 Robert James1,2
Robert James1,2 Thomas Obadia3,4
Thomas Obadia3,4 Lyndes Wini5
Lyndes Wini5 Albino Bobogare5Sarah Charnaud1,2Shazia Ruybal-Pesántez1,2
Albino Bobogare5Sarah Charnaud1,2Shazia Ruybal-Pesántez1,2 Caitlin Bourke1,2Jacob E. Munro1,2
Caitlin Bourke1,2Jacob E. Munro1,2 Brioni R. Moore6,7,8Madhu Page-Sharp6,7
Brioni R. Moore6,7,8Madhu Page-Sharp6,7 Laurens Manning8,9Urijah Liligeto10
Laurens Manning8,9Urijah Liligeto10 Sophie G. Zaloumis11J. Kevin Baird12,13Harin Karunajeewa14†
Sophie G. Zaloumis11J. Kevin Baird12,13Harin Karunajeewa14† Ivo Mueller1,2*†
Ivo Mueller1,2*†- 1Population Health & Immunity Division, Walter + Eliza Hall Institute, Melbourne, VIC, Australia
- 2Department of Medical Biology, Faculty of Medicine & Health Sciences, University of Melbourne, Melbourne, VIC, Australia
- 3Institut Pasteur, Université Paris Cité, Bioinformatics and Biostatistics Hub, Paris, France
- 4Institut Pasteur, Université Paris Cité, G5 Infectious Disease Epidemiology and Analytics, Paris, France
- 5National Vector Borne Disease Control Program, Ministry of Health and Medical Services, Solomon Islands Government, Honiara, Solomon Islands
- 6Curtin Medical School, Curtin University, Bentley, WA, Australia
- 7Curtin Health Innovation Research Institute, Curtin University, Bentley, WA, Australia
- 8Wesfarmers Centre of Vaccines & Infectious Diseases, Telethon Kids Institute, Nedlands, WA, Australia
- 9Medical School, University of Western Australia, Nedlands, WA, Australia
- 10Solomon Islands National University (SINU), Honiara, Solomon Islands
- 11Centre for Epidemiology and Biostatistics, Melbourne School of Population and Global Health, University of Melbourne, Melbourne, VIC, Australia
- 12Oxford University Clinical Research Unit, Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia
- 13Centre for Tropical Medicine and Global Health, Nuffield Department of Medicine, University of Oxford, Oxford, United Kingdom
- 14Department of Medicine, Western Health, University of Melbourne, Melbourne, VIC, Australia
Background: Primaquine (PQ) remains the only 8-aminoquinoline endorsed by the WHO for treatment of latent Plasmodium vivax liver-stage parasites. PQ is a prodrug, with metabolism and therapeutic activity influenced by inherent human CYP2D6 polymorphisms and by poorly understood interactions with variably co-administered blood schizontocidal therapies. With widespread chloroquine resistance in P. vivax, radical cure now requires use of one of several artemisinin-based combination therapies (ACTs).
Methods: From September 2017 to February 2019, a randomised clinical trial was conducted in Guadalcanal, Solomon Islands, to evaluate the safety and efficacy of PQ (0·25 mg/kg/day × 14 days) given concurrently with standard doses of either dihydroartemisinin–piperaquine (DP) or artemether–lumefantrine (AL). A relapse control arm received AL without PQ. The 384 enrolled subjects were followed for 180 days to assess efficacy against relapse, along with CYP2D6 genotyping, methaemoglobin monitoring, and measurement of PQ absorption and metabolism.
Results: Both PQ treatment arms had significantly reduced rates of current P. vivax parasitamiea (PQ-AL: HR=0·50, CI95[0·33–0·75], PQ-DP: HR=0·34, CI95[0·22–0·52] P < 0·001) relative to no PQ. However, neither regimen provided adequate clinical efficacy (PQ-AL: 43·7%, PQ-DP: 34·1%). No significant differences were observed between PQ-AL and PQ-DP in CYP2D6 genotype-predicted activity scores, methaemoglobin levels, or concentrations of PQ and its metabolites (5,6-OQ and CPQ) on day 7 post-initation of dosing.
Conclusions: The dose of PQ administered in this study appears equally inadequate when used in combination with either DP or AL for radical cure. Higher PQ doses are required for effective radical cure in the Western Pacific, where PQ-tolerant Chesson-like strains still appear to commonly occur.
Clinical trial registration: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=372150, identifier ANZCTR 12617000329369, Universal Trial Number (UTN) U1111-1191-4968.
1 Introduction
Over 3 billion people live at risk of Plasmodium vivax malaria, with tens of millions infected each year (Battle et al., 2019). It is the dominant cause of malaria in the Asia–Indo-Pacific and the Americas (World Health Organization, 2024a). Intense P. vivax transmission occurs in much of the Western Pacific. In the Solomon Islands, total malaria cases have doubled since 2010, with over two-thirds identified as P. vivax (World Health Organization, 2024a). In addition to causing acute illness, relapses from dormant parasites in the liver (hypnozoites) contribute to the high burden of clinical P. vivax infections and to sustained asymptomatic transmission, which resists conventional vector-targeted malaria control measures (Mueller et al., 2009). The Chesson strain of P. vivax, isolated from an American soldier in the Western Pacific in 1944, is characterised by high frequency (>80%), rapid (<30 days) and multiple (>3) relapses, and tolerance to standard primaquine (PQ) treatment regimens 3.5 mg/kg total dose) regimens (White, 2011, 2021).
PQ has been combined with chloroquine (CQ) for radical cure since it was first licensed in 1952 (Baird, 2004). Today, widespread parasite resistance renders CQ ineffective across large areas of Southeast Asia and the Western Pacific (Chu et al., 2019). Artemisinin combination therapies (ACTs) have replaced CQ in most countries for clearing asexual blood stages of acute malaria (Baird, 2009). Throughout the Western Pacific, artemether–lumefantrine (AL) has emerged as the first-line treatment for uncomplicated P. vivax, combined with a PQ regimen of 0.25 mg/kg for 14 days (3.5 mg/kg) (World Health Organization, 2022). This lower-dose regimen is often practiced in settings where routine glucose-6-phosphate dehydrogenase (G6PD) testing is unavailable, because PQ can cause acute hemolytic anemia in patients with the commonly inherited G6PD deficiency. A higher total dose (7mg/kg), given over 7 or 14 days, yields superior efficacy (Taylor et al., 2019; Woon et al., 2023) Policy has since been updated to endorse a 0.5 mg/kg, 7- to 14-day PQ regimen for individuals with a negative qualitative G6PD test; otherwise, clinicians are advised to adopt a risk–benefit approach in PQ administration for anti-relapse therapy (World Health Organization, 2024b). That advice is often not followed, and there remains little evidence to suggest poor treatment efficacy of the safer lower-dose PQ regimen within the Western Pacific or of PQ at any dose when combined with AL for radical cure. In addition, recent understanding of human cytochrome P450 2D6 isotype (CYP2D6) polymorphisms impacting PQ efficacy (Marcsisin et al., 2016; Pybus et al., 2013; von Ahsen et al., 2010), along with limited data on their occurrence within the Western Pacific, highlights the complexity and importance of evidence-based optimisation and validation of radical cure strategies. To assess recommended policy and practice for radical cure of P. vivax malaria in the Solomon Islands, we conducted a clinical trial of lower-dose PQ given with either AL or dihydroartemisinin–piperaquine (DP), the second-line ACT for P. vivax.
2 Methods
2.1 Study design and site
This was an open-label, randomised, relapse-controlled, 3-arm clinical trial comparing national first-line radical cure for P. vivax malaria in the Solomon Islands using AL combined with PQ, to the same using DP combined with PQ, or against AL alone: (i) AL plus PQ (AL–PQ: PQ dose 0.25 mg/kg, 14 days); (ii) DP plus PQ (DP–PQ) at the same PQ dose; and (iii) an AL-only relapse-control arm, which is the standard of care where G6PD testing is unavailable (still common in the more remote parts of the Solomon Islands).
The study was conducted in the Tetere region of Guadalcanal Province, near Honiara, Solomon Islands. Participants were recruited from local health posts, a hospital, and the community. Ethical approvals were obtained through the Solomon Islands Health Research and Ethics Review Board (HRE 041/16) and the Walter and Eliza Hall Institute of Medical Research Human Research Ethics Committee (WEHI16-08). The study protocol was registered with the Australia and New Zealand Clinical Trials Registry (ANZCTR 12617000329369).
2.2 Sample size, randomisation, and masking
Sample size was calculated based on a prior study from Vanuatu (Karunajeewa and Mueller, personal communication, (05-2014)), where 40% P. vivax recurrence was observed 3 months after AL–PQ (Safety and Efficacy of Primaquine for P. Vivax, NCT01837992, https://clinicaltrials.gov/study/NCT01837992). The study was designed to detect superiority of Arm 2 (DP–PQ) compared to Arm 1 (AL–PQ), assuming a 25% recurrence rate in Arm 2 (i.e., equivalent to an absolute difference of 15%). A one-sided comparison of recurrence-free survival rates (1 – recurrence rate) after 6 months using the log-rank test with Type 1 error α = 5% and Type II error β = 80% yielded N1 = N2 = 123 participants in both arms. The background rate of hypnozoite relapse in the absence of PQ (Arm 3, AL), assumed to be 75% at 6 months, could be estimated with a 90% confidence level and a 10% margin of error with 51 participants. Therefore, a 2:2:1 (N1 = N2 = 2*N3) recruitment ratio was adopted, assuming 25% attrition during follow-up, raising the target sample size to N1 = N2 = 153 and N3 = 76.
Participants, healthcare workers, and investigators were aware of treatment allocation, but parasitological outcomes were assessed by laboratory staff blinded to treatment allocation. Study participants were randomly assigned using a computer-generated random-number list to one of the three study arms. Randomisation was performed in permuted blocks of five with an allocation ratio of 2:2:1. The allocation was concealed from investigators using sequentially numbered, opaque, sealed envelopes containing randomisation cards, which were opened at participant enrollment after initial screening and consent were obtained.
2.3 Participants
Screening criteria included local residency, age >12 months, weight >10 kg, and uncomplicated P. vivax or mixed P. vivax–P. falciparum malaria detected either by field microscopy or rapid diagnostic test (RDT), without G6PD deficiency as determined by CareStart™ G6PD RDT (test 1 of 3). Participants were excluded if they demonstrated any signs of severe malaria (as per WHO definitions). They were also excluded if presenting with comorbid non-malaria illness; severe malnutrition; permanent disability; recent (<14 days) PQ treatment; known or suspected pregnancy; or breastfeeding.
2.4 Enrollment procedures
A screening team member discussed the study with eligible patients and obtained informed consent in Solomon Islands Pijin. Baseline demographic and clinical characteristics were then collected. Potential participants were transferred to the central study site for repeat G6PD screening with both CareStart™ and BinaxNow™ RDTs (RDT - 2 and RDT - 3); a positive result on either test disqualified individuals from enrollment and randomisation. Despite using a triple-RDT G6PD screening approach, two subjects developed acute haemolytic anemia early in the study (Kosasih et al., 2023), after which an additional screening by quantitative ELISA (R&D DIAGNOSTICS LTD, 41, El. Venizelou str., 15561 Holargos, Greece) was implemented. All enrolled participants had fingerpricked blood samples collected and blood films prepared for detection of parasites by light microscopy (LM) and PCR. haemoglobin (Hb) and methaemoglobin (MetHb) were measured using Hemocue™ (Anglholm, Sweden) and Masimo™ Rad57 (Neuchâtel, Switzerland) portable pulse oximeters, respectively.
2.5 Treatment
AL (2/12 mg/kg) was administered orally with milk twice daily for 3 days. Morning doses were directly observed, and evening doses were self-administered with verification by empty packet. DP (2.5/20 mg/kg) was administered once daily under supervision with water. PQ (0.25 mg/kg) was administered concurrently at study 'Day-0' (enrolment), and once daily with food under the direct supervision of a research worker (days 0, 1, 2, 7, 10, and 14). A community directly observed treatment (DOT) observer documented the other daily doses.
2.6 Follow-up
Participants were actively followed up either at the study base or in their homes on days 1–3, 7, 10, 14, 21, 28, and monthly thereafter until day 168. Tympanic temperature, Giemsa-stained thick and thin blood films, and a finger-prick blood sample on slide and filter paper were collected. During the first month, adverse events were solicited, along with Hb and MetHb measurements. In the event of LM-confirmed recurrent P. vivax, participation ended and subjects were treated with AL–PQ as per national guidelines (SOLOMON ISLANDS 2018 Malaria Case Management Guideline, Solomon Islands Government, Ministry of Health and Medical Services (2018)). Those developing P. falciparum were administered AL alone and continued participation.
2.7 Laboratory assays
Malaria species-specific qPCR was performed after study completion on stored blood or filter paper dried blood spots collected at baseline and follow-up visits (from day 7 to day 168), according to standard methods described in detail in Supplementary Material S1 (Section S1.1.1, “Malaria species-specific qPCR”). CYP2D6 genotyping was performed on stored baseline blood samples as previously described and further detailed in Supplementary Material S1 (section S1.1.2 ‘CYP 2D6 genotyping’).
Concentrations of PQ, 5,6-orthoquinone-PQ (5,6-OQ: a stable derivative of a short-lived putative active quinonimine CYP2D6-derived metabolite of PQ) (Spring et al., 2019), carboxy-PQ (CPQ: an inactive metabolite of PQ), lumefantrine (L), desbutyl-lumefantrine (DBL: an active metabolite of L), and piperaquine (PPQ) were measured from whole blood collected on day 7 (prior to the day 7 PQ dose in participants enrolled in Arms 1 and 2). Assays were performed using a triple quadrupole mass spectrometer (LC-MS/MS 8060, Shimadzu, Kyoto, Japan), as detailed in Supplementary Material S1 (Section S1.1.3, “Metabolite levels by mass spectrometry”).
2.8 Data preparation and statistical analysis
Study data were collected and managed using REDCap™, a web-based interface for clinical and epidemiological data with offline capabilities (Android-based tablets). Data analyses were conducted with R v.4.2 (R Core Team, 2021). The trial’s primary pre-specified analysis was per protocol (PP) (see ANZCTR 12617000329369), restricted to participants with expert microscopy- or PCR-confirmed P. vivax infection at enrollment who underwent the full scheduled treatment course and completed acceptable follow-up until the study endpoint (P. vivax recurrence, follow-up completion at day 168, or censoring after treatment course). A secondary pre-specified modified intention-to-treat (mITT) analysis is presented in Supplementary Material S1 (Section S1.5), which included all patients randomised and receiving a full course of scheduled treatment. The mITT included participants excluded from the PP analysis due to expert microscopy or qPCR failing to confirm the presence of P. vivax parasitemia detected by RDT at enrollment. In both analyses, individuals were considered at risk until they reached the study endpoint, were lost to follow-up (i.e., did not attend two or more consecutive follow-up visits), or reached the end of 6 months of follow-up.
The primary endpoint of the study was time to P. vivax recurrence as detected by LM. This endpoint required concordant microscopic diagnosis of P. vivax by at least two trained microscopists during the designated 6-month follow-up. Where results of the two microscopists were discordant, a third microscopist (blinded to the original results) adjudicated. The secondary pre-specified outcome was any qPCR-confirmed P. vivax recurrence at any time during follow-up, determined from dried blood spots taken on day 7 and all scheduled follow-up visits from days 14–168. Supplementary Table 4 (Supplementary Material S1, Section S1.4.1) details the number of samples analysed at each time point.
Primary and secondary endpoints were analysed using survival analyses: (i) non-parametric Kaplan–Meier estimates and (ii) proportional-hazard Cox regression to estimate P. vivax recurrence hazard ratios. The time at risk for every participant was counted as the number of days between the end of allocated treatment and either first detected P. vivax infection (recurrence) or end of follow-up (censoring). Patients lost to follow-up were censored at their last visit. The proportional-hazard assumption was assessed by testing for associations between scaled Schoenfeld residuals and the transformed time from the Kaplan–Meier estimate of the survival function. Non-proportionality of the estimated hazard was considered statistically significant when the slope of the coefficients differed significantly from 0 (i.e., P < 0.05). If the proportional-hazard assumption was violated, time-stratified Cox regressions were implemented with cutoffs derived from both the study schedule and the shape of the time-dependent regression coefficients. The results of these time-stratified survival analyses are presented in Supplementary Material S1 (Section S1.4.3, “ ‘Survival analyses: time-stratified Cox-proportional hazard regressions”).
3 Results
3.1 Study population
3.1.1 Screening
Participant screening and flow are shown in the CONSORT diagram (Figure 1). Of 629 individuals screened (September 2017–February 2019), 245 were excluded, most commonly due to residence outside the study area, with only 10 (4% of all exclusions, 1.5% of all screened) excluded due to G6PD deficiency on triplicate RDT screening. Those enrolled, randomised, and commenced on allocated treatment were all included in the safety analysis (n = 384). However, 10 participants were withdrawn from the mITT efficacy population (n = 374) due to early withdrawals, mostly because of G6PD deficiency on confirmatory ELISA. A further 13 subjects were excluded from the PP analysis due to withdrawal prior to treatment completion. Another 45 subjects were withdrawn post hoc due to lack of expert microscopy or qPCR confirmation of the positive P. vivax RDT at enrollment. The final per-protocol population was 317 subjects (85% of the mITT population), with baseline characteristics shown in Table 1.
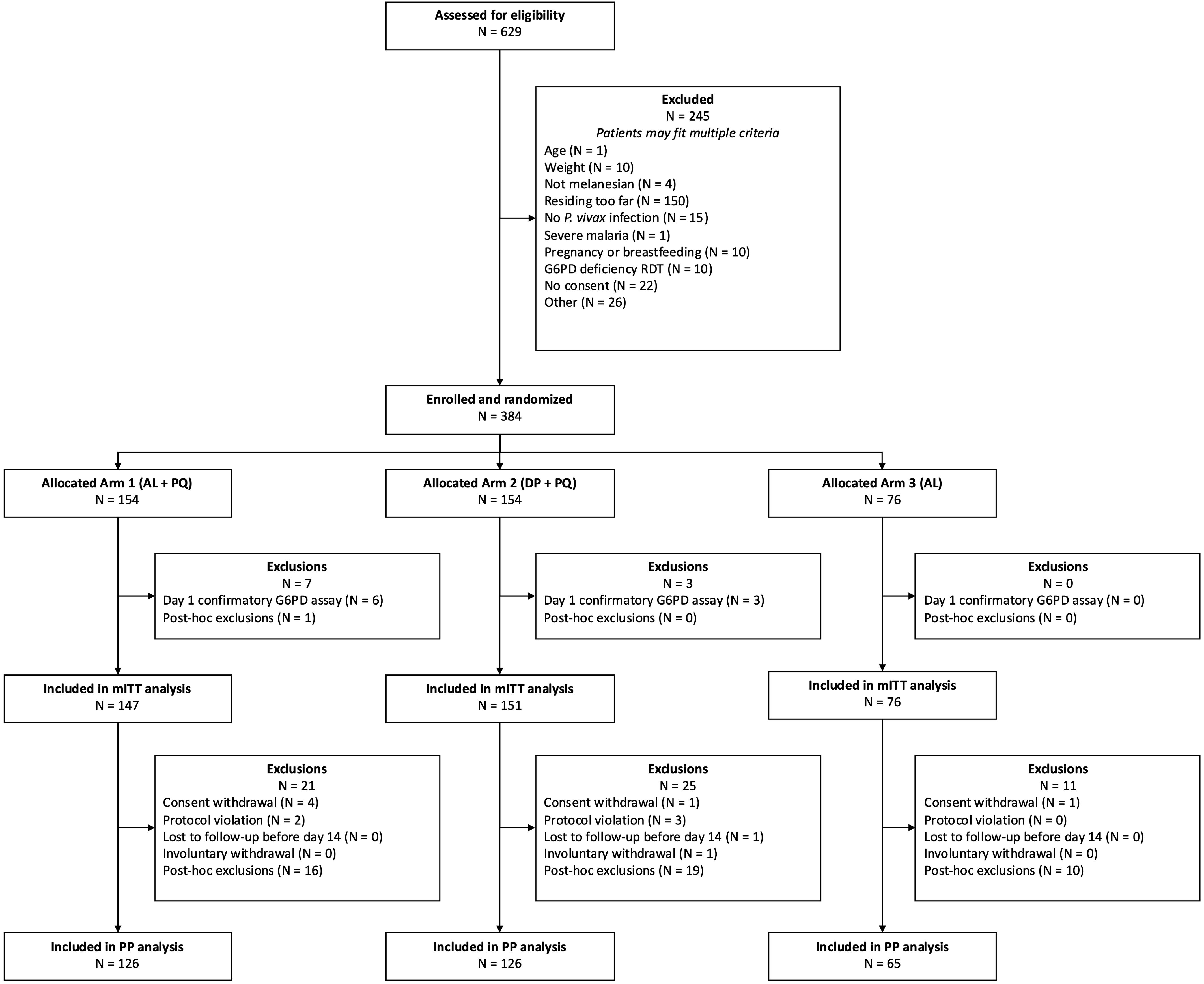
Figure 1. CONSORT diagram.
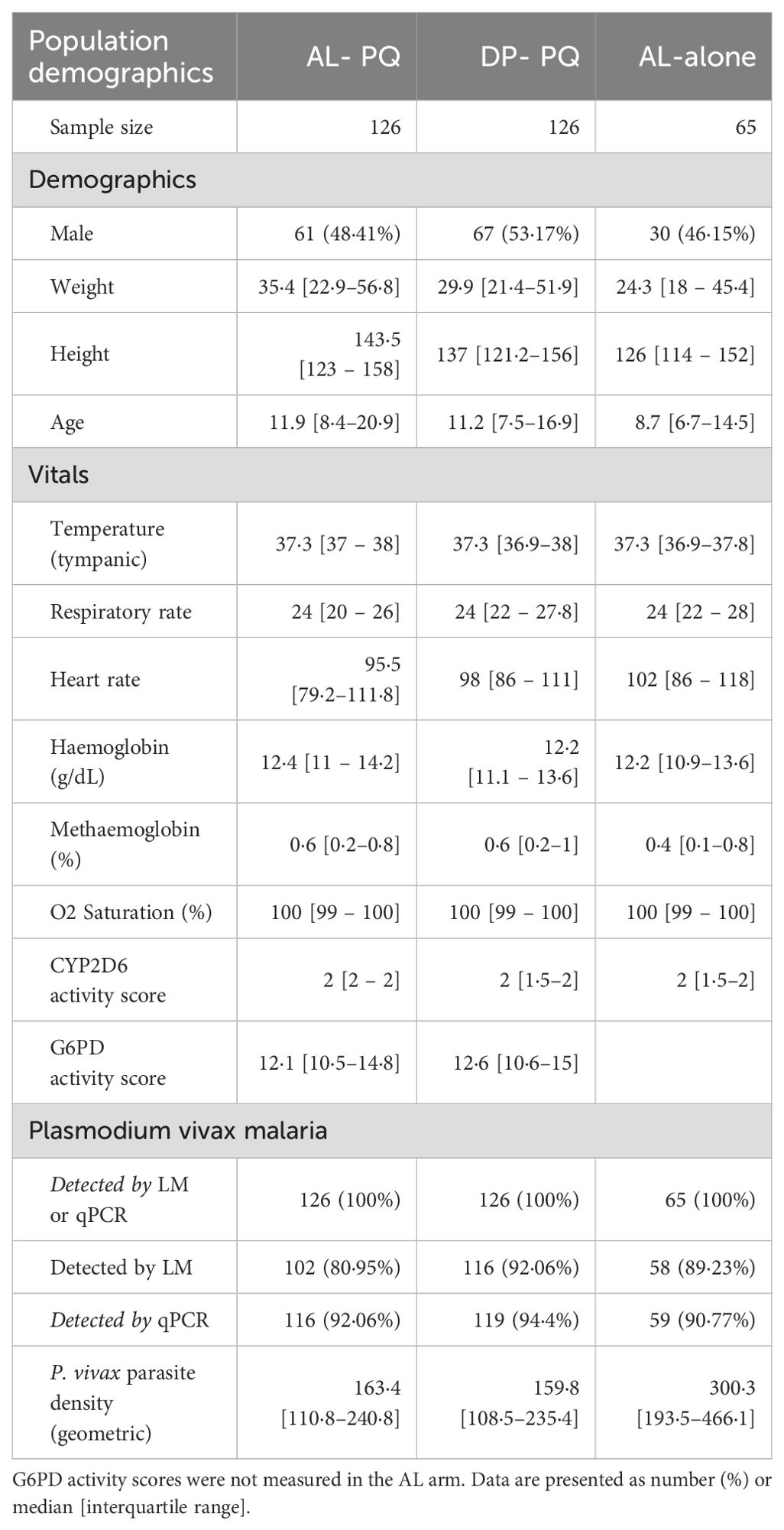
Table 1. Baseline characteristics of the PP cohort.
3.1.2 Follow-up
Twenty-eight subjects (8.8%) who completed treatment were lost to follow-up prior to recurrent parasitemia or the end of the study, with comparable rates of loss in all arms (AL–PQ: 10/126, DP–PQ: 13/126, AL: 5/65; p = 0.79). Among the remaining 289 participants, 99.3% of 4,543 scheduled visits occurred. Details on individuals at risk at each follow-up time point are given in Figure 2, and details on censoring are included in Supplementary Figure 1.
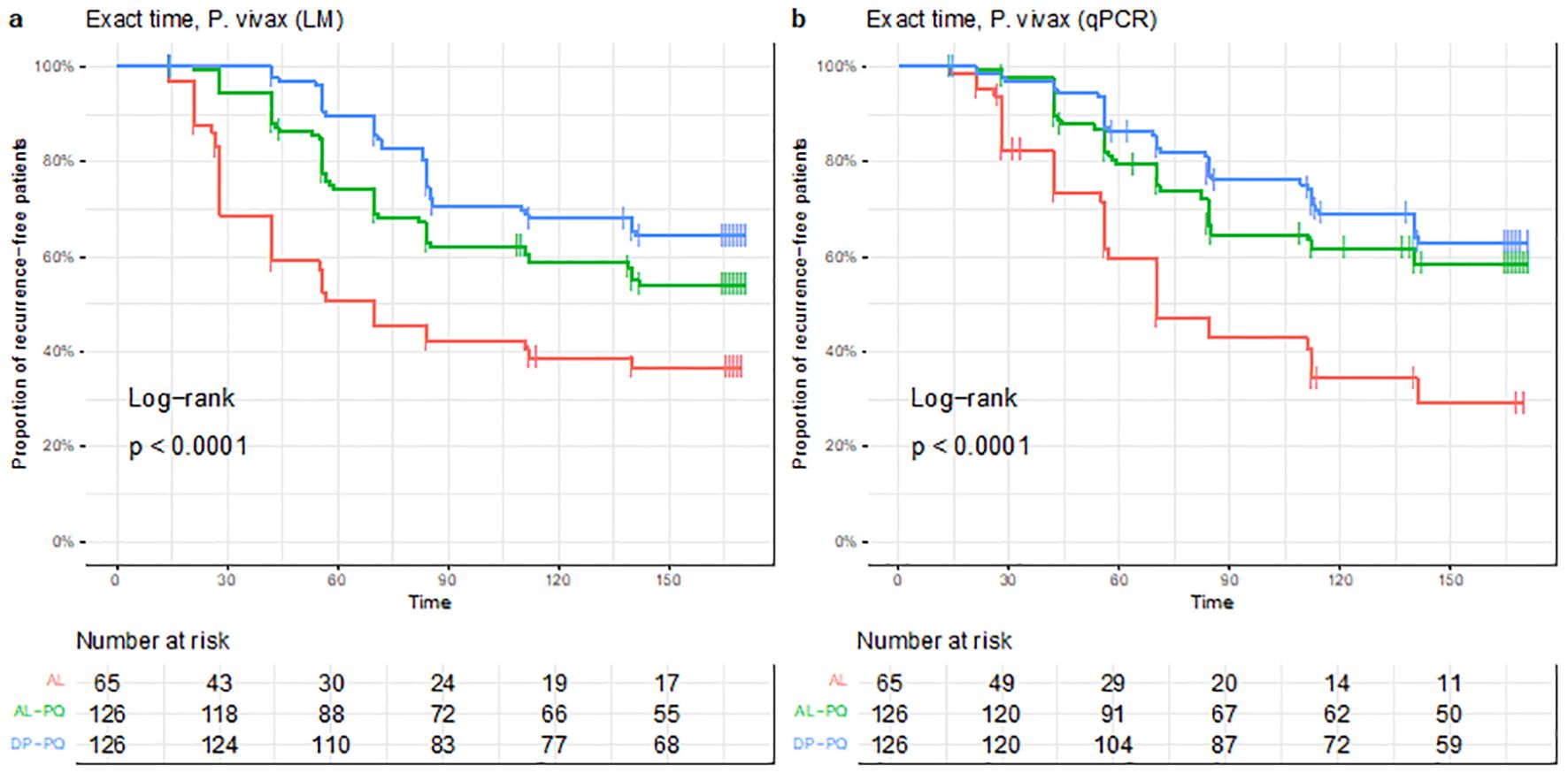
Figure 2. Kaplan–Meier curves with log-rank test results for (a) the primary LM endpoint and (b) the secondary qPCR endpoint in the per-protocol cohort. The P-value shows the result of the log-rank test applied to all three study arms.
3.2 Treatment efficacy
3.2.1 P. vivax recurrence by treatment arm
Over 6 months of follow-up, 39 (60.0%) and 37 (56.9%) of participants in the PP analysis receiving AL alone had LM- or PCR-detectable recurrent P. vivax infections, respectively (Figure 2). This demonstrates a high rate of recurrent P. vivax parasitemia without PQ hypnozoitocidal treatment.
Across all treatment arms, the steepest rate of P. vivax recurrence began between days 15 and 30 post-enrollment and continued through the first 90 days of follow-up (Figure 2). Both PQ treatment arms had significantly lower recurrence rates than the AL-alone relapse-control arm, whether by LM (43.7% vs. 60% for AL–PQ vs. AL alone, P = 0.03; and 34.1% vs. 60% for DP–PQ vs. AL alone, P = 0.0007) or qPCR (37.3% vs. 56.9% for AL–PQ vs. AL alone, P = 0.01; and 34.1% vs. 56.9% for DP–PQ vs. AL alone, P = 0.003). Although somewhat higher recurrence rates were observed in the AL–PQ group compared with the DP–PQ group at the 6-month endpoint (Figure 2), none reached statistical significance, whether by LM (43.7% vs. 34.1% for AL–PQ and DP–PQ, respectively) or by qPCR (37.3% vs. 34.1%). All P values were >0.15 in both PP (Figure 2) and mITT analyses, for which results were similar, albeit with overall higher recurrence rates (Supplementary Material S1, Section S1.5).
3.2.2 Efficacy of radical cure
When analysed by Cox proportional-hazard ratios over 6 months of follow-up, AL–PQ and DP–PQ reduced the hazard of LM-positive recurrent P. vivax infection in the PP population by 50% (P < 0.001) and 66% (P < 0.001), respectively (Table 2). After adjusting for multiple comparisons, DP–PQ showed a nonsignificant protective trend compared with AL–PQ for the LM endpoint (P = 0.1399).

Table 2. Hazard ratios [95% confidence intervals] of P. vivax recurrence calculated using Cox proportional-hazard regressions in the PP cohort.
Model diagnostics, however, indicated that the assumption of proportional hazards did not hold, at least for the LM endpoint. Time-stratified Cox regressions were conducted, guided by visual inspection of the time-dependent hazard function. An inflection point was identified between days 42 – 56, leading to three strata being included in subsequent analyses (Table 3). The hazard of recurrence decreased in both primaquine arms during the first time interval (day 0 through 42) and did not reach statistical significance thereafter. Further time-stratified analyses, including model diagnostics, are available in Supplementary Material S1 (Section S1.4) and can be used to pinpoint when the survival curves differ.
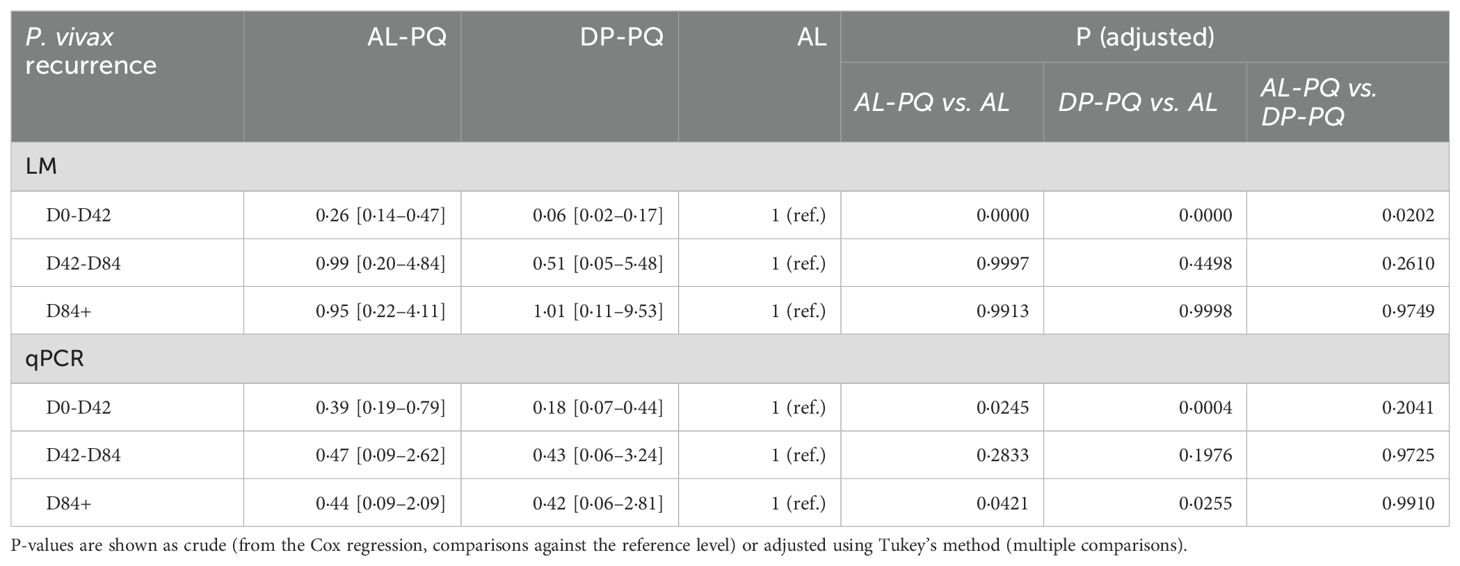
Table 3. Hazard ratios [95% confidence intervals] of P. vivax recurrence calculated using time-stratified Cox proportional-hazard regression in the PP cohort.
3.3 Safety and tolerability
3.3.1 Adverse events
Among the randomised participants (n = 384), two episodes of significant PQ-induced acute haemolytic anemia (AHA) occurred early in the study. Although both participants had normal G6PD RDT results during screening and enrollment, they developed jaundice, fatigue, pallor, and dark urine 3 and 7 days after commencing treatment (Hillmen 5). Both were later confirmed to have G6PD deficiency by ELISA and repeat RDT testing and were found to carry the “Union” G6PD-deficient genotype. They made full recoveries following cessation of PQ at the time haemolysis was identified.
The 16-year-old male participant, who had completed six daily PQ doses, experienced the more severe AHA and was hospitalised for a 46% relative drop in Hb (nadir of 6.4 g/dL). He received a blood transfusion before recovering. Both cases were reported to the study DSMB as treatment related, and after the second case enrollment was immediately halted until quantitative next-day G6PD testing could be implemented. Full details of these two cases are reported separately (Kosasih et al., 2023).
Aside from these two severe adverse events (SAEs), all treatment arms were well tolerated, and there were no other SAEs (Table 4). Two non-G6PD-deficient participants met criteria for mild haemolysis, with minor early reductions in Hb considered attributable to acute malarial illness.
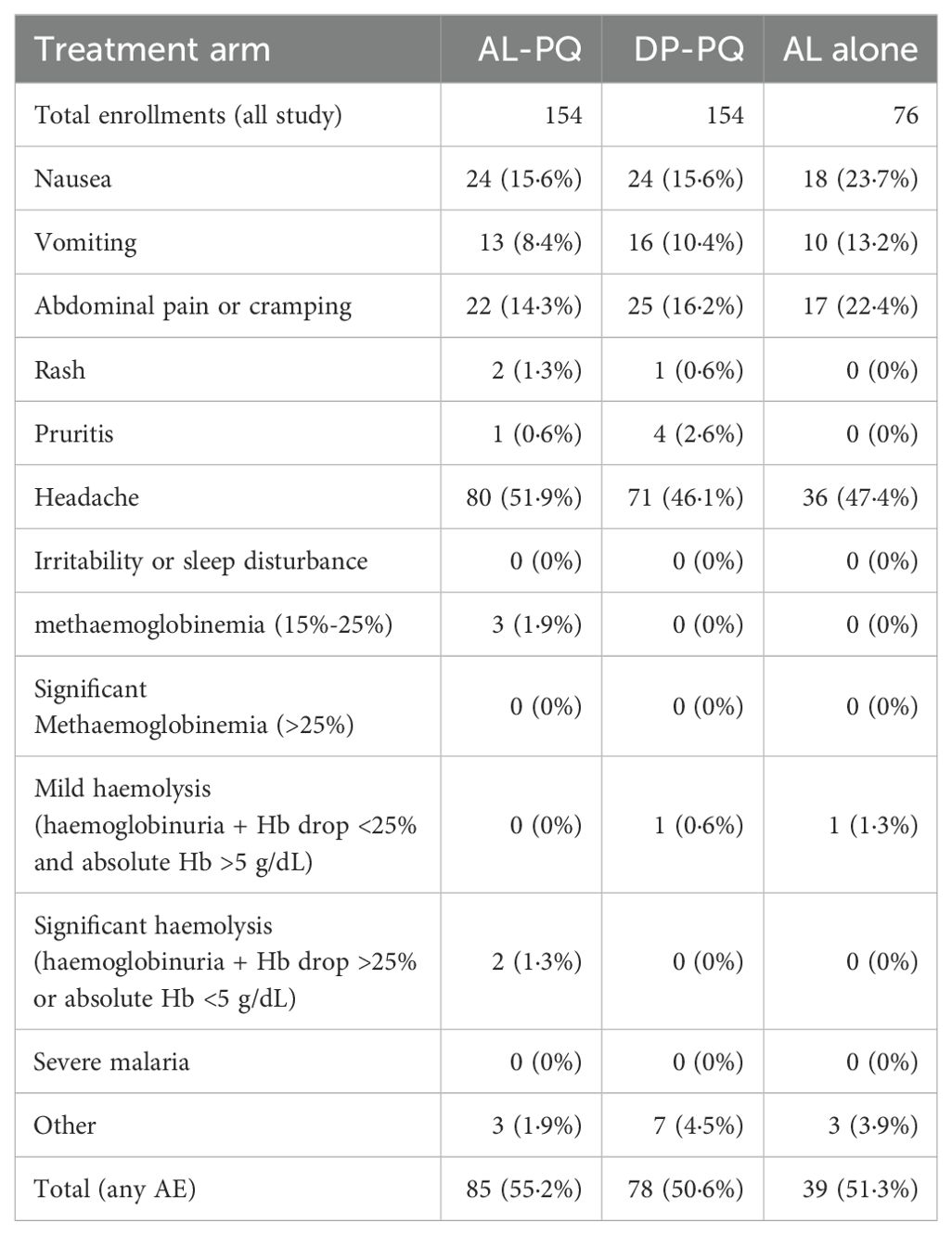
Table 4. Occurrence of any reported adverse events for all enrolled participants across study arms.
3.3.2 Methaemoglobin concentrations
MetHb concentrations according to treatment arm are shown in Figure 3. No difference was observed between the two PQ-containing arms at any time point (P > 0.15), with peak levels occurring at day 7 (median 1.4% and 1.45% for AL–PQ and DP–PQ, respectively). Participants were classified as MetHb “normal sensitivity” or “exaggerated sensitivity” if a MetHb level >5% was observed during PQ therapy. Exaggerated methaemoglobinemia clustered in 25 participants (18 for AL–PQ and 7 for DP–PQ), indicating consistency in individual outlying values (Supplementary Figure 2). The adjusted hazard ratio for recurrent P. vivax by LM among participants with exaggerated sensitivity was 1.06 (95% CI: 0.55–2.05, P = 0.86) relative to those with normal sensitivity.
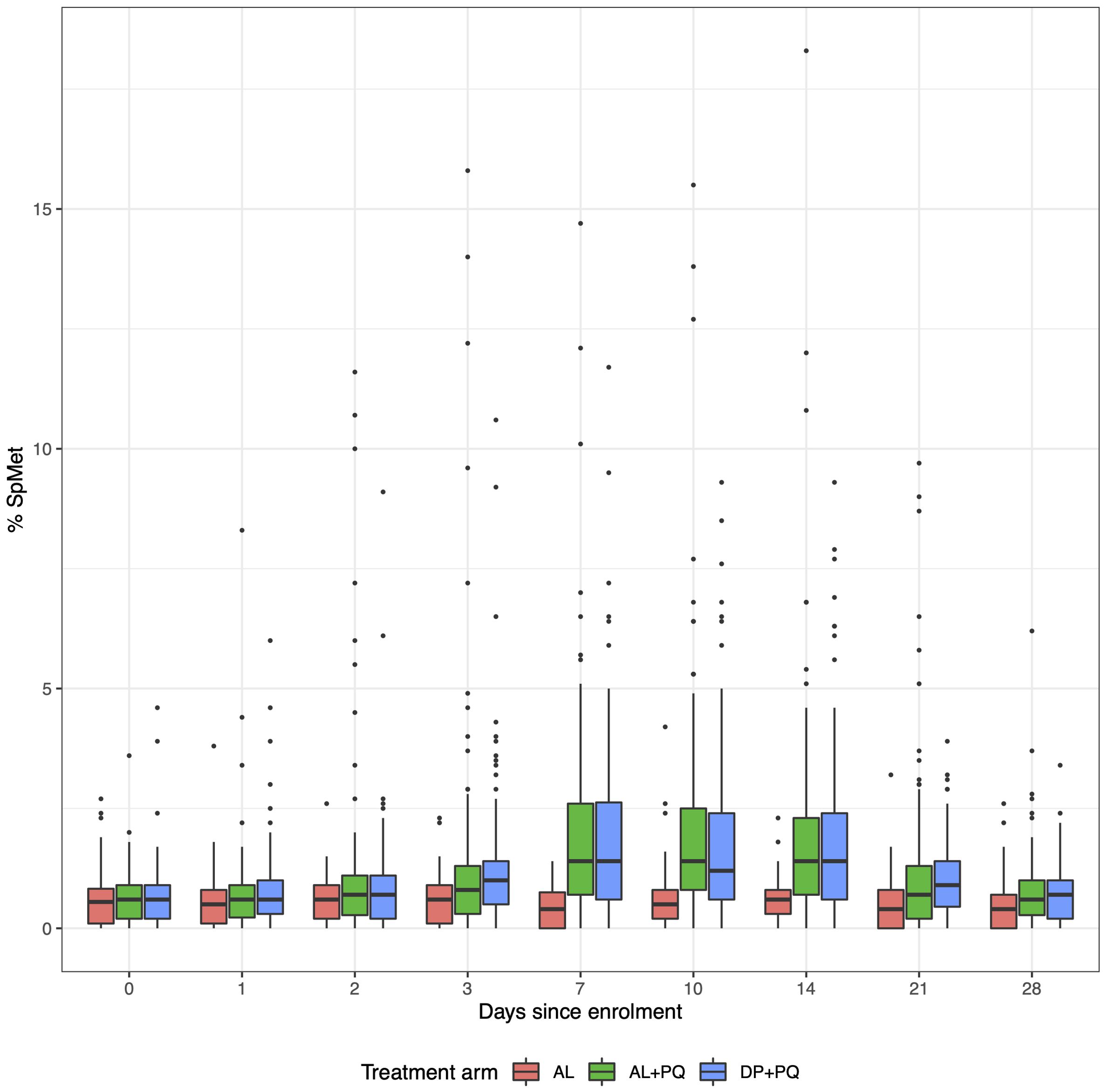
Figure 3. Methaemoglobin levels during the 28 days following treatment initiation.
3.3.3 Day 7 drug concentrations
Day 7 drug and metabolite concentrations for each treatment arm are shown in Figure 4. No significant differences were observed between concentrations of PQ or its metabolites (5,6-OQ and CPQ) when comparing the AL–PQ and DP–PQ arms (PQ: P = 0.46; 5,6-OQ: P = 0.67; CPQ: P = 0.12), nor when comparing L and its metabolite (DBL) in AL vs. AL–PQ arms (L: P = 0.27; DBL: P = 0.50). Participants with early recurrences (i.e. day <42) had substantially lower carboxy-PQ levels than those with later or no parasitemia (Supplementary Figure 6). Fourteen participants not assigned to AL treatment showed evidence of unreported lumefantrine consumption.
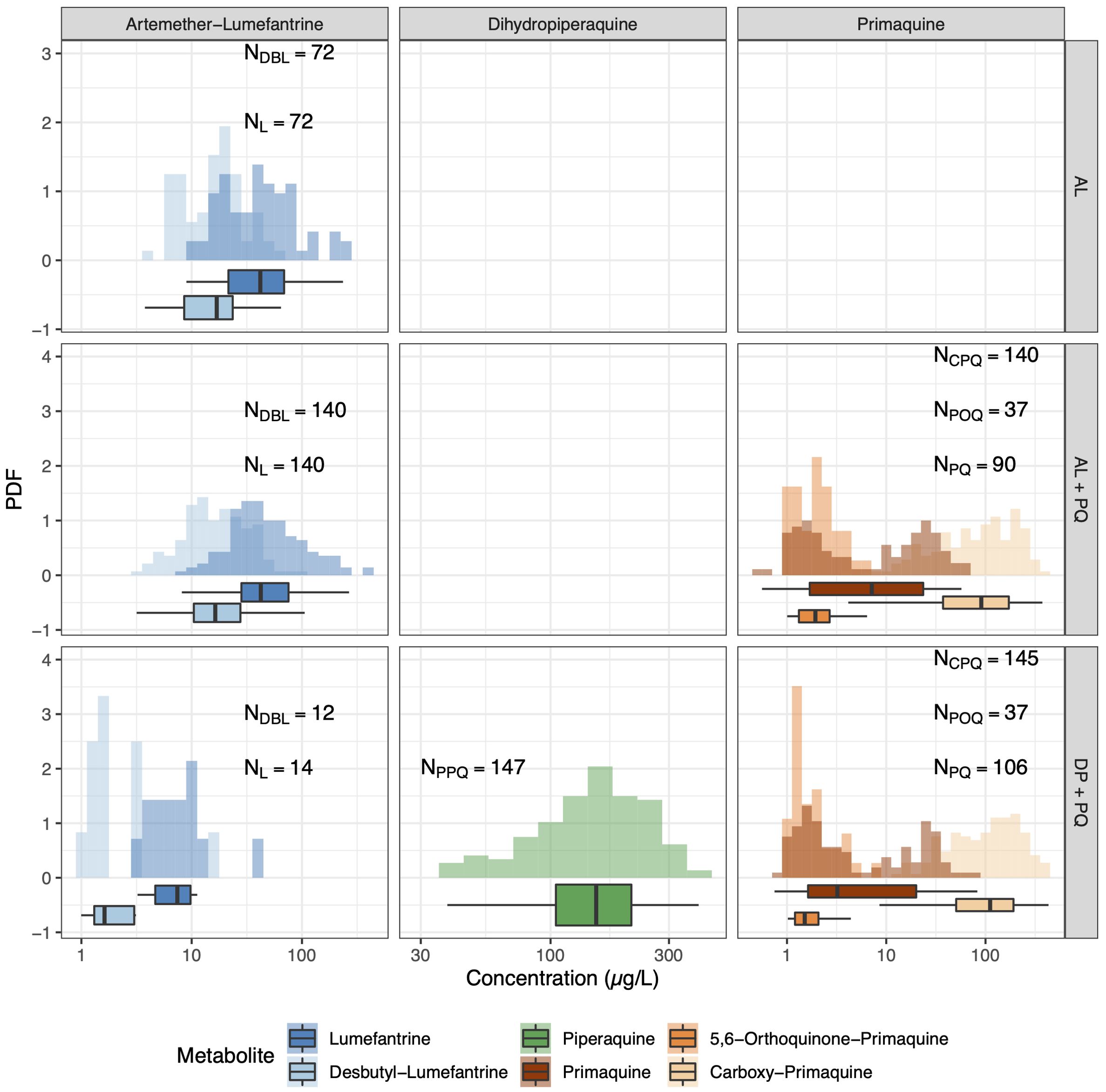
Figure 4. Plasma concentrations of drug metabolites in plasma measured on day 7. Rows correspond to treatment arms, while columns regroup metabolites according to their drug of origin. In Arm 2 (DP+PQ), at least 14 participants showed non-zero AL-related metabolite levels on day 7 that are attributed to undeclared self-medication with previously owned AL tablets.
3.3.4 CYP2D6 genotyping
CYP2D6 genotype was obtained in 346 (92.5%) of enrolled participants, of whom 274 (79.2%) had genotypes that enabled mapping to a standardised phenotypic activity score (AS) for both alleles, based on the PharmGKB database (Whirl-Carrillo et al., 2012);. (https://www.pharmgkb.org/page/cyp2d6RefMaterials). The remaining 72 (20.8%) had at least one allele that was poorly characterised and therefore had no derivable AS.
Among available phenotypes, the vast majority of participants (86.1%) had CYP2D6 genotypes that mapped to normal-metaboliser activity scores (1.25 ≤ AS ≤ 2.25). No poor metabolisers (AS < 0.25) were observed, and only 20 (7.3%) were intermediate metabolisers (0.25 ≤ AS < 1.25), with a further 18 (6.6%) characterised as ultrarapid metabolisers (AS > 2.25). Participants were further aggregated into three groups: slow metabolisers (AS < 1.5, n = 47), normal (1.5 ≤ AS ≤ 2, n = 208), and fast metabolisers (AS > 2, n = 19).
Overall, 227 (71.6%) participants from the per-protocol cohort had a fully characterised AS. There was no difference in the distribution of CYP2D6 metaboliser categories between treatment arms regardless of the cutoff used for categorisation (Fisher’s exact test, PharmGKB classification P = 0.24; aggregated categorization P=0.08). The category of CYP2D6 activity score (slow vs. normal/fast) was not associated with detectability (Fisher’s exact test, P-values ranging 0.44–1.0) or concentrations (Kruskal–Wallis test, P-values ranging 0.18–0.98) of PQ or its CPQ and 5,6-OQ metabolites, nor of PPQ or L/DBL. No associations were found with either treatment outcomes (ANOVA Wald test, LM: P=0.79; qPCR: P=0.63) or MetHb peak level (ANOVA, P=0.22).
4 Discussion
When administered concurrently with either first- or second-line ACT regimens, PQ at 0.25 mg/kg for 14 days demonstrated poor efficacy against relapse by P. vivax in the Solomon Islands. This is the first trial from the Western Pacific or South-East Asia to estimate radical curative efficacy of the commonly used AL-PQ and DP-PQ combinations with the lower 3.5 mg/kg total dose, and it raises concerns regarding the suitability of current policies and practices for radical cure. We found no evidence indicating impaired PQ metabolism as a possible explanation for poor efficacy; instead, the phenomenon appears to stem from inadequacy of the dose. A 2012 review by John et al. found that patients receiving the 7 mg/kg total dose of PQ were five times less likely to experience P. vivax recurrence compared with those receiving the 3.5 mg/kg regimen (John et al., 2012). High radical cure rates with the 7 mg/kg PQ dose have now also been documented with a variety of blood schizontocidal partner drugs—including artesunate, artesunate–pyronaridine, and DP (Nelwan et al., 2015)—making it less likely that drug–drug interactions result in a clinically significant effect on PQ efficacy at the higher dose. A recent systematic review and meta-analysis affirmed the superiority of a higher dose, irrespective of blood schizontocidal therapy co-administered with PQ as radical cure or geographic origin of infection (Commons et al., 2024).
The strengths of the current trial include its large number of participants successfully randomised, treated, and followed with high adherence rates over 6 months. The trial had two important limitations: (i) reinfection may have confounded efficacy estimates; and (ii) the PQ dose was inherently inadequate. Participants remained exposed to reinfection, and some recurrences may have been newly acquired, but we considered this a relatively low-probability event. Other studies show that >80% of P. vivax attacks in most endemic settings originate from hypnozoites rather than from infections caused by recent mosquito bites (Commons et al., 2020). The inadequacy of the PQ dose likely masked the effects of any differential drug–drug interactions (i.e., AL-PQ vs. DP-PQ) or of CYP2D6 polymorphisms on PQ efficacy against relapse. Ample evidence indicates that population variations in CYP2D6 activity do affect PQ efficacy in other populations, including in Asia and the Americas, and particularly at the higher total dose of 7 mg/kg (Baird et al., 2018; Bennett et al., 2013; Park et al., 2022). In the current study, the lack of association between CYP2D6 activity and risk of recurrent P. vivax following PQ therapy may reflect both the inherently inadequate PQ dose (where even normal metabolism was insufficient to prevent relapse) and the relatively low frequency (<15%) of genotypes corresponding to impaired CYP2D6 activity genotypes in this population.
Elevated metHb, peaking around day 7 of treatment is consistently observed during daily 8-aminoquinoline therapy. The same occurred in our study, but at notably lower levels than reported elsewhere for the same PQ dose (Figure 3)—with day 7 mean levels of approximately 2% here compared with 4% in other studies (White et al., 2022). Although metHb levels correlate with PQ dose, it remains unclear whether they independently predict therapeutic response.
Methaemoglobinemia may occur in association with redox recycling of highly reactive 5-hydroxylated PQ metabolites (Fletcher et al., 1988) derived from CYP2D6 activity, and therefore could plausibly be considered as a putative surrogate of bioactive drug concentrations (Marcsisin et al., 2016). In the current study, however, we found no association between metHb elevation and either CYP2D6 activity score (AS) or risk of recurrent parasitemia. Among the 25 participants with metHb >5% during treatment (classified as relatively sensitive to PQ-induced metHb elevation), CYP2D6 AS values ranged from 1 to 3 compared with 0.25 to 4 among metHb-insensitive participants (both groups had a mean of 2.0).
Day 7 MetHb levels among the 15 subjects without recurrent parasitemia by LM were statistically indistinguishable from those among the 10 subjects with post-treatment P. vivax parasitemia: 5.29% and 4.64%, respectively (P = 0.74). Again, the inherently inadequate PQ dose may have obscured any potential association between metHb levels and efficacy, with relapse remaining probable at any metHb level. The same limitation may also partially explain the apparent lack of association between efficacy and withCYP2D6 e-predicted activity scores in this population.
The reluctance to accept the necessity of the 7 mg/kg total PQ dose by many endemic nations (Recht et al., 2018) stems from the risk of acute haemolytic anemia (AHA) in G6PD- deficient (G6PDd) individuals. About 8% of residents of malaria-endemic countries (>400 million people globally) are thus vulnerable (Howes et al., 2012). Some of the most severe variants of G6PDd commonly occur in South and Southeast Asia and the Western Pacific, where >90% of P. vivax infections are found. G6PD Union is one such variant, and in our study, one subject carrying this variant developed severe haemolysys after only six of 14 daily PQ doses at the lower 3.5 mg/kg regimen.
This highlights the unresolved therapeutic dilemma with PQ: withholding or lowering the dose risks recurrent attacks in the majority, while giving higher doses risks severe haemolysis in the G6PD-deficient minority. Recent work has shown that ascending PQ doses may allow delivery of the full high-dose regimen in G6PDd individuals while preventing AHA (Pukrittayakamee et al., 2023). In light of the poor efficacy achieved with our 3.5 mg/kg regimen, safer approaches to delivering higher PQ doses are needed.
There are serious consequences of using no or inadequate PQ for radical cure. Repeated relapses at intervals of <2 months with Chesson-like strains lead to more frequent hospitalisations and are associated with higher all-cause mortality in the year following a diagnosis of P. vivax compared with P. falciparum (Dini et al., 2020; Douglas et al., 2014). Routine administration of highly efficacious radical cure should therefore substantially reduce the morbidity and mortality associated with endemic, frequently relapsing P. vivax malaria. Doing so safely, however, remains a steep challenge where these infections occur, i.e., in the impoverished rural tropics, where access to robust G6PD screening is currently exceedingly rare. As our experience in this trial highlights, no G6PD screening process may be considered free of error, and the risk of AHA with PQ persists. Mitigation strategies—including improved diagnostic platforms, better screening processes, early detection of AHA, and availability of transfusion support—must be considered as integral to any policy involving 8-aminoquinoline anti-relapse therapy.
5 Conclusions
PQ at a total dose of 3.5 mg/kg administered over 14 days did not provide good efficacy against relapse when combined with either AL or DP for radical cure in our patient population in the Solomon Islands. Similar low efficacy is expected in other SW Pacific populations that share the same parasite strains and have comparable host genetics. Whereas good efficacy of DP-PQ at the higher 7.0 mg/kg total dose has been confirmed in other studies from the Western Pacific, the same evidence has not yet been gathered for AL-PQ. Nonetheless, the equally poor efficacy of AL-PQ and DP-PQ in our study suggests they may also have equivalent efficacy at the higher PQ dosing regimen. The higher PQ dose required for effective radical cure carries a greater risk of severe AHA in vulnerable G6PD-deficient patients, but it also promises substantial health benefits by preventing frequent, dangerous relapses and by reducing overall onward transmission. Where G6PD testing is available, WHO now recommends a higher total PQ dose of 7mg/kg for Africa, Southeast Asia, and Oceania (World Health Organization, 2024b). Safer strategies for administering this regimen are therefore essential for the successful implementation of radical cure in vivax-endemic regions of the SW Pacific.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approvals were obtained through the Solomon Islands Health Research and Ethics Review Board (HRE No. 041/16) and the Walter and Eliza Hall Institute of Medical Research Human Research Ethics Committee (WEHI16-08). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
RJ: Formal analysis, Investigation, Project administration, Writing – original draft, Writing – review & editing. TO: Data curation, Formal analysis, Writing – original draft, Writing – review & editing. LW: Investigation, Project administration, Writing – review & editing. AB: Investigation, Project administration, Writing – review & editing. SC: Formal analysis, Investigation, Methodology, Writing – review & editing. SR: Formal analysis, Investigation, Methodology, Writing – original draft. CB: Investigation, Methodology, Writing – original draft. JM: Investigation, Methodology, Writing – review & editing. BM: Investigation, Methodology, Writing – review & editing. MP-S: Investigation, Methodology, Writing – review & editing. LM: Investigation, Methodology, Writing – review & editing. UL: Investigation, Project administration, Writing – review & editing. SZ: Data curation, Formal analysis, Writing – review & editing. JK: Conceptualization, Writing – review & editing. HK: Conceptualization, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. IM: Conceptualization, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. The study was supported by a grant from the Bill and Melinda Gates Foundation (funding grant ID number: OPP1151132, grant title: “Could a significant interaction between artemether-lumefantrine and primaquine be seriously undermining drug-based strategies for malaria elimination?“). IM is supported by an NHMRC Investigator Grant (#2016726). The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Acknowledgments
We would like to acknowledge the invaluable support and technical expertise provided by the Solomon Islands Ministry of Health and Medical Services (SIMHMS), including the Solomon Islands National Vector Borne Disease Control Division, the staff from the National Referral Hospital (Honiara, Solomon Islands), the Good Samaritan Hospital (Tetere, Guadalcanal) and all Solomon Islands staff involved in the preparation of this research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmala.2025.1604498/full#supplementary-material
References
Baird J. K. (2004). Chloroquine resistance in Plasmodium vivax. Antimicrob. Agents Chemother. 48, 4075–4083. doi: 10.1128/AAC.48.11.4075-4083.2004
Baird J. K. (2009). Resistance to therapies for infection by Plasmodium vivax. Clin. Microbiol. Rev. 22, 508–534. doi: 10.1128/CMR.00008-09
Baird J. K., Louisa M., Noviyanti R., Ekawati L., Elyazar I., Subekti D., et al. (2018). Association of impaired cytochrome P450 2D6 activity genotype and phenotype with therapeutic efficacy of primaquine treatment for latent plasmodium vivax malaria. JAMA Netw. Open 1, e181449. doi: 10.1001/jamanetworkopen.2018.1449
Battle K. E., Lucas T. C. D., Nguyen M., Howes R. E., Nandi A. K., Twohig K. A., et al. (2019). Mapping the global endemicity and clinical burden of Plasmodium vivax 2000-17: a spatial and temporal modelling study. Lancet 394, 332–343. doi: 10.1016/s0140-6736(19)31096-7
Bennett J. W., Pybus B. S., Yadava A., Tosh D., Sousa J. C., Mccarthy W. F., et al. (2013). Primaquine failure and cytochrome P-450 2D6 in Plasmodium vivax malaria. N Engl. J. Med. 369, 1381–1382. doi: 10.1056/NEJMc1301936
Chu C. S., Phyo A. P., Turner C., Win H. H., Poe N. P., Yotyingaphiram W., et al. (2019). Chloroquine versus dihydroartemisinin-piperaquine with standard high-dose primaquine given either for 7 days or 14 days in plasmodium vivax malaria. Clin. Infect. Dis. 68, 1311–1319. doi: 10.1093/cid/ciy735
Commons R. J., Rajasekhar M., Edler P., Abreha T., Awab G. R., Baird J. K., et al. (2024). Effect of primaquine dose on the risk of recurrence in patients with uncomplicated Plasmodium vivax: a systematic review and individual patient data meta-analysis. Lancet Infect. Dis. 24, e20230922. doi: 10.1016/s1473-3099(23)00430-9
Commons R. J., Simpson J. A., Watson J., White N. J., and Price R. N. (2020). Estimating the proportion of plasmodium vivax recurrences caused by relapse: A systematic review and meta-analysis. Am. J. Trop. Med. Hyg 103, 1094–1099. doi: 10.4269/ajtmh.20-0186
Dini S., Douglas N. M., Poespoprodjo J. R., Kenangalem E., Sugiarto P., Plumb I. D., et al. (2020). The risk of morbidity and mortality following recurrent malaria in Papua, Indonesia: a retrospective cohort study. BMC Med. 18, e20200220. doi: 10.1186/s12916-020-1497-0
Douglas N. M., Pontororing G. J., Lampah D. A., Yeo T. W., Kenangalem E., Poespoprodjo J. R., et al. (2014). Mortality attributable to Plasmodium vivax malaria: a clinical audit from Papua, Indonesia. BMC Med. 12, e20141118. doi: 10.1186/s12916-014-0217-z
Fletcher K. A., Barton P. F., and Kelly J. A. (1988). Studies on the mechanisms of oxidation in the erythrocyte by metabolites of primaquine. Biochem. Pharmacol. 37, 2683–2690. doi: 10.1016/0006-2952(88)90263-8
Howes R. E., Piel F. B., Patil A. P., Nyangiri O. A., Gething P. W., Dewi M., et al. (2012). G6PD deficiency prevalence and estimates of affected populations in malaria endemic countries: a geostatistical model-based map. PloS Med. 9, e1001339. doi: 10.1371/journal.pmed.1001339
John G. K., Douglas N. M., Von Seidlein L., Nosten F., Baird J. K., White N. J., et al. (2012). Primaquine radical cure of Plasmodium vivax: a critical review of the literature. Malar J. 11, e20120817. doi: 10.1186/1475-2875-11-280
Kosasih A., James R., Chau N. H., Karman M. M., Panggalo L. V., Wini L., et al. (2023). Case series of primaquine-induced haemolytic events in controlled trials with G6PD screening. Pathogens 12, e20230919. doi: 10.3390/pathogens12091176
Marcsisin S. R., Reichard G., and Pybus B. S. (2016). Primaquine pharmacology in the context of CYP 2D6 pharmacogenomics: Current state of the art. Pharmacol. Ther. 161, e20160322. doi: 10.1016/j.pharmthera.2016.03.011
Mueller I., Galinski M. R., Baird J. K., Carlton J. M., Kochar D. K., Alonso P. L., et al. (2009). Key gaps in the knowledge of Plasmodium vivax, a neglected human malaria parasite. Lancet Infect. Dis. 9, 555–566. doi: 10.1016/S1473-3099(09)70177-X
Nelwan E. J., Ekawati L. L., Tjahjono B., Setiabudy R., Sutanto I., Chand K., et al. (2015). Randomized trial of primaquine hypnozoitocidal efficacy when administered with artemisinin-combined blood schizontocides for radical cure of Plasmodium vivax in Indonesia. BMC Med. 13, e20151211. doi: 10.1186/s12916-015-0535-9
Park Y. A., Park K. H., Yoon H. Y., Yee J., and Gwak H. S. (2022). Effects of CYP2D6 genotypes on Plasmodium vivax recurrence after primaquine treatment: A meta-analysis. Travel Med. Infect. Dis. 48, e20220420. doi: 10.1016/j.tmaid.2022.102333
Pukrittayakamee S., Jittamala P., Watson J. A., Hanboonkunupakarn B., Leungsinsiri P., Poovorawan K., et al. (2023). Pharmacometric assessment of primaquine induced haemolysis in glucose-6-phosphate dehydrogenase deficiency (Cambridge: eLife Sciences Publications, Ltd). doi: 10.7554/elife.87318.2
Pybus B. S., Marcsisin S. R., Jin X., Deye G., Sousa J. C., Li Q., et al. (2013). The metabolism of primaquine to its active metabolite is dependent on CYP 2D6. Malaria J. 12, 212. doi: 10.1186/1475-2875-12-212
R&D Diagnostics Ltd OSMMR2000-D G -6-PD Kit. R & D DIAGNOSTICS LTD, 41, El. Venizelou str., 15561 Holargos, Greece.
R Core Team (2021). R: A language and environment for statistical computing (Vienna, Austria: R Foundation for Statistical Computing). https://www.R-project.org/ (Accessed March 8, 2025).
Recht J., Ashley E. A., and White N. J. (2018). Use of primaquine and glucose-6-phosphate dehydrogenase deficiency testing: Divergent policies and practices in malaria endemic countries. PloS Negl. Trop. Dis. 12, e0006230. doi: 10.1371/journal.pntd.0006230
Solomon Islands Government, Ministry of Health and Medical Services (2018). SOLOMON ISLANDS 2018 Malaria Case Management Guideline. Honiara, Solomon Islands.
Spring M. D., Sousa J. C., Li Q., Darko C. A., Morrison M. N., Marcsisin S. R., et al. (2019). Determination of cytochrome P450 isoenzyme 2D6 (CYP2D6) genotypes and pharmacogenomic impact on primaquine metabolism in an active-duty US military population. J. Infect. Dis. 220, 1761–1770. doi: 10.1093/infdis/jiz386
Taylor W. R. J., Thriemer K., Von Seidlein L., Yuentrakul P., Assawariyathipat T., Assefa A., et al. (2019). Short-course primaquine for the radical cure of Plasmodium vivax malaria: a multicentre, randomised, placebo-controlled non-inferiority trial. Lancet 394, e20190718. doi: 10.1016/S0140-6736(19)31285-1
von Ahsen N., Tzvetkov M., Karunajeewa H. A., Gomorrai S., Ura A., Brockmöller J., et al. (2010). CYP2D6 and CYP2C19 in Papua New Guinea: High frequency of previously uncharacterized CYP2D6 alleles and heterozygote excess. Int. J. Mol. Epidemiol. Genet. 1, 310–319.
Whirl-Carrillo M., Mcdonagh E. M., Hebert J. M., Gong L., Sangkuhl K., Thorn C. F., et al. (2012). Pharmacogenomics knowledge for personalized medicine. Clin. Pharmacol. Ther. 92, 414–417. doi: 10.1038/clpt.2012.96
White N. J. (2011). Determinants of relapse periodicity in Plasmodium vivax malaria. Malar J. 10, e20111011. doi: 10.1186/1475-2875-10-297
White N. J. (2021). Anti-malarial drug effects on parasite dynamics in vivax malaria. Malar J. 20, e20210321. doi: 10.1186/s12936-021-03700-7
White N. J., Watson J. A., and Baird J. K. (2022). Methaemoglobinaemia and the radical curative efficacy of 8-aminoquinoline antimalarials. Br. J. Clin. Pharmacol. 88, 2657–2664. doi: 10.1111/bcp.15219
Woon S. A., Moore B. R., Laman M., Tesine P., Lorry L., Kasian B., et al. (2023). Ultra-short course, high-dose primaquine to prevent Plasmodium vivax infection following uncomplicated pediatric malaria: A randomized, open-label, non-inferiority trial of early versus delayed treatment. Int. J. Infect. Dis. 130, 189–195. doi: 10.1016/j.ijid.2023.03.010
World Health Organization (2024a). World malaria report 2024: addressing inequity in the global malaria response (Geneva: World Health Organization (WHO). Available online at: https://iris.who.int/bitstream/handle/10665/379751/9789240104440-eng.pdf?sequence=1 (Accessed June 10, 2025).
World Health Organization (2022). WHO guidelines for malaria, 3 June 2022 (Geneva: World Health Organization). Available online at: https://apps.who.int/iris/bitstream/handle/10665/354781/WHO-UCN-GMP-2022.01-Rev.2-eng.pdf?sequence=1 (Accessed March 12, 2025).
World Health Organization (2024b). WHO guidelines for malaria, 30 November 2024 (Geneva: World Health Organization). Available online at: https://iris.who.int/bitstream/handle/10665/379635/B09146-eng.pdf?sequence=1 (Accessed June 6, 2025).
Keywords: Plasmodium vivax, primaquine radical cure, CYP2D6, artemether-lumefantrine, dihydroartemisinin-piperaquine, G6PD deficiency, methaemoglobinemia, Solomon Islands
Citation: James R, Obadia T, Wini L, Bobogare A, Charnaud S, Ruybal-Pesántez S, Bourke C, Munro JE, Moore BR, Page-Sharp M, Manning L, Liligeto U, Zaloumis SG, Baird JK, Karunajeewa H and Mueller I (2025) Efficacy of low-dose primaquine plus artemether-lumefantrine or dihydroartemisinin-piperaquine for radical cure of Plasmodium vivax in the Solomon Islands: a randomised clinical trial. Front. Malar. 3:1604498. doi: 10.3389/fmala.2025.1604498
Received: 01 April 2025; Accepted: 11 August 2025;
Published: 03 October 2025.
Edited by:
Andre Lin Ouedraogo, Bill and Melinda Gates Foundation, United StatesReviewed by:
Jessica Molina-Franky, Beckman Research Institute, City of Hope, United StatesAnurag Shukla, Drexel University, United States
Shrikant Nema, International Centre for Genetic Engineering and Biotechnology, India
Copyright © 2025 James, Obadia, Wini, Bobogare, Charnaud, Ruybal-Pesántez, Bourke, Munro, Moore, Page-Sharp, Manning, Liligeto, Zaloumis, Baird, Karunajeewa and Mueller. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ivo Mueller, TXVlbGxlckB3ZWhpLmVkdS5hdQ==
†These authors have contributed equally to this work