 Kun Jia1
Kun Jia1 Yan Yang2*
Yan Yang2*- 1Department of Rehabilitation, Beijing Children's Hospital Affiliated to Capital Medical University, Beijing, China
- 2Traditional Chinese Medicine Department, Beijing Children's Hospital Affiliated to Capital Medical University, Beijing, China
Objective: To explore the impact of acupuncture and massage on adolescent idiopathic scoliosis (AIS) and its influence on pain degree.
Methods: One hundred and sixteen adolescent patients with idiopathic scoliosis treated from January 2021 to December 2023 were chosen to be the study objects, followed by dividing into control group and observation group. The control group received brace correction combined posture training. The observation group received traditional Chinese medicine (TCM) acupuncture and bone-setting massage treatment. The Cobb Angle, degree of pain, therapeutic effect, quality of life, incidence of adverse reactions and spinal function were compared in 2 groups.
Results: After therapy, the Cobb Angle value and VAS score were declined in 2 groups, and those in the observation group presented lower when comparing with the control group (P < 0.01). In contrast to the control group, the total effective rate in the observation group was better (P < 0.05), and the SRS-22 score in the observation group was higher (P < 0.05). After therapy, the ODI score was declined and JOA score was elevated in 2 groups, and the improvements of ODI and JOA scores in the observation group were more significant when comparing with the control group (P < 0.01).
Conclusion: Acupuncture and massage can promote the clinical treatment effect, reduce the degree of pain, promote Cobb Angle recovery, promote the quality of life and improve the spinal function of AIS.
Introduction
Adolescent idiopathic scoliosis (AIS) is a common musculoskeletal disorder that affects growth and development in adolescents, with a Cobb Angle >10° serving as the primary diagnostic criterion (1). AIS often presents with vertebral rotation as the initial symptom, followed by physical abnormalities such as uneven shoulder height, thoracic asymmetry, leg length discrepancies, rib humps, pelvic tilt, and reduced height (2). In severe cases, AIS may lead to cardiopulmonary dysfunction, neurological paralysis, and elevated surgical risk (35). Furthermore, the physical deformities associated with AIS can contribute to psychological distress, including low self-esteem and mental health challenges (3). Leg length discrepancy in AIS patients results from pelvic tilt secondary to spinal curvature, while height reduction stems from vertebral rotation and compression of intervertebral spaces (36). Nowadays, AIS has become another significant health concern after adolescents' health faces obesity and myopia (4). According to the survey, 0.47–5.20% of the world's adolescents suffer from AIS, and the number of primary and secondary school students in China has exceeded 3 million, and the number of about 300,000 is increasing year by year (5).
At present, the clinical treatment of AIS mostly uses orthoses or conservative management such as chiropractic, physiotherapy exercise, and axial traction (37). Traditional Chinese medicine (TCM) believes that AIS belongs to the category of “spinal deformity”, and its pathogenesis is closely related to the imbalance of muscles and bones caused by internal and external pathogenic factors invading the body (6). Acupuncture and massage are traditional Chinese medicine therapy, with safety, affordable, effective and other advantages (7). Acupuncture can effectively promote the circulation of qi and blood in the back area, improve the microcirculation of nerve roots, and achieve the balance of muscle strength on both sides of the spine (8). Massage can make the paraspinal muscles and soft tissues fully relaxed, and then look for the scoliosis segment, with the adjustment of the manipulation to correct the vertebral misalignment, so as to restore the normal physiological curvature of the spine (9).
In our study, we explored the effect of acupuncture combined with massage on AIS and its influence on pain degree.
Data and methods
Participants
A total of 116 adolescent patients with idiopathic scoliosis treated between January 2021 and December 2023 were included in the study. Patients were randomly assigned to either the control group or the observation group, with 58 cases in each group. The control group included 30 males and 28 females. The average age was (12.56 ± 1.28) years, ranging from 10 to 16 years. Type of scoliosis: 23 cases in thoracolumbar segment, 18 cases in thoracic segment, 17 cases in lower back segment. There were 29 males and 19 females in the observation group. The average age was (12.52 ± 1.25) years, ranging from 9 to 17 years. Type of scoliosis: thoracolumbar segment in 24 cases, thoracic segment in 19 cases, low back segment in 15 cases. There was no significant difference in general data between 2 groups (P > 0.05). Inclusion criteria: (1) Consistent with AIS diagnostic criteria; (2) The age range was 9–17 years old; (3) Conformance with conservative treatment and Cobb Angle <45°; (4) The legal guardian signed the relevant consent. Exclusion criteria: (1) Patients with congenital spinal malformation; (2) Severe spinal cord injury with cardiopulmonary dysfunction; (3) Participants who had received other physical and exercise therapy interventions within 1 month before participating in this study; (4) People with mental illness or cognitive disorder (Table 1).
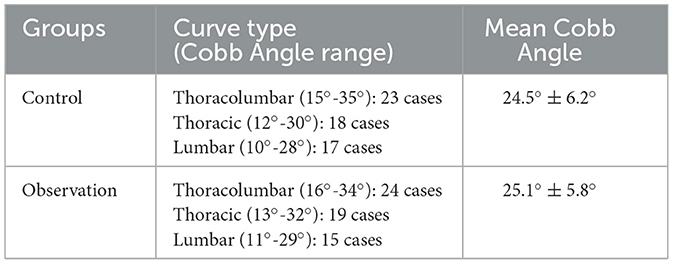
Table 1. Baseline Cobb Angle distribution by scoliosis type in control and observation groups.
Methods
The control group received brace correction combined posture training. Appropriate chest, waist, and sacral braces were selected according to convex vertex, and were worn for no <21 h every day. The change of height was closely paid attention to, and the brace was replaced or adjusted as appropriate. Nurses guided the patient to perform the chest expansion exercise with feet equally equal to shoulder width, assisted the patient to pull the horizontal bar, and asked the patient to pay attention to relax the body, and then stand against the wall, so that the calf, hip, heel and shoulder joints were close to the wall, and the arms were naturally drooping, repeat the above training, 3–5 times/d, 10 min/times. At the same time, nurses asked patients to pay attention to sitting and standing posture in life.
The observation group received TCM acupuncture and bone-setting massage treatment.
Bone-setting massage
The patient was placed in a prone position, and the muscles around the curved spine were stretched for 20 min. Then, the doctor pressed the convex side of the scoliosis with one palm and the opposite shoulder with the other hand, and gave the reaction force along the spine from top to bottom for 5 min. The bone-setting massage was performed twice a week. During the massage, the doctor should pay attention to gentle manipulation.
Acupuncture
The doctor selected YaoShu point, HuanTiao point, ZhiYang point, Sanyinjiao point, Ququan point, Jizhong point, Mingmen point, and Shenzhu point. When acupuncture was performed, 6–8 lumbosacral acupuncture points and 2–4 leg acupuncture points were selected, radian needle expansion method was applied, and moderate stimulation was given. Acupuncture was performed according to WHO Standard Acupuncture Point Locations (38), with needle retention for 30 min.
The intervention was performed for 3 months in both groups.
Observation indicators
(1) The Cobb Angle of the patient was measured on the full-length anteroposterior X-ray film of the spine. The upper and lower vertebrae were located, respectively. Two straight lines were drawn along the upper edge of the upper vertebrae and the lower edge of the lower vertebrae, and then the Angle between the vertical lines of the two lines was measured, which was called Cobb Angle.
(2) Visual analog method (VAS) was implemented for evaluating the pain degree of patients (10). The total score was 10 points. The lower the score was, the less the pain was.
(3) The therapeutic effect criteria are formulated following the Guidelines for the Diagnosis and Treatment of Common Diseases of Traditional Chinese Chiropractic and Chinese Chiropractic. Cured: Radiographic examination showed that the scoliosis deformity disappeared, the signs and symptoms disappeared, and the Cobb Angle was <5°. Effective: Radiographs showed less scoliosis than before, less symptoms, improved function, Cobb Angle decreased ≥5°. Ineffective: Radiographs showed no significant changes in scoliosis, Cobb Angle decreased <5°, and even the scoliosis Angle became larger than before. Total effective rate = (cured cases + effective cases)/Total cases × 100%.
(4) At the end of treatment, the Scoliosis Research Society-22 Patient Questionnaire (SRS-22) was implemented for evaluating the quality of life of patients (11). The full score of the scale was 100, and the higher the score, the better the quality of life.
(5) The incidence of adverse reactions including dizziness, nausea, vomiting, tissue damage and fracture in 2 groups were analyzed.
(6) Oswestry Disability Index (ODI) together with Japanese Orthopedic Association (JOA) was implemented for assessing the spinal function of patients (12, 13). The full score of ODI scale was 50, and the full score of JOA scale was 29. The lower the ODI score, the better the spinal function. The higher the JOA score, the better the spinal function.
Statistical analysis
SPSS 24.0 statistical software was adopted for data analysis. Measurement data were expressed as (x ± s), and t-test was adopted for comparison. Count data were expressed as (n, %), and χ2 test was used for comparison. P < 0.05 meant statistical significance.
Results
Cobb Angle value in 2 groups
It was revealed in Figure 1 and Table 2 that, the no difference was seen in Cobb Angle value between 2 groups before therapy (P > 0.05). After therapy, the Cobb Angle value was declined in 2 groups, and that in the observation group presented lower when comparing with the control group (P < 0.01).
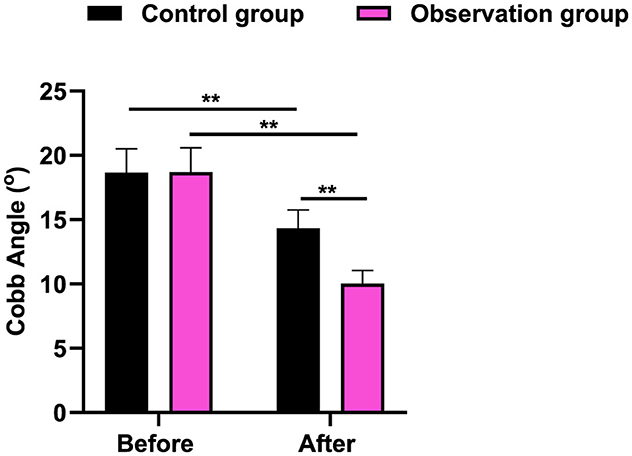
Figure 1. Cobb Angle value in 2 groups. **P < 0.01.
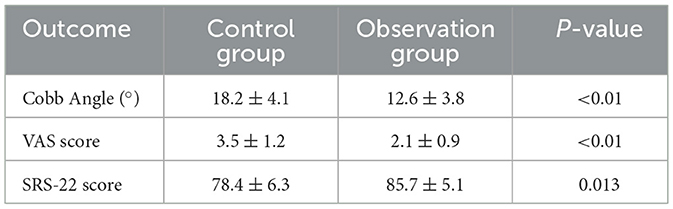
Table 2. Comparison of primary outcomes between groups.
VAS score in 2 groups
It was revealed in Figure 2 that, the no difference was seen in VAS score between 2 groups before therapy (P > 0.05). After therapy, the VAS score was declined in 2 groups, and that in the observation group presented lower when comparing with the control group (P < 0.01).
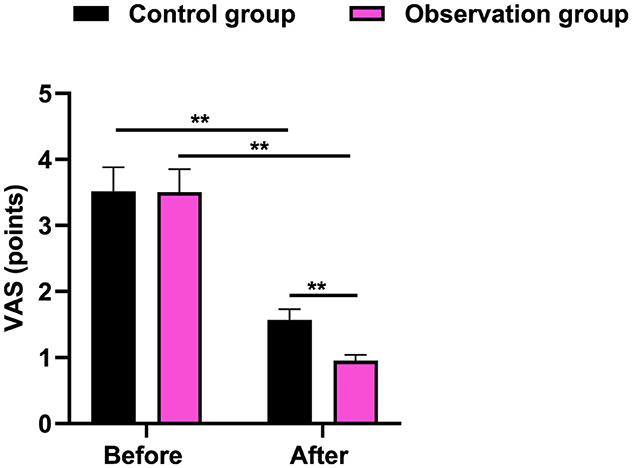
Figure 2. VAS score in 2 groups. **P < 0.01.
Therapeutic effect in 2 groups
Table 3 displayed that in contrast to the control group, the total effective rate in the observation group was better (P < 0.05).

Table 3. Therapeutic effect in 2 groups.
SRS-22 score in 2 groups
Figure 3 and Table 2 displayed that in contrast to the control group, the SRS-22 score in the observation group was higher (P < 0.05).
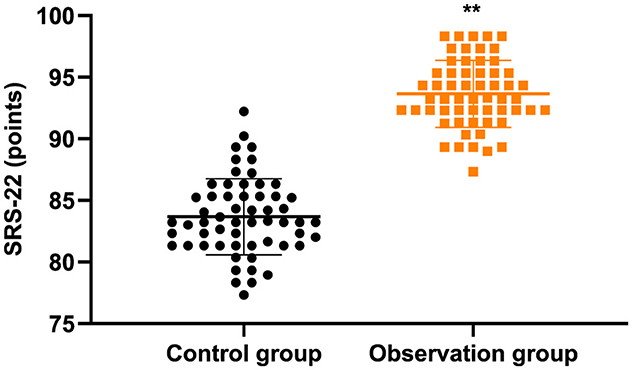
Figure 3. SRS-22 score in 2 groups. **P < 0.01.
Incidence of adverse reactions in 2 groups
There were no adverse reactions containing dizziness, nausea, vomiting, tissue injury, and fracture in the 2 groups during treatment.
Spinal function in 2 groups
It was revealed in Figure 4 that, the no difference was seen in ODI and JOA scores between 2 groups before therapy (P > 0.05). After therapy, the ODI score was declined and JOA score was elevated in 2 groups, and the improvements of ODI and JOA scores in the observation group were more significant when comparing with the control group (P < 0.01).
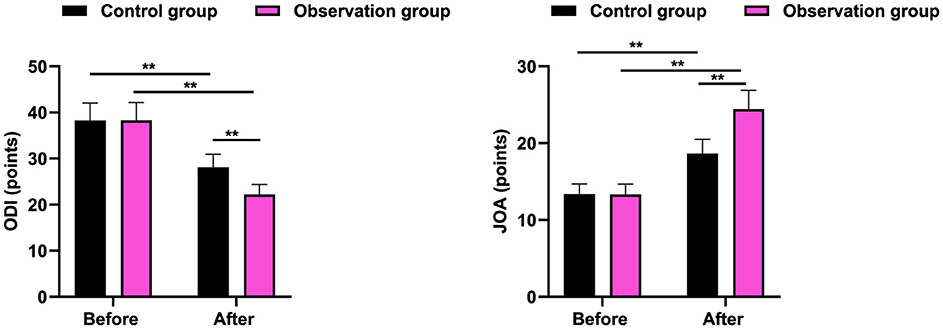
Figure 4. Spinal function in 2 groups. **P < 0.01.
Discussion
Scoliosis is a common clinical condition that can cause contracture of the soft tissues around the spine, resulting in tensile tension, further aggravating the severity of scoliosis (14). Due to the rapid physical development of adolescents, vertebral bones will be further enlarged, if not timely improvement of scoliosis symptoms can seriously affect the normal development of the spine, affecting study, life, and work (15).
TCM believes that scoliosis belongs to the “turtle back” category, and its pathogenesis is considered to be related to the invasion of bone by external and internal pathogens and the loss of muscles and bones, and the imbalance of tendons and bones is an important pathological change (16). At present, there are many clinical treatment methods for AIS, including bone-setting massage and acupuncture, which have certain therapeutic effects (17).
Bone-setting massage can correct vertebral subluxation, facilitate qi and blood flow by stimulating the Du meridian, and promote the recovery of spinal function (18). The release of soft tissue on both sides of the spine can promote scoliosis recovery and facilitate stability after bone-setting. Massage on the concave side of the contracture tissue can make it fully relax and relieve the contracture state. Massage from top to bottom along the side bend can help further relax the contracture tissue, and then bone setting can obtain better results (19). The vertebral displacement can be corrected by boning, the normal anatomical structure of the joint can be restored, and the scoliosis deformity can be effectively corrected. Bone-setting massage is a non-invasive method, basically will not produce side effects and adverse reactions, will not cause secondary damage, easy to be accepted (20).
Acupuncture is a common external treatment of TCM. Based on the meridian theory of TCM, acupuncture can improve the muscle and ligament strength corresponding to the meridian and its distribution tissues by stimulating specific acupoints (21). Currently, acupuncture therapy has been widely applied in the rehabilitation treatment of patients with spinal injuries (22). In this study, the YaoShu point of acupuncture points belongs to the governor meridian, which can dispel cold and dehumidification, and the combination with HuanTiao point can be used to treat the hip pain symptoms caused by waist diseases such as AIS (23). Zhiyang point also belongs to the governor meridian, which can be used to treat strong back pain (24). Sanyinjiao point is the spleen channel, can promote blood and qi (25). Ququan point belongs to the liver channel of foot Jueyin, which can be used for activating channels and clearing dampness and heat (26). The Jizhong point and Mingmen point belong to the governor meridian, which can be used to treat the severe pain of the lumbar spine (27). The Shenzhu point is also a governor meridian, which can be used to calm god and relieve convulsion (28). Acupuncture stimulation of the above points can effectively improve the function of muscles and ligaments in the area covered by the corresponding meridians, and achieve the effect of relaxing muscles and facilitating blood circulation, removing blood stasis and stopping circulation (29). Relevant studies have shown that acupuncture can increase local blood flow by stimulating corresponding acupuncture points, promote nutrient delivery and waste metabolism by improving blood circulation around the spine, and regulate nerve function by stimulating nerve endings (30). In addition to improving the shape of the spine, it can also effectively promote the recovery of spinal function in patients (31).
In our study, the results indicated that after therapy, the Cobb Angle value and VAS score were declined in 2 groups, and those in the observation group presented lower when comparing with the control group. Meanwhile, in contrast to the control group, the total effective rate in the observation group was better. All these results suggested that acupuncture and massage could promote the clinical treatment effect, reduce the degree of pain, and also promote Cobb Angle recovery. Consistently, Wei et al. have pointed that TCM combined therapy can prevent the progression of scoliosis (8). These findings align with prior reviews indicating that adolescent idiopathic scoliosis may benefit from conservative and manual therapy approaches (33, 34).
Besides, our study indicated that in contrast to the control group, the SRS-22 score in the observation group was higher, and after therapy, the ODI score was declined and JOA score was elevated in 2 groups, and the improvements of ODI and JOA scores in the observation group were more significant when comparing with the control group. All these results indicated that acupuncture and massage could promote the quality of life and improve the spinal function of AIS. Likewise, Huang et al. have suggested that massage and acupuncture has a significantly superior effect on reducing chronic spinal pain and improving spinal function (32).
Nevertheless, there were still some limitations for this study. The 3-month follow-up period may not capture long-term effects. Moreover, blinding of practitioners was impractical due to the nature of manual therapies. Future studies should include radiographic assessments beyond Cobb Angle, such as rotational measurements via CT.
In conclusion, Acupuncture combined with massage significantly reduced Cobb Angles (mean reduction: 5.6° vs. 2.3° in controls), suggesting its potential as a complementary approach for mild-to-moderate AIS. Acupuncture and massage are effective in reducing pain severity, improving Cobb Angle recovery, and enhancing quality of life and spinal function in adolescents with AIS.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Ethics statement
The studies involving humans were approved by Ethics Committee of Beijing Children's Hospital Affiliated to Capital Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KJ: Writing – original draft, Writing – review & editing. YY: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Altaf F, Gibson A, Dannawi Z, Noordeen H. Adolescent idiopathic scoliosis. BMJ. (2013) 346:f2508. doi: 10.1136/bmj.f2508
2. Weinstein SL, Dolan LA, Cheng JC, Danielsson A, Morcuende JA. Adolescent idiopathic scoliosis. Lancet. (2008) 371:1527–37. doi: 10.1016/S0140-6736(08)60658-3
3. Peng Y, Wang SR, Qiu GX, Zhang JG, Zhuang QY. Research progress on the etiology and pathogenesis of adolescent idiopathic scoliosis. Chin Med J. (2020) 133:483–93. doi: 10.1097/CM9.0000000000000652
4. Kuznia AL, Hernandez AK, Lee LU. Adolescent idiopathic scoliosis: common questions and answers. Am Fam Physician. (2020) 101:19–23.
5. Zheng Y, Dang Y, Wu X, Yang Y, Reinhardt JD, He C, et al. Epidemiological study of adolescent idiopathic scoliosis in Eastern China. J Rehabil Med. (2017) 49:512–9. doi: 10.2340/16501977-2240
6. Zheng S, Xu N, Jiang Y, Wu Y. A comprehensive therapeutic approach of traditional Chinese medicine for mild adolescent idiopathic scoliosis. Asian J Surg. (2024) 47:2675–6. doi: 10.1016/j.asjsur.2024.03.089
7. Stein DJ. Massage acupuncture, moxibustion, and other forms of complementary and alternative medicine in inflammatory bowel disease. Gastroenterol Clin North Am. (2017) 46:875–80. doi: 10.1016/j.gtc.2017.08.015
8. Wei H, Xu J, Jiang Z, Ye S, Song H, Ning X, et al. Effect of a Traditional Chinese Medicine combined therapy on adolescent idiopathic scoliosis: a randomized controlled trial. J Tradit Chin Med. (2015) 35:514–9. doi: 10.1016/S0254-6272(15)30133-3
9. Wang HY, Kong YP. Effect of traditional Chinese medicine massage on the rehabilitation of spinal function in scoliosis patients undergoing 3D printing orthopedic surgery. Zhongguo Gu Shang. (2022) 35:33–7. doi: 10.12200/j.issn.1003-0034.2022.01.007
10. Shafshak TS, Elnemr R. The visual analogue scale vs. numerical rating scale in measuring pain severity and predicting disability in low back pain. J Clin Rheumatol. (2021) 27:282–5. doi: 10.1097/RHU.0000000000001320
11. Gao A, Li JY, Shao R, Wu TX, Wang YQ, Liu XG, et al. Schroth exercises improve health-related quality of life and radiographic parameters in adolescent idiopathic scoliosis patients. Chin Med J. (2021) 134:2589–96. doi: 10.1097/CM9.0000000000001799
12. McNeely EL, Zhang B, Neuman BJ, Skolasky RL. Estimating measurement error of the Oswestry Disability Index with missing data. Spine J. (2022) 22:975–82. doi: 10.1016/j.spinee.2022.01.013
13. Amako M, Arai T, Iba K, Ikeda M, Ikegami H, Imada H, et al. Japanese Orthopaedic Association (JOA) clinical practice guidelines on the management of lateral epicondylitis of the humerus—Secondary publication. J Orthop Sci. (2022) 27:514–32. doi: 10.1016/j.jos.2021.09.003
14. Gámiz-Bermúdez F, Obrero-Gaitán E, Zagalaz-Anula N, Lomas-Vega R. Corrective exercise-based therapy for adolescent idiopathic scoliosis: Systematic review and meta-analysis. Clin Rehabil. (2022) 36:597–608. doi: 10.1177/02692155211070452
15. Fan Y, Ren Q, To MKT, Cheung JPY. Effectiveness of scoliosis-specific exercises for alleviating adolescent idiopathic scoliosis: a systematic review. BMC Musculoskelet Disord. (2020) 21:495. doi: 10.1186/s12891-020-03517-6
16. Guo J, Lau AH, Chau J, Ng BK, Lee KM, Qiu Y, et al. A validation study on the traditional Chinese version of Spinal Appearance Questionnaire for adolescent idiopathic scoliosis. Eur Spine J. (2016) 25:3186–93. doi: 10.1007/s00586-016-4590-5
17. Zhang H, Pan Y, Ju C, Shen Y, Li X, Ye X, et al. Imaging study of coccygeal morphology in adolescent idiopathic scoliosis. Sci Rep. (2024) 14:727. doi: 10.1038/s41598-024-51276-4
18. Zaproudina N, Hänninen OO, Airaksinen O. Effectiveness of traditional bone setting in chronic neck pain: randomized clinical trial. J Manipulative Physiol Ther. (2007) 30:432–7. doi: 10.1016/j.jmpt.2007.05.004
19. Miriutova NF, Kirichuk SV, Lipina EV. Rehabilitative treatment of idiopathic scoliosis in children and adolescents. Vopr Kurortol Fizioter Lech Fiz Kult. (2009) 4:32–7.
20. Romano M, Negrini S. Manual therapy as a conservative treatment for adolescent idiopathic scoliosis: a systematic review. Scoliosis. (2008) 3:2. doi: 10.1186/1748-7161-3-2
21. Sierpina VS, Frenkel MA. Acupuncture: a clinical review. South Med J. (2005) 98:330–7. doi: 10.1097/01.SMJ.0000140834.30654.0F
22. Shin BC, Lee MS, Kong JC, Jang I, Park JJ. Acupuncture for spinal cord injury survivors in Chinese literature: a systematic review. Complement Ther Med. (2009) 17:316–27. doi: 10.1016/j.ctim.2009.09.001
23. Uema D, Orlandi D, Freitas RR, Rodgério T, Yamamura Y, Tabosa AF. Effect of eletroacupuncture on DU-14 (Dazhui), DU-2 (Yaoshu), and Liv-13 (Zhangmen) on the survival of Wistar rats' dorsal skin flaps. J Burn Care Res. (2008) 29:353–7. doi: 10.1097/BCR.0b013e31816679a6
24. Luo H, Gong R, Zheng R, Tan J, Chen R, Wu J, et al. Dose-effect of long-snake-like moxibustion for chronic fatigue syndrome: a randomized controlled trial. J Transl Med. (2023) 21:430. doi: 10.1186/s12967-023-04250-z
25. Chen HM, Chen CH. Effects of acupressure at the Sanyinjiao point on primary dysmenorrhoea. J Adv Nurs. (2004) 48:380–7. doi: 10.1111/j.1365-2648.2004.03236.x
26. Xu GX, Zhou YM, Sun MS, Luo LJ, Liu XJ, Wang D, et al. Clinical observation on distribution characteristics and rules of pain sensitivity points on body surface in patients with knee osteoarthritis. Zhongguo Zhen Jiu. (2020) 40:1198–201. doi: 10.13703/j.0255-2930.20190928-k0001
27. Wang S, Ye G, Xu C, Jia A, Ru Y, Guan S, et al. Flipping moxibustion of Hui medicine at acupoints in governor vessel combined with acupuncture for vascular dementia. Zhongguo Zhen Jiu. (2018) 38:919–24. doi: 10.13703/j.0255-2930.2018.09.003
28. Li CY, Bai XH. Clinical trial of acupuncture treatment of gastroesophageal reflux disease accompanied with somnipathy at acupoints of governor vessel at back segment]. Zhen Ci Yan Jiu. (2018) 43:516–21. doi: 10.13702/j.1000-0607.170659
29. Weiss HR, Bohr S, Jahnke A, Pleines S. Acupucture in the treatment of scoliosis - a single blind controlled pilot study. Scoliosis. (2008) 3:4. doi: 10.1186/1748-7161-3-4
30. Wong JJ, Shearer HM, Mior S, Jacobs C, Côté P, Randhawa K, et al. Are manual therapies, passive physical modalities, or acupuncture effective for the management of patients with whiplash-associated disorders or neck pain and associated disorders? An update of the Bone and Joint Decade Task Force on Neck Pain and Its Associated Disorders by the OPTIMa collaboration. Spine J. (2016) 16:1598–630. doi: 10.1016/j.spinee.2015.08.024
31. Pennick V, Liddle SD. Interventions for preventing and treating pelvic and back pain in pregnancy. Cochrane Database Syst Rev. (2013) 8:Cd001139. doi: 10.1002/14651858.CD001139.pub3
32. Huang JF, Zheng XQ, Chen D, Lin JL, Zhou WX, Wang H, et al. Can acupuncture improve chronic spinal pain? A systematic review and meta-analysis. Global Spine J. (2021) 11:1248–65. doi: 10.1177/2192568220962440
33. Cheng JC, Castelein RM, Chu WC, Danielsson AJ, Dobbs MB, Grivas TB, et al. Adolescent idiopathic scoliosis. Nat Rev Dis Primers. (2015) 1:15030. doi: 10.1038/nrdp.2015.68
34. Lotan S, Kalichman L. Manual therapy treatment for adolescent idiopathic scoliosis. J Bodyw Mov Ther. (2019) 23:189–93. doi: 10.1016/j.jbmt.2018.01.005
35. Chu EC-P. Presurgical optimization and surgical management of extreme adolescent idiopathic scoliosis: a case report. Cureus. (2025) 17:e81987. doi: 10.7759/cureus.81987
36. Dimkić I, Fira D, Janakiev T, Kabić J, Stupar M, Nenadić M, et al. The microbiome of bat guano: for what is this knowledge important?. Appl Microbiol Biotechnol. (2021) 105:1407–19. doi: 10.1007/s00253-021-11143-y
37. Chu EC-P, Lee WT, Tam DMY, Ng NY, Nur AB. Scoliosis causing cervical dystonia in a chiropractic office. Cureus. (2023) 15:e35802. doi: 10.7759/cureus.35802
Keywords: adolescent idiopathic scoliosis, acupuncture, massage, pain, Cobb Angle, quality of life
Citation: Jia K and Yang Y (2025) Effect of acupuncture and massage on adolescent idiopathic scoliosis and pain severity. Front. Med. 12:1613800. doi: 10.3389/fmed.2025.1613800
Received: 17 April 2025; Accepted: 13 June 2025;
Published: 21 July 2025.
Edited by:
Mark Henry Pitcher, National Center for Complementary and Integrative Health (NIH), United StatesReviewed by:
Elena Amaricai, Victor Babes University of Medicine and Pharmacy, RomaniaEric Chun-Pu Chu, EC Healthcare, Hong Kong SAR, China
Copyright © 2025 Jia and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yan Yang, Ymp5YW5neWFuX2VkdUAxNjMuY29t