 Manuel Almenara-Blasco1*
Manuel Almenara-Blasco1* Tamara Gracia-Cazaña1
Tamara Gracia-Cazaña1 Beatriz Poblador-Plou2,3Clara Laguna-Berna2,3
Beatriz Poblador-Plou2,3Clara Laguna-Berna2,3 Alba Navarro-Bielsa1
Alba Navarro-Bielsa1 Aida Moreno-Juste2,3
Aida Moreno-Juste2,3 Antonio Gimeno-Miguel2,3
Antonio Gimeno-Miguel2,3 Yolanda Gilaberte1
Yolanda Gilaberte1- 1Servicio de Dermatología, Hospital Universitario Miguel Servet, Zaragoza, Spain
- 2EpiChron Group for Research in Chronic Diseases, Aragón Health Research Institute, Zaragoza, Spain
- 3Research Network on Chronicity, Primary Care and Health Promotion (RICAPPS), Barcelona, Spain
Background: Hidradenitis suppurativa (HS) is a chronic, inflammatory skin disorder associated with significant physical and psychological burden. While individual comorbidities have been described in prior studies, a comprehensive analysis of all chronic conditions associated with HS in a large population-based cohort is lacking.
Objectives: To determine the prevalence of hidradenitis suppurativa in a large-scale, population-based study, to describe its comorbidities, and to analyze which diseases are associated with the presence of hidradenitis.
Methods: Retrospective cross-sectional observational study based on the clinical information contained in the electronic health records from the individuals of the EpiChron Cohort (Aragón, Spain) with a diagnosis of hidradenitis suppurativa (1,003 individuals from all ages and sexes) in 2019. We analyzed the prevalence of chronic comorbidities and used logistic regression models adjusted for age, sex and comorbidities to calculate the likelihood of occurrence of each of the comorbidities with a prevalence ≥1% based on the presence of hidradenitis. We used a cut-off point for statistical significance of p-value < 0.05.
Results: The prevalence of hidradenitis suppurativa was 0.10%, and it was more prevalent in women (0.12% vs. 0.08%). The most frequent chronic comorbidities were disorders of lipid metabolism (27.8%), hypertension (19.7%), and anxiety disorders (18.7%). The conditions most associated with hidradenitis were (odds ratio; 95% confidence interval) skin and subcutaneous tissue infections (3.32; 2.56–4.30), diseases of white blood cells (2.11; 1.44–3.07), and schizophrenia and other psychotic disorders (2.17; 1.16–4.06), among others.
Conclusion: HS is associated with a high burden of multimorbidity, encompassing metabolic, neuropsychiatric, musculoskeletal, and infectious conditions. These findings underscore the need for integrated and multidisciplinary management strategies. Further longitudinal research is warranted to explore causal relationships and improve clinical outcomes.
1 Introduction
Hidradenitis suppurativa (HS) is a chronic, inflammatory skin disease that primarily affects intertriginous areas such as the axillae, groin, and anogenital region, where apocrine glands are concentrated (1, 2). It is characterized by recurrent, painful nodules, abscesses, sinus tracts, and scarring. Diagnosis is typically clinical, often utilizing the Hurley staging system to assess severity. Onset usually occurs in early adulthood, and HS can persist for decades, significantly impacting quality of life (1, 2). Global prevalence estimates vary widely (0.00033–4.1%) due to differences in diagnostic criteria, populations studied, and methodologies. Highest rates of HS are reported in Europe (1.4%), followed by North America (0.67%) and Asia (0.42%). HS is more common in women, with reported female-to-male ratios ranging from 1.5:1 to 4:1 (3–5).
Beyond its dermatologic manifestations, HS is increasingly recognized as a systemic condition associated with a wide range of comorbidities that affect multiple organ systems (2, 6, 7). Research has linked HS to various other illnesses, and demonstrated a strong association with components of metabolic syndrome, including obesity, dyslipidemia, hypertension, and type 2 diabetes mellitus (6–9). These conditions are significantly more prevalent in HS patients than in the general population: some studies have reported metabolic syndrome in up to 65% of individuals with HS, versus an estimated 10–25% in the general population (6, 7, 10). Obesity in particular is strongly linked to HS, potentially contributing to its pathogenesis through mechanical stress in skin folds and chronic systemic inflammation. Lipid abnormalities and insulin resistance may also exacerbate disease severity and progression (8, 10).
HS is associated with increased cardiovascular risk (11, 12). Elevated rates of hypertension, cerebrovascular disease, and peripheral vascular disorders have been observed in HS patients, potentially contributing to higher cardiovascular mortality (11, 12). Some studies estimate a 1.7-fold increased risk of cardiovascular-related death in individuals with HS (11, 12). While the independent contribution of HS to cardiovascular risk remains unclear, the frequent co-occurrence of metabolic comorbidities underscores the need for early screening and intervention (10, 13–15).
Gastrointestinal (GI) comorbidities, particularly inflammatory bowel diseases (IBD) such as Crohn’s disease and ulcerative colitis, also more prevalent among patients with HS (16). The mechanisms linking HS and IBD remain poorly understood, but may involve shared genetic susceptibility, dysregulated immune responses, and overlapping environmental risk factors (16). Although reported prevalences vary widely, epidemiological studies reveal a several-fold increased risk of IBD in HS patients, with some case–control studies estimating a 10-fold higher risk of Crohn’s disease (2, 6, 16).
Musculoskeletal comorbidities, especially spondyloarthritis (including ankylosing spondylitis and psoriatic arthritis), are also associated with HS (17). These inflammatory joint disorders are often underdiagnosed but can significantly impair function and quality of life. Prevalence estimates of spondyloarthritis in HS patients range from 1.5 to 40% (17), but rarely exceed 2% in the general population (18). Shared inflammatory pathways, including elevated levels of TNF-α and IL-17, may explain this overlap (17, 18).
Neuropsychiatric comorbidities are common in HS and substantially contribute to disease burden (19). The chronic pain, visible lesions, malodor, and stigma associated with HS likely contribute to the psychological distress experienced by patients. Recent studies have highlighted a possible association between HS and more severe psychiatric conditions such as schizophrenia and other psychotic disorders, potentially pointing to shared inflammatory mechanisms, including systemic cytokine dysregulation (9, 20–22). Prevalence rates of depression (15–65%) and anxiety (13–36%) in HS patients are also significantly higher than those reported in the general population (20–22).
Infectious diseases constitute another important comorbidity category in HA patients, who are at increased risk of secondary skin and soft tissue infections due to impaired barrier function, recurrent abscess formation, and colonization by pathogenic bacteria (1, 2, 9). The increased prevalence of mycoses and chronic skin infections in HS patients can potentially complicate disease management and therapeutic choices (2, 23).
A better understanding of the comorbid profile of HS is essential to improve care. While previous studies have explored individual comorbidities, few have comprehensively evaluated the full spectrum of chronic conditions in a large, unselected population. In this study, we sought to (i) estimate the prevalence of HS in a large population-based cohort in Aragón, Spain; (ii) describe the sociodemographic and clinical characteristics of affected individuals; and (iii) identify chronic comorbidities that are significantly associated with HS.
2 Methods
2.1 Study design, setting and participants
This retrospective cross-sectional study was conducted using the EpiChron Cohort in Aragón, Spain. This database integrates sociodemographic and clinical information from all users of the Aragonese public health system (population 1.3 million; approximately 98% public health system utilization) with at least one chronic condition recorded between 2010 and 2019. The study population included 1,098,383 individuals with chronic conditions, of whom 1,003 had a diagnosis of HS in 2019. HS diagnosis was determined by the presence of an active clinical episode with ICD-9-CM code 705.83 in their electronic health records (EHRs). Individuals without this code served as comparators. Individuals not registered in the health system in 2018, precluding retrospective comorbidity assessment, were excluded. The study was approved by the Clinical Research Ethics Committee of Aragón (CEICA; PI23/607). Due to the epidemiological nature and use of anonymized data, informed consent was waived.
2.2 Study variables and data sources
For each participant, we analyzed sex, age, country of birth, area of residence (rural vs. urban), area-level deprivation index (categorized into quartiles, Q1–Q4, from least to most deprived) (24), smoking status, and all chronic conditions documented in their EHRs. Diagnoses were initially coded using ICPC-1 and mapped to ICD-9-CM codes. Each ICD-9-CM code was then categorized into 226 mutually exclusive clinical categories using the Clinical Classifications Software (CCS) (25). Of these, 153 were classified as chronic using the Chronic Condition Indicator (CCI) open source tool (26) which defines chronic conditions as those lasting ≥ 12 months and meeting at least one of the following criteria: (a) requiring continuous care with high recurrence risk and/or implications for patient management; or (b) causing limitations in self-care, independent living, or social interaction. Demographic variables were retrieved from the user database with mandatory completion, ensuring complete data for all participants. The absence of a registered diagnostic code was considered the absence of the disease, not missing data.
2.3 Statistical analysis
We calculated the prevalence of HS and described its distribution across sociodemographic variables. Logistic regression models were used to estimate crude and age- and sex-adjusted odds ratios (ORs) for HS based on these variables. To identify comorbidities associated with HS, we used logistic regression models to calculate the likelihood of each comorbidity (dependent variable) based on the presence of HS (independent variable). Two models were generated for each comorbidity: one unadjusted (crude OR) and one adjusted for age, sex, and all other comorbidities. Smoking status and obesity were not included in the adjusted models due to underreporting in the database. Statistical significance was set at p < 0.05. Analyses were performed using RStudio.
3 Results
3.1 Prevalence and socio-demographic features of hidradenitis suppurativa
A total of 1,003 patients had a diagnosis of HS during the study period (mean age 40.54 years, SD 16.47; 63.41% women), resulting in an overall prevalence of 0.10% (Table 1). This prevalence was significantly higher in women than men (0.12% vs. 0.08%; OR 1.52, 95% CI 1.34–1.73; Table 1). Compared to Spanish individuals, the prevalence of HS was higher among Sub-Saharan Africans (aOR 2.53; 95% CI 1.68–3.80), Latin Americans (aOR 1.59; 95% CI 1.27–2.00), and North Africans (aOR 2.00; 95% CI 1.43–2.79). Asian, North American, and Eastern European individuals had similar prevalence to Spanish individuals (Table 2). HS was comparably prevalent in rural and urban areas (0.10% vs. 0.10%; aOR 0.99, 95% CI 0.87–1.12), and more prevalent in the most deprived areas (Q4) (0.12%; aOR 1.43, 95% CI 1.21–1.69). No significant differences in prevalence were observed between Q1, Q2, and Q3 (Table 2).
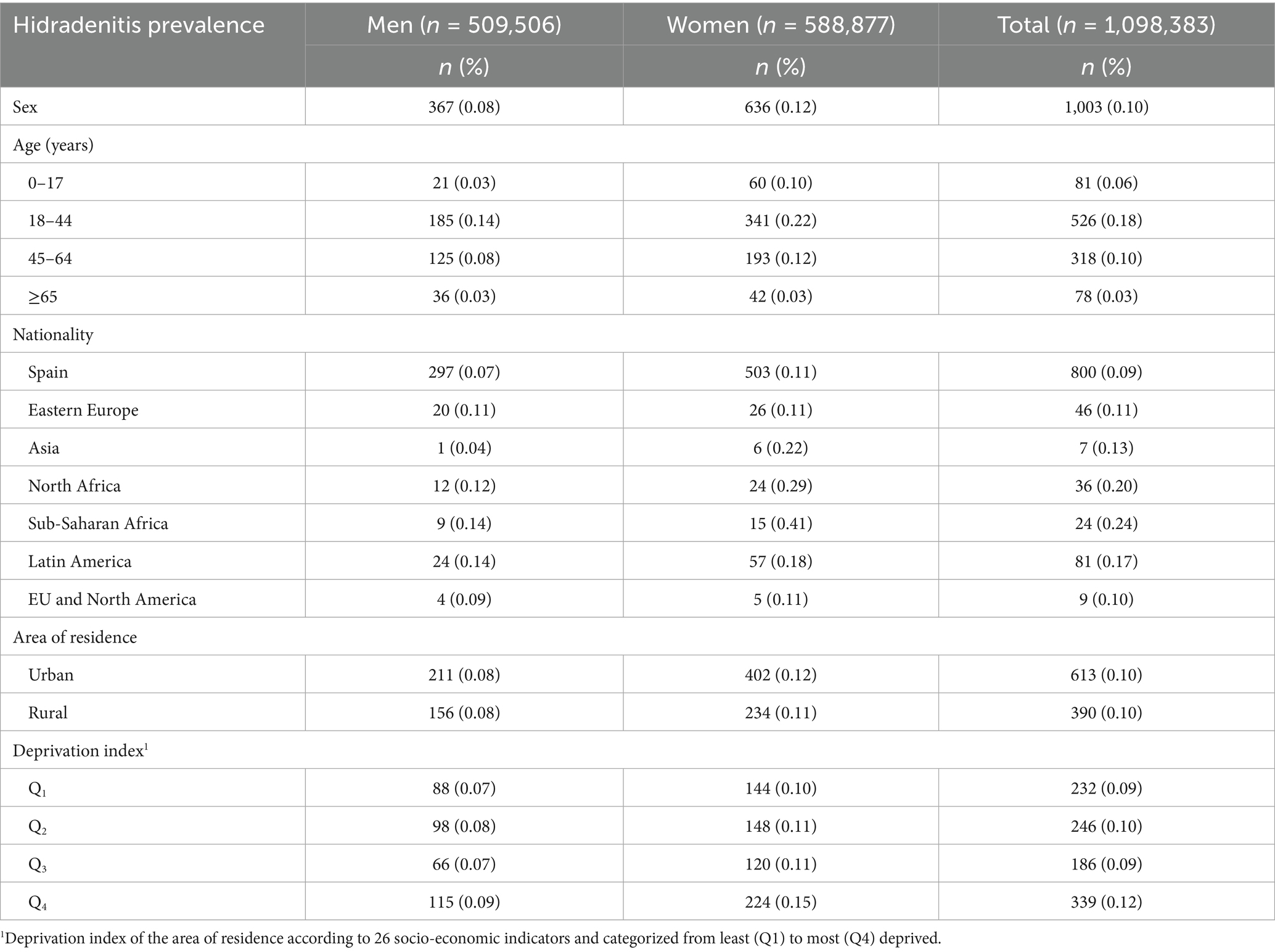
Table 1. Prevalence of hidradenitis suppurativa in the EpiChron Cohort (Aragon, Spain) in 2019 based on sociodemographic variables.
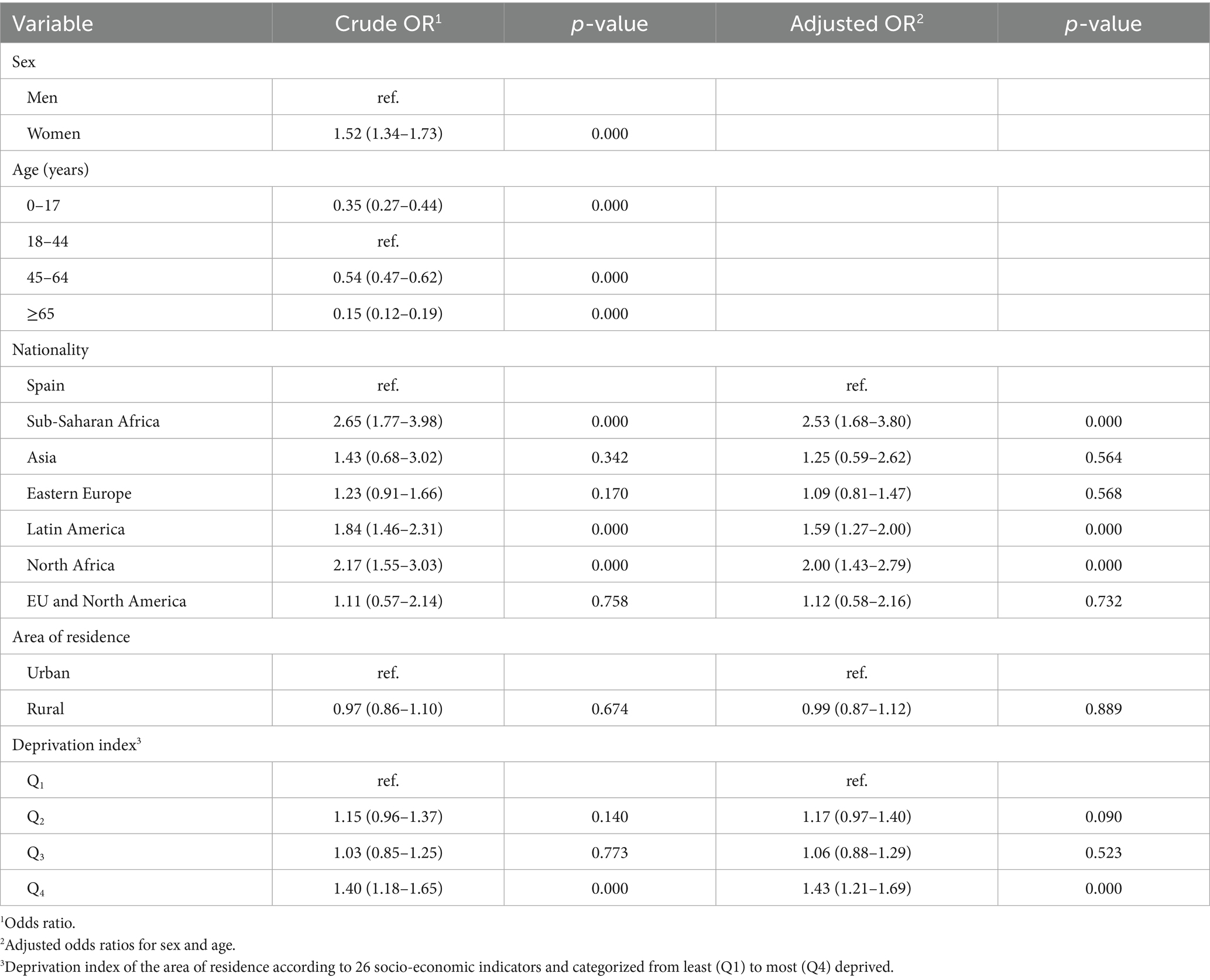
Table 2. Likelihood of presenting with hidradenitis suppurativa based on socio-demographic variables, calculated using logistic regression models.
3.2 Comorbidity of hidradenitis suppurativa
Among patients with HS, 70.99% exhibited multimorbidity, with a mean disease burden of 3.19 (SD 2.51) chronic conditions (Table 3). Approximately one-third of patients with HS had a documented history of smoking in their EHRs (Table 3).

Table 3. Socio-demographic and clinical characteristics of patients with hidradenitis suppurativa in the EpiChron Cohort in 2019.
The most frequent chronic comorbidities in patients with HS were disorders of lipid metabolism (27.82%), hypertension (19.74%), and anxiety disorders (18.74%) (Table 4).
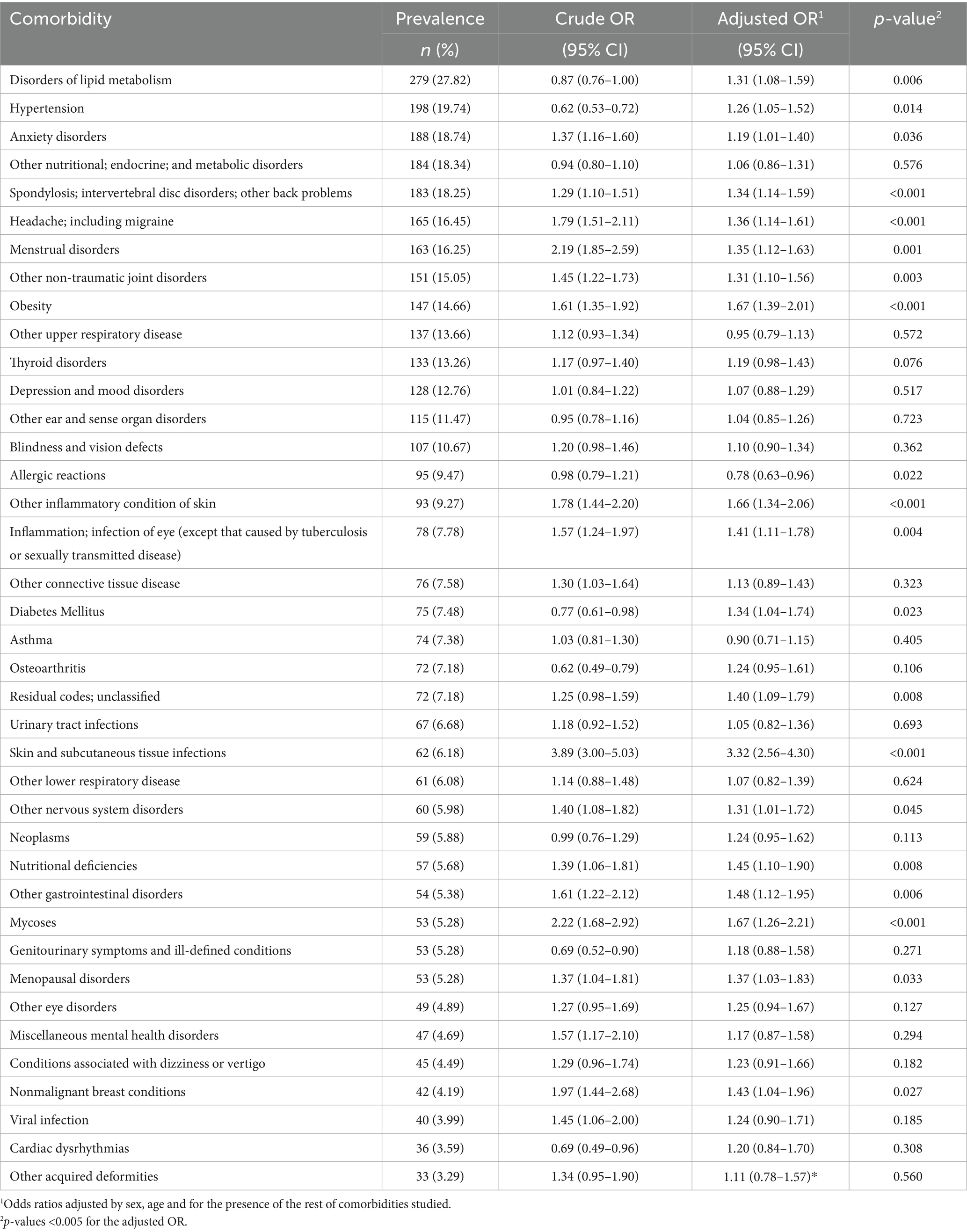
Table 4. Likelihood of comorbidities based on the presence or absence of hidradenitis suppurativa in the EpiChron Cohort.
After adjusting for sex, age, and other comorbidities, the conditions most strongly associated with HS were skin and subcutaneous tissue infections (aOR 3.32; 95% CI 2.56–4.30), diseases of white blood cells (aOR 2.11; 95% CI 1.44–3.07), and schizophrenia and other psychotic disorders (aOR 2.17; 95% CI 1.16–4.06) (Table 4). Other significantly associated comorbidities included obesity, nutritional deficiencies, diabetes mellitus, disorders of lipid metabolism, hypertension, other gastrointestinal disorders, sexual disorders, anxiety disorders, spondylosis, and mycoses. Some comorbidities, including female infertility, asthma, coagulation and hemorrhagic disorders, and acute myocardial infarction, did not show a significant association with HS (See Table 4 for complete results). For osteoporosis and other acquired deformities, the logistic regression models did not converge, precluding calculation of adjusted ORs. Unadjusted ORs for these conditions are presented in Table 4.
4 Discussion
This study comprehensively analyzed the comorbidities of 1,003 patients diagnosed with HS, focusing on the most common chronic diseases and those most strongly associated with HS, irrespective of their overall frequency.
Our finding of a higher HS prevalence in women (52% increased likelihood) aligns with previous epidemiological data reporting a predominance in women, with female:male ration of approximately 3:1 (3, 27). While the reasons for this sex bias are not fully understood, exploring intrinsic and extrinsic sex-biased immunological factors, such as the microbiome and genetics, in related autoimmune conditions may offer insights into the underlying mechanisms (3, 27).
The observed HS prevalence of 0.10% in our study is lower than some global estimates, which range up to 0.40% and are often higher in clinical (1.7%) than population-based samples (0.3%) (4). This variation likely reflects differences in diagnostic criteria, study methodologies, and the populations studied, highlighting the challenges in comparing prevalence estimates across different studies (4). No significant association between HS prevalence and the percentage of women in each study has been reported to date (4).
Our observation of a lower HS prevalence among Spanish individuals compared to Sub-Saharan Africans, Latin Americans, and North Africans is consistent with previous research documenting racial and ethnic disparities in HS: previous studies have reported highest rates in African Americans (1.30%) and lower prevalence in Hispanics (0.07%) (28). The comparable rates found in Asians and Spaniards is also consistent with the relatively low prevalence reported in among Asians (28). However, variations in racial and ethnic classifications across studies complicate direct comparisons.
Consistent with previous research, our study found a higher prevalence of HS in the most deprived areas (Q4) (aOR 1.43, 95% CI 1.21–1.69), suggesting an association between lower socioeconomic status and HS (29, 30). This may be related to lifestyle factors such as diet, smoking, and access to healthcare resources (30). Current smoking status has a higher odds ratio for HS compared with controls without HS, with an OR of 4.26 (31). Approximately one-third of HS patients in our study had a documented history of smoking, which, while potentially an underestimate due to underreporting, falls within the range reported in other studies (40–92%) (31, 32).
To comprehensively understand the comorbidity profile in HS patients, we employed a two-step strategy. First, we outlined the most common comorbidities regardless of their relationship with HS. Next, we highlighted comorbidities with an increased probability of occurring in individuals diagnosed with HS. The interplay between HS and these comorbidities is complex and may involve causal, resulting, or shared etiological factors. Our study supports previous research, revealing that HS patients frequently experience multimorbidity, with almost three in four presenting with multiple diseases and symptoms of different origins.
Previous studies have shown a correlation between HS and obesity. Rates among patients with HS range from 12 to 88%, depending on the specific population studied (31, 33). A meta-analysis across Asia, Europe, and the United States involving 5,878 HS patients and over 13 million controls found that individuals with HS are four times more likely to be obese compared with the general population (pooled OR, 4.02 [2.66–6.06]) (34). In addition, obesity can exacerbate dyslipidemia. Several studies have reported a significant association between HS and lipid abnormalities, including hyperlipidemia and decreased high-density lipoprotein (HDL) cholesterol levels. The largest cross-sectional study of 3,207 HS patients and 6,412 controls found a significantly higher risk of hyperlipidemia in the HS group versus the control population (OR 1.17) (35). A case–control study also reported a significant association between HS and decreased HDL cholesterol levels in both hospital-and population-based HS patients (14).
Type 2 diabetes is a comorbidity of HS: a meta-analysis of 12 studies revealed a notably higher proportion of DM in HS cases than in non-HS healthy controls (16.1% vs. 15.7%), and a 2.17-fold higher risk of HS in patients with DM (8). The prevalence of DM in HS patients in out cohort was lower than that reported in other studies.
HS frequently impacts other vital organ systems, notably the digestive and musculoskeletal systems. While our study did not find significant associations with IBD, it is crucial to acknowledge the complex relationship between HS and conditions like Crohn’s disease and ulcerative colitis. Both HS and IBD are chronic inflammatory conditions predominantly affecting young individuals, and they are thought to share common genetic and environmental factors (16). The challenge in distinguishing between perineal manifestations of both diseases can complicate epidemiological findings. Nevertheless, numerous studies have highlighted a concurrent occurrence of HS and IBD, particularly with Crohn’s disease (36). Reported prevalence figures vary widely, ranging from 1.2 to 23%, depending on the specific populations and methodologies employed (16). For instance, two case–control studies revealed a 2.16- to 10-fold increased likelihood of IBD (encompassing both Crohn’s disease and ulcerative colitis) in individuals with HS (37). Furthermore, a separate cohort study reported a 5.6-fold elevated risk of developing IBD in patients with HS (37).
Musculoskeletal comorbidities represent a significant burden for HS patients. Inflammatory forms of arthritis, including rheumatoid arthritis, spondyloarthritis, and psoriatic arthritis, are well-documented associations. Previous research in HS patients indicates prevalences of 3.6% (OR 2.5; 95% IC 1.6–3.9) for rheumatoid arthritis, 9.1% (3.3; 2.0–5.4) for spondyloarthritis, and 4.9% (3.1; 1.8–5.3) for psoriatic arthritis (17, 18). In our cohort, we observed an association between HS and spondylosis, which may represent a broader category encompassing various forms of inflammatory arthritis, albeit with a lower observed odds ratio than reported in some prior studies (17, 18).
The association between HS and an increased risk of cardiovascular disease is a critical area of concern. Establishing a direct causal link between HS and cardiovascular conditions is challenging, primarily because HS frequently co-occurs with intermediate risk factors such as obesity and dyslipidemia, which themselves can independently alter cardiovascular risk (10, 12, 14). Hypertension, a well-established risk factor for cardiovascular diseases, is positively associated with HS. Our study population revealed a significant association between hypertension and HS, with a prevalence of 19.74% (aOR 1.26; CI 95% 1.05–1.52). However, we observed no significant association with cerebrovascular disease or acute myocardial infarction. Studies conducted in populations similar to ours have reported links between HS and comorbidities prevalent within those groups (11, 12, 38, 39). These divergent findings prompt further inquiry into whether our population exhibits distinct characteristics, or if variations in statistical adjustments might account for these differences.
Neuropsychiatric comorbidities are highly prevalent in HS patients and significantly contribute to their overall disease burden. Conditions such as depression, anxiety, and alcoholism have consistently shown a positive relationship with HS in existing literature, both in terms of occurrence and odds ratios (19–22). However, the reported prevalence rates for these conditions tend to fluctuate notably based on the study type and the specific screening methods employed. In our cohort, rates of related comorbidities including alcohol-related disorders, sexual disorders, anxiety disorders, and depression/mood disorders were slightly lower than those reported previously (21). This variability may be partially explained by the fact that our data were derived from diagnoses made by patients’ physicians, rather than from proactive screening initiatives.
Intriguingly, the neuropsychiatric comorbidity most strongly associated with HS in our study was schizophrenia and other psychotic disorders (aOR 2.17; 95% CI 1.16–4.06). This aligns with the findings of a systematic review and meta-analysis in which the likelihood of having schizophrenia was significantly higher in HS patients than control groups (OR 1.66, 95% CI: 1.53–1.79) (22). Chronic inflammation is posited as a key mechanism underlying the relationship between HS and schizophrenia, given that elevated levels of proinflammatory cytokines have been detected in HS skin lesions, as well as in the serum and cerebrospinal fluid of schizophrenia patients (22). Further supporting this connection, a large study in Finland identified a significant link between HS and schizophrenia, reporting a prevalence of 2.4% in HS patients, which is notably higher than rates observed both in psoriasis patients and the general control population (40).
Several studies have demonstrated a significant association between HS and acne vulgaris, particularly in younger patients (41, 42). Both conditions share common pathophysiological mechanisms, including follicular occlusion and neutrophilic inflammation, suggesting a shared pathogenic basis (42). The prevalence of acne among patients with HS is estimated at 15–20%, with higher rates observed in early-onset HS or syndromic phenotypes (41). In our study, acne was included under the broader coding category of “skin and subcutaneous tissue infections.” This categorization prevented us from establishing the specific prevalence of acne in HS patients. However, the overall prevalence of cutaneous infections in this group was 6.18%, indicating a significant association (aOR 3.32; 95% CI 2.56–4.30), and acne constitutes an important component of this category. This relationship is clinically important, both diagnostically and therapeutically. Azithromycin, a macrolide with anti-inflammatory properties, has shown efficacy in the treatment of acne in adolescents and may offer therapeutic benefits in HS owing to its immunomodulatory and antimicrobial effects (43). Similarly, tetracyclines such as doxycycline and minocycline, widely used in acne management, have shown clinical effectiveness in mild-to-moderate HS through their dual anti-inflammatory and antimicrobial actions (42). These therapeutic parallels underscore the importance of considering acne not only as a frequent comorbidity of HS but also as a potential avenue for shared treatment strategies.
A relationship between HS and neoplasms has been previously described. Recent studies report that patients with HS have an increased overall cancer risk and specifically an elevated risk of squamous cell carcinoma (44). In line with that study, we observed a prevalence of neoplasms of 5.88% in HS patients, but detected no significant association.
Our findings have important implications for the understanding of HS-related comorbidities, and highlight opportunities to refine HS management and improve patient well-being. Nonetheless, it should be noted that correlation does not imply causation, and thus caution is advised when interpreting these findings. While certain associations reported here align with those of earlier studies, others are novel and may necessitate further exploration to elucidate the underlying biological mechanisms.
The main strength of our research stems from the extensive, population-based approach applied, encompassing nearly all HS diagnoses within the reference area. Moreover, our comprehensive analysis of HS-related comorbidities involved a thorough examination of virtually all chronic conditions diagnosed in both primary and hospital care, and was not limited to the most prevalent or pertinent comorbidities. The utilization of Electronic Health Records (EHRs) ensured reliability of the data, which underwent continual quality control checks. However, it should be noted that clinical data were not clinically validated and were dependent on registered diagnostic codes, which may not fully represent the actual clinical status of patients. Another limitation of our study was its retrospective cross-sectional design, which inherently prevents determination of the sequential appearance of diseases, thereby impeding the establishment of cause-and-effect relationships between HS and its comorbidities. Moreover, some relevant variables (e.g., HS severity or staging, genetic information, social variables, patient-reported outcomes) were unavailable. Other variables, such as smoking status and obesity, were clearly underreported, precluding their inclusion in adjusted models. Finally, the grouping of the original diagnostic codes into Clinical Classifications Software (CCS) categories, while improving reproducibility and comparability, could potentially hamper the clinical interpretation of results due to the non-specificity of some diagnostic categories.
5 Conclusion
This large-scale, population-based study provides a comprehensive overview of the comorbidity burden associated with HS. Our findings confirm that HS is not merely a dermatologic condition, but also a systemic disease frequently associated with multiple chronic disorders across metabolic, cardiovascular, neuropsychiatric, musculoskeletal, and infectious domains. Nearly three out of four patients with HS experienced multimorbidity, highlighting the importance of early and integrated management. The strong associations identified between HS and conditions such as obesity, schizophrenia, skin infections, and white blood cell disorders emphasize the need for multidisciplinary care strategies and routine screening for comorbidities. These insights can inform clinical practice and policy by guiding risk stratification, surveillance, and resource allocation. Future longitudinal research is warranted to clarify temporal relationships and underlying mechanisms linking HS to its associated conditions.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethical approval for this study was obtained from the Clinical Research Ethics Committee of Aragón (CEICA) that approved the research protocol for this study (PI23/607). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because Epidemiology study with data from electronic clinical records.
Author contributions
MA-B: Writing – original draft, Writing – review & editing, Methodology, Funding acquisition, Visualization, Conceptualization, Investigation. TG-C: Supervision, Investigation, Methodology, Writing – review & editing, Conceptualization, Visualization, Funding acquisition. BP-P: Formal analysis, Methodology, Data curation, Conceptualization, Software, Investigation, Writing – review & editing. CL-B: Investigation, Methodology, Data curation, Writing – review & editing, Formal analysis. AN-B: Writing – review & editing, Investigation. AM-J: Investigation, Writing – review & editing, Formal analysis, Methodology. AG-M: Resources, Investigation, Writing – original draft, Visualization, Funding acquisition, Data curation, Formal analysis, Supervision, Conceptualization, Project administration, Methodology, Writing – review & editing. YG: Writing – original draft, Project administration, Supervision, Methodology, Visualization, Validation, Conceptualization, Investigation, Resources, Writing – review & editing, Funding acquisition.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by the Carlos III Institute of Health, Ministry of Science and Innovation (Spain), through the Research Network on Chronicity, Primary Care, and Health Promotion (RICAPPS) awarded on the call for the creation of Health Outcomes-Oriented Cooperative Research Networks (grant number RD21/0016/0019), and by Gobierno de Aragón (grant number B01_23R) and co-funded with European Union’s NextGenerationEU funds. The funders played no role in the design of the study, collection, analysis, and interpretation of data, or preparation of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Goldburg, SR, Strober, BE, and Payette, MJ. Hidradenitis suppurativa: epidemiology, clinical presentation, and pathogenesis. J Am Acad Dermatol. (2020) 82:1045–58. doi: 10.1016/j.jaad.2019.08.090
2. Preda-Naumescu, A, Ahmed, HN, Mayo, TT, and Yusuf, N. Hidradenitis suppurativa: pathogenesis, clinical presentation, epidemiology, and comorbid associations. Int J Dermatol. (2021) 60:e449–58. doi: 10.1111/ijd.15579
3. Ingram, JR. The epidemiology of hidradenitis suppurativa*. Br J Dermatol. (2020) 183:990–8. doi: 10.1111/bjd.19435
4. Jfri, A, Nassim, D, O’Brien, E, Gulliver, W, Nikolakis, G, and Zouboulis, CC. Prevalence of hidradenitis Suppurativa: a systematic review and Meta-regression analysis. JAMA Dermatol. (2021) 157:924–31. doi: 10.1001/jamadermatol.2021.1677
5. Lam, M, Lai, C, Almuhanna, N, and Alhusayen, R. Hidradenitis suppurativa and down syndrome: a systematic review and meta-analysis. Pediatr Dermatol. (2020) 37:1044–50. doi: 10.1111/pde.14326
6. Garg, A, Malviya, N, Strunk, A, Wright, S, Alavi, A, Alhusayen, R, et al. Comorbidity screening in hidradenitis suppurativa: evidence-based recommendations from the US and Canadian hidradenitis Suppurativa foundations. J Am Acad Dermatol. (2022) 86:1092–101. doi: 10.1016/j.jaad.2021.01.059
7. Dauden, E, Lazaro, P, Aguilar, MD, Blasco, AJ, Suarez, C, Marin, I, et al. Recommendations for the management of comorbidity in hidradenitis suppurativa. J Eur Acad Dermatol Venereol. (2018) 32:129–44. doi: 10.1111/jdv.14517
8. Phan, K, Charlton, O, and Smith, SD. Hidradenitis suppurativa and diabetes mellitus: updated systematic review and adjusted meta-analysis. Clin Exp Dermatol. (2019) 44:e126–32. doi: 10.1111/ced.13922
9. Nguyen, TV, Damiani, G, Orenstein, LAV, Hamzavi, I, and Jemec, GB. Hidradenitis suppurativa: an update on epidemiology, phenotypes, diagnosis, pathogenesis, comorbidities and quality of life. J Eur Acad Dermatol Venereol. (2021) 35:50–61. doi: 10.1111/jdv.16677
10. Rodríguez-Zuñiga, MJM, García-Perdomo, HA, and Ortega-Loayza, AG. Association between hidradenitis suppurativa and metabolic syndrome: a systematic review and meta-analysis. Actas Dermosifiliogr. (2019) 110:279–88. doi: 10.1016/j.ad.2018.10.020
11. Joseph Bailey, AM, Oi-Yee Li, H, Tan, MG, and Kirchhof, MG. Hidradenitis suppurativa and major adverse cardiac events: a systematic review and meta-analysis. J Am Acad Dermatol. (2021) 84:844–8. doi: 10.1016/j.jaad.2020.10.005
12. Tzellos, T, Zouboulis, CC, Gulliver, W, Cohen, AD, Wolkenstein, P, and Jemec, GBE. Cardiovascular disease risk factors in patients with hidradenitis suppurativa: a systematic review and meta-analysis of observational studies. Br J Dermatol. (2015) 173:1142–55. doi: 10.1111/bjd.14024
13. Gau, S, Hsiao, Y, and Liao, W. Risk of liver dysfunction and non-alcoholic fatty liver diseases in people with hidradenitis suppurativa: a systematic review and meta- analysis of real-world evidences. Front Immunol. (2022) 13:1–10. doi: 10.3389/fimmu.2022.959691
14. Miller, IM, Ellervik, C, Vinding, GR, Zarchi, K, Ibler, KS, Knudsen, KM, et al. Association of metabolic syndrome and hidradenitis suppurativa. JAMA Dermatol. (2014) 150:1273. doi: 10.1001/jamadermatol.2014.1165
15. Lim, ZV, and Oon, HH. Management of hidradenitis suppurativa in patients with metabolic comorbidities. Ann Dermatol. (2016) 28:147–51. doi: 10.5021/ad.2016.28.2.147
16. Phan, K, Tatian, A, Woods, J, Cains, G, and Frew, JW. Prevalence of inflammatory bowel disease (IBD) in hidradenitis suppurativa (HS): systematic review and adjusted meta-analysis. Int J Dermatol. (2020) 59:221–8. doi: 10.1111/ijd.14697
17. Hanna, N, Silverberg, OM, Reaume, M, Gladman, D, Davis, MDP, Piguet, V, et al. Incidence, prevalence, and predictors of inflammatory arthritis in patients with hidradenitis suppurativa: a systematic review and meta-analysis. Int J Dermatol. (2022) 61:1069–79. doi: 10.1111/ijd.15860
18. Almuhanna, N, Finstad, A, and Alhusayen, R. Association between hidradenitis Suppurativa and inflammatory arthritis: a systematic review and Meta-analysis. Dermatology. (2021) 237:740–7. doi: 10.1159/000514582
19. Fabrazzo, M, Cipolla, S, Signoriello, S, Camerlengo, A, Calabrese, G, Giordano, GM, et al. A systematic review on shared biological mechanisms of depression and anxiety in comorbidity with psoriasis, atopic dermatitis, and hidradenitis suppurativa. Eur Psychiatry. (2021) 64:e71. doi: 10.1192/j.eurpsy.2021.2249
20. Patel, ZS, Hoffman, LK, Buse, DC, Grinberg, AS, Afifi, L, Cohen, SR, et al. Pain, psychological comorbidities, disability, and impaired qualify of life in hidradenitis suppurativa. Curr Pain Headache Rep. (2017) 21. doi: 10.1007/s11916-017-0647-3
21. Misitzis, A, Goldust, M, Jafferany, M, and Lotti, T. Psychiatric comorbidities in patients with hidradenitis suppurativa. Dermatol Ther. (2020) 33:e13541. doi: 10.1111/dth.13541
22. Phan, K, Huo, YR, and Smith, SD. Hidradenitis suppurativa and psychiatric comorbidities, suicides and substance abuse: systematic review and meta-analysis. Ann Transl Med. (2020) 8:821–1. doi: 10.21037/atm-20-1028
23. Miller, IM, McAndrew, RJ, and Hamzavi, I. Prevalence, risk factors, and comorbidities of hidradenitis suppurativa. Dermatol Clin. (2016) 34:7–16. doi: 10.1016/j.det.2015.08.002
24. Compés Dea, ML, Olivan Bellido, E, Feja Solana, C, Palacio, A I, García-Carpintero, GRH, and Adiego Sancho, B. Construction of a deprivation index by basic healthcare area in Aragon using population and housing census 2011. Rev Esp Salud Publica. (2018) 92:e201812087
25. Elixhauser, A, Steiner, C, and Palmer, L. (2009) Clinical classifications software (CCS). Available online at: http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp (Accessed July 23, 2020).
26. Agency for Healthcare Research and Quality (2020) Chronic condition indicator (CCI) for ICD-9-CM. Available online at: https://www.hcup-us.ahrq.gov/toolssoftware/chronic/chronic.jsp (Accessed July 23, 2020).
27. Young, KZ, Dimitrion, P, Zhou, L, Adrianto, I, and Mi, QS. Sex-biased immunological processes drive hidradenitis suppurativa. Front Immunol. (2023) 14:1167021. doi: 10.3389/fimmu.2023.1167021
28. Sachdeva, M, Shah, M, and Alavi, A. Race-specific prevalence of hidradenitis Suppurativa. J Cutan Med Surg. (2021) 25:177–87. doi: 10.1177/1203475420972348
29. Deckers, IE, Janse, IC, van der Zee, HH, Nijsten, T, Boer, J, Horváth, B, et al. Hidradenitis suppurativa (HS) is associated with low socioeconomic status (SES): a cross-sectional reference study. J Am Acad Dermatol. (2016) 75:755–759.e1. doi: 10.1016/j.jaad.2016.04.067
30. Choi, ECE, Phan, PHC, and Oon, HH. Hidradenitis suppurativa: racial and socioeconomic considerations in management. Int J Dermatol. (2022) 61:1452–7. doi: 10.1111/ijd.16163
31. Kohorst, JJ, Kimball, AB, and Davis, MDP. Systemic associations of hidradenitis suppurativa. J Am Acad Dermatol. (2015) 73:S27–35. doi: 10.1016/j.jaad.2015.07.055
32. Acharya, P, and Mathur, M. Hidradenitis suppurativa and smoking: a systematic review and meta-analysis. J Am Acad Dermatol. (2020) 82:1006–11. doi: 10.1016/j.jaad.2019.10.044
33. Krajewski, PK, Matusiak, Ł, and Szepietowski, JC. Adipokines as an important link between hidradenitis suppurativa and obesity: a narrative review. Br J Dermatol. (2023) 188:320–7. doi: 10.1093/bjd/ljac107
34. Choi, F, Lehmer, L, Ekelem, C, and Mesinkovska, NA. Dietary and metabolic factors in the pathogenesis of hidradenitis suppurativa: a systematic review. Int J Dermatol. (2020) 59:143–53. doi: 10.1111/ijd.14691
35. Shalom, G, Freud, T, Harman-Boehm, I, Polishchuk, I, and Cohen, AD. Hidradenitis suppurativa and metabolic syndrome: a comparative cross-sectional study of 3207 patients. Br J Dermatol. (2015) 173:464–70. doi: 10.1111/bjd.13777
36. Salgado-Boquete, L, Romaní, J, Carrión, L, and Marín-Jiménez, I. Epidemiología de la hidradenitis supurativa y de la enfermedad inflamatoria intestinal: ¿son enfermedades que se asocian? Actas Dermosifiliogr. (2016) 107:8–12. doi: 10.1016/S0001-7310(17)30003-0
37. Chen, W-T, and Chi, C-C. Association of Hidradenitis Suppurativa with Inflammatory Bowel Disease. JAMA Dermatol. (2019) 155:1022–7. doi: 10.1001/jamadermatol.2019.0891
38. Reddy, S, Strunk, A, Jemec, GBE, and Garg, A. Incidence of myocardial infarction and cerebrovascular accident in patients with hidradenitis Suppurativa. JAMA Dermatol. (2020) 156:65–71. doi: 10.1001/jamadermatol.2019.3412
39. Husein-ElAhmed, H, and Steinhoff, M. Hidradenitis Suppurativa and risk of myocardial infarction: a plausible association? Dermatol Pract Concept. (2023) 13:e2023201. doi: 10.5826/dpc.1304a201
40. Sund, R. Quality of the Finnish hospital discharge register: a systematic review. Scand J Public Health. (2012) 40:505–15. doi: 10.1177/1403494812456637
41. Wertenteil, S, Strunk, A, and Garg, A. Overall and subgroup prevalence of acne vulgaris among patients with hidradenitis suppurativa. J Am Acad Dermatol. (2019) 80:1308–13. doi: 10.1016/j.jaad.2018.09.040
42. Dessinioti, C, Katsambas, A, and Antoniou, C. Hidradenitis suppurrativa (acne inversa) as a systemic disease. Clin Dermatol. (2014) 32:397–408. doi: 10.1016/j.clindermatol.2013.11.006
43. Bardazzi, F, Savoia, F, Parente, G, Tabanelli, M, Balestri, R, Spadola, G, et al. Azithromycin: a new therapeutical strategy for acne in adolescents. Dermatol Online J. (2007) 13:4. doi: 10.5070/D33QF1X5T6
Keywords: hidradenitis suppurativa, comorbidities, Epidemiology, population-based study, multimorbidity
Citation: Almenara-Blasco M, Gracia-Cazaña T, Poblador-Plou B, Laguna-Berna C, Navarro-Bielsa A, Moreno-Juste A, Gimeno-Miguel A and Gilaberte Y (2025) Multimorbidity of hidradenitis suppurativa: a cross-sectional population-based study of its associated comorbidities. Front. Med. 12:1618975. doi: 10.3389/fmed.2025.1618975
Edited by:
Emi Dika, University of Bologna, ItalyReviewed by:
Laşin Özbek, Koç University, TürkiyeElisabetta Magnaterra, University of Bologna, Italy
Copyright © 2025 Almenara-Blasco, Gracia-Cazaña, Poblador-Plou, Laguna-Berna, Navarro-Bielsa, Moreno-Juste, Gimeno-Miguel and Gilaberte. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manuel Almenara-Blasco, bWFudWVsYWxtZW5hcmFibGFzY29AZ21haWwuY29t