 Bezawit Melak Fente1*†
Bezawit Melak Fente1*† Angwach Abrham Asnake2
Angwach Abrham Asnake2 Yohannes Mekuria Negussie3
Yohannes Mekuria Negussie3 Meklit Melaku Bezie4
Meklit Melaku Bezie4 Zufan Alamrie Asmare5
Zufan Alamrie Asmare5 Hiwot Altaye Asebe6
Hiwot Altaye Asebe6 Beminate Lemma Seifu6
Beminate Lemma Seifu6
- 1Department of General Midwifery, School of Midwifery, College of Medicine & Health Sciences, University of Gondar, Gondar, Ethiopia
- 2Department of Epidemiology and Biostatistics, School of Public Health, College of Medicine and Health Sciences, Wolaita Sodo University, Wolaita Sodo, Ethiopia
- 3Department of Medicine, Adama General Hospital and Medical College, Adama, Ethiopia
- 4Department of Public Health Officer, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
- 5Department of Ophthalmology, School of Medicine and Health Science, Debre Tabor University, Debre Tabor, Ethiopia
- 6Department of Public Health, College of Medicine and Health Sciences, Samara University, Samara, Ethiopia
Background: Abortions performed unsafely, unintended births, and missed and unwanted pregnancies are linked to discontinuation of contraception for reasons other than wanting to become pregnant, and these situations raise the risk of maternal morbidity and death. However, a study on the determination of factors contributing to contraceptive discontinuation in Tanzania is limited. Therefore, we aimed to investigate the prevalence and determinants of contraceptive discontinuation among reproductive-age women in Tanzania using recent Tanzania Demographic Health Surveys.
Method: A cross-sectional study was conducted using secondary data analysis from of 2022 Tanzania Demographic Health Survey (DHS). A total weighted sample of 6,467 reproductive-age women were included. To account for the clustering effects of DHS data and the binary nature of the outcome variable, a multilevel binary logistic regression model was applied. An adjusted odds ratio with a 95% confidence interval was reported to declare the statistical significance. In addition, the model that had the lowest deviance was the one that best fit the data.
Result: The prevalence of discontinuation for all contraceptive methods among reproductive-age women was 34% (95% CI: 31.3%, 34.7%). Women who age group of 20–29 years (AOR = 4.45, 95% CI: 1.11, 17.78), women with no formal education (AOR = 1.94, 95% CI: 1.71, 2.93), women having no children (AOR = 4.25, 95% CI: 3.47, 8.06) women who want another child (AOR = 1.89, 95% CI: 1.76, 3.46), distance to the health facility as a big problem (AOR = 2.43, 95% CI: 1.38, 4.26), rural residence (AOR = 1.67, 95% CI: 1.48, 3.23) Were factors strongly associated with contraceptives discontinuation.
Conclusion: Among women of reproductive age, the withdrawal of contraception was 34% and it was determined by several factors. Providing a variety of contraceptive techniques and spreading knowledge about family planning are the primary goals of contraceptive counseling. It is also suggested by prospective investigators to use primary data to address independent factors that were missing.
Introduction
Because family planning has a direct and indirect impact on maternal mortality, it is a vital component of safe motherhood programs (1). Effective contraceptive use may save up to 44% of maternal fatalities, according to studies and it is commonly known that unintended pregnancies influence maternal mortality and morbidity (2). Contraceptive discontinuation reduces the contraceptive utilization coverage and family planning program effectiveness, as well as contributes to undesired fertility (3). Reducing the number of methods of contraception that a client must choose from, along with giving them access to additional information, technical expertise, interpersonal relationships, follow-up and continuity mechanisms, and the right constellation of services, can all help to improve the quality of their overall care (4).
In some low- and middle-income countries (LMIC) rates of contraceptive discontinuation remain high and increasing, even among women who want to avoid pregnancy (5). Results from a 2012 meta-analysis of 60 DHS surveys, which combined all contraceptive methods across 25 LMICs showed that, of women who started using a contraceptive method, on average 38% stopped within the first year, and two-thirds (68%) stopped before 2 years (6). More than half of the women who stopped contraceptive use, had experienced contraceptive discontinuation or had method-related problems, and were still in need of an effective method to prevent unintended pregnancy (7, 8).
Contraceptive discontinuation is a worldwide public health concern in countries with low and middle incomes (9). An estimated 74 million women worldwide become pregnant each year without any prior planning (10). Unwanted pregnancies result from a variety of circumstances, such as inconsistent and improper use of methods of contraception, failure of contraceptives, termination of contraception, and non-use of contraception (6, 11). Discontinuing contraceptive use is characterized as beginning use and then ceasing for whatever reason while being at risk of an unplanned pregnancy (12).
Enhancing service delivery and user uptake of contraception requires an analysis of the causes of discontinuation of contraceptives. For instance, it was discovered that two-thirds of sexually active women who did not wish to become pregnant discontinued due to fear of side effects, health issues, and underestimating the chance of conception (13, 14). Discontinuation because of side effects, may suggest the need for improved counseling and communication (15). Other reported reasons for discontinuation include accessibility to contraceptives, cost of services, opposition and religious beliefs as well as misunderstanding of how to use the contraceptives (12, 16).
Numerous variables may influence the decision to continue or stop using contraceptives, like as; the age of the woman, number of living children (parity), desired number of children, having television and radios, decision-maker to use contraceptives, husband/partner support, perceived benefit to the FP, perceived contraceptive harm, duration of contraceptive use, counseling on FP and contraceptive side effects, experience of side effects, access and availability different type of contraceptive (3, 17–29).
There have been studies into the identification of factors associated with contraceptive use in Tanzania, but as to our search of the literature, there is limited study on the prevalence and associated factors of contraceptive discontinuation among reproductive-age women in Tanzania (30). The findings of this study can provide direction for policymakers, programmers, healthcare providers, and other stakeholders about the impact of contraceptive discontinuations on morbidity and mortality. This study's findings strongly advocated for women's empowerment, partner involvement in the decision-making process around contraception use, and easy access to high-quality counseling regarding the possible negative consequences and alternative birth control methods. To meet the SDGs that aim to reduce maternal mortality of children, policymakers, programmers, and other stak eholders will be better equipped to support family planning and other health intervention initiatives. Therefore, this study investigated the prevalence of contraceptive discontinuation and associated factors among reproductive-age women in Tanzania.
Methods and materials
Data source and sampling procedure
This study was based on the Demographic and Health Survey (DHS) of Tanzania. The Tanzania Demographic and Health Survey (TDHS) is conducted every five years to generate updated health and health-related indicators. The data were derived from the measure DHS program and detailed information about the surveys can be found in each country's DHS reports. The sample design for the 2022 TDHS was carried out in two stages. In the first stage, 629 Enumeration Areas (EAs) were recruited; 211 were from urban areas and 418 were from rural areas. Second stage, 26 households were selected. All women aged 15–49 who were either usual residents or visitors in the household on the night before the survey were eligible to be interviewed in the 2022 TDHS. The sampling frame excluded institutional populations, such as persons in hospitals, hotels, barracks, camps, hostels, and prisons. There are different datasets in DHS, and for this study, we used the Individual Record (IR) file. The dependent and independent variables were extracted from the IR dataset, based on the literature. The final weighted sample size was 6,467.
Study variables
Dependent variable
The outcome variable for this study was modern contraceptive discontinuation (yes/no) among reproductive-age women (women aged 15–49 years), which is measured as the percentage of reproductive-age women who used a method of contraception in the last 12 months before the survey but were not using a method at the time of data collection (19, 25, 29).
Independent variables
Individual level variables respondent's age, occupation, education, marital status, husband's fertility desire, women's fertility preference, decision maker on contraceptive use, number of living children, history of visiting health facility, heard about family planning, household head sex, wealth status, and media exposure on family planning. All of those variables were selected based on the literature review from previous studies. We have categorized respondent age based on the previous literature but other variables were categorized by the DHS data initially.
Community-level variables in addition to place of residence, to assess affect group-level variation which is the community-level poverty and education level of the community were included. Community-level variables are calculated based on the number of clusters included in the study. The community level variable and the clustered are run together in the Stata. The value of those two variables' proportion was calculated in an Excel spreadsheet to get the community-level variable, and then it was dichotomized based on the normality. Finally, mean and median were used for normal and skewed distribution respectively.
Statistical analyses
Descriptive analysis was performed using frequency and percentage distributions to examine the characteristics of respondents and contraceptive discontinuation. This was followed by bivariate multilevel logistic regression to select variables that had a significant association with contraceptive discontinuation at a p-value less than 0.05. A multicollinearity test was performed using variance inflation factor (VIF) for all statistically significant variables at the bivariate multilevel logistic regression. Using the Multilevel Logistic Regression (MLLR) method, we created four different models to assess whether the individual/household and community-level factors had significant associations with the outcome variable (contraceptive discontinuation). The first model was a null model (Model 0), which had no explanatory variables and it showed variance in contraceptive discontinuation. The second model (Model I) comprised individual/household-level factors and the third model (Model II) comprised community-level factors. The last model, (Model III), was the complete model that included factors at both the individual/household and community levels.
All four MLLR models included fixed and random effects (31, 32). The fixed-effect model showed the association between the explanatory variables and the outcome variable, and the random effects signified the measure of variation in the outcome variable based on the primary sampling unit, which was measured by Intra-Cluster Correlation (ICC) (33). The model ft. was assessed using the Akaike's Information Criterion (AIC) (34). We used the “melogit” command to run the MLLR models. The analyses were performed using Stata version-14 software (Stata Corp, College Station, Texas, USA). We also followed the guidelines for Strengthening Observational studies in Epidemiology (STROBE) (35).
Result
Background characteristics of respondents
A total of 6,467 women 5 years preceding the survey were included in this study. About 2,208(36.21%)women were found in the age groups of 20–29 years followed by the age groups of 30–39 years 1,663 (25.72%). Most women (61.12%) lived in rural areas, and nearly half of women (46%) had attained primary education. The majority of women (36.9%) had jobs, more than half of women (60%) were married, and (56.37%) of women heard about family planning (Table 1).
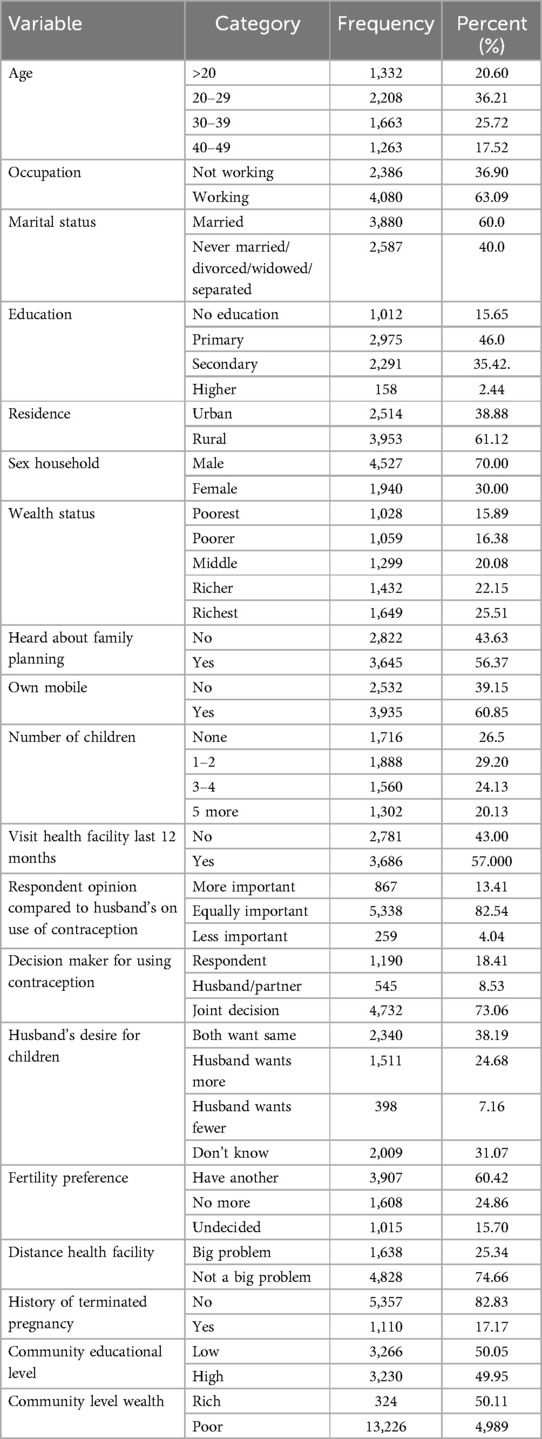
Table 1. Socio-demographic, reproductive, and obstetric characteristics of reproductive-age women in Tanzania, TDHS 2022 (weighted).
Prevalence of contraceptive discontinuation
The prevalence of contraceptive discontinuation among women of reproductive age in Tanzania was 34% with a 95% CI (31.3%, 37.6%). The most common reasons given for discontinuing the contraceptive method were the desire to become pregnant, side effect concerns, wanting more of an effective method, husband/partner disapproval, unexpected conception, and other concerns. More than two-thirds (36.4%) of women who discontinued contraceptive use desired to become pregnant, (12.7%%) of discontinuations were due to changes in menstrual bleeding (19.3%) were concerned about the other side effects, and wanted a more effective method (Table 2).
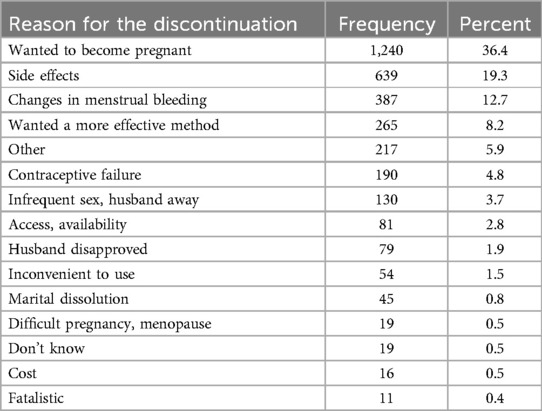
Table 2. Reasons for discontinuation of contraceptives.
Factors associated with contraceptive discontinuation
In the multivariable mixed effect binary logistic regression model, women's age, women's education status, women need more children (fertility preference), and distance from health facility significant individual factors while the place of residence was found to be a statistically significant factor from community-level factors of contraceptive discontinuation among Tanzanian reproductive age women.
Women in who age group of 20–29 years are 4.45 times more likely to discontinue contraceptives (AOR = 4.45 CI: 1.11, 17.78). Women with no formal education were 1.94 times more likely to discontinue contraceptives (AOR = 1.94, 95% CI: 1.71, 2.93). Women having no children (AOR = 4.25, 95% CI: 3.47, 8.06) were 4.25 times more likely to discontinue contraceptives compared to women with five or more children. In addition, women who reported that wanted another child were nearly two times more likely to discontinue contraception (AOR = 1.89, 95% CI: 1.76, 3.46) than those not want more children. The odds of discontinuing contraceptives among women who perceived the distance to the health facility as a big problem was increased by 2.43 times (AOR = 2.43, 95% CI: 1.38, 4.26) than women who perceived the distance to the health facility as not a big problem. Women with rural residences were 1.67 times more likely to discontinue contraceptives (AOR = 1.67, 95% CI: 1.48, 3.23) compared to those women with urban residences (Table 3).
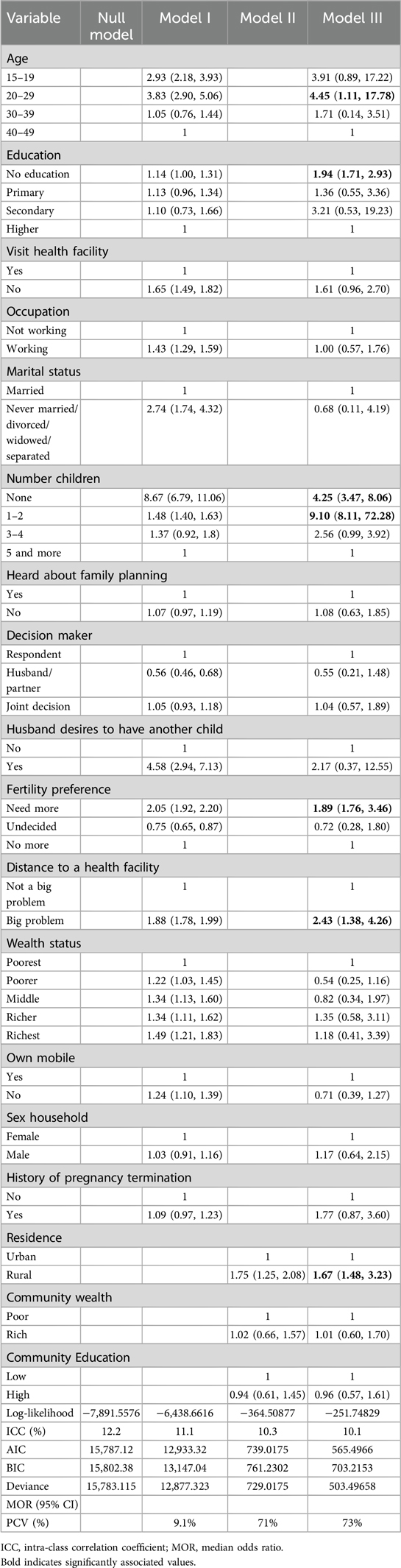
Table 3. Multilevel analysis of factors associated with contraceptive discontinuation and random effect among reproductive-age women in Tanzania, 2022 (N = 6,467).
Random effects (measures of variations) results
The random effect models of the individual/household and community-level factors associated with contraceptive discontinuation are shown in (Table 3). We observed that the values of the AIC and deviance decreased across the models, indicating the best-fitted model was chosen based on the lowest deviance value (503.49658) and AIC (565.966). The ICC in the null model (ICC = 12.2%) showed that the odds of contraceptive discontinuation varied across clusters. The between-cluster variations decreased by 1.1% in the model I, from 12.2% in the null model to 11.1% in the model I. From model I, the ICC decreased again by 2% in model II (ICC = 1.3%) and then declined by 2.1% in the complete model (model III, ICC = 10.1%. These estimates showed that the variations in the likelihood of contraceptive discontinuation can be attributed to the variances in the clustering at the primary sampling units (Table 3).
Discussion
In this study, we investigated contraceptive discontinuation and its individual/household and community-level factors among women of reproductive age using a recent Tanzanian nationally representative dataset. According to the current study; 34% with 95% CI (31.3%, 37.6%). of Tanzanian women who started an episode of contraceptive use preceding TDHS were discontinued within 12 months. It was consistent with studies reported in Southeast Ethiopia which showed that about 2 of women discontinue contraceptives (28). This finding was higher than the DHS survey conducted from 34 countries, which reported a discontinuation rate of 19% (14), and Kenya's 30.5% in 2014 DHS (26), which reported the prevalence of contraceptive discontinuations, However, this finding is lower than study findings from 60 surveys in 25 countries with a discontinuation rate of 38% (28), analysis of Bangladesh DHS with 38.4% (24), Myanmar with 38% (22), Ethiopia (46.1%) (29), and rural Bangladesh (36%) (36). This variation may result from variations in reproductive health services, such as information, counseling, and education that can improve women's comprehensive knowledge of FP, the accessibility and readily accessible nature of various FP methods, and the development of easy and secure services for users of contraceptives. Furthermore, socio-demographic differences, norms, beliefs, and other cultural differences may be the reason for the discrepancy. The study period, sample size, study population, and sampling technique may be the additional cause.
According to this study, the rate of younger women discontinuing any kind of contraception was higher. This finding is consistent with research from Bangladesh (24), and Ghana (37). Our results are not surprising, as the highest levels of fertility are typically found in younger women. Put in another context, as these women are more likely to have started actively producing children, they are also more likely to have stopped taking contraception if they had previously used it.
In this study, women who lived in a rural residence were 1.75 times more likely to discontinue contraceptives compared with those living in an urban residence. This result is supported by other studies (24, 25). This may be explained by the fact that women in the countryside have limited access to services for family planning and reproductive health information (6). Similarly, women who perceived distance to reach health facilities as a big problem had higher odds of discontinuing contraceptives than those who perceived it as not a big problem. It can be explained that women who had poor healthcare access might not use family planning services.
Women with no formal education were two times more likely to discontinue contraceptives. This is also similar to other findings (3, 24, 25, 37). The reason might be that women with no formal education have been deprived of autonomy to make decisions on reproductive health issues including when to use contraceptives. Women who had no children or fewer than three children were more likely to discontinue contraceptives than their counterparts. This finding is supported by other studies (18, 22, 25, 28). The reason might be that women may need to have children to attain their desired number of children; thus they might prefer to discontinue contraceptives.
Another significant predictor of discontinuing contraceptives was women who want more children This was consistent with previous studies (19). This can be because women stop using contraceptives because they want to have more children. This study can provide great information for the policymakers and for the Tanzanian health facilities to improve the morbidity and mortality related to contraceptive discontinuations.
Strengths and limitations of the study
One of the study's advantages was that it used data from a large nationwide survey, which gave it sufficient power to identify the real impact of the independent factors. Secondly, in order to obtain accurate estimates and standard errors, the sample weight was applied during the analysis. Furthermore, by examining the appropriate cessation of contraceptives at the household, and community levels, we were able to investigate hierarchical or clustered patterns that might have an impact on results. One weakness of the study is that it was cross-sectional in nature; therefore it was not possible to establish a causal relationship between the identified independent variables and the discontinuation of contraceptives. Because it depends on self-reported data, the DHS is vulnerable to recall bias.
Conclusion
Contraceptive discontinuation among reproductive-aged women was 34%in Tanzania in this study. Age, educational status, number of children, women's fertility preference, and distance from health facility were significantly associted factors from individual-leve variables while place of residence was significant associated factor from community-level variable with contraceptive discontinuation. Improving family planning awareness through comprehensive reproductive education or counseling could be one of the operational ways to reduce contraceptive discontinuation. Counseling on contraceptives usually focuses on disseminating information on family planning and providing a range of contraceptive methods. Initiation of a contraceptive method has been linked to a lower risk of unplanned pregnancy. Future researchers are also recommended to use advanced or fellow up study to predict the exact cause and effect relationship.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
BF: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AA: Data curation, Investigation, Methodology, Software, Validation, Visualization, Writing – review & editing. YM: Data curation, Investigation, Methodology, Software, Validation, Visualization, Writing – review & editing. MM: Data curation, Investigation, Software, Supervision, Validation, Visualization, Writing – review & editing. ZA: Data curation, Investigation, Methodology, Software, Validation, Visualization, Writing – review & editing. HA: Data curation, Investigation, Methodology, Software, Validation, Visualization, Writing – review & editing. BS: Data curation, Investigation, Methodology, Software, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to thank Measure DHS for their permission to access the TDHS datasets.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AIC, Akaiki's Information Criteria; BIC, Bayesian Information Criteria; DHS, Demographic Health Survey; TDHS, Tanzanian Demographic Health Survey; ICC, Intra-Cluster Correlation Coefficient; IOR, Interval Odds Ratio; MLRM, Multilevel Logistic Regression Model; MOR, Median Odds Ratio; PCV, Proportional Change in Variance; VIF, Variance Inflation Factor; WHO, World Health Organization.
References
1. Brown W, Druce N, Bunting J, Radloff S, Koroma D, Gupta S, et al. Developing the “120 by 20” goal for the global FP2020 initiative. Stud Fam Plann. (2014) 45(1):73–84. doi: 10.1111/j.1728-4465.2014.00377.x
2. Ahmed S, Li Q, Liu L, Tsui AO. Maternal deaths averted by contraceptive use: an analysis of 172 countries. Lancet. (2012) 380(9837):111–25. doi: 10.1016/S0140-6736(12)60478-4
3. Ouédraogo AM, Baguiya A, Compaoré R, Cissé K, Dahourou DL, Somé A, et al. Predictors of contraceptive method discontinuation among adolescent and young women in three West African countries (Burkina Faso, Mali, and Niger). BMC women's Health. (2021) 21(1):1–13. doi: 10.1186/s12905-021-01326-0
4. Nayak SR, Mohanty SK, Mahapatra B, Sahoo U. Spatial heterogeneity in discontinuation of modern spacing method in districts of India. Reprod Health. (2021) 18(1):137. doi: 10.1186/s12978-021-01185-w
5. World Health Organization, Contraception discontinuation and switching in developing countries. Research policy brief (2012).
6. Ali MM, Cleland JG, Shah IH. Causes and consequences of contraceptive discontinuation: evidence from 60 demographic and health surveys (2012).
7. Castle S, Askew I. Population council. Contraceptive discontinuation: reasons, challenges, and solutions (2015).
8. Castle S, Askew I. Contraceptive discontinuation: reasons, challenges, and solutions. New York, NY. (2015). Available at: https://scholar.google.com/citations?user=u6xBeDYAAAAJ&hl=en&oi=sra (Accessed April 15, 2024).
10. World Health Organization, High Rates of Unintended Pregnancies Linked to Gaps in Family Planning Services: New WHO Study, World Health Organization, Switzerland (2020).
11. Wellings K, Brima N, Sadler K, Copas AJ, McDaid L, Mercer CH, et al. Stopping and switching contraceptive methods: findings from contessa, a prospective longitudinal study of women of reproductive age in England. Contraception. (2015) 91(1):57–66. doi: 10.1016/j.contraception.2014.09.008
12. Bellizzi S, Mannava P, Nagai M, Sobel HL. Reasons for discontinuation of contraception among women with a current unintended pregnancy in 36 low and middle-income countries. Contraception. (2020) 101(1):26–33. doi: 10.1016/j.contraception.2019.09.006
13. Gemmill A, Sarnak D, Bradley SEK, Brecker E, Patierno K. Reproductive outcomes following contraceptive discontinuation for method-related reasons: an analysis of 49 demographic and health surveys. PLOS Global Public Health. (2023) 3(11):e0002143. doi: 10.1371/journal.pgph.0002143
14. Jain AK, Obare F, RamaRao S, Askew I. Reducing unmet need by supporting women with met need. Int Perspect Sex Reprod Health. (2013) 39(3):133–41. doi: 10.1363/3913313
15. Hossain MB, Phillips JF. The impact of outreach on the continuity of contraceptive use in rural Bangladesh. Stud Fam Plann. (1996) 27(2):98–106. doi: 10.2307/2138137
16. Casterline JB, El-Zanatay F, El-Zeini LO. Unmet need and unintended fertility: longitudinal evidence from upper Egypt. Int Fam Plan Perspect. (2003) 29(4):158–66. doi: 10.2307/3181044
17. Ali M, Cleland J. Determinants of contraceptive discontinuation in six developing countries. J Biosoc Sci. (1999) 31(3):343–60. doi: 10.1017/S0021932099003430
18. Belete N, Zemene A, Hagos H, Yekoye A. Prevalence and factors associated with modern contraceptive discontinuation among reproductive age group women, a community based cross-sectional study in Humera town, northern Ethiopia. BMC Women's Health. (2018) 18:1–8. doi: 10.1186/s12905-018-0663-4
19. Dadzie LK, Seidu A-A, Ahinkorah BO, Tetteh JK, Salihu T, Okyere J, et al. Contraceptive discontinuation among women of reproductive age in Papua New Guinea. Contracept Reprod Med. (2022) 7(1):8. doi: 10.1186/s40834-022-00170-3
20. Ersek JL, Brunner Huber LR, Thompson ME, Warren-Findlow J. Satisfaction and discontinuation of contraception by contraceptive method among university women. Matern Child Health J. (2011) 15(4):497–506. doi: 10.1007/s10995-010-0610-y
21. Fekadu GA, Omigbodun AO, Roberts OA, Yalew AW. Factors associated with early long-acting reversible contraceptives discontinuation in Ethiopia: evidence from the 2016 Ethiopian demographic and health survey. Arch Public Health. (2020) 78:1–10. doi: 10.1186/s13690-020-00419-w
22. Khaing Nwe Tin KNT, Thae Maung Maung TMM, Thiri Win TW. Factors that affect the discontinuation of family planning methods in Myanmar: analysis of the 2015–16 Myanmar Demographic and Health Survey (2019).
23. Kisuza RK, Kicaber S, Abila DB, Bongomin F, Garimoi CO. Prevalence of discontinuation of contraceptives due to failure among women aged 14 to 49 years in Uganda: a nation wide cross-sectional survey. Contracept Reprod Med. (2023) 8(1):1–11. doi: 10.1186/s40834-022-00210-y
24. Mahumud RA, Hossain G, Sarkar AR, Islam N, Hossain R, Saw Aik S, et al. Prevalence and associated factors of contraceptive discontinuation and switching among Bangladeshi married women of reproductive age. Open Access J Contracept. (2015) 6:13–9. doi: 10.2147/OAJC.S76070
25. Mekonnen BD, Wubneh CA. Prevalence and associated factors of contraceptive discontinuation among reproductive-age women in Ethiopia: using 2016 nationwide survey data. Reprod Health. (2020) 17(1):1–10. doi: 10.1186/s12978-020-01032-4
26. Ontiri S, Were V, Kabue M, Biesma-Blanco R, Stekelenburg J. Patterns and determinants of modern contraceptive discontinuation among women of reproductive age: analysis of Kenya demographic health surveys, 2003–2014. PLoS One. (2020) 15(11):e0241605. doi: 10.1371/journal.pone.0241605
27. Thobani R, Jessani S, Azam I, Reza S, Sami N, Rozi S, et al. Factors associated with the discontinuation of modern methods of contraception in the low income areas of Sukh Initiative Karachi: a community-based case control study. PLoS One. (2019) 14(7):e0218952. doi: 10.1371/journal.pone.0218952
28. Tolesa Bekele TB, Alem Gebremariam AG, Papelon Tura PT. Factors associated with contraceptive discontinuation in Agarfa district, Bale Zone, south east Ethiopia (2015).
29. Weldemariam KT, Gezae KE, Abebe HT. Reasons and multilevel factors associated with unscheduled contraceptive use discontinuation in Ethiopia: evidence from Ethiopian demographic and health survey 2016. BMC Public Health. (2019) 19:1–15. doi: 10.1186/s12889-019-8088-z
30. Safari W, Urassa M, Mtenga B, Changalucha J, Beard J, Church K, et al. Contraceptive use and discontinuation among women in rural North-West Tanzania. Contracept Reprod Med. (2019) 4(1):18. doi: 10.1186/s40834-019-0100-6
31. Austin PC, Merlo J. Intermediate and advanced topics in multilevel logistic regression analysis. Stat Med. (2017) 36(20):3257–77. doi: 10.1002/sim.7336
32. Gelman A, Hill J. Data Analysis Using Regression and Multilevel/hierarchical Models. Cambridge: Cambridge University Press (2006).
33. Perinetti G. Statips part IV: selection, interpretation and reporting of the intraclass correlation coefficient. South Eur J Orthod Dentofac Res. (2018) 5(1):3–5. doi: 10.5937/sejodr4-1283
34. Acquah Hd-G, Comparison of Akaike information criterion (AIC) and Bayesian information criterion (BIC) in selection of an asymmetric price relationship (2010).
35. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. (2014) 12(12):1495–9. doi: 10.1016/j.ijsu.2014.07.013
36. Callahan RL, Becker S. The reliability of calendar data for reporting contraceptive use: evidence from rural Bangladesh. Stud Fam Plann. (2012) 43(3):213–22. doi: 10.1111/j.1728-4465.2012.00319.x
Keywords: prevalence, contraceptive, determinants, discontinuation, women, TDHS 2022, Tanzania
Citation: Fente BM, Asnake AA, Mekuria Negussie Y, Melaku Bezie M, Alamrie Asmare Z, Asebe HA and Seifu BL (2025) Prevalence and determinants of contraceptive discontinuation among reproductive age women: analysis of Tanzania demographic health survey. Front. Glob. Women's Health 6:1393020. doi: 10.3389/fgwh.2025.1393020
Received: 8 May 2024; Accepted: 25 March 2025;
Published: 11 April 2025.
Edited by:
Emmanuel Senanu Komla Morhe, University of Health and Allied Sciences, GhanaReviewed by:
Amy Finnegan, IntraHealth International, United StatesDesmond Klu, University of Health and Allied Sciences, Ghana
Copyright: © 2025 Fente, Asnake, Mekuria Negussie, Melaku Bezie, Alamrie Asmare, Asebe and Seifu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bezawit Melak Fente, YmV6YXdpdG1lbGFrMjAxMUBnbWFpbC5jb20=
†ORCID:
Bezawit Melak Fente
orcid.org/0009-0008-9574-2299