 Anna Gabriela Rezende1†
Anna Gabriela Rezende1† Jefferson Valente2†
Jefferson Valente2† Cássia da Luz Goulart2,3
Cássia da Luz Goulart2,3 Fernanda Facioli1
Fernanda Facioli1 Bernardo Maia2
Bernardo Maia2 Victor Irungu Mwangi2
Victor Irungu Mwangi2 Hector Bonilla4
Hector Bonilla4 Frits M. E. Franssen5
Frits M. E. Franssen5 Camila Miriam Suemi Sato Barros do Amaral2,6Thaís Jordão Perez Sant'Anna Motta1Marcia Alexandre2,7Luiz Carlos de Lima Ferreira1,7
Camila Miriam Suemi Sato Barros do Amaral2,6Thaís Jordão Perez Sant'Anna Motta1Marcia Alexandre2,7Luiz Carlos de Lima Ferreira1,7 Gerson Cipriano Junior3
Gerson Cipriano Junior3 Guilherme Peixoto Tinoco Arêas1
Guilherme Peixoto Tinoco Arêas1 Fernando Almeida-Val1,2,7*†
Fernando Almeida-Val1,2,7*†- 1Universidade Federal do Amazonas, Manaus, Brazil
- 2Universidade do Estado do Amazonas, Manaus, Brazil
- 3Universidade de Brasília, Brasília, Brazil
- 4Stanford University, Stanford, CA, United States
- 5Maastricht University Medical Center, Maastricht, Netherlands
- 6Hospital e Pronto Socorro 28 de Agosto, Manaus, Brazil
- 7Fundação de Medicina Tropical Dr. Heitor Vieira Dourado, Manaus, Brazil
Introduction: It has been postulated that individuals with long COVID have reduced exercise capacity, just as people living with HIV (PLWH), although having even lower exercise capacity. The extent to which long COVID in PLWH resembles long COVID in individuals who presented different COVID-19 phenotypes is unknown, so we aimed to determine if the long COVID profile in PLWH resembled the symptoms experienced by individuals with long COVID following mild/moderate or severe acute COVID-19, 2 years after the initial disease.
Material and methods: A pulmonary function test and a 6-min walk test (6MWT) were performed on adult individuals with PACS (Post-Acute COVID Syndrome) in 3 groups: COVID-19+PLWH (plwHCOV), mild/moderate COVID-19 (mmCOV); severe COVID-19 (seCOV).
Results: Sixty three individuals were included: plwHCOV (n = 12), mmCOV (n = 33) and seCOV (n = 18). Across all groups, males were predominant. BMI was 25 ± 3, 28 ± 4, and 32 ± 7 kg/m2 in plwHCOV, mmCOV, and seCOV, respectively (p = 0.003). The plwHCOV walked 545 m (±93) at the 6MWT, which was comparable to the mmCOV group (555 m ± 63) but significantly higher than the seCOV group (435 m ± 84) (p < 0.0001). The plwHCOV group had worse forced expiratory volume in 1st second (FEV1%, 80 ± 12) (p < 0.0001), forced vital capacity (FVC%, 83 ± 11) (p = 0.002) and FEV1/FVC (0.80 ± 0.1, p = 0.004) when compared to the seCOV group. Interestingly, PLWH had comparable 6MWT, FEV1, FVC, and FEV1/FVC results as mmCOV.
Conclusion: Our results indicate that even 2 years post-COVID-19 infection, PLWH exhibits significantly decreased spirometry compared to the seCOV group. Despite this lung function impairment, their functional capacity was similar to individuals with PACS following mild/moderate COVID-19.
Introduction
COVID-19 and HIV/AIDS are among the most impactful viral diseases of global concern in recent history (1), both of which are known to affect functional and respiratory capacity (2, 3). While most patients recover from acute COVID-19, ~1 in 10 develop long COVID symptoms that can persist for months (4, 5). More than 200 symptoms and conditions, such as postural orthostatic tachycardia syndrome (PoTS) and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), have been associated with long COVID (6). Definitions vary across agencies: the CDC/NIH considers symptoms lasting 4 or more weeks (7), WHO/NICE defines it as symptoms persisting for at least 2 months after 3 months from infection (8), and the RECOVER initiative extends this window to 6 months (6).
Although most long COVID studies focus on prevalence and symptom description in the general population (6, 9–12), fewer have investigated its long-term functional consequences, mainly using objective measures (13, 14). Reduced exercise capacity has been postulated as a hallmark of long COVID (13), yet little is known about how this manifests in specific vulnerable groups.
Globally, nearly 39 million people live with HIV, with rising numbers in Latin America (15, 16). Advances in antiretroviral therapy (ART) have reduced morbidity and mortality (17), but people living with HIV (PLWH) increasingly face challenges such as chronic disease, reduced quality of life, and functional decline linked to viral persistence, frailty, and systemic deterioration (18, 19). Recent evidence suggests that PLWH are at increased risk of developing long COVID, regardless of ART status, CD4 count, or viral load (20, 21). A recent systematic review and meta-analysis further confirmed that HIV infection is associated with a higher likelihood of developing long COVID, with common symptoms including fatigue, cough, and asthenia, and evidence of impaired lung function and immune dysregulation in this population (21).
Despite this elevated risk, the functional profile of PLWH with long COVID remains poorly understood, particularly in comparison to individuals without HIV who experienced different severities of acute COVID-19. Most available studies rely on subjective self-reports, highlighting the need for studies that use objective assessments. Therefore, the present study aims to evaluate the functional profile of PLWH with long COVID in comparison to individuals with long COVID who had mild/moderate or severe acute COVID-19, more than 2 years after initial infection.
Methods
Study design and setting
This retrospective cross-sectional study involved 63 individuals of both sexes, over 18 years old, and residents of Manaus. It was conducted at the Federal University of Amazonas (UFAM) in Manaus, Brazil. All individuals had the first confirmed SARS-CoV-2 infection before the vaccine roll-out in Manaus, which started in January 2021.
Eligibility criteria and study groups
People living with HIV, who had an undetectable viral load (<40 cells/ml), with at least 6 months of adherence to antiretroviral therapy (ART), who had mild/moderate COVID-19 in 2020, and with no history of respiratory or neurological diseases comprised the plwHCOV group, totaling 12 individuals. The comparative groups of people not living with HIV were mmCOV (mild/moderate COVID-19, a total of 33 individuals) and seCOV (severe COVID-19, a total of 18 individuals). The severity of COVID-19 was defined by the provisional clinical guidance of the World Health Organization (WHO) (22). Overall, clinically unstable individuals presenting musculoskeletal, neurological, or respiratory disorders that affected the performance of functional tests were excluded. All subjects had no current or chronic lung disease or health conditions that would interfere with functional and respiratory assessments. The long COVID-19 definition followed the WHO classification (22) and HIV infection was defined as a positive confirmatory molecular test.
Measurements
Patient clinical data, including age, sex, weight, and height (used to calculate the body mass index, BMI), details on past medical history, comorbidities, persistent symptoms, smoking habits, vital signs, severity of respiratory fatigue by the mMRC (Modified Medical Research Council) dyspnea scale (23) and medication usage were collected to characterize the groups.
Pulmonary function and respiratory muscle strength (RMS)
Spirometry (Cosmed®, Italy) was performed for lung function and was interpreted according to the American Thoracic Society (ATS) and European Respiratory Society (ERS) standards. We measured the forced expiratory volume in 1st second (FEV1) and the forced vital capacity (FVC). The predicted values were calculated according to the ERS equation (24). The FEV1 (L, %), FVC (L, %), and FEV1/FVC (%) were recorded (25). Percent-predicted values were determined as per the proposed recommendations by Alberto et al. (26). Maximum inspiratory pressure (MIP) was obtained after the individual expired to residual volume and performed a maximal effort inspiration against a closed valve, during which the pressure was measured. For the maximum expiratory pressure (MEP) assessment, patients underwent an inspiration to total lung capacity, followed by a maximal effort expiration against a closed valve for 2 s, after which the valve was opened (24).
Functional capacity
This was determined using the 6-min walk test (6MWT), during which participants received standardized verbal encouragement and instructions to walk the maximum distance possible within 6 min along a flat corridor measuring 30 m in length. At the beginning and end of the tests, vital signs are measured for hemodynamic monitoring: Systolic and diastolic blood pressure (SBP and DBP), heart rate (HR), peripheral oxygen saturation (SpO2), and perception of dyspnea (BORG Scale). The test followed the guidelines set by the American Thoracic Society (27). All groups underwent spirometry and 6MWT tests (28).
Quality of life - SF-36
The Short Form Health Survey (SF-36) questionnaire was used to assess the Quality of life among individuals living with HIV. This assessment was conducted at an exploratory level, recognizing the challenges related to stigma and social neglect within the PLWH population. The SF-36 evaluates eight quality-of-life domains, which are categorized into physical (functioning, role limitations-physical, pain, general health) and mental health (vitality, social functioning, role limitations-emotional, and emotional/mental health). Scoring was as outlined by Hays et al. (29). Item scores were converted to a scale ranging from 0 to 100 points, where 0 indicated the poorest perception of health, and 100 reflects the best perception of health. Averaging individual items within the subscale and physical composite and mental health determined the domain scores.
Ethical aspects
The Federal University of Amazonas Institutional Review Board approved this study (CAAE 44971221.7.0000.5020). This adhered to the principles outlined in the Declaration of Helsinki and the Good Clinical Practice guidelines of the International Conference on Harmonization. Eligible before enrollment. They were allowed sufficient time to thoroughly review and sign an informed consent form (ICF).
Statistical analysis
The Shapiro-Wilk and Levene's tests assessed data normality and homogeneity, respectively. The results were presented as mean ± standard deviation, median, and interquartile range, or percentage values. The Chi-square test and ANOVA one-way test post hoc Tukey test were used for group characteristic analyses. Pearson's correlation determined the correlation coefficient between variables, considering indices from 0.1–0.3, 0.4–0.6, and 0.7–0.9 with weak, moderate, and strong associations, respectively (30). A p-value < 0.05 was considered statistically significant. The SPSS software version 23.0 (IBM, Chicago, USA) was used for calculations, and GraphPad Prism software version 8.0 (GraphPad, California, USA) was used for creating the images. The sample size was calculated using G*Power 3.1 software for a Pearson correlation analysis, assuming a moderate effect size (r = 0.5), a significance level of α = 0.05, and a statistical power (1–β) of 0.80. Based on these parameters, the minimum required sample size was estimated at 29 participants. The actual number of participants included in each subgroup provided slightly higher statistical power (~86%), reducing the likelihood of a type II error.
Results
Population characteristics for the plwHCOV group
Participants from the plwHCOV group were predominantly male, above 40 years of age, living with HIV for at least 12 months, and adherent to ART. For a detailed individual description of this group, please see Table 1. Clinical, functional, and lung function characteristics of individuals are detailed in Table 2. The most frequent comorbidity in the plwHCOV group was hypertension, while the most reported medication used daily was Losartan. All participants denied engaging in harmful habits and addictions, as described in Table 1. The FEV1 was 2.6 ± 0.7 L, FEV1 predicted 80 ± 12%, FVC 3.3 ± 0.9 L, FVC predicted 83 ± 11%, FEV1/FVC 0.80 ± 0.1 L/s, MIP 92 ± 39 cmH2O, MEP 105 ± 33 cmH2O. The SF-36 mean total score was 51.9 ± 29.4. Details of the quality-of-life assessment are also available in Table 1.
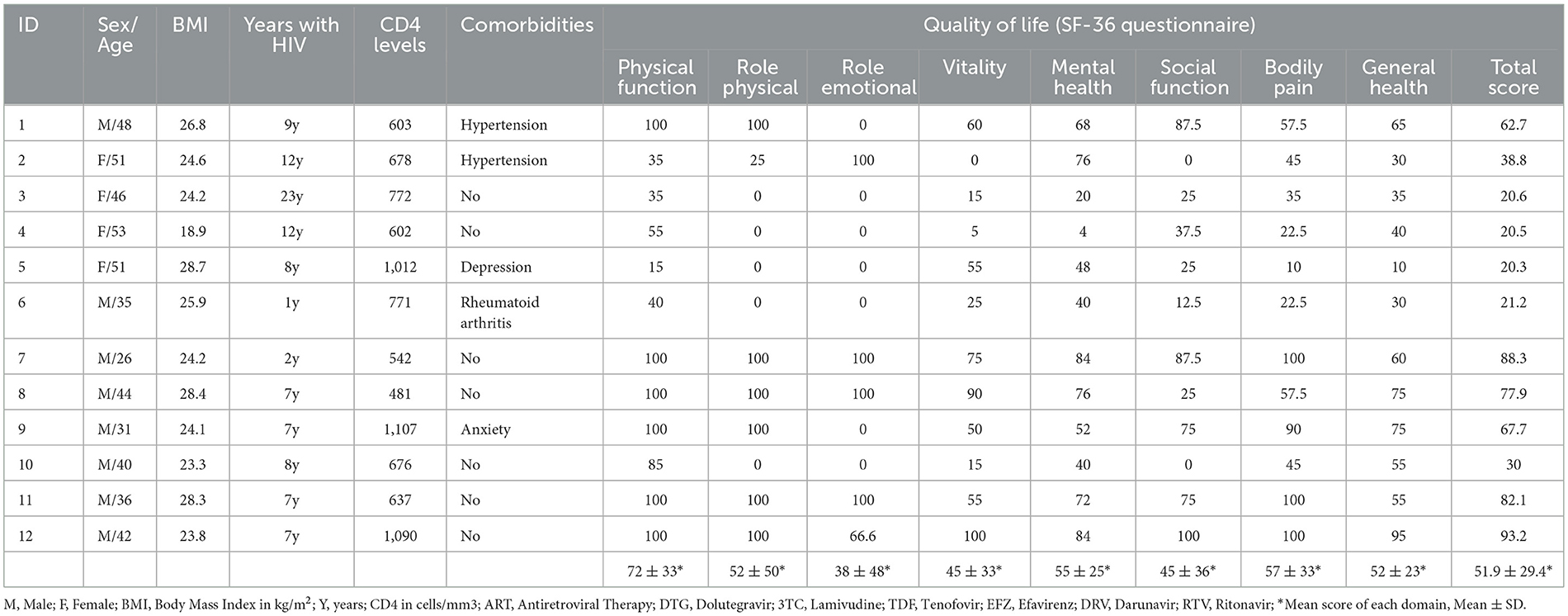
Table 1. Sociodemographic, HIV status and quality of life characteristics of the PLWHCOV group.
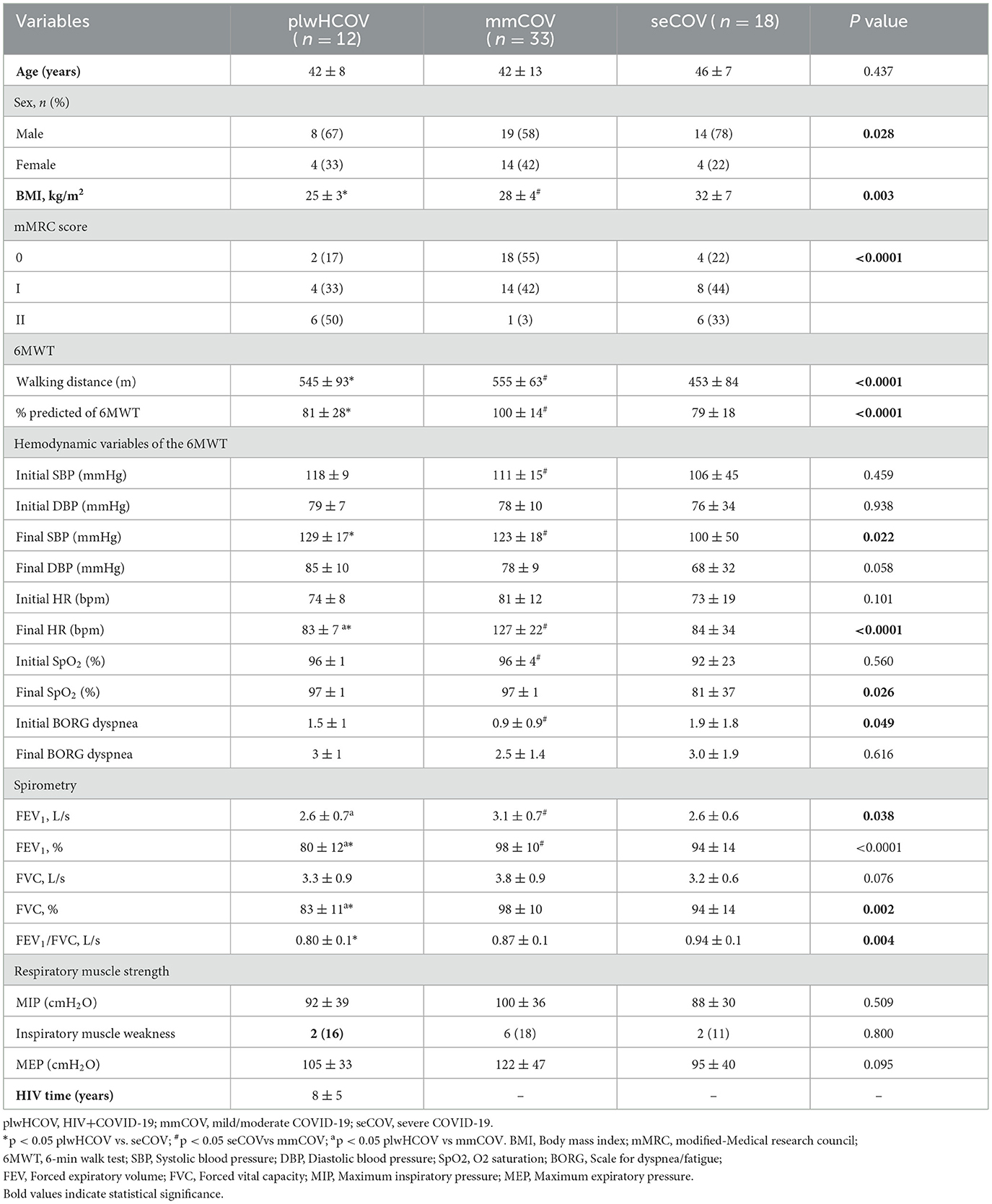
Table 2. Clinical, functional, and lung function characteristics of individuals with COVID.
In the plwHCOV group, we found strong correlations (Figure 1) between D6MWT and MEP (r = 0.700, p = 0.016) and a moderate correlation between SF-36 total score and MEP (cmH2O) (r = 0.633, p = 0.027), demonstrating that respiratory muscle strength directly affects the functional capacity and quality of life.
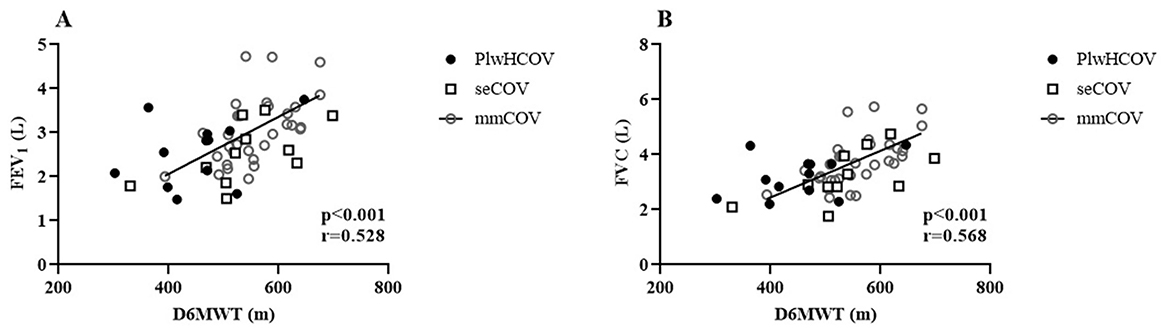
Figure 1. (A) Distance Walked in the 6-Minute Walk Test (D6MWT). (B) Maximum Expiratory Pressure (MEP).
Population characteristics for the mmCOV and seCOV groups
The mmCOV group had an average age of 42 years and a more balanced gender distribution (58% were male). The mean BMI was 28 kg/m2. This group had the best functional performance, covering the longest distance in the 6MWT (555 ± 63 m), reaching 100% of the predicted value. FEV1 (98%) and FVC (98%) were the highest among the groups, indicating better lung function. In the seCOV group, the average age was 46 years, with a male predominance (78%) and the highest BMI (32 kg/m2). Functional capacity was the most impaired, with the shortest 6MWT distance (453 ± 84 m, 79% predicted). Lung function was observed with an FEV1 of 94% and FVC of 94%, along with the highest FEV1/FVC ratio (0.94).
Functional assessment outcomes
The functional assessments in this study were conducted on average 24 ± 5 months after the initial acute COVID-19 in all groups, and all were done before the COVID-19 vaccination roll-out. The proportion of mMRC II scores across groups was 6 (50%), 1 (3%), and 6 (33%) in plwHCOV, mmCOV, and seCOV, respectively. The male sex was predominant across all groups. The plwHCOV group had worse forced expiratory volume in 1st second (FEV1%, 80 ± 12) (p < 0.0001), forced vital capacity (FVC%, 83 ± 11) (p = 0.002) and FEV1/FVC (0.80 ± 0.1, p = 0.004) when compared to the seCOV group. Interestingly, the plwHCOV group responded similarly to the mmCOV group for the 6MWT, FEV1, FVC, and FEV1/FVC (Table 2).
Correlation analysis
We found a moderate correlation association between the walked distance in the 6MWT (6MWD) and FEV1 (L) (r = 0.528, p < 0.001) and D6MWT and FVC (L) (r = 0.568, p < 0.001) (Figure 2) in all three groups. All correlations were tested within the individual populations. For the groups without HIV, the correlation results were: seCOV (p = 0.001, r = 0.60) and mmCOV (p = 0.041, r = 0.61).
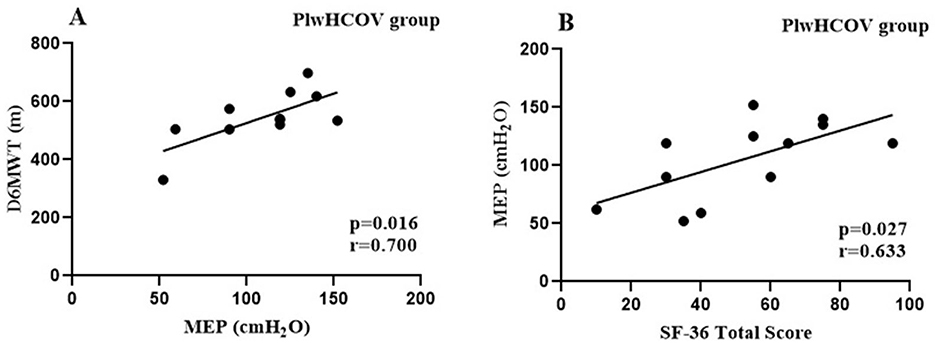
Figure 2. (A) Forced Expiratory Volume in One Second (FEV1). (B) Forced Vital Capacity (FVC).
Discussion
This study showed a significant proportion of individuals living with HIV presenting significant functional and Quality of life deficits long after COVID-19 infection. Comparing the clinical profiles of long COVID between PLWH and individuals who did not live with HIV and had moderate and severe COVID-19, we observed that PLWH presented functional capacity parameters like moderate cases. At the same time, their lung function was worse than individuals who had had severe COVID-19. Furthermore, we observed correlations between respiratory parameters with D6MWT and Quality of life in the group of individuals living with HIV.
The majority of PLH individuals in this study were male and aged above 40 years, similar to other studies (31–36). Here, individuals living with HIV demonstrated a 6MWT walked distance above the average of 400 m previously reported for this population (34). Studies assessing long COVID using the 6MWD outcome report values ranging from 400 to 500 m (13, 37–40) The progression of long COVID-19 is associated with reduced exercise capacity and physical activity levels, which may exacerbate exercise intolerance and ultimately lead to a decline in functional capacity and the ability to perform activities of daily living (41). In this study, the plwHCOV and mmCOV groups showed greater 6MWT distances compared to the seCOV group. Previous studies have shown that severe acute COVID-19 is characterized by more intense symptoms, greater systemic involvement, and longer hospitalization and recovery periods; thus, worse post-illness conditions were expected (11, 37, 42–45). For instance, researchers assessing functional deficiencies post-COVID-19 using the 6MWT in a Mexican population aged above 40 years found that individuals with moderate to severe disease walked shorter distances than those with mild cases, with this decline independently associated with breathing difficulties and respiratory function changes (46). The extent to which the overlap between long COVID and HIV, or the impact of hospitalization and invasive support during severe and critical acute COVID-19, contributes to functional capacity decline in these populations remains largely unknown and warrants further research.
The plwHCOV group also showed reduced lung function compared to the mmCOV group. Previous studies have demonstrated that PLWH may experience pulmonary deficits associated with both HIV itself and opportunistic respiratory conditions (47). In our sample, hypertension was the most frequent comorbidity among PLWH, and losartan was the most commonly used antihypertensive. Although some experimental and preclinical studies have suggested a potential protective effect of losartan against lung fibrosis and inflammation through TGF-β modulation and attenuation of AngII activity (48) these findings have not been supported by robust clinical evidence. A multicenter randomized controlled trial in hospitalized patients with COVID-19 showed that losartan did not improve oxygenation, severity of illness, or other clinical outcomes and even raised concerns about potential adverse effects on hemodynamics and renal function (49). Similarly, a large placebo-controlled trial evaluating losartan in patients with emphysema found no benefit in preventing disease progression or improving pulmonary function (50). Based on this high-quality evidence, it is unlikely that losartan biased pulmonary outcomes in our PLWH group; if anything, its use may have attenuated even poorer results. Importantly, participants in the mmCOV and seCOV groups did not report hypertension or use of losartan, which is shown in the results section to address potential treatment-related confounding.
We also observed a correlation between respiratory muscle strength and the distance walked among PLWH participants, suggesting that respiratory performance directly influences functional capacity, as previously described in the literature (2, 51–53). Collini (54) showed that PLWH on antiretroviral therapy experience faster pulmonary decline than HIV-negative individuals, driven largely by systemic inflammation (55–58). This chronic inflammation, combined with the known respiratory consequences of COVID-19 (22, 59–61), may help explain the reduced lung function observed in the plwHCOV group. The relationship between pulmonary function and functional capacity is well established (38), and our findings reinforce this association, with significant correlations observed between spirometric values and 6MWD across all groups.
Studies have reported that PLWH has lower-than-expected perceptions of Quality of life due to multifactorial factors (62–65); among them, non-use or irregular use of ART was indicative of worse perceptions of Quality of life (66–68). In this study, although the individuals were all on regular ART, their perceptions of Quality of life in the SF-36 questionnaire were below that established in the literature (69). They significantly correlated with the individuals' expiratory muscle strength. Previous studies evaluating respiratory muscle strength in PLWH indicated the influence of respiratory parameters on the general condition of individuals, in addition to the relationship between adequate respiratory muscle strength and Quality of life in other health contexts already established in the literature (19, 70, 71).
Finally, although BMI differed significantly across groups—with higher values in the seCOV group—the spirometry outcomes were expressed as predicted percentages adjusted for age, sex, and height, which minimizes the influence of body composition on interpretation. Moreover, the group with the lowest BMI (plwHCOV) exhibited the most reduced spirometric parameters, suggesting that BMI alone was not the primary factor influencing pulmonary function in this cohort. Nonetheless, we acknowledge that excess body weight may contribute to a restrictive ventilatory pattern in some individuals, particularly within the seCOV group, and this potential influence cannot be entirely excluded.
Our study has some limitations. Due to its cross-sectional design, the study cannot establish causal relationships between the observed outcomes and prior COVID-19 or long COVID. It is therefore unclear whether the reduced functional or respiratory measures observed, particularly in individuals with long COVID, were pre-existing or developed as a consequence of the infection. Additionally, no pre-COVID-19 data on lung function or functional capacity were available for comparison. The relatively small sample size and the fact that this was a single-center study may also limit the generalizability of the findings. Participants were heterogeneous in terms of BMI, which may have influenced the respiratory outcomes. The plwHCOV group was particularly limited in size due to challenges in recruiting individuals living with HIV, many of whom expressed concerns about confidentiality—an issue often driven by persistent social stigma. These concerns also motivated the inclusion of quality of life assessments in this group.
Conclusion
People living with HIV/AIDS showed worse lung function compared to individuals without HIV but had severe COVID-19, yet showed similar results in 6MWT, FEV1, FVC, and FEV1/FVC as those with moderate/mild COVID-19. Our findings highlight persistent deficits in lung function among PLWH even after more than 2 years post-COVID-19 infection, significantly impacting their functional capacity and Quality of life. Targeted interventions involving cardiorespiratory and motor rehabilitation are essential for PLWH experiencing long COVID. Further comprehensive studies are needed to comprehend the contribution of HIV to functional deterioration in long COVID cases.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Federal University of Amazonas Institutional Review Board approved this study (CAAE 44971221.7.0000.5020). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AR: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. JV: Investigation, Supervision, Visualization, Writing – original draft, Writing – review & editing. CG: Methodology, Writing – original draft, Writing – review & editing. FeF: Writing – original draft, Writing – review & editing. BM: Writing – original draft, Writing – review & editing. VM: Writing – original draft, Writing – review & editing. HB: Writing – original draft, Writing – review & editing. FrF: Writing – original draft, Writing – review & editing. CA: Writing – original draft, Writing – review & editing. TM: Writing – original draft, Writing – review & editing. MA: Writing – original draft, Writing – review & editing. LF: Writing – original draft, Writing – review & editing. GC: Writing – original draft, Writing – review & editing. GA: Writing – original draft, Writing – review & editing. FA-V: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study was supported by CAPES (PROCAD Amazonia 88887.200582/2018-00) and CNPq (CNPq/MCTI/CT n°53/2022 and CNPq/MCTI/FNDCT n°18/2021). FA-V received a post-doctoral fellowship from CAPES, Brazil (PROCAD-AM 88887.321243/2019-00). AR, JV, and CA were supported by CNPq technological development grants (CNPq/MCTI/CT n°53/2022).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Udoakang AJ, Djomkam Zune AL, Tapela K, Nganyewo NN, Olisaka FN, Anyigba CA, et al. The COVID-19, tuberculosis and HIV/AIDS: Ménage à Trois. Front Immunol. (2023) 14:1104828. doi: 10.3389/fimmu.2023.1104828
2. Gingo MR, George MP, Kessinger CJ, Lucht L, Rissler B, Weinman R, et al. Pulmonary function abnormalities in HIV-infected patients during the current antiretroviral therapy era. Am J Respir Crit Care Med. (2010) 182:790–6. doi: 10.1164/rccm.200912-1858OC
3. Visconti NRGDR, Cailleaux-Cezar M, Capone D, Santos MIVD, Graça NP, Loivos LPP, et al. Long-term respiratory outcomes after COVID-19: a Brazilian cohort study. Revista Panamericana de Salud Pública. (2022) 46:1. doi: 10.26633/RPSP.2022.187
4. Davis HE, Assaf GS, McCorkell L, Wei H, Low RJ, Re'em Y, et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine. (2021) 38:101019. doi: 10.1016/j.eclinm.2021.101019
5. Chen C, Haupert SR, Zimmermann L, Shi X, Fritsche LG, Mukherjee B. Global prevalence of post-coronavirus disease 2019 (COVID-19) condition or long COVID: a meta-analysis and systematic review. J Infect Dis. (2022) 226:1593–607. doi: 10.1093/infdis/jiac136
6. Thaweethai T, Jolley SE, Karlson EW, Levitan EB, Levy B, McComsey GA, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. (2023) 329:1934. doi: 10.1001/jama.2023.8823
7. Centers for Disease Control and Prevention. Post-COVID Conditions: Information for Healthcare Providers (2023) Available online at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-conditions.html (accessed January 16, 2024).
8. World Health Organization. Post COVID-19 Condition (Long COVID) (2022). Available online at: https://www.who.int/news-room/fact-sheets/detail/post-covid-19-condition-(long-covid) (accessed January 16, 2024).
9. Ballering AV, van Zon SKR, Olde Hartman TC, Rosmalen JGM. Persistence of somatic symptoms after COVID-19 in the Netherlands: an observational cohort study. Lancet. (2022) 400:452–61. doi: 10.1016/S0140-6736(22)01214-4
10. Hernández-Aceituno A, García-Hernández A, Larumbe-Zabala E. COVID-19 long-term sequelae: omicron versus alpha and delta variants. Infect Dis Now. (2023) 53:104688. doi: 10.1016/j.idnow.2023.104688
11. Romero-Duarte Á, Rivera-Izquierdo M, Guerrero-Fernández de Alba I, Pérez-Contreras M, Fernández-Martínez NF, et al. Sequelae, persistent symptomatology and outcomes after COVID-19 hospitalization: the ANCOHVID multicentre 6-month follow-up study. BMC Med. (2021) 19:129. doi: 10.1186/s12916-021-02003-7
12. Korompoki E, Gavriatopoulou M, Hicklen RS, Ntanasis-Stathopoulos I, Kastritis E, Fotiou D, et al. Epidemiology and organ specific sequelae of post-acute COVID19: A narrative review. J Infect. (2021) 83:1–16. doi: 10.1016/j.jinf.2021.05.004
13. Nopp S, Moik F, Klok FA, Gattinger D, Petrovic M, Vonbank K, et al. Outpatient pulmonary rehabilitation in patients with long COVID improves exercise capacity, functional status, dyspnea, fatigue, and quality of life. Respiration. (2022) 101:593–601. doi: 10.1159/000522118
14. Desai AD, Lavelle M, Boursiquot BC, Wan EY. Long-term complications of COVID-19. Am J Physiol Cell Physiol. (2022) 322:C1–C11. doi: 10.1152/ajpcell.00375.2021
15. World Health Organization. Report on the Global HIV and AIDS Epidemic. Available online at: https://www.who.int/news-room/fact-sheets/detail/hiv-aids (accessed November 13, 2023).
16. Organização Pan-Americana da Saúde. HIV/aids - OPAS/OMS | Organização Pan-Americana da Saúde. (2023) Available online at: https://www.paho.org/pt/topicos/hivaids (accessed November 13, 2023).
17. Bandera A, Gori A, Clerici M, Sironi M. Phylogenies in ART: HIV reservoirs, HIV latency and drug resistance. Curr Opin Pharmacol. (2019) 48:24–32. doi: 10.1016/j.coph.2019.03.003
18. Antiretroviral Therapy Cohort Collaboration. Life expectancy of individuals on combination antiretroviral therapy in high-income countries: a collaborative analysis of 14 cohort studies. Lancet. (2008) 372:293–299. doi: 10.1016/S0140-6736(08)61113-7
19. Lima RBH, Barberiz TBDO, Daniel MDC, Seki KLM, Christofoletti G. Síndrome da fragilidade, capacidade pulmonar e funcional em pacientes infectados pelo HIV/AIDS. Fisioterapia e Pesquisa. (2021) 28:18–24. doi: 10.1590/1809-2950/19029128012021
20. Yendewa G, Perez JA, Patil N, McComsey GA. HIV infection is associated with higher risk of post-acute sequelae of SARS-CoV-2 (PASC) however vaccination is protective. SSRN Electron J. (2022) doi: 10.2139/ssrn.4276609
21. Yang X, Shi F, Zhang H, Giang WA, Kaur A, Chen H, et al. Long COVID among people with HIV: a systematic review and meta-analysis. HIV Med. (2025) 26:6–16. doi: 10.1111/hiv.13708
22. World Health Organization. Clinical Management of COVID-19: Living Guideline. Geneva: WHO/2019-nCoV/clinical/2023.1 (2023). Available online at: https://iris.who.int/handle/10665/365580 (accessed March 20, 2023).
23. Paternostro-Sluga T, Grim-Stieger M, Posch M, Schuhfried O, Vacariu G, Mittermaier C, et al. Reliability and validity of the medical research council (MRC) scale and a modified scale for testing muscle strength in patients with radial palsy. J Rehabil Med. (2008) 40:665–71. doi: 10.2340/16501977-0235
24. Laveneziana P, Albuquerque A, Aliverti A, Babb T, Barreiro E, Dres M, et al. ERS statement on respiratory muscle testing at rest and during exercise. Eur Resp J. (2019) 53:1801214. doi: 10.1183/13993003.01214-2018
25. Singh D, Agusti A, Anzueto A, Barnes PJ, Bourbeau J, Celli BR, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. (2019) 53:1900164. doi: 10.1183/13993003.00164-2019
26. Alberto C, Pereira DC, Sato T. New reference values for forced spirometry in white adults in Brazil. J Bras Pneumol. 33:397–406. doi: 10.1590/s1806-37132007000400008
27. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS Statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. (2002) 166:111–117. doi: 10.1164/ajrccm.166.1.at1102
28. Britto RR, Probst VS, Andrade AFD, de Samora GAR, Hernandes NA, Marinho PEM, et al. Reference equations for the six-minute walk distance based on a Brazilian multicenter study. Braz J Phys Ther. (2013) 17:556–63. doi: 10.1590/S1413-35552012005000122
29. Hays RD, Sherbourne CD, Mazel RM. The rand 36-item health survey 10 Health. Econ. (1993) 2:217–27. doi: 10.1002/hec.4730020305
30. Dancey CP, Reidy J. Statistics Without Maths for Psychology, 5th edn Pearson Education. Hoboken, NJ: Prentice Hall (2011).
31. Costa AN, Val F, Macedo ÁE, Cubas-Vega N, Tejo PL Del, Marques MM, et al. Increased prevalence of hypertension among people living with HIV: where to begin? Rev Soc Bras Med Trop. (2020) 53:e20190564. doi: 10.1590/0037-8682-0564-2019
32. Moraes DC de A, Oliveira RC, de Costa SFG. Adherence of men living with HIV/AIDS to antiretroviral treatment. Escola Anna Nery - Revista de Enfermagem. (2014) 18. doi: 10.5935/1414-8145.20140096
33. Knauth DR, Hentges B, Macedo JL, de Pilecco FB, Teixeira LB, Leal AF. O diagnóstico do HIV/aids em homens heterossexuais: a surpresa permanece mesmo após mais de 30 anos de epidemia. Cad Saude Publica. (2020) 36:e00170118. doi: 10.1590/0102-311x00170118
34. Erlandson KM, Schrack JA, Jankowski CM, Brown TT, Campbell TB. Functional impairment, disability, and frailty in adults aging with HIV-infection. Curr HIV/AIDS Rep. (2014) 11:279–90. doi: 10.1007/s11904-014-0215-y
35. Organização Pan-Americana da Saúde (OPAS). HIV/AIDS: Principais fatos (2022). Available online at: https://www.paho.org/pt/brasil (accessed June 18, 2023).
36. Ministério da Saúde, Secretaria de Vigilância em Saúde. Boletim Epidemiológico HIV/AIDS 2023 (2023). Available online at: https://www.gov.br/aids/pt-br/central-de-conteudo/boletins-epidemiologicos/2023/hiv-aids/boletim-epidemiologico-hiv-e-aids-2023.pdf/view (accessed December 3, 2023).
37. Sirayder U, Inal-Ince D, Kepenek-Varol B, Acik C. Long-term characteristics of severe covid-19: respiratory function, functional capacity, and quality of life. Int J Environ Res Public Health. (2022) 19:6304. doi: 10.3390/ijerph19106304
38. Hockele LF, Sachet Affonso JV, Rossi D, Eibel B. Pulmonary and functional rehabilitation improves functional capacity, pulmonary function and respiratory muscle strength in post COVID-19 patients: pilot clinical trial. Int J Environ Res Public Health. (2022) 19:14899. doi: 10.3390/ijerph192214899
39. Cortés-Telles A, López-Romero S, Figueroa-Hurtado E, Pou-Aguilar YN, Wong AW, Milne KM, et al. Pulmonary function and functional capacity in COVID-19 survivors with persistent dyspnoea. Respir Physiol Neurobiol. (2021) 288:103644. doi: 10.1016/j.resp.2021.103644
40. Anastasio F, Barbuto S, Scarnecchia E, Cosma P, Fugagnoli A, Rossi G, et al. Medium-term impact of COVID-19 on pulmonary function, functional capacity and quality of life. Eur Respir J. (2021) 58:2004015. doi: 10.1183/13993003.04015-2020
41. Goulart CDL, Silva RN, Oliveira MR, Guizilini S, Rocco IS, Mendez VMF, et al. Lifestyle and rehabilitation during the COVID-19 pandemic: guidance for health professionals and support for exercise and rehabilitation programs. Expert Rev Anti Infect Ther. (2021) 19:1385–96. doi: 10.1080/14787210.2021.1917994
42. Lucas C, Wong P, Klein J, Castro TBR, Silva J, Sundaram M, et al. Longitudinal analyses reveal immunological misfiring in severe COVID-19. Nature. (2020) 584:463–9. doi: 10.1038/s41586-020-2588-y
43. Olezene CS, Hansen E, Steere HK, Giacino JT, Polich GR, Borg-Stein J, et al. Functional outcomes in the inpatient rehabilitation setting following severe COVID-19 infection. PLoS One. (2021) 16:e0248824. doi: 10.1371/journal.pone.0248824
44. Pretorius E, Venter C, Laubscher GJ, Kotze MJ, Oladejo SO, Watson LR, et al. Prevalence of symptoms, comorbidities, fibrin amyloid microclots and platelet pathology in individuals with long COVID/post-acute sequelae of COVID-19 (PASC). Cardiovasc Diabetol. (2022) 21:148. doi: 10.1186/s12933-022-01579-5
45. Han Q, Zheng B, Daines L, Sheikh A. Long-term sequelae of COVID-19: a systematic review and meta-analysis of one-year follow-up studies on post-covid symptoms. Pathogens. (2022) 11:269. doi: 10.3390/pathogens11020269
46. Wong AW, López-Romero S, Figueroa-Hurtado E, Vazquez-Lopez S, Milne KM, Ryerson CJ, et al. Predictors of reduced 6-minute walk distance after COVID-19: a cohort study in Mexico. Pulmonology. (2021) 27:563–5. doi: 10.1016/j.pulmoe.2021.03.004
47. Varkila MRJ, Vos AG, Barth RE, Tempelman HA, Devillé WLJ, Coutinho RA, et al. The association between HIV infection and pulmonary function in a rural African population. PLoS One. (2019) 14:e0210573. doi: 10.1371/journal.pone.0210573
48. Zeinalian M, Salari-Jazi A, Jannesari A, Khanahmad H. A potential protective role of losartan against coronavirus-induced lung damage. Infect Control Hosp Epidemiol. (2020) 41:752–3. doi: 10.1017/ice.2020.80
49. Puskarich MA, Ingraham NE, Merck LH, Driver BE, Wacker DA, Black LP, et al. Efficacy of losartan in hospitalized patients with COVID-19–induced lung injury. JAMA Netw Open. (2022) 5:e222735. doi: 10.1001/jamanetworkopen.2022.2735
50. Wise RA, Holbrook JT, Brown RH, Criner GJ, Dransfield MT, He J, et al. Clinical trial of losartan for pulmonary emphysema: pulmonary trials cooperative losartan effects on emphysema progression clinical trial. Am J Respir Crit Care Med. (2022) 206:838–45. doi: 10.1164/rccm.202201-0206OC
51. Campo M, Oursler KK, Huang L, Goetz MB, Rimland D, Hoo GS, et al. Association of chronic cough and pulmonary function with 6-minute walk test performance in HIV Infection. JAIDS. (2014) 65:557–63. doi: 10.1097/QAI.0000000000000086
52. Erlandson KM, Allshouse AA, Jankowski CM, MaWhinney S, Kohrt WM, Campbell TB. functional impairment is associated with low bone and muscle mass among persons aging with hiv infection. JAIDS. (2013) 63:209–15. doi: 10.1097/QAI.0b013e318289bb7e
53. O'Dell MW, Crawford A, Bohi ES, Bonner FJ. Disability in persons hospitalized with AIDS. Am J Phys Med Rehabil. (1991) 70:91–95. doi: 10.1097/00002060-199104000-00008
54. Collini P. Lung function declines more rapidly in treated HIV-positive people than in HIV-negative people. Lancet Healthy Longev. (2021) 2:e183–4. doi: 10.1016/S2666-7568(21)00059-3
55. Githinji LN, Gray DM, Hlengwa S, Myer L, Machemedze T, Zar HJ. Longitudinal changes in spirometry in South African adolescents perinatally infected with human immunodeficiency virus who are receiving antiretroviral therapy. Clin Infect Dis. (2020) 70:483–90. doi: 10.1093/cid/ciz255
56. Kunisaki KM, Nouraie M, Jensen RL, Chang D, D'Souza G, Fitzpatrick ME, et al. Lung function in men with and without HIV. AIDS. (2020) 34:1227–35. doi: 10.1097/QAD.0000000000002526
57. Barnett CF, Hsue PY, Machado RF. Pulmonary hypertension: an increasingly recognized complication of hereditary hemolytic anemias and HIV infection. JAMA. (2008) 299:324–31. doi: 10.1001/jama.299.3.324
58. Drummond MB, Huang L, Diaz PT, Kirk GD, Kleerup EC, Morris A, et al. Factors associated with abnormal spirometry among HIV-infected individuals. AIDS. (2015) 29:1691–700. doi: 10.1097/QAD.0000000000000750
59. Hajjar LA, Costa IBS da S, Rizk SI, Biselli B, Gomes BR, Bittar CS, et al. Intensive care management of patients with COVID-19: a practical approach. Ann Intensive Care. (2021) 11:36. doi: 10.1186/s13613-021-00820-w
60. Yongzhi X. COVID-19-associated cytokine storm syndrome and diagnostic principles: an old and new issue. Emerg Microbes Infect. (2021) 10:266–76. doi: 10.1080/22221751.2021.1884503
61. Parasher A. COVID-19: current understanding of its pathophysiology, clinical presentation and treatment. Postgrad Med J. (2021) 97:312–20. doi: 10.1136/postgradmedj-2020-138577
62. Haseli N, Esmaeelzadeh F, Ghahramani F, Alimohamadi Y, Hayati R, Mahboubi M. Health-related quality of life and its related factors in HIV(+) patients referred to shiraz behavioral counseling center, Iran in 2012. Med J Islam Repub Iran. (2014) 28:13.
63. Amini Lari M, Faramarzi H, Shams M, Marzban M, Joulaei H. Sexual dysfunction, depression and quality of life in patients with HIV infection. Iran J Psychiatry Behav Sci. (2013) 7:61–8.
64. Mostafavian Z, Abbasi Shaye Z, Faraj Pour A, Hosseini G. The data on health locus of control and its relationship with quality of life in HIV-positive patients. Data Brief. (2018) 18:1967–71. doi: 10.1016/j.dib.2018.04.131
65. Maleki MR, Derakhshani N, Azami-Aghdash S, Naderi M, Nikoomanesh M. Quality of life of people with HIV/AIDS in Iran: a systematic review and meta-analysis. Iran J Public Health. (2020) 49:1399–1410. doi: 10.18502/ijph.v49i8.3861
66. Rayanakorn A. Ong-artborirak P, Ademi Z, Chariyalertsak S. Predictors of stigma and health-related quality of life among people living with HIV in Northern Thailand. AIDS Patient Care STDS. (2022) 36:186–93. doi: 10.1089/apc.2022.0035
67. Mengistu N, Hareru HE, Shumye S, Yimer S, Sisay D, Kaso AW, et al. Health related quality of life and its association with social support among people living with HIV/AIDS receiving antiretroviral therapy in Ethiopia: a systematic review and meta-analysis. Health Qual Life Outcomes. (2022) 20:77. doi: 10.1186/s12955-022-01985-z
68. Shukla A, Choudhari SG, Gaidhane AM, Quazi Syed Z. Role of art therapy in the promotion of mental health: a critical review. Cureus. (2022) 14:e28026. doi: 10.7759/cureus.28026
69. Guaraldi G, Milic J, Barbieri S, Marchiò T, Caselgrandi A, Volpi S, et al. Resilience and frailty in people living with HIV during the COVID era: two complementary constructs associated with health-related quality of life. JAIDS. (2022) 89:S65–72. doi: 10.1097/QAI.0000000000002865
70. Klein JJ, van der Palen J, Uil SM, Zielhuis GA, Seydel ER, van Herwaarden CLA. Benefit from the inclusion of self-treatment guidelines to a self-management programme for adults with asthma. Eur Respir J. (2001) 17:386–94. doi: 10.1183/09031936.01.17303860
Keywords: HIV, long Covid, functional capacity, pulmonary function, COVID-19
Citation: Rezende AG, Valente J, Goulart CdL, Facioli F, Maia B, Mwangi VI, Bonilla H, Franssen FME, Amaral CMSSBd, Motta TJPS, Alexandre M, Ferreira LCdL, Cipriano Junior G, Arêas GPT and Almeida-Val F (2025) Does long COVID in people living with HIV resemble the functional phenotype of non-HIV individuals who had moderate or severe acute COVID-19? A retrospective cross-sectional study. Front. Med. 12:1533009. doi: 10.3389/fmed.2025.1533009
Received: 28 November 2024; Accepted: 07 April 2025;
Published: 25 April 2025.
Edited by:
Pei-Hui Wang, Shandong University, ChinaReviewed by:
Tope Oyelade, University College London, United KingdomJacques L. Tamuzi, Stellenbosch University, South Africa
Copyright © 2025 Rezende, Valente, Goulart, Facioli, Maia, Mwangi, Bonilla, Franssen, Amaral, Motta, Alexandre, Ferreira, Cipriano Junior, Arêas and Almeida-Val. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fernando Almeida-Val, ZmZhdmFsQGdtYWlsLmNvbQ==
†These authors have contributed equally to this work