 Sidikiba Sidibé1,2*
Sidikiba Sidibé1,2* Fassou Mathias Grovogui3
Fassou Mathias Grovogui3 Karifa Kourouma3
Karifa Kourouma3 Delphin Kolié2
Delphin Kolié2 Bienvenu Salim Camara2,3Alexandre Delamou2,3Seni Kouanda1
Bienvenu Salim Camara2,3Alexandre Delamou2,3Seni Kouanda1
- 1Institut Africain de Santé Publique (IASP/USTA), Saint Thomas D’Aquin University, Ouagadougou, Burkina Faso
- 2African Centre of Excellence in the Prevention and Control of Communicable Diseases (CEA-PCMT), Faculty of Sciences and Health Techniques, Gamal Abdel Nasser University, Conakry, Guinea
- 3Centre National Training and Research Centre in Rural Health of Maferinyah, Forécariah, Guinea
Despite the recent repositioning efforts to increase the use of modern contraceptives, the prevalence of unmet need for contraception remains high among adolescent and young women in Guinea. This study analyzed the individual and contextual factors associated with the unmet need for contraception among adolescent and young women in 2018 in Guinea. We conducted a secondary analysis of the 2018 Demographic and Health Survey data. Multilevel mixed-effects logistic regression models were used to assess the association between individual and contextual characteristics and unmet need for contraception among adolescents and young women. Adjusted odds ratios (AORs) with their 95% confidence intervals (CIs) were calculated, with statistical significance set at p < 0.05. The prevalence of total unmet need for contraception was 22.6% (95% CI, 18.1–27.8). Being an adolescent aged 15–19 years (AOR = 1.44; 95% CI, 1.01–2.05), unmarried (AOR = 5.19; 95% CI, 3.51–7.67), having one or two children (AOR = 3.04; 95% CI, 2.18–4.25), or more than two children (AOR = 4.79; 95% CI, 3.00–7.62) were individual factors associated with the unmet need for contraception. As for community factors, only living in Labé (AOR = 2.54; 95% CI, 1.24–5.18) or Mamou (AOR = 1.73; 95% CI, 1.21–2.48) was significantly associated with the unmet need for contraception. In conclusion, both individual and community characteristics were significantly associated with the unmet need for contraception. This highlights the need to focus and strengthen communication and counseling strategies targeting adolescents and young women and aiming to increase the uptake of family planning in Guinea.
Introduction
Worldwide, 270 million women of reproductive age (15–49 years) had an unmet need for contraception in 2019; this unmet need is projected to increase by 10% by 2030 (1–3). Unmet need for contraception is defined as the proportion of fecund and sexually active women who do not want to become pregnant but are not using any form of contraception (4, 5). Moreover, 24% of women of reproductive age in low-income countries who wanted to avoid pregnancy could not use a modern method of contraception, with the majority of them living in sub-Saharan Africa (SSA) (6, 7). The main consequences of unintended early pregnancy among adolescents and young women include dropping out from school (8, 9), prolonged labor, preterm birth, stillbirths, neonatal deaths, and maternal and perinatal mortality (10). Though the use of modern methods of contraception can reduce maternal and child fatality, the majority of women of reproductive age in SSA are still at high risk of unsafe abortions and their related consequences (7, 11, 12). Furthermore, adolescent girls and young women (aged 15–19 years) represent one of the most burned groups by unmet need for contraception and unintended pregnancies in countries in SSA (6). In fact, more than one in five adolescent and young women has an unmet need for contraception in SSA (13, 14).
This high unmet need for contraception and its related consequences have been reported to be associated with several factors such as individual, sociocultural-, knowledge- (about contraceptive methods), and healthcare service-related factors (15–18). However, most of these studies mainly focused in general on women of reproductive age who were married, highlighting the need of evidence of the unmet need of contraception among adolescents and young women.
In Guinea, the prevalence of contraception among sexually active adolescent girls and young women (aged 15–24 years) using any contraceptive remains low along with a high fertility rate among adolescents (132 per 1,000 adolescents) and young people (205 per 1,000 women) (19). Despite the recent repositioning efforts to increase modern contraceptive prevalence in the country (20), more than 22% of women aged 15–49 years had an unmet need for contraception in Guinea (19). In fact, specific challenges exist in meeting the contraceptive needs of female adolescents and young women. These challenges include, among others, the non-adaptability of sexual and reproductive health services for adolescents, particularly those of family planning (FP), as well as not prioritizing the concerns of adolescent and young women with regard to contraception in available policy (21). This highlights the knowledge gaps of individual and community factors associated with the unmet need for contraception among adolescent and young women in Guinea. Therefore, the aim of the present study was to analyze the individual and community factors associated with the unmet need for contraception among adolescents and young women in Guinea in 2018. This information could be used as evidence for guiding policy and interventions on sexual and reproductive health targeting adolescents and young women.
Materials and methods
Data and population
Data were extracted from the 2018 Guinean Demographic and Health Surveys (DHS 2018). The DHS are nationally representative demographic and household surveys that collect data on a wide range of reproductive, maternal, and child health topics, such as fertility, health-seeking behaviors, and FP methods. A two-stage stratified cluster design was applied in survey sampling based on a list of enumeration areas (EAs) of the 2018 General Population Census of the Republic of Guinea. This study sample included sexually active adolescent and young women aged 15–24 years at the time of the survey. The survey covered the populations living in the strata of Guinea's eight administrative regions (Conakry, Boke, Faranah, Kankan, Kindia, Labe, Mamou, and N’Zérékoré) in Guinea. Women with missing data on the outcome variable were excluded from the analyses.
Definition of variables
Outcome variable
The outcome coded in binary (1 = Yes for unmet need and 0 = No for not unmet need) was generated from a constructed the DHS dataset. Unmet need for contraception was defined as women who do not want to become pregnant but are not using any contraception among all sexually active adolescents and young women (4, 22). Those women include married and/or sexually active unmarried considered fecund but neither pregnant nor in postpartum amenorrhea, and willing to delay their next birth by at least 2 years or limit their pregnancies without using a modern method of FP. This definition includes those currently pregnant or in postpartum amenorrhea but whose current pregnancy or last birth was not desired (4, 22).
Independent variables
Individual- and community-level variables were considered as determinants of the unmet need for contraception for this analysis based on a literature review and in line with our multilevel analytic approach.
Individual-level variables included socio-demographic characteristics (age, level of education, marital status, quintile wealth number of living children, knowledge of modern contraceptive, and exposure to FP messages). For the need of our analyses, the participants' age was recoded into two age groups (15–19 years and 20–24 years). The women's level of education was also recoded into no formal education, primary, secondary, and higher level of education. The participants' marital status was defined as currently in union (married or living in the union) and not in union (single, divorced or widowed, or separated). In the past 6 months, exposure to family planning messages was defined as recalling a family planning message heard or seen from the media, including radio, television, or newspapers.
The women's economic status was measured through the household wealth index as defined in the DHS dataset. The DHS wealth index was calculated using economic status indicators that included the main assets available at the household level at the time of the survey. Wealth index quintiles were defined for each household (poorest, poor, middle, richer, and richest).
Community-level variables included residence (rural and urban), administrative region (Conakry, Kindia, Boké, Labé, Mamou, Faranah, Kankan, N'Zérékoré), religion (Muslim and Christian/Other), and ethnicity (Soussou, Peulh, Malinké, and Others).
Statistical analysis
The data were processed and analyzed using Stata version 16.1. Two levels of statistical analysis applied to the data. At the first level, we described individual and community characteristics and then obtained absolute numbers and weighted percentages of explanatory variables and the prevalence of unmet need for contraception among adolescent and young women. The purpose of weighting the sample data was to improve its representativeness regarding the study population’s size, distribution, and characteristics. We then described the prevalence of unmet need among adolescent and young women.
The second level of analysis consisted of using multilevel modeling to assess adolescents and young women’s individual and community characteristics associated with the unmet need for contraception. Before constructing our models, we first evaluated the collinearity between the independent variables. The purpose was to determine the suitability of the variables selected for inclusion in the analyses. As a rule of thumb in regression analyses, a mean Variance Inflation Factor (VIF) score <5 is tolerated. There was no multicollinearity (all VIF < 5). In contrast, a mean VIF score of 5–10 suggests that the regression coefficients could be mis-estimated (23). Mixed-effects logistic regression (fixed and random) was used for the multivariate analyses to explore the explanatory variables. Fixed effects were estimated using the logistic regression's adjusted odds ratio (AOR), and random effects were estimated using the intra-cluster correlation coefficient (ICC).
Four models were constructed. Model 0 included no independent variables. Model 1 had only individual-level characteristics, while Model 2 was based solely on community-level characteristics (cluster). Finally, a multilevel model (Model 3) was constructed by including the individual- and community-level characteristics. All analyses incorporated design adjustment using sampling weights, clustering, and stratification. Adjusted odds ratios (AORs) measuring the associations between the unmet need for contraception and various covariates were then calculated. A threshold of 5% was considered for all statistical analyses along with a 95% confidence interval (CI).
Results
Individual and community characteristics
Table 1 presents the individual and community characteristics of the study participants. A total of 2,197 sexually active adolescents and young women were included in the analyses (Figure 1). Of these, 1,310 (59.6%) were aged 20–24 years with the majority not currently married (86.3%) and with no formal education (63.4%). Approximately 7 out of 10 (67.0%) participants reported not being exposed to FP messages in the media. However, more than four-fifths (86.9%) reported being familiar with at least one modern method of contraception.
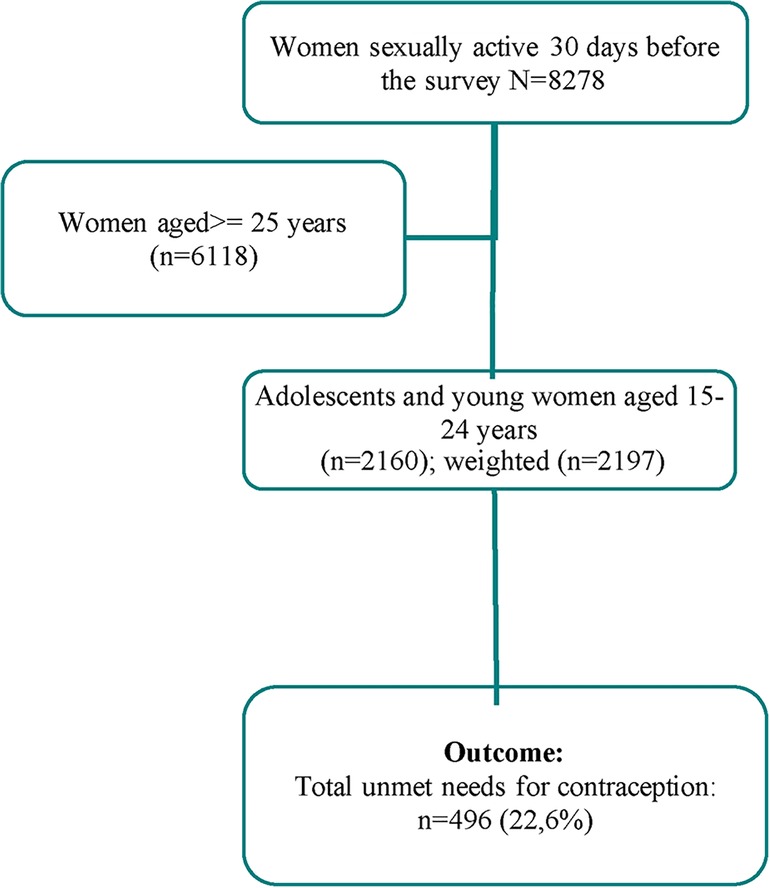
Figure 1. Flow chart of total number of adolescents and young women (aged 15–24), who were sexually active included in the analysis, 2018 Guinea.
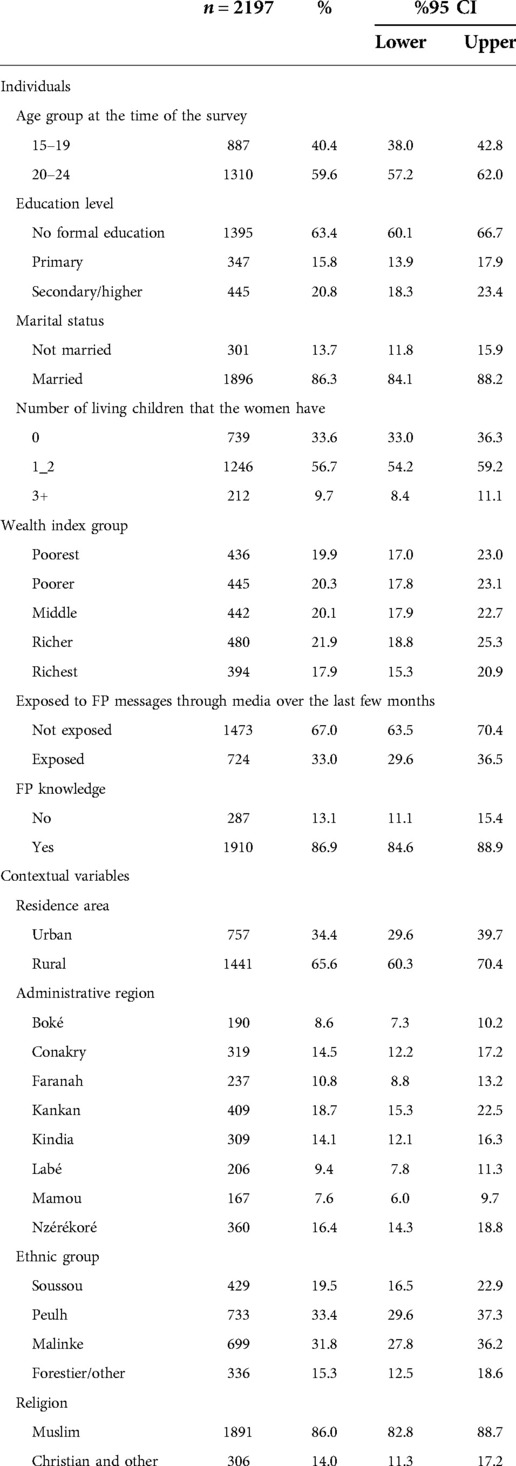
Table 1. Socio-demographic characteristics Adolescent and Young women (aged 15–24), 2018, Guinea.
The participants' community-level characteristics are also presented in Table 1. Overall, 65.6% of the adolescent and young women lived in rural areas, and 86.0% were Muslim.
Prevalence of total unmet need
The overall prevalence of unmet need for contraception among adolescents and young women aged 15–24 years was 22.6% (95% CI, 18.1–27.8). This prevalence was statistically significantly higher among adolescents and unmarried young women (38.5% vs 20.1%; p < 0.001). Other individual and community characteristics that appeared to have a higher prevalence of unmet need for contraception included the number of living children (p = 0.021) and administrative region (p < 0.001) (Table 2).
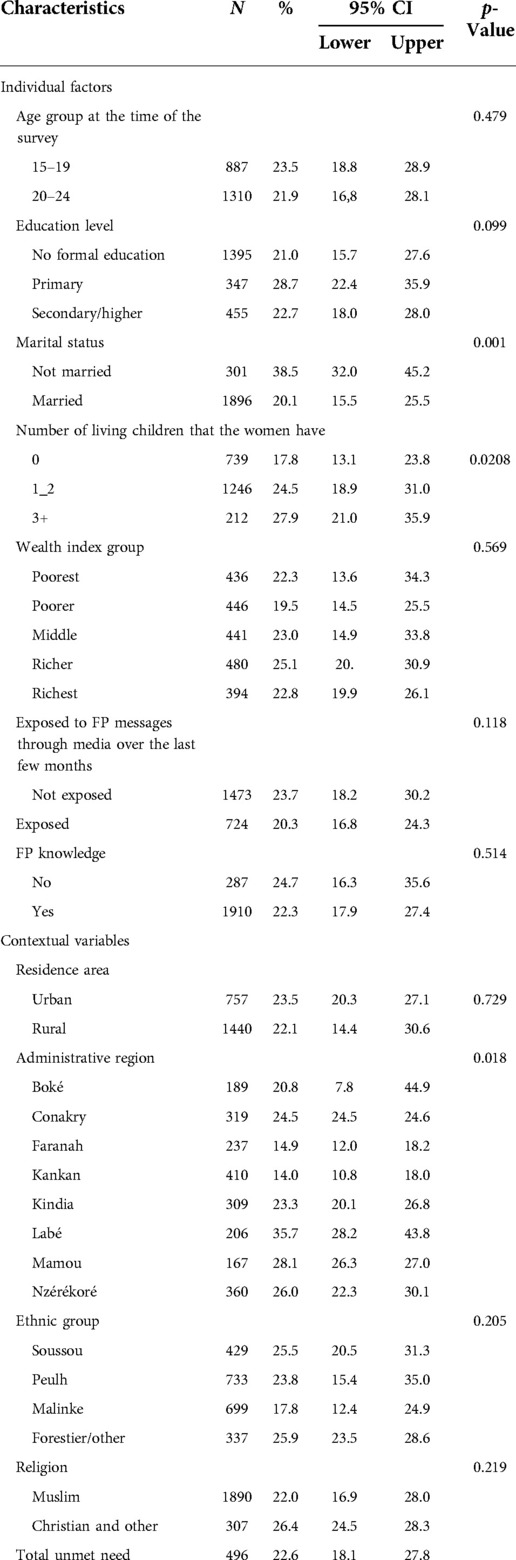
Table 2. Prevalence of total unmet need among sexually active old adolescent and young women aged 15–24 (n = 2197).
Multivariate analysis
Model 3 included both individual- and community-level characteristics (Tables 3, 4).

Table 3. Bivariate and multilevel logistic analysis of factors associated with total unmet need among sexually active old adolescent and young women aged 15–24—Guinea.
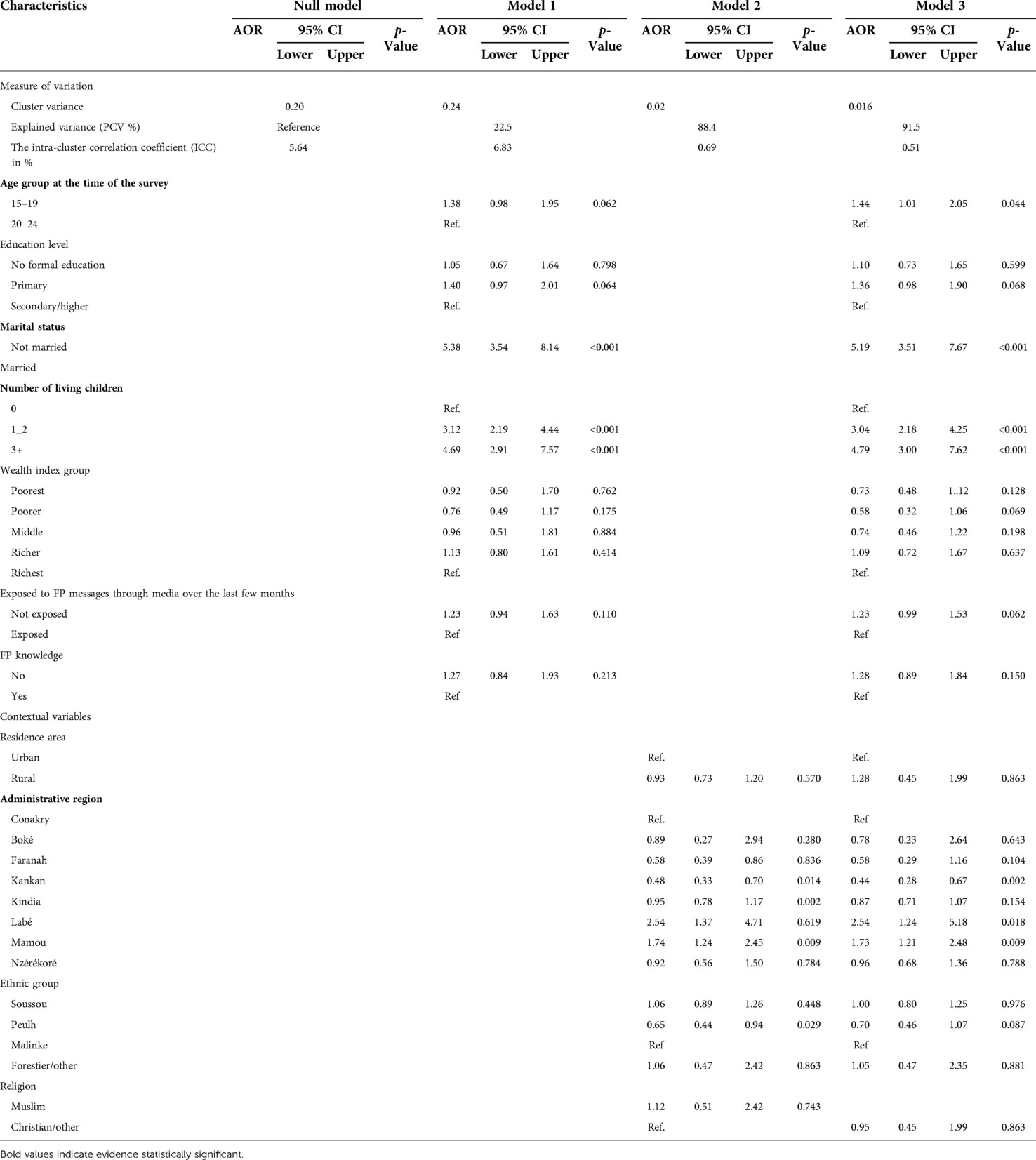
Table 4. Multilevel logistic analysis of factors associated with total unmet need among sexually active old adolescent and young women aged 15–24—Guinea.
After adjusting for individual- and community-level variables, the participants who were adolescents aged 15–19 years (AOR = 1.44; 95% CI, 1.01–2.05), not married (AOR = 5.19; 95% CI, 3.51–7.67), had one to two children (AOR = 3.04; 95% CI, 2.18–4.25) or had more than two children (AOR = 4.79; 95% CI, 3.00–7.62), from Labe (AOR = 2.54, 95% CI, 1.24–5.18) or from Mamou (AOR = 1.73, 95% CI, 1.21–2.48), compared to their counterparts, were more likely to have an unmet need for contraception (Table 3).
Introducing both individual- and community-level characteristics in the model reduced the ICC by 9.15% [(0.196931–0.0169404) * 100/0. 0.196931]. Therefore, the study population characteristics included in our final model explain around 92% of the individual variation in unmet need among adolescents and young women in Guinea (Table 4).
Discussion
The study shows that more than one-fifth of adolescents or young women experienced unmet need for FP in Guinea in 2018. It also shows the higher prevalence among adolescents and unmarried young women, and the unmet need increased with the number of children had by women. The main factors associated with unmet need for contraception among the study population were age, marital status, number of children and administrative region.
The high prevalence (22.6%) of unmet need for contraception among our study participants is one of the factors hampering the achievement of the Sustainable Development Goals, i.e., reducing maternal and neonatal mortality and morbidity. Our results are consistent with those of Malawi (22.0%) (13), Mali (21.4%), and Burkina Faso (23.9%) (14). The observed results can be explained in part by a disparity in access to modern methods of contraception. Access to maternal, reproductive, and child health services was negatively affected by the Ebola epidemic in West Africa between 2014 and 2016 (24–25). Despite this, the country has developed a national plan to reposition FP (2014–2018) to improve access to and use of modern methods of FP, particularly among adolescents and young women (26). A budgeted national FP plan for Guinea 2019–2023 was also developed in 2018 to support these efforts. The plan focuses on FP awareness campaigns in the media and schools, integration of FP services into maternal health services (postabortion care and immunization services), and training of maternal health providers (21). Beyond such efforts, this study reveals the importance of supporting intervention plans adapted to each region and district's local context, emphasizing community engagement and participation, including men as partners.
In our study, adolescents aged 15–19 years were more likely to have an unmet need for contraception than young women aged 20–24 years. Our results confirm the findings reported in other studies conducted in Ghana, Ethiopia, and Zambia (27–30). These results could be explained by the fact that young women generally live in union with the desire to have children. In contrast, adolescent girls typically face stigma in communities about their sexual behavior when using health services outside of marriage. The strategy of improving community awareness and facilitating access to methods of contraception by considering women's real needs is essential to increasing the use of contraception among women in general. However, it is necessary to promote a dialogue between parents and their children on sexuality and the benefits of methods of contraception for birth control.
Marriage and the number of children are two critical aspects of community life in Africa. In our study, these two factors were statistically significantly associated with the unmet need for contraception. Adolescents and unmarried young women were more likely to have an unmet need for contraception. Even more, adolescents and young women who had one or two children and those who had three or more children were three and four times, respectively, more likely to have an unmet need for contraception. These women certainly do not need to limit their number of children. While Guinean women desire, on average, four children, the DHS 2018 (19) showed that the average number of children born alive among adolescents and young women is approximately one and two, respectively. Evidence from Ethiopia shows that the unmet need for contraception among these women are more for birth spacing (31). In the context where the newly married woman must demonstrate her fertility (32), adolescents and young women ever married would like to space out their last birth or current or next pregnancy by a few months or years. This explains the increase in unmet need for contraception with the number of children among the study population. Spacing births is a way for women to organize their socioeconomic life and their motherhood. Some studies report that nearly half of young married women in sub-Saharan Africa have an unmet need for contraception (31, 33–35). Reducing the unmet need for modern FP methods among adolescents and young women requires, therefore, local approaches that address married women’s access to methods of contraception that meet their birth spacing needs. In addition, the involvement of partners as key actors in the strategy will ensure durability.
Our results do not confirm that exposure to FP messages through the media significantly influences the unmet need for contraception among adolescents and young women. Indeed, participants not exposed to FP messages through the media were not significantly associated with the unmet need for contraception. Contrary results have been reported by other studies that found that women not exposed to media or counseling were more likely to have an unmet need for contraception than other women (12, 36–39).
We also found no statistical relationships between adolescents' level of education and young women's unmet need for contraception as expected. In fact, many studies in Africa show that women's use of contraception increases with her level of education (28, 30, 40, 41), particularly among adolescent girls (42–44). The lack of a statistical relationship observed in our study could be explained by more important factors such as the supply of methods of contraception, the costs associated with adopting a method of contraception, or the weight of community values that most influence access to and use of FP methods. In addition, our results show that more than half of the adolescents and young women had no formal education. The relatively low proportion of formally educated adolescents and young women has implications for their access to and use of health information. Therefore, efforts for reducing the unmet need for contraception among adolescents and young women should include improving women's access to education in general, resulting in their financial empowerment and strengthening their decision-making capacity regarding their fertility and better access to health information (31).
Strengths
This study has some strengths that need to be highlighted. It used a nationally representative sample that accounts for complex sampling procedures to examine the individual and community factors associated with the unmet need for contraception among adolescents and young women. In addition, it used a multivariable model that considers differences across communities to adjust for potential confounding factors. These findings could help the Ministry of Health and its partners to support public health interventions to improve adolescents and young women's reproductive health in Guinea. They also point to challenges to address in using modern methods of contraception among this targeted group.
Limitations
The present study has some limitations. First, the temporal relationship between the unmet need for FP among the study population with the covariate could not be established. Second, this study was solely based on variables related to women’s individual and community characteristics but did not include information related to the availability, accessibility, and quality of FP services for adolescents and young women. Moreover, the study did not analyze information related to the study population’s previous experiences of abortions, neonatal mortality, or adverse outcomes, for instance, which may highly influence their need for contraception.
Conclusion
The overall prevalence of unmet need for contraception remains high among adolescents and young women in Guinea. This study revealed individual- and community-level factors associated with the unmet need for contraception among this sexually active population group. These findings suggest that communication strategies for adolescents and young women to reduce the unmet need for contraception should emphasize sexual education and awareness campaigns through the media and venues where young women gather. In addition, individual counseling in sexual and reproductive health services should be better directed toward adolescents and young married women already having children, considering their individual and contextual characteristics.
Data availability statement
Publicly available datasets were analyzed in this study. These data can be found here: https://dhsprogram.com/data/available-datasets.cfm.
Ethics statement
Ethical approval was not needed since the DHS program conducted this study after obtaining ethical approval from the Guinea National Ethics Committee. However, to access and use the dataset, permission was obtained from demographic and health surveys through online request from https://www.dhsprogram.com.
Author contributions
SS, FMG, and AD conceptualized and designed the study protocol. SS, FMG, and AD designed the analysis plan. SS, FMG, and KK performed the data analyses, interpreted the results, and drafted the manuscript with inputs from AD, BSC, DK, and SK. All authors contributed to the article and approved the submitted version.
Funding
This research was part of a Research Scholarship provided by the International Union for the Scientific Study of Population (IUSSP) (grant no. OPP1179495) from the Bill & Melinda Gates Foundation. Additional funding to the lead author was provided by HRP Alliance, part of the UNDP-UNFPA-UNICEF-WHO-World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP), a cosponsored program executed by the World Health Organization (WHO), through a PhD Scholarship granted by Institut Africain de Santé Publique (IASP/USTA) of the Université Saint Thomas D'Aquin, Burkina Faso. Data analysis was supported by the Belgian DGD (ITM-Maferinyah Framework Agreement 4). This article represents the views of the named authors only and does not represent the views of the World Health Organization.
Acknowledgments
We would like to thank the Guinea National Institute of Statistics and the DHS Program for granting access to the datasets.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kantorová V, Wheldon MC, Ueffing P, Dasgupta ANZ. Estimating progress towards meeting women’s contraceptive needs in 185 countries: a Bayesian hierarchical modelling study. PLoS Med. (2020) 17(2):e1003026. doi: 10.1371/journal.pmed.1003026
2. 2019 UN. Family planning and the 2030 agenda for sustainable development (data booklet). New York: United Nations (2019).
3. United Nations 2017. United Nations, Department of Economic and Social Affairs, Population Division (2017). World Family Planning 2017 - Highlights (ST/ESA/SER.A/414). Available from: file:///Users/sidibesidikiba/Desktop/un_2017_worldfamilyplanning_highlights.pdf
4. Bradley SEK, Casterline JB. Understanding unmet need: history, theory, and measurement. Stud Fam Plann. (2014) 45(2):123–50. doi: 10.1111/j.1728-4465.2014.00381.x
5. Sedgh G, Bearak J, Singh S, Bankole A, Popinchalk A, Ganatra B, et al. Abortion incidence between 1990 and 2014: global, regional, and subregional levels and trends. Lancet. (2016) 388(10041):258–67. doi: 10.1016/S0140-6736(16)30380-4
6. Darroch J, Woog V, LS A. Adding it up: Costs and benefits of meeting the contraceptive needs of adolescents. New York: Guttmacher Institute (2016).
7. World Health Organization. Contraception. Evidence brief. Contraception enables people to make informed choices about their sexual and reproductive health. Geneva: WHO/RHR/19.18 (2019).
8. Pizzol D, Di Gennaro F, Boscardin C, Putoto G, Cuppini E, Pita G, et al. Teenage pregnancies in Mozambique: the experience of “Servicios Amigos dos Adolescentes” clinics in Beira. Afr J AIDS Res. (2018) 17(1):32–6. doi: 10.2989/16085906.2017.1405825
9. Mchunu G, Peltzer K, Tutshana B, Seutlwadi L. Adolescent pregnancy and associated factors in South African youth. Af Health Sci. (2013) 12(4):426–34. doi: 10.4314/ahs.v12i4.5
10. Santhya KG, Jejeebhoy SJ. Sexual and reproductive health and rights of adolescent girls: evidence from low- and middle-income countries. Glob Public Health. (2015) 10(2):189–221. doi: 10.1080/17441692.2014.986169
11. Starrs AM, Ezeh AC, Barker G, Basu A, Bertrand JT, Blum R, et al. Accelerate progress—sexual and reproductive health and rights for all: Report of the Guttmacher–Lancet Commission. Lancet. (2018) 391(10140):2642–92. doi: 10.1016/S0140-6736(18)30293-9
12. Nzokirishaka A, Itua I. Determinants of unmet need for family planning among married women of reproductive age in Burundi: a cross-sectional study. Contracept Reprod Med. (2018) 3(1):11. doi: 10.1186/s40834-018-0062-0
13. Nkoka O, Mphande WM, Ntenda PAM, Milanzi EB, Kanje V, Guo SJG. Multilevel analysis of factors associated with unmet need for family planning among Malawian women. BMC Public Health. (2020) 20(1):705. doi: 10.1186/s12889-020-08885-1
14. O’Regan A, Thompson G. Indicators of young women’s modern contraceptive use in Burkina Faso and Mali from Demographic and Health Survey data. Contracept Reprod Med. (2017) 2(1):26. doi: 10.1186/s40834-017-0053-6
15. Stats MA, Hill DR, Ndirias J. Knowledge and misconceptions surrounding family planning among Young Maasai women in Kenya. Glob Public Health. (2020) 15(12):1847–56. doi: 10.1080/17441692.2020.1788112
16. Aziz MM, Elgibaly O, Mohammed HM. Family planning perspectives and practices of married adolescent girls in rural Upper Egypt. Eur J Contracept Reprod Health Care. (2021) 26(3):214–20. doi: 10.1080/13625187.2021.1879781
17. Coulibaly M, Doukouré D, Kouamé J, Ayékoé IA, Mélèdje-Koumi MD, Malik S, et al. Obstacles socioculturels liés à l’utilisation de la contraception moderne en Côte d’Ivoire: Santé Publique. (2020) 32(4):389–97. doi: 10.3917/spub.204.0389
18. Mekonnen AG, Odo DB, Nigatu D. Adolescents’ contraceptive uptake in Ethiopia: a meta-analysis. BioMed Res Int. (2022) 2022:1–7. doi: 10.1155/2022/6104467
19. Institut National de la Statistique de Guinée. Enquête Démographique et de Santé (EDS) 2018-Indicateurs Cles. (2018).
20. Ministère de la Santé. Direction Nationale de la Santé Familiale et de la Nutrition. Plan d’action national de repositionnement de la planification familiale en Guinée 2014-2018. Guinée (2013).
21. Ministère de la Sante. Direction Nationale de la Sante familiale et de la Nutrition. Plan d’Action national budgétisé de planification familiale 2019-2023 de Guinée. (2018).
22. Bradley SEK, Croft TN, Fishel JD, Westoff CF. Revising unmet need for family planning. Calverton, MA: ICF International (2012).
23. Sohil F, Sohali MU, Shabbir J. An introduction to statistical learning with applications in R: by Gareth James, Daniela Witten, Trevor Hastie, and Robert Tibshirani, New York, Springer Science and Business Media, 2013, $41.98, eISBN: 978-1-4614-7137-7. Stat Theory Relat Fields. (2022) 6(1):87–87.
24. Leno NN, Delamou A, Koita Y, Diallo TS, Kaba A, Delvaux T, et al. Ebola virus disease outbreak in Guinea: what effects on prevention of mother-to-child transmission of HIV services? Reprod Health. (2018) 15(1):1–9. doi: 10.1186/s12978-017-0439-6
25. Delamou A, El Ayadi AM, Sidibe S, Delvaux T, Bienvenu S, Sandouno SD, et al.. services in Guinea : a retrospective observational cohort study. Lancet Glob Health. (2017) 5(4):e448–57. doi: 10.1016/S2214-109X(17)30078-5
27. Wulifan JK, Brenner S, Jahn A, De Allegri M. A scoping review on determinants of unmet need for family planning among women of reproductive age in low and middle income countries. BMC Women’s Health. (2016) 16(1):2. doi: 10.1186/s12905-015-0281-3
28. Guure C, Maya ET, Dery S, da-Costa Vrom B, Alotaibi RM, Rezk HR, et al. Factors influencing unmet need for family planning among Ghanaian married/union women: a multinomial mixed effects logistic regression modelling approach. Arch Public Health. (2019) 77(1):11. doi: 10.1186/s13690-019-0340-6
29. Hailemariam A, Haddis F. Factors affecting unmet need for family planning in southern nations, nationalities and peoples region, Ethiopia. Ethiop J Health Sci. (2011) 21(2):77–90. doi: 10.4314/ejhs.v21i2.69048
30. Imasiku ENS, Odimegwu CO, Adedini SA, Ononokpono DN. Variations in unmet need for contraception in Zambia: does ethnicity play a role? J Biosoc Sci. (2014) 46(3):294–315. doi: 10.1017/S0021932013000357
31. Dingeta T, Oljira L, Worku A, Berhane Y. Unmet need for contraception among young married women in eastern Ethiopia. Open Access J Contracept. (2019) 10:89–101. doi: 10.2147/OAJC.S227260
32. Chandra-Mouli V, McCarraher DR, Phillips SJ, Williamson NE, Hainsworth G. Contraception for adolescents in low and middle income countries: needs, barriers, and access. Reprod Health. (2014) 11(1):1. doi: 10.1186/1742-4755-11-1
33. Prata N, Weidert K, Sreenivas A. Meeting the need: youth and family planning in sub-Saharan Africa. Contraception. (2013) 88(1):83–90. doi: 10.1016/j.contraception.2012.10.001
34. Glinski A, Sexton M, Petroni S. Understanding the adolescent family planning evidence base. (2014).
35. Haider TL, Sharma M. Barriers to family planning and contraception uptake in Sub-Saharan Africa: a systematic review. Int Q Community Health Educ. (2013) 33(4):403–13. doi: 10.2190/IQ.33.4.g
36. Letamo G, Navaneetham K. Levels, trends and reasons for unmet need for family planning among married women in Botswana: a cross-sectional study. BMJ Open. (2015) 5(3):e006603. doi: 10.1136/bmjopen-2014-006603
37. Oginni AB, Ahonsi BA, Adebajo S. Trend and determinants of unmet need for family planning services among currently married women and sexually active unmarried women aged 15-49 in Nigeria (2003—2013). Afr Popul Stud. (2015) 29(1):1483. doi: 10.11564/29-1-694
38. Tiruneh FN, Chuang KY, Ntenda PAM, Chuang YC. Factors associated with contraceptive use and intention to use contraceptives among married women in Ethiopia. Women Health. (2016) 56(1):1–22. doi: 10.1080/03630242.2015.1074640
39. Genet E, Abeje G, Ejigu T. Determinants of unmet need for family planning among currently married women in Dangila town administration, Awi Zone, Amhara regional state; a cross sectional study. Reprod Health. (2015) 12(1):42. doi: 10.1186/s12978-015-0038-3
40. Fagbamigbe AF, Afolabi RF, Idemudia ES. Demand and unmet needs of contraception among sexually active in-union women in Nigeria: distribution, associated characteristics, barriers, and program implications. SAGE Open. (2018) 8(1):2158244017754023. doi: 10.1177/2158244017754023
41. Igwegbe O, Ugboaja O, Monago N. Prevalence and determinants of unmet need for family planning in Nnewi, South-East Nigeria. (2009) 1(8):325–9. doi: 10.5897/IJMMS.9000183
42. Nyarko SH. Prevalence and correlates of contraceptive use among female adolescents in Ghana. BMC Women’s Health. (2015) 15:60. doi: 10.1186/s12905-015-0221-2
Keywords: unmet need, multilevel analysis, adolescents and young women, demographic health survey, Guinea, contraception
Citation: Sidibé S, Grovogui FM, Kourouma K, Kolié D, Camara BS, Delamou A and Kouanda S (2022) Unmet need for contraception and its associated factors among adolescent and young women in Guinea: A multilevel analysis of the 2018 Demographic and Health Surveys. Front. Glob. Womens Health 3:932997. doi: 10.3389/fgwh.2022.932997
Received: 30 April 2022; Accepted: 10 October 2022;
Published: 17 November 2022.
Edited by:
Sarah Compton, University of Michigan, United StatesReviewed by:
Kwame Adu-Bonsaffoh, University of Ghana Medical School, GhanaKim Jonas, South African Medical Research Council, South Africa
© 2022 Sidibé, Grovogui, Kourouma, Kolié, Camara, Delamou and Kouanda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sidibe Sidikiba bGF5ZXNpZGlraWJhQGdtYWlsLmNvbQ==
Specialty Section: This article was submitted to Maternal Health, a section of the journal Frontiers in Global Women’s Health