 Yamoussa Youla1,2*†
Yamoussa Youla1,2*† Sidikiba Sidibé3
Sidikiba Sidibé3 Hounmenou GC2,4
Hounmenou GC2,4 Mory1 Kourouma2,3Saidouba Chérif Camara1,2Salifou Talassone Bangoura1,2K. K. J. J. Olivier1,2
Mory1 Kourouma2,3Saidouba Chérif Camara1,2Salifou Talassone Bangoura1,2K. K. J. J. Olivier1,2 Mathias Grovogui3,5Maladho Diaby1,2
Mathias Grovogui3,5Maladho Diaby1,2 Emile Faya Bongono2Oumou Hawa Diallo3Ibrahima Conté3Sékou Traoré1Adama Djigui Keita5A. Touré1,2A. Delamou3,5
Emile Faya Bongono2Oumou Hawa Diallo3Ibrahima Conté3Sékou Traoré1Adama Djigui Keita5A. Touré1,2A. Delamou3,5
- 1Department of Pharmaceutical and Biological Sciences, Faculty of Health Sciences and Technology, Gamal Abdel Nasser University, Conakry, Guinea
- 2Centre de Recherche et de Formation en Infectiologie de Guinée, Université Gamal Abdel Nasser de Conakry, Conakry, Guinea
- 3Department of Medical Sciences, Faculty of Health Sciences and Techniques, Gamal Abdel Nasser University, Conakry, Guinea
- 4IT Department, Centre Universitaire de Labé, Labé, Guinea
- 5Maférinyah Rural Health Research Centre, Ministry of Health and Public Hygiene, Forecariah, Guinea
Introduction: The low use of modern contraceptive methods by female healthcare providers is a real public health problem in Guinea. This study aimed to analyze the prevalence and factors associated with the use of modern contraceptive methods among female healthcare providers in Guinea.
Method: This was a secondary analysis of data from a cross-sectional survey on the use of modern contraceptive methods among female healthcare providers in Guinea between November 1, 2020, and January 31, 2021. The study included 1,743 women from 173 health facilities across the country.
Results: This survey included women whose median age was 29 years, with an interquartile range of (24–39) years. Women with a higher level of education (n = 1,656; 95.5%) and a midwifery profile (n = 838; 48.3%) represented the highest proportions. Among the subjects surveyed, Muslim women were the majority (n = 1,229; 70.9%). The overall prevalence of use of modern contraceptive methods by female healthcare providers in Guinea was 61.9%; CI: 59.6–64.1). Married (aOR = 1.19; CI = 0.95–1.50), having secondary education (aOR = 7.92; CI = 3.68–20.7), women belonging to the Muslim religion (aOR = 1.37; CI = 1.09–1.71) were factors statistically associated with the use of modern contraceptive methods among female healthcare providers.
Conclusion: Improving the national prevalence of modern planning methods requires the involvement of stakeholders at all levels. This study's results show a progression in the implementation of governmental actions and health projects and programs related to sexual reproductive health.
Introduction
From 2015 to 2019, every year, 121 million unwanted pregnancies were counted, of which 61% ended in abortion (1). In 2021, 1.1 billion of the world's 1.9 billion women aged between 15 and 49 were in need of family planning services. Of these, 874 million were using modern contraception, while 164 million were denied access to contraception when they needed it (2). The proportion of women of childbearing age using modern family planning methods is one of the indicators in point 3.7.1 of the Sustainable Development Goals. In recent years, significant progress has been made worldwide in improving contraceptive prevalence among women of childbearing age 15–49 (3). According to the World Health Organization (WHO), contraceptive prevalence rose from 74% to 77% worldwide among women of childbearing age between 2000 and 2020 (4). The proportion of women of childbearing age (15–49) using modern family planning methods was 77.5% worldwide in 2022 (5–7). Despite this progress, disparities persist in access to and use of modern contraceptive methods between different regions of the world (8). In high-income countries, over 70% of women have access to a contraceptive method (9–11). In Africa, where the burden of maternal mortality is highest, barely 24% of women of childbearing age have access to a modern contraceptive method (4). In these countries, more than half (56.0%) of modern contraceptive needs remain unmet (12).
Pregnancies that are too early, too late, too numerous and too close together are responsible for the majority of direct obstetric complications, which account for over 70% of maternal deaths in low-income countries (13, 14). Family planning (FP) can prevent 35% of maternal deaths in poor countries if at least 60% of women of childbearing age use a contraceptive method (7).
In their study of the Democratic Republic of Congo, ZIVICH et al. reported a prevalence of 48% of women using contraception (7, 10, 15). In Burkina Faso in 2023, the prevalence of use of modern contraceptive methods was 18.1% (16). In Mali in 2020, out of a total of 2,097 registered users, 721 women (31.38%) were new users of modern contraceptive methods (17).
Few studies have been conducted on the use of contraceptive methods among female healthcare providers in Africa. In northern Uganda, contraceptive prevalence among women working in the health sector in teaching hospitals was 73.6% (16). This prevalence was 18% at the time of the survey of healthcare professionals and medical students in their clinical year in Ghana (17).
Several factors influence the use of contraceptive methods in the general population in sub-Saharan Africa. The main positive factors are education level, family planning knowledge, multiparity and high wealth index (8, 16–18). The negative factors that reduce contraceptive use are fear of contraceptive side effects, male partner disapproval and socio-cultural norms (16). In a study conducted in Uganda, patient- and provider-related barriers to contraceptive use were identified. Patient-related barriers included religious beliefs, misconceptions about contraception and apprehension about adverse effects. Difficulties associated with providers included lack of knowledge, inadequate training and discomfort (19).
In Guinea, contraceptive prevalence is still low among women of childbearing age (15–49). According to the Demographic and Health Surveys (DHS) results, it rose from 9.0% in 2012 to 11.0% in 2018 (20). Furthermore, most of the studies carried out on contraception in Guinea have focused on adolescent girls and young women. There has been a modest increase in modern contraceptive use among adolescents and young women, from 8.4% in 1999 to 12.8% in 2018 (21). Only 22.6% had unmet contraceptive needs (22). The main factors influencing the use of contraceptive methods were fear of adverse effects, spousal approval, religious and socio-cultural beliefs, and the skills of healthcare providers (21, 23) and women from affluent households (21). No nationwide study has explored and documented the use of modern contraceptive methods among female healthcare providers, hence the interest in carrying out this work. The aim was to analyze the prevalence and factors associated with the use of modern contraceptive methods among female healthcare providers in Guinea.
Method
Study setting
The study was conducted in public and private health facilities [hospitals, communal medical centres (CMC), health centres, and clinics] in the eight (8) administrative regions of Guinea (Figure 1) between November 1, 2020, and January 31, 2021.

Figure 1. Geographical map of Guinea's eight (8) administrative regions and neighbouring countries.
Type, period and study population
This was a secondary analysis of data from a cross-sectional survey on the use of modern contraceptive methods among female healthcare providers in Guinea between November 1, 2020 and January 31, 2021.
The study covered all female healthcare providers (doctors, nurses, midwives, technical health agents, laboratory technicians, pharmacists) working in Guinea's public or private healthcare facilities that provide FP services.
Data sources
Data for this study were extracted from the database of a cross-sectional survey conducted in 2021 across 173 public and private health facilities. These included 19 communal hospitals/medical centers (CMCs), 69 health centers, 41 private hospitals/clinics, and 54 private practices or health centers located in the capitals of the eight administrative regions of Guinea, including the capital city, Conakry. A multi-stage sampling technique was used to select the health facilities and study participants. First, an exhaustive selection of national and regional public hospitals and communal medical centers (CMCs) was conducted in each region. Second, a simple random sampling procedure was applied to select among the remaining eligible health facilities (i.e., health centers, private clinics, medical practices, and NGOs), stratified by public or private status, using a validated list provided by the Ministry of Health. Among the 328 eligible health facilities identified, 173 (52.8%) were selected to participate in the study. Within each selected facility, all female health care providers present on the day of data collection were invited to participate. Female providers with missing data on outcome variables were excluded from the analysis. This sampling strategy was designed to ensure representativeness across regions, types of facilities, and public-private distribution.
Dependent or outcome variable
The primary study variable was the current use of a modern contraceptive method, which was coded as a binary variable: “yes” for providers (respondents) who reported using a modern method of contraception at the time of the survey, and “no” for those who were not using any modern method, including those who were using traditional methods. Modern FP methods were defined as intrauterine devices (IUDs), implants, injectables, contraceptive pills, sterilization (male and female) and male and female condoms.
Independent variable
Independent variables included sociodemographic characteristics such as age at the survey, region of residence, marital status, religion, level of education and occupation. They also included work experience, type of contraceptive method used, work in a family planning service, and participation in family planning training.
The level of education included no education, primary, secondary, and higher education. Religion had two categories: Muslim and Christian/other. Marital status was either single or already married; regions were classified as Conakry, Kindia, Boké, Mamou, Labé, Kankan, Faranah, and N'Nzérékoré.
Statistical analysis
Data were analyzed using R-Studio software version 4.4.1. Descriptive statistics were produced as proportions for qualitative variables and mean with standard deviation (SD) for quantitative variables. The Chi-2 statistical test was used to compare qualitative variables, and the Wilcoxon test for quantitative variables in the univariate analysis. Logistic regression was performed, and odds ratios were calculated, considering the respondents’ use of modern contraceptive methods. The binary logistic regression included all study variables with a P value < 0.20 in the univariate analysis. The significance level was 5%, with 95% confidence intervals (CIs). The Wald and Hosmer-Lemeshow tests were used to assess the significance of independent variables and the goodness-of-fit of the final model, respectively.
Ethical considerations
This study received ethical approval from the Comité National d'Ethique pour la Recherche en Santé of the Republic of Guinea (No: 045/CNERS/19).
Results
Sociodemographic characteristics of care providers and prevalence of FP method use
A total of 1,734 women (aged 20–49) were included in the study. The median age was 29 years, with an interquartile range of (5 24–31). Over half (55.3%) of the women were aged between 25 and 34, and 1,489 (85.9%) worked in public facilities (National/Municipal Hospital and primary health centers). Two-thirds (69.1%) of these women were married. In terms of profession, 838 (48.3%) and 460 (26.5%) of the women were midwives and technical health workers (TWAs), respectively. Moreover, 95.5% of the women had attained a higher level of education, while the remainder had secondary education. Over half (42.5%) of the women had more than 6 years of work experience. Of these providers, nearly 82% had received training in sexual and reproductive health in the twelve months preceding the survey (Table 1).
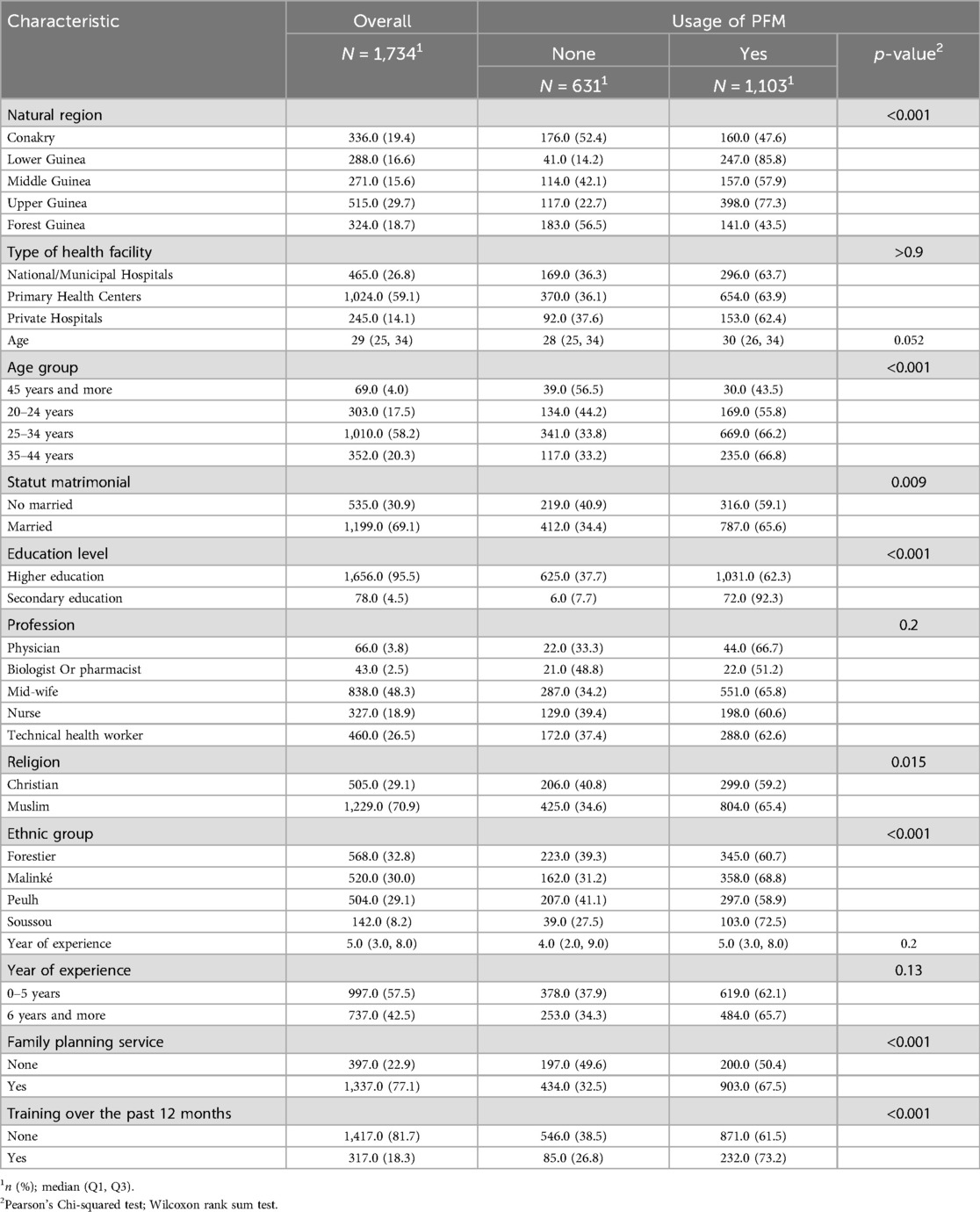
Table 1. Sociodemographic characteristics of female health care providers in the eight (8) administrative regions of Guinea from November 1, 2020, to January 31, 2021 (n = 1,734).
Prevalence of modern contraceptive use
In this study, the overall prevalence of modern contraceptive use among female healthcare providers was 61.9% (95%IC: 59.6–64.1). The highest proportions were recorded among married women (64%), those with a higher level of education, those offering FP services (66%) and those who had received SRH training (71.3%) in the last 12 months following data collection. It varies from region to region (Figure 1). The highest prevalence of use of modern contraceptive methods was observed in Kindia (100% of providers), Kankan (86%), Mamou (65%), Faranah (64.9%) and Boké (64.5%) (Figure 2).
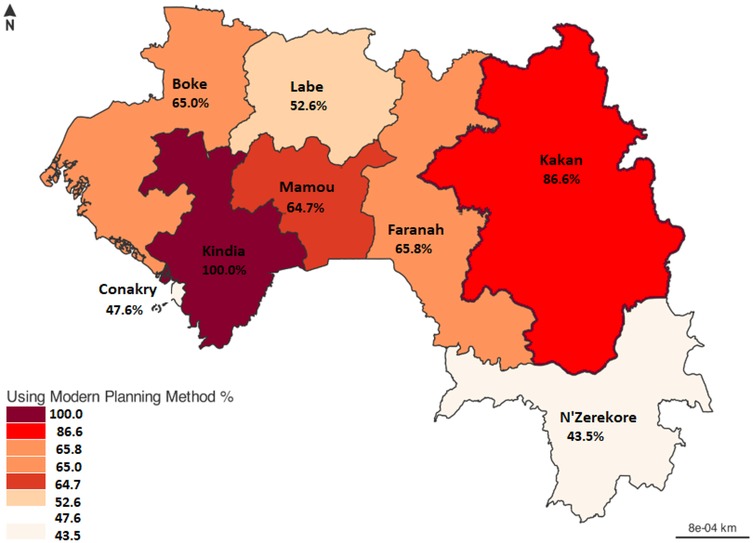
Figure 2. Percentage use of modern contraceptive methods among female health providers from November 1, 2020, to January 31, 2021, in Guinea's eight administrative regions (n = 1,734).
The main modern contraceptive methods used by female providers were implants/norplants/jadelle (42%), pills (20%), depoprovera/injectable (16%) and IUD/Sterilet (14%). Male/female condoms (7.9%).
Factors associated with the use of modern contraceptive methods by female health care providers
In the bivariate analysis, we observed that age, marital status, level of education, religion, working in a planning service, and having received training in the last 12 months prior to data collection were factors significantly associated with the use of modern contraceptive methods among female providers (p-value < 0.05).
However, after adjusting for confounding factors, only age, education level, being involved in the provision of modern contraceptive services, having had training in the last 12 months, and religion were statistically significantly higher—the use of modern methods of contraception among female recipients. Indeed, normally for female beneficiaries aged 45 years or less, those aged 25–34 years (aOR: 3.17: 95% CI: 1.85–5.49) and 35–44 years (aOR: 2.81 95% CI: 1.63–4.89) were more likely to use a modern method of contraception. Female providers with a secondary education level (aOR: 7.92; CI: 3.68–20.7) were eight times more likely to use a modern method of contraception than those with a higher level. Similarly, female providers directly involved in providing contraceptive services (aOR: 1.82; CI: 1.41–2.35) were nearly twice as likely to use a modern contraceptive method as their counterparts counterparts (Table 2).
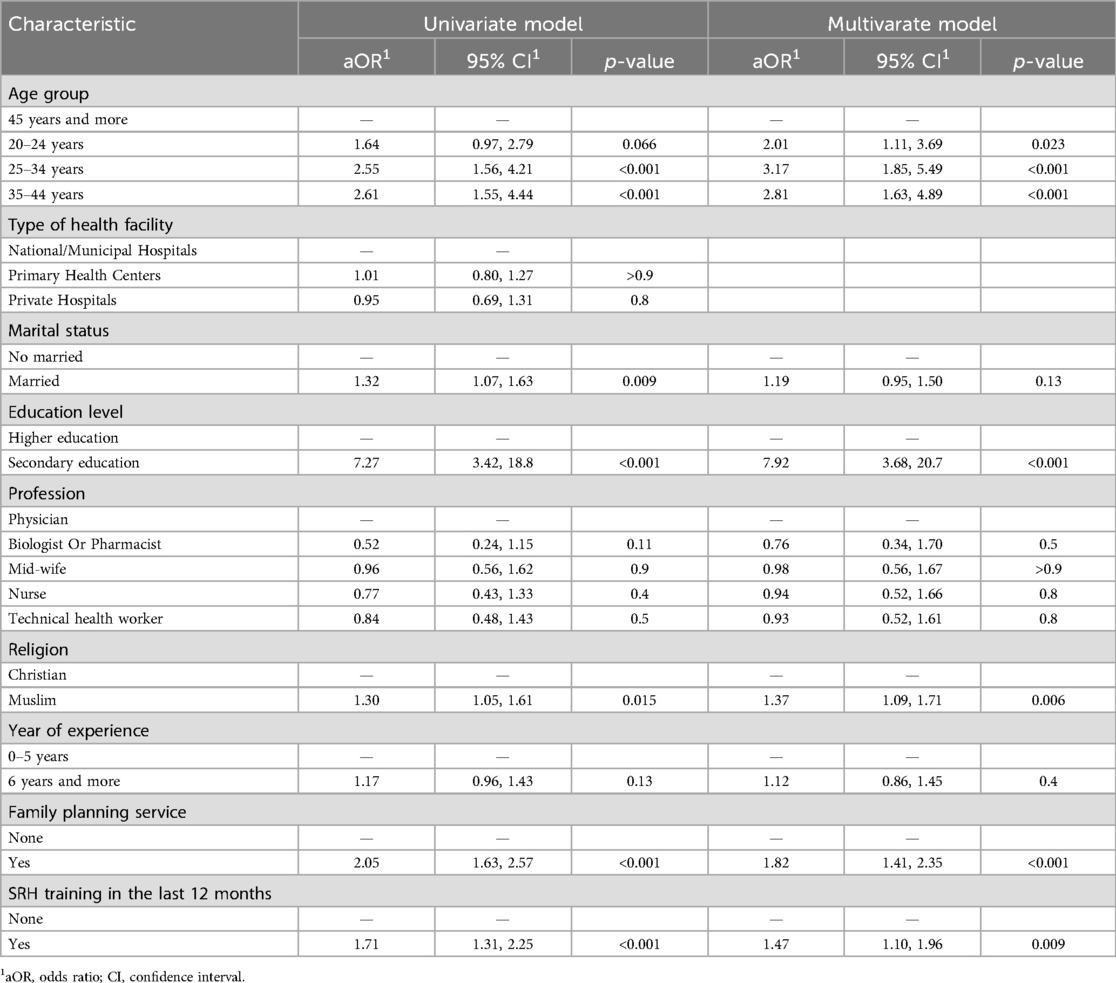
Table 2. Factors associated with the use of modern contraceptives by female health care providers in Guinea.
Female providers who received training in the last 12 months prior to collection were 1.47 times more likely to use modern contraceptive methods. Similarly, Muslim female recipients were 1.37 times more likely to use modern contraceptive methods than their Christian counterparts (Table 2).
Discussion
This study is one of the first to assess the use of modern contraceptive methods among female health care providers in facilities involved in the provision of family planning services in Guinea. It made it possible to estimate the prevalence and identify the factors associated with this use in women of childbearing age. The prevalence observed in our sample was about 62%, a level significantly higher than that reported in the general female population in Guinea according to the 2018 DHS (11%) (24). This difference can be explained by the very nature of our study population, composed exclusively of health professionals, who are probably more informed about the benefits of modern contraceptive methods. Our results are similar to those reported in Uganda (73.6%) (25) and Southern Africa (69%) (26) but higher than those observed in Ghana (18%) (27).
The most commonly used methods in our study were implants, pills, injectable Depo-Provera, and IUD, which is partially consistent with trends observed in other African contexts, although preferences vary by country (17, 24). A disparity in prevalence was observed between administrative regions, with particularly high use in Kindia and Kankan. These results could be attributed to targeted interventions by technical and financial partners in these regions, including capacity-building sessions and the provision of free family planning services (29).
In terms of associated factors, our analysis found a significant association between educational attainment, participation in the provision of modern contraceptive services, having received training in the past 12 months, and religion and use of modern contraceptive methods. Although training in sexual and reproductive health (SRH) services in the past year was significantly associated with contraceptive use in univariate analysis, this association did not persist in the multivariate model. This result could be explained by the confounding influence of other variables, such as job role or previous exposure to family planning programs. Similar observations have been reported in previous studies, where the initial effect of training decreased after adjusting for sociodemographic and institutional factors that had a stronger predictive value for contraceptive use (30). This highlights the fact that while training remains important, it cannot independently lead to behaviour change unless it is complemented by supportive environments and continuous professional development.
Women under the age of 45 were more likely to use a modern contraceptive method. This can be explained by the socio-cultural context of Guinea, where a majority of women marry young (between 15 and 23 years old), which leads them, after reaching the desired number of children, to use contraception more frequently to space or limit births. This finding is consistent with other studies conducted in Africa and the Maghreb (31, 5).
Regarding educational attainment, a counterintuitive result was observed: women with a secondary education were more likely to use a modern contraceptive method than those with a higher level of education. In our population of health care providers, this could be because women at the secondary level are often midwives or health technicians directly involved in the delivery of family planning services. Their hands-on training and daily exposure to contraceptive methods likely increases their familiarity with and adherence to these methods. It is also possible that awareness campaigns will target more mid-level providers, strengthening their personal commitment to contraceptive use.
Limitations and strengths of the study
Our study presents a limitation as well as strengths: From a limiting point of view, it should be mentioned that sexuality is a taboo subject for the population. Talking about family planning makes some people hesitant. Therefore, it is not easy to ensure that women provide honest answers to all questions, particularly those relating to the use of contraceptive methods. Furthermore, our study has strengths. It was conducted on a representative sample of all female providers in the country.
Conclusion
This study shows that more than two-thirds of female healthcare providers use modern contraceptive methods in Guinea, which is generally satisfactory. Factors associated with the use of modern contraceptive methods were young age, secondary education level, religion, women's involvement in family planning services and recent SRH training.
The implications of this study would be to define strategies and interventions focused on the main factors identified. It would be helpful for decision-makers to direct future interventions on the continuing training of providers and emphasize education and awareness campaigns for all stakeholders. The authorities should periodically initiate capacity-building sessions on family planning. They should also think about the One Health aspect by including all staff from all public and private structures as well as NGOs in the implementation of continuing training on SRH and FP.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comité National d'Ethique pour la Rechercche en Santé (CNERS). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
YY: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Software, Validation, Writing – original draft, Writing – review & editing. SS: Formal analysis, Supervision, Methodology, Writing – review & editing. HGC: Data curation, Formal analysis, Writing – review & editing. MK: Project administration, Supervision, Writing – review & editing. SC: Data curation, Formal analysis, Writing – review & editing. SB: Project administration, Supervision, Writing – review & editing. KO: Data curation, Formal analysis, Writing – review & editing. MG: Methodology, Writing – review & editing. MD: Supervision, Writing – review & editing. EB: Supervision, Writing – review & editing. OD: Supervision, Writing – review & editing. IC: Supervision, Writing – review & editing. ST: Supervision, Writing – review & editing. AK: Supervision, Writing – review & editing. AT: Supervision, Writing – review & editing. AD: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors would like to thank the French Embassy in Guinea through the Guinea Infectious Diseases Research and Training Center for its technical and financial support during the workshops for developing scientific articles, which encouraged writing, and the supervisors of the various article development workshops for their technical support and advice during the completion of the study. We also thank the French Development Agency, Expertise France, and TDR for funding the doctoral student.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
FP, family planning; SRH, reproductive sexual health; CMC, municipal medical center; MC, contraceptive method; DRC, Demographic Republic of Congo; NGO, Non-Governmental Organization.
References
1. Bearak J, Popinchalk A, Ganatra B, Moller A-B, Tunçalp Ö, Beavin C, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Health. (2020) 8:e1152–61. doi: 10.1016/S2214-109X(20)30315-6
2. Department of Economic and Social Affairs, Population Division. World Family Planning 2022, Meeting the Changing Needs for Family Planning: Contraceptive use by age and Method. United Nation (2022). Available at: https://www.researchgate.net/publication/368779597_World_Family_Planning_2022_Meeting_the_changing_needs_for_family_planning_Contraceptive_use_by_age_and_method (Accessed June 12, 2025).
3. Vodouhe T, Dangbemey P, Aboubaka M, Tohodjede Y, Tshabu Aguemon C, Denakpo JL. 15-5 - facteurs associés à l’utilisation des méthodes contraceptives chez les femmes en âge de procréer dans un pays de l’Afrique subsaharienne à faible prévalence contraceptive en 2023, république du bénin. J Epidemiol Popul Health. (2024) 72:202625. doi: 10.1016/j.jeph.2024.202625
4. World Health Organization. Monitoring Health for the Sustainable Development Goals (SDGs). Genève: World Health Organization (2016).
5. Dimassi K, Douik F, Douzi MA, Saidi O, Ben Romdhane H. Les déterminants sociaux de l’utilisation des méthodes contraceptives en Tunisie. Rev Epidemiol Sante Publique. (2017) 65:53–9. doi: 10.1016/j.respe.2016.06.330
6. Matungulu CM, Kandolo SI, Mukengeshayi AN, Nkola AM, Mpoyi DI, Mumba SK, et al. Déterminants de l’utilisation des méthodes contraceptives dans la zone de santé mumbunda à lubumbashi, république démocratique du Congo. Pan Afr Med J. (2015) 22:1–9. doi: 10.11604/pamj.2015.22.329.6262
7. Takada K, Yode M. Facteurs associés au non recours aux méthodes contraceptives modernes chez les femmes en union du 6ème Arrondissement de la ville de N’Djamena (2023).
8. Boadu I. Coverage and determinants of modern contraceptive use in Sub-Saharan Africa: further analysis of demographic and health surveys. Reprod Health. (2022) 19:18. doi: 10.1186/s12978-022-01332-x
9. Ntambue AM, Tshiala RN, Malonga FK, Ilunga TM, Kamonayi JM, Kazadi ST, et al. Utilisation des méthodes contraceptives modernes en république démocratique du Congo: prévalence et barrières dans la zone de santé de Dibindi à Mbuji-Mayi. Pan Afr Med J. (2017) 26:1–8. doi: 10.11604/pamj.2017.26.199.10897
10. Tshilonda JCB, Tshibanda AK, Katambue JK, Kabemba GK, Kabemba RK, Ngoyi CK, et al. Rate of use of female condoms in sex professionals in the city of Mbuji-Mayi, democratic Republic of Congo. OALib. (2020) 07:1–9. doi: 10.4236/oalib.1106710
11. Moise KK, Blood BND, Paul CM, Réne MMJ, Odette KM, Benjamin KK, et al. Prevalence of low birth weight in Mbuji-Mayi city, democratic Republic of Congo. OALib. (2017) 04:1–6. doi: 10.4236/oalib.1103474
12. Institut National de la statitique. Enquête Démographique et de Santé. Guinée: u Ministère du Plan et du Développement Économique (2018).
13. Ntambue AM, Tshiala RN, Malonga FK, Ilunga TM, Kamonayi JM, Kazadi ST, et al. Use of modern contraceptive methods in the democratic republic of the Congo: prevalence and barriers in the health zone of Dibindi, Mbuji-Mayi. Pan Afr Med J. (2017) 26:199. doi: 10.11604/pamj.2017.26.199.10897
14. Dramé L, Kolié D, Sidibé S, Yombouno JF, Delamou A. Facteurs associes a l’utilisation des methodes contraceptives chez les jeunes filles eleves en milieu rural guineen. Santé Publique. (2023) 35:129–40. doi: 10.3917/spub.236.0129
15. World Health Organization (WHO). Principaux Faits sur la Planification Familiale/contraception. WHO (2022). Available at: https://www.who.int/fr/news-room/fact-sheets/detail/family-planning-contraception (Accessed September 21, 2024).
16. Blackstone SR, Nwaozuru U, Iwelunmor J. Factors influencing contraceptive use in Sub-Saharan Africa: a systematic review. Int Q Community Health Educ. (2017) 37:79–91. doi: 10.1177/0272684X16685254
17. Ba DM, Ssentongo P, Agbese E, Kjerulff KH. Prevalence and predictors of contraceptive use among women of reproductive age in 17 Sub-Saharan African countries: a large population-based study. Sex Reprod Healthc. (2019) 21:26–32. doi: 10.1016/j.srhc.2019.06.002
18. Asmamaw DB, Eshetu HB, Negash WD. Individual and community-level factors associated with intention to use contraceptives among reproductive age women in Sub-Saharan Africa. Int J Public Health. (2022) 67:1604905. doi: 10.3389/ijph.2022.1604905
19. Opee J, Opiro K, Manano P, Sikoti M, Ayikoru J, Akello H, et al. We provide the methods to others but we don’t use the methods ourselves”: challenges with utilization of modern contraception among female healthcare workers at two tertiary teaching hospitals, northern Uganda. Contracept Reprod Med. (2024) 9:54. doi: 10.1186/s40834-024-00313-8
20. Fatima KD. Evaluatio Rapide de la Situation sur le DMPA-SC en Guinée. Conakry: Ministère de la santé et de l’hygiène publique Guinée (2019).
21. Sidibé S, Delamou A, Camara BS, Dioubaté N, Manet H, El Ayadi AM, et al. Trends in contraceptive use, unmet need and associated factors of modern contraceptive use among urban adolescents and young women in Guinea. BMC Public Health. (2020) 20:1840. doi: 10.1186/s12889-020-09957-y
22. Sidibé S, Grovogui FM, Kourouma K, Kolié D, Camara BS, Delamou A, et al. Unmet need for contraception and its associated factors among adolescent and young women in Guinea: a multilevel analysis of the 2018 demographic and health surveys. Front Glob Women’s Health 2022;3:932997.
23. Manet H, Doucet M-H, Bangoura C, Dioubaté N, El Ayadi AM, Sidibé S, et al. Factors facilitating the use of contraceptive methods among urban adolescents and youth in Guinea: a qualitative study. Reprod Health. (2023) 20:89. doi: 10.1186/s12978-023-01621-z
24. Mpela EA, Bukasa AK, Bukasa MT, Marie-Claire OO, Kumona VB, Badibake AT, et al. Knowledge and practice of contraception by the inhabitants of the health zone of Kansele, city of Mbuji-Mayi, democratic Republic of Congo. Open Access Library Journal. (2023) 10:1–17. doi: 10.4236/oalib.1110641
25. Opiro K, Opee J, Sikoti M, Pebalo PF, Ayikoru JH, Akello H, et al. Utilization of modern contraceptives among female health care workers at Gulu university teaching hospitals in northern Uganda. Contracept Reprod Med. (2024) 9:13. doi: 10.1186/s40834-024-00274-y
26. Gribble J, Haffey J. La Santé Reproductive en Frique Subsaharienne. Afrique Subsaharienne: USAID (2009).
27. Agbeno EK, Osarfo J, Anane-Fenin B, Achampong EK, Neequaye NA, Opoku DA, et al. Attitudes and practices of healthcare professionals and clinical medical students on contraception: a cross-sectional study in Cape Coast, Ghana. Int J Reprod Med. (2021) 2021:6631790. doi: 10.1155/2021/6631790
28. Leye MMM, Faye A, Diongue M, Wone I, Seck I, Ndiaye P, et al. Déterminants de l’utilisation de la contraception moderne dans le district sanitaire de mbacké (sénégal). Santé Publique. (2015) 27:107–16. doi: 10.3917/spub.151.0107
29. Family Planning Estimation Tool (FPET). Ghana: FP2030 Indicator Summary Sheet: 2022 Measurement Report. Guinea: Family Planning Estimation Tool (2022). Available at: https://www.track20.org/pages/data_analysis/core_indicators/progress_report.php (Accessed June 12, 2025).
30. Mwaikambo L, Speizer IS, Schurmann A, Morgan G, Fikree F. What works in family planning interventions: a systematic review. Stud Fam Plann. (2011) 42:67–82. doi: 10.1111/j.1728-4465.2011.00267.x
Keywords: modern contraceptive method, use, Guinea, prevalence, associated factors
Citation: Youla Y, Sidibé S, GC H, Kourouma M, Camara SC, Bangoura ST, Olivier KKJJ, Grovogui M, Diaby M, Bongono EF, Diallo OH, Conté I, Traoré S, Djigui Keita A, Touré A and Delamou A (2025) Prevalence and factors associated with the use of modern contraceptive methods among female healthcare providers in health facilities in Guinea. Front. Glob. Women's Health 6:1567960. doi: 10.3389/fgwh.2025.1567960
Received: 29 January 2025; Accepted: 28 May 2025;
Published: 19 June 2025.
Edited by:
Michael Amoh, University of Health and Allied Sciences, GhanaReviewed by:
Omotade Adebimpe Ijarotimi, Obafemi Awolowo University, NigeriaAboubacar Sidiki Magassouba, International Union Against Tuberculosis and Lung Disease (The Union), France
Copyright: © 2025 Youla, Sidibé, GC, Kourouma, Camara, Bangoura, Olivier, Grovogui, Diaby, Bongono, Diallo, Conté, Traoré, Djigui Keita, Touré and Delamou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yamoussa Youla, eW91bGEyY291bEBnbWFpbC5jb20=
†ORCID:
Yamoussa Youla
orcid.org/0009-0006-9803-6010