 Lucas Blanco Insaurralde da Luz Silva1*
Lucas Blanco Insaurralde da Luz Silva1* Andressa Camilo Oliveira1Anny Gabriela Marçal de Carvalho Araújo1Maria Luiza Ferri Cury2Isabela de Carvalho Florêncio3Amanda Boutrik1Franciely Hyun Su Barakat Kim1
Andressa Camilo Oliveira1Anny Gabriela Marçal de Carvalho Araújo1Maria Luiza Ferri Cury2Isabela de Carvalho Florêncio3Amanda Boutrik1Franciely Hyun Su Barakat Kim1 Egidi Mayara Firmino Silva4Luana Karen dos Santos3Renata Gratão Rezende3Rodolfo Antônio Corona3Gabriel Pereira Braga1,3,†
Egidi Mayara Firmino Silva4Luana Karen dos Santos3Renata Gratão Rezende3Rodolfo Antônio Corona3Gabriel Pereira Braga1,3,†
- 1Faculdade de Medicina, Universidade Federal do Mato Grosso do Sul (UFMS), Campo Grande, Mato Grosso do Sul, Brazil
- 2Department of Internal Medicine, Santa Casa de Misericórdia de Campo Grande, Campo Grande, Mato Grosso do Sul, Brazil
- 3Department of Neurology, Hospital Universitário Maria Aparecida Pedrossian (HUMAP/UFMS), Campo Grande, Mato Grosso do Sul, Brazil
- 4Faculty of Pharmaceutical Sciences, Food and Nutrition (FACFAN), Federal University of Mato Grosso do Sul (UFMS), Campo Grande, Mato Grosso do Sul, Brazil
Introduction: Stroke is often associated with the elderly population, but recent epidemiological data indicate an increasing incidence among young adults. Among the risk factors, estrogenic hormone therapy (HT) has been linked to cerebrovascular events. This report presents the case of a transgender woman who suffered an ischemic stroke during the inappropriate use of HT, highlighting the importance of medical follow-up and risk assessment in gender-affirming therapy.
Case Description: A 30-year-old transgender female patient had been using estrogenic HT purchased on the black market (cyproterone 2 mg + ethinyl estradiol 0.035 mg/day) since the age of 17, without medical supervision. She had a history of HIV infection under irregular treatment and previously treated syphilis. She developed sudden-onset right-sided hemiparesis and homonymous hemianopsia. The initial computed tomography scan revealed no abnormalities, but magnetic resonance imaging showed ischemia in the territory of the left posterior cerebral artery. Etiological investigation with echocardiography, carotid and vertebral Doppler ultrasound, electrocardiogram, Holter monitoring, and thrombophilia panel revealed no abnormalities. The final etiological diagnosis was classified according to the TOAST criteria as “other causes,” attributed to the inappropriate use of estrogenic therapy. She was discharged with antiplatelet therapy, a statin, and fluoxetine, along with the discontinuation of hormone therapy and referral to transgender and vascular neurology outpatient clinics.
Discussion: HT is essential in gender affirmation; however, its use is associated with increased risks of thromboembolic and cerebrovascular events. The patient in this case did not present traditional risk factors for stroke, reinforcing the suspicion of estrogen's role in the event. Studies suggest that supervised hormone therapy carries a lower risk of complications compared to indiscriminate use. Nonetheless, there are still gaps in the literature regarding the correlation between HT and stroke in transgender individuals.
Conclusion: This case highlights the risks of inappropriate use of gender-affirming hormone therapy and the need for rigorous medical supervision. Given the growing access to this treatment, continuous monitoring is essential to minimize complications. Further research is needed to establish safer guidelines for the use of hormone therapy in the transgender population.
1 Introduction
The incidence of stroke occurs predominantly after the fifth decade of life and is considered a condition that mainly affects the elderly population (1). However, studies conducted across multiple centers and diverse populations have identified a global increase in the incidence of stroke among young adults (2–5). It is evident that the epidemiological profile of stroke has been shifting in recent decades, with a growing yearly incidence of cerebrovascular events in younger individuals.
Parallel to the rise in cerebrovascular events among young people, there has been growth in a particularly vulnerable population: transgender individuals. The transgender community has become the focus of various public health discussions, especially concerning the prevention of cerebro-cardiovascular diseases (6). In recent years, literature has indicated an increase in risks and diseases particularly associated with gender transition hormone therapy (6–10).
This report presents a case of ischemic stroke (IS) in a young transgender woman using inappropriate hormone therapy with oral contraceptives—substances often obtained from the black market, especially in countries lacking inclusive public health policies and comprehensive healthcare access (11). In such contexts, hormone use often occurs without medical prescription or professional supervision and is integrated into the gender-affirmation process (11). Therefore, this study stands out by describing an ischemic cerebrovascular event in an underreported population in the scientific literature (9): young transgender women using unsupervised combined hormone therapy. It highlights a critical gap in current scientific production (9, 10, 12), clarifies how inadequate hormone therapy use can trigger cerebrovascular events (9, 10, 12, 13), and reinforces the urgency of developing specific protocols for prevention, education, and healthcare assistance tailored to transgender individuals undergoing hormonal transition.
2 Clinical case
A 30-year-old transgender woman had been using estrogenic hormone therapy—obtained from the black market—without medical supervision since the age of 17 (cyproterone 2 mg + ethinyl estradiol 0.035 mg/day). She was HIV-positive (viral load of 413 on December 4, 2023, and CD4 count of 413 on October 3, 2023) and undergoing irregular treatment (dolutegravir 50 mg once daily, tenofovir + lamivudine 300 + 300 mg once daily), with a history of previously treated syphilis.
One day prior to hospitalization, the patient presented with a moderate-intensity holocranial headache. The following day, she awoke with sudden-onset right-sided hemiparesis and homonymous hemianopsia.
Upon admission to the stroke unit, her blood pressure was 130/80 mmHg, heart rate 104 bpm, oxygen saturation (SpO₂) 99%, and she scored 5 on the National Institutes of Health Stroke Scale (NIHSS). The initial CT scan showed no signs of cerebrovascular injury, but brain magnetic resonance imaging revealed an ischemic lesion in the territory of the left posterior cerebral artery (Figure 1).
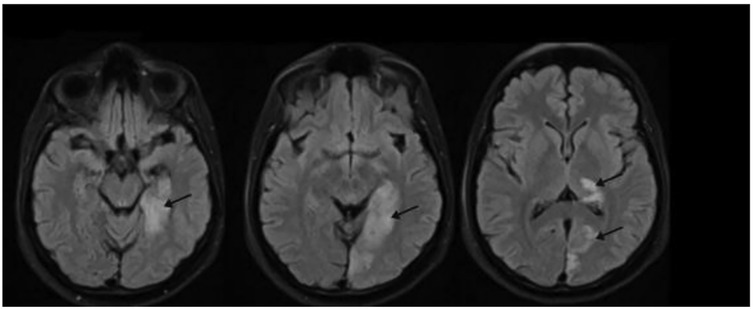
Figure 1. FLAIR sequence of brain magnetic resonance imaging performed on February 5, 2024, post-stroke, showing ischemia (arrow) in the territory of the left posterior cerebral artery.
Thrombolysis was not indicated as the ictus-to-door time exceeded the therapeutic window (over 4 hours and 30 minutes). Conservative treatment for ischemic stroke was initiated, including antiplatelet therapy (acetylsalicylic acid 100 mg/day), anticoagulation (enoxaparin 40 mg/day), blood pressure control, lipid-lowering therapy (simvastatin 40 mg/day), and resumption of antiretroviral therapy (dolutegravir 50 mg/day, tenofovir + lamivudine 300 + 300 mg/day).
The patient underwent infectious screening and cerebrospinal fluid collection due to suspected neurotoxoplasmosis, neurocryptococcosis, neurotuberculosis, and neurosyphilis. Opportunistic neuroinfections were subsequently ruled out.
An etiological investigation for stroke was performed, including transthoracic and transesophageal echocardiography, carotid and vertebral Doppler ultrasound, electrocardiogram, Holter monitoring, arteriography, rheumatologic tests, thrombophilia screening, and metabolic panel—all results were unremarkable. In addition, the patient had no family history of stroke or cardiovascular disease.
Serum testosterone and estrogen levels were not measured due to the unavailability of the test in the public health system at the time of admission.
The final etiological diagnosis was classified according to the TOAST criteria as other causes, attributed to the inappropriate use of estrogenic therapy. After diagnosis, the patient was discharged with antiplatelet therapy (aspirin 100 mg/day), a statin (simvastatin 20 mg/day), and fluoxetine 20 mg/day. Hormone therapy was discontinued, and she was referred for follow-up at transgender and vascular neurology outpatient clinics.
The patient attended only one outpatient appointment and was subsequently lost to follow-up. During the visit, she reported adherence to her prescribed medication and discontinuation of hormone therapy. However, she continued to present with right-sided visual impairment, weakness, and thermal hypoesthesia in the right hemibody. She also reported mood changes, particularly increased aggressiveness. Her NIHSS score was 2 and her Modified Rankin Scale (mRS) score was 2. Due to the loss to follow-up, a more detailed neurological evaluation and assessment of potential complications could not be thoroughly conducted. The chronological progression of clinical manifestations, diagnostic investigations, and therapeutic decisions in the present case report is summarized in Table 1, which outlines the key events during hospitalization.
3 Chronological table of clinical events
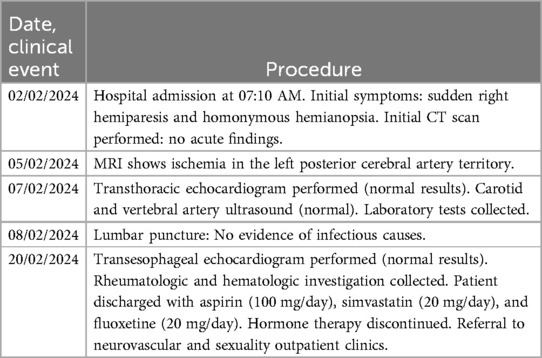
Table 1. Chronological sequence of clinical events, neuroimaging findings, and diagnostic procedures during hospitalization.
4 Discussion
A transgender individual is someone whose biological sex, assigned at birth, differs from their gender identity, which reflects how they self-identify (14). According to a study conducted at the Botucatu School of Medicine, the estimated number of transgender people currently living in Brazil is around 3 million (15). Given this figure, a deeper understanding and exploration of the specificities involved in healthcare delivery to this population has become essential. Among these specific needs are higher rates of conditions such as depression, anxiety, and sexually transmitted infections—particularly syphilis and HIV—as well as a high demand for hormone therapy for gender affirmation (14).
This latter aspect is particularly relevant when considering the increased risk of stroke in this population. Despite its significance, this remains an underexplored topic in the academic literature (9, 10, 12, 16), mainly due to the stigma associated with this population and the healthcare access barriers it faces (9, 11, 17). Hormone therapy for gender transition is one of the main pillars of gender affirmation, consisting of testosterone administration for transgender men and a combination of anti-androgens and estradiol derivatives for transgender women, aiming to develop physical characteristics aligned with their gender identity (18). Therefore, it is important to correlate the risks—particularly those related to estradiol—with the occurrence of stroke in transgender women.
The patient in this case presented with multiple potential risk factors for ischemic stroke (IS), which should be analyzed collectively. First, it is worth highlighting the prolonged use—over 12 years—of a hormonal combination (cyproterone 2 mg + ethinyl estradiol 0.035 mg/day) obtained from the black market and used without medical supervision. Although this formulation is occasionally used as a contraceptive in cisgender women, it is not recommended as standard therapy for transgender women. Self-medication without monitoring may have intensified the prothrombotic risks of estrogenic therapy, as previously reported in the literature (10, 12), especially in transgender populations lacking adequate access to healthcare.
In addition to hormone therapy, the patient was living with HIV infection, diagnosed two years earlier, and was using combination antiretroviral therapy (dolutegravir, tenofovir, lamivudine). Studies have shown that both HIV infection and antiretroviral therapy (ART) itself are associated with increased cardiovascular risk due to mechanisms such as chronic inflammation, endothelial dysfunction, lipid metabolism disorders, and a higher predisposition to atherosclerosis (19–23). Upon admission, the patient had a detectable viral load (43 copies/ml), CD4 count of 349, and CD8 count of 771, indicating moderate immunosuppression (24). Although no opportunistic or neuroinfections related to HIV were identified, her immunological status may have contributed to a baseline inflammatory state that increases the risk of ischemic events.
Regarding prior syphilis, the patient had a reactive serology (VDRL 1:16), but cerebrospinal fluid was non-reactive and showed no pleocytosis, elevated protein, or other alterations suggestive of neurosyphilis (25). Thus, a diagnosis of syphilitic meningitis or meningovascular syphilis was considered unlikely (25). From a metabolic standpoint, laboratory tests (total cholesterol, LDL, HDL, triglycerides) did not reveal dyslipidemia, and imaging studies did not show atherosclerotic plaques.
Considering the absence of cardioembolic, atherosclerotic, and direct infectious causes, the case was classified as an ischemic stroke (IS) of other determined etiology, most likely related to prolonged and unsupervised exposure to estrogenic hormone therapy, combined with the chronic inflammatory state associated with HIV infection and ART.
In this case, a critical factor supporting the hypothesis that the etiology of the IS was primarily caused by estrogenic and anti-androgenic hormone therapy is the absence of conventional risk factors such as smoking, alcohol consumption, substance abuse, obesity, hypertension, dyslipidemia, diabetes, heart disease, previous cerebrovascular events, family history of cardio-cerebrovascular diseases, and neuroinfections. Therefore, it is likely that prolonged use of hormone therapy—particularly estrogens—was associated with the ischemic event (13).
The risk of ischemic stroke and thromboembolic events associated with hormone therapy in transgender women is related to the duration of exposure, dosage, and route of administration, with patterns indicating a progressive increase in risk after two to six years of continuous estrogen use, as demonstrated by longitudinal observational studies (26).
Ethinyl estradiol is a substance capable of inducing alterations at various cardiovascular levels, which explains the high risk of thromboembolic events associated with this hormone therapy (1, 12, 27). These dysfunctions include increased thrombin and other thrombogenic factors; endothelial alterations, which predispose to atherosclerosis (linked to IS) and arterial hypertension (linked to hemorrhagic stroke risk) (28); and a reduction in HDL levels with an increase in LDL levels, contributing to the formation of atherosclerotic plaques (18).
A case-control study demonstrated a higher prevalence of transient ischemic attacks and cerebrovascular diseases in individuals undergoing gender-affirming hormone therapy (6). Similarly, a cohort study reported higher rates of ischemic stroke in transgender women, showing a tenfold increased risk compared to cisgender men (26). Moreover, cardiovascular diseases are the second leading cause of death among transgender individuals undergoing hormone therapy, ranking below suicide, which remains the leading cause of mortality in this population (8).
A recent meta-analysis sought to determine a correlation between cerebrovascular events and the use of hormone therapy in male-to-female transgender individuals (9). Ignacio et al. referenced a cohort study indicating that transgender women were more likely to develop cerebrovascular diseases (26). These findings are supported by data from a Dutch study, which identified a higher incidence rate of stroke among transgender women undergoing hormone replacement therapy compared to cisgender women [standardized incidence ratio, 2.42 (95% CI, 1.65–3.42)] (29). However, despite the presence of other studies cited in this meta-analysis that suggest an increased risk of ischemic stroke associated with hormone therapy, the estimated lifetime stroke risk in transgender women remained significantly lower than that of the general population (2% vs. 24.5%) (9). Therefore, a definitive association between gender-affirming hormone therapy and stroke cannot be established based on current evidence, given the small sample sizes, heterogeneity in routes of administration and dosages, use of convenience sampling methods, and the limited number of studies addressing this relationship (9).
When comparing hormone therapy in transgender women to that in postmenopausal cisgender women, both groups present an increased risk of vascular and cardiovascular events; however, a higher rate of cardiovascular and cerebrovascular mortality has been observed in transgender women compared to the general population (9). Current studies suggest that estrogen doses administered to transgender women should be titrated to achieve mean serum estradiol levels similar to those of postmenopausal cisgender women (10). The Endocrine Society emphasizes the importance of achieving physiologic hormone levels when comparing transgender and postmenopausal cisgender women, and specifically contraindicates the use of ethinyl estradiol for hormone therapy, due to its significantly elevated vascular and ischemic risk profile (27).
Therefore, although several studies suggest a correlation between cerebrovascular and cardiovascular diseases and gender-affirming hormone therapy, this association is not yet clearly defined in the scientific literature (9, 13, 30). The 2024 Guideline for the Primary Prevention of Stroke currently provides specific recommendations for this population, underscoring the importance of controlling additional stroke risk factors to reduce the likelihood of cerebrovascular events, even while undergoing hormone therapy (30). Nonetheless, the guideline also highlights the existing gap in knowledge regarding stroke risk in this community (30).
The use of transdermal hormone therapy, management of metabolic and endocrine profiles (based on physiologic levels), and multidisciplinary follow-up has been associated with a reduction in cerebro-cardiovascular events in the transgender population (31, 32), representing one of the key strategies to be addressed in the clinical management of these patients.
This case report presents some limitations. The loss to follow-up prevented the assessment of medication adherence, potential long-term complications, and a more detailed evaluation of the patient's neurological recovery. The absence of serum testosterone and estrogen measurements hinders comparison with cisgender men and women of the same age group. Another limitation is the lack of biomarkers (such as IGF-1, vitamin D, and microRNAs), which could assist in understanding the relationship between ischemic stroke and estrogenic therapy. Although some studies have explored this correlation in cisgender women (33), there is still insufficient robust data to extrapolate these conclusions to the transgender population undergoing gender-affirming hormone therapy.
Furthermore, as this is a case report, the findings do not allow for generalization and may be subject to selection and information bias. Studies with greater methodological rigor, such as cohort studies and clinical trials, are necessary to confirm the association between estrogenic hormone therapy and stroke risk in transgender women.
5 Conclusion
This case draws attention to the increased risk of stroke in transgender individuals exposed to inadequate hormone therapy without medical supervision. As access to gender-affirming hormone therapy continues to expand, it is essential to strengthen research on the risks and preventive strategies for cerebrovascular diseases in this population.
Healthcare system avoidance among transgender individuals is often driven by factors such as discrimination, lack of inclusive care, fear of hormone therapy being discontinued, transportation difficulties, and bureaucratic barriers within regulatory systems that hinder return to specialized outpatient care. These challenges contribute to self-medication and discontinuation of clinical follow-up (11).
To address this scenario, it is necessary to strengthen specialized transgender health clinics, establish mobile outreach campaigns, train primary care teams, and revise regulatory pathways that restrict access to continuous and safe care.
Finally, cohort studies and population-based research assessing the cerebrovascular health of transgender and gender-diverse individuals are critically important. Such research should take into account factors such as duration, dose, route of administration of hormone therapy, and social determinants of health. This approach is essential for identifying risk mechanisms and guiding effective interventions to reduce ischemic events in this population (30).
6 Patient perspective
The patient reported satisfaction with the care received during hospitalization, highlighting the attention, support, and rehabilitation provided by the healthcare team. After discharge, she was referred to the vascular neurology outpatient clinic located within the same hospital complex. She attended a single appointment but was subsequently lost to follow-up.
In later contact with the present study’s team, the patient expressed interest in resuming outpatient care, as did her family members, showing hope regarding the continuation of specialized follow-up. In response to this request, detailed guidance and the necessary documentation were provided so that she could reenter the referral system and resume treatment at the specialized service. During this contact, she reported no additional complications or adverse events beyond those noted in her last appointment.
Data availability statement
The datasets presented in this article are not readily available because of ethical and privacy restrictions. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Comitê de Ética em Pesquisa do Hospital Universitário Maria Aparecida Pedrossian (Approval number: CEP/HUMAP-UFMS). The studies were conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired from a by- product of routine care or industry. Written informed consent for participation was not required from the participants or the participants legal guardians/next of kin in accordance with the national legislation and institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
LI: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Visualization. AO: Data curation, Validation, Visualization, Writing – review & editing. AA: Data curation, Methodology, Visualization, Writing – review & editing. MC: Data curation, Supervision, Validation, Visualization, Writing – review & editing. IF: Data curation, Validation, Visualization, Writing – review & editing. AB: Validation, Visualization, Writing – review & editing. FK: Validation, Visualization, Writing – review & editing. ES: Validation, Visualization, Writing – review & editing. LS: Validation, Visualization, Writing – review & editing. RR: Validation, Visualization, Writing – review & editing. RC: Validation, Visualization, Writing – review & editing. GB: Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Caplan L. Stroke: etiology, classification, and epidemiology. In: Kasner S, editor. UpToDate (2024). Available online at: https://www.uptodate.com/contents/stroke-etiology-classification-and-epidemiology (Accessed March 04, 2024).
2. Béjot Y, Daubail B, Jacquin A, Durier J, Osseby GV, Rouaud O, et al. Trends in the incidence of ischemic stroke in young adults between 1985 and 2011: the dijon stroke registry. J Neurol Neurosurg Psychiatry. (2014) 85(5):509–13. doi: 10.1136/jnnp-2013-306203
3. Ekker MS, Verhoeven JI, Schellekens MMI, Boot EM, van Alebeek ME, Brouwers PJAM, et al. Risk factors and causes of ischemic stroke in 1322 young adults. Stroke. (2023) 54(2):439–47. doi: 10.1161/STROKEAHA.122.040524
4. Kissela BM, Khoury JC, Alwell K, Moomaw CJ, Woo D, Adeoye O, et al. Age at stroke: temporal trends in stroke incidence in a large, biracial population. Neurology. (2012) 79(17):1781–7. doi: 10.1212/WNL.0b013e318270401d
5. Li L, Scott CA, Rothwell PM. Association of younger vs older ages with changes in incidence of stroke and other vascular events, 2002–2018. JAMA. (2022) 328(6):563–74. doi: 10.1001/jama.2022.12759
6. Wierckx K, Elaut E, Declercq E, Heylens G, De Cuypere G, Taes Y, et al. Prevalence of cardiovascular disease and cancer during cross-sex hormone therapy in a large cohort of trans persons: a case-control study. Eur J Endocrinol. (2013) 169(4):471–8. doi: 10.1530/EJE-13-0493
7. Asscheman H, Giltay EJ, Megens JA, de Ronde WP, van Trotsenburg MA, Gooren LJ. A long-term follow-up study of mortality in transsexuals receiving treatment with cross-sex hormones. Eur J Endocrinol. (2011) 164(4):635–42. doi: 10.1530/EJE-10-1038
8. Dhejne C, Lichtenstein P, Boman M, Johansson AL, Långström N, Landén M. Long-term follow-up of transsexual persons undergoing sex reassignment surgery: cohort study in Sweden. PLoS One. (2011) 6(2):e16885. doi: 10.1371/journal.pone.0016885
9. Ignacio KHD, Diestro JDB, Espiritu AI, Pineda-Franks MC. Stroke in male-to-female transgenders: a systematic review and meta-analysis. Can J Neurol Sci. (2021) 49(1):76–83. doi: 10.1017/cjn.2021.54
10. Pribish AM, Iwamoto SJ. Cardiovascular disease and feminizing gender-affirming hormone therapy: implications for the provision of safe and lifesaving care. Curr Opin Physiol. (2023) 33:100650. doi: 10.1016/j.cophys.2023.100650
11. Reisner SL, Poteat T, Keatley J, Cabral M, Mothopeng T, Dunham E, et al. Global health burden and needs of transgender populations: a review. Lancet. (2016) 388(10042):412–36. doi: 10.1016/S0140-6736(16)00684-X
12. Wright ME, Murphy K. A mini-review of the evidence for cerebrovascular changes following gender-affirming hormone replacement therapy and a call for increased focus on cerebrovascular transgender health. Front Hum Neurosci. (2023) 17:1303871. doi: 10.3389/fnhum.2023.1303871
13. Connelly PJ, Freel EM, Perry C, Ewan J, Touyz RM, Currie G, et al. Gender-affirming hormone therapy, vascular health and cardiovascular disease in transgender adults. Hypertension. (2019) 74(6):1266–74. doi: 10.1161/hypertensionaha.119.13080
14. Abeln B, Love R. Considerations for the care of transgender individuals. Nurs Clin North Am. (2019) 54(4):551–9. doi: 10.1016/j.cnur.2019.07.005
15. Spizzirri G, Eufrásio R, Lima MCP, de Carvalho Nunes HR, Kreukels BPC, Steensma TD, et al. Proportion of people identified as transgender and non-binary gender in Brazil. Sci Rep. (2021) 11(1):81411. doi: 10.1038/s41598-021-81411-4
16. Cicero EC, Reisner SL, Merwin EI, Humphreys JC, Silva SG. The health status of transgender and gender nonbinary adults in the United States. PLoS One. (2020) 15(2):e0228765. doi: 10.1371/journal.pone.0228765
17. Winter S, Diamond M, Green J, Karasic D, Reed T, Whittle S, et al. Transgender people: health at the margins of society. Lancet. (2016) 388(10042):390–400. doi: 10.1016/s0140-6736(16)00683-8
18. Aranda G, Halperin I, Gomez-Gil E, Hanzu FA, Seguí N, Guillamon A, et al. Cardiovascular risk associated with gender affirming hormone therapy in transgender population. Front Endocrinol (Lausanne). (2021) 12:718200. doi: 10.3389/fendo.2021.718200
19. Ismael S, Khan MM, Kumar P, Kodidela S, Mirzahosseini G, Kumar S, et al. HIV-associated risk factors for ischemic stroke and future perspectives. Int J Mol Sci. (2020) 21(15):5306. doi: 10.3390/ijms21155306
20. Lorenz MW, Stephan C, Harmjanz A, Staszewski S, Buehler A, Bickel M, et al. Both long-term HIV infection and highly active antiretroviral therapy are independent risk factors for early carotid atherosclerosis. Atherosclerosis. (2008) 196(2):720–6. doi: 10.1016/j.atherosclerosis.2006.12.022
21. Oliviero U, Bonadies G, Apuzzi V, Foggia M, Bosso G, Nappa S, et al. Human immunodeficiency virus per se exerts atherogenic effects. Atherosclerosis. (2009) 204(2):586–9. doi: 10.1016/j.atherosclerosis.2008.10.012
22. Ross AC, Rizk N, O'Riordan MA, Dogra V, El-Bejjani D, Storer N, et al. Relationship between inflammatory markers, endothelial activation markers, and carotid intima-media thickness in HIV-infected patients receiving antiretroviral therapy. Clin Infect Dis. (2009) 49(7):1119–27. doi: 10.1086/605578
23. Seaberg EC, Benning L, Sharrett AR, Lazar JM, Hodis HN, Mack WJ, et al. Association between human immunodeficiency virus infection and stiffness of the common carotid artery. Stroke. (2010) 41(10):2163–70. doi: 10.1161/STROKEAHA.110.583856
24. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Programa Nacional de DST e Aids. Critérios de Definição de Casos de Aids em Adultos e Crianças. 2nd ed Brasília: Ministério da Saúde (2003). p. 56.
26. Getahun D, Nash R, Flanders WD, Baird TC, Becerra-Culqui TA, Cromwell L, et al. Cross-sex hormones and acute cardiovascular events in transgender persons: a cohort study. Ann Intern Med. (2018) 169(4):205–13. doi: 10.7326/M17-2785
27. Hembree WC, Cohen-Kettenis PT, Gooren L, Hannema SE, Meyer WJ, Murad MH, et al. Endocrine treatment of gender-dysphoric/gender-incongruent persons: an endocrine society clinical practice guideline. Endocr Pract. (2017) 23(12):1437–67. doi: 10.4158/1934-2403-23.12.1437
28. Lima ACS, Martins LCG, de Oliveira Lopes MV, de Araújo TL, Lima FET, de Souza Aquino P, et al. Influence of hormonal contraceptives and the occurrence of stroke: integrative review. Rev Bras Enferm. (2017) 70(3):647–55. doi: 10.1590/0034-7167-2016-0056
29. Nota NM, Wiepjes CM, de Blok CJM, Gooren LJG, Kreukels BPC, den Heijer M. Occurrence of acute cardiovascular events in transgender individuals receiving hormone therapy. Circulation. (2019) 139(11):1461–2. doi: 10.1161/CIRCULATIONAHA.118.038584
30. Bushnell C, Kernan WN, Sharrief AZ, Chaturvedi S, Cole JW, Cornwell WK 3rd, et al. 2024 guideline for the primary prevention of stroke. Stroke. (2024) 55(12):e344–424. doi: 10.1161/STR.0000000000000475
31. Weinand JD, Safer JD. Hormone therapy in transgender adults is safe with provider supervision; A review of hormone therapy sequelae for transgender individuals. J Clin Transl Endocrinol. (2015) 2(2):55–60. doi: 10.1016/j.jcte.2015.02.003
32. Wierckx K, Van Caenegem E, Schreiner T, Haraldsen I, Fisher AD, Toye K, et al. Cross-sex hormone therapy in trans persons is safe and effective at short-time follow-up: results from the European network for the investigation of gender incongruence. J Sex Med. (2014) 11(8):1999–2011. doi: 10.1111/jsm.12571
Keywords: stroke, transgender health, hormone therapy, estrogen, cerebrovascular risk, ischemic stroke
Citation: Insaurralde da Luz Silva LB, Oliveira AC, Araújo AGMC, Cury MLF, Florêncio IC, Boutrik A, Kim FHSB, Silva EMF, dos Santos LK, Rezende RG, Corona RA and Braga GP (2025) Case Report: Ischemic stroke in a young transgender woman due to unsupervised estrogen therapy. Front. Glob. Women's Health 6:1588553. doi: 10.3389/fgwh.2025.1588553
Received: 11 March 2025; Accepted: 4 July 2025;
Published: 8 August 2025.
Edited by:
Riccardo Manca, Brunel University London, United KingdomReviewed by:
Paola Matarrese, National Institute of Health (ISS), ItalyŞenol Turan, Istanbul University Cerrahpasa, Türkiye
Copyright: © 2025 Insaurralde da Luz Silva, Oliveira, Araújo, Cury, Florêncio, Boutrik, Kim, Silva, dos Santos, Rezende, Corona and Braga. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lucas Blanco Insaurralde da Luz Silva, bHVjYXNibGFuY29tc0BnbWFpbC5jb20=
†This author has senior authorship