 Francisco José Parrilla-Gómez1,2*
Francisco José Parrilla-Gómez1,2* Antonio Castelli3
Antonio Castelli3 Riccardo Colombo3
Riccardo Colombo3 Antero do Vale-Fernandes4,5,6,7
Antero do Vale-Fernandes4,5,6,7 Federico Nalesso8David Pestaña-Lagunas9,10
Federico Nalesso8David Pestaña-Lagunas9,10 Fernando Suarez-Sipmann11,12Pierpaolo Terragni13
Fernando Suarez-Sipmann11,12Pierpaolo Terragni13- 1Critical Care Department, Hospital del Mar, Barcelona, Spain
- 2Department of Medicine and Life Sciences (MELIS), Hospital del Mar Research, Institute (IMIM), Critical Illness Research Group (GREPAC), Universidad Pompeu Fabra (UPF), Barcelona, Spain
- 3Anesthesia and Intensive Care Unit, ASST Fatebenefratelli-Sacco, Luigi Sacco Hospital, Milan, Italy
- 4Serviço de Medicina Intensiva, Unidade Local de Saúde Almada - Seixal (ULSAS), Hospital Garcia de Orta, Almada, Portugal
- 5RISE-Health, Faculdade de Ciências da Saúde, Universidade da Beira Interior, Covilhã, Portugal
- 6Faculdade de Ciências da Saúde, Universidade Fernando Pessoa, Porto, Portugal
- 7Faculdade de Medicina da Universidade de Lisboa, Lisbon, Portugal
- 8Nephrology, Dialysis and Transplantation Unit, Department of Medicine, University of Padova, Padova, Italy
- 9Department of Anaesthesia and Intensive Care, Hospital Universitario Ramon y Cajal, IRYCIS, Madrid, Spain
- 10Department of Health Science, School of Medicine, Universidad de Alcalá, Alcalá de Henares, Madrid, Spain
- 11Department of Critical Care, University Hospital La Princesa, ISS La Princesa, Autonomous University of Madrid, Madrid, Spain
- 12CIBERES, Carlos III Health Institute, Madrid, Spain
- 13Department of Medicine, Surgery and Pharmacy, University of Sassari, Sassari, Italy
Technological advancements have facilitated the application of extracorporeal-carbon-dioxide removal (ECCO2R) in managing acute respiratory-failure (ARF), including both hypoxemic and hypercapnic forms. A non-systematic literature review (PubMed, Medline, Embase, Google Scholar; January 2000–November 2024) identified randomized-controlled-trials (RCTs) and real-world evidence (RWE) on ECCO2R, alone or combined with continuous renal replacement therapy (CRRT). A multidisciplinary panel of intensivists, anesthesiologists, and nephrologists from Italy, Portugal, and Spain assessed clinical integration of ECCO2R. Key considerations included identifying ideal candidates, such as patients with acute respiratory distress syndrome (ARDS), chronic obstructive pulmonary disease (COPD), asthma exacerbations, alongside initiation timing and discontinuation criteria. For ARDS, recommended initiation thresholds included driving pressure ≥15 cm H2O, plateau pressure ≥28 cm H2O, pH < 7.28, and respiratory-rate >25 breaths/min. In COPD or asthma exacerbations at risk of non-invasive ventilation (NIV) failure, triggers included pH ≤ 7.25, RR ≥ 30 breaths/min, Intrinsic-PEEP ≥ 5 cm H2O, signs of respiratory fatigue, paradoxical abdominal motion, and severe distress. Absolute contraindications were uncontrolled bleeding, refractory hemodynamic instability, or lack of vascular access. Relative contraindications included moderate coagulopathy and limited access. The panel concluded ECCO2R may support selected adults with ARDS or obstructive lung disease, though further RCTs and high-quality prospective studies are needed to guide practice.
Introduction
Acute respiratory failure (ARF), marked by impaired gas exchange, requires precise interventions (1). Mechanical ventilation (MV), while essential for supporting gas exchange, risks ventilator-induced lung injury (VILI) due to uneven lung distension, leading to systemic inflammation and organ failure (2–4). Extracorporeal CO2 removal (ECCO2R) has emerged as a promising strategy to manage inefficient CO2 elimination, facilitating lung-protective ventilation (LPV) with lower tidal volumes (VT) and airway pressures (5–13).
ECCO2R has diverse applications depending on clinical scenarios. In acute respiratory distress syndrome (ARDS), it reduces the intensity of invasive MV. In obstructive airway pathology, including chronic obstructive pulmonary disease (COPD) and asthma, as well as in lung transplantation (LTX) candidates, it decreases ventilatory workload, facilitates spontaneous breathing, and can prevent intubation (5–13). ECCO2R is particularly effective in managing hypercapnic acidosis, mitigating risks in ARDS and COPD patients and allowing an adjustment of the ventilatory parameters that minimizes lung injury. Compared to extracorporeal membrane oxygenation (ECMO), ECCO2R offers partial gas exchange support depending overall on CO2 decrease with almost no effect on oxygenation, with a much simpler implementation, making it suitable for intubated and non-intubated patients (14–20).
Studies have demonstrated that ECCO2R facilitated enhanced gas exchange and minimized VILI by allowing ultra-protective ventilation with reduced tidal volumes and airway pressures (21). During the COVID-19 crisis, Cambria et al. underscored its utility in stepping down ventilatory support, thereby improving the clinical management of critically ill patients (22). Consequently, ECCO2R has emerged as a pivotal adjunct in managing life-threatening respiratory failure, either as a bridge to recovery or as supportive intervention during pulmonary rehabilitation.
With ongoing technological progress, ECCO2R's clinical indications are broadening within intensive care settings due to its capacity to deliver vital respiratory support. However, updated guidelines from the European Society of Intensive Care Medicine caution against its routine use for non-COVID-19-related acute respiratory distress syndrome (ARDS), unless within the context of randomized controlled trials (23). This position stems from a lack of evidence showing mortality reduction. Similarly, for COVID-19-associated ARDS, the strong recommendation against routine use persists, though it is supported by moderate-certainty evidence due to indirect study designs (23).
In addition, the COVID-19 pandemic highlighted ECCO2R's value, especially when combined with continuous renal replacement therapy (CRRT) (24, 25). Pasero et al. (24) in an observational study, suggested that low-flow ECCO2R with CRRT significantly reduced driving pressures and intensive care unit (ICU) stay in moderate ARDS patients with acute kidney injury (AKI), though it did not impact 28-day mortality. Additionally, ECCO2R benefits patients with air leaks, improving hypercapnia and lung recovery (26).
Despite its advantages, ECCO2R can affect pulmonary and hemodynamic function and is associated with adverse events (AEs) involving the patient, the circuit, or mechanical failures (7, 10–13, 18, 27–30). Major AEs are frequently associated with veno-arterial cannulation, with risk factors influenced by the selection of vascular access and cannula characteristics (12–14, 18, 28–30). However, as the use of veno-arterial cannulation declines, single central venous cannulation with a double-lumen catheter has become the preferred approach. Documented complications of ECCO2R included membrane clotting, hemolysis, thrombocytopenia, significant bleeding, pump malfunction, catheter displacement, and infectious complications (12–14, 18, 28–30).
Additionally, anticoagulation with heparin, which was essential for maintaining ECCO2R performance, contributed to hemorrhagic complications (12–14, 18). However, the relatively high incidence of bleeding complications may be attributable to anticoagulation therapy and the elevated blood trauma associated with centrifugal pumps, which were originally engineered for high-flow systems (such as ECMO), particularly when operating with low blood volume processing (31). These findings underscore the need for advancements in blood pump technology to enhance safety and effectiveness at low flow rates.
This document aims to enhance the understanding and application of ECCO2R support, either alone or in combination with CRRT, in clinical practice, particularly for ARDS and acute COPD/asthma exacerbations. It synthesizes the latest evidence, establishes criteria for patient selection and intervention timing (encompassing initiation and weaning), and provides practical insights into ECCO2R's limitations and implementation, bridging gaps where formal guidelines may be lacking (32, 33).
Methods
On September 16, 2024, a meeting was convened to evaluate the feasibility of conducting a comprehensive review on the use of ECCO2R across various clinical scenarios. The expert panel was composed of specialists in intensive care medicine, anesthesiology, and nephrology, chosen for their expertise and experience in mechanical ventilation and ECCO2R. The panel collaboratively selected and endorsed a set of key topics addressing the indications, strengths, and limitations of ECCO2R support in clinical practice.
Two separate face-to-face meetings were held to facilitate panel member interaction in their native languages: the first on October 3, 2024 for the Iberian Group, and the second on October 30, 2024 for the Italian Group. During these meetings, the panel engaged in extensive discussions on various practical aspects of ECCO2R use in routine clinical practice. Key topics included identifying the patient population most likely to benefit from ECCO2R support, determining the appropriate timing for initiating treatment (with a focus on clinical and gasometrical parameters), and defining the criteria for discontinuing ECCO2R support. These considerations were addressed both for ECCO2R used alone and in combination with CRRT.
Based on the information gathered during the two face-to-face meetings, an initial draft was prepared and subsequently reviewed during a virtual meeting held on November 27, 2024. After incorporating all the suggested revisions agreed upon by the panel members, the final document was reviewed and approved by the two study coordinators (PPT and FJPG). It was then circulated to all panel members for their final review and subsequent approval.
Search strategy and eligibility criteria
A comprehensive but not systematic search of PubMed, Medline, Embase, and Google Scholar databases was conducted to identify randomized controlled trials (RCTs) and real-world evidence (RWE) studies evaluating the use of ECCO2R, either alone or in combination with CRRT, in various clinical conditions from January 2000 to March 31, 2025.
The search strategy employed Medical Subject Headings (MeSH) terms, including “Extracorporeal CO2 removal” OR “ECCO2R.” Additionally, a search was conducted using the MeSH terms “Extracorporeal CO2 removal” OR “ECCO2R” AND “Renal replacement therapy.”
To ensure a comprehensive and unbiased review of the literature on ECCO2R, a structured, multi-step search and selection strategy was employed. The initial search was supplemented by a manual screening of the reference lists from all included studies to identify additional relevant publications not retrieved through database queries. Furthermore, a free-text search of titles and abstracts was conducted using a range of clinically pertinent keywords, including “acute respiratory distress syndrome,” “chronic obstructive pulmonary disease,” “obstructive lung diseases,” “acute exacerbated chronic obstructive pulmonary disease,” “asthma,” and “respiratory dialysis.”
The selection process was performed in two stages. First, titles and abstracts were initially screened to exclude clearly irrelevant articles. Second, the full texts of potentially eligible studies were reviewed to confirm their inclusion based on predefined criteria. Studies were eligible if they evaluated the use of ECCO2R, either as a standalone support or in combination with CRRT, across various clinical scenarios. Exclusion criteria encompassed animal and in vitro studies, editorials, articles lacking clinical data applicable to human care, case reports, and case series with fewer than 10 participants. However, select case reports involving fewer than 10 patients were included when deemed to have significant relevance to the early development and clinical implementation of ECCO2R support. Additionally, only articles published in English, French, Portuguese, Italian, or Spanish were considered.
To minimize selection bias, two independent reviewers (FJPG and PT) conducted the study screening and selection. Discrepancies were resolved through discussion and consensus. This rigorous methodology was designed to provide a thorough and objective synthesis of current evidence regarding ECCO2R technologies and their clinical applications.
Results
Description of panel members characteristics
The panel members were expert clinicians who routinely administer ECCO2R support or support the renal specialist evaluation in patients who undergo CO2 removal treatment at various clinical centers across Italy, Portugal, and Spain.
The panel members had experience using different ECCO2R devices currently available in the European market at the time. All the panel members were familiar with different ECCO2R devices, with a median (interquartile range) experience of 4 (3.0–5.5) years.
Panel members centers protocols
Most panel members centers implement protocols for ECCO2R support (62.5%; 5/8), with variations influenced by regional preferences. Participant centers are guided by pathophysiological principles for lung protection and follow expert panel recommendations outlined in consensus guidelines (21).
The pathophysiological approach incorporated prone positioning for patients with an arterial partial pressure of oxygen to inspired oxygen fraction (PaO2/FiO2) ratio below 150 mmHg while excluding cases of refractory hypoxemia. CRRT initiation focuses on life-threatening acid-base disturbances, prescribing ≥25–30 mL/kg/h dialysate, without pre-dilution and achieving an effective blood flow (Qb) of 450 mL/min.
Clinical applications of ECCO2R
Application of ECCO2R in ARDS
The primary respiratory parameters that, according to the expert panel, guide the decision to initiate or discontinue ECCO2R support in patients with ARDS, along with their respective cut-off values, are presented in Table 1 and Figure 1A.
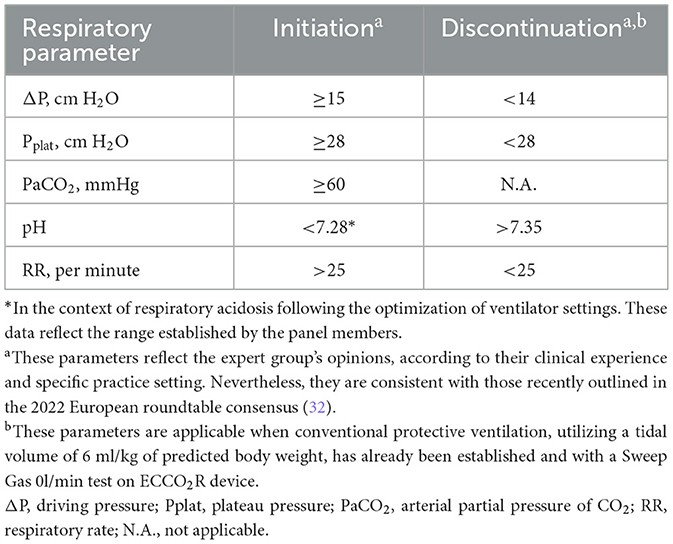
Table 1. Criteria for initiating and discontinuing extracorporeal CO2 removal (ECCO2R) based on respiratory parameter thresholds in patients with moderate acute respiratory distress syndrome (ARDS).
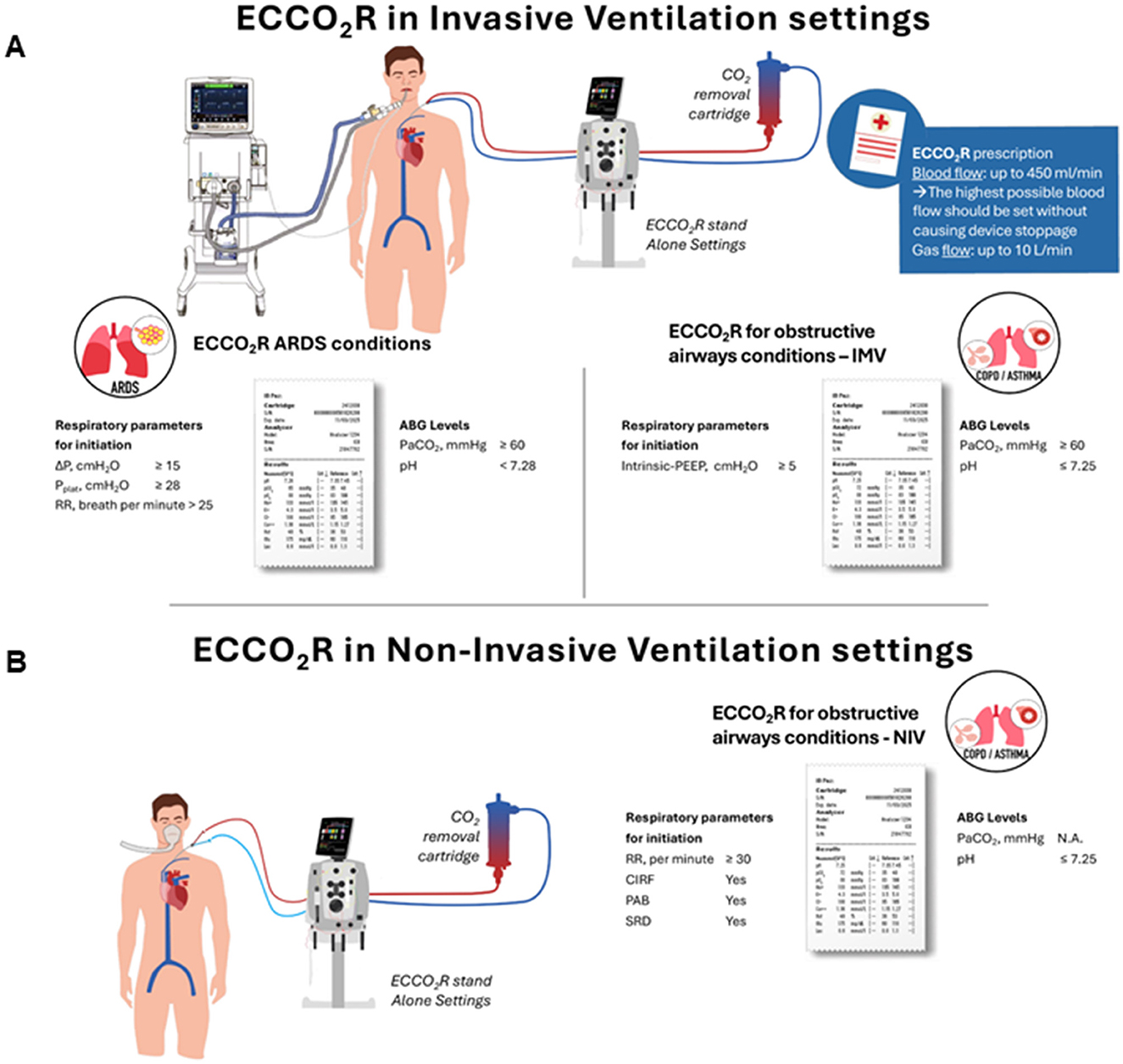
Figure 1. Applications and initiation parameters of extracorporeal CO2 removal in acute respiratory distress syndrome and obstructive airway diseases in invasive (A) and non-invasive (B) mechanical ventilation. Schematic representation of the clinical applications of ECCO2R in ARDS and obstructive airway diseases, under both invasive mechanical ventilation (IMV) and non-invasive ventilation (NIV) settings. The diagram details the respiratory parameters and arterial blood gas (ABG) thresholds for treatment initiation, along with the basic initiation parameters of ECCO2R. ABG, arterial blood gas; ARDS, acute respiratory distress syndrome; ECCO2R, extracorporeal CO2 removal; IMV, invasive mechanical ventilation; NIV, non-invasive ventilation; RR, respiratory rate; CIRF, clinical indicators of respiratory failure; PAB, paradoxical abdominal breathing; SRD, severity of respiratory dyspnea.
Initiation and discontinuation of ECCO2R in supporting protective ventilation for ARDS patients:
• Initiation of the support:
○ Expert panel opinion:
▪ Driving pressure (ΔP), Plateau pressure (Pplat), Arterial partial pressure of CO2 (PaCO2), pH, and respiratory rate (RR) have been identified as key respiratory parameters to evaluate when determining the initiation of ECCO2R in sedated patients with moderate ARDS receiving MV.
• Patients with severe ARDS should be considered only during the early stages of the condition, provided they respond to treatment and show no signs of refractory hypoxemia.
• Discontinuation of the support:
○ Expert panel opinion:
▪ The key respiratory parameters for determining the discontinuation of ECCO2R in patients with moderate ARDS undergoing MV are ΔP, Pplat, PaCO2, pH, and RR.
The rational basis for utilizing ECCO2R in ARDS
ARDS is a life-threatening condition characterized by impaired gas exchange, resulting in oxygenation and/or CO2 elimination failure. With a mortality rate from 27 to 45%, ARDS usually requires invasive MV (9, 34–37). However, some patients continue to experience refractory hypoxia and/or hypercapnia despite optimal ventilation settings. The use of ECCO2R in ARDS is based on insights into VILI (4, 38, 39). The ARDSNet trial showed that reducing VT to 6 ml/kg decreased mortality (40) although 30% of patients still experienced pulmonary hyperinflation, indicating potential benefits from further VT reduction (2, 41). ΔP is the parameter most closely associated with mortality in patients with ARDS (42). It is closely related to respiratory system compliance (Crs) and depends on the set VT as well as the set PEEP (positive end expiratory pressure). Higher VT leads to higher ΔP, whereas higher PEEP also increases ΔP if it results in overdistension. Reducing ΔP has been shown to decrease pro-inflammatory factors in the BAL of patients with ARDS (2). Therefore, reducing the VT or ΔP in these patients is of particular interest when ΔP values exceed 15 cm H2O (39). However, reducing VT below 6 ml/kg can lead to severe hypercapnia and associated complications, which limits feasibility (43–46). Conversely, a post-hoc analysis of the SUPERNOVA trial found that ECCO2R devices with higher CO2 extraction capacity enabled more consistent reduction of tidal volume to 4 ml/kg in ARDS patients and were associated with fewer adverse events, such as hemolysis and bleeding, compared to lower-capacity systems (47).
ECCO2R has emerged as a promising solution to mitigate hypercapnia while enabling further reductions in VT, ΔP, and respiratory rate in ARDS patients. By facilitating CO2 clearance, ECCO2R supports ultra-low VT ventilation, reducing Pplat, ΔP, and mechanical power, all while maintaining clinically acceptable levels of PaCO2 and pH. This approach offers a viable strategy to mitigate VILI (21, 35, 48–51).
The SUPERNOVA study, a multicenter phase II trial involving 95 patients with moderate ARDS (PaO2/FiO2 100–200 mmHg), demonstrated that ECCO2R could facilitate ultraprotective ventilation (VT 4 ml/kg, Pplat ≤ 25 cm H2O). By 8 and 24 h, 78% and 82% of patients achieved the desired ventilation settings, respectively (27). At day 28, 73% of patients were alive, and 62% were discharged alive. ECCO2R was effective in stabilizing pH levels and reducing PaCO2, but adverse events occurred in 39% of patients, including severe complications like brain hemorrhage and pneumothorax. The study also indicated that patients with higher alveolar dead space fraction (ADF) or lower respiratory system compliance (Crs) benefited most from ECCO2R treatment (27, 52). In the study conducted by Fanelli et al. (10), it was demonstrated that a reduction in ΔP of ~5 cm H2O was achieved when ECCO2R support was applied, without any observed changes in PaCO2 or pH in the arterial blood gas analysis.
More recently, the REST trial, however, found no significant reduction in 90-day mortality with ECCO2R combined with low VT ventilation compared to standard care, emphasizing the need for further investigation to clarify its efficacy in larger populations (11).
However, this study had several limitations: first, the inclusion criteria focused on oxygenation (PaO2/FiO2 < 150 mmHg), which is not the primary aim of ECCO2R. In fact, most patients did not meet ECCO2R criteria (injurious ventilation and severe acidosis). A secondary analysis of the trial showed a reduction in mortality in patients with a high ventilatory ratio, a parameter related to dead space and PaCO2, and thus more suitable candidates for ECCO2R (20). Second, the ECCO2R was delivered with a device using a centrifugal pump, which, unlike a roller pump, significantly decreases hydraulic efficiency when blood flow is below 1 L/min, leading to high shear stress, hemolysis, and platelet destruction (53). Third, the protocol involved a 15.5 Fr catheter and anticoagulation targeting an aPTT of 45–90 s, increasing hemorrhage risk. Finally, most centers lacked experience with the technique (11). A recent study by Monet et al. (54) further underscored the critical role of ECCO2R operational parameters, particularly blood pump speed, in determining the efficacy of the technique. The findings emphasized that, beyond the clinical indication, the precise adjustment of both ventilatory and ECCO2R settings was essential for optimizing therapeutic outcomes.
A meta-analysis encompassing 49 studies, including both observational studies and randomized controlled trials, examined adult ICU patients undergoing ECCO2R (51). The findings demonstrated that in patients with ARDS, ECCO2R led to a reduction in PaCO2 and an increase in arterial pH. Additionally, PaO2/FiO2 significantly improved, while Pplat and respiratory rate (RR) decreased. Notably, the reduction in VT reached statistical significance exclusively in ARDS patients (51).
While cohort studies confirm ECCO2R's ability to promptly reduce PaCO2 and correct acidosis, allowing lower RR, tidal volume, and plateau pressures (51), its predictive validity remains limited since randomized trials have not yet shown a mortality benefit and adverse events remain frequent (11).
In summary, ECCO2R is a promising tool for enhancing protective ventilation in moderate-severe conditions of ARDS patients, but evidence regarding outcomes of these patients remains inconclusive, with ongoing studies needed to better define its role and balance the potential benefits against risks such as acidosis and device-related complications (55).
When protective ventilation with low VT is insufficient to safeguard the lungs, and further reduction in VT would result in an unacceptable rise in CO2, leading to respiratory acidosis from alveolar hypoventilation, ECCO2R must be considered.
Application of ECCO2R in COPD/asthma exacerbations
The primary respiratory parameters that, according to the expert panel, guide the decision to initiate or discontinue ECCO2R support in patients with COPD/Asthma Exacerbations are outlined in the Table 2 and Figure 1A, along with their respective cut-off values.
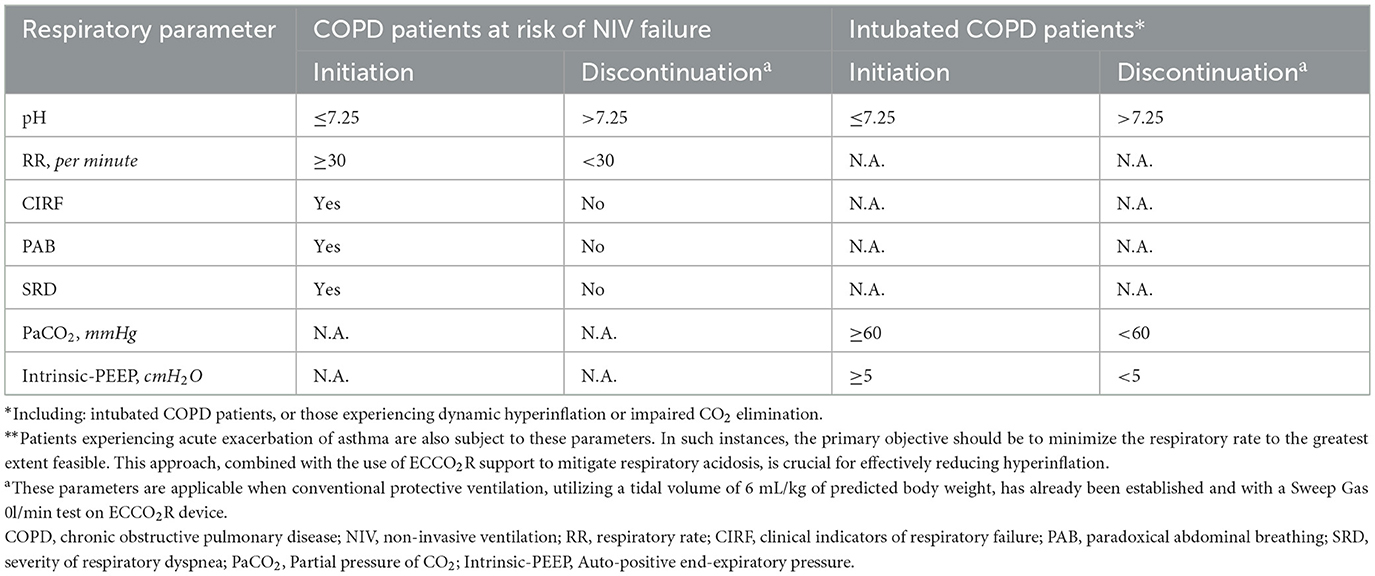
Table 2. Criteria for initiating and discontinuing extracorporeal CO2 removal (ECCO2R) based on respiratory parameter thresholds in patients with obstructive airway pathology, including chronic obstructive pulmonary disease (COPD) and asthma exacerbations**.
Initiation and discontinuation of ECCO2R in supporting protective ventilation for COPD patients:
• Initiation of the support:
○ Expert panel opinion:
▪ In COPD patients at risk of non-invasive ventilation (NIV) failure, key respiratory parameters for assessing the need to initiate ECCO2R include arterial pH, RR, clinical indicators of respiratory failure, paradoxical abdominal breathing, and the severity of respiratory dyspnea (Table 2, Figure 1B).
▪ In intubated COPD patients, or those experiencing dynamic hyperinflation or impaired CO2 elimination, key respiratory parameters for evaluating the need to initiate ECCO2R include arterial pH, PaCO2 and intrinsic-PEEP.
In the context of hyperinflation, distinguishing between static and dynamic hyperinflation is crucial (56). Static hyperinflation arises from excessive PEEP settings, whereas dynamic hyperinflation, prevalent in COPD patients, results from expiratory flow limitation due to bronchial constriction, leading to air trapping (57). Insufficient exhalation time exacerbates this condition, increasing dead space and CO2 levels, perpetuating a vicious cycle (58). Intrinsic-PEEP, while informative, can be misleading as it depends on ventilator settings (57). ECCO2R effectively reduces CO2 levels, contributing to mitigate dynamic hyperinflation in patients on spontaneous ventilation, increasing expiratory time, and thereby supporting MV (56–58).
• Discontinuation of the support:
○ Expert panel opinion:
▪ In COPD patients at risk of NIV failure, key respiratory parameters for assessing the need to discontinue ECCO2R include arterial pH, RR, clinical indicators of respiratory failure, paradoxical abdominal breathing, and the severity of respiratory dyspnea.
▪ In intubated COPD patients, or those experiencing dynamic hyperinflation or impaired CO2 elimination, key respiratory parameters for assessing the need to discontinue ECCO2R include arterial pH, pCO2, and intrinsic-PEEP.
The rational basis for utilizing ECCO2R in obstructive airway pathology and weaning from MV
NIV remains the gold standard for managing acute hypercapnic respiratory failure, particularly in conditions like COPD or Asthma exacerbations (59). However, NIV fails in ~20%−30% of cases, leading to the need for intubation and invasive MV, which is associated with higher mortality rates compared to NIV alone. In these situations, combining ECCO2R support with NIV has emerged as a promising strategy to reduce NIV failure, prevent intubation, and improve patient outcomes (13, 18, 60).
ECCO2R enhances NIV efficacy by lowering respiratory metabolic load, reducing RR, increasing expiratory time and so reducing dynamic hyperinflation, and intrinsic PEEP. By avoiding invasive MV and intubation, ECCO2R could also minimize risks associated with analgo-sedation, such as hemodynamic instability, prolonged weaning, and neurological complications (13, 18). Moreover, ECCO2R reduces the work of breathing, decreasing CO2 production by respiratory muscles and PaCO2, thereby supporting earlier extubation or weaning from MV (14, 61).
In a multicenter and retrospective study, the use of a pumpless extracorporeal assist (PECLA) system in 21 COPD patients who failed NIV resulted in a 90% avoidance of intubation, along with a reduction in PaCO2 levels and improved pH. However, the study did not observe significant differences in mortality or ICU length of stay between the ECCO2R and control groups. The authors concluded that while ECCO2R effectively prevents intubation, its impact on survival remains inconclusive (62).
In addition, Azzi et al. (14) evaluated the effectiveness and safety of ECCO2R in patients with acute exacerbation of COPD experiencing NIV failure. According to the results of this study, ECCO2R improved pH and PaCO2, reduced intubation needs (85% avoided), and shortened ICU (18 vs. 30 days) and hospital length of stay (29 vs. 49 days) compared to the control group. Despite some bleeding complications, major complications were rare. ECCO2R showed lower ventilator-associated pneumonia rates and reduced 90-day mortality (15% vs. 28%), highlighting its potential as a safe and effective alternative to invasive MV (14).
Furthermore, Stommel et al. (51), in their systematic review and meta-analysis, demonstrated that in patients with COPD, ECCO2R significantly reduced PaCO2 and increased arterial pH. While the RR showed a statistically significant decrease, the PaO2/FiO2 ratio and VT did not exhibit significant changes.
Other studies have reported that in COPD patients with NIV failure, ECCO2R reduced intubation rates (26, 60, 63) and hospital mortality (60). However, some discrepancies and concerns have emerged from other studies, highlighting the need for careful patient selection and further research to clarify the safety profile of ECCO2R (64, 65).
A recent European expert consensus established key criteria for initiating ECCO2R support in COPD patients with acute exacerbations of COPD. Indications for ECCO2R initiation included the lack of PaCO2 reduction and failure to decrease RR while on NIV. The treatment goals for these patients were to improve patient comfort, maintain a pH above 7.30–7.35, reduce PaCO2 by 10–20%, decrease RR to 20–25 breaths/min, wean from NIV, decrease bicarbonate (HCO3-), and maintain hemodynamic stability (27, 66).
ECCO2R has also proven beneficial in facilitating weaning from invasive MV in patients with severe respiratory acidosis. In a retrospective analysis, Morelli et al. (63) highlighted the ability of ECCO2R to facilitate weaning from invasive MV, with six out of 12 patients being successfully weaned and surviving to discharge, while five were awake and breathing spontaneously during ECCO2R support.
In a study by Elliot et al. (67), the addition of pumpless ECCO2R allowed for successful weaning from invasive MV in two patients with severe acute asthma by correcting hypercapnia and acidosis. Abrams et al. (68) demonstrated that ECCO2R supported successful extubation in five COPD patients after only 24 h of invasive MV.
Finally, the VENT-AVOID trial, evaluated the impact of ECCO2R on ventilator-free days in patients with COPD exacerbations patients either failing NIV or struggling to wean from invasive MV (69). This study showed that ECCO2R exhibited a trend toward increased ventilator-free days in the invasive MV group, although without statistical significance, although did not improve ventilator-free days in the NIV group. However, this study has several limitations that should be taken into account. These include a small patient sample size, limited experience at the participating centers, unclear indications for ECCO2R use, the application of a centrifugal pump system, the use of a large-bore catheter (15.5 Fr), and the implementation of a permissive anticoagulation protocol (65)”.
In summary, based on the current evidence, ECCO2R represents a valuable intervention for managing acute hypercapnic respiratory failure in obstructive respiratory patterns, especially in COPD exacerbations, by improving the efficacy of NIV, preventing the need for invasive MV, and potentially facilitating earlier extubation in case of invasive MV. While ECCO2R support has demonstrated positive outcomes in reducing NIV failure and aiding weaning from MV, its safety and survival benefits remain uncertain. Observational studies suggest that ECCO2R can reduce complications and enhance patient recovery, but further randomized controlled trials are needed to clarify its role in clinical practice and refine patient selection criteria.
ECCO2R in combination with CRRT
Initiation and discontinuation of ECCO2R in combination with CRRT
• Indications to start CRRT in ECCO2R patients:
○ Potassium (K ≥ 6 mEq/L + electrocardiogram (ECG) anomalies not responsive to medical therapy.
○ pH anomalies (metabolic component in acidosis, pH < 7.10).
○ Hyperhydration not responsive to diuretics (very positive balance with diuresis reduction despite maximum diuretic administration).
○ KDIGO 2012 Guidelines (70):
▪ Start CRRT when life threatening anomalies in fluid, electrolyte and acid-base balance exist.
▪ Consider the broader clinical context, the presence of condition that can be modified with CRRT and the trends of laboratory tests, rather than simple Blood urea nitrogen (BUN) and creatinine thresholds done when making the decision to start CRRT.
• RRT prescription steps during ECCO2R:
○ Dose calculation:
▪ Patient weight x 25–30 ml/kg/h → aim: to reach effluent dose of 20–25 ml/kg/h at least, considering downtime (70).
▪ Keep Prescribed* dose > administered dose → aim: to maintain effluent dose ≥ 20–25 ml/kg/h.
• *Prescribed dose increase depends on downtime that is center-specific and due mainly to the time needed to bag changes and central venous catheter malfunctioning assessments.
○ Dose distribution:
○ Avoid predilution → aim: to avoid the reduction of the real dose administered (due to blood dilution).
▪ Dilution Factor (DF) = Plasma Flow Rate (ml/hr)/[Plasma Flow Rate (ml/hr) + Pre-Filter Replacement Fluid Rate (ml/hr) + Pre Blood-Pump PBP Fluid Rate (ml/hr)].
• Where Plasma Flow Rate (ml/hr) = Blood Flow Rate (ml/min) × 60 (min/hr) × (1 – hematocrit [HCT]).
○ Suggested methods of CRRT
▪ Continuous veno-venous hemodialysis (CVVHD): no convection, no predilution. Effluent dose = dialysate + weight loss (net ultrafiltration).
▪ Continuous veno-venous hemodiafiltration (CVVHDF) just post dilution:
• Pre-dilution, they must consider the dilution factor and correct the previously prescribed depurative dose.
• Effluent dose = dialysate + post dilution + weight loss (net ultrafiltration).
• Suggestion: to set up a post dilution with a filtration fraction (FF) ≤ 20%.
○ Filtration Factor (FF)= total ultrafiltration (UF) rate/plasma flow rate.
○ Considering PBP and predilution 0.
○ Not considering drop in weight in this calculation.
An overview of CRRT prescription steps during ECCO2R is shown in Figure 2.
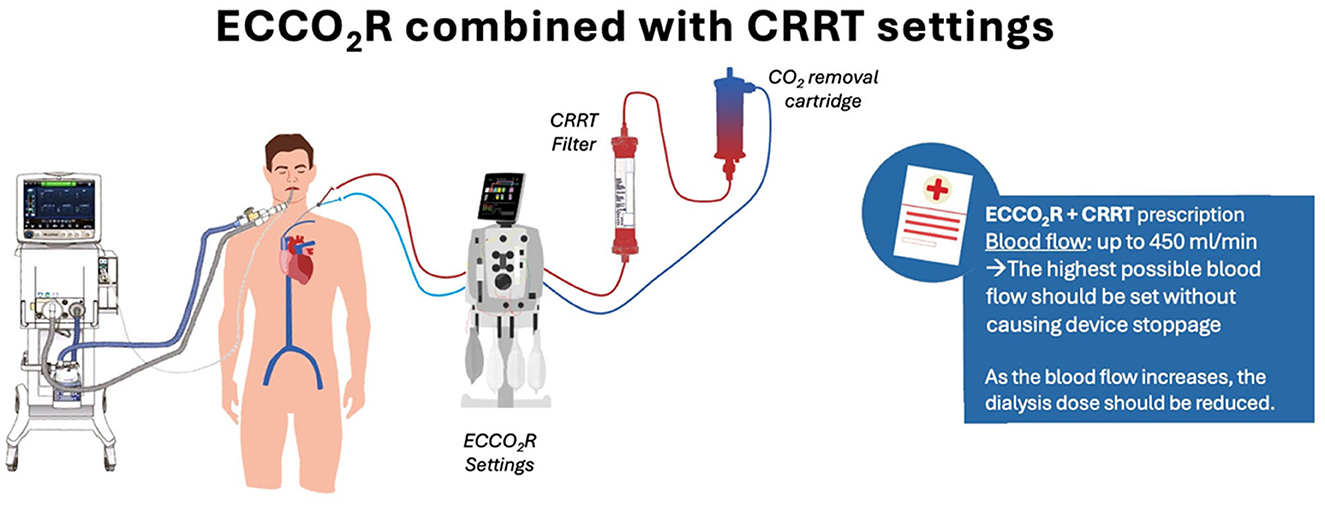
Figure 2. Applications and initiation parameters of extracorporeal CO2 removal in combination with continuous renal replacement therapies. Schematic representation of the clinical applications of ECCO2R in combination with CRRT. The process follows KDIGO 2012 AKI guidelines (See reference 70), emphasizing the importance of clinical context, fluid balance, and laboratory trends over isolated blood urea nitrogen and creatinine thresholds. Key considerations include dose calculation (25–30 mL/kg/h to achieve an effluent dose of ≥20–25 ml/kg/h), dose distribution (diffusive vs. post-dilution convective dose), and the impact of pre-dilution on effective clearance. Clinical insights highlight thresholds for initiating CRRT, the importance of maintaining prescribed vs. administered dose, and minimizing downtime. AKI, acute kidney injury; CRRT, continuous renal replacement therapy; ECCO2R, extracorporeal CO2 removal.
The rational basis for utilizing ECCO2R in in combination with CRRT
Lung-kidney crosstalk refers to the bidirectional physiological and pathological interactions between these organs, crucial for maintaining homeostasis. The lungs regulate pH by managing CO2 levels, while the kidneys maintain acid-base balance through bicarbonate reabsorption and hydrogen ion excretion. Disruptions in one system often exacerbate dysfunction in the other (71, 72).
Pathological conditions, such as pulmonary-renal syndromes, fluid imbalances, and blood gas disturbances (e.g., hypoxemia, hypercapnia), illustrate this interplay. Pulmonary disorders can provoke systemic inflammation, worsening kidney injury, while renal dysfunction can hinder acid-base regulation, causing pulmonary complications (71, 73).
In critically ill patients, such as those with ARDS, lung-kidney interactions become increasingly significant. Pulmonary disorders lead to systemic inflammation, hypoxemia, and hypercapnia, impairing renal perfusion and function through venous congestion and hemodynamic changes (71, 74, 75). Conversely, kidney dysfunction exacerbates pulmonary complications by causing fluid overload, metabolic acidosis, and impaired gas exchange, further increasing respiratory effort (76, 77). MV compounds this interplay by reducing renal blood flow and contributing to oxidative stress and systemic mediator release (78).
ECCO2R can be implemented by integrating a membrane lung into standard RRT platforms, thereby enabling simultaneous extracorporeal respiratory and renal support (79, 80). Incorporating a hollow-fiber gas exchanger into a CRRT platform offers several practical benefits. These include technical simplicity and broader applicability, particularly in non-tertiary care settings, as the system typically does not require additional vascular access beyond that used for CRRT (12, 13).
Notably, the combination of ECCO2R with CRRT had been explored prior to the COVID-19 pandemic (5, 81–83). Nevertheless, this combined approach may be particularly beneficial in patients with COVID-19–associated ARDS, given several pathophysiological and clinical considerations. First, AKI is frequently observed in critically ill patients with COVID-19, with ~20% requiring RRT during their ICU stay (84). Second, mechanical ventilation has been identified as an independent predictor of mortality in individuals with AKI (85, 86). Third, the presence of elevated physiological dead space and reduced respiratory system compliance—hallmarks of COVID-19–related ARDS—may undermine the effectiveness of conventional lung-protective ventilation strategies (87–89).
The integration of ECCO2R with CRRT offers a promising solution for managing simultaneous respiratory and renal failure (79, 81, 90). This combined approach facilitates CO2 clearance and addresses metabolic derangements, improving outcomes in conditions such as hypercapnic acidosis and oliguric AKI (91–93).
This dual support shows potential to enhance clinical outcomes and reduce intensive care burdens, especially in patients with multi-organ dysfunction. While evidence supports its effectiveness, further research is necessary to optimize protocols and validate these findings in larger, more diverse populations (92).
The role of anticoagulation in ECCO2R
Anticoagulation is essential in extracorporeal circuits to mitigate thromboembolic complications, especially in low-flow ECCO2R systems that are particularly prone to circuit clotting. Despite its critical role, no standardized anticoagulation protocol for ECCO2R has been universally established. Preventing system coagulation requires avoiding device stoppage caused by increased pre-pump pressure, which may result from suboptimal catheter positioning, patient hypovolemia, or excessively high blood flow rates. Therefore, blood flow should be maintained at the highest possible level without triggering device interruption.
Systemic anticoagulation with heparin is the most employed approach in both clinical trials and routine practice, using either unfractionated heparin (UFH) or low-molecular-weight heparin. However, this strategy carries risks such as bleeding and heparin-induced thrombocytopenia (94). In the absence of ECCO2R-specific randomized trials, anticoagulation management is largely extrapolated from veno-venous ECMO experience, where UFH remains the preferred anticoagulant. Under standard flow conditions, activated partial thromboplastin time (aPTT) targets typically range from 1.5 to 2.0 times baseline (~50–70 s). In low-flow ECCO2R (< 0.5 L/min), these targets are lowered to ~1.3 to 1.5 times baseline (40–55 s) to balance bleeding and thrombotic risks (95, 96).
Best practices include monitoring aPTT every 4–6 h after initiation or dose changes, daily platelet counts, and routine visual inspection of the circuit for clot formation. These ECMO-derived strategies are reasonable to apply in ECCO2R anticoagulation management (97–101). Table 3 summarizes anticoagulation strategies, aPTT targets, and monitoring recommendations adapted from existing ECMO evidence.
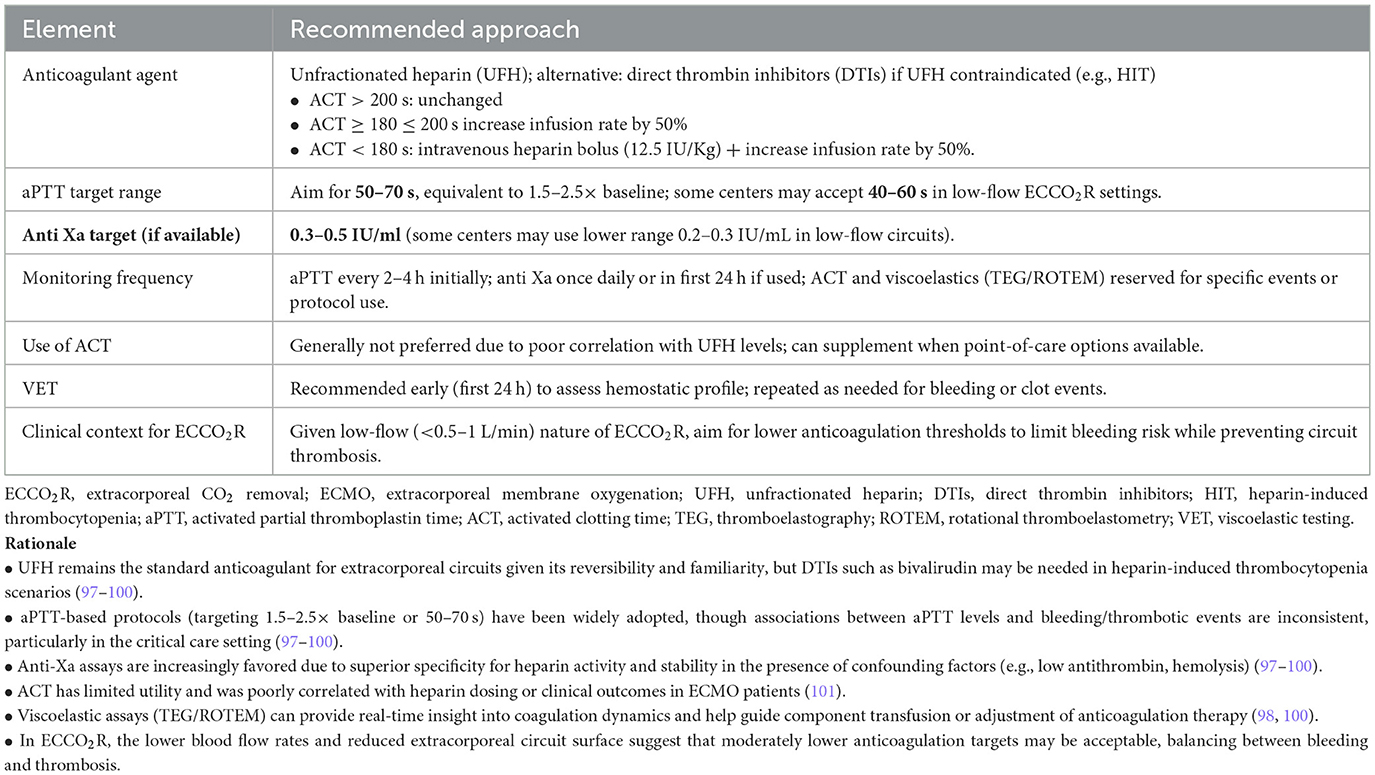
Table 3. Anticoagulation strategies for extracorporeal CO2 removal (ECCO2R): Adapted targets and monitoring guidance based on extracorporeal membrane oxygenation (ECMO) evidence.
Anticoagulation practices for ECCO2R:
• Expert panel opinions:
○ Universal agreement on anticoagulation:
▪ All panel members concur on the necessity of anticoagulation to ensure safe and effective ECCO2R implementation.
▪ Unfractionated heparin is universally used as the anticoagulant of choice in ECCO2R procedures.
▪ It is essential to prioritize appropriate anticoagulation practices to mitigate risks and safeguard patients undergoing ECCO2R support.
Contraindications for ECCO2R: ensuring safe and optimal patient selection
The use of ECCO2R might be limited by several absolute and relative contraindications that must be carefully evaluated to ensure patient safety and treatment efficacy (3, 12, 13, 18, 30, 50, 51, 102). Almost all contraindications for ECCO2R are associated with anticoagulation.
Absolute contraindications include conditions with high risks of complications. They include active bleeding or the inability to establish vascular access is another absolute contraindication (3, 12, 13, 18, 30, 50, 51, 102).
Although hemodynamic instability that is refractory to medical therapy (i.e. severe shock or cardiovascular collapse) might be constituted an absolute contraindication for ECCO2R, as it may exacerbate hemodynamic stress, current evidence supports that if the instability is secondary to respiratory failure (i.e., failing right ventricle due to hyperinflation or severe respiratory acidosis), ECCO2R would probably be the solution. The hemodynamic benefits of ECCO2R in pulmonary hypertension secondary to hypercapnia and right ventricular (RV) dysfunction stem from its ability to modulate the pathophysiological cascade linking hypercapnia, respiratory acidosis, and pulmonary vasoconstriction. Hypercapnia-induced pulmonary vasoconstriction increases RV afterload, potentially exacerbating RV failure, particularly in patients with compromised cardiac reserve (18, 103–105). ECCO2R rapidly lowers PaCO2 and corrects acidosis, attenuating pulmonary vasoconstriction and reducing pulmonary arterial pressures and RV afterload (18, 103). This may improve cardiac output and stabilize hemodynamics when hypercapnia is the primary driver of RV strain. Furthermore, ECCO2R facilitates lung-protective ventilation strategies, potentially mitigating further RV compromise (18, 103).
Relative contraindications involve situations where risks are manageable but require cautious assessment. These include moderate to severe coagulopathy and limited vascular access. The presence of severe coagulopathy, such as an international normalized ratio (INR) > 2.5 or a platelet count < 30,000/μl, or instances of uncontrolled bleeding, poses significant challenges to the use of anticoagulation necessary for ECCO2R. While ECCO2R can technically be implemented without anticoagulation, these parameters necessitate a careful, individualized evaluation of its use. In such cases, it is imperative to operate without heparin, acknowledging the heightened risk of circuit failure due to recurrent clotting. This underscores the need for meticulous clinical judgment and consideration of patient-specific risks and benefits when deciding on ECCO2R in this context.
Other relative contraindications are inability to tolerate anticoagulation, or poor overall prognosis with advanced multi-organ failure, where ECCO2R is unlikely to provide meaningful benefit (3, 12, 13, 18, 30, 50, 51, 102).
The Table 4 outlines the critical absolute and relative contraindications for the use of ECCO2R, providing a comprehensive overview to guide safe and appropriate patient selection.
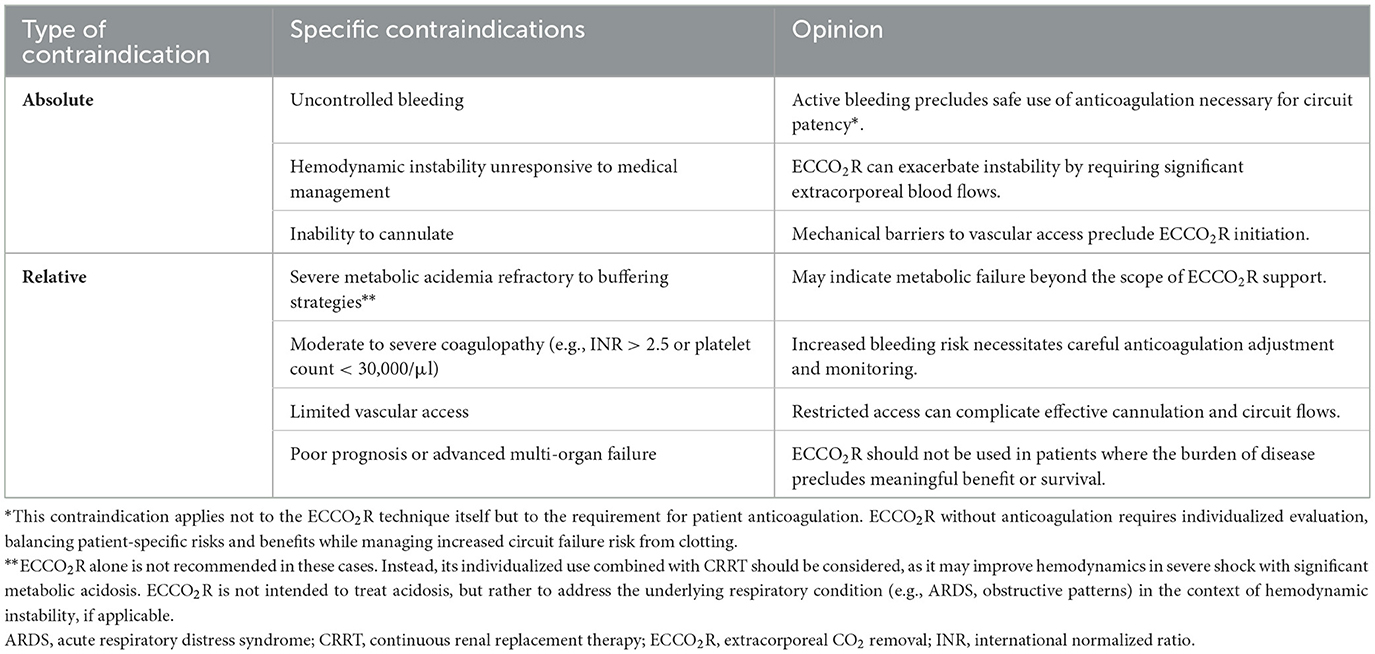
Table 4. Key contraindications for extracorporeal CO2 removal: a comprehensive overview of absolute and relative criteria.
Unmet needs in ECCO2R: key knowledge gaps and critical areas for future research
This paper reviewed the available evidence on the use of ECCO2R, both alone and in combination with CRRT, across various clinical settings, including ARDS and acute exacerbations of COPD and asthma with or without kidney failure. A critical analysis of the data revealed several key observations. First, all studies agreed that ECCO2R, whether standalone or integrated with CRRT, effectively managed hypercapnia and respiratory acidosis in mechanically ventilated patients. This was crucial, as regulating PaCO2 was essential for enabling lung-protective ventilation strategies (3, 12, 13, 18, 30, 50, 51, 102). Moreover, ECCO2R–CRRT allowed for CO2 removal with low blood flow, which improved clinical management and minimized adverse treatment effects (3, 12, 13, 18, 30, 50, 51, 102).
However, significant limitations existed. Notably, there was currently no evidence demonstrating that ECCO2R or ECCO2R–CRRT improved patient outcomes or reduced mortality (3, 12, 13, 18, 30, 50, 51, 94). This finding was common in studies involving critically ill patients, likely due to the complexity of the cases, small sample sizes, and short treatment durations. Furthermore, the studies were highly heterogeneous, involving diverse patient populations, outcomes, devices, and treatment parameters (12, 50, 51). A standardized ventilation protocol with predefined goals was often lacking, reducing the generalizability of the results (12, 50, 51).
Moreover, it would be advisable to emphasize the preferential use of roller pumps, as centrifugal pumps are not recommended for blood flows below 1–2 L/min due to their suboptimal performance at low flow rates (53). In ECCO2R therapies, both the pump type and the rate of blood flow are critical factors influencing the incidence of hemolysis. Evidence suggests that at higher flow rates, magnetically levitated pumps are associated with reduced hemolysis compared to conventional rotary pumps. However, under low-flow conditions (i.e., < 0.5 L/min), magnetically levitated pumps may paradoxically induce greater hemolysis than their rotary counterparts. Given that this review supports the application of low-flow ECCO2R modalities, the preferential use of peristaltic pumps over magnetically levitated systems may be advisable in such settings (53, 106).
In studies involving kidney failure, kidney outcomes and recovery were poorly reported, leaving the effectiveness of renal support provided by ECCO2R–CRRT treatment unclear (3, 12, 13, 18, 30, 50, 51, 102). Several other aspects remained underexplored, such as the optimal circuit configuration (e.g., positioning of the membrane oxygenator and hemofilter), the impact of dialysis buffers on systemic acid-base balance, and the management of anticoagulation (13, 107). These gaps highlighted the need for further research and caution in translating experimental findings into clinical practice.
Study limitations
This review has several limitations that should be acknowledged. First, although a comprehensive search strategy was employed, including manual screening of reference lists and keyword-based free-text searches, there remains the possibility that relevant studies may have been missed, particularly unpublished data or articles indexed in databases not included in our search. Second, the review was limited to articles published in English, French, Portuguese, Italian, or Spanish, which may have introduced language bias and excluded relevant studies published in other languages. Third, case reports and small case series (fewer than 10 participants) were excluded to enhance the quality and generalizability of the findings; however, this may have led to the omission of potentially valuable insights, especially in rare or emerging clinical scenarios. Additionally, heterogeneity in study designs, patient populations, and outcome measures across the included studies may limit the ability to draw definitive conclusions regarding the efficacy and safety of ECCO2R in various clinical settings. Finally, as this is a narrative review and not a systematic review or meta-analysis, the level of evidence synthesis is inherently limited by the absence of quantitative data pooling.
Conclusions
In conclusion, ECCO2R shows potential benefits for optimizing ventilatory strategies in respiratory failure patients. While it offers potentially relevant clinical advantages, its impact on patient prognosis, particularly in critically ill patients with multi-organ failure, requires further clarification.
The combination of ECCO2R and CRRT provides a flexible, cost-effective approach for patients with respiratory failure and kidney dysfunction. ECCO2R can be easily implemented in non-specialized centers using existing CRRT equipment, with appropriate training of the team in the technical handling of the device and the subsequent management of changes in ventilatory parameters that may benefit the patient. However, low-flow techniques may be insufficient for some patients, and ECMO should be considered for the most severely hypoxemic patients who do not respond to increasing PEEP.
Despite its effectiveness in managing hypercapnia and metabolic acidosis, the current ESICM guidelines (23, 32) recommend caution in using ECCO2R for ARDS outside of RCTs, stressing the need for further research.
Although evidence is limited, ECCO2R showed promising results, especially for hypercapnic respiratory failure, but additional well-designed trials are needed to fully assess its clinical impact. Given the challenges of large-scale trials in critically ill populations, ongoing clinical experience and cohort studies are essential for refining treatment protocols and identifying the most appropriate patient groups.
Author contributions
FP-G: Resources, Project administration, Data curation, Writing – original draft, Conceptualization, Funding acquisition, Writing – review & editing, Validation, Supervision, Methodology. AC: Writing – review & editing, Methodology, Writing – original draft, Conceptualization, Visualization, Validation. RC: Writing – review & editing, Methodology, Conceptualization, Investigation, Writing – original draft, Data curation, Validation. AV-F: Validation, Methodology, Writing – review & editing, Data curation, Conceptualization, Investigation, Writing – original draft. FN: Visualization, Validation, Supervision, Writing – review & editing, Writing – original draft, Methodology. DP-L: Software, Visualization, Data curation, Validation, Methodology, Conceptualization, Writing – review & editing, Writing – original draft. FS-S: Validation, Methodology, Data curation, Software, Writing – original draft, Conceptualization, Writing – review & editing. PT: Writing – review & editing, Writing – original draft, Methodology, Supervision, Conceptualization, Investigation, Funding acquisition, Resources, Data curation.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The advisory boards of healthcare professionals, from whose discussion and in-depth work the article “The role of Extracorporeal CO2 removal from pathophysiology to clinical applications with focus on potential combination with RRT: an expert opinion document” resulted, were carried out by the service provider Medical Net S.r.l. with the support of Vantive S.r.l.
Acknowledgments
Medical writing and editorial assistant services have been provided by Ciencia y Deporte S.L. Support for this assistance was funded by Vantive S.r.l. Vantive S.r.l. was not involved in the preparation of the recommendations nor did the company influence in any way the scientific consensus reached. The logistics for the advisory boards of healthcare professionals have been managed by the service provider, Medical Net S.r.l.
Conflict of interest
FP-G has received remuneration for clinical sessions delivered in the context of ECCO2R from Baxter and Cardiolink Group. DP-L has received honoraria as speaker from Braun, Baxter, and Maquet. FS-S has received payments for clinical sessions delivered in the context of ECCO2R from Baxter. He is member of the medical advisory boards of Getinge and Hamilton and have received research grants from Timpel and Air Liquide. PT has received payments for lectures from Baxter and Braun.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Roussos C, Koutsoukou A. Respiratory failure. Eur Respir J Suppl. (2003) 47:3s−14s. doi: 10.1183/09031936.03.00038503
2. Terragni PP, Rosboch G, Tealdi A, Corno E, Menaldo E, Davini O, et al. Tidal hyperinflation during low tidal volume ventilation in acute respiratory distress syndrome. Am J Respir Crit Care Med. (2007) 175:160–6. doi: 10.1164/rccm.200607-915OC
3. Shekar K, Mullany DV, Thomson B, Ziegenfuss M, Platts DG, Fraser JF. Extracorporeal life support devices and strategies for management of acute cardiorespiratory failure in adult patients: a comprehensive review. Crit Care. (2014) 18:219. doi: 10.1186/cc13865
4. Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. (2013) 369:2126–36. doi: 10.1056/NEJMra1208707
5. Terragni PP, Del Sorbo L, Mascia L, Urbino R, Martin EL, Birocco A, et al. Tidal volume lower than 6 ml/kg enhances lung protection: role of extracorporeal carbon dioxide removal. Anesthesiology. (2009) 111:826–35. doi: 10.1097/ALN.0b013e3181b764d2
6. Gramaticopolo S, Chronopoulos A, Piccinni P, Nalesso F, Brendolan A, Zanella M, et al. Extracorporeal CO2 removal—a way to achieve ultraprotective mechanical ventilation and lung support: the missing piece of multiple organ support therapy. Contrib Nephrol. (2010) 165:174–84. doi: 10.1159/000313757
7. Camporota L, Barrett N. Current applications for the use of extracorporeal carbon dioxide removal in critically ill patients. Biomed Res Int. (2016) 2016:9781695. doi: 10.1155/2016/9781695
8. Grasso S, Stripoli T, Mazzone P, Pezzuto M, Lacitignola L, Centonze P, et al. Low respiratory rate plus minimally invasive extracorporeal CO2 removal decreases systemic and pulmonary inflammatory mediators in experimental ARDS. Crit Care Med. (2014) 42:e451–60. doi: 10.1097/CCM.0000000000000312
9. Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of care, and mortality for patients with ARDS in ICUs in 50 countries. JAMA. (2016) 315:788–800. doi: 10.1001/jama.2016.0291
10. Fanelli V, Ranieri MV, Mancebo J, Moerer O, Quintel M, Morley S, et al. Feasibility and safety of low-flow extracorporeal carbon dioxide removal to facilitate ultra-protective ventilation in moderate ARDS. Crit Care. (2016) 20:36. doi: 10.1186/s13054-016-1211-y
11. McNamee JJ, Gillies MA, Barrett NA, Perkins GD, Tunnicliffe W, Young D, et al. REST investigators. Effect of lower tidal volume ventilation facilitated by extracorporeal carbon dioxide removal vs standard care ventilation on 90-day mortality in patients with acute hypoxemic respiratory failure: the REST randomized clinical trial. JAMA. (2021) 326:1013–23. doi: 10.1001/jama.2021.21948
12. Yu TZ, Tatum RT, Saxena A, Ahmad D, Yost CC, Maynes EJ, et al. Utilization and outcomes of ECCO2R: systematic review and meta-analysis of AV and VV approaches. Artif Organs. (2022) 46:763–74. doi: 10.1111/aor.14130
13. Cappadona F, Costa E, Mallia L, Sangregorio F, Nescis L, Zanetti V, et al. ECCO2R: from pathophysiology to clinical applications; focus on combined CRRT. Biomedicines. (2023) 11:142. doi: 10.3390/biomedicines11010142
14. Azzi M, Aboab J, Alviset S, Ushmorova D, Ferreira L, Ioos V, et al. ECCO2R in acute COPD exacerbation unresponsive to non-invasive ventilation. BMJ Open Respir Res. (2021) 8:e001089. doi: 10.1136/bmjresp-2021-001089
15. Ricard JD, Dreyfuss D, Saumon G. Ventilator-induced lung injury. Eur Respir J Suppl. (2003) 42:2s−9s. doi: 10.1183/09031936.03.00420103
16. Fan E Brodie D Slutsky AS ARDS advances in diagnosis and treatment. JAMA. (2018) 319:698–710. doi: 10.1001/jama.2017.21907
17. Tiruvoipati R, Pilcher D, Buscher H, Botha J, Bailey M. Effects of hypercapnia and hypercapnic acidosis on hospital mortality in mechanically ventilated patients. Crit Care Med. (2017) 45:e649–56. doi: 10.1097/CCM.0000000000002332
18. Giraud R, Banfi C, Assouline B, De Charrière A, Cecconi M, Bendjelid K. The use of ECCO2R in acute respiratory failure. Ann Intensive Care. (2021) 11:43. doi: 10.1186/s13613-021-00824-6
19. Inal V, Efe S. ECCO2R in COPD and ARDS with severe hypercapnic respiratory failure: a retrospective case-control study. Turk J Med Sci. (2021) 51:2127–35. doi: 10.3906/sag-2012-151
20. Dianti J, McNamee JJ, Slutsky AS, Fan E, Ferguson ND, McAuley DF, et al. Determinants of effect of ECCO2R in hypoxemic respiratory failure. NEJM Evid. (2023) 2:EVIDoa2200295. doi: 10.1056/EVIDoa2200295
21. Combes A, Schmidt M, Hodgson CL, Fan E, Ferguson ND, Fraser JF, et al. Extracorporeal life support for adults with acute respiratory distress syndrome. Intensive Care Med. (2020) 46:2464–76. doi: 10.1007/s00134-020-06290-1
22. Cambria G, Spelde AE, Olia SE, Biscotti M, Mackay E, Ibrahim M, et al. Extracorporeal carbon dioxide removal to de-escalate venovenous ECMO in severe COVID-19 ARDS. J Cardiothorac Vasc Anesth. (2024) 38:717–23. doi: 10.1053/j.jvca.2023.12.029
23. Grasselli G, Calfee CS, Camporota L, Poole D, Amato MBP, Arabi YM, et al. ESICM guidelines on acute respiratory distress syndrome: definition, phenotyping and respiratory support strategies. Intensive Care Med. (2023) 49:727–59. doi: 10.1007/s00134-023-07050-7
24. Pasero D, Pistidda L, Piredda D, Liperi C, Cossu A, Esposito R, et al. Lung (ECCO2R) and renal (CRRT) support in COVID-19 and non-COVID-19 ARDS: a case-control study. J Anesth Analg Crit Care. (2024) 4:27. doi: 10.1186/s44158-024-00164-4
25. Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, et al. Characteristics and outcomes of 5700 patients hospitalized with COVID-19 in NYC. JAMA. (2020) 323:2052–9. doi: 10.1001/jama.2020.6775
26. Ferrer Gómez C, Gabaldón T, Hernández Laforet J. Ultraprotective ventilation via ECCO2R in air leak patients: is it effective? J Pers Med. (2023) 13:1081. doi: 10.3390/jpm13071081
27. Barbič B, Bianchi C, Madotto F, Sklar MC, Karagiannidis C, Fan E, et al. The failure of ECCO2R may be a failure of technology. Am J Respir Crit Care Med. (2024) 209:884–7. doi: 10.1164/rccm.202309-1628LE
28. Bein T, Weber-Carstens S, Goldmann A, Müller T, Staudinger T, Brederlau J, et al. Lower tidal volume (≈3 ml/kg) + ECCO2R vs 6 ml/kg ventilation in severe ARDS: the Xtravent study. Intensive Care Med. (2013) 39:847–56. doi: 10.1007/s00134-012-2787-6
29. Burki NK, Mani RK, Herth FJF, Schmidt W, Teschler H, Bonin F, et al. A novel ECCO2R system: pilot study in COPD with hypercapnic respiratory failure. Chest. (2013) 143:678–86. doi: 10.1378/chest.12-0228
30. Combes A, Fanelli V, Pham T, Ranieri VM, European Society of Intensive Care Medicine Trials Group and the “Strategy of Ultra-Protective lung ventilation with Extracorporeal CO2 Removal for New-Onset moderate to severe ARDS” (SUPERNOVA) investigators. Feasibility and safety of ECCO2R in ARDS: the SUPERNOVA study. Intensive Care Med. (2019) 45:592–600. doi: 10.1007/s00134-019-05567-4
31. Karagiannidis C, Hesselmann F, Fan E. Physiological and technical considerations of ECCO2R. Crit Care. (2019) 23:75. doi: 10.1186/s13054-019-2367-z
32. Angus DC, Seymour CW, Bibbins-Domingo K. Caring for ARDS patients: 2023 ESICM guidelines summary. JAMA. (2023) 330:368–71. doi: 10.1001/jama.2023.6812
33. Venkatesan P. Updated ESICM guidelines on ARDS. Lancet Respir Med. (2024) 12:16–8. doi: 10.1016/S2213-2600(23)00460-5
34. ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. (2012) 307:2526–33. doi: 10.1001/jama.2012.5669
35. Combes A, Auzinger G, Camporota L, Capellier G, Consales G, Couto AG, et al. Expert perspectives on ECCO2R for acute hypoxemic respiratory failure: consensus of a 2022 European roundtable meeting. Ann Intensive Care. (2024) 14:132. doi: 10.1186/s13613-024-01353-8
36. Fuehner T, Kuehn C, Hadem J, Wiesner O, Gottlieb J, Tudorache I, et al. Extracorporeal membrane oxygenation in awake patients as bridge to lung transplantation. Am J Respir Crit Care Med. (2012) 185:763–8. doi: 10.1164/rccm.201109-1599OC
37. Sloane PJ, Gee MH, Gottlieb JE, Albertine KH, Peters SP, Burns JR, et al. A multicenter registry of patients with ARDS: physiology and outcome. Am Rev Respir Dis. (1992) 146:419–26. doi: 10.1164/ajrccm/146.2.419
38. Dreyfuss D, Saumon G. Ventilator-induced lung injury: lessons from experimental studies. Am J Respir Crit Care Med. (1998) 157:294–323. doi: 10.1164/ajrccm.157.1.9604014
39. Frank JA, Parsons PE, Matthay MA. Pathogenetic significance of biological markers of ventilator-associated lung injury. Chest. (2006) 130:1906–14. doi: 10.1378/chest.130.6.1906
40. Acute Respiratory Distress Syndrome Network, Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes vs traditional volumes in ALI and ARDS. N Engl J Med. (2000) 342:1301–08. doi: 10.1056/NEJM200005043421801
41. Hager DN, Krishnan JA, Hayden DL, Brower RG. Tidal volume reduction in ALI when plateau pressures are not high. Am J Respir Crit Care Med. (2005) 172:1241–5. doi: 10.1164/rccm.200501-048CP
42. Amato MB, Meade MO, Slutsky AS, Brochard L, Costa EL, Schoenfeld DA, et al. Driving pressure and survival in ARDS. N Engl J Med. (2015) 372:747–55. doi: 10.1056/NEJMsa1410639
43. Curley G, Contreras MM, Nichol AD, Higgins BD, Laffey JG. Hypercapnia and acidosis in sepsis: a double-edged sword? Anesthesiology. (2010) 112:462–72. doi: 10.1097/ALN.0b013e3181ca361f
44. Vadász I, Hubmayr RD, Nin N, Sporn PH, Sznajder JI. Hypercapnia: a nonpermissive environment for the lung. Am J Respir Cell Mol Biol. (2012) 46:417–21. doi: 10.1165/rcmb.2011-0395PS
45. Richard JC, Marque S, Gros A, Muller M, Prat G, Beduneau G, et al. Feasibility and safety of ultra-low tidal volume ventilation without extracorporeal support in ARDS. Intensive Care Med. (2019) 45:1590–8. doi: 10.1007/s00134-019-05776-x
46. Feihl F, Eckert P, Brimioulle S, Jacobs O, Schaller MD, Mélot C, et al. Permissive hypercapnia impairs pulmonary gas exchange in ARDS. Am J Respir Crit Care Med. (2000) 162:209–15. doi: 10.1164/ajrccm.162.1.9907119
47. Combes A, Tonetti T, Fanelli V, Pham T, Pesenti A, Mancebo J, et al. Efficacy and safety of lower versus higher CO2 extraction devices to allow ultraprotective ventilation: secondary analysis of the SUPERNOVA study. Thorax. (2019) 74:1179–81. doi: 10.1136/thoraxjnl-2019-213591
48. Bein T, Weber F, Philipp A, Prasser C, Pfeifer M, Schmid FX, et al. A new pumpless extracorporeal interventional lung assist in critical hypoxemia/hypercapnia. Crit Care Med. (2006) 34:1372–7. doi: 10.1097/01.CCM.0000215111.85483.BD
49. Schmidt M, Jaber S, Zogheib E, Godet T, Capellier G, Combes A. ECCO2R with renal replacement platform to enhance lung-protective ventilation in ARDS. Crit Care. (2018) 22:122. doi: 10.1186/s13054-018-2038-5
50. Zhou Z, Li Z, Liu C, Wang F, Zhang L, Fu P. ECCO2R for acute respiratory failure: a systematic review and meta-analysis. Ann Med. (2023) 55:746–59. doi: 10.1080/07853890.2023.2172606
51. Stommel A, Herkner H, Kienbacher CL, Wildner B, Hermann A, Staudinger T. Effects of ECCO2R on gas exchange and ventilator settings: a systematic review. Crit Care. (2024) 28:146. doi: 10.1186/s13054-024-04927-x
52. Goligher EC, Combes A, Brodie D, Ferguson ND, Pesenti AM, Ranieri VM, et al. Determinants of ECCO2R effect in the SUPERNOVA trial: implications for trial design. Intensive Care Med. (2019) 45:1219–30. doi: 10.1007/s00134-019-05708-9
53. Gross-Hardt S, Hesselmann F, Arens J, Steinseifer U, Vercaemst L, Windisch W, et al. Low-flow evaluation of ECMO/ECCO2R rotary pumps and potential hemocompatibility impacts. Crit Care. (2019) 23:348. doi: 10.1186/s13054-019-2622-3
54. Monet C, Renault T, Aarab Y, Pensier J, Prades A, Lakbar I, et al. Ultra-low volume ventilation (≤3 ml/kg) combined with ECCO2R in acute respiratory failure. Crit Care. (2024) 28:433. doi: 10.1186/s13054-024-05168-8
55. Akkanti B, Jagpal S, Darwish R, Saavedra RR, Scott LK, Dinh K, et al. Improvement in respiratory acidosis using ECCO2R with Hemolung system in severe COVID-19. Crit Care Explor. (2021) 3:e0372. doi: 10.1097/CCE.0000000000000372
56. Roesthuis LH, van der Hoeven JG, Guérin C, Doorduin J, Heunks LMA. Three bedside techniques to quantify dynamic pulmonary hyperinflation in mechanically ventilated COPD patients. Ann Intensive Care. (2021) 11:167. doi: 10.1186/s13613-021-00948-9
57. O'Donnell DE, Webb KA, Neder JA. Lung hyperinflation in COPD: applying physiology to clinical practice. COPD Res Pract. (2015) 1:4. doi: 10.1186/s40749-015-0008-8
58. Parrilla FJ, Morán I, Roche-Campo F, Mancebo J. Ventilatory strategies in obstructive lung disease. Semin Respir Crit Care Med. (2014) 35:431–40. doi: 10.1055/s-0034-1382155
59. Dave C, Wharton S, Mukherjee R, Faqihi BM, Stockley RA, Turner AM, et al. Development and relevance of hypercapnia in COPD. Can Respir J. (2021) 2021:6623093. doi: 10.1155/2021/6623093
60. Del Sorbo L, Pisani L, Filippini C, Fanelli V, Fasano L, Terragni P, et al. ECCO2R in hypercapnic patients at risk of NIV failure: a matched cohort study. Crit Care Med. (2015) 43:120–7. doi: 10.1097/CCM.0000000000000607
61. Pisani L, Fasano L, Corcione N, Comellini V, Guerrieri A, Ranieri MV, et al. Effects of ECCO2R on inspiratory effort and respiratory pattern in patients failing weaning. Am J Respir Crit Care Med. (2015) 192:1392–4. doi: 10.1164/rccm.201505-0930LE
62. Kluge S, Braune SA, Engel M, Nierhaus A, Frings D, Ebelt H, et al. Avoiding invasive mechanical ventilation with ECCO2R in NIV failure. Intensive Care Med. (2012) 38:1632–9. doi: 10.1007/s00134-012-2649-2
63. Morelli A, D'Egidio A, Orecchioni A, Alessandri F, Mascia L, Ranieri VM. ECCO2R in hypercapnic patients who fail NIV and refuse intubation: a case series. Intensive Care Med Exp. (2015) 3:A824. doi: 10.1186/2197-425X-3-S1-A824
64. Braune S, Burchardi H, Engel M, Nierhaus A, Ebelt H, Metschke M, et al. ECCO2R to avoid intubation in NIV failure: a cost analysis. BMC Anesthesiol. (2015) 15:160. doi: 10.1186/s12871-015-0139-0
65. Del Sorbo L, Fan E, Nava S, Ranieri VM. ECCO2R in COPD exacerbation: patient and strategy selection. Intensive Care Med. (2016) 42:1830–1. doi: 10.1007/s00134-016-4493-2
66. Combes A, Auzinger G, Capellier G, du CD, Clement I, Consales G, et al. ECCO2R therapy in the ICU: consensus of a European round table meeting. Crit Care. (2020) 24:490. doi: 10.1186/s13054-020-03210-z
67. Elliot SC, Paramasivam K, Oram J, Bodenham AR, Howell SJ, Mallick A. Pumpless ECCO2R for life-threatening asthma. Crit Care Med. (2007) 35:945–8. doi: 10.1097/01.CCM.0000257462.04514.15
68. Abrams DC, Brenner K, Burkart KM, Agerstrand CL, Thomashow BM, Bacchetta M, et al. Pilot study of ECCO2R to facilitate extubation and ambulation in COPD exacerbations. Ann Am Thorac Soc. (2013) 10:307–14. doi: 10.1513/AnnalsATS.201301-021OC
69. Duggal A, Conrad SA, Brochard L, Brodie D, Hill NS. ECCO2R to avoid invasive ventilation in COPD exacerbations: the VENT-AVOID trial. Am J Respir Crit Care Med. (2024) 209:529–42. doi: 10.1164/rccm.202403-0618LE
70. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. (2012) 120:c179–84. doi: 10.1159/000339789
71. Husain-Syed F, Slutsky AS, Ronco C. Lung–kidney cross-talk in the critically ill patient. Am J Respir Crit Care Med. (2016) 194:402–14. doi: 10.1164/rccm.201602-0420CP
72. Mendes RdS, Silva PL, Robba C, Battaglini D, Lopes-Pacheco M, Caruso-Neves C, et al. Advancements in understanding the mechanisms of lung–kidney crosstalk. Intensive Care Med Exp. (2024) 12:81. doi: 10.1186/s40635-024-00672-1
73. Sharkey RA, Mulloy EM, O'Neill SJ. Acute effects of oxygen and carbon dioxide on renal vascular resistance in COPD exacerbation. Chest. (1999) 115:1588–92. doi: 10.1378/chest.115.6.1588
74. van den Akker JP, Egal M, Groeneveld AB. Invasive ventilation as a risk factor for acute kidney injury: systematic review and meta-analysis. Crit Care. (2013) 17:R98. doi: 10.1186/cc12743
75. Murray PT. The kidney in respiratory failure and mechanical ventilation. Contrib Nephrol. (2010) 165:159–65. doi: 10.1159/000313755
76. Ronco C, Bellomo R, Kellum JA, Ricci Z. Critical Care Nephrology. Amsterdam: Elsevier Health Sciences (2019).
77. Alge J, Dolan K, Angelo J, Thadani S, Virk M, Akcan AA. Two to tango: kidney–lung interaction in AKI and ARDS. Front Pediatr. (2021) 9:744110. doi: 10.3389/fped.2021.744110
78. Kuiper JW, Groeneveld AB, Slutsky AS, Plötz FB. Mechanical ventilation and acute renal failure. Crit Care Med. (2005) 33:1408–15. doi: 10.1097/01.CCM.0000165808.30416.EF
79. Fanelli V, Cantaluppi V, Alessandri F, Costamagna A, Cappello P, Brazzi L, et al. Extracorporeal CO2 removal may improve renal function in patients with ARDS and AKI: an open-label study. Am J Respir Crit Care Med. (2018) 198:687–90. doi: 10.1164/rccm.201712-2575LE
80. Ronco C, Bagshaw SM, Bellomo R, Clark WR, Husain-Syed F, Kellum JA, et al. Extracorporeal blood purification and organ support in critically ill patients during the COVID-19 pandemic: expert review and recommendation. Blood Purif. (2021) 50:17–27. doi: 10.1159/000508125
81. Forster C, Schriewer J, John S, Eckardt K, Willam C. Low-flow CO2 removal integrated into a renal replacement circuit can reduce acidosis and decrease vasopressor requirements. Crit Care. (2013) 17:R154. doi: 10.1186/cc12833
82. Quintard JM, Barbot O, Thevenot F, de Matteis O, Benayoun L, Leibinger F. Partial extracorporeal carbon dioxide removal using a standard continuous renal replacement therapy device: a preliminary study. ASAIO J. (2014) 60:564–69. doi: 10.1097/MAT.0000000000000114
83. Allardet-Servent J, Castanier M, Signouret T, Soundaravelou R, Lepidi A, Seghboyan JM. Safety and efficacy of combined extracorporeal CO2 removal and renal replacement therapy in patients with acute respiratory distress syndrome and acute kidney injury: the pulmonary and renal support in acute respiratory distress syndrome study. Crit Care Med. (2015) 43:2570–81. doi: 10.1097/CCM.0000000000001296
84. Ronco C, Reis T, Husain-Syed F. Management of acute kidney injury in patients with COVID-19. Lancet Respir Med. (2020) 8:738–42. doi: 10.1016/S2213-2600(20)30229-0
85. Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. (2005) 294:813–8. doi: 10.1001/jama.294.7.813
86. McNicholas BA, Rezoagli E, Pham T, Madotto F, Guiard E, Fanelli V, et al. Impact of early acute kidney injury on management and outcome in patients with ARDS: secondary analysis of a multicenter observational study. Crit Care Med. (2019) 47:1216–25. doi: 10.1097/CCM.0000000000003832
87. Grasselli G, Tonetti T, Protti A, Langer T, Girardis M, Bellani G, et al. Pathophysiology of COVID-19-associated acute respiratory distress syndrome: a multicentre prospective observational study. Lancet Respir Med. (2020) 8:1201–8. doi: 10.1016/S2213-2600(20)30370-2
88. Nuckton TJ, Alonso JA, Kallet RH, Daniel BM, Pittet JF, Eisner MD, et al. Pulmonary dead-space fraction as a risk factor for death in acute respiratory distress syndrome. N Engl J Med. (2002) 346:1281–6. doi: 10.1056/NEJMoa012835
89. Tonetti T, Grasselli G, Rucci P, Alessandri F, Dell'Olio A, Boscolo A, et al. Synergistic effect of static compliance and D-dimers to predict outcome in COVID-19 ARDS: a prospective multicenter study. Biomedicines. (2021) 9:1228. doi: 10.3390/biomedicines9091228
90. Boyle AJ, Sklar MC, McNamee JJ, Brodie D, Slutsky AS, Brochard L, et al. Extracorporeal carbon dioxide removal for lowering the risk of mechanical ventilation: research questions and clinical potential for the future. Lancet Respir Med. (2018) 6:874–84. doi: 10.1016/S2213-2600(18)30326-6
91. Romagnoli S, Ricci Z, Ronco C. Novel extracorporeal therapies for combined renal-pulmonary dysfunction. Semin Nephrol. (2016) 36:71–7. doi: 10.1016/j.semnephrol.2016.01.002
92. Consales G, Zamidei L, Turani F, Atzeni D, Isoni P, Boscolo G, et al. Combined renal-pulmonary extracorporeal support with low blood flow techniques: a retrospective observational study (CICERO study). Blood Purif. (2022) 51:299–308. doi: 10.1159/000517280
93. Zanella A, Castagna L, Salerno D, Scaravilli V, Abd El Aziz El Sayed Deab S, Magni F, et al. Respiratory electrodialysis. A novel, highly efficient extracorporeal CO2 removal technique. Am J Respir Crit Care Med. (2015) 192:719–26. doi: 10.1164/rccm.201502-0289OC
94. Menajovsky LB. Heparin-induced thrombocytopenia: clinical manifestations and management strategies. Am J Med. (2005) 118(Suppl 8A):21S−30S. doi: 10.1016/j.amjmed.2005.06.005
95. Protti A, L'Acqua C, Panigada M. The delicate balance between pro-(risk of thrombosis) and anti-(risk of bleeding) coagulation during extracorporeal membrane oxygenation. Ann Transl Med. (2016) 4:139. doi: 10.21037/atm.2016.03.06
96. Panigada M, Iapichino GE, Brioni M, Panarello G, Protti A, Grasselli G, et al. Thromboelastography-based anticoagulation management during extracorporeal membrane oxygenation: a safety and feasibility pilot study. Ann Intensive Care. (2018) 8:7. doi: 10.1186/s13613-017-0352-8
97. Zeibi Shirejini S, Carberry J, McQuilten ZK, Burrell AJC, Gregory SD, Hagemeyer CE. Current and future strategies to monitor and manage coagulation in ECMO patients. Thromb J. (2023) 21:11. doi: 10.1186/s12959-023-00452-z
98. Pacheco-Reyes AF, Plata-Menchaca EP, Mera A, Bonilla C, Sosa M, Torrella P, et al. Coagulation management in patients requiring extracorporeal membrane oxygenation support: a comprehensive narrative review. Ann Blood. (2024) 9:1–7. doi: 10.21037/aob-23-28
99. Jung C, Stueber T, Mirus M, Heubner L, Spieth PM. Anticoagulation in venovenous extracorporeal membrane oxygenation. Front Med. (2025) 12:1530411. doi: 10.3389/fmed.2025.1530411
100. Vajter J, Volod O. Anticoagulation management during ECMO: narrative review. JHLT Open. (2025) 8:100216. doi: 10.1016/j.jhlto.2025.100216
101. Rajsic S, Schwaiger D, Schausberger L, Breitkopf R, Treml B, Jadzic D, et al. Anticoagulation monitoring using activated clotting time in patients receiving extracorporeal membrane oxygenation: a meta-analysis of correlation coefficients. J Cardiothorac Vasc Anesth. (2024) 38:2651–60. doi: 10.1053/j.jvca.2024.07.048
102. Sklar MC, Beloncle F, Katsios CM, Brochard L, Friedrich JO. Extracorporeal carbon dioxide removal in patients with chronic obstructive pulmonary disease: a systematic review. Intensive Care Med. (2015) 41:1752–62. doi: 10.1007/s00134-015-3921-z
103. Combes A, Brodie D, Aissaoui N, Bein T, Capellier G, Dalton HJ, et al. Extracorporeal carbon dioxide removal for acute respiratory failure: a review of potential indications, clinical practice and open research questions. Intensive Care Med. (2022) 48:1308–21. doi: 10.1007/s00134-022-06796-w
104. Vonk Noordegraaf A, Chin KM, Haddad F, Hassoun PM, Hemnes AR, Hopkins SR, et al. Pathophysiology of the right ventricle and of the pulmonary circulation in pulmonary hypertension: an update. Eur Respir J. (2019) 53:1801900. doi: 10.1183/13993003.01900-2018 Erratum in: Eur Respir J. (2025) 65:2050414. doi: 10.1183/13993003.50414-2020
105. Hemnes AR, Celermajer DS, D'Alto M, Haddad F, Hassoun PM, Prins KW, et al. Pathophysiology of the right ventricle and its pulmonary vascular interaction. Eur Respir J. (2024) 64:2401321. doi: 10.1183/13993003.01321-2024
106. Schöps M, Groß-Hardt SH, Schmitz-Rode T, Steinseifer U, Brodie D, Clauser JC, et al. Hemolysis at low blood flow rates: in-vitro and in-silico evaluation of a centrifugal blood pump. J Transl Med. (2021) 19:2. doi: 10.1186/s12967-020-02599-z
107. Pistolesi V, Morabito S, Pota V, Valente F, Di Mario F, Fiaccadori E, et al. Regional citrate anticoagulation (RCA) in critically ill patients undergoing renal replacement therapy (RRT): expert opinion from the SIAARTI-SIN joint commission. J Anesth Analg Crit Care. (2023) 3:7. doi: 10.1186/s44158-023-00091-w
Keywords: extracorporeal CO2 removal, acute distress respiratory syndrome, asthma, chronic obstructive pulmonary disease, mechanical ventilation, continuous renal replacement therapy
Citation: Parrilla-Gómez FJ, Castelli A, Colombo R, do Vale-Fernandes A, Nalesso F, Pestaña-Lagunas D, Suarez-Sipmann F and Terragni P (2025) The role of extracorporeal CO2 removal from pathophysiology to clinical applications with focus on potential combination with RRT: an expert opinion document. Front. Med. 12:1651213. doi: 10.3389/fmed.2025.1651213
Received: 21 June 2025; Accepted: 18 August 2025;
Published: 01 September 2025.
Edited by:
Francesco Murgolo, University of Bari Aldo Moro, ItalyReviewed by:
Andrea Meli, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, ItalyTomás Lamas, CUF Infante Santo Hospital, Portugal
Copyright © 2025 Parrilla-Gómez, Castelli, Colombo, do Vale-Fernandes, Nalesso, Pestaña-Lagunas, Suarez-Sipmann and Terragni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francisco José Parrilla Gómez, ZmNvcGFycmlsbGFAZ21haWwuY29t