 Jin Ma
Jin Ma Xiaolong Zhu1
Xiaolong Zhu1- 1Department of Emergency Medicine, the People’s Hospital of Atushi, Atushi, China
- 2Administration Office, the People’s Hospital of Atushi, Atushi, China
The Xinjiang region of China has long been a high-prevalence area for respiratory diseases, especially pulmonary tuberculosis and chronic obstructive pulmonary disease (COPD). This retrospective, cross-sectional study aimed to analyze the epidemiological characteristics of patients visiting the emergency department (ED) of the People’s Hospital of Atushi in Xinjiang, China, from January to December 2024. This study focused on the prevalence and distribution of respiratory diseases. A total of 8,837 patients were included, and respiratory diseases emerged as the most prevalent condition, accounting for 35.2% of the cohort. The leading respiratory conditions were acute upper respiratory infections (18.4%), pulmonary tuberculosis (4.1%), and COPD (4.6%). Respiratory diseases were significantly more common in older patients and were associated with both gender and ethnicity, with the Uygur ethnic group showing the highest prevalence. The findings suggest that age, gender, ethnicity, and environmental factors, such as the region’s climate, play pivotal roles in the epidemiology of respiratory diseases. These results underscore the need for targeted public health interventions aimed at managing respiratory conditions, especially for vulnerable populations such as the elderly and ethnic minorities in Xinjiang, China.
Introduction
Respiratory diseases represent a major global health burden, with millions of people affected by conditions such as acute upper respiratory infections (1–5). Respiratory diseases contribute significantly to morbidity and mortality, and their prevalence is influenced by factors such as air pollution, climate, age, and ethnic disparities (6–8). Despite growing awareness of these diseases, epidemiological data from less studied regions, such as Xinjiang, remains limited.
Xinjiang, home to diverse ethnic groups such as Uygur, Han, and Kyrgyz, has unique climatic and geographical characteristics that could influence disease prevalence (9–11). The Atushi region, part of the Kizilsu Kirgiz Autonomous Prefecture, which experiences a temperate continental climate with extreme seasonal variations and low rainfall. These environmental conditions, combined with a high ethnic diversity, present a complex landscape for the study of respiratory diseases. Previous research has indicated that climate and environmental factors are crucial factors of respiratory health (12–15). Additionally, the interaction between genetic factors, socio-economic status, and access to healthcare further complicates disease distribution (16–19).
While studies from other parts of China, such as large urban centers, have explored the epidemiology of respiratory diseases, data from regions like Xinjiang remains scarce. Moreover, ethnic and geographical differences in the prevalence of these diseases have not been adequately addressed in the literature. The aim of this study is to analyze the demographic and clinical profiles of patients visiting the emergency department (ED) of The People’s Hospital of Atushi, with a focus on the prevalence and distribution of respiratory diseases.
Materials and methods
Study design and data collection
Data for this cross-sectional study were extracted from the electronic medical record (EMR) system of the People’s Hospital of Atushi from January 2024 to December 2024. Atushi People’s Hospital, established in 1972, is a comprehensive secondary-level hospital providing medical, health, rehabilitation, prevention, teaching, and family planning services. The hospital serves as a primary healthcare facility for both the urban and rural populations of the region. According to the results of the Seventh National Population Census, the permanent resident population of Atushi was approximately 290,900 in 2020. The hospital has 285 beds and employs 476 staff members. Annually, it admits over 14,000 patients, performs more than 2,000 surgeries, and handles upward of 40,000 outpatient visits. Respiratory diseases have a relatively high prevalence in the Atushi region of Xinjiang, which is hypothesized to be related to both the climate and the ethnic composition. This study aims to investigate the epidemiological characteristics of emergency department patients in the Atushi region of Xinjiang, with a particular focus on respiratory diseases, including acute upper respiratory infections, pulmonary tuberculosis, and chronic obstructive pulmonary disease (COPD).
Inclusion criteria were patients aged 14 years or older who visited the ED during the study period. Exclusion criteria included patients with missing data, which were identified and removed from the dataset. This study has been approved by the Medical Ethics Committee of the People’s Hospital of Atushi (No. ATSRMYY-KY-2025001).
Participant characteristics
The demographic and clinical characteristics of patients were recorded, including age, gender, ethnicity, occupation, time of visit, season of visit, disease classification, and vital signs. Data were collected using a structured, electronic data entry form integrated into the hospital’s EMR system. This instrument was developed by the People’s Hospital of Atushi, pilot-tested for clarity and accuracy, and refined accordingly. Regarding the time of visit, the 24 h day was divided into eight 3 h intervals. Vital signs measured included systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate, respiratory rate, temperature, and oxygen saturation (SpO2). Patients were diagnosed with specific diseases based on clinical examination, laboratory tests, and imaging studies.
The classification of patients according to severity was based on the “Guidelines for Triage of Emergency Patients (Draft)” issued by the National Health and Family Planning Commission of China (20). This classification system divides patients into four categories: Level I (Extreme Danger): Immediate and critical condition, Level II (Severe): Urgent and requires immediate intervention, Level III (Emergency): Serious but stable condition, and Level IV (Non-Urgent): Minor and stable condition.
Statistical analysis
Descriptive statistics were used to summarize patient characteristics, including means, standard deviations (SD), and proportions for continuous and categorical variables, respectively. The Chi-square test (χ2) was performed to assess the association between categorical variables such as age, gender, and ethnicity with the presence of respiratory diseases (pulmonary tuberculosis, acute upper respiratory infection, and COPD. A p-value of < 0.05 was considered statistically significant. All statistical analyses were conducted using SPSS version 26.0 (IBM Corp., Released 2019, IBM SPSS Statistics for Windows, Armonk, NY, United States).
Results
Patient demographics and baseline characteristics
Information on 8,963 participants was collected from the EMRs, of which 126 were excluded. A total of 8,837 patients were included in this study, consisting of 4,327 males (49.0%) and 4,510 females (51.0%) (Table 1). The age distribution of the patients was as follows: 3,996 patients (45.2%) were aged 14–34 years, 2,945 (33.3%) were aged 35–59 years, 1,819 (20.6%) were aged 60–84 years, and 77 patients (0.9%) were aged ≥ 85 years. The majority of patients were from the Uygur ethnic group (82.5%), followed by Han (13.7%), and Kyrgyz (3.8%) ethnicities.
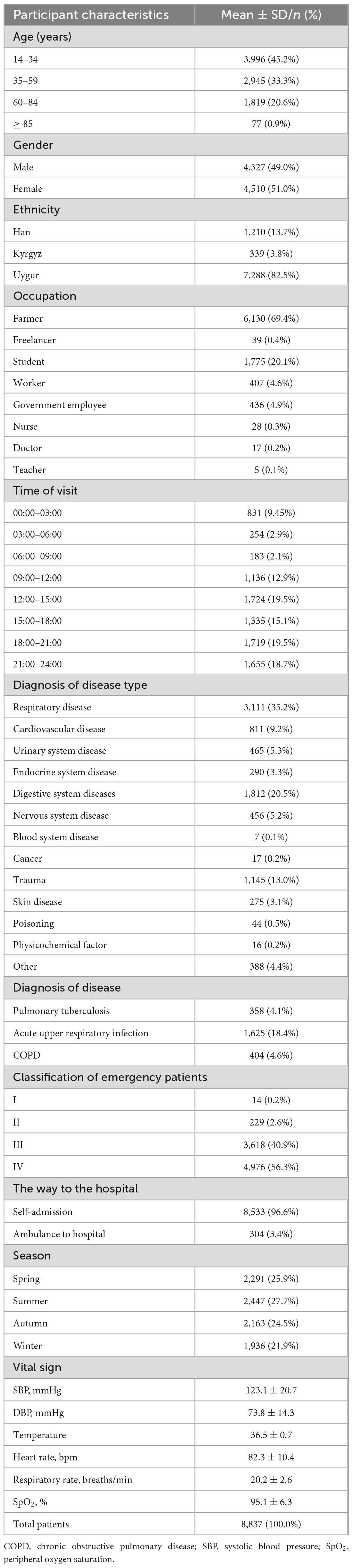
Table 1. Baseline characteristics of patients.
The mean and standard deviation of vital signs at the patient’s arrival were as follows: systolic blood pressure (SBP) was 123.1 ± 20.7 mmHg, diastolic blood pressure (DBP) was 73.8 ± 14.3 mmHg, temperature was 36.5 ± 0.7°C, heart rate was 82.3 ± 10.4 bpm, respiratory rate was 20.2 ± 2.6 breaths/min, and oxygen saturation (SpO2) was 95.1 ± 6.3%. In terms of triage classification, 14 patients (0.2%) were classified as Level I (extremely critical), 229 patients (2.6%) as Level II (severe), 3,618 patients (40.9%) as Level III (emergency), and 4,976 patients (56.3%) as Level IV (non-urgent).
Disease prevalence and distribution
Out of the 8,837 patients, 3,111 (35.2%) were diagnosed with respiratory diseases (Table 1). The three primary types of respiratory diseases included acute upper respiratory infection (n = 1,625; 18.4%), pulmonary tuberculosis (n = 358; 4.1%), and COPD (n = 404; 4.6%). Other common disease categories included digestive system diseases (n = 1,812; 20.5%), trauma (n = 1,145; 13.0%), and cardiovascular diseases (n = 811; 9.2%). The remaining diseases, including those of the urinary, endocrine, nervous, and other systems, accounted for a smaller proportion of the cases.
Respiratory diseases
Overall respiratory diseases
The prevalence of respiratory diseases was significantly higher among older patients (p < 0.001) (Table 2). Specifically, the prevalence of respiratory diseases was 34.0% in patients aged 14–34 years, 27.0% in patients aged 35–59 years, 50.0% in those aged 60–84 years, and 59.7% in those aged ≥ 85 years. There was also a statistically significant gender difference, with a higher prevalence in females (37.2%) compared to males (33.1%) (p < 0.001). Ethnicity was another significant factor, with the Uygur ethnic group having the highest prevalence of respiratory diseases (34.6%), followed by the Kyrgyz group (40.4%) and the Han group (37.1%) (p = 0.031).
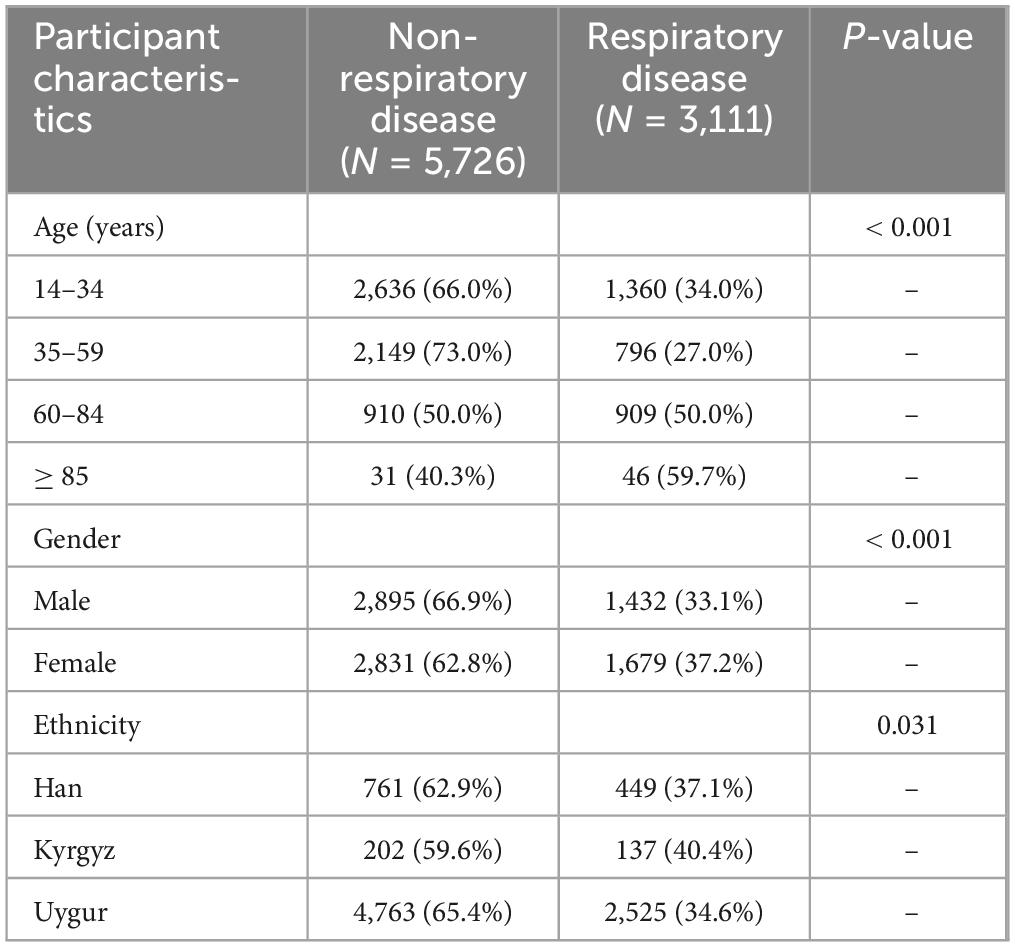
Table 2. The association between respiratory diseases and patient gender, age, and ethnicity.
Acute upper respiratory infection
Among the 1,625 patients diagnosed with acute upper respiratory infection, the prevalence was notably higher in younger age groups (Table 3). Specifically, 26.8% of patients aged 14–34 years, 15.9% of patients aged 35–59 years, and 4.7% of patients aged 60–84 years had acute upper respiratory infections (p < 0.001). Female patients had a higher prevalence of acute upper respiratory infection (20.2%) compared to male patients (16.5%) (p < 0.001). Ethnically, Uygur patients had the highest proportion of acute upper respiratory infection (16.6%), followed by Han (28.7%) and Kyrgyz patients (19.8%) (p < 0.001).
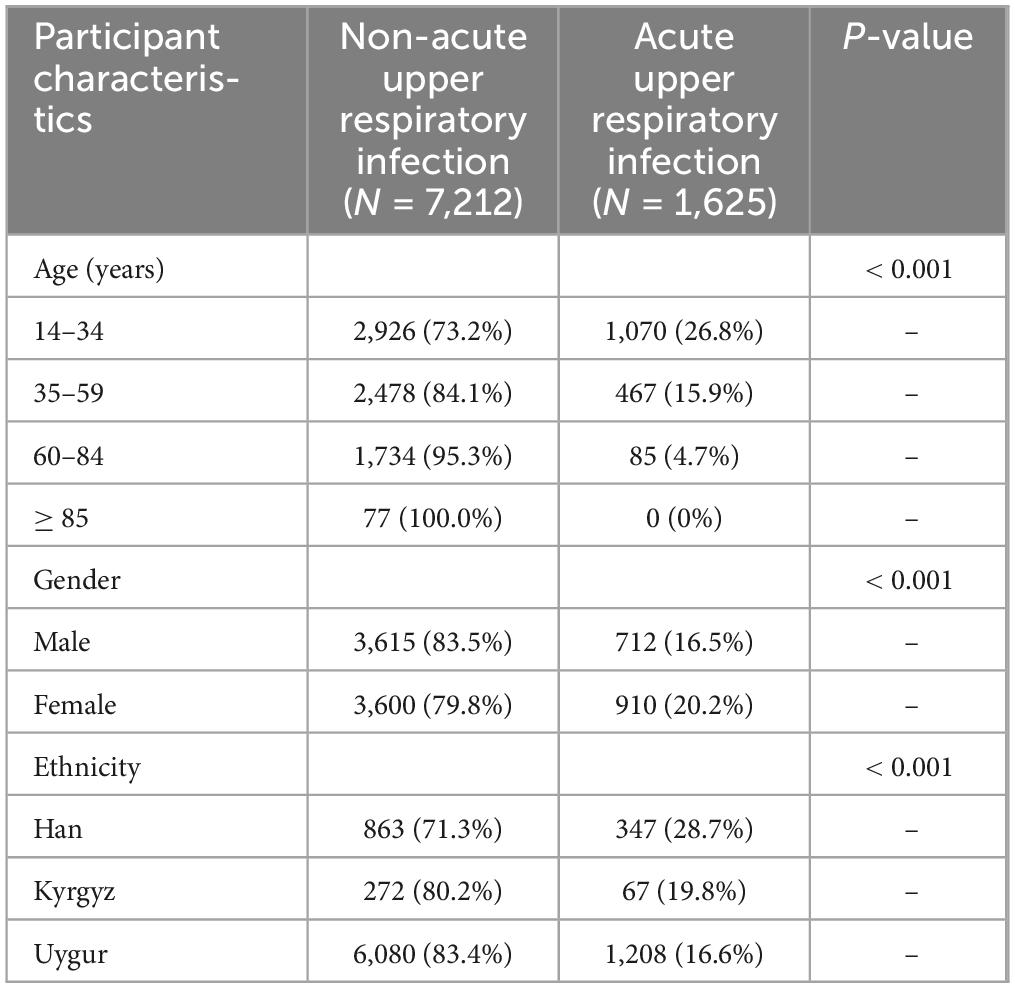
Table 3. The association between acute upper respiratory infection and patient gender, age, and ethnicity.
Pulmonary tuberculosis
A total of 358 patients were diagnosed with pulmonary tuberculosis (Table 4). The prevalence of pulmonary tuberculosis was significantly higher in older patients, with 16.8% of those aged 60–84 years and 24.7% of those aged ≥ 85 years diagnosed with the disease (p < 0.001). There were no significant gender differences in pulmonary tuberculosis diagnosis (p = 0.939). The Uygur ethnic group had the highest prevalence of pulmonary tuberculosis (4.6%), followed by the Kyrgyz group (5.6%) and the Han group (0.2%) (p < 0.001).
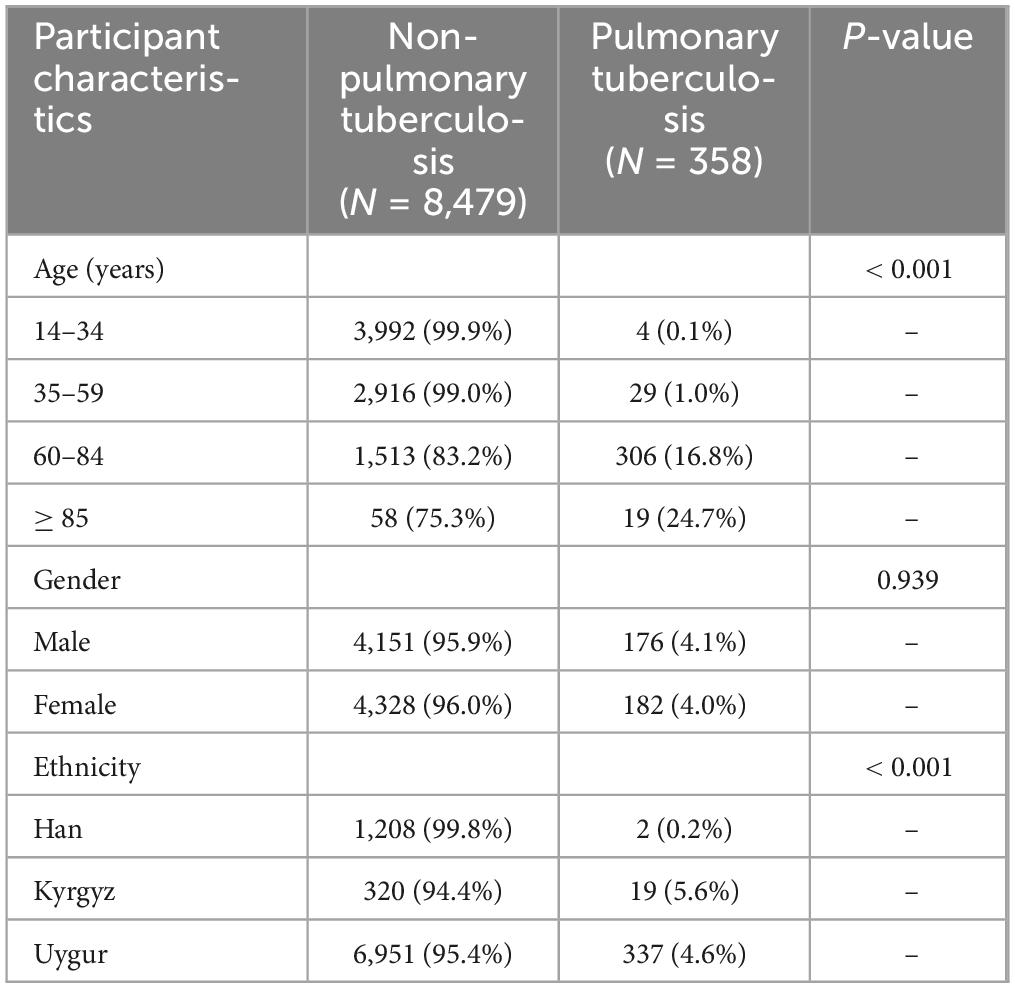
Table 4. The association between pulmonary tuberculosis and patient gender, age, and ethnicity.
COPD
Chronic obstructive pulmonary disease was diagnosed in 404 patients, with the prevalence significantly increasing with age (Table 5). Among the patients aged 14–34 years, none were diagnosed with COPD, while 2.6% of patients aged 35–59 years, 17.0% of patients aged 60–84 years, and 23.4% of patients aged ≥ 85 years were diagnosed with COPD (p < 0.001). No significant gender differences were found in COPD prevalence (p = 0.192). Ethnically, the Uygur group had the highest prevalence of COPD (5.4%), followed by the Kyrgyz group (2.7%) and the Han group (0.2%) (p < 0.001).
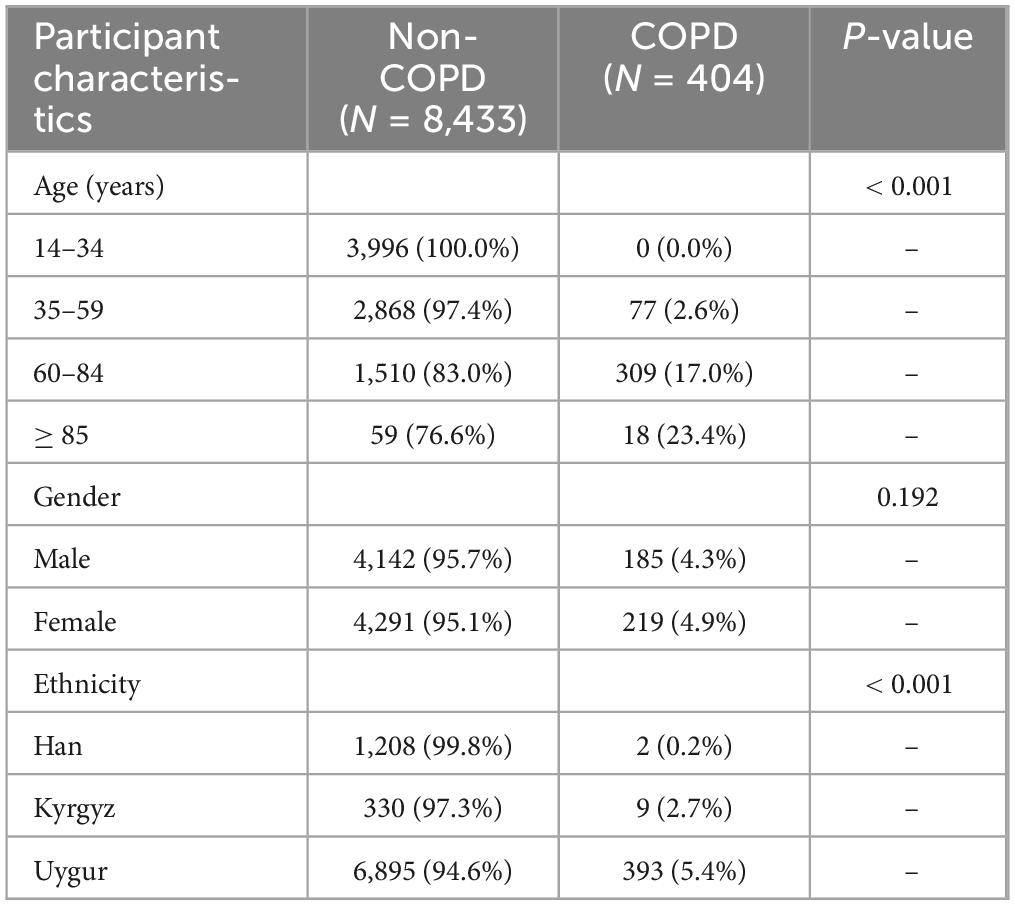
Table 5. The association between chronic obstructive pulmonary disease (COPD) and patient gender, age, and ethnicity.
Discussion
Our study identified a high prevalence of respiratory diseases, with 35.2% of patients presenting with respiratory conditions. The analysis of the demographic and clinical characteristics of emergency department patients further revealed significant associations between age, gender, and ethnicity with the prevalence of respiratory diseases. Older age, female gender, and Uygur ethnicity were found to be risk factors for respiratory diseases.
Although the prevalence of pulmonary tuberculosis in China has been decreasing in recent decades, the southern region of Xinjiang remains a high-endemic area for tuberculosis, with a prevalence significantly higher than the national average (21–24). Pulmonary tuberculosis has long been associated with poverty, overcrowded living conditions, and underdeveloped healthcare infrastructure, all of which may disproportionately affect older populations who have had prolonged exposure to risk factors (25–27). Ethnically, the Uygur population had the highest prevalence of pulmonary tuberculosis, which aligns with earlier studies suggesting that some Uygur population are at higher risk for pulmonary tuberculosis due to genetic factors and healthcare access (28–30).
Chronic obstructive pulmonary disease, with a prevalence of 4.6%, followed the expected age-related trend, as older adults are more susceptible to chronic lung diseases (31, 32). No gender differences were found in the prevalence of COPD. Interestingly, the Uygur ethnic group again had the highest prevalence of COPD. Both previous studies and this study indicate that the prevalence of COPD among the Uyghur population is significantly higher than in other regions of China (33–36). Analysis by Li et al. (36) shows that lifestyle factors such as kitchen ventilation, cooking, and smoking are significantly associated with COPD. Uyghurs may have a greater preference for eating grilled meat, and since grilling food releases harmful substances like formaldehyde, benzene, and acrolein, this may exacerbate respiratory symptoms, reduce lung function, and increase the risk of developing COPD (36).
This study has several strengths. First, it is one of the few studies focusing on the epidemiology of respiratory diseases in the southwest Xinjiang, thus providing valuable insights into the health burdens faced by a unique population. In addition, the large sample size and detailed demographic data contribute to the robustness of the findings, allowing for nuanced analysis of factors such as age, gender, and ethnicity in the distribution of respiratory diseases.
However, there are several limitations that must be acknowledged. The single-center design limits the generalizability of the findings to other regions of China. The absence of data on certain environmental and lifestyle factors—such as air quality, smoking rates, and nutrition—means that some important confounders could not be accounted for.
In conclusion, this study provides an important contribution to understanding the epidemiology of respiratory diseases in the Atushi region of Xinjiang. The high burden of respiratory diseases in the ED is not only a reflection of current disease prevalence but also a signal that many cases might be avoided or better managed outside the emergency setting. For instance, a significant number of patients with exacerbated COPD or pulmonary tuberculosis complications could potentially receive timely and effective interventions through enhanced primary care. The higher burden of respiratory diseases among the elderly and ethnic minorities, especially the Uygur population, calls for targeted healthcare interventions and preventive measures tailored to the unique needs of these groups. For the elderly, public health interventions should include tailored screening programs, regular preventive care (like vaccinations), and simplified, accessible services—such as mobile or home-based visits—to enable early detection and prompt treatment. For ethnic minorities, health communications must be adapted to their language and cultural context while ensuring accessible preventive services, including TB screening, asthma/COPD management, and immunizations.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Medical Ethics Committee of the People’s Hospital of Atushi. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because Patient consent was waived due to the retrospective nature of the study.
Author contributions
JM: Data curation, Investigation, Project administration, Writing – original draft, Writing – review and editing. XZ: Data curation, Formal Analysis, Resources, Supervision, Writing – original draft. QT: Data curation, Formal Analysis, Software, Writing – original draft. SL: Data curation, Formal Analysis, Writing – original draft. WZ: Conceptualization, Data curation, Investigation, Resources, Writing – original draft, Writing – review and editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Nicholson K, Kent J, Hammersley V, Cancio E. Acute viral infections of upper respiratory tract in elderly people living in the community: Comparative, prospective, population based study of disease burden. BMJ. (1997) 315:1060–4. doi: 10.1136/bmj.315.7115.1060
2. Wodniak N, Gharpure R, Feng L, Lai X, Fang H, Tian J, et al. Costs of influenza illness and acute respiratory infections by household income level: Catastrophic health expenditures and implications for health equity. Influenza Other Respir Viruses. (2025) 19:e70059. doi: 10.1111/irv.70059
3. Fahim M, Deghedy O, Alim W, Kamel R, Hassan H, Mohsen A, et al. The national burden of influenza-associated respiratory illness across levels of severity in Egypt, 2016-2019. Influenza Other Respir Viruses. (2024) 18:e70061. doi: 10.1111/irv.70061
4. Boender T, Cai W, Schranz M, Kocher T, Wagner B, Ullrich A, et al. Using routine emergency department data for syndromic surveillance of acute respiratory illness, Germany, week 10 2017 until week 10 2021. Euro Surveill. (2022) 27:2100865. doi: 10.2807/1560-7917.ES.2022.27.27.2100865
5. Gbd Chronic Respiratory Diseases Collaborators. Global burden of chronic respiratory diseases and risk factors, 1990-2019: An update from the global burden of disease study 2019. EClinicalMedicine. (2023) 59:101936. doi: 10.1016/j.eclinm.2023.101936
6. Szyszkowicz M, Kousha T, Castner J, Dales R. Air pollution and emergency department visits for respiratory diseases: A multi-city case crossover study. Environ Res. (2018) 163:263–9. doi: 10.1016/j.envres.2018.01.043
7. Madani N, Carpenter D. Patterns of emergency room visits for respiratory diseases in New York state in relation to air pollution, poverty and smoking. Int J Environ Res Public Health. (2023) 20:3267. doi: 10.3390/ijerph20043267
8. Rodríguez-Villamizar L, Rojas-Roa N, Fernández-Niño J. Short-term joint effects of ambient air pollutants on emergency department visits for respiratory and circulatory diseases in Colombia, 2011-2014. Environ Pollut. (2019) 248:380–7. doi: 10.1016/j.envpol.2019.02.028
9. Cao C, Wang Y, Peng L, Wu W, Yang H, Li Z. Asthma and other respiratory diseases of children in relation to personal behavior, household, parental and environmental factors in West China. Toxics. (2023) 11:964. doi: 10.3390/toxics11120964
10. Wang L, Wang W, Wang J, Zhu L, Luo J. Correlation between inflammatory markers and pathogenic bacteria in children’s winter respiratory infections in Xinjiang. Int J Gen Med. (2025) 18:331–43. doi: 10.2147/IJGM.S499696
11. Yang Z, Li C, Wang C, Nie Y, Zhang Y, Tian M, et al. Assessing the impact of meteorological conditions on outpatient visits for childhood respiratory diseases in Urumqi, China. J Occup Environ Med. (2022) 64:e598–605. doi: 10.1097/JOM.0000000000002640
12. Tran H, Tsai F, Lee Y, Chang J, Chang L, Chang T, et al. The impact of air pollution on respiratory diseases in an era of climate change: A review of the current evidence. Sci Total Environ. (2023) 898:166340. doi: 10.1016/j.scitotenv.2023.166340
13. Guan W, Zheng X, Chung K, Zhong N. Impact of air pollution on the burden of chronic respiratory diseases in China: Time for urgent action. Lancet. (2016) 388:1939–51. doi: 10.1016/S0140-673631597-5
14. Jia H, Xu J, Ning L, Feng T, Cao P, Gao S, et al. Ambient air pollution, temperature and hospital admissions due to respiratory diseases in a cold, industrial city. J Glob Health. (2022) 12:04085. doi: 10.7189/jogh.12.04085
15. Hughes H, Morbey R, Hughes T, Locker T, Pebody R, Green H, et al. Emergency department syndromic surveillance providing early warning of seasonal respiratory activity in England. Epidemiol Infect. (2016) 144:1052–64. doi: 10.1017/S0950268815002125
16. Du M, Zhu L, Liu M, Liu J. Mutual associations of healthy behaviours and socioeconomic status with respiratory diseases mortality: A large prospective cohort study. Nutrients. (2023) 15:1872. doi: 10.3390/nu15081872
17. Jalasto J, Lassmann-Klee P, Schyllert C, Luukkonen R, Meren M, Larsson M, et al. Occupation, socioeconomic status and chronic obstructive respiratory diseases - The EpiLung study in Finland, Estonia and Sweden. Respir Med. (2022) 191:106403. doi: 10.1016/j.rmed.2021.106403
18. Polak M, Genowska A, Szafraniec K, Fryc J, Jamiołkowski J, Pająk A. Area-based socio-economic inequalities in mortality from lung cancer and respiratory diseases. Int J Environ Res Public Health. (2019) 16:1791. doi: 10.3390/ijerph16101791
19. Patarčić I, Gelemanović A, Kirin M, Kolčić I, Theodoratou E, Baillie K, et al. The role of host genetic factors in respiratory tract infectious diseases: Systematic review, meta-analyses and field synopsis. Sci Rep. (2015) 5:16119. doi: 10.1038/srep16119
20. Zhiting G, Jingfen J, Shuihong C, Minfei Y, Yuwei W, Sa W. Reliability and validity of the four-level Chinese emergency triage scale in mainland China: A multicenter assessment. Int J Nurs Stud. (2020) 101:103447. doi: 10.1016/j.ijnurstu.2019.103447
21. Yang LJ, Li T, Chen W. [Study on spatial clustering characteristics of tuberculosis in China, 2013-2018]. Zhonghua Liu Xing Bing Xue Za Zhi (2020) 41:1843–7. doi: 10.3760/cma.j.cn112338-20200114-00029
22. Zheng Y, Zhang L, Zhang X, Wang K, Zheng Y. Forecast model analysis for the morbidity of tuberculosis in Xinjiang, China. PLoS One. (2015) 10:e0116832. doi: 10.1371/journal.pone.0116832
23. Wang Y, Gao C, Zhao T, Jiao H, Liao Y, Hu Z, et al. A comparative study of three models to analyze the impact of air pollutants on the number of pulmonary tuberculosis cases in Urumqi, Xinjiang. PLoS One. (2023) 18:e0277314. doi: 10.1371/journal.pone.0277314
24. Guo G, Zheng Y, Ma X, Sun L, Wushouer Q, Jia B, et al. eDOTS: Improving the treatment of pulmonary tuberculosis in Xinjiang, China. Infect Drug Resist. (2023) 7497–505. doi: 10.2147/IDR.S438962
25. Dong Z, Wang Q, Yu S, Huang F, Liu J, Yao H, et al. Age-period-cohort analysis of pulmonary tuberculosis reported incidence, China, 2006-2020. Infect Dis Poverty. (2022) 11:85. doi: 10.1186/s40249-022-01009-4
26. Orcau À, Caylà JA, Martínez JA. Present epidemiology of tuberculosis. Prevention and control programs. Enferm Infecc Microbiol Clin. (2011) 29:2–7. doi: 10.1016/S0213-005X70011-8
27. Meghji J, Mortimer K, Agusti A, Allwood B, Asher I, Bateman ED, et al. Improving lung health in low-income and middle-income countries: From challenges to solutions. Lancet. (2021) 397:928–40. doi: 10.1016/S0140-673600458-X
28. Wang X, Cao X, Zhang W, Zhang L, Lu L, Li X, et al. Association of human leukocyte antigens-DQB2/DPA1/DPB1 polymorphism and pulmonary tuberculosis in the Chinese Uygur population. Mol Genet Genomic Med. (2019) 7:e544. doi: 10.1002/mgg3.544
29. Shang B, Wei C, Wang C, Zheng Y, Zhang L. Interactions among tuberculosis, geographic environment and aerosols: Evidence from the Kashgar region of China. Front Public Health. (2025) 13:1519330. doi: 10.3389/fpubh.2025.1519330
30. Tusun D, Abulimiti M, Mamuti X, Liu Z, Xu D, Li G, et al. The epidemiological characteristics of pulmonary tuberculosis - Kashgar prefecture, Xinjiang Uygur autonomous region, China, 2011-2020. China CDC Wkly. (2021) 3:557–61. doi: 10.46234/ccdcw2021.144
31. López-Campos J, Tan W, Soriano J. Global burden of COPD. Respirology. (2016) 21:14–23. doi: 10.1111/resp.12660
32. Wacker M, Kitzing K, Jörres R, Leidl R, Schulz H, Karrasch S, et al. The contribution of symptoms and comorbidities to the economic impact of COPD: An analysis of the German COSYCONET cohort. Int J Chron Obstruct Pulmon Dis. (2017) 12:3437–48. doi: 10.2147/COPD.S141852
33. Raherison C, Girodet P. Epidemiology of COPD. Eur Respir Rev. (2009) 18:213–21. doi: 10.1183/09059180.00003609
34. Holtjer J, Bloemsma L, Beijers R, Cornelissen M, Hilvering B, Houweling L, et al. Identifying risk factors for COPD and adult-onset asthma: An umbrella review. Eur Respir Rev. (2023) 32:230009. doi: 10.1183/16000617.0009-2023
35. Tang L, Zhong X, Gong H, Tuerxun M, Ma T, Ren J, et al. Analysis of the association of ANO3/MUC15, COL4A4, RRBP1, and KLK1 polymorphisms with COPD susceptibility in the Kashi population. BMC Pulm Med. (2022) 22:178. doi: 10.1186/s12890-022-01975-3
Keywords: epidemiological, emergency department, ethnic, respiratory diseases, region’s climate
Citation: Ma J, Zhu X, Tang Q, Liu S and Zhou W (2025) Epidemiological characteristics of respiratory diseases in emergency department patients from different ethnic groups in the Atushi region, Xinjiang. Front. Med. 12:1569629. doi: 10.3389/fmed.2025.1569629
Received: 01 February 2025; Accepted: 26 May 2025;
Published: 16 June 2025.
Edited by:
Mabel Kamweli Aworh, North Carolina State University, United StatesReviewed by:
Abdulhakeem Olorukooba, Ahmadu Bello University, NigeriaOluwafolayemi Doyeni, Oak Street Health, United States
Copyright © 2025 Ma, Zhu, Tang, Liu and Zhou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Weiwei Zhou, d2VpZ29vMTIyNEAxNjMuY29t