 Hirofumi Hirakawa
Hirofumi Hirakawa Takeshi Terao
Takeshi Terao Kentaro Kohno
Kentaro Kohno Akari Sakai
Akari Sakai Nobuko Kawano
Nobuko Kawano- 1Department of Neuropsychiatry, Faculty of Medicine, Oita University, Yufu, Japan
- 2Oita Occupational Health Management Center, Nishinihon Occupational Health Center, Oita, Japan
- 3Department of Psychology, Faculty of Welfare and Health Sciences, Oita University, Oita, Japan
Background: Professional choice is an important aspect of one’s life and is associated with biopsychosocial and economic factors. Medical and co-medical professional choices may involve a noble intention to contribute to patients. Thus, this study aimed to investigate the association between medical and co-medical professional choices and affective temperament, parental bonding, and intelligence.
Methods: The dataset included 130 individuals (19 with medical or co-medical professional choices and 111 without). Data on participants’ demographics, intelligence levels, affective temperament, and parental bonding were collected and subsequently compared among the two groups using an unpaired t-test and χ2 test. Thereafter, binomial logistic regression analysis using the likelihood ratio and forward method was performed, with medical or co-medical professional choice as the dependent variable and potentially significant variables (p < 0.2) in the above t-test or χ2 test as independent variables.
Results: Only higher paternal care was significantly associated with medical and co-medical professional choices.
Conclusion: Our study findings suggest that paternal care is associated with medical or co-medical professional choices. Further prospective studies are required to determine causal relationships and investigate other factors related to such choices, given the non-association of all other variables in the study.
1 Introduction
The notion that temperament plays a role in professional choice goes back to Aristotle, who wondered why poets, philosophers, and politicians all had a melancholic temperament (1). In 1931, Kretschmer wrote a fascinating monograph on individuals of genius, largely German poets and musicians, and based on the existing biographical data, declared them cyclothymic (1). Since World War II, the most impressive findings have been the association of cyclothymic temperament with artistic creativity and that of hyperthymic temperament with leadership (2). With respect to creativity, students enrolled in arts schools (i.e., those preparing for creative artistic professions) exhibited higher scores on cyclothymic, hyperthymic, and irritable temperaments compared with university students in disciplines that are expected to lead to professions primarily requiring the application of the learned rules (e.g., law, engineering, and foreign language studies) (3). Moreover, tango dancers, representing one of the most characteristic Argentine folk dance–musical repertoires, showed higher scores on hyperthymic and irritable temperaments compared with the general population (4). Although the relationship between temperament and career choice has been noted since ancient times, modern research has revealed that this relationship has been studied more concretely, particularly among health professionals.
Professional choice is an important aspect of one’s life and is associated with both biopsychosocial and economic factors. Especially, medical or co-medical professionals may have noble intentions to contribute to patients. Akiskal et al. (1) showed that physicians had nearly twice as much depressive temperament as controls (21% vs. 12%) and nearly twice as many obsessive-compulsive traits (32% vs. 17%). Figueira et al. (5) showed that psychology and nursing students predominantly presented with depressive and anxious temperaments, whereas medical students had the lowest scores of hyperthymic and cyclothymic temperaments. Jaracz et al. also confirmed that nurses had a higher anxious temperament than firefighters, athletes, paramedics, and civil servants (6, 7). On the other hand, emergency medicine professionals exhibited elevated levels of hyperthymic temperament compared with other temperaments. This finding suggests that hyperthymic temperament may represent a desirable trait in emergency medicine professionals who must work under high levels of risk and perform complex medical tasks under extreme conditions (8).
However, to the best of our knowledge, no study has investigated the association between parental bonding and medical or co-medical professional choices. It seems plausible that higher levels of maternal and paternal care can foster the noble intention to contribute to patients with the aspiration to be a medical or co-medical professional. Finally, a certain level of intelligence is also required to achieve medical or co-medical education. Therefore, we hypothesized that medical or co-medical professionals would have higher depressive and anxious temperaments, higher maternal and paternal bonding, and higher intelligence than the others. This study aimed to test this hypothesis.
2 Subjects and methods
2.1 Subjects
We used data from a previous study (9) on psychotherapy in apparently healthy participants. In the previous study, the inclusion criterion was individuals aged ≥ 20 years who provided written informed consent. Participants were recruited via electronic bulletin boards, physical bulletin boards, and flyers. Individuals with serious psychiatric disorders, as determined by the mini-international neuropsychiatric interview (M.I.N.I.), were excluded. The Institutional Review Board of Oita University Faculty of Medicine approved the trial (number B16-023). All participants provided written informed consent. Although the previous study (9) had 137 subjects, our previous opt-out study (10) excluded seven subjects and created the dataset of 130 subjects because of missing data. In this opt-out study, we used the dataset of 130 subjects, which included 108 women and 22 men, with a mean age of 49.3 years (SD = 12.1). This opt-out study was approved by the ethics committee of the Oita University Faculty of Medicine on 12 June 2023 (approval number 2536).
2.2 Medical professionals
We defined medical or co-medical staff as doctors, nurses, public health nurses, psychotherapists, occupational therapists, social workers, and medical students, as they work for patients and families; medical students were included as they aspire to become doctors. We called them the medical group and the others the non-medical group.
2.3 Measures
2.3.1 Affective temperament
We used the Temperament Evaluation of Memphis, Pisa, Paris, and San Diego-auto questionnaire (TEMPS-A) to assess participants’ affective temperament. It is a 110-item true–false questionnaire that assesses five temperament dimensions: depressive, cyclothymic, hyperthymic, irritable, and anxious (11). TEMPS-A has been translated into Japanese, and its reliability and validity have been sufficiently established (12).
2.3.2 Parental bonding style
The Parental Bonding Instrument (PBI) is a retrospective self-assessment measure of parental rearing attitudes experienced in childhood (13). The PBI consists of 25 items divided over two subscales of “care (12 items)” and “overprotection (13 items).” A high score for “care” indicates more appropriate rearing (less rejection and indifference), whereas a high score for “overprotection” indicates inappropriate overprotection (less encouragement of self-reliance). Each item is assessed on a four-point Likert scale. The PBI has been translated into Japanese with well-established reliability and validity (14, 15).
2.3.3 Intelligence
The National Adult Reading Test (NART) (16) is a widely used measure of premorbid IQ in English-speaking patients with dementia. The Japanese version of the NART (JART) uses 50 irregular Japanese words, all of which are kanji (ideographic script) compound words, which have a well-established reliability and validity (17). The JART has also been used in studies assessing IQ (particularly Verbal IQ) in healthy adults without a medical history of psychiatric disorders (18, 19).
2.4 Data analysis
First, demographic data, affective temperament, parental bonding, and intelligence scores were compared among the two groups (medical and non-medical groups) using an unpaired t-test or χ2 test. Second, binomial logistic regression analysis using the likelihood ratio and forward method was performed, with medical professional choice as the dependent variable and potentially significant variables (p < 0.2) in the above t-test or χ2 test as independent variables. We used IBM SPSS Statistics Ver 27.
3 Results
Among the 130 participants, 19 were from the medical group, including seven nurses, three social workers, two psychotherapists, two occupational therapists, two public health nurses, two medical students, and one medical doctor. The remaining 111 individuals were from the non-medical group, including 27 office workers, 11 housewives, 10 part-time workers, 8 public servants, etc. The medical group included 18 women and only 1 man, whereas the non-medical group included 90 women and 21 men. However, gender was not significantly different (χ2 = 2.15, p = 0.142). The medical group also had significantly higher paternal care scores than the non-medical group (Table 1).
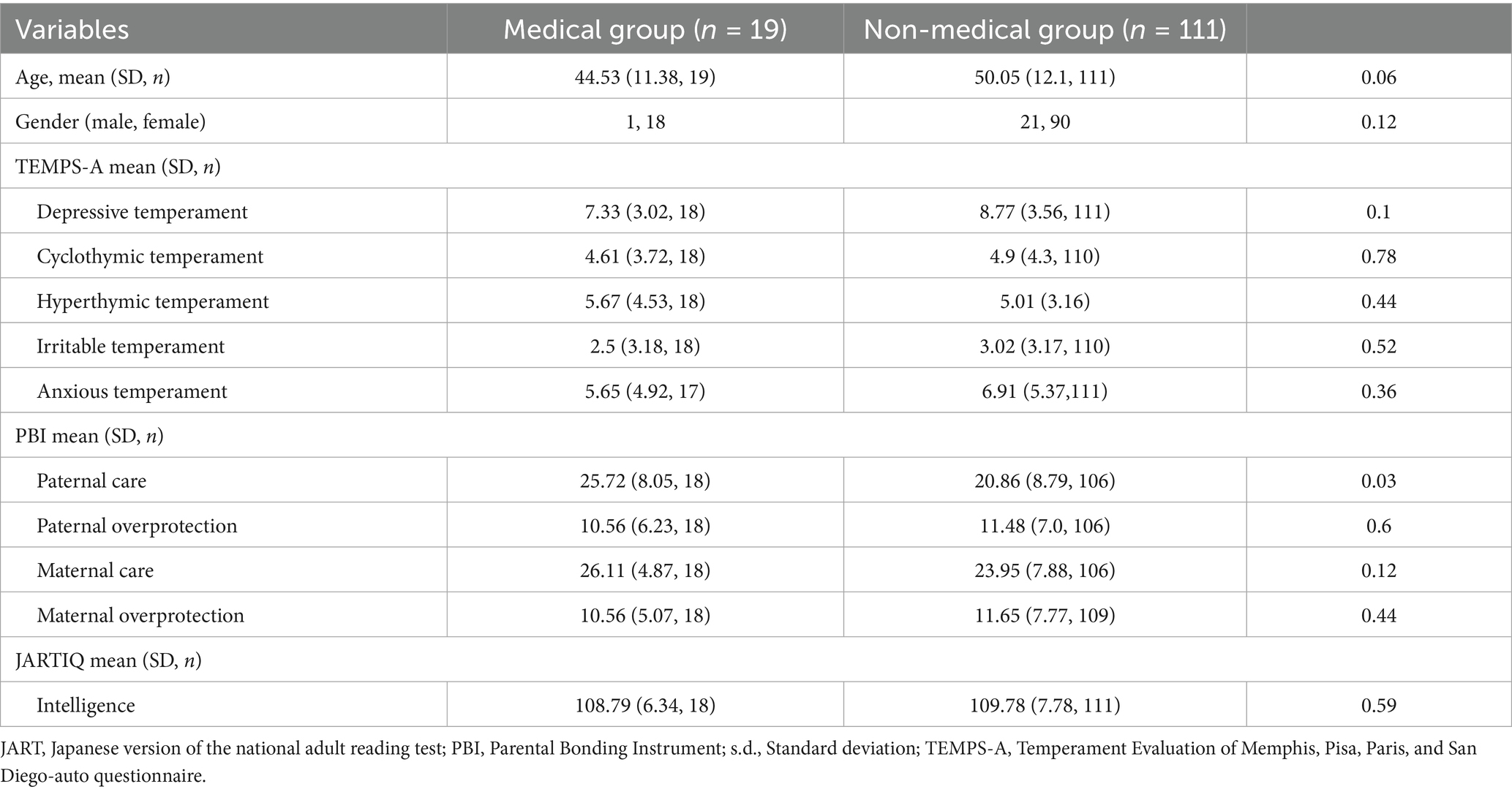
Table 1. Comparison of age, gender, affective temperament, parental bonding, and intelligence between medical and non-medical groups.
As previously mentioned, binomial logistic regression analysis using the likelihood ratio and forward method was performed, with medical professional choice as the dependent variable and potentially significant variables, which showed p < 0.2 in the t-test or χ2 test as independent variables they were gender, age, depressive temperament, paternal care, and maternal care. As a result, only paternal care remained significant in the final model (Table 2).
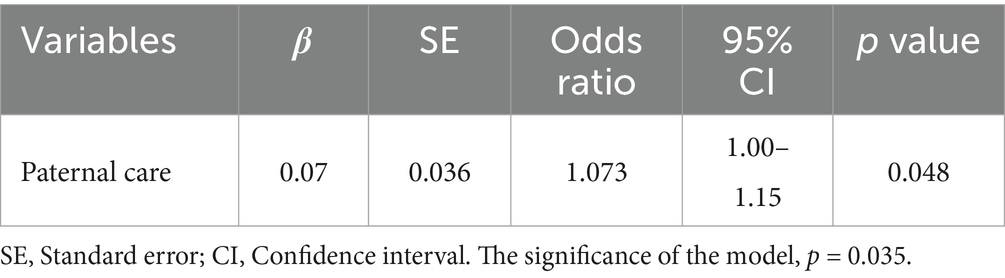
Table 2. Binomial logistic regression analysis for medical professional choice as dependent variable.
4 Discussion
This study aimed to investigate whether medical or co-medical professional choices are associated with individuals’ affective temperament, parental bonding, and intelligence. Only paternal care was significantly associated with medical and co-medical professional choice, and this did not change after binomial logistic regression analysis.
Based on the previous studies (1, 5–7), we hypothesized that medical or co-medical professionals may have higher depressive and anxious temperaments, higher maternal and paternal bonding, and higher intelligence than the others, but this was mostly rejected. However, our hypothesis was only partially supported by the association between paternal bonding and medical or co-medical professional choice. To the best of our knowledge, this is the first study to demonstrate such an association. Interestingly, another study showed that maternal but not paternal care was significantly associated with educational level and marital status (20). It is uncertain why paternal care was significantly associated with medical or co-medical professional choice. Although highly speculative, paternal care may foster the noble intention of physically and/or psychologically contributing to weak individuals, such as patients. However, the reason for the non-association between medical or co-medical professional choice and depressive or anxious temperaments or intelligence may possibly be the heterogeneity of medical professionals in this study.
This study has some limitations that must be considered. First, this was a cross-sectional, retrospective study, and causal relationships could not be determined. Second, the sample size was relatively small, which precluded to establish a definite conclusion. Third, the JARTIQ does not measure total intelligence. Finally, this study focused only on psychological aspects. Biological, social, economic, and cultural aspects should also be considered while studying these associations. In particular, parental occupation may also have influenced individuals’ professional choices (e.g., parents’ occupations may reflect their financial situation, and children may become familiar with or aspire to their parents’ professions). However, this study did not take parental occupation into account.
5 Conclusion
The present findings suggest that paternal care may be associated with medical or co-medical professional choices. Further prospective studies are required to determine causal relationships and investigate other factors related to such choices, given the non-association of all other variables in the study.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: because we are making other papers using the data. Requests to access these datasets should be directed to TT, dGVyYW9Ab2l0YS11LmFjLmpw.
Ethics statement
The studies involving humans were approved by the ethics committee of the Oita University Faculty of Medicine. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because this is an opt-out study.
Author contributions
HH: Conceptualization, Formal analysis, Validation, Writing – original draft, Writing – review & editing. TT: Conceptualization, Formal analysis, Supervision, Writing – original draft, Writing – review & editing. KK: Writing – original draft, Writing – review & editing. AS: Data curation, Writing – original draft, Writing – review & editing. NK: Data curation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Akiskal, KK, Savino, M, and Akiskal, HS. Temperament profiles in physicians, lawyers, managers, industrialists, architects, journalists, and artists: a study in psychiatric outpatients. J Affect Disord. (2005) 85:201–6. doi: 10.1016/j.jad.2004.08.003
2. Rovai, L, Maremmani, AGI, Leonardi, A, Bacciardi, S, Rugani, F, Dell’Osso, L, et al. TEMPS-A[P] temperament profile related to professional choice. Differences between applicants to become a cadet officer in the Italian air force or navy. J Affect Disord. (2013) 145:106–10. doi: 10.1016/j.jad.2012.07.021
3. Vellante, M, Zucca, G, Preti, A, Sisti, D, Rocchi, MBL, Akiskal, KK, et al. Creativity and affective temperaments in non-clinical professional artists: an empirical psychometric investigation. J Affect Disord. (2011) 135:28–36. doi: 10.1016/j.jad.2011.06.062
4. Lolich, M, Vázquez, GH, Zapata, S, Akiskal, KK, and Akiskal, HS. Affective temperaments in tango dancers. J Affect Disord. (2015) 173:27–30. doi: 10.1016/j.jad.2014.10.018
5. Figueira, ML, Caeiro, L, Ferro, A, Cordeiro, R, Duarte, PM, Akiskal, HS, et al. Temperament in Portuguese university students as measured by TEMPS-A: implications for professional choice. J Affect Disord. (2009) 123:30–5. doi: 10.1016/j.jad.2009.10.005
6. Jaracz, M, Rosiak, I, Bertrand-Bucińska, A, Jaskulski, M, Nieżurawska, J, and Borkowska, A. Affective temperament, job stress and professional burnout in nurses and civil servants. PLoS One. (2017) 12:e0176698. doi: 10.1371/journal.pone.0176698
7. Jaracz, M, Bialczyk, K, Ochocinski, A, Szwed, M, Jaracz, K, and Borkowska, A. Contributions of affective temperament traits to professional choice: evidence from the study of firefighters, musicians, athletes, bank managers, nurses and paramedics. Psychol Res Behav Manag. (2021) 14:827–34. doi: 10.2147/PRBM.S313191
8. Jaracz, M, Paciorek, P, Buciński, A, and Borkowska, A. Affective temperament and executive functions in emergency medicine professionals. J Affect Disord. (2014) 168:192–6. doi: 10.1016/j.jad.2014.07.004
9. Sakai, A, Terao, T, Kawano, N, Akase, M, Hatano, K, Shirahama, M, et al. Existential and mindfulness-based intervention to increase self-compassion in apparently healthy subjects (the EXMIND study): a randomized controlled trial. Front Psych. (2019) 10:538. doi: 10.3389/fpsyt.2019.00538
10. Eto, M, Terao, T, Satoh, M, Kawano, N, Sakai, A, Akase, M, et al. The association of self-compassion with depressive temperament and reading habit. Acad Ment Health Well-Being. (2024) 1–4. doi: 10.20935/MHealthWellB6176
11. Akiskal, HS, Akiskal, KK, Haykal, RF, Manning, JS, and Connor, PD. TEMPS-A: Progress towards validation of a self-rated clinical version of the temperament evaluation of the Memphis, Pisa, Paris, and San Diego autoquestionnaire. J Affect Disord. (2005) 85:3–16. doi: 10.1016/j.jad.2004.12.001
12. Matsumoto, S, Akiyama, T, Tsuda, H, Miyake, Y, Kawamura, Y, Noda, T, et al. Reliability and validity of TEMPS-A in a Japanese non-clinical population: application to unipolar and bipolar depressives. J Affect Disord. (2005) 85:85–92. doi: 10.1016/j.jad.2003.10.001
13. Parker, G, Tupling, H, and Brown, LB. A parental bonding instrument. Br J Med Psychol. (1979) 52:1–10. doi: 10.1111/j.2044-8341.1979.tb02487.x
14. Kitamura, T, and Suzuki, T. A validation study of the parental bonding instrument in a Japanese population. Jpn J Psychiatry Neurol. (1993) 47:29–36. doi: 10.1111/j.1440-1819.1993.tb02026.x
15. Ogawa, M. A study of the reliability and validity of the Japanese version of the PBI (parental bonding instrument). Jpn J Psychiatr Treat. (1991) 6:1193–201.
17. Matsuoka, K, Uno, M, Kasai, K, Koyama, K, and Kim, Y. Estimation of premorbid IQ in individuals with Alzheimer’s disease using Japanese ideographic script (kanji) compound words: Japanese version of National Adult Reading Test. Psychiatry Clin Neurosci Japanese version. (2006) 60:332–9. doi: 10.1111/j.1440-1819.2006.01510.x
18. Hidese, S, Ota, M, Matsuo, J, Ishida, I, Yokota, Y, Hattori, K, et al. Association of body mass index and its classifications with gray matter volume in individuals with a wide range of body mass index group: a whole-brain magnetic resonance imaging study. Front Hum Neurosci. (2022) 16:926804. doi: 10.3389/fnhum.2022.926804
19. Nakayama, R, Uetsuki, M, Maruya, K, and Takemura, H. Evaluating correlations between reading ability and psychophysical measurements of dynamic visual information processing in Japanese adults. Sci Rep. (2024) 14:29546. doi: 10.1038/s41598-024-80172-0
Keywords: professional choice, medical doctors, nurses, psychologists, paternal care
Citation: Hirakawa H, Terao T, Kohno K, Sakai A and Kawano N (2025) Comparison of affective temperament, parental bonding, and intelligence between individuals who chose medical and non-medical professions. Front. Med. 12:1647460. doi: 10.3389/fmed.2025.1647460
Edited by:
Hikaru Hori, Fukuoka University, JapanReviewed by:
Hiroko Sugawara, Fukuoka University, JapanMerve Yazar Renkyorgancı, KTO Karatay University, Türkiye
Copyright © 2025 Hirakawa, Terao, Kohno, Sakai and Kawano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Takeshi Terao, dGVyYW9Ab2l0YS11LmFjLmpw