 Hye Sang Park1‡
Hye Sang Park1‡ Petra Díaz del Campo2*†‡
Petra Díaz del Campo2*†‡ Maria Nieves Plana3,4,5*†‡Jessica Polo y La Borda6Mercedes Guerra-Rodríguez2Mireia Moreno7,8
Maria Nieves Plana3,4,5*†‡Jessica Polo y La Borda6Mercedes Guerra-Rodríguez2Mireia Moreno7,8 Juan D. Cañete9
Juan D. Cañete9- 1Rheumatology Department, Hospital de la Santa Creu i Sant Pau, Biomedical Research Institute (IIB Sant Pau), Universitat Autònoma de Barcelona, Barcelona, Spain
- 2Research Unit, Spanish Society of Rheumatology (SER), Madrid, Spain
- 3Health Technology Assessment Unit, Hospital Universitario Ramón y Cajal (IRYCIS), Madrid, Spain
- 4Department of Surgery, Medical and Social Sciences, Faculty of Medicine and Health Sciences, University of Alcala, Madrid, Spain
- 5CIBER Epidemiology and Public Health (CIBERESP), Madrid, Spain
- 6Rheumatology Department, Hospital Central de la Defensa Gómez Ulla, Health Research Institute-Fundación Jiménez Díaz (IIS-FJD), Madrid, Spain
- 7Department of Reumatology, Parc Taulí Hospital Universitari, Institut d'Investigació i Innovació Parc Taulí (I3PT-CERCA), Taulí de Sabadell, Spain
- 8Department of Medicine, Universitat Autònoma de Barcelona, Sabadell, Spain
- 9Arthritis Unit, Rheumatology Department, Hospital Clínic and IDIBAPS, Barcelona, Spain
Objectives: To assess efficacy of withdrawal or tapering biologic disease-modifying antirheumatic drugs (bDMARDs) vs. maintaining a standard regimen in patients with axial spondyloarthritis (axSpA) to sustain remission.
Methods: We conducted a systematic review of randomized controlled trials (RCTs) through July 2025, comparing treatment discontinuation or tapering against standard bDMARDs regimens in axSpA. We included RCTs of axSpA patients randomized to treatment interruption or tapering compared with standard treatment regimens. Outcomes measures included remission or flare measured by Ankylosing Spondylitis Disease Activity Score (ASDAS), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), and acute phase reactants. We rated the certainty of evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system. We presented dichotomous outcomes as risk ratios (RR) with their 95% confidence intervals (CI). We used a random-effect model to perform a pooled analysis.
Results: Eight RCTs involving 1,384 participants were analyzed. For those in sustained remission >6 months, withdrawal led to a significantly lower rate of inactive disease state (RR 0.58, CI 0.45–0.76; high certainty) and increased risks of flare (RR 1.79, CI 1.34–2.38; high certainty) and partial flares (RR 1.57, CI 1.25–1.97; high certainty) compared to the standard regimen. Patients with short-term remission <6 months and treatment withdrawal experienced significantly higher rates of flares (RR 0.41 CI 0.23–0.72, low certainty) and increased disease activity (RR 0.36 CI 0.15–0.86, low certainty). Tapering in 211 patients showed non-significant risk reductions in maintaining remission or low disease activity (RR 0.89, CI 0.66–1.18; moderate certainty).
Conclusion: Treatment withdrawal reduces the likelihood of maintaining inactive or low disease activity. Tapering does not significantly compromise the maintenance of remission or low disease activity offering a safer alternative to complete treatment withdrawal.
1 Introduction
Over the past three decades, the primary goal of patient treatment in rheumatology has been tightly focused on disease control. However, in recent years, there has been a notable shift in interest toward achieving optimal control of disease comorbidities and enhancing patients' quality of life. While the American College of Rheumatology (ACR) guideline of 2019 does not recommend tapering or withdrawal of treatment (1), updated recommendations from the European League Against Rheumatism (EULAR) suggest that tapering strategies may be a viable approach (2). To date, systematic literature reviews (SLRs) examining the efficacy and safety of tapering and withdrawal strategies in axial spondyloarthritis (axSpA) have been published (3–5) including mostly studies prior to 2019, with a smaller pool of studies and patients, as well as increased heterogeneity in the findings.
To address these gaps and provide updated guidance, we have conducted a SLR and meta-analysis as part of the development process for updating the Spanish Society of Rheumatology's guideline for axial spondyloarthritis (ESPOGUIA) (6). We have incorporated more recent randomized controlled trials (RCTs) focusing on treatment withdrawal and tapering according to previous remission duration. We aim to provide clinicians with updated guidance informed by the latest evidence and tailored to the diverse needs of patients with axSpA.
The objective of this study was to evaluate the efficacy of withdrawal or tapering treatment compared to continuing a standard regimen of biologic disease-modifying antirheumatic drugs (bDMARDs) in maintaining remission in patients with axSpA. The results of this study are relevant to inform clinical decisions regarding long-term treatment of axAspA, which could lead to optimized patient outcomes and resource utilization in clinical practice.
2 Methods
Our results are reported, and our analyses conducted, in accordance with the guidelines of the Cochrane Collaboration and the Preferred Reporting Items for SLR and Meta-analysis (PRISMA) (7). This study, being a meta-analysis, involved the secondary use of existing, publicly available, and de-identified data. According to the European General Data Protection Regulation (GDPR), such studies do not require formal ethics approval. Therefore, our protocol was not reviewed by the Ethics Committee.
2.1 Inclusion criteria
The research question was formulated according to the Population, Intervention, Comparison, Outcome and Study design (PICOS) method, in which each of the items was defined as specified below.
We selected for inclusion randomized clinical trials including adult patients (≥18 years) diagnosed with axSpA.
Interventions included were: withdrawal (Placebo), dose reduction, or tapering (increased administration interval) of bDMARDs including Infliximab, Etanercept, Adalimumab, Certolizumab, Golimumab, Secukinumab, Ixekizumab, and Bimekizumab.
Comparison interventions included bDMARDs indicated for axSpA at their standard doses and administration intervals.
Outcomes of interest were: remission and low disease activity, defined by Ankylosing Spondylitis Disease Activity Score (ASDAS) with C-Reactive Protein (CRP); or Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) <4 and low serum CRP concentration; disease flare according to ASDAS or BASDAI.
There were no restrictions on minimum follow-up time or sample size.
2.2 Search strategy
A thorough bibliographic search was conducted by a documentary specialist (MG) to identify studies meeting the inclusion criteria in the Pubmed (MEDLINE), EMBASE, and Cochrane Library databases up to July 2025.
Our search strategy included both medical subject headings (MeSH) and free text terms relevant to the population, intervention, comparison, and outcome framework. The MeSH terms used included: “axial spondyloarthritis” [Mesh] OR “spondylitis, Ankylosing” [Mesh] OR “axial SpA” AND “interrupt*” OR “discontin*” OR “termination” OR “withdraw*.”
Language restriction was not applied.
2.3 Study selection and data extraction
We included RCTs that evaluated the impact of withdrawal or tapering bDMARDs compared to the standard regimen on disease activity in patients with axSpA. Additionally, we included prior rigorous SLR to identify further studies relevant to our research question. Two reviewers (HSP and JPB) independently conducted an initial screening of titles and abstracts. Subsequently, the articles considered as potentially relevant were assessed in full-text. Any disagreements between the reviewers were resolved through consensus or consultation with expert reviewers (PDC or MNP). Data extracted included study design, population characteristics, interventions, comparators, sample size, and results. Additionally, authors were contacted via email to clarify uncertainties or to retrieve missing data.
2.4 Critical appraisal
The risk of bias in included studies was assessed using RoB2 (Cochrane risk-of-bias tool for randomized trials) (8). The overall certainty of the evidence was rated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach (9). Initial evaluations were conducted by HSP, and subsequently verified by expert reviewers, MNP and PDC. Any discrepancies were rigorously discussed until a consensus was achieved among the reviewers.
2.5 Statistical analysis
We used risk ratios (RR) with 95% confidence intervals (CIs) and random effects models to pooled data. The statistical heterogeneity of meta-analysis estimates was assessed using the I2 statistic. We used STATA V17 for data analysis.
3 Results
3.1 Study selection
A total of 3,209 references were identified across several databases–1,596 in Pubmed, 819 in EMBASE, and 794 in the Cochrane Library. After eliminating 191 duplicates, two reviewers initially screened the titles and abstracts of 3,018 references. Through this screening, 2,995 studies were excluded, leaving 23 for full text review (Figure 1). Ultimately, eight RCTs were chosen for inclusion. The references of the excluded studies and the reasons for their exclusion are detailed in Supplementary Material.

Figure 1. Flowchart of the study selection process.
3.2 Characteristics of the RCTs
The RCTs were published between 2013 and 2023, with most being phase 4 (10–14), except for three that were phase 3 (15–17). Table 1 summarizes the characteristics and risk of bias of the eight studies included.
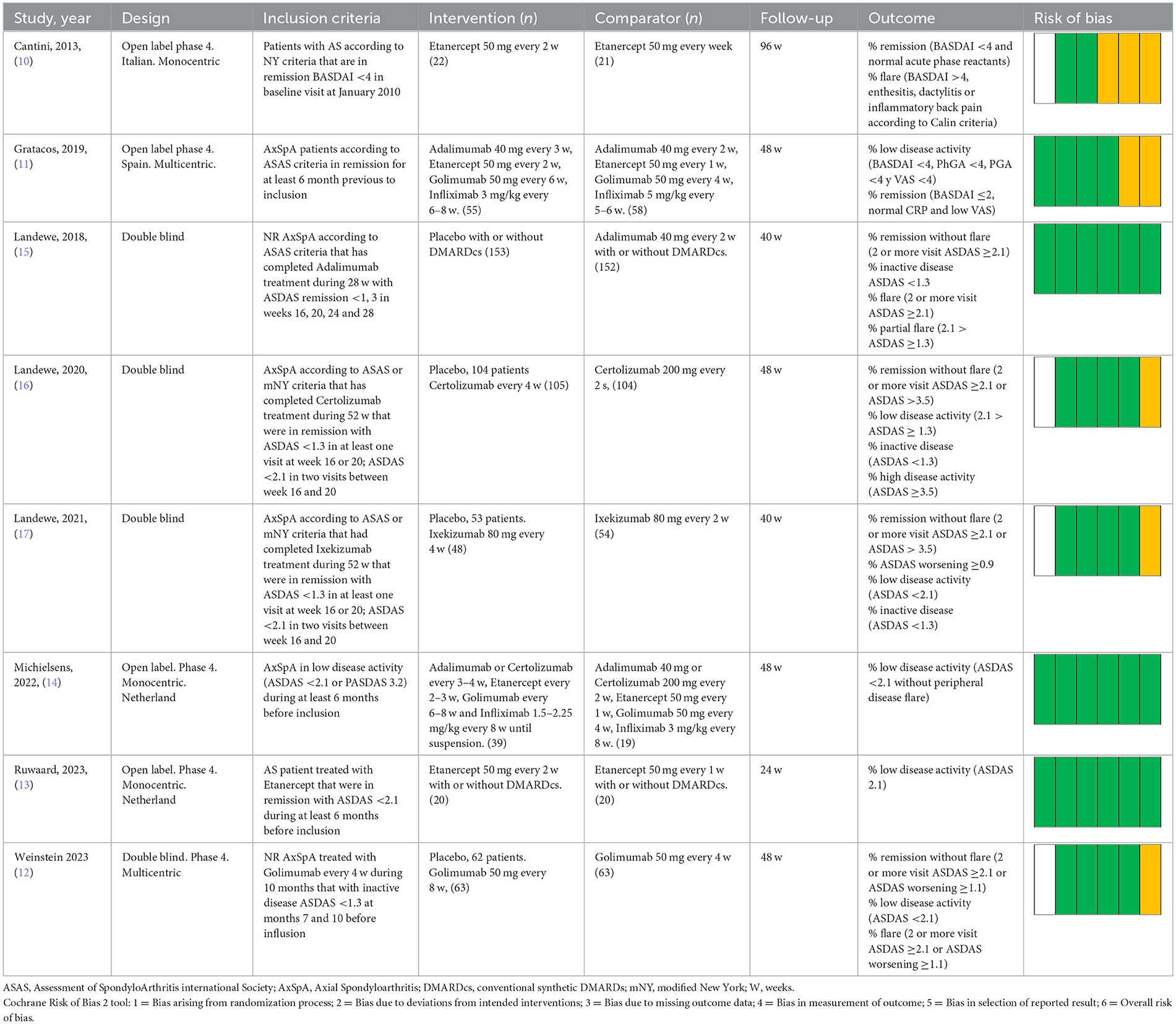
Table 1. Characteristics of the RCT included and risk of bias.
In total, 1,286 patients were included across all studies. Participants' ages ranged from 18 to 65 years. The proportion of females varied between 15.9 and 38%. Participants in the studies were primarily selected based on diagnostic criteria from the ASAS or the modified New York criteria, with remission status defined by BASDAI or ASDAS scores at baseline. The specific criteria for remission at inclusion and the precise operational definitions for all primary and secondary outcomes for each study are detailed in Table 2. Two studies included only non-radiographic axial spondyloarthritis (nr-axSpA).
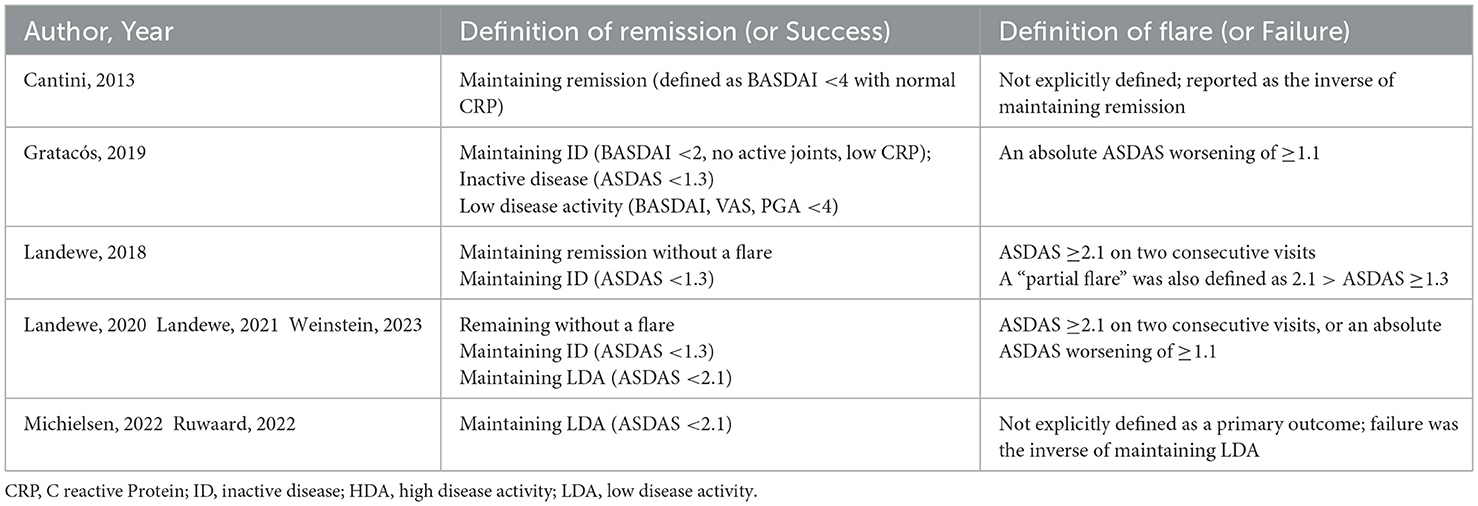
Table 2. Remission criteria and flare definition of the studies included.
Clinically, participants were enrolled in the studies during periods of remission or while exhibiting low disease activity. Disease duration varied depending on inclusion criteria, ranging from newly diagnosed individuals and those with long-standing disease. The interventions involved mostly anti-TNFα treatment except for one trial that involved Ixekizumab.
Detailed description of the demographical and clinical characteristics of the participants is summarized in Table 3.
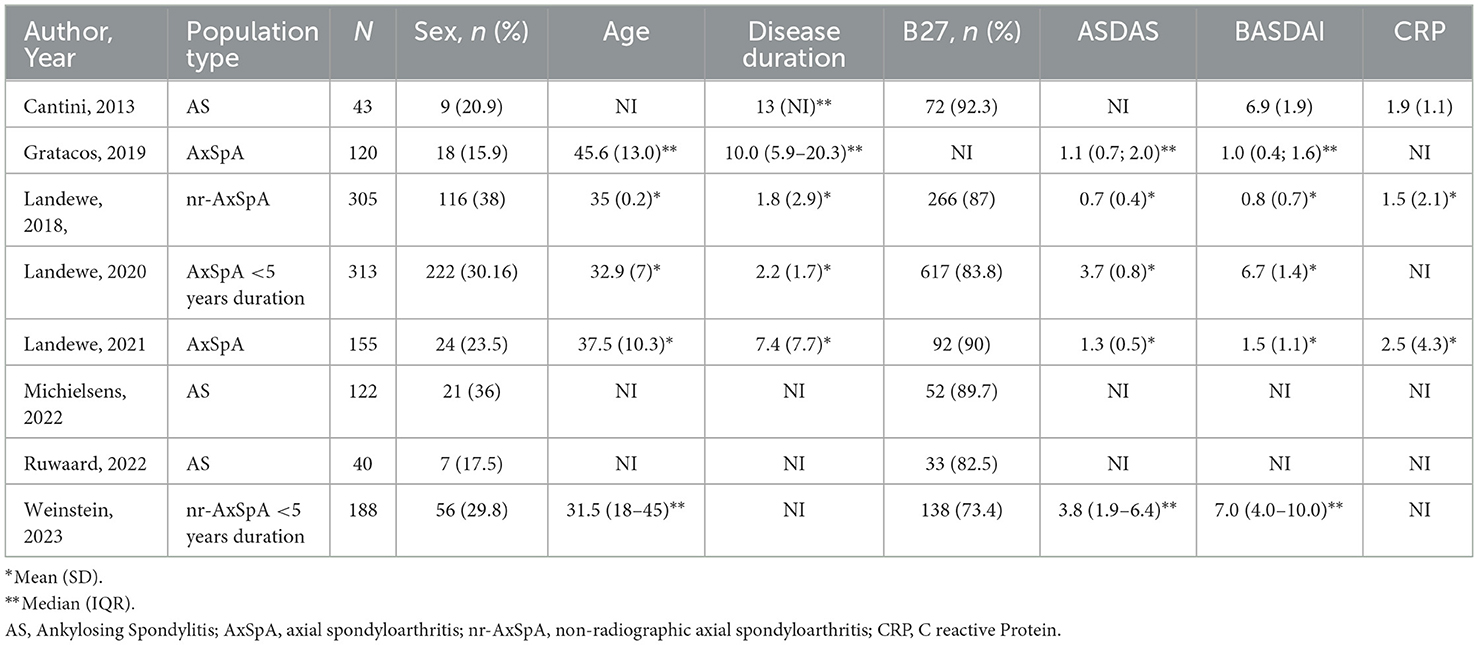
Table 3. Demographic and clinical characteristics of participants.
The follow-up periods ranged from 24 to 96 weeks. The risk of bias was assessed as low in three of the RCTs and remained uncertain in the other five, largely due to incomplete details on randomization processes and allocation concealment.
3.3 Efficacy of treatment withdrawal
3.3.1 Patients with sustained remission (at least 6 months)
Only one study, by Landewé et al. (15), assessed the efficacy of treatment withdrawal in patients with at least 6 months prior to inclusion. The study included 305 patients with nr-axSpA and compared the outcomes of withdrawing Adalimumab to continuing with the standard regimen over a period of 10 months.
In this study, it was found that 47.1% patients of the withdrawal group had maintained remission without experiencing a flare, compared to 70.4% patients who continued on the standard regimen (RR 0.66, 95% CI 0.55–0.81; high certainty evidence). Additionally, 33.3% patients of the withdrawal group maintained a state of inactive disease (ASDAS <1.3) as opposed to 57.2% patients on the standard regimen (RR 0.58, 95% CI 0.45–0.76; high certainty evidence).
Conversely, 52.9% patients of the withdrawal group experienced a disease flare (ASDAS ≥2.1 on two consecutive visits) compared to 29.6% patients in the standard regimen group (RR 1.79, 95% CI 1.34–2.38; high certainty evidence). Furthermore, 64.1% patients of the withdrawal group experienced a partial flare (2.1 > ASDAS ≥ 1.3) in contrast to 40.8% patients who continued with the standard regimen (RR 1.57, 95% CI 1.25–1.97; one trial; high certainty evidence).
Table 4 summarizes outcome results and certainty of evidence. Figure 2 shows the forest plot of the meta-analysis of the outcomes.

Table 4. Synthesis and certainty of evidence.
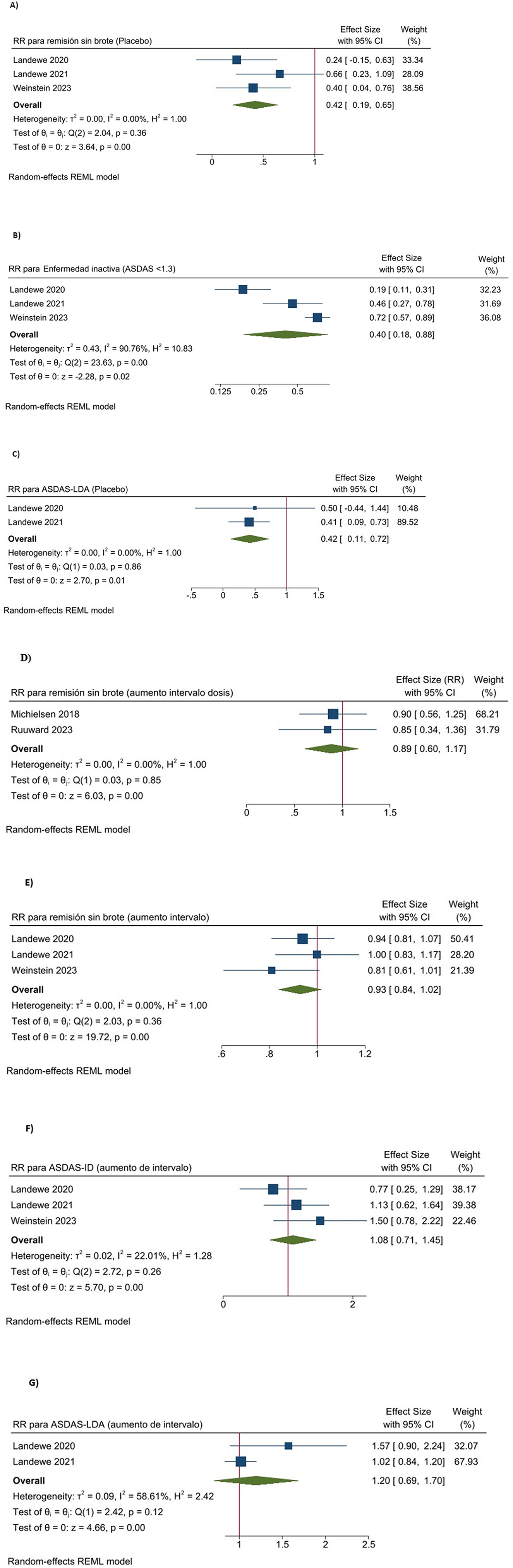
Figure 2. Forest plot of the meta-analysis combining the results of the RCTs. (A) Efficacy of treatment discontinuation in patients with short term remission: remission without flare. (B) Efficacy of treatment discontinuation in patients with short term remission: inactive disease. (C) Efficacy of treatment discontinuation in patients with short term remission: low disease activity. (D) Efficacy of treatment tapering in patients with sustained remission: low disease activity. (E) Efficacy of treatment tapering in patients with short term remission: remission without flare. (F) Efficacy of treatment tapering in patients with short term remission: inactive disease. (G) Efficacy of treatment tapering in patients with short term remission: low disease activity.
3.3.2 Patients with short term remission (<6 months)
Three double-blind RCTs—Landewé et al. (16, 17), and Weinstein et al. (12)—assessed the efficacy of treatment withdrawal in maintaining remission in 440 patients with axSpA who had achieved sustained remission between months 4 and 10 post-treatment initiation. These studies evaluated the withdrawal of Certolizumab (16), Ixekizumab (17), and Golimumab (12) compared to the standard regimen over a follow-up period of 10–12 months.
Pooled analysis of the three studies (12, 16, 17) showed that 32.4% patients of the withdrawal group remained without a flare (defined as ≥ASDAS 2.1 on two consecutive visits or an ASDAS worsening ≥1.1), compared to 83.7% patients of the standard regimen group (RR 0.41, 95% CI 0.19–0.65; three trials; moderate certainty evidence; Table 4, Figure 2A).
Landewé et al. (17), observed that 30.2% patients of the withdrawal group remained in remission without an ASDAS worsening ≥0.9 compared to 74.1% patients in the standard regimen group (RR 0.41, 95% CI 0.26–0.63; one trial; low certainty evidence).
Moreover, according to the three RCTs (12, 16, 17), 29.7% patients of the withdrawal group remained in an inactive disease state (ASDAS <1.3) compared to 71.5% patients of the standard regimen group (RR 0.40, 95% CI 0.18–0.88; three trials; moderate certainty evidence; Table 4, Figure 2B).
Additionally, according to Landewe et al. (16, 17), 28% patients of the withdrawal group maintained low disease activity (ASDAS <2.1) as opposed to 82.9% patients on standard regimen group (RR 0.36, 95% CI 0.15–0.86; two trials; moderate certainty evidence; Table 4, Figure 2C).
In the study of Weinstein et al. (12), 61.3% (38/62) patients of the withdrawal group experienced a flare (≥2 consecutive ASDAS ≥2.1 or worsening ≥1.1) compared to 16.1% patients of the standard regimen group (RR 3.86, 95% CI 2.12–7.05; one trial; low certainty evidence).
3.4 Efficacy of treatment tapering
3.4.1 Patients with sustained remission (at least 6 months)
Three open randomized clinical trials—Gratacós et al. (11), Michielsens et al. (14), and Ruwaard et al. (13)—explored the efficacy of treatment tapering in maintaining remission among 211 patients with axSpA who had been in sustained remission for at least 6 months. The studies focused on tapering anti-TNFα treatment (11, 14) and Etanercept (13) compared to the standard regimen over a follow-up period of 6–12 months.
According Gratacos et al. (11), 78.2% of patients in the treatment tapering group maintained inactive disease status according to BASDAI (characterized by BASDAI <2, no joint activity, and low CRP) compared to 83.7% in the standard regimen group, with no significant difference (risk difference −5.5%, 95% CI −20.6% to 9.7%; 1 trial; low certainty evidence). Furthermore, 53.5% of the tapering group maintained inactive disease status according to ASAS (ASDAS <1.3) vs. 61.4% in the standard regimen group, with no significant difference (risk difference 7.8%, 95% CI −10% to 25.8%; 1 trial; low certainty evidence) (11). The same study revealed that 81.3% patients remained with low disease activity (defined by BASDAI, VAS, and PGA <4) after tapering, vs. 83.8% patients in the standard regimen group, with no significant difference (risk difference −2.5%, 95% CI −16.6% to 11.7%; one trial; low certainty evidence) (11). Regarding flares, Gratacos et al. (11) observed that 12.7% of the tapering group experienced a new flare (ASDAS worsening ≥1.1) compared to 6.6% in the standard regimen group, with no significant difference (risk difference −6.1%, 95% CI −25.2% to 12.9%; low certainty evidence).
According to Michielsens et al. and Ruwaard et al. (13, 14), 62.7% of the patients in the tapering groups maintained low disease activity by ASDAS compared to 82.1% in the standard regimen groups, with a non-significant lower risk in the tapering groups (RR 0.89, 95% CI 0.66–1.18; two trials; moderate certainty evidence; Table 4, Figure 2D).
3.4.2 Patients with short-term remission (<6 months)
Three double-blind RCTs—Landewe et al. (16, 17), and Weinstein et al. (12)—investigated the efficacy of treatment tapering in maintaining remission in 437 patients with axSpA who had achieved sustained remission between months 4 and 10 post-treatment initiation. These studies compared tapering Certolizumab, Ixekizumab, and Golimumab against a standard regimen over a follow-up period of 10–12 months.
Pooled analysis of the three RCTs (12, 16, 17), showed that 76.9% of patients in the treatment tapering groups remained in remission without a flare, compared to 83.7% patients with the standard regimen, suggesting slightly lower but non-significant risk for tapering (RR 0.93, 95% CI 0.84–1.02; three trials; moderate certainty evidence; Table 4, Figure 2E).
It was observed by Landewe et al. (17) that 72.9% patients of the tapering group remained in remission without ASDAS worsening compared to 74.1% patients with the standard regimen, indicating a marginally higher but non-significant risk for tapering (RR 0.98, 95% CI 0.78–1.24; one trial; low certainty evidence).
Regarding inactive disease status, all three studies (12, 16, 17), showed that 64.8% of the patients in the tapering groups kept an ASDAS <1.3, compared to 71.5% patients with the standard regimen, indicating a slightly higher but non-significant risk for tapering (RR 1.08, 95% CI 0.71–1.45; three trials; moderate certainty evidence; Table 4, Figure 2F).
Regarding low disease activity, Landewe et al. (16, 17), showed that 76.5% of patients in the tapering groups maintained an ASDAS <2.1, compared to 82.9% with the standard regimen, with a slight but non-significant decrease in risk associated with tapering (RR 0.94, 95% CI 0.81–1.09; two trials; moderate certainty evidence; Table 4, Figure 2G).
Regarding flares, only Weinstein et al. found that, 23.8% of patients in the tapering group experienced a flare compared to 15.9% with the standard regimen, suggesting a higher but non-significant risk with tapering (RR 1.5, 95% CI 0.73–3.08; one trial; low certainty evidence) (12).
3.4.3 Patients in remission at inclusion (duration not specified)
Only one trial by Cantini et al. (10) assessed the efficacy of treatment tapering in 43 patients with axSpA who were in remission (defined as BASDAI <4 with normal CRP) at the time of inclusion, though the duration of remission prior to the study was not specified. This study compared the outcomes of Etanercept tapering against a standard regimen over a follow-up period of 24 months.
In this study 86.3% of patients in the tapering group had maintained remission compared to 90.4% in the standard regimen group, suggesting a non-significant minor risk for tapering (RR 0.95, 95% CI 0.77–1.18; one trial; low certainty evidence) (10). Regarding flares, 13.6% of patients in the tapering group experienced a flare compared to 9.5% in the standard regimen group, with a non-significant higher risk for tapering (RR 1.43, 95% CI 0.27–7.73; one trial; low certainty evidence).
4 Discussion
The current meta-analysis aimed to determine whether withdrawal or tapering of bDMARD in comparison to the standard regimen, could maintain remission or low disease activity in axSpA patients who had already achieved these states. The results showed that treatment withdrawal significantly decreased the likelihood of maintaining remission with a RR of 0.66 (95% CI 0.55–0.81). In contrast, tapering treatment only slightly reduced the probability of sustaining remission with an RR of 0.93 (95% CI 0.84–1.02), which was not statistically significant.
In terms of flare risk, withdrawal was associated with a significantly higher risk RR 1.79 (95% CI 1.34–2.38), while tapering resulted in non-significant increase in flare risk RR 1.5 (95% CI 0.79–3.08). These outcomes were consistent across all subgroups, regardless of whether patients had been in remission for more than 6 months, <6 months, or were in remission at the time of inclusion. Notably, patients with shorter remission durations at inclusion showed an increased flare risk upon withdrawal. However, flare risk remained stable across all subgroups during tapering, irrespective of the remission duration at inclusion. The current meta-analysis extends previous research on the withdrawal or tapering of biological DMARDs in rheumatic diseases. Our findings are consistent with several other analyses that support de-escalation. A SLR published in 2019 by Navarro-Compán et al. (3), which primarily synthesized observational studies and included only one RCT with biologic therapy, also found that tapering strategies may maintain remission or low disease activity.
Webers et al. (4) performed a SLR that informed the 2022 ASAS-EULAR recommendations for axSpA, focusing on flare risks associated with bDMARD withdrawal. The findings from this study found that withdrawal leads to higher flare risks. Tapering was not evaluated. Qualitative studies have shown a broad range of attitudes toward tapering among both patients and physicians (18, 19). The present study contributes to evidence-based decision-making for both physicians and patients, which is important given the lack of biomarkers of remission or flare. Similar results was also observed more recently by Balay-Dustrude et al. (20), the latter performing also a qualitative synthesis of two RCTs and six observational studies.
In contrast, other meta-analyses have reported different results, though methodological differences in study populations and interventions likely explain these discrepancies. An earlier meta-analysis by Uhrenholdt et al. (5), which included randomized controlled trials (RCTs) up to 2019 with participants having rheumatoid arthritis (RA) or spondyloarthritis (SpA), revealed that the risk of flare was increased for both tapering and withdrawing treatment compared to a standard regimen, with relative risks (RR) of 1.45 and 2.28, respectively. A sensitivity analysis showed that the risk of flare was higher in patients with RA than in those with SpA. It is possible that the differences observed compared to our study may be due to patients with SpA being more likely to maintain remission than those with RA, a finding that is also supported by more recent studies published after 2019.
Additionally, a meta-analysis of RCTs conducted by Lawson et al. (21) included some studies that were excluded from our analysis due to differences in inclusion criteria, such as population with active disease state or differing outcome measures. This study concluded that dose reduction had higher risk of relapse and disease flare.
Finally, the meta-analysis by Min et al. (22) concluded that dose reduction could increase flare risk, but their analysis combined data from distinct withdrawal and dose-reduction strategies across various SpA subtypes, which may have led to conclusions that are difficult to interpret when assessing tapering alone.
A significant finding of our analysis is the robustness of the outcomes, which remained consistent despite heterogeneity in both patient populations and disease activity definitions used across the source trials. Our review included trials enrolling patients across the axSpA spectrum, including radiographic, non-radiographic, and mixed cohorts. Although a formal subgroup analysis was precluded by heterogeneity, the data of the individual studies revealed no clear differences in de-escalation success, a finding that supports the current view of axSpA as a single disease entity (23). Similarly, outcomes were comparable whether remission was defined by various ASDAS thresholds or by the established BASDAI <4 standard. That our central findings—the significant risk of flare upon withdrawal and the relative safety of tapering—held true across these varied methodologies suggests the observed effect is a genuine clinical phenomenon, not an artifact of a specific patient subgroup or measurement tool.
Further strengths of our meta-analysis include the deliberate decision to include only randomized controlled trials (RCTs). By focusing exclusively on this highest level of evidence, we aimed to minimize the potential for selection bias inherent in observational data. Furthermore, by segregating the analysis based on previous remission duration, we took a clinical approach that other meta-analyses may have missed due to limited available data. Across most domains, our analysis demonstrated moderate to high certainty, suggesting our conclusions are fairly reliable and robust.
Despite these strengths, some limitations should be considered. Some of the included studies exhibited an unclear risk of bias, primarily stemming from inadequate information regarding the randomization sequence. Furthermore, certain outcomes were associated with low certainty, primarily due to limited sample sizes in some studies; to mitigate this limitation, efforts were made for rigorous analysis and cautious interpretation of the findings.
This established consistency provides a solid foundation for future research, which can now address more nuanced questions. Future studies should investigate the most efficacious treatment tapering strategy, identify prognostic factors for disease remission, and focus on populations with longer sustained remission to enhance understanding and improve management of long-term outcomes. With the emergence of refined assessment tools, such as the new data-driven BASDAI cut-offs proposed by Georgiadis et al. (24), the field is also positioned to investigate whether the depth of remission can predict de-escalation success. Finally, several highly anticipated trials—including SPACING (NCT01610947), SPARTACUS (NCT04435288), BIOTAPE (NCT05115903), and TAPER (NCT04429776)—are expected to provide definitive data on which patients are the optimal candidates for these refined de-escalation strategies. In conclusion, this meta-analysis demonstrates that withdrawal significantly compromises the ability to sustain remission, whereas tapering appears to be a potentially safer alternative, regardless of the duration of prior remission.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
HP: Data curation, Formal analysis, Funding acquisition, Investigation, Project administration, Writing – original draft, Writing – review & editing. PD: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing, Writing – original draft. MP: Formal analysis, Methodology, Validation, Writing – review & editing, Writing – original draft. JP: Investigation, Resources, Visualization, Writing – review & editing. MG-R: Formal analysis, Resources, Writing – review & editing. MM: Supervision, Writing – review & editing. JC: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Spanish Society of Rheumatology (Sociedad Española de Reumatología) as part of the development process of the update of Espoguía -Guía de Práctica Clínica sobre el manejo de los pacientes con Espondiloartritis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ward MM, Deodhar A, Gensler LS, Dubreuil M, Yu D, Khan MA, et al. 2019 update of the American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and treatment network recommendations for the treatment of ankylosing spondylitis and non-radiographic axial spondyloarthritis. Arthritis Care Res. (2019) 71:1285–99. doi: 10.1002/acr.24025
2. Ramiro S, Nikiphorou E, Sepriano A, Ortolan A, Webers C, Baraliakos X, et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update. Ann Rheum Dis. (2023) 82:19–34. doi: 10.1136/ard-2023-223937
3. Navarro-Compán V, Plasencia-Rodríguez C, De Miguel E, Balsa A, Martín-Mola E, Seoane-Mato D, et al. Anti-TNF discontinuation and tapering strategies in patients with axial spondyloarthritis: a systematic literature review. Rheumatology. (2016) 55:1188–94. doi: 10.1093/rheumatology/kew033
4. Webers C, Nikiphorou E, Boonen A, Ramiro S. Tapering or discontinuation of biological disease-modifying antirheumatic drugs in axial spondyloarthritis: a review of the literature and discussion on current practice. Joint Bone Spine. (2023) 90:105482. doi: 10.1016/j.jbspin.2022.105482
5. Uhrenholt L, Christensen R, Dinesen WKH, Liboriussen CH, Andersen SS, Dreyer L, et al. Risk of flare after tapering or withdrawal of biologic/targeted synthetic disease-modifying anti-rheumatic drugs in patients with rheumatoid arthritis or axial spondyloarthritis: a systematic review and meta-analysis. Rheumatology. (2022) 61:3107–22. doi: 10.1093/rheumatology/keab902
6. Díaz del Campo Fontecha P, Brito-García N, Guerra-Rodríguez M, Herrera-López S, Díaz-González F. Management, development and methodology of the clinical practice guidelines and recommendations of the Spanish society of rheumatology. Reumatol Clín (English Edition). (2024) 20:392–7. doi: 10.1016/j.reumae.2024.07.010
7. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
8. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
9. Brozek JL, Canelo-Aybar C, Akl EA, Bowen JM, Bucher J, Chiu WA, et al. GRADE Guidelines 30: the GRADE approach to assessing the certainty of modeled evidence-an overview in the context of health decision-making. J Clin Epidemiol. (2021) 129:138–50. doi: 10.1016/j.jclinepi.2020.09.018
10. Cantini F, Niccoli L, Cassara E, Kaloudi O, Nannini C. Duration of remission after halving of the etanercept dose in patients with ankylosing spondylitis: a randomized, prospective, long-term, follow-up study. Biologics. (2013) 7:1–6. doi: 10.2147/BTT.S31474
11. Gratacós J, Pontes C, Juanola X, Sanz J, Torres F, Avendaño C, et al. Non-inferiority of dose reduction versus standard dosing of TNF-inhibitors in axial spondyloarthritis. Arthritis Res Ther. (2019) 21:11. doi: 10.1186/s13075-018-1772-z
12. Weinstein CLJ, Sliwinska-Stanczyk P, Hála T, Stanislav M, Tzontcheva A, Yao R, et al. Efficacy and safety of golimumab in patients with non-radiographic axial spondyloarthritis: a withdrawal and retreatment study (GO-BACK). Rheumatology. (2023) 62:3601–9. doi: 10.1093/rheumatology/kead112
13. Ruwaard J, L' Ami MJ, Kneepkens EL, Krieckaert C, Nurmohamed MT, Hooijberg F, et al. Interval prolongation of etanercept in rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis: a randomized controlled trial. Scand J Rheumatol. (2023) 52:129–36. doi: 10.1080/03009742.2022.2028364
14. Michielsens CA, Den Broeder N, Van Den Hoogen FH, Mahler EA, Teerenstra S, Van Der Heijde D, et al. Treat-to-target dose reduction and withdrawal strategy of TNF inhibitors in psoriatic arthritis and axial spondyloarthritis: a randomised controlled non-inferiority trial. Ann Rheum Dis. (2022) 81:1392–9. doi: 10.1136/annrheumdis-2022-222260
15. Landewé R, Sieper J, Mease P, Inman RD, Lambert RG, Deodhar A, et al. Efficacy and safety of continuing versus withdrawing adalimumab therapy in maintaining remission in patients with non-radiographic axial spondyloarthritis (ABILITY-3): a multicentre, randomised, double-blind study. Lancet. (2018) 392:134–44. doi: 10.1016/S0140-6736(18)31362-X
16. Landewé RB, Van Der Heijde D, Dougados M, Baraliakos X, Van Den Bosch FE, Gaffney K, et al. Maintenance of clinical remission in early axial spondyloarthritis following certolizumab pegol dose reduction. Ann Rheum Dis. (2020) 79:920–8. doi: 10.1136/annrheumdis-2019-216839
17. Landewé RB, Gensler LS, Poddubnyy D, Rahman P, Hojnik M, Li X, et al. Continuing versus withdrawing ixekizumab treatment in patients with axial spondyloarthritis who achieved remission: efficacy and safety results from a placebo-controlled, randomised withdrawal study (COAST-Y). Ann Rheum Dis. (2021) 80:1022–30. doi: 10.1136/annrheumdis-2020-219717
18. Edwards CJ, Fautrel B, Schulze-Koops H, Huizinga TWJ, Kruger K. Dosing down with biologic therapies: a systematic review and clinicians' perspective. Rheumatology. (2017) 56:1847–56. doi: 10.1093/rheumatology/kew464
19. Hazlewood GS, Loyola-Sanchez A, Bykerk V, Hull PM, Marshall D, Pham T, et al. Patient and rheumatologist perspectives on tapering DMARDs in rheumatoid arthritis: a qualitative study. Rheumatology. (2022) 61:606–16. doi: 10.1093/rheumatology/keab330
20. Balay-Dustrude E, Fennell J, Baszis K, Goh YI, Horton DB, Lee T, et al. Approaches and outcomes of adalimumab discontinuation in patients with well-controlled inflammatory arthritis: a systematic search and review. Pediatr Rheumatol Online J. (2024) 22:112. doi: 10.1186/s12969-024-01046-3
21. Lawson DO, Eraso M, Mbuagbaw L, Joanes M, Aves T, Leenus A, et al. Tumor necrosis factor inhibitor dose reduction for axial spondyloarthritis: a systematic review and meta-analysis of randomized controlled trials. Arthritis Care Res. (2021) 73:861–72. doi: 10.1002/acr.24184
22. Min HK, Kim HR, Lee SH, Nam B, Shin JH, Kim TH. Risk of disease flare in spondyloarthritis patients after tapering tumor necrosis factor inhibitors: a meta-analysis and literature review. Int Immunopharmacol. (2024) 134:112167. doi: 10.1016/j.intimp.2024.112167
23. Poddubnyy D. Challenges in non-radiographic axial spondyloarthritis. Joint Bone Spine. (2023) 90:105468. doi: 10.1016/j.jbspin.2022.105468
Keywords: tapering, discontinuation, withdrawal, suspension, antirheumatic agents, disease modifying antirheumatic drugs, spondyloarthritis
Citation: Park HS, Díaz del Campo P, Plana MN, Polo y La Borda J, Guerra-Rodríguez M, Moreno M and Cañete JD (2025) Efficacy of withdrawal or tapering of bDMARDs vs. standard regimen in axial spondyloarthritis patients: systematic review and meta-analysis informing the update of the Spanish Society of Rheumatology Guideline. Front. Med. 12:1621313. doi: 10.3389/fmed.2025.1621313
Received: 30 April 2025; Accepted: 11 August 2025;
Published: 10 September 2025.
Edited by:
Faisal A. Nawaz, Emirates Health Services (EHS), United Arab EmiratesReviewed by:
Roberta Ramonda, University of Padua, ItalyEric Toussirot, INSERM CIC1431 Centre d'Investigation Clinique Besançon, France
Copyright © 2025 Park, Díaz del Campo, Plana, Polo y La Borda, Guerra-Rodríguez, Moreno and Cañete. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Nieves Plana, cGxhbmFmbkBnbWFpbC5jb20=; Petra Díaz del Campo, UGV0cmEuZGlhekBzZXIuZXM=
†These authors have contributed equally to this work
‡ORCID: Hye Sang Park orcid.org/0000-0002-4972-9527
Petra Díaz del Campo orcid.org/0000-0003-0235-7233
Maria Nieves Plana orcid.org/0000-0003-0921-7954