 Solomiia Zaremba1†
Solomiia Zaremba1† Daniele Focosi2†
Daniele Focosi2† Wyatt W. Pruter1
Wyatt W. Pruter1 Massimo Franchini3Diana B. Collantes Hoyos1
Massimo Franchini3Diana B. Collantes Hoyos1 Mario Cruciani3Alex J. Miller1
Mario Cruciani3Alex J. Miller1 Juan G. Ripoll1
Juan G. Ripoll1 Arturo Casadevall4Sidna M. Tulledge-Scheitel5
Arturo Casadevall4Sidna M. Tulledge-Scheitel5 Nathalie Rufer6,7Thomas Hueso8,9Justin E. Juskewitch10Camille M. van Buskirk10
Nathalie Rufer6,7Thomas Hueso8,9Justin E. Juskewitch10Camille M. van Buskirk10 Petros Ioannou11,12Francesco Lanza13
Petros Ioannou11,12Francesco Lanza13 Raymund R. Razonable14Ferenc Magyari15
Raymund R. Razonable14Ferenc Magyari15 László Imre Pinczés15
László Imre Pinczés15 Ravindra Ganesh16Claudia M. Denkinger17,18Ryan T. Hurt16
Ravindra Ganesh16Claudia M. Denkinger17,18Ryan T. Hurt16 Maike Janssen19
Maike Janssen19 James R. Stubbs10Carsten Müller-Tidow19,20
James R. Stubbs10Carsten Müller-Tidow19,20 Jeffrey L. Winters10
Jeffrey L. Winters10 Karin Holm21Sameer A. Parikh22Gordana Simeunovic23
Karin Holm21Sameer A. Parikh22Gordana Simeunovic23 Neil E. Kay22,24
Neil E. Kay22,24 Bart J. Rijnders25,26
Bart J. Rijnders25,26 Scott R. Wright27Nahema Issa28Hélène Chaussade28
Scott R. Wright27Nahema Issa28Hélène Chaussade28 Rickey E. Carter29Darrell R. Schroeder30
Rickey E. Carter29Darrell R. Schroeder30 Jonathon W. Senefeld31*‡
Jonathon W. Senefeld31*‡ Michael J. Joyner1*‡
Michael J. Joyner1*‡- 1Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN, United States
- 2North-Western Tuscany Blood Bank, Pisa University Hospital, Pisa, Italy
- 3Department of Transfusion Medicine and Hematology, Carlo Poma Hospital, Mantua, Italy
- 4Department of Molecular Microbiology and Immunology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, United States
- 5Division of Community Internal Medicine, Mayo Clinic, Rochester, MN, United States
- 6Interregional Blood Transfusion SRC, Epalinges, Switzerland
- 7Department of Oncology, Lausanne University Hospital and University of Lausanne, Epalinges, Switzerland
- 8Department of Hematology, Gustave Roussy, Villejuif, France
- 9Department of Early Drug Development, Gustave Roussy, Villejuif, France
- 10Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN, United States
- 11School of Medicine, University of Crete, Heraklion, Greece
- 12Department of COVID-19, University Hospital of Heraklion, Heraklion, Greece
- 13Hematology Unit, Romagna Transplant Network for HSCT, Ravenna Hospital, University of Bologna, Bologna, Italy
- 14Division of Public Health, Infectious Diseases, and Occupational Medicine, Mayo Clinic, Rochester, MN, United States
- 15Division of Hematology, Department of Internal Medicine, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 16Division of General Internal Medicine, Mayo Clinic, Rochester, MN, United States
- 17Division of Infectious Disease and Tropical Medicine, Department of Infectious Diseases, Heidelberg University Hospital, Heidelberg, Germany
- 18German Center for Infection Research, Partner Site Heidelberg University Hospital, Heidelberg, Germany
- 19Department of Internal Medicine V, Heidelberg University Hospital, Heidelberg, Germany
- 20National Center for Tumor Diseases, Heidelberg, Germany
- 21Division of Infection Medicine, Department of Clinical Sciences, Lund University, Lund, Sweden
- 22Division of Hematology, Mayo Clinic, Rochester, MN, United States
- 23Corewell Health West/Michigan State University College of Human Medicine, Grand Rapids, MI, United States
- 24Department of Immunology, Mayo Clinic, Rochester, MN, United States
- 25Department of Internal Medicine, Section of Infectious Diseases, University Medical Center, Rotterdam, Netherlands
- 26Department of Medical Microbiology and Infectious Diseases, Erasmus MC, University Medical Center, Rotterdam, Netherlands
- 27Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN, United States
- 28Services de Médecine Interne et Maladies Infectieuses, CHU Bordeaux, Bordeaux, France
- 29Department of Quantitative Health Sciences, Mayo Clinic, Jacksonville, FL, United States
- 30Division of Quantitative Health Sciences, Mayo Clinic, Rochester, MN, United States
- 31Department of Health and Kinesiology, University of Illinois Urbana-Champaign, Urbana, IL, United States
COVID-19 convalescent plasma (CCP) obtained from recently recovered people is safe and effective against SARS-CoV-2. Currently available CCP is a “hybrid” product with antibodies from individuals who had both infection and vaccination (vaccine-boosted CCP). B-cell depleted patients are at risk of not producing antibodies after either infection or vaccination, hence conceivably among those who would benefit the most from CCP. We thus conducted a systematic review and individual participant data meta-analysis to assess characteristics associated with 60-day survival in B-cell depleted patients transfused with CCP. The protocol was registered with PROSPERO (CRD42024516513) on March 1st, 2024. The last search was on April 2nd, 2024, and included all studies using CCP in B-cell depleted patients. Whenever not available, we requested individual participant data from corresponding authors of eligible studies. Risk of bias was assessed using Joanna Briggs Institute Critical Appraisal Tools. Data were analyzed using conditional logistic regression. The overall 60-day survival rate was 86.5% in our cohort of 570 patients (85 included studies). After controlling for age, sex, calendar year of infection and World Health Organization (WHO) disease severity, we found a significant association between 60-day survival and transfusion of vaccine-boosted CCP (OR = 9.49; 95% CI 2.01–44.82; p = 0.005). Overall survival in our cohort of B-cell depleted patients was consistent with prior meta-analysis of randomized controlled trials on survival of immunocompromised patient transfused with CCP (~84%). A novel finding from this analysis is that vaccine-boosted CCP is associated with a high survival benefit.
Introduction
Anti-CD20 monoclonal antibodies (e.g., rituximab) are commonly used for the treatment of patients with hematologic malignancies and autoimmune disorders (1, 2). By selectively targeting B-lymphocytes, such treatments impair the host ability to produce infection-neutralizing antibodies. Full recovery of the B-cell pool to normal levels can take up to 12 months after the last dose of anti-CD20 therapy (3). In this way, B-cell depleted patients are unlikely to mount robust endogenous antibody responses to either vaccine (4, 5) or natural infections, and thus are at higher risk of infections (including SARS-CoV-2 infection) and mortality. Indeed, treatment with anti-CD20 monoclonal antibodies has been shown to be associated with prolonged SARS-CoV-2 shedding (6–10). Persistent SARS-CoV-2 viremia in immunocompromised patients has also been shown to be associated with clinical severity of COVID-19 and mortality, highlighting the importance of prompt viral neutralization (11). Additionally, uncontrolled infection may lead to viral evolution and generation of novel SARS-CoV-2 variants in such patients (12).
COVID-19 convalescent plasma (CCP) has a robust safety and efficacy profile against SARS-CoV-2 among patients with immunodeficiencies (13–15). CCP contains polyclonal antibodies from donors that can neutralize a broad range of SARS-CoV-2 variants, and is one of the first therapeutic options deployed before the availability of monoclonal antibodies and vaccines (16, 17). Expert guidance on the use of CCP for immunocompromised patients includes anti-CD20 B-cell depleted patients (among others) as a target population recommended for CCP therapy (14), because in such patients CCP transfusion can benefit both acute symptomatic SARS-CoV-2 infection and protracted COVID-19.
However, there remains a limited number of studies on the clinical efficacy of CCP in B-cell depleted patients. Because CCP provides the viral-neutralizing antibodies B-cell depleted patients are lacking, this patient population may be among those who benefit the most from such therapy. Thus, we aimed to describe characteristics and outcomes of B-cell depleted patients infected with SARS-CoV-2 and transfused with CCP, whose cases were reported in the literature. Our overall goal was to gain insight into the characteristics of the patients, CCP treatment timing, and CCP quality that might influence outcomes in immunocompromised patients.
Consequently, we conducted a systematic review and individual participant data (IPD) meta-analysis to summarize available reports on the use of CCP in patients with secondary immunodeficiency due to anti-CD20 B-cell depletion.
Methods
Protocol and registration
The protocol for this systematic review and individual participant data meta-analysis was registered with PROSPERO (CRD42024516513) on March 1st, 2024.
Information sources and search
This systematic review and IPD meta-analysis aimed to evaluate outcomes of patients who have undergone B-cell depleting therapy with anti-CD20 medications and were transfused with CCP. Our review was conducted according to the guidance provided in the PRISMA-IPD (Preferred Reporting Items for Systematic reviews and Meta-Analyses, Supplementary Table S10). A previously published systematic review on the impact of CCP transfusion on COVID-19 mortality in patients with immunodeficiencies (15) was used to identify potentially eligible studies. That review included studies published between January 1st 2020 and August 12th 2022. Sources for the search included PubMed, MEDLINE, Google Scholar and medRχiv. An additional search to update the results was conducted between August 12th 2022 and April 2nd 2024. Keywords and Medical Subject Heading (MeSH) terms used for the search were similar to those used in the previous systematic review, although more specific to the type of immunodeficiency: (COVID-19 OR SARS-CoV-2 OR coronavirus disease 2019) AND (convalescent plasma OR immune plasma OR hyperimmune plasma) AND (immunosuppression OR immunodeficiency OR immunocompromised OR cancer OR malignancy OR hematological OR oncologic OR lymphoma OR leukemia OR myeloma OR multiple sclerosis OR agammaglobulinemia OR hypoglobulinemia OR autoimmune disorder OR BCDT OR B-cell depletion). Full-text translation to English was required for the inclusion of the article.
This search yielded 850 studies, including 145 studies from the previous review (15) and 705 studies from the additional search (Figure 1).
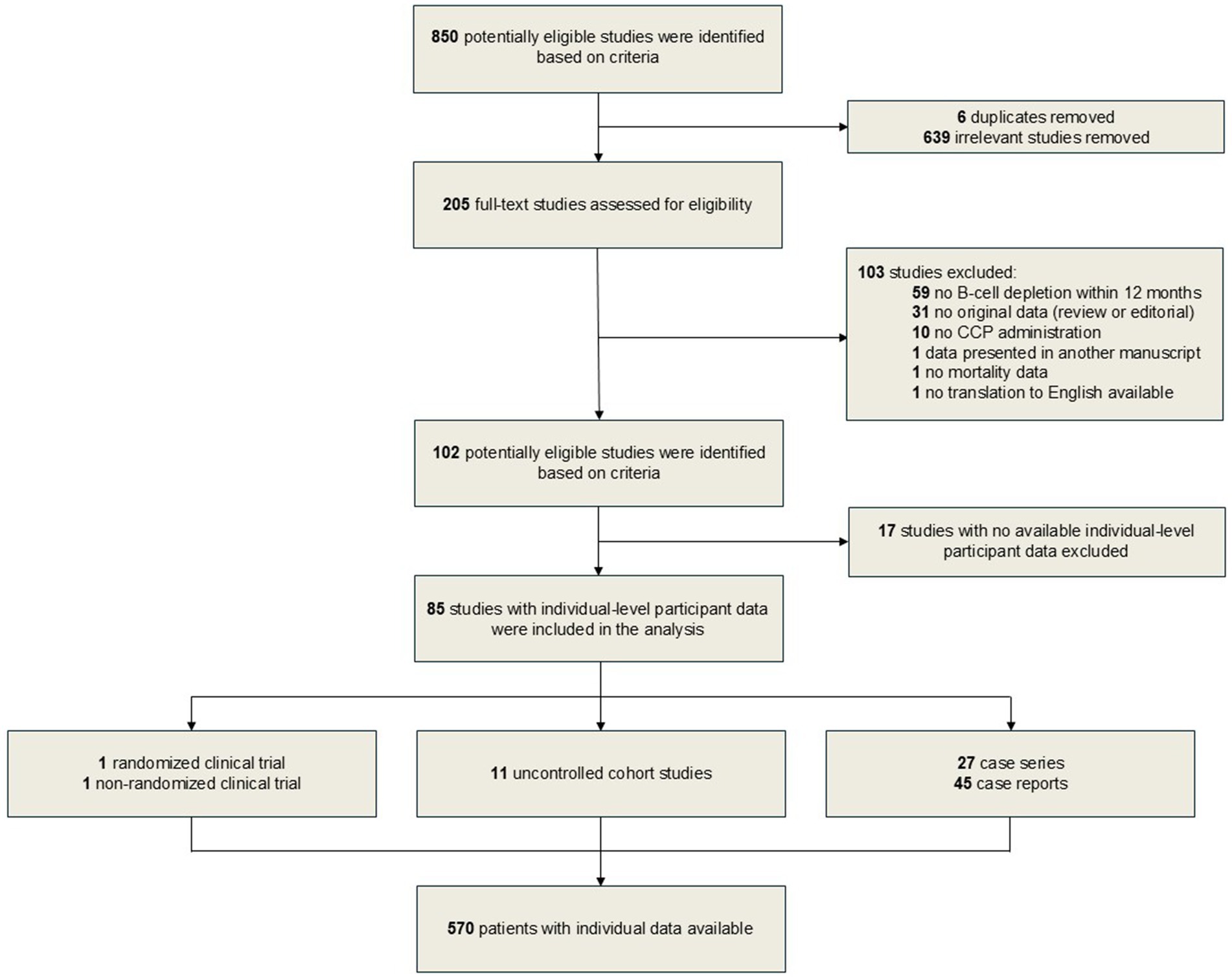
Figure 1. Flowchart of studies inclusion and exclusion criteria.
Study selection and data collection processes
After initial screening of 850 potentially eligible manuscripts, we removed 639 irrelevant studies and six duplicates. A total of 205 full-text manuscripts were then further assessed for eligibility. Studies that included only patients with primary immunodeficiencies were excluded. We then contacted the authors who reported patients with secondary immunodeficiencies transfused with CCP but did not specify the underlying cause of immunodeficiency or did not report individual patient-level data. This review did not have restrictions on study type, thus randomized controlled trials (RCT), non-RCT, cohort studies, case series and case reports were all eligible for inclusion. However, manuscripts with no original data (reviews and editorials) were excluded. Studies were excluded if IPD was unavailable, patients did not receive a B-cell depleting therapy within 12 months prior to COVID-19 diagnosis, if patients did not receive CCP treatment for COVID-19, if the study did not report our primary outcome of interest (i.e., mortality), if data were already included in another manuscript as part of larger cohort, and if no translation to English was available. The full-text screening process resulted in exclusion of 103 studies (Figure 1). Out of 102 potentially eligible studies, we received or abstracted individual patient data from 85 studies. Corresponding authors directly input IPD into a combined dataset for all eligible patients. For the studies that included IPD in primary text, two independent reviewers out of potentially available four reviewers extracted the data from each manuscript (D. F., S. Z., D. C. H., A. J. M.), then disagreements were resolved by third reviewer (J. W. S.).
Abstracted data included: patient age and sex, clinical status before CCP transfusion [8-point World Health Organization (WHO) COVID-19 disease severity score (18), need for mechanical ventilation, and serum anti-Spike antibody status], underlying condition and concomitant therapies, type(s) of B-cell depleting agents, CCP therapy (number of CCP units administered, volume of plasma per CCP unit, total volume of CCP transfused), use of vaccine-boosted CCP, time since the symptoms onset to first CCP transfusion, time since the first hospital admission to first CCP transfusion (if applicable), concomitant COVID-19 therapies (intravenous immunoglobulin, anti-spike monoclonal antibodies, steroids, remdesivir, nirmatrelvir/ritonavir, hydroxychloroquine), patient clearance of SARS-CoV-2, rapid clinical improvement (defined as symptoms improvement and/or reduction in supplemental oxygen requirement within 5 days of CCP transfusion), duration of follow-up in days, and all-cause mortality. We collected all data possible within the constraints of availability, as not all the data were available for each patient. Our primary outcome of interest was 60-day survival following CCP transfusion or initial CCP transfusion in the cases of multiple CCP transfusions. For the primary outcome of 60-day survival, eligibility required that patients had sufficient data to classify survival status. This was defined as either (1) a reported time-to-death or (2) confirmation of survival through at least 60 days of follow-up. Patients who were censored before 60 days but remained alive at last contact were conservatively classified as survivors through day 60. No patients with completely missing outcome data were included in the analysis. This approach is consistent with conventional methods for censored survival data (19). The term “vaccine-boosted CCP” is used in this manuscript as a pragmatic proxy for plasma with presumably higher antibody potency. We recognize that this designation reflects both donor vaccination and convalescence history rather than direct antibody or neutralization titers. Quantitative antibody data were rarely reported across the included studies and, when reported, were derived from heterogeneous assay platforms that lack standardized thresholds, precluding pooled analyses.
Eligibility criteria
Eligible participants were patients with secondary immunodeficiencies due to treatment with anti-CD20 monoclonal antibodies who were diagnosed with COVID-19 and were then transfused with CCP. Both hospitalized and non-hospitalized patients with COVID-19 were considered. Patients were excluded if the most recent B-cell depleting therapy was more than 12 months before COVID-19 diagnosis. No control participants were included in this systematic review and IPD meta-analysis. Participants who did not meet these criteria were excluded on the individual level. If no IPD were presented in the manuscript, studies with potentially eligible cohorts (e.g., COVID-19 patients with hematologic malignancies transfused with CCP, COVID-19 patients with autoimmune disorders transfused with CCP) were considered for inclusion. After obtaining further details on the patient’s underlying condition and treatment (anti-CD20 B-cell depletion status in question) from the corresponding authors, patients were included on the individual basis if fulfilled these criteria. Additionally, a study was considered eligible if at least one participant from the cohort met inclusion criteria. Studies were excluded if no information on anti-CD20 treatment was available.
Ethical approval and quality assessment
This study was exempt from institutional review board approval at Mayo Clinic, as only previously published data were included. Thus, patient informed consent was waived. Joanna Briggs Institute (JBI) Critical Appraisal Tools were used for risk of bias assessment: each study was assessed depending on the study type (RCT, non-RCT, cohort study, case series, case report) (20–23). Two reviewers (S. Z., W. W. P.) independently applied respective tools, discrepancies were discussed with a third reviewer (J. W. S.) until consensus was achieved. The results of assessment depending on the proportion of “yes” answers were scored in the following way: ≤49% yes = high risk of bias, 50–69% yes = moderate risk of bias, ≥70% yes = low risk of bias.
Statistical analysis
Patient and treatment characteristics are presented overall, and according to 60-day survival, using median (25th, 75th percentile) for continuous variables and frequency count (%) for nominal variables. Since the predominant variants of SARS-CoV-2, patient demographics, and disease severity changed over the study period, analyses to assess the association of patient and treatment characteristics with 60-day survival were performed using conditional logistic regression with 48 strata defined by calendar year (2020, 2021, 2022/2023), age (≤49, 50–59, 60–69, ≥70), sex (male, female), and WHO disease severity score (≤4, ≥5). For continuous variables, initial analyses were performed using a restricted cubic spline with three knots to test the linearity assumption. From these analyses, the linearity assumption was valid for all variables except the days since the last anti-CD20 dose. For the days since the last anti-CD20 dose, the log-odds of survival increased in a linear fashion up to 100 days and then remained relatively unchanged beyond 100 days. For this reason, the days since the last anti-CD20 dose was modeled using a linear term with the number of days truncated at 100 for those with values greater than 100. Separate conditional logistic regression models were fit for each patient and treatment characteristic with results summarized by presenting the odds ratio with corresponding 95% confidence interval. For these analyses, two-tailed p < 0.05 was considered statistically significant. To further explore which characteristics had the greatest impact on 60-day survival, a machine learning model was developed with XGBoost chosen as the modeling framework because of its ability to handle missing data. For the XGBoost algorithm the outcome was 60-day survival and logarithmic loss was the evaluation metric to be minimized. Grid optimization of the learning algorithm was used to evaluate the effect of the learning rate (eta: 0.01, 0.1, or 0.3), maximum tree depth (3, 5, 7, or 10), minimum child weight (1, 3, or 5), subsample rate (80 or 100%), number of columns per tree (70 or 100%) and regularization (L1: 0 or 0.05; L2: 0.9 or 1). Using this search space, each combination of hyperparameter settings was trained using fivefold cross-validation and using early stopping to determine the optimum number of trees. The final selected hyperparameters were eta = 0.1, maximum tree depth = 3, minimum child weight = 5, subsample rate = 0.8, columns per tree = 0.7, L1 regularization = 0, L2 regularization = 0.9 and the number of trees = 35. Using the final hyperparameters, the model was retrained with training terminated after 35 iterations. A plot based on Shapley Additive Explanation (SHAP) values was constructed to quantify the relative importance of the variables in the final model. Receiver operating characteristic curve analysis was used to select a threshold based on the Youden index. Statistical analyses were performed using SAS statistical software, version 9.4 (SAS Institute Inc., Cary, NC) and R statistical software, version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study selection and characteristics
The process of study selection for this meta-analysis is presented in the PRISMA flow diagram (Figure 1). One RCT (24) with one eligible patient, one non-RCT (25) with one patient, 11 cohort studies (10, 11, 26–34) with a total of 268 eligible patients, 27 case series (35–60) with a total of 253 eligible patients, and 45 case reports (61–105) with a total of 47 patients met our inclusion criteria.
Thus, the final analysis cohort included 570 patients from 85 studies. Only subgroups of patients were included from cohort studies, RCT and non-RCT, thus limiting the scope of attainable analysis to individual-level and rendering the use of a control group unfeasible. This was due to the lack of large studies primarily focused on the outcomes of B-cell depleted patients transfused with CCP, as these patients were often included into a cohort of immunocompromised patients. Data for the studies included in this work were collected mostly during the high-volume phases of the pandemic and thus represent a challenging data collection environment for the investigators, so variables of interest were not always available. Counts of total number of individuals with available data per variable are presented in Tables 1, 2. Descriptive and exploratory analyses were performed on the synthesized IPD from all included studies.
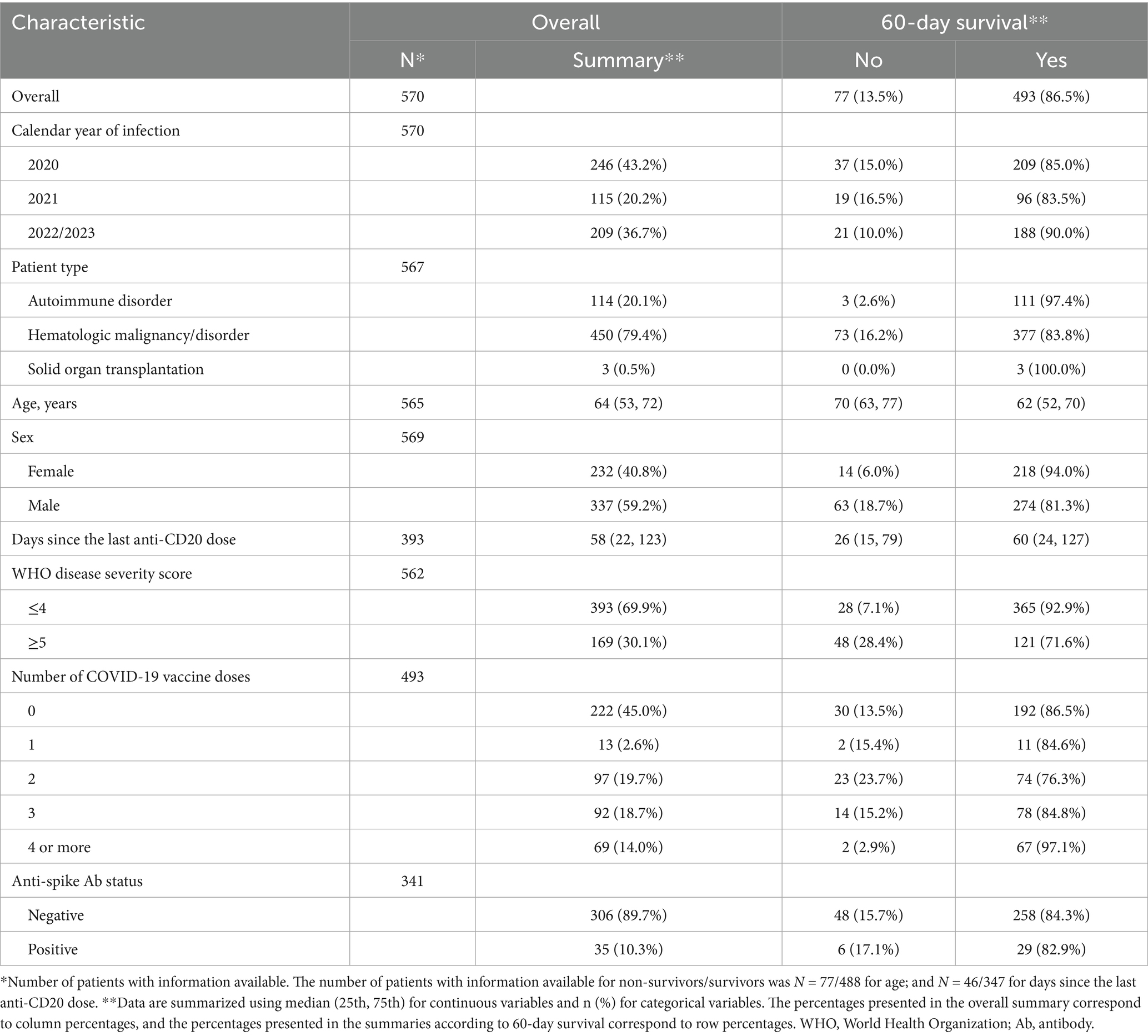
Table 1. Patient characteristics.
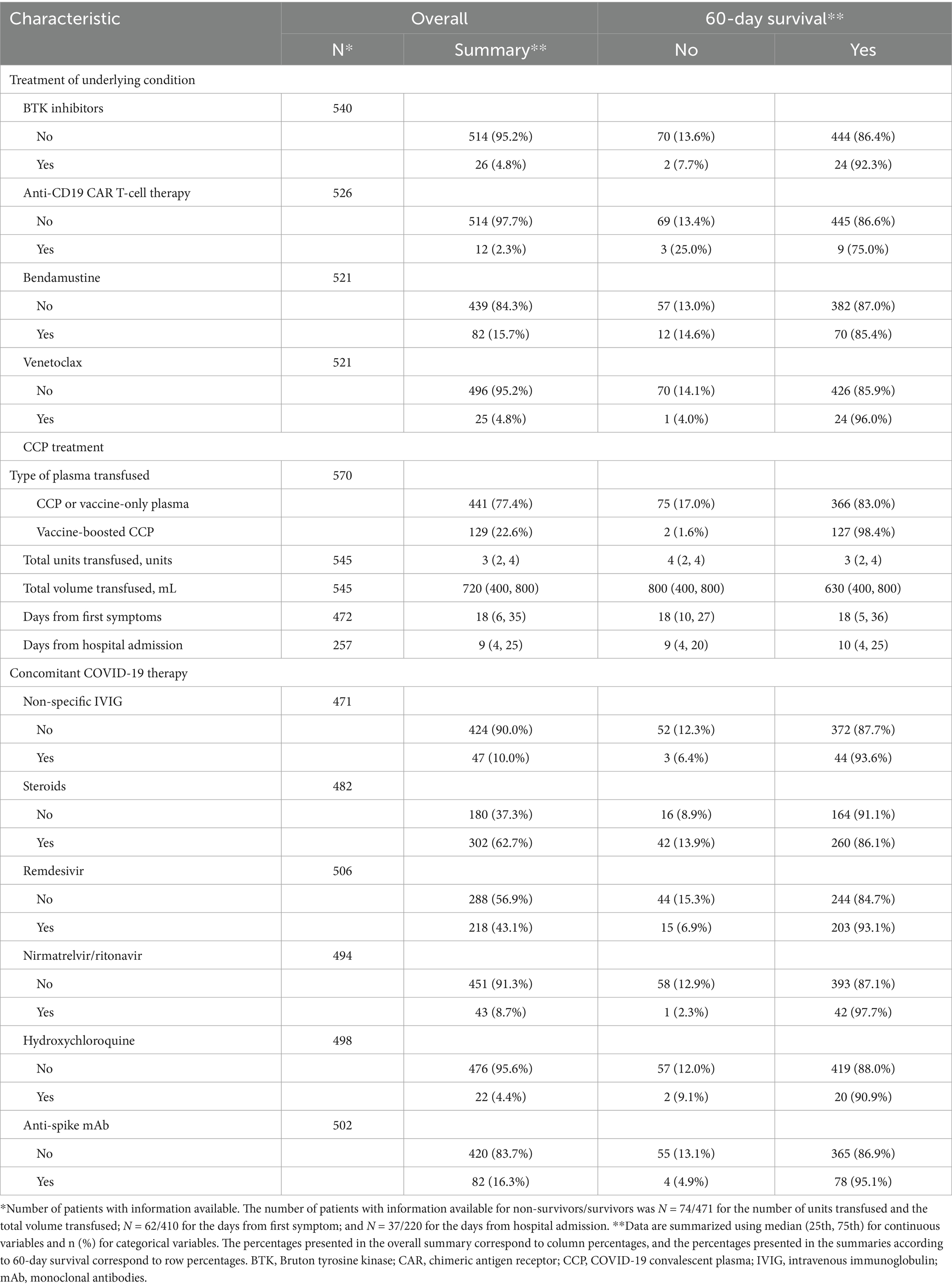
Table 2. Treatment characteristics.
Risk assessment
The results of the risk of bias assessment are presented in Supplementary Tables S4–S8. Both RCT and non-RCT showed low risk of bias. Eight of 11 cohort studies showed low risk of bias, while only one cohort study showed high risk. Among 27 case series 21 were assessed to have low risk of bias, and three had high risk. When risk of bias assessment tool was applied to case reports, 40 of 45 studies showed low risk, and only one showed high risk of bias.
Exploratory analyses of individual participant data
The final cohort included 570 patients who were B-cell depleted due to treatment of other diseases with anti-CD20 monoclonal antibodies and who were transfused with CCP for COVID-19. Overall, 60-day survival was 86.5% (493 of 570 patients), while 70.1% of patients achieved viral clearance (288 of 411 patients) and 64.3% had clinical improvement within 5 days of CCP transfusion (286 of 445 patients).
Patient and treatment characteristics of our synthesized cohort overall and according to 60-day survival outcome are presented in Tables 1, 2 (overall characteristics with stratification based on calendar year are in Supplementary Tables S1, S2). As expected, patients who survived 60-days were observed to be younger [median (Q1, Q3) age of 62 (52, 70) versus 70 (63, 77) years for those who did not survive 60-days]. WHO disease severity scale utilized in the final cohort is presented in Supplementary Table S9. Survival was better for patients with lower WHO disease severity (92.9% vs. 71.6% for WHO ≤4 versus WHO ≥5), females (94.0% versus 81.3% for females versus males), and those treated later during the pandemic (85.0, 83.5, and 90.0% for calendar year 2020, 2021, and 2022/2023 respectively). Results from conditional logistic regression analyses assessing the association of the other patient and treatment characteristics with 60-day survival after controlling for calendar year, age, sex, and WHO disease severity are summarized in Table 3. After controlling for these variables, 60-day survival was found to be significantly higher for autoimmune disorders (OR = 6.88, 95% CI 1.50–31.63, p = 0.013), longer time since the last anti-CD20 dose (OR = 1.16 per 10-day increase, 95% CI 1.04–1.29, p = 0.007), and treatment with vaccine-boosted CCP (OR = 9.49, 95% CI 2.01 to 44.82, p = 0.005). Additionally, patient outcomes according to year of infection are presented in Supplementary Table S3.
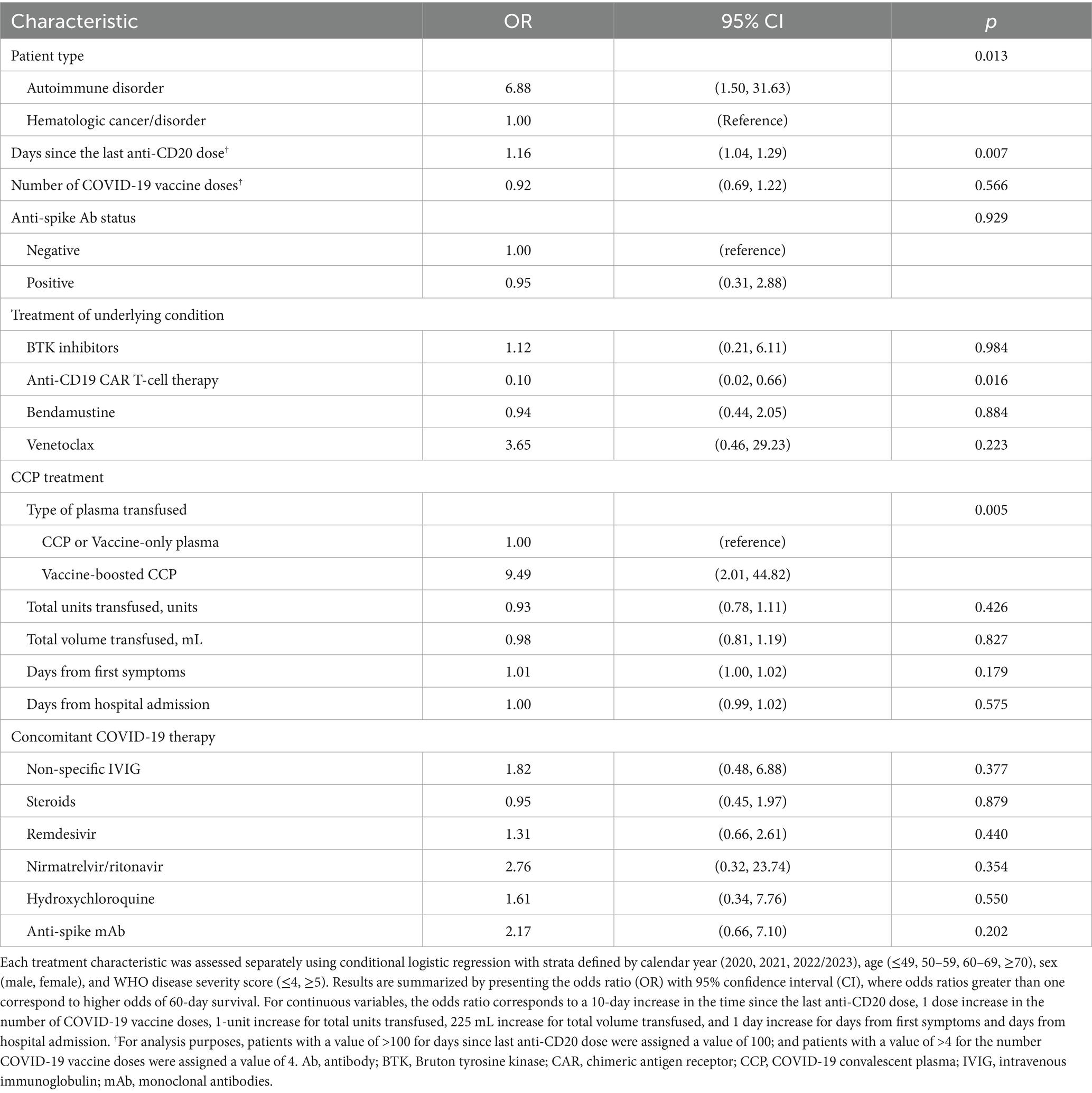
Table 3. Conditional logistic regression results.
To further explore which characteristics had the greatest impact on 60-day survival, a machine learning based model was developed using XGBoost. The model performance for the final model is shown in Supplementary Figure S1. The XGBoost model achieved an AUC of 0.916 (95% CI 0.887–0.946) when trained and evaluated on the same dataset; we note this is an exploratory finding and may overestimate model performance given the absence of external validation. Using a threshold of 0.83 or higher, the observed accuracy, sensitivity and specificity were 80.5% (459/570, 95% CI 77.0–83.7%), 78.7% (388/493, 95% CI 74.8–82.2%) and 92.2% (71/77, 95% CI 83.8–97.1%) respectively. A plot of the Shapley Additive Explanation (SHAP) values, demonstrating variable importance for the final XGBoost model, is shown in Figure 2. In order of importance, the top five variables were WHO disease severity ≥5, age, male sex, days since the last anti-CD20 dose, and treatment with vaccine-boosted CCP.
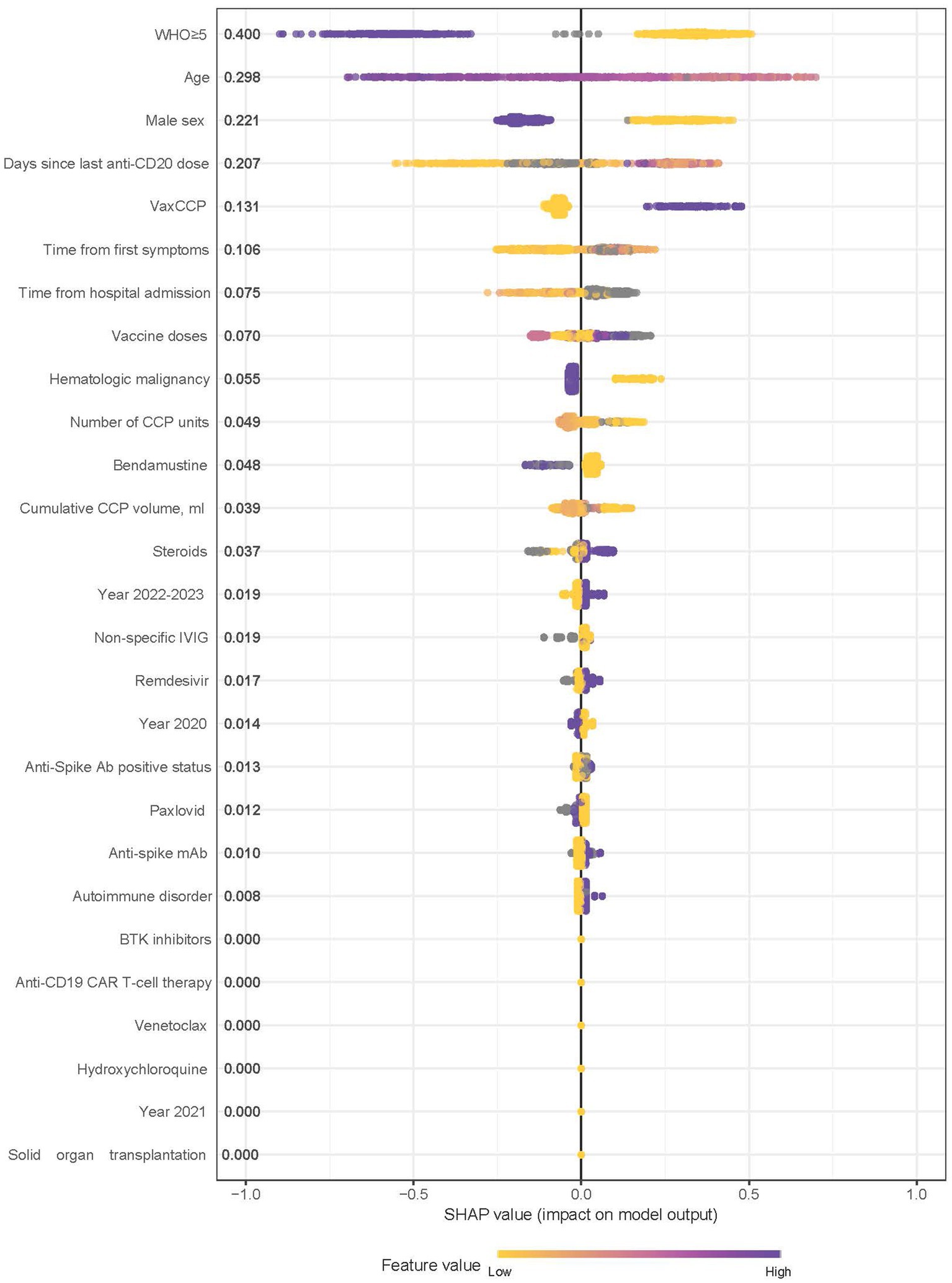
Figure 2. Shapley additive explanation (SHAP) values demonstrating variable importance, and direction, for the final XGBoost model. The SHAP value accounts for the interrelationship between the model features. Positive SHAP values indicate a higher likelihood of 60-day survival. Relative importance is presented after each variable with those having higher importance listed higher on the graph. Color is used to show the relative influence based on the value of the given variable, with yellow representing lower values and purple representing higher values. WHO, World Health Organization; VaxCCP, vaccine-boosted COVID-19 convalescent plasma; IVIG, intravenous immunoglobulin; mAb, monoclonal antibodies; BTK, Bruton tyrosine kinase; CAR, chimeric antigen receptor.
Discussion
This study is the first systematic review and IPD meta-analysis to describe CCP efficacy in a clearly defined iatrogenic immunodeficiency, namely B-cell deficiency from anti-CD20 mAb therapy. This aspect of our study distinguishes it from the previous work in a more heterogenous population of immunocompromised patients. CCP transfusion in patients with B-cell deficiencies is akin to immunoglobulin replacement therapy, which is commonly used in antibody deficiencies.
This systematic review and IPD meta-analysis of B-cell depleted patients has four main findings. First, COVID-19 treatment with CCP in B-cell depleted patients was associated with a survival rate similar to the population of patients with different types of primary and secondary immunodeficiencies, transfused with CCP (15). Second, vaccine-boosted CCP, which likely had higher neutralizing antibody content, was associated with a survival benefit. Third, remdesivir did not show significant interaction with CCP when administered concomitantly in patients with different severities of COVID-19. Fourth, among B-cell depleted patients, underlying hematologic malignancies were associated with higher mortality when compared to patients who received B-cell depletion for autoimmune disorders.
In mid-2021, a novel vaccine-boosted convalescent plasma became available. Vaccine-boosted CCP contains 10–100 times more or higher antibody titers than the CCP used early in the pandemic (106). Vaccine-boosted CCP is derived from individuals who have both recovered from SARS-CoV-2 and received vaccination against SARS-CoV-2, or from vaccinated individuals after breakthrough infections. Previous research has shown higher titer CCP to be associated with survival benefit among patients not requiring mechanical ventilation before CCP transfusion (107)—a finding which was recapitulated in our results. Patients with WHO score ≤4 (did not require mechanical ventilation) had higher survival rates when transfused with vaccine-boosted CCP as opposed to conventional CCP.
Patients with autoimmune diseases had a higher survival rate (97.4%) than patients with hematologic malignancies (83.8%). After adjustment for year of infection, age, sex, and COVID-19 severity, autoimmune disorders were associated with better survival prognosis. This might be due to morbidity secondary to the underlying malignancies and the use of more aggressive concomitant immunosuppressive treatments in these patients. In a recent cohort study published after our systematic search was conducted, 92 patients with autoimmune disorders transfused with CCP had a similar survival rate of 97% (108). While another study reporting on outcomes of patients with hematologic diseases shows survival rates of 76.9% among the 81 B-cell depleted patients (34). That study included only hospitalized cases, however our combined group included both in- and out-patient individuals with COVID-19, thus potentially affecting discrepancies in survival rates.
Biological sex and age have been known risk factors affecting survival in not only immunocompromised, but also in the general population of COVID-19 patients (109): our machine learning model shows that these associations remain the same in patients with B-cell depletion. Similarly, we confirm that B-cell depleted patient with milder presentations of COVID-19 (lower WHO severity score and lower requirements of ventilatory support) have better prognosis. It should also be noted that T-cell–mediated immunity may contribute to protection against SARS-CoV-2 in this population. Prior studies have demonstrated that functional T-cell responses can persist despite impaired B-cell function, and these responses may partly explain variability in outcomes among B-cell depleted patients (110, 111).
It is noteworthy that time from first symptom onset to first CCP transfusion had a wide range from 1 to 217 days, with a median of 18 days. These findings show that CCP remains effective in B-cell depleted patients even when administered late in COVID-19 course. Despite the protracted disease course, a majority of B-cell depleted patients achieved rapid clinical improvement (within 5 days of plasma transfusion) and were finally able to clear the virus. However, CCP characteristics such as number of units and total volume of transfused CCP did not significantly affect survival in our cohort. This observation might be attributed to protracted course of infection, non-standardized protocols of CCP transfusion with re-infusions at different time points of the disease and does not necessarily reflect lack of dose–response effect. Cases presented herein were challenging and did not always respond to standard treatment protocols, thus patient management was complex.
Our findings suggest that the time since last dose of anti-CD20 monoclonal antibodies represents a key factor associated with patient outcomes, as more recent anti-CD20 treatment was associated with higher mortality.
The COVID-19 pandemic has been so far associated with several different SARS-CoV-2 variants, including heterogenous wild-type genotypes early in the pandemic, supplanted by Alpha (B.1.1.7) and Beta (B.1.351) variants of concern (VOC) in early 2021, Delta VOC (B.1.617.2) in mid-2021, and Omicron VOC and its subvariants thereafter. In our study, patients with B-cell depletion who received CCP transfusion later in the pandemic (2022/2023) had better survival compared to patients receiving CCP before 2022. These differences in survival may be partly attributed to any of the following: advances in COVID-specific treatments and testing tools, emergence of biologically less virulent Omicron VOC, and also to the more precise identification of CCP units with high titer of neutralizing antibodies and earlier transfusion during later phases of the pandemic.
Studies have reported survival benefit in immunocompromised patients treated with remdesivir (10, 112), while nirmatrelvir/ritonavir has shown to be associated with reduced mortality in non-immunocompromised population (113). However, our analysis did not show an interaction between remdesivir and CCP when administered concomitantly. Similarly, concomitant treatment with nirmatrelvir/ritonavir did not elicit significant interaction. We infer that this might be due different factors, such as protracted course of COVID-19 or CCP being already effective per se and masking the efficacy of remdesivir and nirmatrelvir/ritonavir.
Our study had some limitations. First, the exploratory analysis included data from lower tiers of evidence, such as case series and case reports (72 of 85 studies included). Although, these data cannot provide robust evidence of treatment effects, it can provide insights into the optimal use of an approved therapeutic with demonstrated safety and efficacy, such as CCP for treatment of B-cell depleted patients with COVID-19. Second, in our analysis we were limited to individual-level data analysis, since only two small cohort studies (10, 26) met our inclusion criteria on the group data level. Third, our synthesized cohort lacks control group that did not receive CCP. Fourth, a key limitation of this review is the absence of standardized antibody titer or neutralization data. While antibody potency is central to the biological rationale for CCP, studies included in this analysis rarely reported such data, and when reported, results were derived from diverse assays with limited cross-platform comparability. In prior work, we and others demonstrated that concordance across FDA-authorized assays for designating “high-titer” CCP varied markedly, with agreement ranging from only 26.5–82.7% (114). Accordingly, we framed “vaccine-boosted CCP” as an indirect surrogate for higher potency plasma. Our finding of an odds ratio of 9.49 for survival with vaccine-boosted CCP should therefore be interpreted as hypothesis-generating and underscores the need for future studies with harmonized, quantitative antibody measurements to validate and extend these observations.
Fifth, antibody status of individual patients was not consistently reported across studies. Although patients receiving B-cell depleting therapy generally exhibit impaired humoral responses, we cannot confirm that all included individuals lacked detectable anti-SARS-CoV-2 antibodies. Sixth, our dataset was not powered to assess outcomes by specific anti-CD20 monoclonal antibody. Last, the machine learning analysis was exploratory, as sample size constraints precluded conventional cross-validation or external validation. Reported AUC values should therefore be interpreted cautiously and require confirmation in larger datasets.
Conclusion
This systematic review and IPD meta-analysis supports the efficacy profile of CCP as a treatment strategy in B-cell depleted patients with COVID-19 and identifies cases with better survival rates after treatment. As may be anticipated based on biological principles of antibody therapy (115), these data show that the benefit of CCP was most apparent in patients who received CCP containing higher levels of antibodies—vaccine-boosted CCP.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found at: This secondary research did not generate original data, which remain available at the cited references.
Author contributions
SZ: Investigation, Writing – review & editing, Data curation, Visualization, Writing – original draft. DF: Conceptualization, Writing – review & editing, Writing – original draft. WP: Writing – review & editing, Data curation. MF: Data curation, Conceptualization, Writing – review & editing. DC: Data curation, Writing – review & editing. MC: Data curation, Writing – review & editing. AM: Data curation, Writing – review & editing. JR: Writing – review & editing. AC: Data curation, Writing – review & editing. ST-S: Writing – review & editing. NR: Data curation, Writing – review & editing. TH: Data curation, Writing – review & editing. JJ: Writing – review & editing. Cv: Writing – review & editing. PI: Data curation, Writing – review & editing. FL: Data curation, Writing – review & editing. RR: Writing – review & editing. FM: Writing – review & editing. LP: Writing – review & editing. RG: Writing – review & editing. CD: Writing – review & editing. RH: Writing – review & editing. MJ: Data curation, Writing – review & editing. JRS: Writing – review & editing. CM-T: Writing – review & editing. JW: Writing – review & editing. KH: Writing – review & editing. SP: Writing – review & editing. GS: Writing – review & editing. NK: Writing – review & editing. BR: Writing – review & editing. SW: Writing – review & editing. NI: Writing – review & editing. HC: Writing – review & editing. RC: Formal analysis, Writing – review & editing. DS: Visualization, Writing – original draft, Writing – review & editing, Formal analysis. JWS: Writing – review & editing, Supervision, Conceptualization. MJJ: Writing – review & editing, Supervision, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1658593/full#supplementary-material
References
1. Hawker, K, O’Connor, P, Freedman, MS, Calabresi, PA, Antel, J, Simon, J, et al. Rituximab in patients with primary progressive multiple sclerosis: results of a randomized double-blind placebo-controlled multicenter trial. Ann Neurol. (2009) 66:460–71. doi: 10.1002/ana.21867
2. Salles, G, Barrett, M, Foà, R, Maurer, J, O’Brien, S, Valente, N, et al. Rituximab in B-cell hematologic malignancies: a review of 20 years of clinical experience. Adv Ther. (2017) 34:2232–73. doi: 10.1007/s12325-017-0612-x
3. McLaughlin, P, Grillo-López, AJ, Link, BK, Levy, R, Czuczman, MS, Williams, ME, et al. Rituximab chimeric anti-CD20 monoclonal antibody therapy for relapsed indolent lymphoma: half of patients respond to a four-dose treatment program. J Clin Oncol. (2023) 41:154–62. doi: 10.1200/JCO.22.02403
4. Greenberger, LM, Saltzman, LA, Senefeld, JW, Johnson, PW, DeGennaro, LJ, and Nichols, GL. Antibody response to SARS-CoV-2 vaccines in patients with hematologic malignancies. Cancer Cell. (2021) 39:1031–3. doi: 10.1016/j.ccell.2021.07.012
5. Greenberger, LM, Saltzman, LA, Senefeld, JW, Johnson, PW, DeGennaro, LJ, and Nichols, GL. Anti-spike antibody response to SARS-CoV-2 booster vaccination in patients with B cell-derived hematologic malignancies. Cancer Cell. (2021) 39:1297–9. doi: 10.1016/j.ccell.2021.09.001
6. Aydillo, T, Gonzalez-Reiche, AS, Aslam, S, van de Guchte, A, Khan, Z, Obla, A, et al. Shedding of viable SARS-CoV-2 after immunosuppressive therapy for Cancer. N Engl J Med. (2020) 383:2586–8. doi: 10.1056/NEJMc2031670
7. Choi, B, Choudhary, MC, Regan, J, Sparks, JA, Padera, RF, Qiu, X, et al. Persistence and evolution of SARS-CoV-2 in an immunocompromised host. N Engl J Med. (2020) 383:2291–3. doi: 10.1056/NEJMc2031364
8. Shah, V, Ko Ko, T, Zuckerman, M, Vidler, J, Sharif, S, Mehra, V, et al. Poor outcome and prolonged persistence of SARS-CoV-2 RNA in COVID-19 patients with haematological malignancies; king’s college hospital experience. Br J Haematol. (2020) 190:e279–82. doi: 10.1111/bjh.16935
9. Tepasse, PR, Hafezi, W, Lutz, M, Kühn, J, Wilms, C, Wiewrodt, R, et al. Persisting SARS-CoV-2 viraemia after rituximab therapy: two cases with fatal outcome and a review of the literature. Br J Haematol. (2020) 190:185–8. doi: 10.1111/bjh.16896
10. Magyari, F, Pinczés, LI, Páyer, E, Farkas, K, Ujfalusi, S, Diószegi, Á, et al. Early administration of remdesivir plus convalescent plasma therapy is effective to treat COVID-19 pneumonia in B-cell depleted patients with hematological malignancies. Ann Hematol. (2022) 101:2337–45. doi: 10.1007/s00277-022-04924-6
11. Destremau, M, Chaussade, H, Hemar, V, Beguet, M, Bellecave, P, Blanchard, E, et al. Convalescent plasma transfusion for immunocompromised viremic patients with COVID-19: a retrospective multicenter study. J Med Virol. (2024) 96:e29603. doi: 10.1002/jmv.29603
12. Marques, AD, Graham-Wooten, J, Fitzgerald, AS, Leonard, AS, Cook, EJ, Everett, JK, et al. SARS-CoV-2 evolution during prolonged infection in immunocompromised patients. MBio. (2024) 15:e00110–24. doi: 10.1128/mbio.00110-24
13. Senefeld, JW, Klassen, SA, Ford, SK, Senese, KA, Wiggins, CC, Bostrom, BC, et al. Use of convalescent plasma in COVID-19 patients with immunosuppression. Transfusion. (2021) 61:2503–11. doi: 10.1111/trf.16525
14. Bloch, EM, Focosi, D, Shoham, S, Senefeld, J, Tobian, AAR, Baden, LR, et al. Guidance on the use of convalescent plasma to treat immunocompromised patients with coronavirus disease 2019. Clin Infect Dis. (2023) 76:2018–24. doi: 10.1093/cid/ciad066
15. Senefeld, JW, Franchini, M, Mengoli, C, Cruciani, M, Zani, M, Gorman, EK, et al. COVID-19 convalescent plasma for the treatment of immunocompromised patients: a systematic review and Meta-analysis. JAMA Netw Open. (2023) 6:e2250647. doi: 10.1001/jamanetworkopen.2022.50647
16. Focosi, D, Franchini, M, Pirofski, L-a, Burnouf, T, Fairweather, D, Joyner, MJ, et al. COVID-19 convalescent plasma is more than neutralizing antibodies: a narrative review of potential beneficial and detrimental co-factors. Viruses. (2021) 13:1594. doi: 10.3390/v13081594
17. Senefeld, JW, Casadevall, A, and Joyner, MJ. Convalescent plasma to deliver therapeutic antibodies against COVID-19. Trends Mol Med. (2022) 28:435–6. doi: 10.1016/j.molmed.2022.02.005
18. Rubio-Rivas, M, Mora-Luján, JM, Formiga, F, Arévalo-Cañas, C, Lebrón Ramos, JM, Villalba García, MV, et al. WHO ordinal scale and inflammation risk categories in COVID-19. Comparative study of the severity scales. J Gen Intern Med. (2022) 37:1980–7. doi: 10.1007/s11606-022-07511-7
19. Clark, TG, Bradburn, MJ, Love, SB, and Altman, DG. Survival analysis part I: basic concepts and first analyses. Br J Cancer. (2003) 89:232–8. doi: 10.1038/sj.bjc.6601118
20. Barker, TH, Stone, JC, Sears, K, Klugar, M, Tufanaru, C, Leonardi-Bee, J, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evid Synth. (2023) 21:494–506. doi: 10.11124/JBIES-22-00430
21. Barker, TH, Habibi, N, Aromataris, E, Stone, JC, Leonardi-Bee, J, Sears, K, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for quasi-experimental studies. JBI Evid Synth. (2024) 22:378–88. doi: 10.11124/JBIES-23-00268
22. Munn, Z, Barker, TH, Moola, S, Tufanaru, C, Stern, C, McArthur, A, et al. Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI Evid Synth. (2020) 18:2127–33. doi: 10.11124/JBISRIR-D-19-00099
23. Munn, Z, Stone, JC, Aromataris, E, Klugar, M, Sears, K, Leonardi-Bee, J, et al. Assessing the risk of bias of quantitative analytical studies: introducing the vision for critical appraisal within JBI systematic reviews. JBI Evid Synth. (2023) 21:467–71. doi: 10.11124/JBIES-22-00224
24. Denkinger, CM, Janssen, M, Schäkel, U, Gall, J, Leo, A, Stelmach, P, et al. Anti-SARS-CoV-2 antibody-containing plasma improves outcome in patients with hematologic or solid cancer and severe COVID-19: a randomized clinical trial. Nat Cancer. (2023) 4:96–107. doi: 10.1038/s43018-022-00503-w
25. Marconato, M, Abela, IA, Hauser, A, Schwarzmüller, M, Katzensteiner, R, Braun, DL, et al. Antibodies from convalescent plasma promote SARS-CoV-2 clearance in individuals with and without endogenous antibody response. J Clin Invest. (2022) 132:e158190. doi: 10.1172/JCI158190
26. Ioannou, P, Katsigiannis, A, Papakitsou, I, Kopidakis, I, Makraki, E, Milonas, D, et al. Convalescent plasma treatment of patients previously treated with B-cell-depleting monoclonal antibodies suffering COVID-19 is associated with reduced re-admission rates. Viruses. (2023) 15:756. doi: 10.3390/v15030756
27. Richier, Q, De Valence, B, Chopin, D, Gras, E, Levi, LI, Abi Aad, Y, et al. Convalescent plasma therapy in immunocompromised patients infected with the BA.1 or BA.2 omicron SARS-CoV-2. Influenza Other Respir Viruses. (2024) 18:e13272. doi: 10.1111/irv.13272
28. Brown, L-AK, Moran, E, Goodman, A, Baxendale, H, Bermingham, W, Buckland, M, et al. Treatment of chronic or relapsing COVID-19 in immunodeficiency. J Allergy Clin Immunol. (2022) 149:557–61.e1. doi: 10.1016/j.jaci.2021.10.031
29. Thümmler, L, Lindemann, M, Horn, PA, Lenz, V, Konik, M, Gäckler, A, et al. Early treatment with monoclonal antibodies or convalescent plasma reduces mortality in non-vaccinated COVID-19 high-risk patients. Viruses. (2023) 15:119. doi: 10.3390/v15010119
30. Lanza, F, Monaco, F, Ciceri, F, Cairoli, R, Sacchi, MV, Guidetti, A, et al. Lack of efficacy of convalescent plasma in COVID-19 patients with concomitant hematological malignancies: an Italian retrospective study. Hematol Oncol. (2022) 40:857–63. doi: 10.1002/hon.3060
31. Weinbergerová, B, Demel, I, Víšek, B, Válka, J, Čerňan, M, Jindra, P, et al. Successful early use of anti-SARS-CoV-2 monoclonal neutralizing antibodies in SARS-CoV-2 infected hematological patients – a Czech multicenter experience. Hematol Oncol. (2022) 40:280–6. doi: 10.1002/hon.2974
32. Aiello, TF, Peyrony, O, Chumbita, M, Monzó, P, Lopera, C, Puerta-Alcalde, P, et al. Real-life comparison of antivirals for SARS-CoV-2 omicron infection in patients with hematologic malignancies. Influenza Other Respir Viruses. (2024) 18:e13264. doi: 10.1111/irv.13264
33. Weisser, M, Khanna, N, Hedstueck, A, Sutter, ST, Roesch, S, Stehle, G, et al. Characterization of pathogen-inactivated COVID-19 convalescent plasma and responses in transfused patients. Transfusion. (2022) 62:1997–2011. doi: 10.1111/trf.17083
34. Hueso, T, Godron, AS, Lanoy, E, Pacanowski, J, Levi, LI, Gras, E, et al. Convalescent plasma improves overall survival in patients with B-cell lymphoid malignancy and COVID-19: a longitudinal cohort and propensity score analysis. Leukemia. (2022) 36:1025–34. doi: 10.1038/s41375-022-01511-6
35. Bronstein, Y, Adler, A, Katash, H, Halutz, O, Herishanu, Y, and Levytskyi, K. Evolution of spike mutations following antibody treatment in two immunocompromised patients with persistent COVID-19 infection. J Med Virol. (2022) 94:1241–5. doi: 10.1002/jmv.27445
36. D’Abramo, A, Vita, S, Maffongelli, G, Beccacece, A, Agrati, C, Cimini, E, et al. Clinical Management of Patients with B-cell depletion agents to treat or prevent prolonged and severe SARS-COV-2 infection: defining a treatment pathway. Front Immunol. (2022) 13:911339. doi: 10.3389/fimmu.2022.911339
37. Delgado-Fernández, M, García-Gemar, GM, Fuentes-López, A, Muñoz-Pérez, MI, Oyonarte-Gómez, S, Ruíz-García, I, et al. Treatment of COVID-19 with convalescent plasma in patients with humoral immunodeficiency – three consecutive cases and review of the literature. Enferm Infecc Microbiol Clin. (2022) 40:507–16. doi: 10.1016/j.eimc.2021.01.013
38. Franchini, M, Focosi, D, Percivalle, E, Beccaria, M, Garuti, M, Arar, O, et al. Variant of concern-matched COVID-19 convalescent plasma usage in seronegative hospitalized patients. Viruses. (2022) 14:1443. doi: 10.3390/v14071443
39. Martínez-Barranco, P, García-Roa, M, Trelles-Martínez, R, Arribalzaga, K, Velasco, M, Guijarro, C, et al. Management of persistent SARS-CoV-2 infection in patients with follicular lymphoma. Acta Haematol. (2021) 145:384–93. doi: 10.1159/000521121
40. Oliva, A, Cancelli, F, Brogi, A, Curtolo, A, Savelloni, G, Siccardi, G, et al. Convalescent plasma for haematological patients with SARS-CoV-2 pneumonia and severe depletion of B-cell lymphocytes following anti-CD20 therapy: a single-Centre experience and review of the literature. New Microbiol. (2022) 45:62–72.
41. Prasad, RM, Srivastava, S, Wang, E, Liu, JZ, Gami, R, Abdelgadir, A, et al. Effect of immunosuppressive diseases and rituximab infusions on allowing COVID-19 infection to relapse. Perm J. (2022) 26:123–31. doi: 10.7812/TPP/21.035
42. Rüfenacht, S, Gantenbein, P, Boggian, K, Flury, D, Kern, L, Dollenmaier, G, et al. Remdesivir in coronavirus disease 2019 patients treated with anti-CD20 monoclonal antibodies: a case series. Infection. (2022) 50:783–90. doi: 10.1007/s15010-022-01821-y
43. Furlan, A, Forner, G, Cipriani, L, Vian, E, Rigoli, R, Gherlinzoni, F, et al. Dramatic response to convalescent Hyperimmune plasma in association with an extended course of Remdesivir in 4 B cell–depleted non-Hodgkin lymphoma patients with SARS-Cov-2 pneumonia after rituximab therapy. Clin Lymphoma Myeloma Leuk. (2021) 21:e731–5. doi: 10.1016/j.clml.2021.05.013
44. Gharbharan, A, GeurtsvanKessel, CH, Jordans, CCE, Blaauw, M, van der Klift, M, Hassing, R-J, et al. Effects of treatment of coronavirus disease 2019 with convalescent plasma in 25 B-cell–depleted patients. Clin Infect Dis. (2021) 74:1271–4. doi: 10.1093/cid/ciab647
45. Gentile, S, Sullivan, LR, Brooks, H, and Simeunovic, G. A descriptive, retrospective analysis of COVID-19 passive antibody therapy and its effects on morbidity and mortality in patients receiving B-cell-depleting therapies. Diseases. (2024) 12:33. doi: 10.3390/diseases12020033
46. Gachoud, D, Pillonel, T, Tsilimidos, G, Battolla, D, Dumas, D, Opota, O, et al. Antibody response and intra-host viral evolution after plasma therapy in COVID-19 patients pre-exposed or not to B-cell-depleting agents. Br J Haematol. (2022) 199:549–59. doi: 10.1111/bjh.18450
47. Gachoud, D, Bertelli, C, and Rufer, N. Understanding the parameters guiding the best practice for treating B-cell-depleted patients with COVID-19 convalescent plasma therapy. Br J Haematol. (2023) 200:e25–7. doi: 10.1111/bjh.18540
48. Erber, J, Wiessner, JR, Huberle, C, Schneider, J, Mijočević, H, von Bomhard, D, et al. Convalescent plasma therapy in B-cell-depleted and B-cell sufficient patients with life-threatening COVID-19 – a case series. Transfus Apher Sci. (2021) 60:103278. doi: 10.1016/j.transci.2021.103278
49. Kremer, AE, Kremer, AN, Willam, C, Völkl, S, Verhagen, J, Achenbach, S, et al. Successful treatment of COVID-19 infection with convalescent plasma in B-cell-depleted patients may promote cellular immunity. Eur J Immunol. (2021) 51:2478–84. doi: 10.1002/eji.202149277
50. Kenig, A, Ishay, Y, Kharouf, F, and Rubin, L. Treatment of B-cell depleted COVID-19 patients with convalescent plasma and plasma-based products. Clin Immunol. (2021) 227:108723. doi: 10.1016/j.clim.2021.108723
51. Hueso, T, Pouderoux, C, Péré, H, Beaumont, A-L, Raillon, L-A, Ader, F, et al. Convalescent plasma therapy for B-cell–depleted patients with protracted COVID-19. Blood. (2020) 136:2290–5. doi: 10.1182/blood.2020008423
52. Da Silva, L, Klopfenstein, T, Gendrin, V, Clouet, J, Toko, L, Richier, Q, et al. Prolonged SARS-CoV-2 infection in patients receiving anti-CD20 monoclonal antibodies: a diagnostic challenged by negative nasopharyngeal RT-PCR and successful treatment with COVID-19 high-titer convalescent plasma. Viruses. (2023) 15:2220. doi: 10.3390/v15112220
53. Focosi, D, Senefeld, JW, Joyner, MJ, Sullivan, D, Casadevall, A, Bloch, EM, et al. Lower anti-spike levels in B-cell-depleted patients after convalescent plasma transfusion suggest the need for repeated doses. Br J Haematol. (2023) 200:e22–4. doi: 10.1111/bjh.18544
54. Ripoll, JG, Gorman, EK, Juskewitch, JE, Razonable, RR, Ganesh, R, Hurt, RT, et al. Vaccine-boosted convalescent plasma therapy for patients with immunosuppression and COVID-19. Blood Adv. (2022) 6:5951–5. doi: 10.1182/bloodadvances.2022008932
55. Ljungquist, O, Lundgren, M, Iliachenko, E, Månsson, F, Böttiger, B, Landin-Olsson, M, et al. Convalescent plasma treatment in severely immunosuppressed patients hospitalized with COVID-19: an observational study of 28 cases. Infect Dis. (2022) 54:283–91. doi: 10.1080/23744235.2021.2013528
56. Kluger, MA, Czogalla, J, Schmidt-Lauber, C, Peine, S, Schmiedel, S, Bangert, K, et al. Convalescent plasma treatment for early post-kidney transplant acquired COVID-19. Transpl Infect Dis. (2021) 23:e13685. doi: 10.1111/tid.13685
57. Cusi, MG, Conticini, E, Gandolfo, C, Anichini, G, Savellini, GG, Valente, S, et al. Hyperimmune plasma in three immuno-deficient patients affected by non-severe, prolonged COVID-19: a single-center experience. BMC Infect Dis. (2021) 21:630. doi: 10.1186/s12879-021-06321-2
58. Ferrari, S, Caprioli, C, Weber, A, Rambaldi, A, and Lussana, F. Convalescent hyperimmune plasma for chemo-immunotherapy induced immunodeficiency in COVID-19 patients with hematological malignancies. Leuk Lymphoma. (2021) 62:1490–6. doi: 10.1080/10428194.2021.1872070
59. Huygens, S, Gharbharan, A, Serroukh, Y, Snoek, B, Franken, B, Oude Munnink, BB, et al. High-titer convalescent plasma plus nirmatrelvir/ritonavir treatment for non-resolving COVID-19 in six immunocompromised patients. J Antimicrob Chemother. (2023) 78:1644–8. doi: 10.1093/jac/dkad144
60. Nissen-Meyer, LSH, Macpherson, ME, Skeie, LG, Hvalryg, M, Llohn, AH, Steinsvåg, TT, et al. COVID-19 patients treated with convalescent plasma. Tidsskr Nor Laegeforen. (2023) 143. doi: 10.4045/tidsskr.22.0577
61. Baang, JH, Smith, C, Mirabelli, C, Valesano, AL, Manthei, DM, Bachman, MA, et al. Prolonged severe acute respiratory syndrome coronavirus 2 replication in an immunocompromised patient. J Infect Dis. (2020) 223:23–7. doi: 10.1093/infdis/jiaa666
62. Adedoyin, O, Brijmohan, S, Lavine, R, and Lisung, FG. Undetectable SARS-CoV-2 active adaptive immunity-post-vaccination or post-COVID-19 severe disease-after immunosuppressants use. BMJ Case Rep. (2021) 14:e246308. doi: 10.1136/bcr-2021-246308
63. Aviv, R, Weber, A, Anzum, T, Federbush, M, Horowitz, D, and Singas, E. Prolonged coronavirus disease 2019 in a patient with rheumatoid arthritis on rituximab therapy. J Infect Dis. (2021) 224:557–9. doi: 10.1093/infdis/jiab248
64. Baek, YJ, Park, G, Choi, JY, Kim, EJ, Kim, BI, Gwack, J, et al. Within-host evolution of SARS-CoV-2 in a B-cell depleted patient with successful treatment. J Korean Med Sci. (2023) 38:e175. doi: 10.3346/jkms.2023.38.e175
65. Balashov, D, Trakhtman, P, Livshits, A, Kovalenko, I, Tereshenko, G, Solopova, G, et al. SARS-CoV-2 convalescent plasma therapy in pediatric patient after hematopoietic stem cell transplantation. Transfus Apher Sci. (2021) 60:102983. doi: 10.1016/j.transci.2020.102983
66. Basheer, M, Saad, E, Laskar, O, Schuster, O, Rechnitzer, H, Zisman-Rozen, S, et al. Clearance of the SARS-CoV-2 virus in an immunocompromised patient mediated by convalescent plasma without B-cell recovery. Int J Mol Sci. (2021) 22:8902. doi: 10.3390/ijms22168902
67. Belcari, G, Conti, A, Mazzoni, A, Lanza, M, Mazzetti, P, and Focosi, D. Clinical and Virological response to convalescent plasma in a chronic lymphocytic leukemia patient with COVID-19 pneumonia. Life. (2022) 12:1098. doi: 10.3390/life12071098
68. Bruiners, N, Guerrini, V, Ukey, R, Dikdan, RJ, Yang, JH, Mishra, PK, et al. Longitudinal analysis of biologic correlates of COVID-19 resolution: case report. Front Med. (2022):9. doi: 10.3389/fmed.2022.915367
69. Casarola, G, D’Abbondanza, M, Curcio, R, Alcidi, R, Campanella, T, Rossi, R, et al. Efficacy of convalescent plasma therapy in immunocompromised patients with COVID-19: a case report. Clin Infect Pract. (2021) 12:100096. doi: 10.1016/j.clinpr.2021.100096
70. Chen, RX, Mai, YL, Shen, KN, Zhang, T, Shi, JH, and Yang, YL. A case of follicular lymphoma with recurrent fever and pulmonary infiltrates. Zhonghua Jie He He Hu Xi Za Zhi. (2024) 47:222–7. doi: 10.3760/cma.j.cn112147-20230829-00112
71. Clark, E, Guilpain, P, Filip, IL, Pansu, N, Le Bihan, C, Cartron, G, et al. Convalescent plasma for persisting COVID-19 following therapeutic lymphocyte depletion: a report of rapid recovery. Br J Haematol. (2020) 190:e154–6. doi: 10.1111/bjh.16981
72. Colombo, D, Gatti, A, Alabardi, P, Bompane, D, Bonardi, G, Mumoli, N, et al. COVID-19-associated pneumonia in a B-cell-depleted patient with non-Hodgkin lymphoma: recovery with Hyperimmune plasma (2022) 11:77–80. doi: 10.14740/jh845
73. Garcia-Vidal, C, Iglesias-Caballero, M, Puerta-Alcalde, P, Mas, V, Cuesta-Chasco, G, Garcia-Pouton, N, et al. Emergence of progressive mutations in SARS-CoV-2 from a hematologic patient with prolonged viral replication. Front Microbiol. (2022) 13:826883. doi: 10.3389/fmicb.2022.826883
74. Gibson, EG, Pender, M, Angerbauer, M, Cook, C, Jones, B, Spivak, AM, et al. Prolonged SARS-CoV-2 illness in a patient receiving Ocrelizumab for multiple sclerosis. Open Forum Infect Dis. (2021) 8:ofab176. doi: 10.1093/ofid/ofab176
75. Helleberg, M, Niemann, CU, Moestrup, KS, Kirk, O, Lebech, A-M, Lane, C, et al. Persistent COVID-19 in an immunocompromised patient temporarily responsive to two courses of Remdesivir therapy. J Infect Dis. (2020) 222:1103–7. doi: 10.1093/infdis/jiaa446
76. Honjo, K, Russell, RM, Li, R, Liu, W, Stoltz, R, Tabengwa, EM, et al. Convalescent plasma-mediated resolution of COVID-19 in a patient with humoral immunodeficiency. Cell Reports Medicine. (2021) 2:100164. doi: 10.1016/j.xcrm.2020.100164
77. Hughes, CM, Gregory, GP, Pierce, AB, Druce, JD, Catton, M, Chong, B, et al. Clinical illness with viable severe acute respiratory coronavirus virus 2 (SARS-CoV-2) virus presenting 72 days after infection in an immunocompromised patient. Infect Control Hosp Epidemiol. (2022) 43:820–2. doi: 10.1017/ice.2021.120
78. Jassem, J, Marek-Trzonkowska, NM, Smiatacz, T, Arcimowicz, Ł, Papak, I, Jassem, E, et al. Successful treatment of persistent SARS-CoV-2 infection in a B-cell depleted patient with activated cytotoxic T and NK cells: a case report. Int J Mol Sci. (2021) 22:10934. doi: 10.3390/ijms222010934
79. Karaolidou, F, Loutsidi, N-E, Mellios, Z, Jahaj, E, Eleftheriou, K, Pagoni, M, et al. Convalescent plasma therapy in an immunocompromised patient with multiple COVID-19 flares: a case report. Respirology Case Reports. (2021) 9:e0858. doi: 10.1002/rcr2.858
80. Khatamzas, E, Antwerpen, MH, Rehn, A, Graf, A, Hellmuth, JC, Hollaus, A, et al. Accumulation of mutations in antibody and CD8 T cell epitopes in a B cell depleted lymphoma patient with chronic SARS-CoV-2 infection. Nat Commun. (2022) 13:5586. doi: 10.1038/s41467-022-32772-5
81. Lancman, G, Mascarenhas, J, and Bar-Natan, M. Severe COVID-19 virus reactivation following treatment for B cell acute lymphoblastic leukemia. J Hematol Oncol. (2020) 13:131. doi: 10.1186/s13045-020-00968-1
82. Librizzi, G, Modi, V, and Lier, AJ. SARS-CoV-2 persistence in immunocompromised patients requiring treatment with convalescent plasma: a case report. Cureus. (2024) 16:e54564. doi: 10.7759/cureus.54564
83. Malsy, J, Veletzky, L, Heide, J, Hennigs, A, Gil-Ibanez, I, Stein, A, et al. Sustained response after Remdesivir and convalescent plasma therapy in a B-cell–depleted patient with protracted coronavirus disease 2019 (COVID-19). Clin Infect Dis. (2020) 73:e4020–4. doi: 10.1093/cid/ciaa1637
84. Martínez-Chinchilla, C, Vazquez-Montero, L, Palazón-Carrión, N, Fernández-Román, IM, López-Barba, J, de la Cruz-Merino, L, et al. Persistence of SARS-CoV-2 infection in severely immunocompromised patients with complete remission B-cell lymphoma and anti-CD20 monoclonal antibody therapy: a case report of two cases. Front Immunol. (2022) 13:860891. doi: 10.3389/fimmu.2022.860891
85. Martinot, M, Jary, A, Fafi-Kremer, S, Leducq, V, Delagreverie, H, Garnier, M, et al. Emerging RNA-dependent RNA polymerase mutation in a Remdesivir-treated B-cell Immunodeficient patient with protracted coronavirus disease 2019. Clin Infect Dis. (2020) 73:e1762–5. doi: 10.1093/cid/ciaa1474
86. McKemey, E, Shields, AM, Faustini, SE, Hill, HJ, Barnskaya, A, Stamataki, Z, et al. Resolution of persistent COVID-19 after convalescent plasma in a patient with B cell aplasia. J Clin Immunol. (2021) 41:926–9. doi: 10.1007/s10875-021-00996-7
87. Moore, JL, Ganapathiraju, PV, Kurtz, CP, and Wainscoat, B. A 63-year-old woman with a history of non-Hodgkin lymphoma with persistent SARS-CoV-2 infection who was seronegative and treated with convalescent plasma. Am J Case Rep. (2020) 21:e927812. doi: 10.12659/AJCR.927812
88. Moutinho-Pereira, S, Calisto, R, Sabio, F, and Guerreiro, L. High-titre convalescent plasma therapy for an immunocompromised patient with systemic lupus erythematosus with protracted SARS-CoV-2 infection. BMJ Case Rep. (2021) 14:e244853. doi: 10.1136/bcr-2021-244853
89. Niu, A, McDougal, A, Ning, B, Safa, F, Luk, A, Mushatt, DM, et al. COVID-19 in allogeneic stem cell transplant: high false-negative probability and role of CRISPR and convalescent plasma. Bone Marrow Transplant. (2020) 55:2354–6. doi: 10.1038/s41409-020-0972-8
90. Ordaya, EE, Abu Saleh, OM, Stubbs, JR, and Joyner, MJ. Vax-plasma in patients with refractory COVID-19. Mayo Clin Proc. (2022) 97:186–9. doi: 10.1016/j.mayocp.2021.11.001
91. Ormazabal Vélez, I, Induráin Bermejo, J, Espinoza Pérez, J, Imaz Aguayo, L, Delgado Ruiz, M, and García-Erce, JA. Two patients with rituximab associated low gammaglobulin levels and relapsed covid-19 infections treated with convalescent plasma. Transfus Apher Sci. (2021) 60:103104. doi: 10.1016/j.transci.2021.103104
92. Reuken, PA, Stallmach, A, Pletz, MW, Brandt, C, Andreas, N, Hahnfeld, S, et al. Severe clinical relapse in an immunocompromised host with persistent SARS-CoV-2 infection. Leukemia. (2021) 35:920–3. doi: 10.1038/s41375-021-01175-8
93. Rnjak, D, Ravlić, S, Šola, AM, Halassy, B, Šemnički, J, Šuperba, M, et al. COVID-19 convalescent plasma as long-term therapy in immunodeficient patients? Transfus Clin Biol. (2021) 28:264–70. doi: 10.1016/j.tracli.2021.04.004
94. Rodriguez-Pla, A, Vikram, HR, Khalid, V, and Wesselius, LJ. COVID-19 pneumonia in a patient with granulomatosis with polyangiitis on rituximab: case-based review. Rheumatol Int. (2021) 41:1509–14. doi: 10.1007/s00296-021-04905-4
95. Schenker, C, Hirzel, C, Walti, LN, Zeerleder, SS, Andres, M, Ramette, A, et al. Convalescent plasma and remdesivir for protracted COVID-19 in a patient with chronic lymphocytic leukaemia: a case report of late relapse after rapid initial response. Br J Haematol. (2022) 196:e27–9. doi: 10.1111/bjh.17806
96. Sepulcri, C, Dentone, C, Mikulska, M, Bruzzone, B, Lai, A, Fenoglio, D, et al. The longest persistence of viable SARS-CoV-2 with recurrence of viremia and relapsing symptomatic COVID-19 in an immunocompromised patient-a case study. Open Forum Infect Dis. (2021) 8:ofab217. doi: 10.1093/ofid/ofab217
97. Seth-Smith, H, Vesenbeckh, S, Egli, A, and Ott, S. SARS-CoV-2 in an immunocompromised host: convalescent plasma therapy and viral evolution elucidated by whole genome sequencing. BMJ Case Rep. (2023) 16:e255255. doi: 10.1136/bcr-2023-255255
98. Spinicci, M, Mazzoni, A, Coppi, M, Antonelli, A, Salvati, L, Maggi, L, et al. Long-term SARS-CoV-2 asymptomatic carriage in an immunocompromised host: clinical, immunological, and Virological implications. J Clin Immunol. (2022) 42:1371–8. doi: 10.1007/s10875-022-01313-6
99. Szwebel, T-A, Veyer, D, Robillard, N, Eshagh, D, Canoui, E, Bruneau, T, et al. Usefulness of plasma SARS-CoV-2 RNA quantification by droplet-based digital PCR to monitor treatment against COVID-19 in a B-cell lymphoma patient. Stem Cell Rev Rep. (2021) 17:296–9. doi: 10.1007/s12015-020-10107-5
100. Taha, Y, Wardle, H, Evans, AB, Hunter, ER, Marr, H, Osborne, W, et al. Persistent SARS-CoV-2 infection in patients with secondary antibody deficiency: successful clearance following combination casirivimab and imdevimab (REGN-COV2) monoclonal antibody therapy. Ann Clin Microbiol Antimicrob. (2021) 20:85. doi: 10.1186/s12941-021-00491-2
101. Tomisti, L, Angelotti, F, Lenzi, M, Amadori, F, Sarteschi, G, Porcu, A, et al. Efficacy of convalescent plasma to treat long-standing COVID-19 in patients with B-cell depletion. Life. (2023) 13:1266. doi: 10.3390/life13061266
102. Villaseñor-Echavarri, R, Gomez-Romero, L, Martin-Onraet, A, Herrera, LA, Escobar-Arrazola, MA, Ramirez-Vega, OA, et al. SARS-CoV-2 genome variations in viral shedding of an immunocompromised patient with non-Hodgkin’s lymphoma. Viruses. (2023) 15:377. doi: 10.3390/v15020377
103. Wright, Z, Bersabe, A, Eden, R, Bradley, J, and Cap, A. Successful use of COVID-19 convalescent plasma in a patient recently treated for follicular lymphoma. Clin Lymphoma Myeloma Leuk. (2021) 21:66–8. doi: 10.1016/j.clml.2020.06.012
104. Zhu, W, Xie, T, Xu, M, Chen, R, and Zhang, T. Migratory pulmonary infiltrates in a B-cell-depleted COVID-19 patient. Infect Drug Resist. (2023) 16:7205–8. doi: 10.2147/IDR.S439795
105. Zimmerli, A, Monti, M, Fenwick, C, Eckerle, I, Beigelman-Aubry, C, Pellaton, C, et al. Case report: stepwise anti-inflammatory and anti-SARS-CoV-2 effects following convalescent plasma therapy with full clinical recovery. Front Immunol. (2021) 12:613502. doi: 10.3389/fimmu.2021.613502
106. Schmidt, F, Weisblum, Y, Rutkowska, M, Poston, D, DaSilva, J, Zhang, F, et al. High genetic barrier to SARS-CoV-2 polyclonal neutralizing antibody escape. Nature. (2021) 600:512–6. doi: 10.1038/s41586-021-04005-0
107. Joyner, MJ, Carter, RE, Senefeld, JW, Klassen, SA, Mills, JR, Johnson, PW, et al. Convalescent plasma antibody levels and the risk of death from Covid-19. N Engl J Med. (2021) 384:1015–27. doi: 10.1056/NEJMoa2031893
108. Dequidt, T, Richier, Q, Louapre, C, Ader, F, Merad, Y, Lauwerier, N, et al. Convalescent plasma in patients receiving rituximab or ocrelizumab for multiple sclerosis or neuromyelitis optica spectrum disorder with Covid-19: a multicenter retrospective study. Int J Infect Dis. (2025) 151:107323. doi: 10.1016/j.ijid.2024.107323
109. Li, Y, Ashcroft, T, Chung, A, Dighero, I, Dozier, M, Horne, M, et al. Risk factors for poor outcomes in hospitalised COVID-19 patients: a systematic review and meta-analysis. J Glob Health. (2021) 11:10001. doi: 10.7189/jogh.11.10001
110. Madelon, N, Lauper, K, Breville, G, Sabater Royo, I, Goldstein, R, Andrey, DO, et al. Robust T-cell responses in anti-CD20-treated patients following COVID-19 vaccination: a prospective cohort study. Clin Infect Dis. (2022) 75:e1037–45. doi: 10.1093/cid/ciab954
111. Gadani, SP, Reyes-Mantilla, M, Jank, L, Harris, S, Douglas, M, Smith, MD, et al. Discordant humoral and T cell immune responses to SARS-CoV-2 vaccination in people with multiple sclerosis on anti-CD20 therapy. EBioMedicine. (2021) 73:103636. doi: 10.1016/j.ebiom.2021.103636
112. Mozaffari, E, Chandak, A, Gottlieb, RL, Chima-Melton, C, Read, SH, Jiang, H, et al. Remdesivir reduced mortality in immunocompromised patients hospitalized for COVID-19 across variant waves: findings from routine clinical practice. Clin Infect Dis. (2023) 77:1626–34. doi: 10.1093/cid/ciad460
113. Zong, K, Xu, L, Luo, C, Luo, C, Liu, B, Chen, J, et al. Paxlovid reduces the 28-day mortality of patients with COVID-19: a retrospective cohort study. BMC Infect Dis. (2024) 24:767. doi: 10.1186/s12879-024-09482-y
114. Larkey, NE, Ewaisha, R, Lasho, MA, Roforth, MM, Granger, D, Jerde, CR, et al. Limited correlation between SARS-CoV-2 serologic assays for identification of high-titer COVID-19 convalescent plasma using FDA thresholds. Microbiol Spectr. (2022) 10:e0115422. doi: 10.1128/spectrum.01154-22
Keywords: convalescent plasma, COVID-19, B-cell depletion, anti-CD20 therapy, immunodeficiency, SARS-CoV-2
Citation: Zaremba S, Focosi D, Pruter WW, Franchini M, Collantes Hoyos DB, Cruciani M, Miller AJ, Ripoll JG, Casadevall A, Tulledge-Scheitel SM, Rufer N, Hueso T, Juskewitch JE, van Buskirk CM, Ioannou P, Lanza F, Razonable RR, Magyari F, Pinczés LI, Ganesh R, Denkinger CM, Hurt RT, Janssen M, Stubbs JR, Müller-Tidow C, Winters JL, Holm K, Parikh SA, Simeunovic G, Kay NE, Rijnders BJ, Wright SR, Issa N, Chaussade H, Carter RE, Schroeder DR, Senefeld JW and Joyner MJ (2025) COVID-19 convalescent plasma for B-cell depleted patients: a systematic review and individual patient data meta-analysis. Front. Med. 12:1658593. doi: 10.3389/fmed.2025.1658593
Edited by:
Deborah Fuller, University of Washington, United StatesReviewed by:
Johannes Fessler, Medical University of Graz, AustriaJanmejay Singh, Translational Health Science and Technology Institute (THSTI), India
Copyright © 2025 Zaremba, Focosi, Pruter, Franchini, Collantes Hoyos, Cruciani, Miller, Ripoll, Casadevall, Tulledge-Scheitel, Rufer, Hueso, Juskewitch, van Buskirk, Ioannou, Lanza, Razonable, Magyari, Pinczés, Ganesh, Denkinger, Hurt, Janssen, Stubbs, Müller-Tidow, Winters, Holm, Parikh, Simeunovic, Kay, Rijnders, Wright, Issa, Chaussade, Carter, Schroeder, Senefeld and Joyner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael J. Joyner, am95bmVyLm1pY2hhZWxAbWF5by5lZHU=; Jonathon W. Senefeld, c2VuZWZlbGRAaWxsaW5vaXMuZWR1
†These authors share first authorship
‡These authors share senior authorship