 Rebekah Wood1*†
Rebekah Wood1*† Anna Borodova1,†
Anna Borodova1,† Sophie Wolter1Micheline N’Guessan2Amadou Aziz Diallo3Mamadou Kamis Diallo3Katharina Heldt4
Sophie Wolter1Micheline N’Guessan2Amadou Aziz Diallo3Mamadou Kamis Diallo3Katharina Heldt4 Carlos Rocha1Ibrahima Nabé3Bamourou Diané2Mahamoud Sama Cherif3
Carlos Rocha1Ibrahima Nabé3Bamourou Diané2Mahamoud Sama Cherif3 Sophie Alice Müller1
Sophie Alice Müller1
- 1Centre for International Health Protection, Robert Koch Institute, Berlin, Germany
- 2University Hospital Bouaké, Bouaké, Côte d'Ivoire
- 3Faranah Regional Hospital, Faranah, Guinea
- 4Methods Development, Research Infrastructure and Information Technology, Robert Koch Institute, Berlin, Germany
Surgical site infections are among the most common healthcare associated infections worldwide and pose a significant risk in cesarean section procedures, which are the most frequently performed surgical operations globally. Our scoping review aimed to synthesize available literature from studies conducted in sub-Saharan Africa on the prevalence of post-caesarean surgical site infections, as well as on reported associated factors. In this scoping review we included studies retrieved in OVID from January 2014 to January 15, 2024 without restrictions on the language of publication or publication status focusing on studies from sub-Saharan African countries. The review was registered on the Open Science Framework platform. The reported rates of surgical site infection across the 73 included studies ranged from 2.0%–56.0%. A forest plot showed that the studies were highly heterogeneous, whereby only 11.0% showed a surgical site infection rate above 20.0%. Most surgical site infections surfaced within two-weeks after a caesarean section. The strongest and most frequently cited risk factors were: duration of labour ≥8 h, surgical duration, multiple vaginal examinations, stored water usage, and premature rupture of membrane. The following protective factors were also determined: Pfannenstiel/transversal incisions, caesarean section at term, having health insurance, normal body mass index, <1 h of surgical intervention, <24 h of premature rupture of membrane, low intraoperative blood loss and absorbable sutures. Staphylococcus aureus was the most commonly isolated pathogen among studies with bacteriological reporting. Our scoping review provides first guidance for regions with limited resources for surveillance, such as sub-Saharan Africa, by outlining most common associated factors and a minimum screening period of two weeks. While utilizing minimal resources effectively, this targeted surveillance could capture the majority of cases and thereby enhancing maternal patient safety.
Systematic Review Registration: https://osf.io/qe7bf/
Introduction
Surgical site infections (SSIs) in general are a major cause for post-surgical mortality and morbidity (1). With a global incidence between 3.0 and 15.0% (2), SSIs are among the most common healthcare associated infections worldwide (3). In low-resource settings, there are limited surveillance systems and hence scarce data on prevalence and associated factors of SSIs (4), but existing evidence suggests highest prevalence rates up to 30.9% in the African region (4). The most commonly performed operations around the world are caesarean sections (CSs) (5). In the African region, up to 20.0% of CSs result in SSIs leading to increased maternal morbidity and mortality, longer hospital stays and higher treatment costs (3). A recent systematic review and meta analysis on SSIs after CS reports global risk factors related to comorbidities. These reported risk factors were obesity, diabetes, hypertension, prolonged hospital stays, inappropriate timing of antibiotics, and environmental factors such as overcrowded living conditions and improper hygiene (1). In the African region, there is currently no comprehensive review on SSIs and their risk factors following caesarean section. For the African region, up to now there is no review on SSIs and associated risk factors after CS.
Our scoping review aims to synthesize literature on prevalence of SSIs after CS across sub-Saharan Africa (SSA), while elucidating associated risk and protective factors. This summarization of available evidence and hence deeper understanding of associated factors can potentially guide SSA healthcare stakeholders such as hospitals and practitioners in risk assessment and mitigation for increased maternal patient safety.
Methods
We conducted a scoping review following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) (6) and the Joanna Briggs Institute (JBI) methodology for scoping reviews (7). We adapted our search strategy for the African continent from the strategy used by Barth and colleagues (8) in conjunction with the definition of SSA from the World Bank (9). The protocol including the search strategy was published on Open Science Framework (OSF) (10). At the time the protocol was uploaded, no similar reviews were registered in either OSF or PROSPERO. We searched the platform OVID for publications between January 2014 and January 15, 2024 without restrictions on the language of publication or publication status. We used Rayyan (11) for deduplication and EndNote X7 (Clarivate Analytics, PA, USA) for screening and study selection (conducted by AB, RW and SM). Screening of titles and abstracts for assessment as well as screening of full text against the inclusion criteria for the review was done in pairs by the research team (AB, RW, SM, SW). Any disagreement arising at each stage of the selection process was resolved through discussion with first and supervisory authors. Studies were considered eligible if they included women who received CSs in health settings in SSA. All types of studies, including clinical trials, cohort or case-control studies were included. In the case of intervention studies, reported sample size and prevalence for the baseline were used in order to show generalisable prevalence rates. Articles in English and French were included.
Data extraction was done in double and independently by the research team (AB, RW, SM, SW) into a structured form in Microsoft Excel. The extracted variables included: author, publication year, title, journal, publication status, study type, study period, City/Country, sample size, sampling strategy, response rate, inclusion criteria, exclusion criteria, age, SSI prevalence, clinical appearance, sample collection, testing strategy, testing rate, type of infection, type of test, test name, factors investigated, factors associated, level of analysis and additional data. A forest plot was used to display results descriptively and given the hetereogeneity of included studies, a meta analysis was not performed.
Results
Selection of studies
The search identified a total of 395 articles; following the removal of duplicates and critical assessment of title and abstracts, 117 potentially relevant articles were identified for full-text screening (Figure 1). Application of the pre-set eligibility criteria resulted in a final inclusion of 73 articles. All included studies were conducted between January 2009 and March 2023.
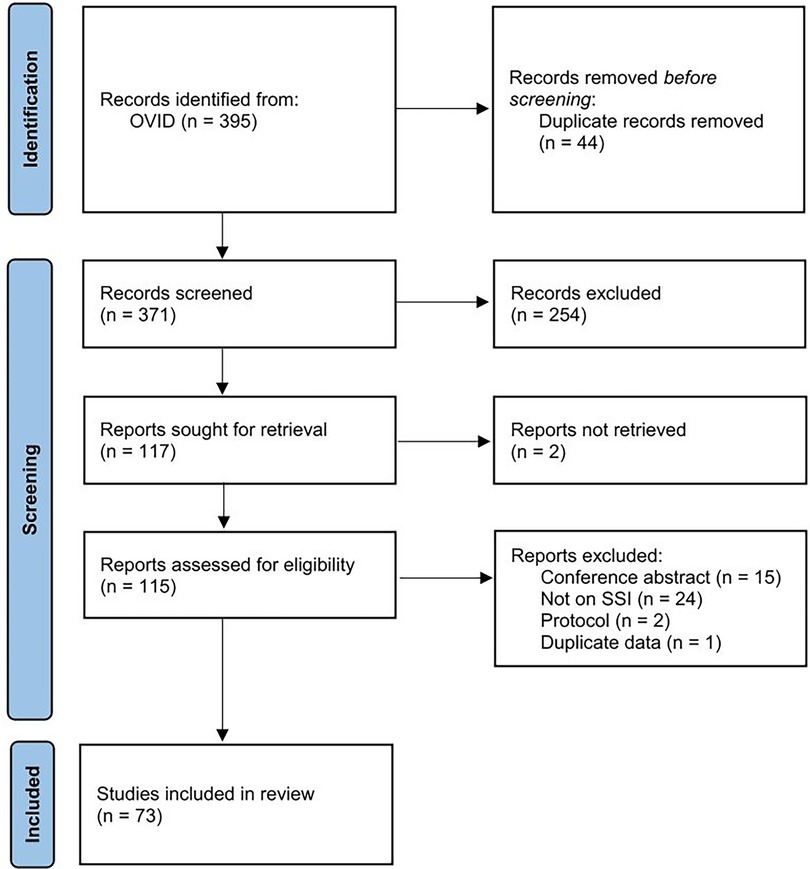
Figure 1. PRISMA flow diagram.
Study characteristics
The included studies contain SSI prevalence data on 51,695 women from 20 countries across SSA, with most studies from Ethiopia (17/73), Nigeria (12/73), Rwanda (11/73) and Tanzania (9/73) (Figure 2, Table 1). The most frequently analyzed health settings were university, teaching or tertiary hospitals 37.0% (27/73), followed by referral, district or regional hospitals 32.9% (24/73). No study included private hospitals. The majority of studies included women who underwent CS at the study site regardless of the indication, whereby 5.5% (4/73) focused on emergency and 2.7% (2/73) on elective CSs only (Table 1).
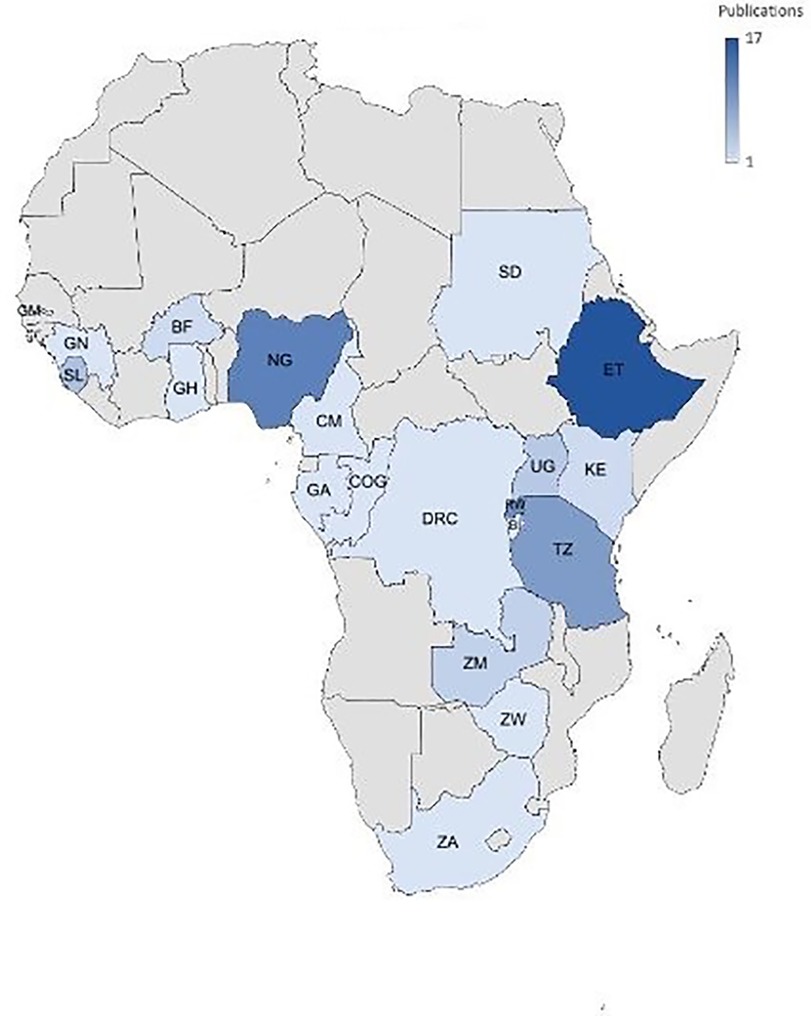
Figure 2. Country distribution of included publications.

Table 1. Results of included studies.
In terms of study type, 43.8% (32/73) of included studies were cohort, 28.8% (21/73) cross-sectional studies and 19.2% (14/73) randomized control studies and 8.2% (6/73) case control (Table 1).
Regarding the applied SSI definition, the majority of studies (54.5%, 40/74) reported to have used the Center for Disease Control guidelines (85), but only a slim majority of 52.5% (21/40) of these also conducted patient follow-up for the full recommended 30-day period. In total, a 37.0% (27/73) minority of studies reported full tracking of patients up to 30 days regardless of the definition applied (Table 1).
SSI rate and appearance time
Reported SSI rates among studies ranged from 2.0% (36)–56.0% (30) (Figure 3). The forest plot showed that the studies were highly heterogeneous (I2 = 100.0%, p < 0.001), and only 11.0% (8/73) of studies showed an SSI rate above 20.0% (Table 1). Regarding the indication for CSs, SSI rates for emergency CS ranged between 7.4% (22) and 48.7% (26), whereby SSI after elective CS from 3.1% (14)–43.0% (26).
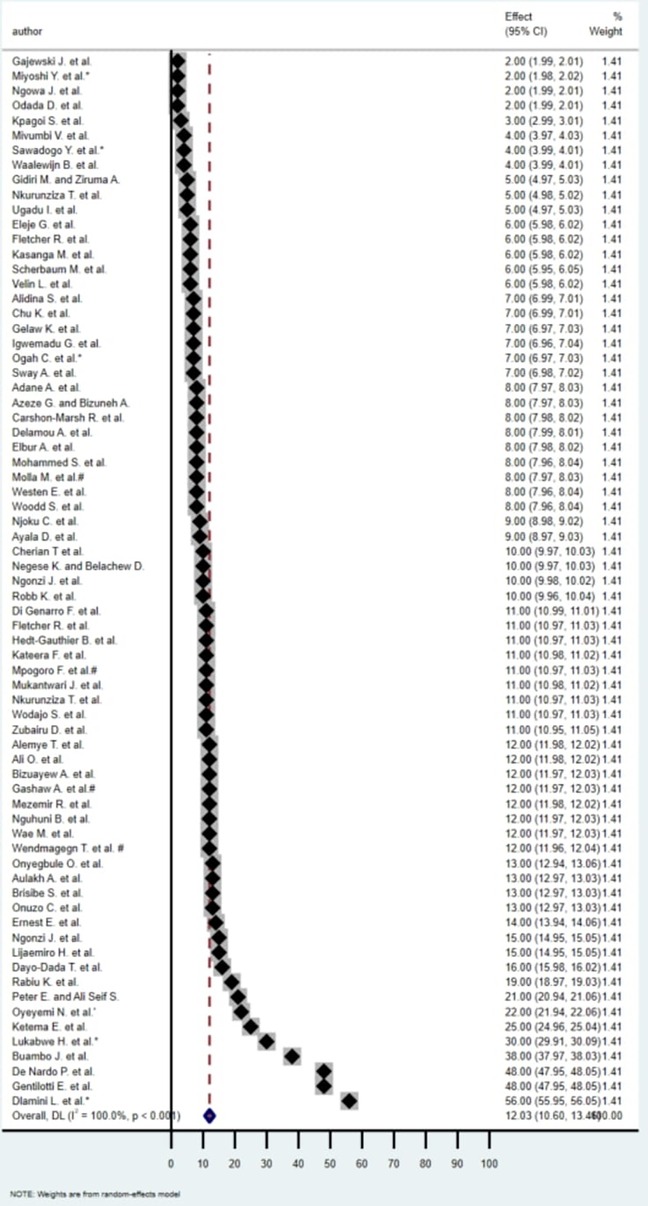
Figure 3. Forest plot of SSI rates of included publications.
Superficial SSIs had rates as high as 100.0% and were described in 32.3% (24/73) of studies followed by 24.7% (18/73) of studies reporting deep SSIs with highest rate of 32%, and 16.4% (12/73) detailing organ SSIs with rates up to 30.9% (Table 2).
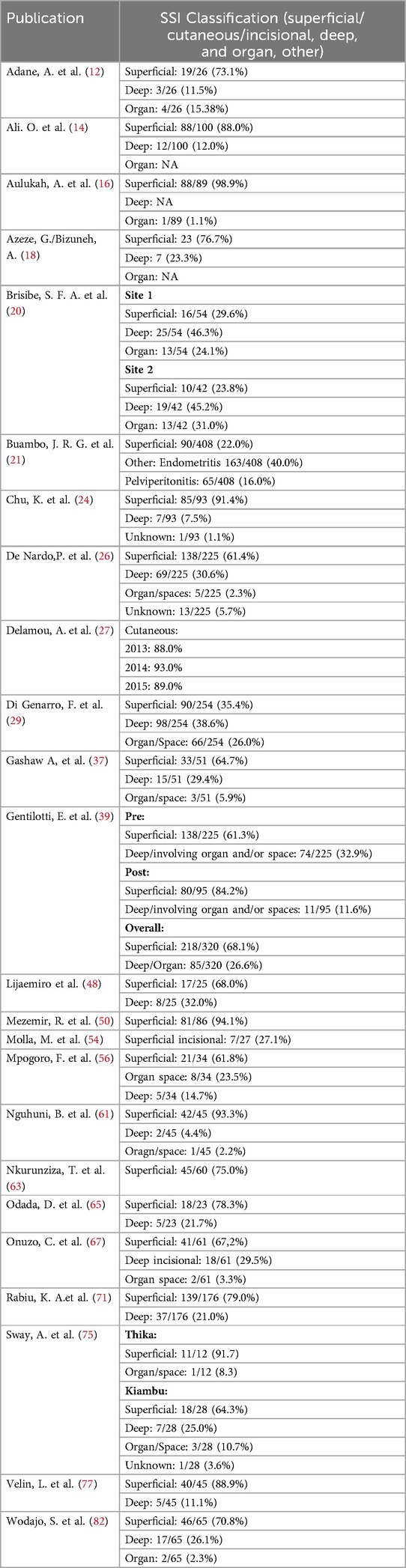
Table 2. SSI classification in included studies.
Appearance time of an SSI was reported by 42.5% (31/73) of included studies. A majority 61.3% (19/31) of those studies stated that most SSIs appear during the first two weeks after CS. Additionally, some studies reported SSI appearance time terms of pre/post-discharge (8/31) out of which a 75% majority (6/8) of SSIs appeared during post-discharge (Table 1).
Associated factors
Associated factors in the development of SSIs were reported in 38.0% (28/73) of the studies (Table 1). Duration of labour ≥8 h presented as the strongest risk factor (aOR 75.6) (67) and was mentioned in 9.6% (7/73) of the included studies (Table 1). Extended surgical duration, mentioned six times as a risk factor, also presented a substantial risk (aOR 21.1) (21) (Table 1).
A high number (greater than five) of vaginal examinations was mentioned multiple times with a risk of up to 13.1 (48), as well as stored water with aOR of 18.6 (48).
Additionally, chorioamnionitis (aOR 16.2) (80), an infection of the amniotic fluid, also significantly elevated the risk of post-caesarean SSI and was mentioned in five of the included studies (Table 1).
Premature rupture of membrane (PROM), was observed in 14 of the included studies (Table 1), making it the most frequent risk factor with reported aOR of up to 13.9 (18). Anaemia (also reported as low-haemoglobin/haematocrit/packed cell volume) throughout the surgical intervention was mentioned nine times (Table 1) with the highest aOR of 6.9 (28). Vertical/midline skin incisions (aOR 12.6) (67) were also notably high-risk factors compared to Pfannenstiel/transversal incisions which were reported as protective factors (aOR 0.21) (68).
The analysis of protective factors for post-CS outcomes identified several key factors, whereby CS at term (aOR 0.02) (48) presented the strongest protective effect against SSIs.
Having health insurance (aOR 0.06) (57) as well as tertiary level of education (aOR 0.24) (84), demonstrated as protective factors. Within the same study, all other associated factors were found to be protective including parity <4 (aOR 0.23) (84). Women with a normal body mass index (18.5–24.9) showed a protective aOR of 0.63 (39).
As opposed to the demonstrated risk factors of prolonged duration of labour, extended surgery duration and PROM, a <12 h duration of labour (aOR 0.07) (68), less than a 1 h surgical intervention (aOR 0.03) (62) and <24 h of membrane rupture (aOR 0.52) (62) were reported as protective factors.
Other surgical factors such as intraoperative blood loss of <1,000 ml (aOR 0.10) (80) and absorbable sutures (aOR 0.52) (39) were strong protective factors. Lastly, hospital stays of less than seven days had a protective aOR of 0.37 (50).
Bacteriological profiles
Only a minority of studies (17.8%; 13/73) reported bacteriological test results (Table 1). Staphylococcus aureus (S. aureus) was isolated in all thirteen of the studies with detection rates of up to 52.6% (70), and three of these studies also reported Methicillin-resistant S. aureus (MRSA) (26, 39, 67) which in turn was detected in rates of up to 79.0% (26, 39). One study measuring a 79.0% MRSA rate was able to reduce to a rate of only 21.0% following interventive measures (39).
Gram-negative bacteria were also prominent, particularly Escherichia coli which was identified in nine of the studies, and Klebsiella pneumoniae which was mentioned in seven studies, with two other studies also reporting Klebsiella species. Gram-negative bacteria was also reported as being resistant to ampicillin (100.0%), amoxicillin/clavulanate (93.0%), and trimethoprim/sulfamethoxazole (78.5%) (56) and susceptible or resistant to ceftriaxone (92.1%) and cefepime (84.6%) (77).
Discussion
This scoping review has a wide geographical representation with included data from 20 SSA countries, whereby most studies came from Ethiopia and Nigeria, possibly reflecting these countries as research epicenters in the region.
Our scoping review found a varying rate of SSIs. However, a large majority reported rates equal or below 20%, reflecting the WHO reporting for the African region (3).
CS are the most commonly performed major operation globally (5), thus surveillance of SSI after CS can be a good starting point for SSI surveillance (3). However, full patient follow-up to day 30 was only conducted in a small minority of studies, demonstrating a possible discordance between international guidelines and their feasibility in resource-limited settings. Given that the majority of SSI were diagnosed within the first two weeks after CS, this time frame could potentially be taken into consideration in the pending update to the WHO SSI surveillance protocol for resource-limited settings (3). Additionally, eight studies examined SSI occurrences in relation to discharge timing, with six reporting that SSIs primarily emerged post-discharge. This highlights the need to follow-up discharged patients, especially within the first two weeks after CS.
Given the limited-resource setting in SSA, the introduction of surveillance systems could start by targeted SSI screening of patients with the risk factors identified as most frequent such as PROM, prolonged labor, duration of surgery, anemia and multiple vaginal examinations. In addition to this targeted surveillance, we would recommend considering measures to mitigate certain risk factors, such as, treating anemia, applying hygiene measures during vaginal examinations and ensuring the provision of clean water. Additionally, certain surgical techniques such as Pfannenstiel (horizontal/transversal) incisions and absorbable sutures should be prioritized given their potential to minimize foreign body reaction (86) and decrease the likelihood of SSIs. SSIs can lead to increased hospital stays, costs, morbidities and mortalities, making their prevention and prompt management a priority (87). Incorporating these protective factors into clinical practice can potentially enhance patient recovery and reduce complication rates and hospitalisation duration. Such incorporation should be done in accordance with the WHO global guidelines for SSI prevention which also specify known protective measures (88).
Our scoping review found a considerable lack in the provision of data on bacteriological profiles. This weakness is in line with recent literature, showing that only 1.0% of laboratories in SSA are formally assigned to deliver bacterial testing (36). However, our synthesized data highlights Staphylococcus aureus as the most frequently reported pathogen causing SSI aligning with data from a recent meta-analysis (30). This is an area of concern considering corresponding reported rates of Methicillin-resistant S. aureus. Prevalence of Gram-negative Klebsiella pneumonia and Escherichia coli also emphasizes the burden of enterobacteria in SSI.
Current literature promotes antibiotic stewardship measures such as selecting the proper antibiotic for prophylaxis in accordance with current resistance data, but acknowledges that stewardship recommendations can be difficult to implement in settings like SSA that have limited antibiotic resources and resistance data (89). These findings, therefore, highlight the urgent need for enhanced bacteriological surveillance and antimicrobial resistance monitoring to inform effective SSI management strategies in the SSA region.
Limitations
This scoping review has several limitations. Despite our inclusive approach and the inclusion of all studies conducted in SSA, only 20 out of 48 of SSA countries were represented with highest representation of Ethiopia and Nigeria. We did not limit our search to English articles, nevertheless, we were only able to retrieve two French publications. As such, we reran the OVID search using French terms, but still did not retrieve additional French articles. Our search strategy only included studies published from 2014 onwards, potentially excluding older but relevant data. Due to the lack of available data in included studies, as well as missing correlation between symptom data and SSI, and vague distinction between wound infection symptoms and other issues such as endometritis, we dropped the analysis of SSI symptom data. Lastly, no private hospitals were included in the selected studies, therefore our findings may not be applicable in those settings.
Conclusion
Findings from this study can aid those who wish to follow the WHO recommendations in using post-caesarean section SSIs as a practical entry point for healthcare associated infection surveillance. However, low reporting on aspects such as full 30-day follow-up and bacteriological testing from included studies suggests difficulty in implementation of some surveillance measures. As most reported SSIs surfaced within the first two-weeks, this time frame can be taken into consideration as a first step in surveillance implementation. Regions such as SSA that have limited-resources for surveillance and treatment can also consider targeted SSI screening of patients with frequent risk factors, and promotion of reported protective measures. Furthermore, bacteriological diagnostic capacity building is greatly needed in the region in order to improve data gaps and antibiotic treatment recommendations. Utilization of these recommendations can ideally contribute towards improved safety for women undergoing CS in SSA.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
RW: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AB: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SW: Data curation, Formal analysis, Software, Writing – original draft. MN: Funding acquisition, Writing – review & editing. AD: Funding acquisition, Writing – review & editing. MD: Writing – review & editing. KH: Conceptualization, Investigation, Methodology, Software, Writing – original draft. CR: Conceptualization, Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. IN: Conceptualization, Funding acquisition, Project administration, Writing – review & editing. BD: Conceptualization, Funding acquisition, Supervision, Writing – review & editing. MC: Funding acquisition, Writing – review & editing. SM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by the Global Health Protection Program (# ZMI5-2523GHP029) under project PAcCI (Public Health Actions Ivory Coast) and (# ZMI5-2523GHP024) under project PASQUALE (Partnership to Improve Patient Safety and Quality of Care).
Acknowledgments
We would like to thank Dr. Francisco Pozo Martin for his experienced insight and guidance in the drafting of this review. Additionally, we thank all the past participants of the many studies included in this scoping review.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
aOR, adjusted odds ratio; BMI, body mass index; CDC, center for disease control and prevention; CI, confidence interval; CS, caesarean section; HIV, human immunodeficiency virus; JBI, Joanna Briggs institute; MRSA, methicillin-resistant staphylococcus aureus; OR, pdds ratio; OSF, open science framework; PRISMA-ScR, preferred reporting items for systematic reviews and meta-analysis extension for scoping reviews; SDGs, sustainable development Goals; SSA, sub-saharan Africa; SSI, surgical site infection; WBG, world bank group; WHO, world health organization.
References
1. Farid Mojtahedi M, Sepidarkish M, Almukhtar M, Eslami Y, Mohammadianamiri F, Behzad Moghadam K, et al. Global incidence of surgical site infections following caesarean section: a systematic review and meta-analysis. J Hosp Infect. (2023) 139:82–92. doi: 10.1016/j.jhin.2023.05.019
2. Zuarez-Easton S, Zafran N, Garmi G, Salim R. Postcesarean wound infection: prevalence, impact, prevention, and management challenges. Int J Womens Health. (2017) 9:81–8. doi: 10.2147/IJWH.S98876
3. WHO. Protocol for Surgical Site Infection Surveillance with a Focus on Settings with Limited Resources. Geneva: World Health Organization (2018).
4. Nejad SB, Allegranzi B, Syed S, Ellis B, Pittet D. Health-care-associated infection in Africa: a systematic review. Bull World Health Organ. (2011) 89(10):757–65. doi: 10.2471/BLT.11.088179
5. Gialdini C, Chamillard M, Diaz V, Pasquale J, Thangaratinam S, Abalos E, et al. Evidence-based surgical procedures to optimize caesarean outcomes: an overview of systematic reviews. EClinicalMedicine. (2024) 72:102632. doi: 10.1016/j.eclinm.2024.102632
6. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169(7):467–73. doi: 10.7326/M18-0850
7. Peters M, Godfrey C, McInerney P, Soares C, Khalil H, Parker D. Methodology for JBI scoping reviews. In: Aromataris E, editor. The Joanna Briggs Institute Reviewers Manual. Adelaide, SA: Joanna Briggs Institute (2015). p. 3–24.
8. Barth DD, Mayosi BM, Jabar A, Engel ME. Prevalence of group A streptococcal disease in North and Sub-Saharan Africa: a systematic review protocol. BMJ Open. (2015) 5(8):e008646. doi: 10.1136/bmjopen-2015-008646
9. WBG. Sub-Saharan Africa (2024). Available online at: https://data.worldbank.org/country/sub-saharan-africa (Accessed August 21, 2024).
10. Borodova A, Wood R, Müller S. Surgical Site Infections after Caesarean Section Across sub-Sahara Africa (2024). Available online at: https://osf.io/qe7bf/ (Accessed February 04, 2025).
11. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. (2016) 5(1):210. doi: 10.1186/s13643-016-0384-4
12. Adane A, Gedefa L, Eyeberu A, Tesfa T, Arkew M, Tsegaye S, et al. Predictors of surgical site infection among women following cesarean delivery in Eastern Ethiopia: a prospective cohort study. Ann Med Surg. (2023) 85(4):738–45. doi: 10.1097/MS9.0000000000000411
13. Alemye T, Oljira L, Fekadu G, Mengesha MM. Post cesarean section surgical site infection and associated factors among women who delivered in public hospitals in Harar city, Eastern Ethiopia: a hospital-based analytic cross-sectional study. PLoS One. (2021) 16(6):e0253194. doi: 10.1371/journal.pone.0253194
14. Ali O, Kassahun D, Rade BK, Atnafu A. Maternal factors are important predictors for surgical site infection following cesarean section in Northwest Ethiopian. Clin Epidemiol Glob Health. (2022) 13:100936. doi: 10.1016/j.cegh.2021.100936
15. Alidina S, Menon G, Staffa SJ, Alreja S, Barash D, Barringer E, et al. Outcomes of a multicomponent safe surgery intervention in Tanzania's Lake Zone: a prospective, longitudinal study. Int J Qual Health Care. (2021) 33(2):mzab087. doi: 10.1093/intqhc/mzab087
16. Aulakh A, Idoko P, Anderson ST, Graham W. Caesarean section wound infections and antibiotic use: a retrospective case-series in a tertiary referral hospital in the Gambia. Trop Dr. (2018) 48(3):192–9. doi: 10.1177/0049475517739539
17. Ayala D, Tolossa T, Markos J, Yilma MT. Magnitude and factors associated with surgical site infection among mothers underwent cesarean delivery in Nekemte town public hospitals, western Ethiopia. PLoS One. (2021) 16(4 April 2021):e0250736. doi: 10.1371/journal.pone.0250736
18. Azeze GG, Bizuneh AD. Surgical site infection and its associated factors following cesarean section in Ethiopia: a cross-sectional study. BMC Res Notes. (2019) 12(1):288. doi: 10.1186/s13104-019-4325-x
19. Bizuayew H, Abebe H, Mullu G, Bewuket L, Tsega D, Alemye T. Post-cesarean section surgical site infection and associated factors in East Gojjam zone primary hospitals, Amhara region, North West Ethiopia, 2020. PLoS One. (2021) 16(12 December):e0261951. doi: 10.1371/journal.pone.0261951
20. Brisibe SFA, Ordinioha B, Gbeneolol PK. The effect of hospital infection control policy on the prevalence of surgical site infection in a tertiary hospital in South-South Nigeria. Niger Med J. (2015) 56(3):194–8. doi: 10.4103/0300-1652.160393
21. Buambo JR, Eouani EM, Potokoué NS, Landou DJ, Itoua C, Mokoko JC, et al. Determinants associated with post-cesarean operating site infections from January 01, 2013 to June 30, 2019 at the Brazzaville university hospital center. East Afr Med J. (2019) 96(1):2296–301. Available at: https://www.ajol.info/index.php/eamj/article/view/194049
22. Carshon-Marsh R, Squire JS, Kamara KN, Sargsyan A, Delamou A, Camara BS, et al. Incidence of surgical site infection and use of antibiotics among patients who underwent caesarean section and herniorrhaphy at a regional referral hospital, Sierra Leone. Int J Environ Res Public Health. (2022) 19(7):4048. doi: 10.3390/ijerph19074048
23. Cherian T, Hedt-Gauthier B, Nkurunziza T, Sonderman K, Gruendl MA, Nihiwacu E, et al. Diagnosing post-cesarean surgical site infections in rural Rwanda: development, validation, and field testing of a screening algorithm for use by community health workers. Surg Infect (Larchmt). (2020) 21(7):613–20. doi: 10.1089/sur.2020.062
24. Chu K, Maine R, Trelles M. Cesarean section surgical site infections in sub-Saharan Africa: a multi-country study from medecins sans frontieres. World J Surg. (2015) 39(2):350–5. doi: 10.1007/s00268-014-2840-4
25. Dayo-Dada TO, Ojo AA, Akpor OA. Prevalence of surgical site infection among caesarean section patients in a teaching hospital in Ekiti State, Nigeria: an eight-year review. Sci Afr. (2022) 16:e01216. doi: 10.1016/j.sciaf.2022.e01216
26. De Nardo P, Gentilotti E, Nguhuni B, Vairo F, Chaula Z, Nicastri E, et al. Post-caesarean section surgical site infections at a Tanzanian tertiary hospital: a prospective observational study. J Hosp Infect. (2016) 93(4):355–9. doi: 10.1016/j.jhin.2016.02.021
27. Delamou A, Camara BS, Sidibé S, Camara A, Dioubaté N, El Ayadi AM, et al. Trends of and factors associated with cesarean section related surgical site infections in Guinea. J Public Health Afr. (2019) 10(1):1–5. doi: 10.4081/jphia.2019.818
28. Dessu S, Samuel S, Gebremeskel F, Basazin A, Tariku Z, Markos M. Determinants of post cesarean section surgical site infection at public hospitals in Dire Dawa administration, Eastern Ethiopia: case control study. PLoS One. (2021) 16(4):e0250174. doi: 10.1371/journal.pone.0250174
29. Di Gennaro F, Marotta C, Pisani L, Veronese N, Pisani V, Lippolis V, et al. Maternal caesarean section infection (MACSI) in Sierra Leone: a case-control study. Epidemiol Infect. (2020) 148:e40. doi: 10.1017/S0950268820000370
30. Dlamini LD, Sekikubo M, Tumukunde J, Kojjo C, Ocen D, Wabule A, et al. Antibiotic prophylaxis for caesarean section at a Ugandan hospital: a randomised clinical trial evaluating the effect of administration time on the incidence of postoperative infections. BMC Pregnancy Childbirth. (2015) 15(91):1–7. doi: 10.1186/s12884-015-0514-3
31. Elbur AI, Yousif MA, El Sayed ASA, Abdel-Rahman ME. Misuse of prophylactic antibiotics and prevalence of postoperative wound infection in obstetrics and gynecology department in a Sudanese hospital. Health. (2014) 6(2):158–64. doi: 10.4236/health.2014.62025
32. Eleje GU, Ugwu EO, Enebe JT, Okoro CC, Okpala BC, Ezeora NC, et al. Cesarean section rate and outcomes during and before the first wave of COVID-19 pandemic. SAGE Open Med. (2022) 10:20503121221085453. doi: 10.1177/20503121221085453
33. Ernest EC, Hellar A, Varallo J, Tibyehabwa L, Bertram MM, Fitzgerald L, et al. Reducing surgical site infections and mortality among obstetric surgical patients in Tanzania: a pre-evaluation and postevaluation of a multicomponent safe surgery intervention. BMJ Glob Health. (2021) 6(12):e006788. doi: 10.1136/bmjgh-2021-006788
34. Fletcher RR, Schneider G, Bikorimana L, Rukundo G, Niyigena A, Miranda E, et al. The use of Mobile thermal imaging and deep learning for prediction of surgical site infection. Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society. Annual International Conference, 2021 (2021). p. 5059–62.
35. Fletcher RR, Schneider G, Hedt-Gauthier B, Nkurunziza T, Alayande B, Riviello R, et al. Use of convolutional neural nets and transfer learning for prediction of surgical site infection from color images. Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society. Annual International Conference, 2021 (2021). p. 5047–50.
36. Gajewski J, Cheelo M, Bijlmakers L, Kachimba J, Pittalis C, Brugha R. The contribution of non-physician clinicians to the provision of surgery in rural Zambia—a randomised controlled trial. Hum Resour Health. (2019) 17(60):1–8. doi: 10.1186/s12960-019-0398-9
37. Gashaw A, Fantu S, Tarekegn M. Factor associated with surgical site infection of women who undergone cesarean section in Hawassa university comprehensive specialized hospital southern Ethiopia, retrospective study design. Int J Surg Open. (2022) 44:100506. doi: 10.1016/j.ijso.2022.100506
38. Gelaw KA, Aweke AM, Astawesegn FH, Demissie BW, Zeleke LB. Surgical site infection and its associated factors following cesarean section: a cross sectional study from a public hospital in Ethiopia. Patient Saf Surg. (2017) 11(1):18. doi: 10.1186/s13037-017-0131-3
39. Gentilotti E, De Nardo P, Nguhuni B, Piscini A, Damian C, Vairo F, et al. Implementing a combined infection prevention and control with antimicrobial stewardship joint program to prevent caesarean section surgical site infections and antimicrobial resistance: a Tanzanian tertiary hospital experience. Antimicrob Resist Infect Cont. (2020) 9(1):69. doi: 10.1186/s13756-020-00740-7
40. Gidiri MF, Ziruma A. A randomized clinical trial evaluating prophylactic single-dose vs prolonged course of antibiotics for caesarean section in a high HIV-prevalence setting. J Obstet Gynaecol. (2014) 34(2):160–4. doi: 10.3109/01443615.2013.832737
41. Hedt-Gauthier B, Miranda E, Nkurunziza T, Hughes O, Boatin AA, Gaju E, et al. Telemedicine for surgical site infection diagnosis in rural Rwanda: concordance and accuracy of image reviews. World J Surg. (2022) 46(9):2094–101. doi: 10.1007/s00268-022-06597-8
42. Igwemadu GT, Eleje GU, Eno EE, Akunaeziri UA, Afolabi FA, Alao AI, et al. Single-dose versus multiple-dose antibiotics prophylaxis for preventing caesarean section postpartum infections: a randomized controlled trial. Women’s Health. (2022) 18:17455057221101071. doi: 10.1177/17455057221101071
43. Kaboré B, Soudouem G, Seck I, Millogo T, Evariste Yaméogo WM, Kouanda S. A case-control study of risk factors for surgical site infection after cesarean delivery in eastern Burkina Faso. Int J Gynecol Obstet. (2016) 135(Supplement 1):S107–10. doi: 10.1016/j.ijgo.2016.08.018
44. Kasanga M, Chileshe M, Mudenda S, Mukosha R, Kasanga M, Daka V, et al. Antibiotic prescribing patterns and prevalence of surgical site infections in caesarean section deliveries at two tertiary hospitals in Lusaka, Zambia. Pharmacol Pharm. (2022) 13(8):313–30. doi: 10.4236/pp.2022.138024
45. Kateera F, Riviello R, Goodman A, Nkurunziza T, Cherian T, Bikorimana L, et al. The effect and feasibility of mHealth-supported surgical site infection diagnosis by community health workers after cesarean section in rural Rwanda: randomized controlled trial. JMIR Mhealth Uhealth. (2022) 10(6):e35155. doi: 10.2196/35155
46. Ketema DB, Wagnew F, Assemie MA, Ferede A, Alamneh AA, Leshargie CT, et al. Incidence and predictors of surgical site infection following cesarean section in North-west Ethiopia: a prospective cohort study. BMC Infect Dis. (2020) 20(1):902. doi: 10.1186/s12879-020-05640-0
47. Kpagoi SSTK, Kamara KN, Carshon-Marsh R, Delamou A, Manzi M, Kamara RZ, et al. Assessing changes in surgical site infections and antibiotic use among caesarean section and herniorrhaphy patients at a regional hospital in Sierra Leone following operational research in 2021. Trop Med Infect Dis. (2023) 8(8):385. doi: 10.3390/tropicalmed8080385
48. Lijaemiro H, Berhe Lemlem S, Tesfaye Deressa J. Incidence of surgical site infection and factors associated among cesarean deliveries in selected government hospitals in Addis Ababa, Ethiopia, 2019. Obstet Gynecol Int. (2020) 2020:9714640. doi: 10.1155/2020/9714640
49. Lukabwe H, Kajabwangu R, Mugisha D, Mayengo H, Munyanderu B, Baluku A, et al. Effectiveness of preoperative bath using chloroxylenol antiseptic soap on the incidence of post emergency cesarean section surgical site infection at Mbarara regional referral hospital, Uganda: a randomized controlled trial. Pan Afr Med J. (2022) 41:92. doi: 10.11604/pamj.2022.41.92.23687
50. Mezemir R, Olayemi O, Dessie Y. Incidence, bacterial profile and predictors of surgical site infection after cesarean section in Ethiopia, a prospective cohort study. Int J Women’s Health. (2023) 15:1547–60. doi: 10.2147/IJWH.S425632
51. Mivumbi VN, Little SE, Rulisa S, Greenberg JA. Prophylactic ampicillin versus cefazolin for the prevention of post-cesarean infectious morbidity in Rwanda. Int J Gynecol Obstet. (2014) 124(3):244–7. doi: 10.1016/j.ijgo.2013.09.017
52. Miyoshi Y. Maternal and perinatal outcomes in urgent referral and non-referral cases of emergency cesarean section at a district hospital in zambia: a retrospective observational study. Pan Afr Med J. (2019) 33:324. doi: 10.11604/pamj.2019.33.324.19832
53. Mohammed S, A Shuaibu S, Gaya S, Rabiu A. The efficacy of two doses versus 7 days’ course of prophylactic antibiotics following cesarean section: an experience from Aminu Kano teaching hospital. Ann Afr Med. (2020) 19(2):103–12. doi: 10.4103/aam.aam_39_19
54. Molla M, Temesgen K, Seyoum T, Melkamu M. Surgical site infection and associated factors among women underwent cesarean delivery in debretabor general hospital, northwest Ethiopia: hospital based cross sectional study. BMC Pregnancy Childbirth. (2019) 19(1):317. doi: 10.1186/s12884-019-2442-0
55. Mothiba MS, Tshepuwane TC, Adefolalu AO, Monokoane TS. Alexis O-ring wound retractor versus traditional metal retractors for the prevention of postcaesarean surgical site infections. S Afr Fam Pract (2004). (2023) 65(1):a5651. doi: 10.4102/safp.v65i1.5651
56. Mpogoro FJ, Mshana SE, Mirambo MM, Kidenya BR, Gumodoka B, Imirzalioglu C. Incidence and predictors of surgical site infections following caesarean sections at Bugando medical centre, Mwanza, Tanzania. Antimicrob Resist Infect Cont. (2014) 3(1):25. doi: 10.1186/2047-2994-3-25
57. Mukantwari J, Gatete JdD, Niyigena A, Alayande BT, Nkurunziza T, Mazimpaka C, et al. Late and persistent symptoms suggestive of surgical site infections after cesarean section: results from a prospective cohort study in rural Rwanda. Surg Infect (Larchmt). (2023) 24(10):916–23. doi: 10.1089/sur.2023.100
58. Ketemaw N, Dereje Zeleke B. Maternal complications and associated factors among mothers who underwent a cesarean section at Gebretsadik Shewa general hospital: an institution based cross-sectional study. Front Glob Women’s Health. (2023) 4:1091863. doi: 10.3389/fgwh.2023.1091863
59. Ngonzi J, Bebell LM, Boatin AA, Owaraganise A, Tiibajuka L, Fajardo Y, et al. Impact of an educational intervention on WHO surgical safety checklist and pre-operative antibiotic use at a referral hospital in southwestern Uganda. Int J Qual Health Care. (2021) 33(3):mzab089. doi: 10.1093/intqhc/mzab089
60. Ngowa JDK, Ngassam A, Fouogue FT, Metogo J, Medou A, Kasia JM. [Early maternal complications of cesarean section: about 460 cases in two university hospitals in Yaounde, Cameroon]. Complications maternelles precoces de la cesarienne: a propos de 460 cas dans deux hopitaux universitaires de Yaounde, Cameroun. Pan Afr Med J. (2015) 21:265. doi: 10.11604/pamj.2015.21.265.6967
61. Nguhuni B, De Nardo P, Gentilotti E, Chaula Z, Damian C, Mencarini P, et al. Reliability and validity of using telephone calls for post-discharge surveillance of surgical site infection following caesarean section at a tertiary hospital in Tanzania. Antimicrob Resist Infect Cont. (2017) 6(1):43. doi: 10.1186/s13756-017-0205-0
62. Njoku CO, Njoku AN. Microbiological pattern of surgical site infection following caesarean section at the university of Calabar teaching hospital. Open Access Maced J Med Sci. (2019) 7(9):1430–5. doi: 10.3889/oamjms.2019.286
63. Nkurunziza T, Kateera F, Sonderman K, Gruendl M, Nihiwacu E, Ramadhan B, et al. Prevalence and predictors of surgical-site infection after caesarean section at a rural district hospital in Rwanda. Br J Surg. (2019) 106(2):e121–8. doi: 10.1002/bjs.11060
64. Nkurunziza T, Williams W, Kateera F, Riviello R, Niyigena A, Miranda E, et al. mHealth-community health worker telemedicine intervention for surgical site infection diagnosis: a prospective study among women delivering via caesarean section in rural Rwanda. BMJ Glob Health. (2022) 7(7):e009365. doi: 10.1136/bmjgh-2022-009365
65. Odada D, Shah J, Mbithi A, Shah R. Surgical site infections post cesarean section and associated risk factors: a retrospective case-control study at a tertiary hospital in Kenya. Infect Prev Pract. (2024) 6(1):100333. doi: 10.1016/j.infpip.2023.100333
66. Ogah CO, Anikwe CC, Ajah LO, Ikeotuonye AC, Lawani OL, Okorochukwu BC, et al. Preoperative vaginal cleansing with chlorhexidine solution in preventing post-cesarean section infections in a low resource setting: a randomized controlled trial. Acta Obstet Gynecol Scand. (2020) 100(4):694–703. doi: 10.1111/aogs.14060
67. Onuzo CN, Sefogah PE, Nuamah MA, Ntumy M, Osei M-M, Nkyekyer K. Surgical site infections following caesarean sections in the largest teaching hospital in Ghana. Infect Prev Pract. (2022) 4(2):100203. doi: 10.1016/j.infpip.2022.100203
68. Onyegbule O, Akujobi C, Ezebialu I, Nduka A, Anahalu I, Okolie V, et al. Determinants of post-caesarean wound infection in Nnewi, Nigeria. Br J Med Med Res. (2015) 5(6):767–74. doi: 10.9734/BJMMR/2015/10297
69. Oyeyemi N, Oyeneyin L, Oluwole A, Oyeyemi A, Afolabi B. Post-operative management in uncomplicated caesarean delivery: a randomised trial of short-stay versus traditional protocol at the Lagos university teaching hospital, Nigeria. Niger Postgrad Med J. (2019) 26(1):31–7. doi: 10.4103/npmj.npmj_166_18
70. Peter EG, Ali Seif S. The influence of home environment and wound care practice on surgical site infection among post cesarean section women in Dodoma- Tanzania. Int J Africa Nurs Sci. (2022) 17:100474. doi: 10.1016/j.ijans.2022.100474
71. Rabiu K, Akinlusi F, Adewunmi A, Alausa T, Durojaiye I. Risk factors for postcesarean wound infection in a tertiary hospital in Lagos, Nigeria. Niger Med J. (2020) 61(5):262–8. doi: 10.4103/nmj.NMJ_1_20
72. Robb KA, Habiyakare C, Kateera F, Nkurunziza T, Dusabe L, Kubwimana M, et al. Variability of water, sanitation, and hygiene conditions and the potential infection risk following cesarean delivery in rural Rwanda. J Water Health. (2020) 18(5):741–52. doi: 10.2166/wh.2020.220
73. Sawadogo YA, Komboigo E, Kiemtore S, Zamane H, Ouedraogo I, Kain DP, et al. Parietal suppurations after cesarean section at the Yalgado OueDraogo university hospital, Burkina Faso: epidemiological clinical, therapeutic and prognostic aspects. Pan Afr Med J. (2019) 32:35. doi: 10.11604/pamj.2019.32.35.17167
74. Scherbaum M, Kösters K, Mürbeth RE, Ngoa UA, Kremsner PG, Lell B, et al. Incidence, pathogens and resistance patterns of nosocomial infections at a rural hospital in Gabon. BMC Infect Dis. (2014) 14:1–8. doi: 10.1186/1471-2334-14-124
75. Sway A, Wanyoro A, Nthumba P, Aiken A, Ching P, Maruta A, et al. Prospective cohort study on timing of antimicrobial prophylaxis for post-cesarean surgical site infections. Surg Infect (Larchmt). (2020) 21(6):552–7. doi: 10.1089/sur.2018.226
76. Ugadu IO, Egede JO, Nwigboji WN, Igwe CP, Nwali AS, Adebayo JA, et al. Pre-operative vs. post-operative vaginal cleansing with povidone-iodine and post-caesarean infectious morbidity: a randomized controlled study. J West Afr Coll Surg. (2022) 12(4):64–74. doi: 10.4103/jwas.jwas_159_22
77. Velin L, Umutesi G, Riviello R, Muwanguzi M, Bebell LM, Yankurije M, et al. Surgical site infections and antimicrobial resistance after cesarean section delivery in rural Rwanda. Ann Glob Health. (2021) 87(1):77. doi: 10.5334/aogh.3413
78. Waalewijn BP, van Duinen A, Koroma AP, Rijken MJ, Elhassein M, Bolkan HA. Learning curve characteristics for caesarean section among associate clinicians: a prospective study from Sierra Leone. World J Surg. (2017) 41(12):2998–3005. doi: 10.1007/s00268-017-4202-5
79. Melkamu BW, Fanuel B, Niguse M, Feleke H. Magnitude of maternal complications and associated obstetric factors among women who gave birth by cesarean section at arba-minich general hospital, southern Ethiopia: retrospective cohort. J Public Health Epidemiol. (2017) 9(5):133–44. doi: 10.5897/JPHE2016.0898
80. Wendmagegn TA, Abera GB, Tsehaye WT, Gebresslasie KB, Tella BG. Magnitude and determinants of surgical site infecion among women underwent cesarean section in Ayder comprehensive specialized hospital Mekelle City, Tigray region, Northern Ethiopia, 2016. BMC Pregnancy Childbirth. (2018) 18(1):489. doi: 10.1186/s12884-018-2075-8
81. Westen EH, Kolk PR, Van Velzen CL, Unkels R, Mmuni NS, Hamisi AD, et al. Single-dose compared with multiple day antibiotic prophylaxis for cesarean section in low-resource settings, a randomized controlled, noninferiority trial. Acta Obstet Gynecol Scand. (2015) 94(1):43–9. doi: 10.1111/aogs.12517
82. Wodajo S, Belayneh M, Gebremedhin S. Magnitude and factors associated with post-cesarean surgical site infection at hawassa university teaching and referral hospital, southern Ethiopia: a cross-sectional study. Ethiop J Health Sci. (2017) 27(3):283–90. doi: 10.4314/ejhs.v27i3.10
83. Woodd SL, Kabanywanyi AM, Rehman AM, Campbell OMR, Kagambo A, Martiasi W, et al. Postnatal infection surveillance by telephone in Dar es Salaam, Tanzania: an observational cohort study. PLoS One. (2021) 16(7):e0254131. doi: 10.1371/journal.pone.0254131
84. Zubairu UD, Abdul MA, Bawa US, Madugu NH, Ghazzali S. Incidence, timing, and possible risk factors for post-cesarean wound infection among low-risk patients in Zaria, Nigeria: a cross-sectional study. Niger J Basic Clin Sci. (2023) 20(2):177–81. doi: 10.4103/njbcs.njbcs_20_23
86. Maehara Y, Shirabe K, Kohnoe S, Emi Y, Oki E, Kakeji Y, et al. Impact of intra-abdominal absorbable sutures on surgical site infection in gastrointestinal and hepato-biliary-pancreatic surgery: results of a multicenter, randomized, prospective, phase II clinical trial. Surg Today. (2017) 47(9):1060–71. doi: 10.1007/s00595-017-1480-3
87. Badia JM, Casey AL, Petrosillo N, Hudson PM, Mitchell SA, Crosby C. Impact of surgical site infection on healthcare costs and patient outcomes: a systematic review in six European countries. J Hosp Infect. (2017) 96(1):1–15. doi: 10.1016/j.jhin.2017.03.004
88. WHO. Global Guidelines for the Prevention of Surgical Site Infection. Geneva: World Health Organization (2018). p. 184. Available at: https://www.who.int/publications/i/item/9789241550475 (Accessed March 01, 2025).
Keywords: surgical site infection, wound infection, caesarean, sub-Saharan Africa, scoping review
Citation: Wood R, Borodova A, Wolter S, N’Guessan M, Diallo AA, Diallo MK, Heldt K, Rocha C, Nabé I, Diané B, Cherif MS and Müller SA (2025) Surgical site infections after caesarean section across sub-Sahara Africa: a scoping review of prevalence and associated factors. Front. Glob. Women's Health 6:1605049. doi: 10.3389/fgwh.2025.1605049
Received: 15 April 2025; Accepted: 12 June 2025;
Published: 1 July 2025.
Edited by:
Bandit Chumworathayi, Khon Kaen University, ThailandReviewed by:
Andrew Mgaya, Muhimbili National Hospital, TanzaniaAkmal El-Mazny, Cairo University, Egypt
Copyright: © 2025 Wood, Borodova, Wolter, N’Guessan, Diallo, Diallo, Heldt, Rocha, Nabé, Diané, Cherif and Müller. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rebekah Wood, d29vZHJAcmtpLmRl
†These authors have contributed equally to this work and share first authorship