 José Ángel García-Sáenz1*
José Ángel García-Sáenz1* Álvaro Rodríguez-Lescure2
Álvaro Rodríguez-Lescure2 Silvia Antolin3
Silvia Antolin3 Blanca Cantos4
Blanca Cantos4 Miguel Ángel Seguí5María Antonia Gimón6Raül Rubio Renau7Carlota Solà Marsiñach7Jesús Martín Illán8Rocío Fonseca Vallejo8Yaiza Gimeno Guadalupe9Noelia Alfaro Oliver9Joaquín Gavilá10
Miguel Ángel Seguí5María Antonia Gimón6Raül Rubio Renau7Carlota Solà Marsiñach7Jesús Martín Illán8Rocío Fonseca Vallejo8Yaiza Gimeno Guadalupe9Noelia Alfaro Oliver9Joaquín Gavilá10- 1Oncology Department, Hospital Ruber Internacional, Madrid, Spain
- 2Department of Medical Oncology, University General Hospital of Elche, Elche, Spain
- 3Oncology Department, A Coruña University Hospital Complex (CHUAC), A Coruña, Spain
- 4Department of Medical Oncology, Puerta de Hierro University Hospital Majadahonda, Majadahonda, Spain
- 5Oncology Department, Parc Taulí University Hospital, Sabadell, Spain
- 6Spanish Federation of Breast Cancer FECMA, Presidency, Madrid, Spain
- 7Evidence Generation Department, A Piece of Pie, Barcelona, Spain
- 8Medical Department, Daiichi Sankyo Spain, Madrid, Spain
- 9Medical Department, AstraZeneca Farmacéutica Spain, Madrid, Spain
- 10Oncology Department, Instituto Valenciano de Oncologia, Valencia, Spain
Introduction and objectives: Qualitative evidence regarding the structural barriers embedded in healthcare ecosystems impacting Human Epidermal Growth Factor Receptor 2 metastatic breast cancer (HER2+ MBC) patients’ communication and information needs is scarce. This study explored patient and healthcare professionals’ perspectives on said structural barriers and communication delivery.
Methods: Ethnographic, qualitative, observational, multicenter and cross-sectional study with HER2+ MBC patients and Health Care Professionals. Qualitative data collected through remote semi-structured interviews with patients (n = 14) and healthcare professionals (n = 10). The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ)-C30 and the disease-specific EORTC QLQ-BR45 questionnaires were collected as Quality of Life measures.
Results: Regarding the communication and information needs of patients, there were four areas these were lacking most: (1) disease and treatment, (2) psychosexual support, (3) navigation of the healthcare and social security systems to reduce the financial burdens, and (4) patient associations. In reference to delivery of information from healthcare professionals, there were four areas that were lacking: (1) time, (2) interpersonal skills and communications training, (3) specialized oncology nursing training, and (4) lack of an evaluation system assessing patient-centered care and patient satisfaction.
Conclusion: Results emphasize how structural barriers embedded in healthcare systems can lead to and intensify information and communication gaps, which therefore emphasizes that to provide optimal, patient-centric care, these structural barriers must be addressed.
1 Introduction
Breast cancer (BC) remains a significant and highly prevalent cancer, accounting for 24.5% of all cancer cases and 15.5% of all cancer related mortalities worldwide (1, 2). Projections suggest a 31% increase in new BC cases by 2040, with mortality rates expected to rise due to population growth and aging (1). In Spain, BC accounts for 12% of all diagnosed cancers, and around 5–6% of cases are already metastasized at the time of diagnosis (3). The human epidermal growth factor receptor 2 (HER2) is a tyrosine kinase receptor that signals to promote several growth-related pathways. BC that overexpress this receptor are classified as HER2-positive (HER2+), accounting for 15–20% of all BC cases worldwide (4–6). In Spain, early estimates approximate that HER2+/Hormone Receptor-positive (HR+) and HER2+/HR-negative (HR-) account for 16% and 9.4% BC cases, respectively (7). HER2+/HR- BC patients experience more aggressive disease and worse outcomes than HR+ patients, requiring targeted anti-HER2 therapies with chemotherapy, and endocrine therapy (8). These treatments have improved patient survival rates in recent years and they often require long-term care (9, 10).
This study is situated within the Spanish context, where a publicly funded National Health System operates. The system is structured as a decentralized health network governed by the Autonomous Communities and implements integrated cancer care strategies aligned with the national Cancer Strategy 2006–2014 (11). In 2024, 36.395 new BC cases were diagnosed in Spain, representing the most common cancer among women (12). Although the patient experience of metastatic BC has been only briefly explored in Spain, one qualitative study mapping BC patient journeys identified significant gaps in emotional and social support among patients at an incurable stage, highlighting the need to implement a stronger psychological care approach (13) Limited access to new therapies is also an area of concern in the Spanish context, since the country experiences longer delays than most EU countries between drug approval from the European Medicines Agency and reimbursement from the health system, a necessary condition for prescription (14). This delay may negatively impact patients’ treatment trajectories and increase the psychosocial burden associated with BC. Several studies have reported on the unmet needs of patients with BC and, to a lesser extent, HER2+ metastatic breast cancer (MBC). These highlight impacts on physical/daily life, psychological impacts, symptoms burden, and patient care, as well as communication and information needs (15–20). Given that patient-centric communication is increasingly being recognized to positively impact treatment adherence, quality of care, management of chronic disease and other health outcomes (21), there is a significant amount of literature discussing the information needs of oncological patients more generally, and BC patients in particular (17, 22–25). This literature is frequently paired with recommendations to improve doctor-patient communication, asking healthcare professionals (HCPs) to be mindful of the emotional and psychosocial needs of patients, and so on (26–28). This is considered essential for patients struggling to cope with parts of their journey, such as diagnosis, treatment, and the impact on inter-personal relationships and social engagements (26–28).
However, there is a relative dearth of research into the constraints faced by HCPs within the healthcare system and how they impact information delivery. Notable constraints include geographical limitations, cost restrictions, inadequate HCP training, and time pressures (29–35). Acknowledging these barriers is essential, since addressing patients’ information needs without considering the characteristics of the healthcare system places unrealistic expectations on HCPs.
To address this gap, this paper presents the perspectives of both patients and HCPs. It gives voice to women with HER2+ MBC, illustrating how HCPs could enhance communication delivery from the patients’ viewpoint. Additionally, it outlines the structural barriers faced by oncologists and nurses when it comes to addressing communication delivery. We focus on patients with a diagnosis of HER2+ stage IV BC, a unique clinical subgroup characterized both by therapeutic advances and ongoing challenges. The appearance of targeted therapies in recent years has significantly improved disease outcomes and survival rates (36). Nevertheless, HER2+ stage IV BC remains incurable, situating patients in a complex clinical and emotional situation which is different from early-stage diagnosis (37). This clinical scenario gives rise to specific complexities related to patients’ informational needs, mainly because they face prognostic uncertainty and navigate the blurry boundaries between palliative and chronic care, as we have shown in a separate publication (57).
2 Patients and methods
2.1 Study design
The EtnobreastHER2 Study is an ethnographic, qualitative, observational, multicenter and cross-sectional study that aimed to recruit 20 patients with HER2+ MBC, five oncologists specialized in the treatment of BC and five nurses routinely seeing patients with BC from five university hospitals in Spain. Patients were recruited face-to-face during their routine visits. After obtaining informed consent, doctors compiled information related to patients’ personal characteristics, disease and treatment. This contact information was shared with an anthropologist, who scheduled and conducted the interviews with patients. The interviewer was female, white and Spanish, and had 10 years of experience conducting interviews with patients in the medical field. Interview questions were open-ended and aimed to elucidate the lived experience of HER2+ MBC patients. HCPs were recruited by the principal investigators of the study from the participating hospitals. HCPs were interviewed after almost all patient interviews were conducted, with the aim of complementing their view. Interview questions were also open-ended but covered the themes identified in patient interviews.
2.2 Sample and recruitment
All patients to be included in the study had to have a documented diagnosis of locally advanced or HER2+ MBC, be receiving second line treatment according to SEOM (Spanish Society of Medical Oncology) clinical guidelines after having progressed from first line treatment at the time of the inclusion and be ≥ 18 years at the time of consent. Participating in a clinical trial, being hospitalized at the time of inclusion, having been previously diagnosed with cancer, being under treatment for other types of cancer, or holding a managing position in a patient association were all exclusion criteria. Participants were recruited consecutively. Of the 17 patients who initially agreed to participate, three withdrew their consent: two of them stopped responding to requests to participate without providing any reason, and one responded she did not feel well enough to participate in an interview. Patients who agreed to participate were recruited from four university hospitals in Spain. All 10 HCPs had to routinely see patients with BC. Participating HCPs were four oncologists and six nurses.
Literature discussing sample sizes in qualitative research estimate that a sample size of 10 or more is considered sufficient to reach empirical saturation –the point in which increasing the number of observations does not provide new data– in ethnographic studies (38). With a sample size of 24 participants, our study falls within the recommended guidelines and allowed us to reach saturation.
2.3 Data gathering and analysis
Patients and HCPs participated in semi-structured interviews –2h long for patients and 90-min long for HCPs–. Interviews were aimed to be carried out in-person but were allowed to be performed remotely if local healthcare authorities or medical centers recommended preventive measures against covid-19, or if the patient preferred so. In such cases, remote interviews were to be performed using encrypted tools such as Zoom, Teams or Skype to ensure the protection of patients’ private data. Eventually, all interviews were conducted remotely via Teams, following participants’ preferences. Semi-structured interviews allowed participants to raise issues of concern while simultaneously covering the researcher’s areas of interest, and only the participant and the interviewer were present. There was no relationship between the interviewer and participants prior to the study. At the beginning of the interview, patients were informed of the interviewer’s position and the research goals. The study was neither pilot tested nor were repeat interviews conducted. Fieldnotes were made during and after the interview to complement the data collected, which was used in the analysis for this paper. Transcripts were not returned to participants for comment or correction, and they did not provide feedback on the findings.
Additionally, patients completed two patient-reported outcome measures (PROMs) at the beginning of the interviews in the presence of the ethnographer but without intervention. These were the generic European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) and the disease-specific EORTC QLQ-BR45 questionnaires. PROMs were used as a conversation starter, to approach sensitive topics, and to prompt patients to self-reflect on their condition without the intervention of the ethnographer. The information gathered with these PROMs was analyzed descriptively.
Two anthropologists independently coded all fieldwork materials following a phenomenological perspective, which aims to elucidate the lived experience of a disease and the conditions shaping said experience (39, 40). The analytical process was both inductive and deductive, meaning that themes were identified by topics emerging directly from the data (inductive inference) and applying prior knowledge (deductive inference) (41). Only themes which reached empirical saturation, the point at which new data no longer emerge, were selected for analysis (42, 43). A vast amount of themes emerging from the EtnobreastHER2 Study reached saturation. To be able to present them in depth, this study solely focuses on those related to information needs and barriers to patient-centered care. Additionally, there is a description of minor themes in the results and discussion parts of this article.
3 Results
3.1 Participant characteristics
The final sample consisted of 24 participants: 14 patients, four oncologists and six nurses. All patients interviewed had stage IV HER2+ BC and were receiving second line treatment after having progressed from a first line. Patients’ mean age was 53,5 years, and their mean time since diagnosis was 5,2 years. HCPs were 80% female. Participants’ demographic and clinical characteristics are compiled in Table 1.
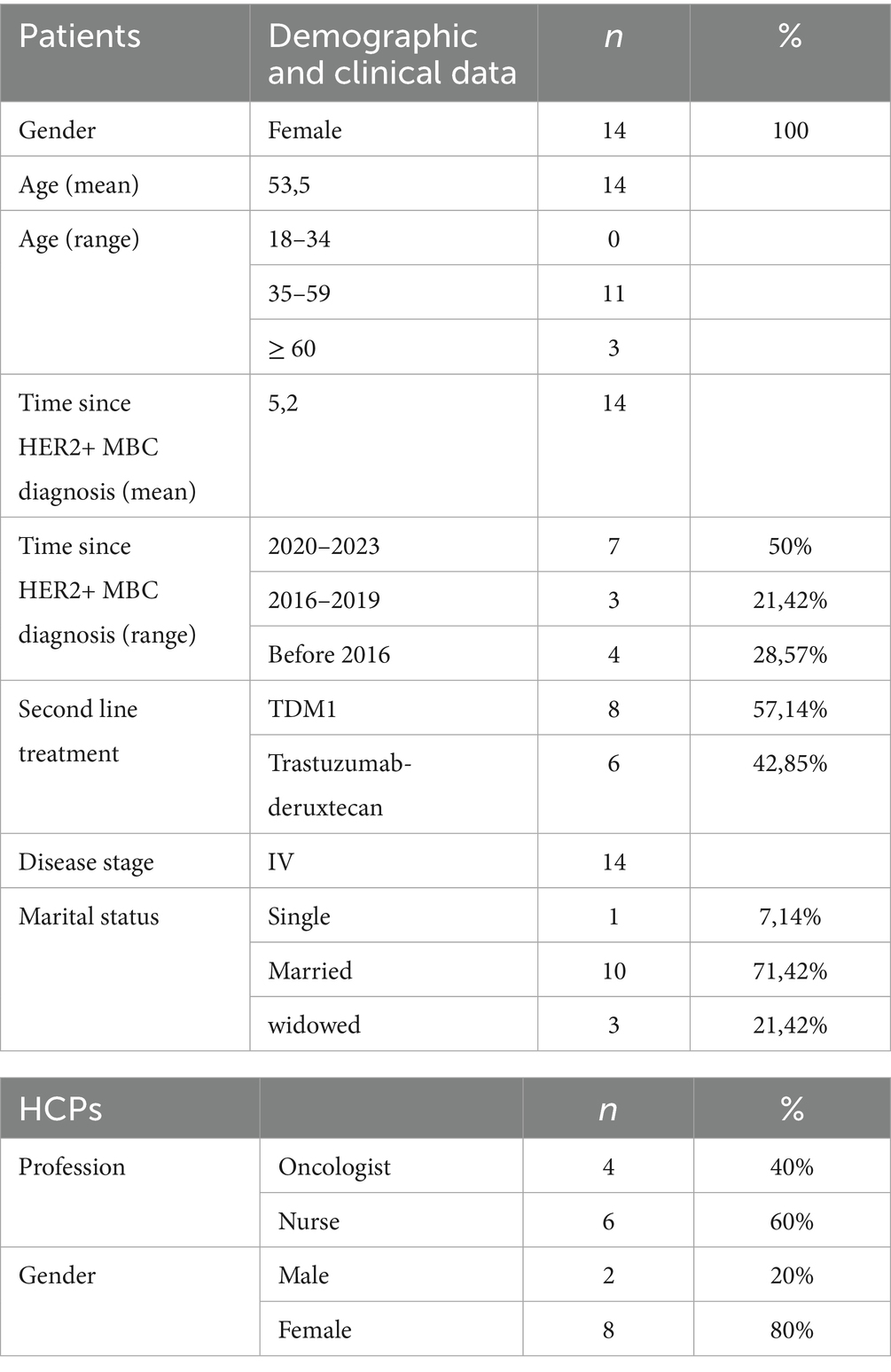
Table 1. Participant characteristics.
3.2 Delivery of patient-centric communication: the patients’ perspective
Patients in our study identified several areas of improvement in the delivery of patient-centric communication for HER2+ MBC. Illustrative quotes on this topic can be found in Table 2.
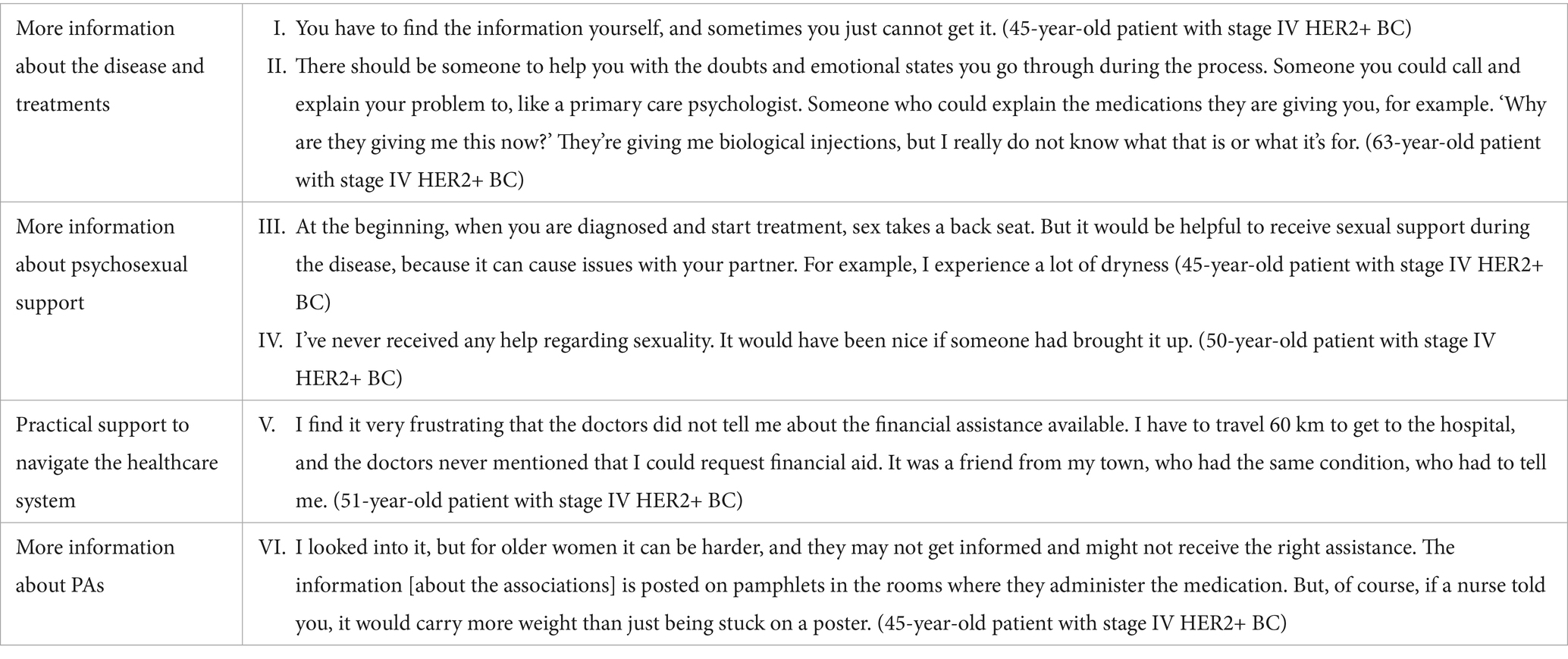
Table 2. Delivery of patient-centric communication: the patients’ perspective.
First, eight patients (57%) were not satisfied with the amount and kind of information received regarding the disease and treatments. Some preferred to have more time to ask questions and lengthier explanations, while others preferred to receive simpler explanations with less medical jargon. Reasons for this included: (a) not understanding the information provided and (b) not being able to properly transmit to their caregivers the seriousness of their condition. As a result of point (a), patients stopped asking questions, anticipating they would not understand HCPs’ answers, and looked for information online. As a result of point (b), patients’ sense of being misunderstood and unsupported by their social circles increased, thus negatively impacting their mood (Table 2; verbatims I-II).
Second, eight patients (57%) wanted to receive more information on psychosexual support. Most patients explained not being interested in sexual activity (Table 2; verbatims III-IV). Due to their loss of libido and decreased engagement in sexual activity, some women felt they could not satisfy their partners, with some fearing their partners would leave them. Others felt that being sexually active and enjoying sexual activity was part of being healthy and returning to normalcy and therefore strived to achieve it. The descriptive analysis of the EORTC QLQ-BR45 showed that more than half of the women were ‘not at all interested’ in sex (eight), six were only ‘a little interested,’ and none were ‘quite a bit interested’ or ‘very much interested.’ Furthermore, nine were ‘not at all sexually active,’ five were ‘a little active,’ and none were ‘quite a bit’ or ‘very much active’. From those who were sexually active, none did ‘not enjoy sexual activity,’ five ‘enjoyed it a little,’ and none ‘enjoyed it quite a bit’ or ‘enjoyed it very much.’ PROM results regarding this topic can be found in Table 3.
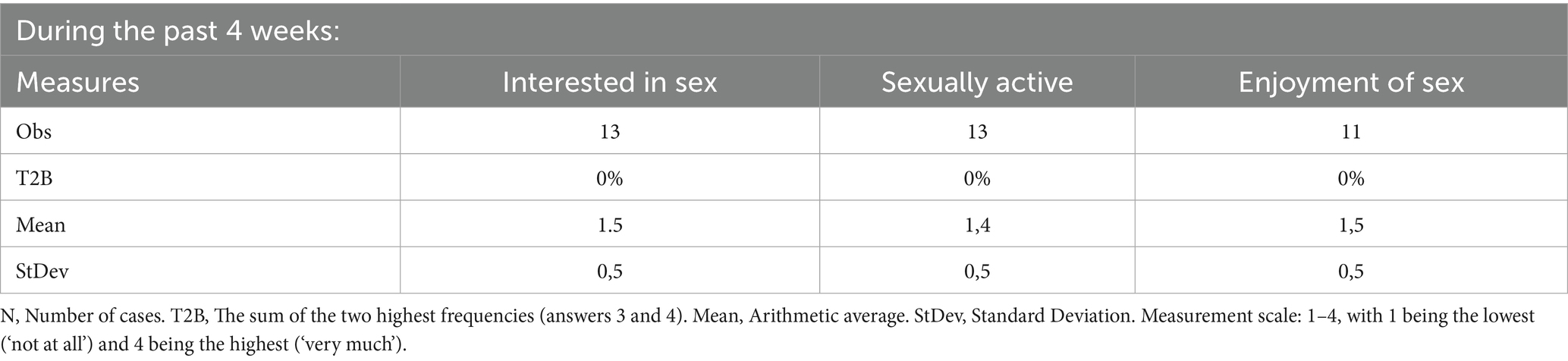
Table 3. Responses to EORTC QLQ-BR45 questions on sexuality.
Third, eight patients (57%) wanted to receive practical support on how to navigate the healthcare and social security systems to reduce the financial burden the disease had on themselves and their families. Some patients would have liked their HCPs to recommend resources where to obtain wigs and creams for free if possible, or at a reasonable price. Others would have liked their HCPs to draw attention to social security services or non-governmental organizations (NGOs) that could help with their homecare or transportation needs, especially when they had to travel long distances to access care. These patients had found in retrospect, via friends or acquaintances, that such services existed and that they could benefit from them (Table 2; verbatim V).
Fourth, seven patients (50%) wanted to receive more information about patient associations (PAs). Some patients were members of PAs and benefited from sharing their experiences with other patients. However, they had heard about said groups from their acquaintances, when they would have rather heard about them from their HCPs (Table 2; verbatim VI). Other patients did not want to socialize with other patients, arguing that they did not feel emotionally prepared to face others in similar circumstances. Nevertheless, many of these patients were unaware that socializing with other patients is not the only role provided by PAs; in retrospect, they found out about the resources provided by these groups, such as psychological support and practical resources to improve QoL, such as discounted sports activities and social aid. These patients said they would have appreciated information from their HCPs clarifying this role of PAs.
3.3 Doctor-patient communication: the HCPs’ perspective
HCPs were mostly aware of the perspective of the patients regarding information delivery. All 10 HCPs considered important to address it to improve patient-centered care. However, they argued that there were structural barriers hindering the process. Illustrative quotes regarding this topic can be found in Table 4.
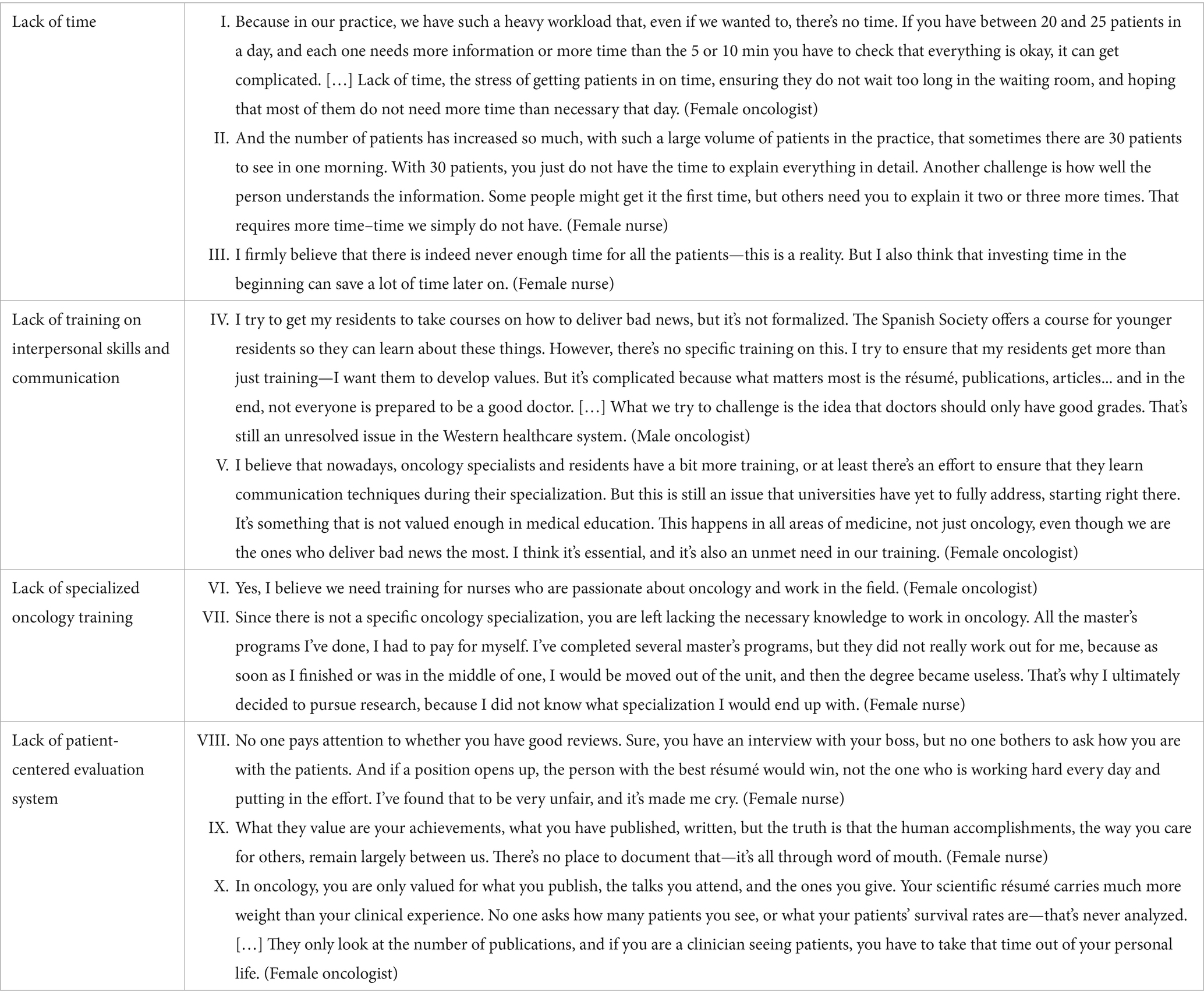
Table 4. Delivery of patient-centric communication: the HCPs’ perspective.
The first barrier, identified by all 10 HCPs (100%), was the lack of time to dedicate to each of their patients due to an overburdened healthcare system. This precluded the possibility to provide more information regarding all the unresolved issues raised by patients (Table 4; verbatims I-III). Several HCPs reported that they usually lacked sufficient time to provide detailed explanations during consultations. The average duration of five to 10 min per patient was described as insufficient for thoroughly addressing all patients’ questions or providing more comprehensive explanations, particularly to those who struggled to understand medical information. This limitation was also identified in relation to psychosexual health, a topic that patients rarely raised spontaneously and, as a result, was often overlooked during medical visits. All HCPs emphasized the negative impact that limited time during consultations had on patients’ satisfaction.
The second barrier, identified by nine HCPs (90%), was a lack of training in interpersonal skills and the communicative aspects of the profession. HCPs emphasized that training on adequate communication, delivery of bad news, and so on, would help them address the needs of patients. HCPs emphasized their lack of training to be an emotional pillar in times of need, highlighting that the relevant skills were acquired with practice and trial and error. These left young HCPs, and young nurses in particular, feeling inadequate in their ability to emotionally support their patients (Table 4; verbatims IV-V). This difficulty was also evident in the limited information provided to patients regarding PAs, as highlighted in patients’ accounts. HCPs considered they often lacked enough knowledge about the specific forms of support PAs could offer. According to their accounts, specific training programs for professionals should be implemented to enhance their understanding of the support offered by PAs, as well as the existing financial assistance and public subsidies available to patients.
The third barrier, identified by seven HCPs (70%), was a lack of specialized oncology training in nursing. As reported by HCPs, there is no formal specialization in oncology in the five-year nursing degree in Spain. In order to specialize in oncology, nurses can either undertake self-funded specialized courses or master’s degrees or obtain on-the-job experience while in a position in an oncology department after graduation. Both courses of action were presented by nurses as difficult to attain, since a position in an oncology department was never guaranteed due to the frequency of rotation between posts and specializations. As a result, nurses explained that they generally did not invest in specialized oncology courses. According to HCPs, lack of oncology nursing specialization may lead to suboptimal care for oncology patients. Overall, their lack of knowledge hindered them from supporting oncologists in the delivery of information and the provision of emotional and practical support (Table 4; verbatims VI-VII). More in particular, the lack of specialized oncology training for nurses was identified as a missed opportunity to address certain patient needs that oncologists were unable to meet due to the barriers explained above. Nurses reported not having enough preparation to advise patients on the impact of the illness on their sexual lives, hair loss, or skin care. They also expressed feeling unprepared to effectively guide patients through the complexities of the healthcare system and emphasized the need for a specific training program to address these gaps.
The fourth barrier, identified by six HCPs (60%), was the lack of an evaluation system assessing patient-centered care and patient satisfaction. According to HCPs, the current evaluation system is focused on congress attendance and publications, and rewards only those HCPs who excel at these rather than at delivering patient-centered care (Table 4; verbatims VIII-X). In this sense, demonstrating empathy and communicating effectively with patients were perceived as an “invisible” effort, and therefore, could fail to motivate HCPs to develop a better understanding of how to support patients beyond strictly clinical follow-up. In addition, the use of patient questionnaires was identified as a helpful tool that could be implemented to facilitate conversations about sexuality, a topic that HCPs perceived as taboo for numerous patients.
4 Discussion and conclusion
4.1 Discussion
The results of this paper identified areas of improvement in oncologists’ and nurses’ communication delivery from the perspectives of both HER2+ MBC patients and their treating physicians, while at the same time highlighting the structural barriers hindering the provision of said communication delivery from the perspective of HCPs.
There are several studies discussing the communication needs of oncological patients more generally, and BC patients in particular. Many draw attention to patients’ information needs regarding the disease and treatments and to the need for psychosocial support (17–25). For patients with MBC, there are many areas where patients are lacking information. Examples include symptoms of metastases, treatment options, side effects, pain management, clinical trials, immunotherapy, acupuncture, social security assistance, and types of treatment, all of which have been shown to relate to increased levels of anxiety, depression, sexual difficulties, self-image, and pain (44–46). Patients who are living with HER2+ MBC also have a gap in communication in supporting physical, emotional and psychosocial concerns that result in tiredness, decreased sexual interest, less satisfaction with relationships, sore muscles, anxiety, difficulty sleeping, and joint pain (47, 48). Resonating with the literature, patients in our study agreed with the need to receive more information on the disease, treatments, and psychosexual support, confirming these needs for the Spanish context. Furthermore, they provided granularity to identified needs for social security assistance and social support with the necessity to obtain resources such as accessibility to transportation, access to charities, knowledge on PAs, and reasonably priced creams, wigs, and so on. To increase patient-centered information delivery, these needs should be addressed in communication encounters between HER2+ MBC patients and their oncologists and nurses. Additionally, having a dedicated support staff to ensure this information is provided throughout the journey could alleviate the negative impact of not receiving this information on overall mood.
Unfortunately, studies reporting on information needs of oncological patients tend to not consider the structural barriers that the healthcare system imposes on HCPs. For instance, a review meta-analysis conducted by Sisk and colleagues shows that out of 109 studies on communication needs of cancer patients, the vast majority focused on individual-level barriers rather than team, organization/system, collaborating hospital, community, or policy-level barriers (22). Therefore, a common conclusion of these type of studies is to make recommendations that appeal to HCPs as individuals (17, 20, 21, 49). Examples of these include asking HCPs to dedicate more time and energy to providing patient-centered information, or asking them to assess and address the psychosocial wellbeing of patients (17, 20, 21, 49).
Of the few studies that do address the structural barriers faced during the communication encounters in oncology, most of them discuss low and middle income countries (LMICs) (50–53). For instance, Paz-Soldán and colleagues conducted a qualitative study in Peru drawing attention to the structural barriers to screening for and treatment of cervical cancer in the country (50). In LMICs there are numerous structural barriers that women face in accessing healthcare services for breast cancer. These can range from issues of accessibility due to geographical and infrastructural challenges, costs associated with screening, and healthcare system challenges, such as inadequate HCP trainings and a lack of culturally competent medical care (29–32). All of these challenges can make women feel isolated and unsupported in clinical settings.
Instead, studies addressing structural barriers to communication delivery between HCPs and oncology patients in high income countries are scarce. Dencker et al. conducted a qualitative study in Denmark with doctors and nurses working with patients with gynecological and hematological cancers and in neurointensive care to identify the barriers hindering HCPs from communicating with patients about their children. They identified several emotional and structural barriers, the latter being ‘lack of space in the medical recording system,’ ‘professional code,’ ‘time pressure,’ and ‘lack of training.’ (33) Haussmann et al. analyzed structural barriers to promoting physical activity to cancer patients among physicians and nurses in Germany, and found that ‘not enough time per patient’ was the most cited barrier (34). In addition to HCPs’ workload, timing, coordination, information material for HCPs and patients, and availability of exercise programs were all identified as structural barriers to the promotion of physical activity (35).
Our study adds to this body of literature for patients with HER2+ MBC and their treating oncologists and nurses in Spain. HCPs in our study were perfectly aware of the potential room for improvement in their communicative encounters with patients. They identified lack of time as the main structural barrier hindering optimal communication with them, coinciding with the studies of Dencker et al. and Haussmann et al., while lack of training on interpersonal skills and communication was identified in both our study and that of Dencker et al. Furthermore, HCPs in our study presented two new structural barriers to communication not identified in the literature: having an evaluation system not assessing patient-centered care and patient satisfaction and lacking a specialized oncology training in nursing.
The figure of the specialized oncology nurse, present in other countries, has been found to be essential in the provision of patient-centric communication (54, 55). Specifically, studies have identified the need to empower oncology nurses to recognize emotional distress in their patients, as it is ‘the sixth vital sign which should regularly be monitored’ (27, 28). Moreover, research has identified that the lack of education on patients’ mental health, particularly on how to evaluate this, results in disregarding emotional states as part of their duty of care (28, 56). This paper agrees with these findings, arguing that specialized oncology nurses would be better prepared to share with oncologists the burden of information delivery regarding the topics identified in this study.
Although certain sections of our interview guides were specifically designed to explore the experiences of HER2+ patients, we believe that the findings of this study are applicable to the general BC population. Informational needs and barriers to access and understand medical information are challenges faced by patients across all BC subtypes, not exclusively those with HER2+ disease.
4.1.1 Strengths and limitations
A limitation of this study is the small sample size of 14 patients recruited at five university hospitals, which may not represent the full diversity of people diagnosed with stage IV HER2+ BC. A further limitation is that the study is cross-sectional with a single interview per patient, not providing patient perceptions as their disease evolves. However, the fact that participants correspond to a relatively homogenous population provides a compelling picture of the disease. Furthermore, the interviews with oncologists and nurses have been used to validate and complement patients’ insights.
4.2 Conclusion
This study has identified HER2+ MBC patients’ perspectives about the communication delivery they receive from their HCPs regarding the disease and treatments, psychosexual support, navigating the healthcare and social security systems, and PAs. This particular group of patients was selected for the study based on the specificities of their clinical and emotional experience. Living with a disease that is treatable yet incurable, they are confronted with the practical and conceptual ambiguity of navigating chronic and palliative models of care. In the specific Spanish context, improved psychological support and more tailored information provision have been identified as two key areas for better addressing the needs of these patients (13, 38). By also including the voices of HCPs, we have provided a wholistic, nuanced perspective on the gap between patient information needs and HCPs capacities and have demonstrated how these become magnified by inadequate healthcare ecosystems.
The deepened appreciation of how a healthcare system can pressurize on HCPs and lead to inadequate support can help policy makers and medical educators to tailor programs to the real-world needs of HCPs. In turn, they would be better equipped to support their patients through a challenging physical and emotional patient journey, which could result in improved patient outcomes and experiences.
To provide optimal, patient-centric care for HER2+ MBC patients, we conclude that individual level improvements are insufficient, and that it is paramount to consider and address the structural barriers imposed on HCP care delivery by the Spanish healthcare system.
4.3 Implications for practice
This article highlights the specific issues encountered by patients during interactions with their doctors and nurses. We consider these insights to be a powerful tool with the potential to inform the improvement of policies and protocols within the healthcare system and administration. Regarding the difficulties evoked by professionals, the lack of oncological specialization for nurses only represents a minor aspect of a broader issue. More generally, it is necessary to work on the improvement of communication channels and joint work between nurses and oncologists. This collaboration would have a positive impact on patients’ experiences.
Data availability statement
The datasets presented in this article are not readily available because the data underlying this article cannot be shared publicly due to the privacy of individuals that participated in the study, as established by the ethics committee. The data underlying this article will be shared upon reasonable request to the corresponding author. Requests to access the datasets should be directed to amFnc2FlbnpAeWFob28uY29t.
Ethics statement
All study materials were reviewed and approved by the Research Ethics Committee of the General University Hospital of Elche, code: D9673R00015. In addition to the written informed consent form, participants’ verbal informed consent and permission for the interview to be recorded and transcribed were recorded before the beginning of the interview. All data was anonymized to protect participant confidentiality. The study followed the principles outlined in the revised version of the Declaration of Helsinki, Good Clinical Practices (GCPs).
Author contributions
JG-S: Conceptualization, Project administration, Writing – review & editing. ÁR-L: Resources, Writing – review & editing. SA: Resources, Writing – review & editing. BC: Resources, Writing – review & editing. MAS: Resources, Writing – review & editing. MAG: Supervision, Writing – review & editing. RRR: Conceptualization, Formal analysis, Methodology, Project administration, Writing – review & editing. CSM: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Writing – original draft. JMI: Conceptualization, Writing – review & editing. RFV: Conceptualization, Writing – original draft. YGG: Writing – original draft. NAO: Project administration, Supervision, Writing – review & editing. JG: Conceptualization, Project administration, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was financed by the alliance AstraZeneca-Daiichi Sankyo.
Acknowledgments
We would like to thank the Spanish Breast Cancer Federation (FECMA) and APICES. We also thank Laura Madera and Coral Berriochoa, as Patient Safety Managers of AstraZeneca Farmacéutica Spain, SA. for their support during the study. We also extend our gratitude to the study coordinators, who ensured this study was smoothly executed.
Conflict of interest
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: José Ángel García- Sáenz has consultation or advisory fees, speaking and lecture fees and travel reimbursement from the following institutions: AstraZeneca, Roche, Lilly, Pfizer, Novartis, Daiichi-Sankyo, MSD, Gilead. Álvaro Rodrígez-Lescure has consultation or advisory fees, speaking and lecture fees and travel reimbursement from the following institutions: AstraZeneca, Roche, Lilly, Pfizer, Novartis, Daiichi-Sankyo, MSD, Gilead. Blanca Cantos has board membership, consultation or advisory fees, speaking and lecture fees and travel reimbursement from the following institutions: Astrazeneca, Daiichi Sankyo, Novartis, Pfizer, Lilly. Raül Rubio Renau and Carlota Solà Marsiñach have received funding from AstraZeneca to conduct this study. Jesús Martín Illán and Rocío Fonseca Vallejo are employees of Daiichi Sankio. Yaiza Gimeno Guadalupe and Noelia Alfaro Oliver are employees of AstraZeneca. Joaquín Gavilá has board membership, consultation or advisory fees, speaking and lecture fees and travel reimbursement from the following institutions: AstraZeneca, Daiichi Sankyo, Roche, Seagen.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Arnold, M, Morgan, E, Rumgay, H, Mafra, A, Singh, D, Laversanne, M, et al. Current and future burden of breast cancer: global statistics for 2020 and 2040. Breast. (2022) 66:15–23. doi: 10.1016/j.breast.2022.08.010
2. Lei, S, Zheng, R, Zhang, S, Wang, S, Chen, R, Sun, K, et al. Global patterns of breast cancer incidence and mortality: a population-based cancer registry data analysis from 2000 to 2020. Cancer Commun. (2021) 41:1183–94. doi: 10.1002/cac2.12207
3. Vegaa, IG, Rescalvob, AG, Morenoc, F, Ballesterd, P, Guisadoe, AM, and Sisóf, C. A retrospective study of do-not-do practice recommendations in metastatic breast cancer in Spain. Rev Senol Patol Mam. (2024) 37:593. doi: 10.1016/j.senol.2024.100593
4. Paracha, N, Reyes, A, Diéras, V, Krop, I, Pivot, X, and Urruticoechea, A. Evaluating the clinical effectiveness and safety of various HER2-targeted regimens after prior taxane/trastuzumab in patients with previously treated, unresectable, or metastatic HER2-positive breast cancer: a systematic review and network meta-analysis. Breast Cancer Res Treat. (2020) 180:597–609. doi: 10.1007/s10549-020-05577-7
5. Piccart, M, Procter, M, Fumagalli, D, De Azambuja, E, Clark, E, Ewer, MS, et al. Adjuvant Pertuzumab and Trastuzumab in early HER2-positive breast Cancer in the APHINITY trial: 6 years’ follow-up. J Clin Oncol. (2021) 39:1448–57. doi: 10.1200/JCO.20.01204
6. OncLive. Global trends in HER2+ MBC. OncLive (2021). Available online at: https://www.onclive.com/view/global-trends-in-her2-mbc (Accessed September 13, 2024).
7. DeKoven, M, Bonthapally, V, Jiao, X, Ganguli, A, Pathak, P, Lee, WC, et al. Treatment pattern by hormone receptors and HER2 status in patients with metastatic breast cancer in the UK, Germany, France, Spain and Italy (EU-5): results from a physician survey. J Comp Eff Res. (2012) 1:453–63. doi: 10.2217/cer.12.43
8. Goutsouliak, K, Veeraraghavan, J, Sethunath, V, De Angelis, C, Osborne, CK, Rimawi, MF, et al. Towards personalized treatment for early stage HER2-positive breast cancer. Nat Rev Clin Oncol. (2020) 17:233–50. doi: 10.1038/s41571-019-0299-9
9. Jerusalem, G, Lancellotti, P, and Kim, S-B. HER2+ breast cancer treatment and cardiotoxicity: monitoring and management. Breast Cancer Res Treat. (2019) 177:237–50. doi: 10.1007/s10549-019-05303-y
10. Loibl, S, and Gianni, L. HER2-positive breast cancer. Lancet. (2017) 389:2415–29. doi: 10.1016/S0140-6736(16)32417-5
11. National Health System. Cancer strategy of the Spanish National System. National Health System (2024).
12. Red Española de Registros de Cáncer. Estimaciones de la incidencia de cáncer en España, 2024. Red Española de Registros de Cáncer (2024).
13. Ciria-Suarez, L, Jiménez-Fonseca, P, Palacín-Lois, M, Antoñanzas-Basa, M, Fernández-Montes, A, Manzano-Fernández, A, et al. Breast cancer patient experiences through a journey map: a qualitative study. PLoS One. (2021) 16:e0257680. doi: 10.1371/journal.pone.0257680
14. Salvador, J, Urtasun, JA, Duart, FJB, García-Campelo, R, Carbonero, RG, Lianes, P, et al. Equity, barriers and cancer disparities: study of the Spanish Society of Medical Oncology on the access to oncologic drugs in the Spanish regions. Clin Transl Oncol. (2017) 19:341–56. doi: 10.1007/s12094-016-1535-8
15. Bu, X, Jin, C, Fan, R, Cheng, ASK, Ng, PHF, Xia, Y, et al. Unmet needs of 1210 Chinese breast cancer survivors and associated factors: a multicentre cross-sectional study. BMC Cancer. (2022) 22:135. doi: 10.1186/s12885-022-09224-w
16. Lo-Fo-Wong, DNN, de Haes, HCJM, Aaronson, NK, van Abbema, DL, den Boer, MD, van Hezewijk, M, et al. Risk factors of unmet needs among women with breast cancer in the post-treatment phase. Psychooncology. (2020) 29:539–49. doi: 10.1002/pon.5299
17. Husson, O, Mols, F, and van de Poll-Franse, LV. The relation between information provision and health-related quality of life, anxiety and depression among cancer survivors: a systematic review. Ann Oncol. (2011) 22:761–72. doi: 10.1093/annonc/mdq413
18. Aapro, M, Cardoso, F, Curigliano, G, Eniu, A, Gligorov, J, Harbeck, N, et al. Current challenges and unmet needs in treating patients with human epidermal growth factor receptor 2-positive advanced breast cancer. Breast. (2022) 66:145–56. doi: 10.1016/j.breast.2022.07.011
19. Swain, SM, Shastry, M, and Hamilton, E. Targeting HER2-positive breast cancer: advances and future directions. Nat Rev Drug Discov. (2023) 22:101–26. doi: 10.1038/s41573-022-00579-0
20. Şengün İnan, F, Yedigün, T, and Er, İ. Exploring the unmet supportive care needs of breast Cancer survivors experiencing psychological distress: qualitative study. Semin Oncol Nurs. (2023) 39:151449. doi: 10.1016/j.soncn.2023.151449
21. Elkefi, S, and Asan, O. The impact of patient-centered care on Cancer patients’ QOC, self-efficacy, and trust towards doctors: analysis of a National Survey. J Patient Exp. (2023) 10:1533. doi: 10.1177/23743735231151533
22. Sisk, BA, Harvey, K, Friedrich, AB, Antes, AL, Yaeger, LH, Mack, JW, et al. Multilevel barriers and facilitators of communication in pediatric oncology: a systematic review. Pediatr Blood Cancer. (2022) 69:e29405. doi: 10.1002/pbc.29405
23. Estes, JM, and Karten, C. Nursing expertise and the evaluation of psychosocial distress in patients with cancer and survivors. Clin J Oncol Nurs. (2014) 18:598–600. doi: 10.1188/14.CJON.598-600
24. Pålsson, MB, and Norberg, A. Breast cancer patients’ experiences of nursing care with the focus on emotional support: the implementation of a nursing intervention. J Adv Nurs. (1995) 21:277–85. doi: 10.1111/jan.13016
25. Anderson, K, and Bohnenkamp, S. Managing the storm of emotions exhibited by patients with Cancer: part I. Sch J. (2022) 31:195–7.
26. Gundelach, A, and Henry, B. Cancer-related psychological distress: a concept analysis. Clin J Oncol Nurs. (2016) 20:630–4. doi: 10.1188/16.CJON.630-634
27. Cormio, C, Caporale, F, Spatuzzi, R, Lagattolla, F, Lisi, A, and Graziano, G. Psychosocial distress in oncology: using the distress thermometer for assessing risk classes. Support Care Cancer. (2019) 27:4115–21. doi: 10.1007/s00520-019-04694-4
28. Lyu, X-C, Jiang, H-J, Lee, L-H, Yang, C-I, and Sun, X-Y. Oncology nurses’ experiences of providing emotional support for cancer patients: a qualitative study. BMC Nurs. (2024) 23:58. doi: 10.1186/s12912-024-01718-1
29. Islam, RM, Billah, B, Hossain, MN, and Oldroyd, J. Barriers to cervical cancer and breast cancer screening uptake in low-income and middle-income countries: a systematic review. Asian Pac J Cancer Prev. (2017) 18:1751–63. doi: 10.22034/APJCP.2017.18.7.1751
30. Ponce-Chazarri, L, Ponce-Blandón, JA, Immordino, P, Giordano, A, and Morales, F. Barriers to breast Cancer-screening adherence in vulnerable populations. Cancer. (2023) 15:604. doi: 10.3390/cancers15030604
31. Srinath, A, van Merode, F, Rao, SV, and Pavlova, M. Barriers to cervical cancer and breast cancer screening uptake in low- and middle-income countries: a systematic review. Health Policy Plan. (2023) 38:509–27. doi: 10.1093/heapol/czac104
32. Nduka, IJ, Ejie, IL, Okafor, CE, Eleje, GU, and Ekwunife, OI. Interventions to increase mammography screening uptake among women living in low-income and middle-income countries: a systematic review. BMJ Open. (2023) 13:e066928. doi: 10.1136/bmjopen-2022-066928
33. Dencker, A, Rix, BA, Bøge, P, and Tjørnhøj-Thomsen, T. A qualitative study of doctors’ and nurses’ barriers to communicating with seriously ill patients about their dependent children. Psychooncology. (2017) 26:2162–7. doi: 10.1002/pon.4440
34. Haussmann, A, Ungar, N, Gabrian, M, Tsiouris, A, Sieverding, M, Wiskemann, J, et al. Are healthcare professionals being left in the lurch? The role of structural barriers and information resources to promote physical activity to cancer patients. Support Care Cancer. (2018) 26:4087–96. doi: 10.1007/s00520-018-4279-x
35. Haussmann, A, Gabrian, M, Ungar, N, Jooß, S, Wiskemann, J, Sieverding, M, et al. What hinders healthcare professionals in promoting physical activity towards cancer patients? The influencing role of healthcare professionals’ concerns, perceived patient characteristics and perceived structural factors. Eur J Cancer Care (Engl). (2018) 27:e12853. doi: 10.1111/ecc.12853
36. Swain, SM, Baselga, J, Kim, S-B, Ro, J, Semiglazov, V, Campone, M, et al. Pertuzumab, Trastuzumab, and docetaxel in HER2-positive metastatic breast Cancer. N Engl J Med. (2015) 372:724–34. doi: 10.1056/nejmoa1413513
37. Cardoso, F, Harbeck, N, Mertz, S, and Fenech, D. Evolving psychosocial, emotional, functional, and support needs of women with advanced breast cancer: results from the count us, know us, join us and Here & now surveys. Breast. (2016) 28:5–12. doi: 10.1016/j.breast.2016.04.004
38. Guest, G, Namey, E, and Chen, M. A simple method to assess and report thematic saturation in qualitative research. PLoS One. (2020) 15:e0232076. doi: 10.1371/journal.pone.0232076
39. Carel, H. Phenomenology and its application in medicine. Theor Med Bioeth. (2011) 32:33–46. doi: 10.1007/s11017-010-9161-x
40. Desjarlais, R, and Throop, JC. Phenomenological approaches in anthropology. Annu Rev Anthropol. (2011) 40:87–102. doi: 10.1146/annurev-anthro-092010-153345
41. Lipscomb, M. Abductive reasoning and qualitative research: abductive reasoning. Nurs Philos. (2012) 13:244–56. doi: 10.1111/j.1466-769X.2011.00532.x
42. Saunders, B, Sim, J, Kingstone, T, Baker, S, Waterfield, J, Bartlam, B, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. (2018) 52:1893–907. doi: 10.1007/s11135-017-0574-8
43. Hennink, M, and Kaiser, BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. (2022) 292:114523. doi: 10.1016/j.socscimed.2021.114523
44. Seah, DS, Lin, NU, Curley, C, Weiner, EP, and Partridge, AH. Informational needs and the quality of life of patients in their first year after metastatic breast cancer diagnosis. J Community Support Oncol. (2014) 12:347–54. doi: 10.12788/jcso.0077
45. Mayer, M. Lessons learned from the metastatic breast Cancer community. Semin Oncol Nurs. (2010) 26:195–202. doi: 10.1016/j.soncn.2010.05.004
46. Kadravello, A, Tan, S-B, Ho, G-F, Kaur, R, and Yip, C-H. Exploring unmet needs from an online metastatic breast cancer support group: a qualitative study. Medicina (Mex). (2021) 57:693. doi: 10.3390/medicina57070693
47. Mayer, M. IN24 patient perspectives on symptom control. Breast. (2013) 22:S26–7. doi: 10.1016/S0960-9776(13)70037-7
48. Mayer, M, Lang, K, Hurvitz, S, Lalla, D, Federico, V, Brammer, M, et al. Symptom burden and quality of life among women with HER2 + metastatic breast Cancer. Breast J. (2015) 21:208–10. doi: 10.1111/tbj.12374
49. Faller, H, Brähler, E, Härter, M, Keller, M, Schulz, H, Wegscheider, K, et al. Unmet needs for information and psychosocial support in relation to quality of life and emotional distress: a comparison between gynecological and breast cancer patients. Patient Educ Couns. (2017) 100:1934–42. doi: 10.1016/j.pec.2017.05.031
50. Paz-Soldán, VA, Bayer, AM, Nussbaum, L, and Cabrera, L. Structural barriers to screening for and treatment of cervical cancer in Peru. Reprod Health Matters. (2012) 20:49–58. doi: 10.1016/S0968-8080(12)40680-2
51. Zamanzadeh, V, Rassouli, M, Abbaszadeh, A, Nikanfar, A, Alavi-Majd, H, and Ghahramanian, A. Factors influencing communication between the patients with Cancer and their nurses in oncology wards. Indian J Palliat Care. (2014) 20:12–20. doi: 10.4103/0973-1075.125549
52. Afiyanti, Y, Milanti, A, Rosdiana, M, and Juliastuti, D. Deficient health care services as barriers to meet care needs of gynecological Cancer survivors in Indonesia: a qualitative inquiry. Semin Oncol Nurs. (2021) 37:151206. doi: 10.1016/j.soncn.2021.151206
53. Sisk, BA, Friedrich, AB, Kaye, EC, Baker, JN, Mack, JW, and DuBois, JM. Multilevel barriers to communication in pediatric oncology: clinicians’ perspectives. Cancer. (2021) 127:2130–8. doi: 10.1002/cncr.33467
54. Galassi, A, Anwarali, S, and Challinor, J. Global challenges and initiatives in oncology nursing education. Ann Palliat Med. (2023) 12:633–45. doi: 10.21037/apm-22-1120
55. Cheung, RB, Aiken, LH, Clarke, SP, and Sloane, DM. Nursing care and patient outcomes: international evidence. Enferm Clin. (2008) 18:35–40. doi: 10.1016/s1130-8621(08)70691-0
56. Granek, L, Nakash, O, Ariad, S, Shapira, S, and Ben-David, M. Mental health distress: oncology nurses’ strategies and barriers in identifying distress in patients with Cancer. Clin J Oncol Nurs. (2019) 23:43–51. doi: 10.1188/19.CJON.43-51
57. Gavilá, J, Rodríguez-Lescure, Á, Antolín, S, Cantos, B, Seguí, MÁ, Gimon, MA, et al. Do patients with HER2+ MBC and their HCPs speak the same language? Perceptions and uses of chronic disease and metastatic treatment arising from the EtnobreastHER2 study. Patient Education and Counseling. (2025) 140:109289. doi: 10.1016/j.pec.2025.109289
Keywords: human epidermal growth factor receptor 2 metastatic breast cancer, oncology, patient-centered care, informational needs, doctor-patient communication, structural barriers
Citation: García-Sáenz JÁ, Rodríguez-Lescure Á, Antolin S, Cantos B, Seguí MÁ, Gimón MA, Rubio Renau R, Solà Marsiñach C, Martín Illán J, Fonseca Vallejo R, Gimeno Guadalupe Y, Alfaro Oliver N and Gavilá J (2025) Information needs and barriers to patient-centered care in oncology: EtnobreastHER2, an ethnographic study with HER2+ MBC patients and their healthcare providers. Front. Med. 12:1592380. doi: 10.3389/fmed.2025.1592380
Edited by:
Jacqueline G. Bloomfield, The University of Sydney, AustraliaReviewed by:
Austin Young Shull, Presbyterian College, United StatesAadya Nagpal, Peter MacCallum Cancer Centre, Australia
Copyright © 2025 García-Sáenz, Rodríguez-Lescure, Antolin, Cantos, Seguí, Gimón, Rubio Renau, Solà Marsiñach, Martín Illán, Fonseca Vallejo, Gimeno Guadalupe, Alfaro Oliver and Gavilá. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Ángel García-Sáenz, amFnc2FlbnpAeWFob28uY29t