 Fabián Darío Arias Rodríguez1
Fabián Darío Arias Rodríguez1 Mercedes Larenas1Santiago Paredes1Guillermina Giuliano1Andrés López-Cortés2
Mercedes Larenas1Santiago Paredes1Guillermina Giuliano1Andrés López-Cortés2 Juan S. Izquierdo-Condoy3*
Juan S. Izquierdo-Condoy3*- 1Hospital Zonal General de Agudos Dr. Ricardo Gutierrez, La Plata, Argentina
- 2Cancer Research Group (CRG), Faculty of Medicine, Universidad de Las Américas, Quito, Ecuador
- 3One Health Research Group, Universidad de las Américas, Quito, Ecuador
Introduction: Malignant otitis externa (MOE) is a severe and potentially life-threatening infection of the external auditory canal, most frequently caused by Pseudomonas aeruginosa. Although typically seen in immunocompromised individuals—especially those with diabetes mellitus—up to 45% of cases have been reported in non-diabetic patients, highlighting the importance of recognizing atypical presentations. Rare pathogens, such as Proteus mirabilis, have been identified in only a few documented cases. Early diagnosis and prompt intervention are essential to prevent serious complications, including osteomyelitis and intracranial extension.
Objectives: This report describes a really uncommon case of malignant otitis externa caused by P. mirabilis in a non-diabetic, immunocompetent patient.
Case presentation: A 53-year-old male with no relevant medical history presented with a four-month history of left-sided otorrhea, otalgia, and preauricular pain. Examination and imaging revealed purulent discharge and bone erosion, suggestive of MOE. Empirical treatment with amoxicillin/clavulanic acid was ineffective. Culture identified Proteus mirabilis, resistant to multiple antibiotics but sensitive to piperacillin/tazobactam, which was administered with supportive care. After 17 days of intravenous therapy, the patient improved and was discharged on oral ciprofloxacin to complete a three-month course. Follow-up confirmed clinical resolution without recurrence.
Conclusion: This case report highlights an exceptionally rare occurrence of MEO caused by P. mirabilis in an immunocompetent, non-diabetic patient. It emphasizes the need to consider uncommon pathogens and atypical clinical profiles in MOE. Early diagnosis, microbiological confirmation, and tailored antimicrobial therapy were critical for favorable outcomes.
1 Introduction
Malignant otitis externa (MOE) is a severe and potentially life-threatening infection of the external auditory canal that extends beyond the cutaneous lining, beginning as cellulitis and potentially progressing to chondritis, periostitis, or osteomyelitis. The condition is most commonly caused by Pseudomonas aeruginosa and can spread to adjacent soft tissues or even intracranial structures in advanced stages (1, 2). Although MOE is rare, its incidence has increased in at-risk populations—particularly among immunocompromised individuals—with diabetes mellitus reported in approximately 55–95% of cases (2–4).
The clinical presentation of MOE includes intense otalgia, headache, purulent discharge, and edema of the external auditory canal. Facial paralysis, often involving the facial nerve, is a frequent complication and underscores the importance of early diagnosis and timely treatment to prevent progression to severe outcomes such as osteomyelitis and meningitis (5, 6).
Recent studies have reported a rising incidence of MOE in non-diabetic individuals, accounting for 5 to 15% of all cases. For instance, Sideris et al. (7) found that approximately 11% of EOM cases occurred in patients without diabetes, highlighting other possible risk factors such as immunosuppression or foreign body exposure (7, 8). Other large-scale epidemiological studies from the United States and Taiwan have documented even higher proportions, with up to 45% of MOE cases occurring in non-diabetic patients, although diabetes remains strongly associated with MOE (OR = 7.50; 95% CI: 6.22–9.03) (3, 9).
Proteus mirabilis, a Gram-negative bacillus commonly associated with urinary tract and wound infections, is an infrequent but noteworthy pathogen in MOE. Compared to Pseudomonas aeruginosa, it has been less documented in this context. A study by Arsovic et al. (10) identified Proteus mirabilis in only one out of 30 positive cultures from MOE patients, underscoring its rarity and emerging clinical significance (11).
This report describes a really uncommon case of malignant otitis externa caused by Proteus mirabilis in a non-diabetic patient.
2 Case presentation
A 53-year-old male presented with a progressive four-month history of left-sided otorrhea, otalgia, and retro- and preauricular pain. He had no significant past medical history, including no diagnosis of diabetes mellitus. Prior treatment with amoxicillin/clavulanic acid had yielded no clinical improvement.
Physical examination revealed signs of cutaneous infection and bone erosion involving the anteroinferior and inferior walls of the external auditory canal (EAC). Otoendoscopy showed abundant yellowish, foul-smelling otorrhea (Figure 1). Based on these findings, the patient was admitted with a presumptive diagnosis of MOE for further evaluation and intravenous therapy.
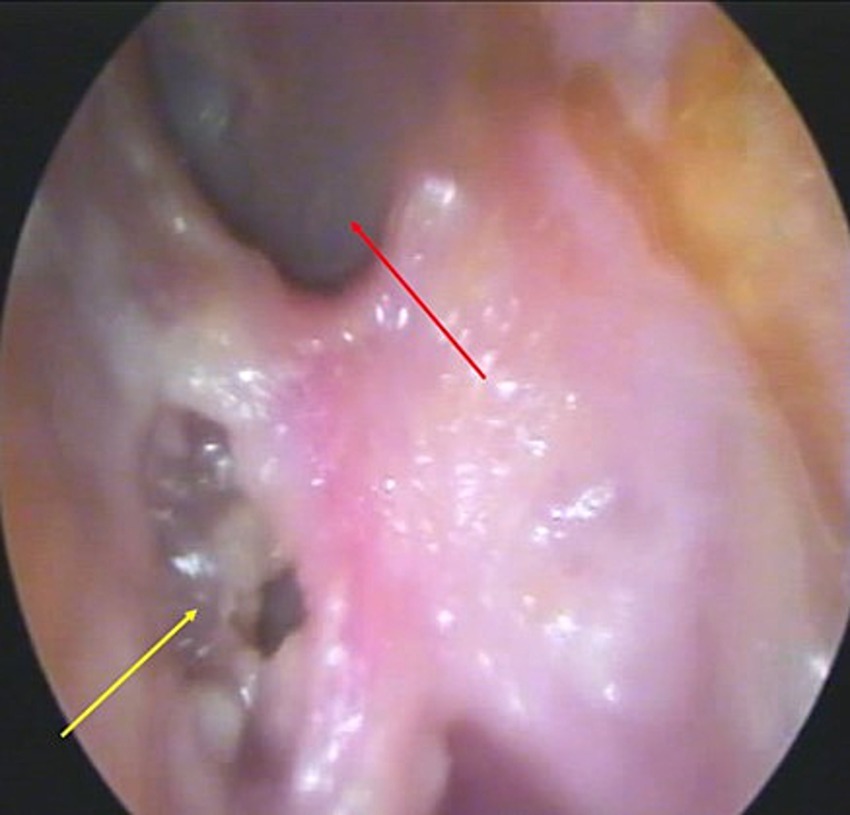
Figure 1. Otoendoscopy of the left ear. Showing bone erosion in the inferior wall of the external auditory canal (yellow arrow) with purulent otorrhea and an intact tympanic membrane (red arrow).
Initial laboratory investigations revealed leukocytosis of 20,050 cells/μL (reference: 3,600–10,500/μL) with 86% neutrophils, a normal blood glucose level of 91 mg/dL (reference: 70–110 mg/dL), and elevated C-reactive protein (CRP) at 2.4 mg/dL (reference: 0.0–2.0 mg/dL). Serological tests for VDRL and HIV were non-reactive, and blood cultures were negative. Culture of the ear secretion identified Proteus mirabilis, resistant to ampicillin, ampicillin/sulbactam, cefazolin, and TMP-SMX but sensitive to azithromycin, cefotaxime, ciprofloxacin, imipenem, meropenem, and piperacillin/tazobactam. Fungal culture was negative (Table 1).
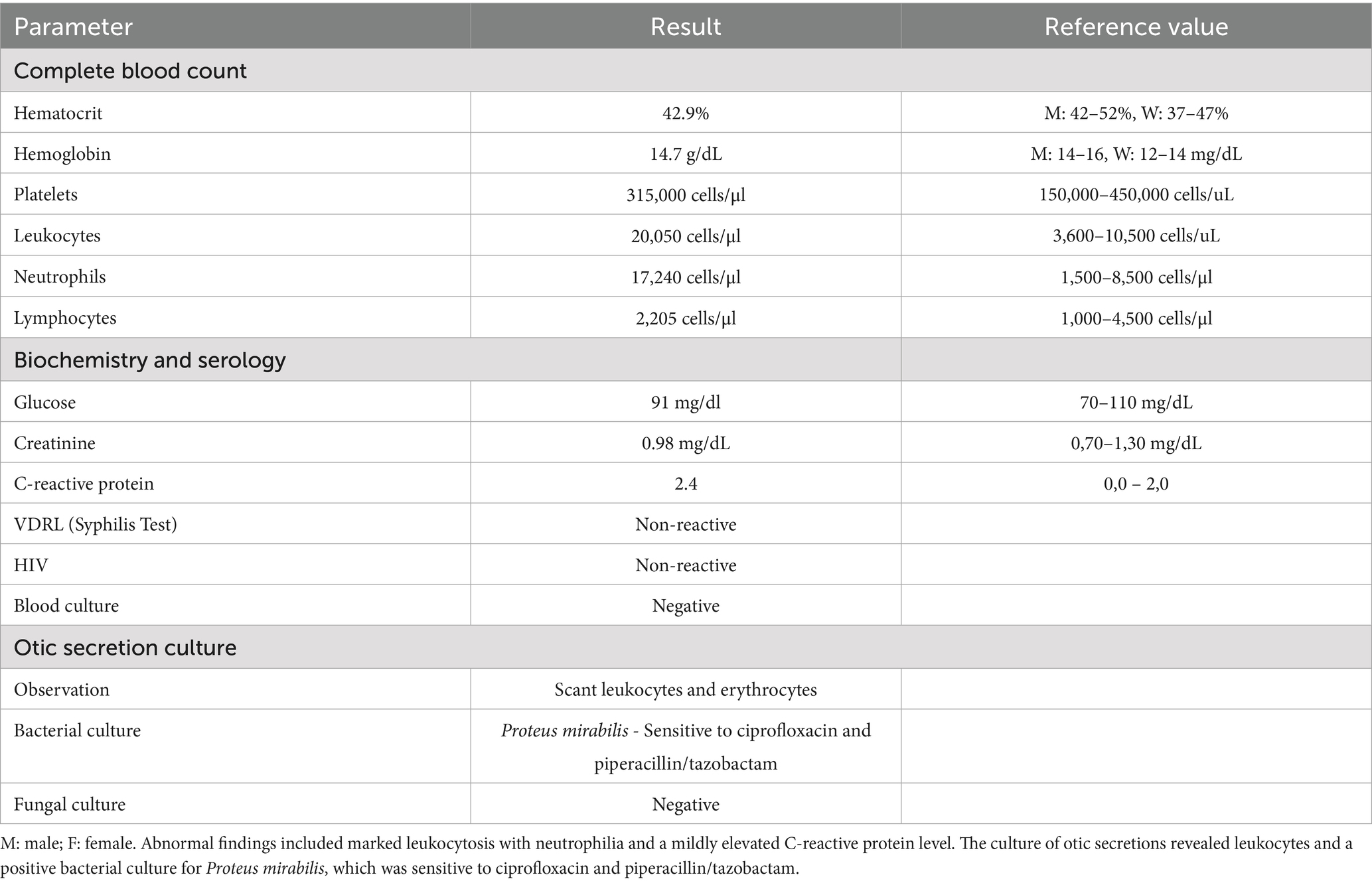
Table 1. Summary of laboratory and microbiological findings of patient with MOE.
On the third day of hospitalization, magnetic resonance imaging (MRI) was performed, revealing mastoid cell occupation on the left side, with signal intensity alterations along the lower border of the EAC. A 13 mm × 9 mm fluid-filled lesion in the inner third of the EAC demonstrated peripheral enhancement following gadolinium administration (Figure 2A). As part of the diagnostic workup, a computed tomography (CT) scan was also obtained, confirming soft tissue density in the anteroinferior wall of the EAC, with associated bone erosion—consistent with damage to the underlying bony structures of the anteroinferior EAC wall (Figures 2B,C).
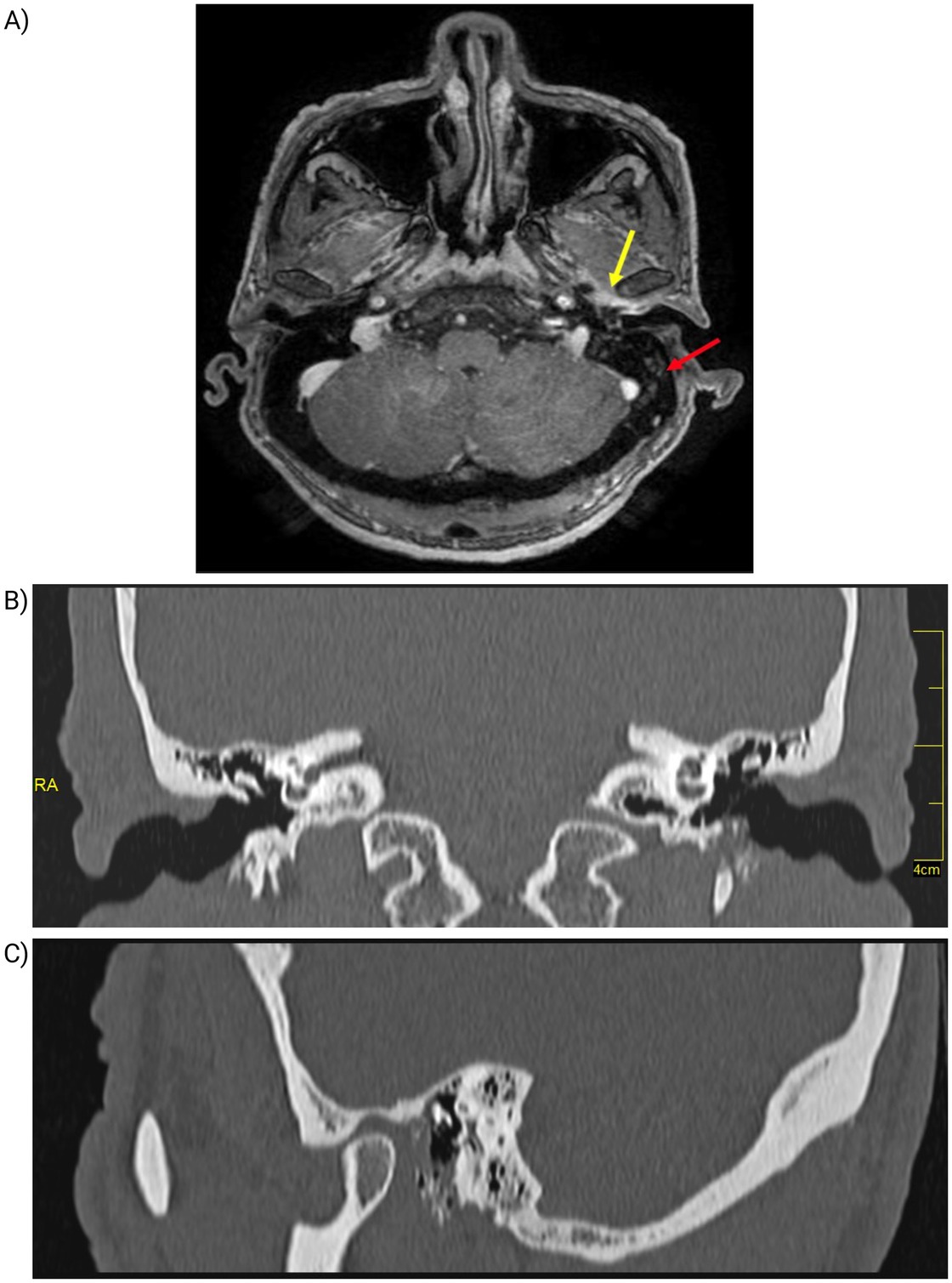
Figure 2. Imaging findings of the left ear. (A) Magnetic resonance imaging (MRI) of the left ear. Demonstrating opacification of the mastoid air cells (red arrow) and altered signal intensity at the inferior margin of the external auditory canal (yellow arrow). (B,C) Computed Tomography of the Left Ear. (B) Coronal CT scan shows bone erosion in the anteroinferior and inferior walls of the external auditory canal (red arrow). (C) CT scan shows soft tissue density with bone involvement (yellow arrow).
Based on culture sensitivity results, intravenous piperacillin/tazobactam (4.5 g every 6 h) was initiated, along with analgesics and anti-inflammatory agents including dexamethasone, diclofenac, and paracetamol. Multiple aspirations of purulent material were performed during hospitalization, revealing granulation tissue and necrotic debris, which were debrided.
After 7 days of treatment, leukocyte counts declined to 11,700 cells/μL, with normalization of neutrophil levels. Liver and metabolic function tests remained within normal ranges. The patient continued intravenous piperacillin/tazobactam throughout his 17-day hospital stay, showing consistent clinical improvement. At discharge (day 17), he was transitioned to oral ciprofloxacin (500 mg every 12 h) and omeprazole (20 mg daily) to complete a three-month antibiotic regimen. Outpatient follow-up was scheduled biweekly for the first 2 months and monthly thereafter for a total of 6 months.
At the three-month follow-up, the patient demonstrated substantial clinical improvement. Repeat otoendoscopy showed near-complete resolution of the infection (Figure 3). Long-term monitoring remains ongoing to ensure full recovery and prevent recurrence. This case report was prepared in accordance with the CARE (CAse REport) guidelines to ensure transparency and completeness in clinical case reporting.
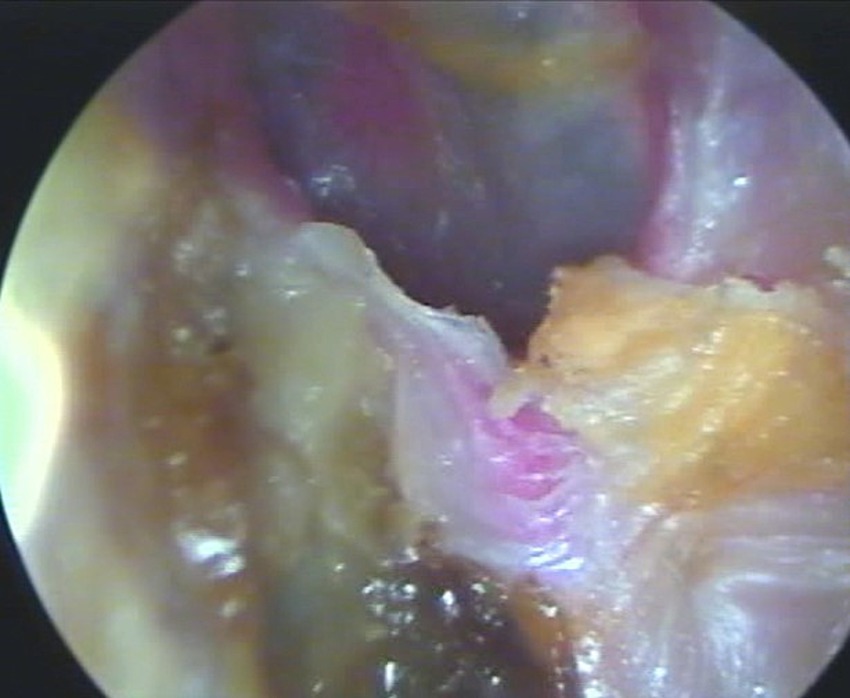
Figure 3. Follow-up otoendoscopy of the left ear. The image shows a dry ear without purulent discharge, cerumen production, and an intact tympanic membrane.
3 Discussion
MOE is a severe infection of the external auditory canal that primarily affects elderly and immunocompromised individuals, with diabetes mellitus being the most common underlying condition associated with its development (7). This case emphasizes the importance of early diagnosis and appropriate treatment, even in atypical presentations. Notably, the patient in this report had no underlying comorbidities, such as diabetes mellitus or other immunosuppressive states (2, 12, 13) (Figure 4).
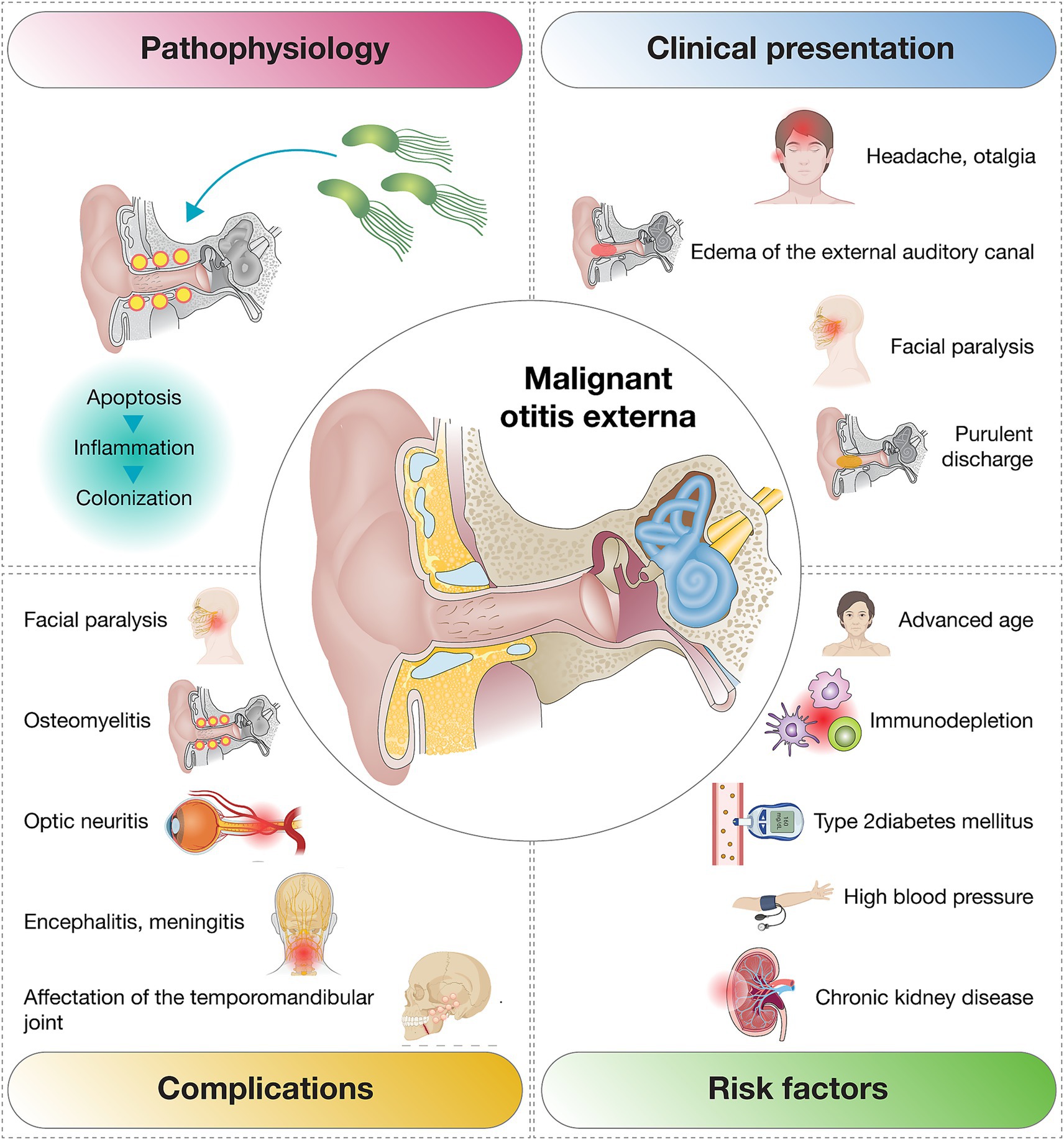
Figure 4. Overview of the most frequent clinical presentations, complications, and risk factors associated with malignant otitis externa.
In this case, the clinical presentation included otalgia and otorrhea in the absence of systemic symptoms, aside from leukocytosis noted on admission. This highlights the need for high clinical suspicion and timely diagnostic intervention to prevent the aggressive progression often seen in MOE (14). The patient presented with persistent, severe otalgia, purulent otorrhea, inflammation of the external auditory canal, and bone necrosis, as confirmed by otoscopic and imaging findings. Both CT and MRI were performed to confirm the diagnosis and assess the extent of bony involvement. Additional diagnostic modalities, such as bone scintigraphy, can also be considered to evaluate skull base involvement when needed (15).
Moreover, inflammatory biomarkers such as the erythrocyte sedimentation rate (ESR) may serve as useful adjuncts in the diagnosis and monitoring of MOE (16). Although ESR was not measured in this case, its inclusion is supported by literature, particularly in patients with suspected systemic inflammatory responses or advanced disease. Future case series and clinical guidelines should consider incorporating ESR as part of the standard diagnostic workup for MOE.
The clinical and radiological features in this case met the major and minor diagnostic criteria proposed by Cohen and Friedman in 1987, reaffirming the enduring relevance of these criteria, especially in resource-limited settings (15).
Given the initial clinical and imaging findings, carcinoma of the external auditory canal was considered as a differential diagnosis. This was based on the lesion’s appearance and imaging characteristics, which raised suspicion for a malignant process. Although no biopsy was performed, the absence of suspicious masses on imaging, the lack of progressive lesion growth, and the favorable response to targeted antibiotic therapy supported a non-neoplastic etiology. Culture of the ear discharge revealed a predominant inflammatory process with no evidence of malignancy, thereby excluding carcinoma and redirecting management toward MOE (10, 15).
The clinical manifestations observed in this case align with those reported by Arsovic et al. (10), who identified otalgia (76%), otorrhea (79%), external auditory canal edema (45%), and granulation tissue (31%) as the primary symptoms among 30 MOE patients. Such consistency underscores the importance of recognizing these hallmark symptoms in clinical practice.
Identification of the causative pathogen is critical for achieving favorable outcomes in MOE. While Pseudomonas aeruginosa is implicated in over 95% of cases, Aspergillus accounts for a smaller proportion (11). However, rare pathogens like Proteus mirabilis have been documented in isolated cases. For instance, Arsovic et al. (10) reported P. mirabilis in only one out of 30 MOE cases, a finding corroborated by AlSharhan et al. (17), who identified P. mirabilis as the causative agent in just one of 28 patients with otogenic skull base osteomyelitis. The identification of P. mirabilis in this patient highlights the need to consider uncommon pathogens in MOE, particularly in atypical presentations or non-immunosuppressed patients.
Antimicrobial resistance presents an increasing challenge in the management of MOE, underscoring the necessity of obtaining cultures and antibiotic susceptibility testing to guide treatment (18). In this case, the P. mirabilis was resistant to several agents, including ampicillin (a resistance rate reported in 10–20% of isolates), but was sensitivity to piperacillin-tazobactam, ciprofloxacin, and other agents, allowing targeted treatment. Multidisciplinary management, involving otorhinolaryngologists and infectious disease specialists, proved instrumental in achieving a favorable outcome (19). Intravenous piperacillin-tazobactam combined with serial aspiration of purulent discharge successfully controlled the infection, consistent with literature advocating aggressive antibiotic therapy to prevent complications such as sepsis or temporal bone osteomyelitis (17, 20). Additional interventions, such as surgical debridement or hyperbaric oxygen therapy, are typically reserved for refractory cases or poor responses to medical treatment (21–23).
This case broadens the diagnostic and therapeutic understanding of MOE, particularly in non-immunosuppressed patients. It underscores the importance of continuing education for healthcare professionals to improve awareness of MOE, including its risk factors, clinical presentation, and management strategies in atypical scenarios. Enhanced awareness could improve early diagnosis, guide tailored treatment, and ultimately lead to better outcomes for affected patients.
4 Conclusion
This case report describes an exceptionally rare instance of MEO caused by P. mirabilis in a non-immunocompromised patient, broadening the understanding of the clinical spectrum and etiological diversity of this condition. It underscores the need to consider atypical pathogens in cases where traditional risk factors, such as diabetes mellitus or immunosuppression, are absent.
The favorable outcome in this patient highlights the pivotal role of early diagnosis, thorough microbiological evaluation, and tailored antibiotic therapy in the successful management of MEO. The infection was effectively controlled through the use of broad-spectrum antibiotics, selected based on culture and sensitivity testing, combined with supportive interventions such as serial aspiration of purulent secretions. This case emphasizes the importance of a comprehensive and individualized approach to managing this potentially life-threatening condition.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
FA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Writing – original draft. ML: Conceptualization, Formal analysis, Investigation, Methodology, Resources, Validation, Writing – original draft. SP: Conceptualization, Data curation, Investigation, Methodology, Resources, Validation, Writing – original draft. GG: Conceptualization, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft. AL-C: Data curation, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. JI-C: Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sando, I, Harada, T, Okano, Y, Saito, R, and Caparosa, RJ. Temporal bone histopathology of necrotizing external otitis. A case report. Ann Otol Rhinol Laryngol. (1981) 90:109–15. doi: 10.1177/000348948109000203
2. Treviño González, JL, Reyes Suárez, LL, and Hernández de León, JE. Malignant otitis externa: an updated review. Am J Otolaryngol. (2021) 42:102894. doi: 10.1016/j.amjoto.2020.102894
3. Yang, T-H, Xirasagar, S, Cheng, Y-F, Wu, C-S, Kao, Y-W, Shia, B-C, et al. Malignant otitis externa is associated with diabetes: a population-based case-control study. Ann Otol Rhinol Laryngol. (2020) 129:585–90. doi: 10.1177/0003489419901139
4. Hodgson, SH, Sinclair, VJ, Arwyn-Jones, J, Oh, K, Nucken, K, Perenyei, M, et al. Characteristics, management and outcome of a large necrotising otitis externa case series: need for standardised case definition. J Laryngol Otol. (2022) 136:604–10. doi: 10.1017/S002221512100462X
5. Di Lullo, AM, Russo, C, Piroli, P, Petti, A, Capriglione, P, Cantone, E, et al. Malignant otitis external: our experience and literature review. Am J Case Rep. (2020) 21:e925060. doi: 10.12659/AJCR.925060
6. Mahdyoun, P, Pulcini, C, Gahide, I, Raffaelli, C, Savoldelli, C, Castillo, L, et al. Necrotizing otitis externa: a systematic review. Otol Neurotol. (2013) 34:620–9. doi: 10.1097/MAO.0b013e3182804aee
7. Sideris, G, Latzonis, J, Avgeri, C, Malamas, V, Delides, A, and Nikolopoulos, T. A different era for malignant otitis externa: the non-diabetic and non-immunocompromised patients. J Int Adv Otol. (2022) 18:20–4. doi: 10.5152/iao.2022.21313
8. Glikson, E, Sagiv, D, Wolf, M, and Shapira, Y. Necrotizing otitis externa: diagnosis, treatment, and outcome in a case series. Diagn Microbiol Infect Dis. (2017) 87:74–8. doi: 10.1016/j.diagmicrobio.2016.10.017
9. Sylvester, MJ, Sanghvi, S, Patel, VM, Eloy, JA, and Ying, Y-LM. Malignant otitis externa hospitalizations: analysis of patient characteristics. Laryngoscope. (2017) 127:2328–36. doi: 10.1002/lary.26401
10. Arsovic, N, Radivojevic, N, Jesic, S, Babac, S, Cvorovic, L, and Dudvarski, Z. Malignant otitis externa: causes for various treatment responses. J Int Adv Otol. (2020) 16:98–103. doi: 10.5152/iao.2020.7709
11. Muraleedharan, M, Keshri, A, Rao, RN, Mehrotra, A, Das, KK, Dubey, A, et al. Aspergillus infections of lateral skull base: a case series. Eur Arch Otorrinolaringol. (2024) 281:1221–9. doi: 10.1007/s00405-023-08218-z
12. Liu, X-L, Peng, H, Mo, T-T, and Liang, Y. Malignant otitis externa in a healthy non-diabetic patient. Eur Arch Otorrinolaringol. (2016) 273:2261–5. doi: 10.1007/s00405-015-3738-y
13. Unadkat, S, Kanzara, T, and Watters, G. Necrotising otitis externa in the immunocompetent patient: case series. J Laryngol Otol. (2018) 132:71–4. doi: 10.1017/S0022215117002237
14. Ali, T, Meade, K, Anari, S, ElBadawey, MR, and Zammit-Maempel, I. Malignant otitis externa: case series. J Laryngol Otol. (2010) 124:846–51. doi: 10.1017/S0022215110000691
15. Cohen, D, and Friedman, P. The diagnostic criteria of malignant external otitis. J Laryngol Otol. (1987) 101:216–21. doi: 10.1017/s0022215100101562
16. Al Aaraj, MS, and Kelley, C. Necrotizing (Malignant) Otitis Externa. Treasure Island, FL: StatPearls Publishing (2025).
17. AlSharhan, SS, Alwazzeh, MJ, Alshrefy, AJ, Albahrani, NA, Telmesani, LS, AA, AG, et al. Microbial spectrum, management challenges, and outcome in patients with otogenic skull base osteomyelitis. Infez Med. (2024) 32:340–51. doi: 10.53854/liim-3203-8
18. Frost, J, and Samson, AD. Standardised treatment protocol for necrotizing otitis externa: retrospective case series and systematic literature review. J Glob Antimicrob Resist. (2021) 26:266–71. doi: 10.1016/j.jgar.2021.06.015
19. Dhariwal, A, Manjaly, JG, Patel, B, Morris-Jones, S, David, K, Khetarpal, P, et al. Management and clinical outcomes of 37 patients with necrotizing otitis externa: retrospective review of a standardized 6-week treatment pathway. J Int Adv Otol. (2023) 19:223–7. doi: 10.5152/iao.2023.22637
20. Lambor, DV, Das, CP, Goel, HC, Tiwari, M, Lambor, SD, and Fegade, MV. Necrotising otitis externa: clinical profile and management protocol. J Laryngol Otol. (2013) 127:1071–7. doi: 10.1017/S0022215113002259
21. Álvarez-Álvarez, M, Benito-Orejas, JI, Carranza-Calleja, MA, Cámara-Arnaz, JA, Viveros-Díez, P, Santos-Pérez, J, et al. Otitis externa maligna. Experiencia a lo largo de 25 años en un hospital de tercer nivel. Revista. ORL. (2023) 14:63. doi: 10.14201/orl.31063
22. Balcázar Rincón, LE, and Ramírez Alcántara, YL. Otitis externa maligna. Rev Esp Méd Quirúrg. (2014) 19:104–9.
Keywords: malignant otitis externa, Proteus mirabilis, atypical presentation, targeted antibiotic therapy, non-immunocompromised patient
Citation: Arias Rodríguez FD, Larenas M, Paredes S, Giuliano G, López-Cortés A and Izquierdo-Condoy JS (2025) Expanding the diagnostic spectrum of malignant otitis externa: a case report of proteus infection in a non-immunosuppressed patient. Front. Med. 12:1577525. doi: 10.3389/fmed.2025.1577525
Edited by:
Xin Zhou, Stanford University, United StatesReviewed by:
Therese Ovesen, Aarhus University, DenmarkChristos Tsilivigkos, National and Kapodistrian University of Athens, Greece
Copyright © 2025 Arias Rodríguez, Larenas, Paredes, Giuliano, López-Cortés and Izquierdo-Condoy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan S. Izquierdo-Condoy, anVhbjFpenF1aWVyZG8xMUBnbWFpbC5jb20=