 Tommaso Pettenuzzo1,2†
Tommaso Pettenuzzo1,2† Francesco Zarantonello2†Alessandro Zambianchi1Gianluca Lumetti1Domenico Ruggerini1Giorgia Pacchiarini2
Francesco Zarantonello2†Alessandro Zambianchi1Gianluca Lumetti1Domenico Ruggerini1Giorgia Pacchiarini2 Elisa Pistollato2Valentina Fincati1
Elisa Pistollato2Valentina Fincati1 Giulia Mormando1
Giulia Mormando1 Alessandro De Cassai1,2
Alessandro De Cassai1,2 Nicolò Sella1,2*
Nicolò Sella1,2* Annalisa Boscolo1,2,3‡$Paolo Navalesi1,2‡$
Annalisa Boscolo1,2,3‡$Paolo Navalesi1,2‡$- 1Department of Medicine, University of Padua, Padua, Italy
- 2Institute of Anesthesia and Intensive Care, University Hospital of Padua, Padua, Italy
- 3Department of Cardiac, Thoracic, Vascular Sciences, and Public Health, University of Padua, Padua, Italy
Mechanical ventilation is a fundamental intervention in intensive care medicine, providing vital support for patients with severe respiratory failure. However, this life-sustaining therapy also carries the risk of harm. Ventilator-induced lung injury (VILI) is now predominantly understood in terms of lung overdistension, characterized by excessive stress and strain on pulmonary tissue. In recent years, a variety of novel monitoring strategies have emerged, from refined measurements of respiratory mechanics to advanced imaging and physiologic modeling, to help in bedside detection of excessive lung stress and strain. Electrical impedance tomography is a non-invasive tool providing real-time imaging of regional ventilation and assisting in the diagnosis of overdistension and its minimization through positive end-expiratory pressure titration, also during partial support ventilation. Pleural and lung ultrasound might also suggest the occurrence of overdistension, although clinical data are still preliminary. Bedside maneuvers, such as changing patient positioning or applying abdominal weights, can help identify overdistension by observing change in respiratory mechanics. Ventilator-based methods like the recruitment-to-inflation ratio and the overdistension index help assess the risk of overdistension, despite requiring careful interpretation and validation. Biomarkers such as Clara cell secretory protein-16 and stretch-induced gene signatures represent a promising avenue for real-time monitoring of lung injury, though further validation is needed. These tools aim to help clinicians individualize ventilator settings, balancing adequate gas exchange with lung protection. Despite this progress, most techniques remain in the realm of research. Few have undergone the rigorous physiological and clinical validation necessary for routine bedside use. As the critical care community moves toward more personalized ventilation strategies, establishing reliable, real-time methods to assess lung stress and strain at the bedside will be key to translating innovation into improved patient outcomes.
Introduction
The notion that mechanical ventilation can be harmful dates back centuries. In 1744, John Fothergill described the successful resuscitation of an apneic and pulseless coal miner by William Tossach, who used mouth-to-mouth ventilation to inflate the patient’s lungs and restore a heartbeat. Fothergill also expressed concern that mechanical bellows might cause more harm than manual insufflation, as the force delivered by bellows could not be regulated as precisely as a human breath. This early recognition of potential harm from mechanical ventilation foreshadowed the modern concept of ventilator-induced lung injury (VILI) (1).
In the 1940s, Macklin and Macklin demonstrated that elevated airway pressures could rupture alveolar walls, allowing air to dissect into surrounding tissues, an observation that contributed to the definition of “barotrauma” (1). In the 1960s, growing concern over oxygen toxicity, particularly based on studies in animals and neonates, led clinicians to favor high tidal volumes (Vt) as a means of improving oxygenation while avoiding the risks associated with high fractions of inspired oxygen (FiO₂) (1). As a result, in the early era of modern mechanical ventilation, barotrauma became a frequent complication, spurring significant research into its pathophysiology.
A pivotal 1974 study by Webb and Tierney demonstrated in animal models that high distending pressures could cause fatal pulmonary edema, highlighting the risks of excessive lung stretch (2). In 1988, Dreyfuss and colleagues showed that lung injury was primarily due to excessive end-inspiratory lung volume rather than airway pressure alone, laying the foundation for the concept of “volutrauma” (3).
The distinction between barotrauma and volutrauma is theoretical, as lung overdistension results from any Vt that generates an excessive transpulmonary pressure, i.e., the transmural pressure gradient across the alveolar wall (4). The primary mechanical determinants of lung overdistension for a given Vt are lung compliance, airway pressure variation and the pressure generated by inspiratory muscles (5). Lower lung compliance implies a smaller aerated lung volume, leading to greater dynamic lung strain, defined as the ratio of Vt to resting lung volume (6). Additionally, reduced lung compliance lowers the ratio of lung to total respiratory system compliance, resulting in higher end-inspiratory transpulmonary pressure (lung stress) for a given airway pressure (4). Finally, stronger inspiratory efforts in patients receiving partial ventilatory support also increase end-inspiratory transpulmonary pressure by generating excessively negative pleural pressure (5).
Several studies provide strong evidence that VILI increases mortality in patients receiving controlled mandatory ventilation (7). Therefore, timely and accurate assessment of lung stress and strain is key to improving patients’ outcomes. Each of the static components of the respiratory cycle, namely tidal volume (Vt), plateau pressure (Pplat), and positive end-expiratory pressure (PEEP), may require adjustment in order to mitigate the risk of lung overdistension. The individual patient’s response to these ventilator settings should be evaluated to balance their benefits and potential side effects. For example, PEEP may be beneficial in patients with adequate potential for lung recruitment, reducing atelectrauma (injury related to the repetitive opening and closing of alveolar units), while minimizing dynamic strain and improving ventilation-perfusion matching and oxygenation. Conversely, in patients with limited recruitment potential, high PEEP levels may lead to overdistension, increased dead space, and hemodynamic compromise (8).
Over the years, various techniques have been proposed to estimate lung stress and strain at the bedside, including assessment of breathing patterns and respiratory mechanics (e.g., Vt, Pplat, driving pressure [ΔP], transpulmonary pressure [Ptp], stress index [SI], C20/C ratio) (7, 9–11), as well as chest computed tomography (CT) (12). Recently, several innovative methods have emerged as promising tools to estimate the risk of lung overdistension. Imaging modalities, such as pleural and lung ultrasound (LUS) and electrical impedance tomography (EIT), have shown growing utility. Novel applications of respiratory mechanics, assessed directly at the ventilator following specific changes in ventilator settings or patient positioning, may also provide valuable insights.
The aim of this narrative review is to present emerging techniques that, over the last few years, have shown potential to support critical care physicians in identifying non-physiologic stress and strain at the bedside (Table 1). As such, we will not discuss other mechanisms of VILI, such as atelectrauma and ergotrauma (injury resulting from mechanical energy delivered to the respiratory system during each breath) (13), nor will we address the hemodynamic effects of non-physiologic stress and strain (5).
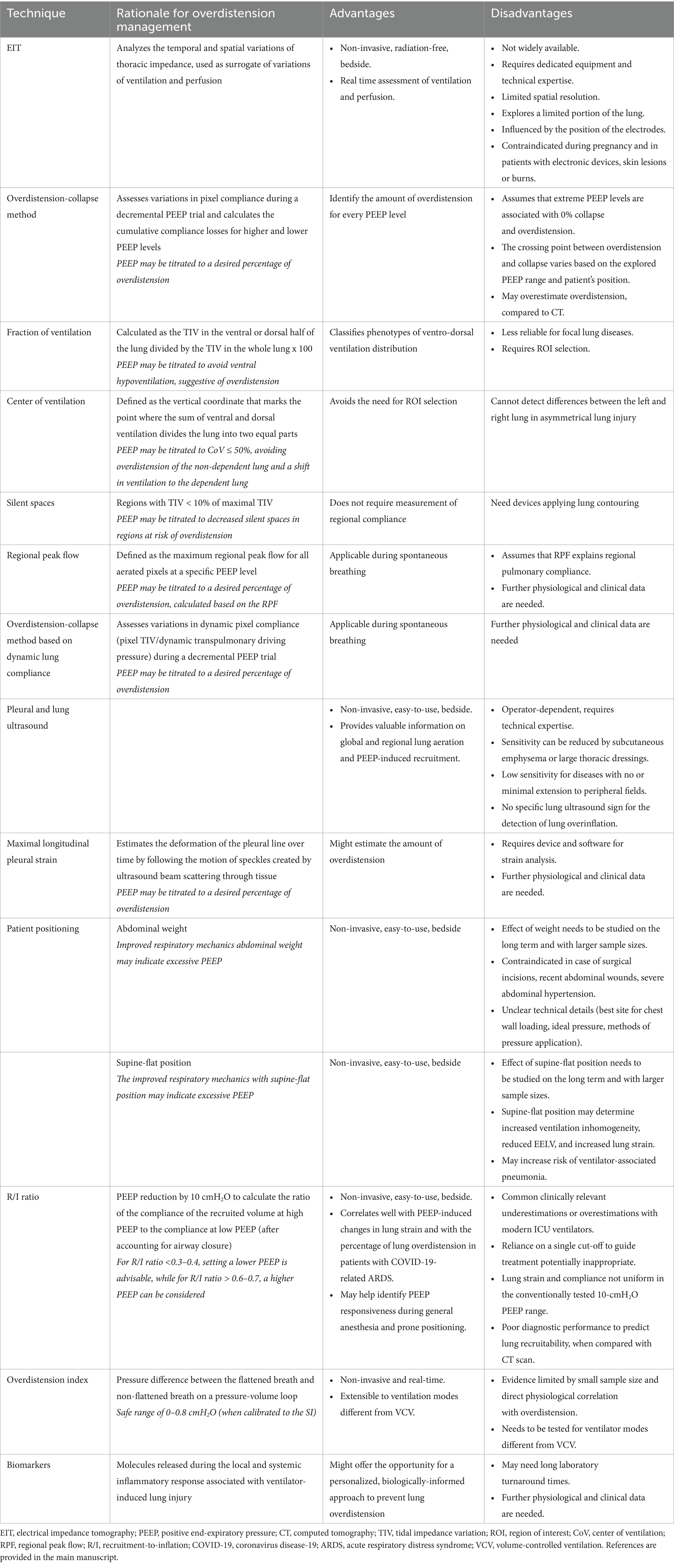
Table 1. New frontiers in bedside assessment of lung stress and strain.
Electrical impedance tomography
EIT is a non-invasive, radiation-free, and validated bedside technique for real-time, continuous evaluation of the regional distribution of ventilation and perfusion (14). EIT analyzes the temporal and spatial variations in thoracic impedance in response to very small alternating electrical currents applied through pairs of electrodes embedded in a belt wrapped around the patient’s chest (14). Impedance variations during air and blood movement are used as surrogates for ventilation and perfusion, respectively (14).
Multiple applications of EIT in both invasive and non-invasive mechanical ventilation have been described (15). One of the most common is PEEP titration, which is critical for enhancing the physiological benefits, while minimizing the potential adverse effects, of PEEP. During a decremental PEEP trial, regional compliance changes are estimated pixel by pixel as the ratio of tidal impedance variation (TIV), defined as the amplitude of impedance changes between end-expiration and end-inspiration, to ΔP, calculated as the difference between Pplat and PEEP (16). Compliance losses at higher and lower PEEP levels are interpreted as overdistension and collapse, respectively, and summed across all pixels in the lung region where the belt is positioned. The optimal PEEP is typically defined as the level corresponding to the intersection point of the cumulative compliance loss curves across the explored PEEP range, representing the minimal difference between the percentages of overdistension and collapse (16). This “overdistension-collapse method” has been primarily applied for PEEP selection during continuous mandatory ventilation (15). Despite known limitations (Table 1), this technique offers a unique opportunity to quantify and monitor the regional extent of overdistension and to adjust PEEP to target a desired level.
Alternative EIT-based approaches for PEEP titration aiming at minimizing overdistension assess changes in the spatial distribution of TIV. A decrease in TIV, especially in non-dependent lung regions, after a PEEP increase, may indicate regional overdistension (17). These distributional ventilation changes can be quantified using the dorsal-to-global or ventral-to-global ventilation fractions, calculated as the proportion of ventilation occurring in the dorsal or ventral regions, respectively, relative to total ventilation detected in the image. In a cohort of 128 postoperative patients at high risk for pulmonary complications, a ventilation pattern characterized by dorsal predominance and ventral hypoventilation, suggestive of ventral overdistension, was associated with higher complication rates and delayed oxygen weaning (18, 19).
PEEP can also be titrated by assessing changes in compliance across four horizontal lung regions following a PEEP increase, to evaluate recruitability, and ΔP reduction, to evaluate alveolar cycling and overdistension (20). In 20 patients with ARDS, this EIT-based protocol led to improved oxygenation and reduced alveolar cycling without promoting global overdistension (20).
The ventro-dorsal center of ventilation (CoV) represents the weighted geometric center of the ventilation distribution (21). A CoV greater than 50% indicates predominant dependent ventilation and may suggest overinflation of the non-dependent (ventral) lung, thereby assisting in the identification of excessive PEEP (22).
An increase in “silent spaces,” defined as those pixels exhibiting less than a specified percentage of the maximum TIV, within regions at risk for overdistension (e.g., above the CoV) may support the decision to reduce PEEP (23–25). In 43 patients with coronavirus disease-19 (COVID)-associated acute respiratory distress syndrome (ARDS), Taenaka et al. found that, among patients with high lung recruitability, the combination of high PEEP and prone positioning achieved the best oxygenation and minimized dependent silent spaces (indicative of potential collapse), without increasing non-dependent silent spaces (indicative of overdistension). In contrast, among low recruiters, high PEEP, compared to low PEEP, increased non-dependent silent spaces, in both supine and prone positions (25).
EIT also allows quantitative estimations of the overall degree of spatial ventilation heterogeneity. The global inhomogeneity index (GI) is calculated as the sum of the differences between each pixel’s TIV and the median TIV, normalized by the total TIV within the lung area (26). In a series of 14 patients with ARDS and chronic obstructive pulmonary disease, a PEEP titration strategy based on the minimum GI index value, compared to the ARDS Network lower PEEP/FiO2 table, improved the ventilatory ratio, reduced mechanical power, and enhanced cardiac index and oxygen delivery (27). However, some reports found this strategy to be associated with higher ΔP and overdistension, compared to other methods of PEEP titration (28).
Finally, EIT enables detection of regional aeration changes and quantification of regional strain (29) and may aid in identifying regional overdistension (30) and predicting PEEP responsiveness (31).
Although EIT is not yet widely available, requires technical expertise, and presents some contraindications and limitations (14) and although many EIT-derived techniques for assessing overdistension still lack physiological and clinical validation, EIT remains a promising tool to complement other strategies for the prevention and diagnosis of lung overdistension (Table 1). Preliminary clinical evidence suggests that EIT-guided PEEP titration may be associated with improved respiratory system mechanics and patient survival (32).
Pleural and lung ultrasound
Pleural and lung ultrasound (LUS) is a non-invasive, easy-to-use bedside tool that, despite known limitations (33), provides valuable information not only on global and regional lung aeration but also on PEEP-induced recruitment (34). Some experts have suggested that reduced lung sliding in non-dependent regions may be indicative of lung overdistension (35). However, clinical evidence remains very limited.
Tonelotto et al. observed that, in 18 patients with healthy lungs under general anesthesia, the presence of six or more horizontal reverberation lines may indicate lung overdistension, as evaluated by EIT (36). Preliminary clinical data from pilot studies have explored the use of pleural strain measurement, defined as the deformation of the pleural line over time, for this purpose. In a study involving 10 patients undergoing general anesthesia for elective surgery, Girard et al. demonstrated the feasibility and reproducibility of pleural strain measurement using ultrasound elastography, which showed significant correlations with Vt (37). Maximal longitudinal pleural strain (MLPS), assessed by speckle tracking, an ultrasound technique following the motion of speckles created by ultrasound beam scattering through tissue, has also been suggested for this purpose. In a recent study of 30 patients with acute hypoxemic respiratory failure, Persona et al. found a significant correlation between MLPS and PEEP-induced overdistension, as estimated by EIT. Specifically, an MLPS value <10 was associated with EIT-derived overdistension ≥10%, while values <7 were indicative of severe overdistension (≥30%) (38).
These findings are extremely preliminary and warrant confirmation in larger patient cohorts, as well as validation using other techniques, such as chest CT, before LUS can be considered a reliable tool for assessing lung overdistension (Table 1).
Bedside maneuvers
In addition to instrumental techniques, several bedside maneuvers have been proposed to offer clinically useful insights into lung overdistension (Table 1). Recent studies, primarily involving patients with COVID-19-related ARDS, have reported that applying an external weight to the sternum or abdomen paradoxically reduces airway pressure, Pplat, and ΔP, while increasing respiratory system compliance, contrary to expected physiological responses (39). This counterintuitive phenomenon has been termed the “mechanical paradox” (40).
In 2025, Pacchiarini et al. conducted a prospective interventional study to investigate the underlying mechanisms of this paradox (39). Twenty patients receiving invasive mechanical ventilation for acute hypoxemic respiratory failure were enrolled and studied during a decremental PEEP trial under EIT and esophageal pressure monitoring. Variable external weights were applied to the abdomen to induce a 5-mmHg increase in intra-abdominal pressure. At each PEEP level, three sequential phases were performed: weight-off, weight-on, and weight-off. The study demonstrated that the physiological response to abdominal loading depended on whether lung overdistension or collapse was predominant. In cases where PEEP-induced overdistension prevailed, i.e., PEEP levels above the EIT-defined optimal PEEP according the overdistension-collapse method, abdominal loading led to a decrease in peak, plateau, and driving pressures and an increase in both lung and respiratory system compliance. These effects were accompanied by a reduction in end-expiratory lung impedance (EELI), likely reflecting a decrease in end-expiratory lung volume (EELV). The effect of the abdominal weight needs to be studied over the long term and in larger sample sizes and the optimal pressure to apply, as well as the method of application, remains unclear. However, these findings suggest that abdominal loading may serve as a simple bedside maneuver to identify overdistension and assist in PEEP titration. Specifically, a decrease in peak, plateau, and driving pressures in response to abdominal weight application may indicate excessive PEEP, which should be adjusted downward.
Patient positioning is also a critical determinant of respiratory mechanics in both the operating room and the intensive care unit (ICU). Recent evidence indicates that certain positions may influence the risk of overdistension. Pearce et al. evaluated the effects of supine versus semi-recumbent positioning in 14 mechanically ventilated patients with ARDS (41). Using EIT and standard respiratory mechanics, they showed that moving from a semi-recumbent (35–40°) to a supine-flat position significantly improved respiratory system compliance and reduced ΔP. This positional change was also associated with a mild ventral redistribution of ventilation, potentially relieving ventral overdistension caused by gravitational pleural pressure gradients from the lung apex to base (41).
Similar findings were reported by Marrazzo et al. in two studies on patients with COVID-19-associated ARDS. In the first study, reducing trunk inclination from 40° to 0° significantly decreased end-inspiratory Ptp and increased lung compliance (42). The second study confirmed these results and further demonstrated improved ventral regional compliance and redistribution of tidal ventilation toward ventral regions in the supine-flat position. These improvements were attributed primarily to reduced lung overdistension, as also reflected by an improved ventilatory ratio (43).
Additionally, Bouchant et al. studied 30 patients with ARDS undergoing progressive trunk elevation (from 30° semi-seated to 0°, 30°, 60°, and 90° verticalization without body flexion). They found that both transpulmonary ΔP and EELV, as estimated using the nitrogen wash-in/wash-out method, increased progressively up to the straight 60° position, while lung strain decreased until the straight 30° position (44). These results suggest that verticalizing the patient from 0° to 60° may promote alveolar recruitment but at the cost of increased overdistension and reduced ventilator efficiency.
Overall, these findings support the potential utility of a simple and widely applicable maneuver, i.e., placing the patient in a supine-flat position, to help identify lung overdistension. Such a maneuver may prompt re-evaluation of ventilator settings, such as PEEP, once the patient is returned to the semi-recumbent position, which remains the recommended posture due to its association with a lower risk of ventilator-associated pneumonia (44).
Mechanical ventilator maneuvers
Some recently described mechanical ventilator maneuvers may aid in assessing the risk of lung overdistension during invasive mechanical ventilation (Table 1).
Chen et al. validated a single-breath bedside method to estimate lung recruitability in patients with ARDS, including those with airway closure. Forty-five patients underwent an abrupt PEEP reduction from 15 to 5 cmH2O, and the recruitment-to-inflation (R/I) ratio was calculated as the ratio of the compliance of the recruited volume at high PEEP to the compliance at low PEEP. Based on the median R/I ratio of the study population, patients were classified as high recruiters (R/I ratio ≥ 0.5) or low recruiters (R/I ratio < 0.5). In 41 patients with airway closure below 15 cmH2O, the recruited volume estimated by this single-breath method correlated strongly with the reference pressure-volume curve method (45).
Despite several limitations (Table 1), the R/I ratio is a promising tool for bedside assessment of PEEP-related protection against lung overdistension. It has been shown to correlate well with PEEP-induced changes in lung strain (46, 47). Furthermore, it demonstrated a strong inverse correlation with the percentage of lung overdistension, as measured by EIT, in patients with COVID-19-related ARDS (25, 48). A weaker but still significant correlation was also observed in patients undergoing ultraprotective ventilation during veno-venous extracorporeal membrane oxygenation support (49). Moreover, the R/I ratio may help identify PEEP responsiveness during general anesthesia and prone positioning (50, 51).
Recruitment maneuvers (RMs), although potentially beneficial for reopening collapsed alveoli, may induce overdistension in already well-aerated regions, leading to clinically evident barotrauma, worsened ventilation-perfusion mismatch, and hemodynamic compromise (52). Recently, Santarisi et al. performed a post-hoc analysis of the EPVent2 trial, a multicenter, randomized, phase II study comparing a Ptp-guided ventilation strategy to a high-PEEP strategy for improving 28-day mortality and ventilator-free days in patients with ARDS (53). The authors examined the dose–response relationship between end-inspiratory Ptp after RM and subsequent changes in lung elastance as a surrogate of overdistension. Their results demonstrated that higher end-inspiratory Ptp were significantly associated with increased likelihood of elevated lung elastance, supporting the use of Ptp as a physiologic target to avoid overdistension during RMs (54). Additionally, patient-specific characteristics, markers of disease severity, and ventilatory parameters were identified as predictors of elevated Ptp during RMs, suggesting the potential for personalized optimization of recruitment strategies (54).
Another parameter for assessing overdistension is the stress index (SI), derived from the shape of the airway pressure–time waveform during volume-controlled ventilation. A concave upward shape (SI greater than 1.1) suggests overdistension, whereas the non-injurious SI range is considered to be 0.95–1.05 (10, 55, 56). However, SI is limited to volume-controlled ventilation, while a broader range of modes is commonly used in clinical practice. To overcome these limitations, Sun et al. proposed a novel overdistension index (OD), based on analysis of the pressure–volume loop. As peak inspiratory pressure increases, flattening of the end-inspiratory segment of the pressure–volume loop may indicate potential overdistension. The OD is calculated as the pressure difference between the end-inspiration of a “flattened” breath and the expected pressure of a “non-flattened” breath. In a cohort of 19 patients with ARDS, OD strongly correlated with SI, especially in those with moderate-to-severe ARDS. Calibration of OD to SI identified a potentially safe OD range of 0–0.8 cmH2O (57). Although these results are preliminary and not yet validated against direct physiological evidence of overdistension, they suggest that OD could help detect overdistension across a broader range of ventilation modes.
Biomarkers
One of the emerging frontiers in the assessment of lung overdistension during mechanical ventilation is the use of molecular biomarkers. Structural lung damage associated with VILI can trigger a local and systemic inflammatory response, termed “biotrauma,” mediated by mechano-transduction intracellular pathways, which may contribute to the development of multiorgan failure (58). Key biomarkers implicated in biotrauma include tumor necrosis factor-alpha (TNF-α), interleukins 6 and 8 (IL-6, IL-8), surfactant protein-D (SP-D), and Clara cell secretory protein-16 (CC-16). Notably, CC-16 is a lung-specific protein secreted by epithelial cells in the small airways and has been strongly associated with lung overdistension (59).
Several clinical studies have reported associations between plasma or bronchoalveolar lavage (BAL) biomarker levels and mechanical ventilation strategies involving higher versus lower PEEP and/or Vt (60). Recently, López-Martínez et al. conducted sequential pooled transcriptomic analyzes to identify micro-ribonucleic acids and genes involved in the cellular response to cyclic stretch (61). These molecular signatures were subsequently validated in multiple experimental models, including in vivo animal models of stretch-induced lung injury, ex vivo human lung preparations, BAL samples from patients exposed to mechanical ventilation, and serum samples from mechanically ventilated patients with COVID-19. The authors identified two distinct transcriptomic signatures, comprising six micro-ribonucleic acids and six genes, respectively, that were capable of specifically detecting lung stretch (61).
Although further physiological and clinical validation is necessary, these findings offer a promising foundation for personalized, biologically-guided mechanical ventilation strategies aimed at preventing lung overdistension.
Overdistension in the spontaneously breathing patient
Spontaneous breathing during mechanical ventilation has been associated with several advantages, including enhanced gas exchange and hemodynamics, reduced sedative requirements, and a decreased risk of diaphragmatic atrophy (62–64). However, growing evidence also highlights its potential to cause harm (65).
Patient self-inflicted lung injury (P-SILI) refers to lung damage resulting from excessive inspiratory efforts driven by elevated respiratory drive, particularly in patients with preexisting lung injury. Several mechanisms for P-SILI have been postulated, such as excessive transpulmonary pressure, pendelluft (gas shifts within the lung during inspiration, causing transient regional overdistension and localized injury), intra-tidal recruitment, local lung volutrauma, and negative pressure pulmonary edema (66).
Recognizing patients at risk for P-SILI is crucial, as unchecked respiratory effort can exacerbate lung injury. Various methods have been proposed over the years to assess this risk (66). Recent physiological studies in patients with COVID-19-related ARDS suggest that individuals receiving non-invasive ventilation who generate high inspiratory efforts, estimated by large negative deflections in esophageal pressure, and correspondingly elevated transpulmonary ΔP may face a higher risk of intubation (67, 68). Therefore, monitoring these physiological variables may be essential for the prevention and management of P-SILI. Nonetheless, additional clinical data are required to establish the utility of esophageal pressure monitoring during non-invasive ventilation.
Furthermore, strategies have been developed to enable the use of EIT during partial support ventilation by overcoming the challenges of PEEP titration in this setting, such as variable inspiratory effort, fluctuating compliance, and motion artifacts. The regional peak flow (RPF) method has recently been shown to be both feasible and comparable to the overdistension-collapse method (69, 70). RPF is calculated as the maximum first derivative of the inspiratory limb of the impedance signal. Relative changes in RPF, which are independent of a stable plateau pressure phase, are then used to estimate overdistension and collapse, similar to the overdistension-collapse approach (16), based on the assumption that regional peak airflow reflects regional pulmonary compliance (69). Additionally, EIT has been combined with dynamic Ptp measurements to apply the overdistension-collapse method during pressure support ventilation (PSV). In a study of 30 patients with ARDS on PSV, Mauri et al. found that titrating PEEP to the level minimizing the difference between the percentages of overdistension and collapse, as estimated via dynamic transpulmonary compliance, led to reduced respiratory drive and lower inspiratory effort, compared to PEEP titrated based on the lower PEEP-FiO2 table (71).
EIT has also been employed in the detection of pendelluft. In a retrospective observational study of 94 patients receiving PSV, pendelluft was detected in 41% of cases and was associated with a higher GI index, indicating more uneven ventilation distribution (72). Patients with pendelluft had fewer ventilator-free days at day 14 and longer ICU stays (72). In 108 difficult-to-wean ICU patients undergoing a T-piece spontaneous breathing trial (SBT), pendelluft was present in 70% and correlated with longer mechanical ventilation, fewer ventilator-free days, and significantly higher 28-day mortality (73). In another observational study of 20 patients undergoing sequential 2-cmH2O reductions in pressure support level during PSV, pendelluft volumes correlated positively with clinical markers of respiratory distress, including higher respiratory rate and P0.1 (74).
Finally, EIT has been recently employed to monitor the homogeneity of ventilation during SBTs. In a prospective observational study of 98 patients, Phoophiboon et al. observed that patients who were successfully weaned from mechanical ventilation (40 out of 98 patients) exhibited consistently smaller ventral-to-dorsal ventilation differences throughout the SBT, compared to those who failed the trial (75).
Conclusion
Mechanical ventilation, while lifesaving, can also cause lung injury, an idea recognized as early as the 18th century and now referred to as VILI. Modern understanding of VILI focuses on lung stress and strain, which are influenced by factors such as Vt, lung compliance, airway pressure, and inspiratory muscle pressure. Timely assessment of lung overdistension is critical for optimizing ventilatory support and several innovative techniques have been investigated in recent years for this purpose. While an expanding array of tools is enriching the armamentarium of the modern intensivist for detecting lung overdistension (Figure 1), most still await rigorous physiological and clinical validation before they can reliably inform real-time, bedside assessments of stress and strain.

Figure 1. An expanding array of tools is enriching the future intensivist’s armamentarium for bedside detection of non-physiologic lung stress and strain. The physician is performing pleural and lung ultrasound to measure maximal longitudinal pleural strain in real time, while titrating positive end-expiratory pressure (PEEP) to minimize dynamic lung strain with an electrical impedance tomography belt. The ventilator screen displays a single-breath 10-cmH2O PEEP reduction used to perform the recruitment-to-inflation ratio maneuver. The presence of overdistension during tidal ventilation is also assessed by evaluating respiratory mechanics after the application of an abdominal weight. An esophageal catheter is used for estimating patient’s inspiratory effort and transpulmonary driving pressure during partial assist ventilator support. This image is illustrative. Many of the described techniques still require rigorous physiological and clinical validation before adoption into routine bedside practice.
Author contributions
TP: Visualization, Formal analysis, Validation, Supervision, Methodology, Writing – review & editing, Writing – original draft, Investigation, Conceptualization. FZ: Investigation, Formal analysis, Writing – original draft, Visualization, Supervision, Methodology, Writing – review & editing, Conceptualization, Validation. AZ: Visualization, Investigation, Writing – original draft, Conceptualization, Validation. GL: Investigation, Conceptualization, Validation, Writing – original draft, Visualization. DR: Validation, Conceptualization, Writing – original draft, Investigation, Visualization. GP: Validation, Visualization, Writing – review & editing. EP: Writing – review & editing, Visualization, Validation. VF: Visualization, Validation, Writing – review & editing. GM: Validation, Visualization, Writing – review & editing. AC: Visualization, Validation, Writing – review & editing. NS: Supervision, Writing – review & editing, Visualization, Validation. AB: Writing – review & editing, Supervision, Validation, Visualization. PN: Validation, Supervision, Writing – review & editing, Visualization.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
TP, FZ, and NS received speaking fees from Getinge. AB received grants from Gilead. PN received grants/research equipment from Draeger, Intersurgical SPA, and Gilead and speaking fees from Getinge, Mindray, Intersurgical SPA, Gilead, GSK, and Draeger.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that Gen AI was used in the creation of this manuscript. Figure 1 was generated using GPT-5 (August 2025 ChatGPT release), a large language model developed by OpenAI (OpenAI, 2025) with the careful input and revision by the authors. The figure was checked to ensure it accurately reflects the content presented in the manuscript and it is free from plagiarism.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Slutsky, AS. History of mechanical ventilation. From Vesalius to ventilator-induced lung injury. Am J Respir Crit Care Med. (2015) 191:1106–15. doi: 10.1164/rccm.201503-0421PP
2. Webb, HH, and Tierney, DF. Experimental pulmonary edema due to intermittent positive pressure ventilation with high inflation pressures. Protection by positive end-expiratory pressure. Am Rev Respir Dis. (1974) 110:556–65. doi: 10.1164/arrd.1974.110.5.556
3. Dreyfuss, D, Soler, P, Basset, G, and Saumon, G. High inflation pressure pulmonary edema. Respective effects of high airway pressure, high tidal volume, and positive end-expiratory pressure. Am Rev Respir Dis. (1988) 137:1159–64. doi: 10.1164/ajrccm/137.5.1159
4. Chiumello, D, Carlesso, E, Cadringher, P, Caironi, P, Valenza, F, Polli, F, et al. Lung stress and strain during mechanical ventilation for acute respiratory distress syndrome. Am J Respir Crit Care Med. (2008) 178:346–55. doi: 10.1164/rccm.200710-1589OC
5. Gattinoni, L, Marini, JJ, Collino, F, Maiolo, G, Rapetti, F, Tonetti, T, et al. The future of mechanical ventilation: lessons from the present and the past. Crit Care. (2017) 21:183. doi: 10.1186/s13054-017-1750-x
6. Gattinoni, L, Marini, JJ, Pesenti, A, Quintel, M, Mancebo, J, and Brochard, L. The "baby lung" became an adult. Intensive Care Med. (2016) 42:663–73. doi: 10.1007/s00134-015-4200-8
7. Grasselli, G, Calfee, CS, Camporota, L, Poole, D, Amato, MBP, Antonelli, M, et al. ESICM guidelines on acute respiratory distress syndrome: definition, phenotyping and respiratory support strategies. Intensive Care Med. (2023) 49:727–59. doi: 10.1007/s00134-023-07050-7
8. Sahetya, SK, Goligher, EC, and Brower, RG. Fifty years of research in ARDS. Setting positive end-expiratory pressure in acute respiratory distress syndrome. Am J Respir Crit Care Med. (2017) 195:1429–38. doi: 10.1164/rccm.201610-2035CI
9. Amato, MB, Meade, MO, Slutsky, AS, Brochard, L, Costa, EL, Schoenfeld, DA, et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. (2015) 372:747–55. doi: 10.1056/NEJMsa1410639
10. Grasso, S, Terragni, P, Mascia, L, Fanelli, V, Quintel, M, Herrmann, P, et al. Airway pressure-time curve profile (stress index) detects tidal recruitment/hyperinflation in experimental acute lung injury. Crit Care Med. (2004) 32:1018–27. doi: 10.1097/01.ccm.0000120059.94009.ad
11. Fisher, JB, Mammel, MC, Coleman, JM, Bing, DR, and Boros, SJ. Identifying lung overdistention during mechanical ventilation by using volume-pressure loops. Pediatr Pulmonol. (1988) 5:10–4. doi: 10.1002/ppul.1950050104
12. Chiumello, D, Marino, A, Brioni, M, Menga, F, Cigada, I, Lazzerini, M, et al. Visual anatomical lung CT scan assessment of lung recruitability. Intensive Care Med. (2013) 39:66–73. doi: 10.1007/s00134-012-2707-9
13. Marini, JJ. Dissipation of energy during the respiratory cycle: conditional importance of ergotrauma to structural lung damage. Curr Opin Crit Care. (2018) 24:16–22. doi: 10.1097/MCC.0000000000000470
14. Sella, N, Pettenuzzo, T, Zarantonello, F, Andreatta, G, De Cassai, A, Schiavolin, C, et al. Electrical impedance tomography: a compass for the safe route to optimal PEEP. Respir Med. (2021) 187:106555. doi: 10.1016/j.rmed.2021.106555
15. Scaramuzzo, G, Pavlovsky, B, Adler, A, Baccinelli, W, Bodor, DL, Damiani, LF, et al. Electrical impedance tomography monitoring in adult ICU patients: state-of-the-art, recommendations for standardized acquisition, processing, and clinical use, and future directions. Crit Care. (2024) 28:377. doi: 10.1186/s13054-024-05173-x
16. Costa, EL, Borges, JB, Melo, A, Suarez-Sipmann, F, Toufen, C Jr, Bohm, SH, et al. Bedside estimation of recruitable alveolar collapse and hyperdistension by electrical impedance tomography. Intensive Care Med. (2009) 35:1132–7. doi: 10.1007/s00134-009-1447-y
17. Frerichs, I, Schädler, D, and Becher, T. Setting positive end-expiratory pressure by using electrical impedance tomography. Curr Opin Crit Care. (2024) 30:43–52. doi: 10.1097/MCC.0000000000001117
18. Iwata, H, Yoshida, T, Hoshino, T, Aiyama, Y, Maezawa, T, Hashimoto, H, et al. Electrical impedance tomography-based ventilation patterns in patients after major surgery. Am J Respir Crit Care Med. (2024) 209:1328–37. doi: 10.1164/rccm.202309-1658OC
19. Morais, CCA, Berra, L, Kassis, EB, Cornejo, RA, Campos, SL, Brandão, DC, et al. Electrical impedance tomography-based ventilation patterns for evaluating proper ventilator settings and to classify lung morphofunction. Am J Respir Crit Care Med. (2024) 209:1516–8. doi: 10.1164/rccm.202403-0573LE
20. Becher, T, Buchholz, V, Hassel, D, Meinel, T, Schädler, D, Frerichs, I, et al. Individualization of PEEP and tidal volume in ARDS patients with electrical impedance tomography: a pilot feasibility study. Ann Intensive Care. (2021) 11:89. doi: 10.1186/s13613-021-00877-7
21. Frerichs, I, Zhao, Z, and Becher, T. Simple electrical impedance tomography measures for the assessment of ventilation distribution. Am J Respir Crit Care Med. (2020) 201:386–8. doi: 10.1164/rccm.201908-1502LE
22. Yoshida, T, Piraino, T, Lima, CAS, Kavanagh, BP, Amato, MBP, and Brochard, L. Regional ventilation displayed by electrical impedance tomography as an incentive to decrease positive end-expiratory pressure. Am J Respir Crit Care Med. (2019) 200:933–7. doi: 10.1164/rccm.201904-0797LE
23. Ukere, A, März, A, Wodack, KH, Trepte, CJ, Haese, A, Waldmann, AD, et al. Perioperative assessment of regional ventilation during changing body positions and ventilation conditions by electrical impedance tomography. Br J Anaesth. (2016) 117:228–35. doi: 10.1093/bja/aew188
24. Spadaro, S, Mauri, T, Böhm, SH, Scaramuzzo, G, Turrini, C, Waldmann, AD, et al. Variation of poorly ventilated lung units (silent spaces) measured by electrical impedance tomography to dynamically assess recruitment. Crit Care. (2018) 22:26. doi: 10.1186/s13054-017-1931-7
25. Taenaka, H, Yoshida, T, Hashimoto, H, Firstiogusran, AMF, Ishigaki, S, Iwata, H, et al. Personalized ventilatory strategy based on lung recruitablity in COVID-19-associated acute respiratory distress syndrome: a prospective clinical study. Crit Care. (2023) 27:152. doi: 10.1186/s13054-023-04360-6
26. Zhao, Z, Möller, K, Steinmann, D, Frerichs, I, and Guttmann, J. Evaluation of an electrical impedance tomography-based global inhomogeneity index for pulmonary ventilation distribution. Intensive Care Med. (2009) 35:1900–6. doi: 10.1007/s00134-009-1589-y
27. Liu, X, Liu, X, Meng, J, Liu, D, Huang, Y, Sang, L, et al. Electrical impedance tomography for titration of positive end-expiratory pressure in acute respiratory distress syndrome patients with chronic obstructive pulmonary disease. Crit Care. (2022) 26:339. doi: 10.1186/s13054-022-04201-y
28. Zarantonello, F, Pettenuzzo, T, Pretto, C, Boscolo, A, Sella, N, and Navalesi, P. Setting positive end-expiratory pressure in primary lung graft dysfunction: a prospective physiologic study. J Cardiothorac Vasc Anesth. (2024) 38:1434–6. doi: 10.1053/j.jvca.2024.02.018
29. Gogniat, E, Madorno, M, Rodriguez, PO, Dianti, J, Otero, PE, Krukewitt, L, et al. Dynamic relative regional lung strain estimated by electrical impedance tomography in an experimental model of ARDS. Respir Care. (2022) 67:906–13. doi: 10.4187/respcare.09682
30. Scaramuzzo, G, Spadaro, S, Waldmann, AD, Böhm, SH, Ragazzi, R, Marangoni, E, et al. Heterogeneity of regional inflection points from pressure-volume curves assessed by electrical impedance tomography. Crit Care. (2019) 23:119. doi: 10.1186/s13054-019-2417-6
31. Grivans, C, and Stenqvist, O. Gas distribution by EIT during PEEP inflation: PEEP response and optimal PEEP with lowest trans-pulmonary driving pressure can be determined without esophageal pressure during a rapid PEEP trial in patients with acute respiratory failure. Physiol Meas. (2022) 43:114001. doi: 10.1088/1361-6579/ac8ccc
32. Songsangvorn, N, Xu, Y, Lu, C, Rotstein, O, Brochard, L, Slutsky, AS, et al. Electrical impedance tomography-guided positive end-expiratory pressure titration in ARDS: a systematic review and meta-analysis. Intensive Care Med. (2024) 50:617–31. doi: 10.1007/s00134-024-07362-2
33. Mojoli, F, Bouhemad, B, Mongodi, S, and Lichtenstein, D. Lung ultrasound for critically ill patients. Am J Respir Crit Care Med. (2019) 199:701–14. doi: 10.1164/rccm.201802-0236CI
34. Mongodi, S, Cortegiani, A, Alonso-Ojembarrena, A, Biasucci, DG, Bos, LDJ, Bouhemad, B, et al. ESICM-ESPNIC international expert consensus on quantitative lung ultrasound in intensive care. Intensive Care Med. (2025) 51:1022–49. doi: 10.1007/s00134-025-07932-y
35. Pesenti, A, Musch, G, Lichtenstein, D, Mojoli, F, Amato, MBP, Cinnella, G, et al. Imaging in acute respiratory distress syndrome. Intensive Care Med. (2016) 42:686–98. doi: 10.1007/s00134-016-4328-1
36. Tonelotto, B, Pereira, SM, Tucci, MR, Vaz, DF, Vieira, JE, Malbouisson, LM, et al. Intraoperative pulmonary hyperdistention estimated by transthoracic lung ultrasound: a pilot study. Anaesth Crit Care Pain Med. (2020) 39:825–31. doi: 10.1016/j.accpm.2020.09.009
37. Girard, M, Roy Cardinal, MH, Chassé, M, Garneau, S, Cavayas, YA, Cloutier, G, et al. Regional pleural strain measurements during mechanical ventilation using ultrasound elastography: a randomized, crossover, proof of concept physiologic study. Front Med (Lausanne). (2022) 9:935482. doi: 10.3389/fmed.2022.935482
38. Persona, P, Valeri, I, Zarantonello, F, Forin, E, Pivetta, E, Giacon, TA, et al. Lung ultrasound to detect overdistension in mechanically ventilated patients: a pilot study. Am J Respir Crit Care Med. (2025) 211:415–7. doi: 10.1164/rccm.202404-0861RL
39. Pacchiarini, G, Pettenuzzo, T, Zarantonello, F, Sella, N, Lumetti, G, Boscolo, A, et al. The "mechanical paradox" unveiled: a physiological study. Crit Care. (2025) 29:194. doi: 10.1186/s13054-025-05385-9
40. Selickman, J, Tawfik, P, Crooke, PS, Dries, DJ, Shelver, J, Gattinoni, L, et al. Paradoxical response to chest wall loading predicts a favorable mechanical response to reduction in tidal volume or PEEP. Crit Care. (2022) 26:201. doi: 10.1186/s13054-022-04073-2
41. Pearce, AK, McGuire, WC, Elliott, AR, Goligher, EC, Prisk, GK, Butler, JP, et al. Impact of supine versus semirecumbent body posture on the distribution of ventilation in acute respiratory distress syndrome. Crit Care Explor. (2023) 5:e1014. doi: 10.1097/CCE.0000000000001014
42. Marrazzo, F, Spina, S, Forlini, C, Guarnieri, M, Giudici, R, Bassi, G, et al. Effects of trunk inclination on respiratory mechanics in patients with COVID-19-associated acute respiratory distress syndrome: let's always report the angle! Am J Respir Crit Care Med. (2022) 205:582–4. doi: 10.1164/rccm.202110-2360LE
43. Marrazzo, F, Spina, S, Zadek, F, Forlini, C, Bassi, G, Giudici, R, et al. Ventilation distribution during changes in trunk inclination in patients with ARDS. Respir Care. (2024) 69:222–6. doi: 10.4187/respcare.11175
44. Bouchant, L, Godet, T, Arpajou, G, Aupetitgendre, L, Cayot, S, Guerin, R, et al. Physiological effects and safety of bed verticalization in patients with acute respiratory distress syndrome. Crit Care. (2024) 28:262. doi: 10.1186/s13054-024-05013-y
45. Chen, L, Del Sorbo, L, Grieco, DL, Junhasavasdikul, D, Rittayamai, N, Soliman, I, et al. Potential for lung recruitment estimated by the recruitment-to-inflation ratio in acute respiratory distress syndrome: a clinical trial. Am J Respir Crit Care Med. (2020) 201:178–87. doi: 10.1164/rccm.201902-0334OC
46. Grieco, DL, Pintaudi, G, Bongiovanni, F, Anzellotti, GM, Menga, LS, Cesarano, M, et al. Recruitment-to-inflation ratio assessed through sequential end-expiratory lung volume measurement in acute respiratory distress syndrome. Anesthesiology. (2023) 139:801–14. doi: 10.1097/ALN.0000000000004716
47. Covotta, M, Claroni, C, Torregiani, G, Menga, LS, Venti, E, Gazzè, G, et al. Recruitment-to-inflation ratio to assess response to PEEP during laparoscopic surgery: a physiologic study. J Clin Anesth. (2024) 98:111569. doi: 10.1016/j.jclinane.2024.111569
48. Pettenuzzo, T, Sella, N, Lorenzoni, G, Calore, A, Zarantonello, F, Andreatta, G, et al. The recruitment-to-inflation ratio is correlated with EIT-derived collapse and overdistention in COVID-19 ARDS. Am J Respir Crit Care Med. (2022) 206:1284–6. doi: 10.1164/rccm.202203-0555LE
49. Coppens, A, Aissi James, S, Roze, H, Juvin, C, Repusseau, B, Lebreton, G, et al. Optimum electrical impedance tomography-based PEEP and recruitment-to-inflation ratio in patients with severe ARDS on venovenous ECMO. Crit Care. (2025) 29:195. doi: 10.1186/s13054-025-05437-0
50. Rosà, T, Menga, LS, Mastropietro, C, Settanni, D, Russo, A, Frassanito, L, et al. Evaluation of the potential for lung recruitment with the recruitment-to-inflation ratio during general anesthesia. Anesthesiology. (2025). doi: 10.1097/ALN.0000000000005677 [ahead of print].
51. Del Sorbo, L, Tisminetzky, M, Chen, L, Brochard, L, Arellano, D, Brito, R, et al. Association of lung recruitment and change in recruitment-to-inflation ratio from supine to prone position in acute respiratory distress syndrome. Crit Care. (2023) 27:140. doi: 10.1186/s13054-023-04428-3
52. Fan, E, Checkley, W, Stewart, TE, Muscedere, J, Lesur, O, Granton, JT, et al. Complications from recruitment maneuvers in patients with acute lung injury: secondary analysis from the lung open ventilation study. Respir Care. (2012) 57:1842–9. doi: 10.4187/respcare.01684
53. Beitler, JR, Sarge, T, Banner-Goodspeed, VM, Gong, MN, Cook, D, Novack, V, et al. Effect of titrating positive end-expiratory pressure (PEEP) with an esophageal pressure-guided strategy vs an empirical high PEEP-FiO₂ strategy on death and days free from mechanical ventilation among patients with acute respiratory distress syndrome: a randomized clinical trial. JAMA. (2019) 321:846–57. doi: 10.1001/jama.2019.0555
54. Santarisi, A, Suleiman, A, Redaelli, S, von Wedel, D, Beitler, JR, Talmor, D, et al. Transpulmonary pressure as a predictor of successful lung recruitment: reanalysis of a multicenter international randomized clinical trial. Respir Care. (2024) 70:1–9. doi: 10.4187/respcare.11736
55. Grasso, S, Terragni, P, Birocco, A, Urbino, R, Del Sorbo, L, Filippini, C, et al. ECMO criteria for influenza a (H1N1)-associated ARDS: role of transpulmonary pressure. Intensive Care Med. (2012) 38:395–403. doi: 10.1007/s00134-012-2490-7
56. Terragni, PP, Filippini, C, Slutsky, AS, Birocco, A, Tenaglia, T, Grasso, S, et al. Accuracy of plateau pressure and stress index to identify injurious ventilation in patients with acute respiratory distress syndrome. Anesthesiology. (2013) 119:880–9. doi: 10.1097/ALN.0b013e3182a05bb8
57. Sun, Q, Chase, JG, Zhou, C, Tawhai, MH, Knopp, JL, Möller, K, et al. Non-invasive over-distension measurements: data driven vs model-based. J Clin Monit Comput. (2023) 37:389–98. doi: 10.1007/s10877-022-00900-7
58. Curley, GF, Laffey, JG, Zhang, H, and Slutsky, AS. Biotrauma and ventilator-induced lung injury: clinical implications. Chest. (2016) 150:1109–17. doi: 10.1016/j.chest.2016.07.019
59. Lesur, O, Hermans, C, Chalifour, JF, Picotte, J, Lévy, B, Bernard, A, et al. Mechanical ventilation-induced pneumoprotein CC-16 vascular transfer in rats: effect of KGF pretreatment. Am J Physiol Lung Cell Mol Physiol. (2003) 284:L410–9. doi: 10.1152/ajplung.00384.2001
60. Sutherasan, Y, Vargas, M, and Pelosi, P. Protective mechanical ventilation in the non-injured lung: review and meta-analysis. Crit Care. (2014) 18:211. doi: 10.1186/cc13778
61. López-Martínez, C, Martín-Vicente, P, Amado-Rodríguez, L, López-Alonso, I, Fernández-Rodríguez, M, González-López, A, et al. Prediction of lung overdistension during mechanical ventilation using micro-RNA and gene expression. Intensive Care Med Exp. (2025) 13:60. doi: 10.1186/s40635-025-00768-2
62. Putensen, C, Zech, S, Wrigge, H, Zinserling, J, Stüber, F, Von Spiegel, T, et al. Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury. Am J Respir Crit Care Med. (2001) 164:43–9. doi: 10.1164/ajrccm.164.1.2001078
63. Sassoon, CS, Zhu, E, and Caiozzo, VJ. Assist-control mechanical ventilation attenuates ventilator-induced diaphragmatic dysfunction. Am J Respir Crit Care Med. (2004) 170:626–32. doi: 10.1164/rccm.200401-042OC
64. Futier, E, Constantin, JM, Combaret, L, Mosoni, L, Roszyk, L, Sapin, V, et al. Pressure support ventilation attenuates ventilator-induced protein modifications in the diaphragm. Crit Care. (2008) 12:R116. doi: 10.1186/cc7010
65. Yoshida, T. The dark side of spontaneous breathing during noninvasive ventilation: from hypothesis to theory. Am J Respir Crit Care Med. (2020) 202:482–4. doi: 10.1164/rccm.202005-1612ED
66. Pettenuzzo, T, Sella, N, Zarantonello, F, De Cassai, A, Geraldini, F, Persona, P, et al. How to recognize patients at risk of self-inflicted lung injury. Expert Rev Respir Med. (2022) 16:963–71. doi: 10.1080/17476348.2022.2128335
67. Tonelli, R, Fantini, R, Tabbì, L, Castaniere, I, Pisani, L, Pellegrino, MR, et al. Early inspiratory effort assessment by esophageal manometry predicts noninvasive ventilation outcome in de novo respiratory failure: a pilot study. Am J Respir Crit Care Med. (2020) 202:558–67. doi: 10.1164/rccm.201912-2512OC
68. Grieco, DL, Menga, LS, Raggi, V, Bongiovanni, F, Anzellotti, GM, Tanzarella, ES, et al. Physiological comparison of high-flow nasal cannula and helmet noninvasive ventilation in acute hypoxemic respiratory failure. Am J Respir Crit Care Med. (2020) 201:303–12. doi: 10.1164/rccm.201904-0841OC
69. de Jongh, SAM, Heines, SJH, de Jongh, FHC, Segers, RPJ, van der Horst, ICC, van Bussel, BCT, et al. Regional peak flow as a novel approach to assess regional pulmonary mechanics by electrical impedance tomography: an observational validation study. Ann Transl Med. (2023) 11:253. doi: 10.21037/atm-22-3420
70. Heines, SJH, de Jongh, SAM, de Jongh, FHC, Segers, RPJ, Gilissen, KMH, van der Horst, ICC, et al. A novel positive end-expiratory pressure titration using electrical impedance tomography in spontaneously breathing acute respiratory distress syndrome patients on mechanical ventilation: an observational study from the MaastrICCht cohort. J Clin Monit Comput. (2025) 39:127–39. doi: 10.1007/s10877-024-01212-8
71. Mauri, T, Grieco, DL, Spinelli, E, Leali, M, Perez, J, Chiavieri, V, et al. Personalized positive end-expiratory pressure in spontaneously breathing patients with acute respiratory distress syndrome by simultaneous electrical impedance tomography and transpulmonary pressure monitoring: a randomized crossover trial. Intensive Care Med. (2024) 50:2125–37. doi: 10.1007/s00134-024-07695-y
72. Chi, Y, Zhao, Z, Frerichs, I, Long, Y, and He, H. Prevalence and prognosis of respiratory pendelluft phenomenon in mechanically ventilated ICU patients with acute respiratory failure: a retrospective cohort study. Ann Intensive Care. (2022) 12:22. doi: 10.1186/s13613-022-00995-w
73. Liu, W, Chi, Y, Zhao, Y, He, H, Long, Y, and Zhao, Z. Occurrence of pendelluft during ventilator weaning with T piece correlated with increased mortality in difficult-to-wean patients. J Intensive Care. (2024) 12:23. doi: 10.1186/s40560-024-00737-z
74. Coppadoro, A, Grassi, A, Giovannoni, C, Rabboni, F, Eronia, N, Bronco, A, et al. Occurrence of pendelluft under pressure support ventilation in patients who failed a spontaneous breathing trial: an observational study. Ann Intensive Care. (2020) 10:39. doi: 10.1186/s13613-020-00654-y
Keywords: ventilator-induced lung injury, overdistension, lung stress, lung strain, electrical impedance tomography, lung ultrasound, respiratory mechanics, pendelluft
Citation: Pettenuzzo T, Zarantonello F, Zambianchi A, Lumetti G, Ruggerini D, Pacchiarini G, Pistollato E, Fincati V, Mormando G, De Cassai A, Sella N, Boscolo A and Navalesi P (2025) Real-time stress and strain monitoring at the bedside: new frontiers in mechanical ventilation. Front. Med. 12:1692488. doi: 10.3389/fmed.2025.1692488
Edited by:
Michele Bertoni, University of Brescia, ItalyReviewed by:
Yalim Dikmen, Istanbul University Cerrahpasa, TürkiyeMichael Wilson, Imperial College London, United Kingdom
Copyright © 2025 Pettenuzzo, Zarantonello, Zambianchi, Lumetti, Ruggerini, Pacchiarini, Pistollato, Fincati, Mormando, De Cassai, Sella, Boscolo and Navalesi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nicolò Sella, bmljb2wmI3gwMDBGMjsuc2VsbGFAdW5pcGQuaXQ=
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share senior authorship
$These authors have contributed equally to this work and share last authorship