 Lucrecia Mena-Meléndez
Lucrecia Mena-Meléndez- Department of Applied Health Science, Indiana University, Bloomington, IN, United States
Introduction: In Latin America, 26 percent of women use sterilization to avert unwanted pregnancies. Although sterilization provides first-tier effectiveness, long-acting continuation over time, and life-long cost-benefit, previous research has documented persistent inequalities in access and use worldwide.
Methods: This study uses Demographic and Health Survey (DHS) data for Bolivia, Colombia, Guatemala, and Peru (1986-2015), to explore ethnoracial, geographic, socioeconomic, individual, and reproductive differences in female sterilization [N (level-1 women) = 112,135; N (level-2 clusters) = 4,946].
Results: Results from descriptive analyses and logistic multilevel regression models indicate that ethnoracial minorities and rural women had lower odds of reporting female sterilization as their current contraceptive method. Compared to Bolivian women, Colombian and Guatemalan women had higher odds of reporting sterilization, while Peruvian women had lower odds. Older, wealthier, more educated, and those employed outside the home had higher odds of reporting sterilization. Additionally, those older at first birth, with higher parity, with a longer interval since preceding birth, and with previous experience with unintended pregnancies had higher odds of reporting sterilization.
Discussion: Findings suggest that social, geographic, and structural factors may shape equitable access to sterilization for some groups. Future efforts should prioritize reducing access gaps between ethnoracial groups and rural-urban populations by strengthening health systems and ensuring culturally appropriate, equitable care.
1 Introduction
More than one-fourth of married or cohabiting women of reproductive age in the world—who use any contraceptive method—rely on sterilization (1). With approximately 219 million globally, this makes sterilization the most commonly used contraceptive method. Latin America and the Caribbean is a highly reliant region, with 26 percent of women of reproductive age using sterilization to avert unwanted pregnancies (1). Through either a minilaparotomy or laparoscopy procedure, female sterilization involves obstruction of the fallopian tubes (with ligatures, clips, bands, or electrocoagulation), impeding sperm transport to the tube, where fertilization of the egg occurs (2, 3). Permanent contraception (PC), such as sterilization, provides superior benefits compared to short-acting reversible contraception (SARC) and equal to and/or superior benefits to long-acting reversible contraception (LARC).1 First, sterilization is a first-tier highly effective method, with fewer than 1 in 100 (0.01%) women getting pregnant within 1 year of having the surgery; second, it offers long-acting continuation over time given that it is considered, for the most part, a permanent contraceptive method; third, it provides life-long cost-benefits as it involves one single procedure, which typically requires no follow-up care, and which becomes cheaper over the long-term than other methods (2, 4).
Despite this, previous research has documented persistent inequalities in sterilization access and use worldwide, particularly concerning socioeconomic status, race/ethnicity, education, geography, fertility goals and intentions, and other individual characteristics (5–8). On the one hand, some studies have found that female sterilization remains most common among socioeconomically disadvantaged and ethnoracial minorities worldwide (7–10). In the United States, researchers have documented differences in sterilization by race, with minority women more likely to undergo the procedure than non-minority women (11, 12). Other research has also looked at the geography of sterilization, finding that where someone lives may determine their sterilization outcome (13). On the one hand, research has found that rural women have an increased likelihood of undergoing sterilization compared to urban and suburban women (14), while other research has found the opposite (15).
More broadly on sexual and reproductive health in Latin America and the Caribbean, researchers have found wealth-related inequalities in the use and prevalence of LARC (16). Other research has also assessed differences in contraceptive nonuse in the region, finding that women who reported more wealth, more education, were employed in industries outside the home, were married/living together, and were older, had a lower risk of reporting contraceptive nonuse (17). Despite this, research on the use and access of sterilization in this region is much more limited. Some research in Colombia has reported observed differences in sterilization rates, with disadvantaged women, such as young, poor, and less educated, relying on sterilization more than others (18). Other research reported that public sterilization programs have used economic incentives to increase the number of sterilization procedures among Afro-Colombian women (19). However, in a multi-county research study, Ugaz et al. (20) found that female sterilization is most common among people with higher wealth, particularly in Latin America and the Caribbean.
Compared to SARC and LARC use, which are reversible methods more commonly used to decrease, delay, or space pregnancies (21), sterilization is more commonly used by women who want to prevent pregnancy permanently, given that they do not want any more children (22, 23). Arguably, in these cases, sterilization is a preferred contraceptive method to prevent childbearing because it helps overcome poor human compliance and errors that may arise with other contraceptive regimes (24). However, if sterilization inequalities exist—across socioeconomic status, ethnoracial identity, geography, or other characteristics—and some women are unable to access or use sterilization to prevent future pregnancies despite wanting to, this may signify that social, geographic, and structural determinants are impeding women's abilities to exercise their reproductive rights and control their bodies and fertility. With very limited previous research that has assessed female sterilization in Latin America, more research on this is warranted. The present study aims to fill this gap by exploring ethnoracial, geographic, socioeconomic, individual, and reproductive differences in female sterilization in Bolivia, Colombia, Guatemala, and Peru.
2 Material and methods
2.1 Data and sample
This analysis uses pooled cross-sectional Demographic and Health Survey (DHS) data from Bolivia, Colombia, Guatemala, and Peru—collected between 1986 and 2015—to conduct a population-based cross-sectional study of female sterilization. DHS data is a publicly-available, nationally-representative survey of women aged 15–49 collected by ICF International in collaboration with host country governments (25). The survey employs a two-stage stratified cluster-sampling design to randomly select women within households and clusters.2
For this study, country selection was guided by both theoretical and practical considerations. Theoretically, Bolivia, Colombia, Guatemala, and Peru have sizable indigenous, afro-descendent, and/or other minority populations and distinct histories of reproductive governance (26), making them relevant for understanding ethnoracial disparities in sterilization. According to their most recent national censuses, these populations represent approximately 41% of the population in Bolivia, 14% in Colombia, 44% in Guatemala, and 26% in Peru. Practically, these four countries were the only ones in Latin America with recent and multiple waves of DHS data collected between 1986 and 2015 that included both contraceptive use and measures of ethnoracial identity. Other Latin American countries with high ethnic and/or racial diversity (e.g., Brazil, Ecuador, Mexico) were excluded due to outdated surveys, the availability of only a single DHS wave, or the absence of relevant variables. Supplementary Figure S1 provides a detailed country and sample selection process. The sample was limited to women of reproductive age (15–49 years), married or cohabitating, using contraception, and with complete survey data on contraceptives and sterilization.3 The total study sample includes 112,135 women (level-1) and 4,946 clusters (level-2). This study was approved by the Institutional Review Board at the University of California, Los Angeles.
2.2 Measures
2.2.1 Dependent Variable
The dependent variable in this study is female sterilization, which indicates whether a woman relies on sterilization as their contraceptive method. A dichotomous outcome was constructed using a variable that was originally categorical. Participants were asked: “Which [contraceptive] method are you using?” and provided with a list of 15 modern and traditional contraceptive methods.4 The responses for women who reported using sterilization as their contraceptive method were coded as one (1) and the responses for women who reported not using sterilization as their contraceptive method (using another modern or traditional contraceptive method) were coded as zero (0). Participants who reported not using contraception were excluded from the analysis. Table 1 presents percentage distributions of the prevalence of sterilization and ethnoracial self-identification by and across countries.
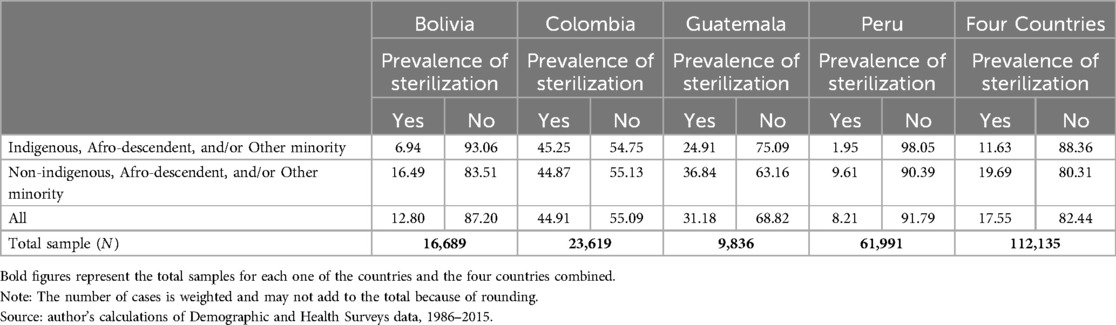
Table 1. Percentage distribution of prevalence of sterilization and ethnoracial self-identification of women (married or cohabitating, using contraception, aged 15–49) by and across countries.
2.2.3 Independent variables
The primary independent variable in this study is ethnoracial self-identification, operationalized as a dichotomous variable indicating whether a woman self-identifies as indigenous, afro-descendent, and/or other minority or not. Self-identified ethnicity (Colombia: Indigenous, Gypsy/Rom, Raizal, Palenquero, Black/Mulatto/Afro-Colombian/Afro-descendant; Guatemala: Maya, Garifuna, Xinca, Other) and language spoken at home (Bolivia: Quechua, Aymara, Guaraní, Other; Peru: Quechua, Aymara, Other) was used to construct this measure. While DHS datasets provide ethnoracial indicators, the structure and categories vary by country and survey year. To enable cross-national comparison and maintain analytic consistency, these categories were harmonized into a binary classification: indigenous, afro-descendent, and/or other minority (1) compared to non-indigenous, afro-descendent, and/or other minority (0). This decision was informed by limitations in available categories across surveys, small sample sizes in some subgroups, and inconsistencies in coding over time. However, this dichotomization may obscure important intra-group variation and reduce cultural specificity. These trade-offs are acknowledged as a limitation, particularly in the interpretation of cross-country differences. Self-identified ethnicity and language are standard measures of ethnoracial identity used in previous research (27–29). While other research recommends using multiple self-identification measures, interviewer-ascribed phenotypic classifications, and multiple sub-categories of race and ethnicity (30, 31), DHS data does not consistently collect such measures across countries, or has only started collecting such data. Supplementary Table S1 presents percentage distributions of ethnoracial self-identification by country. Supplementary Table S2 compares how DHS survey questionnaires ask about ethnoracial self-identification in these four countries.
This study also controlled for place of residence (rural, urban), household wealth (poorest, poorer, middle, richer, and richest), years of education (0, 1–3, 4–6, 7–9, ≥10 years), occupation (not working, managerial, clerical, sales, agricultural, domestic and other services, manual labor), husband's education (0–23), age (15–19, 20–24, 25–34, 35–49), age at-first-birth (8–14, 15–19, 20–34, 35+), number of living children (1–2, 3–4, 5+), interval since preceding birth (>2, 2–4, 4+), intention of last pregnancy (intended, unintended), and previous abortion (yes, no). Table 2 presents percentage distributions of selected characteristics by ethnoracial self-identification and the entire sample.
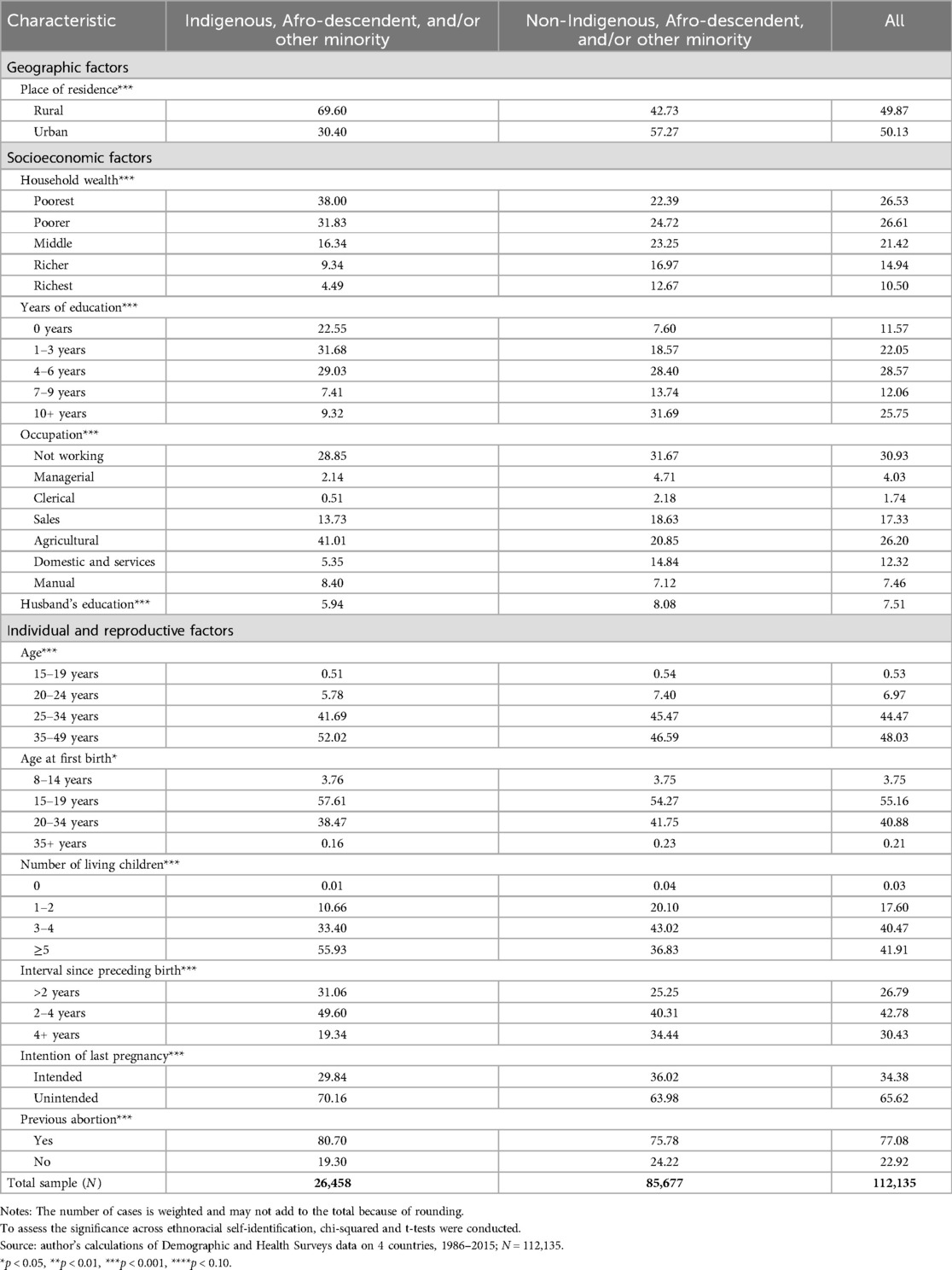
Table 2. Sample characteristics of women (married or cohabitating, using contraception, aged 15–49), by ethnoracial self-identification.
2.3 Analyses
To explore the relationship between ethnoracial self-identification and female sterilization across pooled waves and countries, DHS recommendations (32) were followed to de-normalize the women's individual standard weight (for each wave and each country) by dividing the women's individual standard weight (v005) by 1,000,000. Then, a new sample weight was created by multiplying the de-normalized weight by the estimated population of women aged 15–49 in the country during the year of the DHS survey (as reported by the World Bank Open Data), and then dividing by the number of women aged 15–49 interviewed in that survey. This step adjusts for differences in survey sample size and ensures that each country contributes proportionally to the pooled analysis. This approach follows guidance outlined in DHS Analytical Reports and comparative survey methodology documentation. After weight construction, all datasets were appended, and survey design variables were specified using the svyset command in Stata 16 (33). Primary sampling units (v021), stratification [region (v024), urban/rural (v025)], and adjusted weights were specified to account for the complex survey design and to produce valid standard errors. All descriptive statistics and multilevel analyses were weighted accordingly. Analyses were conducted in three steps. First, the distribution of the characteristics described above was assessed across ethnoracial self-identification. Second, chi-square tests were conducted to examine bivariate associations. Third, three multilevel logistic regression models were constructed to measure the relative odds of female sterilization by ethnoracial self-identification, while controlling for selected characteristics. To respect the hierarchical design of DHS data, a two-level multilevel logistic regression approach was used, whereby individual women units (level-1) were nested within survey cluster units (level-2).5 The models include a random intercept at the cluster-level—to capture unobserved heterogeneity among clusters—and fixed effects for all other individual-level coefficients. Finally, survey year and country fixed effects were included in all models to account for temporal and contextual variation. Model 1 regressed female sterilization on survey year, ethnoracial self-identification, and geographic factors. Model 2 controlled for socioeconomic factors. Finally, Model 3 controlled for additional individual and reproductive factors.
Across all models, an interaction term was also included between ethnoracial self-identification and place of residence to examine the extent that place of residence moderated the relationship between ethnoracial self-identification and sterilization. Previous research indicates that in non-linear models, the product of the interaction (i.e., coefficient) can be misleading and insufficient for drawing conclusions (34–36). Based on methodological recommendations, the margins command in Stata was used to calculate the predicted probabilities (from the coefficient estimates in Model 3) and relied on tests of the predictive probabilities to determine whether an interactive effect existed between ethnoracial self-identification and place of residence. Supplementary File S1 presents annotated Stata code used for weight construction, model estimation, and marginal predictions. Additional code or details are available upon request. Unless noted otherwise, any differences mentioned in the following sections are statistically significant.
3 Results
3.1 Multivariate results for female sterilization by ethnoracial, geographic, socioeconomic, individual, and reproductive factors
Table 3 presents the results of the multilevel logistic models predicting female sterilization of married or cohabitating women aged 15–49 [N (level-1) = 112,135; N (level-2) = 4,946]. Results from Model 1 indicate that indigenous, afro-descendent, and/or other minority women had significantly lower odds of reporting female sterilization as their current contraceptive method compared to non-indigenous, afro-descendent, and/or other minority women (OR = 0.56, p < 0.001). In addition, the odds of reporting sterilization varied by geographic factors. Colombian and Guatemalan women had higher odds of reporting sterilization than Bolivian women (OR = 4.21, p < 0.001; OR = 2.47, p < 0.001, respectively), whereas Peruvian women had lower odds (OR = 0.50, p < 0.001). Additionally, rural women had significantly lower odds of reporting sterilization compared to urban women (OR = 0.46, p < 0.001).
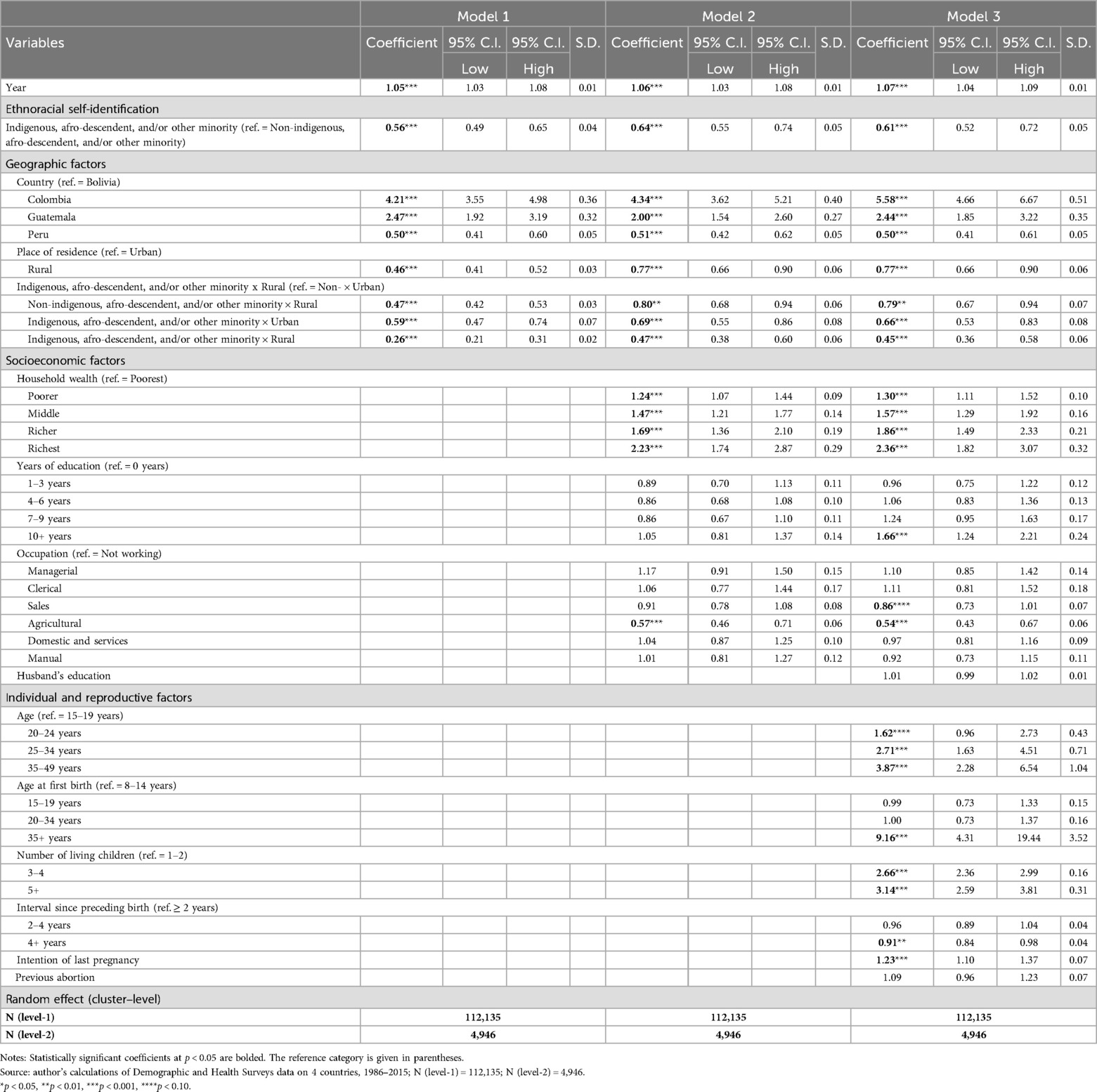
Table 3. Odds ratios from multilevel logistic regression analysis predicting sterilization of women (married or cohabitating, using contraception, aged 15–49).
Even after controlling for socioeconomic factors, results from Model 2 indicate that ethnoracial self-identification continues to be associated with lower odds of reporting female sterilization as a current contraceptive method (OR = 0.64, p < 0.001). Additionally, women who reported higher wealth—richest (OR = 2.23, p < 0.001)—had higher odds of reporting sterilization. Conversely, women who reported living in rural areas (OR = 0.77, p < 0.001) and working in agriculture (OR = 0.57, p < 0.001) had lower odds of reporting sterilization.
Model 3 presents the fully adjusted model after controlling for all remaining individual and reproductive factors. Once again, ethnoracial self-identification was associated with significantly lower odds of reporting female sterilization as their current contraceptive method (OR = 0.61, p < 0.001). Additionally, results indicate that older women—35–49 years (OR = 3.87, p < 0.001); older at first-birth—35 + years (OR = 9.16, p < 0.001); with 3–4 and 5+ living children (OR = 2.66, p < 0.001; OR = 3.14, p < 0.001); and with previous experiences with unintended pregnancies (OR = 1.23, p < 0.001) had higher odds of reporting sterilization. On the other hand, women who reported living in rural areas (OR = 0.77, p < 0.001), working in agriculture (OR = 0.54, p < 0.001), and with a longer interval since preceding birth—4 + years (OR = 0.91, p < 0.01)—had lower odds of reporting sterilization.
To properly examine the interaction between ethnoracial self-identification and place of residence on female sterilization, predicted probabilities were calculated from the fully adjusted multilevel logistic regression model (Table 3, Model 3) using the margins command in Stata and relying on tests of the predictive probabilities. Figure 1 presents the predicted probabilities with 95% confidence intervals and the tests of first and second differences. The first differences capture the effect of place of residence given respondents’ ethnoracial self-identification. The second difference test whether the effect of place of residence significantly differs by respondents’ ethnoracial self-identification Results indicate that among non-indigenous, afro-descendent, and/or other minority respondents, those living in rural areas had a lower predicted probability of reporting sterilization as their current contraceptive method (Pr = 0.173, 95% CI: 0.160–0.185) compared to those in urban areas (Pr = 0.201, 95% CI: 0.187–0.214; Δ = −0.028, p < 0.01). Similarly, among indigenous, afro-descendent, and/or other minority respondents, those living in rural areas had a lower probability of reporting sterilization as their current contraceptive method (Pr = 0.116, 95% CI: 0.099–0.132) than those in urban areas (Pr = 0.152, 95% CI: 0.131–0.174; Δ = −0.036, p < 0.01). The test of second difference was not statistically significant (Δ = −0.008, p > 0.05), indicating that the effect of place of residence does not vary significantly by respondents’ ethnoracial self-identification. In other words, women in urban areas had a higher probability of reporting sterilization as their current contraceptive method, regardless of ethnoracial self-identification.
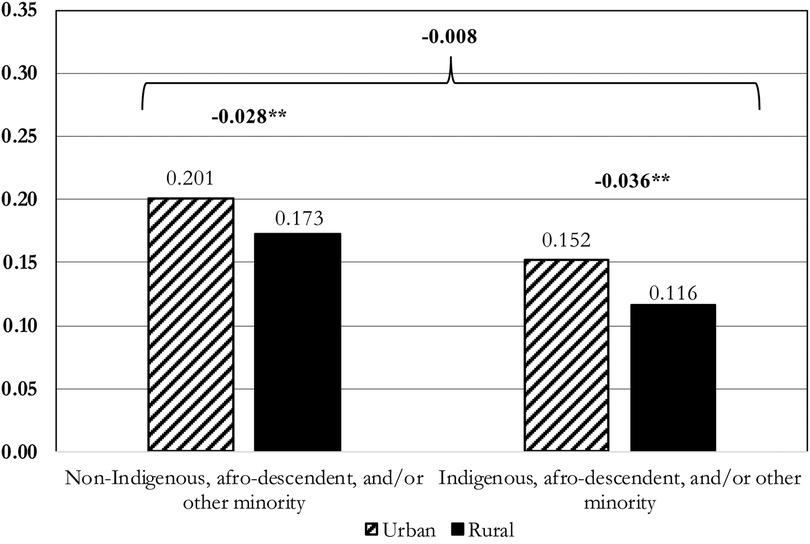
Figure 1. Probabilities of sterilization of women (married or cohabitating, using contraception, aged 15–49), by ethnoracial self-identification and place of residence. Source: author's calculations of Demographic and Health Surveys data on 4 countries, 1986-2015; N (level-1) = 12,135; N (level-2) = 4,946.Notes: Predicted probabilities and 95% confidence intervals are based on margins computed from the fully adjusted multilevel logistic regression (Model 3). Estimates are as follows:
• Non-Indigenous, afro-descendent, and/or other minority, Urban: 0.201 [95% CI: 0.187, 0.214]
• Non-Indigenous, afro-descendent, and/or other minority, Rural: 0.173 [95% CI: 0.160, 0.185]
• Indigenous, afro-descendent, and/or other minority, Urban: 0.152 [95% CI: 0.131, 0.174]
• Indigenous, afro-descendent, and/or other minority, Rural: 0.116 [95% CI: 0.099, 0.132]
4 Discussion
The present study used Demographic and Health Survey (DHS) data (1986–2015) to explore ethnoracial, geographic, socioeconomic, individual, and reproductive differences in female sterilization in Bolivia, Colombia, Guatemala, and Peru. Very few studies to date have examined female sterilization in this region. Four key findings emerged from this study.
First, even after controlling for all factors, ethnoracial minority women have lower odds of reporting female sterilization as their current contraceptive method compared to non-ethnoracial minority women. This finding conflicts with research in the United States that reports that minority women are more likely to undergo sterilization than non-minority women (11, 12). However, the experiences of ethnic-minority women in Latin America are substantially different from those of women in the United States, or to that end, from those of women in other parts of the world, so we should be careful when comparing across regions. In Latin America, most minorities live in extreme poverty, have high illiteracy rates, work in informal occupations, have worse health outcomes, and have limited to no access to insurance or healthcare systems (37–39). Previous research in the United States and Latin America has found that insurance and socioeconomic status are strong predictors of female sterilization (40–42). Thus, lack of insurance and/or limited access to healthcare may provide one possible explanation of why ethnoracial minority women have lower odds of reporting sterilization than non-ethnoracial minorities. This finding can also be understood through the lens of reproductive justice, which emphasizes the right to have children, not have children, and to parent in safe and sustainable communities (43). Lower odds of reporting sterilization may reflect not only limited access to insurance or healthcare systems, but also institutional discrimination—defined as the systemic exclusion of marginalized groups from reproductive autonomy through policy, provider bias, and health system neglect (44, 45). In Latin America, the intersection of poverty, rural residence, and minoritized status may restrict the conditions under which women can make fully informed and supported contraceptive choices (46).
Second, results from this study indicate that female sterilization differs across geographical factors. More generally, rural women are less likely to report sterilization. Previous research in this area is conflicting, but this finding does align with research from Latin America and other developing regions (15, 47). Generally, urban women have better sexual and reproductive health outcomes than rural women because urban areas have greater, expanded, and improved access to, delivery of, and funding for modern family planning methods and services (48, 49). In addition, it is possible that higher sterilization in urban areas is explained by normative, socio-demographic, and cultural differences between rural-urban women. For example, the desire for smaller families, higher costs of childbearing, or changes in gender and family expectations and dynamics in urban areas. Findings also indicate differences by country, with Colombian and Guatemalan women more likely to report sterilization compared to Bolivian women, while Peruvian women are less likely. These cross-country variations are reported widely in the literature and may be explained by the history of sterilization availability, promotion, and acceptance in a given country (50, 51). Despite sharing close geographic proximity, as well as centuries of ethnolinguistic, geopolitical, and historically communal legacies (52), each one of these countries is also unique, so these differences are to be expected.
Third, the findings from this study indicate significant differences in sterilization by socioeconomic factors, particularly wealth, education, and occupation. While some research has found that female sterilization remains most common among socioeconomically disadvantaged women (7), some research in Latin America has found the opposite—that female sterilization is most common among wealthier women (20, 41). Given that many countries’ public health systems do not cover the procedure, or require extensive wait times or paperwork (41), women with more wealth or education, who may also be able to afford private insurance, may have more access to information about sterilization and have the financial opportunity to undergo the procedure itself.
Fourth, findings also suggest disparities by individual and reproductive factors, particularly age, age at first birth, parity, interval since preceding birth, and previous unintended pregnancies. That is, results indicate that those who had achieved their desired fertility were more likely to report sterilization. These findings are consistent with previous research that has found that sterilization prevalence increases with age, parity, and prior experience with an unintended pregnancy (50, 53, 54). Other research has also found that providers assess risk factors for sterilization regret and adjust their advice or recommendation for the procedure depending on a patient's age, parity, and spousal agreement (55). Some research has found evidence that women have been dissuaded or refused from undergoing the procedure due to their age or parity, due to possible procedural regret (56). Given the present findings, it is possible that younger women, younger mothers, and those with fewer children, but who do not want more children, are not receiving information or advice about sterilization as a possible permanent contraceptive option, which may be compromising their reproductive autonomy. Future research could incorporate in-depth interviews to explore further how institutional, structural, and cultural factors shape women's access to sterilization in different contexts. This includes investigating the roles of consent protocols, provider bias, and localized social norms, especially for ethnoracial minority and rural women. Longitudinal or mixed-methods studies could also help assess how access and decision-making around sterilization evolve over time, particularly as health systems and policy landscapes shift. Attention to intersecting inequalities—such as geography, race/ethnicity, and insurance status—can further illuminate the social determinants of sterilization access and unmet need across Latin America.
4.1 Limitations
Although this study has made a substantial set of contributions, the following limitations and the need for future research should be acknowledged. First, the analyses relied on self-reported data, so the results depend on the information that respondents selectively chose to share and/or failed to recall about current or previous experiences. Particularly, the measure for ethnicity and/or race relied exclusively on self-reported ethnicity or language, which may be a conservative measure given that some individuals may not speak traditional ethnic languages or dialects, or may identify with an ethnic minority but may choose not to self-identify because of stigma and discrimination against minority identities or languages (37). Ideally, future research should use multiple measures or dimensions of race and ethnicity, including measures that account for phenotypic classifications and classifications made by others (31).
In addition, the harmonization of ethnoracial self-identification into a binary classification—indigenous, afro-descendent, and/or other minority vs. non-indigenous, afro-descendent, and/or other minority—represents a trade-off between analytical consistency and cultural specificity. While necessary for cross-national comparison, this simplification may obscure meaningful intra-group variation and reduce the precision of interpreting results across countries. These limitations are particularly relevant given the country-specific differences in how DHS surveys measure and categorize ethnoracial identity.
Second, to make comparable analytical variables across countries and waves, categorical responses were collapsed, which may have led to the loss of significant information. Additionally, pooling data across countries and waves may have artificially inflated the effective sample size, potentially resulting in overestimated statistical power and underestimated standard errors due to design effects and clustering (57). However, pooling datasets together also decreases errors from interviewer noise, poorly worded questions, data entry mistakes, and sampling variability (58). To further address this concern, recommendations from DHS (32) were followed to de-normalize the standard weight to ensure the appropriate contribution of data within each wave and country. Third, this study is unable to control for country- and period-specific characteristics not collected by the DHS (e.g., ethnoracial discrimination, religion, religious beliefs, implementation of consent procedures). Finally, this analysis is limited to four countries in Latin America, so these results cannot be blindly generalized.
5 Conclusion
This study used Demographic and Health Survey (DHS) data for Bolivia, Colombia, Guatemala, and Peru (1986–2015) to examine ethnoracial, geographic, socioeconomic, individual, and reproductive differences in female sterilization. Results indicate consistent differences in female sterilization across these characteristics. These disparities suggest that some groups—particularly ethnoracial minority women, rural residents, and those with fewer resources—may face structural barriers to sterilization as a contraceptive method. There is an urgent need to examine how social, geographic, and institutional factors shape who is offered, informed about, or able to obtain sterilization. Improving equity in family planning will require programs that are attentive to group-specific barriers and that promote informed, voluntary contraceptive use across diverse populations. Future efforts should prioritize reducing access gaps between ethnoracial groups and rural-urban populations by strengthening health systems and ensuring culturally appropriate, equitable care.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The study involving humans was approved by Institutional Review Board at the University of California, Los Angeles. The study was conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
LM-M: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Support for open access publication charges provided by Indiana University Libraries.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgwh.2025.1582729/full#supplementary-material
Supplementary Data Sheet 1 | Supplementary STATA Code.
Footnotes
1. ^SARCs include oral pills (combination or progestin-only), injectable, transdermal patch, vaginal ring, male condom, female condom, diaphragm, sponge, cervical cap, and spermicides and gels; LARCs include intrauterine devices and implants.
2. ^DHS data is collected as follows: First, each province or region of a country is divided into small census Enumeration Areas (EAs). Using probability proportional to size (PPS), some of the areas are then selected randomly to be representative of the region or province, or their urban and rural parts, and are the primary sampling units (PSUs). The PSUs form the survey cluster units (level-2). Within each PSU, about 25-30 households are randomly selected, and all women of reproductive age in the households are interviewed. Women represent the individual women units (level-1) (26).
3. ^As per DHS reporting, this study’s sample included very minimal missing data (coded as values that are missing because of nonresponse or invalid codes assigned by DHS as 96, 97, 98, or 99). For the variables included in the analysis, the ones with missing data were self-reported ethnicity (total missing=0.01%), occupation (total missing=0.07%), husband’s education (total missing=1.43%), age (total missing=0.01%), and pregnancy intention (total missing=0.07%). While minimal, any observations with missing data were excluded from this analysis.
4. ^Modern methods: the pill, IUD, injection, diaphragm, NorplantTM or implant, condom, female condom, foam and jelly, female sterilization, male sterilization, other contraceptive methods, and country-specific contraceptive methods. Traditional or folk methods: lactational amenorrhea, periodic abstinence (rhythm), and withdrawal.
5. ^Compared with single-level regression analysis that assumes that all individuals are independent, this methodology accounts for the fact that individuals in the same cluster may have similar characteristics (33).
References
1. United Nations Department of Economic and Social Affairs. World Family Planning 2022: Meeting the Changing Needs for Family Planning: Contraceptive use by age and Method. New York, N.Y: United Nations (2022). Report No.: UN DESA/POP/2022/TR/NO. 4.
2. American College of Obstetricians and Gynecologists. Sterilization for Women and Men. Washington, DC: American College of Obstetricians and Gynecologists (2023). Available online at: https://www.acog.org/womens-health/faqs/sterilization-for-women-and-men (Accessed March 2, 2024).
3. Melville C, Bigrigg A. Male and female sterilization. Obstet Gynaecol Reprod Med. (2008) 18(12):330–4. doi: 10.1016/j.ogrm.2008.09.003
4. KFF. Sterilization as a Family Planning Method. San Francisco, CA: KFF (2018). Available online at: https://www.kff.org/womens-health-policy/fact-sheet/sterilization-as-a-family-planning-method/ (Accessed March 2, 2024).
5. Anita P, Nzabona A, Tuyiragize R. Determinants of female sterilization method uptake among women of reproductive age group in Uganda. Contracept Reprod Med. (2020) 5(1):25. doi: 10.1186/s40834-020-00131-8
6. Das M, Anand A, Hossain B, Ansari S. Inequalities in short-acting reversible, long-acting reversible and permanent contraception use among currently married women in India. BMC Public Health. (2022) 22:1264. doi: 10.1186/s12889-022-13662-3
7. Eeckhaut MCW. Intersecting inequalities: education, race/ethnicity, and sterilization. J Fam Issues. (2020) 41(10):1905–29. doi: 10.1177/0192513X19900529
8. Shreffler KM, McQuillan J, Greil AL, Johnson DR. Surgical sterilization, regret, and race: contemporary patterns. Soc Sci Res. (2015) 50:31–45. doi: 10.1016/j.ssresearch.2014.10.010
9. Open Society Foundations. Against her Will: Forced and Coerced Sterilization of Women Worldwide. New York, NY: Open Society Foundations (2011). Available online at: https://www.opensocietyfoundations.org/publications/against-her-will-forced-and-coerced-sterilization-women-worldwide (Accessed February 15, 2024).
10. Zampas C, Lamačková A. Forced and coerced sterilization of women in Europe. Int J Gynaecol Obstet. (2011) 114(2):163–6. doi: 10.1016/j.ijgo.2011.05.002
11. Borrero S, Schwarz EB, Reeves MF, Bost JE, Creinin MD, Ibrahim SA. Race, insurance Status, and tubal sterilization. Obstet Gynecol. (2007) 109(1):94. doi: 10.1097/01.AOG.0000249604.78234.d3
12. Volscho TW. Sterilization racism and pan-ethnic disparities of the past decade: the continued encroachment on reproductive rights. Wicazo Sa Rev. (2010) 25(1):17–31. doi: 10.1353/wic.0.0053
13. Arora KS, Ascha M, Wilkinson B, Verbus E, Montague M, Morris J, et al. Association between neighborhood disadvantage and fulfillment of desired postpartum sterilization. BMC Public Health. (2020) 20(1):1440. doi: 10.1186/s12889-020-09540-5
14. Lunde B, Rankin K, Harwood B, Chavez N. Sterilization of rural and urban women in the United States. Obstet Gynecol. (2013) 122(2 Pt 1):304. doi: 10.1097/AOG.0b013e31829b5a11
15. Olakunde BO, Pharr JR, Chien LC, Benfield RD, Sy FS. Individual- and country-level correlates of female permanent contraception use in sub-Saharan Africa. PLoS One. (2020) 15(12):e0243316. doi: 10.1371/journal.pone.0243316
16. Leon Rd, Ewerling F, Serruya SJ, Silveira MF, Sanhueza A, Moazzam A, et al. Contraceptive use in Latin America and the Caribbean with a focus on long-acting reversible contraceptives: prevalence and inequalities in 23 countries. Lancet Glob Health. (2019) 7(2):e227–35. doi: 10.1016/S2214-109X(18)30481-9
17. Mena-Meléndez L. Rural-urban differences in unintended pregnancies, contraceptive nonuse, and terminated pregnancies in Latin America and the Caribbean. Womens Reprod Health. (2022) 9(2):119–42. doi: 10.1080/23293691.2021.2016135
18. Folch BM, Betstadt S, Li D, Whaley N. The rise of female sterilization: a closer Look at Colombia. Matern Child Health J. (2017) 21(9):1772–7. doi: 10.1007/s10995-017-2296-x
19. Navarro Valencia MC. Uniones, maternidad y salud sexual y reproductiva de las afrocolombianas de buenaventura. Una perspectiva antropológica. Rev Colombiana Antropol. (2009) 45(1):38–68. doi: 10.22380/2539472X.984
20. Ugaz JI, Chatterji M, Gribble JN, Banke K. Is household wealth associated with use of long-acting reversible and permanent methods of contraception? A multi-country analysis. Glob Health Sci Pract. (2016) 4(1):43–54. doi: 10.9745/GHSP-D-15-00234
22. Landry E. How and why women choose sterilization: results from six follow-up surveys. Stud Fam Plann. (1990) 21(3):143–51. doi: 10.2307/1966713
23. Rindfuss RR, Liao F. Medical and contraceptive reasons for sterilization in the United States. Stud Fam Plann. (1988) 19(6):370–80. doi: 10.2307/1966631
24. Grimes DA. Forgettable contraception. Contraception. (2009) 80(6):497–9. doi: 10.1016/j.contraception.2009.06.005
25. Croft TN, Allen CK, Zachary BW. Guide to DHS Statistics. Rockville, MD: ICF International (2023). Available online at: https://dhsprogram.com/publications/publication-dhsg1-dhs-questionnaires-and-manuals.cfm (Accessed March 5, 2024)
26. Montenegro RA, Stephens C. Indigenous health in Latin America and the Caribbean. Lancet. (2006) 367(9525):1859–69. doi: 10.1016/S0140-6736(06)68808-9
27. Telles EE. Pigmentocracies: Ethnicity, Race, and Color in Latin America. 1st Eds Chapel Hill, NC: University of North Carolina Press (2014). p. 297.
28. Telles EE. Multiple measures of ethnoracial classification in Latin America. Ethn Racial Stud. (2017) 40(13):2340–6. doi: 10.1080/01419870.2017.1344275
29. Telles EE, Torche F. Varieties of indigeneity in the Americas. Soc Forces. (2019) 97(4):1543–70. doi: 10.1093/sf/soy091
30. Perreira KM, Telles EE. The color of health: skin color, ethnoracial classification, and discrimination in the health of Latin Americans. Soc Sci Med. (2014) 116:241–50. doi: 10.1016/j.socscimed.2014.05.054
31. Telles EE, Flores RD, Urrea-Giraldo F. Pigmentocracies: educational inequality, skin color and census ethnoracial identification in eight Latin American countries. Res Soc Stratif Mobil. (2015) 40:39–58. doi: 10.1016/j.rssm.2015.02.002
32. Ren R. Note on DHS Standard Weight de-normalization. Reston, VA: ICF International. Available online at: https://userforum.dhsprogram.com/index.php?t=getfile&id=535& (Accessed December 20, 2023).
33. Guo G, Zhao H. Multilevel modeling for binary data. Annu Rev Sociol. (2000) 26(1):441–62. doi: 10.1146/annurev.soc.26.1.441
34. Berry WD, DeMeritt JH, Esarey J. Testing for interaction in binary logit and probit models: is a product term essential? Am J Pol Sci. (2010) 54(1):248–66. doi: 10.1111/j.1540-5907.2009.00429.x
35. Long JS, Freese J. Regression Models for Categorical Dependent Variables Using Stata. College Station, Texas: Stata Press; 2001. 341.
36. Mize T. Best practices for estimating, interpreting, and presenting nonlinear interaction effects. Soc Sci. (2019) 6:81–117. doi: 10.15195/v6.a4
37. Bello Á, Rangel M. Equity and exclusion in Latin America and the Caribbean: the case of indigenous and afro-descendant peoples. CEPAL Rev. (2002) (76):35–53.
38. Casas JA, Dachs JNW, Bambas A. Health Disparities in Latin America and the Caribbean: The Role of Social and Economic Determinants. Washington, DC: Pan American Health Organization (2001). p. 22–49. Available online at: https://scholar.google.com/scholar_lookup?title=Health%20disparities%20in%20Latin%20America%20and%20the%20Caribbean%3A%20The%20role%20of%20social%20and%20economic%20determinants&author=J.A.%20Casas&publication_year=2001&pages=22-49 (Accessed March 4, 2024).
39. Mena-Meléndez L. Ethnoracial child health inequalities in Latin America: multilevel evidence from Bolivia, Colombia, Guatemala, and Peru. SSM Popul Health. (2020) 12:100673. doi: 10.1016/j.ssmph.2020.100673
40. Baldwin MK, Rodriguez MI, Edelman AB. Lack of insurance and parity influence choice between long-acting reversible contraception and sterilization in women postpregnancy. Contraception. (2012) 86(1):42–7. doi: 10.1016/j.contraception.2011.11.005
41. Fagan T, Dutta A, Rosen J, Olivetti A, Klein K. Family planning in the context of Latin America’s universal health coverage agenda. Glob Health Sci Pract. (2017) 5(3):382–98. doi: 10.9745/GHSP-D-17-00057
42. White K, Potter JE. Reconsidering racial/ethnic differences in sterilization in the United States. Contraception. (2014) 89(6):550–6. doi: 10.1016/j.contraception.2013.11.019
43. Ross L, Solinger R. Reproductive Justice: An Introduction. Berkeley, CA: University of California Press (2017).
44. Roberts D. Killing the Black Body: Race, Reproduction, and the Meaning of Liberty. New York, NY: Vintage (1997).
45. Ewig C. Second-Wave Neoliberalism : Gender, Race, and Health Sector Reform in Peru. PA: University Park, Penn State University Press (2011).
46. Ginsburg FD, Rapp R. Conceiving the New World Order: The Global Politics of Reproduction. Berkeley, CA: University of California Press (1995).
47. Ali MM, Cleland J, Shah IH. Trends in reproductive behavior among young single women in Colombia and Peru: 1985–1999. Demography. (2003) 40(4):659–73. doi: 10.1353/dem.2003.0031
48. Lerch M. Regional variations in the rural-urban fertility gradient in the Global South. PLoS One. (2019) 14(7):e0219624. doi: 10.1371/journal.pone.0219624
49. Mmari K, Astone N. Urban adolescent sexual and reproductive health in low-income and middle-income countries. Arch Dis Child. (2014) 99(8):778–82. doi: 10.1136/archdischild-2013-304072
50. Ross JA. Sterilization: past, present, future. Stud Fam Plann. (1992) 23(3):187–98. doi: 10.2307/1966727
51. Ross JA, Huber DH, Hong S. Worldwide trends in voluntary sterilization. Int Fam Plan Perspect. (1986) 12(2):34–9. doi: 10.2307/2947947
52. Inglehart R, Carballo M. Does Latin America exist? (and is there a confucian culture?): a global analysis of cross-cultural differences. PS Polit Sci Polit. (1997) 30(1):34–47. doi: 10.2307/420668
53. Borrero S, Moore CG, Qin L, Schwarz EB, Akers A, Creinin MD, et al. Unintended pregnancy influences racial disparity in tubal sterilization rates. J Gen Intern Med. (2010) 25(2):122–8. doi: 10.1007/s11606-009-1197-0
54. Schoen R, Astone NM, Nathanson CA, Kim YJ, Murray N. The impact of fertility intentions on behavior: the case of sterilization. Soc Biol. (2000) 47(1–2):61–76. doi: 10.1080/19485565.2000.9989010
55. Lawrence RE, Rasinski KA, Yoon JD, Curlin FA. Factors influencing physicians’ advice about female sterilization in USA: a national survey. Hum Reprod. (2011) 26(1):106–11. doi: 10.1093/humrep/deq289
56. Borrero S, Nikolajski C, Rodriguez KL, Creinin MD, Arnold RM, Ibrahim SA. “Everything I know I learned from my mother..or not”: perspectives of African-American and white women on decisions about tubal sterilization. J Gen Intern Med. (2009) 24(3):312–9. doi: 10.1007/s11606-008-0887-3
57. Heeringa SG, West BT, Berglund PA. Applied Survey Data Analysis. 2nd Eds New York: Chapman and Hall/CRC (2017). p. 590.
Keywords: female sterilization, indigenous, afro-descendent, ethnoracial minorities, rural-urban inequality, Latin America
Citation: Mena-Meléndez L (2025) Ethnoracial and rural-urban differences in female sterilization in Bolivia, Colombia, Guatemala, and Peru. Front. Glob. Women's Health 6:1582729. doi: 10.3389/fgwh.2025.1582729
Received: 25 February 2025; Accepted: 7 July 2025;
Published: 4 August 2025.
Edited by:
Berna Dilbaz, University of Health Sciences, TürkiyeReviewed by:
Saheed Akinmayowa Lawal, Babcock University, NigeriaEtiele Maldonado Gomes, Federal University of Pampa, Brazil
Copyright: © 2025 Mena-Meléndez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lucrecia Mena-Meléndez, bG1lbmFtZWxAaXUuZWR1