky T, Nwomeh B, Snyder CL, Bruns NE, et al. Telemedicine in pediatric surgery. J Pediatr Surg. (2019) 54(3):587–94. doi: 10.1016/j.jpedsurg.2018.04.038
16. Kolbe L, Jaywant A, Gupta A, Vanderlind WM, Jabbour G. Use of virtual reality in the inpatient rehabilitation of COVID-19 patients. Gen Hosp Psychiatry. (2021) 71:76–81. doi: 10.1016/j.genhosppsych.2021.04.008
17. Kichloo A, Albosta M, Dettloff K, Wani F, El-Amir Z, Singh J, et al. Telemedicine, the current COVID-19 pandemic and the future: a narrative review and perspectives moving forward in the USA. Fam Med Community Health. (2020) 8(3):e000530. doi: 10.1136/fmch-2020-000530
18. Mishkind MC, Shore JH, Schneck CD. Telemental health response to the COVID-19 pandemic: virtualization of outpatient care now as a pathway to the future. Telemed J e-Health. (2021) 27(7):70–711. doi: 10.1089/tmj.2020.0303
19. Davis TM, Barden C, Dean S, Gavish A, Goliash I, Goran S, et al. American Telemedicine association guidelines for TeleICU operations. Telemed J e-Health. (2016) 22(12):971–80. doi: 10.1089/tmj.2016.0065
20. Theurer L, Bashshur R, Bernard J, Brewer T, Busch J, Caruso D, et al. American Telemedicine Association guidelines for teleburn. Telemed J e-Health. (2017) 23(5):365–75. doi: 10.1089/tmj.2016.0279
21. American Telemedicine Association. Best practices in videoconferencing-based telemental health (2018). Available at: https://www.americantelemed.org/resource_categories/practice-guidelines/ (Accessed September 30, 2024).
22. American Psychological Association. APA guidelines for the practice of telepsychology (2024). Available at: https://www.apa.org/practice/guidelines/telepsychology-revision.pdf (Accessed September 30, 2024).
23. American Psychiatric Association. Telepsychiatry toolkit (2024). Available at: https://www.psychiatry.org/psychiatrists/practice/telepsychiatry/toolkit (Accessed September 30, 2024).
24. American Medical Association. AMA telehealth practice implementation (2023). Available at: https://www.ama-assn.org/practice-management/digital/ama-telehealth-practice-implementation (Accessed September 30, 2024).
25. Galpin K, Sikka N, King SL, Horvath KA, Shipman SA, the AAMC Telehealth Advisory Committee. Expert consensus: telehealth skills for health care professionals. Telemed J e-Health. (2021) 27(7):820–4. doi: 10.1089/tmj.2020.0420
26. McCord C, Bernhard P, Walsh M, Rosner C, Console K. A consolidated model for telepsychology practice. J Clin Psychol. (2020) 76(6):1060–82. doi: 10.1002/jclp.22954
27. Maheu MM, Drude KP, Hertlein KM, Lipschutz R, Wall K, Hilty DM. Correction to: an interprofessional framework for telebehavioral health competencies. J Technol Behav Sci. (2018) 3:108–40. doi: 10.1007/s41347-018-0046-6
28. Noronha C, Lo MC, Nikiforova T, Jones D, Nandiwada DR, Leung TI, et al. Telehealth competencies in medical education: new frontiers in faculty development and learner assessments. J Gen Intern Med. (2022) 37:3168–73. doi: 10.1007/s11606-022-07564-8
29. Munzer BW, Khan MM, Shipman B, Mahajan P. Augmented reality in emergency medicine: a scoping review. J Med Internet Res. (2019) 21(4):e12368. doi: 10.2196/12368
30. Orser BA, Spadafora SM. Competence-based training and immersion virtual reality: paradigm-shifting advances in medical education. Anesth Analg. (2022) 135(2):220–2. doi: 10.1213/ANE.0000000000006116
31. George EI, Brand CT, Marescaux J. Origins of robotic surgery: from skepticism to standard of care. J of the Soc of Laparoendosc Surg. (2018) 22(4):e2018.00039. doi: 10.4293/jsls.2018.00039
32. Zayeni D, Raynaud JP, Revet A. Therapeutic and preventive use of video games in child and adolescent psychiatry: a systematic review. Front Psychiatry. (2020) 11:36. doi: 10.3389/fpsyt.2020.00036
33. Hilty DM, Armstrong CM, Edwards-Stewart A, Gentry MT, Luxton DD, Krupinski EA. Sensor, wearable, and remote patient monitoring competencies for clinical care and training: scoping review. J Technol Bev Sci. (2021) 6(2):252–77. doi: 10.1007/s41347-020-00190-3
34. Secinaro S, Calandra D, Secinaro A, Muthurangu V, Biancone P. The role of artificial intelligence in healthcare: a structured literature review. BMC Med Inform Decis Mak. (2021) 21(1):1–23. doi: 10.1186/s12911-021-01488-9
35. de Oliveira Lima L, Saragiotto BT, Costa LOP, Nogueira LC, Meziat-Filho N, Reis FJJ. Self-guided web-based pain education for people with musculoskeletal pain: a systematic review and meta-analysis. Phys Ther. (2021) 101(10):pzab167. doi: 10.1093/ptj/pzab167
36. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J Clin Epidemiol. (2021) 134:103–12. doi: 10.1016/j.jclinepi.2021.02.003
37. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8(1):19–32. doi: 10.1080/1364557032000119616
38. Mak S, Thomas A. Steps for conducting a scoping review. J Grad Med Educ. (2022) 14(5):565–7. doi: 10.4300/JGME-D-22-00621.1
39. Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. (2020) 18(10):2119–26. doi: 10.11124/JBIES-20-00167
40. Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Scoping reviews. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. JBI (2024). p. 417–76. Available at: https://jbi-global-wiki.refined.site/space/MANUAL (Accessed September 30, 2024).
41. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan – A web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1086/s13643-016-0384-4
42. Anil K, Bird AR, Abey S. Telehealth competencies for allied health professionals: a scoping review. J Telemed Telecare. (2023):1–13. doi: 10.1177/1357633X231201877
43. Arends R, Gibson N, Marckstadt S, Britson V, Nissen MK, Voss J. Enhancing the nurse practitioner curriculum to improve telehealth competency. J Am Assoc Nurse Pract. (2021) 33:391–7. doi: 10.1097/JXX.0000000000000303
44. Hart A, Romney D, Sarin R, Mechanic O, Hertelendy AJ, Larson D, et al. Developing telemedicine curriculum competencies for graduate medical education: outcomes of a modified delphi process. Acad Med. (2022) 97:577–85. doi: 10.1097/ACM.0000000000004463
45. Hilty D, Chan S, Torous J, Luo J, Boland R. A framework for competencies for the use of mobile technologies in psychiatry and medicine: scoping review. JMIR Ment Health. (2020) 8(2):e12229. doi: 10.2196/12229
46. Maheu MM, Wright SD, Neufeld J, Drude KP, Hilty DM, Baker DC, et al. Interprofessional telebehavioral health competencies framework: implications for telepsychology. Prof Psychol Res Pr. (2021) 52(5):439–48. doi: 10.1037/pro0000400
47. Mateen FJ, Oh J, Tergas AI, Bhayani NH, Kamdar BB. Titles versus titles and abstracts for initial screening of articles for systematic reviews. Clin Epidemiol. (2013) 5:89–95.23526335
49. Timmons AC, Duong JB, Fiallo NS, Lee T, Vo HPQ, Ahle MW, et al. A call to action on assessing and mitigating bias in artificial intelligence applications for mental health. Perspect Psychol Sci. (2023) 18(5):1062–96. doi: 10.1177/17456916221134490
50. Maggio LA, Larsen K, Thomas A, Costello JA, Artino AR Jr. Scoping reviews in medical education: a scoping review. Med Educ. (2021) 55(6):689–700. doi: 10.1111/medu.14431
51. Gleason KT, Peereboom D, Wec A, Wolff JL. Patient portals to support care partner engagement in adolescent and adult populations: a scoping review. JAMA Netw Open. (2022) 5(12):e2248696. doi: 10.1001/jamanetworkopen.2022.48696
52. Haslam A, Tuia J, Prasad V. Scoping review of published oncology meta-analyses in high-impact oncology journals. JAMA Netw Open. (2023) 6(6):e2318877. doi: 10.1001/jamanetworkopen.2023.18877
53. Valenta AL, Berner ES, Boren SA, Deckard GJ, Eldredge C, Fridsma DB, et al. AMIA board white paper: AMIA 2017 core competencies for applied health informatics education at the master’s degree level. J Am Med Inform Assoc. (2018) 25(12):1657–68. doi: 10.1093/jamia/ocy132
54. Kirkpatrick DL. Great ideas revisited. Techniques for evaluating training programs. Train Dev. (1996) 50(1):54–9.
55. Hilty DM, Crawford A, Teshima J, Chan S, Sunderji N, Yellowlees PM, et al. A framework for telepsychiatric training and e-health: competency-based education, evaluation and implications. Int Rev Psychiatry. (2015) 27(6):569–92. doi: 10.3109/09540261.2015.1091292
56. Smidt A, Balandin S, Sigafoos J, Reed VA. The kirkpatrick model: a useful tool for evaluating training outcomes. J Intellect Dev Disabil. (2009) 34(3):266–74. doi: 10.1080/13668250903093125
57. Dreyfus SE, Dreyfus HL. A five-stage model of the mental activities involved in directed skill acquisition (ORC 80-2). University of California, Operations Research Center (1980). Available at: https://apps.dtic.mil/sti/citations/ADA084551 (Accessed September 30, 2024).
58. Dreyfus HL, Dreyfus SE. Mind Over Machine: The Power of Human Intuition and Expertise in the era of the Computer. New York, NY: Free Press (1986).
59. Perle JG. Introduction to telehealth for clinical psychologists: a novel course designed to improve general knowledge and hands-on expertise with technology-based modalities. J Technol Beh Sci. (2020) 5:383–94. doi: 10.1007/s41347-020-00147-6
60. Moit H, Dwyer A, De Sutter M, Heinzel S, Crawford D. A standardized robotic training curriculum in a general surgery program. J Soc Laparoendosc Surg. (2019) 23(4):e2019–00045. doi: 10.4293/JSLS.2019.00045
61. Greenberg AL, Syed SM, Alseidi A, O'Sullivan PS, Chern H. Robotic training for medical students: feasibility of a pilot simulation curriculum. J Robot Surg. (2023) 17:1029–38. doi: 10.1007/s11701-022-01508-4
62. American Psychological Association. Commission on Accreditation implementing regulation: Section c: IRs related to the standards of accreditation (n.d.). Available at: https://irp.cdn-website.com/a14f9462/files/uploaded/apa-ir-section-c-082224.pdf (Accessed March 07, 2025).
63. Accreditation Council for Graduate Medical Education. Common program requirements (2025). Available at: https://www.acgme.org/programs-and-institutions/programs/common-program-requirements/ (Accessed March 07, 2025).
64. Accreditation Council for Graduate Medical Education. Specialty-specific program requirements: Direct supervision using telecommunication technology (2023). Available at: https://www.acgme.org/globalassets/pdfs/specialty-specific-requirement-topics/dio-direct_supervision_telecommunication.pdf (Accessed March 07, 2025).
Keywords: telehealth, telemedicine, technology, competency, training, education
Citation: Perle JG, Chandran DN, Brezler E, Coleman M, Deziel J, Nahhas P, McDonald G and Jent JF (2025) Technology-enhanced practice competencies: scoping review and novel model development. Front. Digit. Health 7:1571518. doi: 10.3389/fdgth.2025.1571518
Received: 5 February 2025; Accepted: 9 April 2025;
Published: 25 April 2025.
Edited by:
Asmaa Abdelnasser, Ibn Sina National College for Medical Studies, Saudi ArabiaReviewed by:
Nagwa Nashat Hegazy, University of Menoufia, EgyptErini Efat, Faculty of Medicine Suez Canal University, Egypt
Copyright: © 2025 Perle, Chandran, Brezler, Coleman, Deziel, Nahhas, McDonald and Jent. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jonathan G. Perle, am9uYXRoYW4ucGVybGVAaHNjLnd2dS5lZHU=