Abstract
Background:
Intractable hiccups (IH) have diverse causes, including central lesions (e.g., stroke, intracranial injury) and peripheral triggers (e.g., gastrointestinal disease, tumors, chemotherapy, cirrhosis, surgery). IH significantly impairs quality of life, delays recovery, and increases the risk of complications. Acupuncture is frequently used as a complementary or alternative therapy for IH in China, but no prior study has systematically compared different acupuncture modalities within a unified framework.
Objective:
To assess the comparative effectiveness and safety of multiple acupuncture therapies for treating IH via network meta-analysis.
Methods:
RCTs on acupuncture for IH published from January 2015 to January 2025 were retrieved from eight databases and four clinical trial registries. Study quality was assessed via the Cochrane risk of bias tool. Meta-analysis was performed with Stata software.
Results:
The 41 included studies were all conducted in China and published in Chinese and no studies or data from other countries. The studies covered a total of 3,060 patients with IH and 15 types of acupuncture-related intervention measures. Manual acupuncture combined with acupoint injection showed the highest efficacy in improving both total effective rate and quality of life. Electroacupuncture combined with conventional medicine was most effective in reducing hiccup symptoms. Among monotherapies, auricular acupressure achieved the greatest improvement in total effective rate. All acupuncture therapies demonstrated acceptable safety, with no serious adverse events reported.
Conclusion:
Acupuncture appears effective and safe for treating IH in China. Combination therapies outperformed monotherapies, with manual acupuncture plus acupoint injection showing the greatest efficacy and acceptable safety. Electroacupuncture with conventional medication was most effective for symptom relief. However, limitations of linguistic and geographical scope, potential favorable bias and uneven methodological quality warrant further high-quality international studies.
Systematic review registration:
https://www.crd.york.ac.uk/prospero/, identifier: CRD42025638314.
1 Introduction
Hiccups are a common but frequently underestimated symptom. Most people experience occasional hiccups, especially after overeating or consuming cold drinks. These episodes typically last from a few minutes to several hours and are considered acute and self-limiting, requiring no medical intervention. However, when hiccups persist for more than 48 h or occur in patients with underlying conditions, they may indicate a potential pathological process (1). This condition is referred to as intractable hiccups (IH) and is most commonly associated with gastrointestinal disorders (62.5%) and central nervous system diseases (33.3%) (2, 3). From a mechanistic perspective, the “hiccup reflex arc” involves afferent, central, and efferent components (4, 5). The afferent pathway consists of the phrenic nerve, vagus nerve, and sympathetic fibers arising from T6 to T12 (6, 7). The efferent pathway includes the phrenic nerve, intercostal nerves, the anterior scalene muscle, and the recurrent laryngeal branch of the vagus nerve (3). The effectors involved are the diaphragm, intercostal muscles, and anterior scalene muscles (8). The central nervous system regions implicated in the hiccup response include the cervical spinal cord segments (C3–C5), the medullary brainstem near the respiratory centers, the reticular formation, and the hypothalamus (5, 9, 10). The efferent response of the reflex is transmitted via the phrenic nerve to the diaphragm, resulting in diaphragmatic contraction and the characteristic hiccup.
Any disturbance affecting the afferent, central, or efferent components of the reflex arc can lead to hiccups. Owing to the long trajectory of the afferent and efferent nerves and the diffuse central process of the hiccup reflex arc (11) and considering the participation of anatomical structures with different main functions, it is not surprising that hiccups are a complication of a large number of various underlying diseases. Central causes include conditions such as stroke, brain tumors, and intracranial injury (4). Peripheral neurological disorders, such as gastrointestinal neurosis, gastritis, liver cirrhosis, and fulminant hepatitis, may also disrupt neurotransmitter balance within the hiccup reflex arc (3, 12). Additionally, ~3.9%−4.5% of cancer patients receiving chemotherapy, as well as some perioperative patients, experience hiccups (13). This may be associated with factors such as preoperative anxiety, the use of sedatives or anesthetics during surgery, the presence of tumors located near the diaphragm or phrenic nerve, and oropharyngeal intubation (14, 15).
The potential hazards of IH must not be underestimated. When incessant hiccups fail to resolve and interfere with oral intake, they can significantly disrupt a patient's nutritional status, emotional wellbeing, and sleep quality (16–18). Persistent hiccups may also delay recovery, prolong hospitalization, and increase the risk of aspiration pneumonia, respiratory distress and malnutrition (16, 17, 19, 20). Perhaps due to the prevalence of IH in both internal medicine and surgery, as well as in oncology and intense care units, and because it often complicates existing treatments, in the absence of agreed-upon management guidelines, chlorpromazine is currently the only FDA-approved medication for hiccups, while other agents such as baclofen and metoclopramide are used off-label, often limited by adverse effects including sedation and extrapyramidal symptoms (4).
Against this backdrop, acupuncture—a nonpharmacological procedure rooted in traditional Chinese medicine (TCM)—has garnered considerable attention for its promising potential in treating hiccups. Several randomized controlled trials have demonstrated its effectiveness in reducing the duration and frequency of hiccup episodes (21–24), and it appears to avoid the above adverse effects of conventional drugs (25, 26). Moretto et al. (1) compared different acupuncture techniques for persistent and intractable hiccups, but included only four studies—likely due to limited access to Chinese databases—and could not perform a meta-analysis due to methodological heterogeneity. In contrast, three meta-analyses confirmed the beneficial effects of acupuncture in cancer-related and poststroke hiccups (14, 27, 28). However, these studies are limited to specific populations and often include cases of acute hiccups lasting < 48 h. As a result, they do not offer a comprehensive assessment of IH across diverse etiologies. The heterogeneity of acupuncture and its technical variants, such as electroacupuncture (EA), transcutaneous electrical acupoint stimulation (TEAS), acupoint injection (AI), auricular acupressure (AA), etc. further complicates clinical decision-making. Owing to the relative scarcity of earlier studies, the level of evidence supporting acupuncture was previously low. In contrast, the number of high-quality studies on these techniques has gradually increased in recent years. To date, no study has systematically compared the efficacy and safety of different acupuncture modalities for intractable hiccups in a unified analytic framework. This study seeks to fill that gap by synthesizing direct and indirect evidence, providing a ranking of acupuncture interventions, and guiding future practice and research.
2 Materials and methods
This review was reported following the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) for Network Meta-Analyses (NMA) (29) and was registered on the International Prospective Register of Systematic Reviews (PROSPERO) website (https://www.crd.york.ac.uk/prospero/) in January 2025 with the registration number CRD42025638314.
2.1 Inclusion and exclusion criteria
2.1.1 Type of participants
Adult patients 18 years or above with a clinical diagnosis of intractable hiccups (hiccups lasting more than 48 h), regardless of gender, etiology, ethnic group, and severity.
2.1.2 Types of interventions
The expected conventional acupuncture approaches include manual acupuncture (MA), moxibustion (Mox), electroacupuncture (EA), warm acupuncture (WA), auricular acupressure (AA), acupoint injection (AI), and transcutaneous electrical acupoint stimulation (TEAS), among others. The aforementioned acupuncture approaches may be used individually or in combination, regardless of the needling technique or acupoint selection. In addition, acupuncture combined with other therapies, such as Chinese herbal medicine (CHM) or conventional medications (CM), was also included within the scope of our analysis.
2.1.3 Types of comparisons
Sham acupuncture (SA), CM, waiting list (WL), or acupuncture methods different from those used in the intervention group were considered control groups.
2.1.4 Types of outcome indicators
The primary outcome is Total Effective Rate (TER), measured according to two common standards (30, 31), as cure rate + marked effective rate + remission rate. This will be judged by calculating clinical symptom scores, including parameters such as hiccup duration and frequency, etc. Secondary outcomes included the Hiccup Symptom Score (HSS), quality of life assessments (covering three items: diet, sleep, and mental status), and the incidence of adverse events.
2.1.5 Type of study
Randomized controlled trials (RCTs) in Chinese and English were included.
2.1.6 Exclusion criteria
-
a. Patients with hiccups lasting < 48 h.
-
b. Special acupuncture techniques such as scalp acupuncture, ocular acupuncture, wrist-ankle acupuncture, acupoint application, finger acupuncture, bee venom acupuncture, and bloodletting therapy.
-
c. Studies in which three or more types of therapies were used simultaneously.
-
d. Control groups that received the same type of acupuncture as the intervention group, differing only in needling techniques or selected acupoints.
-
e. Outcome indicators not related to IH.
-
f. Studies with unclear randomization methods or non-RCTs.
-
g. Studies with a treatment group sample size of 10 or fewer participants.
2.2 Information sources and search strategy
Two reviewers independently performed a comprehensive search of the following electronic databases: four English databases [PubMed, Embase, Cochrane Library, and Web of Science (WOS)] and four Chinese databases [China National Knowledge Infrastructure (CNKI), SinoMed, CQVIP, and Wanfang Database]. Additionally, four clinical trial registration platforms were searched: the World Health Organization International Clinical Trials Registry Platform (http://www.who.int/ictrp/en/), the Chinese Clinical Trial Registry (https://www.chictr.org.cn/), Clinical Trials.gov (https://www.clinicaltrials.govclinicaltrials.gov/) and the International Traditional Medicine Clinical Trial Registry (http://itmctr.ccebtcm.org.cn/) for acupuncture therapies for IH from January 2015 to January 2025. The following terms were imposed: (a) clinical conditions: hiccup, hiccough, singultus, etc.; (b) acupuncture therapy-related words: acupuncture, moxibustion, auricular acupressure, electroacupuncture, acupoint injection, etc.; and (c) trial type: an RCT. The terms “and” and “or” were combined between the search terms. Search strategies for these sources are shown in the Supplementary material.
2.3 Literature screening and data extraction
The exclusion of duplicate studies was performed in Endnote V.20 software, and then preliminary screening was performed by reading the title and abstract. After that, the full texts were further screened to exclude studies that did not meet the inclusion criteria. For data extraction, two researchers (LD and JC) separately conducted data extraction on the basis of the inclusion and exclusion criteria. If there was any disagreement, the third researcher (HZ) would make a final decision. The data extraction content included title, author, publication year and month, sample size, diagnostic criteria, interventions of treatment group and control group, dosage, course of treatment, and outcome indicators, among others.
2.4 Evaluation of the risk of bias
The quality evaluation was performed by two separate researchers (YZ and XT) using RCT Bias Risk Assessment Tool of the Cochrane System Review Manual Version 5.1.0, and a third researcher (HZ) would assist in judging the divergence between the two researchers. The evaluation items included random sequence generation, allocation concealment, blinding of patients and investigators, blinding of outcome evaluators, incomplete result data, selective reporting, and other biases.
2.5 Assessing certainty of the evidence
The Confidence in Network Meta-Analysis (CINeMA) system, a free and open-source CINeMA software (https://cinema.ispm.unibe.ch/), was used to assess credibility of results from network meta-analyses, which is based on the Grading of Recommendations Assessment, Development and Evaluation (GRADE)s and simplifies the evaluation process (32, 33). Six domains were evaluated, including: (a) within- study bias, (b) reporting bias, (c) indirectness, (d) imprecision, (e) heterogeneity, and (f) incoherence. Each domain was rated at 3 levels “no concerns,” “some concerns,” or “major concerns.”
2.6 Statistical analysis
Pairwise meta-analyses were conducted using Stata software V.17.0. The I2 statistic and P-value were used to identify and measure the heterogeneity among the studies. If P ≥ 0.05 and I2 < 50%, heterogeneity was considered not significant, and a fixed-effects model was used for meta-analysis. If P < 0.05 and I2 ≥ 50%, significant heterogeneity was assumed, and a random effects model was applied. In addition, for meta-analyses involving three-arm RCTs, the arms were separated into two-group comparisons for all possible pairwise combinations. For continuous variables, standardized mean difference (SMD) was used as the summary statistic, while risk ratio (RR) was used for dichotomous outcomes. Both effect measures were reported with 95% confidence intervals (CIs). A result was considered statistically significant when the 95% CI for RR did not include 1 or the 95% CI for SMD did not include 0.
The NMA was conducted within a frequentist framework using the network and mvmeta packages in Stata software. A network plot was generated to illustrate the comparisons between interventions, where the size of each node represented the sample size and the thickness of connecting lines indicated the number of studies contributing to each comparison. The surface under the cumulative ranking curve (SUCRA) was calculated to rank the probabilities of each intervention being the most effective. A SUCRA value closer to 100% indicates a higher probability of the intervention being the most effective. Additionally, publication bias and small-study effects were assessed using comparison-adjusted funnel plots. Finally, a two-outcomes cluster ranking plot was generated to illustrate the combined performance of each intervention in terms of both efficacy and safety.
3 Results
3.1 Literature screening results
A total of 4,119 studies were retrieved, and 41 RCTs, including 3,060 patients, were ultimately included (15, 21–26, 34–67) after the preliminary screening and rescreening process. The literature screening process is shown in Figure 1.
Figure 1

PRISMA flow diagram of the study selection process.
3.2 Characteristics of the included studies
All 41 included studies were conducted in China and published in Chinese. Among them, only two were three-arm trials (24, 65), while the rest were two-arm trials. The five most frequently used treatment modalities in the intervention groups were MA+AI (21, 38, 49, 58, 62, 65, 67), MA (26, 40, 43, 44, 47, 48, 54), MA+CHM (34, 39, 45, 63, 64), EA (24, 36, 50, 53, 55), and MA+CM (15, 37, 57, 60, 66). In contrast, AI+CHM (35), EA+CM (59), AA (56), and TEAS+AI (42) were the least frequently used methods. Except for one study, all included trials reported total effective rate (TER). Eleven studies reported HSS (21, 23, 25, 26, 48, 51, 52, 57, 59, 62, 67); nine studies assessed diet, sleep, and mental status scores (23, 25, 38, 43, 44, 47, 48, 52, 62); and 17 studies reported the occurrence of adverse events (21, 23–26, 38, 43, 47, 49, 52, 53, 56, 61–63, 65, 67). Due to the very limited number of studies reporting outcomes on hiccup duration and frequency and the considerable heterogeneity in intervention types, substantial between-study heterogeneity was observed. Consequently, neither pairwise meta-analysis nor NMA was feasible for these outcomes, and no further description or analysis was performed. Detailed characteristics of the included studies are presented in Table 1.
Table 1
| Studies | Primary diseases* | Allocation ratio | Sample size | Age | Gender: M/F | (A) | (B) | (C) | Duration of treatment | Efficacy and safety criteria | Main results |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Treatment group | Control group I | Control group II | |||||||||
| Wang 2024 | Stroke | 1:1 | 86 | A:60.83 ± 5.82 B:61.37 ± 5.07 |
A:24/19 B:27/16 | MA on Neiguan (PC 6), Cuanzhu (BL 2), with stimulation 1 × /day +(B) | AI [100 mg × 1/day dose of phenobarbital sodium injection on Zusanli (ST 36)] | / | 7 days | 1.Total effective rate; 2.Hiccup symptom score; 3.Adverse events |
1.A>B; 2.A>B; 3.A=B |
| Xu 2023 | Severe craniocerebral injury | 1:1 | 60 | A:47.86 ± 5.10 B:48.20 ± 4.98 | A:19/11 B:18/12 | MA on Zhongwan (RN 12), Neiguan (PC 6), Zusanli (ST 36), with stimulation 1 × /day +(B) | CM (10 mg × 1/day dose of metoclopramide hydrochloride injection for intramuscular injection) | / | 3 days | Total effective rate | A>B |
| Li 2022 | NR | 1:1:1 | 120 | A:49.68 ± 13.82 B:51.80 ± 11.80 C:53.93 ± 11.87 | A:38/2 B:36/4 C:38/2 | MA on Yingxiang (LI 20), Jingming (BL 1) Zusanli (ST 36), with stimulation 1 × /day +(C) | MA on Zhongwan (RN 12), Danzhong (RN 17), Geshu (BL 17), Neiguan (PC 6), Zusanli (ST 36), with stimulation 1 × /day | AI [1 ml/day dose of vitamin B6 and B12 injections on Zusanli (ST 36)] | 3 days | 1.Total effective rate; 2.Adverse events |
1.A>B>C 2.A=B=C |
| Qin 2022 | After cardiothoracic surgery | 1:1:1 | 178 | A:52.61 ± 15.54 B:53.22 ± 16.37 C:52.76 ± 15.54 | A:47/23 B:46/22 C:28/12 | EA on Neiguan (PC 6), Zusanli (ST 36), with continuous wave and low frequency stimulation 1 × /day | WA on Zhongkui (EX-UE4) with stimulation 1 × /day | CM (25–50 mg × 1/day dose of chlorpromazine hydrochloride injection for intramuscular injection) | 5 days | 1.Total effective rate; 2.Adverse events; |
1.A>C>B 2.A=B>C |
| Fan 2021 | After chemotherapy for lung carcinoma | 1:1 | 63 | A:59.22 ± 6.10 B:57.61 ± 7.58 | A:27/5 B:25/6 | AA on ear center (HX1), Shenmen (TF4), heart (CO15), with stimulation 3 × /day;MA on Neiguan (PC 6), Zusanli (ST 36), Cuanzhu (BL 2), with stimulation 1 × /day | CM (10 mg × 1/day dose of metoclopramide hydrochloride injection for intramuscular injection) | / | 7 days | 1.Total effective rate; 2.Hiccup symptom score 3.Dietary status score 4.Sleep status score 5.Mental status score 6.Adverse events |
1.A>B; 2.A>B 3. A>B 4. A>B 5. A>B 6. A=B |
| Huang 2021 | After radiotherapy or chemotherapy for malignant tumors | 1:1 | 67 | A:32–78 B:35–75 | A:19/15 B:17/16 | MA on Geshu (BL 17), Danzhong (RN 17), Tiantu (RN 22), Yifeng (SJ 17), Zhongwan (RN 12), Neiguan (PC 6), Zusanli (ST 36), Gongsun (SP 4), Cuanzhu (BL 2), with stimulation 1 × /day +(B) | CM (10 mg × 1/day dose of metoclopramide hydrochloride injection for intramuscular injection) | / | 7 days | Total effective rate | A>B |
| Luo 2021 | Stroke | 1:1 | 86 | A:44.13 ± 0.19 B:43.21 ± 0.15 | A:20/23 B:21/22 | TEAS on Neiguan (PC 6), Zhongwan (RN 12), Zusanli (ST 36), Geshu (BL 17), with 15 Hz stimulation 1 × /day; CHM (150 ml × 3/day dose of herbal decoction for oral) | CM [Two arms: (1) 5 mg × 3/day dose of metoclopramide tablets for oral. (2) 50 mg × 3/day dose of eperisone hydrochloride tablets for oral.] | / | 7 days | 1. Total effective rate; 2. Adverse events |
1.A>B; 2.A>B |
| Ou yang 2021 | NR | 1:1 | 122 | A:46.11 ± 3.09 B:46.74 ± 3.11 | A:34/27 B:32/29 | AI [10 mg/day dose of metoclopramide hydrochloride injection on Zusanli (ST 36)]+(B) | MA on Neiguan (PC 6), Zhongwan (RN 12), Cuanzhu (BL 2), Zusanli (ST 36), Shuigou (DU 26), with stimulation 1 × /day | / | 2 weeks | 1. Total effective rate 2. Hiccup symptom score 3. Dietary status score 4. Sleep status score 5. Mental status score 6. Adverse events |
1.A>B; 2. A>B 3. A>B 4. A>B 5. A>B 6. A=B |
| Wang 2021 | NR | 1:1 | 86 | A:42.50 ± 6.30 B:42.80 ± 5.60 | A:21/22 B:23/20 | MA on Tiantu (RN 22), Neiguan (PC 6), Zhongwan (RN 12), Zusanli (ST 36), Taichong (LR 3), with stimulation 1 × /day; CHM (200 ml × 1/day dose of herbal decoction for oral) | CM [(Two arms: (1) 0.6 mg × 2/day dose of Scopolamine injection for intramuscular injection; (2) 50 mg × 1/day dose of chlorpromazine hcl tablet for oral)] | / | 5 days | 1. Total effective rate 2. Adverse events |
1. A>B 2. A=B |
| Yang 2021 | After radiotherapy or chemotherapy for malignant tumors | 1:1 | 60 | A:54.0 ± 2.1 B:47.0 ± 1.9 | A:16/14 B:17/13 | MA on Cuanzhu (BL 2), Yuyao (EX-HN4), Neiguan (PC 6), Waiguan (SJ 5), Zusanli (ST 36), Yinlingquan (SP 9), with stimulation 1 × /day+(B) | CHM (200 ml × 2/day dose of herbal decoction for oral) | / | 7 days | Total effective rate | A>B |
| Gan 2020 | After transcatherter arterial chemoembolization (TACE) for hepatoma | 1:1 | 82 | A:49.23 ± 4.75 B:48.35 ± 5.12 | A:30/11 B:28/13 | MA on Dazhui (DU 14), Neiguan (PC 6), Danzhong (RN 17), Zhongwan (RN 12), Zusanli (ST 36), Shenque (RN 8), with stimulation 1 × /day+(B) | CM (10 mg × 2/day dose of metoclopramide hydrochloride injection for intramuscular injection) | / | 7 days | Total effective rate | A>B |
| Liu 2020 | NR | 1:1 | 66 | A:38.66 ± 10.15 B:37.72 ± 9.56 | A:15/18 B:16/17 | AI [5–10 mg/day dose of racemic anisodamine hydrochloride injection on cervical Jiaji (C3-C5)]+(B) | MA on Neiguan (PC 6), Zhongwan (RN 12), Zusanli (ST 36), Danzhong (RN 17), Geshu (BL 17), with stimulation 1 × /day | / | 10 days | 1.Total effective rate 2.Adverse events |
1.A>B 2.A=B |
| Lu 2020 | NR | 1:1 | 86 | A:54.24 ± 9.22 B:53.68 ± 9.43 | A:21/22 B:22/21 | EA on Geshu (BL 17), Weishu (BL 21), Neiguan (PC 6), Zusanli (ST 36), with dilatational wave stimulation 1 × /day+(B) | CM (50 mg × 3/day dose of itopride hydrochloride tablets for oral) | / | 7 days | 1.Total effective rate 2.Hiccup symptom score |
1.A>B 2.A>B |
| Shen 2019 | NR | 1:1 | 60 | A:38.7 ± 10.7 B:38.5 ± 10.9 | A:18/12 B:17/13 | MA on Geshu (BL 17), Neiguan (PC 6), Zhongwan (RN 12), Zusanli (ST 36), Tiantu (RN 22), Danzhong (RN 17), with stimulation 1 × /day | CM (10 mg × 2/day dose of Racemic anisodamine hydrochloride injection for intramuscular injection) | / | 7 days | Total effective rate | A>B |
| Gao 2019 | NR | 1:1 | 60 | A:43.4 ± 13.75 B:44.8 ± 13.87 | A:17/13 B:16/14 | EA on Cuanzhu (BL 2) with dilatational wave and high frequency stimulation 1 × /day | CM (5 mg × 2/day dose of Baclofen tablets for oral) | / | 5 days | Total effective rate | A>B |
| Liu 2019 (1) | Traumatic brain injury, gastric surgery, stroke and fractured ribs | 1:1 | 82 | A:58.72 ± 10.65 B:59.01 ± 10.40 | A:27/14 B:29/12 | AA on ear center (HX1), Shenmen (TF4), stomach (CO4), sympathetic nerve (AH6a), subcortex (AT4), spleen (CO13), triple energizer (CO17), lung (CO14), with stimulation 3 × /day | CM (25 mg × 1/day dose of chlorpromazine hydrochloride injection for intramuscular injection) | / | 12 days | 1.Total effective rate 2.Adverse events |
1.A>B 2.A>B |
| Liu 2019 (2) | Stroke | 1:1 | 50 | A:61.02 ± 3.16 B:60.77 ± 3.09 |
A:13/13 B:13/11 | MA on Danzhong (RN 17), Neiguan (PC 6), Zhongwan (RN 12), Shuigou (DU 26), Cuanzhu (BL 2), Zusanli (ST 36), with stimulation 1 × /day | CM (25 mg × 3/day dose of chlorpromazine hydrochloride tablets for oral) | / | 10 days | 1.Total effective rate 2.Hiccup symptom score 3.Adverse events |
1.A>B 2.A>B 3.A=B |
| Liu 2019 (3) | Stroke | 1:1 | 60 | A:57.22 ± 6.57 B:56.71 ± 6.09 | A:19/11 B:17/13 | MA on Cuanzhu (BL 2), Neiguan (PC 6), Zhongwan (RN 12), Zusanli (ST 36), Taichong (LR 3), with stimulation 1 × /day; AA on ear center (HX1), Shenmen (TF4), sympathetic nerve (AH6a), stomach (CO4), Liver (CO12), with stimulation 3 × /day | CM (5–10 mg × 3/day dose of baclofen tablets for oral) | / | 6 days | 1.Total effective rate 2.Hiccup symptom score 3.Dietary status score 4.Sleep status score 5.Mental status score 6.Adverse events |
1.A>B 2.A>B 3.A>B 4.A=B 5.A>B 6.A=B |
| Wang 2019 | Stroke | 1:1 | 100 | A:62.35 ± 4.2 B:59.6 ± 5.5 | A:36/14 B:35/15 | MA on Shuigou (DU 26), Cuanzhu (BL 2), Neiguan (PC 6), Danzhong (RN 17), Zhongwan (RN 12), Zusanli (ST 36), with stimulation 1 × /day+(B) | CM (10 mg × 2/day dose of metoclopramide hydrochloride injection for intramuscular injection) | / | 7 days | Hiccup symptom score | A>B |
| Chen 2018 | Stroke | 1:1 | 68 | A:60.79 ± 8.33 B:61.95 ± 6.72 | A:21/14 B:18/15 | AI (5 mg × 1/day dose of haloperidol injection on Zusanli (ST 36)) | CM (10 mg × 2/day dose of haloperidol injection for intramuscular injection) | / | 7 days | Total effective rate | A>B |
| Fan 2018 | NR | 1:1 | 112 | A:48.6 ± 7.64 B:49.18 ± 7.56 | A:35/21 B:37/19 | MA on Sanyinjiao (SP 6), Danzhong (RN 17), Zusanli (ST 36), Taichong (LR 3), Neiguan (PC 6), with stimulation 1 × /day;AI [5 mg × 1/day dose of haloperidol injection on Zusanli (ST 36)] | CM (10 mg × 1/day dose of metoclopramide hydrochloride injection for intramuscular injection) | / | 7 days | 1.Total effective rate 2.Adverse events |
1.A>B 2.A=B |
| Li 2018 | NR | 1:1 | 60 | A:44.3 ± 13.95 B:45.9 ± 12.78 | A:18/12 B:17/13 | EA on Cuanzhu (BL 2), Tianding (LI 17), with dense wave stimulation 1 × /day | CM (5 mg × 2/day dose of baclofen tablets for oral) | / | 5 days | Total effective rate | A>B |
| Wang 2018 | Cerebral hemorrhage | 1:1 | 120 | A:68.5 ± 7.3 B:68.2 ± 7.9 | A:56/4 B:52/8 | MA on Shuigou (DU 26) with stimulation 1 × /day; AA on ear center (HX1), Shenmen (TF4), Stomach (CO4), with stimulation 3 × /day | MA on Zhongwan (RN 12), Shangwan (RN 13), Zusanli (ST 36), Geshu (BL 17), with stimulation 1 × /day | / | 10 days | 1.Total effective rate 2.Hiccup symptom score |
1.A>B 2.A>B |
| Yang 2018 | After radiotherapy or chemotherapy for malignant tumors | 1:1 | 60 | A:55.02 ± 6.53 B:54.68 ± 6.48 | A:19/11 B:15/15 | MA on Neiguan (PC 6), Zusanli (ST 36), Cuanzhu (BL 2), Danzhong (RN 17), Zhongwan (RN 12), with stimulation 1 × /day; AA on Ear center (HX1), Stomach (CO4), Sympathetic nerve (AH6a), Subcortex (AT4), with stimulation 3 × /day | CM (20 mg × 1/day dose of metoclopramide hydrochloride injection for intramuscular injection) | / | 3 days | 1.Total effective rate 2.Hiccup symptom score 3.Dietary status score 4.Sleep status score 5.Mental status score 6.Adverse events |
1.A>B 2.A>B 3.A>B 4.A>B 5. A>B 6.A=B |
| Zhang 2018 | After resection of hepatic neoplasms | 1:1 | 39 | A:47.1 ± 5.1 B:49.0 ± 5.5 | A:12/8 B:12/7 | EA on cervical Jiaji (C3-C5), with sparse wave stimulation 2 × /day | CM (Two arms: (1) 20 mg × 2/day dose of chlorpromazine hydrochloride injection for intramuscular injection; (2) 10 mg × 1/day dose of metoclopramide injection for intravenous infusion) | / | 3 days | 1. Total effective rate 2. Adverse events |
1.A>B 2.A=B |
| Guo 2017 | NR | 1:1 | 60 | A:53.40 ± 15.37 B:48.63 ± 10.00 | A:12/18 B:14/16 | MA on cervical Jiaji (C3–C5), with stimulation 1 × /day | CM (10 mg × 1/day dose of racemic anisodamine hydrochloride injection for intramuscular injection) | / | 10 days | 1.Total effective rate 2.Dietary status score 3.Sleep status score 4.Mental status score 5.Adverse events |
1.A>B 2.A>B 3.A>B 4.A>B 5.A>B |
| Qiu 2017 | Stroke | 1:1 | 60 | A:58.7 ± 10.76 B:61.57 ± 9.14 | A:18/12 B:16/14 | MA on Yangbai (GB 14), Yuyao (EX-HN4), Lianquan (RN 23), with stimulation 1 × /day | CM (10 mg × 1/day dose of racemic anisodamine hydrochloride injection for intramuscular injection) | / | 10 days | 1.Total effective rate 2.Hiccup symptom score 3.Dietary status score 4.Sleep status score 5.Mental status score |
1.A>B 2.A>B 3.A>B 4.A>B 5.A>B |
| Zhong 2017 | Stroke | 1:1 | 120 | A:66.0 ± 10.9 B:67.5 ± 11.1 | A:28/32 B:19/41 | MA on Danzhong (RN 17), Neiyingxiang (EX-HN9), Neiguan (PC 6), Gongsun (SP 4), Zusanli (ST 36), with stimulation 1 × /day;AI [10 mg × 1/day dose of metoclopramide hydrochloride injection on Neiguan (PC 6), Zusanli (ST 36)] | CM (Two arms: (1) 10 mg × 3/day dose of Baclofen tablets for oral; (2) 10 mg × 2/day dose of metoclopramide hydrochloride injection for Intramuscular injection) | / | 7 days | 1.Total effective rate 2.Hiccup symptom score 3.Adverse events |
1.A>B 2.A>B 3.A=B |
| Cao 2016 | NR | 1:1 | 60 | A:40.12 ± 12.11 B:40.78 ± 13.44 | A:11/19 B:14/16 | MA on Dingchuan (EX-B1), Geshu (BL 17), Feishu (BL 13), Danzhong (RN 17), Neiguan (PC 6), Cuanzhu (BL 2), with stimulation 1 × /day | CM (10 mg × 2/day dose of racemic anisodamine hydrochloride injection for intramuscular injection) | / | 10 days | 1.Total effective rate 2.Dietary status score 3.Sleep status score 4.Mental status score 5.Adverse events |
1.A>B 2.A>B 3.A>B 4.A>B 5.A>B |
| Guo 2016 | NR | 1:1 | 60 | A:51.30 ± 16.22 B:48.10 ± 17.26 | A:17/13 B:16/14 | MA on Yuyao (EX-HN4), Zhongkui (EX-UE4), with stimulation 1 × /day | CM (10 mg × 2/day dose of baclofen tablets for oral) | / | 10 days | 1.Total effective rate 2.Dietary status score 3.Sleep status score 4.Mental status score |
1.A>B 2.A=B 3.A>B 4.A=B |
| Liu 2016 | After chemotherapy for malignant tumors | 1:1 | 48 | A:54.5 B:52.2 | A:16/8 B:15/9 | MA on Neiguan (PC 6), Gongsun (SP 4), Zhongwan (RN 12), Danzhong (RN 17), with stimulation 1 × /day; CHM (200 ml × 2/day dose of herbal decoction for oral) | CM (20 mg × 1/day dose of metoclopramide hydrochloride injection for Intramuscular injection) | / | 3 days | Total effective rate | A>B |
| Wu 2016 | NR | 1:1 | 60 | A:51.42 ± 10.63 B:49.25 ± 11.09 | A:18/12 B:17/13 | AI (5 mg × 1/day dose of chlorpromazine hydrochloride injection on Zusanli (ST 36)) | CM (20 mg × 1/day dose of racemic anisodamine hydrochloride injection for intramuscular injection) | / | 3 days | Total effective rate | A>B |
| Gao 2015 | NR | 1:1 | 85 | A:42.64 ± 10.52 B:42.35 ± 10.38 | A:24/18 B:25/18 | MA on Zhongwan (RN 12), Neiguan (PC 6), Zusanli (ST 36), Fenglong (ST 40), Taichong (LR 3), Shenque (RN 8), with stimulation 1 × /day+(B) | CHM (eight pills × 3/day dose of herbal pill for oral) | / | 7 days | Total effective rate | A>B |
| Ke 2015 | NR | 1:1 | 76 | A:45.9 ± 1.8 B:46.8 ± 1.3 | A:21/17 B:19/19 | AI [10 mg × 1/day dose of metoclopramide hydrochloride injection on Neiguan (PC 6)];CHM (150 ml × 2/day dose of herbal decoction for oral) | CM (10 mg × 1/day dose of metoclopramide hydrochloride injection for Intramuscular injection) | / | 10 days | 1.Total effective rate 2.Adverse events |
1.A>B 2.A=B |
| Li 2015 | Postoperative of oral cavity, abdomen, waist, and lower limbs | 1:1 | 67 | A:33 ± 12 B:33 ± 12 | A:15/19 B:16/17 | EA on Geshu (BL 17), Weishu (BL 21), with dilatational wave stimulation 1 × /day | CM [Two arms: (1) 10 mg × 2/day dose of metoclopramide hydrochloride injection for Intramuscular injection; (2) 10 mg × 2/day dose of Baclofen tablets for oral] | / | 2 weeks | Total effective rate | A>B |
| Liao 2015 | Postoperative of intracranial tumors | 1:1 | 84 | 19–58 | 39/45 | MA on Futu (LI 18), Neiguan (PC 6), Taichong (LR 3), with stimulation 1 × /day+(B) | CM (10 mg × 1/day dose of flunarizine hydrochloride capsules for oral) | / | 2 weeks | Total effective rate | A>B |
| Lin 2015 | NR | 1:1 | 60 | A:42.4 ± 6.93 B:41.7 ± 5.57 | A:16/14 B:17/13 | AI [10 mg × 1/day dose of metoclopramide hydrochloride injection on Neiguan (PC 6)]+(B) | MA on Cuanzhu (BL 2), Danzhong (RN 17), Zhongwan (RN 12), Neiguan (PC 6), Geshu (BL 17), Zusanli (ST 36), with stimulation 1 × /day | / | 18 days | 1.Total effective rate 2.Dietary status score 3.Sleep status score 4.Mental status score 5.Adverse events |
1.A>B 2.A>B 3.A>B 4.A>B 5.A=B |
| Song 2015 | Stroke | 1:1 | 80 | A:63.94 ± 8.36 B:62.31 ± 8.15 | A:26/14 B:21/19 | MA on Neiguan (PC 6), Zusanli (ST 36), Yintang (DU 29), Cuanzhu (BL 2) with stimulation 1 × /day; CHM (150 ml × 2/day dose of herbal decoction for oral) | CM (10 mg × 1/day dose of metoclopramide hydrochloride injection for Intramuscular injection) | / | 7 days | Total effective rate | A>B |
| Zhang 2015 (1) | NR | 1:1 | 30 | A:67.4 ± 3.3 B:65.8 ± 3.2 | A:8/7 B:6/9 | MA on Zhongwan (RN 12), Xiawan (RN 10), Zusanli (ST 36), Shuigou (DU 26), Hegu (LI 4), Neiguan (PC 6), Tianshu (ST 25), Shangjuxu (ST 37), Taichong (LR 3), with stimulation 1 × /day | CM (10 mg × 1/day dose of metoclopramide hydrochloride injection for Intramuscular injection) | / | 7 days | Total effective rate | A>B |
| Zhang 2015 (2) | NR | 1:1 | 30 | A:42.60 ± 12.56 B:43.87 ± 15.12 | A:7/8 B:9/6 | EA on Cuanzhu (BL 2), Neiguan (PC 6), Danzhong (RN 17), Zhongwan (RN 12), Zusanli (ST 36), with continuous wave stimulation 1 × /day;CHM (150 ml × 2/day dose of herbal decoction for oral) | CM (5 mg × 3/day dose of racemic anisodamine tablets for oral) | / | 10 days | Total effective rate | A>B |
| Zhang 2015 (3) | Stroke | 1:1 | 47 | 68.0 ± 7.2 | 29/18 | TEAS on Neiguan (PC 6), Yifeng (SJ 17), with stimulation 1 × /day+(B) | AI (20 mg × 1/day dose of ritalin on Zusanli (ST 36)) | / | 3 days | Total effective rate | A>B |
Characteristics of the included studies.
MA, manual acupuncture; CM, conventional medications; AI, acupoint injection; EA, electroacupuncture; AA, auricular acupressure; WA, warm acupuncture; CHM, Chinese herbal medicine; TEAS, transcutaneous electrical acupoint stimulation; NR, not reported.
*All studies reporting primary diseases mentioned that subjects received symptomatic underlying treatment for the primary diseases.
>The outcome or adverse events in the former is better than the latter by statistical analysis.
=There was no statistical difference between the former and the latter in this outcome.
3.3 Risk of bias among the included RCTs
The risk of bias was assessed for each included study, and the results are presented in Figure 2. All studies explicitly described their randomization methods; four studies (36, 37, 46, 49) were rated as having a high risk of bias because group allocation was based on the order of patient visits, and one study (42) used coin tossing for randomization. The remaining studies adopted the random number table method. Three studies (25, 45, 52) reported using sealed, opaque envelopes for allocation concealment, whereas the remaining studies did not mention any method of concealment. Due to the nature of acupuncture procedure, blinding of practitioners was not feasible; thus, all studies were rated as having a high risk of performance bias. Except for two studies (21, 47), the blinding of outcome assessors and statisticians was not reported, resulting in an unclear risk of detection bias. All included studies had complete outcome data, and no selective reporting was identified. One study (24) was rated as high risk in the domain of other biases due to imbalanced baseline data.
Figure 2
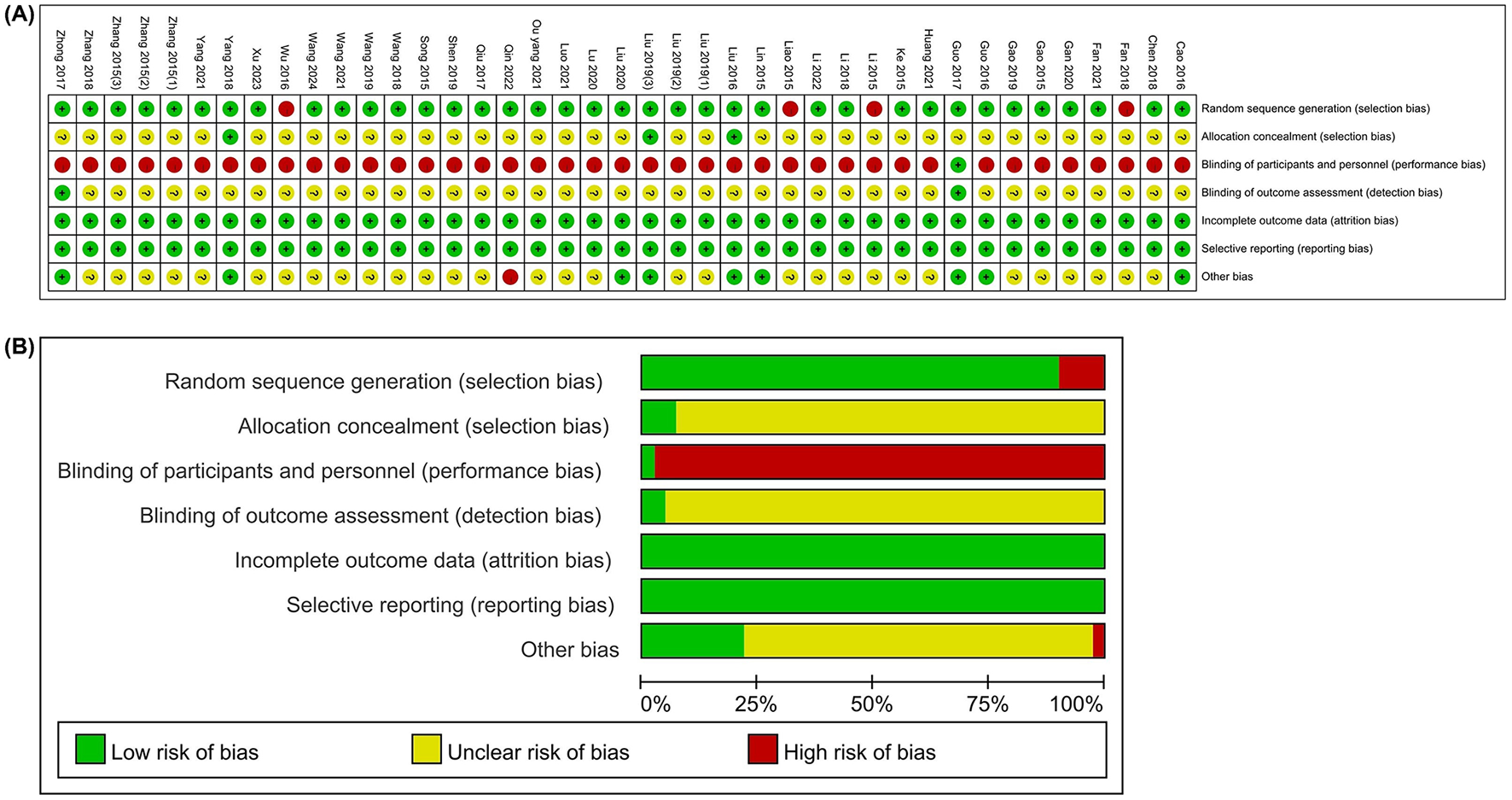
Risk of bias. (A) Risk of bias summary; (B) Risk of bias graph.
3.4 Pairwise meta-analysis results
3.4.1 Comparison of TER
A pairwise meta-analysis revealed that multiple acupuncture-related interventions were significantly more effective than CM or single treatments in improving TER among patients with IH. Specifically, MA+AI showed superior efficacy compared to both AI alone [two RCTs, RR = 1.20, 95% CI (1.05, 1.37)] and CM [two RCTs, RR = 1.35, 95% CI (1.18, 1.55)]. Similarly, MA+CM demonstrated a notable advantage over CM alone [four RCTs, RR = 1.35, 95% CI (1.21, 1.51)]. MA itself also showed enhanced effects when compared to CM [seven RCTs, RR = 1.27, 95% CI (1.15, 1.40)], and MA+CHM outperformed both CM [three RCTs, RR = 1.23, 95% CI (1.10, 1.38)] and CHM alone [two RCTs, RR = 1.47, 95% CI (1.23, 1.76)]. Moreover, EA was more effective than CM [five RCTs, RR = 1.28, 95% CI (1.17, 1.40)], and AI alone also showed better outcomes than CM [two RCTs, RR = 1.32, 95% CI (1.11, 1.58)]. In addition, other combined therapies, such as MA+AA, also showed superiority over CM [three RCTs, RR = 1.20, 95% CI (1.06, 1.36)], whereas TEAS+CHM was also more effective than CM [two RCTs, RR = 1.32, 95% CI (1.10, 1.58)]. Comparisons involving AA vs. CM, MA+AA vs. MA, and other combination therapies (such as AI+CHM, TEAS+AI, etc.) also demonstrated statistically significant advantages over their respective control groups, although some were based on a single study. Detailed results are presented in Table 2.
Table 2
| Comparison categories | Number of studies | I 2 | RR (95% CI) | P-value |
|---|---|---|---|---|
| MA+AI vs. AI | 2 | 0% | 1.20 (1.05, 1.37) | 0.006 |
| MA+AI vs. CM | 2 | 0% | 1.35 (1.18, 1.55) | < 0.0001 |
| MA+CM vs. CM | 4 | 32% | 1.35 (1.21, 1.51) | < 0.00001 |
| MA+AI vs. MA | 4 | 0% | 1.18 (1.09, 1.28) | < 0.0001 |
| AI vs. CM | 2 | 0% | 1.32 (1.11, 1.58) | 0.002 |
| AI+CHM vs. CM | 1 | – | 1.38 (1.10, 1.74) | 0.005 |
| EA vs. WA | 1 | – | 1.14 (1.00, 1.31) | 0.05 |
| EA vs. CM | 5 | 77% | 1.28 (1.17, 1.40) | < 0.00001 |
| EA+CM vs. CM | 1 | – | 1.28 (1.00, 1.62) | 0.05 |
| MA+AA vs. CM | 3 | 0% | 1.20 (1.06, 1.36) | 0.005 |
| MA+AA vs. MA | 1 | – | 1.11 (1.01, 1.23) | 0.03 |
| AA vs. CM | 1 | – | 1.30 (1.07, 1.58) | 0.009 |
| MA vs. CM | 7 | 2% | 1.27 (1.15, 1.40) | < 0.00001 |
| TEAS+CHM vs. CM | 2 | 68% | 1.32 (1.10, 1.58) | 0.003 |
| TEAS+AI vs. AI | 1 | – | 1.54 (1.01, 2.34) | 0.04 |
| MA+CHM vs. CM | 3 | 0% | 1.23 (1.10, 1.38) | 0.0004 |
| MA+CHM vs. CHM | 2 | 0% | 1.47 (1.23, 1.76) | < 0.0001 |
| MA vs. AI | 1 | – | 1.23 (0.93, 1.62) | =0.14 |
| WA vs. CM | 1 | – | 0.95 (0.81, 1.10) | =0.49 |
Pairwise meta-analysis of total effective rate.
The bold font indicates a statistical difference.
3.4.2 Comparison of HSS
A total of eight pairwise comparisons were reported on HSS. Compared with AI alone, MA+AI demonstrated superior symptom relief [one RCT, SMD = −0.86, 95% CI (−1.35, −0.37)], MA alone [one RCT, SMD = −1.20, 95% CI (−1.59, −0.81)], as well as CM [one RCT, SMD = −0.82, 95% CI (−1.16, −0.48)]. MA alone also significantly outperformed CM [two RCTs, SMD = −1.49, 95% CI (−2.14, −0.85)], and its combination with CM (MA+CM) produced even greater symptom improvement [one RCT, SMD = −2.04, 95% CI (−2.59, −1.49)]. Furthermore, EA+CM showed stronger efficacy than CM did [one RCT, SMD = −2.10, 95% CI (−2.79, −1.41)]. MA+AA also resulted in better symptom relief than CM [three RCTs, SMD = −1.32, 95% CI (−2.02, −0.61)] or MA alone [one RCT, SMD = −2.05, 95% CI (−2.71, −1.39)]. Detailed results are presented in Table 3.
Table 3
| Comparison categories | Number of studies | I 2 | SMD (95% CI) | P-value |
|---|---|---|---|---|
| MA+AI vs. AI | 1 | – | −0.86 (−1.35, −0.37) | 0.0005 |
| MA+AA vs. CM | 3 | 52% | −1.32 (−2.02, −0.61) | 0.0003 |
| MA+AI vs. MA | 1 | – | −1.20 (−1.59, −0.81) | < 0.00001 |
| EA+CM vs. CM | 1 | – | −2.10 (−2.79, −1.41) | < 0.00001 |
| MA vs. CM | 2 | 0% | −1.49 (−2.14, −0.85) | < 0.00001 |
| MA+CM vs. CM | 1 | – | −2.04 (−2.59, −1.49) | < 0.00001 |
| MA+AA vs. MA | 1 | – | −2.05 (−2.71, −1.39) | < 0.00001 |
| MA+AI vs. CM | 1 | – | −0.82 (−1.16, −0.48) | < 0.00001 |
Pairwise meta-analysis of hiccup symptom score.
The bold font indicates a statistical difference.
3.4.3 Comparison of quality-of-life scores
In terms of quality-of-life scores, three intervention comparisons were conducted here. The results revealed that MA+AI demonstrated significantly greater improvements across the three domains compared with MA alone (two RCTs). Specifically, improvements were observed in dietary status [SMD = 0.85, 95% CI (0.65, 1.06)], sleep status [SMD = 0.52, 95% CI (0.31, 0.72)], and mental status [SMD = 0.47, 95% CI (0.29, 0.65)]. Similarly, MA+AA was superior to CM in all three domains (three RCTs), with significant improvements in dietary status [SMD = 0.57, 95% CI (0.37, 0.78)], sleep status [SMD = 0.37, 95% CI (0.19, 0.55)], and mental status [SMD = 0.60, 95% CI (0.42, 0.78)]. In addition, MA alone also had more favorable effects than CM did (four RCTs). Improvements were observed in dietary status [SMD = 0.70, 95% CI (0.02, 1.38)], sleep status [SMD = 0.47, 95% CI (0.26, 0.69)], and mental status [SMD = 0.68, 95% CI (0.47, 0.90)], suggesting the potential of MA to alleviate relevant symptoms. Detailed results are presented in Table 4.
Table 4
| Comparison categories | Number of studies | Dietary status score | Sleep status score | Mental status score | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| I 2 | SMD (95% CI) | P -value | I 2 | SMD (95% CI) | P -value | I 2 | SMD (95% CI) | P -value | ||
| MA+AI vs. MA | 2 | 0% | 0.85 (0.65, 1.06) | < 0.00001 | 0% | 0.52 (0.31, 0.72) | < 0.00001 | 54% | 0.47 (0.29, 0.65) | < 0.00001 |
| MA+AA vs. CM | 3 | 8% | 0.57 (0.37, 0.78) | < 0.00001 | 77% | 0.37 (0.19, 0.55) | < 0.0001 | 37% | 0.60 (0.42, 0.78) | < 0.00001 |
| MA vs. CM | 4 | 89% | 0.70 (0.02, 1.38) | < 0.00001 | 43% | 0.47 (0.26, 0.69) | < 0.0001 | 51% | 0.68 (0.47, 0.90) | < 0.00001 |
Pairwise meta-analysis of dietary/sleep/mental status score.
The bold font indicates a statistical difference.
3.5 Network meta-analysis results
3.5.1 Network plot for multiple interventions
In Figure 3, the thickness of the line is positively correlated with the two intervention methods, whereas the size of the points is proportional to the weight of the sample size in the intervention. A total of 40 studies reported the TER, involving 19 different interventions and 2,960 participants, forming six closed loops. Eleven studies reported HSS, covering seven treatment strategies and 927 participants, forming two closed loops. Nine studies assessed quality-of-life in three domains—dietary, sleep, and mental status—across four treatment approaches and a total of 605 participants; no closed loop was formed.
Figure 3
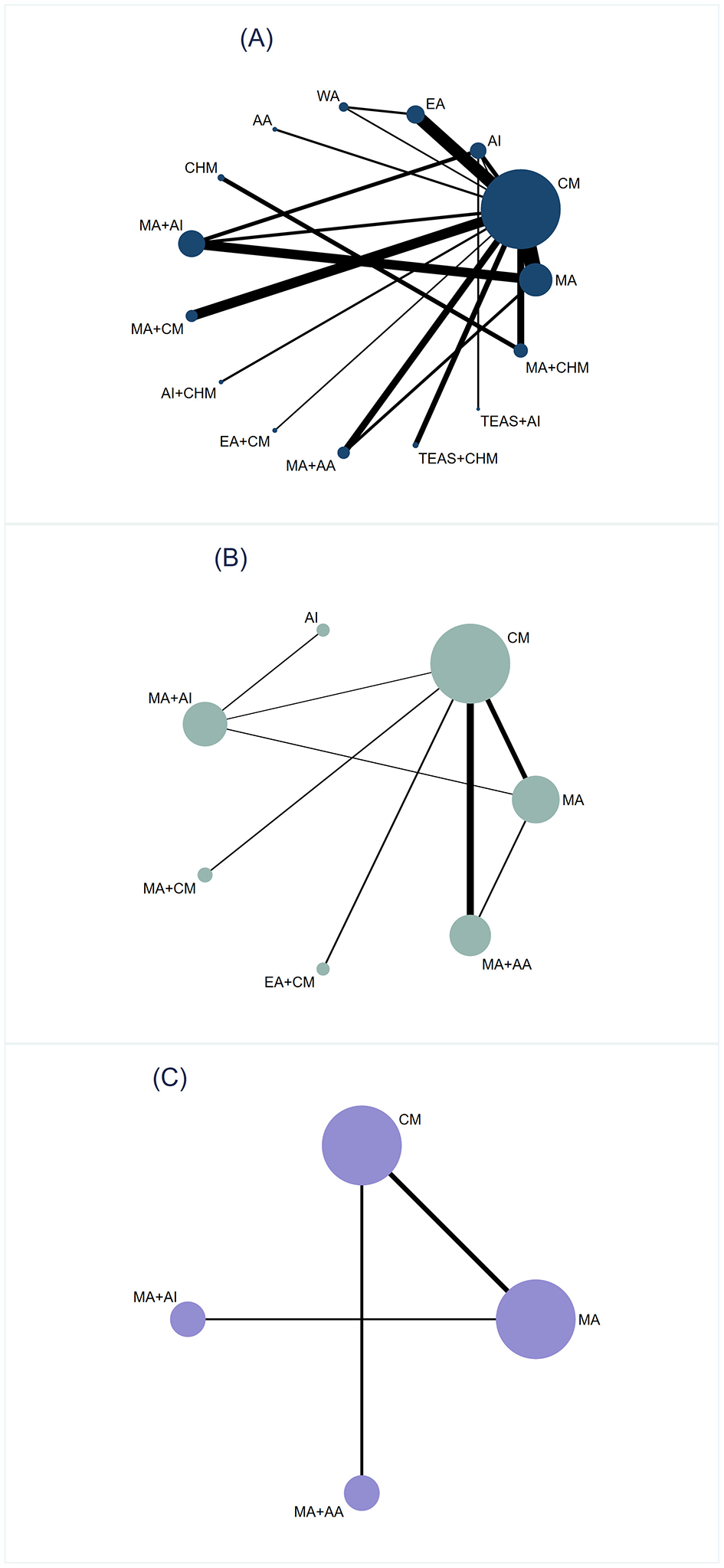
Network plot. (A) Total effective rate. (B) Hiccup symptom score. (C) Dietary/Sleep/Mental status score.
3.5.2 Inconsistency test
The inconsistency test was conducted on the six triangular closed loops formed by the study of TER, and the results showed that Loop (A-B-L) P = 0.082, Loop (B-C-H) P = 0.065, Loop (A-B-H) P = 0.073, Loop (A-B-C) P = 0.191, Loop (A-C-H) P = 0.435, Loop (B-D-E) P = 0.607. All P-values were >0.05, indicating good consistency between direct and indirect evidence. Inconsistency test was performed on the two closed loops formed by the study of reporting HSS, and the results showed that: Loop (A-B-G) P = 0.002, Loop (A-B-D) P = 0.000. All P-values were < 0.05, revealing statistically significant inconsistency, suggesting potential discrepancies between direct and indirect comparisons. Detailed results are presented in Figure 4. In order to identify the source of the inconsistency, we rechecked the data and coding, and conducted a node splitting analysis. We found that MA vs. CM (A-B) contributed the most to the inconsistency (P < 0.001). Since the studies reporting dietary, sleep, and mental status scores did not form any closed loops, inconsistency tests could not be performed.
Figure 4
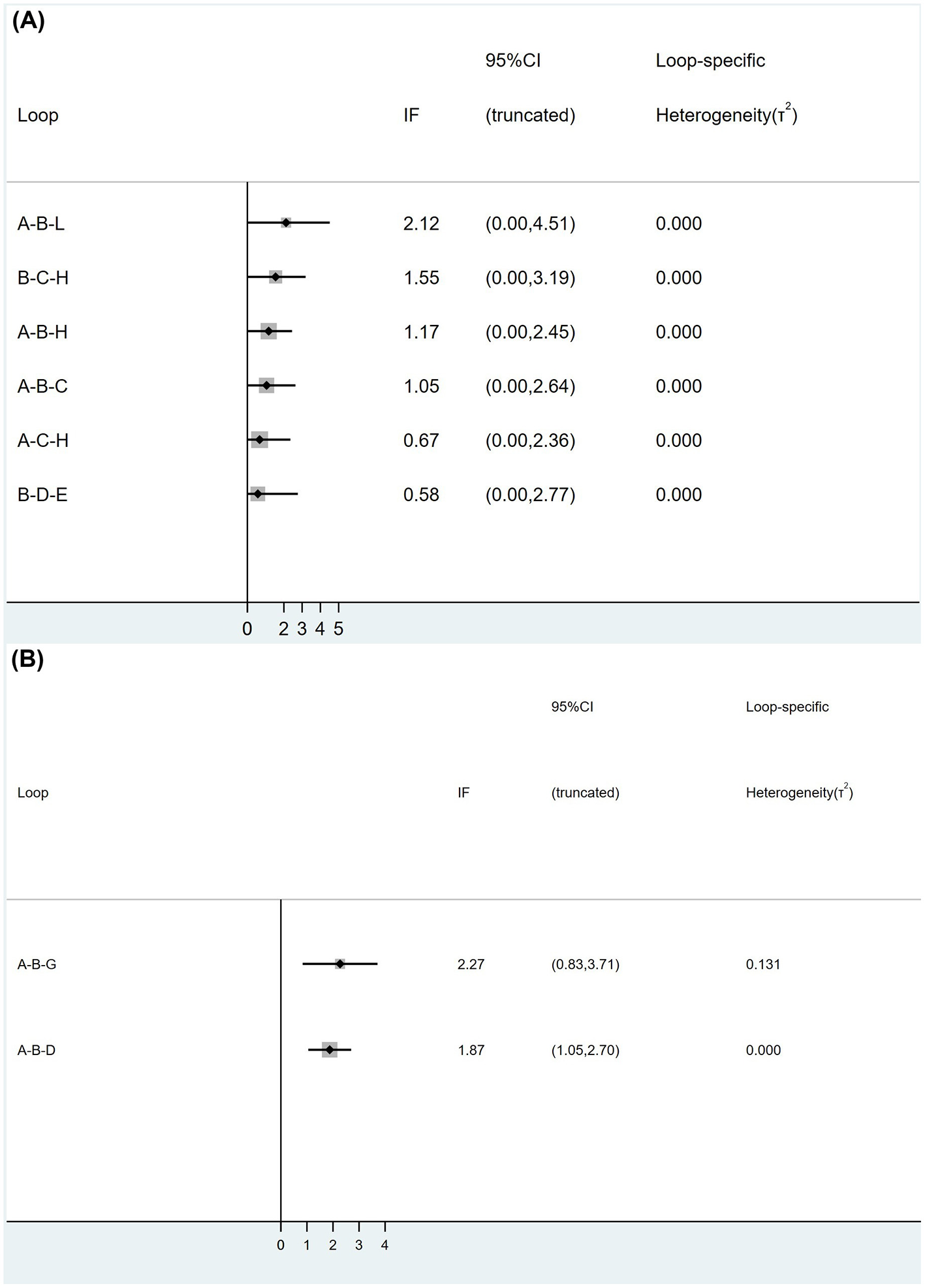
The inconsistency test conducted on the closed loops formed by the three intervention points of TER (A) and HSS (B).
3.5.3 NMA results of TER
In the comparison of single interventions, MA was significantly more effective than WA [RR = 4.38, 95% CI (1.29, 14.84)] and CHM [RR = 6.08, 95% CI (1.30, 28.49)] were effective; EA outperformed both WA [RR = 8.48, 95% CI (2.45, 29.35)] and CHM [RR = 11.77, 95% CI (2.28, 60.85)] were effective; and AA was also superior to WA [RR = 0.10, 95% CI (0.01, 0.70)] and CHM [RR = 13.72, 95% CI (1.59, 118.34)]. Overall, WA and CHM consistently showed lower RR values compared with other treatments, suggesting that their therapeutic efficacy may be relatively limited. Moreover, combined interventions demonstrated greater advantages over single interventions, likely due to synergistic effects. MA+AI was superior to MA [RR = 0.34, 95% (0.19, 0.62)], AI [RR = 0.27, 95% (0.13, 0.54)], WA [RR = 0.08, 95% (0.02, 0.28)], and CHM [RR = 0.06, 95% (0.01, 0.27)]; MA+CM outperformed AI [RR = 0.32, 95% (0.11, 0.95)], WA [RR = 0.09, 95% (0.02, 0.38)], and CHM [RR = 0.07, 95% (0.01, 0.36)]; and TEAS+AI was more effective than AI [RR = 0.23, 95% (0.06, 0.89)], WA [RR = 0.07, 95% (0.01, 0.44)], and CHM [RR = 0.05, 95% (0.01, 0.40)]. However, EA+CM showed no advantage over any other intervention except CM [RR = 2.98, 95% (1.02, 8.70)]. Compared with the control intervention CM, all the other treatments, except WA and CHM, showed significant efficacy. Detailed results are presented in Table 5.
Table 5
| MA | ||||||||||||||
| 1.28 (0.65, 2.55) | AI | |||||||||||||
| 0.52 (0.21, 1.26) | 0.40 (0.15, 1.10) | EA | ||||||||||||
| 4.38 (1.29, 14.84) | 3.41 (0.92, 12.65) | 8.48 (2.45, 29.35) | WA | |||||||||||
| 0.44 (0.08, 2.32) | 0.35 (0.06, 1.93) | 0.86 (0.15, 4.92) | 0.10 (0.01, 0.70) | AA | ||||||||||
| 6.08 (1.30, 28.49) | 4.74 (0.94, 23.85) | 11.77 (2.28, 60.85) | 1.39 (0.22, 8.77) | 13.72 (1.59, 118.34) | CHM | |||||||||
| 0.34 (0.19, 0.62) | 0.27 (0.13, 0.54) | 0.66 (0.26, 1.70) | 0.08 (0.02, 0.28) | 0.77 (0.14, 4.15) | 0.06 (0.01, 0.27) | MA+AI | ||||||||
| 0.41 (0.15, 1.09) | 0.32 (0.11, 0.95) | 0.78 (0.25, 2.44) | 0.09 (0.02, 0.38) | 0.91 (0.15, 5.52) | 0.07 (0.01, 0.36) | 1.18 (0.42, 3.33) | MA+CM | |||||||
| 0.38 (0.07, 1.99) | 0.30 (0.05, 1.66) | 0.74 (0.13, 4.23) | 0.09 (0.01, 0.60) | 0.86 (0.09, 8.04) | 0.06 (0.01, 0.54) | 1.11 (0.21, 5.99) | 0.94 (0.16, 5.68) | AI+CHM | ||||||
| 1.07 (0.33, 3.46) | 0.83 (0.23, 2.96) | 2.06 (0.56, 7.60) | 0.24 (0.05, 1.15) | 2.40 (0.36, 16.22) | 0.18 (0.03, 1.08) | 3.11 (0.92, 10.52) | 2.63 (0.66, 10.38) | 2.79 (0.41, 18.84) | EA+CM | |||||
| 0.66 (0.26, 1.68) | 0.51 (0.17, 1.49) | 1.27 (0.41, 3.91) | 0.15 (0.04, 0.61) | 1.48 (0.25, 8.88) | 0.11 (0.02, 0.59) | 1.91 (0.70, 5.25) | 1.62 (0.48, 5.40) | 1.72 (0.29, 10.31) | 0.62 (0.16, 2.42) | MA+AA | ||||
| 0.58 (0.16, 2.06) | 0.45 (0.12, 1.75) | 1.12 (0.28, 4.48) | 0.13 (0.03, 0.67) | 1.30 (0.18, 9.32) | 0.09 (0.01, 0.62) | 1.68 (0.45, 6.24) | 1.42 (0.33, 6.10) | 1.51 (0.21, 10.83) | 0.54 (0.11, 2.66) | 0.88 (0.21, 3.75) | TEAS+CHM | |||
| 0.29 (0.06, 1.35) | 0.23 (0.06, 0.89) | 0.57 (0.10, 3.08) | 0.07 (0.01, 0.44) | 0.66 (0.07, 5.93) | 0.05 (0.01, 0.40) | 0.86 (0.19, 3.96) | 0.72 (0.13, 4.15) | 0.77 (0.09, 6.88) | 0.28 (0.04, 1.77) | 0.45 (0.08, 2.53) | 0.51 (0.07, 3.48) | TEAS+AI | ||
| 0.63 (0.22, 1.83) | 0.49 (0.15, 1.58) | 1.23 (0.37, 4.08) | 0.14 (0.03, 0.63) | 1.43 (0.23, 9.00) | 0.10 (0.03, 0.32) | 1.85 (0.61, 5.60) | 1.56 (0.44, 5.60) | 1.66 (0.26, 10.46) | 0.59 (0.14, 2.48) | 0.97 (0.27, 3.44) | 1.10 (0.24, 4.97) | 2.16 (0.36, 12.94) | MA+CHM | |
| 3.17 (1.95, 5.16) | 2.47 (1.25, 4.88) | 6.14 (2.92, 12.89) | 0.72 (0.24, 2.21) | 7.15 (1.47, 34.71) | 0.52 (0.12, 2.26) | 9.26 (5.19, 16.50) | 7.82 (3.31, 18.46) | 8.31 (1.71, 40.32) | 2.98 (1.02, 8.70) | 4.84 (2.07, 11.30) | 5.50 (1.70, 17.82) | 10.81 (2.36, 49.43) | 5.01 (1.94, 12.89) | CM |
Network meta-analysis of total effective rate [RR (95% CI)].
The bold font indicates a statistical difference.
3.5.4 NMA results of HSS
Comparisons among acupuncture-related therapies revealed that only MA+AI was significantly more effective than MA [SMD = 0.78, 95% CI (0.10, 1.47)], and MA+AA outperformed MA [SMD = 0.66, 95% CI (0.05, 1.27)]; other comparisons did not reach statistical significance. Except for MA and AI, all other interventions showed greater benefit compared to CM, specifically: MA+AI [SMD = −1.18, 95% CI (−1.86, −0.49)], MA+CM [SMD = −1.44, 95% CI (−2.36, −0.52)], EA+CM [SMD = −1.28, 95% CI (−2.21, −0.35)], and MA+AA [SMD = −1.05, 95% CI (−1.55, −0.56)]. Detailed results are presented in Table 6.
Table 6
| MA | ||||||
| 0.04 (−1.10, 1.19) | AI | |||||
| 0.78 (0.10, 1.47) | 0.74 (−0.18, 1.66) | MA+AI | ||||
| 1.05 (−0.01, 2.11) | 1.00 (−0.46, 2.47) | 0.26 (−0.88, 1.41) | MA+CM | |||
| 0.88 (−0.19, 1.95) | 0.84 (−0.63, 2.31) | 0.10 (−1.05, 1.25) | −0.16 (−1.47, 1.14) | EA+CM | ||
| 0.66 (0.05, 1.27) | 0.62 (−0.60, 1.83) | −0.12 (−0.92, 0.67) | −0.39 (−1.43, 0.66) | −0.22 (−1.28, 0.83) | MA+AA | |
| −0.39 (−0.92, 0.14) | −0.44 (−1.58, 0.71) | −1.18 (−1.86, −0.49) | −1.44 (−2.36, −0.52) | −1.28 (−2.21, −0.35) | −1.05 (−1.55, −0.56) | CM |
Network meta-analysis of hiccup symptom score [SMD (95% CI)].
The bold font indicates a statistical difference.
3.5.5 NMA results of quality-of-life scores
As shown in Table 7, only four intervention strategies were included in the analysis of quality-of-life scores. In terms of improving dietary status, both MA [SMD = 0.92, 95% CI (0.13, 1.71)] and MA+AI [SMD = 1.95, 95% CI (0.60, 3.30)] were significantly more effective than CM, while the difference between MA+AA and CM was not statistically significant. For sleep status, MA [SMD = −0.52, 95% CI (−0.92, −0.12)], MA+AI [SMD = −1.22, 95% CI (−1.88, −0.55)], and MA+AA [SMD = −0.58, 95% CI (−1.05, −0.12)] all showed superior effects compared to CM. Regarding improvements in mental status (Table 8), CM showed no advantage over MA [SMD = 0.75, 95% CI (0.46, 1.03)], MA+AI [SMD = 1.54, 95% CI (1.10, 1.99)], or MA+AA [SMD = 1.00, 95% CI (0.67, 1.34)]. Notably, MA combined with AI showed significantly greater improvements in both sleep status [SMD = 0.69, 95% CI (0.16, 1.23)] and mental status [SMD = −0.80, 95% CI (−1.14, −0.45)] compared to MA alone, indicating a potential synergistic effect.
Table 7
| MA | 0.69 (0.16, 1.23) | 0.06 (−0.55, 0.67) | −0.52 (−0.92, −0.12) |
| −1.03 (−2.13, 0.06) | MA+AI | −0.63 (−1.44, 0.18) | −1.22 (−1.88, −0.55) |
| 0.06 (−1.15, 1.26) | 1.09 (−0.54, 2.72) | MA+AA | −0.58 (−1.05, −0.12) |
| 0.92 (0.13, 1.71) | 1.95 (0.60, 3.30) | 0.86 (−0.05, 1.77) | CM |
Network meta-analysis of dietary status score (lower left quadrant) and sleep status score [right upper quadrant; SMD (95% CI)].
The bold font indicates a statistical difference.
Table 8
| MA | |||
| −0.80 (−1.14, −0.45) | MA+AI | ||
| −0.26 (−0.70, 0.18) | 0.54 (−0.02, 1.10) | MA+AA | |
| 0.75 (0.46, 1.03) | 1.54 (1.10, 1.99) | 1.00 (0.67, 1.34) | CM |
Network meta-analysis of mental status score [SMD (95% CI)].
The bold font indicates a statistical difference.
3.5.6 SUCRA probability ranking results
First, the top four interventions with the highest TER were all combination therapies: MA+AI (82.2%), TEAS+AI (81.5%), MA+CM (74.8%), and AI+CHM (72.9%). Among the monotherapies, the most effective were AA (69.1%), EA (65.4%), and MA (37.9%), while CM ranked the lowest (11.2%). Second, in terms of reducing HSS, the interventions ranked from most to least effective were: EA+CM (77.9%), MA+CM (75.8%), MA+AA (71.6%), MA+AI (57.8%), MA (30.6%), AI (28.0%), and CM (8.3%). Finally, the interventions ranked identically across improvements in dietary, sleep, and mental status scores: MA+AI > MA > MA+AA > CM. Detailed results are presented in Figures 5, 6 and Table 9.
Figure 5

SUCRA plot. (A) TER; (B) HSS.
Figure 6

SUCRA plot. (A) Dietary status score; (B) sleep status score; (C) mental status score.
Table 9
| Treatment | TER | HSS | Dietary status score | Sleep status score | Mental status score | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| SUCRA (%) | Rank | SUCRA (%) | Rank | SUCRA (%) | Rank | SUCRA (%) | Rank | SUCRA (%) | Rank | |
| MA | 37.9 | 11 | 30.6 | 5 | 56.0 | 2 | 54.2 | 2 | 51.5 | 2 |
| CM | 11.2 | 13 | 8.3 | 7 | 1.5 | 4 | 0.4 | 4 | 0.0 | 4 |
| AI | 29.9 | 12 | 28.0 | 6 | – | – | – | – | – | – |
| EA | 65.4 | 6 | – | – | – | – | – | – | – | – |
| WA | 7.4 | 14 | – | – | – | – | – | – | – | – |
| AA | 69.1 | 5 | – | – | – | – | – | – | – | – |
| CHM | 4.7 | 15 | – | – | – | – | – | – | – | – |
| MA+AI | 82.2 | 1 | 57.8 | 4 | 96.8 | 1 | 98.8 | 1 | 99.3 | 1 |
| MA+CM | 74.8 | 3 | 75.8 | 2 | – | – | – | – | – | – |
| AI+CHM | 72.9 | 4 | – | – | – | – | – | – | – | – |
| EA+CM | 38.4 | 10 | 77.9 | 1 | – | – | – | – | – | – |
| MA+AA | 56.0 | 9 | 71.6 | 3 | 45.6 | 3 | 46.6 | 3 | 49.2 | 3 |
| TEAS+CHM | 61.2 | 7 | – | – | – | – | – | – | – | – |
| TEAS+AI | 81.5 | 2 | – | – | – | – | – | – | – | – |
| MA+CHM | 57.4 | 8 | – | – | – | – | – | – | – | – |
Ranking of interventions based on SUCRA value (%).
3.5.7 Publication bias
Comparison-adjusted funnel plots were constructed for the primary outcome TER and the secondary outcome HSS to assess the potential for publication bias. As shown in Figure 7A, studies related to TER were generally symmetrically distributed around the vertical axis in the central part of the inverted funnel, suggesting a low risk of publication bias. A few studies appeared at the bottom of the plot, which may be attributed to smaller sample sizes. Figure 7B shows that some studies reporting HSS were clustered along the vertical line, while the rest were scattered asymmetrically, indicating the potential presence of publication bias or small-study effects within the research network. Given that fewer than 10 studies reported quality-of-life scores, funnel plot analysis was not conducted due to insufficient power to detect asymmetry.
Figure 7

The comparison-adjusted funnel plots showed no major asymmetry for TER (A), suggesting a low likelihood of substantial publication bias. In contrast, the HSS (B) funnel plot displayed visible asymmetry and a left-tilted regression line, indicating potential small-study effects and possible overestimation of treatment efficacy. Given the limited number of HSS studies and greater instability in their distribution.
3.6 The confidence assessment results of NMA
The CINeMA system (https://cinema.ispm.unibe.ch/) based on the GRADE framework was used to classify the confidence in the results of NMA, which six domains was evaluated, including: (a) within- study bias, (b) reporting bias, (c) indirectness, (d) imprecision, (e) heterogeneity, and (f) incoherence. Among the 19 confidence ratings for the comparisons, six were rated as “very low,” seven as “low,” only six as “moderate,” and none of the comparisons received a “high” rating. The detailed assessment content is presented in Table 10.
Table 10
| Comparison | Number of studies | Within-study bias | Reporting bias | Indirectness | Imprecision | Heterogeneity | Incoherence | Confidence rating | Reason(s) for downgrading |
|---|---|---|---|---|---|---|---|---|---|
| AA:CM | 1 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | [“Within-study bias,” “incoherence”] |
| AI:CM | 2 | Some concerns | Low risk | No concerns | No concerns | Major concerns | Major concerns | Very low | [“Within-study bias,” “heterogeneity,” “incoherence”] |
| AI:MA | 1 | Some concerns | Low risk | No concerns | Major concerns | No concerns | No concerns | Low | [“Within-study bias,” “imprecision”] |
| AI:MA+AI | 2 | Some concerns | Low risk | No concerns | No concerns | No concerns | No concerns | Moderate | [“Within-study bias”] |
| AI:TEAS+AI | 1 | Some concerns | Low risk | No concerns | No concerns | Major concerns | Major concerns | Very low | [“Within-study bias,” “heterogeneity,” “incoherence”] |
| AI+CHM:CM | 1 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | [“Within-study bias,” “incoherence”] |
| CHM:MA+CHM | 2 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | [“Within-study bias,” “incoherence”] |
| CM:EA | 5 | Major concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Very low | [“Within-study bias,” “incoherence”] |
| CM:EA+CM | 1 | Some concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | [“Within-study bias,” “imprecision,” “incoherence”] |
| CM:MA | 7 | Some concerns | Low risk | No concerns | No concerns | No concerns | No concerns | Moderate | [“Within-study bias”] |
| CM:MA+AA | 3 | Some concerns | Low risk | No concerns | No concerns | No concerns | No concerns | Moderate | [“Within-study bias”] |
| CM:MA+AI | 2 | Some concerns | Low risk | No concerns | No concerns | No concerns | No concerns | Moderate | [“Within-study bias”] |
| CM:MA+CHM | 3 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | [“Within-study bias,” “incoherence”] |
| CM:MA+CM | 4 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | [“Within-study bias,” “incoherence”] |
| CM:TEAS+CHM | 2 | Some concerns | Low risk | No concerns | No concerns | No concerns | Major concerns | Low | [“Within-study bias,” “incoherence”] |
| CM:WA | 1 | Major concerns | Low risk | No concerns | Major concerns | No concerns | Major concerns | Very low | [“Within-study bias,” “imprecision,” “incoherence”] |
| EA:WA | 1 | Major concerns | Low risk | No concerns | No concerns | Major concerns | Major concerns | Very low | [“Within-study bias,” “heterogeneity,” “incoherence”] |
| MA:MA+AA | 1 | Some concerns | Low risk | No concerns | Major concerns | No concerns | No concerns | Moderate | [“Within-study bias,” “imprecision”] |
| MA:MA+AI | 4 | Some concerns | Low risk | No concerns | No concerns | No concerns | No concerns | Moderate | [“Within-study bias”] |
The confidence assessment result of NMA.
3.7 Safety
The occurrence of adverse events was mentioned in 17 studies. Overall, the number of adverse events reported in the treatment groups receiving various acupuncture-related therapies was significantly lower than that in the CM group, and no serious adverse reactions were observed, indicating the safety of acupuncture-based interventions (Table 11).
Table 11
| Studies | Comparisons | Adverse events | |
|---|---|---|---|
| Treatment group | Control group | ||
| Wang 2024 | MA+AI vs. AI | Two cases of rash, one case of general weakness | One case of rash, two cases of headache, one case of constipation, one case of general weakness |
| Li 2022 | MA+AI vs. MA vs. AI | One case of nasal swelling and pain | MA: one case of needle sickness; AI: None |
| Qin 2022 | EA vs. WA vs. CM | One case of inappetence, one case of acupoint swelling and pain | CM: two cases of inappetence, two cases of drowsiness, four cases of palpitation, two case of acupoint swelling and pain; WA: one case of acupoint swelling and pain |
| Fan 2021 | MA+AA vs. CM | None | Two cases of severe fatigue, constipation and thirst |
| Luo 2021 | TEAS+CHM vs. CM | None | Two cases of drowsiness, three cases of inappetence, two cases of constipation, three cases of fatigue, one case of dizziness |
| Ou yang 2021 | MA+AI vs. MA | None | None |
| Wang 2021 | MA+CHM vs. CM | None | None |
| Liu 2019 (1) | AA vs. CM | One case of dizziness | Three cases of dizziness, two cases of inappetence, one case of drowsiness |
| Liu 2019 (2) | MA vs. CM | One case of rash, two cases of diarrhea and constipation, one case of dizziness | Two cases of rash, two cases of diarrhea and constipation, one case of dizziness, two cases of mild sleep dysfunction |
| Liu 2019 (3) | MA+AA vs. CM | One case of subcutaneous hematoma | Two cases of dizziness |
| Fan 2018 | MA+AI vs. CM | None | None |
| Yang 2018 | MA+AA vs. CM | None | None |
| Zhang 2018 | EA vs. CM | None | None |
| Guo 2017 | MA vs. CM | One case of drowsiness, one case of thirst | Two cases of drowsiness, three cases of fatigue, one case of diarrhea, five cases of thirst, one case of blurred vision |
| Zhong 2017 | MA+AI vs. CM | One case of fatigue | One case of fatigue, two cases of dizziness, one case of drowsiness |
| Cao 2016 | MA vs. CM | One case of fatigue, one case of drowsiness | Five case of fatigue, three case of drowsiness, four cases of dizziness, three cases of diarrhea, two cases of eyes dry |
| Lin 2015 | MA+AI vs. MA | None | None |
Adverse events of included studies.
3.8 Cluster ranking plot for multiple interventions
A cluster analysis based on the SUCRA values for TER and the incidence of adverse events was conducted to evaluate different interventions (Figure 8). A total of 10 interventions were included, which were grouped into four distinct clusters, each represented by a different color. Interventions such as MA+AI, AA, and EA demonstrated both high efficacy and good safety, making them the most favorable options. Although TEAS+CHM showed the best safety profile, its efficacy was inferior compared to the aforementioned interventions. MA+AA and MA+CHM exhibited relatively balanced profiles, with moderate-to-high efficacy and acceptable safety.
Figure 8

The cluster analysis, which demonstrates that the intervention measures have both good overall efficiency and safety performance.
4 Discussion
4.1 Main results
Our study assessed the effects of various acupuncture techniques—applied individually or in combination—on five key outcomes in patients with IH: TER, HSS, and quality-of-life parameters, including dietary, sleep, and mental status. TER, a commonly reported composite outcome in TCM research, is defined as the proportion of patients achieving predefined clinical improvement or cure (30). Its binary nature facilitates direct comparisons across interventions and reflects changes across multiple symptoms (68). HSS provides a continuous measure of symptom severity, encompassing frequency, intensity, and duration, allowing detection of partial yet clinically meaningful improvements (23). The impact of IH on patients' quality of life can be devastating (69). For example, cancer patients often avoid eating to prevent hiccup episodes, leading to malnutrition and delayed recovery (69–71). Hiccup-related sleep disturbances, such as doubled sleep latency, may induce chronic psychological stress and further frustrate patients with comorbid speech disorders (72, 73). This burden may worsen underlying conditions or provoke psychiatric symptoms, including poststroke depression (73, 74). Therefore, dietary, sleep and mental status were included as patient-centered secondary outcomes. These dimensions have been highlighted in prior meta-analyses on cancer-related and poststroke hiccups, showing that quality-of-life improvements often mirror symptom relief (27, 28).
The clinical benefits of acupuncture for IH observed in our NMA can be reconciled with mechanistic data at both peripheral and central levels. Hiccups are generated by a reflex arc involving vagal and phrenic afferents, brainstem networks (including the nucleus tractus solitarius and adjacent respiratory centers), and phrenic efferents (3–7). Acupuncture, particularly MA and EA, can regulate this reflex arc through multisite neural activation. Experimental studies have shown that EA improves gastric motility and heart rate variability via vagovagal modulation, reflecting enhanced parasympathetic tone and inhibition of abnormal reflex excitability (75, 76). At the spinal and supraspinal levels, EA has been demonstrated to modulate neuronal activity in specific autonomic circuits controlling gastrointestinal function (77) and to reduce aberrant excitability in reflex-related interneurons through TRPV1-dependent mechanisms (78). AA involves attaching Vaccaria seeds or magnetic beads to specific auricular points with appropriate pressure stimulation (79). The ear is richly innervated and vascularized, with dense neural networks—particularly involving the auricular branch of the vagus nerve—concentrated in the cavum conchae and triangular fossa (80). Gao et al. (81) suggest that stimulating these auricular points may activate the auricular branch of the vagus nerve, which, through the auricle–central–visceral axis, modulates visceral activities such as gastrointestinal motility to suppress hiccups. AI combines the mechanical stimulation of acupuncture with the pharmacologic effects of injected substances, producing synergistic modulation of local microcirculation and neurochemical signaling, which may further contribute to reflex inhibition (82). Compared with intramuscular injection, AI has been shown to reduce hiccup frequency and alleviate symptoms more effectively under the same dosage and medication conditions (22, 83). From a physiological perspective, by activating cutaneous afferents and downstream central networks, acupuncture can modulate autonomic outflow, inflammatory signaling, and neuroendocrine responses (84, 85). Together, these findings support that acupuncture alleviates IH through an integrated neurophysiological mechanism involving vagovagal reflex modulation, spinal inhibitory network activation, and neurochemical homeostasis restoration.
Our study yielded relatively reliable results by directly and indirectly comparing the effectiveness of different acupuncture interventions for IH. Regarding the TER, pairwise meta-analysis revealed that among monotherapies, AI, MA, EA, and AA were all more effective than CM. Moreover, combination therapies were generally superior to single modalities—for example, MA+AI was more effective than both AI and MA; MA+AA outperformed MA; TEAS+AI was superior to AI; and acupuncture combined with CM (e.g., MA+CM, EA+CM) was more effective than CM alone. According to the SUCRA-based probability ranking, MA+AI was the most effective, followed by TEAS+AI, MA+CM, and AI+CHM. In terms of reducing HSS, pairwise meta-analyses indicated that EA+CM was superior to CM, and MA—whether used alone or in combination with AI, AA, or CM—was consistently more effective than CM. The NMA results ranked EA+CM as the most effective for lowering HSS, followed by MA and MA+AA. In terms of quality of life, both MA monotherapy and its combination with AA demonstrated statistically significant improvements. NMA results further suggested that MA+AI was the most effective intervention across all quality-of-life domains, regardless of diet, sleep, or mental state. Overall, although effectiveness varied across different outcomes, MA+AI consistently ranked first for both TER and quality-of-life improvements. While its incidence of adverse events was not the lowest, MA+AI appears to be the optimal choice for treating IH, given its superior efficacy and acceptable safety profile. It should be noted that MA+AI was the most frequently reported intervention among studies evaluating TER (n = 8), and it generally outperformed the control group. This “high connection density” enhanced the statistical stability, amplified the therapeutic effect trend after aggregation, and thus formed the optimal result in the network comparison.
4.2 Limitations
Our review has important limitations that should be considered with caution. First, all included trials were conducted in China and published in Chinese, introducing substantial language and regional publication bias. Therefore, the results of this NMA chiefly reflect the clinical context and practice patterns in China. This concentrated geographic and linguistic source not only elevates the risk of selective reporting but also limits the external validity and generalizability of our findings to global clinical settings, where practitioner training, acupuncture techniques, standard care, and patient expectations may differ. Second, based on the confidence assessment results, all of the evidence levels range from “very low” to “moderate,” with none achieving a “high” level of certainty. This indicates that the overall quality of evidence supporting the comparative effectiveness of acupuncture interventions for IH remains suboptimal. The downgrading was primarily due to the high or unclear risk of bias, inconsistency among studies, and imprecision of the estimated effects. As acknowledged, blinding of acupuncturists and participants was not feasible because of the nature of acupuncture procedure. Moreover, most studies did not adequately describe allocation concealment or blinding of outcome assessors, resulting in potential performance and detection bias. These methodological weaknesses may have inflated the observed treatment effects. Participants who were aware of receiving active treatment may have experienced expectancy-related improvements, especially for subjective outcomes. Likewise, the absence of assessor blinding could introduce observer bias, further amplifying efficacy estimates. Since all outcomes in this study were based on self-reports or assessments by unblinded evaluators, the results are particularly vulnerable to such biases. In addition, the use of non-standardized outcome definitions also affects comparability across studies and may reduce the generalizability of the findings. Third, the node-splitting analysis revealed significant inconsistency in the comparisons involving MA vs. CM (P < 0.001). This may be attributed to the fact that MA–CM formed the core linkage of several triangular loops, amplifying any discrepancy between direct and indirect evidence. Clinically, MA and CM generally show relatively modest differences in efficacy, whereas the indirect comparisons often involve combination therapies with stronger effects (such as MA+AI or MA+AA). This imbalance in treatment magnitude may have exaggerated inconsistencies in the overall network. Additionally, variations in pharmacological regimens (Liu 2019 (2): chlorpromazine/Qiu 2017: anisodamine), acupoint selection, and needling manipulation across studies may further contribute to this divergence, thereby reducing the confidence in network estimates for the HSS. Fourth, none of the included studies involved a WL or SA, which restricts our ability to determine the specific efficacy of acupuncture interventions beyond nonspecific or placebo effects. Consequently, while the included trials demonstrate comparative effectiveness among active treatments, the absolute magnitude of benefit attributable solely to acupuncture remains unclear. Fifth, since the variety of acupuncture interventions, there are inconsistencies in acupoint selection, treatment duration and frequency, which may lead to heterogeneity. In addition, we suggest that acupuncture-related RCTs should be designed according to the CONSORT (86) and STRICTA (87) to control the quality of future studies.
5 Conclusion
This network meta-analysis highlights the effectiveness and safety of acupuncture in treating intractable hiccups within the clinical setting of China, particularly in terms of total effective rate, symptom relief, and quality of life improvement. After a comprehensive comparison of 15 different interventions, the results indicate that combination therapies outperform monotherapies. Manual acupuncture combined with acupoint injection emerged as the most effective approach for improving both total effective rate and quality of life, and given its favorable safety profile, it may represent the optimal treatment option for intractable hiccups. Nonetheless, the statistically generated favorable bias and numerical dominance that amplify the observed trend of efficacy should also be taken into account. On the other hand, electroacupuncture combined with conventional medications was the most effective for reducing hiccup symptoms. Of course, these findings are based on the premise that the primary diseases of intractable hiccups can be accurately diagnosed and appropriately treated. In clinical practice, the choice of therapy should also be tailored to the patient's specific condition. Given the limited number of existing studies and their suboptimal methodological quality, coupled with geographical and linguistic constraints, more rigorously designed mechanism studies and international, strictly conducted randomized controlled trials are needed to validate our findings.
Statements
Data availability statement
All data analyzed in this systematic review and network meta-analysis are derived from previously published studies. The full search strategies, list of included studies, and extracted data are available within the Supplementary material of this article. No new primary data were generated.
Author contributions
YZ: Conceptualization, Methodology, Resources, Software, Writing – original draft, Writing – review & editing. Y-YH: Conceptualization, Resources, Writing – review & editing. Z-FJ: Methodology, Writing – review & editing. GL: Data curation, Writing – review & editing. LD: Formal analysis, Investigation, Writing – review & editing. JC: Formal analysis, Investigation, Writing – review & editing. XT: Formal analysis, Methodology, Writing – review & editing. X-ML: Software, Writing – review & editing. HZhai: Formal analysis, Methodology, Writing – review & editing. R-LM: Formal analysis, Writing – review & editing. Z-XW: Investigation, Supervision, Writing – review & editing. HZhan: Funding acquisition, Investigation, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the “Xinglin Scholars” Subject Talent Research Promotion Plan of Chengdu University of Traditional Chinese Medicine (XKTD2021004) and the State Administration of Traditional Chinese Medicine 2022 National Famous Old Chinese Medicine Expert Inheritance Studio Construction Project.
Acknowledgments
The authors express their gratitude to the “Xinglin Scholars” Subject Talent Research Promotion Plan of Chengdu University of Traditional Chinese Medicine (XKTD2021004) and the State Administration of Traditional Chinese Medicine 2022 National Famous Old Chinese Medicine Expert Inheritance Studio construction project for their support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1676850/full#supplementary-material
Abbreviations
IH, intractable hiccups; RCT, randomized controlled trial; TCM, traditional Chinese medicine; WOS, web of science; CNKI, China national knowledge infrastructure; PRISMA, preferred reporting items for systematic reviews and meta-analyses; CI, confidence interval; SMD, standard mean difference; RR, risk ratio; MA, manual acupuncture; EA, electroacupuncture; TEAS, transcutaneous electrical acupoint stimulation; AI, acupoint injection; AA, auricular acupressure; CHM, Chinese herbal medicine; CM, conventional medications; SA, sham acupuncture; WL, waiting list; NMA, network meta-analysis; TER, total effective rate; HSS, hiccup symptom score; SUCRA, the surface under the cumulative ranking curve; CINeMA, the confidence in network meta-analysis system; GRADE, grading of recommendations assessment, development and evaluations.
References
1.
Moretto EN Wee B Wiffen PJ Murchison AG . Interventions for treating persistent and intractable hiccups in adults. Cochrane Database Syst Rev. (2013). doi: 10.1002/14651858.CD008768.pub2
2.
Rouse S Wodziak M . Intractable hiccups. Curr Neurol Neurosci Rep. (2018) 18:51. doi: 10.1007/s11910-018-0856-0
3.
He J Guan A Yang T Fu L Wang Y Wang S et al . Pathogenesis and treatment of perioperative hiccups: a narrative review. Ann Med. (2025) 57:2474173. doi: 10.1080/07853890.2025.2474173
4.
Steger M Schneemann M Fox M . Systemic review: the pathogenesis and pharmacological treatment of hiccups. Aliment Pharmacol Ther. (2015) 42:1037–50. doi: 10.1111/apt.13374
5.
Kohse EK Hollmann MW Bardenheuer HJ Kessler J . Chronic hiccups: an underestimated problem. Anesth Analg. (2017) 125:1169–83. doi: 10.1213/ANE.0000000000002289
6.
Kondo T Toyooka H Arita H . Hiccup reflex is mediated by pharyngeal branch of glossopharyngeal nerve in cats. Neurosci Res. (2003) 47:317–21. doi: 10.1016/S0168-0102(03)00225-6
7.
De Vloo P Dallapiazza RF Lee DJ Zurowski M Peng PW Chen R et al . Long-term relief of intractable hiccups with vagal nerve stimulation. Brain Stimul. (2018) 11:1385–7. doi: 10.1016/j.brs.2018.08.002
8.
Eisenächer A Spiske J . Persistent hiccups (singultus) as the presenting symptom of medullary cavernoma. Dtsch Arztebl Int. (2011) 108:822–6. doi: 10.3238/arztebl.2011.0822
9.
Al Deeb SM Sharif H Al Moutaery K Biary N . Intractable hiccup induced by brainstem lesion. J Neurol Sci. (1991) 103:144–50. doi: 10.1016/0022-510X(91)90157-3
10.
Amirjamshidi A Abbassioun K Parsa K . Hiccup and neurosurgeons: a report of 4 rare dorsal medullary compressive pathologies and review of the literature. Surg Neurol. (2007) 67:395–402. doi: 10.1016/j.surneu.2006.10.070
11.
Chang F-Y Lu C-L . Hiccup: mystery, nature and treatment. J Neurogastroenterol Motil. (2012) 18:123–30. doi: 10.5056/jnm.2012.18.2.123
12.
Wang B Jiang S . Progress of traditional Chinese medicine treatment of intractable hiccup. Res Integr Tradit Chin West Med. (2019) 11:316–8. doi: 10.3969/j.issn.1674-4616.2019.06.014
13.
Porzio G Aielli F Verna L Aloisi P Galletti B Ficorella C . Gabapentin in the treatment of hiccups in patients with advanced cancer: a 5-year experience. Clin Neuropharmacol. (2010) 33:179–80. doi: 10.1097/WNF.0b013e3181de8943
14.
Guo Z Liang Y Liu W Huang B Zheng H Cui S et al . Effectiveness and safety of acupuncture for cancer-related hiccups: a systematic review and meta-analysis. Front Neurol. (2024) 15:2024. doi: 10.3389/fneur.2024.1480656
15.
Gan D Liu Y Bi C Wang Z Wang Y Hu X et al . Nursing effective observation of acupoint acupuncture intervention on intractable hiccup after TACE for patients with hepatic carcinoma. J Sichuan Tradit Chin Med. (2020) 38:210–3.
16.
Hendrix K Wilson D Kievman MJ Jatoi A . Perspectives on the medical, quality of life, and economic consequences of hiccups. Curr Oncol Rep. (2019) 21:113. doi: 10.1007/s11912-019-0857-4
17.
Krakauer EL Zhu AX Bounds BC Sahani D McDonald KR Brachtel EF . Case 6-2005 — a 58-year-old man with esophageal cancer and nausea, vomiting, and intractable hiccups. N Engl J Med. (2005) 352:817–25. doi: 10.1056/NEJMcpc049037
18.
Kim JE Lee MK Lee DK Choi SS Park JS . Continuous cervical epidural block: treatment for intractable hiccups. Medicine. (2018) 97:e9444. doi: 10.1097/MD.0000000000009444
19.
Marinella MA . Diagnosis and management of hiccups in the patient with advanced cancer. J Support Oncol. (2009) 7:122–7, 30.
20.
Vanner RG . Gastro-oesophageal reflex and hiccup during anaesthesia. Anaesthesia. (1993) 48:92–3. doi: 10.1111/j.1365-2044.1993.tb06830.x
21.
Zhong R-C Liu X Guo H . Clinical observation of acupuncture combined with acupoint injection in the treatment of post-stroke intractable hiccup. Chin J Prim Med Pharm. (2017) 24:550–4.
22.
Chen Z-L . Observation on the therapeutic effect of haloperidol acupoint injection in the treatment of refractory hiccups in patients with cerebral infarction. Zhejiang J Integr Tradit Chin West Med. (2018) 28:838–40.
23.
Fan G-H Sun J-Y Xu X-X Song Y-N Ji J . Effect of press-needle in auricular points combined with acupoints in treating intractable hiccups induced by chemotherapy for lung cancer. J Clin Med Pract. (2021) 25:42–5. doi: 10.7619/jcmp.20212412
24.
Qin H-C Liu F-Y Wang X . Observation on the therapeutic effect of electroacupuncture on intractable hiccups after cardiothoracic surgery. World J Integr Tradit West Med. (2022) 17:1200–3. doi: 10.13935/j.cnki.sjzx.220625
25.
Liu Y . Observation on the Therapeutic Effect of Acupuncture Combined with Ear Acupoint Burying Beans in the Treatment of Intractable Hiccups After Stroke of Liver-Stomach Disharmony Type. Hefei, Anhui, China: Anhui University of Chinese Medicine (2019).
26.
Liu L . Effect of acupuncture on patients with intractable hiccups after stroke. Med J Chin People Health. (2019) 31:98–9. doi: 10.3969/j.issn.1672-0369.2019.24.041
27.
Choi T-Y Lee MS Ernst E . Acupuncture for cancer patients suffering from hiccups: a systematic review and meta-analysis. Complement Ther Med. (2012) 20:447–55. doi: 10.1016/j.ctim.2012.07.007
28.
Yue J Liu M Li J Wang Y Hung E-S Tong X et al . Acupuncture for the treatment of hiccups following stroke: a systematic review and meta-analysis. Acupunct Med. (2017) 35:2–8. doi: 10.1136/acupmed-2015-011024
29.
Hutton B Salanti G Caldwell DM Chaimani A Schmid CH Cameron C et al . The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. (2015) 162:777–84. doi: 10.7326/M14-2385
30.
Zheng X . Guiding Principles for Clinical Research of New Traditional Chinese Medicines: Trial Implementation. Beijing: China Medical Science and Technology Press (2002).
31.
Medicine SAoTC . Standards for Diagnostic and Efficacy of Traditional Chinese Medicine Diseases and Syndrome. Nanjing: Nanjing University Press (1994).
32.
Nikolakopoulou A Higgins JPT Papakonstantinou T Chaimani A Del Giovane C Egger M et al . CINeMA: an approach for assessing confidence in the results of a network meta-analysis. PLoS Med. (2020) 17:e1003082. doi: 10.1371/journal.pmed.1003082
33.
Guyatt G Oxman AD Akl EA Kunz R Vist G Brozek J et al . GRADE guidelines: 1. introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. (2011) 64:383–94. doi: 10.1016/j.jclinepi.2010.04.026
34.
Gao L-Y . Observation on the therapeutic effect of acupuncture and medicine on intractable hiccups. Guangzhou: Prevention and Treatment of Cardiovascular Disease (2015). p. 117–9.
35.
Ke M-Z . Observation on the therapeutic effect of oral administration of Banxia Houpu decoction combined with acupoint injection in the treatment of intractable hiccups. Guangxi J Tradit Chin Med. (2015) 38:41–2.
36.
Li C-X . Therapeutic observation of electroacupuncture for post-operative intractable hiccups. Shanghai J Acupunct Moxibust. (2015) 34:737–8. doi: 10.13460/j.issn.1005-0957.2015.08.0737
37.
Liao W Yu T Zhao G-Y . The efficacy observation of acupuncture to stimulate phrenic nerve in the treatment of intracranial tumor postoperative intractable hiccups. Chin Mod Doctor. (2015) 53:124–6.
38.
Lin L-R . Observing Clinical Efficacy on Intractable Hiccups Treated by Metoclopramide Point Injection Combination with Body Acupuncture. Wuhan, Hubei, China: Hubei University of Chinese Medicine (2015).
39.
Song X-X . Observation on the therapeutic effect of acupuncture combined with medicine in the treatment of intractable hiccups after stroke. Shanxi J Tradit Chin Med. (2015) 31:31.
40.
Zhang H-M Yang B . Clinical observation on curative effect of acupuncture treatment for intractable hiccup by modulating fu and qi. Chin J Acupunct Moxibust. (2015) 4:8–9. doi: 10.3877/cma.j.issn.2095-3240.2015.02.003
41.
Zhang Y-N . Observation on the therapeutic effect of Xuanfu Daizhe decoction combined with electroacupuncture in the treatment of intractable hiccups. Chin J Trauma Disabil Med. (2015) 23:108–9. doi: 10.13214/j.cnki.cjotadm.2015.12.084
42.
Zhang G-Y Su Q . Effect of acupoint transcutaneus electrical nerve stimulation combined with ritalin on intractable hiccup for stroke patients. J Nurs. (2015) 22:66–7. doi: 10.16460/j.issn1008-9969.2015.14.066
43.
Cao Y-H . Breathing Reducing Method is Given Priority to Acupuncture Clinical Research for the Treatment of Intractable Hiccups. Changchun, Jilin, China: Changchun University of Chinese Medicine (2016).
44.
Guo G-T Yuan B-F Li T-F . Clinical observation on the treatment of intractable hiccups by acupuncture of Yuyao and Zhongkui. J Anhui Univ Chin Med. (2016) 35:65–7. doi: 10.3969/j.issn.2095-7246.2016.03.021
45.
Liu L-R Bai J-P Li Y Liu Y-H Zhu Y-J Qu Y-C . Effects of acupuncture combined with xuanfudaizhe decoction on intractable hiccups caused by cisplatin-based chemotherapy. J Chengdu Univ Tradit Chin Med. (2016) 39:74–6+89. doi: 10.13593/j.cnki.51-1501/r.2016.03.074
46.
Wu Q-X Yue Y-Y Wu X-J Zhao H-B . Clinical observation on 30 cases of intractable hiccups treated with chlorpromazine acupoint injection into Zusanli. J North Pharm. (2016) 13:192–3.
47.
Guo Q-F . The Clinical Effect Observation on the Treatment of Intractable Hiccups with Neck Paravertebrals Acupuncture as the Main Method. Kunming, Yunnan, China: Yunnan University of Traditional Chinese Medicine (2017).
48.
Qiu W-Z . Clinical Study on the Treatment of Intractable Hiccups Based on Acupoints of Yangbai Penetrating Yuyao. Changchun, Jilin, China: Changchun University of Chinese Medicine (2017).
49.
Fan R-H Liu L-L Shu P . Randomized parallel control study of acupuncture combined with methochloropamine injection at two sides of Zusanli acupoint for treatment of intractable diaphragm spasm(hiccup). J Pract Tradit Chin Intern Med. (2018) 32:40–2. doi: 10.13729/j.issn.1671-7813.Z20180030
50.
Li W-H Bai L-J . Acupuncture at cuanzhu (BL 2) and tianding (LI 17) in the treatment of intractable hiccup for 30 cases. Chin Med Mod Distance Educ China. (2018) 16:128–9. doi: 10.3969/j.issn.1672-2779.2018.10.056
51.
Wang H . Observation on the therapeutic effect of acupuncture at Shuigou acupoint combined with auricular acupuncture for the treatment of intractable hiccups after cerebral hemorrhage. Hubei J Tradit Chin Med. (2018) 40:46–8.
52.
Yang C-P . Clinical Observation on the Therapeutic Effect of Auricular Acuppressure Combined with Acupuncture Therapy in the Treatment of Intractable Hiccups Caused by Radiotherapy and Chemotherapy of Malignant Tumors. Shenyang, Liaoning, China: Liaoning University of Traditional Chinese Medicine (2018).
53.
Zhang S-K Gao W-B Liu Y He H . Therapeutic effect of cervical Jiaji electroacupuncture on postoperative intractable hiccup of liver neoplasms. Chin J Oncol. (2018) 40:138–40. doi: 10.3760/cma.j.issn.0253-3766.2018.02.011
54.
Shen L-L . Study on the efficacy of acupuncture therapy in treating intractable hiccups. Contemp Med Symp. (2019) 17:79–80.
55.
Gao J-L Gao H . Observation on the curative effect of 30 cases of obstinate hiccup treated by Cuan Zhu acupoint with strong stimulation of electro-acupuncture dilatational wave. J Yangzhou Polytech Coll. (2019) 23:41–4. doi: 10.15954/j.cnki.cn32-1529/g4.2019.04.011
56.
Liu H-C . Clinical effect of auricular acupuncture and needle embedding in the treatment of patients with intractable hiccups. Med Equip. (2019) 32:112–3.
57.
Wang J-H . Analysis of the value of acupuncture in treating intractable hiccups after stroke. Guide Chin Med. (2019) 17:170–1. doi: 10.15912/j.cnki.gocm.2019.18.138
58.
Liu Y . Clinical Study on the Treatment of Obstinate Hiccup by Acupuncture and Injection at Cervical Spine. Kunming, Yunnan, China: Yunnan University of Chinese Medicine (2020).
59.
Lu Y-Y . Clinical observation on electroacupuncture combined with itopride in the treatment of intractable hiccups. Chin Health Care Nutr. (2020) 30:339.
60.
Huang Y-W Wang T-F . Clinical observation on the therapeutic effect of acupuncture on intractable hiccups after radiotherapy and chemotherapy of tumors. Health Care Guide. (2021) 35.
61.
Luo Y-J . Clinical study on Wuzhuyu decoction combined with low-frequency pulse electrotherapy in the treatment of intractable hiccups after stroke. Shaanxi J Tradit Chin Med. (2021) 42:1379–81+1403. doi: 10.3969/j.issn.1000-7369.2021.10.013
62.
Ouyang G Xu G-J . Effect of acupoint injection of metoclopramide combined with acupuncture in the treatment of patients with intractable hiccups. Med J Chin People Health. (2021) 33:61–3. doi: 10.3969/j.issn.1672-0369.2021.12.025
63.
Wang Z-B . Clinical effect of traditional Chinese medicine acupuncture combined with Xuefu Zhuyu decoction in the treatment of patients with intractable hiccups. Med Equip. (2021) 34:47–8.
64.
Yang L-L Wang Z Ye P-Z . Clinical observation of point-through-point acupuncture combined with traditional Chinese medicine in the treatment of intractable hiccup after radiotherapy and chemotherapy for malignant tumor. Chin Med Herald. (2021) 18:135–8. doi: 10.20047/j.issn1673-7210.2021.02.034
65.
Li B-G Zhang D-S . Clinical study on the treatment of intractable hiccups with three needles. Chin Med Mod Distance Educ China. (2022) 20:111–4. doi: 10.3969/j.issn.1672-2779.2022.17.041
66.
Xu Z-D Pan W-J Xie D . Clinical observation on acupuncture and moxibustion treatment of severe craniocerebral injury complicated with intractable hiccup. Capital Food Med. (2023) 30:166–8.
67.
Wang J-K . Observation on the therapeutic effect of combined traditional Chinese and western medicine in treating intractable hiccups after stroke. J Pract Trad Chin Med. (2024) 40:578–80.
68.
Zhang Y-Y Shen C Zhang Y Liu J-P . Misunderstandings in using “total effective rate” as an index for evaluating the therapeutic effect of traditional Chinese medicine. Chin J Drug Eval. (2020) 37:337–40.
69.
Palese A Condolo G Dobrina R Skrap M . Persistent hiccups in advanced neuro-oncology patients: findings from a descriptive phenomenological study. J Hosp Palliat Nurs. (2014) 16:396–401. doi: 10.1097/NJH.0000000000000087
70.
Ge AXY Ryan ME Giaccone G Hughes MS Pavletic SZ . Acupuncture treatment for persistent hiccups in patients with cancer. J Altern Complement Med. (2010) 16:811–6. doi: 10.1089/acm.2009.0456
71.
Moro C Sironi P Berardi E Beretta G Labianca R . Midazolam for long-term treatment of intractable hiccup. J Pain Symptom Manage. (2005) 29:222–3. doi: 10.1016/j.jpainsymman.2005.01.001
72.
Arnulf I Boisteanu D Whitelaw WA Cabane J Garma L Derenne JP . Chronic hiccups and sleep. Sleep. (1996) 19:227–31.
73.
Ferdinand P Oke A . Intractable hiccups post stroke: case report and review of the literature. J Neurol Neurophysiol. (2012) 3:140. doi: 10.4172/2155-9562.1000140
74.
Maximov GK Kamnasaran D . The adjuvant use of lansoprazole, clonazepam and dimenhydrinate for treating intractable hiccups in a patient with gastritis and reflux esophagitis complicated with myocardial infarction: a case report. BMC Res Notes. (2013) 6:327. doi: 10.1186/1756-0500-6-327
75.
Imai K Ariga H Chen C Mantyh C Pappas TN Takahashi T . Effects of electroacupuncture on gastric motility and heart rate variability in conscious rats. Auton Neurosci. (2008) 138:91–8. doi: 10.1016/j.autneu.2007.11.003
76.
Lu M-J Yu Z He Y Yin Y Xu B . Electroacupuncture at ST36 modulates gastric motility via vagovagal and sympathetic reflexes in rats. World J Gastroenterol. (2019) 25:2315–26. doi: 10.3748/wjg.v25.i19.2315
77.
Zhang M-t Liang Y-f Dai Q Gao H-r Wang H Chen L et al . A spinal neural circuit for electroacupuncture that regulates gastric functional disorders. J Integr Med. (2025) 23:56–65. doi: 10.1016/j.joim.2024.11.005
78.
Guo Z-L Fu L-W Su H-F Tjen-A-Looi SC Longhurst JC . Role of TRPV1 in acupuncture modulation of reflex excitatory cardiovascular responses. Am J Physiol Regul Integr Comp Physiol. (2018) 314:R655–66. doi: 10.1152/ajpregu.00405.2017
79.
Jiang Z-F Liu G Sun X-X Zhi N Li X-M Sun R et al . Auricular acupressure for constipation in adults: a systematic review and meta-analysis. Front Physiol. (2023) 14:1257660. doi: 10.3389/fphys.2023.1257660
80.
Tu N-F Zhang Y-H Xu M . Analysis of acupoint selection rules for auricular acupressure in the treatment of intractable hiccups based on data mining. J Nurs Sci. (2024) 39:48–51. doi: 10.3870/j.issn.1001-4152.2024.13.048
81.
Gao X-Y . Auricular Acupuncture Therapy and Auriculo-Vagi-Visceral Reflex. Beijing, China: China Academy of Chinese Medical Sciences (2005).
82.
Sha T Gao LL Zhang CH Zheng JG Meng ZH . An update on acupuncture point injection. QJM. (2016) 109:639–41. doi: 10.1093/qjmed/hcw055
83.
Kong L-C Zhang D-W Fan S Zhang H-T . Zusanli acupoint injection combined with haloperidol in the treatment of 30 cases of prolonged hiccups after cerebral hemorrhage. Chin Med Res. (2018) 31:62–3. doi: 10.3969/j.issn.1001-6910.2018.04.25
84.
He T Zheng Y Yan J Xia Y Wang B Zhang Z et al . Skin-brain axis: neural pathways in acupuncture treatment. Chin Med. (2025) 20:163. doi: 10.1186/s13020-025-01213-y
85.
Fan Z Dou B Wang J Wu Y Du S Li J et al . Effects and mechanisms of acupuncture analgesia mediated by afferent nerves in acupoint microenvironments. Front Neurosci. (2024) 17:1239839. doi: 10.3389/fnins.2023.1239839
86.
Schulz KF Altman DG Moher D . CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. (2010) 340:c332. doi: 10.1136/bmj.c332
87.
MacPherson H Altman DG Hammerschlag R Youping L Taixiang W White A et al . Revised standards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. PLoS Med. (2010) 7:e1000261. doi: 10.1371/journal.pmed.1000261
Summary
Keywords
intractable hiccups, acupuncture therapy, effectiveness, network meta-analysis, systematic review, randomized controlled trials
Citation
Zhai Y, Hui Y-Y, Jiang Z-F, Liu G, Ding L, Cheng J, Tang X, Li X-M, Zhai H, Ma R-L, Wan Z-X and Zhang H (2025) Effectiveness and safety of acupuncture therapies for intractable hiccups: a systematic review and network meta-analysis. Front. Med. 12:1676850. doi: 10.3389/fmed.2025.1676850
Received
28 August 2025
Accepted
03 November 2025
Published
19 November 2025
Volume
12 - 2025
Edited by
Xuancheng Zhou, Southwest Medical University, China
Reviewed by
Weixing Pan, Howard Hughes Medical Institute (HHMI), United States
Yanjuan Song, Hubei University of Chinese Medicine, China
Updates
Copyright
© 2025 Zhai, Hui, Jiang, Liu, Ding, Cheng, Tang, Li, Zhai, Ma, Wan and Zhang.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hong Zhang, hzhang0123@foxmail.com; Zhao-Xin Wan, 873284730@qq.com
†These authors have contributed equally to this work and share first authorship
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.