 Felicien Izaturwanaho1*†
Felicien Izaturwanaho1*† Marie E. Ward1,2,†Clíona Ní Cheallaigh3,4,†Maeve Moran1,†Geraldine Fitzgerald5,†
Marie E. Ward1,2,†Clíona Ní Cheallaigh3,4,†Maeve Moran1,†Geraldine Fitzgerald5,† David Mockler5,†Una Geary2,†Siobhán Corrigan1,†
David Mockler5,†Una Geary2,†Siobhán Corrigan1,†
- 1Centre for Innovative Human Systems, School of Psychology, Trinity College Dublin, Dublin, Ireland
- 2Quality and Safety Improvement Directorate, St James’s Hospital, Dublin, Ireland
- 3Inclusion Health Service, St James’s Hospital, Dublin, Ireland
- 4Department of Clinical Medicine, School of Medicine, Trinity College Dublin, Dublin, Ireland
- 5The Library of Trinity Dublin College, Trinity College Dublin, Dublin, Ireland
Background: Research into mobile health record apps has focused on narrow outcomes, such as medication adherence for persons experiencing chronic conditions. However, no review has examined their use in the context of social exclusion. Persons experiencing social exclusion (PESE) face complex health needs, limited healthcare access, and increased exposure to traumatic life experiences. It is imperative to consider a trauma-informed and integrated care approaches when developing an app for them, and they should be involved as key stakeholders to ensure equitable care. This review examined these apps’ functionalities and features that support PESE in relation to their reported outcomes and the delivery of a trauma-informed and/or integrated care.
Methods: A systematic search of ten databases: Web of Science Core Collection, Medline, PsycINFO, CINAHL, Cochrane, Embase, Scopus, ProQuest Dissertations and Theses A&I, Lenus and OpenGrey International were undertaken, and was supplemented with non-indexed and grey literature. Searches were undertaken in April 2024 in English with no date limit, and used the PRISMA 2020 guidelines. Studies were deemed eligible if they met the SPIDER framework criteria.
Results: One thousand three hundred and thirty-two papers were found eligible for the review, of which eleven qualified for inclusion following screening and quality assessment using QATSDD and MMAT tools. Four themes were found (supporting integrated and connected care; enhancement of user engagement and care coordination; improving data accuracy and access to care; and provision of ongoing monitoring and feedback) related to apps’ functionalities and features, which in turn were linked to reported outcomes. Although a few of these apps’ functionalities and features were aligned with the six principles of trauma-informed care, none of them were implemented considering a trauma-informed care and/or integrated care.
Conclusion: This review provided insights into the complexities of implementing a mobile health record app for PESE. However, limited available data restricted a comprehensive understanding of these apps’ functionalities and features in their specific implementation settings in relation to their reported outcomes. Next steps include translating these findings into survey and interview questions to identify end-user requirements for developing an app for PESE from a trauma-informed perspective to promote integrated care.
Systematic review registration: PROSPERO CRD42024535090.
1 Introduction
Social exclusion is defined as a state in which an individual, because of certain characteristics, has markedly reduced access to resources including housing, education, occupation and financial security, and increased exposure to adversity including poverty, homelessness, incarceration, traumatic experiences and stigma (1, 2). Social exclusion is inherently intersectional; individuals frequently experience a combination of overlapping factors that contribute to their marginalisation process, for instance, they may belong to minoritised groups like Black, Traveller, or Roma communities, struggle with severe and enduring mental health or substance use disorders (SUD), and/or face challenges as refugees or as part of the LGBTQI community (3).
Persons experiencing social exclusion (PESE) have much higher rates of ill-health, multimorbidity, early ageing and shorter life expectancy than the general population (4). Difficulty accessing high-quality healthcare is a cardinal feature of social exclusion and is more pronounced in fragmented healthcare systems and where healthcare is privatised (1, 5). PESE frequently experience systemic barriers when trying to access healthcare, which can include social stigma, discrimination, lack of entitlements, and personal barriers, such as self-stigma and a lack of knowledge about available and affordable healthcare options (6–8). This may result in these persons receiving suboptimal medical care.
Trauma-informed care (TIC) is an approach which recognises the impact of traumatic life experiences on individuals and communities and is widely recognised as key to providing equitable care to PESE (9, 10). Central to the philosophy of TIC is acknowledging the effect of historical and current power imbalances and the role this plays in creating health inequities (11). TIC seeks to create safety for PESE by understanding the impact of traumatic life events on health and behaviours (12). Taking a TIC approach focuses on creating safe spaces that minimise potential harm for patients by using the Substance Abuse and Mental Health Services Administration (SAHMSA)'s six TIC principles: safety; trust; collaboration; peer support; empowerment, voice and choice; and awareness of cultural, historical and gender issues (13–15). Any intervention which is developed for PESE should be evaluated against TIC principles to cater to their needs.
A trauma-informed computing framework has been developed to improve technology experiences for PESE (16). The framework enables human-computer interaction (HCI) to embrace TIC to a certain extent, with the aim of minimising harm and reducing the risk of re-traumatisation to enhance user experience, particularly for persons affected by trauma (16, 17). The design of any app's user interface – including both the HCI aspects of task support tools and the information presented to users – is determined by the underlying process design (18). The framework adapts the SAHMSA's six TIC principles to safety, trust, peer support, collaboration, enablement, and intersectionality (16). A trauma-informed perspective to design supports the assessment of functionalities and features by considering how the effects of trauma could be influencing the behaviours of patients and healthcare professionals when using an app (17, 19).
An integrated care approach recognises the complex needs of persons accessing healthcare by addressing both health and social care aspects. The approach aims to address the fragmentation and lack of care coordination often experienced by persons with chronic and complex conditions (20). This approach is vital for effective organisational design and performance (20) and clearly aligns with TIC given that integrated care promotes empowerment of patients and collaboration between services and patients (21), but lacks a universally accepted definition (22). From a patient's perspective, it can be defined as: “I can plan my care with people who work together to understand me and my carer(s), allow me control, and bring together services to achieve the outcomes important to me” (23, 24). The benefits of integrated care include fewer patient appointments, better continuity of care, better coordination of services, more personalised care, reduced cost, improved quality of life and safety (25). This improves healthcare processes in a coordinated manner to promote care continuity.
The International Foundation for Integrated Care indicates that the digital solutions pillar is one of the nine pillars of integrated care (26). Digital solutions, such as electronic health records (EHR), can be considered integral parts that connect various building blocks in healthcare to support integrated care (27). These technologies serve as a unifying mechanism by ensuring a flow of information in the healthcare system (28, 29), but this vital role of these technologies can be compromised if healthcare professionals, for instance, find the EHR to be disorganised or overly complex to use, potentially leading to adverse health outcomes (30). Overall, research has found that regular use of electronic records can lead to better patient care and safety (31), improved organisational efficiency (32, 33), and promote integrated care (27).
Recent years have seen the development of personal health record (PHR) systems (34), such as the My Health Record (MyHR) system (35). In this study, the term PHR refers to “an electronic application through which individuals can access, manage, and share their health information, and that of others for whom they are authorised, in a private, secure, and confidential environment” (36). This comprehensive definition was provided in a personal health working group final report by the Connecting for Health collaborative, a public-private effort led by the Markle Foundation to develop interoperable health information infrastructures (37), and is supported by standards from organisations like the International Organisation for Standardisation (38).
The primary advantage of PHR lies in the patients’ capacity to manage their own health information (39, 40). Nonetheless, numerous obstacles must be addressed to facilitate the widespread adoption of PHR, such as achieving interoperability with EHR systems and addressing privacy and security issues that may arise from their use (41). Even though the term PHR can denote records in various formats, including paper, they are usually implemented electronically and can be accessed through mobile devices (39). For this study, the term “mobile health record app” is used to reflect a mobile and web-based application that can serve as a digital repository for a patient's health data, which can be controlled and managed by a patient or authorised representative (38, 42, 43).
Even with these advances in healthcare, there is still a critical issue: PESE who often have the highest care needs, continue to have the worst access to healthcare services. This disparity illustrates Tudor Hart's Inverse Care Law, which posits that those most in need of healthcare are least likely to receive it (44). The leverage of the ongoing evolution of technological advances such as electronic record-keeping, mobile health record app presents a promising opportunity to address this gap. A mobile health record app, which is a PHR and EHR, has the potential to promote health and social care coordination and planning, to increase patient safety, control and empowerment and to redress power imbalances. However, it is crucial to understand the end-user requirements for such an app from a trauma-informed design approach, which aims to minimise harm and re-traumatisation while improving user experiences, particularly for persons affected by trauma (16, 17, 19). Otherwise, such an app (as well as other elements of technological progress) runs the risk of inadvertently reducing access to healthcare for PESE and/or increasing levels of disempowerment and thereby worsening health inequalities and retraumatising PESE.
Systematic literature reviews (SLRs) on mobile health record apps have been published (34, 35, 39, 45–48), but there has been no review to date to look at the use of such apps in the context of social exclusion, traumatic life experiences and health inequalities. Mobile health record apps are complex interventions whose effectiveness is influenced by the context in which they are used. The aim of this study was to understand which mobile health record apps support PESE. The primary objective of this review was to assess the functionalities and features of mobile health record apps that support PESE in relation to their reported outcomes and the delivery of trauma-informed and/or integrated healthcare. The secondary research objectives included (i) identifying the main users of the apps and describing their recruitment methods, and (ii) assessing the key features of the apps, with particular attention to their multiplatform accessibility and interoperability within healthcare systems.
2 Methods
2.1 Defining the review scope
2.1.1 Protocol and registration
This review adhered to Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 2020 guidelines (49). The protocol has been registered with PROSPERO under registration number CRD42024535090.
2.1.2 Eligibility criteria
The research team members (CNC, MEW and FI) outlined the inclusion and exclusion criteria as per the Sample, Phenomenon of Interest, Design, Evaluation, Research type (SPIDER) framework (50). The SPIDER question framework is highly effective for qualitative or mixed methods research topics focused on samples rather than populations (50). Only intervention-based studies were included so therefore survey-based studies were excluded. Studies were deemed eligible if they met the SPIDER framework criteria as outlined in Table 1. Papers were screened for eligibility for inclusion by the three co-authors, of whom two, CNC and MEW, are senior academics with experience in conducting SLRs, to define the eligibility criteria. There were no restrictions on geography or publication year if the study was in English for practical reasons.
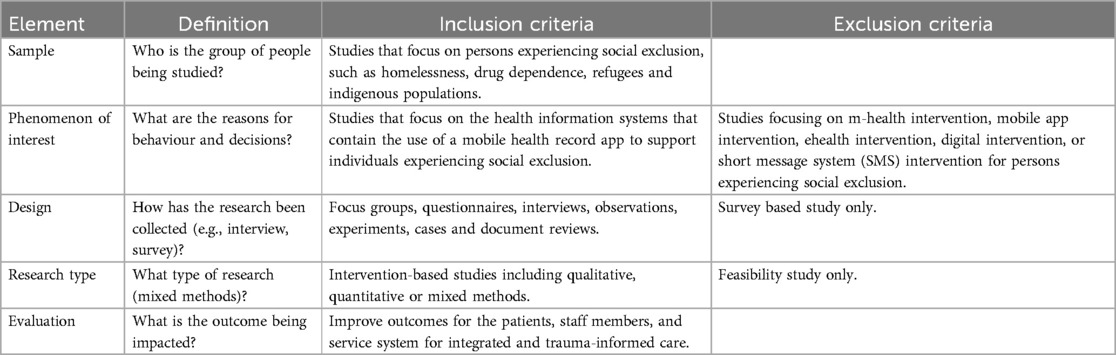
Table 1. Eligibility criteria.
2.2 Search strategy
A systematic electronic search of the English-language literature, with no date limits, was conducted across ten electronic bibliographic databases recognised for their relevance to technology and health research between April 1 and April 29, 2024. Seven bibliographic databases; Embase.com (date of inception 1971), Medline ALL via Ovid (1946 to Daily Update), Web of Science Core Collection, SCOPUS, CENTRAL trial registry and PsycINFO/CINAHL via EBSCOhost, along with three grey literature databases; ProQuest Dissertations and Theses A&I, Lenus, and OpenGrey International, were searched. Search terms were developed based on the research question to identify mobile health record apps supporting socially excluded individuals. The search contained terms for (1) socially excluded people, (2) mobile applications, and (3) electronic health records. Terms were combined with the Boolean operators (AND, OR) and proximity operators to form search phrases. The process was conducted with the support from a subject matter librarian and a co-author (GF). The searches were refined by using relevant thesaurus terms from Emtree for Embase and Medical Subject Headings (MeSH) for Medline, with additional support from another subject matter librarian and co-author (DM). These searches were then adapted to other bibliographic databases. Detailed search strategies for Medline, Embase, and other bibliographic databases are provided in Supplementary File S1, with a sample search strategy for Web of Science Core Collection shown in Table 2. Additional publications were also identified through manual search and consultation with two senior international academics in the field to capture non-indexed and grey literature.
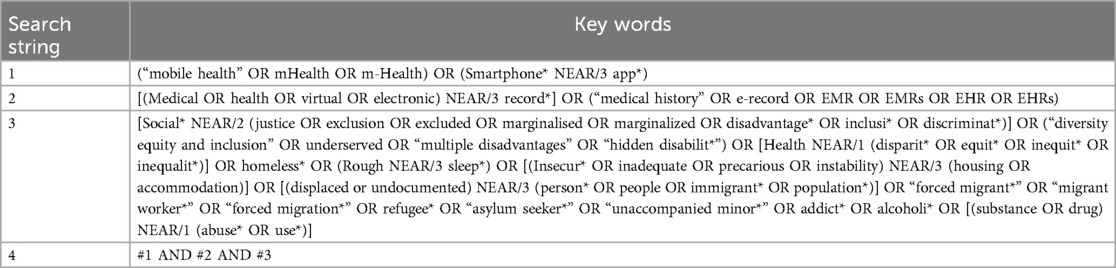
Table 2. A sample of search strategy and combination of keywords for Web of Science Core Collection.
2.3 Choosing and appraising the evidence
2.3.1 Choosing the evidence
All papers were imported into Covidence software to support the screening process (51). Papers were independently screened by title and abstract for inclusion or exclusion by two members of the research team (MM and FI). All conflicts were resolved without the involvement of a third person. The papers which passed the aforementioned stage were subjected to full-text review once more independently by members of the research team working in pairs (MEW and CNC) and (FI and SC). The authors deliberated on each paper's eligibility criteria during both screenings and resolved any conflicts without the involvement of a third person.
2.3.2 Appraising the evidence
The selected tool for quality appraisal was the Quality Assessment Tool for Studies with Diverse Designs (QATSDD) (52). The QATSDD is a 16-item quality assessment tool that was created to assess research that integrates various study designs and has been used for the appraisal of mixed-methods studies only [e.g., (53)]. The tool contains 16 criteria questions that are scored on a Likert scale ranging from 0 to 3, with a score range of 0 to 48. The QATSDD appraisal tool was complemented by the Mixed Methods Appraisal Tool (MMAT) in order to facilitate the evaluation of studies that incorporate mixed studies (qualitative, quantitative, and mixed methods studies) (54, 55). The MMAT enables the concurrent evaluation and description of the methodological quality of three methodological domains: mixed, qualitative, and quantitative (also subdivided into three subdomains: randomised controlled, non-randomised, and descriptive) (54, 55).
2.4 Extracting and synthesising data
The process used for data extraction was important in terms of its completeness, and the research team reviewed data extraction to make sure it was appropriate. The extraction table was developed by the primary author (FI) and was improved after discussion with a senior author (MEW). Specific information about each mobile health record app was gathered, including details about the app's main features, interoperability, multiplatform capabilities and the setting in which it was implemented. Furthermore, contextual information regarding user types and recruitment processes were collected to understand factors that facilitated or hindered implementation and their resultant outcomes. This supported the data analysis, which resulted in four themes that provided a clearer representation of functionalities and features that contributed to the observed results across the studies.
3 Results
3.1 Evidence selected and quality assessment
One thousand three hundred and thirty-two papers were found eligible for the SLR, of which eleven qualified for inclusion following quality assessment and screening. Please see the PRISMA Flow Diagram (Figure 1) for more details. The range of scores for the studies from the QATSDD was between 24 and 38 with a mean score of 28, which is in a good quality range (52). This indicates that studies with this mean score are at a relatively low risk of bias (52). The papers were evaluated by the primary author, and the list of papers with their evaluation scores is available in Supplementary File S2. MMAT appraisal tool was used to supplement QATSDD tool in terms of appraising methodologies of included studies. The calculation of an overall score from the ratings of each criterion is not recommended (54). Instead, it is recommended that a more comprehensive presentation of the ratings of each criterion be provided to enhance the quality of the studies included (54). The ratings for MMAT can be found in Supplementary File S3.
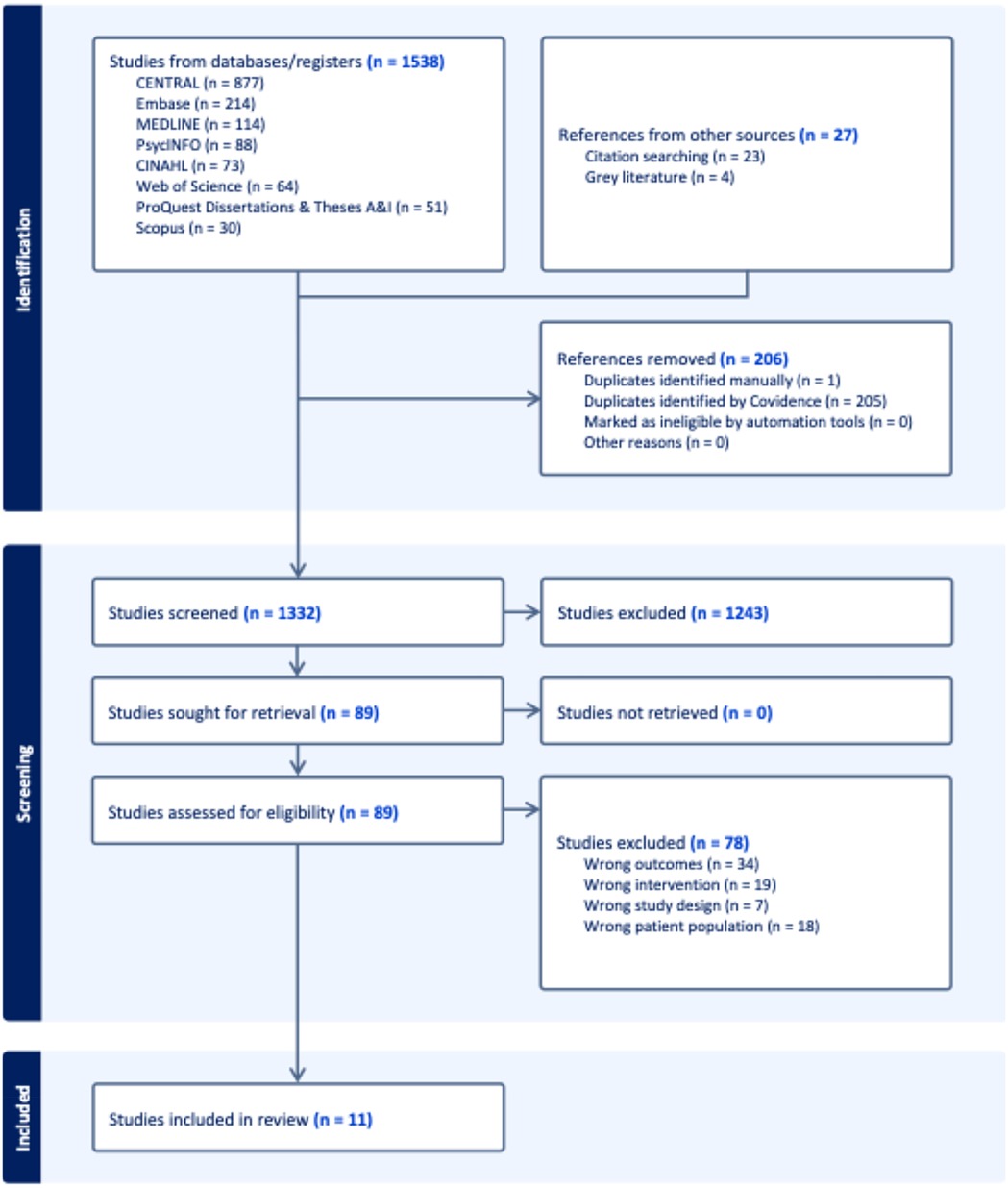
Figure 1. PRISMA flow diagram.
3.2 Key study characteristics
Table 3 depicts key characteristics of included studies. This review included studies conducted in Bangladesh (N = 1) (56), the United States of America (N = 4) (57–60), Pakistan and Afghanistan (N = 1) (61), Kenya (N = 1) (62), Italy (N = 1) (63), China (N = 1) (64), Lebanon and Jordan (N = 1) (65), and Canada (N = 1) (66). Most studies were conducted in a primary healthcare setting (N = 7) (56–61, 66), followed by humanitarian setting (N = 3) (62, 63, 65), and community-based setting (N = 1) (64).
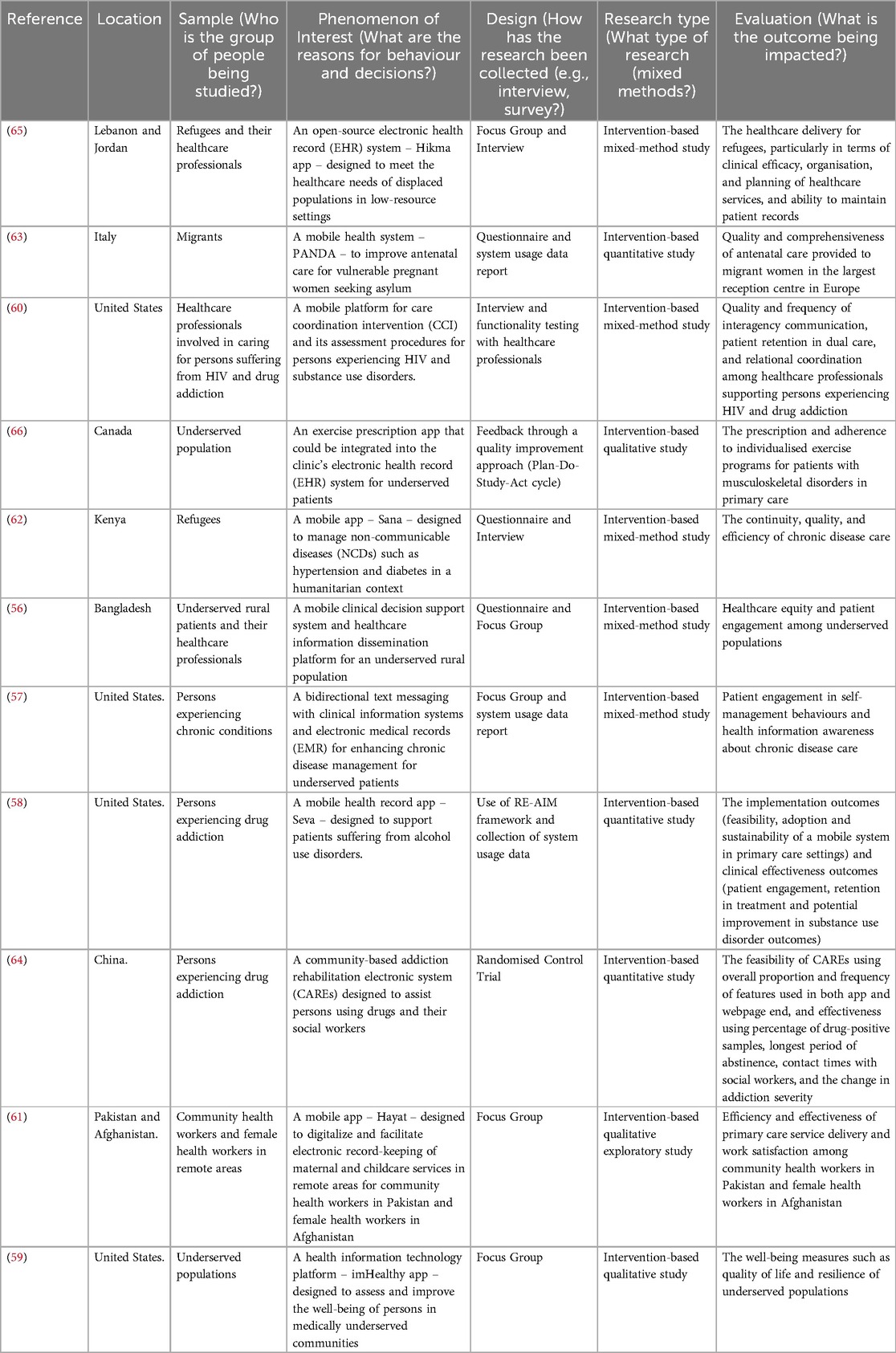
Table 3. Key study characteristics.
None of the eleven studies pertaining to the implementation of the mobile health record apps focused on persons experiencing homelessness or indigenous populations. The map of evidence is shown below as Figure 2 to demonstrate where there are gaps and evidence clusters. A large number of studies focused on developing mobile health records infrastructure for digitalising health records of PESE in their respective healthcare settings (56, 59, 65) and drug dependence (58, 60, 64). A few numbers of studies focused on maternal and childcare services (61, 63), chronic disease like diabetes (57, 62), and musculoskeletal conditions in the context of social exclusion (66).
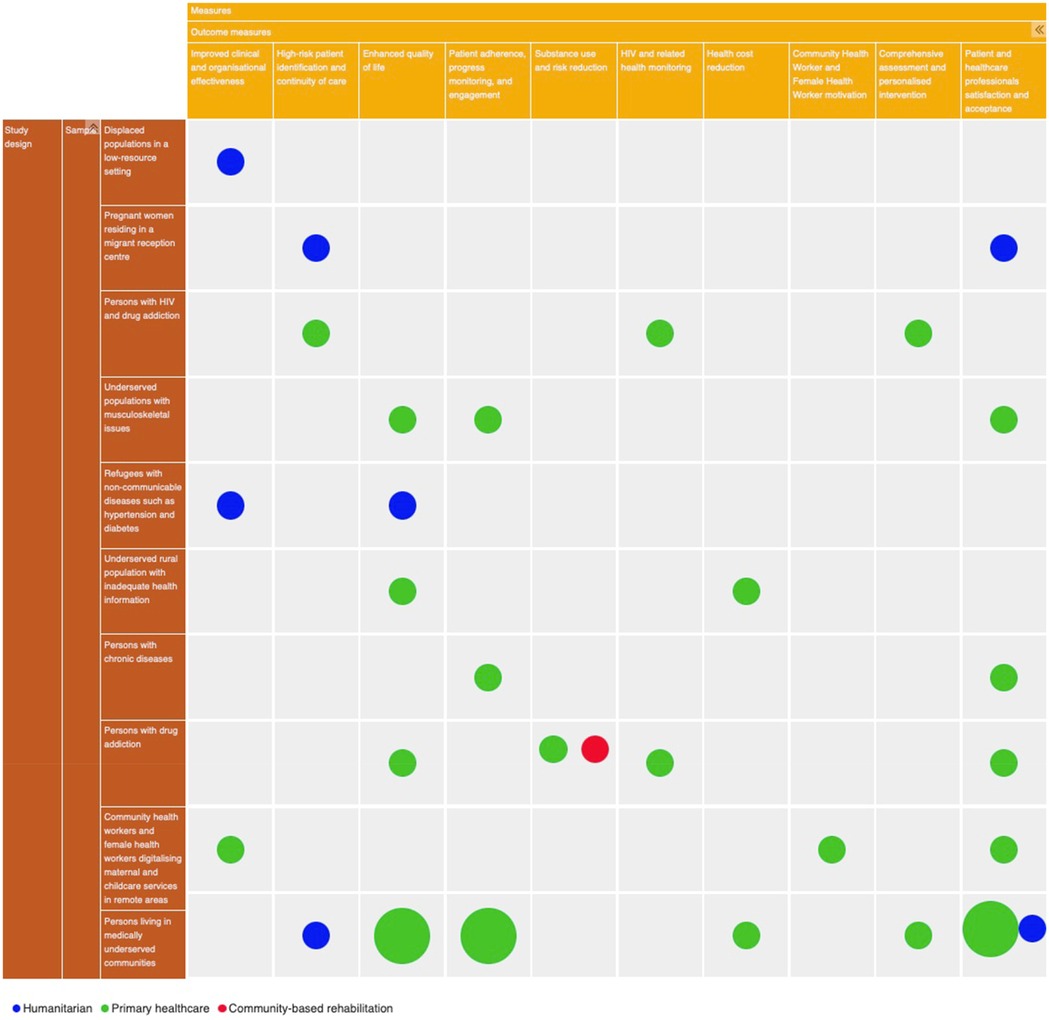
Figure 2. Evidence map.
3.3 Primary research question
The primary objective of this review was to assess the functionalities and features of mobile health record apps that support PESE in relation to their reported outcomes and the delivery of trauma-informed and/or integrated healthcare. A thematic map depicted in Figure 3 indicates four themes that emerged from the literature review, including:
(i) Theme 1 Enhancement of user engagement and coordination of care; includes functionalities and features, such as provision of tools for instantaneous health data generation, appointment reminders, multilingual support with real-time translation into the user's preferred language and offline functionality, that would improve continuity of care and access across healthcare services and systems, particularly in supporting PESE.
(ii) Theme 2 Supporting integrated and connected care; involves functionalities and features, such as the capability of synchronising with existing health information technology systems, combined with secure documentation and standardised access to patient records, that would enable healthcare professionals to leverage longitudinal patient data for decision-making, to address the issue of healthcare services fragmentation often caused by siloed systems.
(iii) Theme 3 Emproving data accuracy and access to care; includes functionalities and features, such as the customisation of app features to align with patients’ specific needs and supporting patients with recording their questions and the responses of healthcare professionals, that would improve health information quality and access to personalised care.
(iv) Theme 4 Provision of ongoing monitoring and feedback; involves functionalities and features, such as being accessible to healthcare professionals on both smartphones and desktop web browsers in relation to wireless transmission of health records securely and provision of real time feedback and support, that enhance standard of care and monitoring of patients.
![Diagram with a central oval labelled \“Themes\” connected to four rectangles. Top left: \“Enhance user engagement and coordination of care [65, 60, 57, 58, 61, 64].\” Top right: \“Provide ongoing monitoring and feedback [63, 64].\” Bottom left: \“Support integrated and connected care [66, 57, 62, 59, 63].\” Bottom right: \“Improve data accuracy and access to care [63, 56, 61].\” Each rectangle is connected to the central oval with arrows.](https://www.frontiersin.org/files/Articles/1629289/fdgth-07-1629289-HTML-r1/image_m/fdgth-07-1629289-g003.jpg)
Figure 3. Themes from the synthesis of included studies.
The most commonly cited theme across the studies was the enhancement of user engagement and coordination of care, which was mentioned in six studies (57, 58, 60, 61, 64, 65). This was followed by supporting integrated and connected care, which appeared in five studies (57, 59, 62, 63, 66). Improving data accuracy and access to care was the next most frequently cited theme, which was mentioned in three studies (56, 61, 63). Lastly, the provision of ongoing monitoring and feedback was the least cited theme, which appeared in two studies (63, 64). These findings are presented in Table 4 which facilitated clearer representation of the complex interplay of functionalities and features of mobile health record app that contribute to the resultant outcomes across eleven studies in their respective implementation healthcare settings.
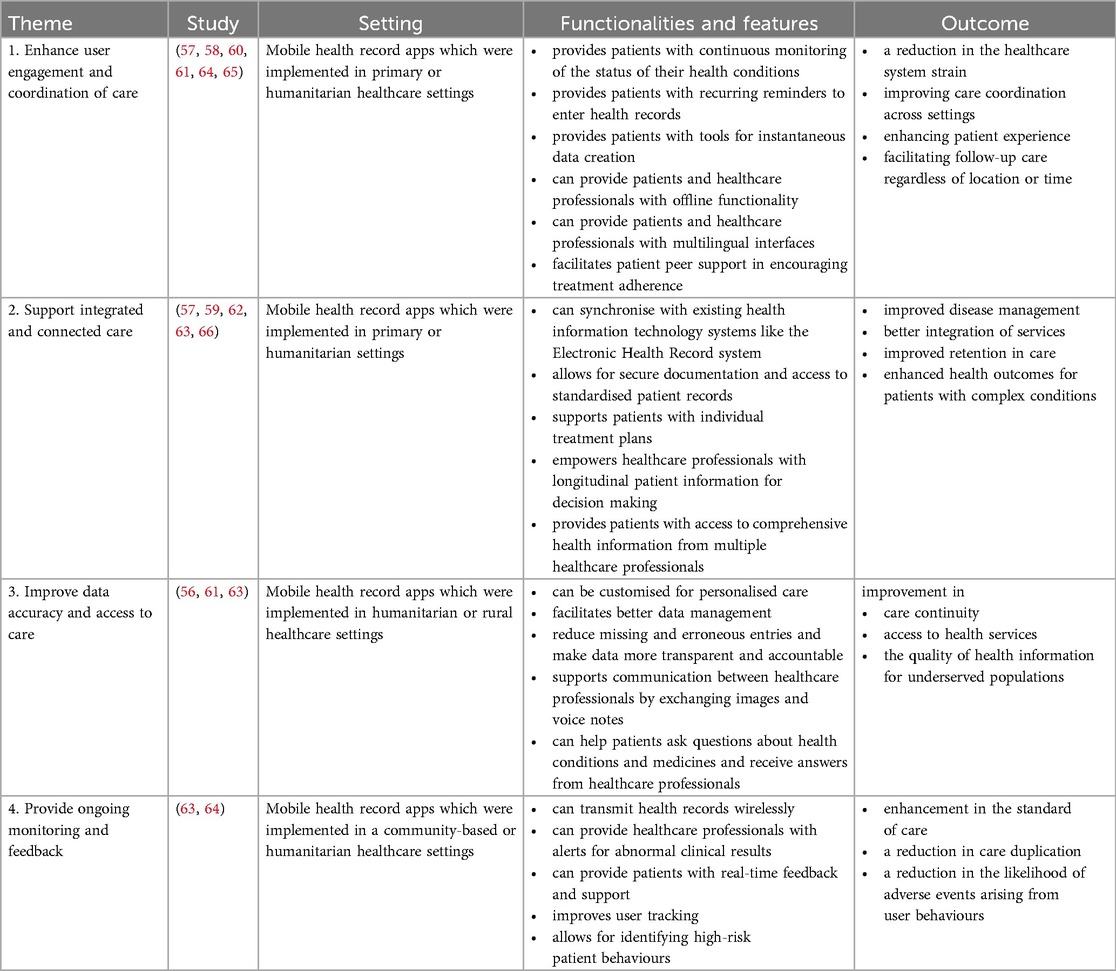
Table 4. Functionalities and features of Mobile health record apps that support PESE in relation to their reported outcomes.
None of the eleven papers pertaining to the implementation of a mobile health record app within healthcare settings considered their use from a TIC perspective or focused specifically on the impact of the mobile health record app on integration of care. One study noted that the app implementation team worked in an integrated care model (66). The apps' functionalities and features were mapped out against six principles of the trauma-informed computing framework, as illustrated in Table 5. While a few functionalities and features corresponded to each of the six principles of the framework, there were no examples related to the Safety and Trust principles – apart from allowing users to access secure documentation and standardised patient records. This feature is consistent with one Safety principle aspect, which emphasises the importance of safeguarding users from digital hazards, including malicious software and unauthorised access (16). There was no element that was consistent with the other aspect of the Safety principle, psychological safety, in relation to the usage or navigation of these apps (16). In addition, there was no feature and functionality that falls into the Trust principle. Safety and Trust principles are closely connected; trustworthy computing requires that technology, processes, and organisations function transparently, predictably, and reliably, while also enabling users to learn from errors and make corrections as needed (16, 67).

Table 5. A mapping of functionalities and features against six trauma-informed computing principles.
3.4 Secondary research questions
The secondary research objectives included (i) identifying the main users of the apps and describing their recruitment methods, and (ii) assessing the key features of the apps, with particular attention to their multiplatform accessibility and interoperability within healthcare systems. These questions will now be addressed.
3.4.1 Mobile health record app main users and their recruitment process
Table 6 below presents the types of users involved in the eleven studies and their recruitment methods. In most studies, there were two types of users for the mobile health record app: PESE served as the primary users in the majority of cases (56–58, 64), and healthcare professionals as secondary users (56–59, 63). Fewer studies have reversed these roles, with healthcare professionals (including community health workers and female health workers) as primary users (60–63, 65, 66), and PESE as secondary users (66). Additionally, a smaller number of studies included social workers as either primary (59) or secondary users (64).
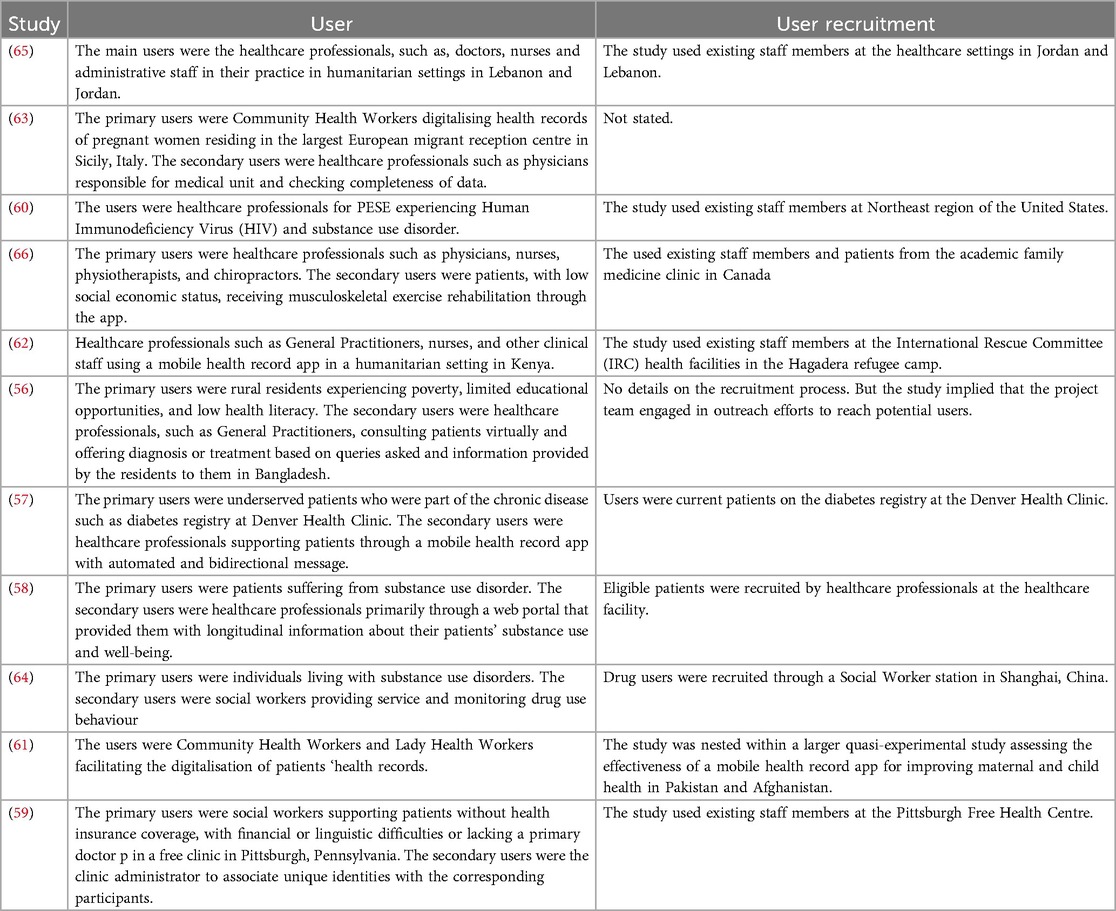
Table 6. App main users and their recruitment methods.
Most studies used existing channels within their respective healthcare settings to recruit staff members and patients to participate in the studies (57–62, 64–66), while a few studies did not specify their recruitment methods (56, 63).
3.4.2 Mobile health record app multiplatform accessibility and interoperability within healthcare systems
Table 7 illustrates the interoperability and multi-platform accessibility of mobile health record apps. Most studies indicated that the apps supported integration with existing health information technology systems (56, 60, 61, 66, 68); though fewer were integrated with existing systems in their respective implementation context (59, 62), while one had a wireless transmission functionality (63). A limited number of studies have not addressed this feature (64, 65), and one study explicitly stated that the app lacked integration capability (58). Regarding platform accessibility, most studies did not specify iOS and Android compatibility (56–62, 64, 65). While a significant number described the apps as mobile device-compatible (56, 58, 62, 64, 65), fewer specified web-based and mobile app functionality (57, 61), and others mentioned tablet compatibility (59, 60). One study noted that the app worked on Android smartphones and was available in English and French (63).
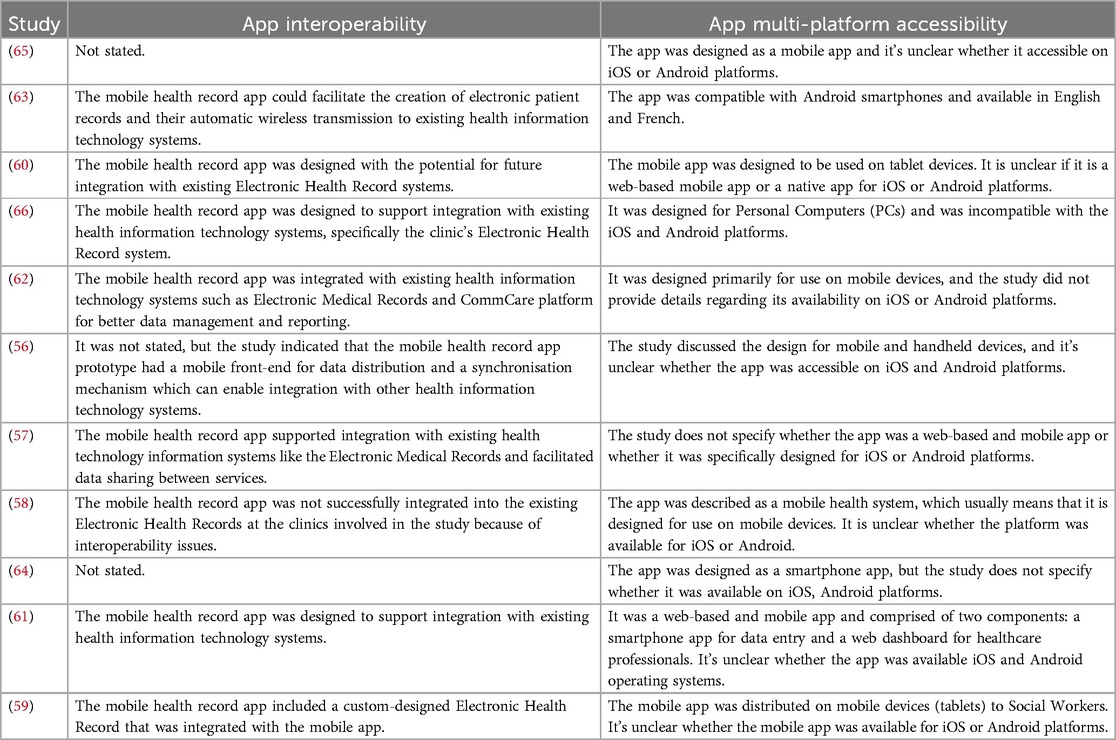
Table 7. App multiplatform accessibility and interoperability within healthcare systems.
4 Discussion
This SLR is the first to specifically focus on identifying the functionalities and features of mobile health record apps implemented in healthcare settings supporting PESE to promote integrated, trauma-informed care. The SLR facilitated an understanding of the use of these apps in various healthcare settings through a systematic and transparent review of the relevant literature. None of the eleven studies on the implementation of mobile health record apps considered their alignment with the principles of TIC. The study contributes to the existing literature because no previous study has focused on which mobile health record apps support the PESE until now.
This study builds upon previous SLRs of mobile health record apps (34, 35, 39, 45–48). Four key themes: health information fragmentation, health information quality and access, adverse medical events and duplication of care, and care coordination, were identified in the SLR conducted on the use of PHR in the general Australian population (35). Their findings revealed mixed outcomes regarding the success of PHR implementation in Australia. For instance, the study indicated that the PHR system has the potential to decrease fragmentation of health information; however, challenges related to workforce adoption were recognised as an issue (35). In our study, we also found four themes, with enhancement of user engagement and coordination of care as the most cited theme. This is important as mobile health record apps can be designed and implemented to enable integrated care across different healthcare settings that are involved in caring for the persons irrespective of geographical location and time.
Contradictory results in relation to supporting coordination of care were found (35). However, our study found that (as per Theme 1), a mobile health record app can enhance engagement of users; either patients or healthcare professionals, and improve the overall coordination of care, especially for PESE who may experience challenges in accessing and using healthcare services in primary, humanitarian, or community-based healthcare settings. For instance, our study findings indicated that such an app would empower patients by providing tools for instantaneous health data generation, appointment reminders, multilingual support with real-time translation into the user's preferred language, and offline functionality to enhance care continuity access across healthcare services and systems, particularly in supporting PESE (58, 60, 61, 64, 65). The offline functionality means that users may use it without needing constant internet connectivity, which may be particularly important in humanitarian settings or for patients who lack access to the internet (61, 65). The functionality for creating data, for example, would enable patients to create summary care records and scan of documents that may be needed for different services e.g., identity details, and proof of payment and address, which could enhance communication and coordination across healthcare settings. The SLR on PHR taxonomy and their challenges compliments this by indicating that photos and scanned documents are the data types that are included in the PHR system (39), and would be critical for the continuity of care across time and space for PESE (45). In addition, the multilingual support and instantaneous translation to one's mother tongue feature signifies that the mobile health record app could cater to the needs of PESE, such as refugees, who may have difficulties with the language of the country in which they find themselves (65). This is further support by the SLR on the important design features of PHRs to improve medication adherence for persons experiencing chronic conditions, which highlighted design features in mobile health record apps – such as reminders, medical appointment management, diaries, and self-monitoring – that improve medication adherence for patients with chronic conditions (34).
The study offered insights into the complexities of using a mobile health record app for PESE and could help in understanding the dynamics that could contribute towards success or failure of such apps in healthcare systems. Our findings indicated that a mobile health record app could address healthcare fragmentation across different health settings for PESE (as per Theme 2). These study findings are supported by results of the SLR on PHR in the general Australian population, which, despite highlighting challenges in adoption by both patients and healthcare professionals, stressed its potential benefits (35) and are complemented by the findings of the SLR on PHR, which demonstrated that participants attributed a high level of value to this technology in relation to the co-location, viewing, updating, and sharing of health information with clinicians (69). Our findings suggested that, for example, implementing a mobile health record app capable of synchronising with existing health information technology systems, combined with secure documentation and standardised access to patient records, would enable healthcare professionals to leverage longitudinal patient data for decision-making, to address the issue of healthcare services fragmentation often caused by siloed systems (59, 60, 62, 63). The synchronisation capability, which would enable health data sharing across multiple health information technology systems, could address the interoperability challenge (39), that hindered the effective implementation of mobile health record apps in their respective clinical settings, e.g., (58). In a study on practical and ethical issues for patients and physicians using PHR, the results suggested that a PHR that can efficiently integrate information from multiple sources may save time and healthcare costs by providing a useful summary, but physicians may not be able to use the data if it contains data that were generated by a patient, which can be susceptible to incomplete, inaccurate, and outdated information (43). A functionality for standardising patient record with clear representation of user-entered information and an intuitive display for healthcare professionals would be an important step towards care quality and continuity (57). Furthermore, a functionality for empowering healthcare professionals with longitudinal health records (e.g., blood pressure measurements) would strengthen decision-making in chronic disease management (58, 62). This is illustrated in the SLR, which assesses the functionality and utility of PHR in the clinical context of record-keeping health information, such as medical history, medications, laboratory tests, and vaccinations (46).
This SLR highlighted that a mobile health record app could improve data accuracy and access to care (as per Theme 3). The results of the SLR on the use of PHR in the general Australian population supports this finding by reporting improvements in health information access, despite issues related to data reliability and completeness (35). Our study findings demonstrated that, for instance, the customisation of app features to align with patients' specific needs and a functionality to support patients with recording their questions and the responses of healthcare professionals would improve health information quality and access to personalised care (56, 61, 63). The customisation feature would mean that, for example, there could be a “read-only” access option in the app for essential documents such as prescriptions and vaccination records. This opportunity for customisation would be possible due to the interactive interface of the mobile health record app (48). Recording patient questions and responses from healthcare professionals would address shared decision-making (SDM) in managing for PESE's health conditions (56). Recording a patient's questions was reported as one of the features of a mobile health record app in the SLR on the attributes of PHR for patients with multiple sclerosis (47). This would help with health information management and facilitate administrative reporting. It would also facilitate SDM and improve overall condition management. SDM involves the healthcare professional and the person working collaboratively to make informed decisions about the person's care (70, 71).
The study found that, despite previous limited research support, the mobile health record app could still play a significant role in supporting ongoing monitoring and feedback, as outlined in Theme 4. The findings of this study demonstrated that, for example, wireless health records transmission and integrated alert functionalities for abnormal clinical results have enabled healthcare professionals in reducing the likelihood of patient safety events in a community-based and humanitarian setting (63, 64). An app that could be accessible to healthcare professionals on both smartphones and desktop web browsers in relation to wireless transmission of health records securely would be another beneficial feature in relation to ongoing monitoring of patients. This is corroborated by the findings of a study on the types and sources of diagnostic errors in primary care settings, which demonstrated that accessing patients' health records helped healthcare professionals like General Practitioners (GPs) make better decisions and prevent patient safety events like drug interactions (31). An integrated alert function for patients, such as PESE, to contact healthcare professionals for support would be a key feature for the app. This is reflected in the SLR on the important design features of PHRs to improve medication adherence for persons facing chronic conditions, which identified specific design features in mobile health record apps like feedback and alerts and health condition management in mobile health records which contribute to improved medication adherence among patients with chronic illnesses (34).
This study does have some limitations. There was a lack of detailed information in the literature regarding the implementation of mobile health record apps for PESE in their respective healthcare settings. Only eleven papers met the criteria for final synthesis, despite an initial high number of potential studies (one thousand three hundred and thirty-two) identified through database searches and grey literature. This is partially because the field for designing mobile health record app from a TIC perspective to promote integrated care is relatively new (16, 17, 19). There are limitations inherent in the included studies. These selected studies often lacked important information: eight didn't specify the project team's expertise and composition (56, 58, 61–65), four omitted a guiding theoretical framework (57, 59, 62, 64), one was unclear about user recruitment methods (63), two didn't provide details about app interoperability (64, 65), and nine were unclear about multi-platform accessibility (iOS and/or Android compatibility) (56–61, 64, 65). These information gaps limited the available data for synthesis and impacted a comprehensive understanding of functionalities and features of these mobile health record apps in relation to their reported outcomes in their respective implementation contexts. This, in turn, had an impact on the study's capacity to draw conclusions and provide insights into the usage of mobile health record apps that support PESE.
As with most research, the included studies had certain methodological limitations. Two lacked standardised outcome measures (65, 66), one had limited outcome measures (63), one had unclear evaluation criteria and outcome measures (56), and one lacked quantitative outcomes (57), three studies had a potential bias due to its reliance on self-reported data (60, 63, 65), five had a potential selection bias (56–58, 61, 64), and one had a non-random recruitment (66). Furthermore, six studies had a small, or unrepresentative samples which can limit the generalisability of their findings (57, 58, 60, 62–64), one had data collection issues such as gaps in pharmacy data requiring ongoing manual data review (57) or non-verbatim transcription of native language discussions (61), one study described a mobile health record intervention that is currently in the research protocol development stage (60), and four studies were unclear about ethical considerations with inadequate consent and confidentiality information (56, 57, 59, 65). Despite the methodological limitations of the included studies, conducting this review remains essential for providing a comprehensive understanding of the topic.
This review has limitations in relation to its scope and methodology. For instance, the search was restricted to the English language for practical reasons, which may have resulted in the exclusion of pertinent studies published in other languages. Furthermore, as research on mobile health record app is rapidly evolving, it is possible that some recent publications were not captured in our review. Lastly, this study emphasised the most significant findings from the literature about the functionalities and features of mobile health record apps that support PESE for promoting trauma-informed and integrated care. Nevertheless, it is impossible to address all of the aspects we found in relation to the implementation of mobile health record apps in healthcare settings to promote trauma-informed and integrated care in a limited space. Acknowledging these limitations allows for a more nuanced interpretation of the findings while still contributing valuable insights to the existing body of knowledge (69).
The strength of this study lies in its ability to examine the functionalities and features of mobile health record apps that support PESE in their implementation context and resultant outcomes. The majority of research on mobile health record apps does not specifically look at their use by PESE or social workers working with PESE. Furthermore, research into mobile health record apps has focused on narrow outcomes like medication adherence for persons experiencing chronic conditions, rather than more complex outcomes, such as integration of care or implementation of the principles of trauma-informed care. This study contributes to the existing body of literature by illustrating the characteristics of the limited number of studies that have examined the implementation of mobile health record apps in their respective healthcare settings for PESE.
Conclusion
The primary objective of this review was to evaluate the functionalities and features of mobile health record apps that support PESE in relation to their reported outcomes and the delivery of trauma-informed and/or integrated healthcare. Secondary objectives included: (i) identifying the primary users of these apps and describing their recruitment methods, and (ii) assessing key app features, with particular focus on multiplatform accessibility and interoperability within healthcare systems. Although there is growing evidence on this topic, more research is needed, especially concerning persons experiencing homelessness and indigenous populations. Four key themes emerged from the literature: (i) support for integrated and connected care; (ii) enhancement of user engagement and care coordination; (iii) improvement of data accuracy and access to care; and (iv) provision of ongoing monitoring and feedback. Importantly, none of the studies reviewed were implemented within their respective health settings using a trauma-informed approach to promote integrated care. Additionally, few app functionalities aligned with the six principles of the trauma-informed computing framework. It is essential to recognise that these mobile health record apps do not function as isolated interventions; rather, their effectiveness depends on the specific healthcare contexts and conditions in which they are used. PESE were typically the primary users of these apps, while healthcare professionals – including social workers and community health workers – acted as secondary users, or vice versa. Most of the studies used existing channels to recruit the participants and a few studies were unclear about it. Only a few mobile health record apps demonstrated integration with existing health information technologies, and most studies did not clearly specify whether the apps were compatible with iOS or Android platforms. The next step in this research is to use these findings to inform the design of a survey instrument and interview questions for key stakeholders. This will help formulate a comprehensive set of end-user requirements for developing a mobile health record app to be implemented in the hospital from a trauma-informed manner to promote integrated care. This process of firstly developing an understanding of functionalities and features of these apps in their respective implementation contexts supports the creation of a rich bank of questions that will add to the development of a set of end-user requirements. That will help identify practical and effective strategies for PESE in accessing healthcare in the future.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
FI: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Visualization, Writing – original draft. MW: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing. CNC: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing. MM: Formal analysis, Validation, Writing – review & editing. GF: Data curation, Software, Validation, Writing – review & editing. DM: Data curation, Software, Validation, Writing – review & editing. UG: Validation, Writing – review & editing. SC: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This publication has emanated from research conducted with the financial support of Taighde Éireann –Research Ireland under Grant number 18/CRT/6222.
Acknowledgments
We express our gratitude to the persons with lived experiences who have been contributing to this study, and to the Inclusion Health Service team at St James's Hospital for their support. We also acknowledge the support of the Research Ireland - Centre for Research Training in Advanced Networks for Sustainable Societies (ADVANCECRT).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdgth.2025.1629289/full#supplementary-material
References
1. Aldridge RW, Story A, Hwang SW, Nordentoft M, Luchenski SA, Hartwell G, et al. Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: a systematic review and meta-analysis. Lancet. (2018) 391(10117):241–50. doi: 10.1016/S0140-6736(17)31869-X
2. O'Donnell P, O'Donovan D, Elmusharaf K. Measuring social exclusion in healthcare settings: a scoping review. Int J Equity Health. (2018) 17(1):15. doi: 10.1186/s12939-018-0732-1
3. Vickery J. Using an intersectional approach to advance understanding of homeless persons’ vulnerability to disaster. Environ Sociol. (2017) 4(1):136–47. doi: 10.1080/23251042.2017.1408549
4. Ní Cheallaigh C, Cullivan S, Sears J, Lawlee AM, Browne J, Kieran J, et al. Usage of unscheduled hospital care by homeless individuals in Dublin, Ireland: a cross-sectional study. BMJ Open. (2017) 7(11):e016420. doi: 10.1136/bmjopen-2017-016420
5. Luchenski S, Maguire N, Aldridge RW, Hayward A, Story A, Perri P, et al. What works in inclusion health: overview of effective interventions for marginalised and excluded populations. Lancet. (2018) 391(10117):266–80. doi: 10.1016/S0140-6736(17)31959-1
6. Davila JA, Cabral HJ, Maskay MH, Marcus R, Yuan Y, Chisolm N, et al. Risk factors associated with multi-dimensional stigma among people living with HIV/AIDS who are homeless/unstably housed. AIDS Care. (2018) 30(10):1335–40. doi: 10.1080/09540121.2018.1484069
7. Ponka D, Agbata E, Kendall C, Stergiopoulos V, Mendonca O, Magwood O, et al. The effectiveness of case management interventions for the homeless, vulnerably housed and persons with lived experience: a systematic review. PLoS One. (2020) 15(4):e0230896. doi: 10.1371/journal.pone.0230896
8. Jaeger FN, Pellaud N, Laville B, Klauser P. The migration-related language barrier and professional interpreter use in primary health care in Switzerland. BMC Health Serv Res. (2019) 19(1):429. doi: 10.1186/s12913-019-4164-4
9. Reeves E. A synthesis of the literature on trauma-informed care. Issues Ment Health Nurs. (2015) 36(9):698–709. doi: 10.3109/01612840.2015.1025319
10. Sweeney A, Clement S, Filson B, Kennedy A. Trauma-informed mental healthcare in the UK: what is it and how can we further its development? Mental Health Rev J. (2016) 21(3):174–92. doi: 10.1108/MHRJ-01-2015-0006
11. Kimberg L, Wheeler M. Trauma and Trauma-Informed Care. Trauma-Informed Healthcare Approaches. Cham: Springer (2019). p. 25–56.
12. Raja S, Hasnain M, Hoersch M, Gove-Yin S, Rajagopalan C. Trauma informed care in medicine: current knowledge and future research directions. Fam Community Health. (2015) 38(3):216–26. doi: 10.1097/FCH.0000000000000071
13. Covington SS. Women and addiction: a trauma-informed approach. J Psychoactive Drugs. (2008) Suppl 5:377–85. doi: 10.1080/02791072.2008.10400665
14. Strand V, Popescu M, Abramovitz R, Richards S. Building agency capacity for trauma-informed evidence-based practice and field instruction. J Evid Inf Soc Work. (2016) 13(2):179–97. doi: 10.1080/23761407.2015.1014124
15. Hopper EK, Bassuk EL, Olivet J. Shelter from the storm: trauma-informed care in homelessness services settings. Open Health Serv Policy J. (2010) 3(2):80–100. doi: 10.2174/1874924001003020080
16. Chen XJ, McDonald A, Zou Y, Tseng E, Roundy AK, Tamersoy A, et al. Trauma-Informed computing: towards safer technology experiences for all. In: CHI Conference on Human Factors in Computing Systems; (2022). p. 1–20.
17. Marcu G. Toward trauma-informed design of behavioral interventions: a case study on classroom management. In: Proceedings of the 20th European Conference on Computer-Supported Cooperative Work: The International Venue on Practice-centred Computing on the Design of Cooperation Technologies - Notes, Reports of the European Society for Socially Embedded Technologies. Coimbra: European Society for Socially Embedded Technologies (EUSSET) (2022).
18. Bergström J, Hornbæk K. DIRA: a model of the user interface. Int J Hum Comput Stud. (2025) 193:103381. doi: 10.1016/j.ijhcs.2024.103381
19. Eggleston M, Noel LA. Trauma-informed design: leveraging usability heuristics on a social services website. J User Exp. (2025) 19(3):123–38.
20. Kodner DL. All Together now: A Conceptual Exploration of Integrated Care. Toronto, ON: Healthcare Quarterly (2009). 13 Spec No. p. 6–15.
21. Vallières F, Ward ME, Shields D, Geary U, Gardner C, King D, et al. Co-developing, piloting, and evaluating a translational simulation (TS) delivery model for the promotion of psychological trauma-informed care (TIC) to improve service delivery within acute hospital settings: a research protocol. HRB Open Res. (2023) 6. doi: 10.12688/hrbopenres.13727.1
22. Armitage GD, Suter E, Oelke ND, Adair CE. Health systems integration: state of the evidence. Int J Integr Care. (2009) 9:e82. doi: 10.5334/ijic.316
23. Goodwin N. Understanding integrated care. Int J Integr Care. (2016) 16(4):6. doi: 10.5334/ijic.2530
24. Lewis R, Rosen R, Goodwin N, Ifer Dixon J. Where next for integrated care organisations in the English NHS? (2010).
25. Carrigan A, Roberts N, Clay-Williams R, Hibbert P, Austin E, Pulido DF, et al. What do consumer and providers view as important for integrated care? A qualitative study. BMC Health Serv Res. (2023) 23(1):11. doi: 10.1186/s12913-022-08997-x
26. International Foundation for Integrated Care. The Nine Pillars of Integrated Care (2025). Available online at: https://integratedcarefoundation.org/nine-pillars-of-integrated-care (Accessed April 7, 2025).
27. Ovretveit J. Digital technologies supporting person-centered integrated care - A perspective. Int J Integr Care. (2017) 17(4):6. doi: 10.5334/ijic.3051
28. Tulchinsky TH, Varavikova EA. A history of public health. In: New Public Health. 3rd ed. San Diego: Elsevier, Academic Press (2014). p. 1–42. doi: 10.1016/B978-0-12-415766-8.00001-X
29. Donzé P-Y, Fernández Pérez P. Health industries in the twentieth century. Bus Hist. (2019) 61(3):385–403. doi: 10.1080/00076791.2019.1572116
30. Asthana S, Jones R, Sheaff R. Why does the NHS struggle to adopt eHealth innovations? A review of macro, meso and micro factors. BMC Health Serv Res. (2019) 19(1):984. doi: 10.1186/s12913-019-4790-x
31. Singh H, Giardina TD, Meyer AN, Forjuoh SN, Reis MD, Thomas EJ. Types and origins of diagnostic errors in primary care settings. JAMA Intern Med. (2013) 173(6):418–25. doi: 10.1001/jamainternmed.2013.2777
32. Lee D, Hong KS, Kim NY. Effects of hospital leadership, organizational systems, and ESWOS on medical error reduction. Serv Bus. (2014) 10(1):159–77. doi: 10.1007/s11628-014-0262-x
33. Brady AM, Fortune J, Ali AH, Prizeman G, To WT, Courtney G, et al. Multidisciplinary user experience of a newly implemented electronic patient record in Ireland: an exploratory qualitative study. Int J Med Inform. (2024) 185:105399. doi: 10.1016/j.ijmedinf.2024.105399
34. Andrikopoulou E, Scott P, Herrera H, Good A. What are the important design features of personal health records to improve medication adherence for patients with long-term conditions? A systematic literature review. BMJ Open. (2019) 9(9):e028628. doi: 10.1136/bmjopen-2018-028628
35. Mesquita RCD, Edwards I. Systematic literature review of my health record system. Asia Pac J Health Manag. (2020) 15(1):14–25. doi: 10.24083/apjhm.v15i1.311
36. Tang PC, Ash JS, Bates DW, Overhage JM, Sands DZ. Personal health records: definitions, benefits, and strategies for overcoming barriers to adoption. J Am Med Inform Assoc. (2006) 13(2):121–6. doi: 10.1197/jamia.M2025
38. International organisation for standardisation. Health informatics — personal health records — definition, scope and context. (2012).
39. Roehrs A, da Costa CA, Righi RD, de Oliveira KS. Personal health records: a systematic literature review. J Med Internet Res. (2017) 19(1):e13. doi: 10.2196/jmir.5876
40. Alsahafi YA, Gay V. An overview of electronic personal health records. Health Policy Technol. (2018) 7(4):427–32. doi: 10.1016/j.hlpt.2018.10.004
41. Heath M, Porter TH, Dunegan K. Obstacles to continued use of personal health records. Behav Inf Technol. (2020) 41(3):574–87. doi: 10.1080/0144929X.2020.1829051
42. Baird A, North F, Raghu TS. Personal health records (PHR) and the future of the physician-patient relationship. In: Proceedings of the 2011 IConference (iConference ‘11) Association for Computing Machinery; New York, NY, USA (2011). p. 281–8.
43. Wynia M, Dunn K. Dreams and nightmares: practical and ethical issues for patients and physicians using personal health records. Medicoleg News. (2010) 38(1):64–73. doi: 10.1111/j.1748-720X.2010.00467.x
44. Hart TJ. The inverse care law. Lancet. (1971) 297(7696):405–12. doi: 10.1016/S0140-6736(71)92410-X
45. Archer N, Fevrier-Thomas U, Lokker C, McKibbon KA, Straus SE. Personal health records: a scoping review. J Am Med Inform Assoc. (2011) 18(4):515–22. doi: 10.1136/amiajnl-2011-000105
46. Kim MI, Johnson KB. Personal health records: evaluation of functionality and utility. J Am Med Inform Assoc. (2002) 9(2):171–80. doi: 10.1197/jamia.M0978
47. Aslani N, Ahmadi M, Samadbeik M. A systematic review of the attributes of electronic personal health records for patients with multiple sclerosis. Health Technol (Berl). (2019) 10(3):587–99. doi: 10.1007/s12553-019-00387-4
48. Kharrazi H, Chisholm R, VanNasdale D, Thompson B. Mobile personal health records: an evaluation of features and functionality. Int J Med Inf. (2012) 81(9):579–93. doi: 10.1016/j.ijmedinf.2012.04.007
49. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6(7):e1000097. doi: 10.1371/journal.pmed.1000097
50. Cooke A, Smith D, Booth A. Beyond PICO: the SPIDER tool for qualitative evidence synthesis. Qual Health Res. (2012) 22(10):1435–43. doi: 10.1177/1049732312452938
51. Veritas Health Innovation. Covidence Systematic Review Software. (2024). Available online at: https://www.covidence.org (Accessed April 7, 2025).
52. Sirriyeh R, Lawton R, Gardner P, Armitage G. Reviewing studies with diverse designs: the development and evaluation of a new tool. J Eval Clin Pract. (2012) 18(4):746–52. doi: 10.1111/j.1365-2753.2011.01662.x
53. Kavanagh R, Ward ME. What is known about near miss events in the operating room? A systematic review of studies of mixed methods design. Ir J Med Sci. (2024) 194:297–310. doi: 10.1007/s11845-024-03822-2
54. Quan N, Hong PP, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Mixed Methods Appraisal Tool (MMAT) version 2018 user guide (2018).
55. Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, et al. The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. (2018) 34(4):285–91. doi: 10.3233/EFI-180221
56. Miah SJ, Hasan N, Hasan R, Gammack J. Healthcare support for underserved communities using a mobile social media platform. Inf Syst. (2017) 66:1–12. doi: 10.1016/j.is.2017.01.001
57. Moore SL, Fischer HH, Steele AW, Joshua Durfee M, Ginosar D, Rice-Peterson C, et al. A mobile health infrastructure to support underserved patients with chronic disease. Healthc (Amst). (2014) 2(1):63–8. doi: 10.1016/j.hjdsi.2013.12.016
58. Quanbeck A, Gustafson DH, Marsch LA, Chih MY, Kornfield R, McTavish F, et al. Implementing a Mobile health system to integrate the treatment of addiction into primary care: a hybrid implementation-effectiveness study. J Med Internet Res. (2018) 20(1):e37. doi: 10.2196/jmir.8928
59. Zhou L, Watzlaf V, Abernathy P, Abdelhak M. A health information system for scalable and comprehensive assessment of well-being: a multidisciplinary team solution. Perspect Health Inf Manag. (2017) 14:1d.28855857
60. Claborn K, Becker S, Ramsey S, Rich J, Friedmann PD. Mobile technology intervention to improve care coordination between HIV and substance use treatment providers: development, training, and evaluation protocol. Addict Sci Clin Pract. (2017) 12(1):8. doi: 10.1186/s13722-017-0073-1
61. Zaidi S, Kazi AM, Riaz A, Ali A, Najmi R, Jabeen R, et al. Operability, usefulness, and task-technology fit of an mHealth app for delivering primary health care services by community health workers in underserved areas of Pakistan and Afghanistan: qualitative study. J Med Internet Res. (2020) 22(9):e18414. doi: 10.2196/18414
62. Lyles E, Paik K, Kiogora J, Hussein H, Cordero Morales A, Kiapi L, et al. Adoption of electronic medical records for chronic disease care in Kenyan refugee camps: quantitative and qualitative prospective evaluation. JMIR Mhealth Uhealth. (2023) 11:e43878. doi: 10.2196/43878
63. Borsari L, Stancanelli G, Guarenti L, Grandi T, Leotta S, Barcellini L, et al. An innovative Mobile health system to improve and standardize antenatal care among underserved communities: a feasibility study in an Italian hosting center for asylum seekers. J Immigr Minor Health. (2018) 20(5):1128–36. doi: 10.1007/s10903-017-0669-2
64. Xu X, Chen S, Chen J, Chen Z, Fu L, Song D, et al. Feasibility and preliminary efficacy of a community-based addiction rehabilitation electronic system in substance use disorder: pilot randomized controlled trial. JMIR Mhealth Uhealth. (2021) 9(4):e21087. doi: 10.2196/21087
65. Ashworth H, Ebrahim S, Ebrahim H, Bhaiwala Z, Chilazi M. A free, open-source, offline digital health system for refugee care. JMIR Med Inform. (2022) 10(2):e33848. doi: 10.2196/33848
66. Edgar MC, Lambert C, Abbas A, Young JJ, McIsaac W, Monteiro R, et al. Development of a low resource exercise rehabilitation application for musculoskeletal disorders to help underserved patients in a primary care setting. J Can Chiropr Assoc. (2022) 66(2):130–45.36275080
67. Li H, Gupta A, Zhang J, Sarathy R. Examining the decision to use standalone personal health record systems as a trust-enabled fair social contract. Decis Support Syst. (2014) 57:376–86. doi: 10.1016/j.dss.2012.10.043
68. Delargy I, Crowley D, Van Hout MC. Twenty years of the methadone treatment protocol in Ireland: reflections on the role of general practice. Harm Reduct J. (2019) 16(1):5. doi: 10.1186/s12954-018-0272-4
69. Weitzman ER, Kaci L, Mandl KD. Acceptability of a personally controlled health record in a community-based setting: implications for policy and design. J Med Internet Res. (2009) 11(2):e14. doi: 10.2196/jmir.1187
70. Gurtner C, Schols J, Lohrmann C, Halfens RJG, Hahn S. Conceptual understanding and applicability of shared decision-making in psychiatric care: an integrative review. J Psychiatr Ment Health Nurs. (2021) 28(4):531–48. doi: 10.1111/jpm.12712
71. National Institute for Health and Care Excellence. Shared decision making (2025). Available online at: https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/nice-guidelines/shared-decision-making#:∼:text=Shared%20decision%20making%20is%20a,individual%20preferences%2C%20beliefs%20and%20values (Accessed April 7, 2025).
Keywords: inclusion health, end-user requirements, mobile health record app, integrated care, homelessness, opiate substitution therapy, personal health record, trauma-informed care
Citation: Izaturwanaho F, Ward ME, Ní Cheallaigh C, Moran M, Fitzgerald G, Mockler D, Geary U and Corrigan S (2025) What are the functionalities and features of mobile health record apps supporting persons experiencing social exclusion? A systematic literature review. Front. Digit. Health 7:1629289. doi: 10.3389/fdgth.2025.1629289
Received: 15 May 2025; Accepted: 15 August 2025;
Published: 15 September 2025.
Edited by:
Björn Wolfgang Schuller, Imperial College London, United KingdomReviewed by:
M. Dulce Estêvão, University of Algarve, PortugalSujarwoto Sujarwoto, University of Brawijaya, Indonesia
Copyright: © 2025 Izaturwanaho, Ward, Ní Cheallaigh, Moran, Fitzgerald, Mockler, Geary and Corrigan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Felicien Izaturwanaho, aXphdHVyd2ZAdGNkLmll
†ORCID:
Felicien Izaturwanaho
orcid.org/0009-0007-0085-8954
Marie E. Ward
orcid.org/0000-0002-6638-8461
Clíona Ní Cheallaigh
orcid.org/0000-0002-0842-425X
Maeve Moran
orcid.org/0000-0002-9675-5488
Geraldine Fitzgerald
orcid.org/0000-0001-8045-0295
David Mockler
orcid.org/0000-0001-6171-8751
Una Geary
orcid.org/0000-0002-8811-2685
Siobhán Corrigan
orcid.org/0000-0003-2046-8252