 Alina Volkmar1Cay-Benedict von der Decken2,3,4,5Stefan Kleinert2,6Kirsten Karberg2,7Georg Gauler2,8Michael Klennert9Jana Klennert9Peer Malte Aries2,10Sonja Froschauer11Sarah Wildenhain11Theresia Muth11Susanna Späthling-Mestekemper2,12Christoph Kuhn2,13Wolfgang Vorbrüggen2,4Martin Welcker2,14Peter Bartz-Bazzanella2,5
Alina Volkmar1Cay-Benedict von der Decken2,3,4,5Stefan Kleinert2,6Kirsten Karberg2,7Georg Gauler2,8Michael Klennert9Jana Klennert9Peer Malte Aries2,10Sonja Froschauer11Sarah Wildenhain11Theresia Muth11Susanna Späthling-Mestekemper2,12Christoph Kuhn2,13Wolfgang Vorbrüggen2,4Martin Welcker2,14Peter Bartz-Bazzanella2,5 Matthias Englbrecht15*
Matthias Englbrecht15*- 1Faculty of Life Sciences, University of Applied Sciences, Hamburg, Germany
- 2RHADAR – RheumaDatenRheport GbR, Erlangen, Germany
- 3Medizinisches Versorgungszentrum, Rheumatologie, Stolberg, Germany
- 4Verein zur Förderung der Rheumatologie e.V., Würselen, Germany
- 5Klinik für Internistische Rheumatologie, Rhein-Maas-Klinikum, Würselen, Germany
- 6Praxisgemeinschaft Rheumatologie-Nephrologie, Erlangen, Germany
- 7Rheumatologisches Versorgungszentrum Steglitz, Berlin, Germany
- 8Rheumatology Practice, Osnabrück, Germany
- 9STAR Healthcare Management GmbH, Köln, Germany
- 10Immunologikum Hamburg, Hamburg, Germany
- 11BDRh Service GmbH, Grünwald, Germany
- 12Rheumapraxis München, München, Germany
- 13Praxis für Rheumatologie, Karlsruhe, Germany
- 14M.B.W.-Welcker GbR, Planegg, Germany
- 15Freelance Healthcare Data Scientist, Greven, Germany
Introduction: Inflammatory rheumatic diseases (IRDs) are chronic autoimmune conditions affecting the musculoskeletal system, leading to pain, disability, and reduced quality of life. Despite advances in medical treatments, barriers such as delayed diagnosis, workforce shortages, and low adherence to self-management strategies remain critical challenges. Digital health applications are emerging as promising tools to enhance disease management. The aim of this study was to conduct a systematic literature review (SLR) to evaluate self-care outcomes associated with digital health applications in IRDs.
Methods: We conducted a systematic literature review according to PRISMA guidelines across four electronic databases (PubMed, Embase, CINAHL, Cochrane) from inception to July 2024. Randomized controlled trials (RCTs) and systematic reviews focusing on digital interventions to promote self-management and self-care in individuals with IRDs were included. Key outcomes were extracted and the quality of the included studies was assessed using the Critical Appraisal Skills Programme (CASP) checklist.
Results: Fifteen RCTs with a total of 1912 participants were analyzed. Primary outcomes, including self-management/self-care, showed mixed results. Some studies demonstrated significant improvements in self-efficacy, pain reduction, depression/anxiety symptoms, and physical function, while others showed no notable changes. Secondary outcomes, including disease activity and medication adherence, revealed heterogeneous findings. Variability in study design, sample size, and intervention duration posed challenges for drawing definitive conclusions about the effectiveness of digital interventions.
Discussion: Digital health applications show promise as cost-effective and scalable solutions to complement standard IRD care by empowering patients in their disease management. However, significant heterogeneity and limited generalizability highlight the need for more robust and long-term research to validate the efficacy of specific tools and identify best options for improving outcomes. Tailored digital interventions could bridge the gap in care for IRD patients and support their autonomy.
1 Introduction
The umbrella term inflammatory rheumatic diseases (IRDs) refers to a group of autoimmune diseases that are highly diverse and often chronic. IRDs are characterized by systemic inflammation that typically affects the joints, tendons, muscles, ligaments and bones, but may also involve internal organs such as the heart, lungs, and kidneys (1, 2). Conditions considered to be IRDs include rheumatoid arthritis (RA), psoriatic arthritis (PsA), axial spondylarthritis (axSpA), systemic lupus erythematosus (SLE), and gout.
IRDs are among the most common chronic diseases worldwide and can affect all age groups. If not properly managed, they can result in irreversible joint damage and cartilage breakdown. The resulting disease symptoms may manifest as considerable pain, disability, and decreased quality of life (QoL) (3). IRDs are further complicated by frequent physical comorbidities, including cardiovascular diseases and osteoporosis (4), and psychological comorbidities, most notably anxiety and depression (5, 6). In addition to the physical and mental effects of IRDs, socioeconomic consequences for individuals, caretakers, and society are substantial, particularly with respect to decreased work productivity and early retirement (7).
In Germany, IRDs affect approximately 2.2 to 3.0% of the adult population, which equates to approximately 1.5–2.1 million individuals (8). Although recent global prevalence data for IRDs are not available, the most common IRD, RA, currently affects an estimated 17.6 million people worldwide; forecasts indicate this number will almost double to 31.7 million by 2050 (9).
The increasing number of people with IRDs is juxtaposed with a shortage of rheumatologists in Germany (10) and elsewhere (11–14). In some developed countries, rheumatology workforces are about half the recommended level (10, 11, 14). These deficits are further exacerbated by the complexity of current rheumatology care, which typically involves “treat to target” strategies (15–17) and close monitoring of potential treatment side effects (14). Shortages in the rheumatology workforce have the potential to jeopardize optimal rheumatologic patient care by delaying early diagnosis and treatment and impacting patient follow-up care (10).
With the rising numbers of patients with IRDs and the current lack of patient care resources, innovative solutions are necessary. Digital healthcare applications (apps) present a promising route for addressing these challenges. Corresponding tools for IRDs range from those designed to streamline the diagnostic process to those that monitor treatment effectiveness and tolerability. Additionally, apps can aid in the identification and treatment of comorbidities, convey patient education and rehabilitation information, and provide tailored expert knowledge for both patients and medical professionals (18, 19). Both clinicians and patients have expressed strong interest in using digital healthcare tools to assist with disease management (18). In 2018, 67% of rheumatologists planned to incorporate medical apps into routine care, up from 47% in 2016 (18).
In Germany, the trend toward digital health solutions has been further propelled by the introduction of the Digital Healthcare Act (DVG), which came into effect in 2020. The DVG includes provisions for patients to have access to specific apps (“prescription apps”), known as digital health applications, which are reimbursed by statutory health insurance providers (18). Other countries are introducing similar programs, with various reimbursement models (20, 21).
An important use of digital health applications is to empower patients to take a proactive role in managing their health by providing guidance on self-management and self-care. In this context, self-management, which encompasses self-care and self-efficacy and is also termed patient activation, refers to the ability and willingness of patients to manage their health conditions (22). There are a multitude of opportunities to integrate apps designed to improve self-management into the care of patients with IRDs. For instance, digital interventions can reduce pain interference in chronic pain conditions, including IRDs (23). Digital strategies may also be able to enhance long-term treatment adherence, which can be suboptimal in patients with IRDs, leading to greater disability and reduced effectiveness of therapy (24). Another possible avenue is management of depression and anxiety (25), which may affect self-management behavior and treatment adherence (6). These findings suggest that digital health applications have the potential to provide a valuable resource for managing the physical and mental health aspects of IRDs.
The goal of this systematic literature review (SLR) was to investigate the current landscape and relevance of digital tools in enhancing self-management and related outcomes in patients with IRDs. This assessment may be of use in future development of digital interventions for the self-management of IRDs.
2 Methods
The SLR presented here adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, a 27-item checklist designed to enhance the completeness and transparency of systematic review reporting (26). An electronic databank search was conducted in June and July 2024 across four databases: PubMed, Cochrane, Embase, and Cumulated Index in Nursing and Allied Health Literature (CINAHL). Those four databases were chosen as they collectively offer extensive coverage of medical, clinical, and allied health literature necessary to capture the various dimensions of the topic. Because of the study design, this SLR was not registered in a clinical study database. A separate protocol was not prepared.
Studies were sought that focused on different digital tools such as websites, apps, and wearable devices for self-management and self-care in people with IRDs. The aim was to evaluate whether such digital programs (in addition to usual care) resulted in improvement in patients’ self-management of the disease, including reduction in pain, fewer symptoms of depression and anxiety, and less functional impairment.
2.1 Search strategy
The literature search included published articles (including those published online first) listed in the specified databases up until the day of the search (July 10, 2024 for PubMed and July 15, 2024 for Cochrane, Embase, and CINAHL). All included studies were required to be published in German or English. The framework for the search was based on the Patients, Intervention, Comparator, Outcome (PICO) format (27) (Table 1). The search terms included Medical Subject Headings (MeSH) terms, keywords, and wildcard terms found in the title or abstract. Briefly, included studies involved patients with IRDs, interventions with digital tools, a comparison to patients who did not use digital tools, and an outcome involving self-management/self-care and related assessments as shown in Table 1. The abbreviated PubMed search strategy is shown in Table 2 and detailed search strategies for the four databases are provided in Supplementary file S1. Only studies that were either a randomized controlled trial (RCT) or an SLR/meta-analysis were eligible for inclusion.
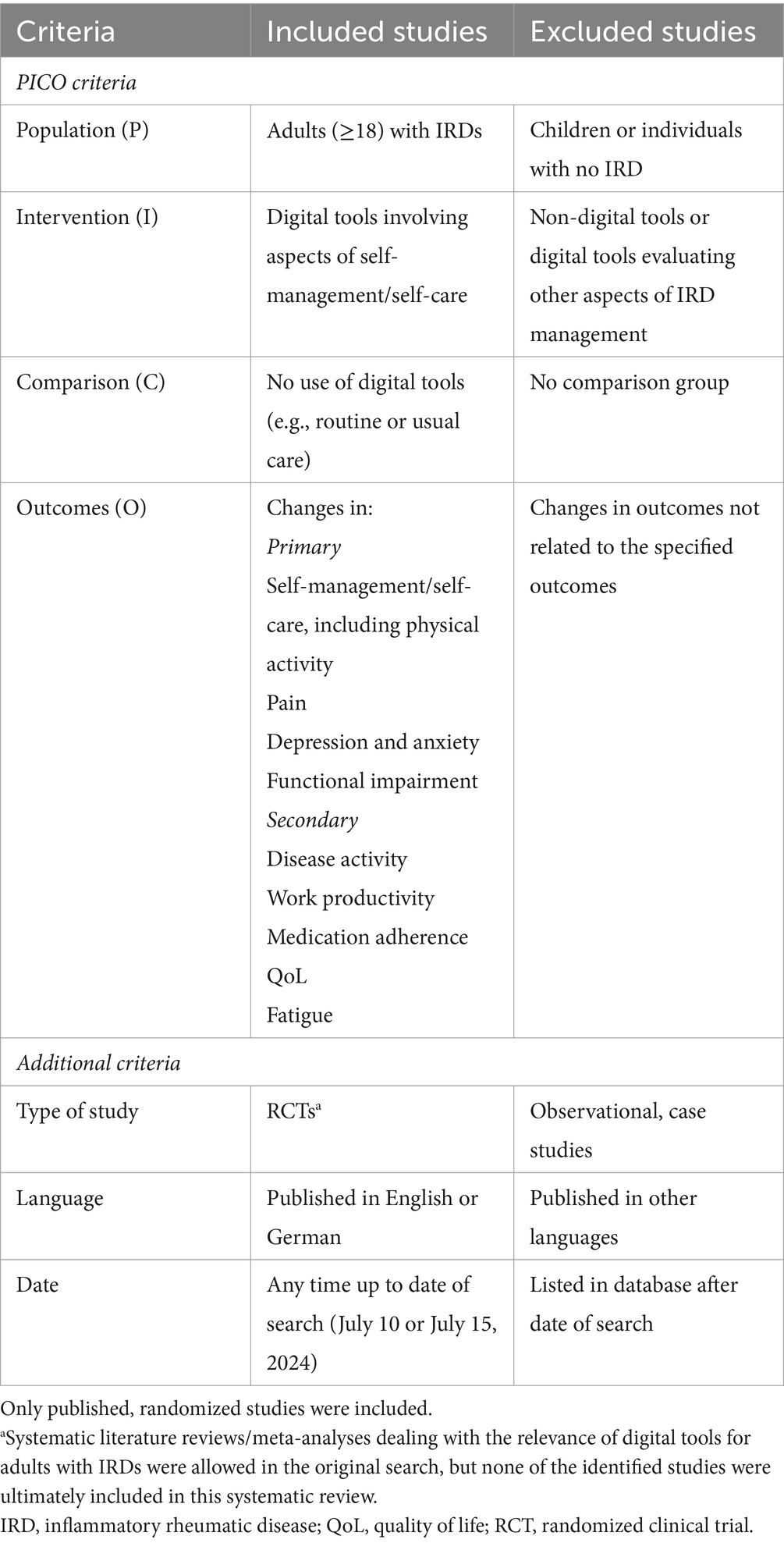
Table 1. Digital application systematic literature review entry criteria.
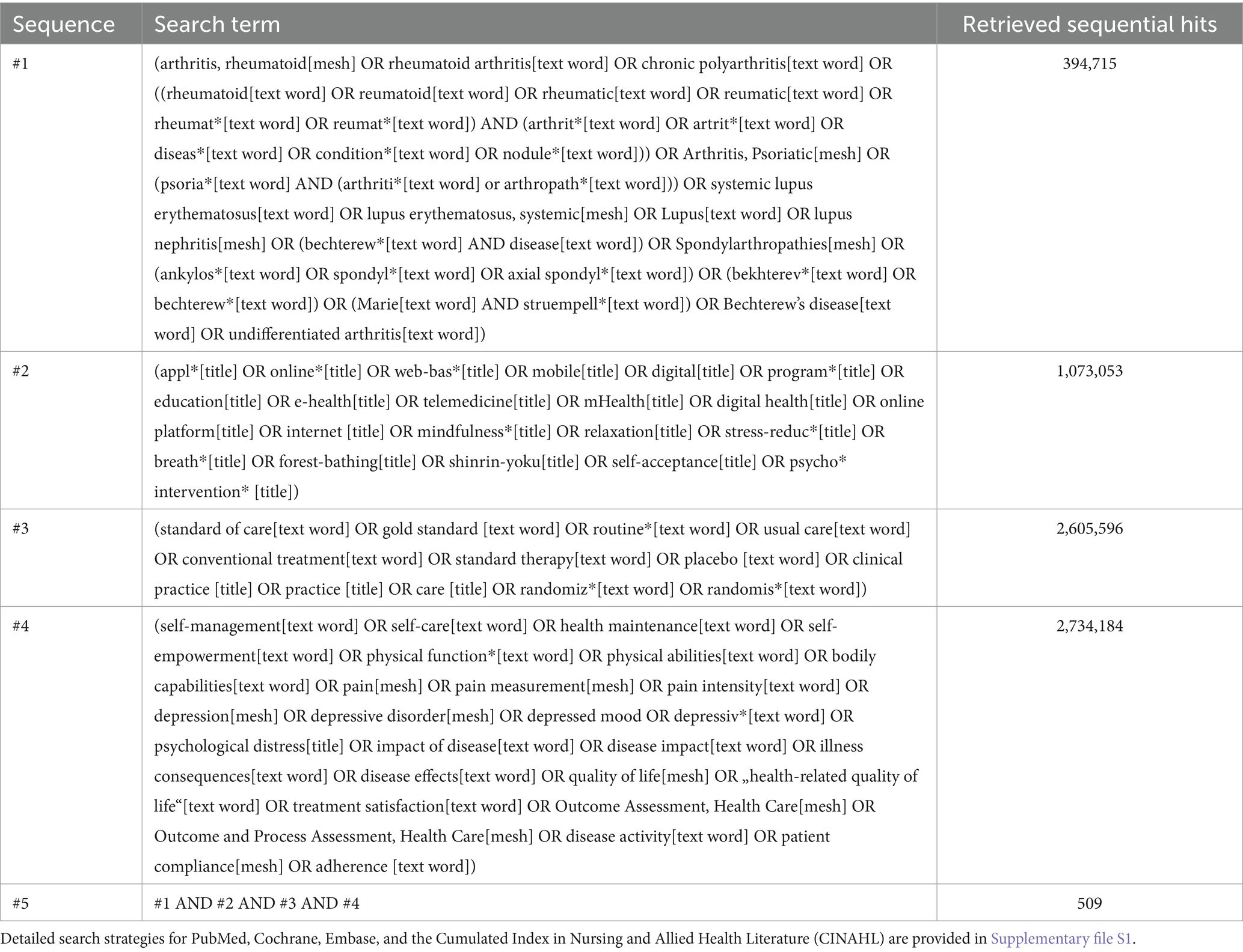
Table 2. Abbreviated PubMed search strategy.
2.2 Selection of studies
For the purposes of this SLR, we chose four primary outcomes of interest: self-management (including patient activation and physical activity), pain, depression/anxiety, and functional impairment (including impairment in activities of daily living). These outcomes were not necessarily designated as primary outcomes in the original study. We also evaluated several secondary outcomes for this systematic review, including disease activity, work productivity, medication adherence, QoL, including health-related QoL (HR-QoL), and fatigue (Table 1).
The suitability of studies was evaluated by two reviewers (AV and ME) using Rayyan as a digital platform for literature screening (28). Discrepancies were discussed to ensure consistency of inclusion and exclusion criteria. Studies not meeting the inclusion criteria based on the title or abstract were excluded. A reason for exclusion was recorded for each study to document the exclusion process and generate a list of exclusion reasons. The reasons were prioritized and coded as follows:
1. Wrong population (not an IRD).
2. Wrong outcome (not a self-management intervention or lacking self-management components).
3. Wrong intervention (not a digital intervention).
4. Wrong study design (not an RCT or an SLR/meta-analysis).
2.3 Data extraction and quality assessment
The selection of information to be extracted from the identified studies and included in the results table was initially made by AV and subsequently cross-checked by ME. After discussing and agreeing on the appropriate table headings, AV extracted the data to complete the results table. The results were manually entered into the table to minimize the risk of errors.
The quality of the studies was assessed using the established Critical Appraisal Skills Programme (CASP) checklist which is a standardized critical appraisal tool for RCTs (29). The CASP checklist is broadly divided into four sections: Section A evaluates the appropriateness of the study design for a RCT, section B assesses the methodological rigor of the study, section C investigates the reported results, and section D considers the applicability of these results in a local context (29).
2.4 Statistical analyses
Extracted data, including study characteristics and reported outcomes of interest, were summarized descriptively. If the mean age for the full study cohort was not reported, a weighted mean age was calculated using the mean ages of the intervention and control groups. No additional statistical analyses were conducted. Effect sizes and p values included in this SLR are as reported by the cited study.
3 Results
3.1 Retrieved articles
A total of 2111 records were identified and 886 duplicate records were removed, leaving 1225 records for title/abstract screening (Figure 1). Of these, 1166 were excluded, usually due to not evaluating an outcome of interest or not involving adults with IRDs. Fifty-nine reports were retrieved and assessed for eligibility, of which 15 met all study eligibility criteria. The two most common reasons for exclusion during this phase of selection were wrong intervention (no digital application) and wrong population (Figure 1).
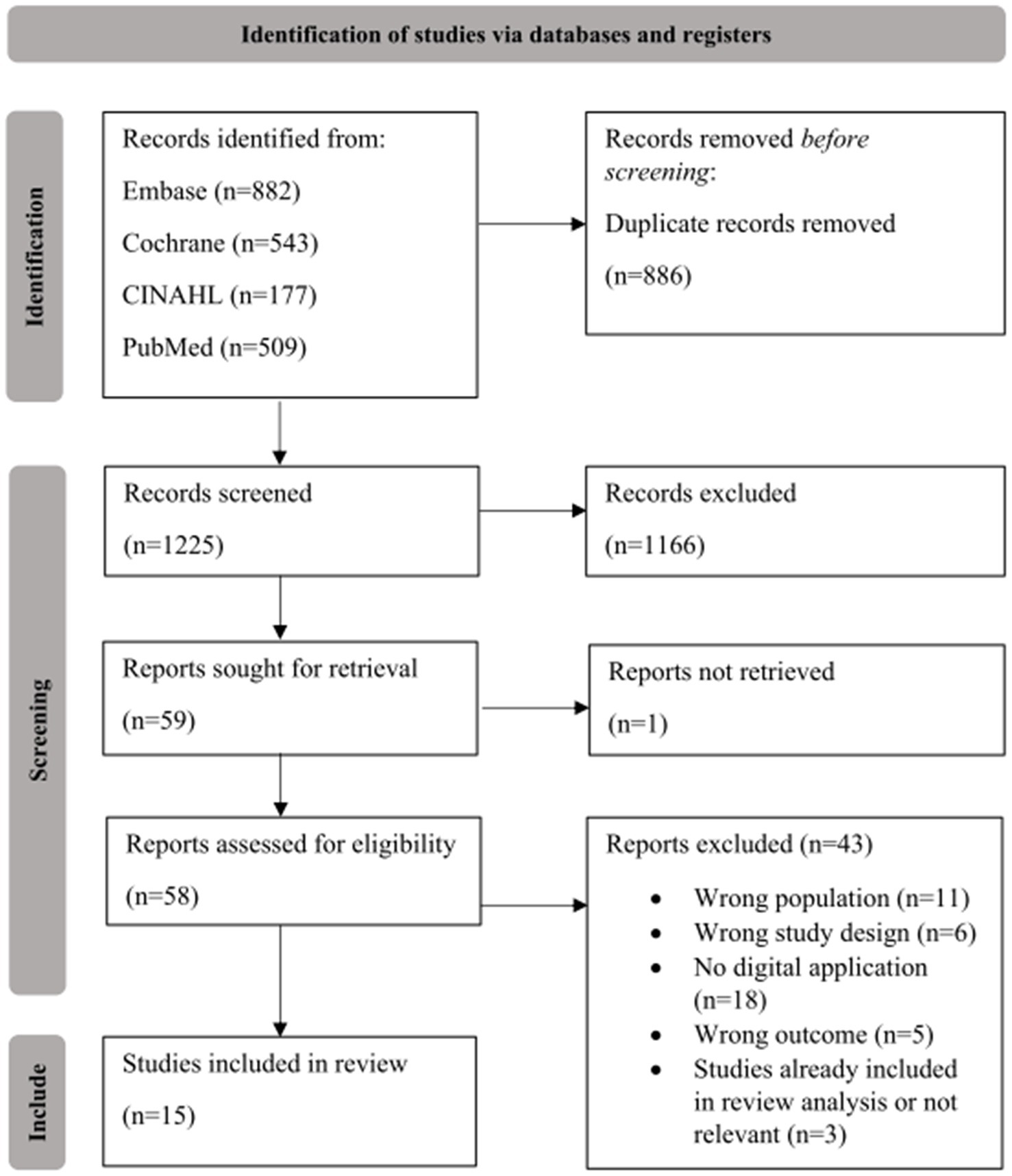
Figure 1. PRISMA flow chart. The suitability of studies was evaluated by two reviewers (AV and ME).
Although SLRs and meta-analyses were eligible for study inclusion, all included studies were RCTs. Three SLRs, Srikesavan et al. (30), Griffiths et al. (31), and Ritschl et al. (32), were initially marked as included after the full-text screening. However, during data extraction, these studies were ultimately excluded for the following reasons: Srikesavan et al. (30) included studies already identified as eligible for the current systematic review and Griffiths et al. (31) and Ritschl et al. (32) included studies that did not meet the inclusion criteria for our analysis.
3.2 Characteristics of included studies
3.2.1 Study overview
The 15 RCTs included in this SLR encompassed a total of 1912 participants (Table 3) (23, 33–46). Only one of the studies had a sample size over 200, five had a sample size between 150 and 200, six had a sample size between 100 and 150, and three had a sample size <50. Data of the included studies were from Europe (n = 8, four from the Netherlands and one each from Spain, Germany, Switzerland and Denmark), North America (n = 6, three from Canada and three from the US), and Asia (n = 1, from China). Publication dates ranged from 2006 to 2025; the article published in 2025 was published online first on December 28, 2023 (39). The proportion of women across the studies varied widely, with reported values ranging from 21 to 96%, while three studies did not report this information or reported this information for the control and intervention groups separately but not for the overall sample. The mean age of participants spanned from 30 to 62 years (Table 3).
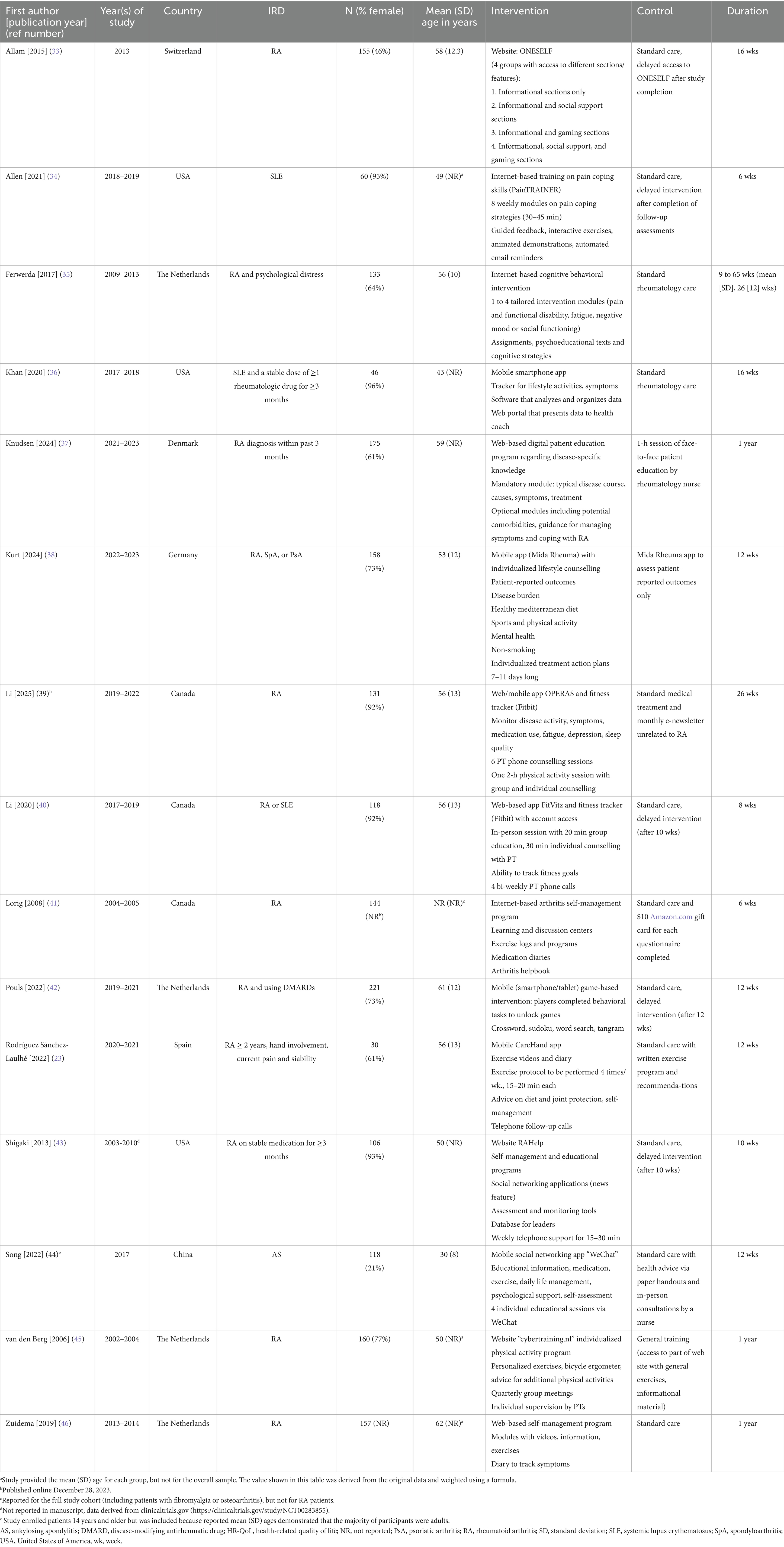
Table 3. Overview of the 15 studies included in the systematic review.
Twelve of the 15 included studies investigated individuals with RA (Table 3). Ten of these studies included only patients with RA, one involved individuals with RA or SLE, and one enrolled individuals with RA, spondyloarthritis (SpA), or PsA. In addition to the study of patients with RA or SLE, two other studies focused only on people with SLE. One study included individuals with ankylosing spondylitis (AS) (Table 3).
Digital interventions included the use of websites/internet programs in nine studies, mobile apps in five studies, and one study that was available as both a web app and a mobile app (Table 3). In four of the studies, the intervention included a non-digital component, such as individual counseling or telephone support (39, 40, 43, 45). The durations of the interventions varied widely, ranging from a minimum of six weeks to a maximum of one year. The control group received different kinds of care across the 15 studies, most frequently standard care (12 studies), in some cases with additional features such as gift cards or a written exercise program and recommendations. In five studies the control groups received the intervention after the RCT was completed (delayed intervention) (Table 3).
The study by Lorig et al. (41) included patients with RA, osteoarthritis, and fibromyalgia. Because the focus of this SLR was on IRDs, only analyses relevant to patients with RA were included; these data were presented in the original publication as subgroup analyses. The RCT conducted by Song et al. (44) was included despite initially meeting the exclusion criterion of involving participants younger than 18 years. This study was retained because the reported mean ages and standard deviations demonstrated that the majority of participants were significantly older than 14 [mean (SD) age of total sample 29.9 (8.23) years, intervention group 30.8 (8.82) years, and control group 29.1 (7.58) years] (44).
3.2.2 Per-protocol analyses and adjusted models
The study by Allen et al. (34) was challenged by the fact that only 50% (15/30) of the intervention group (IG) actually used the digital intervention in this study (PainTRAINER program). In addition to examining the overall IRD cohort, this study also evaluated the subgroup that logged onto the program, which they characterized as “PainTRAINER users” (PTU). Four other studies presented per protocol (PP) analyses in addition to intention-to-treat (ITT) analyses (35, 36, 42, 45). In three of these studies, outcomes that were not significantly impacted by the digital intervention in the ITT analysis showed significant between-group differences in the PP analysis (35, 36, 45). In this review, both the ITT and PP results are presented for studies that included these analyses.
In addition to presenting unadjusted differences between IG and control, Li et al. (39) also used a generalized linear mixed-effect model (GLMM) to evaluate the intervention effect. GLMM models were adjusted for sex and accounted for data missing at random without the need to perform imputations. For one of the outcomes evaluated in this study, there was a difference between IG and control in the GLMM but not in the unadjusted data. Both unadjusted and GLMM data are presented for the Li et al. study (39).
3.3 Assessment of study quality
Each study was evaluated individually with the CASP checklist (Supplementary file S2). Overall, most studies were methodologically sound. The most common methodological flaw was the absence of participant blinding, which can be difficult to achieve in evaluations of digital tools. Only one study, Allam et al. (33), met criteria for participant blinding by using parallel experimental groups, and six met criteria for investigator blinding (23, 34, 38, 39, 44, 45). Most did not mention whether the people analyzing the outcomes were blinded (Supplementary file S2). The other most common methodological issue was not reporting confidence intervals (six studies) or effect sizes (three studies). In the study by Ferwerda et al. (35), the intervention group was not well-balanced with the control group with respect to mood and certain physical ability assessments.
3.4 Outcomes of relevance
The most frequent primary outcomes evaluated in the 15 studies was various aspects of self-management/self-care/self-efficacy (n = 11), including six studies that evaluated physical activity (interventions to encourage exercise and other physical activities), and functional impairment (n = 11) (Table 3). Pain was evaluated in ten studies, and depression/anxiety was assessed in six (all six evaluated depression and three evaluated anxiety, including one study that used a composite measure for depression and anxiety). For secondary outcomes, disease activity (n = 7) and fatigue (n = 7) were the most frequent outcomes assessed.
Table 4 shows a summary of evaluated outcomes and significant differences between the IG and control group. The following sections discuss each of the primary outcomes individually and summarize the secondary outcomes. An alternative presentation showing all relevant outcomes reported by each study is presented in Supplementary file S3.
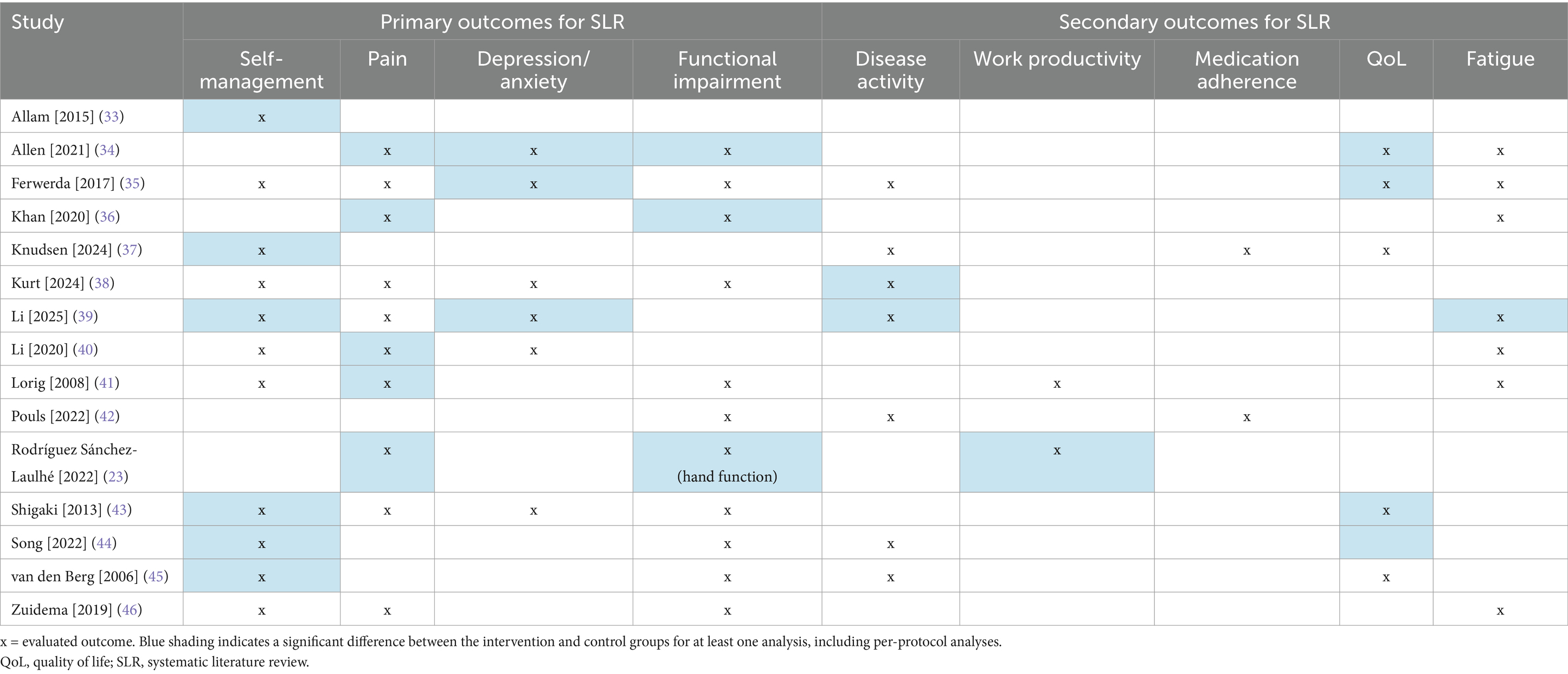
Table 4. Summary of significant differences in favor of digital interventions vs. control in the included studies.
3.5 Primary outcomes
3.5.1 Self-management, including physical activity
For self-management outcomes, we included interventions designed to improve self-empowerment, self-care, self-efficacy, self-management, patient activation, and physical activity (fitness outcomes such as time spent exercising or fitness tracker data) (Table 5). These studies had a broad spectrum of results. Of the eleven studies that evaluated self-management, six reported a significant difference in favor of the IG, including three that found significant improvements in self-efficacy with digital interventions (37, 43, 44). Two of the six studies that evaluated physical activity reported a positive result associated with the intervention (33, 44), but four did not (38–41).
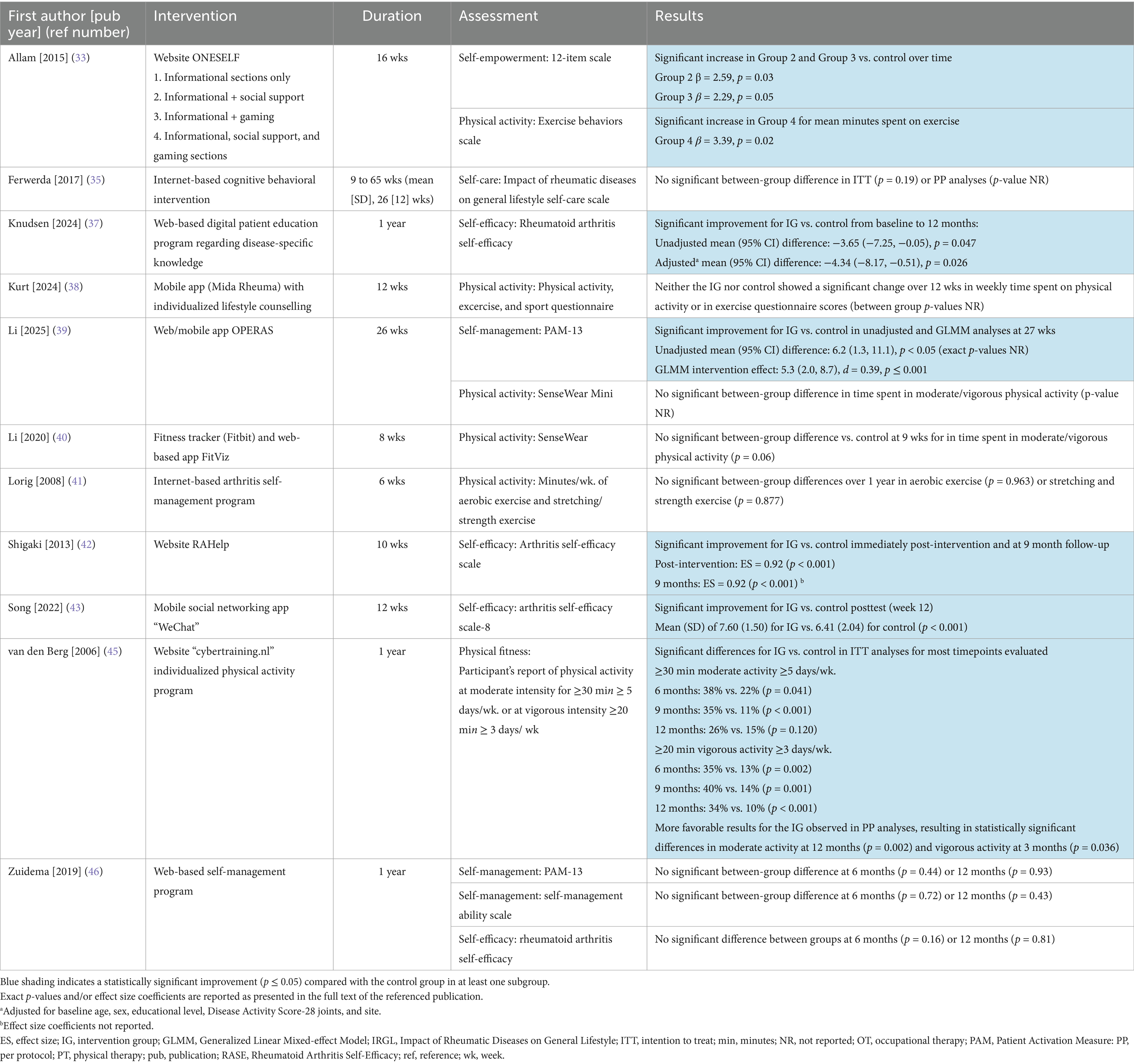
Table 5. Results of digital interventions on self-management in IRD patients.
3.5.2 Pain
Pain outcomes in the included studies also showed mixed results (Table 6). Five of the ten studies showed improvements in pain in the IG vs. control, including one study of the “CareHand” app in which overall pain intensity was similar between the two groups, but significant improvements were observed in pain in the hands/wrists (23). Longer durations for interventions did not appear to result in a greater likelihood of positive pain outcomes, as studies with the longest durations (one year, 9 to 65 weeks, and 26 weeks) failed to show significant improvements in pain.
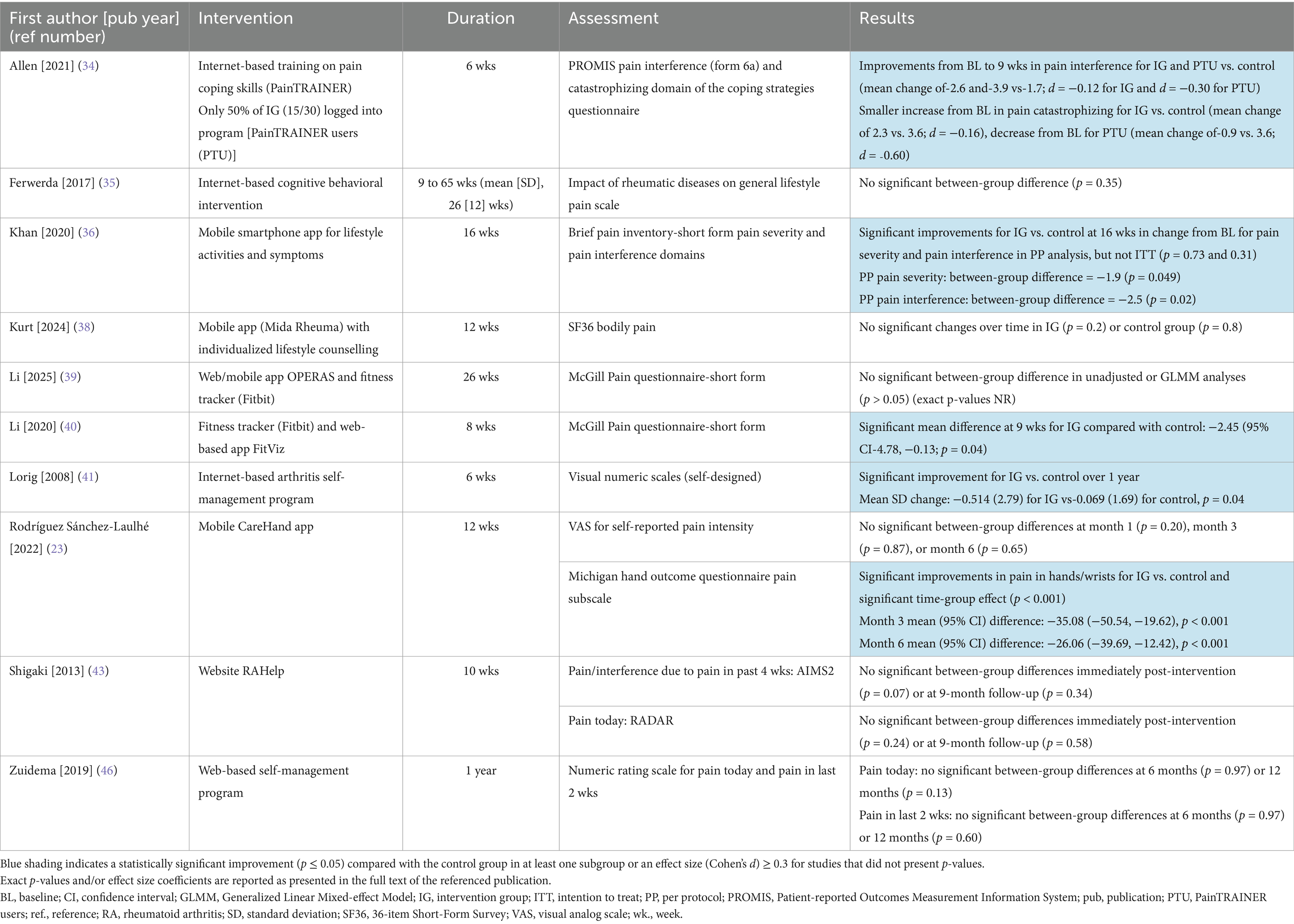
Table 6. Results of digital interventions on reduction of pain in IRD patients.
3.5.3 Symptoms of depression and anxiety
Three of the six (50%) studies that evaluated mood disorder observed a positive effect with digital interventions (Table 7). Three of the studies evaluating depressive symptoms alone and one of the studies evaluating anxiety symptoms alone reported improvements in patients in the IG vs. control. The only two studies with interventions >12 weeks showed positive results (35, 39), suggesting that longer durations may be beneficial for psychological health outcomes.
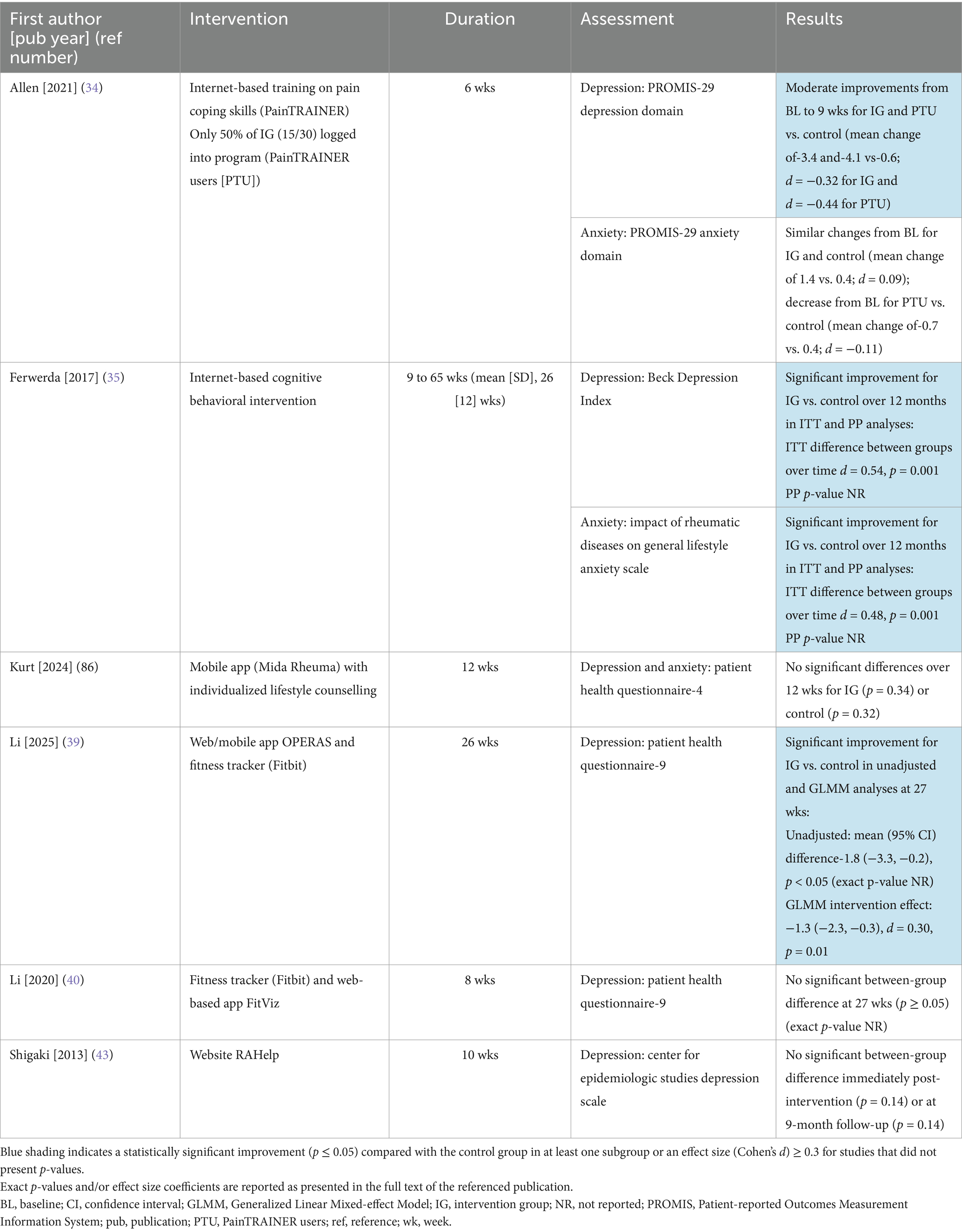
Table 7. Results of digital interventions on reducing symptoms of depression and/or anxiety in IRD patients.
3.5.4 Functional impairment
Functional impairment assessments included outcomes for non-disease-specific (e.g., Short-Form 36 physical function subscale, Health Assessment Questionnaire disability index) and disease-specific (e.g., Bath Ankylosing Spondylitis Functional Index) functional ability; many of the assessments involved the ability to perform activities of daily living. Only three of eleven studies showed a positive effect on functional impairment in patients receiving digital interventions (Table 8), and one of these positive studies was specifically focused on hand function (23).
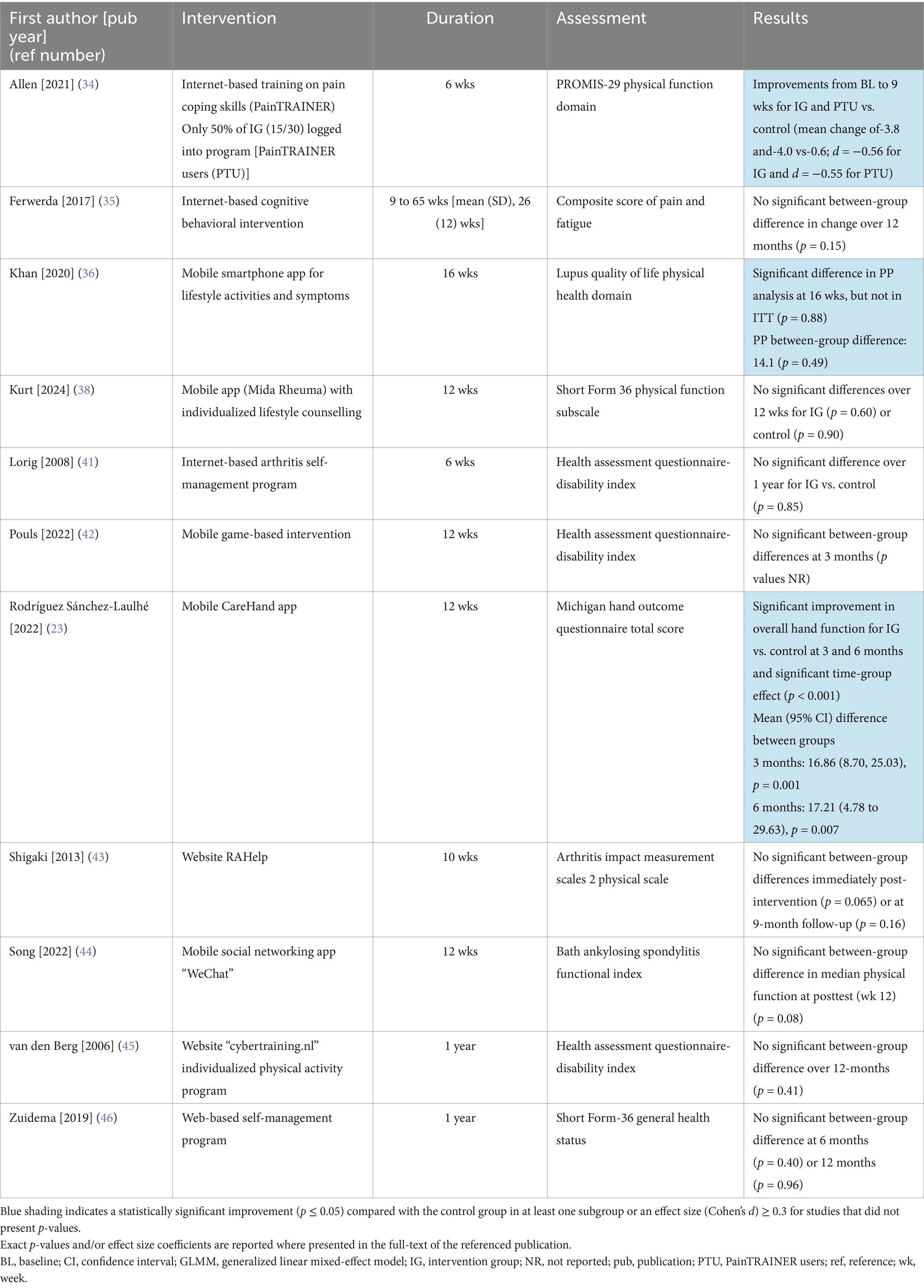
Table 8. Results of digital interventions on functional impairment in IRD patients.
3.6 Secondary outcomes
Analyses of the secondary outcomes identified for this SLR found good effects for digital interventions in some areas, but not others (Table 4; Supplementary file S4). Neither of the two studies involving medication adherence and only two of the seven studies that evaluated disease activity found differences between IG vs. control, but both studies that assessed work-related outcomes (23, 41) reported improvements with digital interventions. Three of five studies that assessed QoL found improvements for IG vs. control; in one study, the improvement was observed in the PP analysis and not in the ITT analysis (35). Two of seven studies of fatigue also found improvements.
4 Discussion
The goal of this SLR was to identify the relevance of digital tools for improving self-management and related outcomes in individuals with IRDs. Data from the 15 included studies, all of which were RCTs, reveal a mixed yet promising landscape for digital tools aimed at improving the health status of individuals with IRDs by enhancing self-management and self-care activities. While several objectives demonstrated significant benefits, others showed negligible effects, underscoring the different approaches to designing digital interventions and identifying suitable outcome measures in a heterogeneous patient population. This variability complicates direct comparisons but highlights the potential for these low-cost, scalable interventions to complement traditional care. Within a given study, the digital intervention typically affected some outcomes but not others, suggesting that improvement of disease management through the use of digital tools may not apply to all facets of IRDs.
The majority of studies that evaluated self-management outcomes not related to physical activity [5/7 (71.4%)] reported significant improvements in assessments of self-care, self-empowerment, self-efficacy, or patient activation. The two that did not were both web-based interventions that were primarily educational in nature (35, 46). It is possible that the lack of engagement fostered by these programs may have contributed to the negative findings. Physical activity levels showed an improvement in two studies (33, 45), but not in four others. Pain outcomes also revealed a broad spectrum of results. Half (5/10) of the studies highlighted significant pain reductions among participants in intervention groups, supporting the potential of digital programs to address one of the most debilitating symptoms of IRDs. The evaluation of depression and anxiety similarly yielded mixed results. While three of six (50%) interventions demonstrated significant reductions in depression symptoms (34, 35, 39), the other three found no substantial improvements (38, 40, 43). Of the two studies that specifically evaluated anxiety outcomes, one found a significant improvement (35) while the other did not (34). The limited success of digital interventions in managing mood disorders may relate to the complexity of addressing psychological well-being in the context of IRDs, as these conditions often require multi-faceted, long-term interventions that go beyond the scope of most digital programs. Furthermore, many of the interventions had a duration of only a few weeks, and longer time periods may be required for changes in psychological health. A study of cognitive behavioral therapy in medication-free patients with major depressive disorder found that depressive symptoms continued to improve over three months of therapy (47). Only three of the eleven studies that evaluated functional impairment found improvements for IG vs. control, and one of these was specifically focused on hand function (23).
With respect to the secondary outcomes identified for this SLR, only two of seven studies found a change in objective assessments of disease activity following digital interventions, which likely reflects the need for pharmaceutical approaches as the backbone for IRD disease management. Only two studies evaluated medication adherence and neither found improvements for IG vs. control. Although the lack of success with digital tools in improving medication adherence is consistent with another review of medication adherence in chronic conditions (diabetes and hypertension) (48), it should be noted that this field is one of active investigation and favorable results have been reported in some studies (49, 50). Evaluations of QoL and fatigue were positive in some studies, but not in others. Both studies that evaluated work productivity found improvements for IG vs. control (23, 41). Given the profound impact of IRDs on work participation and productivity (51, 52), these observed benefits suggest the use of digital tools to improve work outcomes deserves further study.
In addition to the seven studies that reported objective assessments of disease activity, the study by Rodríguez Sánchez-Laulhé et al. (23) evaluated the objective measures of hand grip strength and pinch strength, neither of which were affected by the digital intervention. The other studies (7/15) focused solely on patient-reported outcomes and did not include objective assessments. This approach allows large amounts of data to be collected more conveniently, but has the limitation of lacking data on the effect of the intervention on outcome measures such as joint counts or laboratory markers.
The heterogeneity of included studies poses a significant challenge to drawing overarching conclusions. Interventions varied widely in their design, content, and delivery methods, ranging from gamified programs to structured educational modules. This variability makes direct comparisons difficult and highlights the importance of tailoring interventions to meet the specific needs of diverse patient populations. Although all of the studies involved patients with IRDs, care needs may vary within this group of diseases depending on the specific disease and its characteristics. For instance, individuals with RA may require tools focused on joint protection and pain management, while those with SLE may benefit more from tools that address the systemic nature of the disease and its psychological impacts. The potential differences in response to digital tools across IRDs is supported by subgroup analyses in the study by Li et al. (40), which showed significant improvements in physical activity and pain for patients with RA, but not those with SLE. Moreover, some studies included highly specific participant groups, which may have influenced the results. For example, the study by Rodríguez Sánchez-Laulhé et al. specifically targeted patients with RA affecting the hands, wrists, or fingers for at least two years who reported current pain and disability (23). Selecting individuals with specific needs may allow more precise tailoring of the intervention, while focusing on patients who are already experiencing significant pain and functional limitations may provide more opportunity for improvement compared with studies of patients with better-controlled symptoms, potentially increasing the likelihood of a positive outcome.
There were also marked variations in the assessment tools used, even for a single symptom such as pain or fatigue. The potential effects of different assessments is illustrated by QoL evaluations in the study by Allen et al., which did not find a significant difference between IG and control in patients with SLE using the Patient Reported Outcomes Measurement Information System (PROMIS)-29, a general QoL assessment tool, but did observe a significant difference with the more disease-specific LupusPRO tool (34).
For some studies, findings may have been influenced by the duration of the digital intervention. The intervention lasted one year in three of the studies (37, 45, 46), but most of the others had intervention durations of 6 to 12 weeks. Longer studies may be more likely to capture the long-term effects of interventions on certain symptoms, such as chronic pain and fatigue, but also have the challenge of maintaining user engagement once the “novelty” of the tool has worn off. In this SLR no clear pattern was observed between the length of the intervention and the likelihood of positive outcomes. This suggests that other factors, such as the nature of the intervention, the content provided, and participant engagement, may play a more significant role in determining the effectiveness of the intervention than the duration alone.
Additional factors could have also influenced the presented results. The potential for “contamination” in control groups is a concern; in many studies it could not be guaranteed that participants in the control groups refrained from accessing alternative digital tools or platforms, which could have diluted observed between-group differences. As for all interventions, adherence is an important issue for digital tools. In one study, results of the intervention group were further divided into results obtained with patients documented to have logged onto the website (34). Several of the evaluated outcomes were positive for the user group, but not for the IG as a whole. Other studies reported PP analyses in addition to ITT analyses including all IG patients (35, 36, 42, 45), and this resulted in modest differences in significant outcomes in three of them (35, 36, 45). A better understanding of why patients do—and do not—choose to engage in digital interventions may be an important factor in integrating these tools into everyday use.
Given the variability among studies, our literature review was not designed to address which type of digital intervention (web-based, mobile app, or fitness tracker) was more effective. In addition, some interventions had non-digital components (telephone support, counseling sessions, etc.) (39, 40, 43, 45). Thus, it remains debatable whether the digital intervention alone would have resulted in similar results.
Despite the variability of the results, the findings of this review are largely encouraging, particularly given the low cost and scalability of digital interventions. Automated, internet-based programs hold significant potential for widespread dissemination and use, especially among younger, tech-savvy populations. The results of some included studies, such as the one by Ferwerda et al. (33), indicate that digital interventions are largely consistent with outcomes from face-to-face tailored cognitive behavioral therapy trials in patients with RA, thus suggesting that the online applications appear to be an effective platform for delivering this type of intervention. The observed improvements in self-efficacy, pain reduction, and other outcomes, although variable, suggest that these tools can play a valuable role in complementing traditional care. The results are particularly relevant considering the large and growing numbers of individuals affected by IRDs and limited patient-care resources in rheumatology (9). Future research should prioritize standardization of intervention designs, incorporation of longer follow-up periods, and expansion of studies to more diverse populations and settings. Tailored strategies to enhance engagement among older adults and individuals with limited digital literacy will also be critical. While current evidence highlights the promise of digital interventions, addressing gaps in study design, adherence, and implementation will be essential for maximizing their impact on the self-management and overall well-being of individuals with IRDs.
Safety is another important consideration in studies of digital health applications, but this outcome is seldom investigated or reported. Safety concerns tend to fall into several general areas, including patient harm [patient deterioration due to less frequent visits, injury due to actions proposed by the health application, such as exercise movements (40), or misinformation/misunderstanding leading to harm] and data security (53). Other potential safety issues include addictive behavior or increased stress and depression related to digital monitoring (54). Future studies should endeavor to evaluate these outcomes in addition to the benefits of digital health applications.
It should be noted that this is a field of active and ongoing investigation and new digital applications are constantly being explored. In addition to the studies and interventions included in this SLR, there are other digital health applications that may be of use in patients with rheumatologic conditions that did not meet the entry criteria for this study. As an example, the RheCORD Plus patient support and information app, which supports disease documentation and self-care and was developed through the collaborative efforts of several groups, including the German Society for Rheumatologists (BDRh), is currently recruiting patients for a clinical trial (55). Albrecht et al. (56) recently reported on twelve different prescribable digital tools used in German patients with rheumatologic conditions to manage associated symptoms such as pain and insomnia. To date, no prescribable digital health applications specifically for use in patients with inflammatory arthritis have been approved. There are also other digital interventions whose trials were published after cut-off for this SLR, such as the cognitive-behavioral tool reclarit (25) for patients with RA, or that have not yet had publications of randomized clinical trials, including the Axia (57) and YogiTherapy (58) exercise apps for patients with axial spondyloarthritis and the RheumaBuddy app for patients with RA (59). Other digital health applications are being developed for rheumatologic conditions not included in this SLR, including systemic sclerosis. A new digital app for this condition, the SALVE app, combines photography with patient-reported assessments to track patient hand outcomes (60). A complete list of all the apps being explored in the field of rheumatology is beyond the scope of this publication, but it is important to highlight the wide breadth and rapid advancement of this area.
In addition to the previously discussed variability in study designs, this SLR has several additional limitations related to the search scope, potential biases, and generalizability of the results that should be considered when interpreting the findings. The search was conducted exclusively through the databases CINAHL, PubMed, Embase and Cochrane. Although these databases are comprehensive, it is possible that relevant studies in other databases were missed. Only published studies were included, which may introduce publication bias by limiting findings to studies with predominantly positive results. This bias arises from the higher likelihood of studies with statistically significant positive outcomes being published compared to those reporting non-significant or negative findings (61). Various digital interventions in IRDs are being intensively investigated, so after the search cut-off date other relevant studies have been published, including one by Betz et al. (25). Studies were restricted to publications in English and German, potentially omitting valuable research in other languages (62). Only studies involving digital interventions were included. Other intervention types that are potentially beneficial for self-management in people with IRDs were not considered. The selection was limited to RCTs and SLRs/meta-analyses in order to ensure a higher quality of reporting; additional relevant insights might have been found in observational studies or qualitative research. The included studies evaluated outcomes in adults and therefore these findings do not necessarily apply to individuals under 18 years of age. Additionally, some studies included in this review lack comprehensive data on confounding factors, such as comorbid conditions or variations in treatment adherence, which could influence the reported outcomes.
5 Conclusion
This systematic review investigated the potential and relevance of digital tools for aspects of self-management and self-care in individuals with IRDs. Overall, certain interventions demonstrated significant benefits in fatigue, pain interference, symptoms of depression, and self-efficacy outcomes. Improvements in physical activity and disease activity were evident in some studies but not consistently across all metrics. The findings underscore the value of tailored interventions, with notable effects in specific subgroups.
As the number of patients with IRDs and the complexity of care continue to increase, digital tools are likely to constitute a critical component of patient management and provide a way to bridge the gap in care for people with IRDs. Further research is warranted to explore long-term effects and optimize intervention strategies.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material. Further inquiries can be directed to the corresponding author.
Author contributions
AV: Formal analysis, Writing – original draft, Data curation, Investigation, Writing – review & editing, Visualization, Methodology, Conceptualization, Validation. C-Bv: Conceptualization, Methodology, Funding acquisition, Writing – review & editing. SK: Funding acquisition, Writing – original draft, Writing – review & editing, Methodology, Supervision, Conceptualization, Project administration. KK: Writing – review & editing, Conceptualization, Funding acquisition, Methodology. GG: Writing – review & editing, Methodology, Conceptualization, Funding acquisition. MK: Writing – review & editing, Conceptualization, Methodology. JK: Conceptualization, Methodology, Writing – review & editing. PA: Methodology, Conceptualization, Writing – review & editing, Funding acquisition. SF: Methodology, Writing – review & editing, Conceptualization. SW: Conceptualization, Methodology, Writing – review & editing. TM: Conceptualization, Writing – review & editing, Methodology. SS-M: Methodology, Conceptualization, Funding acquisition, Writing – review & editing. CK: Methodology, Conceptualization, Writing – review & editing, Funding acquisition. WV: Writing – review & editing, Funding acquisition, Methodology, Conceptualization. MW: Writing – review & editing, Funding acquisition, Conceptualization, Methodology. PB-B: Methodology, Conceptualization, Writing – review & editing, Funding acquisition. ME: Supervision, Writing – original draft, Writing – review & editing, Data curation, Investigation, Validation, Methodology, Conceptualization, Project administration.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by the RheumaDatenRhePort (RHADAR) GbR (A Network of Rheumatologists), Erlangen, Germany, RheCORD Healthcare GmbH and Co. KG, Planegg, Germany, and Star Healthcare Management GmbH, Köln, Germany. The funding parties were not involved in the design of the systematic literature review, its data collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Acknowledgments
We thank Prof. Dr. Ralf Reintjes (University of Applied Sciences Hamburg, Hamburg, Germany) for his guidance, BDRh Service GmbH, the management company of the Professional Association of German Rheumatologists (BDRh e. V.), for advising on this research, and Sharon L. Cross, PhD, who provided medical writing support under the direction of the authors with funding from RheumaDatenRhePort (RHADAR) GbR (A Network of Rheumatologists).
Conflict of interest
SF, SW, and TM were employed by company BDRh Service GmbH.
C-BvdD received travel/meeting support from AbbVie and Galapagos/Alpha sigma. SK received grants from AbbVie, Novartis, and Sparrow, and consulting and/or speaker’s fees from AbbVie, Celgene, Chugai, Galapagos, Novartis, and Siemens Healthineers. KK received speaker’s fees from AbbVie, Galapagos, Novartis, Rheumakademie, and UCB and travel/meeting support from UCB. GG received speaker’s fees from AbbVie, Galapagos, and Novartis and travel/meeting support from AbbVie and Novartis. SS-M received speakers fees from AbbVie, Boehringer Ingelheim, Eli Lilly, GSK, Janssen-Cilag, Novartis, and UCB. MW received consulting and/or speaker’s fees from AbbVie, Fresenius, Galapagos, Lilly, and UCB and travel/meeting support from AbbVie, Galapagos, GSK, Lilly, and UCB. PB-B received speaker’s fees from AbbVie, Boehringer Ingelheim, Chugai/Roche, Janssen-Cilag, Novartis, Pfizer, and UCB and travel/meeting support from AbbVie. ME received funding for the present study for data analysis from RHADAR GbR and Star Healthcare Management GmbH, and also received consulting fees from AbbVie and RHADAR, speaker’s fees from AbbVie, Janssen-Cilag, Sanofi, and Swedish Orphan Biovitrum. C-BvdD, SK, KK, GG, SS-M, CK, WV, MW, and PB-B are members of RheumaDatenRhePort (RHADAR) GbR.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Correction note
This article has been corrected with minor changes. These changes do not impact the scientific content of the article.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1617151/full#supplementary-material
References
1. Robert Koch Institut. Entzündlich-rheumatische Erkrankungen (2010). Available online at: https://www.gbe-bund.de/pdf/rheumatische_erkrankungen.pdf (Accessed February 12, 2025).
2. Hoffmann, T, Oelzner, P, Busch, M, Franz, M, Teichgräber, U, Kroegel, C, et al. Organ manifestation and systematic organ screening at the onset of inflammatory rheumatic diseases. Diagnostics. (2021) 12:67. doi: 10.3390/diagnostics12010067
3. Van Middendorp, H, and Evers, AWM. The role of psychological factors in inflammatory rheumatic diseases: from burden to tailored treatment. Best Pract Res Clin Rheumatol. (2016) 30:932–45. doi: 10.1016/j.berh.2016.10.012
4. Baillet, A, Gossec, L, Carmona, L, Wit, MD, Van Eijk-Hustings, Y, Bertheussen, H, et al. Points to consider for reporting, screening for and preventing selected comorbidities in chronic inflammatory rheumatic diseases in daily practice: a EULAR initiative. Ann Rheum Dis. (2016) 75:965–73. doi: 10.1136/annrheumdis-2016-209233
5. Callhoff, J, Berger, K, Albrecht, K, and Strangfeld, A. Depression, anxiety and cognitive function in persons with inflammatory rheumatic diseases: cross-sectional results from the German National Cohort (NAKO). RMD Open. (2024) 10:e004808. doi: 10.1136/rmdopen-2024-004808
6. Vestergaard, SB, Esbensen, BA, Klausen, JM, Glintborg, B, Lau, L, Yilmaz Jantzen, C, et al. Prevalence of anxiety and depression and the association with self-management behaviour in >12 000 patients with inflammatory rheumatic disease: a cross-sectional nationwide study. RMD Open. (2024) 10:e003412. doi: 10.1136/rmdopen-2023-003412
7. Jacobs, P, Bissonnette, R, and Guenther, LC. Socioeconomic burden of immune-mediated inflammatory diseases -- focusing on work productivity and disability. J Rheumatol Suppl. (2011) 88:55–61. doi: 10.3899/jrheum.110901
8. Albrecht, K, Binder, S, Minden, K, Poddubnyy, D, Regierer, AC, Strangfeld, A, et al. Systematic review to estimate the prevalence of inflammatory rheumatic diseases in Germany. Z Rheumatol. (2024) 83:20–30. doi: 10.1007/s00393-022-01302-5
9. Black, RJ, Cross, M, Haile, LM, Culbreth, GT, Steinmetz, JD, Hagins, H, et al. Global, regional, and national burden of rheumatoid arthritis, 1990–2020, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. (2023) 5:e594–610. doi: 10.1016/S2665-9913(23)00211-4
10. Braun, J, Albrecht, K, Callhoff, J, Haase, I, Krause, A, Lakomek, H-J, et al. Rheumatologische Versorgung in Deutschland: Memorandum der Deutschen Gesellschaft für Rheumatologie und Klinische Immunologie 2024. Z Rheumatol. (2024) 83:249–84. doi: 10.1007/s00393-024-01539-2
11. Battafarano, DF, Ditmyer, M, Bolster, MB, Fitzgerald, JD, Deal, C, Bass, AR, et al. American College of Rheumatology Workforce Study: supply and demand projections of adult rheumatology workforce, 2015–2030. Arthritis Care Res. (2015) 70:617–26. doi: 10.1002/acr.23518
12. Kulhawy-Wibe, SC, Widdifield, J, Lee, JJY, Thorne, JC, Yacyshyn, EA, Batthish, M, et al. Results from the 2020 Canadian rheumatology association’s workforce and wellness survey. J Rheumatol. (2022) 49:635–43. doi: 10.3899/jrheum.210990
13. Kilian, A, Upton, LA, Battafarano, DF, and Monrad, SU. Workforce trends in rheumatology. Rheum Dis Clin N Am. (2019) 45:13–26. doi: 10.1016/j.rdc.2018.09.002
14. Puchner, R, Vavrovsky, A, Pieringer, H, Hochreiter, R, and Machold, KP. The supply of rheumatology specialist care in real life. Results of a nationwide survey and analysis of supply and needs. Front Med. (2020) 7:16. doi: 10.3389/fmed.2020.00016
15. Smolen, JS, Landewé, RBM, Bijlsma, JWJ, Burmester, GR, Dougados, M, Kerschbaumer, A, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. (2020) 79:685–99. doi: 10.1136/annrheumdis-2019-216655
16. Smolen, JS, Schöls, M, Braun, J, Dougados, M, FitzGerald, O, Gladman, DD, et al. Treating axial spondyloarthritis and peripheral spondyloarthritis, especially psoriatic arthritis, to target: 2017 update of recommendations by an international task force. Ann Rheum Dis. (2018) 77:3–17. doi: 10.1136/annrheumdis-2017-211734
17. Fraenkel, L, Bathon, JM, England, BR, St Clair, EW, Arayssi, T, Carandang, K, et al. American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. (2021) 73:1108–23. doi: 10.1002/art.41752
18. Krusche, M, Ruffer, N, Grahammer, M, and Knitza, J. Apps und ihre Anwendungsgebiete in der Rheumatologie. Z Rheumatol. (2020) 79:554–61. doi: 10.1007/s00393-020-00822-2
19. Knitza, J, Gupta, L, and Hügle, T. Rheumatology in the digital health era: status quo and quo vadis? Nat Rev Rheumatol. (2024) 20:747–59. doi: 10.1038/s41584-024-01177-7
20. Arcà, E, Heldt, D, and Smith, M. Comparison of health technology assessments for digital therapeutics in Germany, the United Kingdom and France. Digit Health. (2025) 11:20552076241308704. doi: 10.1177/20552076241308704
21. van Kessel, R, Srivastava, D, Kyriopoulos, I, Monti, G, Novillo-Ortiz, D, Milman, R, et al. Digital health reimbursement strategies of 8 European countries and Israel: scoping review and policy mapping. JMIR Mhealth Uhealth. (2023) 11:e49003. doi: 10.2196/49003
22. Hibbard, JH, Greene, J, Becker, ER, Roblin, D, Painter, MW, Perez, DJ, et al. Racial/ethnic disparities and consumer activation in health. Health Aff (Millwood). (2008) 27:1442–53. doi: 10.1377/hlthaff.27.5.1442
23. Rodríguez Sánchez-Laulhé, P, Luque-Romero, LG, Barrero-García, FJ, Biscarri-Carbonero, Á, Blanquero, J, Suero-Pineda, A, et al. An exercise and educational and self-management program delivered with a smartphone app (CareHand) in adults with rheumatoid arthritis of the hands: randomized controlled trial. JMIR Mhealth Uhealth. (2022) 10:e35462. doi: 10.2196/35462
24. Anghel, L-A, Farcaş, A, and Oprean, R. Medication adherence and persistence in patients with autoimmune rheumatic diseases: a narrative review. Patient Prefer Adherence. (2018) 12:1151–66. doi: 10.2147/PPA.S165101
25. Betz, LT, Jacob, GA, Knitza, J, Koehm, M, and Behrens, F. Efficacy of a cognitive-behavioral digital therapeutic on psychosocial outcomes in rheumatoid arthritis: randomized controlled trial. Npj Ment Health Res. (2024) 3:41. doi: 10.1038/s44184-024-00085-8
26. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372, 1–9. doi: 10.1136/bmj.n71
27. Cochrane Library. (2025). What is PICO? Available online at: https://www.cochranelibrary.com/about-pico (Accessed March 10, 2025).
28. Rayyan. Faster systematic literature reviews (2025). Available online at: rayyan.ai (Accessed March 10, 2025).
29. Critical Appraisal Skills Programme. CASP checklist (2018). Available online at: https://casp-uk.net/checklists-archive/CASP-Randomised-Controlled-Trial-Checklist-2018.pdf (Accessed March 10, 2025).
30. Srikesavan, C, Bryer, C, Ali, U, and Williamson, E. Web-based rehabilitation interventions for people with rheumatoid arthritis: a systematic review. J Telemed Telecare. (2019) 25:263–75. doi: 10.1177/1357633X18768400
31. Griffiths, AJ, White, CM, Thain, PK, and Bearne, LM. The effect of interactive digital interventions on physical activity in people with inflammatory arthritis: a systematic review. Rheumatol Int. (2018) 38:1623–34. doi: 10.1007/s00296-018-4010-8
32. Ritschl, V, Ferreira, RJO, Santos, EJF, Fernandes, R, Juutila, E, Mosor, E, et al. Suitability for e-health of non-pharmacological interventions in connective tissue diseases: scoping review with a descriptive analysis. RMD Open. (2021) 7:e001710. doi: 10.1136/rmdopen-2021-001710
33. Allam, A, Kostova, Z, Nakamoto, K, and Schulz, PJ. The effect of social support features and gamification on a web-based intervention for rheumatoid arthritis patients: randomized controlled trial. J Med Internet Res. (2015) 17:e14. doi: 10.2196/jmir.3510
34. Allen, KD, Beauchamp, T, Rini, C, Keefe, FJ, Bennell, KL, Cleveland, RJ, et al. Pilot study of an internet-based pain coping skills training program for patients with systemic lupus erythematosus. BMC Rheumatol. (2021) 5:20. doi: 10.1186/s41927-021-00191-6
35. Ferwerda, M, Van Beugen, S, Van Middendorp, H, Spillekom-van Koulil, S, Donders, ART, Visser, H, et al. A tailored-guided internet-based cognitive-behavioral intervention for patients with rheumatoid arthritis as an adjunct to standard rheumatological care: results of a randomized controlled trial. Pain. (2017) 158:868–78. doi: 10.1097/j.pain.0000000000000845
36. Khan, F, Granville, N, Malkani, R, and Chathampally, Y. Health-related quality of life improvements in systemic lupus erythematosus derived from a digital therapeutic plus tele-health coaching intervention: randomized controlled pilot trial. J Med Internet Res. (2020) 22:e23868. doi: 10.2196/23868
37. Knudsen, LR, Ndosi, M, Hauge, E-M, Lomborg, K, Dreyer, L, Aaboe, S, et al. Effectiveness of a novel digital patient education programme to support self-management of early rheumatoid arthritis: a randomized controlled trial. Rheumatology. (2024) 63:2547–56. doi: 10.1093/rheumatology/keae177
38. Kurt, T, Vossen, D, Schumacher, F, Strunk, J, Fedkov, D, Peine, C, et al. Effect of lifestyle counselling via a mobile application on disease activity control in inflammatory arthritis: a single-blinded, randomized controlled study. Nutrients. (2024) 16:1488. doi: 10.3390/nu16101488
39. Li, LC, Xie, H, Feehan, LM, Shaw, C, Lu, N, Ramachandran, S, et al. Effect of digital monitoring and counselling on self-management ability in patients with rheumatoid arthritis: a randomised controlled trial. Rheumatology. (2025) 64:310–20. doi: 10.1093/rheumatology/kead709
40. Li, LC, Feehan, LM, Xie, H, Lu, N, Shaw, C, Gromala, D, et al. Efficacy of a physical activity counseling program with use of a wearable tracker in people with inflammatory arthritis: a randomized controlled trial. Arthritis Care Res. (2020) 72:1755–65. doi: 10.1002/acr.24199
41. Lorig, KR, Ritter, PL, Laurent, DD, and Plant, K. The internet-based arthritis self-management program: a one-year randomized trial for patients with arthritis or fibromyalgia. Arthritis Care Res. (2008) 59:1009–17. doi: 10.1002/art.23817
42. Pouls, BPH, Bekker, CL, Gundogan, F, Hebing, RC, Van Onzenoort, HA, Van De Ven, LI, et al. Gaming for adherence to medication using Ehealth in rheumatoid arthritis (GAMER) study: a randomised controlled trial. RMD Open. (2022) 8:e002616. doi: 10.1136/rmdopen-2022-002616
43. Shigaki, CL, Smarr, KL, Siva, C, Ge, B, Musser, D, and Johnson, R. RAHelp: an online intervention for individuals with rheumatoid arthritis. Arthritis Care Res. (2013) 65:1573–81. doi: 10.1002/acr.22042
44. Song, Y, Reifsnider, E, Chen, Y, Wang, Y, and Chen, H. The impact of a theory-based mHealth intervention on disease knowledge, self-efficacy, and exercise adherence among ankylosing spondylitis patients: randomized controlled trial. J Med Internet Res. (2022) 24:e38501. doi: 10.2196/38501
45. van den Berg, MH, Ronday, HK, Peeters, AJ, Le Cessie, S, Van Der Giesen, FJ, Breedveld, FC, et al. Using internet technology to deliver a home-based physical activity intervention for patients with rheumatoid arthritis: a randomized controlled trial. Arthritis Care Res. (2006) 55:935–45. doi: 10.1002/art.22339
46. Zuidema, R, Van Dulmen, S, Nijhuis-van Der Sanden, M, Meek, I, Van Den Ende, C, Fransen, J, et al. Efficacy of a web-based self-management enhancing program for patients with rheumatoid arthritis: explorative randomized controlled trial. J Med Internet Res. (2019) 21:e12463. doi: 10.2196/12463
47. Thase, ME, Wright, JH, Eells, TD, Barrett, MS, Wisniewski, SR, Balasubramani, GK, et al. Improving the efficiency of psychotherapy for depression: computer-assisted versus standard CBT. Am J Psychiatry. (2018) 175:242–50. doi: 10.1176/appi.ajp.2017.17010089
48. Conway, CM, and Kelechi, TJ. Digital health for medication adherence in adult diabetes or hypertension: an integrative review. JMIR Diabetes. (2017) 2:e20. doi: 10.2196/diabetes.8030
49. Krackhardt, F, Jörnten-Karlsson, M, Waliszewski, M, Knutsson, M, Niklasson, A, Appel, K-F, et al. Results from the “me & my heart” (eMocial) study: a randomized evaluation of a new smartphone-based support tool to increase therapy adherence of patients with acute coronary syndrome. Cardiovasc Drugs Ther. (2023) 37:729–41. doi: 10.1007/s10557-022-07331-1
50. Li, Y, Gong, Y, Zheng, B, Fan, F, Yi, T, Zheng, Y, et al. Effects on adherence to a mobile app–based self-management digital therapeutics among patients with coronary heart disease: pilot randomized controlled trial. JMIR Mhealth Uhealth. (2022) 10:e32251. doi: 10.2196/32251
51. Rogier, C, De Jong, PHP, Van Der Helm- Mil, AHM, and Van Mulligen, E. Work participation is reduced during the development of RA, months before clinical arthritis manifests. Rheumatology. (2022) 61:2583–9. doi: 10.1093/rheumatology/keab793
52. Ukkola-Vuoti, L, Karlsson, A, Tuominen, S, Lassenius, MI, Aaltonen, J, Ranta, M, et al. Burden of idiopathic inflammatory rheumatic diseases in occupational healthcare: increased absenteeism and healthcare resource utilization. Scand J Work Environ Health. (2023) 49:341–9. doi: 10.5271/sjweh.4095
53. Su, JJ, Chan, MHS, Ghisi, GLM, Kwan, RYC, Wong, AKC, Lin, R, et al. Real-world mobile health implementation and patient safety: multicenter qualitative study. J Med Internet Res. (2025) 27:e71086. doi: 10.2196/71086
54. Grosman-Rimon, L, and Wegier, P. With advancement in health technology comes great responsibility - ethical and safety considerations for using digital health technology: a narrative review. Medicine (Baltimore). (2024) 103:e39136. doi: 10.1097/MD.0000000000039136
55. German Clinical Trials Register. (2025). Evaluation of RheCORD PLUS as patient support and information as DiGA (RhPID). https://drks.de/search/en/trial/DRKS00032185/details (Accessed March 10, 2025).
56. Albrecht, A, Taubmann, J, Minopoulou, I, Hatscher, L, Kleinert, S, Mühlensiepen, F, et al. Real-world-evidence of digital health applications (DiGAs) in rheumatology: insights from the DiGAReal registry. Rheumatol Ther. (2025) 12:267–82. doi: 10.1007/s40744-025-00744-y
57. Strunz, PP, Le Maire, M, Heusinger, T, Klein, J, Labinsky, H, Fleischer, A, et al. The exercise-app Axia for axial spondyloarthritis enhances the home-based exercise frequency in axial spondyloarthritis patients - a cross-sectional survey. Rheumatol Int. (2024) 44:1143–54. doi: 10.1007/s00296-024-05600-w
58. Grube, L, Petit, P, Vuillerme, N, Nitschke, M, Nwosu, OB, Knitza, J, et al. Complementary app-based yoga home exercise therapy for patients with axial spondyloarthritis: usability study. JMIR Form Res. (2024) 8:e57185. doi: 10.2196/57185
59. RheumaBuddy. Available online at: https://rheumabuddy.com/ (Accessed May 30, 2025).
60. Davison, AK, Krishan, A, New, RP, Murray, A, Dinsdale, G, Manning, J, et al. Development of a measuring app for systemic sclerosis-related digital ulceration (SALVE: scleroderma app for lesion VErification). Rheumatology (Oxford). (2024) 63:3297–305. doi: 10.1093/rheumatology/keae371
61. Richards, GC, and Onakpoya, IJ. Reporting biases. Catalog of Bias (2019). Available online at: https://catalogofbias.org/biases/reporting-biases/ (Accessed March 10, 2025).
62. Brassey, J, Spencer, EA, and Heneghan, C. Language biases. Catalog of Bias (2017). Available online at: https://catalogofbias.org/biases/language-bias/ (Accessed March 10, 2025).
Keywords: digital applications, inflammatory rheumatic diseases, systematic review, self-management, pain, depression, self-care, functional impairment
Citation: Volkmar A, von der Decken C-B, Kleinert S, Karberg K, Gauler G, Klennert M, Klennert J, Aries PM, Froschauer S, Wildenhain S, Muth T, Späthling-Mestekemper S, Kuhn C, Vorbrüggen W, Welcker M, Bartz-Bazzanella P and Englbrecht M (2025) Potential of digital applications for self-management and other outcomes in inflammatory rheumatic diseases: a systematic literature review. Front. Med. 12:1617151. doi: 10.3389/fmed.2025.1617151
Edited by:
Alexander Pfeil, University Hospital Jena, GermanyReviewed by:
Patrick-Pascal Strunz, University Hospital of Wuerzburg, GermanyTobias Hoffmann, University Hospital Jena, Germany
Copyright © 2025 Volkmar, von der Decken, Kleinert, Karberg, Gauler, Klennert, Klennert, Aries, Froschauer, Wildenhain, Muth, Späthling-Mestekemper, Kuhn, Vorbrüggen, Welcker, Bartz-Bazzanella and Englbrecht. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matthias Englbrecht, cG1hbmFnZW1lbnRAc3RhdHNjb2FjaC5kZQ==