 Pedro Renato Chocair1*
Pedro Renato Chocair1* Precil Diego Miranda de Menezes Neves1
Precil Diego Miranda de Menezes Neves1 Victor Augusto Hamamoto Sato1
Victor Augusto Hamamoto Sato1 Sara Mohrbacher1Érico Souza Oliveira1Leonardo Victor Barbosa Pereira1Alessandra Martins Bales1
Sara Mohrbacher1Érico Souza Oliveira1Leonardo Victor Barbosa Pereira1Alessandra Martins Bales1 Fagner Pereira da Silva2John A. Duley3Américo Lourenço Cuvello-Neto1
Fagner Pereira da Silva2John A. Duley3Américo Lourenço Cuvello-Neto1- 1Internal Medicine and Nephrology Service, Hospital Alemão Oswaldo Cruz, São Paulo, Brazil
- 2Nursing Department, Hospital Alemão Oswaldo Cruz, São Paulo, Brazil
- 3School of Pharmacy, The University of Queensland, Brisbane, QLD, Australia
Background: Insulin resistance and/or hyperinsulinemia are closely linked to adiposity, metabolic syndrome (MetS) and prolonged inflammatory processes.
Methods: We retrospectively analyzed 1,018 adult individuals with a mean age of 46 years (74% male) and classified them as: Metabolically normal: without any of the five criteria of the International Diabetes Federation (IDF) used for the diagnosis of MetS, plus normal fasting insulin (Men < 8 mU/L, Women < 10 mU/L); Level 1 MetS: with one or two IDF criteria, plus hyperinsulinemia (Men: ≥ 8 mU/L), and Women: ≥ 10 mU/L); Level 2 MetS: with three or more IDF criteria, plus hyperinsulinemia.
Results: The mean values for fasting insulinemia in metabolically normal individuals was 4.6 ± 1.8 mU/L and 5.6 ± 2.3 mU/L, while their means for the Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) were 1.0 and 1.2 for men and women, respectively. In addition, the mean values for insulin (and HOMA-IR) for individuals with two normal anthropometric parameters (body mass index and waist girth), or two normal anthropometric parameters plus no IDF criteria, were similar to the metabolically normal group. Based on the obtained mean + 2 SD, we established the following insulin (and HOMA-IR) values as diagnostic cut-offs for hyperinsulinemia: Men: ≥ 8 mU/L (≥ 1.5), and Women: ≥ 10 mU/L (≥ 2.0). The mean serum insulin was significantly higher for individuals with Level 1 MetS (approx. 9 mU/L for both genders) compared with metabolically normal individuals, as was the prevalence of hepatic steatosis, which was more evident in men. Thus, the presence of one or two abnormal IDF criteria, combined with hyperinsulinemia and/or raised HOMA-IR, suggests the presence of MetS and insulin resistance. Patients of both genders with Level 2 MetS had higher serum insulin and/or HOMA-IR values than Level 1, as well as a higher prevalence of hypertension and hepatic steatosis, being more pronounced among men. The process was progressive and proportional to the degree of hyperinsulinemia.
Conclusion: It is proposed that intervention against MetS progression should be started in individuals with Level 1 MetS, rather than waiting for more criteria for diagnostic confirmation, which this should help to reduce the occurrence of known complications such as type 2 diabetes, atherosclerosis, hypertension, and chronic kidney disease, among others.
Background
Metabolic syndrome (MetS) is a serious disorder that results from prolonged subclinical systemic inflammation originating in adipose tissue (1–4). It is increasingly prevalent worldwide (5, 6) and threatens the continued growth of life expectancy that has been observed over the last two centuries (7).
The major factor responsible for its increased prevalence is certainly the pandemic of obesity, which is primarily caused by diets containing an excess of carbohydrates and by sedentary lifestyles (1, 8, 9). Yet, despite its recognized importance, there is no homogeneous definition of MetS. The most commonly used definitions are those of the European Group for the Study of Insulin Resistance, (10) the American Association of Clinical Endocrinologists, (11) the International Diabetes Federation (IDF), (12) and the National Cholesterol Education Program Adult Treatment Panel III 2005 (13). The first three consider insulin resistance to be a mandatory condition for diagnosis, while the latter requires the presence of three or more of the following five IDF criteria: (1) triglycerides ≥ 150 mg/dL; (2) high density lipoprotein-cholesterol (HDL-C) < 40 mg/dL in men and < 50 mg/dL in women, or patient receiving fibrate; (3) blood glucose ≥ 100 mg/dL; (4) increased waist girth (variable with ethnicity); and (5) hypertension ≥ 130 and/or/85 mm Hg, or patient receiving antihypertensive treatment (13).
Insulin resistance, hyperinsulinemia, and MetS are closely related to each other and to various medical complications such as type 2 diabetes, chronic kidney disease, hepatic steatosis, neoplasms, urinary calculosis, polycystic ovary syndrome, arthropathies, hypertension, cardiovascular diseases, and skin diseases including psoriasis (13–24).
Despite the recognized importance of MetS, the limits for diagnosing hyperinsulinemia and insulin resistance are still not clear. In this paper, we aimed to define normal values for insulin and the Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) index based on a Brazilian cohort, and to suggest a new and simpler classification for MetS. We propose that this will provide early recognition and promote preventive therapeutic intervention for complications.
Materials and methods
Participants and study design
This was a cross-sectional, retrospective, single-center study that aimed to define the diagnostic cut-offs for fasting blood insulin and HOMA-IR in Brazilian adults of both genders. A cohort of 1,015 adult study participants (751 men, 264 women), with a mean age of 46.5 years ± 8.91, were recruited from participants who underwent elective screening consultations (check-ups) from October 2020 to March 2021. Patients were examined for comorbidities such as hypertension, diabetes, dyslipidemia, and obesity, due to their relevance to the proposed analyses.
Patient numbers varied slightly in different categories of results as some participants did not undergo a specific examination (i.e., ultrasound), and these have been noted in the text.
This study was approved by the Ethics and Research Committee of Hospital Alemão Oswaldo Cruz de São Paulo (CAAE: 46489021.6.0000.0070).
Clinical evaluation and sample collection for laboratory tests
Blood pressure was measured during clinical evaluations using the auscultatory method with a manual sphygmomanometer, in a seated position after at least 5 min of rest. Waist girth (cm) was measured at the midpoint between the last rib and the iliac crest. Body mass index (BMI) was calculated after confirming weight and height.
The five criteria used by the IDF for the diagnosis of MetS (13)—as listed above—were assessed, and each participant also authorized an additional blood sample and an isolated urine sample to be used for the determination of fasting serum insulin and microalbuminuria. The samples were collected after 10–12 h fasting and were analyzed in addition to the standard tests pre-defined by the check-up program of Hospital Alemão Oswaldo Cruz (São Paulo), at no additional cost to customers, companies, or healthcare providers.
Patients were considered normal if they had no previous diagnosis of the conditions considered criteria for MetS and which were not on regular use of drugs to treat them. Patients were diagnosed with MetS if they fulfilled the diagnostic criteria according to IDF criteria.
The standard laboratory analyses were conducted on the day of the allocated appointment, with their respective evaluation methods and reference values considered by the analysis laboratory, and included:
• Creatinine, kinetic method, colorimetric
• Blood glucose: enzymatic method
• Fasting insulin: electro chemiluminometric assay
• HOMA-IR (Homeostatic Model Assessment for Insulin Resistance
• HDL-C (high density lipoprotein cholesterol): homogeneous enzyme assay
• Triglycerides: enzymatic assay
• Microalbumin in an isolated urine sample: by immunoturbidimetry (mg/g creatinine).
In addition, hepatic steatosis was assessed using abdominal ultrasound by the same team and equipment.
Statistical analysis
The D’Agostino-Pearson omnibus and Shapiro–Wilk tests were used to assess the distribution of variables. Variables with parametric distribution were expressed as mean ± standard deviation and compared using the Student’s t-test when in two groups and using analysis of variance (ANOVA) when in three or more groups. Where data distributions were non-parametric, the variables were expressed as median and interquartile ranges, and compared using the Mann–Whitney U test for two groups or the Kruskal–Wallis test among three or more groups. Nominal variables were expressed as absolute and percentage counts and were analyzed using the Chi-squared or Fisher’s exact test. We used the analysis of Receiver Operator Characteristics (ROC) curves to evaluate the accuracy of insulin and HOMA-IR values for the prediction of metabolic syndrome for male and female patients. Values of p < 0.05 or, in the case of multiple comparisons, q less than 0.05 were considered statistically significant. Statistical analyses were performed using GraphPad Prism version 8.00 (GraphPad Software, San Diego, CA, United States) and SPSS 25.0 (IBM Corp, Armonk, NY, United States) software programs.
Results
The cohort of 1,015 adult study participants (751 men, 264 women) had a mean age of 46.5 ± 8.9 years old. The baseline characteristics of patients are described on Table 1. The relationship between ranges of two anthropometric parameters (BMI, Waist girth) compared with insulin and HOMA-IR are described on Table 2.
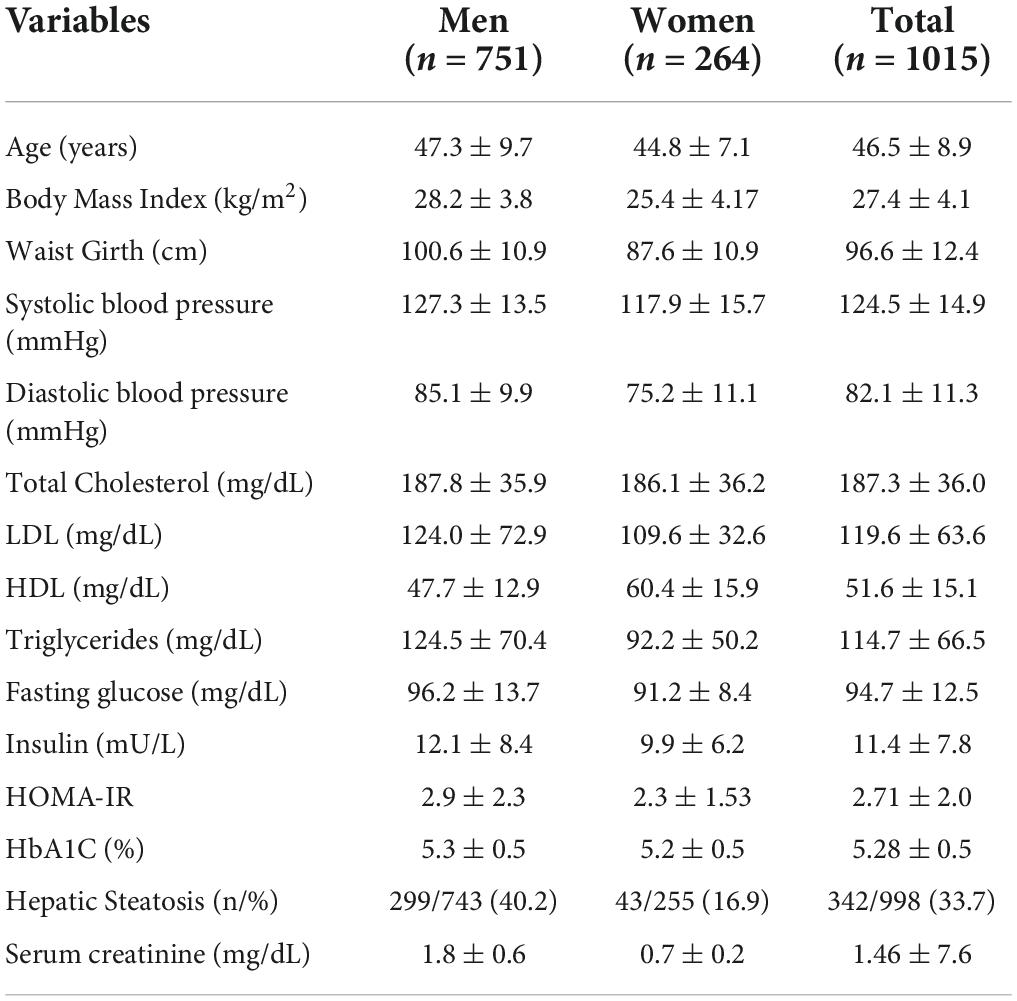
Table 1. Baseline characteristics of patients.
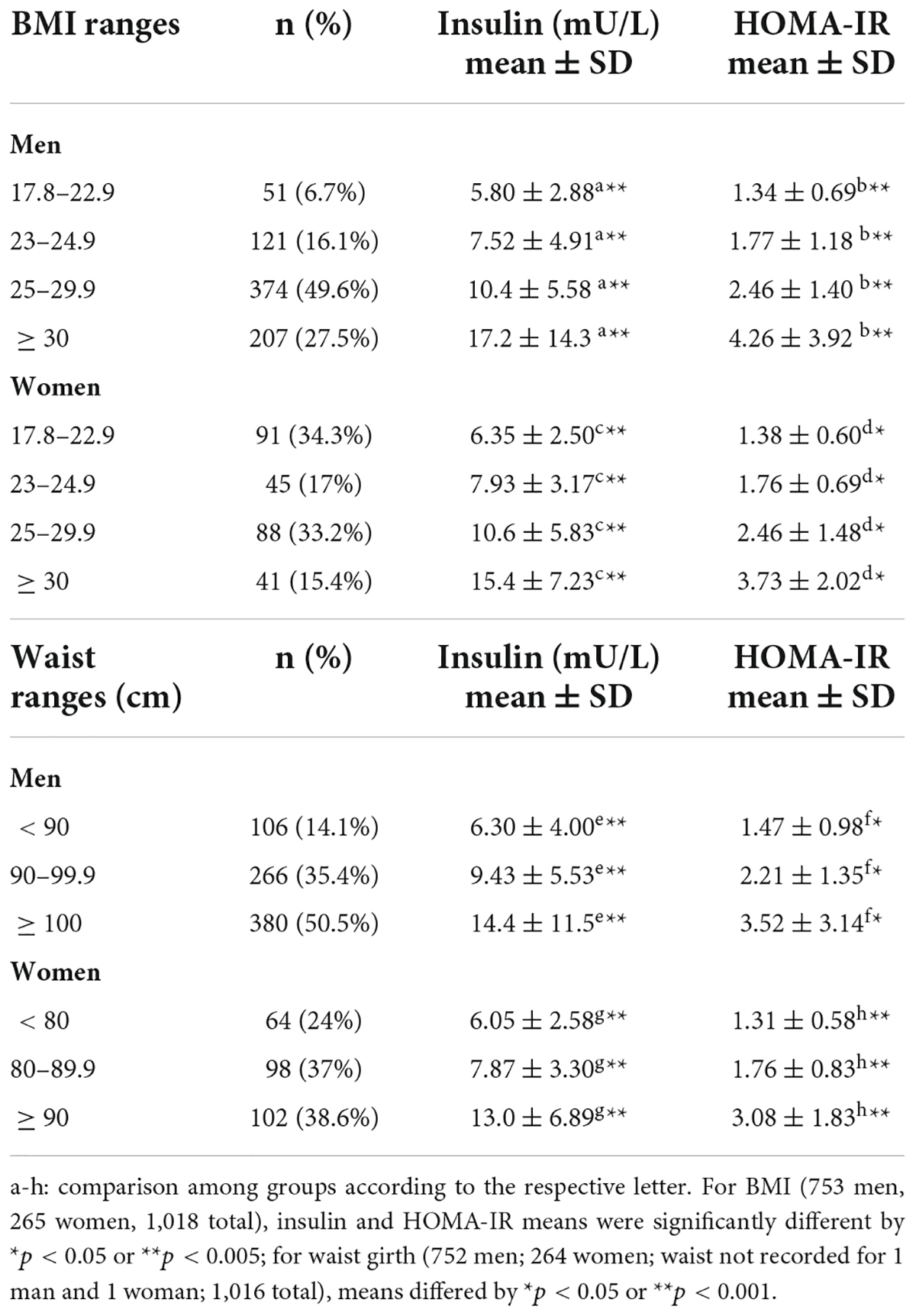
Table 2. Anthropometric parameters of BMI and Waist Girth compared to insulin and HOMA-IR in men and women.
The lowest ranges of these two anthropometric parameters were used to define normal insulin and HOMA-IR values: BMI < 23 for men and women; Waist < 90 cm and < 80 cm for men and women, respectively. These anthropometric normal ranges were then combined in an analysis with the five IDF criteria for MetS (Table 2).
Based on the mean + 2 SD values for insulin and HOMA-IR observed in Table 3, as well as a ROC curve co-ordinates, we defined the following diagnostic cut-offs for hyperinsulinemia (and raised HOMA-IR): Men ≥ 8 mU/L (sensitivity: 82.4% and specificity: 58%) and HOMA-IR ≥ 1.5 (sensitivity: 91.3% and specificity: 51%) and Women ≥ 10 mU/L (sensitivity: 78.6% and specificity: 72.5%) and HOMA-IR ≥ 2.0 (sensitivity: 83.9% and specificity: 70.2%).
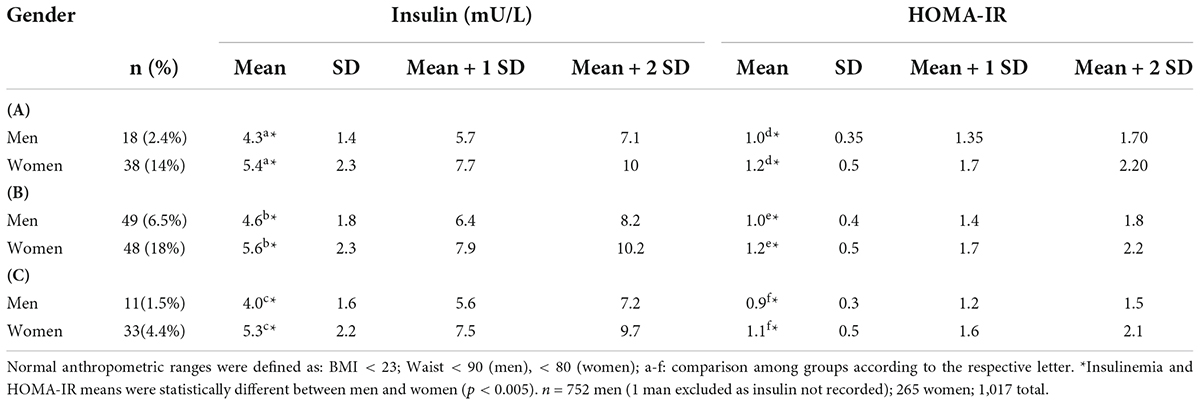
Table 3. Insulin and HOMA-IR values of participants with: (A) normal anthropometric parameters (BMI and Waist); (B) no IDF criteria; or (C) normal anthropometric parameters (BMI and Waist) and no IDF criteria.
Based on those data, a new classification for diagnosis of MetS is proposed:
• Metabolically normal: fasting insulinemia Men < 8 mU/L, Women < 10 mU/L, and no IDF criteria for the diagnosis of MetS.
• Level 1 MetS: hyperinsulinemia, plus one or two IDF criteria for the diagnosis of MetS.
• Level 2 MetS: hyperinsulinemia, plus three or more IDF criteria for the diagnosis of MetS.
The proportion of metabolically normal and MetS patients (Level 1 and Level 2) according to insulinemia below and above the established cut-off may be observed in Figure 1. The statistical differences for the men with insulinemia ≥ 8 mU/L were highly significant (p < 0.001) between normal, Level 1 MetS, and Level 2 MetS. These highly significant trends were repeated for women with insulin ≥ 10 mU/L.
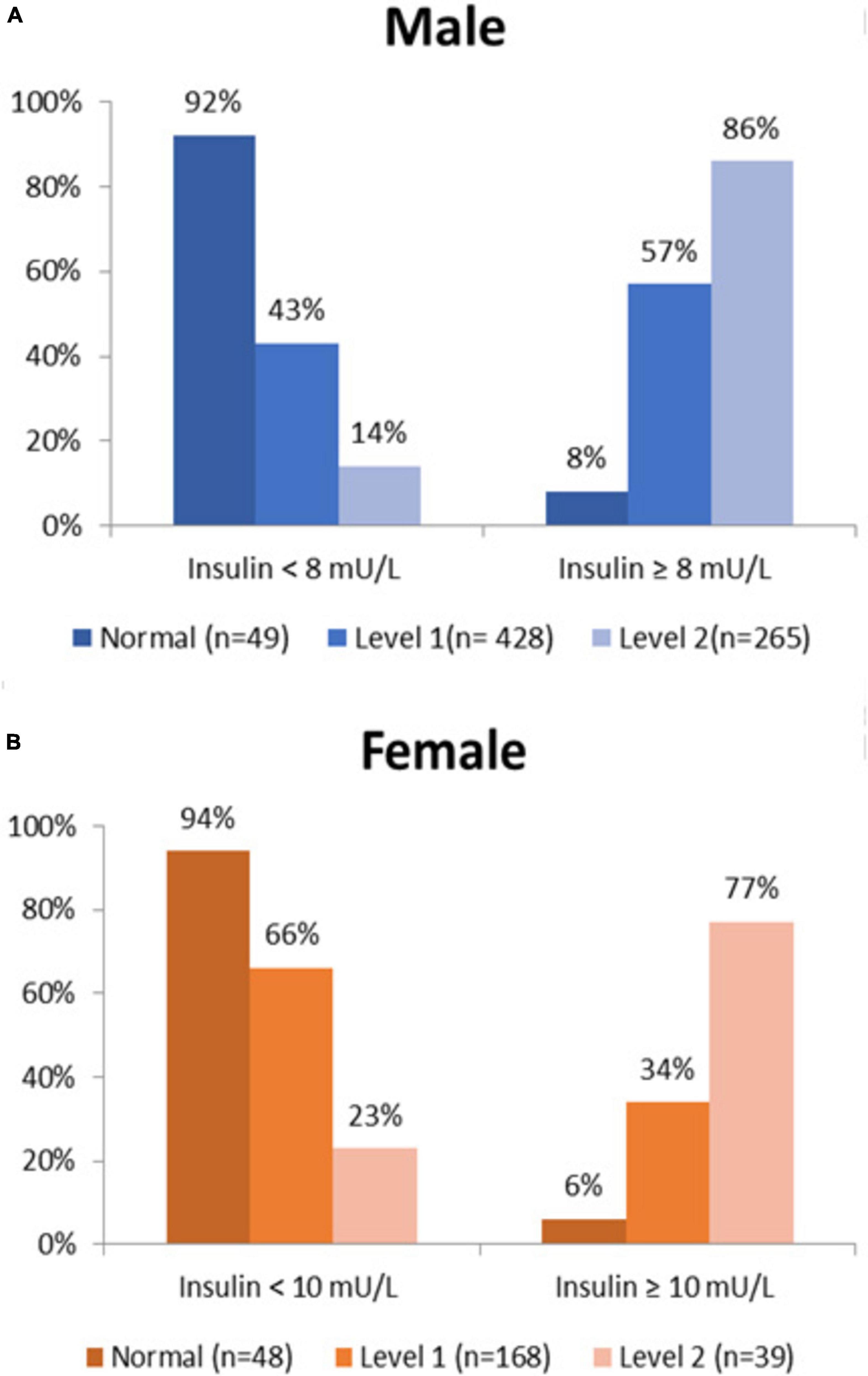
Figure 1. Proportion of normal and MetS patients vs. insulin cut-offs for (A) men and (B) women.
The participants were then conveniently subdivided into insulin ranges from 2–4, 5–7, 8–10, 11–15 and ≥ 16 mU/L (Figure 2). This showed a lower percentage of normal individuals and a higher percentage of patients with MetS in parallel with the increase in serum insulin values.
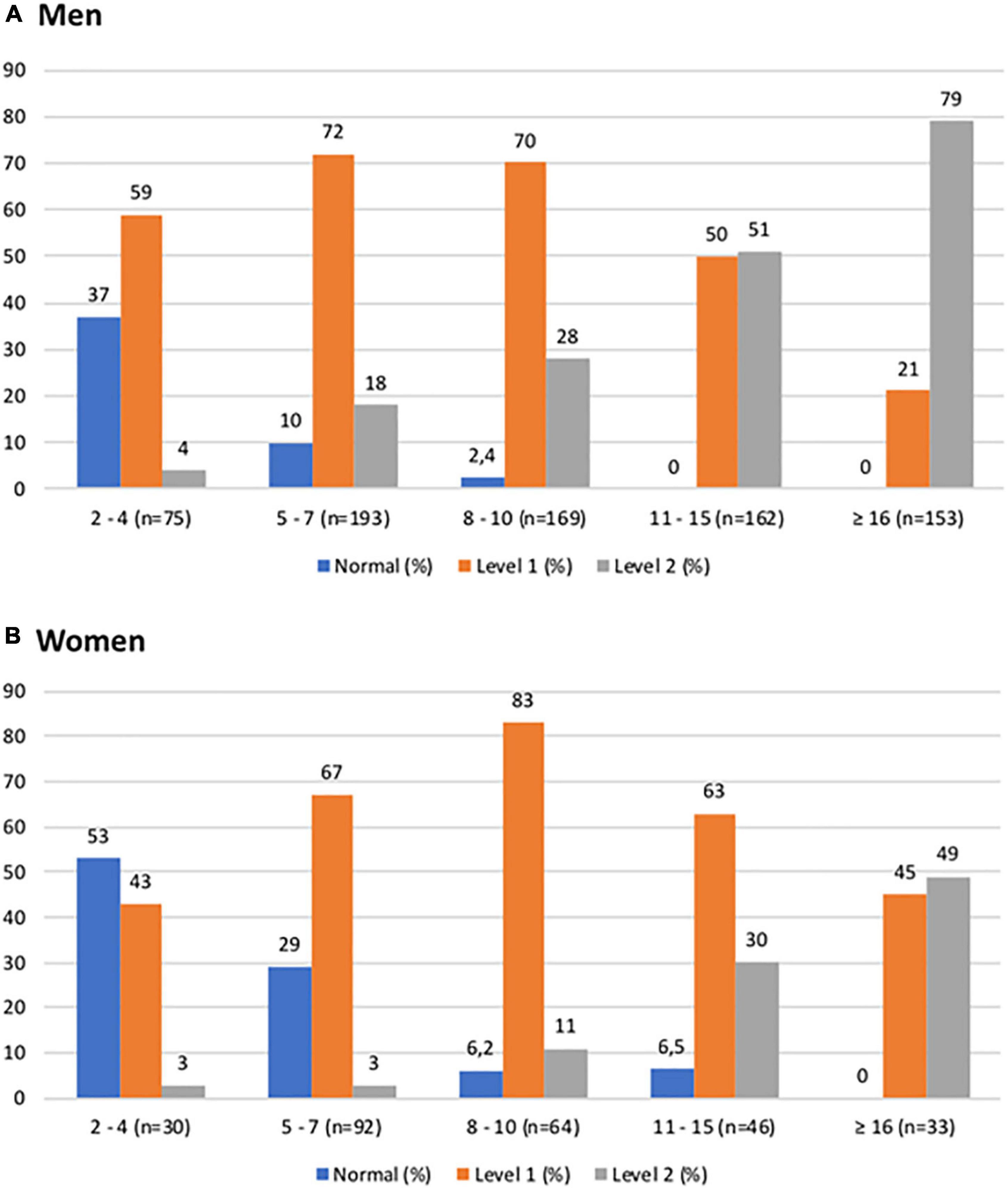
Figure 2. Proportion of patients classified as normal, Level 1 MetS, or Level 2 MetS, vs. ranges of fasting insulin (mU/L) for (A) men and (B) women.
According to our definition (Table 4), metabolically normal individuals are normotensive. The mean insulin concentrations found in both male and female participants with Level 1 MetS and Level 2 MetS were significantly higher than the insulin means of metabolically normal patients. The mean insulin of Level 2 MetS patients was also statistically higher to that of Level 1 MetS (e.g., the higher the MetS level of MetS, the higher the insulin values in men and women). These highly significant differences were also reflected in the HOMA-IR values.
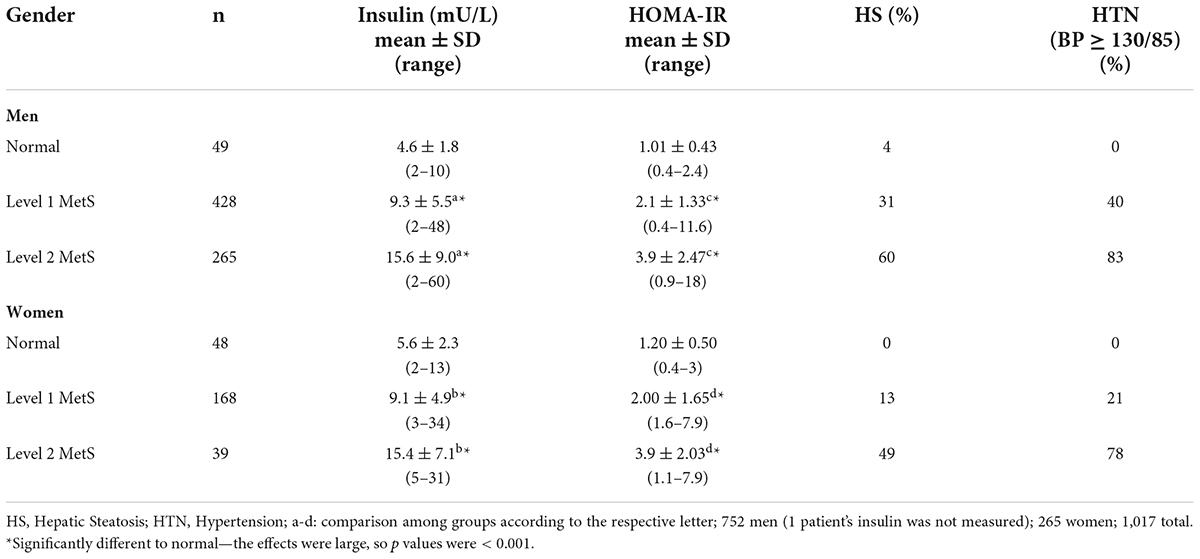
Table 4. Insulin and HOMA-IR parameters in normal, Level 1 MetS, or Level 2 MetS patients, and% hepatic steatosis (HS) and hypertension (HTN) in each group.
Similar trends for insulin and HOMA-IR were also observed for the proportions of hepatic steatosis (HS) in both men and women. However, 10% of men with two normal anthropometric parameters (and 4% of men with no IDF criteria) were found to have hepatic steatosis, possibly related to alcohol intake or another cause. The proportion of patients with hypertension was significantly greater among men with Level 2 MetS compared to men with Level 1 MetS, and this trend was also observed among the women.
As metabolic syndrome may progress to renal failure and albuminuria, renal function was also assessed in the patient cohort by serum creatinine and microalbuminuria. However, no significant differences were found between the normal and MetS groups. This may have been the result of the late evolution of renal complications.
Discussion
The prevalence of metabolic syndrome (MetS) varies between countries and between regions of the same country. In a study conducted in a city in the southern region of Brazil (Paraná State), MetS was confirmed in approximately 50% of the adult population over 40 years of age and in both genders (25). In another study carried out in the city of Niterói (Southeast Region, Brazil), a prevalence of about 60% was observed in older adults, based on the criteria defined by the IDF (26).
MetS is a set of clinical abnormalities which include obesity, hypertension, dyslipidemia, hyperglycemia, and hyperinsulinemia. It is associated with a prolonged subclinical inflammatory process evidenced by a series of biomarkers such as pro-inflammatory cytokines, pro-oxidants, and prothrombotic factors (1, 4, 27–31).
Hyperinsulinemia has long been considered secondary to insulin resistance resulting from an inflammatory process generated by adiposity. However, it has more recently been found to be directly responsible for the inflammatory condition and for obesity (32–37). Insulin has a double action in the endothelium. It normally plays a protective role by increasing the production of nitric oxide, which is an important vasodilator and anti-aggregant that limits the growth of muscle cells. Insulin can also interfere with the release of endothelin ET-1, which is a potent vasoconstrictor. However, the beneficial effects of insulin that predominate under normal conditions are reversed in the face of insulin resistance and hyperinsulinemia (29).
Hyperinsulinemia increases the apoptosis of endothelial progenitor cells that are important for the maintenance of endothelial function and that may promote both muscle cell proliferation and atherogenesis (29, 30, 38, 39). It can also cause a specific form of cardiomyopathy, which is characterized by diastolic dysfunction, fibrosis, and heart failure, regardless of hypertension and atherosclerosis. This is secondary to abnormal coronary microcirculation, and activation of the sympathetic nervous and renin-angiotensin-aldosterone systems (17). It should be noted that hyperinsulinemia is a risk factor regardless of whether the patient is thin or obese, (40) diabetic or not (41).
The presence of hyperinsulinemia is clearly responsible for MetS damage, yet despite this importance, the reference points for insulin levels are variable and often incorrect. Some clinical analysis laboratories have established normal insulin limits up to 25 mU/L, or more. Other authors (37, 42) have defined fasting hyperinsulinemia as insulin levels of above 12 mU/L, while still others have suggested limits below 10 mU/L (43). Hyperinsulinemia has also been defined as the 75th percentile of the sum of the distribution in the normotensive, non-obese group, with normal glycemia (44).
The cut-offs obtained for the diagnosis of hyperinsulinemia (and raised HOMA-IR) in the present study [i.e., Men ≥ 8 mU/L (≥ 1.5), Women ≥ 10 mU/L (≥ 2.0)], are lower than those considered as the reference points by most clinical analysis laboratories. As can be observed, only 8% of men and 6% of women with insulin above the cut-offs defined for the diagnosis of hyperinsulinemia were considered metabolically normal in our cohort.
The proportion of participants considered metabolically normal significantly decreased with insulin values above the cut-offs and increased in participants with Level 1 or Level 2 MetS. This distribution clearly differentiated between the groups, validating the cut-off defined for the diagnosis of hyperinsulinemia, and consolidating the importance of the metabolic classes proposed in this analysis (normal, Level 1, and Level 2 MetS). These data were even more evident in Figure 2, which expanded the hyperinsulinemia ranges.
The various criteria used for diagnosis of MetS and its associated complications certainly do not appear concurrently. Instead, they appear over time and are preceded by prolonged exposure to hyperinsulinemia, which can be an earlier marker of metabolic risk (21–24, 30, 31, 43, 45–49).
A clear definition of the diagnostic cut-off for hyperinsulinemia will allow for early prevention and therapeutic intervention, before the emergence of the recognized and multiple morbidities associated with MetS, such as type 2 diabetes, cardiovascular diseases, and neoplasms. Our proposal to classify individuals as metabolically normal, Level 1 MetS, or Level 2 MetS is aimed at recognizing the clinical importance of hyperinsulinemia and the early stages of the syndrome, regardless of the number of IDF criteria exhibited by a patient.
Insulin values were significantly higher in patients with Level 1 MetS than in those considered metabolically normal (i.e., without any of the five IDF criteria defined previously), as was the prevalence of steatosis and hypertension. This showed that the presence of one or two of the IDF criteria already suggests the presence of insulin resistance and metabolic dysfunction. Without effective medical intervention, these individuals will likely develop MetS to its fullest extent over time, as evidenced by participants with Level 2 MetS who had even greater hyperinsulinemia and/or HOMA-IR values, and a higher prevalence of HTN and HS, compared to patients with Level 1 MetS. No significant changes in renal function, as assessed by the means for serum creatinine or microalbuminuria, were detected between the normal vs. the MetS groups, probably because these are late complications.
Our study has some limitations. First, it is a retrospective study with data from Brazilian patients who underwent annual check-up exams, which makes the study findings valid only for Brazil. However, such design of study can serve as a model for other countries and, perhaps, contribute to standardization of insulin reference levels at a global level. In addition, there is no information about the dietary and physical activity patterns of these individuals what may contribute to the MetS.
In summary, studies to evaluate the benefits of an early approach of patients with fasting insulin values above normal cut-offs, i.e., 8 mU/L in men and 10 mU/L in women (and/or HOMA-IR upper limits of 1.5 and 2.0), despite the number of diagnostic criteria for MetS (Level 1 MetS) to reduce cardiovascular events are necessary.
Data availability statement
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
This study was approved by the ethics and research committee of Hospital Alemão Oswaldo Cruz de São Paulo (CAAE: 46489021.6.0000.0070). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
PC: conception and design, data acquisition, analysis and interpretation, drafting the article, critically revising the article, funding acquisition, and supervision of the research group. JD: data interpretation, drafting the article, and critically revising the article. VS, PM, and AC-N: data analysis and interpretation, drafting the article, and critically revising the article. SM, ÉO, LP, AB, and FS: data analysis and interpretation and critically revising the article. All authors have read and approved the final version of the manuscript.
Funding
This work was supported by Hospital Alemão Oswaldo Cruz.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
BMI, Body mass index; HDL-C, high density lipoprotein cholesterol; HS, hepatic steatosis; HOMA-IR, Homeostatic Model Assessment for Insulin Resistance; HTN, Hypertension; IDF, International Diabetes Federation; MetS, Metabolic Syndrome.
References
1. Saltiel AR, Olefsky JM. Inflammatory mechanisms linking obesity and metabolic disease. J Clin Invest. (2017). 127:1–4. doi: 10.1172/JCI92035
3. Svarovskaya AV, Teplyakov AT, Gusakova AM, Garganeeva AA. Role of markers of inflammation and endothelial dysfunction in the prognosis of the development of cardiovascular complications in patients with coronary artery disease and metabolic syndrome after coronary stenting. Kardiologiia. (2020) 60:98–105. doi: 10.18087/cardio.2020.8.n966
4. Yudkin JS. Inflammation, obesity, and the metabolic syndrome. Horm Metab Res. (2007) 39:707–9. doi: 10.1055/s-2007-985898
5. Ansarimoghaddam A, Adineh HA, Zareban I, Iranpour S, HosseinZadeh A, Kh F. Prevalence of metabolic syndrome in Middle-East countries: Meta-analysis of cross-sectional studies. Diabetes Metab Syndr. (2018) 12:195–201. doi: 10.1016/j.dsx.2017.11.004
6. Owen JG, Reisin E. Anti-hypertensive drug treatment of participants with and the metabolic syndrome and obesity: a review of evidence, meta-analysis, post hoc and guidelines publications. Curr Hypertens Rep. (2005) 17:558. doi: 10.1007/s11906-015-0558-9
7. Olshansky SJ, Passaro DJ, Hershow RC, Layden J, Carnes BA, Brody J, et al. A potential decline in life expectancy in the United States in the 21st century. N Engl J Med. (2005) 352:1138–45. doi: 10.1056/NEJMsr043743
8. Legeza B, Marcolongo P, Gamberucci A, Varga V, Bánhegyi G, Benedetti A, et al. Fructose, glucocorticoids and adipose tissue: implications for the metabolic syndrome. Nutrients. (2017) 9:426. doi: 10.3390/nu9050426
9. Rask-Madsen C, Kahn CR. Tissue-specific insulin signaling, metabolic syndrome, and cardiovascular disease. Arterioscler Thromb Vasc Biol. (2012) 32:2052–9. doi: 10.1161/ATVBAHA.111.241919
10. Balkau B, Charles MA. Comment on the provisional report from the WHO consultation. European Group for the Study of Insulin Resistance (EGIR). Diabet Med. (1999) 16:442–3. doi: 10.1046/j.1464-5491.1999.00059.x
11. Bloomgarden ZT. American Association of Clinical Endocrinologists (AACE) consensus conference on the insulin resistance syndrome: 25-26 August 2002, Washington, DC. Diabetes Care. (2003) 26:933–9. doi: 10.2337/diacare.26.3.933
12. Zimmet P, Magliano D, Matsuzawa Y, Alberti G, Shaw J. The metabolic syndrome: a global public health problem and a new definition. J Atheroscler Thromb. (2005) 12:295–300. doi: 10.5551/jat.12.295
13. Huang PL. A comprehensive definition for metabolic syndrome. Dis Model Mech. (2009) 2:231–7. doi: 10.1242/dmm.001180
14. Choudhary S, Pradhan D, Pandey A, Khan MK, Lall R, Ramesh V, et al. The association of metabolic syndrome and psoriasis: a systematic review and meta-analysis of observational study. Endocr Metab Immune Disord Drug Targets. (2020) 20:703–17. doi: 10.2174/1871530319666191008170409
15. Feng Y, Yang H. Metformin - a potentially effective drug for gestational diabetes mellitus: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. (2017) 30:1874–81. doi: 10.1080/14767058.2016.1228061
16. Gacci M, Russo GI, De Nunzio C, Sebastianelli A, Salvi M, Vignozzi L, et al. Meta-analysis of metabolic syndrome and prostate cancer. Prostate Cancer Prostatic Dis. (2017) 20:146–55. doi: 10.1038/pcan.2017.1
17. Jia G, DeMarco VG, Sowers JR. Insulin resistance and hyperinsulinaemia in diabetic cardiomyopathy. Nat Rev Endocrinol. (2016) 12:144–53. doi: 10.1038/nrendo.2015.216
18. Lithell HO. Effect of antihypertensive drugs on insulin, glucose, and lipid metabolism. Diabetes Care. (1991) 14:203–9. doi: 10.2337/diacare.14.3.203
19. Owen JG, Reisin E. Anti-hypertensive drug treatment of patients with and the metabolic syndrome and obesity: a review of evidence, meta-analysis, post hoc and guidelines publications. Curr Hypertens Rep. (2015) 17:558. doi: 10.1007/s11906-015-0558-9
20. Thomas G, Sehgal AR, Kashyap SR, Srinivas TR, Kirwan JP, Navaneethan SD. Metabolic syndrome and kidney disease: a systematic review and meta-analysis. Clin J Am Soc Nephrol. (2011) 6:2364–73. doi: 10.2215/CJN.02180311
21. Wang F, Han L, Hu D. Fasting insulin, insulin resistance and risk of hypertension in the general population: A meta-analysis. Clin Chim Acta. (2017) 464:57–63. doi: 10.1016/j.cca.2016.11.009
22. Wang Y, Qiao S, Han DW, Rong XR, Wang YX, Xue JJ, et al. Telmisartan improves insulin resistance: a meta-analysis. Am J Ther. (2018) 25:e642–51. doi: 10.1097/MJT.0000000000000733
23. Xun P, Wu Y, He Q, He K. Fasting insulin concentrations and incidence of hypertension, stroke, and coronary heart disease: a meta-analysis of prospective cohort studies. Am J Clin Nutr. (2013) 98:1543–54. doi: 10.3945/ajcn.113.065565
24. Yin DT, He H, Yu K, Xie J, Lei M, Ma R, et al. The association between thyroid cancer and insulin resistance, metabolic syndrome and its components: A systematic review and meta-analysis. Int J Surg. (2018) 57:66–75. doi: 10.1016/j.ijsu.2018.07.013
25. Bortoletto MSS, Souza RKT, Cabrera MAS, González AD. Metabolic syndrome, components and associated factors in adults aged 40 years or older from a city in southern Brazil. Cadernos Saúde Coletiva. (2016) 24:32–40.
26. Saad MA, Cardoso GP, Martins Wde A, Velarde LG, Cruz Filho RA. Prevalence of metabolic syndrome in elderly and agreement among four diagnostic criteria. Arq Bras Cardiol. (2014) 102:263–9. doi: 10.5935/abc.20140013
27. Ahmad R, Thomas R, Kochumon S, Sindhu S. Increased adipose tissue expression of IL-18R and its ligand IL-18 associates with inflammation and insulin resistance in obesity. Immun Inflamm Dis. (2017) 5:318–35. doi: 10.1002/iid3.170
28. Gluvic Z, Zaric B, Resanovic I, Obradovic M, Mitrovic A, Radak D, et al. Link between Metabolic Syndrome and Insulin Resistance. Curr Vasc Pharmacol. (2017) 15:30–9. doi: 10.2174/1570161114666161007164510
29. Janus A, Szahidewicz-Krupska E, Mazur G, Doroszko A. Insulin resistance and endothelial dysfunction constitute a common therapeutic target in cardiometabolic disorders. Mediat Inflamm. (2016) 2016:3634948. doi: 10.1155/2016/3634948
30. Montecucco F, Steffens S, Mach F. Insulin resistance: a proinflammatory state mediated by lipid-induced signaling dysfunction and involved in atherosclerotic plaque instability. Mediat Inflamm. (2008) 2008:767623. doi: 10.1155/2008/767623
31. Srikanthan K, Feyh A, Visweshwar H, Shapiro JI, Sodhi K. Systematic review of metabolic syndrome biomarkers: a panel for early detection, management, and risk stratification in the west virginian population. Int J Med Sci. (2016) 13:25–38. doi: 10.7150/ijms.13800
32. Gray SL, Donald C, Jetha A, Covey SD, Kieffer TJ. Hyperinsulinemia precedes insulin resistance in mice lacking pancreatic beta-cell leptin signaling. Endocrinology. (2010) 151:4178–86. doi: 10.1210/en.2010-0102
33. Kitamura T, Kahn CR, Accili D. Insulin receptor knockout mice. Annu Rev Physiol. (2003) 65:313–32. doi: 10.1146/annurev.physiol.65.092101.142540
34. Odeleye OE, de Courten M, Pettitt DJ, Ravussin E. Fasting hyperinsulinemia is a predictor of increased body weight gain and obesity in Pima Indian children. Diabetes. (1997) 46:1341–5. doi: 10.2337/diab.46.8.1341
35. Pedersen DJ, Guilherme A, Danai LV, Heyda L, Matevossian A, Cohen J, et al. A major role of insulin in promoting obesity-associated adipose tissue inflammation. Mol Metab. (2015) 4:507–18. doi: 10.1016/j.molmet.2015.04.003
36. van Vliet S, Koh HE, Patterson BW, Yoshino M, LaForest R, Gropler RJ, et al. Obesity Is Associated With Increased Basal and Postprandial β-Cell Insulin Secretion Even in the Absence of Insulin Resistance. Diabetes. (2020) 69:2112–9. doi: 10.2337/db20-0377
37. Zhang AMY, Wellberg EA, Kopp JL, Johnson JD. Hyperinsulinemia in obesity, inflammation, and cancer. Diabetes Metab J. (2021) 45:285–311. doi: 10.4093/dmj.2020.0250
38. Tan Q, Li Y, Li X, Zhang S. Hyperinsulinemia impairs functions of circulating endothelial progenitor cells. Acta Diabetol. (2019) 56:785–95. doi: 10.1007/s00592-019-01314-9
39. Weidmann P, Bohlen L, de Courten M. Insulin resistance and hyperinsulinemia in hypertension. J Hypertens. (1995) 13:S65–72. doi: 10.1097/00004872-199508001-00010
40. Tsujimoto T, Kajio H, Sugiyama T. Association between hyperinsulinemia and increased risk of cancer death in nonobese and obese people: A population-based observational study. Int J Cancer. (2017) 141:102–11. doi: 10.1002/ijc.30729
41. Kim NH, Chang Y, Lee SR, Ryu S, Kim HJ. Glycemic status, insulin resistance, and risk of pancreatic cancer mortality in individuals with and without diabetes. Am J Gastroenterol. (2020) 115:1840–8. doi: 10.14309/ajg.0000000000000956
42. McAuley KA, Williams SM, Mann JI, Walker RJ, Lewis-Barned NJ, Temple LA, et al. Diagnosing insulin resistance in the general population. Diabetes Care. (2001) 24:460–4. doi: 10.2337/diacare.24.3.460
43. Szybiński Z, Szurkowska M. Insulinemia–a marker of early diagnosis and control of efficacy of treatment of type II diabetes. Pol Arch Med Wewn. (2001) 106:793–800.
44. Modan M, Halkin H, Almog S, Lusky A, Eshkol A, Shefi M, et al. Hyperinsulinemia. A link between hypertension obesity and glucose intolerance. J Clin Invest. (1985) 75:809–17. doi: 10.1172/JCI111776
45. Fernández-Real JM, Ricart W. Insulin resistance and chronic cardiovascular inflammatory syndrome. Endocr Rev. (2003) 24:278–301. doi: 10.1210/er.2002-0010
46. Laakso M. Cardiovascular disease in type 2 diabetes: challenge for treatment and prevention. J Intern Med. (2001) 249:225–35. doi: 10.1046/j.1365-2796.2001.00789.x
47. McDonagh MS, Dana T, Selph S, Devine EB, Cantor A, Bougatsos C, et al. Treatments for Schizophrenia in Adults: A Systematic Review [Internet]. Rockville, MD: Agency for Healthcare Research and Quality (2017).
48. Sarafidis PA, Bakris GL. Review: Insulin and endothelin: an interplay contributing to hypertension development? J Clin Endocrinol Metab. (2007) 92:379–85. doi: 10.1210/jc.2006-1819
Keywords: diabetes, HOMA-IR, insulin, hyperinsulinemia, obesity, metabolic syndrome
Citation: Chocair PR, de Menezes Neves PDM, Sato VAH, Mohrbacher S, Oliveira ÉS, Pereira LVB, Bales AM, da Silva FP, Duley JA and Cuvello-Neto AL (2022) Proposal for standardizing normal insulin ranges in Brazilian patients and a new classification of metabolic syndrome. Front. Med. 9:984001. doi: 10.3389/fmed.2022.984001
Received: 01 July 2022; Accepted: 23 August 2022;
Published: 09 September 2022.
Edited by:
I-Shiang Tzeng, National Taipei University, TaiwanReviewed by:
Serena Cabaro, University of Naples Federico II, ItalyRavindra Shukla, All India Institute of Medical Sciences Jodhpur, India
Copyright © 2022 Chocair, de Menezes Neves, Sato, Mohrbacher, Oliveira, Pereira, Bales, da Silva, Duley and Cuvello-Neto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pedro Renato Chocair, cGVkcm9jaG9jYWlyQHlhaG9vLmNvbS5icg==