 Emilia Daghir-Wojtkowiak1,†
Emilia Daghir-Wojtkowiak1,† Javier Alfaro1,†Michele Mastromattei2Aleksander Palkowski1Mark Stares3Ana Roca-Umbert4Andraz Krajnc5Riccardo Leoni6Anne Boland7Aria Nourbaksh2Ashwin Kallor1Camille Ducki8Davide Venditti2Carla Montesano2Chiara Cipriani2Daniel Faria9Delphine Pflieger10Elisa Zago11Etienne Bardet10Filipa Serrano9Florian Jeanneret10Damien Alouges10Liangwei Yin10Elodine Coquelet10Apolline Bacquet10Francesco Bonchi12Francesco Maiorino2Francesco Torino2Georges Bedran1Jean-Alexandre Long8Laura Balbi9Laurent Guyon10Liana Bevilacqua13Manuel Fiorelli2Marie-Catherine Wagner14Mario Reyes12Mario Roselli2Marta Contreiras Silva9Michal Waleron1Nikolas Dovrolis15Odile Filhol-Cochet10In Hwa Um16Georg Wolflein16Patrícia Eugénio9Pauline Bazelle10Pavlos Golnas17Peter Thorpe5Pierluigi Bove2Piyush Borole18Roberta Bernardini2Rohit Kumar12Rosella Cicconi2Saskia Kaltenbrunner14Saverio Gravina6Simona Brezar5Stefan Symeonides3Steven McGinn7Susana Nunes9Ted Hupp19Yuri Gordienko20Dimitrios Varvaras17Sergii Stirenko20Luciano Xumerle11Stefania Mariani11Assilah Bouzit8Stéphane Gazut9Heiko Poth21Kyriakos Souliotis17Hector Katifelis15Elena Verzoni13Giuseppe Procopio13Sarah Schoch22Francisco Lupiáñez-Villanueva4,23Sandra Türk21Katarzyna Barud14Dimitri Koroliouk20,‡Juan Caubet12,‡Yamir Moreno24,‡Jean-Luc Descotes8,‡Christina Golna17,‡Valentina Guadalupi13,‡Paolo Garagnani11,‡Maria Gazouli15,‡Jean-François Deleuze7,‡Frans Folkvord4,25,‡Nikolaus Forgó14,‡David J. Harrison16,‡Håkan Axelson22,‡Armando Stellato2,‡Maurizio Mattei2,‡Ajitha Rajan18,‡Alexander Laird3,‡Christophe Battail10,‡Catia Pesquita9,‡
Javier Alfaro1,†Michele Mastromattei2Aleksander Palkowski1Mark Stares3Ana Roca-Umbert4Andraz Krajnc5Riccardo Leoni6Anne Boland7Aria Nourbaksh2Ashwin Kallor1Camille Ducki8Davide Venditti2Carla Montesano2Chiara Cipriani2Daniel Faria9Delphine Pflieger10Elisa Zago11Etienne Bardet10Filipa Serrano9Florian Jeanneret10Damien Alouges10Liangwei Yin10Elodine Coquelet10Apolline Bacquet10Francesco Bonchi12Francesco Maiorino2Francesco Torino2Georges Bedran1Jean-Alexandre Long8Laura Balbi9Laurent Guyon10Liana Bevilacqua13Manuel Fiorelli2Marie-Catherine Wagner14Mario Reyes12Mario Roselli2Marta Contreiras Silva9Michal Waleron1Nikolas Dovrolis15Odile Filhol-Cochet10In Hwa Um16Georg Wolflein16Patrícia Eugénio9Pauline Bazelle10Pavlos Golnas17Peter Thorpe5Pierluigi Bove2Piyush Borole18Roberta Bernardini2Rohit Kumar12Rosella Cicconi2Saskia Kaltenbrunner14Saverio Gravina6Simona Brezar5Stefan Symeonides3Steven McGinn7Susana Nunes9Ted Hupp19Yuri Gordienko20Dimitrios Varvaras17Sergii Stirenko20Luciano Xumerle11Stefania Mariani11Assilah Bouzit8Stéphane Gazut9Heiko Poth21Kyriakos Souliotis17Hector Katifelis15Elena Verzoni13Giuseppe Procopio13Sarah Schoch22Francisco Lupiáñez-Villanueva4,23Sandra Türk21Katarzyna Barud14Dimitri Koroliouk20,‡Juan Caubet12,‡Yamir Moreno24,‡Jean-Luc Descotes8,‡Christina Golna17,‡Valentina Guadalupi13,‡Paolo Garagnani11,‡Maria Gazouli15,‡Jean-François Deleuze7,‡Frans Folkvord4,25,‡Nikolaus Forgó14,‡David J. Harrison16,‡Håkan Axelson22,‡Armando Stellato2,‡Maurizio Mattei2,‡Ajitha Rajan18,‡Alexander Laird3,‡Christophe Battail10,‡Catia Pesquita9,‡ Fabio Massimo Zanzotto2*§
Fabio Massimo Zanzotto2*§
- 1International Centre for Cancer Vaccine Science, University of Gdansk, Gdansk, Poland
- 2University of Rome “Tor Vergata”, Rome, Italy
- 3Urology Department, Western General Hospital, NHS Lothian, Edinburgh, United Kingdom
- 4PredictBy Research and Consulting SLU, Barcelona, Spain
- 5Caretronic d.o.o. Kranj, Slovenia
- 6DSTECH S.r.l., Rome, Italy
- 7CEA, Centre National de Recherche en Génomique Humaine, Université Paris-Saclay, Evry, France
- 8Centre Hospitalier Universitaire de Grenoble (CHU), Grenoble, France
- 9LASIGE, Faculdade de Ciências, Universidade de Lisboa, Lisboa, Portugal
- 10IRIG, Laboratoire Biosciences et Bioingénierie Pour la Santé, UA2 INSERM-CEA-UGA, Université Grenoble Alpes, Grenoble, France
- 11Personal Genomics Srl, Verona, Italy
- 12Eurecat, Centre Tecnològic de Catalunya, Barcelona, Spain
- 13Fondazione IRCCS Istituto Nazionale dei Tumori (INT), Milan, Italy
- 14Department of Innovation and Digitalisation in Law, University of Vienna, Vienna, Austria
- 15Laboratory of Biology, Medical School, National and Kapodistrian University of Athens, Athens, Greece
- 16School of Medicine, University of St Andrews, St Andrews, United Kingdom
- 17Health Policy Institute (HPI), Maroussi, Greece
- 18School of Informatics, University of Edinburgh, Edinburgh, United Kingdom
- 19Institute of Genetics and Cancer, University of Edinburgh, Edinburgh, United Kingdom
- 20National Technical University of Ukraine Igor Sikorsky Kyiv Polytechnic Institute, Kyiv, Ukraine
- 21EURICE, Heinrich-Hertz-Allee 1, St. Ingbert, Germany
- 22Division of Translational Cancer Research, Department of Laboratory Medicine, Lund University, Lund, Sweden
- 23Open University of Catalonia, Barcelona, Spain
- 24Institute for Biocomputation and Physics of Complex Systems and Department of Theoretical Physics, University of Zaragoza, Zaragoza, Spain
- 25Department of Communication and Cognition, Tilburg School of Humanities and Digital Sciences, Tilburg, Netherlands
Integrating multi-modal patient data to support personalized medicine has gained a lot of interest across different health domains over the past decade. Addressing this challenge requires the development and implementation of an informed, evidence-based AI-driven decision-support system continuously maintained and updated to align with the latest clinical guidelines. A key challenge to ensure its real-life adoption lies in translating the outcomes of complex AI-driven data integration and modeling into a form easily understood by the clinical audience. To ensure explainability, knowledge graphs have emerged as data models integrating multi-omics data sources and representing them as interconnected networks. Knowledge graphs offer a framework which AI models can progressively refine, highlighting the most influential features and relationships facilitating transparency of complex interactions and interdependencies. In this perspective we present major components and challenges upon developing a knowledge-based explainable AI system. Additionally, we showcase a current effort undertaken by the Knowledge at the Tips of your Fingers (KATY) consortium to develop the infrastructure for an explainable system supporting best treatment decision for a renal cancer patient.
Introduction
Integrating multi-modal patient data—such as genetic information, expression profiles, imagining and molecular data—into a unified framework has gained a lot of interest in different health domains over the past decade (1, 2). The recent increase in computational power and algorithm performance boost, have made it possible to feed AI models with extensive patient-specific data, paving the way for the development of software solutions that enable more personalized diagnoses and treatments (3, 4). Crucial to achieving this vision is not only the development and implementation of disease-focused, knowledge-based decision-support system but also its continuous maintenance and regular update to align with the latest clinical practice guidelines (5). Up to now, several tools supporting the vision of precision medicine have emerged.
IBM Watson for Oncology (WFO) was the first knowledge-based system leveraging natural language processing (NLP) supporting evidence-based treatment decisions categorized as recommended, for consideration, or not recommended across seven types of cancer. Alongside the NLP-driven WFO, OncoDoc2 emerged as a decision-tree-based system designed to integrate clinical data from electronic health records (EHR), to suggest optimal treatments for non-metastatic breast cancer (6) Similarly, a guideline-based decision support system developed as part of the DESIREE European project aimed at creating web-based services for managing primary breast cancer (7, 8).
In the field of medical image analysis including x-rays, CT images, and MRI scans, deep learning techniques have significantly enhanced tumor detection, localization, assessment of muscle invasiveness and tumor grading. These advancements facilitated the distinction between disease subtypes enabling more effective treatment planning and better patient stratification (9–16). As an example, a 3D deep radiomics pipeline has been successfully used for analyzing CT scans of metastatic urothelial cancer patients, demonstrating capability of differentiating between disease, control and progression in response to immunotherapy (17).
While creating a straightforward decision support system is technically feasible, a key challenge lies in translating the outcomes of complex AI-driven big data integration and modeling into a form easily understood by the clinical audience and in parallel compliant with binding legal provisions. To address this challenge, efforts are focused on integrating medical knowledge, biological pathways, and clinical guidelines into knowledge-based models. Developing a knowledge graph (KG) and incorporating it into AI model architecture, may provide explainable visualizations of the AI model's complex reasoning enhancing AI-supported, knowledge-based diagnosis and treatment recommendations within a specific biomedical domain. In this perspective we present challenges upon developing a knowledge-based explainable AI system and describe a current effort undertaken by the KATY consortium to develop the infrastructure for ready-to-use explainable decision-support system that can be deployed in clinical reality.
How knowledge-based models interplay with AI model
Knowledge-based models integrate various multi-modal biomedical data sources by developing ontologies, which are structured frameworks for organizing information that define the relationships between key concepts and categories within a specific domain. These ontologies establish a formalized vocabulary, hierarchy of terms, relationships and rules to describe large volumes of heterogeneous biomedical data. Examples include HPO (Human Phenotype Ontology) (18), UMLS (Unified Medical Language System) (19), NCIT (National Cancer Institute Thesaurus) (20) and OMIM (Online Mendelian Inheritance in Men) (21) which serve as semantic “building blocks” for biomedical knowledge models. These structered, hierarchical ontologies and knowledge bases enable the development and enrichment of the knowledge models by defining standardizing terms, concepts, and relationships. They support transparent mapping between patient data, phenotypes, genotypes, and clinical concepts, facilitating tracability and interpretability.
Building on this foundation, knowledge graphs can represent diverse data sources as networks of interconnected entities (nodes) and relationships (edges) capable of capturing dynamic, real-world interactions and associations (22, 23). When tailored to a specific biomedical domain, KGs enhance data accessibility, interoperability and integration, facilitating more efficient data analysis and further interpretation.
A key challenge in building KGs is the scattered and inconsistent nature of information across disease-specific domains. In the cancer field, despite significant efforts made by consortia to develop standardized datasets, information from various organizational levels of datasets is dispersed across studies. Unstandardized data repositories, evolving ontologies, and the need to continuously adapt to ever-changing clinical guidelines (24) adds huge complexity to harmonization and integration of diverse data sources.
Building cohesive and functional KGs for cancer research faces several challenges related to: (i) Scalability - developing KGs requires manual labor and expensive expert input, making it difficult to scale; (ii) Variation in Cancer Representation Across Biomedical Data Repositories - cancer descriptions in medical repositories often do not follow standardized naming conventions or alignment with clinical guidelines, complicating large-scale data harmonization which hinders its usability and interoperability; and (iii) Ambiguity in Distinguishing Cancer Types - symptoms, causes, and manifestations of various cancers often overlap, making precise categorization of subtypes challenging.
Despite those intricacies, we observe constant efforts in building KGs from biomedical literature and clinical records. The Human Diseases Network (HDN) and Human Symptoms-Disease Network (HSDN) (25) have demonstrated the utility of disease-centric KGs via exploring the intricate relationships between clinical symptoms and diseases through molecular interactions enabling exploration of disease taxonomy and pathogenesis. The Scalable Precision Medicine Open Knowledge Engine (SPOKE) (26) has linked various biomedical databases to integrate individual patient data providing more personalized and data-driven healthcare insights. More recently PrimeKG, has offered a comprehensive and multi-modal view of diseases incorporating disease-associated perturbations in the proteome, biological processes, molecular pathways as well as anatomical and phenotypic scales, environmental exposures, and a range of approved and experimental drugs along with their therapeutic actions (24). Unlike the broad disease- or drug-oriented KGs, the Genetic and Rare Diseases Information Center (GARD) (27) focuses exclusively on rare diseases, aiming to advance understanding of unmet clinical needs and evidence-based research. In addition, over a thousand biomedical ontologies are emerging in BioPortal (28) - a comprehensive repository covering various cancer fields such as breast, thyroid, and prostate cancer. Despite their availability, leveraging these ontologies effectively remains challenging. Many were developed with a specific perspective and purpose in mind tailored to specific research goals or projects, which may not align with other use cases or compatibility with new applications.
In addition to existing disease-focused ontologies, there is a growing interest in building stage- and grade-specific ontologies aimed at deeper conceptualizations of a specific disease, however this concept has not been explored much in biomedical domains. In addition, transferring the knowledge embedded in KGs for the identification and characterization of rare disease is also of interest as nowadays, research in the rare diseases field is oriented towards the collection and analysis of omics data in case-study scenarios. Adoption of the KG could interconnect between several studies, synthesizing state-of-the-art knowledge and providing greater explainability of rare diseases not only to clinicians and patients but also generally to the field.
Leveraging knowledge graphs can streamline the learning process of AI models enhancing their explainability and transparency. Consequently, this interplay between both components significantly boosts interpretability (29) as KGs offers a framework that AI models can progressively refine. Through iterative learning, neural network architectures which naturally form graph-like structures (as entities encoded within these networks are interrelated), refine ontologies and highlight the most influential features and relationships. In consequence, the refined KG incorporates new information while eliminating inconsistencies, redundancies and duplicates. This refinement process facilitates improved detection of patterns, correlations and identification of broader categories or clusters within the data that have not been immediately apparent.
The interplay between the KG and the AI model would definitely support more robust AI-driven insights and decision-making, and is especially important for developing explainable recommendation systems which should ideally be responsive and adaptive to real-time changes.
Enhancing explainability and interpretability of AI models
When dealing with unstructured multi-modal data, black-box models with more free parameters are preferred for capturing complex relationships in labeling, clustering, and pattern recognition tasks. While these models enhance the overall understanding of a system and its outputs, they do not inherently provide explanations that human experts can understand and comprehend (30, 31). Ensuring explainability and interpretability remains one of the biggest challenges in deploying AI-based models in real-world applications. Different models of explainability such as text-based, visual, and feature relevance explanations, are possible and should be adjusted to domain-specific research (30, 32, 33).
Recent work by Anthropic [https://transformer-circuits.pub/2024/scaling-monosemanticity/index.html] demonstrated that neuron-level interpretability in large language models is becoming achievable through advanced scaling techniques. Their approach aims to enhance model transparency by identifying monosemantic units—individual neurons that consistently represent specific, human-interpretable concepts—enabling a form of parameter-level understanding previously inaccessible in deep neural networks. While this aspect is significant for foundational AI safety and transparency, its direct applicability to clinical settings remains limited. In the context of medical AI, the primary focus should shift away from internal model mechanisms and instead emphasize whether the system demonstrates clinically reliable, safe, and interpretable behavior at the input–output level. Consequently, traditional validation frameworks such as sensitivity, specificity, and outcome-based performance metrics seem to align more closely with established clinical paradigms and are more trusted by healthcare professionals. Anthropic's findings suggest that medical AI systems should prioritize behavior-centric evaluations which is more practical and trusted forms of interpretability in healthcare applications.
To date, one study has utilized the knowledge graph fed with multi-source clinical data including basic clinical data, disease history, medical test results, and other Diabetic Macular Edema-related factors to predict this disease (34). In the field of precision radiotherapy, Niraula et al. developed a clinical decision-support system leveraging knowledge-based AI-assisted decision-making in response-adaptive radiotherapy (ARCliDS). The system was designed to adjust optimal daily dosage of radiation being the first web-based software with GUI dedicated to assist knowledge-based response-adaptive radiotherapy with multi-omics data improving the outcomes in dynamic treatment regime (35). Lately, the xDECIDE system has been developed and tested on various types of cancer as a tool to support clinical decision making effectively closing the learning loop through continuous, multi-source feedback integration. Central to this approach is the incorporation of expert-derived treatment recommendations from virtual tumor boards, which are used to iteratively train and refine the AI-based model (xCORE). In addition to expert input, the system incorporates real-world clinical data, such as treatment decisions made by patients and physicians, longitudinal clinical outcomes such as tumor response, adverse events, biomarker trajectories, and survival. The outcome data provide a foundation for retrospective performance evaluation and model recalibration. Furthermore, the xDECIDE platform leverages aggregated real-world evidence from the XCELSIOR registry (“Xperience Clinical Evidence Led System for Investigating Outcomes in Real-World Oncology”) to refine its knowledge base and decision-making heuristics. This closed-loop framework links what was recommended, what was implemented, and how patients responded to dynamically update treatment rationales and recommendations as new data is available. This idea of closing the learning loop not only has the potential of enhancing the relevance and accuracy of AI-driven guidance but also strengthens transparency, explainability, and clinical trust (36).
Despite these efforts, a systematic analysis of how explanations should be structured within disease-specific domains remains lacking. For AI-assisted diagnostic and treatment recommendation tools, explanations must be clear, comprehensive and conceptually coherent. Only then can these models provide transparency and interpretability essential for building trust within the medical community and establishing domain-expert interpretation and inference that align with current medical knowledge. Due to data sparsity, we need to leverage knowledge from publicly available omics data repositories and build knowledgeable databases within the context of specific diseases. Only by this we can advance knowledge-driven model development and promote explainable AI in healthcare (37–39).
To the best of our knowledge, there is no study which has utilized a knowledge graph-based explainable AI pipeline that integrates foundation models of omics data: genomics, transcriptomics, proteomics, to enhance diagnosis and/or treatment decision-making within the sparse data context in a specific biomedical domain. This effort has been undertaken by the Knowledge at the Tips of your Fingers (KATY) consortium funded in the H2020-EU.3.1. - SOCIETAL CHALLENGES - Health, demographic change and well-being programme under a call “AI for Genomics and Personalized Medicine” aims at implementing AI-assisted strategies for enhancing the contribution of -omics studies in personalized medicine.
Effort of the KATY consortium towards developing explainable AI system
The KATY project develops a non-linear expert system capable of utilizing incomplete multi-modal omics information to predict the optimal treatment scheme in patients with metastatic clear cell renal cell carcinoma (ccRCC).
ccRCC accounts for 75% of total RCC incidence which increases worldwide and accounts for 2% of cancer diagnoses, affecting approximately 10/100,000 in the United States and Western Europe (40). Current treatment choice is largely driven by clinical trial inclusion criteria and guideline recommendations from the European Association of Urology (41), European Society of Medical Oncology (42) and American Society of Clinical Oncology (43) recommending first line treatment with combination immune checkpoint inhibitors (ICI) and tyrosine kinase inhibitors (TKI) therapy, or dual ICI for intermediate or poor risk disease. Despite these recommendations and the resultant improved survival benefit, still the response to treatment varies from individual to individual, complete response remains relatively rare, some patients develop significant adverse reactions to treatment and most patients eventually progress requiring a change in treatment (44).
Therefore, the greatest challenge is not only to gather more molecular or clinical information, but rather to better use and process the information that has already been gathered and is publicly available through the incorporation of pre-existing or newly developed foundation models. Despite a progress in AI-assisted noninvasive characterization of kidney tumors using CT imaging, better characterization of grading system (45), existence of clinical, pathological markers as well as genomic or transcriptomic signatures reported, potentially useful to guide treatment selection and predict response to systemic therapy, choosing the most optimal therapy with best treatment response at a patient-specific level is currently the biggest unmet need (46).
This is where the KATY project steps in developing a system which is interactively trained rather than being strictly programmed allowing for prediction without predefined rules and providing explainability to end users. The AI-assisted KATY Platform is built around the (i) KATY Holistic Neural Network (KATYHoNN) black-box model and the (ii) Distributed Knowledge Graph offering post-hoc explainability.
Datasets and ontologies
To build the knowledge graph for the KATYHoNN model we utilize two type of datasets:
(i) data from clinical trials evaluating the efficiency of targeted therapies, immunotherapies and combination of both,
(ii) publicly-available omics datasets for ccRCC patients.
We divided these dense and multi-modal datasets into “main” and “support” datasets. The “main dataset” makes use of (i) data from clinical trials and associated ontologies to address the question on the treatment effectiveness measured for each antitumor drug and estimate response-to-treatment metrics [i.e., tumor shrinkage, overall response rate (ORR), progression-free survival (PFS), and overall survival (OS)].
The “support dataset” makes use of (ii) publicly-available omics datasets and associated ontologies to predict features which are not directly linked to response-to-therapy.
Both data types are integrated into a knowledge graph through a network of ontologies, to offer comprehensive, interconnected and explainable representation of treatment effectiveness and influencing factors for a single patient (Figure 1).
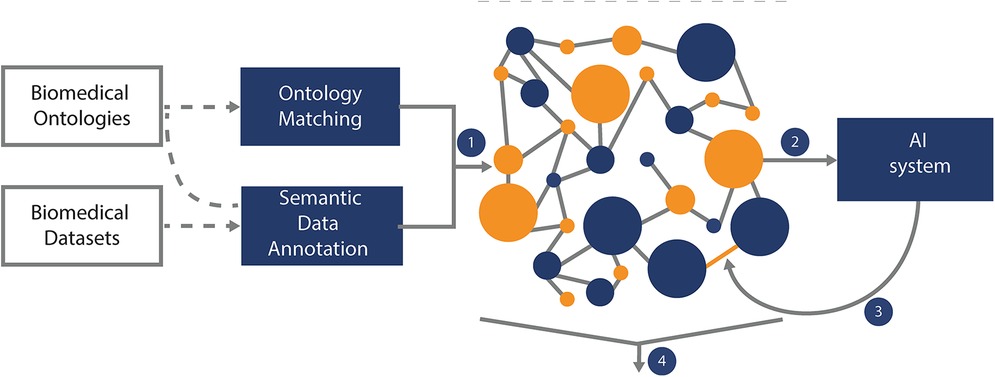
Figure 1. Knowledge graph construction and design. The Knowledge Graph is built using techniques of Ontology Matching and Semantic Annotation over renal cell carcinoma ontologies and KATY datasets stored in the data lake (the Knowledge Graph is stored in a GraphDB instance that supports fast loading, querying and visualization of the graph) (1). Upon development, the Knowledge Graph can be used as a source of knowledge-enriched features for the AI system (2). The outcomes of the AI-supported system can refine the Knowledge Graph (3). The data and outcomes as represented in the Knowledge Graph can be used to support explanation generation (4). Querying and visualizing the Knowledge Graph is supported by intelligent graphical user interfaces to present explanations to end-users.
KATY model
The KATY model consists of sub-networks that are trained using data from clinical trials and omics data for ccRCC patients and also more widely available -omics data, for example T-cell antigen landscapes published across over 2,300 published samples. Sub-division of the KATYHoNN model into sub-networks (trained either on specific omics dataset or on all omics datasets together) makes the realization of the final model easier and more precise, as each component is trained for a specific task and can be easily handled in the event of errors or changes. This training strategy mitigates the missing data problem, where there may be sufficient data for a specific task but insufficient data for all tasks combined. In case of insufficient data for model training, data from different cancer types can be used to pre-train specific sub-networks which can then be transferred to the ccRCC model. With this approach referred to as transfer learning, the KATYHoNN model can exploit future datasets enabling real-time training of the entire model. In this way the KATYHoNN model is easily modifiable, as at the same time, it is possible to add new components within the KATYHoNN model and modify the existing ones by deleting or linking them. The results from the KATYHoNN model deployed onto a dedicated KATY Platform and supported with the knowledge graph will allow physicians to predict survival/response to therapy when uploading patient's test results (Figure 2).
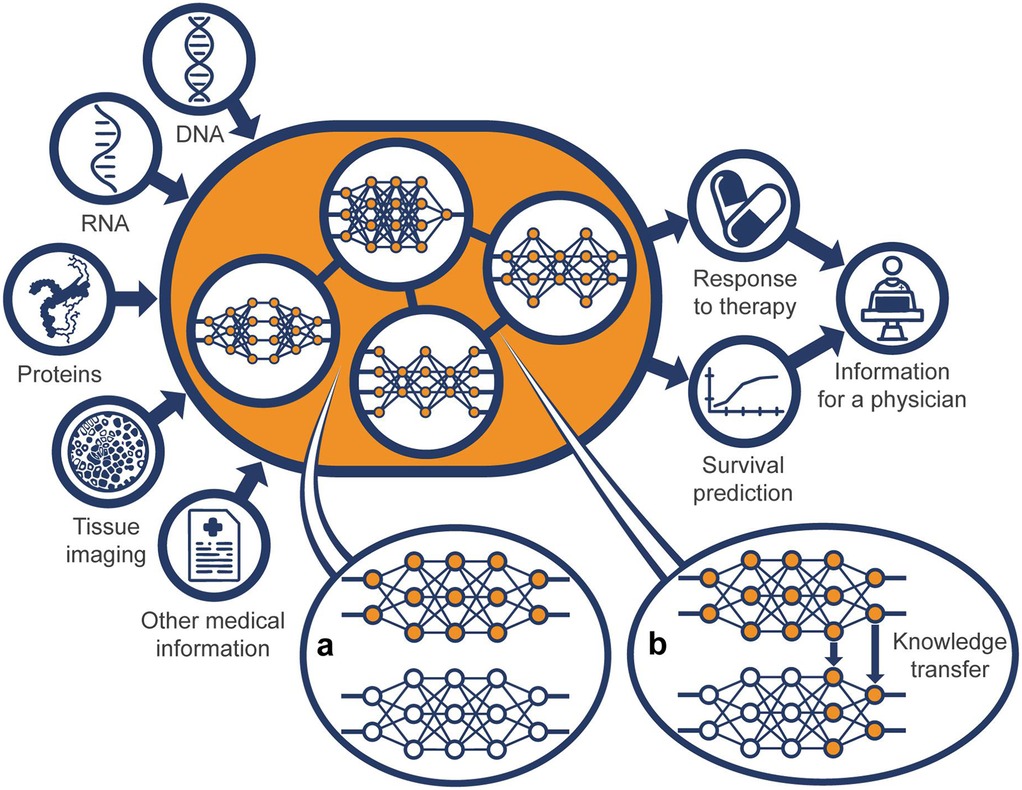
Figure 2. General representation of the KATY holistic neural network model (KATYHoNN). The KATYHoNN model input leverages publicly-available datasets for ccRCC patients and data from clinical trials evaluating the efficiency of therapies. The heart of the model is composed of individual sub-networks for which the input is available omics data and clinical patient data. The sub-networks can be trained either on: (i) singular specific task (e.g., either genomics or transcriptomics or proteomics or RNA-Seq data) via transfer learning (b), or (ii) all tasks together (patients data evaluating the efficiency of therapies) via multi-task learning (a) to compile the general network. The result of a multi-task learning (a) is prediction of response-to-therapy, while the results from transfer learning (b) is prediction of other features not directly related to treatment choice. The KATYHoNN model deployed on a dedicated KATY Platform will allow a physician to upload a patient's test results and gain the best treatment recommendation in parallel with KG-driven explanation based on which features such a treatment was proposed and what the survival rate for that patient is.
Legal compliance
The KATY project ensures that the development and usage of the KATY Platform, as well as the use and re-use of the data generated and collected in the KATY project, is conducted in accordance with binding legal provisions. The project monitors and addresses the requirements set forth in the EU legal acts concerning (personal) data protection (especially with regard to special categories of data, i.e., data concerning health and genetic data), AI and data governance. Once the data protection and privacy principles have been identified, technical solutions such as data access management, encryption, cryptographic components, pseudonymisation and, where achievable, anonymisation of data, data minimisation, secure storage of data and secure data transfer, have been included in the design of the KATY Platform allowing for the European Union's General Data Protection Regulation (GDPR)-compliant processing of the data and usage of the platform.
Summing up, the KATY project develops the infrastructure for a ready-to-use explainable decision-support system that complies with all legal requirements (11).
Discussion
To realize the vision of an AI-empowered Personalized Medicine in the clinical workflow, we need to tackle a challenge of developing a multi-tiered AI-supported system capable of handling complexity of multi-modal data simultaneously being adaptable to new knowledge and constantly changing treatment guidelines. To enhance maintainability and scalability of the system, it should accommodate 3 tiers: the Data Tier, which ensures secure storage and interoperability of diverse medical data; the Application Tier, which processes data and generates recommendations; and the Presentation Tier, which provides user-friendly interfaces for clinicians and patients. The separation between 3 tiers facilitates managing of the whole system, so that changes in one tier do not necessarily affect the other tiers (47–49).
Over the next several years, we anticipate the establishment of digital medicine centers that will invest in human resources, assembling well-connected medical, IT, and research teams to make these advancements a reality. Domain experts who are constantly supported by physicians will evolve to accommodate constantly evolving treatments, and build disease-oriented knowledge models in a domain-specific field.
With real-time explainable treatment recommendations, the next step would be to link post-treatment (follow-up) data of individual patients with potential side effects and drug interactions, personalized to their medical history and current medications. To fully leverage AI-supported systems linked to knowledge-based models, we must start collecting omics data for each patient within the healthcare system while simultaneously training and motivating doctors on how and why to use these systems in their daily practice. In the future, those who incorporate AI-supported tools into their routine will probably replace those who do not.
Encouraging transparent communication about the complexity and data sparsity in biomedical AI areas, like personalized cancer treatment, is essential for aligning funding institutions and stakeholders on feasible solutions. Valuable clinical trial data and -omic data is hidden by numerous legal agreements, creating a significant barrier to integrating and making this data accessible for AI systems. In these clinical trial contexts, patient health is prioritized over data volume, leading to the use of simpler, transparent models developed to address specific clinical questions. A modern approach may involve leveraging foundation models—large, pre-trained AI models for specific data types that can be fine-tuned for various tasks—and using them as black-box models with post-hoc explainability rooted in visual representation and feature relevance.
Despite efforts to build AI-supported decision systems, a systematic study of explanations for decisions within disease-specific domains is still missing. The explanations offered by AI decision-support systems must provide understandable and conceptually coherent knowledge. Only then can AI models provide transparent, human-interpretable explanations of AI-assisted diagnosis and treatment recommendations, facilitating their adoption in real clinical settings. Building on how the AI model explains its predictions is important for gaining trust from the medical community and establishing domain-expert interpretation and inference grounded in current medical findings. Addressing these gaps in explanation structure and knowledge leveraging is essential for advancing knowledge-based model development driving explainable AI.
We believe that continuous interaction between physicians and AI provided by the system's architecture, along with dynamically curated databases and ongoing feedback from doctors, is essential for ensuring evidence-based, data-driven and research-supported recommendations for specific disease areas. However, we also recognize that without real-world outcome data—such as predicted or observed survival curves for patients across different treatment regimens—these systems are unlikely to significantly impact clinical decision-making. This challenge is particularly important in rare cancers, where data scarcity limits the generation of robust comparative insights. In this context, recent advances in reasoning-oriented large language models, such as OpenAI's o3 and o4 series, may offer a promising direction. These models are capable of integrating structured biomedical knowledge, disclosing their internal reasoning processes, and producing auditable, evidence-supported treatment rationales—potentially bridging the gap between algorithmic outputs and clinically actionable insight.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
ED-W: Writing – original draft, Visualization, Investigation, Conceptualization, Resources, Writing – review & editing. JA: Conceptualization, Writing – review & editing, Writing – original draft, Supervision. MiM: Conceptualization, Writing – review & editing. AP: Conceptualization, Writing – review & editing. MS: Conceptualization, Writing – review & editing. AR-U: Conceptualization, Writing – review & editing. AKr: Conceptualization, Writing – review & editing. RL: Conceptualization, Writing – review & editing. AnB: Conceptualization, Writing – review & editing. AN: Conceptualization, Writing – review & editing. AKa: Conceptualization, Writing – review & editing. CD: Conceptualization, Writing – review & editing. DVe: Conceptualization, Writing – review & editing. CM: Conceptualization, Writing – review & editing. CC: Conceptualization, Writing – review & editing. DF: Conceptualization, Writing – review & editing. DP: Conceptualization, Writing – review & editing. EZ: Conceptualization, Writing – review & editing. EB: Conceptualization, Writing – review & editing. FS: Conceptualization, Writing – review & editing. FJ: Conceptualization, Writing – review & editing. DA: Conceptualization, Writing – review & editing. LY: Conceptualization, Writing – review & editing. EC: Conceptualization, Writing – review & editing. ApB: Conceptualization, Writing – review & editing. FB: Conceptualization, Writing – review & editing. FM: Conceptualization, Writing – review & editing. FT: Conceptualization, Writing – review & editing. GB: Conceptualization, Writing – review & editing. J-AL: Conceptualization, Writing – review & editing. LaB: Conceptualization, Writing – review & editing. LG: Conceptualization, Writing – review & editing. LiB: Conceptualization, Writing – review & editing. MF: Conceptualization, Writing – review & editing. M-CW: Conceptualization, Writing – review & editing. MRe: Conceptualization, Writing – review & editing. MRo: Conceptualization, Writing – review & editing. MCS: Conceptualization, Writing – review & editing. MW: Conceptualization, Writing – review & editing. ND: Conceptualization, Writing – review & editing. OF-C: Conceptualization, Writing – review & editing. IU: Conceptualization, Writing – review & editing. GW: Conceptualization, Writing – review & editing. PE: Conceptualization, Writing – review & editing. PBaz: Conceptualization, Writing – review & editing. PG: Conceptualization, Writing – review & editing. PT: Conceptualization, Writing – review & editing. PBov: Conceptualization, Writing – review & editing. PBor: Conceptualization, Writing – review & editing. RB: Conceptualization, Writing – review & editing. RK: Conceptualization, Writing – review & editing. RC: Conceptualization, Writing – review & editing. SK: Conceptualization, Writing – review & editing. SGr: Conceptualization, Writing – review & editing. SB: Conceptualization, Writing – review & editing. SSy: Conceptualization, Writing – review & editing. SMc: Conceptualization, Writing – review & editing. SN: Conceptualization, Writing – review & editing. TH: Conceptualization, Writing – review & editing. YG: Conceptualization, Writing – review & editing. DVa: Conceptualization, Writing – review & editing. SSt: Conceptualization, Writing – review & editing. LX: Conceptualization, Writing – review & editing. SMa: Conceptualization, Writing – review & editing. AsB: Conceptualization, Writing – review & editing. SGa: Conceptualization, Writing – review & editing. HP: Conceptualization, Writing – review & editing. KS: Conceptualization, Writing – review & editing. HK: Conceptualization, Writing – review & editing. EV: Conceptualization, Writing – review & editing. GP: Conceptualization, Writing – review & editing. SSc: Conceptualization, Writing – review & editing. FL-V: Conceptualization, Writing – review & editing. ST: Conceptualization, Writing – review & editing. KB: Conceptualization, Writing – review & editing. DK: Conceptualization, Writing – review & editing. JC: Conceptualization, Writing – review & editing. YM: Conceptualization, Writing – review & editing. J-LD: Conceptualization, Writing – review & editing. CG: Conceptualization, Writing – review & editing. VG: Conceptualization, Writing – review & editing. PG: Conceptualization, Writing – review & editing. MG: Conceptualization, Writing – review & editing. J-FD: Conceptualization, Writing – review & editing. FF: Conceptualization, Writing – review & editing. NF: Conceptualization, Writing – review & editing. DH: Conceptualization, Writing – review & editing. HA: Conceptualization, Writing – review & editing. AS: Conceptualization, Writing – review & editing. MaM: Conceptualization, Writing – review & editing. AR: Conceptualization, Writing – review & editing. AL: Conceptualization, Writing – review & editing. CB: Conceptualization, Writing – review & editing. CP: Conceptualization, Writing – review & editing. FZ: Writing – original draft, Writing – review & editing, Resources, Supervision, Methodology.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by the European Union programme Horizon 2020 under the call H2020-SCI-FA-DTS-2020-1 (contract number 101017453).
Acknowledgments
We gratefully acknowledge Poland's high-performance Infrastructure PLGrid ACK Cyfronet AGH, for providing computer facilities and support within computational grant no PLG/2023/016653.
Conflict of interest
AR-U, FL-V, FF were employed by PredictBy Research and Consulting SLU. RL, SGr were employed by DSTECH S.r.l. EZ, LX, SMa, PG were employed by Personal Genomics Srl. AK, PT and SB were employed by Caretronic d.o.o.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ulrich H, Kock-Schoppenhauer AK, Deppenwiese N, Gött R, Kern J, Lablans M, et al. Understanding the nature of metadata: systematic review. J Med Internet Res. (2022) 11:24(1):e25440. doi: 10.2196/25440
2. Montaner J, Ramiro L, Simats A, Tiedt S, Makris K, Jickling GC, et al. Multilevel omics for the discovery of biomarkers and therapeutic targets for stroke. Nat Rev Neurol. (2020) 16(5):247–64. doi: 10.1038/s41582-020-0350-6
3. Chua IS, Gaziel-Yablowitz M, Korach ZT, Kehl KL, Levitan NA, Arriaga YE, et al. Artificial intelligence in oncology: path to implementation. Cancer Med. (2021) 10:4138–49. doi: 10.1002/cam4.3935
4. Schwantes IR, Axelrod DA. Technology-enabled care and artificial intelligence in kidney transplantation. Curr Transplant Rep. (2021) 8(3):235–40. doi: 10.1007/s40472-021-00336-z
5. Lamb BW, Brown KF, Nagpal K, Vincent C, Green JS, Sevdalis N. Quality of care management decisions by multidisciplinary cancer teams: a systematic review. Ann Surg Oncol. (2011) 18(8):2116–25. doi: 10.1245/s10434-011-1675-6
6. Bouaud J, Spano JP, Lefranc JP, Cojean-Zelek I, Blaszka-Jaulerry B, Zelek L, et al. Physicians’ attitudes towards the advice of a guideline-based decision support system: a case study with OncoDoc2 in the management of breast cancer patients. Stud Health Technol Inform. (2015) 216:264–9.26262052
7. Séroussi B, Guézennec G, Lamy JB, Muro N, Larburu N, Sekar BD, et al. Reconciliation of multiple guidelines for decision support: a case study on the multidisciplinary management of breast cancer within the DESIREE project. AMIA Annu Symp Proc. (2018) 16:1527–36.
8. Jie Z, Zhiying Z, Li L. A meta-analysis of Watson for Oncology in clinical application. Sci Rep. (2021) 11:5792. doi: 10.1038/s41598-021-84973-5
9. Feretzakis G, Juliebø-Jones P, Tsaturyan A, Sener TE, Verykios VS, Karapiperis D, et al. Emerging trends in AI and radiomics for bladder, kidney, and prostate cancer: a critical review. Cancers (Basel). (2024) 16(4):810. doi: 10.3390/cancers16040810
10. Rodriguez-Ruiz A, Lång K, Gubern-Merida A, Broeders M, Gennaro G, Clauser P, et al. Stand-alone artificial intelligence for breast cancer detection in mammography: comparison with 101 radiologists. J Natl Cancer Inst. (2019) 111:916–22. doi: 10.1093/jnci/djy222
11. Wang B, Jin S, Yan Q, Xu H, Luo C, Wei L, et al. AI-assisted CT imaging analysis for COVID-19 screening: building and deploying a medical AI system. Appl Soft Comput. (2021) 98:106897. doi: 10.1016/j.asoc.2020.106897
12. Stammes MA, Lee JH, Meijer L, Naninck T, Doyle-Meyers LA, White AG, et al. Medical imaging of pulmonary disease in SARS-CoV-2-exposed non-human primates. Trends Mol Med. (2022) 28(2):123–42. doi: 10.1016/j.molmed.2021.12.001
13. Kurt Bayrakdar S, Orhan K, Bayrakdar IS, Bilgir E, Ezhov M, Gusarev M, et al. A deep learning approach for dental implant planning in cone-beam computed tomography images. BMC Med Imaging. (2021) 21:86. doi: 10.1186/s12880-021-00618-z
14. Xia TY, Zhou ZH, Meng XP, Zha JH, Yu Q, Wang WL, et al. Predicting microvascular invasion in hepatocellular carcinoma using CT-based radiomics model. Radiology. (2023) 307(4). doi: 10.1148/radiol.222729
15. Kim H, Kang SW, Kim JH, Nagar H, Sabuncu M, Margolis DJA, et al. The role of AI in prostate MRI quality and interpretation: opportunities and challenges. Eur J Radiol. (2023) 165:110887. doi: 10.1016/j.ejrad.2023.110887
16. Song J, Hahm J, Lee J, Lim CY, Chung MJ, Youn J, et al. Comparative validation of AI and non-AI methods in MRI volumetry to diagnose parkinsonian syndromes. Sci Rep. (2023) 13(1):7188. doi: 10.1038/s41598-023-33774-z
17. Rundo F, Bersanelli M, Urzia V, Friedlaender A, Cantale O, Calcara G, et al. Three-dimensional deep noninvasive radiomics for the prediction of disease control in patients with metastatic urothelial carcinoma treated with immunotherapy. Clin Genitourin Cancer. (2021) 19:396–404. doi: 10.1016/j.clgc.2021.03.012
18. Köhler S, Gargano M, Matentzoglu N, Carmody LC, Lewis-Smith D, Vasilevsky NA, et al. The human phenotype ontology in 2021. Nucleic Acids Res. (2021) 49(8):D1207–17. doi: 10.1093/nar/gkaa1043
19. Bodenreider O. The unified medical language system (UMLS): integrating biomedical terminology. Nucleic Acids Res. (2004) 32:267–70. doi: 10.1093/nar/gkh061
20. Sioutos N, Coronado S, Haber MW, Hartel FW, Shaiu WL, Wright LW. NCI Thesaurus: a semantic model integrating cancer-related clinical and molecular information. J Biomed Inform. (2007) 40(1):30–43. doi: 10.1016/j.jbi.2006.02.013
21. Amberger JS, Bocchini CA, Scott AF, Hamosh A. OMIM.Org: leveraging knowledge across phenotype–gene relationships. Nucleic Acids Res. (2019) 47(D1):D1038–43. doi: 10.1093/nar/gky1151
22. Fang C, Arango Argoty GA, Kagiampakis I, Khalid MH, Jacob E, Bulusu KC, et al. Integrating knowledge graphs into machine learning models for survival prediction and biomarker discovery in patients with non-small-cell lung cancer. J Transl Med. (2024) 22(1):726. doi: 10.1186/s12967-024-05509-9
23. Chang D, Balažević I, Allen C, Chawla D, Brandt C, Taylor RA. Benchmark and best practices for biomedical knowledge graph embeddings. Proceedings of the 19th SIGBioMed Workshop on Biomedical Language Processing (2020). p. 167–76
24. Chandak P, Huang K, Zitnik M. Building a knowledge graph to enable precision medicine. Sci Data. (2023) 10(1):67. doi: 10.1038/s41597-023-01960-3
25. Zhou X, Menche J, Barabási AL, Sharma A. Human symptoms–disease network. Nat Commun. (2014) 5:4212. doi: 10.1038/ncomms5212
26. Himmelstein DS, Lizee A, Hessler C, Brueggeman L, Chen SL, Hadley D, et al. Systematic integration of biomedical knowledge prioritizes drugs for repurposing. ELife. (2017) 6:e26726. doi: 10.7554/eLife.26726
27. Zhu Q, Nguyen DT, Grishagin I, Southall N, Sid E, Pariser A. An integrative knowledge graph for rare diseases, derived from the genetic and rare diseases information center (GARD). J Biomed Semantics. (2020) 11(1):13. doi: 10.1186/s13326-020-00232-y
28. Salvadores M, Alexander PR, Musen MA, Noy NF. Bioportal as a dataset of linked biomedical ontologies and terminologies in RDF. Semant Web. (2013) 4(3):277–84.25214827
29. Silva MC, Eugénio P, Faria D, Pesquita C. Ontologies and knowledge graphs in oncology research. Cancers (Basel). (2022) 14(8):1906. doi: 10.3390/cancers14081906
30. Barredo Arrietaa A, Díaz-Rodríguez N, Del Ser J, Bennetot A, Tabikg A, Barbado A, et al. Explainable artificial intelligence (XAI): concepts, taxonomies, opportunities and challenges toward responsible AI. Information Fusion. (2020) 58:82–115. doi: 10.1016/j.inffus.2019.12.012
31. Rudin C. Stop explaining black box machine learning models for high stakes decisions and use interpretable models instead. Nat Mach Intell. (2019) 1(5):206–15. doi: 10.1038/s42256-019-0048-x
32. Loyola-González O. Black-box vs. white-box: understanding their advantages and weaknesses from a practical point of view. IEEE. (2019) 7:154096–113.
33. Scarpato N, Nourbakhsh A, Ferroni P, Riondino S, Roselli M, Fallucchi F, et al. Evaluating explainable machine learning models for clinicians. Cogn Comput. (2024) 16:1436–46. doi: 10.1007/s12559-024-10297-x
34. Li ZQ, Fu ZX, Li WJ, Fan H, Li SN, Wang XM, et al. Prediction of diabetic macular edema using knowledge graph. Diagnostics (Basel). (2023) 13(11):1858. doi: 10.3390/diagnostics13111858
35. Niraula D, Sun W, Jin J, Dinov ID, Cuneo K, Jamaluddin J, et al. A clinical decision support system for AI-assisted decision-making in response-adaptive radiotherapy (ARCliDS). Sci Rep. (2023) 13(1):5279. doi: 10.1038/s41598-023-32032-6
36. Shapiro MA, Stuhlmiller TJ, Wasserman A, Kramer GA, Federowicz B, et al. AI-augmented clinical decision support in a patient-centric precision oncology registry. AI Precis Oncol. (2024) 1:58–68. doi: 10.1089/aipo.2023.0001
37. Athieniti E, Spyrou GM. A guide to multi-omics data collection and integration for translational medicine. Comput Struct Biotechnol J. (2022) 21:134–49. doi: 10.1016/j.csbj.2022.11.050
38. Durán JM. Dissecting scientific explanation in AI (sXAI): a case for medicine and healthcare. Artif Intell. (2021) 297:103498. doi: 10.1016/j.artint.2021.103498
39. Wysocka M, Wysocki O, Zufferey M, Landers D, Freitas A. A systematic review of biologically-informed deep learning models for cancer: fundamental trends for encoding and interpreting oncology data. BMC Bioinformatics. (2023) 24(1):198. doi: 10.1186/s12859-023-05262-8
40. Dembrower K, Crippa A, Colón E, Eklund M, Strand F, ScreenTrustCAD Trial Consortium. Artificial intelligence for breast cancer detection in screening mammography in Sweden: a prospective, population-based, paired-reader, non-inferiority study. Lancet Digit Health. (2023) 5(10):703–11. doi: 10.1016/S2589-7500(23)00153-X
41. Ljungberg B, Albiges L, Abu-Ghanem Y, Bedke J, Capitanio U, Dabestani S, et al. European Association of Urology guidelines on renal cell carcinoma: the 2022 update. Eur Urol. (2022) 82:399–410. doi: 10.1016/j.eururo.2022.03.006
42. Powles T, Albiges L, Bex A, Grünwald V, Porta C, Procopio G, et al. ESMO clinical practice guideline update on the use of immunotherapy in early stage and advanced renal cell carcinoma. Ann Oncol. (2021) 32:1511–9. doi: 10.1016/j.annonc.2021.09.014
43. Rathmell WK, Rumble RB, Van Veldhuizen PJ, Al-Ahmadie H, Emamekhoo H, Hauke RJ, et al. Management of metastatic clear cell renal cell carcinoma: ASCO guideline. J Clin Oncol. (2022) 40:2957–95. doi: 10.1200/JCO.22.00868
44. Heng DY, Xie W, Regan MM, Warren MA, Golshayan AR, Sahi C, et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. J Clin Oncol. (2009) 27:5794–9. doi: 10.1200/JCO.2008.21.4809
45. Rasmussen R, Sanford T, Parwani AV, Pedrosa I. Artificial intelligence in kidney cancer. Am Soc Clin Oncol Educ Book. (2022) 42:1–11. doi: 10.1200/EDBK_350862
46. Choueiri TK, Albiges L, Atkins MB, Bakouny Z, Bratslavsky G, Braun DA, et al. From basic science to clinical translation in kidney cancer: a report from the second kidney cancer research summit. Clin Cancer Res. (2022) 28:831–9. doi: 10.1158/1078-0432.CCR-21-3238
47. Shoaib M, Mustafee N, Madan K, Ramamohan V. Leveraging multi-tier healthcare facility network simulations for capacity planning in a pandemic. Socioecon Plann Sci. (2023) 88:101660. doi: 10.1016/j.seps.2023.101660
48. Chu S, Cesnik B. A three-tier clinical information systems design model. Int J Med Inf. (2000) 57(2-3):91–107. doi: 10.1016/S1386-5056(00)00057-5
49. Hendriks MP, Jager A, Ebben KCWJ, van Til JA, Siesling S. Clinical decision support systems for multidisciplinary team decision-making in patients with solid cancer: composition of an implementation model based on a scoping review. Crit Rev Oncol Hematol. (2024) 195:104267. doi: 10.1016/j.critrevonc.2024.104267
Keywords: personalized cancer treatment, knowledge graphs, explainability, AI, foundation models, clinical decision-making
Citation: Daghir-Wojtkowiak E, Alfaro J, Mastromattei M, Palkowski A, Stares M, Roca-Umbert A, Krajnc A, Leoni R, Boland A, Nourbaksh A, Kallor A, Ducki C, Venditti D, Montesano C, Cipriani C, Faria D, Pflieger D, Zago E, Bardet E, Serrano F, Jeanneret F, Alouges D, Yin L, Coquelet E, Bacquet A, Bonchi F, Maiorino F, Torino F, Bedran G, Long J-A, Balbi L, Guyon L, Bevilacqua L, Fiorelli M, Wagner M-C, Reyes M, Roselli M, Silva MC, Waleron M, Dovrolis N, Filhol-Cochet O, Um IH, Wolflein G, Eugénio P, Bazelle P, Golnas P, Thorpe P, Bove P, Borole P, Bernardini R, Kumar R, Cicconi R, Kaltenbrunner S, Gravina S, Brezar S, Symeonides S, McGinn S, Nunes S, Hupp T, Gordienko Y, Varvaras D, Stirenko S, Xumerle L, Mariani S, Bouzit A, Gazut S, Poth H, Souliotis K, Katifelis H, Verzoni E, Procopio G, Schoch S, Lupiáñez-Villanueva F, Türk S, Barud K, Koroliouk D, Caubet J, Moreno Y, Descotes J-L, Golna C, Guadalupi V, Garagnani P, Gazouli M, Deleuze J-F, Folkvord F, Forgó N, Harrison DJ, Axelson H, Stellato A, Mattei M, Rajan A, Laird A, Battail C, Pesquita C and Zanzotto FM (2025) Leveraging knowledge for explainable AI in personalized cancer treatment: challenges and future directions. Front. Digit. Health 7:1637195. doi: 10.3389/fdgth.2025.1637195
Received: 28 May 2025; Accepted: 15 August 2025;
Published: 29 September 2025.
Edited by:
Gokce Banu Laleci Erturkmen, Software Research and Development Consulting, TürkiyeReviewed by:
Mark Shapiro, xCures Inc, United StatesCopyright: © 2025 Daghir-Wojtkowiak, Alfaro, Mastromattei, Palkowski, Stares, Roca-Umbert, Krajnc, Leoni, Boland, Nourbaksh, Kallor, Ducki, Venditti, Montesano, Cipriani, Faria, Pflieger, Zago, Bardet, Serrano, Jeanneret, Alouges, Yin, Coquelet, Bacquet, Bonchi, Maiorino, Torino, Bedran, Long, Balbi, Guyon, Bevilacqua, Fiorelli, Wagner, Reyes, Roselli, Silva, Waleron, Dovrolis, Filhol-Cochet, Um, Wolflein, Eugénio, Bazelle, Golnas, Thorpe, Bove, Borole, Bernardini, Kumar, Cicconi, Kaltenbrunner, Gravina, Brezar, Symeonides, McGinn, Nunes, Hupp, Gordienko, Varvaras, Stirenko, Xumerle, Mariani, Bouzit, Gazut, Poth, Souliotis, Katifelis, Verzoni, Procopio, Schoch, Lupiáñez-Villanueva, Türk, Barud, Koroliouk, Caubet, Moreno, Descotes, Golna, Guadalupi, Garagnani, Gazouli, Deleuze, Folkvord, Forgó, Harrison, Axelson, Stellato, Mattei, Rajan, Laird, Battail, Pesquita and Zanzotto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabio Massimo Zanzotto, ZmFiaW8ubWFzc2ltby56YW56b3R0b0B1bmlyb21hMi5pdA==
†These authors have contributed equally to this work
‡These authors share senior authorship
§ORCID:
Fabio Massimo Zanzotto
orcid.org/0000-0002-7301-3596