 Daniel Muñoz-Barba1,2
Daniel Muñoz-Barba1,2 Carmen García-Moronta1,2
Carmen García-Moronta1,2 Miguel Limeres-De la Rosa1,2
Miguel Limeres-De la Rosa1,2 Manuel Sánchez-Díaz1,2,3*
Manuel Sánchez-Díaz1,2,3* Salvador Arias-Santiago1,2,3,4
Salvador Arias-Santiago1,2,3,4- 1Dermatology Unit, Hospital Universitario Virgen de las Nieves, Granada, Spain
- 2Dermatology Department, School of Medicine, University of Granada, Granada, Spain
- 3Institute of Biosanitary Research IBS, Granada, Spain
- 4Trichology Clinic, Hospital Universitario Virgen de las Nieves, Granada, Spain
Introduction: Alopecia areata (AA) is a chronic immune-mediated disorder associated with substantial psychosocial burden. Generic dermatology instruments, such as the DLQI, may fail to capture AA-specific concerns, prompting the development of targeted questionnaires like the AA-QLI. However, existing tools show methodological limitations and inconsistent use. This study aimed to validate the Spanish Alopecia Areata–Life Impact Questionnaire (SAALIQ) by assessing its reliability, validity, and responsiveness, providing a robust instrument for evaluating the quality-of-life (QoL) impact of AA in Spanish-speaking patients.
Methods: A single-center cross-sectional study was conducted between June 2024 and June 2025. Adults with AA, recruited sequentially regardless of disease severity, duration, or prior treatments, were included. QoL was assessed using generic and disease-specific questionnaires, including the SAALIQ, developed in collaboration with the Alopecia Association of the Community of Madrid. Psychometric validation included assessment of internal consistency, test–retest reliability, and convergent validity. Receiver-operating characteristic (ROC) analyses were performed to determine cut-off points.
Results: A total of 85 patients with AA were included (72.94% women, 27.06% men) with a mean age of 37.55 years. The mean disease duration was 10.12 years, and the mean baseline SALT score was 36.52%. Cronbach’s α ranged from 0.73 to 0.80 across emotional, functional, and social domains. Intraclass correlation coefficient (ICC) for the total score was 0.947. Convergent validity was confirmed by moderate-to-strong correlations with DLQI, Hospital Anxiety and Depression Scale (HADS-A, HADS-D), and a strong correlation with the AA-QLI (r = 0.603; ρ = 0.714; p < 0.0001). Greater SAALIQ scores were observed in women, in patients with AA totalis (AAT) or multiple patch involvement, and in those with longer disease duration (p < 0.05). ROC analysis identified SAALIQ cut-offs of <20 for absent/mild, ≥20 for moderate, and >26 for severe QoL impairment.
Conclusion: The SAALIQ is a disease-specific and culturally adapted tool that enables accurate measurement of the QoL impact of AA in Spanish-speaking patients. Its psychometric performance, validated cut-off points, and ability to capture domains overlooked by generic measures make it an essential resource for patient-centered care, clinical trials, and international research. Further studies are warranted to confirm the generalizability of our findings.
Introduction
Alopecia areata (AA) is a chronic, immune-mediated disorder characterized by non-scarring hair loss that can progress to complete scalp or total body hair loss (1). Although AA is not physically disabling, its unpredictable course, visible nature, and potential for long-term persistence can exert a substantial psychosocial impact. Patients frequently experience emotional distress, anxiety, depressive symptoms, and reduced self-esteem, which may lead to social withdrawal and impaired quality of life (QoL) (2–4).
Assessment of the health-related quality of life (HRQoL) impact in AA has traditionally relied on generic dermatology instruments, such as the Dermatology Life Quality Index (DLQI) (5). While widely used, these measures may not adequately capture the disease-specific domains relevant to AA, including the psychological consequences of unpredictable relapses, concerns about public perception, and the functional impact of hair loss in daily activities. To address this gap, several disease-specific tools have been developed (6), including the Alopecia Areata Quality of Life Index (AA-QLI) (7).
Although these instruments have demonstrated acceptable psychometric performance, several methodological limitations remain, particularly the lack of patient participation in their development. Furthermore, their use has not been consistent across AA studies, which raises concerns regarding reproducibility. This inconsistency may be partly due to their considerable length or interpretative complexity, which often hinders both completion by patients and integration into routine clinical practice.
The objective of the present study was to validate the Spanish Alopecia Areata–Life Impact Questionnaire (SAALIQ) Questionnaire for use in Spanish-speaking patients with AA. The validation process evaluated internal consistency, test–retest reliability, construct validity, and responsiveness to clinical change, with comparisons to established measures such as the DLQI and AA-QLI. A robust, validated instrument is expected to provide clinicians and researchers with a reliable tool for assessing the specific QoL impact of AA in Spanish-speaking populations.
Methods
Study design
A review of existing AA-specific QoL measures was conducted (8). This was followed by semi-structured interviews with patient focus groups, members of the Community of Madrid Alopecia Association, and dermatologists and psychologists with expertise in the management of AA, in order to identify relevant thematic domains. Based on these findings, a preliminary version of the questionnaire was drafted with the objective of generating clear, relevant, and easily understood items. The previous expert panel subsequently reviewed each item for relevance, clarity, and representativeness to ensure content validity and conceptual coverage. The questionnaire was initially administered to a sample of 20 patients who were not included in the study. Based on their feedback, all 10 items were retained, although some questions were reformulated to enhance comprehension and minimize the risk of misinterpretation. After that, a single-center cross-sectional study was conducted including patients with AA attending the Dermatology Department in a third-level center between June 2024 and June 2025. Sequential sampling was applied. After providing written informed consent, patients were invited to share their clinical information and complete a series of questionnaires designed to assess the impact of AA on QoL.
Inclusion criteria
The inclusion criteria were: (a) patients with a clinical diagnosis of AA, regardless of disease severity, duration and previous or current treatments; (b) being diagnosed with AA for almost 6 months; (c) age 18 years or older; (d) informed consent to be included in the study; (e) understanding of Spanish language so as to make it possible to complete the questionnaires.
Exclusion criteria
The exclusion criteria were: (a) patient’s refusal to participate in the study; (b) patients who had any other major disease that may have impacted their mood or QoL.
Ethics
The current study was approved by the Research Ethics Committee of Granada and was performed in accordance with the principles of the Declaration of Helsinki.
Variables
Main Variables: The study focused on variables related to QoL and mood disorders. Data were collected using a set of questionnaires, classified into two categories: instruments specifically designed for patients with AA, and non-disease-specific instruments:
i. Spanish Alopecia Areata–Life Impact Questionnaire (SAALIQ): It includes 10 questions referring to the 8 weeks prior to the medical consultation. Items 1 to 4 were related to emotional domain; items 5 to 7 were questions about functional domain; and items 8–10 questions were related to social domain. A Likert-type response format was employed, with a 4-point scale where 1 = “No,” 2 = “Yes, a little,” 3 = “Yes, quite a lot,” and 4 = “Yes, very much.” The total score ranges from 10 to 40, with higher scores indicating a greater negative impact (40 = worst QoL) and lower scores reflecting less impairment (10 = best QoL). The questionnaire was refined following interviews with 15 patients. Based on their initial feedback, several items were reworded to enhance clarity and ensure comprehension. The final version of the questionnaire was then administered to all study participants (details can be seen in Supplementary material).
ii. Alopecia Areata Quality of Life Index (AA-QLI): It is a disease-specific instrument designed to assess the QoL in patients with AA. It measures the psychosocial and functional impact of the condition across domains such as self-perception, emotional well-being, and daily activities. The questionnaire comprises 21 items, each scored on a Likert-type scale, with higher scores reflecting greater impairment. Domain and total scores are calculated by summing item responses (7).
iii. Dermatology Life Quality Index (DLQI): This instrument assesses overall dermatological QoL in individuals aged 16 years and older. It contains 10 items, each scored on a 4-point Likert scale from 0 (no impact) to 3 (maximum impact). Responses are based on the patient’s experiences during the previous week (5, 9).
iv. World Health Organization-Five Well-Being Index (WHO-5): This brief questionnaire evaluates mental well-being over the preceding 2 weeks. It comprises five items, each scored from 0 to 5 on a Likert scale, with higher values reflecting better well-being. Item scores are summed, multiplied by four, and expressed on a scale from 0 to 100. Scores below 50 suggest reduced mental well-being (10).
v. Hospital Anxiety and Depression Scale (HADS): This validated tool consists of 14 items, each rated on a Likert scale. It includes two subscales: odd-numbered items measure anxiety and even-numbered items assess depression. Scores of 8 or higher on either subscale indicate probable anxiety or depression, respectively (11, 12).
Secondary Variables: Sociodemographic variables were collected through a multiple-choice section included at the beginning of the self-administered patient questionnaires, while clinical variables were obtained from the electronic medical records completed during the consultation. The severity of was assessed following Severity of Alopecia Tool (SALT) (13).
Statistical analysis
The psychometric evaluation of the SAALIQ was performed in relation to the DLQI, HADS, and AA-QLI. Reliability was assessed through internal consistency, calculated using Cronbach’s α (considered acceptable when >0.7), and reproducibility, evaluated using the intraclass correlation coefficient (ICC; acceptable when >0.7). Test–retest reliability was determined by calculating the ICC for the total score. Convergent validity, defined as the degree to which measures of the same construct are related, was examined using Pearson’s correlation coefficient to assess associations between SAALIQ raw scores and those of the DLQI, HADS, and AA-QLI. Cut-off values for categorizing QoL impairment were established through receiver operating characteristic (ROC) curve analysis, using DLQI categories as references.
Continuous variables are reported as mean ± standard deviation (SD) and categorical variables as relative (absolute) frequencies. Normality of continuous data was tested with the Kolmogorov–Smirnov test. Mean differences in quantitative variables were assessed using Student’s t-test, and associations between qualitative variables were examined using the χ2 test. Statistical significance was set at p < 0.05 (two-tailed). Data analysis was performed using SPSS Statistics, version 24.0 (SPSS Inc., Chicago, IL, United States).
For sample size estimation, a minimum of four participants per variable was considered necessary for questionnaire validation (14). Given that the SAALIQ comprises 10 items, the target sample size was at least 40 participants.
Results
Sociodemographic and clinical characteristics of the sample
A total of 85 patients with AA were included in the study. The mean age was 37.55 years (SD 14.58), with a predominance of females (72.94%, n = 62) over males (27.06%, n = 23). Tobacco use was reported by 31.76% of patients. Most participants had completed higher education (62.35%), were employed (61.15%), and were either single (45.88%) or married (38.83%; details can be seen in Table 1).
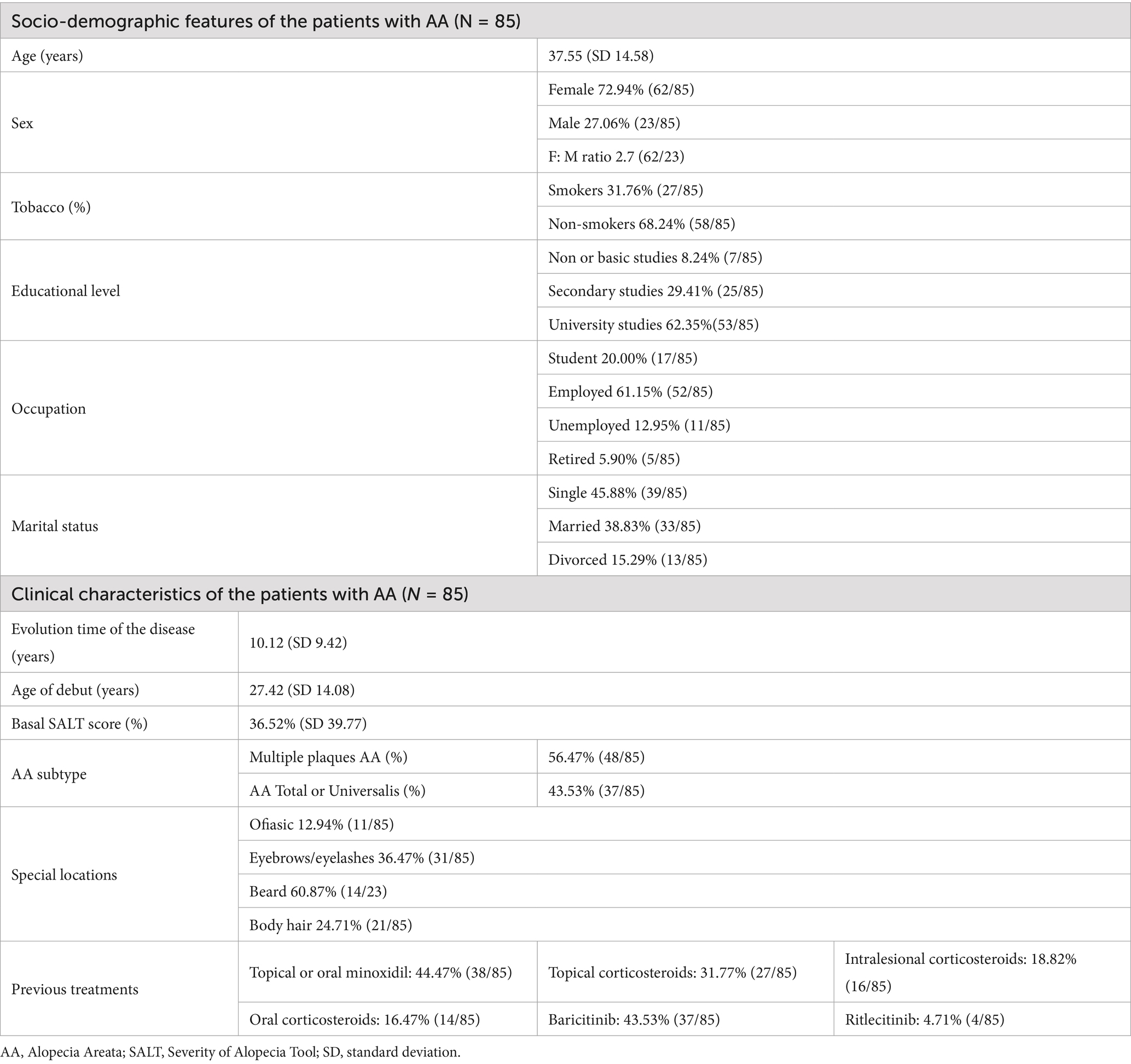
Table 1. Socio-demographic and clinical features of patients with AA of the sample.
The mean disease duration was 10.12 years (SD 9.42), with a mean age of onset of 27.42 years (SD 14.08). The mean baseline SALT score was 36.52% (SD 39.77). Multiple patch AA was present in 56.47% (n = 48) of patients, while 43.53% (n = 37) had total or universal AA (AAT or AAU). Special site involvement included ophiasis pattern (12.94%), eyebrows/eyelashes (36.47%), beard (60.87% of males), and body hair (24.71%). Regarding current treatments, 44.47% (n = 38) were receiving topical or oral minoxidil, 31.77% (n = 27) topical corticosteroids, 18.82% (n = 16) intralesional corticosteroids, and 16.47% (n = 14) oral corticosteroids. Systemic therapies included methotrexate in 2.23% (n = 2), baricitinib in 43.53% (n = 37), and ritlecitinib in 4.71% (n = 4; details can be seen Table 1).
Impact of AA on QoL based on questionnaire scores
In the study population, the mean DLQI score was 5.49 ± 6.36, with 32.5% of patients reporting no impact on QoL, 31.25% mild impact, and 36.25% moderate-to-extreme impact. The mean HADS-A score was 9.16 ± 5.24, with 60% of participants presenting anxiety symptoms. The mean HADS-D score was 5.19 ± 4.33, with depressive symptoms identified in 28.75% of cases. The WHO-5 Well-Being Index mean score was 13.54 ± 6.08, with 42.5% of patients exhibiting low well-being. The mean SAALIQ score was 21.59 ± 6.78, with 61.25% of participants showing moderate-to-severe disease-specific quality-of-life impairment. When analyzing the SAALIQ by domains, the highest mean raw score corresponded to the emotional domain (10.64 ± 3.32), followed by the functional (7.11 ± 2.70) and social domains (5.21 ± 2.47). The mean original AA-QLI score was 49.73 ± 16.52. Scores were also standardized to a 0–100 scale to enable comparability in subsequent analyses (details can be seen in Table 2).
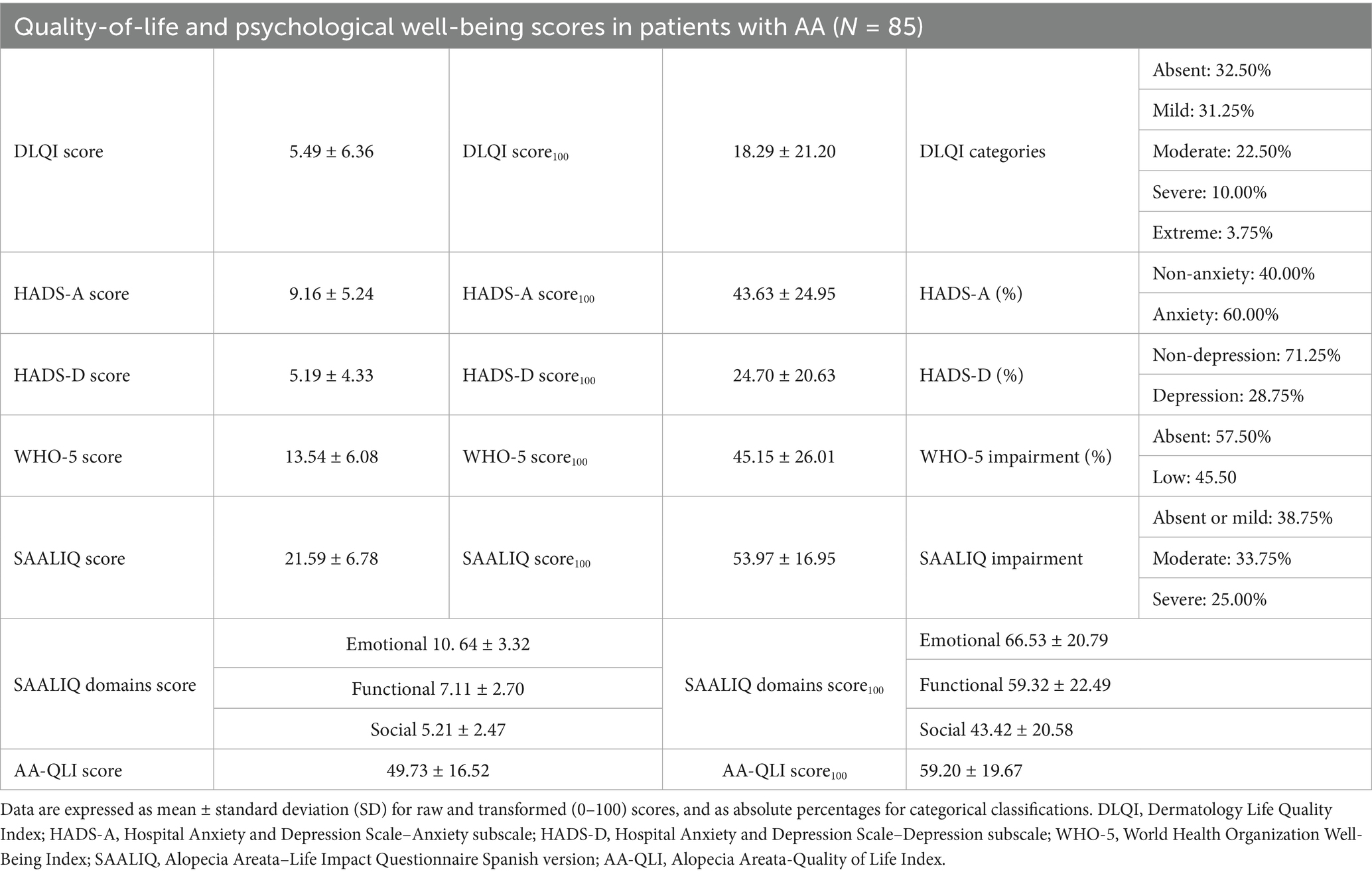
Table 2. Descriptive statistics for quality-of-life and psychological well-being measures in the study population.
Psychometric validation of the SAALIQ
Reliability was evaluated through internal consistency and temporal stability. Internal consistency, assessed using Cronbach’s α for each of the three domains, yielded values of 0.7785 for the emotional domain, 0.7294 for the functional domain, and 0.8023 for the social domain. The most internally consistent items within each domain were items 1, 6, and 9, respectively. Temporal stability was examined in a subsample of 25 patients with AA using ICC between test and retest administrations, with an interval of 30 days. The ICC for the total score was 0.9475, indicating excellent reproducibility, with no significant changes observed that could be attributed to ongoing treatment during this period (details can be seen in Table 3).
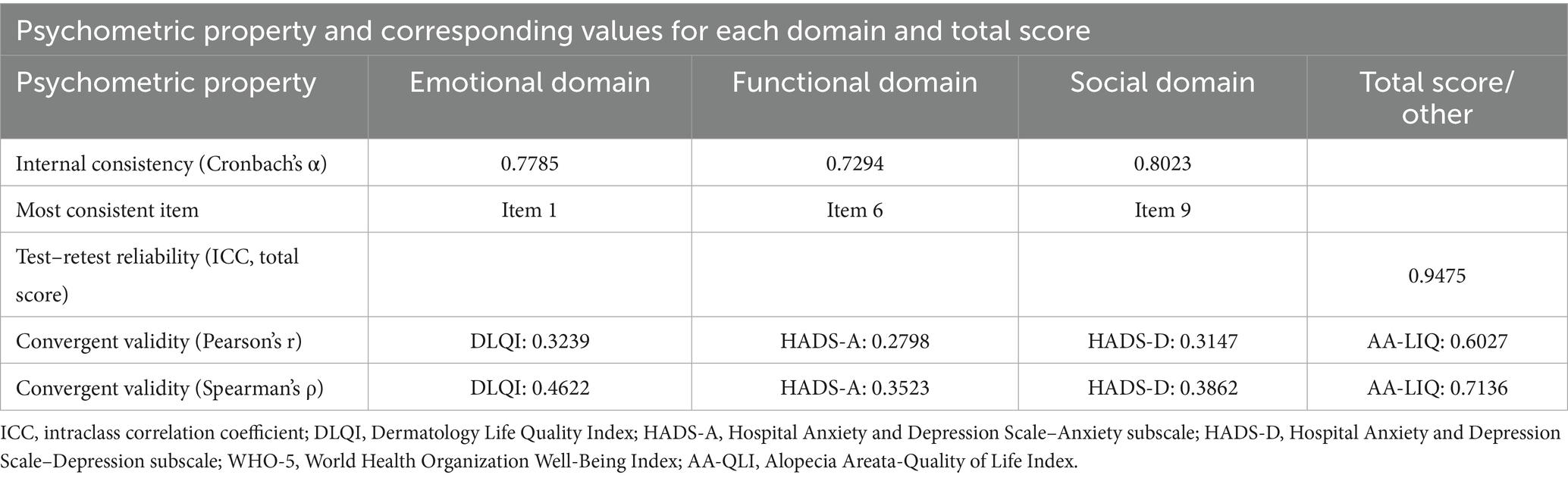
Table 3. Summary of the psychometric properties of the SAALIQ.
Validity was assessed through convergent and criterion-related approaches. Convergent validity was determined by comparing SAALIQ scores with those from other instruments assessing the impact of AA, standardized to a 0–100 scale. In parametric analyses, the SAALIQ showed moderate positive correlations with the DLQI (r = 0.3239), the HADS-A anxiety subscale (r = 0.2798), and the HADS-D depression subscale (r = 0.3147), and a strong correlation with the AA-LIQ (r = 0.6027). Non-parametric Spearman analyses confirmed these associations, with significant correlations observed for the DLQI (ρ = 0.4622), HADS-A (ρ = 0.3523), HADS-D (ρ = 0.3862), and AA-LIQ (ρ = 0.7136; all p values < 0.0001; details can be seen in Table 3).
Criterion validity was explored by assessing associations between SAALIQ scores and sociodemographic or clinical variables. Univariate analysis showed significantly higher mean scores in females than in males (p = 0.02) and in patients with multiple-type and AAT compared with single-type AA (23.07 ± 0.69 vs. 18.19 ± 1.15). Longer disease duration was also positively associated with higher scores (coefficient = 0.13 ± 0.06; p = 0.04). No significant associations were found with age, age at onset, baseline SALT score, overall disease severity, or special site involvement (all p > 0.05; details can be seen in Table 4).
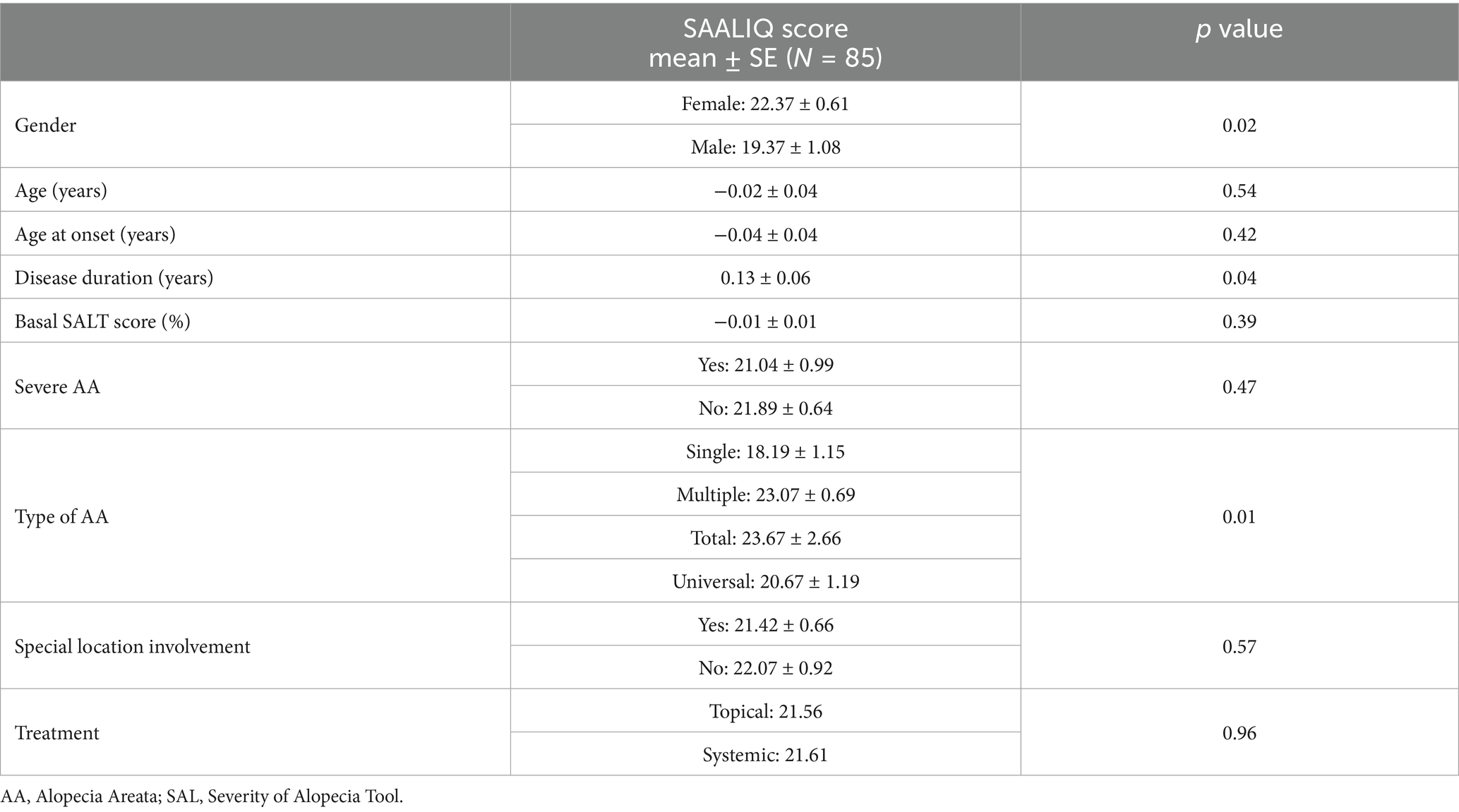
Table 4. Univariate analysis to explore association between sociodemographic and clinical characteristics and SAALIQ scores (N = 85).
Determination of SAALIQ cut-off points for categorizing QoL impairment
Cut-off point was delimited by comparing the values for the SAALIQ and DLQI. The DLQI was used because it yielded the acceptable correlation values. The ROC curve analysis showed that values < 20 in the SAALIQ corresponded to patients with absent or mild QoL impairment measured by DLQI, with a sensitivity of 66% and a specificity of 78.57% (AUC = 0.746, p < 0.001). The ROC curve analysis showed that values ≥ 20 in the SAALIQ corresponded to patients with moderate QoL impairment measured by DLQI, with a sensitivity of 83.33% and a specificity of 46.67% (AUC = 0.640, p < 0.001). The ROC curve analysis showed that values > 26 in the SAALIQ corresponded to patients with severe QoL impairment measured by DLQI, with a sensitivity of 70% and a specificity of 80.88% (AUC = 0.785, p < 0.001; details can be seen in Figures 1–3).
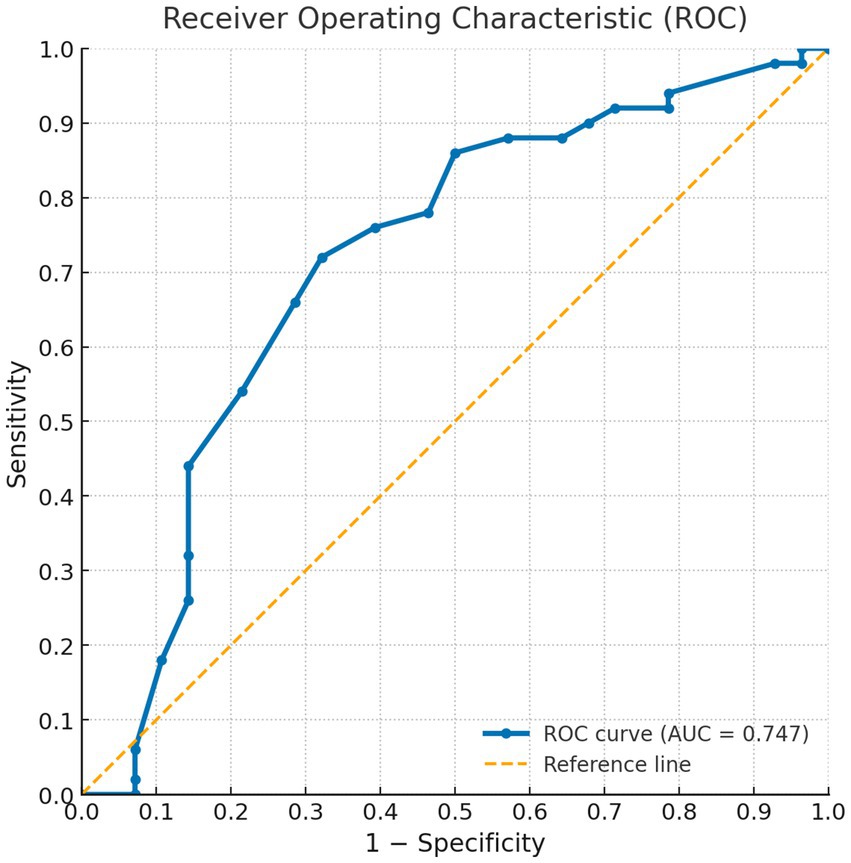
Figure 1. ROC curve for the SAALIQ questionnaire in discriminating patients with absent or mild QoL impairment (SAALIQ < 20), using the dichotomised DLQI as the reference standard. The area under the curve (AUC) was 0.747.
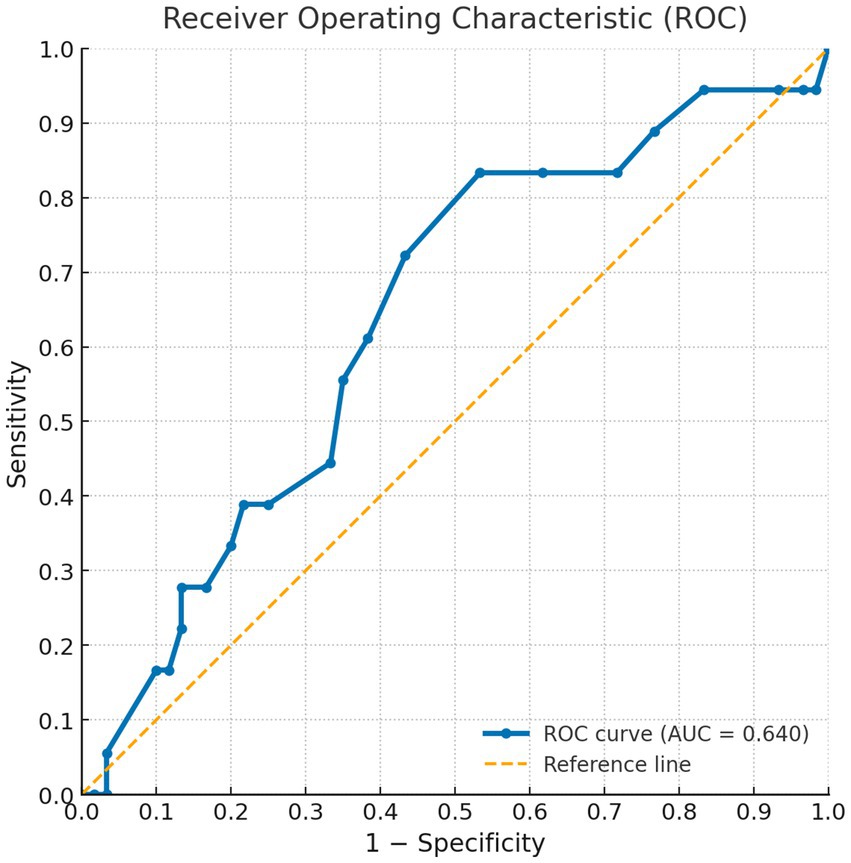
Figure 2. ROC curve for the SAALIQ questionnaire in discriminating patients with moderate QoL impairment (SAALIQ ≥ 20), using the dichotomised DLQI as the reference standard. The area under the curve (AUC) was 0.640.
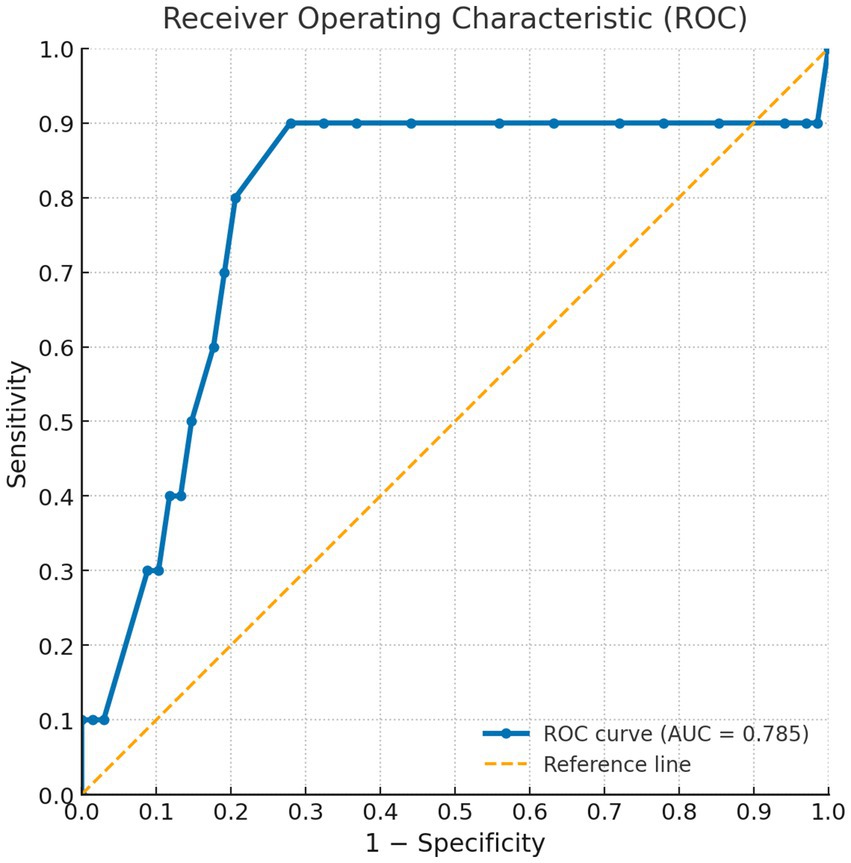
Figure 3. ROC curve for the SAALIQ questionnaire in discriminating patients with severe QoL impairment (SAALIQ > 26), using the dichotomised DLQI as the reference standard. The area under the curve (AUC) was 0.785.
Discussion
The results of this study confirm that AA has a significant impact on patients’ QoL, with over one-third of the sample experiencing moderate-to-extreme impairment according to the DLQI and more than 60% presenting moderate-to-severe disease-specific impairment as measured by the SAALIQ. This is likely attributable to the greater ability of the SAALIQ in detecting QoL impairment directly related to AA. Furthermore, these findings are consistent with previous literature reporting a substantial psychosocial burden in AA (15–17), often comparable to that observed in chronic inflammatory dermatoses such as psoriasis (18) or atopic dermatitis (19).
Compared with generic dermatology instruments such as the DLQI, the SAALIQ also demonstrated greater specificity in capturing domains particularly relevant to AA, including the functional limitations of hair loss, social avoidance due to visible alopecia, and emotional distress related to disease unpredictability. Such disease-specific sensitivity is essential for accurately detecting changes in patient-reported outcomes, particularly in clinical trials or interventions targeting psychosocial health, and for avoiding the limitations inherent to non-specific measures.
Female patients reported significantly higher SAALIQ scores compared with males, consistent with prior literature suggesting that the psychosocial consequences of hair loss may be more pronounced in women due to societal and cultural perceptions of appearance (20–22). Similarly, individuals with more extensive clinical phenotypes—such as multiple-type AA and AAT—had markedly higher scores than those with single-plaque disease. However, no correlation was observed between SAALIQ scores and baseline SALT values (p > 0.10). This aligns with heterogeneous findings in the literature, where factors other than SALT, such as anxiety and depression, often emerge as stronger determinants of QoL than the extent of AA, underscoring the inconsistent relationship between objective severity and patient-reported impairment (23). Moreover, longer disease duration was positively associated with higher SAALIQ scores, indicating a cumulative psychosocial impact over time (24) as it occurs in other dermatosis (25, 26). We believe that this lifelong accumulated impact may play a more decisive role in determining the overall disease burden than the mere extent of AA.
The availability of a validated Spanish-language instrument such as the SAALIQ represents a significant advance for both clinical practice and research. Notable strengths include its development through close collaboration between AA specialists and patients, ensuring that it addresses the most relevant concerns and domains affected by the disease, thereby enhancing external validity. Furthermore, the inclusion of patients with mild disease and those undergoing a wide range of treatments increases the representativeness of the sample. In routine clinical practice, the SAALIQ can help dermatologists identify patients in need of psychological support and monitor changes over time, while in research settings it facilitates the collection of relevant and comparable data regarding QoL impairment. Moreover, it showed an adequate correlation with the previously validated AA-QLI (7), supporting its construct validity. Compared with the latter, the SAALIQ offers several advantages. Its shorter format, with only 10 items versus the 21 of the AA-QLI, enables faster completion and reduces respondent fatigue, as it can be completed in approximately half the time. In addition, its straightforward structure facilitates clearer interpretation by clinicians. Most importantly, the SAALIQ provides validated cut-off points to categorize the degree of QoL impairment, thereby offering a practical framework for therapeutic decision-making and ensuring comparability across studies. Finally, SAALIQ extends the recall period to the 8 weeks prior to the visit, encouraging deeper reflection on the long-term impact of the disease without incurring recall bias. Moreover, it has to be taken into account that other disease-specific questionnaires have been developed for other specific alopecias, such as scarring alopecias (27).
This study has certain limitations. The sample size, although adequate for psychometric validation, limits the ability to perform subgroup analyses. The single-center design may restrict the generalizability of the findings, and potential selection bias cannot be excluded, as participants were recruited from a tertiary dermatology clinic. Furthermore, the cross-sectional design precludes assessment of the instrument’s responsiveness to clinical change over time. Moreover, this questionnaire has been validated in a specific area of Spain, not in other Spanish-talking areas such as Latin America.
Future research should focus on longitudinal studies to confirm the sensitivity of the SAALIQ to changes in disease activity and treatment response. Its application in clinical trials could provide more accurate estimates of patient-reported outcomes and help define clinically meaningful changes in QoL scores. Additionally, cross-cultural adaptation and validation in other languages would allow for broader international comparability and facilitate multinational research collaborations.
Conclusion
The SAALIQ is a disease-specific and culturally adapted tool that enables accurate measurement of the QoL impact of AA in Spanish-speaking patients. Its strong psychometric performance, validated cut-off points, and ability to capture domains overlooked by generic measures make it an essential resource for patient-centered care, clinical trials, and international research. Further studies are warranted to confirm the generalizability of our findings.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of Hospital Universitario Virgen de las Nieves. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DM-B: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Software, Writing – original draft, Writing – review & editing. CG-M: Data curation, Formal analysis, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. ML: Formal analysis, Investigation, Project administration, Validation, Writing – original draft, Writing – review & editing. MS-D: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SA-S: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors wish to express their deepest gratitude to all the patients and specialists who participated in this study. Their willingness to share personal and sensitive experiences has been fundamental to advancing knowledge in this important and often neglected area of alopecia areata. This research would not have been possible without their valuable collaboration and trust. This article will be part of the Doctoral Tesis of Daniel Muñoz Barba.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1706110/full#supplementary-material
Abbreviations
AA, Alopecia Areata; AA-QLI, Alopecia Areata–Quality of Life Index; AAU, Alopecia Areata Universalis; AAT, Alopecia Areata Totalis; AUC, Area Under the Curve; DLQI, Dermatology Life Quality Index; HADS, Hospital Anxiety and Depression Scale; HADS-A, Hospital Anxiety and Depression Scale – Anxiety subscale; HADS-D, Hospital Anxiety and Depression Scale – Depression subscale; HRQoL, Health-Related Quality of Life; ICC, Intraclass Correlation Coefficient; QoL, Quality of Life; ROC, Receiver Operating Characteristic; SAALIQ, Spanish Alopecia Areata–Life Impact Questionnaire; SALT, Severity of Alopecia Tool; SD, Standard Deviation; WHO-5, World Health Organization–Five Well-Being Index.
References
1. Sibbald, C. Alopecia Areata: an updated review for 2023. J Cutan Med Surg. (2023) 27:241–59. doi: 10.1177/12034754231168839
2. Lauron, S, Plasse, C, Vaysset, M, Pereira, B, D’Incan, M, Rondepierre, F, et al. Prevalence and odds of depressive and anxiety disorders and symptoms in children and adults with alopecia Areata: a systematic review and Meta-analysis. JAMA Dermatol. (2023) 159:281–8. doi: 10.1001/jamadermatol.2022.6085
3. Aldhouse, NVJ, Kitchen, H, Knight, S, Macey, J, Nunes, FP, Dutronc, Y, et al. «“you lose your hair, what’s the big deal?” I was so embarrassed, I was so self-conscious, I was so depressed:» a qualitative interview study to understand the psychosocial burden of alopecia areata. J Patient Rep Outcomes. (2020) 4:76. doi: 10.1186/s41687-020-00240-7
4. Sánchez-Díaz, M, Montero-Vílchez, T, Cuenca-Barrales, C, Molina-Leyva, A, and Arias-Santiago, S. Prevalence and implications of type D personality in patients with alopecia areata: a marker of quality-of-life impairment and mood status disturbances, a comparative study. J Eur Acad Dermatol Venereol. (2023) 37:1064–70. doi: 10.1111/jdv.18733
5. Finlay, AY, and Khan, GK. Dermatology life quality index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. (1994) 19:210–6.
6. Renert-Yuval, Y, Correa da Rosa, J, Garcet, S, Pavel, AB, Bares, J, Chima, M, et al. Analysis of alopecia areata surveys suggests a threshold for improved patient-reported outcomes. Br J Dermatol. (2022) 187:539–47. doi: 10.1111/bjd.21696
7. Fabbrocini, G, Panariello, L, De Vita, V, Vincenzi, C, Lauro, C, Nappo, D, et al. Quality of life in alopecia areata: a disease-specific questionnaire. J Eur Acad Dermatol Venereol. (2013) 27:e276–81. doi: 10.1111/j.1468-3083.2012.04629.x
8. Chernyshov, PV, Tomas-Aragones, L, Finlay, AY, Manolache, L, Marron, SE, Sampogna, F, et al. Quality of life measurement in alopecia areata. Position statement of the European academy of dermatology and venereology task force on quality of life and patient oriented outcomes. J Eur Acad Dermatol Venereol. (2021) 35:1614–21. doi: 10.1111/jdv.17370
9. de Tiedra, AG, Mercadal, J, Badía, X, Mascaró, JM, Herdman, M, and Lozano, R. Adaptación transcultural al español del cuestionario Dermatology Life Quality Index (DLQI): El Índice de Calidad de Vida en Dermatología. Actas Dermosifiliogr. (1998) 89:692–700.
10. Carrozzino, D, Christensen, KS, Patierno, C, Woźniewicz, A, Møller, SB, Arendt, IMTP, et al. Cross-cultural validity of the WHO-5 well-being index and Euthymia scale: a clinimetric analysis. J Affect Disord. (2022) 311:276–83. doi: 10.1016/j.jad.2022.05.111
11. Zigmond, AS, and Snaith, RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70.
12. Vilela-Estrada, AL, Villarreal-Zegarra, D, Copez-Lonzoy, A, Esenarro-Valencia, L, Sánchez-Ramírez, JC, Lamas-Delgado, F, et al. Psychometric properties of the Spanish version of the hospital anxiety and depression scale in cancer patients. Front Psychol. (2024) 15:1497946. doi: 10.3389/fpsyg.2024.1497946
13. Olsen, EA, and Canfield, D. SALT II: a new take on the severity of alopecia tool (SALT) for determining percentage scalp hair loss. J Am Acad Dermatol. (2016) 75:1268–70. doi: 10.1016/j.jaad.2016.08.042
14. Terwee, CB, Bot, SDM, de Boer, MR, van der Windt, DAWM, Knol, DL, Dekker, J, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. (2007) 60:34–42. doi: 10.1016/j.jclinepi.2006.03.012
15. Alhanshali, L, Buontempo, MG, Lo Sicco, KI, and Shapiro, J. Alopecia Areata: burden of disease, approach to treatment, and current unmet needs. CCID. (2023) 16:803–20. doi: 10.2147/CCID.S376096
16. Macbeth, AE, Holmes, S, Harries, M, Chiu, WS, Tziotzios, C, de Lusignan, S, et al. The associated burden of mental health conditions in alopecia areata: a population-based study in UK primary care. Br J Dermatol. (2022) 187:73–81. doi: 10.1111/bjd.21055
17. Mesinkovska, N, King, B, Mirmirani, P, Ko, J, and Cassella, J. Burden of illness in alopecia Areata: a cross-sectional online survey study. J Investig Dermatol Symp Proc. (2020) 20:S62–8. doi: 10.1016/j.jisp.2020.05.007
18. de Arruda, LH, and De Moraes, AP. The impact of psoriasis on quality of life. Br J Dermatol. (2001) 144:33–6. doi: 10.1046/j.1365-2133.2001.00034.x
19. Talamonti, M, Galluzzo, M, Silvaggio, D, Lombardo, P, Tartaglia, C, and Bianchi, L. Quality of life and psychological impact in patients with atopic dermatitis. J Clin Med. (2021) 10:1298. doi: 10.3390/jcm10061298
20. Muñoz-Barba, D, Díaz-Calvillo, P, De Francisco, SH, Martínez-Lopez, A, Sánchez-Díaz, M, and Arias-Santiago, S. Comparative study on sexual dysfunction in alopecia areata: prevalence and associated factors. J Deutsche Derma Gesell. (2024) 22:1611–8. doi: 10.1111/ddg.15527
21. Toussi, A, Barton, VR, Le, ST, Agbai, ON, and Kiuru, M. Psychosocial and psychiatric comorbidities and health-related quality of life in alopecia areata: a systematic review. J Am Acad Dermatol. (2021) 85:162–75. doi: 10.1016/j.jaad.2020.06.047
22. Abedini, R, Hallaji, Z, Lajevardi, V, Nasimi, M, Karimi Khaledi, M, and Tohidinik, HR. Quality of life in mild and severe alopecia areata patients. Int J Womens Dermatol. (2018) 4:91–4. doi: 10.1016/j.ijwd.2017.07.001
23. Rencz, F, Gulácsi, L, Péntek, M, Wikonkál, N, Baji, P, and Brodszky, V. Alopecia areata and health-related quality of life: a systematic review and meta-analysis. Br J Dermatol. (2016) 175:561–71. doi: 10.1111/bjd.14497
24. Muñoz-Barba, D, Soto-Moreno, A, Haselgruber-de Francisco, S, Sánchez-Díaz, M, and Arias-Santiago, S. Impact of alopecia Areata on major life-changing decisions: prevalence and associated factors. Acta Derm Venereol. (2025) 105:adv43039. doi: 10.2340/actadv.v105.43039
25. Castellano-Lopezosa, L, Ureña Paniego, C, Haselgruber, S, Blasco-Morente, G, and Arias-Santiago, S. Impact of vitiligo on major life-changing decisions and perceived stigmatization: a cross-sectional study. Acta Derm Venereol. (2025) 105:adv44198. doi: 10.2340/actadv.v105.44198
26. Kimball, A, Gieler, U, Linder, D, Sampogna, F, Warren, R, and Augustin, M. Psoriasis: is the impairment to a patient’s life cumulative? Acad Dermatol Venereol. (2010) 24:989–1004. doi: 10.1111/j.1468-3083.2010.03705.x
Keywords: alopecia areata, quality of life, questionnaire validation, psychodermatology, trichology
Citation: Muñoz-Barba D, García-Moronta C, Limeres-De la Rosa M, Sánchez-Díaz M and Arias-Santiago S (2025) Psychometric validation of the Spanish alopecia areata–life impact questionnaire. Front. Med. 12:1706110. doi: 10.3389/fmed.2025.1706110
Edited by:
Virginia Velasco-Tamariz, University Hospital October 12, SpainReviewed by:
Laura Ghanem, Lebanese University, LebanonMiguel Antonio Lasheras-Pérez, University and Polytechnic Hospital of La Fe, Spain
Copyright © 2025 Muñoz-Barba, García-Moronta, Limeres-De la Rosa, Sánchez-Díaz and Arias-Santiago. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manuel Sánchez-Díaz, bWFub2xvLjk0LnNhbmNoZXpAZ21haWwuY29t