 J. J. Sandra Kooij1,2*
J. J. Sandra Kooij1,2* Maxime de Jong2
Maxime de Jong2 Jessica Agnew-Blais3Silvia Amoretti4Kathrine Bang Madsen5,6Isabella Barclay7
Jessica Agnew-Blais3Silvia Amoretti4Kathrine Bang Madsen5,6Isabella Barclay7 Sven Bölte8,9,10
Sven Bölte8,9,10 Charlotte Borg Skoglund11,12Thomas Broughton3
Charlotte Borg Skoglund11,12Thomas Broughton3 Sara Carucci13Dorenda K. E. van Dijken14Julia Ernst15,16
Sara Carucci13Dorenda K. E. van Dijken14Julia Ernst15,16 Blandine French17,18Matilda A. Frick19,20
Blandine French17,18Matilda A. Frick19,20 Cédric Galera21,22
Cédric Galera21,22 Annabeth P. Groenman23,24,25Helena Kopp Kallner26,27Julia Kerner auch Koerner28,29Sarah Kittel-Schneider30,31
Annabeth P. Groenman23,24,25Helena Kopp Kallner26,27Julia Kerner auch Koerner28,29Sarah Kittel-Schneider30,31 Iris Manor32Joanna Martin7
Iris Manor32Joanna Martin7 Emilia Matera33Valeria Parlatini34,35
Emilia Matera33Valeria Parlatini34,35 Alexandra Philipsen36Josep Anthoni Ramos-Quiroga4,37,38Iris L. Rapoport39Karl Lundin Remnélius8Amandine Sénéquier3
Alexandra Philipsen36Josep Anthoni Ramos-Quiroga4,37,38Iris L. Rapoport39Karl Lundin Remnélius8Amandine Sénéquier3 Lisa Thorell12Janneke M. E. Wittekoek40
Lisa Thorell12Janneke M. E. Wittekoek40 Dora Wynchank2
Dora Wynchank2
- 1Department of Psychiatry, Amsterdam University Medical Center/VUmc, Amsterdam, Netherlands
- 2Expertise Center Adult ADHD, PsyQ, Psycho-medical Programs, The Hague, Netherlands
- 3Department of Psychology, School of Biological and Behavioural Sciences, Queen Mary University of London, London, United Kingdom
- 4Group of Psychiatry, Mental Health and Addictions, Vall D'Hebron Research Institute (VHIR), Biomedical Research Networking Centre Consortium on Mental Health (CIBERSAM), Barcelona, Spain
- 5Department of Clinical Research, University of Southern Denmark, Odense, Denmark
- 6National Centre for Register-based Research, Department of Public Health, Aarhus University, Aarhus, Denmark
- 7Centre for Neuropsychiatric Genetics and Genomics & Wolfson Centre for Young People’s Mental Health, Cardiff University, Cardiff, United Kingdom
- 8Center of Neurodevelopmental Disorders (KIND), Department of Women’s and Children’s Health, Centre for Psychiatry Research, Karolinska Institutet & Region Stockholm, Stockholm, Sweden
- 9Child and Adolescent Psychiatry, Stockholm Health Care Services, Region Stockholm, Stockholm, Sweden
- 10Curtin Autism Research Group, Curtin School of Allied Health, Curtin University, Perth, WA, Australia
- 11Department of Womens and Childrens Health, Uppsala University, Uppsala, Sweden
- 12Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden
- 13Department of Medical Sciences and Public Health, University of Cagliari and Child and Adolescent Unit P.O. Microcitemico ASL Cagliari, Cagliari, Italy
- 14Department of Gynaecology, OLVG Hospital, Amsterdam, Netherlands
- 15Department of Child and Adolescent Psychiatry and Psychotherapy, Central Institute of Mental Health, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany
- 16German Center for Mental Health (DZPG), Partner Site Mannheim-Heidelberg-Ulm, Mannheim, Germany
- 17School of Psychology, University of Nottingham, Nottingham, United Kingdom
- 18Institute of Mental Health, University of Nottingham, Nottingham, United Kingdom
- 19Department of Medical Sciences, Uppsala University, Uppsala, Sweden
- 20Department of Psychology, Stockholm University, Stockholm, Sweden
- 21University of Bordeaux, INSERM, BPH, U1219, Bordeaux, France
- 22Department of Child and Adolescent Psychiatry, Centre Hospitalier Perrens, Bordeaux, France
- 23Research Institute of Child Development and Education, University of Amsterdam, Amsterdam, Netherlands
- 24Department of Child and Adolescent Psychiatry, University Medical Center Groningen, University of Groningen, Groningen, Netherlands
- 25Accare Child Study Center, Groningen, Netherlands
- 26Department of Clinical Sciences, Danderyd Hospital Karolinska Institutet, Stockholm, Sweden
- 27Department of Obstetrics and Gynecology, Danderyd Hospital, Stockholm, Sweden
- 28Institute for Psychology in Education, University of Münster, Münster, Germany
- 29IDeA - Center for Research on Individual Development and Adaptive Education of Children at Risk, Frankfurt am Main, Germany
- 30Department of Psychiatry and Neurobehavioural Science, University College Cork, Cork, Ireland
- 31APC Microbiome, University College Cork, Cork, Ireland
- 32ADHD Clinic, Geha Mental Health Center, Petach-Tiqva, Israel
- 33Department of Precision and Regenerative Medicine and Ionic Area, University of Bari, Bari, Italy
- 34Child and Adolescent Psychiatry, University of Southampton/Hampshire, Southampton, United Kingdom
- 35IOW Healthcare NHS Foundation Trust, Southampton, United Kingdom
- 36Department of Psychiatry and Psychotherapy, University Hospital Bonn, Bonn, Germany
- 37Department of Mental Health, Hospital Universitari Vall d’Hebron, Barcelona, Spain
- 38Department of Psychiatry and Forensic Medicine, Universitat Autònoma de Barcelona, Barcelona, Spain
- 39Research Institute of Child Development and Education, University of Amsterdam, Amsterdam, Netherlands
- 40HeartLife Clinics Utrecht, Utrecht, Netherlands
Introduction: Attention-Deficit/Hyperactivity Disorder (ADHD) in girls and women is under-recognised and under-researched, despite increasing awareness of clinical challenges and unmet needs. This review by the Eunethydis Special Interest Group on Female ADHD, addresses current knowledge and identifies research gaps for future work. Issues in women with ADHD across the lifespan such as late diagnosis, pubertal development, sexual health, hormonal birth control, executive function difficulties, and gynaecological disorders associated with ADHD are highlighted.
Methods: The review synthesises existing literature and self-reported experiences of women with ADHD to explore the impact of hormonal fluctuations [puberty, menstrual cycle, pregnancy, (peri)menopause] on ADHD symptoms and mood disturbances. It examines the interplay of oestrogen and progesterone with dopaminergic pathways, when periods of lower oestrogen may affect cognition, as well as the manifestation of executive function deficits, and the intersection of ADHD with reproductive health.
Results: Hormonal transitions exacerbate ADHD symptoms and mood disturbances, yet pharmacological research and tailored treatments are lacking. Executive function deficits manifest differently in girls and women with ADHD and are influenced by neuropsychological and neurobiological profiles. Diagnostic practices and sociocultural factors contribute to delayed diagnoses, increasing the risk of comorbidities, impaired functioning, and diminished quality of life. Undiagnosed women have increased vulnerability to premenstrual dysphoric disorder, postpartum depression, and cardiovascular disease during perimenopause.
Discussion: Longitudinal, sex-specific studies incorporating hormonal status and lived experience are needed. Individualised interventions should be developed to address the unique needs of girls and women with ADHD. Addressing these gaps will advance more equitable diagnosis, management, and support for girls and women with ADHD, improving outcomes across the female lifespan.
1 Introduction
In October 2024, a “Special Interest Group (SIG) on Female ADHD” was initiated at the Annual Meeting of Eunethydis in Cagliari, Italy. Eunethydis is the European Network for Hyperactivity Disorders, an international network that aims to facilitate high quality science of Attention-Deficit/Hyperactivity Disorder (ADHD), and its wider societal impact through clinical and basic science researchers collaborating across Europe and beyond. Forty-two researchers joined the SIG, and many participated in writing this first paper on “Female ADHD: Current Research and Future Directions”. We used the self-reported research needs of women with ADHD as our starting point (detailed below). The aim of this paper is to identify what we know and what we need to know about people assigned female at birth having ADHD, formulating the next research questions and collaborating internationally to speed up the progress.
1.1 Self-reported research needs of women with ADHD
Recently, ADDitude, an online media platform that represents the voice of, and advocates for, the ADHD community, inventoried the research needs identified by 750 women with self-reported ADHD (1). These results, similar to those produced by other authors, and by the Duke Center in 2024 (with data from 1,350 women, mostly with self-reported ADHD), highlighted hormonal symptoms and their impact on ADHD symptoms and mood as an area that is both important and needs to be understood better (Table 1) (2).
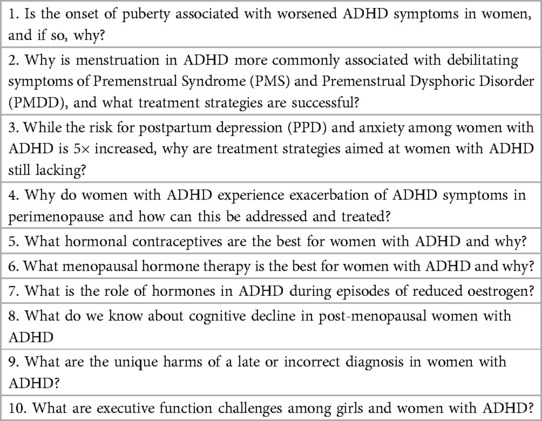
Table 1. Research needs according to ADDitude (1–6) and the Duke center (7–10).
1.2 Self-reported symptoms related to hormonal changes across the lifespan
The overwhelming cry for research into “hormonal issues and ADHD” is hardly surprising when one considers the self-reported struggles of women with ADHD throughout life, with exacerbations of symptoms in different periods. According to ADDitude, women with ADHD reported that their adolescence was marked by feelings of sadness or depression (70%), rejection sensitive dysphoria (63%), and greater worry or anxiety (58%). Throughout the reproductive phase of their lives, two-thirds of women said they had experienced PMS and/or PMDD. They experienced the following symptoms in their premenstrual week: irritability (80%), mood swings (79%), cramps or discomfort (79%), tension/anxiety (68%), and lack of focus/concentration (66%).
During pregnancy, for 20% of women, this episode brought greater focus, drive, organisation, and improved sleep. However, 44% of women noticed no difference in ADHD symptoms during pregnancy, perhaps because raised hormone levels were offset by the fact that 98% of women discontinued stimulant medication use. Another 36% said their ADHD symptoms worsened in pregnancy with exhaustion, poor memory, emotional dysregulation, and sensitivity.
The rate of self-reported PPD was 61%. Women reported that symptoms of PPD lasted roughly one year, and included the following: crying spells (76%), feelings of worthlessness, shame, guilt, or inadequacy (72%), mood swings (66%), irritability (62%), lack of concentration (58%), and sleep problems (57%).
In 2022, ADDitude also surveyed 4,000 women with ADHD about the impact of (peri)menopause. 70% of women said ADHD had a “life-altering” impact in their 40s and 50s, with 50% of women calling their ADHD “extremely severe”. The most debilitating symptoms were procrastination and time management (79%), working memory problems (74%), feelings of being overwhelmed (72%), and greater disorganisation (70%).
The conclusion is that there has been a strong call from the community for more research that needs to be taken seriously. Current knowledge however is relatively limited, we therefore aim in this Position paper to provide a comprehensive summary and discuss the available knowledge in the following Subsections:
1. The unique harms of late or incorrect diagnosis
2. The role of hormones in female ADHD
3. The executive function challenges in girls and women with ADHD
4. Pubertal development in girls with ADHD
5. Sexual health and risky sexual behaviour in girls with ADHD
6. The benefits and risks of hormonal birth control for women with ADHD
7. Maternal ADHD in the peripartum period
8. Hormonal and gynaecological disorders associated with ADHD [Polycystic Ovarian Syndrome (PCOS), Premature Ovarian Insufficiency (POI), endometriosis]
9. Neurocognitive decline and executive function in women with ADHD across the menopausal transition.
Finally, we collaboratively formulated research priorities to improve the debilitating symptoms and quality of life of girls and women with ADHD across the lifespan. While much of the existing research focuses on cisgender women, it is important to acknowledge that ADHD affects a diverse range of individuals, including children, non-binary individuals, and transgender men.
2.1 The unique harms of late or incorrect diagnosis
ADHD is not only diagnosed less frequently in girls than boys, but also at a later age (3–5). Often, women with ADHD seek help for other mental health difficulties such as anxiety or depression, rather than ADHD, leading to delayed or missed ADHD diagnoses (4, 6, 7). Compared to male individuals, females with ADHD face higher risks of co-occurring neurodevelopmental and psychiatric conditions, use of psychiatric medications and healthcare services (5, 8, 9). Many risks are worsened with late or missed diagnosis, including teenage pregnancy, risky sexual behaviour, self-harm or eating disorders (10). Late diagnoses also adversely impact relationships, mental health, confidence, and self-esteem in women (11).
Several factors result in delayed diagnosis, including diagnostic practices (e.g., male-biased criteria that may miss female manifestations) and sociocultural reasons (e.g., gendered expectations and masking symptoms (12), and access to inadequate services (13). Women with ADHD often adhere strongly to social norms, using compensatory strategies to mask their symptoms. While these mechanisms help them cope temporarily, they can lead to missed diagnoses, accumulation of secondary comorbid symptoms, and diminished self-esteem (14).
A formal ADHD diagnosis is essential for accessing self-education and other support (e.g., educational or workplace) and treatment (e.g., stimulant medication), which significantly improve long-term outcomes (15–17). However, girls and women are less likely to receive ADHD medications even when diagnosed (3, 18, 19).
2.1.1 Research gaps
Future research should investigate why girls and women are still underdiagnosed or diagnosed late and explore strategies and what symptoms of female ADHD should prompt proper diagnostic measures and improve early identification. Mixed-methods longitudinal studies and the involvement of women with lived ADHD experiences in research are essential to address these gaps.
2.2 The role and impact of hormones in female ADHD
For several decades, clinicians have observed changes in the severity of ADHD and mood symptoms during periods of hormonal fluctuations in women with ADHD (20–22). Currently, research is slowly catching up, providing the numbers to back up this clinical observation: the first self-report study of 209 women with clinically diagnosed ADHD found significantly higher premenstrual depressive symptoms than in the general population (45% vs. 28%) (23). Also, PPD symptoms were three times more prevalent (58% vs. 19%), and perimenopausal complaints showed a large effect size (Cohen's d 3.71). Vice versa, ADHD prevalence also has been shown to be increased in women with PMDD (24).
The question remains: why do these symptoms increase during periods of hormonal change in women with ADHD? One proposed mechanism involves the interplay between the neurotransmitter dopamine (25, 26), and fluctuations in oestrogen and progesterone levels throughout the female lifespan (27–32). Both the female sex hormones and dopamine have been associated with cognitive function and they reinforce each other's actions: oestrogen modulates dopamine (33–35), its synthesis, maintenance and the inhibition of its degradation (36, 37). Research in neurotypical women (n = 32) found increased hyperactivity and impulsivity during the early follicular and luteal phases (38), especially in those with high trait impulsivity, suggesting that hormonal changes may exacerbate ADHD symptoms especially in those with higher overall levels of ADHD characteristics. Another possible explanation may be inflammatory mechanisms, involved in the complex pathophysiology of ADHD (39–41), and in the menstrual cycle (42–44), however findings are preliminary.
It is understandable that when oestrogen is low or declining in an individual in whom important neurotransmitters such as dopamine are already low or dysregulated, these 'shortages' reinforce each other. Thus, women with ADHD may experience increased impairment in their mood, cognition, memory, sleep, and other domains of functioning.
Hormonal decline during perimenopause also increases the risk of cardiovascular disease (CVD), with CVD being the number one cause of death in women in general (45). One study showed that during perimenopause women with lifetime ADHD symptoms were overrepresented in a cardiology clinic (35% of n = 300 women) and were two years younger than the other women (46). It is possible that beyond the classical lifestyle risk factors such as a high Body Mass Index (BMI), diabetes, smoking, increased blood pressure and triglycerides, and a sedentary lifestyle, inflammation and stress-induced microvascular coronary artery spasm may play a role in this increased prevalence of CVD in women with ADHD symptoms (47, 48).
2.2.1 Research gaps
Understanding the interplay between female hormones and neurotransmitters is crucial for improving the diagnosis and treatment of ADHD in women. Given the impact of hormonal fluctuations on mood, cognition, and overall functioning, individualised treatment strategies—such as optimising stimulant dosages across menstrual phases (49), and/or offering SSRIs (50) and/or hormonal therapy (51), may improve symptom management. Future research should identify the mechanisms underlying these interactions as well as the interplay with cardiovascular health, and develop potential therapeutic targets to mitigate the heightened symptom burden.
2.3 Executive function challenges among girls and women with ADHD
Deficits in executive functions (EF) — such as inhibition, planning, working memory and task-switching — are a hallmark of ADHD. However, several studies identify sex differences in their presentation (52, 53). For instance, boys and men show worse response inhibition, slower processing speed, and more deficits in motor functioning (54–59) than girls and women. A recent meta-analysis confirmed greater deficits in inhibition and in cognitive flexibility in boys and men compared to girls and women, but no differences in working memory, planning and attention (60). In other studies, female children and adults with ADHD may experience more challenges with vocabulary, intellectual abilities, visuo-spatial reasoning and arousal/speed (55, 56, 59, 61). Girls are also more sensitive to small(er) immediate rewards than boys (62). It is also worth noting that EF may be affected by hormonal changes related to the menstrual cycle. Low oestrogen levels may induce hyperactivity-impulsivity symptoms post-ovulation and inattention symptoms peri-menstrually (27). However, these results must be interpreted with caution considering that a study in children aged 7 to 13 noted no significant sex difference in EF (63), suggesting that differences may emerge later, potentially influenced by pubertal hormonal changes.
Systematic reviews of magnetic resonance imaging studies have elucidated anatomical and functional alterations underlying executive dysfunction in ADHD, involving fronto-striato-parieto-cerebellar networks (64, 65). Most studies focused on male or mixed samples, however, there is preliminary evidence of both shared and specific sex-related brain alterations. For instance, studies reported sex-related effects on grey and white matter anatomy in frontal regions subserving impulse control and attention, such as smaller grey matter volumes in girls and white matter volumes in boys, as well as in their functional interaction with the default mode network during attention-demanding tasks, which was more compromised in boys (66–68). Despite these insights, research on EF in girls and women with ADHD remains limited, as most studies have been male-dominated.
2.3.1 Research gaps
Larger and more diverse female ADHD samples are essential to understand better sex-specific neuropsychological and neurobiological patterns. Hormonal interactions (oestrogen and progesterone) and their impact on ADHD symptoms and EF in girls and women require a systematic investigation. Further, longitudinal studies may clarify whether early EF deficits differentially impact longer-term outcomes, guiding preventive, and therapeutic interventions. Future studies may need to take hormonal status into consideration and should be timed according to menstrual phase or take ovulation inhibition into consideration. As prior studies have suggested that functional brain differences at various time points in the menstrual cycle, future studies need to investigate if intra-individual variability across the menstrual cycle phase is more pronounced than inter-individual variations related to underlying conditions.
2.4 Pubertal development in girls with ADHD
Adolescence is a period of social, psychological, and biological change that includes puberty, a time of hormonal changes that lead to reproductive maturity (69). Deviation from standard age of pubertal onset (early or late puberty), is associated with higher risk for later physical (70), mental (71–73) and social problems (74). While there is evidence for deviating pubertal timing in other neurodivergent groups such as autism [e.g., (75, 76)], there is currently limited evidence that ADHD itself is associated with a differential pubertal timing (77–79).
One study found that prepubertal use of stimulants was associated with a later age at menarche (i.e., first menstruation) in an all-female adolescent sample with ADHD. This effect might be driven by a lower BMI in those who started stimulant treatment at prepubertal age (77). Another study in Taiwan found girls with ADHD had higher risk for precocious puberty than girls without, but that stimulant medication had no effect on this association (and overall the condition was very rare, approximately 1 in 24,000 children) (80, 81).
Regarding stimulant use during adolescence, a pharmacovigilance analysis of United States Food and Drug Administration (FDA) report found that female adolescents over the age of 13 using methylphenidate, atomoxetine, and amphetamines, reported different and more frequent adverse events than male individuals (82). We currently do not know why these differences arise. The adolescent period could be associated with differential treatment needs during pubertal development, also since a decrease in hyperactivity (but not inattention) is seen in female adolescents during this period (83). Importantly, adolescence is not merely a period of biological change, but also of rapid social and psychological transition, characterised by shifting societal expectations (27) and greater need for autonomy (84). Both biological and psychosocial change should be taken into account when considering diagnosis and treatment, however how this should be done is currently not known.
2.4.1 Research gaps
Research into ADHD and puberty, and into the effects of stimulant use on pubertal development in girls with ADHD is scarce, as is research on the impact of pubertal development on the effectiveness of stimulants. Large longitudinal case-control studies incorporating validated measures, as well as thorough mapping of stimulant treatment history is needed. We currently have little information on pharmacokinetics under the influence of hormonal fluctuations. Here we need both preclinical work, as well as pharmacological MRI in women and men with and without ADHD. Moreover, we know little about differential treatment needs in the light of changing ADHD characteristics and (societal) expectations, which could be investigated using mixed methods designs to elucidate ADHD specific expectations arising during puberty.
2.5 Sexual health and risky sexual behaviour
Women with ADHD are more likely to engage in risky sexual behaviours compared to their non-ADHD peers. These include increased likelihood of having multiple sexual partners and choosing risky sexual partners (85), earlier sexual activity (86), less frequent use of contraception (87), higher frequency of sexually transmitted diseases (88), and higher rates of unplanned and teenage pregnancies (89, 90).
Regarding the quality of their sexual life, women with ADHD also present with less sexual satisfaction and more sexual dysfunctions (91). These behaviours are often linked to emotional dysregulation, impulsivity, and oppositional symptoms (92). Women might feel strong expectations to fit in socially and feel under more peer pressure to act a certain way (11, 93). Additional social factors such as use of alcohol or drugs and staying out all night have been linked to increased risks of sexual risk-taking behaviours (94).
Finally, it is important to note that women with ADHD are also more likely than their peers to be victims of sexual abuse (95) and sexual victimisation (96, 97). Such risk increases in the event of identification with gender and sexual minority groups; women with ADHD are in fact more prone to identify as transgender and/or non-heterosexual gender identity compared to neurotypical individuals (92, 98, 99).
2.5.1 Research gaps
In addition to these findings, there is a need for more nuanced research focusing specifically on girls and women with ADHD. Future studies should aim to disentangle the roles of socio-demographic correlates and co-occurring conditions (e.g., autism, substance use) and environmental factors (e.g., childhood adversities) in contributing to risky sexual behaviours. Additionally, exploring the effectiveness of non-pharmacological and pharmacological interventions in reducing risky sexual behaviours and their consequences among women with ADHD is crucial.
To address these research priorities, it is essential to conduct large-scale, longitudinal studies that include diverse populations. Raising awareness of these increased risks in clinical settings is also essential for healthcare staff supporting girls and women with ADHD, ensuring a holistic view to ADHD that encompasses their sexual health and safety.
2.6 The benefits and risks of hormonal birth control for women with ADHD
Hormonal contraception for women with ADHD is a critical consideration, given their increased risk of early motherhood and engagement in risky sexual behaviour. Women with ADHD are six times more likely to become mothers before age 20, highlighting the importance of effective contraception for this population (89).
Long-acting reversible contraceptives (LARCs: hormonal IUDs, non-hormonal copper IUDs, hormonal implants) show promise for women with ADHD, with 74.2% of young women continuing use beyond 24 months, compared to only 14.9% for short-acting methods (100). This suggests that LARCs may be more suitable contraceptives, given the impulsivity and forgetfulness associated with ADHD.
Combined oral contraceptives (COCs) and progestin-only pills (POPs) have been shown to increase the risk of depression up to five times in women with ADHD compared to unaffected women, regardless of hormonal content (101). Thus, women with ADHD may be more sensitive to adverse mood effects from oral hormonal contraception, and/or mood changes due to forgetting the pill.
2.6.1 Research gaps
Further research is needed to understand the specific interactions between ADHD symptoms, hormonal contraceptives, and mood regulation. Priorities include investigating tailored contraceptive counselling that increase the use of safe and tolerable contraceptive methods in young women with ADHD. Also investigating the effects of oral and non-oral hormonal methods on mood and ADHD symptoms and quality of life (23).
To address these research priorities, longitudinal studies comparing different contraceptive methods among women with ADHD are necessary. Collaboration between psychiatrists, gynaecologists, and endocrinologists is crucial to design comprehensive studies that address both reproductive health and mental health aspects of contraceptive use in women with ADHD.
2.7 Maternal ADHD in the peripartum period
Currently, there is scarce evidence about maternal ADHD during pregnancy and after childbirth (the peripartum period). As mentioned earlier, women with ADHD are more likely to experience unplanned pregnancies. They are also more likely to continue smoking and alcohol consumption during pregnancy (102).
Pregnant women with ADHD often experience higher stress levels, less social support, and are at increased risk for depression and anxiety (103). There is a higher incidence of pregnancy and birth complications among mothers with ADHD, including pre-eclampsia, unplanned caesarean sections, premature births, and infections (104). High blood pressure is a symptom of pre-eclampsia, again hinting at a higher risk of cardiovascular diseases in women with ADHD.
Mothers with ADHD have a significantly higher risk (5–6 times) of developing postpartum depression and anxiety disorders (103). Children of mothers with peripartum depression have an increased risk of ADHD symptoms (105). It has been suggested that at least in subgroups of women with peripartum depression, inflammatory mechanisms may play a role (106). The relevance of this for women with ADHD remains to be investigated.
A Canadian study, analysing nearly 900,000 pregnancies in Ontario, found an almost 11-fold increase in ADHD stimulant medication use during pregnancy between 2000 and 2021, with a high rate of discontinuation during pregnancy and a partial resumption postpartum (107). The study also identified specific maternal characteristics associated with stimulant medication use during pregnancy, including lower income, higher BMI, smoking during pregnancy, and concurrent use of other psychotropic medications. Moreover, a study using Swedish registry data, found no increased risk of neurodevelopmental disorders, including ADHD and autism spectrum disorder, in children exposed to ADHD medications in utero, consistent across various medication types and exposure durations. The findings, also supported by a meta-analysis combining data of a previous Danish study, provide crucial safety data for methylphenidate, amphetamines, and atomoxetine (108). Other studies, found that the use of methylphenidate during pregnancy and breastfeeding is considered relatively safe, while amphetamine and lisdexamphetamine are contraindicated during breastfeeding due to potential accumulation in the child (102). There are few data about the safety of atomoxetine during breastfeeding, but if a non-stimulant drug is needed, bupropion is emerging as the preferred treatment option (109, 110). ADHD in mothers can affect parent-child interactions, leading to both positive (increased warmth) and negative (increased stress, lax or over reactive parenting) outcomes (102).
2.7.1 Research gaps
There is a need for more research on pregnancy and birth complications, peripartum anxiety and depression in women with ADHD, as well as safe and novel pharmacological and psychological treatment options. Additionally, more studies are required to investigate mother-child bonding and interactions during the early postnatal period. Given that ADHD is highly heritable, with environmental and developmental risk factors also contributing, early infancy represents a particularly vulnerable period. Therefore, research is needed to identify potential targets for prevention and early intervention to support optimal child development and mitigate the risk of adverse outcomes associated with perinatal and early infancy risk factors in children with a genetic predisposition to ADHD.
2.8 Hormonal and gynaecological disorders associated with ADHD
Research about hormonal and gynaecological disorders in ADHD remains scarce, despite emerging evidence suggesting that women with ADHD may experience elevated rates of polycystic ovarian syndrome (PCOS) (111–113) and possibly premature (or primary) ovarian insufficiency (POI) (114). Women with endometriosis have an increased risk of a later diagnosis of ADHD (115).
Five to eight percent of women of reproductive age are affected by PCOS, a heterogeneous endocrine syndrome characterised by two or more of the following criteria: hyperandrogenism, anovulation marked by infrequent or absent periods, and polycystic ovaries (116, 117). Prenatal exposure to excess androgens in utero may be linked to a higher incidence (42% chance) of ADHD in the offspring of mothers with PCOS (118), notably for female offspring (119), although causality is not established. The putative causal mechanisms linking PCOS and ADHD remain understudied.
In endometriosis, tissue resembling the endometrium is located outside the uterine cavity that causes an inflammatory reaction and sometimes scar tissue [see (120) for clinical guidelines]. Endometriosis occurs in approximately 2%–10% of women, usually during the reproductive years, and is associated with a higher risk of infertility (120). Symptoms can include pain during menstruation, during ovulation or sexual intercourse (dyspareunia), chronic pelvic pain, and fatigue. Women with endometriosis are more likely to be diagnosed with ADHD compared to those without endometriosis and to the general female population in Sweden (115). However, it is not known whether this is genetic confounding, or due to other links between ADHD and endometriosis.
Finally, POI refers to premature menopause (before the age of 40) and occurs in about 1% of women. POI is associated with oestrogen loss, and if untreated, it increases risk for cardiovascular disease, osteoporosis, and dementia (121). The causes of POI are often unknown and can include autoimmune disease or a mutation in the FMR1 gene (fragile X) (114). Women with a premutation of the FMR1 gene and a high number of CGG repeats may be more likely to have ADHD (114), but more studies are needed to investigate links between POI and ADHD.
2.8.1 Research gaps
Amid calls to study the impact of reproductive life transitions and the menstrual cycle on female ADHD (13, 122, 123), substantial research is needed to bridge the gaps in the understanding of hormonal and gynaecological disorders in female ADHD. Too little is known about whether women with ADHD are at higher risk of these disorders than their counterparts, as well as whether hormonal and gynaecological disorders play a role in inter-individual differences between women with ADHD in terms of ADHD presentation, mental health, and treatment outcomes. Furthermore, there may be complex underlying relationships which remain to be explored between ADHD, hormonal and gynaecological disorders, and inflammatory processes. Indeed, hormonal and gynaecological disorders have been linked to inflammatory processes (124–129) as well as cardiometabolic risk factors (130), and preliminary studies – if heterogeneous and sometimes contradictory – provide possible evidence of elevated inflammatory markers in ADHD (40, 131).
2.9 Neurocognitive decline and executive function in women with ADHD across the menopause transition
Women with ADHD experiencing menopause face unique cognitive challenges. There is evidence for neurocognitive and executive function decline in this group as post-menopausal women frequently report subjective cognitive decline (SCD) associated with reductions in medial temporal lobe volume, attention, verbal and working memory (132–134). This is also described in women taking oestrogen-decreasing treatments (134). SCD may be a marker for future Alzheimer's disease (134).
While less is known about neurocognition in women with ADHD, a genome wide association study showed an association with earlier onset of natural menopause (135), which is linked to Alzheimer's disease and late-life memory decline (136, 137). In older adults, ADHD increased susceptibility to cognitive impairment, especially with white matter hyperintensities (138). Women with ADHD have increased risk for (peri)menopausal symptoms (23), and a study assessing women with and without ADHD found that sleep problems, anxiety, and depression accounted for poorer executive functioning among post vs. premenopausal women (139).
No studies have specifically examined executive function decline in women with ADHD across the menopausal transition, but overlaps can be inferred from those without ADHD. Menopausal symptoms, like difficulty concentrating, can resemble ADHD, suggesting that hormonal changes may contribute to ADHD symptoms during midlife (140). Small studies found that treatments for ADHD (lisdexamphetamine and atomoxetine) significantly improved executive function difficulties in peri- and postmenopausal women without an ADHD diagnosis (141, 142). Menopausal sleep disorders impact cognitive function and overlap with ADHD symptoms (29, 30). The prevalence of sleep disorders among postmenopausal women is 51.6% (143) and about 60% in adults with ADHD (similar in men and women (144),. Given that (earlier) menopause, sleep loss and ADHD all contribute to poorer executive functioning, it is plausible that post-menopausal women with ADHD experience compounded executive function decline.
2.9.1 Research gaps
Longitudinal analyses of cognition and brain imaging studies among women with and without ADHD are important across the stages of menopause. Additionally, the impact of menopausal hormone therapy on cognition and the effectiveness of ADHD treatments should be investigated.
3 Concluding discussion
ADHD in girls and women has long been under-recognised, under-researched, and under-treated, and research was limited to cisgender women. This position paper identifies multiple critical knowledge gaps and highlights the need for a paradigm shift that considers more the complex interplay between neurodevelopment, hormonal dynamics, and gender-specific psychosocial factors.
• Longitudinal inclusive cohort studies that track individuals with ADHD of different genders across life stages to examine developmental trajectories, executive function profiles, and mental and physical health outcomes.
• Clinical trials exploring sex and gender-specific pharmacological treatments, including menstrual-cycle-adjusted stimulant dosing, SSRI treatment, and hormonal interventions (e.g., contraceptives, menopausal hormone therapy) to optimise ADHD symptom management.
• Comorbidity-focused research examining the bidirectional associations between ADHD and conditions such as PMDD, PCOS, endometriosis, cardiovascular disease, and cognitive decline, with attention to inflammatory pathways.
• Studies on the impact of puberty, pregnancy, menopause, and transition on cognitive function, risk-taking behaviours, and treatment efficacy, particularly in relation to stimulant pharmacokinetics and hormonal fluctuations.
• Research on the peripartum period, including risks of postpartum depression and impaired mother-infant bonding, to inform early interventions and impact of intergenerational ADHD transmission.
• Diagnostic innovation, including the development of sex and gender-sensitive tools that account for female-typical symptom expression, masking behaviours, and internalising comorbidities.
Addressing these research gaps requires interdisciplinary collaboration across psychiatry, endocrinology, gynaecology, cardiology, and neuroscience. By prioritising hormonal and inflammatory pathways and adopting inclusive, lifespan-focused research designs, the field can advance towards more effective, gender-sensitive ADHD care.
Author contributions
SK: Conceptualization, Writing – original draft, Writing – review & editing. MJ: Conceptualization, Writing – original draft, Writing – review & editing. JA-B: Writing – original draft, Writing – review & editing. SA: Writing – original draft, Writing – review & editing. KB: Writing – original draft, Writing – review & editing. IB: Writing – review & editing. SB: Writing – review & editing. CB: Writing – original draft, Writing – review & editing. TB: Writing – review & editing. SC: Writing – original draft, Writing – review & editing. DD: Writing – original draft, Writing – review & editing. JE: Writing – review & editing. BF: Writing – original draft, Writing – review & editing. MF: Writing – original draft, Writing – review & editing. CG: Writing – original draft, Writing – review & editing. AG: Writing – original draft, Writing – review & editing. HK: Writing – review & editing. JK: Writing – original draft, Writing – review & editing. SK-S: Writing – original draft, Writing – review & editing. IM: Writing – original draft, Writing – review & editing. JM: Writing – original draft, Writing – review & editing. EM: Writing – review & editing. VP: Writing – original draft, Writing – review & editing. AP: Writing – review & editing. JR-Q: Writing – review & editing. IR: Writing – original draft, Writing – review & editing. KR: Writing – review & editing. AS: Writing – review & editing. LT: Writing – review & editing. JW: Writing – review & editing. DW: Conceptualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We acknowledge the contributions on the self-reported research needs of women with ADHD by ADDitude, and the Duke Center for Girls & Women with ADHD, in particular Jennifer Gierisch, Julia Schechter, and Maura Devito.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Rodgers AL. We demand attention! A call for greater research on women with ADHD: ADDitude (2024). Available at: https://www.additudemag.com/health-equity-adhd-in-women-research/ (Accessed December 17, 2024).
2. Rodgers AL. Duke project narrows top research priorities for, and by, women with ADHD: ADDitude (2024). Available at: https://www.additudemag.com/adhd-symptoms-in-adult-women-duke-research/ (Accessed May 24, 2024).
3. Dalsgaard S, Thorsteinsson E, Trabjerg BB, Schullehner J, Plana-Ripoll O, Brikell I, et al. Incidence rates and cumulative incidences of the full spectrum of diagnosed mental disorders in childhood and adolescence. JAMA Psychiatry. (2020) 77(2):155–64. doi: 10.1001/jamapsychiatry.2019.3523
4. Martin J, Langley K, Cooper M, Rouquette OY, John A, Sayal K, et al. Sex differences in attention-deficit hyperactivity disorder diagnosis and clinical care: a national study of population healthcare records in Wales. J Child Psychol Psychiatry. (2024) 65(12):1648–58. doi: 10.1111/jcpp.13987
5. Skoglund C, Sundström Poromaa I, Leksell D, Ekholm Selling K, Cars T, Giacobini M, et al. Time after time: failure to identify and support females with ADHD–a Swedish population register study. J Child Psychol Psychiatry. (2024) 65(6):832–44. doi: 10.1111/jcpp.13920
6. Klefsjö U, Kantzer AK, Gillberg C, Billstedt E. The road to diagnosis and treatment in girls and boys with ADHD–gender differences in the diagnostic process. Nord J Psychiatry. (2021) 75(4):301–5. doi: 10.1080/08039488.2020.1850859
7. Powell V, Agha SS, Jones RB, Eyre O, Stephens A, Weavers B, et al. ADHD in adults with recurrent depression. J Affect Disord. (2021) 295:1153–60. doi: 10.1016/j.jad.2021.09.010
8. Ottosen C, Larsen JT, Faraone SV, Chen Q, Hartman C, Larsson H, et al. Sex differences in comorbidity patterns of attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. (2019) 58(4):412–22.e3. doi: 10.1016/j.jaac.2018.07.910
9. Solberg BS, Halmøy A, Engeland A, Igland J, Haavik J, Klungsøyr K. Gender differences in psychiatric comorbidity: a population-based study of 40 000 adults with attention deficit hyperactivity disorder. Acta Psychiatr Scand. (2018) 137(3):176–86. doi: 10.1111/acps.12845
10. French B, Daley D, Groom M, Cassidy S. Risks associated with undiagnosed ADHD and/or autism: a mixed-method systematic review. J Atten Disord. (2023) 27(12):1393–410. doi: 10.1177/10870547231176862
11. French B, Cassidy S. “Going through life on hard mode”—the experience of late diagnosis of autism and/or ADHD: a qualitative study. Autism Adulthood. (2024):1–10. doi: 10.1089/aut.2024.0085
12. Martin J. Why are females less likely to be diagnosed with ADHD in childhood than males? Lancet Psychiatry. (2024) 11(4):303–10. doi: 10.1016/S2215-0366(24)00010-5
13. Young S, Adamo N, Ásgeirsdóttir BB, Branney P, Beckett M, Colley W, et al. Females with ADHD: an expert consensus statement taking a lifespan approach providing guidance for the identification and treatment of attention-deficit/hyperactivity disorder in girls and women. BMC Psychiatry. (2020) 20:1–27. doi: 10.1186/s12888-020-02707-9
14. Merkt J, Gawrilow C. Health, dietary habits, and achievement motivation in college students with self-reported ADHD diagnosis. J Atten Disord. (2016) 20(9):727–40. doi: 10.1177/1087054714523127
15. Chang Z, D’Onofrio BM, Quinn PD, Lichtenstein P, Larsson H. Medication for attention-deficit/hyperactivity disorder and risk for depression: a nationwide longitudinal cohort study. Biol Psychiatry. (2016) 80(12):916–22. doi: 10.1016/j.biopsych.2016.02.018
16. Shaw M, Hodgkins P, Caci H, Young S, Kahle J, Woods AG, et al. A systematic review and analysis of long-term outcomes in attention deficit hyperactivity disorder: effects of treatment and non-treatment. BMC Med. (2012) 10:1–15. doi: 10.1186/1741-7015-10-99
17. Young S, Asherson P, Lloyd T, Absoud M, Arif M, Colley WA, et al. Failure of healthcare provision for attention-deficit/hyperactivity disorder in the United Kingdom: a consensus statement. Front Psychiatry. (2021) 12:649399. doi: 10.3389/fpsyt.2021.649399
18. Kok FM, Groen Y, Fuermaier AB, Tucha O. The female side of pharmacotherapy for ADHD—a systematic literature review. PLoS One. (2020) 15(9):e0239257. doi: 10.1371/journal.pone.0239257
19. Russell A, Ford T, Russell G. Barriers and predictors of medication use for childhood ADHD: findings from a UK population-representative cohort. Soc Psychiatry Psychiatr Epidemiol. (2019) 54:1555–64. doi: 10.1007/s00127-019-01720-y
20. Littman E, Dean JM, Wagenberg B, Wasserstein J. ADHD in females across the lifespan and the role of estrogen. ADHD Rep. (2021) 29(5):1–8. doi: 10.1521/adhd.2021.29.5.1
21. Quinn PO, Nadeau KG, Littman E. Understanding Girls with AD/HD. Silver Spring, MD: Advantage Books (1999).
22. Solden S. Women With Attention Deficit Disorder: Embrace Your Differences and Transform Your Life. Nevada City, CA: Underwood Books (2012).
23. Dorani F, Bijlenga D, Beekman ATF, van Someren EJW, Kooij JJS. Prevalence of hormone-related mood disorder symptoms in women with ADHD. J Psychiatr Res. (2021) 133:10–5. doi: 10.1016/j.jpsychires.2020.12.005
24. Lin P-C, Long C-Y, Ko C-H, Yen J-Y. Comorbid attention deficit hyperactivity disorder in women with premenstrual dysphoric disorder. J Womens Health. (2024) 33(9):1267–75. doi: 10.1089/jwh.2023.0907
25. Volkow ND, Wang GJ, Kollins SH, Wigal TL, Newcorn JH, Telang F, et al. Evaluating dopamine reward pathway in ADHD: clinical implications. JAMA. (2009) 302(10):1084–91. doi: 10.1001/jama.2009.1308
26. MacDonald HJ, Kleppe R, Szigetvari PD, Haavik J. The dopamine hypothesis for ADHD: an evaluation of evidence accumulated from human studies and animal models. Front Psychiatry. (2024) 15:1492126. doi: 10.3389/fpsyt.2024.1492126
27. Eng AG, Nirjar U, Elkins AR, Sizemore YJ, Monticello KN, Petersen MK, et al. Attention-deficit/hyperactivity disorder and the menstrual cycle: theory and evidence. Horm Behav. (2024) 158:105466. doi: 10.1016/j.yhbeh.2023.105466
28. Haimov-Kochman R, Berger I. Cognitive functions of regularly cycling women may differ throughout the month, depending on sex hormone status; a possible explanation to conflicting results of studies of ADHD in females. Front Hum Neurosci. (2014) 8:191. doi: 10.3389/fnhum.2014.00191
29. Barth C, Villringer A, Sacher J. Sex hormones affect neurotransmitters and shape the adult female brain during hormonal transition periods. Front Neurosci. (2015) 9:37. doi: 10.3389/fnins.2015.00037
30. Diekhof EK, Ratnayake M. Menstrual cycle phase modulates reward sensitivity and performance monitoring in young women: preliminary fMRI evidence. Neuropsychologia. (2016) 84:70–80. doi: 10.1016/j.neuropsychologia.2015.10.016
31. Frey BN, Dias RS. Sex hormones and biomarkers of neuroprotection and neurodegeneration: implications for female reproductive events in bipolar disorder. Bipolar Disord. (2014) 16(1):48–57. doi: 10.1111/bdi.12151
32. Turek J, Gąsior Ł. Estrogen fluctuations during the menopausal transition are a risk factor for depressive disorders. Pharmacol Rep. (2023) 75(1):32–43. doi: 10.1007/s43440-022-00444-2
33. Jacobs E, D'Esposito M. Estrogen shapes dopamine-dependent cognitive processes: implications for women’s health. J Neurosci. (2011) 31(14):5286–93. doi: 10.1523/JNEUROSCI.6394-10.2011
34. Sacher J, Okon-Singer H, Villringer A. Evidence from neuroimaging for the role of the menstrual cycle in the interplay of emotion and cognition. Front Hum Neurosci. (2013) 7:374. doi: 10.3389/fnhum.2013.00374
35. Shanmugan S, Epperson CN. Estrogen and the prefrontal cortex: towards a new understanding of estrogen’s effects on executive functions in the menopause transition. Hum Brain Mapp. (2014) 35(3):847–65. doi: 10.1002/hbm.22218
36. Crider A, Pillai A. Estrogen signaling as a therapeutic target in neurodevelopmental disorders. J Pharmacol Exp Ther. (2017) 360(1):48–58. doi: 10.1124/jpet.116.237412
37. Diekhof EK. Be quick about it. Endogenous estradiol level, menstrual cycle phase and trait impulsiveness predict impulsive choice in the context of reward acquisition. Horm Behav. (2015) 74:186–93. doi: 10.1016/j.yhbeh.2015.06.001
38. Roberts B, Eisenlohr-Moul T, Martel MM. Reproductive steroids and ADHD symptoms across the menstrual cycle. Psychoneuroendocrinology. (2018) 88:105–14. doi: 10.1016/j.psyneuen.2017.11.015
39. Akinci MA, Uzun N. Evaluation of hematological inflammatory markers in children and adolescents with attention deficit/hyperactivity disorder. Bratisl Lek Listy. (2021) 122(4):256–62. doi: 10.4149/BLL_2021_042
40. Anand D, Colpo GD, Zeni G, Zeni CP, Teixeira AL. Attention-deficit/hyperactivity disorder and inflammation: what does current knowledge tell US? A systematic review. Front Psychiatry. (2017) 8:228. doi: 10.3389/fpsyt.2017.00228
41. Vázquez-González D, Carreón-Trujillo S, Alvarez-Arellano L, Abarca-Merlin DM, Domínguez-López P, Salazar-García M, et al. A potential role for neuroinflammation in ADHD. Adv Exp Med Biol. (2023) 1411:327–56. doi: 10.1007/978-981-19-7376-5_15
42. Chaireti R, Lindahl TL, Byström B, Bremme K, Larsson A. Inflammatory and endothelial markers during the menstrual cycle. Scand J Clin Lab Invest. (2016) 76(3):190–4. doi: 10.3109/00365513.2015.1129670
43. Merino PM, Martínez D, Iñiguez G, Lopez P, Cassorla F, Perez-Bravo F, et al. Elevation of C-reactive protein during the luteal phase in healthy adolescents. Gynecol Endocrinol. (2015) 31(4):260–3. doi: 10.3109/09513590.2014.982086
44. Sahin Aydınyurt H, Yuncu YZ, Tekin Y, Ertugrul AS. IL-6, TNF-α levels and periodontal status changes during the menstrual cycle. Oral Dis. (2018) 24(8):1599–605. doi: 10.1111/odi.12917
45. Curtin SC, Tejada-Vera B, Bastian BA. Deaths: leading causes for 2021. Natl Vital Stat Rep. (2024) 73(4):1–116.
46. Ter Beek LS, Böhmer MN, Wittekoek ME, Kooij JJS. Lifetime ADHD symptoms highly prevalent in women with cardiovascular complaints. A cross-sectional study. Arch Womens Ment Health. (2023) 26(6):851–5. doi: 10.1007/s00737-023-01356-7
47. Kupper N, van den Houdt S, Kuijpers P, Widdershoven J. The importance, consequences and treatment of psychosocial risk factors in heart disease: less conversation, more action! Neth Heart J. (2024) 32(1):6–13. doi: 10.1007/s12471-023-01831-x
48. Thapar AK, Riglin L, Blakey R, Collishaw S, Davey Smith G, Stergiakouli E, et al. Childhood attention-deficit hyperactivity disorder problems and mid-life cardiovascular risk: prospective population cohort study. Br J Psychiatry. (2023) 223(4):472–7. doi: 10.1192/bjp.2023.90
49. De Jong M, Wynchank D, Van Andel E, Beekman A, Kooij J. Female-specific pharmacotherapy in ADHD: premenstrual adjustment of psychostimulant dosage. Front Psychiatry. (2023) 14:1306194. doi: 10.3389/fpsyt.2023.1306194
50. Marjoribanks J, Brown J, O'Brien PM, Wyatt K. Selective serotonin reuptake inhibitors for premenstrual syndrome. Cochrane Database Syst Rev. (2013) 2013(6):Cd001396. doi: 10.1002/14651858.CD001396.pub3
51. Panay N, Ang SB, Cheshire R, Goldstein SR, Maki P, Nappi RE. Menopause and MHT in 2024: addressing the key controversies - an international menopause society white paper. Climacteric. (2024) 27(5):441–57. doi: 10.1080/13697137.2024.2394950
52. Carucci S, Narducci C, Bazzoni M, Balia C, Donno F, Gagliano A, et al. Clinical characteristics, neuroimaging findings, and neuropsychological functioning in attention-deficit hyperactivity disorder: sex differences. J Neurosci Res. (2023) 101(5):704–17. doi: 10.1002/jnr.25038
53. Castellano-García F, Benito A, Jovani A, Fuertes-Sáiz A, Marí-Sanmillán MI, Haro G. Sex differences in substance use, prevalence, pharmacological therapy, and mental health in adolescents with attention-deficit/hyperactivity disorder (ADHD). Brain Sci. (2022) 12(5):590. doi: 10.3390/brainsci12050590
54. Hasson R, Fine JG. Gender differences among children with ADHD on continuous performance tests: a meta-analytic review. J Atten Disord. (2012) 16(3):190–8. doi: 10.1177/1087054711427398
55. Nussbaum NL. ADHD and female specific concerns: a review of the literature and clinical implications. J Atten Disord. (2012) 16(2):87–100. doi: 10.1177/1087054711416909
56. Rucklidge JJ. Gender differences in attention-deficit/hyperactivity disorder. Psychiatr Clin North Am. (2010) 33(2):357–73. doi: 10.1016/j.psc.2010.01.006
57. DeRonda A, Zhao Y, Seymour KE, Mostofsky SH, Rosch KS. Distinct patterns of impaired cognitive control among boys and girls with ADHD across development. Res Child Adolesc Psychopathol. (2021) 49:835–48. doi: 10.1007/s10802-021-00792-2
58. Ojuri B, DeRonda A, Plotkin M, Mostofsky SH, Rosch KS. The impact of sex on cognitive control in ADHD: girls slow to inhibit, boys inhibit less, and both show higher response variability. J Atten Disord. (2024) 28(9):1275–88. doi: 10.1177/10870547241237242
59. Lin YJ, Lai MC, Yang LK, Gau SS. Sex-differential patterns of neuropsychological functioning in adults with attention-deficit/hyperactivity disorder. Compr Psychiatry. (2024) 131:152464. doi: 10.1016/j.comppsych.2024.152464
60. Loyer Carbonneau M, Demers M, Bigras M, Guay M-C. Meta-analysis of sex differences in ADHD symptoms and associated cognitive deficits. J Atten Disord. (2021) 25(12):1640–56. doi: 10.1177/1087054720923736
61. Gaub M, Carlson CL. Gender differences in ADHD: a meta-analysis and critical review. J Am Acad Child Adolesc Psychiatry. (1997) 36(8):1036–45. doi: 10.1097/00004583-199708000-00011
62. Doidge JL, Flora DB, Toplak ME. A meta-analytic review of sex differences on delay of gratification and temporal discounting tasks in ADHD and typically developing samples. J Atten Disord. (2021) 25(4):540–61. doi: 10.1177/1087054718815588
63. Sjöwall D, Roth L, Lindqvist S, Thorell LB. Multiple deficits in ADHD: executive dysfunction, delay aversion, reaction time variability, and emotional deficits. J Child Psychol Psychiatry. (2013) 54(6):619–27. doi: 10.1111/jcpp.12006
64. Parlatini V, Itahashi T, Lee Y, Liu S, Nguyen TT, Aoki YY, et al. White matter alterations in attention-deficit/hyperactivity disorder (ADHD): a systematic review of 129 diffusion imaging studies with meta-analysis. Mol Psychiatry. (2023) 28(10):4098–123. doi: 10.1038/s41380-023-02173-1
65. Kowalczyk OS, Mehta MA, O’Daly OG, Criaud M. Task-based functional connectivity in attention-deficit/hyperactivity disorder: a systematic review. Biol Psychiatry Glob Open Sci. (2022) 2(4):350–67. doi: 10.1016/j.bpsgos.2021.10.006
66. Mahone EM, Ranta ME, Crocetti D, O'Brien J, Kaufmann WE, Denckla MB, et al. Comprehensive examination of frontal regions in boys and girls with attention-deficit/hyperactivity disorder. J Int Neuropsychol Soc. (2011) 17(6):1047–57. doi: 10.1017/S1355617711001056
67. Mills BD, Miranda-Dominguez O, Mills KL, Earl E, Cordova M, Painter J, et al. ADHD and attentional control: impaired segregation of task positive and task negative brain networks. Netw Neurosci. (2018) 2(02):200–17. doi: 10.1162/netn_a_00034
68. Peterson RK, Duvall P, Crocetti D, Palin T, Robinson J, Mostofsky SH, et al. ADHD-related sex differences in frontal lobe white matter microstructure and associations with response control under conditions of varying cognitive load and motivational contingencies. Brain Imaging Behav. (2023) 17(6):674–88. doi: 10.1007/s11682-023-00795-1
69. Spear LP. The adolescent brain and age-related behavioral manifestations. Neurosci Biobehav Rev. (2000) 24(4):417–63. doi: 10.1016/S0149-7634(00)00014-2
70. Fuhrman BJ, Moore SC, Byrne C, Makhoul I, Kitahara CM, Berrington de González A, et al. Association of the age at menarche with site-specific cancer risks in pooled data from nine cohorts. Cancer Res. (2021) 81(8):2246–55. doi: 10.1158/0008-5472.CAN-19-3093
71. Copeland WE, Worthman C, Shanahan L, Costello EJ, Angold A. Early pubertal timing and testosterone associated with higher levels of adolescent depression in girls. J Am Acad Child Adolesc Psychiatry. (2019) 58(12):1197–206. doi: 10.1016/j.jaac.2019.02.007
72. Deardorff J, Marceau K, Johnson M, Reeves JW, Biro FM, Kubo A, et al. Girls’ pubertal timing and tempo and mental health: a longitudinal examination in an ethnically diverse sample. J Adolesc Health. (2021) 68(6):1197–203. doi: 10.1016/j.jadohealth.2021.01.020
73. Lynch SJ, Sunderland M, Newton NC, Chapman C. A systematic review of transdiagnostic risk and protective factors for general and specific psychopathology in young people. Clin Psychol Rev. (2021) 87:102036. doi: 10.1016/j.cpr.2021.102036
74. Mensah FK, Bayer JK, Wake M, Carlin JB, Allen NB, Patton GC. Early puberty and childhood social and behavioral adjustment. J Adolesc Health. (2013) 53(1):118–24. doi: 10.1016/j.jadohealth.2012.12.018
75. Pohl A, Cassidy S, Auyeung B, Baron-Cohen S. Uncovering steroidopathy in women with autism: a latent class analysis. Mol Autism. (2014) 5:1–12. doi: 10.1186/2040-2392-5-27
76. Groenman AP, Van der Oord S, Geurts HM. Navigating adolescence: pubertal development in autism spectrum conditions and its relation to mental health. Arch Womens Mental Health. (2024) 27(6):913–21. doi: 10.1007/s00737-023-01414-0
77. Rosenthal EA, Hinshaw SP. Pubertal timing in adolescents with ADHD: extension and replication in an all-female sample. Eur Child Adolesc Psychiatry. (2024) 33:1133–41. doi: 10.1007/s00787-023-02239-z
78. Greenfield B, Hechtman L, Stehli A, Wigal T. Sexual maturation among youth with ADHD and the impact of stimulant medication. Eur Child Adolesc Psychiatry. (2014) 23:835–9. doi: 10.1007/s00787-014-0521-3
79. Friedel E, Vijayakumar N, Staniland L, Silk TJ. Puberty and ADHD: a scoping review and framework for future research. Clin Psychol Rev. (2025) 117:102567. doi: 10.1016/j.cpr.2025.102567
80. Pai L-F, Wang D-S, Hsu W-F, Huang S-W, Chung C-H, Chen S-J, et al. New insights into precocious puberty and ADHD: a nationwide cohort study. Pediatr Res. (2022) 92(6):1787–94. doi: 10.1038/s41390-022-02028-5
81. Carucci S, Zuddas A, Lampis A, Man KKC, Balia C, Buitelaar J, et al. The impact of methylphenidate on pubertal maturation and bone age in ADHD children and adolescents: results from the ADHD drugs use chronic effects (ADDUCE) Project. J Attention Disord. (2024) 28(5):722–39. doi: 10.1177/10870547241226726
82. Wei W, Chen L, Zhou H, Liu J, Zhang Y, Feng S, et al. Safety profiles of methylphenidate, amphetamine, and atomoxetine: analysis of spontaneous reports submitted to the food and drug administration adverse event reporting system. Front Pharmacol. (2023) 14:1208456. doi: 10.3389/fphar.2023.1208456
83. Eng AG, Phan JM, Shirtcliff EA, Eisenlohr-Moul TA, Goh PK, Martel MM. Aging and pubertal development differentially predict symptoms of ADHD, depression, and impairment in children and adolescents: an eight-year longitudinal study. Res Child Adolesc Psychopathol. (2023) 51(6):819–32. doi: 10.1007/s10802-023-01030-7
84. Steinberg L. The family at adolescence: transition and transformation. J Adolesc Health. (2000) 27(3):170–8. doi: 10.1016/S1054-139X(99)00115-9
85. Hosain GM, Berenson AB, Tennen H, Bauer LO, Wu ZH. Attention deficit hyperactivity symptoms and risky sexual behavior in young adult women. J Womens Health. (2012) 21(4):463–8. doi: 10.1089/jwh.2011.2825
86. Flory K, Molina BS, Pelham J, William E, Gnagy E, Smith B. Childhood ADHD predicts risky sexual behavior in young adulthood. J Clin Child Adolesc Psychol. (2006) 35(4):571–7. doi: 10.1207/s15374424jccp3504_8
87. Young S, Klassen LJ, Reitmeier SD, Matheson JD, Gudjonsson GH. Let’s talk about sex… and ADHD: findings from an anonymous online survey. Int J Environ Res Public Health. (2023) 20(3):2037. doi: 10.3390/ijerph20032037
88. Soldati L, Deiber MP, Schockaert P, Köhl J, Bolmont M, Hasler R, et al. Sexually transmitted diseases and attention-deficit/hyperactivity disorder: a systematic literature review. J Psychiatr Pract. (2024) 30(4):259–65. doi: 10.1097/PRA.0000000000000789
89. Skoglund C, Kallner HK, Skalkidou A, Wikström A-K, Lundin C, Hesselman S, et al. Association of attention-deficit/hyperactivity disorder with teenage birth among women and girls in Sweden. JAMA Netw Open. (2019) 2(10):e1912463-e. doi: 10.1001/jamanetworkopen.2019.12463
90. Owens EB, Zalecki C, Gillette P, Hinshaw SP. Girls with childhood ADHD as adults: cross-domain outcomes by diagnostic persistence. J Consult Clin Psychol. (2017) 85(7):723–36. doi: 10.1037/ccp0000217
91. Soldati L, Bianchi-Demicheli F, Schockaert P, Köhl J, Bolmont M, Hasler R, et al. Sexual function, sexual dysfunctions, and ADHD: a systematic literature review. J Sex Med. (2020) 17(9):1653–64. doi: 10.1016/j.jsxm.2020.03.019
92. Hertz PG, Turner D, Barra S, Biedermann L, Retz-Junginger P, Schöttle D, et al. Sexuality in adults with ADHD: results of an online survey. Front Psychiatry. (2022) 13:868278. doi: 10.3389/fpsyt.2022.868278
93. Guo C. Specific impairments and challenges in women with ADHD. J Educ Hum Soc Sci. (2024) 29:34–9. doi: 10.54097/vrh8jk90
94. White J, Buehler C, Weymouth BB. Childhood attention deficit hyperactive disorder (ADHD) symptoms and adolescent female sexual victimisation: mediating and moderating effects of risky behaviours. J Sex Aggression. (2014) 20(1):23–39. doi: 10.1080/13552600.2013.782429
95. Wymbs BT, Gidycz CA. Examining link between childhood ADHD and sexual assault victimization. J Atten Disord. (2021) 25(11):1612–22. doi: 10.1177/1087054720923750
96. White JW, Buehler C. Adolescent sexual victimization, ADHD symptoms, and risky sexual behavior. J Fam Violence. (2012) 27:123–32. doi: 10.1007/s10896-012-9411-y
97. Guendelman MD, Ahmad S, Meza JI, Owens EB, Hinshaw SP. Childhood attention-deficit/hyperactivity disorder predicts intimate partner victimization in young women. J Abnorm Child Psychol. (2016) 44(1):155–66. doi: 10.1007/s10802-015-9984-z
98. Bijlenga D, Vroege JA, Stammen AJM, Breuk M, Boonstra AM, van der Rhee K, et al. Prevalence of sexual dysfunctions and other sexual disorders in adults with attention-deficit/hyperactivity disorder compared to the general population. Atten Defic Hyperact Disord. (2018) 10(1):87–96. doi: 10.1007/s12402-017-0237-6
99. Garthe RC, Hidalgo MA, Hereth J, Garofalo R, Reisner SL, Mimiaga MJ, et al. Prevalence and risk correlates of intimate partner violence among a multisite cohort of young transgender women. LGBT Health. (2018) 5(6):333–40. doi: 10.1089/lgbt.2018.0034
100. McTaggart JSC, Kopp Kallner H. Tailored contraception for young females with ADHD - Long-acting reversible contraceptives favor twenty-four-month continuation.
101. Lundin C, Wikman A, Wikman P, Kallner HK, Sundström-Poromaa I, Skoglund C. Hormonal contraceptive use and risk of depression among young women with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. (2023) 62(6):665–74. doi: 10.1016/j.jaac.2022.07.847
102. Kittel-Schneider S, Quednow BB, Leutritz AL, McNeill RV, Reif A. Parental ADHD in pregnancy and the postpartum period–A systematic review. Neurosci Biobehav Rev. (2021) 124:63–77. doi: 10.1016/j.neubiorev.2021.01.002
103. Andersson A, Garcia-Argibay M, Viktorin A, Ghirardi L, Butwicka A, Skoglund C, et al. Depression and anxiety disorders during the postpartum period in women diagnosed with attention deficit hyperactivity disorder. J Affect Disord. (2023) 325:817–23. doi: 10.1016/j.jad.2023.01.069
104. Murray AL, Taut D, Baban A, Hemady CL, Walker S, Osafo J, et al. Associations between ADHD symptoms and maternal and birth outcomes: an exploratory analysis in a multi-country cohort of expectant mothers. J Atten Disord. (2022) 26(14):1882–94. doi: 10.1177/10870547221105064
105. Tusa BS, Alati R, Ayano G, Betts K, Weldesenbet AB, Dachew B. The risk of attention deficit hyperactivity disorder symptoms in offspring of mothers with perinatal depression: a systematic review and meta-analysis. Asian J Psychiatr. (2024) 102:104261. doi: 10.1016/j.ajp.2024.104261
106. Payne JL, Maguire J. Pathophysiological mechanisms implicated in postpartum depression. Front Neuroendocrinol. (2019) 52:165–80. doi: 10.1016/j.yfrne.2018.12.001
107. Nitchske A, Salmanpour A, Kaur P, do Valle HA, Elwood C, Gadermann A, et al. Prevalence trends and patterns of perinatal ADHD stimulant medication use in British Columbia, Canada. Pharmacoepidemiol Drug Saf. (2025) 34(4):e70129. doi: 10.1002/pds.70129
108. Bang Madsen K, Larsson H, Skoglund C, Liu X, Munk-Olsen T, Bergink V, et al. In utero exposure to methylphenidate, amphetamines and atomoxetine and offspring neurodevelopmental disorders – a population-based cohort study and meta-analysis. Mol Psychiatry. (2025):1–10. doi: 10.1038/s41380-025-02968-4
109. di Giacomo E, Confalonieri V, Tofani F, Clerici M. Methylphenidate and atomoxetine in pregnancy and possible adverse fetal outcomes: a systematic review and meta-analysis. JAMA Netw Open. (2024) 7(11):e2443648. doi: 10.1001/jamanetworkopen.2024.43648
110. Ornoy A, Koren G. The effects of drugs used for the treatment of attention deficit hyperactivity disorder (ADHD) on pregnancy outcome and breast-feeding: a critical review. Curr Neuropharmacol. (2021) 19(11):1794–804. doi: 10.2174/1570159X18666201127164000
111. Brutocao C, Zaiem F, Alsawas M, Morrow AS, Murad MH, Javed A. Psychiatric disorders in women with polycystic ovary syndrome: a systematic review and meta-analysis. Endocrine. (2018) 62:318–25. doi: 10.1007/s12020-018-1692-3
112. Rodriguez-Paris D, Remlinger-Molenda A, Kurzawa R, Głowińska A, Spaczyński R, Rybakowski F, et al. Psychiatric disorders in women with polycystic ovary syndrome. Psychiatr Pol. (2019) 53(4):955–66. doi: 10.12740/PP/OnlineFirst/93105
113. May T, Adesina I, McGillivray J, Rinehart NJ. Sex differences in neurodevelopmental disorders. Curr Opin Neurol. (2019) 32(4):622–6. doi: 10.1097/WCO.0000000000000714
114. Gabis LV, Shaham M, Attia OL, Kowal T, David S, Banet-Levi Y, et al. An escalating continuum of learning and attention difficulties from premutation to full mutation in female carriers of FMR1 expansion. Front Neurol. (2023) 14:1135630. doi: 10.3389/fneur.2023.1135630
115. Gao M, Koupil I, Sjöqvist H, Karlsson H, Lalitkumar S, Dalman C, et al. Psychiatric comorbidity among women with endometriosis: nationwide cohort study in Sweden. Am J Obstet Gynecol. (2020) 223(3):415.e1–e16. doi: 10.1016/j.ajog.2020.02.033
116. Azziz R, Woods KS, Reyna R, Key TJ, Knochenhauer ES, Yildiz BO. The prevalence and features of the polycystic ovary syndrome in an unselected population. J Clin Endocrinol Metab. (2004) 89(6):2745–9. doi: 10.1210/jc.2003-032046
117. ESHRE TR, Group A-SPCW. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. (2004) 81(1):19–25. doi: 10.1016/j.fertnstert.2003.10.004
118. Maleki A, Bashirian S, Soltanian AR, Jenabi E, Farhadinasab A. Association between polycystic ovary syndrome and risk of attention-deficit/hyperactivity disorder in offspring: a meta-analysis. Clin Exp Pediatr. (2021) 65(2):85. doi: 10.3345/cep.2021.00178
119. Cesta CE, Öberg AS, Ibrahimson A, Yusuf I, Larsson H, Almqvist C, et al. Maternal polycystic ovary syndrome and risk of neuropsychiatric disorders in offspring: prenatal androgen exposure or genetic confounding? Psychol Med. (2020) 50(4):616–24. doi: 10.1017/S0033291719000424
120. Becker CM, Bokor A, Heikinheimo O, Horne A, Jansen F, Kiesel L, et al. ESHRE guideline: endometriosis. Hum Reprod Open. (2022) 2022(2):hoac009. doi: 10.1093/hropen/hoac009
121. Panay N, Anderson RA, Bennie A, Cedars M, Davies M, Ee C, et al. Evidence-based guideline: premature ovarian insufficiency. Hum Reprod Open. (2024) 2024(4):hoae065. doi: 10.1093/hropen/hoae065
122. Rapoport IL, Groenman AP. A review of sex and gender factors in stimulant treatment for ADHD: knowledge gaps and future directions. J Atten Disord. (2025) 29(8):602–16. doi: 10.1177/10870547251315601
123. Hinshaw SP, Nguyen PT, O’Grady SM, Rosenthal EA. Annual research review: attention-deficit/hyperactivity disorder in girls and women: underrepresentation, longitudinal processes, and key directions. J Child Psychol Psychiatry. (2022) 63(4):484–96. doi: 10.1111/jcpp.13480
124. Aboeldalyl S, James C, Seyam E, Ibrahim EM, Shawki HE, Amer S. The role of chronic inflammation in polycystic ovarian syndrome-a systematic review and meta-analysis. Int J Mol Sci. (2021) 22(5):1–31. doi: 10.3390/ijms22052734
125. Alesi S, Teede HJ, Moran L, Enticott JC, De Silva K, Mousa A. Exploring causal associations between serum inflammatory markers and female reproductive disorders: a Mendelian randomisation study. Biomolecules. (2024) 14:1–14. doi: 10.3390/biom14121544
126. Özay AC, Özay ÖE. The importance of inflammation markers in polycystic ovary syndrome. Rev Assoc Med Bras. (2021) 67(3):411–7. doi: 10.1590/1806-9282.20200860
127. Artimani T, Karimi J, Mehdizadeh M, Yavangi M, Khanlarzadeh E, Ghorbani M, et al. Evaluation of pro-oxidant-antioxidant balance (PAB) and its association with inflammatory cytokines in polycystic ovary syndrome (PCOS). Gynecol Endocrinol. (2018) 34(2):148–52. doi: 10.1080/09513590.2017.1371691
128. Sanverdi I, Kilicci C, Cogendez E, Abide Yayla C, Ozkaya E. Utility of complete blood count parameters to detect premature ovarian insufficiency in cases with oligomenorrhea/amenorrhea. J Clin Lab Anal. (2018) 32(5):e22372. doi: 10.1002/jcla.22372
129. Ferencova N, Visnovcova Z, Ondrejka I, Hrtanek I, Bujnakova I, Kovacova V, et al. Peripheral inflammatory markers in autism Spectrum disorder and attention deficit/hyperactivity disorder at adolescent age. Int J Mol Sci. (2023) 24(14):1–27. doi: 10.3390/ijms241411710
130. AlAshqar A, Patzkowsky K, Afrin S, Wild R, Taylor HS, Borahay MA. Cardiometabolic risk factors and benign gynecologic disorders. Obstet Gynecol Surv. (2019) 74(11):661–73. doi: 10.1097/OGX.0000000000000718
131. Gedek A, Modrzejewski S, Gedek M, Antosik AZ, Mierzejewski P, Dominiak M. Neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and monocyte to lymphocyte ratio in ADHD: a systematic review and meta-analysis. Front Psychiatry. (2023) 14:1258868. doi: 10.3389/fpsyt.2023.1258868
132. Schaafsma M, Homewood J, Taylor A. Subjective cognitive complaints at menopause associated with declines in performance of verbal memory and attentional processes. Climacteric. (2010) 13(1):84–98. doi: 10.3109/13697130903009187
133. Thilers PP, Macdonald SW, Nilsson LG, Herlitz A. Accelerated postmenopausal cognitive decline is restricted to women with normal BMI: longitudinal evidence from the Betula project. Psychoneuroendocrinology. (2010) 35(4):516–24. doi: 10.1016/j.psyneuen.2009.08.018
134. Reuben R, Karkaby L, McNamee C, Phillips NA, Einstein G. Menopause and cognitive complaints: are ovarian hormones linked with subjective cognitive decline? Climacteric. (2021) 24(4):321–32. doi: 10.1080/13697137.2021.1892627
135. Demontis D, Walters RK, Martin J, Mattheisen M, Als TD, Agerbo E, et al. Discovery of the first genome-wide significant risk loci for attention deficit/hyperactivity disorder. Nat Genet. (2019) 51(1):63–75. doi: 10.1038/s41588-018-0269-7
136. Sochocka M, Karska J, Pszczołowska M, Ochnik M, Fułek M, Fułek K, et al. Cognitive decline in early and premature menopause. Int J Mol Sci. (2023) 24(7):1–16. doi: 10.3390/ijms24076566
137. Ding H, Li Y, Ang TFA, Liu Y, Devine S, Au R, et al. Reproductive markers in Alzheimer’s disease progression: the framingham heart study. J Prev Alzheimers Dis. (2023) 10(3):530–5. doi: 10.14283/jpad.2023.28
138. Callahan BL, Becker S, Ramirez J, Taylor R, Shammi P, Gao F, et al. Vascular burden moderates the relationship between ADHD and cognition in older adults. Am J Geriatr Psychiatry. (2024) 32(4):427–42. doi: 10.1016/j.jagp.2023.10.018
139. Page CE, Soreth B, Metcalf CA, Johnson RL, Duffy KA, Sammel MD, et al. Natural vs. surgical postmenopause and psychological symptoms confound the effect of menopause on executive functioning domains of cognitive experience. Maturitas. (2023) 170:64–73. doi: 10.1016/j.maturitas.2023.01.007
140. Pines A. Midlife ADHD in women: any relevance to menopause? Climacteric. (2016) 19(5):423–5. doi: 10.3109/13697137.2016.1152536
141. Epperson CN, Shanmugan S, Kim DR, Mathews S, Czarkowski KA, Bradley J, et al. New onset executive function difficulties at menopause: a possible role for lisdexamfetamine. Psychopharmacology (Berl). (2015) 232(16):3091–100. doi: 10.1007/s00213-015-3953-7
142. Epperson CN, Pittman B, Czarkowski KA, Bradley J, Quinlan DM, Brown TE. Impact of atomoxetine on subjective attention and memory difficulties in perimenopausal and postmenopausal women. Menopause. (2011) 18(5):542–8. doi: 10.1097/gme.0b013e3181fcafd6
143. Salari N, Hasheminezhad R, Hosseinian-Far A, Rasoulpoor S, Assefi M, Nankali S, et al. Global prevalence of sleep disorders during menopause: a meta-analysis. Sleep Breath. (2023) 27(5):1883–97. doi: 10.1007/s11325-023-02793-5
Keywords: ADHD, female, consensus, sex hormones, lifespan, sex specific, menstrual cycle, self-reported needs
Citation: Kooij JJS, de Jong M, Agnew-Blais J, Amoretti S, Bang Madsen K, Barclay I, Bölte S, Borg Skoglund C, Broughton T, Carucci S, van Dijken DKE, Ernst J, French B, Frick MA, Galera C, Groenman AP, Kopp Kallner H, Kerner auch Koerner J, Kittel-Schneider S, Manor I, Martin J, Matera E, Parlatini V, Philipsen A, Ramos-Quiroga JA, Rapoport IL, Remnélius KL, Sénéquier A, Thorell L, Wittekoek JME and Wynchank D (2025) Research advances and future directions in female ADHD: the lifelong interplay of hormonal fluctuations with mood, cognition, and disease. Front. Glob. Women's Health 6:1613628. doi: 10.3389/fgwh.2025.1613628
Received: 17 April 2025; Accepted: 19 May 2025;
Published: 7 July 2025.
Edited by:
Frances Louise Dark, Metro South Addiction and Mental Health Services, AustraliaReviewed by:
Stephen Hinshaw, University of California, Berkeley, United StatesCatrin Borneskog Sinclair, Dalarna University, Sweden
Copyright: © 2025 Kooij, de Jong, Agnew-Blais, Amoretti, Bang Madsen, Barclay, Bölte, Borg Skoglund, Broughton, Carucci, van Dijken, Ernst, French, Frick, Galera, Groenman, Kopp Kallner, Kerner auch Koerner, Kittel-Schneider, Manor, Martin, Matera, Parlatini, Philipsen, Ramos-Quiroga, Rapoport, Remnélius, Sénéquier, Thorell, Wittekoek and Wynchank. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: J. J. Sandra Kooij, cy5rb29pakBwc3lxLm5s