 Monira Parvin Moon
Monira Parvin Moon- Department of Rural Development, Gazipur Agricultural University (GAU), Gazipur, Bangladesh
Background: Married Bangladeshi women of reproductive age have improved their contraceptive use in recent decades. This review study searched PubMed, Scopus, and Google Scholar to examine how age and education affect Bangladeshi women's contraceptive behaviors.
Results: Modern approaches were most used by 15–19-year-olds. Between 2011 and 2017–2018, fewer educated women read a newspaper or magazine at least once a week, suggesting older women watch more TV. Over time, elderly adults utilize none of the three media at least once a week. According to the findings, elderly women are the least likely to receive weekly media coverage of their contraceptive treatments. In short, the study found that younger women utilize current contraceptive techniques, while older women may employ them less frequently, and better education significantly enhances contraceptive use, as there is a strong correlation between educational attainment and the utilization of contraception. Moreover, the results indicated that women who were not exposed to the media were less likely than those who were to use contemporary techniques.
Conclusion: The report strongly recommends improving the education of disadvantaged people, particularly Bangladeshi women. To boost the nation's usage of contraceptives, women need effective health behavior education, family planning, and counseling programs.
Highlights
• There are age-related influences on contraceptive use among women.
• Contraceptive methods among women are influenced by education.
• Media influences women's use of contraception in Bangladesh.
Introduction
Contraceptive behavior is a significant public health concern globally, especially for women (1–3). The term “contraception” originally referred to a method of birth control (4). Rahman et al. (5) and Haq et al. (6) found contraception effective for family planning and fertility control, but approximately 200 million women worldwide struggle with safe and effective methods. Bangladesh's contraception prevalence rate (CPR) has plateaued, as, having increased to 61.0% in 2011, it was 62.4% in 2014 and 62.0% in 2017 (7). Subsequently, increasing the prevalence of contraception in Bangladesh from 62% to 75% by 2020 was one of the primary goals (8). Reproductive health outcomes in underdeveloped nations are also influenced by a woman's capacity for decision-making (9–11). Bangladesh has made progress in health and family welfare, but reproductive and sexual healthcare access remains challenging, with increased contraceptive use being a goal of various organizations and sectors (5, 6). To achieve this, 69 of the world's poorest countries established the Family Planning agenda in the wake of the 2012 London Summit on Family Planning. The agenda aims to provide 120 million more women and girls in 69 of the world's poorest countries with access to family planning information, services, and supplies by 2020 (8, 9). Contraception is now used by 64% of married or cohabiting women worldwide between the ages of 15 and 49, but it is only used by 40% in the least developed countries (12, 13).
Bangladesh has made notable progress in terms of the percentage of married women of reproductive age who take contraceptives, increasing from 8% in 1975 to 62% in 2014 (14). Further benefits include reducing health risks related to pregnancy and maternal death, improving perinatal outcomes for newborns and infant mortality, empowering individuals, and enhancing education when population growth and contraceptive use are reduced (15, 16). Contemporary forms of contraception encompass oral contraceptive pills, implants, injectable contraceptives, contraceptive patches, rings, intrauterine devices (IUDs), and condoms. The conventional contraceptive methods encompass the rhythm technique and coitus interruptus (15). These persistent public health issues in low- and middle-income countries (LMICs) significantly contribute to the increased prevalence of unplanned pregnancies, shorter intervals between pregnancies, and a greater rate of pregnancy terminations (17). The availability of contemporary contraceptive methods, as opposed to the absence or use of traditional contraceptive methods, can effectively tackle these concerns by empowering women to exert autonomy over their reproductive decisions, allowing them to space pregnancies and strategically schedule childbirth (18). Bangladesh's prevalence of contraceptive use (62%) is higher than that of other South Asian countries, such as India (58%), Nepal (50%), Pakistan (35%), and Afghanistan (23%), but it is still very close to the global prevalence of contraception (64%). The usage of contraceptives by Bangladeshi women was likewise linked to a preference for boys (19).
Previous studies conducted in Bangladesh have found that several sociodemographic considerations, such as age, education, and the wealth of the household, are strongly linked to contraceptive use (6, 20). Although previous research has examined the determinants of modern contraceptive use, only a small number of studies have considered both traditional and modern approaches (6, 21, 22). Nevertheless, contraceptive use, as a binary outcome variable, was analyzed using binary logistic regression in these investigations. Understanding the factors associated with the use and selection of contraceptive techniques is crucial, as the current use of these methods is suboptimal (20). Bangladeshi women use both modern and traditional contraceptive methods, highlighting the need for a deeper understanding of the factors influencing their use (22, 23). Furthermore, because a high contraceptive prevalence rate is always expected for birth control in densely populated areas like Bangladesh, it is vital to periodically assess prevalence and risk factors to monitor the current situation. Consequently, this study will help to fill the gaps in the literature. Therefore, this study investigates the prevalence of contraceptive behaviors and media influence among women in Bangladesh, with the effects of age and education from the Bangladesh Demographic and Health Survey (BDHS) (24–26).
Methodology
Search strategy
Following PRISMA criteria, the study used data from the 1993 to 2024 Bangladesh Demographic and Health Surveys and searched PubMed, Scopus, Google Scholar, and peer-reviewed publications for related studies (27). The study searched for articles on Bangladeshi women's contraceptive habits and media influence based on age and education.
The key search terms for this study were as follows: “Reproductive Health,” “Contraceptive use,” “developing countries,” “contraception,” “family planning,” “Women Autonomy and fertility,” “Decision-making Autonomy,” “Fertility Preferences,” “Media exposure to contraception,” “systematic reviews,” and “Bangladesh” (Table 1).
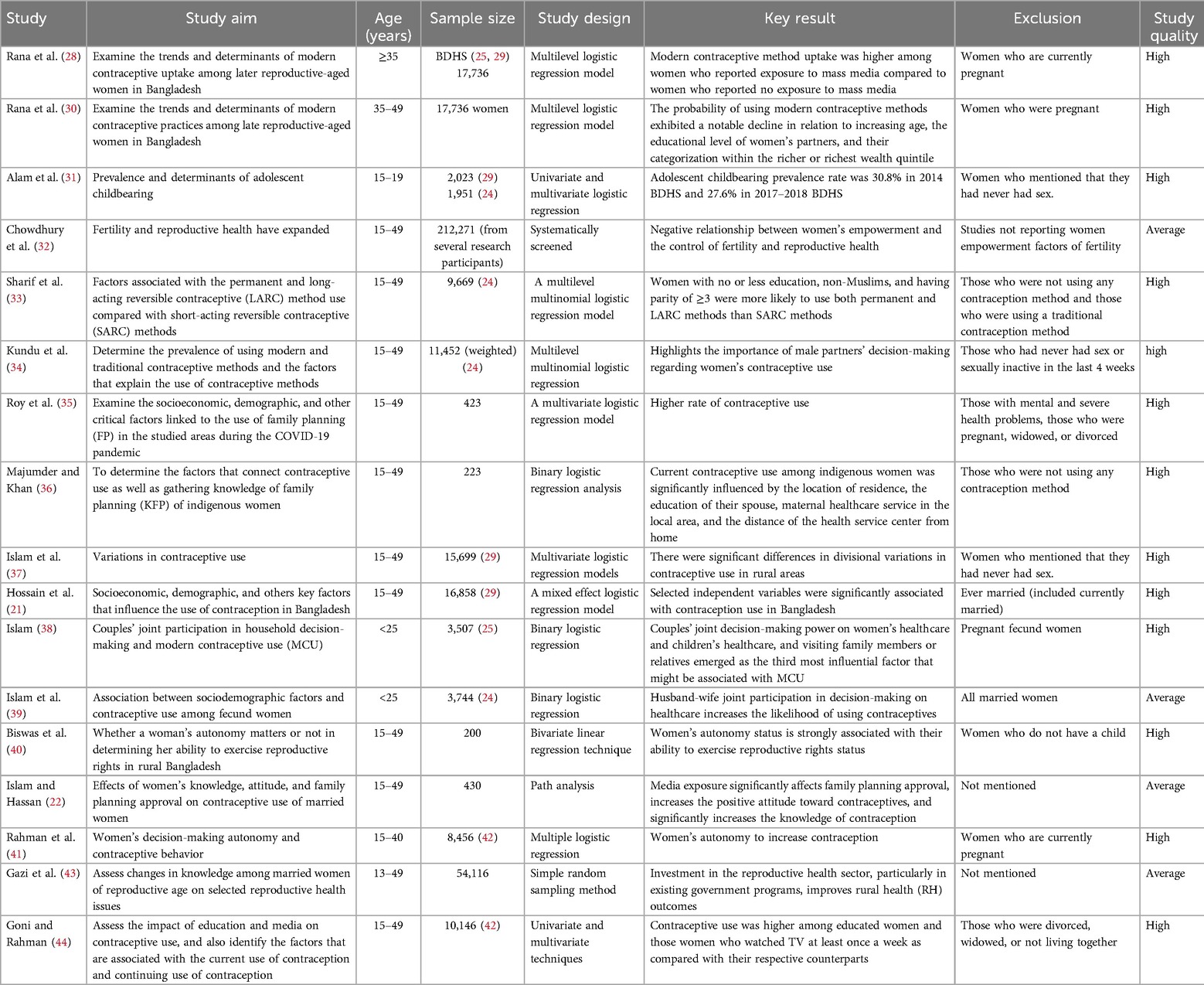
Table 1. Relevant studies on contraceptive behaviors among women in Bangladesh.
Research questions identification
Iterative research idea generation was described by Arksey and O'Malley (45). The research questions have been presented in Figure 1, which will lead this study.
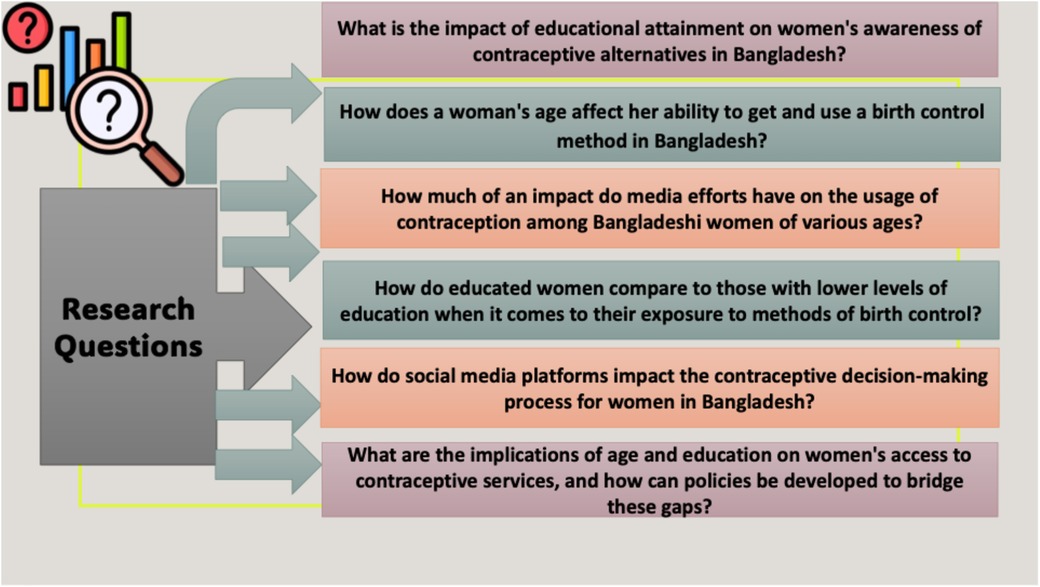
Figure 1. Research questions for the study.
Identification and screening
The reference lists of every article that was chosen were also examined. A total of 3,310 papers were initially identified through the systematic search and an additional 55 articles were discovered by searching different databases. Among the 3,010 publications that were assessed, 2,900 were excluded after abstract screening. A total of 210 full-text articles were evaluated to determine whether or not they were eligible for inclusion in this study. Five such articles were chosen to be included in the review of references. Following careful consideration of a number of aspects, a final selection of 17 articles was made for additional research. In total, 198 full-text articles were disregarded for a variety of reasons, including but not limited to: substandard quality (86), unavailable primary data (19), absence of intervention (11), not aligning with the prescribed conceptual framework (26), and being conference papers (17). After removing 198 full-text articles, the study identified 12 articles that were incorporated into the review of cited records (5). Ultimately, 17 pertinent publications were selected for the synthesized review (Figure 2). Table 1 describes the 17 studies on contraceptive behaviors among women in Bangladesh, along with the aim, age group, sample size, study design, key results, exclusions, and study quality. The majority of the noteworthy results were linked to the following: women's autonomy status is strongly associated with their ability to exercise their reproductive rights status; contraceptive use was higher among educated women; and media exposure significantly affects family planning approval, increases positive attitudes toward contraception, and significantly increases knowledge about contraception.
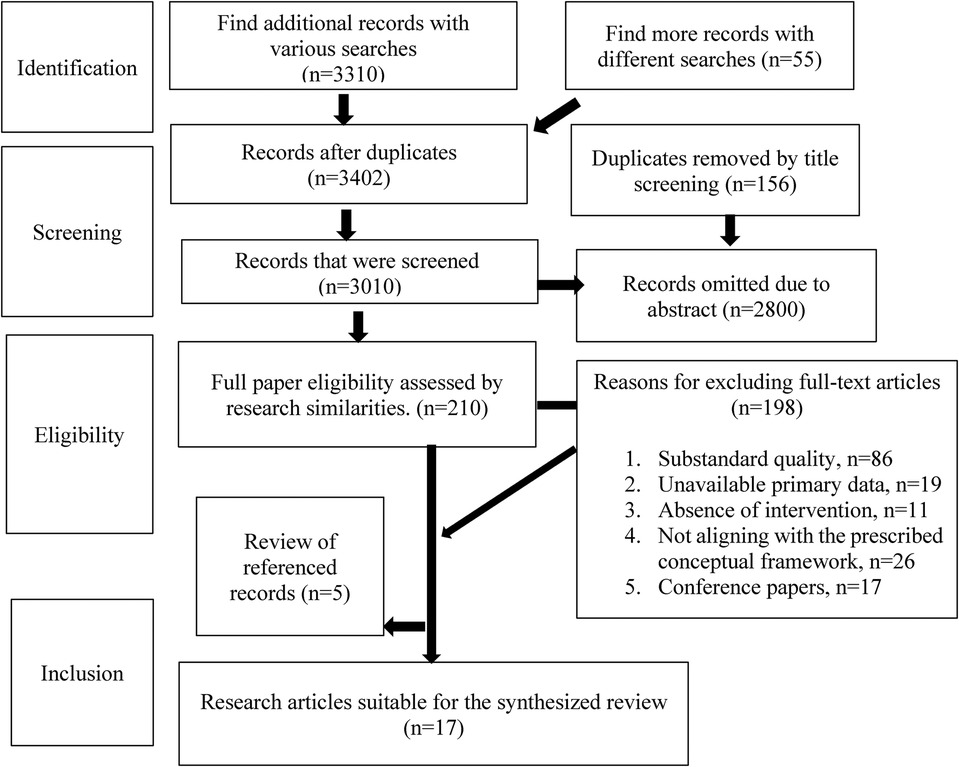
Figure 2. PRISMA flowchart for the systematic review.
Study selection criteria
For current studies of contraceptive behaviors and media influence among women in Bangladesh, we used extensive inclusion and exclusion criteria. The review included studies on women and excluded studies that included men. In addition, reports from other developing and developed nations are included to allow for comparing the actual pictures of the contraceptive behaviors and media influence among women. In addition, only articles written in English have been included.
Extracting data
The extraction process was carried out using data from the 1993 to 2024 Bangladesh Demographic and Health Surveys and from searches of PubMed, Scopus, Google Scholar, and peer-reviewed publications for related studies. The PRISMA method has been used to explore the contraceptive behaviors and media influence among women in Bangladesh.
Results and discussion
The CPR increased slightly from 61.2% in the 2011 BDHS to 62.4% in the 2014 BDHS, according to the BDHS data (14). After controlling for other variables, Kibria et al. (46) found no link between the use of contraceptives and a variety of variables, including the working status of women and spouses’ education level. This finding is significant because earlier studies (47, 48) have found a relationship between these characteristics and the use of contraceptives. Figure 3 represents the contraception prevalence rate from 1993 to 2022, showing eight types of practices, including any method, any modern method, pill, injectables, condom, female sterilization, male sterilization, and condom. The study showed that the prevalence of any method (64%), any modern method (54.7%), and use of condom practices (8.1%) significantly increased from 1993 to 2022 in Bangladesh. Using the pill (highest 28.5%), injectables (highest 12.4%), and male sterilization had fluctuations. In contrast, using female sterilization (highest 8.1%) and IUDs (highest 2.2%) had a significant decrease over the years.
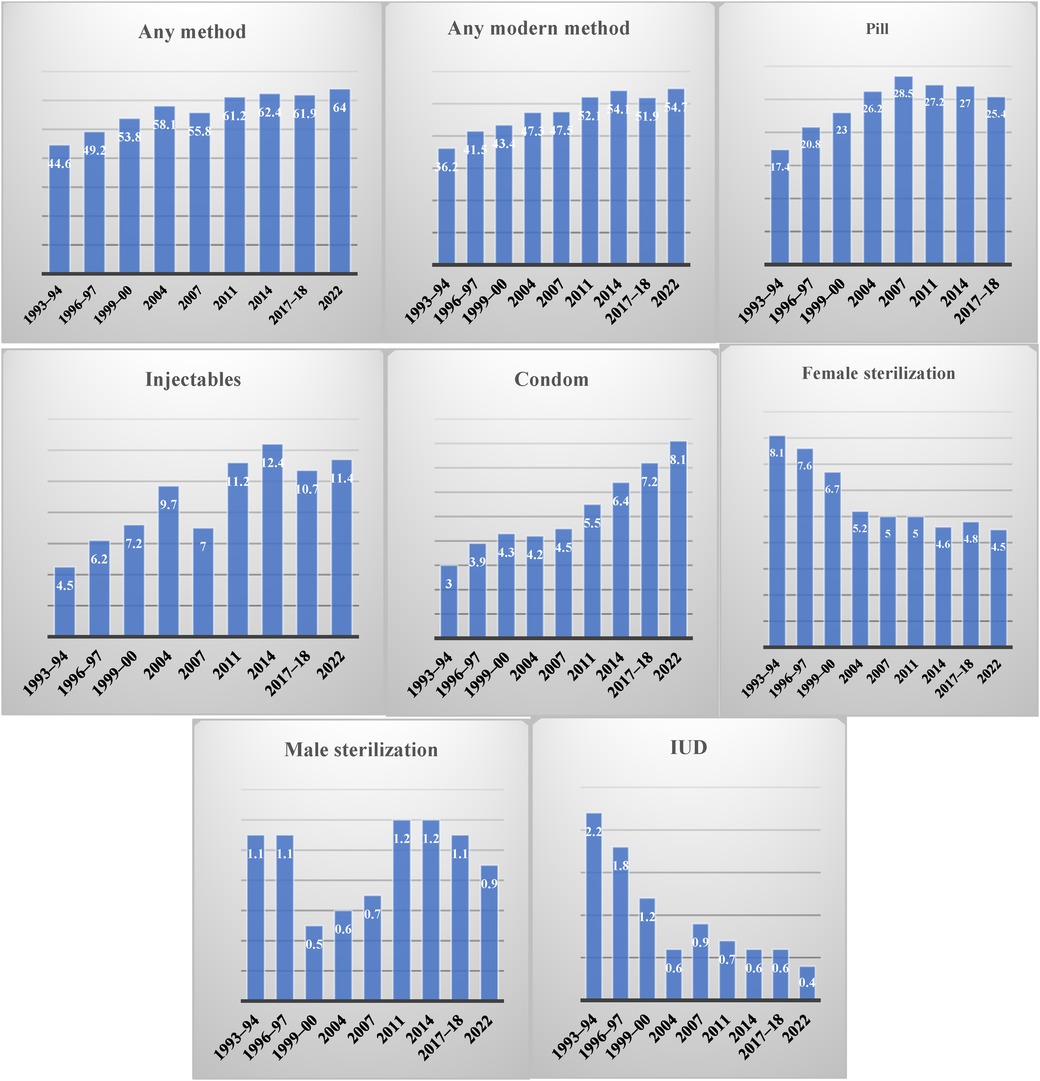
Figure 3. CPR from 1993 to 2022 in Bangladesh.
Age-specific CPR currently in use
The probability of using CPR decreased as age increased and rose as age at marriage increased among fertile women under 25 years old. Hence, the creation of service centers accessible to young individuals in suitable locations and the provision of necessary resources would effectively promote the utilization of reproductive health services among young people (49). Figure 4 shows the data for current use of contraception by age using the data from BDHS (24, 25, 29, 50), showing three categories including any modern method, any traditional method, and not currently using. The CPR was 64% among married women aged 15–49, with 55% using modern techniques and 9% using traditional methods. In 2022, any modern method and any traditional method had a fluctuation. The prevalence of any modern method was highest in the age group 15–19 in 2022 (48.1%), and it was lowest for the age group of 35–39, while it had a significant decrease in the 45–49 age group. However, the prevalence of any traditional methods was highest for the 45–49 age group (15.3%) and lowest for the 15–19 age group (5.8%). Similarly, for 2017–2018, 2014, and 2011, this study found that the prevalence of the use of any modern methods was higher among the 15–19 age group, while the use of any traditional method was the lowest in this age group. A common explanation for why fewer older women were using birth control is their declining fertility, whereas fewer younger women using it is often associated with their desire to have more children (44). Among women aged 25–34, the use of modern methods of contraception was most prevalent, with almost two-thirds of women reporting doing so (34). This study's results are consistent with those of a previous study by Forty et al. (51) that found that adolescent girls and women are more likely to plan to use contraception. Haq et al. (6) also found that the usage of contraceptives decreases with age, which suggests that older women are less likely to utilize contraceptives than their younger counterparts. Similar to the findings of another study that has already been conducted (52), this kind of association between age and the use of contraceptives has been identified. Among women of all age categories, the pill was the most commonly utilized contraceptive technique, with the exception among those aged 45–49, who were more inclined to practice intermittent abstention. Research by Hossain et al. (21) revealed a comparable trend among women aged 30–49 who had a higher likelihood of undergoing sterilization compared to younger women. In a cross-sectional study conducted in the Narsingdi District in the Dhaka division, Islam (53) similarly documented comparable findings, indicating that the prevalence rate of contraception was lower among younger women as compared to older women. Contraception may be used less frequently by older women because they are less likely to engage in sexual activity or have decreased the frequency of their sexual encounters. In contrast, younger women may not desire to have children at such a young age (51).
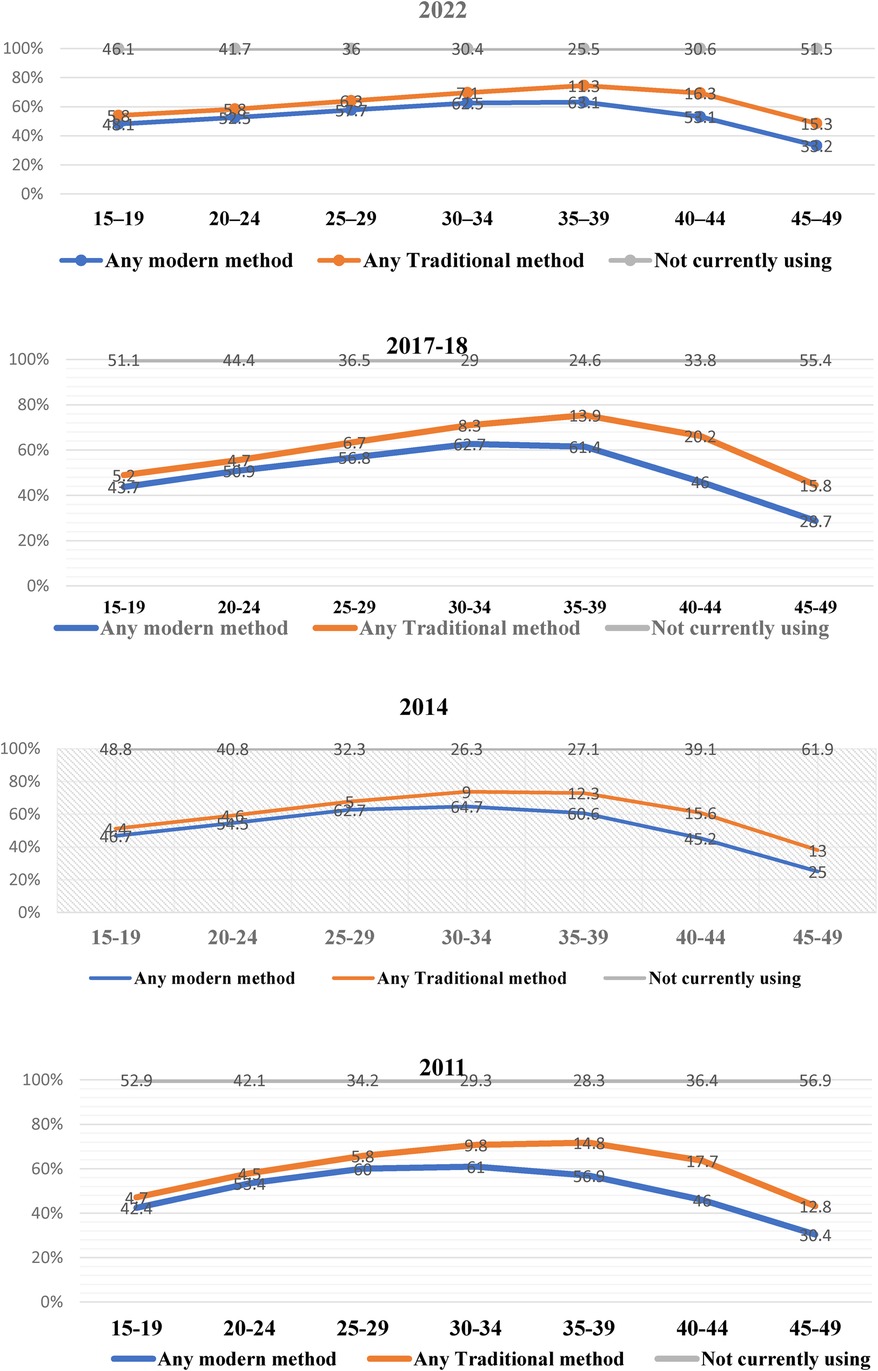
Figure 4. Age-specific CPR currently in use from the BDHS (24–26, 50). The proportion of married women aged 15–49 using contraceptives by age.
Numerous studies have shown that the use of contraception can significantly decrease fertility rates and eventually enhance the health of both mothers and children. However, the rate of not using any contraception was constant over the periods of 2022, 2017–2018, 2014, and 2011. The study conducted by Rana et al. (28) revealed that over 54% of women aged 35 and above do not utilize contemporary contraceptive techniques. Furthermore, there have been no notable changes in their utilization during the years investigated. The likelihood of modern contraceptive method adoption was shown to be lower among women aged 40–45 and 45–49 compared to those aged 35–39. According to Kundu et al. (34), the prevalence of contemporary contraceptive techniques among women in Bangladesh was 72.16%, while traditional methods were utilized by 14.58% of women. The reluctance to utilize modern contraceptive techniques was higher among older women (35–49 years) compared to women in the 15–24 years age group.
Present status of CPR in the field of education level
It has been found that when women have access to quality education, they are more likely to be receptive to novel family planning methods (54). Furthermore, women who have completed a greater number of years of schooling are more likely to have professional or other forms of work, which may cause them to be less inclined to have a large family. Among Bangladeshi women, those with higher levels of education were more likely to use birth control than those with lower levels of education (49). Furthermore, the results indicate that women who had completed elementary school education had a greater likelihood of utilizing contraceptives compared to their uneducated counterparts. These findings align with prior research that has demonstrated a comparable correlation between educational level and contraceptive usage (55–58). Education empowers women to make independent decisions regarding fertility-related issues and also enhances their ability to exercise their reproductive health rights, in contrast to women who have received limited education. Furthermore, women who have acquired an education are likely to have a more thorough understanding of the benefits of using contraception to reduce unintended pregnancies compared to women who lack education. Thus, it is crucial for family planning service providers to give priority and address the needs of women who have little or no education during family planning interventions. Such would empower individuals to obtain essential knowledge on reproductive health, hence improving their acceptance of contraceptive methods.
Figure 5 shows the current use of CPR by education over the years from the BDHS (24, 25, 29, 50). The figure indicates that the use of any contraceptive method among women with no educational background in the years of 2011, 2014, 2017–2018, and 2022 was 61.4%, 61.5%, 62.5%, and 62.6%, respectively. Among the respondents with a primary education, the prevalence of any modern method, male sterilization, implants, and withdrawal increased. A prior study (20) provided evidence that young girls and women were more inclined to intend to use contraception, which supports the results of our study. Furthermore, Haq et al. (6) examined the correlation between women who had received an elementary education and those with secondary and higher levels of education, and their propensity to take contraceptives, in comparison with women with no education. A reason for this is that an increased level of education can offer the chance to acquire more knowledge about contraceptive methods and ensure improved availability of services. However, the prevalence of using an IUD, injectables, male condoms, any traditional method, other methods, and not currently using contraception among the respondents with incomplete primary education decreased.
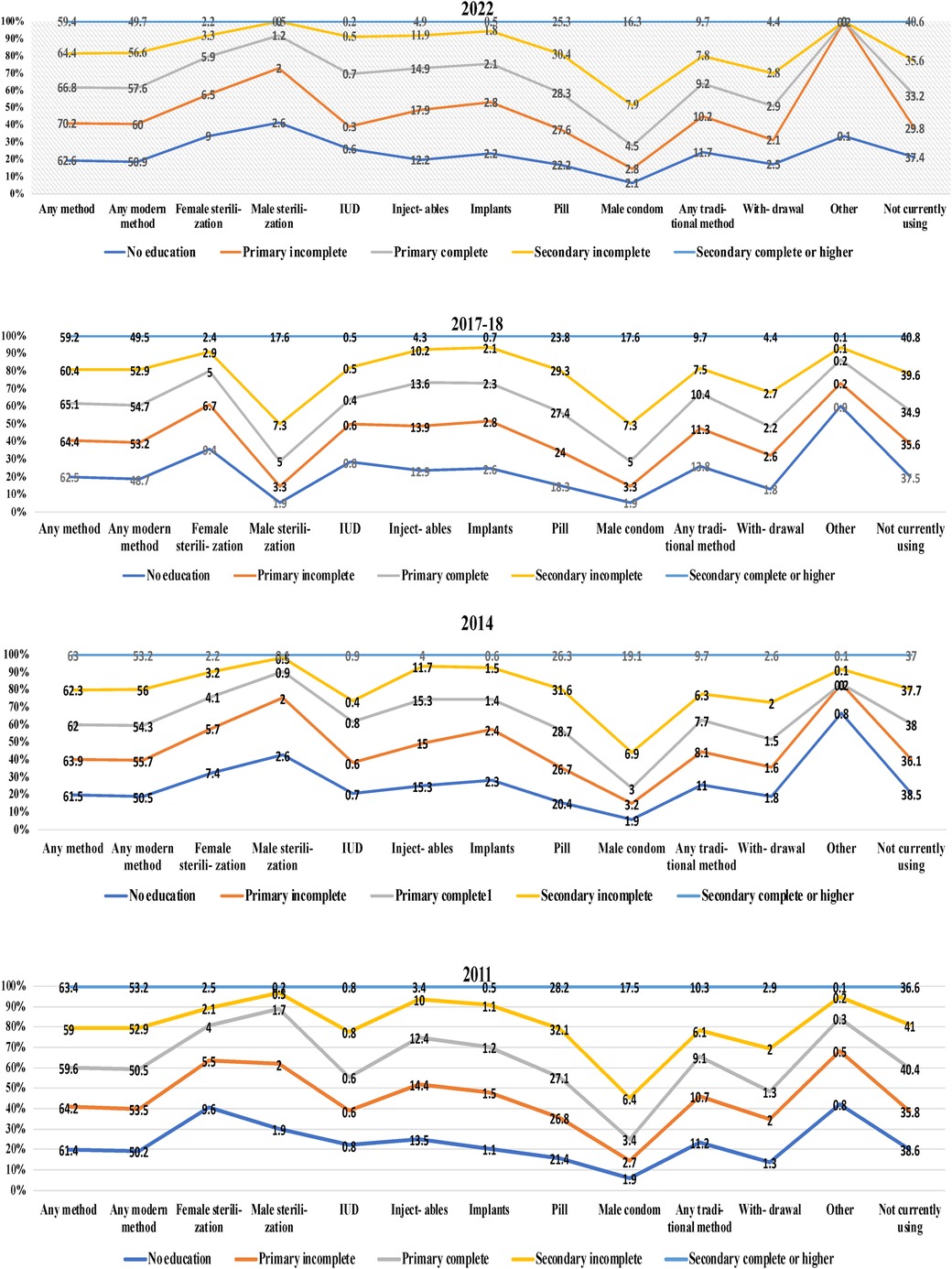
Figure 5. Present status of the CPR by education. Distribution of current contraceptive methods among married women in Bangladesh in 2022, 2017–2018, 2014, and 2011 according to education data from the BDHS.
The percentage of individuals in the complete primary education group who used any technique, any modern method, female sterilization, injectables, pills, male condoms, and withdrawal while they were using an IUD increased, whereas the percentage of individuals who used any method decreased. However, the use of any traditional method and other methods did not change. Among those with a secondary education, the use of any method, any modern method, female sterilization, male condom, any traditional method, and withdrawal increased from 2011 to 2022, while the use of male sterilization, IUD, injectables, and pills, and not currently using a contraception method decreased, and others were constant from 2011 to 2022. Ultimately, data revealed that possessing a secondary education or higher maintained a consistent perspective on activities across the years. Thus, from this figure, we can depict that the current use of contraception has increased over the years due to education. In the research carried out by Hossain et al. (21), it was discovered that 72% of the individuals who took part in the study were employing modern methods of birth control. This is an increase from the 62% of women in Bangladesh who were using these methods in 2014. The utilization of conventional methods of birth control has also reached 14.6% in this survey, which is in accordance with the present study. In 2014, this percentage was just 8.1%. According to Hossain et al. (21), in 2014, over 37% of Bangladeshi women did not make use of any method of birth control. However, according to recently conducted research, this figure has dropped to 13%. To achieve a contraceptive prevalence of 75% by the year 2020, the Health, Population and Nutrition Sector Development Programme (HPNSDP) of Bangladesh established strategic objectives to improve the overall utilization of family planning. These objectives were designed to ensure that family planning services are accessible, affordable, and acceptable to all men and women who are in their reproductive years (8, 59).
Education, contraception use, and reproductive practices are linked, and highly educated women are more active in childbearing decisions (60). Kabir et al. (61) found that women with higher education used contemporary contraceptives more, rising by 3% over time. Over time, women's employment status, husband's education, number of live children, and fertility desires decreased modern contraceptive use. Illiterate women used contraception less than educated women. Higher education greatly boosts contraception use (62, 70). Educational achievement is strongly connected with contraceptive use. Fleischer (63) states that a woman's education affects fertility management and contraceptive use. Women with higher levels of education are more likely to use contemporary contraception, according to research by Hossain et al. (64) and Pazol et al. (65). They concluded that women have more control over their reproductive health, family planning decisions, and access to contraception when they receive more education. More access to education, particularly in rural areas, could help reduce the population of Bangladesh by increasing the number of women who utilize contraception. There is evidence from research conducted by Gurmu and Tariku (66), Howlader et al. (67), and Tamirat et al. (68) that suggests that women who have a higher level of education are less likely to engage in risky reproductive behaviors in comparison to women who have a lower level of education. Educated women utilize modern birth control more than uneducated women because more educated women know about and can use modern contraception (69).
Exposure to various forms of mass media with CPR
Exposure to mass media, such as radio and television, has an important influence on reproductive behavior. Figure 6 illustrates the percentage of ever-married women aged 15–49 who were exposed to specific media on a weekly basis according to age and education from BDHS (24–26). The figure shows that women aged between 25 and 29 read a newspaper or magazine at least once a week, which is the highest, while women aged between 15 and 19 had the lowest percentage at 3.7% and 1.6% for 2017–2018, respectively. The findings of Haq et al. (6) showed a noteworthy correlation between the utilization of contraceptive methods and being exposed to family planning information in the media. In each of the three studies, the findings indicated that there was a large amount of exposure to messages about family planning through the various kinds of mass media. This finding is consistent with the findings of previous research carried out in Bangladesh (85). Women who had no exposure to mass media were less likely to employ modern methods than those who had exposure to media (49). This was the case among the respondents who were asked about their usage of modern methods.
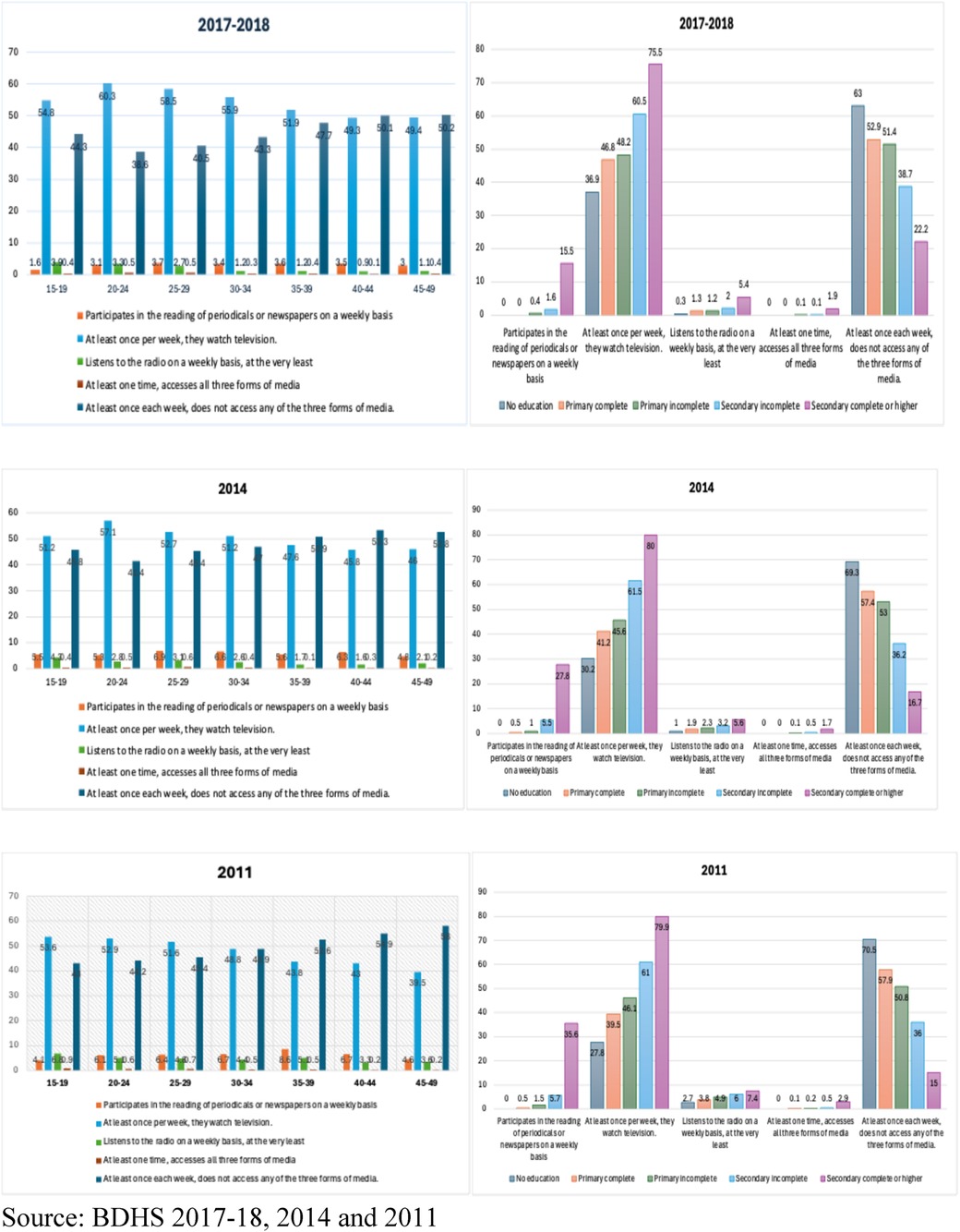
Figure 6. Exposure to mass media. Proportion of never-married women (15–49 years old) who, based on their age and level of education, were exposed to particular media on a weekly basis.
This study found that women aged 25–29 and 35–39 read a newspaper or magazine at least once a week, which is the highest, while women aged 45–49 and 15–19 had the lowest percentage at 6.9% and 4.8%, and 8.6% and 4.1% for 2014 and 2011, respectively. Women with a complete secondary or higher education had the highest prevalence of reading a newspaper or magazine at least once a week at 15.5%, 27.8%, and 35.6%, respectively. Thus, the prevalence of women with higher education reading a newspaper or magazine at least once a week decreased from 2011 to 2018. Moreover, the prevalence of watching television at least once a week was higher among those aged 20–24 (60.3%), 20–24 (57.1%), and 15–19 (53.6%) compared to those aged 40–44 (49.3%), 40–44 (45.8%), and 45–49 (39.5%) in 2017–2018, 2014, and 2011, respectively. This study found that the younger the women were, the greater the tendency to watch television at least once a week. Furthermore, those with complete secondary or higher education had the highest prevalence of watching television at least once a week at 75.5%, 80%, and 79.9%, respectively.
Furthermore, listening to the radio at least once a week was more prevalent among those aged 15–19 (3.9% and 6.8%) than among those aged 40–44 (0.9%) and 30–34 (4.4%) in 2017–2018 and 2011, but less prevalent among those aged 15–19 (4.3%) than those aged 40–44 (45.8%) in 2014 respectively. This study found that the younger the women were, the greater the tendency to listen to the radio at least once a week. Here, those with a complete secondary or higher education had the highest portion of watching television at least once a week at 5.4%, 5.6%, and 7.4%, respectively. In addition, accessing all three media at least once a week was higher among those aged 20–24 and 25–29 (0.5%), 25–29 (0.6%), and 15–19 (0.9%) compared to those aged 40–44 (0.1%), 35–39 (0.1%), and 40–44 and 45–49 (0.2%) in 2017–2018, 2014, and 2011, respectively. This study found that the younger the women were, the greater the tendency to listen to the radio at least once a week. Here, those with a complete secondary or higher education had the highest prevalence of watching television at least once a week at 1.9%, 1.7%, and 2.9%, respectively. In contrast, accessing none of the three media at least once a week was higher among those aged 45–49 (50.2%), 45–49 (52.8%), and 45–49 (58%) compared to those aged 20–24 (38.6%), 20–24 (41.4%), and 40–44 and 15–19 (43%) in 2017–2018, 2014 and 2011 respectively. This study found that the older the women were, the greater the tendency to access none of the three media at least once a week. Here, uneducated women had the highest prevalence of not accessing any of the three media at least once a week at 63%, 69.3%, and 70.5%, respectively.
Our findings are consistent with several research studies. For instance, mass media like TV and radio can impact people's perspectives on healthy lifestyles and family planning (70). Radio and television expose both sexes to current views and opinions on healthcare, family planning, and related matters. According to Fleischer (63), more people are using contraception because of what they see in the media. Furthermore, misperceptions about family planning and contraception are dispelled, and people are encouraged to use these methods by media depictions (71–73), indicating a substantial correlation between media exposure and modern birth control methods. The usage of modern methods of birth control increased with time among women who were less exposed to mass media. Even though this finding contradicts previous studies, we maintain our belief that media exposure significantly influences the use of contraceptive methods.
Studies have shown that the media is the main source of information regarding modern contraceptives’ benefits. Osman et al. (74) and Aslam et al. (75) found that media exposure increased modern contraception use. Ferrara et al. (76) found in Brazil that soap operas promote modest families, as individual choices diminish the birth rate. Television access reduced the birth rate in Indonesia, according to Dewi et al. (77). Barber and Axinn (78) discovered that mainstream media is linked to childbearing, small family preference, reduced son preference, and contraceptive tolerance in Nepal. In addition, women who were exposed to media about family planning were more likely to use contraception, according to research by Haq et al. (6). All three surveys found statistically significant levels of exposure to messages on family planning in various types of mass media. Islam et al. (39), Hussain (79), Kamal and Mohsena (80), Saleem and Pasha (81), and Mohsena and Kamal (54) all found comparable results in their studies on South Asia. Islam et al. (39) found that among Indian women, those who lacked exposure to mass media were less likely to use modern techniques. There was a concomitant shift in the ideal family size and the prevalence of contraception (82). The media's ability to understand and inspire couples, especially on delicate topics such as their reproductive means and objectives, may be a contributing factor to this finding. Findings from our study corroborate those of previous research (18, 83) that found that women with more formal education, occupations, and media exposure were more likely to use modern methods of contraception. Therefore, we can conclude that media exposure, especially television, is linked to current and future contraception use.
Figure 7 shows the number of ever-married women aged 15–49 who were exposed to specific media on a weekly basis from the BDHS (24–26). The 25–29 and 20–24 age groups had the highest number of women with 3,679, 3,390, and 3,514 in 2017–2018, 2014, and 2011, respectively. The lowest numbers belonged to the 45–49 age group with 2,285, 1,766, and 1,820, respectively. Thus, the figure depicts that the older the women, the lower the number of those exposed to media about their contraception practices on a weekly basis.
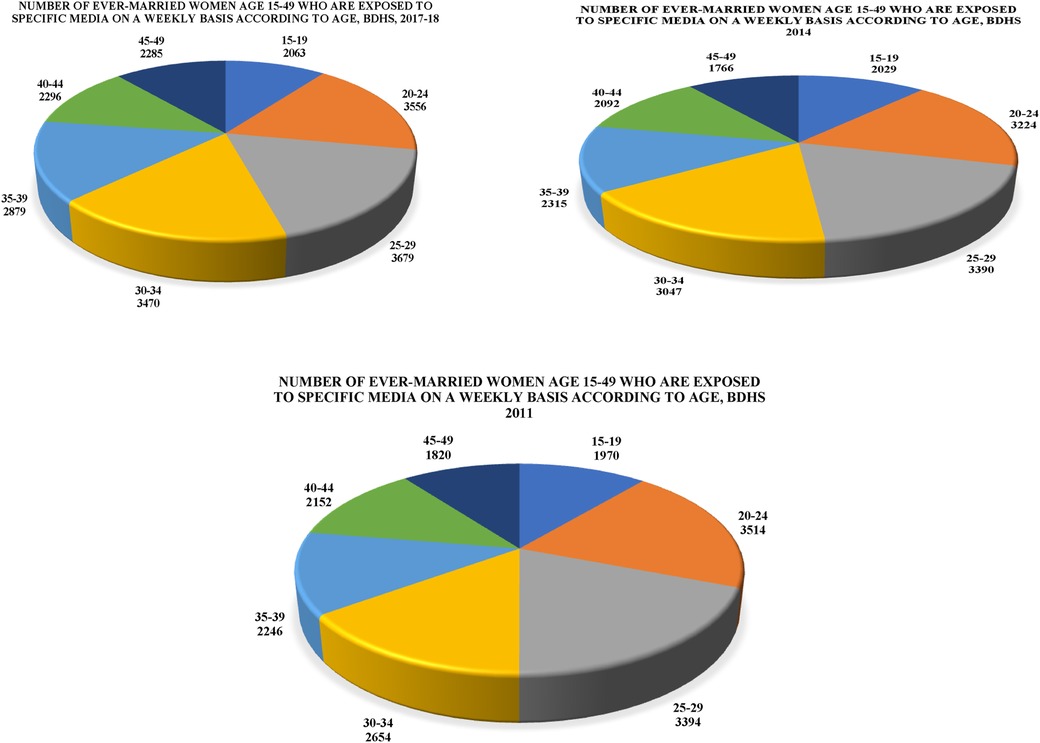
Figure 7. Exposure to mass media. Number of ever-married women aged 15–49 who were exposed to specific media on a weekly basis from the BDHS (24–26).
Despite Bangladesh's achievement in reducing the birth rate, reproductive-age women must use contraception. Bangladesh has a long way to go to reach the desired CPR of above 70% (84). Bangladesh has extensively studied the factors that affect contraceptive use (46, 84, 85). The majority of this study used nationally representative sample surveys. Comparative studies using national surveys from different years can reveal the factors that affect contraceptive use in Bangladesh. During the past two decades, there has been a significant surge in the usage of contraception worldwide, especially in poorer nations. The increasing adoption of contraceptive technologies in underdeveloped nations has resulted in a 40% decrease in unwanted pregnancies and maternal deaths. Furthermore, research carried out in Bangladesh (86) presented data indicating that the incidence of unintended pregnancies was greater (33%) among women who used contraceptives before their most recent pregnancy compared to women (23%) who did not use any reproductive methods. In general, the findings of these studies suggest that women's autonomy essentially facilitates their greater role in decision-making related to contraceptive use, and makes women more capable to overcome barriers related to contraceptive use such as resisting family and social pressure of having more children, avoiding misconceptions about contraception, and taking initiatives to deal with any side effects of using contraception (87).
Overall, the results of this research indicated a positive correlation between maternal age, level of education, and media exposure with contraceptive usage in Bangladesh. One study revealed that women aged 35 and older have a reduced frequency of contraceptive use due to their heightened apprehension about perceived health issues (88). Adolescent women use contraception more than older women because they are more aware of preventing unwanted pregnancies and want to postpone childbearing (89). Women with higher education are more likely to utilize contraception than women with lower levels of education because they are more aware of the detrimental effects of having more children on the health of both mothers and children. It is expected of spouses to limit the number of children their wife has through family planning. According to Kamal et al. (90), there is evidence that women broach the topic of contraception with their spouses, but that men ultimately make the choice because they are the ones who provide the money. Due to the power disparities in many relationships, women may experience fear of violence when family planning or the use of contraceptives is discussed. As a result, this study's findings expand on our understanding of the role that decision-making authority plays in both Bangladesh's population and the current prevalence of contraception.
Strengths and drawbacks of the study
The utilization of nationally representative data allows for a detailed examination of the findings, which is the principal strength of this study. This study provided a thorough explanation of the modern and traditional methods of birth control used by Bangladeshi women. However, this study has certain drawbacks. Men's perceptions of their female partners’ acceptance of barrier methods of contraception or any other contemporary technique of contraception were excluded. This study started by comparing the results to those of other rich and poor countries. However, because this study used secondary datasets, we could not include many important factors due to data limitations. The study did not ask about the interviewees’ family situations. In addition, the study failed to consider whether couples live in a nuclear or shared family structure, which could have limited the generalizability of the results. Not including relevant variables in the datasets also meant that the study's findings did not account for how healthcare access, family planning programs, and public views on contraception have evolved over time. Notwithstanding these drawbacks, the study offers insightful information about the patterns and factors influencing Bangladeshi women's adoption of both traditional and modern forms of contraception, laying the groundwork for further investigations and policy creation.
Conclusion and recommendations
Our review provides a substantial body of evidence on contraceptive behavioral practices and media influence among women in Bangladesh based on the effects of age and education. Since its independence, Bangladesh has seen varied contraceptive behavioral practices associated with factors like age and education, which have played a significant role. Age and education influence the autonomy of contraception and the choice of using a specific method, which plays a vital role in the reproductive health of women. When considering women's autonomy in decision-making about contraception practices aimed at slowing rapid population growth, prioritizing women's empowerment becomes crucial. Mass media should be active and try to find out the problems faced by women with the cooperation of the health workers, so that they can express their views and get age-appropriate contraception suggestions from the health workers. The number of educational facilities should be increased so that women can gather relevant information about contraception and hence, unwanted pregnancies will be reduced. Finally, as it is difficult to disaggregate the effectiveness of individual techniques, we recommend further in-depth research to understand which techniques are especially effective for women according to their age category. In particular, we recommend performing an additional in-depth study on solutions to problems, techniques for improving performance, and interventions providing social support. It is likely that the only method of birth control that will be effective is a mix of several behavioral routines. To effectively promote women's empowerment in terms of health, it is necessary to employ subtle communication strategies that encourage women to participate in the process of planning and determining the size of their family, while simultaneously dispelling any negative beliefs or misunderstandings that may exist regarding modern methods of contraception. As a result, this study has some implications for public policy, including the provision of information that is necessary to comprehend the adverse effects of overpopulation on a country like Bangladesh, the implementation of a face-to-face communication program, the provision of family planning education that is based in institutions, and the guarantee of exposure to electronic media. To boost the nation's usage of contraceptives, health promotion and educational initiatives should focus on workplaces, schools, mosques, churches, and temples.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
MM: Writing – original draft, Writing – review & editing.
Funding
The author declares that no financial support was received for the research and/or publication of this article.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hubach RD, Zipfel R, Munoz FA, Brongiel I, Narvarte A, Servin AE. Barriers to sexual and reproductive care among cisgender, heterosexual and LGBTQIA+ adolescents in the border region: provider and adolescent perspectives. Reprod Health. (2022) 19:93. doi: 10.1186/s12978-022-01394-x
2. Matin BK, Williamson HJ, Karyani AK, Rezaei S, Soofi M, Soltani S. Barriers in access to healthcare for women with disabilities: a systematic review in qualitative studies. BMC Womens Health. (2021) 21:44. doi: 10.1186/s12905-021-01189-5
3. Nguyen TT, Neal S. Contraceptive prevalence and factors influencing utilization among women in Pakistan: a focus on gender-based violence. Fulbright Rev Econ Policy. (2021) 1:119–34. doi: 10.1108/FREP-05-2021-0032
5. Rahman M, Begum M, Uddin M, Rahman M. Factors affecting health status of urban aged population: evidence from syLhet, Bangladesh. Indian J Gerontol. (2018) 32:103–18.
6. Haq I, Sakib S, Talukder A. Sociodemographic factors on contraceptive use among ever-married women of reproductive age: evidence from three demographic and health surveys in Bangladesh. Med Sci (Basel). (2017) 5(4):31. doi: 10.3390/medsci5040031
7. National Institute of Population Research and Training (NIPORT). Bangladesh Demo-Graphic and Health Survey 2017–2018. Dhaka: Mitra and Associates, and ICF International (2018). Available at: https://niport.portal.gov.bd/sites/default/files/files/niport.portal.gov.bd/miscellaneous_info/d0ad2ea3_b7f9_4b60_a5f5_f91116e941ee/91a3ead5e08efd2385d37c2919595c83.pdf
8. FP. Commitment Maker. Family Planning 2020 Commitment: Bangladesh. (2020). Available at: https://fp2030.org/bangladesh (Accessed September 5, 2024)
9. Kc H, Shrestha M, Pokharel N, Niraula SR, Pyakurel P, Parajuli SB. Women’s empowerment for abortion and family planning decision making among marginalized women in Nepal: a mixed method study. Reprod Health. (2021) 18:28. doi: 10.1186/s12978-021-01087-x
10. Duvendack M, Palmer-Jones R. Microfinance, women’s empowerment and fertility decline in Bangladesh: how important was women’s agency? J Dev Stud. (2017) 53:664–83. doi: 10.1080/00220388.2016.1205731
11. Toufique MMK. The context specific factors affecting women empowerment and empowerment’s implications for resource allocation, awareness and fertility: an econometric analysis. Int Lett Soc Hum Sci. (2016) 66:38–44. doi: 10.18052/www.scipress.com/ILSHS.66.38
12. UN (United Nations). Trends in Contraceptive Use Worldwide Population Division, Department of Economic and Social Affairs. New York: United Nations (2015). Available at: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/undesa_pd_report_2015_trends_contraceptive_use
13. Central Statistics Organization (CSO). Ministry of Public Health (MoPH), and ICF. Afghanistan Demographic and Health Survey 2015. Kabul, Afghanistan: Central Statistics Organization (2017). Available at: www.DHSprogram.com
14. National Institute of Population Research and Training (NIPORT). Bangladesh Demographic and Health Survey 2014. Dhaka, Bangladesh: Mitra and Associates and ICF International (2016). Available at: http://www.dhsprogram.com/publications/publication-FR311-DHS-Final-Reports.cfm
15. Cleland J, Conde-Agudelo A, Peterson H, Ross J, Tsui A. Contraception and health. Lancet. (2016) 380(9837):149–56. doi: 10.1016/S0140-6736(12)60609-6
16. Chola L, McGee S, Tugendhaft A, Buchmann E, Hofman K. Scaling up family planning to reduce maternal and child mortality: the potential costs and benefits of modern contraceptive use in South Africa. PLoS One. (2015) 10(6):e0130077. doi: 10.1371/journal.pone.0130077
17. Bearak J, Popinchalk A, Ganatra B, Moller AB, Tuncalp O, Beavin C. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Health. (2020) 8(9):e1152–61. doi: 10.1016/S2214-109X(20)30315-6
18. Khan MN, Harris M, Loxton D. Modern contraceptive use following an unplanned birth in Bangladesh: an analysis of national survey data. Int Perspect Sex Reprod Health. (2020) 46:77–87. doi: 10.1363/46e8820
19. Hoq MN. Influence of the preference for sons on contraceptive use in Bangladesh: a multivariate analysis. Heliyon. (2020) 6:e05120. doi: 10.1016/j.heliyon.2020.e05120
20. Bishwajit G, Tang S, Yaya S, Feng Z. Unmet need for contraception and its association with unintended pregnancy in Bangladesh. BMC Pregnancy Childbirth. (2017) 17:1–9. doi: 10.1186/s12884-017-1379-4
21. Hossain M, Khan M, Ababneh F, Shaw JEH. Identifying factors influencing contraceptive use in Bangladesh: evidence from BDHS 2014 data. BMC Public Health. (2018) 18(1):1–14. doi: 10.1186/s12889-018-5098-1
22. Islam MS, Hassan M. Women knowledge, attitude, approval of family planning and contraceptive use in Bangladesh. Asia Pac J Multidiscip Res. (2016) 4(2):76–82.
23. Blackstone SR, Iwelunmor J. Determinants of contraceptive use among Nigerian couples: evidence from the 2013 demographic and health survey. Contracept Reprod Med. (2017) 2:1–8. doi: 10.1186/s40834-017-0037-6
24. Bangladesh Demographic Health Survey (BDHS). National Institute of Population Research and Training-NIPORT/Bangladesh, Mitra and Associates, and ICF International. Dhaka, Bangladesh: NIPORT, Mitra and Associates, and ICF International (2017-2018).
25. Bangladesh Demographic Health Survey (BDHS). National Institute of Population Research and Training-NIPORT/Bangladesh, Mitra and Associates, and ICF International. Dhaka, Bangladesh: NIPORT, Mitra and Associates, and ICF International (2011).
26. Bangladesh Demographic Health Survey (BDHS). National Institute of Population Research and Training-NIPORT/Bangladesh, Mitra and Associates, and ICF International. Dhaka, Bangladesh: NIPORT, Mitra and Associates, and ICF International (1993-1994).
27. Page MJ, McKenzie JE, Bossuyt PM. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
28. Rana MS, Khanam SJ, Alam MB, Hassen MT, Kabir MI, Khan MN. Exploration of modern contraceptive methods using patterns among later reproductive-aged women in Bangladesh. PLoS One. (2024) 19(4):e0291100. doi: 10.1371/journal.pone.0291100
29. Bangladesh Demographic Health Survey (BDHS). National Institute of Population Research and Training-NIPORT/Bangladesh, Mitra and Associates, and ICF International. Dhaka, Bangladesh: NIPORT, Mitra and Associates, and ICF International (2014).
30. Rana MS, Alam MD, Hassen MT, Kabir MI, Khanam SJ, Khan MN. BMJ Yale. (2023). doi: 10.1101/2023.08.23.23294471
31. Alam N, Mollah MMH, Naomi SS. Prevalence and determinants of adolescent childbearing: comparative analysis of 2017–18 and 2014 Bangladesh demographic health survey. Front Public Health. (2023) 11:1088465. doi: 10.3389/fpubh.2023.108846
32. Chowdhury S, Rahman MM, Haque MA. Role of women’s empowerment in determining fertility and reproductive health in Bangladesh: a systematic review. Am J Obstet Gynecol Glob Rep. (2023) 3(3):100239. doi: 10.1016/j.xagr.2023.100239
33. Sharif AB, Hasan MT, Naziat MH. Permanent, long-acting and short-acting reversible contraceptive methods use among women in Bangladesh: an analysis of Bangladesh demographic and health survey 2017–2018 data. BMJ Open. (2023) 13:e073469. doi: 10.1136/bmjopen-2023-073469
34. Kundu S, Kundu S, Rahman MA. Prevalence and determinants of contraceptive method use among Bangladeshi women of reproductive age: a multilevel multinomial analysis. BMC Public Health. (2022) 22:2357. doi: 10.1186/s12889-022-14857-4
35. Roy N, Amin MB, Maliha MJ, Sarker B, Aktarujjaman M, Hossain E. Prevalence and factors associated with family planning during COVID-19 pandemic in Bangladesh: a cross-sectional study. PLoS One. (2021) 16(9):e0257634. doi: 10.1371/journal.pone
36. Majumder UK, Khan MS. Knowledge of family planning and contraceptive use among indigenous women in Dinajpur, Bangladesh: a cross-sectional study. Int J Community Med Public Health. (2021) 8(1):75–84. doi: 10.18203/2394-6040.ijcmph20205679
37. Islam MK, Haque MR, Hema PS. Regional variations of contraceptive use in Bangladesh: a disaggregate analysis by place of residence. PLoS One. (2020) 15(3):e0230143. doi: 10.1371/journal.pone.0230143
38. Islam AZ. Factors affecting modern contraceptive use among fecund young women in Bangladesh: does couples’ joint participation in household decision making matter? Reprod Health. (2018) 15:112. doi: 10.1186/s12978-018-0558-8
39. Islam AZ, Rahman M, Mostofa MG. Association between contraceptive use and socio-demographic factors of young fecund women in Bangladesh. Sex Reprod Healthc. (2017) 13:1–7. doi: 10.1016/j.srhc.2017.05.001
40. Biswas AK, Shuvo TEA, Aich M, Mondal S. Women’s autonomy and control to exercise reproductive rights: a sociological study from rural Bangladesh. SAGE Open. (2017) 7(2). doi: 10.1177/2158244017709862
41. Rahman MM, Mostofa MG, Hoque MA. Women’s household decision-making autonomy and contraceptive behavior among Bangladeshi women. Sex Reprod Healthc. (2014) 5(1):9–15. doi: 10.1016/j.srhc.2013.12.003
42. BDHS (2007). Bangladesh Demographic and Health Survey. National Institute of Population Research and Training (NIPORT) Dhaka, Bangladesh. Available at: https://dhsprogram.com/pubs/pdf/FR207/FR207%5BApril-10-2009%5D.pdf (Accessed August 25, 2024).
43. Gazi R, Kabir H, Saha NC. Changes in the selected reproductive health indicators among married women of reproductive age in low performing areas of Bangladesh: findings from an evaluation study. BMC Public Health. (2014) 14:478. doi: 10.1186/1471-2458-14-478
44. Goni A, Rahman M. The impact of education and media on contraceptive use in Bangladesh: a multivariate analysis. Int J Nurs Pract. (2012) 18(6):565–73. doi: 10.1111/ijn.12013
45. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8(1):19–32. doi: 10.1080/1364557032000119616
46. Kibria GMA, Hossen S, Barsha RAA, Sharmeen A, Paul SK, Uddin SMI. Factors affecting contraceptive use among married women of reproductive age in Bangladesh. J Mol Stud Med Res. (2016) 02(01):70–9. doi: 10.18801/jmsmr.020116.09
47. Kamal SM, Islam MA. Contraceptive use: socioeconomic correlates and method choices in rural Bangladesh. Asia Pac J Public Health. (2010) 22:436–50. doi: 10.1177/1010539510370780
48. Dias JG, de Oliveira IT. Multilevel effects of wealth on women’s contraceptive use in Mozambique. PLoS One. (2015) 10(3):e0121758. doi: 10.1371/journal.pone
49. Islam AZ. Association between modern contraceptive use and socio- demographic factors among fecund young women in Bangladesh. J Womens Health Issues Care. (2017) 6:5. doi: 10.4172/2325-9795.1000286
50. Bangladesh Demographic Health Survey (BDHS). National Institute of Population Research and Training-NIPORT/Bangladesh, Mitra and Associates, and ICF International. Dhaka, Bangladesh: NIPORT, Mitra and Associates, and ICF International (2022). Availavle at: https://dhsprogram.com/pubs/pdf/PR148/PR148.pdf
51. Forty J, Rakgoasi SD, Keetile M. Patterns and determinants of modern contraceptive use and intention to use contraceptives among Malawian women of reproductive ages (15–49 years). Contracept Reprod Med. (2021) 6:1–12. doi: 10.1186/s40834-021-00163-8
52. Osmani AK, Reyer JA, Osmani AR, Hamajima N. Factors influencing contraceptive use among women in Afghanistan: secondary analysis of Afghanistan health survey 2012. Nagoya J Med Sci. (2015) 77:551–61.26663934
53. Islam MS. Determinants of contraceptive method choice in Bangladesh: male perspectives. Southeast Asia J Public Health. (2014) 3(1):50–6. doi: 10.3329/seajph.v3i1.17711
54. Mohsena M, Kamal M. Determinants of contraceptive use in Bangladesh. Ibrahim Med Coll J. (2014) 8:34–40. doi: 10.3329/imcj.v8i2.26676
55. Tekelab T, Melka AS, Wirtu D. Predictors of modern contraceptive methods use among married women of reproductive age groups in western Ethiopia: a community based cross-sectional study. BMC Womens Health. (2015) 15:52. doi: 10.1186/s12905-015-0208-z
56. Mekonnen W, Worku A. Determinants of low family planning use and high unmet need in Butajira district, south central Ethiopia. Reprod Health. (2011) 8:37. doi: 10.1186/1742-4755-8-37
57. Adanu RM, Seffah JD, Hill AG, Darko R, Duda RB, Anarfi JK. Contraceptive use by women in Accra, Ghana: results from the 2003 Accra women’s health survey. Afr J Reprod Health. (2009) 13(1):123–33. Available at: https://www.jstor.org/stable/2061709920687270
58. Nketiah-Amponsah E, Arthur E, Aaron A. Correlates of contraceptive use among Ghanaian women of reproductive age (15–49 years). Afr J Reprod Health. (2012) 16(3):155–70. Available at: http://www.jstor.org/stable/2348570323437509
59. MOHFW (Ministry of health and family welfare) [Bangladesh]. Strategic Plan for Health, Population, and Nutrition Sector Development Program 2011–16. Dhaka: DGHS (Deterorate General of Health Services) (2011). Available at: http://www.nationalplanningcycles. org/planning-cycle/BGD (Accessed September 05, 2024).
60. Kim J. Female education and its impact on fertility. IZA World of Labor (2016). p. 228. doi: 10.15185/izawol.228.v2
61. Kabir S, Tareq M, Hossain MI. Examining the decline in modern contraception usage among married women in Bangladesh: applying Blinder-Oaxaca decomposition analysis. PLoS One. (2024) 19(5):e0304122. doi: 10.1371/journal.pone.0304122
62. Mitra and Associates. Bangladesh Demographic and Health Survey 1999–2000. Dhaka, Bangladesh and Calverton, Maryland, USA: ORC Macro (2011).
63. Fleischer A. Population Dynamics in Bangladesh: A case study on the causes and effects of demographic change in Bangladesh. Division of Health and Social Protection GTZ-section: New Political Prospective. (2010).
64. Hossain S, Akter T, Mohsin M, Islam MM, Chowdhury PB, Khudri MM. Contraceptive uses among married women in Bangladesh: a systematic review and meta-analyses. J Health Popul Nutr. (2024) 2024:10. doi: 10.1186/s41043-024-00502-w
65. Pazol K, Zapata LB, Tregear SJ, Mautone-Smith N, Gavin LE. Impact of contraceptive education on contraceptive knowledge and decision making. Am J Prev Med. (2015) 9(2 Suppl 1):S46–56. doi: 10.1016/j.amepre.2015.03.031
66. Gurmu E, Tariku D. Correlates of high risk fertility behaviour in Ethiopia: a multilevel analysis of the 2011 Ethiopian demographic and health survey data. J Heal Med Nurs. (2017) 39:86–95.
67. Howlader MH, Roshid HO, Kundu S, Halder HR, Chanda SK, Rahman MA. Determinants associated with high-risk fertility behaviors among reproductive aged women in Bangladesh: a cross-sectional study. Reprod Health. (2022) 19:17. doi: 10.1186/s12978-022-01333-w
68. Tamirat KS, Tesema GA, Tessema ZT. Determinants of maternal high-risk fertility behaviors and its correlation with child stunting and anemia in the east Africa region: a pooled analysis of nine east African countries. PLoS One. (2021) 16(6):e0253736. doi: 10.1371/journal.pone.0253736
69. Goleen S, Diana GF, Lauren JR, Corinne HR. Pregnancy preferences and contraceptive use among US women. Contraception. (2019) 101(2):79–85. doi: 10.1016/j.contraception.2019.10.007
70. Goni MA. Fertility and contraceptive use in Bangladesh: the role of women’s education and mass media. J Asian Prof. (2010) 38:191–208.
71. Sserwanja Q, Turimumahoro P, Nuwabaine L, Kamara K, Musaba MW. Association between exposure to family planning messages on different mass media channels and the utilization of modern contraceptives among young women in Sierra Leone: insights from the 2019 Sierra Leone demographic health survey. BMC Womens Health. (2022) 22. doi: 10.1186/s12905-022-01974-w
72. Nsanya MK, Atchison CJ, Bottomley C, Doyle AM, Kapiga SH. Modern contraceptive use among sexually active women aged 15–19 years in north-western Tanzania: results from the adolescent 360 (A360) baseline survey. BMJ Open. (2019) 9:e030485. doi: 10.1136/bmjopen-2019-030485
73. Casey SE, Gallagher MC, Kakesa J, Kalyanpur A, Muselemu JB, Rafanoharana RV. Contraceptive use among adolescent and young women in north and South Kivu, Democratic Republic of Congo: a cross-sectional population-based survey. PLoS Med. (2020) 17:e1003086. doi: 10.1371/journal.pmed.1003086
74. Osman A, Wong JL, Bagge CL, Freedenthal S, Gutierrez PM, Lozano G. The depression anxiety stress scales-21 (DASS-21): further examination of dimensions, scale reliability, and correlates. J Clin Psychol. (2012) 68(12):1322–38. doi: 10.1002/jclp.21908
75. Aslam SK, Zaheer S, Qureshi MS, Aslam SN, Shafique K. Socio-economic disparities in use of family planning methods among Pakistani women: findings from Pakistan demographic and health surveys. PLoS One. (2016) 11(4):e0153313. doi: 10.1371/journal.pone.0153313
76. Ferrara EL, Chong A, Duryea S. Soap operas and fertility: evidence from Brazil. Am Econ J Appl Econ. (2012) 4(4):1–31. doi: 10.1257/app.4.4.1
77. Dewi RK, Suryadharma D, Suryahadi A. The Impact of Expansion of Television Coverage on Fertility: Evidence from Indonesia. Jakarta: The SMERU Research Institute (2013).
78. Barber JS, Axinn WG. New ideas and fertility limitation: the role of mass media. J Marriage Fam. (2004) 66(5):1180–200. doi: 10.1111/j.0022-2445.2004.00086.x
79. Hussain N. Demographic, socio-economic and cultural factors affecting knowledge and use of contraception differentials in Malda district, West Bengal. J Community Med Health Educ. (2011) 1:102. doi: 10.4172/jcmhe.1000102
80. Kamal N, Mohsena M. Twenty years of field visits by family planning workers in Bangladesh: are they still needed? Indian J Fam Welf. (2011) 57:10–21. Available at: https://www.researchgate.net/publication/259192347_TWENTY_YEARS_OF_FIELD_VISITS_BY_FP_WORKERS_IN_BANGLADESH_ARE_THEY_STILL_NEEDED
81. Saleem A, Pasha GR. Women’s reproductive autonomy and barriers to contraceptive use in Pakistan. Eur J Contracept Reprod Health Care. (2008) 13:83–9. doi: 10.1080/01443610701577107
82. Retherford RD, Mishra V. Media exposure increases contraceptive use. Natl Fam Health Surv Bull7. (1997) (7):1–4. Available at: https://scholarspace.manoa.hawaii.edu/server/api/core/bitstreams/5c116703-89e6-4a42-88c9-0498115c3245/content
83. Khan MN, Islam MM. Exploring rise of pregnancy in Bangladesh resulting from contraceptive failure. Sci Rep. (2022) 12(1):2353. doi: 10.1038/s41598-022-06332-2
84. NIPORT (National Institute of Population Research and Training, Mitra and Associates). Bangladesh Demographic and Health Survey, 2011; Preliminary Report. Dhaka, Bangladesh; Calverton, MD, USA: National Institute of Population Research and Training, Mitra and Associates (2012).
85. Kamal SM. Socioeconomic factors associated with contraceptive use and method choice in urban slums of Bangladesh. Asia Pac J Public Health. (2015) 27(2):2661–76. doi: 10.1177/1010539511421194
86. Noor FR, Rahman MM, Rob U, Bellows B. Unintended pregnancy among rural women in Bangladesh. Int Q Community Health Educ. (2012) 32:101–13. doi: 10.2190/IQ.32.2.b
87. Hameed W, Azmat SK, Ali M, Sheikh MI, Abbas G, Temmerman M, et al. Women’s empowerment and contraceptive use: the role of independent versus couples’ decision-making, from a lower middle income country perspective. PLoS One. (2014) 9(8):1–9. doi: 10.1371/journal.pone.0104633
88. Moon MP. Decision-Making ability of tribal women in Chittagong hill tracts of Bangladesh. Middle East J Sci Res. (2023) 31(1):15–21. doi: 10.5829/idosi.mejsr.2023.15.21
89. Blanc AK, Tsui AO, Croft TN, Trevitt JL. Patterns and trends in adolescents’ contraceptive use and discontinuation in developing countries and comparisons with adult women. Int Perspect Sex Reprod Health. (2009) 35(2):63–71. doi: 10.1363/3506309
90. Kamal HM, Nazrul IM, Nazniz AM. Reproductive health rights of women in the rural areas of Meherpur district in Bangladesh. J Reprod Infertil. (2011) 12(1):23–32. Available at: https://pubmed.ncbi.nlm.nih.gov/2392649623926496
91. Islam MK. Contraceptive use, method choice and discontinuation of contraception in south Asia. Am J Sociol Res. (2017) 7:109–16. doi: 10.5923/j.sociology.20170704.02
92. Ministry of health and family welfare (MOHFW) [Bangladesh]. Health, Population and Nutrition Sector Development Program (2011–2016), Program Implementation Plan Volume I. Dhaka: DGHS (Deterorate General of Health Services) (2016). Available at: http://www.nationalplanningcycles.org/planning-cycle/BGD
Keywords: contraceptive behavioral practices, media exposure, age effects, education effects, Bangladeshi women
Citation: Moon MP (2025) Contraceptive behaviors and media influence among women in Bangladesh: exploring the effects of age and education. Front. Glob. Women's Health 6:1492105. doi: 10.3389/fgwh.2025.1492105
Received: 6 September 2024; Accepted: 26 March 2025;
Published: 16 May 2025.
Edited by:
Stephen Kennedy, University of Oxford, United KingdomReviewed by:
Toyoko Yoshizawa, Kansai University of International Studies, JapanEleonora Hristova-Atanasova, Medical University of Plovdiv, Bulgaria
Ayesha Khan, Akhter Hameed Khan Foundation, Pakistan
Ahmad Khan, Aga Khan University, Pakistan
Copyright: © 2025 Moon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Monira Parvin Moon, bW9uaXJhbW9vbkBic21yYXUuZWR1LmJk
†ORCID:
Monira Parvin Moon
orcid.org/0000-0002-6596-4623