 Elena M. D. Schönthaler
Elena M. D. Schönthaler Nina Dalkner*
Nina Dalkner* Tatjana Stross
Tatjana Stross Susanne Bengesser
Susanne Bengesser Julia Ilic
Julia Ilic Frederike Fellendorf
Frederike Fellendorf Alexander FinnerEva Fleischmann
Alexander FinnerEva Fleischmann Alfred HäusslJohanna GeorgiAlexander Maget
Alfred HäusslJohanna GeorgiAlexander Maget Melanie LengerAnnamaria Painold
Melanie LengerAnnamaria Painold Martina Platzer
Martina Platzer Robert Queissner
Robert Queissner Franziska SchmiedhoferStefan SmolleAdelina Tmava-Berisha
Franziska SchmiedhoferStefan SmolleAdelina Tmava-Berisha Eva Z. Reininghaus
Eva Z. Reininghaus- Clinical Division of Psychiatry and Psychotherapeutic Medicine, Medical University of Graz, Graz, Austria
Background: Bipolar disorder is associated with impairments in cognition and psychosocial functioning. Although these impairments occur frequently, often persist during euthymic times, and worsen quality of life, the impact of cognitive abilities on functioning has not yet been fully elucidated.
Methods: The current study investigated the effects of cognitive domains (attention/psychomotor speed, verbal learning/memory, executive function) on psychosocial functioning cross-sectionally. Data from 210 euthymic individuals with bipolar disorder [101 female, 109 male; M(age) = 44.47; SD(age) = 14.25] were included into the analysis. A neurocognitive test battery was administered and the Global Assessment of Functioning was used to depict psychosocial functioning. Correlation analyses were conducted to observe the associations between functioning and the cognitive domains. Moreover, three hierarchical regression analyses were applied to predict functioning by each of the cognitive domains, while considering age, sex, and education as control variables.
Results: Correlation analyses revealed that functioning was positively associated with attention/psychomotor speed and verbal learning/memory. However, the consecutive hierarchical regression analyses found that none of the cognitive domains were able predict functioning beyond the control variables age, sex, and education.
Conclusion: Our findings indicate that greater abilities in the domains of attention/psychomotor speed and verbal learning/memory are associated with better functioning. However, this association can be explained by other relevant variables such as age or education, indicating that cognitive abilities are not the sole contributor of psychosocial functioning. Investigating other measurements of functioning or cognitive abilities could lead to different results. Nevertheless, promoting cognitive abilities and autonomy in daily life remains an important aspect of therapy in bipolar disorder.
1 Introduction
Bipolar disorder (BD) is a neuropsychiatric disorder characterized by recurring (hypo) manic and depressive episodes with an estimated prevalence of 1–2% worldwide (Blanco et al., 2017). Common symptoms of manic episodes include an expansive or irritated mood, highly elevated activity, decreased need for sleep, overconfidence, grandiosity, talkativeness, and impulse disinhibition (Carvalho et al., 2020). Contrary, depressive episodes encompass, among others, persistent sadness, loss of interest or pleasure, fatigue, sleep disturbances, and feelings of worthlessness or guilt (Dilling and Freyberger, 2019). In both mood states, cognitive deficits including attention, memory, and executive function impairments occur frequently and often persist during euthymia, especially in longer illness durations (Chen et al., 2023; Tsapekos et al., 2021). Due to these debilitating symptoms, BD was ranked as one of the 20 leading causes of disability worldwide (Anyayo et al., 2021; Arvilommi et al., 2022), and the worldwide prevalence of moderate to severe disability for BD is estimated at approximately 22 million individuals (Chen et al., 2019). One of the driving aspects of disability in BD is the low level of functioning, which differs slightly across mood states (Rosa et al., 2009; Van Der Voort et al., 2015) and serves as a key domain of illness outcome (Gitlin and Miklowitz, 2017), low quality of life, productivity loss (Kato et al., 2021), and suicidality (Rosa et al., 2008).
Functioning represents a multidimensional concept, including the ability to perform and engage in various life situations (World Health Organization, 2015), as well as managing aspects of the environment that help or hinder these life experiences (Chen et al., 2019). Over the past decades, the term global functioning, which subsumes the measurement of several types of functioning, has emerged (Aas, 2010). Global functioning encompasses, among others, psychosocial functioning (i.e., the ability to sustain social relationships and engage in activities of daily life; Michalak et al., 2010), occupational and educational functioning (i.e., the ability to perform work-related skills; Duarte et al., 2016), cognitive functioning (using cognitive function in real-world settings; Miskowiak et al., 2012), and physical functioning (e.g., mobility, dexterity, carrying out instrumental activities of daily living; World Health Organization, 2015). Individuals with BD often show low levels of functioning in these areas (Gitlin and Miklowitz, 2017; Sylvia et al., 2017), which affects them and their social structures (Baune and Malhi, 2015). For instance, they report severe work impairment (Boland et al., 2015; Marwaha et al., 2013), high unemployment rates (Holm et al., 2020), decreased social resources (Greenberg et al., 2014; Studart et al., 2015), and more barriers to higher education (Kruse and Oswal, 2018; Mojtabai et al., 2015). These functional impairments persist into symptomatic remission (Gitlin and Miklowitz, 2017; Léda-Rêgo et al., 2020), show great heterogeneity among individuals with BD (Solé et al., 2018), and lead to several difficulties in daily life (Chen et al., 2019). Since for many individuals with BD and their caregivers, functioning is at times more important than symptomatic outcome, much research has been dedicated to identifying its determinants. For instance, male sex, lower levels of education, lower socio-economic status, longer illness duration, a higher number of episodes, the presence of comorbid psychiatric disorders, and a greater current number of psychopharmacological medications have been found to predict functional impairment in BD (Burdick et al., 2022; Hower et al., 2019; Sanchez-Moreno et al., 2018; Wingo et al., 2010). Moreover, persistent subsyndromal symptoms, especially residual depressive symptoms, a history of psychosis (Bonnín et al., 2019; Bowie et al., 2010), and the number of admissions have been reported to have a negative impact on functioning (Sanchez-Moreno et al., 2017). Next to clinical and demographic variables, cognition has been found to be a predictor of functioning in BD in some studies (Burdick and Millett, 2021; Depp et al., 2012; Van Rheenen et al., 2019).
Cognition is usually conceptualized in terms of hierarchically ordered domains of cognitive function (i.e., the bottom domains refer to basic sensory and perceptual processes, and the top domains refer to executive function and cognitive control). The cognitive function domains encompass attention and concentration, memory, executive function, processing speed, and language/verbal skills (Harvey, 2019). In BD, a study revealed that 30–50% show impairments in cognition, predominantly in the areas of verbal memory, processing speed, executive function, attention, working memory, and social cognition (average illness duration: 15.61 years, average episode number: 11.28 episodes; Lima et al., 2019). Former studies reported that cognitive dysfunction is also related to demographic [e.g., age (Frías et al., 2017; Rabelo-da-Ponte et al., 2022; Mann-Wrobel et al., 2011), education (Rabelo-da-Ponte et al., 2022; Mann-Wrobel et al., 2011), sex (Martín-Parra et al., 2024)] and clinical outcomes [e.g., symptomatology; (Frías et al., 2017), number of hospitalizations (Rabelo-da-Ponte et al., 2022), illness duration (Mann-Wrobel et al., 2011), illness onset (Bortolato et al., 2015)]. Moreover, cognitively impaired individuals with BD were shown to display more functional disabilities than those without cognitive impairment (Jensen et al., 2016). The strength of the association between cognitive abilities and psychosocial functioning in BD was previously reported to be similar to that seen in schizophrenia (Depp et al., 2012). This may exacerbate the challenges that individuals with BD face in daily life, leading to greater difficulties in managing personal, social, and occupational responsibilities.
A paucity of studies have reported on the association between cognition and functioning in BD (e.g., Anaya et al., 2015; Martínez-Arán et al., 2004; Miskowiak et al., 2023; Chen et al., 2021), with most of them finding that specific cognitive abilities are predictors of functional outcomes (Bonnín et al., 2010; Lee et al., 2015; Lomastro et al., 2020; López-Villarreal et al., 2020; Ponsoni et al., 2020). While some of the studies identified executive function, verbal learning/memory (Martínez-Arán et al., 2004; Bonnín et al., 2010), verbal fluency, and working memory (Chen et al., 2021) as the predictors with the most impact on psychosocial functioning, others found that sustained attention and psychomotor speed are also important within this context (Lee et al., 2015; López-Villarreal et al., 2020). To strengthen the knowledge on these complex associations, the current study aimed to investigate the cross-sectional association between cognitive abilities and functioning. Based on previous findings, it was hypothesized that (a) there would be a significantly positive relationship between the cognitive abilities (a) attention/psychomotor speed, (b) verbal learning/memory, and (c) executive function and psychosocial functioning. Moreover, it was hypothesized that (d) attention/psychomotor speed, (e) verbal learning/memory, and (f) executive function can predict psychosocial functioning, independently of age, sex, and educational level.
2 Materials and methods
2.1 Sample
Participants were recruited and examined at the research unit and outpatient center for BD at the Medical University Graz, Clinical Department of Psychiatry and Psychotherapeutic Medicine. The current study was part of the ongoing longitudinal BIPFAT/BIPLONG study, which aims to investigate the actual and lifetime psychiatric history of BD and its association with lifestyle, metabolism, brain function, and cognition. To determine these aspects, psychiatric symptomatology, psychiatric and somatic comorbidities, anthropometric measurements, fasting blood samples, neuropsychological tests, electroencephalogram measurements, magnetic resonance imaging of the brain, and psychological questionnaires are administered semi-annually. For more information about the study design and preliminary longitudinal results see previously published reports (e.g., Dalkner et al., 2021; Fellendorf et al., 2021; Liebing et al., 2023; Queissner et al., 2024; Reininghaus et al., 2022).
In total, data from 349 individuals with a BD diagnosis were collected since the start of the study in 2012. The inclusion criteria were a diagnosis of BD, which was verified by the structured clinical interview for DSM-IV (Wittchen et al., 1997), age between 18 and 70 years, and a premorbid intelligence quotient of ≥80. Moreover, individuals were required to be euthymic at the time of testing, which was examined using the Hamilton Rating Scale for Depression (HAMD) (Hamilton, 1960) and the Young Mania Rating Scale (YMRS) (Young et al., 1978). In the current study, a HAMD score ≤ 11 and a YMRS score ≤ 8 at the time of the examination denoted a state of euthymia. Individuals were excluded if their medical history showed a diagnosis of dementia, or severe medical or neurological comorbidities such as active cancer, chronic obstructive lung disease, rheumatoid arthritis, systemic lupus erythematosus, Parkinson’s disease, Huntington’s disease, and multiple sclerosis. Overall, one individual was excluded due to a premorbid intelligence quotient of ≤80, and 95 individuals were excluded because they were not euthymic at the measurement time. Data of 43 individuals were excluded due to missing GAF scores. Thus, the final sample size comprised N = 210 individuals [101 female, 109 male; M(age) = 44.47; SD(age) = 14.25]. A sensitivity power analysis for F-tests (linear multiple regression analyses) using G*Power (version 3.1) (Faul et al., 2007) indicated that, when considering this sample size, an α of 5%, and a power of 80%, the analyses were able to detect a minimum effect size of f2 = 0.05. All participants provided written informed consent before participating in the study. The study was approved by the local ethics committee (Medical University of Graz, Austria; EC-number: 25–335 ex 11/12) and conducted in accordance with the Declaration of Helsinki.
2.2 Materials
2.2.1 Cognitive domains
Attention/psychomotor speed. To calculate the cognitive composite score of attention and psychomotor speed, the Trail Making Test (TMT) (Reitan, 1958) was administered. Participants were asked to connect digits in an ascending order [part A of the TMT (TMT-A)]. The outcome measure of the TMT-A is the time to correctly complete the task. Moreover, the Digit Span Test [forward recall; subtest of the Wechsler Adult Intelligence Scale 4th edition (WAIS-IV) Wechsler, 2008] was administered, in which participants were asked to recall sequences of digits in the same order as previously read to them. The outcome measure of this test is the number of correctly recalled digit sequences.
Verbal learning/memory. To create the cognitive composite score of verbal learning and memory, the German version of the California Verbal Learning Test (CVLT) (Niemann et al., 2008) was used. Participants were instructed to memorize a list of 16 nouns drawn from four different semantic categories. This list was read to them five times in a fixed order (list A) and they were asked to recall as many words as possible in any order after each repetition (recall trials 1–5). Subsequently, a list of distractor words (list B) was presented, followed by free recall of list B. Hereafter, free and cued recalls of list A were tested immediately (short-delay free recall, short-cued recall), and again after 20 min (long-delay free recall, long-delay cued recall). Within the cued recalls, participants were prompted with the semantic word category. Finally, they were presented with a recognition task consisting of 44 words from either list A or other distractor lists. Participants were asked to indicate whether the presented word stems from list A or is a distractor word. The outcome measures of the CVLT are the numbers of correctly recalled words.
Executive function. Part B of the TMT (TMT-B) (Reitan, 1958) was used to measure the cognitive domain of executive function. Participants were asked to connect digits and letters in an ascending order. The outcome measure for the TMT-B was the time to correctly complete the task. Moreover, the difference between TMT-B and TMT-A was calculated to assess task-switching ability, which is part of the executive function. Further, the Digit Span Test (backward recall; Wechsler, 2008) was administered, in which participants were asked to recall number sequences in the reverse order, as previously read to them. The outcome measure for the Digit Span Test is the sum of correctly recalled digits. Moreover, the Digit Symbol Substitution Test [subtest of the Wechsler Adult Intelligence Scale 4th edition (WAIS-IV); Wechsler, 2008] was administered, which requires matching symbols to numbers according to a key located on top of the page. Participants were asked to copy the symbols into spaces below a row of numbers. The outcome measure for this test is the number of correctly copied symbols within the allowed time of 120 s.
2.2.2 Clinical parameters
Global Assessment of Functioning (GAF) (American Psychiatric Association, 2002). The GAF is a summary score, which measures overall psychosocial impairment caused by mental disorders. The score was assigned by medical professionals or clinical psychologists based on the information gathered during the collection of anamnestic data and the observation of the participant’s behavior during the testing session. GAF scores range from 0 to 100, with higher scores indicating better functioning.
2.3 Procedure
Participants were recruited via the outpatient center of the Clinical Division of Psychiatry and Psychotherapeutic Medicine, Medical University of Graz, and were invited semi-annually for the testing sessions. However, only data of the first measurement time were used for this study. First, anthropometric and fasting biochemical measurements, which were performed for the superordinate research project, anamnestic data, and psychiatric history (e.g., BD type I/type II, illness duration, history of suicidal behavior, history of psychosis, number of affective episodes, age of onset, mood stabilizing medication, psychiatric and somatic comorbidities) were assessed by trained research staff. Subsequently, the neuropsychological test battery was administered, followed by questionnaires regarding personality and lifestyle, which were not part of the current analysis. Finally, functioning was evaluated by medical professionals or clinical psychologists using the GAF, among other psychiatric external assessments (e.g., YMRS, HAMD). Overall, the entire testing session took 2–3 h.
2.4 Statistical analysis
Data were analyzed using IBM SPSS Statistics (version 29).1 To create cognitive composite scores for attention/psychomotor speed, verbal learning/memory, and executive function, the approach outlined by Hasan et al. (2016) was applied: Initially, measures of reaction time (in which higher scores indicate inferior performance) were multiplied by −1 to ensure that higher scores are indicative of enhanced performance across all variables. Secondly, all variables were transformed to standardized z-scores, which were summed up for each of the three domains according to their allocation to a specific cognitive domain (see Table 1). However, most of these scores exhibited non-normal distributions, which led to a renewed z-transformation of the scores using Rankit’s formula, followed by a summation according to the domain allocation.
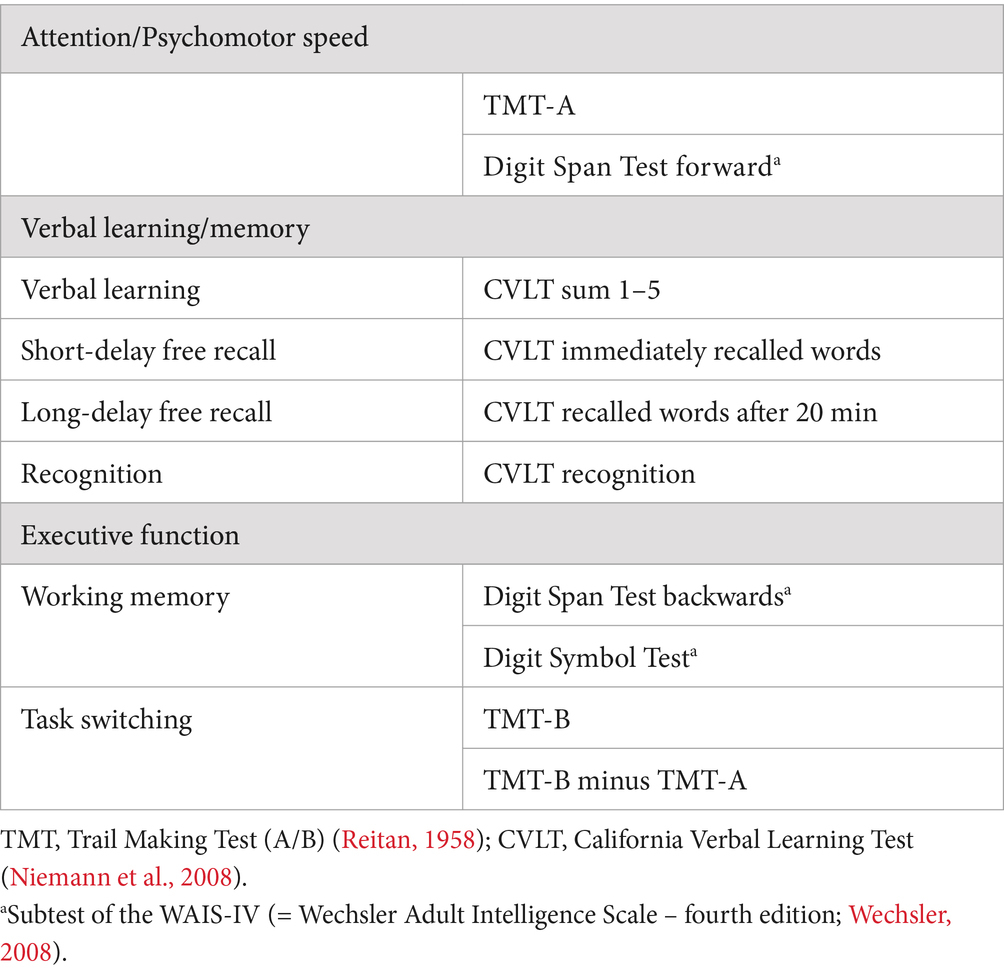
Table 1. Allocation of the neuropsychological tests scores to the cognitive domains.
To test our hypotheses, three hierarchical linear regression analyses were conducted, using the GAF score as dependent variable and each of the cognitive composite scores as independent variables. Moreover, to determine possible influencing factors, Bonferroni-corrected bivariate Pearson- and Spearman correlation analyses between the cognitive composite scores, the GAF score, and the variables age, sex, and education were conducted beforehand. If any of these variables showed a significant relationship with either the cognitive composite score or the GAF score, they were considered as covariates and entered into the hierarchical regression analysis in a first step. Moreover, for the respective regression analysis, missing values in the cognitive composite scores were temporarily excluded. Assumptions to conduct all analyses were fulfilled, unless otherwise noted. Data, data codes, and a list of variables can be accessed via https://doi.org/10.17605/OSF.IO/ZDM45.
3 Results
3.1 Descriptive statistics
Table 2 provides a detailed description of the study sample and its psychometric properties.
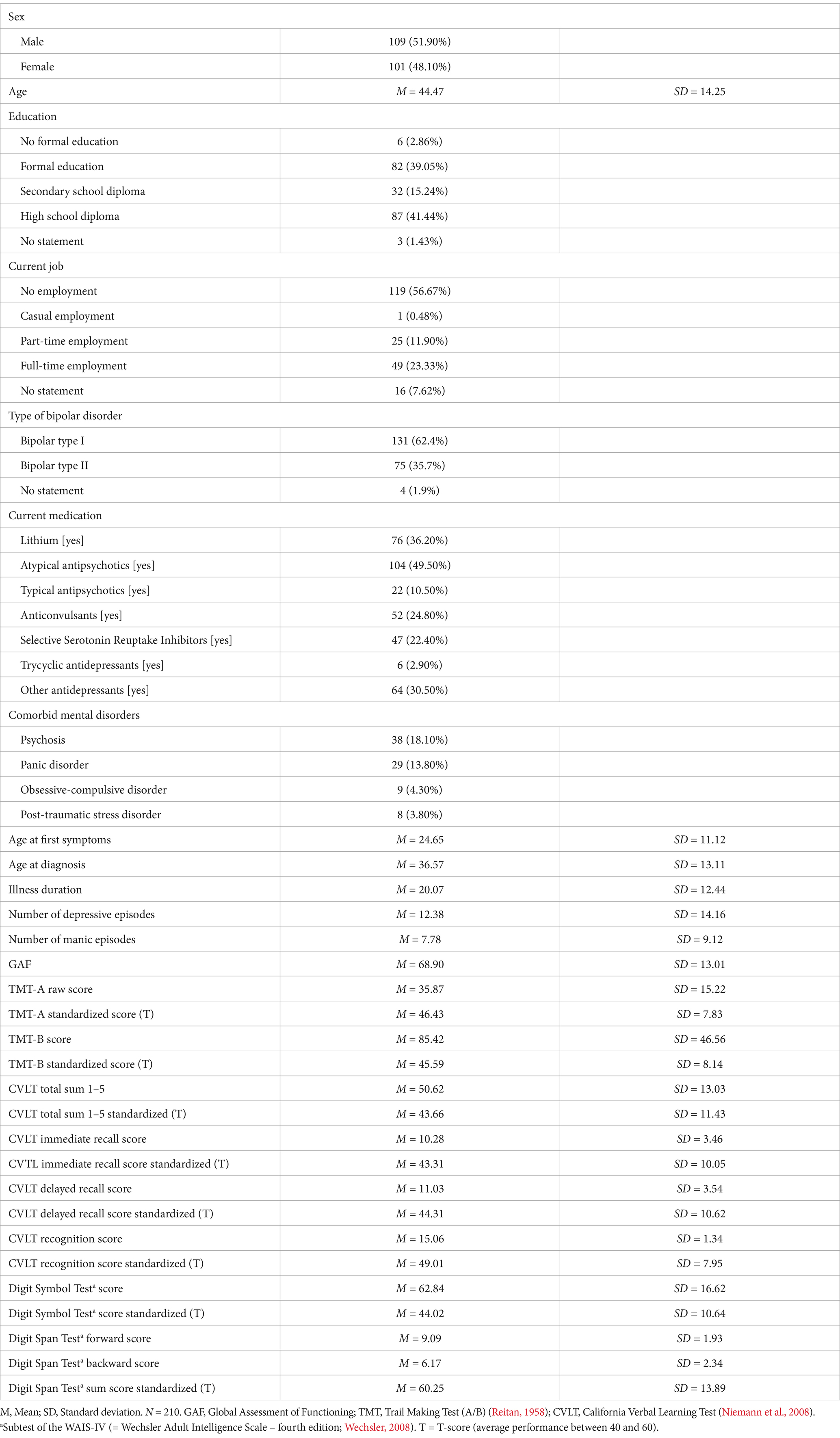
Table 2. Descriptive analysis of the sample and psychometric properties.
3.2 Pearson- and Spearman correlation analyses
The correlation analyses indicated that the GAF score was significantly correlated with all cognitive composite scores, however, after applying the Bonferroni correction, only the correlations of attention/psychomotor speed and verbal learning/memory remained significant. Moreover, age was significantly negatively correlated, and education was significantly positively correlated with all cognitive composite scores, indicating that higher age and lower educational level are associated with lower cognitive abilities in all domains. Finally, sex was significantly correlated with verbal learning/memory, indicating that women exhibited greater cognitive abilities within this domain than men (see Table 3 for exact values).
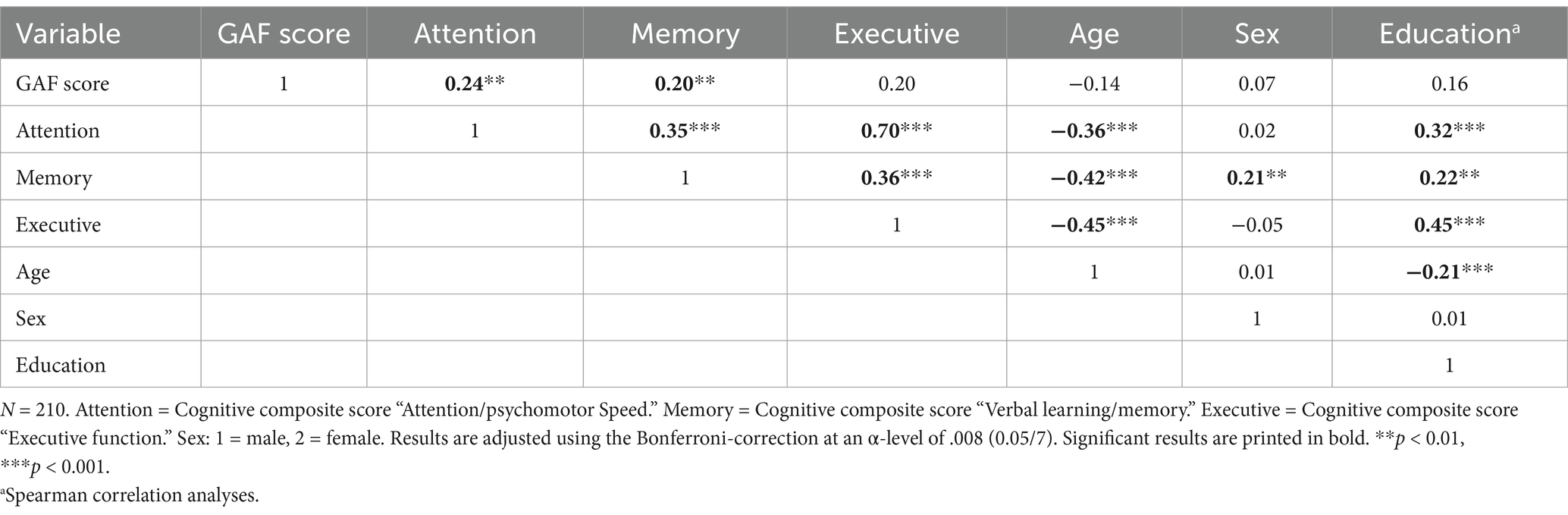
Table 3. Pearson- and Spearman correlation analyses of the cognitive composite scores, Global Assessment of Functioning (GAF) score, as well as age, sex, and education.
3.3 Hierarchical regression analyses
The hierarchical regression analysis calculating the prediction of the GAF score by attention/psychomotor speed and the control variables age and education showed that all predictors were able to collectively explain 8.7% of the variance in the GAF score. The control variables entered in a first step accounted for 6.1% of the variance, with only education contributing significant unique variance to the prediction of the GAF score. The inclusion of attention/psychomotor speed in a second step explained additional 2.6% of the variance, however, this finding did not reach statistical significance, and thus this cognitive composite score does not meaningfully contribute to functioning as measured by the GAF. Hence, only education was able to explain significant variance in functioning within this model. Table 4 shows the results of the analysis.
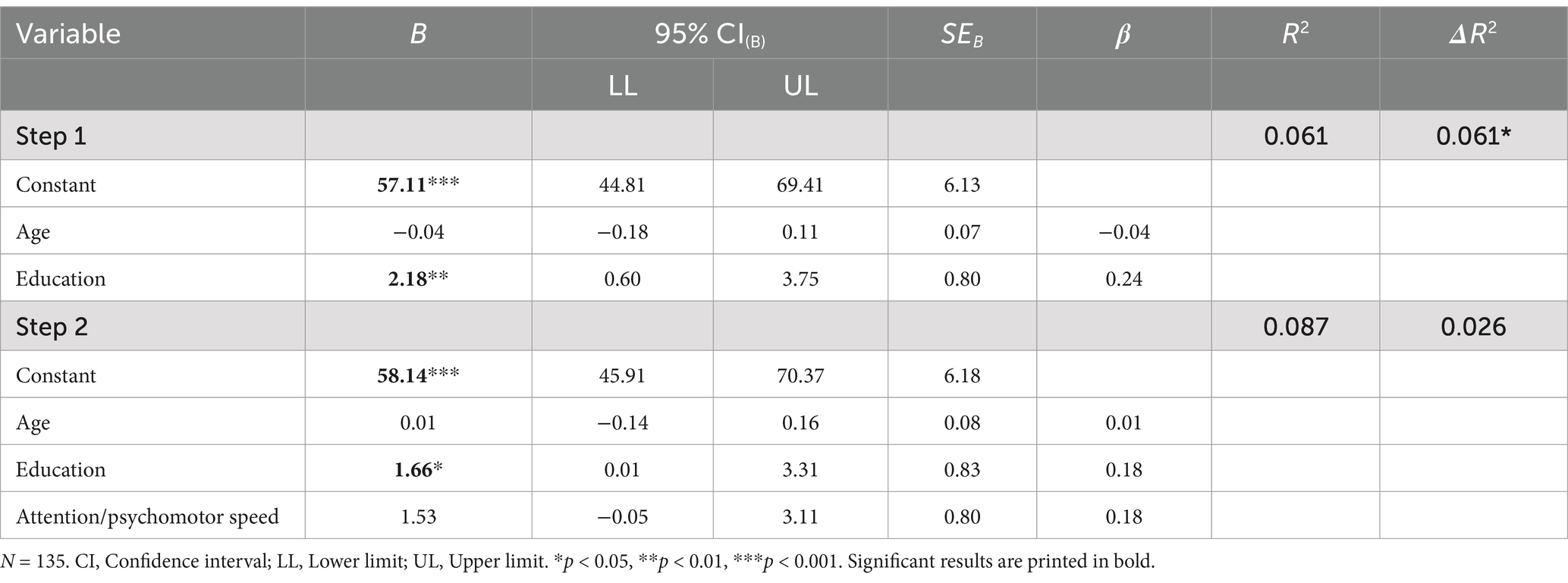
Table 4. Hierarchical regression results for attention/psychomotor speed predicting psychosocial functioning as measured by the Global Assessment of Functioning (GAF).
Moreover, the hierarchical regression analysis administered to predict the GAF score from verbal learning/memory and the control variables age, education, and sex, revealed that the predictors explained 6.3% of the total variance in the GAF score. Specifically, the control variables entered in the first step accounted for 5.1% of the variance, but only the variable age made a significantly negative unique contribution to the GAF score, indicating that higher age predicts lower psychosocial functioning. Further, the inclusion of verbal learning/memory in a second step explained additional 1.2% of the incremental variance, but this result did not reach statistical significance. This indicates that verbal learning/memory does not account for variance in functioning beyond the considered control variables (see Table 5 for exact values).
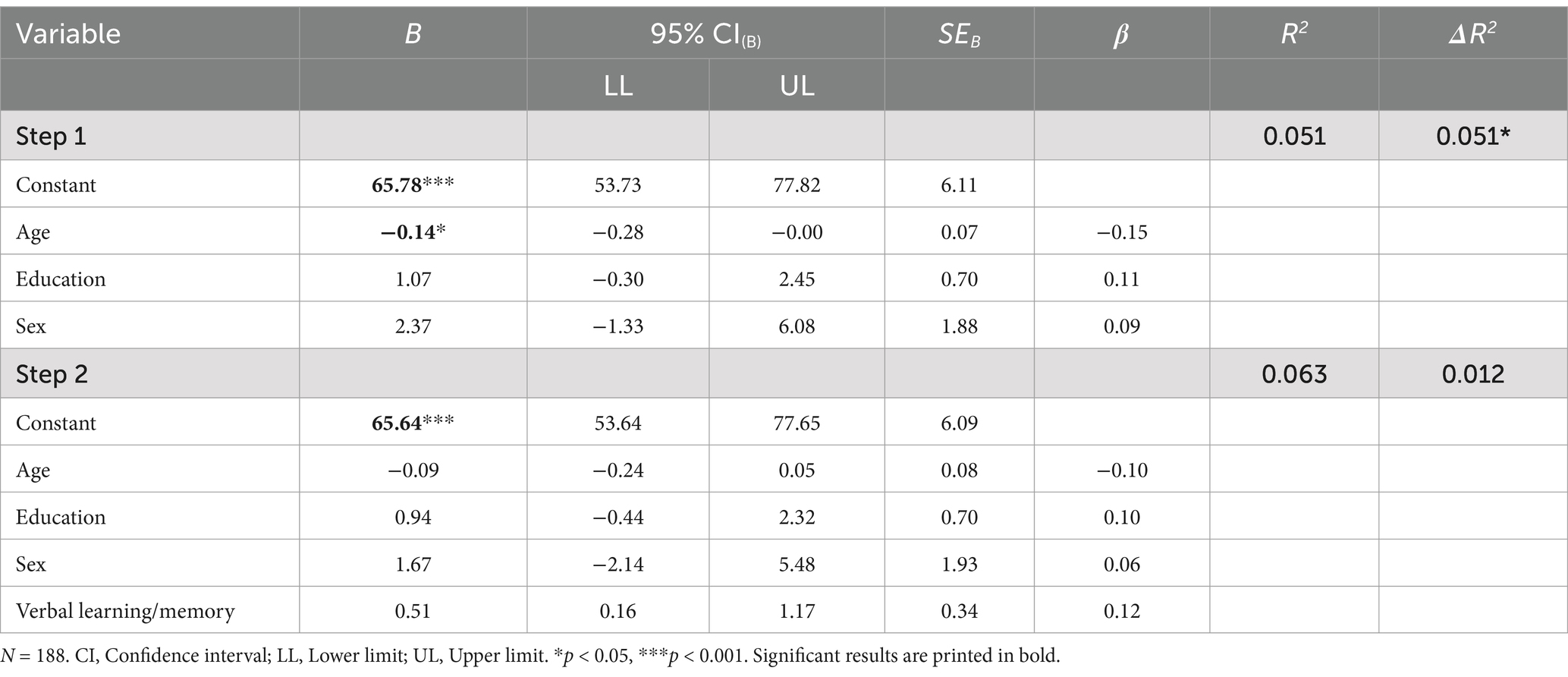
Table 5. Hierarchical regression results for verbal learning/memory predicting psychosocial functioning as measured by the Global Assessment of Functioning (GAF).
Finally, the hierarchical regression analysis, which was conducted to predict the GAF score from executive function and the control variables age and education, revealed that the predictors collectively explained 6% of the variance in the GAF score. In particular, the control variables entered in a first step accounted for 4.7% of the total variance, however, only education made a significantly positive unique contribution to the GAF score. This indicates that higher education predicts better psychosocial functioning as measured by the GAF score. The consideration of executive function in a second step accounted for another 1.3%, however, this finding lacks statistical significance. Thus, executive function is not able to explain significant variance in psychosocial functioning beyond the considered control variables. Table 6 shows all results of this analysis.
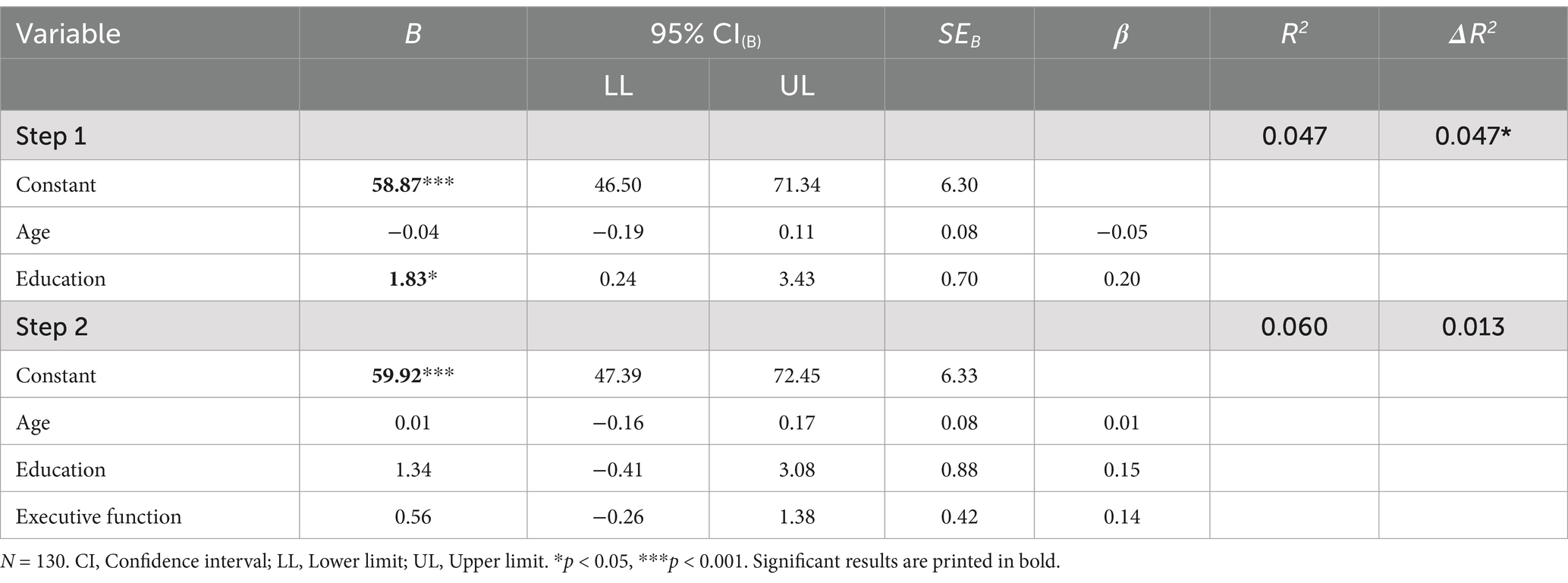
Table 6. Hierarchical regression results for executive function predicting psychosocial functioning as measured by the Global Assessment of Functioning (GAF).
4 Discussion
The current study investigated the association and prediction of psychosocial functioning by the cognitive domains attention/psychomotor speed, verbal learning/memory, and executive function. Our cross-sectional analysis showed a significantly positive association between attention/psychomotor speed, verbal learning/memory and functioning, indicating that greater abilities within these domains are related to better functioning. However, when considering the control variables age, sex, and education within hierarchical regression analyses, no cognitive domain was able to explain significant unique variance in functioning. This reflects that cognitive abilities are not predictors of psychosocial functioning beyond age, sex, and education in individuals with BD. Instead, other factors are more likely to explain psychosocial functioning of patients with psychiatric disorders, such as emotion regulation, social support, and illness-related variables. In addition, the self-assessment of cognitive deficits has also recently been linked to functioning and has been identified as an independent predictor of functional outcomes in schizophrenia (Silberstein and Harvey, 2019).
However, our hypotheses, which state that there is a significantly positive relationship between the cognitive domains (a) attention/psychomotor speed, (b) verbal learning/memory, (c) executive function and psychosocial functioning, can partly be confirmed by our results. Our finding of a positive association between attention/psychomotor speed, verbal learning/memory, and functioning is in line with previous studies, which found that impaired abilities in the domains verbal learning/memory (Bonnín et al., 2010) and attention (Jaeger et al., 2007), specifically sustained attention, were related to reduced functional disability (Lee et al., 2015). Moreover, another study found that lower performance in verbal memory, working memory, verbal fluency, and processing speed was associated with decreased functioning in BD (Sanchez-Moreno et al., 2018). Other studies reported that verbal memory represents a core deficit in BD and is one of the best predictors of functioning (Martínez-Arán et al., 2004), specifically occupational functioning (Burdick et al., 2010). The finding that none of the cognitive domains predicted functioning beyond the control variables age, sex, and education contradicts our hypotheses (d-f) and the existing literature. Most previous studies point toward a neurocognitive impairment as a main predictor of psychosocial functioning (for a review, see Keramatian et al., 2021). It should be noted that psychosocial functioning is a complex construct influenced by various non-cognitive factors, such as emotional regulation (Van Rheenen and Rossell, 2014), social support (Wang et al., 2018), illness severity (Goldstein et al., 2009; Schaub et al., 2011), and psychosocial treatment (Reinares et al., 2014). It is possible that these factors play a more dominant role in determining functional outcomes (Depp et al., 2012), thereby diminishing the predictive value of cognitive abilities in our regression analyses.
Another explanation for the non-significant regression analyses results might be the use of a single global functioning scale (the GAF as an external rating) and the creation of overarching cognitive composite scores. Studies that found an effect of cognitive abilities on functional outcomes often used measurements, which differentiated in more detailed aspects of both functioning (e.g., functioning in employment, relationship, and independent living, such as the Functioning Assessment Short Test (Rosa et al., 2007) or Work and Social Adjustment Scale (Mundt et al., 2002)) and/or cognitive domains (e.g., psychomotor speed, sustained attention; Lee et al., 2015; Flaaten et al., 2024). Possibly, the lack of differentiation into the sub-facets of both functioning and cognition might have led to a non-significant association. In addition, the participants in our sample reached test scores within 1.5 standard deviations below and above the normative performance of each test (T-scores of all cognitive tests ranged between M = 43.31–60.25 and SD = 7.83–13.89). This indicates that, on average, our sample showed unimpaired cognitive performance, which might have contributed to the non-significant association between cognitive abilities and psychosocial functioning. We also included individuals from our outpatient clinic, who might have a greater level of functioning, as reflected by a mean GAF score of 68.90 (SD = 13.01). Investigating our hypotheses in a sample with a greater range of functioning might have led to different results. Moreover, we only used data from individuals, who met the criteria for current euthymia. Other studies, which found that cognition predicts functioning in BD, analyzed data of individuals in a current affective episode (e.g., Platania et al., 2023; Torres et al., 2011; Karantonis et al., 2020), which might have led to different study outcomes. One study, which investigated the effect of clinical and cognitive variables on functioning at two measurement times in a five-year interval, reported that verbal memory at baseline and change in sustained attention during follow-up explained only 6–10%, but clinical variables (e.g., number of hospitalizations) explained up to 30% of the variance in psychosocial functioning (López-Villarreal et al., 2020). This strengthens again the assumption that other variables might exert a greater influence on functioning than cognition, such as clinical course, medication, life events, or coping styles (Fletcher et al., 2014; Sato et al., 2018; Miskowiak et al., 2023). These findings are in line with the results of the current study, which depict that demographic variables such as age and education play a more important role in explaining variance in functioning than cognitive abilities.
4.1 Limitations and implications
Our results should be interpreted with caution due to the following limitations. First, a major limitation is the sole use of the GAF score as representative of functioning. Using a single score of functioning might not adequately depict the distinct functioning aspects, which might otherwise be associated with cognition. Moreover, the GAF score does not address age- or sex-specific functional issues and was reported to be influenced by factors other than functional impairment (e.g., symptom severity; Bacon et al., 2002; Carrión et al., 2019). Future research should thus use additional measures of functioning, which differentiate between various aspects of functioning [e.g., Specific Level of Functioning scale (SLOF) (Schneider and Struening, 1983); UCSD (University of California, San Diego) performance-based skills assessment battery (UPSA) (Patterson et al., 2001)], and measure functioning independently of sex, age, and psychiatric symptoms (e.g., Global Functioning: Social and Role Scale; Cornblatt et al., 2007). Moreover, informant-rated or self-report measurement tools should be additionally used to assess cognitive functioning, such as the Everyday Cognition Scale (ECog) (Farias et al., 2008) or the Cognitive Functioning Self-Assessment Scale (CFSS) (Annunziata et al., 2012), since they might have an effect on the link between objective cognitive abilities and functioning. Secondly, the lack of analysis of control group data prevents a comparison between individuals with BD and mentally healthy controls. Third, the cross-sectional nature of the study prevents from drawing conclusions about causality. Finally, the results can only be interpreted for individuals with BD during euthymia, which limits the generalizability of the results.
Despite these caveats, our findings are relevant to both research and clinical contexts. The results reflect that functioning, cognition, and BD are multifaceted constructs, which need to be investigated under the consideration of several different determinants. Since functioning remains an important concept for individuals with BD, their caregivers, and treating mental health professionals, future research should continue to investigate this matter. When more data will be available, we will also re-analyze the long-term relationship between cognitive ability and level of functioning over a longer time interval in the BIPLONG cohort. Additionally, we have initiated the process of having our patients with BD assess their own cognitive abilities, as introspective accuracy has been established as an independent predictor of functioning in schizophrenia (Silberstein and Harvey, 2019). This approach may provide valuable insights into how self-perceptions of cognitive deficits correlate with actual functional outcomes in individuals with BD.
5 Conclusion
This study investigated the relationship between cognitive domains and psychosocial functioning in individuals with BD, revealing a positive association between attention/psychomotor speed, verbal learning/memory, and functioning. However, when controlling for age, sex, and education, these cognitive domains did not significantly predict functioning, which highlights the predominant role of demographic factors in this model. These factors are known to have a substantial impact on both cognitive performance and functional outcomes, potentially reducing the unique predictive power of cognitive domains when considered together, which needs to be considered in further studies in this area. To conclude, while our findings support prior research, which demonstrates an association between cognitive abilities and functioning, they also challenge existing literature that refers to cognition as a main predictor of functioning. Future research should incorporate more detailed functional and cognitive assessments and consider clinical variables to clarify the complex mechanisms between cognition and psychosocial functioning. Understanding these relationships is essential for developing targeted interventions that facilitate daily life in individuals with BD.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: Open Science Framework repository (https://doi.org/10.17605/OSF.IO/ZDM45).
Ethics statement
The studies involving humans were approved by ethics committee of the Medical University of Graz. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
ES: Conceptualization, Data curation, Formal analysis, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. ND: Conceptualization, Data curation, Formal analysis, Investigation, Project administration, Resources, Software, Supervision, Validation, Writing – review & editing. TS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Validation, Writing – review & editing. SB: Conceptualization, Investigation, Writing – review & editing. JI: Data curation, Writing – review & editing. FF: Conceptualization, Investigation, Writing – review & editing. AF: Data curation, Writing – review & editing. EF: Writing – review & editing. AH: Data curation, Writing – review & editing. JG: Writing – review & editing. AM: Conceptualization, Investigation, Writing – review & editing. ML: Conceptualization, Investigation, Writing – review & editing. AP: Writing – review & editing. MP: Conceptualization, Investigation, Writing – review & editing. RQ: Conceptualization, Investigation, Writing – review & editing. FS: Conceptualization, Investigation, Writing – review & editing. SS: Conceptualization, Investigation, Writing – review & editing. AT-B: Conceptualization, Investigation, Writing – review & editing. ER: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to thank our participants for their participation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
Aas, I. M. (2010). Global Assessment of Functioning (GAF): properties and frontier of current knowledge. Ann. General Psychiatry 9:9. doi: 10.1186/1744-859X-9-20
American Psychiatric Association (2002). “Multiaxial assessment” in DSM-IV-TR: diagnostic and statistical manual of mental disorders. 4th ed (Washington, DC: American Psychiatric Association).
Anaya, C., Torrent, C., Caballero, F. F., Cieta, E., del Mar, B. C., Ayuso-Mateos, J. L., et al. (2015). Cognitive reserve in bipolar disorder: relation to cognition, psychosocial functioning and quality of life. Acta Psychiatr. Scand. 133, 386–398. doi: 10.1111/acps.12535
Annunziata, M., Muzzatti, B., Giovannini, L., and Lucchini, G. (2012). Cognitive functioning self- assessment scale (CFSS): preliminary psychometric data. Psychol. Health Med. 17, 207–212. doi: 10.1080/13548506.2011.596552
Anyayo, L., Ashaba, S., Kaggwa, M. M., Maling, S., and Nakimuli-Mpungu, E. (2021). Health-related quality of life among patients with bipolar disorder in rural southwestern Uganda: a hospital based cross sectional study. Health Qual. Life Outcomes 19:84. doi: 10.1186/s12955-021-01729-5
Arvilommi, P., Pallaskorpi, S., Linnaranta, O., Suominen, K., Leppämäki, S., Valtonen, H., et al. (2022). Long-term work disability due to type I and II bipolar disorder: findings of a six-year prospective study. Int. J. Bipolar. Disord. 10:19. doi: 10.1186/s40345-022-00264-6
Bacon, S. F., Collins, M. J., and Plake, E. V. (2002). Does the Global Assessment of Functioning assess functioning? J. Ment. Health Counsel. 24, 202–212.
Baune, B. T., and Malhi, G. S. (2015). A review on the impact of cognitive dysfunction on social, occupational, and general functional outcomes in bipolar disorder. Bipolar Disord. 17, 41–55. doi: 10.1111/bdi.12341
Blanco, C., Compton, W. M., Saha, T. D., Goldstein, B. I., Ruan, W. J., Huang, B., et al. (2017). Epidemiology of DSM-5 bipolar I disorder: results from the National Epidemiologic Survey on alcohol and related conditions – III. J. Psychiatr. Res. 84, 310–317. doi: 10.1016/j.jpsychires.2016.10.003
Boland, E. M., Stange, J. P., Molz Adams, A., LaBelle, D. R., Ong, M. L., Hamilton, J. L., et al. (2015). Associations between sleep disturbance, cognitive functioning and work disability in bipolar disorder. Psychiatry Res. 230, 567–574. doi: 10.1016/j.psychres.2015.09.051
Bonnín, C. M., Martínez-Arán, A., Torrent, C., Pacchiarotti, I., Rosa, A. R., Franco, C., et al. (2010). Clinical and neurocognitive predictors of functional outcome in bipolar euthymic patients: a long-term, follow-up study. J. Affect. Disord. 121, 156–160. doi: 10.1016/j.jad.2009.05.014
Bonnín, C. D. M., Reinares, M., Martínez-Arán, A., Jiménez, E., Sánchez-Moreno, J., Solé, B., et al. (2019). Improving functioning, quality of life, and well-being in patients with bipolar disorder. Int. J. Neuropsychopharmacol. 22, 467–477. doi: 10.1093/ijnp/pyz018
Bortolato, B., Miskowiak, K. W., Köhler, C. A., Vieta, E., and Carvalo, A. F. (2015). Cognitive dysfunction in bipolar disorder and schizophrenia: a systematic review of meta-analyses. Neuropsychiatr. Dis. Treat. 11, 3111–3125. doi: 10.2147/NDT.S76700
Bowie, C. R., Depp, C., McGrath, J. A., Wolyniec, P., Mausbach, B. T., Thornquist, M. H., et al. (2010). Prediction of real-world functional disability in chronic mental disorders: a comparison of schizophrenia and bipolar disorder. Am. J. Psychiatry 167, 1116–1124. doi: 10.1176/appi.ajp.2010.09101406
Burdick, K. E., Goldberg, J. F., and Harrow, M. (2010). Neurocognitive dysfunction and psychosocial outcome in patients with bipolar I disorder at 15-year follow-up. Acta Psychiatr. Scand. 122, 499–506. doi: 10.1111/j.1600-0447.2010.01590.x
Burdick, K. E., and Millett, C. E. (2021). Cognitive heterogeneity is a key predictor of differential functional outcome in patients with bipolar disorder. Eur. Neuropsychopharmacol. 53, 4–6. doi: 10.1016/j.euroneuro.2021.06.008
Burdick, K. E., Millett, C. E., Yocum, A. K., Altimus, C. M., Andreassen, O. A., Aubin, V., et al. (2022). Predictors of functional impairment in bipolar disorder: results from 13 cohorts from seven countries by the global bipolar cohort collaborative. Bipolar Disord. 24, 709–719. doi: 10.1111/bdi.13208
Carrión, R. E., Auther, A. M., McLaughlin, D., Olsen, R., Addington, J., Bearden, C. E., et al. (2019). The global functioning: social and role scales-further validation in a large sample of adolescents and Young adults at clinical high risk for psychosis. Schizophr. Bull. 45, 763–772. doi: 10.1093/schbul/sby126
Carvalho, A. F., Firth, J., and Vieta, E. (2020). Bipolar disorder. N. Engl. J. Med. 383, 58–66. doi: 10.1056/NEJMra1906193
Chen, M., Fitzgerald, H. M., Madera, J. J., and Tohen, M. (2019). Functional outcome assessment in bipolar disorder: a systematic literature review. Bipolar Disord. 21, 194–214. doi: 10.1111/bdi.12775
Chen, W. Y., Huang, M. C., Lee, Y. C., Chang, C. E., Lin, S. K., Chiu, C. C., et al. (2021). The heterogeneity of longitudinal cognitive decline in euthymic bipolar I disorder with clinical characteristics and functional outcomes. Front. Psych. 12:684813. doi: 10.3389/fpsyt.2021.684813
Chen, H., Wang, L., Li, H., Song, H., Zhang, X., and Wang, D. (2023). Altered intrinsic brain activity and cognitive impairment in euthymic, unmedicated individuals with bipolar disorder. Asian J. Psychiatry 80:103386. doi: 10.1016/j.ajp.2022.103386
Cornblatt, B. A., Auther, A. M., Niendam, T., Smith, C. W., Zinberg, J., and Bearden, C. E. (2007). Preliminary findings for two new measures of social and role functioning in the prodromal phase of schizophrenia. Schizophr. Bull. 33, 688–702. doi: 10.1093/schbul/sbm029
Dalkner, N., Bengesser, S., Birner, A., Rieger, A., Seebauer, J., Platzer, M., et al. (2021). Body mass index predicts decline in executive function in bipolar disorder: preliminary data of a 12-month follow-up study. Neuropsychobiology 80, 1–11. doi: 10.1159/000505784
Depp, C. A., Mausbach, B. T., Harell, A. L., Savla, G. N., Bowie, C. R., Harvey, P. D., et al. (2012). Meta-analysis of the association between cognitive abilities and everyday functioning in bipolar disorder. Bipolar Disord. 14, 217–226. doi: 10.1111/j.1399-5618.2012.01011.x
Dilling, H., and Freyberger, H. J. (2019). Taschenführer zur ICD-10-Klassifikation psychischer Störungen; nach dem Pocket Guide von J. E. Cooper [Pocket guide for the ICD-10 classification of psychiatric disorders]. Göttingen: Hogrefe.
Duarte, W., Becerra, R., and Cruise, K. (2016). The relationship between neurocognitive functioning and occupational functioning in bipolar disorder: a literature review. Eur. J. Psychol. 12, 659–678. doi: 10.5964/ejop.v12i4.909
Farias, S. T., Mungas, D., Reed, B. R., Cahn-Weiner, D., Jagust, W., Baynes, K., et al. (2008). The measurement of everyday cognition (ECog): scale development and psychometric properties. Neuropsychology 22, 531–544. doi: 10.1037/0894-4105.22.4.531
Faul, F., Erdfelder, E., Lang, A. G., and Buchner, A. (2007). G*power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191. doi: 10.3758/BF03193146
Fellendorf, F. T., Gostner, J. M., Lenger, M., Platzer, M., Birner, A., Maget, A., et al. (2021). Tryptophan metabolism in bipolar disorder in a longitudinal setting. Antioxidants 10:1795. doi: 10.3390/antiox10111795
Flaaten, C. B., Melle, I., Bjella, T., Engen, M. J., Åsbø, G., Wold, K. F., et al. (2024). Long-term course of cognitive functioning in bipolar disorder: a ten-year follow-up study. Bipolar Disord. 26, 136–147. doi: 10.1111/bdi.13364
Fletcher, K., Parker, G., and Manicavasagar, V. (2014). The role of psychological factors in bipolar disorder: prospective relationships between cognitive style, coping style and symptom expression. Acta Neuropsychiatr 26, 81–95. doi: 10.1017/neu.2013.41
Frías, A., Dickstein, D. P., Merranko, J., Gill, M. K., Goldstein, T. R., Goldstein, B. I., et al. (2017). Longitudinal cognitive trajectories and associated clinical variables in youth with bipolar disorder. Bipolar Disord. 19, 273–284. doi: 10.1111/bdi.12510
Gitlin, M. J., and Miklowitz, D. J. (2017). The difficult lives of individuals with bipolar disorder: a review of functional outcomes and their implications for treatment. J. Affect. Disord. 209, 147–154. doi: 10.1016/j.jad.2016.11.021
Goldstein, T. R., Birmaher, B., Axelson, D., Goldstein, B. I., Gill, M. K., Esposito-Smythers, C., et al. (2009). Psychosocial functioning among bipolar youth. J. Affect. Disord. 114, 174–183. doi: 10.1016/j.jad.2008.07.001
Greenberg, S., Rosenblum, K. L., McInnis, M. G., and Muzik, M. (2014). The role of social relationships in bipolar disorder: a review. Psychiatry Res. 219, 248–254. doi: 10.1016/j.psychres.2014.05.047
Hamilton, M. (1960). A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 23, 56–62. doi: 10.1136/jnnp.23.1.56
Harvey, P. D. (2019). Domains of cognition and their assessment. Dialog. Clin. Neurosci. 21, 227–237. doi: 10.31887/DCNS.2019.21.3/pharvey
Hasan, A., Guse, B., Cordes, J., Wölwer, W., Winterer, G., Gaebel, W., et al. (2016). Cognitive effects of high-frequency rTMS in schizophrenia patients with predominant negative symptoms: results from a multicenter randomized sham-controlled trial. Schizophr. Bull. 42, 608–618. doi: 10.1093/schbul/sbv142
Holm, M., Taipale, H., Tanskanen, A., Tiihonen, J., and Mitterdorfer-Rutz, E. (2020). Employment among people with schizophrenia or bipolar disorder: a population-based study using nationwide registers. Acta Psychiatr. Scand. 143, 61–71. doi: 10.1111/acps.13254
Hower, H., Lee, E. J., Jones, R. N., Birmaher, B., Strober, M. A., Goldstein, B. I., et al. (2019). Predictors of longitudinal psychosocial functioning in bipolar youth transitioning to adults. J. Affect. Disord. 246, 578–585. doi: 10.1016/j.jad.2018.12.108
Jaeger, J., Berns, S., Loftus, S., Gonzalez, C., and Czobor, P. (2007). Neurocognitive test performance predicts functional recovery from acute exacerbation leading to hospitalization in bipolar disorder. Bipolar Disord. 9, 93–102. doi: 10.1111/j.1399-5618.2007.00427.x
Jensen, J. H., Knorr, U., Vinberg, M., Kessing, L. V., and Miskowiak, K. W. (2016). Discrete neurocognitive subgroups in fully or partially remitted bipolar disorder: associations with functional abilities. J. Affect. Disord. 205, 378–386. doi: 10.1016/j.jad.2016.08.018
Karantonis, J. A., Rossell, S. L., Carruthers, S. P., Sumner, P., Hughes, M., Green, M. J., et al. (2020). Cognitive validation of cross-diagnostic cognitive subgroups on the schizophrenia-bipolar spectrum. J. Affect. Disord. 266, 710–721. doi: 10.1016/j.jad.2020.01.123
Kato, T., Baba, K., Guo, W., Chen, Y., and Nosaka, T. (2021). Impact of bipolar disorder on health-related quality of life and work productivity: estimates from the national health and wellness survey in Japan. J. Affect. Disord. 295, 203–214. doi: 10.1016/j.jad.2021.07.104
Keramatian, K., Torres, I. J., and Yatham, L. N. (2021). Neurocognitive functioning in bipolar disorder: what we know and what we don’t. Dial. Clin. Neurosci. 23, 29–38. doi: 10.1080/19585969.2022.2042164
Kruse, A. K., and Oswal, S. K. (2018). Barriers to higher education for students with bipolar disorder: a critical social model perspective. Soc. Inclus. 6, 194–206. doi: 10.17645/SI.V6I4.1682
Léda-Rêgo, G., Bezerra Filho, S., and Scippa, Â. M. (2020). Functioning in euthymic patients with bipolar disorder: a systematic review and meta-analysis using the functioning assessment short test. Bipolar Disord. 22, 569–581. doi: 10.1111/bdi.12904
Lee, R. S. C., Hermens, D. F., Naismith, S. L., Lagopoulos, J., Jones, A., Scott, J., et al. (2015). Neuropsychological and functional outcomes in recent-onset major depression, bipolar disorder and schizophrenia-spectrum disorders: a longitudinal cohort study. Transl. Psychiatry 5:e555. doi: 10.1038/tp.2015.50
Liebing, S., Dalkner, N., Ischebeck, A., Bengesser, S. A., Birner, A., Fellendorf, F. T., et al. (2023). A one-year view on the association of metabolic syndrome and cognitive function in bipolar disorder - preliminary data. J. Affect. Disord. 323, 251–256. doi: 10.1016/j.jad.2022.11.067
Lima, F. M., Rabelo-da-Ponte, F. D., Bücker, J., Czepielewski, L. S., Hasse-Sousa, M., Telesca, R., et al. (2019). Identifying cognitive subgroups in bipolar disorder: a cluster analysis. J. Affect. Disord. 246, 252–261. doi: 10.1016/j.jad.2018.12.044
Lomastro, M. J., Valerio, M. P., Blasco, M. B., Tagni, M. F., and Martino, D. J. (2020). Predictors of high psychosocial functioning in bipolar disorder. J. Nerv. Ment. Dis. 208, 904–907. doi: 10.1097/NMD.0000000000001224
López-Villarreal, A., Sánchez-Morla, E. M., Jiménez-López, E., Martínez-Vizcaíno, V., Aparicio, A. I., Mateo-Sotos, J., et al. (2020). Predictive factors of functional outcome in patients with bipolar I disorder: a five-year follow-up. J. Affect. Disord. 272, 249–258. doi: 10.1016/j.jad.2020.03.140
Mann-Wrobel, M. C., Carreno, J. T., and Dickinson, D. (2011). Meta-analysis of neuropsychological functioning in euthymic bipolar disorder: an update and investigation of moderator variables. Bipolar Disord. 13, 334–342. doi: 10.1111/j.1399-5618.2011.00935.x
Martínez-Arán, A., Vieta, E., Colom, F., Torrent, C., Sánchez-Moreno, J., Reinares, M., et al. (2004). Cognitive impairment in euthymic bipolar patients: implications for clinical and functional outcome. Bipolar Disord. 6, 224–232. doi: 10.1111/j.1399-5618.2004.00111.x
Martín-Parra, S., Torrent, C., Bort, R. M., Fico, G., Oliva, V., Prisco, M. D., et al. (2024). Sex differences in neurocognitive performance in older adults with bipolar disorder. Eur. Psychiatry 67:S440. doi: 10.1192/j.eurpsy.2024.912
Marwaha, S., Durrani, A., and Singh, S. (2013). Employment outcomes in people with bipolar disorder: a systematic review. Acta Psychiatr. Scand. 128, 179–193. doi: 10.1111/acps.12087
Michalak, E. E., Murray, G., and CREST, B. D. (2010). Development of the QoL.BD: a disorder-specific scale to assess quality of life in bipolar disorder. Bipolar Disord. 12, 727–740. doi: 10.1111/j.1399-5618.2010.00865.x
Miskowiak, K. W., Hansen, K. B., Mariegaard, J., and Kessing, L. V. (2023). Association between childhood trauma, cognition, and psychosocial function in a large sample of partially or fully remitted patients with bipolar disorder and healthy participants. Int. J. Bipolar. Disord. 11:31. doi: 10.1186/s40345-023-00311-w
Miskowiak, K. W., Kjaerstad, H. L., Lemvigh, C. K., Ambrosen, K. S., Thorvald, M. S., Kessing, L. V., et al. (2023). Neurocognitive subgroups among newly diagnosed patients with schizophrenia spectrum or bipolar disorders: a hierarchical cluster analysis. J. Psychiatr. Res. 163, 278–287. doi: 10.1016/j.jpsychires.2023.05.025
Miskowiak, K., Vinberg, M., Christensen, E. M., and Kessing, L. (2012). Is there a difference in subjective experience of cognitive function in patients with unipolar disorder versus bipolar disorder? Nord. J. Psychiatry 66, 389–395. doi: 10.3109/08039488.2012.658862
Mojtabai, R., Stuart, E. A., Hwang, I., Eaton, W. W., Sampson, N., and Kessler, R. C. (2015). Long-term effects of mental disorders on educational attainment in the National Comorbidity Survey ten-year follow-up. Soc. Psychiatry Psychiatr. Epidemiol. 50, 1657–1668. doi: 10.1007/s00127-015-1097-z
Mundt, J. C., Marks, I. M., Shear, M. K., and Greist, J. M. (2002). The work and social adjustment scale: a simple measure of impairment in functioning. Br. J. Psychiatry 180, 461–464. doi: 10.1192/bjp.180.5.461
Niemann, H., Sturm, W., Thöne-Otto, A. I. T., and Willmes, K. (2008). CVLT California verbal learning test. German adaptation. Frankfurt: Pearson Assessment.
Patterson, T. L., Goldman, S., McKibbin, C. L., Hughs, T., and Jeste, D. V. (2001). UCSD performance-based skills assessment: development of a new measure of everyday functioning for severely mentally ill adults. Schizophr. Bull. 27, 235–245. doi: 10.1093/oxfordjournals.schbul.a006870
Platania, G. A., Savia Guerrera, C., Sarti, P., Varrasi, S., Pirrone, C., Popovic, D., et al. (2023). Predictors of functional outcome in patients with major depression and bipolar disorder: a dynamic network approach to identify distinct patterns of interacting symptoms. PLoS One 18:e0276822. doi: 10.1371/journal.pone.0276822
Ponsoni, A., Damiani Branco, L., Cotrena, C., Milman Shansis, F., and Fonseca, R. P. (2020). The effects of cognitive reserve and depressive symptoms on cognitive performance in major depression and bipolar disorder. J. Affect. Disord. 274, 813–818. doi: 10.1016/j.jad.2020.05.143
Queissner, R., Fellendorf, F. T., Dalkner, N., Bengesser, S. A., Maget, A., Birner, A., et al. (2024). The influence of chronic inflammation on the illnesscourse of bipolar disorder: a longitudinal study. J. Psychiatr. Res. 174, 258–262. doi: 10.1016/j.jpsychires.2024.04.024
Rabelo-da-Ponte, F. D., Moreira Lima, F., Martínez-Aran, A., Kapczinski, F., Vieta, E., Ribeiro Rosa, A., et al. (2022). Data-driven cognitive phenotypes in subjects with bipolar disorder and their clinical markers of severity. Psychol. Med. 52, 1728–1735. doi: 10.1017/S0033291720003499
Reinares, M., Sánchez-Moreno, J., and Fountoulakis, K. N. (2014). Psychosocial interventions in bipolar disorder: what, for whom, and when. J. Affect. Disord. 156, 46–55. doi: 10.1016/j.jad.2013.12.017
Reininghaus, B., Dalkner, N., Schörkhuber, C., Fleischmann, E., Fellendorf, F. T., Ratzenhofer, M., et al. (2022). Nutrition, overweight, and cognition in euthymic bipolar individuals compared to healthy controls. Nutrients 14:1176. doi: 10.3390/nu14061176
Reitan, R. M. (1958). Validity of the trail making test as an Indicator of organic brain damage. Percept. Motor Skills 8, 271–276. doi: 10.2466/pms.1958.8.3.271
Rosa, A. R., Franco, C., Martínez-Ara, A., Sánchez-Moreno, J., Salamero, M., Valenti, M., et al. (2008). Functional impairment and previous suicide attempts in bipolar disorder. Acta Neuropsychiatr. 20, 300–306. doi: 10.1111/j.1601-5215.2008.00339.x
Rosa, A. R., Reinares, M., Franco, C., Comes, M., Torrent, C., Sánchez-Moreno, J., et al. (2009). Clinical predictors of functional outcome of bipolar patients in remission. Bipolar Disord. 11, 401–409. doi: 10.1111/j.1399-5618.2009.00698.x
Rosa, A. R., Sánchez-Moreno, J., Martínez-Aran, A., Salamero, M., Torrent, C., Reinares, M., et al. (2007). Validity and reliability of the functioning assessment short test (FAST) in bipolar disorder. Clin. Pract. Epidemiol. Ment. Health 3:5. doi: 10.1186/1745-0179-3-5
Sanchez-Moreno, J., Bonnin, C. M., González-Pinto, A., Amann, B. L., Solé, B., Balanzá-Martinez, V., et al. (2018). Factors associated with poor functional outcome in bipolar disorder: sociodemographic, clinical, and neurocognitive variables. Acta Psychiatr. Scand. 138, 145–154. doi: 10.1111/acps.12894
Sanchez-Moreno, J., Bonnín, C., González-Pinto, A., Amann, B. L., Solé, B., Balanzá-Martínez, V., et al. (2017). Do patients with bipolar disorder and subsyndromal symptoms benefit from functional remediation? A 12-month follow-up study. Eur. Neuropsychopharmacol. 27, 350–359. doi: 10.1016/j.euroneuro.2017.01.010
Sato, A., Hashimoto, T., Kimura, A., Niitsu, T., and Iyo, M. (2018). Psychological distress symptoms associated with life events in patients with bipolar disorder: a cross-sectional study. Front. Psych. 9:200. doi: 10.3389/fpsyt.2018.00200
Schaub, D., Brüne, M., Jaspen, E., Pajonk, F.-G., Bierhoff, H.-W., and Juckel, G. (2011). The illness and everyday living: close interplay of psychopathological syndromes and psychosocial functioning in chronic schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 261, 85–93. doi: 10.1007/s00406-010-0122-1
Schneider, L. C., and Struening, E. L. (1983). SLOF: a behavioral rating scale for assessing the mentally ill. Soc. Work Res. Abstracts. 19, 9–21. doi: 10.1093/swra/19.3.9
Silberstein, S., and Harvey, P. D. (2019). Impaired introspective accuracy in schizophrenia: an independent predictor of functional outcomes. Cogn. Neuropsychiatry 24, 28–39. doi: 10.1080/13546805.2018.1549985
Solé, B., Bonnin, M., Jiménez, E., Torrent, C., Torres, I., Varo, C., et al. (2018). Heterogeneity of functional outcomes in patients with bipolar disorder: a cluster-analytic approach. Acta Psychiatr. Scand. 137, 516–527. doi: 10.1111/acps.12871
Studart, P., Filho, S. J., Studart, A. P., Almeida, A., and Miranda-Scippa, Â. M. (2015). Social support and bipolar disorder. Rev. Psiquiatr. Clin. 42, 95–99. doi: 10.1590/0101-60830000000057
Sylvia, L. G., Montana, R. E., Deckersbach, T., Thase, M. E., Tohen, M., Reilly-Harrington, N., et al. (2017). Poor quality of life and functioning in bipolar disorder. Int. J. Bipolar Disord. 5:10. doi: 10.1186/s40345-017-0078-4
Torres, I. J., DeFreitas, C. M., DeFreitas, V. G., Bond, D. J., Kunz, M., Honer, W. G., et al. (2011). Relationship between cognitive functioning and 6-month clinical and functional outcome in patients with first manic episode bipolar I disorder. Psychol. Med. 41, 971–982. doi: 10.1017/S0033291710001613
Tsapekos, D., Strawbridge, R., Cella, M., Wykes, T., and Young, A. H. (2021). Cognitive impairment in euthymic patients with bipolar disorder: prevalence estimation and model selection for predictors of cognitive performance. J. Affect. Disord. 294, 497–504. doi: 10.1016/j.jad.2021.07.036
Van Der Voort, T. Y. G., Van Meijel, B., Hoogendoorn, A. W., Goossens, P. J. J., Beekman, A. T. F., and Kupka, R. W. (2015). Collaborative care for patients with bipolar disorder: effects on functioning and quality of life. J. Affect. Disord. 179, 14–22. doi: 10.1016/j.jad.2015.03.005
Van Rheenen, T. E., Lewandowski, K. E., Bauer, I. E., Kapczinski, F., Miskowiak, K., Burdick, K. E., et al. (2019). Current understandings of the trajectory and emerging correlates of cognitive impairment in bipolar disorder: an overview of evidence. Bipolar Disord. 22, 13–27. doi: 10.1111/bdi.12821
Van Rheenen, T. E., and Rossell, S. L. (2014). Objective and subjective psychosocial functioning in bipolar disorder: an investigation of the relative importance of neurocognition, social cognition and emotion regulation. J. Affect. Disord. 162, 134–141. doi: 10.1016/j.jad.2014.03.043
Wang, J., Mann, F., Lloyd-Evans, B., Ma, R., and Johnson, S. (2018). Associations between loneliness and perceived social support and outcomes of mental health problems: a systematic review. BMC Psychiatry 18:156. doi: 10.1186/s12888-018-1736-5
Wechsler, D. (2008). Wechsler Adult Intelligence Scale. 4th Edn. San Antonio, TX: Pearson Assessment.
Wingo, A. P., Baldessarini, R. J., Compton, M. T., and Harvey, P. D. (2010). Correlates of recovery of social functioning in types I and II bipolar disorder patients. Psychiatry Res. 177, 131–134. doi: 10.1016/j.psychres.2010.02.020
Wittchen, H. U., Zaudig, M., and Fydrich, T. (1997). Strukturiertes Klinisches interview für DSM-IV [Structured clinical interview for DSM-IV]. Göttingen, Germany: Hogrefe.
World Health Organization (2015) World report on ageing and health. World Health Organization Available online at: https://www.who.int/publications/i/item/9789241565042 (Accessed August 12, 2024).
Keywords: bipolar disorder, cognition, functioning, mood disorders, attention, memory, executive function
Citation: Schönthaler EMD, Dalkner N, Stross T, Bengesser S, Ilic J, Fellendorf F, Finner A, Fleischmann E, Häussl A, Georgi J, Maget A, Lenger M, Painold A, Platzer M, Queissner R, Schmiedhofer F, Smolle S, Tmava-Berisha A and Reininghaus EZ (2025) Cognitive abilities and psychosocial functioning in bipolar disorder: findings from the BIPLONG study. Front. Hum. Neurosci. 19:1479648. doi: 10.3389/fnhum.2025.1479648
Edited by:
J. R. C. Almeida, The University of Texas at Austin, United StatesReviewed by:
Ala Yankouskaya, Bournemouth University, United KingdomErin Logue, The University of Texas at Austin, United States
Copyright © 2025 Schönthaler, Dalkner, Stross, Bengesser, Ilic, Fellendorf, Finner, Fleischmann, Häussl, Georgi, Maget, Lenger, Painold, Platzer, Queissner, Schmiedhofer, Smolle, Tmava-Berisha and Reininghaus. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nina Dalkner, bmluYS5kYWxrbmVyQG1lZHVuaWdyYXouYXQ=