 Annalisa Boscolo1,2,†
Annalisa Boscolo1,2,† Nicolò Sella2,†
Nicolò Sella2,† Francesco Zarantonello2
Francesco Zarantonello2 Raimondo Pittorru3
Raimondo Pittorru3 Giulia Mormando4Carlo Alberto Bertoncello1Elena Curmaci1Roberta Ceccato1Valentina Fincati1Paola Masetti Zannini1Angela Bianco1Giordana Coniglio1Elisa Pistollato1Alessandro Zambianchi1Mustaj Sindi1Sabrina Congedi1Gabriella Roca3Arianna Peralta2Luisa Muraro2Giorgia Pacchiarini2
Giulia Mormando4Carlo Alberto Bertoncello1Elena Curmaci1Roberta Ceccato1Valentina Fincati1Paola Masetti Zannini1Angela Bianco1Giordana Coniglio1Elisa Pistollato1Alessandro Zambianchi1Mustaj Sindi1Sabrina Congedi1Gabriella Roca3Arianna Peralta2Luisa Muraro2Giorgia Pacchiarini2 Federico Migliore3Manuel De Lazzari3Tommaso Pettenuzzo2*
Federico Migliore3Manuel De Lazzari3Tommaso Pettenuzzo2* Federico Rea3Martina Perazzolo Marra3
Federico Rea3Martina Perazzolo Marra3
- 1Section of Anaesthesiology and Intensive Care, Department of Medicine (DIMED), University of Padua, Padova, Italy
- 2Institute of Anesthesia and Intensive Care, Padua University Hospital, Padova, Italy
- 3Department of Cardiac, Thoracic, Vascular Sciences and Public Health, University of Padua, Padova, Italy
- 4Department of Medicine (DIMED), University of Padua, Padova, Italy
Introduction: Lung transplantation (LT) is the standard treatment for end-stage chronic respiratory failure that does not respond to other therapies. Advances in surgical techniques and perioperative care have improved survival rates. However, postoperative complications, particularly atrial arrhythmias (AA) remain clinically significant. Although AAs are frequently observed in the early postoperative period, data regarding their incidence and impact on outcomes are scarce. This observational study aims to: (i) assess the incidence of new-onset postoperative AA within one month of bilateral LT; (ii) evaluate their impact on short- and mid-term outcomes; and iii) identify potential predictors.
Materials and methods: We retrospectively reviewed all consecutive bilateral LT recipients admitted to the Intensive Care Unit (ICU) of the University Hospital of Padua between October 2021 and December 2023. Clinical variables, perioperative right heart catheterization data, and echocardiographic measurements were collected.
Results: A total of 85 LT recipients were enrolled. Postoperative AA occurred in 27 patients (32%), with atrial fibrillation emerging as the most common arrhythmia (55.6%). The remaining 58 (68%) patients did not develop any arrhythmic disorder. Many AA patients (22, 81.5%) required treatment with antiarrhythmic drugs or electrical cardioversion. Compared to the control group, AA patients were older (p-value 0.002) and usually affected by coronary heart disease (18.5% vs. 5.2%, p-value 0.05) and obstructive respiratory disease (55.5% vs. 27.7%, p-value 0.004). AA patients more frequently experienced difficult weaning from mechanical ventilation, a higher incidence of postoperative V-A ECMO, more frequent anastomotic complications, and longer ICU stays, as compared to controls. Multivariate analysis identified older age (OR 1.11, 95% CI 1.01–1.25, p-value 0.047) and higher postoperative dobutamine dosage (OR 2.25, 95% CI 1.15–5.01, p-value 0.026) as the only significant predictors of new-onset AA within one month of LT.
Conclusions: In our cohort, the incidence of new-onset AAs was 32% after bilateral LT. AA patients experienced worse short- and mid-term outcomes compared to controls. Furthermore, this study highlights older age and postoperative dobutamine administration as significant predictors of new-onset AA following bilateral LT. Further research is needed to clarify the causal relationships and long-term implications of AA on the clinical course of LT recipients.
1 Introduction
Lung transplantation (LT) is the established treatment for end-stage chronic respiratory failure not amenable to other medical or surgical therapies (1). Several clinical conditions require LT, including cystic fibrosis, chronic obstructive pulmonary disease, and interstitial lung disease. LT recipients represent a special and growing population. Advances in surgical techniques and perioperative care have significantly improved the one-year survival rate for LT, increasing from 73% in the 1990s to approximately 84% today (2). Furthermore, the number of LT recipients has doubled since 2000, with approximately 2,000–2,500 single or bilateral lung transplants performed annually in the United States and over 4,000 worldwide, yielding an estimated five-year survival rate of 50% (1–4).
Among the postoperative complications of LT, arrhythmias emerge as a significant risk factor associated with negative prognostic implications; however, few studies and limited data are available on this topic (5–8). Atrial arrhythmias (AA), including atrial fibrillation (AF), atrial flutter (AFL), and atrial tachycardia (AT), are the most commonly observed arrhythmias following LT (6). These arrhythmias occur in approximately 19%–46% of LT patients during the immediate postoperative period and in about 14% during long-term follow-up (5, 6). Specifically, postoperative AF is defined as a new-onset cardiac arrhythmia arising in the immediate postoperative period, with an incidence ranging from 2% to 30% and peaking between postoperative days 2–4 (9). Postoperative AF is associated with an increased risk of stroke, myocardial infarction, and death compared to AF of non-postoperative origin (9).
It is important to distinguish between early postoperative atrial tachyarrhythmias, which occur before hospital discharge or within three months post-LT, and late atrial tachyarrhythmias, occurring more than 3–6 months post-LT (6).
Indeed, our observational study aims to assess: (i) the incidence of new-onset postoperative AAs within one month of bilateral LT; (ii) their impact on short- and mid-term outcomes; and identifying (iii) potential predictors.
2 Materials and methods
The study was approved by the local Institutional Ethic Committee (reference 4539_AO_18) and conducted in accordance with the principles of Good Clinical Practice outlined in the Declaration of Helsinki. The informed consent was obtained from all participants. This article was written in accordance with the STROBE checklist (Supplementary Table S1) (10). All consecutive patients, undergoing to the first bilateral LT at Padua University Hospital, were retrospectively screened between October 2021 and December 2023. Predefined exclusion criteria were: (1) age < 18 years old; (2) single transplant; (3) re-transplant; (4) incomplete records (i.e., missing echocardiographic data and/or outcomes of interest); and (5) refusal of consent. The study flowchart is depicted in Figure 1.
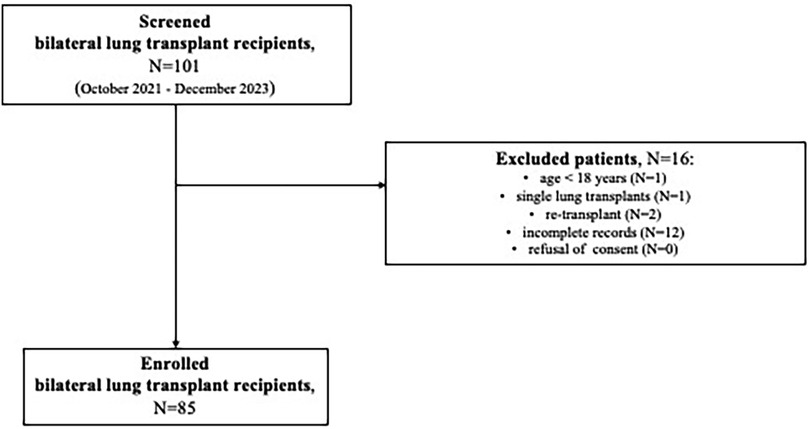
Figure 1. Study flowchart.
The following variables were collected from electronic health records (Tables 1–3): (i) demographic data [age, gender, body mass index (BMI)]; (ii) comorbidities; (iii) therapies at home (i.e., corticosteroids or O2-therapy); (iv) underlying diseases leading to LT (septic, interstitial, obstructive or others) (see full description in Table 1); (v) preoperative cardiac measurements (including parameters derived from right heart catheterization (11, 12) and ecographic measurements of cardiac function (11, 13) (see full description in Table 2); (vi) intra-operative characteristics and management; (vii) hemodynamic characteristics after ICU admission [i.e., pulse contour cardiac output (PICCO) parameters, vasoactive and inotropic support]; (viii) incidence of arrhythmic events and treatments (see full description in Table 3); and then (xi) outcomes of interest (see full description in Table 4).
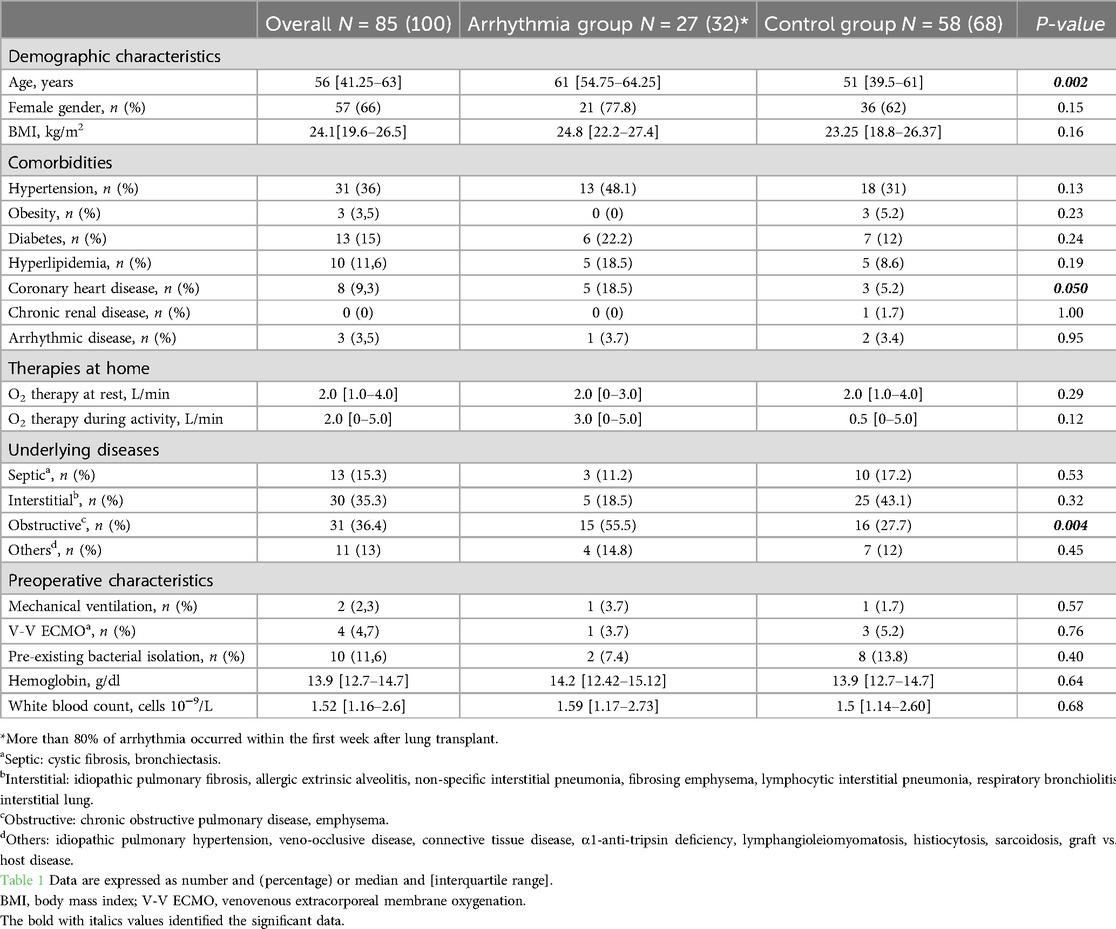
Table 1. Baseline characteristics of bilateral lung transplant recipients.
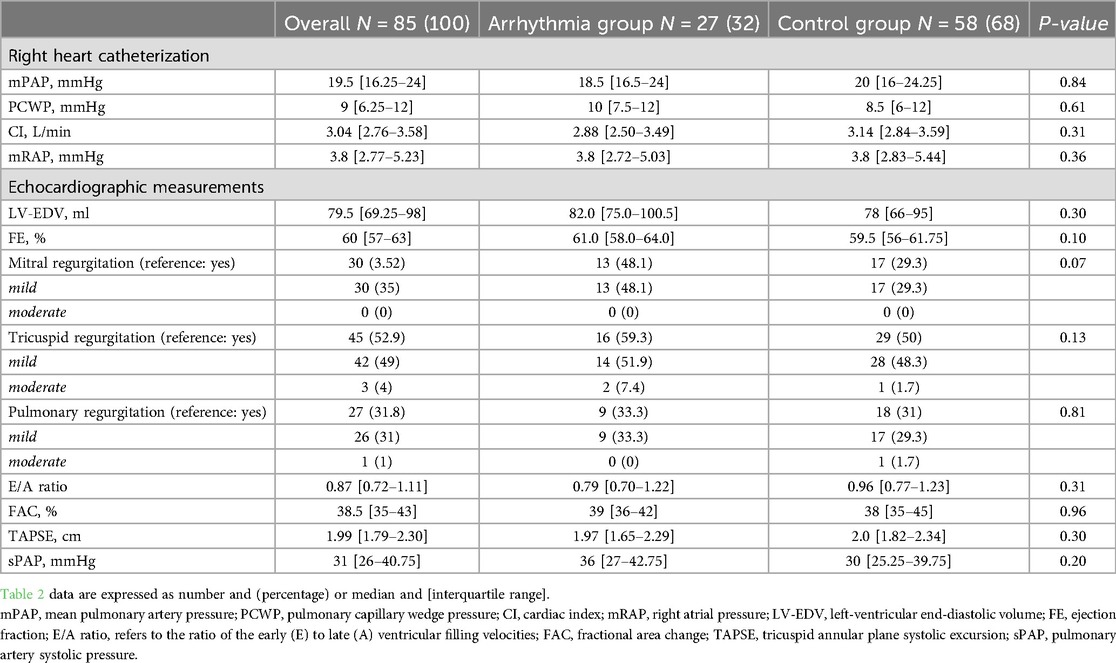
Table 2. Preoperative cardiac measurements.
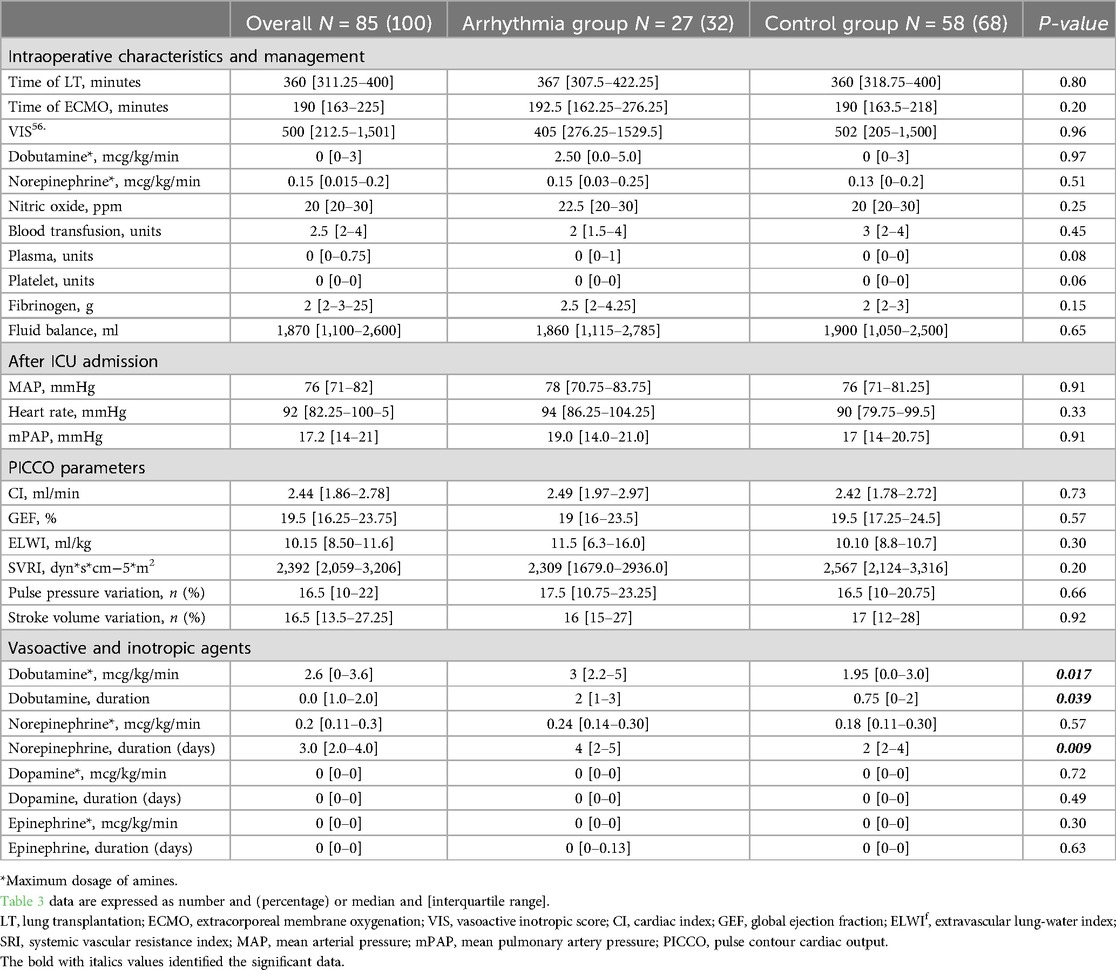
Table 3. Characteristics of bilateral lung transplant recipients.
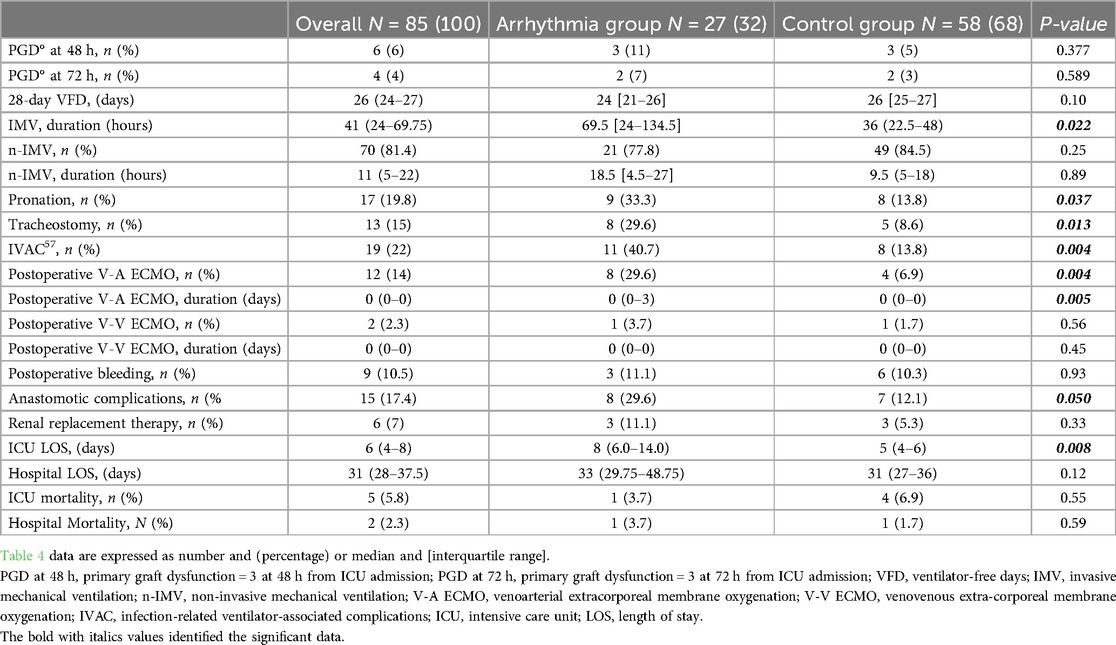
Table 4. Outcomes of bilateral lung transplant recipients.
Specifically, all right heart catheterizations and echocardiographic examinations were performed within routine clinical practice by multiple trained cardiologists and sonographers using diverse commercially available machines and then, patients' measurements were reviewed by expert cardiologists (PMM and CD). All echocardiographic measurements were evaluated and graded according to international guidelines (9, 14–16).
All transplants were performed with a central V-A ECMO support (17–19). Intraoperative inotropic and vasoactive support was administered according to the clinical judgement of the anesthesiologist in charge on the basis of advanced hemodynamic monitoring, including transpulmonary thermodilution, pulmonary artery catheter, and transesophageal echocardiography (20). Anesthetic management, immunosuppressive treatments and ventilations protocols were standardized in our institution, since 2021, consistently with international recommendations (18, 21–26). The 28-day ventilator free days were defined as the number of days of unassisted breathing to day 28 without having to reinstitute invasive ventilation. Patients who died before day 28 were assigned 0 (27). The follow-up is continued up to 3 months after surgery.
2.1 Statistical analysis
Continuous data were presented as mean and standard deviation (SD) when normally distributed or as the median with interquartile range [IQR] when non-normally distributed. Categorical data were summarized using absolute and (relative frequencies). Comparison of two groups of categorical variables were performed using Student's t-test of unpaired samples, while in case of non-normality or small sample size, Mann–Whitney U test was used. No imputation for missing data has been planned.
A multiple univariable logistic regression model was used to identify independent risk factors for AA. In multivariable logistic regression analysis we use significant variables from the univariate analysis that recorded a p-value < 0.1 (Supplementary Table S2). Moreover, the univariable analysis was applied to all clinical variables shown in Tables 1–3. Models were checked for collinearity and variables with Variance Inflation Factor (VIF) greater than 4 were excluded. All statistical tests were 2-tailed, and statistical significance was defined as p < 0.05. All analyses have been conducted using R version 4.0.3 (R foundation for Statistical Computing, Vienna, Austria).
3 Results
3.1 Baseline clinical characteristics
This study screened 101 LTs and finally analyzed 85, divided into two groups: the AA Group (27 patients, 32%) and the control Group (58 patients, 68%). Sixteen patients were excluded for the following reasons: age < 18 years (n. 1), single lung transplants (n. 1), re-transplant (n. 2), incomplete records (n. 12), refusal of consent (n. 0) (Figure 1).
Among patients in the AA group, AF was the most common arrhythmia (15, 55.6%), followed by paroxysmal supraventricular tachycardia (8, 29.6%) and mixed arrhythmias (4, 14.8%). Most patients (22, 81.5%) received either antiarrhythmic drugs or electrical cardioversion, while four subjects (14.8%) required a combination of both. One patient (3.7%) did not receive any treatment. Amiodarone was the primary antiarrhythmic used (26, 96%). Of those, 4 (15%) patients were also treated with beta-blockers.
With regards to baseline characteristics, patients in the AA Group were significantly older (median 61 years) compared to the control Group (median 51 years, p-value 0.002) (Table 1). Coronary heart diseases were more frequent in the AA Group (18.5% vs. 5.2%, p-value 0.05), while all other comorbidities were comparable between groups. According to end-stage underlying diseases, obstructive lung disease (e.g., COPD, emphysema) was significantly more common in the AA Group (55.5%) than in the control Group (27.7%) (p-value 0.004) (Table 1).
As shown in Tables 2, 3, there were no significant differences in preoperative cardiac measurements, intraoperative characteristics, blood transfusion requirements (including red blood cells, plasma, platelets, and fibrinogen) between groups (Table 3). Similarly, after ICU admission, mean arterial pressure, heart rate, mean pulmonary artery pressure, PICCO parameters (including cardiac index, global ejection fraction, extravascular lung-water index, systemic vascular resistance index, pulse pressure variation, and stroke volume variation) did not differ significantly (Table 3).
Interestingly, AA-patients required higher doses (p-value 0.017) and more prolonged infusions of dobutamine (p-value 0.039), as compared to controls. Similarly, norepinephrine duration was significantly longer in the AA group than in the control group (4 vs. 2 days, p-value 0.009) (Table 3).
3.2 Secondary outcomes
The incidence of primary graft dysfunction (PGD) at both 48- and 72 h post-LT was similar between the AA and control groups (81.5% vs. 77.6% at 48 h, p-value 0.10; 81.5% vs. 75.8% at 72 h, p-value 0.55). However, patients in the AA group required significantly longer invasive mechanical ventilation (IMV) compared to controls (69.5 vs. 36 h, p-value 0.022) (Table 4). Patients in the AA group had a significantly higher rate of pronation therapy (33.3% vs. 13.8%, p-value 0.037) and tracheostomes (29.6% vs. 8.6%, p-value 0.013), indicating a more complex postoperative respiratory course (Table 4). The need for ECMO and its postoperative duration were greater in the AA group compared to the control group (29.6% vs. 6.9%, p-value 0.004), with a longer ECMO duration (p-value 0.005) (Table 4). Patients in the AA group had a significantly higher incidence of infection-related ventilator-associated complications (40.7% vs. 13.8%, p-value 0.004) and anastomotic complications (29.6% vs. 12.1%, p-value 0.050) (Table 4). Finally, the ICU length of stay (LOS) was significantly longer in the AA group compared to the control group (8 vs. 5 days, p-value 0.008) (Table 4).
3.3 Risk factors for developing Aa
The multivariate results indicate that only age (OR 1.11, 95% CI 1.01–1.25, p-value of 0.047) (Table 5) and a high postoperative dobutamine dosage (OR 2.25, 95% CI 1.15–5.01, p-value 0.026) were significant predictors of postoperative new-onset AA (Table 5).
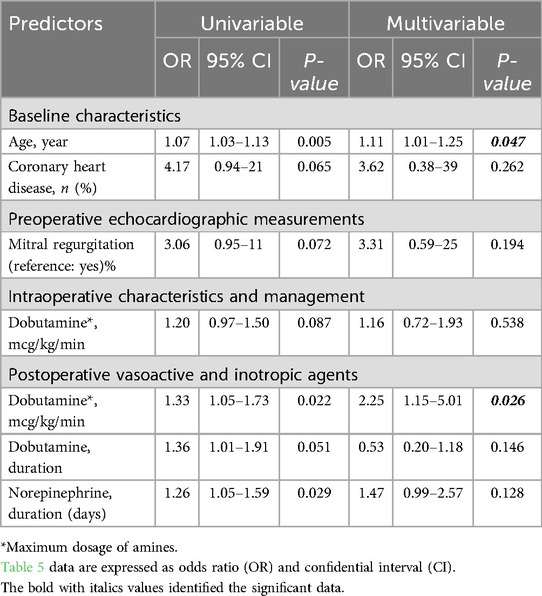
Table 5. Logistic regressions.
Finally, at 3 months postoperatively, there were no new cases of AA. Only one patient (3.7%) remained on oral anticoagulation, while six patients (22.2%) were still taking antiarrhythmic drugs.
4 Discussion
This single center observational study, conducted in a homogeneous cohort of bilateral LT, aims to assess the incidence and predictors of new-onset AA after LT, as well as the potential impact of postoperative AA on patients' outcomes.
The results demonstrate that the AA Group had significant differences in baseline characteristics, including older age and a higher prevalence of coronary heart disease and obstructive lung disease. These findings suggest that patients in the AA Group had more comorbidities, which could potentially contribute to the higher incidence of AA post-LT. In fact, the etiology of postoperative AA is multifactorial, involving surgical manipulation (28), ischemia-reperfusion injury (29), electrolyte imbalances (30), and heightened sympathetic activity and comorbidities, including smoking, hypertension (31), and diabetes mellitus (32).
Hypertension, and diabetes mellitus are well-established comorbidities associated with up to a two-fold increased risk of AF, inducing oxidative stress, inflammation, atrial fibrosis (33), and promoting structural and electrical remodeling of the atrium (31, 32, 34, 35).
The study found that AF was the most common arrhythmia in the AA Group, which is consistent with previous literature that reports a higher incidence of AAs in post-lung LT patients (6, 28). Many of these patients were treated with antiarrhythmic drugs, primarily amiodarone, highlighting the importance of managing arrhythmias in this cohort (36–38). Notably, no new cases of AF were observed at 3 months after LT, and most patients had discontinued antiarrhythmic drugs by this time, suggesting that arrhythmias may resolve or become manageable with appropriate treatment, as recently published (28, 39).
The occurrence of AA seems to contribute to a more complicated respiratory recovery and a longer need for postoperative V-A ECMO could be related to a higher postoperative cardiovascular instability associated with arrhythmias. Moreover, patients in the AA Group had a significantly higher incidence of IVAC and anastomotic complications. This may suggest that arrhythmias contribute to a more fragile postoperative state, increasing susceptibility to infections and other complications.
Keeping in line, the occurrence of AA after noncardiac thoracic surgery in the elderly population strongly correlates with worse outcomes, such as increased ICU LOS and mortality (40–42). Nowadays, neither effective screening strategies nor targeted prophylaxis have been tested, therefore, a close monitoring could be recommended to the higher risk patients.
The multivariate analysis revealed that age and postoperative dobutamine administration were significant predictors of postoperative AA. This finding emphasizes the role of age as a risk factor for AA, as older patients may have a lower cardiovascular reserve, making them more prone to arrhythmic events. Likewise, previous data in literature reported age older than 50 years as an independent risk factor for higher prevalence of AA and more severe arrhythmia type (43), suggesting for each unit increased in age, a greater odds to develop AA of 4.5% (44). This multifactorial relationship has not yet been well understood, although the disruption of the intracellular calcium regulation system, the scars and the effects of other chronic pathologies have been held countable (45, 46). Additionally, also the use of dobutamine, a β1-adrenergic agonist commonly used to enhance cardiac output in patients with low cardiac function, was identified as a key predictor of new-onset AA, suggesting that the use of dobutamine may be both a consequence and a contributing factor to arrhythmias after LT. However, its stimulatory effect on the myocardium can predispose patients to AA, particularly AF (47–49).
Despite the significant findings, several limitations should be considered. The sample size was relatively small, and the study was an observational, retrospective and single-center investigation, meaning causality cannot be definitively established. Additionally, while the study provides valuable insights into the relationship between AA and postoperative complications, other unmeasured variables, such as genetic predisposition, may also contribute to the observed outcomes. Further research is needed to elucidate the causal relationships and long-term implications of AA on the clinical course of LT recipients.
In conclusion, this study, showing an incidence of new-onset AA after LT of 32%, highlights that age and postoperative dobutamine administration are significant predictors of new-onset AA following bilateral LT. Moreover, AA patients experienced worse short- and mid-term outcomes (higher rate of pronation therapy, tracheostomy, complex postoperative respiratory course, greater rate of prolonged V-A ECMO, IVAC, anastomotic complications and longer ICU LOS). Indeed, clinicians should be aware that new-onset atrial arrhythmias are common after bilateral lung transplantation, particularly in older patients and those receiving postoperative dobutamine. These arrhythmias are associated with more complex respiratory recovery, a higher risk of postoperative complications, and longer ICU stays. Early identification and close monitoring of high-risk patients are essential to improve outcomes and guide timely management of arrhythmias in this setting.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Padua Hospital Ethic Committee (reference 4539_AO_18). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AB: Writing – original draft, Conceptualization, Data curation. NS: Writing – review & editing, Methodology, Conceptualization. FZ: Writing – review & editing, Formal analysis, Data curation. RP: Writing – review & editing, Conceptualization, Data curation. GM: Formal analysis, Software, Writing – review & editing. CB: Investigation, Writing – review & editing, Data curation. EC: Data curation, Writing – review & editing, Software. RC: Writing – review & editing, Methodology, Data curation. VF: Methodology, Software, Writing – review & editing. PM: Investigation, Writing – review & editing, Data curation. AB: Methodology, Writing – review & editing, Software. GC: Data curation, Conceptualization, Writing – review & editing. EP: Writing – original draft, Formal analysis, Supervision. AZ: Methodology, Writing – review & editing, Investigation. MS: Data curation, Investigation, Writing – review & editing. SC: Writing – original draft, Writing – review & editing. GR: Formal analysis, Supervision, Writing – review & editing. AP: Supervision, Software, Writing – review & editing. LM: Writing – review & editing, Conceptualization, Resources. GP: Data curation, Conceptualization, Writing – review & editing. FM: Supervision, Writing – original draft, Conceptualization. MD: Investigation, Writing – review & editing, Methodology. TP: Conceptualization, Writing – original draft, Formal analysis. FR: Validation, Writing – review & editing, Supervision. MP: Conceptualization, Writing – original draft, Methodology.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Correction Note
This article has been corrected with minor changes. These changes do not impact the scientific content of the article.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frtra.2025.1601228/full#supplementary-material
Abbreviations
PGD, primary graft dysfunction; LT, lung transplant; ICU, intensive care unit; IMV, invasive mechanical ventilation; V-V, venovenous; V-A, venous-arterial; ECMO, extracorporeal membrane oxygenation; SD, standard deviation; BMI, body max index; HR, hazard ratio; CI, confidence interval; n, number; mo, months; LOS, length of stay; H, hospital; RV, right ventricle; h, hour; r, Spearman's correlation coefficient.
References
1. Chambers DC, Yusen RD, Cherikh WS, Goldfarb SB, Kucheryavaya AY, Khusch K, et al. The registry of the international society for heart and lung transplantation: thirty-fourth adult lung and heart-lung transplantation report-2017; focus theme: allograft ischemic time. J Heart Lung Transplant Off Publ Int Soc Heart Transplant. (2017) 36(10):1047–59. doi: 10.1016/j.healun.2017.07.016
2. Valapour M, Lehr CJ, Schladt DP, Smith JM, Goff R, Mupfudze TG, et al. OPTN/SRTR 2021 annual data report: lung. Am J Transplant Off J Am Soc Transplant Am Soc Transpl Surg. (2023) 23(2 Suppl 1):S379–442. doi: 10.1016/j.ajt.2023.02.009
3. Yusen RD, Edwards LB, Dipchand AI, Goldfarb SB, Kucheryavaya AY, Levvey BJ, et al. The registry of the international society for heart and lung transplantation: thirty-third adult lung and heart-lung transplant report-2016; focus theme: primary diagnostic indications for transplant. J Heart Lung Transplant Off Publ Int Soc Heart Transplant. (2016) 35(10):1170–84. doi: 10.1016/j.healun.2016.09.001
4. Stehlik J, Bavaria JE, Bax J, Cronenwett JL, Edwards LB, Fairman RM, et al. Heart, lung, and vascular registries: evolving goals, successful approaches, and ongoing innovation. J Heart Lung Transplant Off Publ Int Soc Heart Transplant. (2016) 35(10):1149–57. doi: 10.1016/j.healun.2016.08.021
5. Dizon JM, Chen K, Bacchetta M, Argenziano M, Mancini D, Biviano A, et al. A comparison of atrial arrhythmias after heart or double-lung transplantation at a single center: insights into the mechanism of post-operative atrial fibrillation. J Am Coll Cardiol. (2009) 54(22):2043–8. doi: 10.1016/j.jacc.2009.08.029
6. Chaikriangkrai K, Jyothula S, Jhun HY, Chang SM, Graviss EA, Shuraih M, et al. Incidence, risk factors, prognosis, and electrophysiological mechanisms of atrial arrhythmias after lung transplantation. JACC Clin Electrophysiol. (2015) 1(4):296–305. doi: 10.1016/j.jacep.2015.05.009
7. Fan J, Zhou K, Li S, Du H, Che G. Incidence, risk factors and prognosis of postoperative atrial arrhythmias after lung transplantation: a systematic review and meta-analysis. Interact Cardiovasc Thorac Surg. (2016) 23(5):790–9. doi: 10.1093/icvts/ivw208
8. Waldron NH, Klinger RY, Hartwig MG, Snyder LD, Daubert JP, Mathew JP. Adverse outcomes associated with postoperative atrial arrhythmias after lung transplantation: a meta-analysis and systematic review of the literature. Clin Transplant. (2017) 31(4). doi: 10.1111/ctr.12926
9. Halvorsen S, Mehilli J, Cassese S, Hall TS, Abdelhamid M, Barbato E, et al. 2022 ESC guidelines on cardiovascular assessment and management of patients undergoing non-cardiac surgery. Eur Heart J. (2022) 43(39):3826–924. doi: 10.1093/eurheartj/ehac270
10. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. (2007) 4(10):e296. doi: 10.1371/journal.pmed.0040296
11. Rajagopalan N, Borlaug BA, Bailey AL, Eckman PM, Guglin M, Hall S, et al. Practical guidance for hemodynamic assessment by right heart catheterization in management of heart failure. JACC Heart Fail. (2024) 12(7):1141–56. doi: 10.1016/j.jchf.2024.03.020
12. Krishnan A, Markham R, Savage M, Wong YW, Walters D. Right heart catheterisation: how to do it. Heart Lung Circ. (2019) 28(4):e71–8. doi: 10.1016/j.hlc.2018.08.005
13. Celestin BE, Bagherzadeh SP, Ichimura K, Santana EJ, Sanchez PA, Tobore T, et al. Identifying consistent echocardiographic thresholds for risk stratification in pulmonary arterial hypertension. Pulm Circ. (2024) 14(2):e12361; =14. doi: 10.1002/pul2.12361
14. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, et al. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr Off Publ Am Soc Echocardiogr. (2003) 16(7):777–802. doi: 10.1016/S0894-7317(03)00335-3
15. Mukherjee M, Rudski LG, Addetia K, Afilalo J, ’Alto D, Freed M, et al. Guidelines for the echocardiographic assessment of the right heart in adults and special considerations in pulmonary hypertension: recommendations from the American society of echocardiography. J Am Soc Echocardiogr Off Publ Am Soc Echocardiogr. (2025) 38(3):141–86. doi: 10.1016/j.echo.2025.01.006
16. Nagueh SF, Smiseth OA, Appleton CP, Byrd BF, Dokainish H, Edvardsen T, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American society of echocardiography and the European association of cardiovascular imaging. J Am Soc Echocardiogr Off Publ Am Soc Echocardiogr. (2016) 29(4):277–314. doi: 10.1016/j.echo.2016.01.011
17. Hoechter DJ, von Dossow V, Winter H, Müller HH, Meiser B, Neurohr C, et al. The Munich lung transplant group: intraoperative extracorporeal circulation in lung transplantation. Thorac Cardiovasc Surg. (2015) 63(8):706–14. doi: 10.1055/s-0035-1556873
18. Boscolo A, Dell’Amore A, Pettenuzzo T, Sella N, De Cassai A, Pistollato E, et al. The impact of new treatments on short- and MID-term outcomes in bilateral lung transplant: a propensity score study. J Clin Med. (2022) 11(19):5859. doi: 10.3390/jcm11195859
19. Martin AK, Mercier O, Fritz AV, Gelzinis TA, Hoetzenecker K, Lindstedt S, et al. ISHLT Consensus statement on the perioperative use of ECLS in lung transplantation: part II: intraoperative considerations. J Heart Lung Transplant Off Publ Int Soc Heart Transplant. (2024) S1053-2498(24):01830–8. doi: 10.1016/j.healun.2024.08.027
20. Rocca D, Brondani G, Costa A, G M. Intraoperative hemodynamic monitoring during organ transplantation: what is new? Curr Opin Organ Transplant. (2009) 14(3):291–6. doi: 10.1097/MOT.0b013e32832d927d
21. Marczin N, de Waal EEC, Hopkins PMA, Mulligan MS, Simon A, Shaw AD, et al. International consensus recommendations for anesthetic and intensive care management of lung transplantation. An EACTAIC, SCA, ISHLT, ESOT, ESTS, and AST approved document. J Heart Lung Transplant Off Publ Int Soc Heart Transplant. (2021) 40(11):1327–48. doi: 10.1016/j.healun.2021.07.012
22. Nardo D, Tikkanen M, Husain J, Singer S, Cypel LG, Ferguson M, et al. Postoperative management of lung transplant recipients in the intensive care unit. Anesthesiology. (2022) 136(3):482–99. doi: 10.1097/ALN.0000000000004054
23. Boscolo A, Sella N, Pettenuzzo T, Pistollato E, Calabrese F, Gregori D, et al. Diaphragm dysfunction predicts weaning outcome after bilateral lung transplant. Anesthesiology. (2023) 140(1):126–36. doi: 10.1097/ALN.0000000000004729
24. Boscolo A, Sella N, Pettenuzzo T, De Cassai A, Crociani S, Schiavolin C, et al. Multidrug-resistant and extended-spectrum β-lactamase gram-negative Bacteria in bilateral lung transplant recipients: incidence, risk factors, and in-hospital mortality. Chest. (2022) 162(6):1255–64. doi: 10.1016/j.chest.2022.06.046
25. Boscolo A, Sella N, Lorenzoni G, Pettenuzzo T, Pasin L, Pretto C, et al. Static compliance and driving pressure are associated with ICU mortality in intubated COVID-19 ARDS. Crit Care Lond Engl. (2021) 25(1):263. doi: 10.1186/s13054-021-03667-6
26. Sella N, Pettenuzzo T, Zarantonello F, Andreatta G, De Cassai A, Schiavolin C, et al. Electrical impedance tomography: a compass for the safe route to optimal PEEP. Respir Med. (2021) 187:106555. doi: 10.1016/j.rmed.2021.106555
27. Renard Triché L, Futier E, De Carvalho M, Piñol-Domenech N, Bodet-Contentin L, Jabaudon M, et al. Sample size estimation in clinical trials using ventilator-free days as the primary outcome: a systematic review. Crit Care Lond Engl. (2023) 27(1):303. doi: 10.1186/s13054-023-04562-y
28. See VY, Roberts-Thomson KC, Stevenson WG, Camp PC, Koplan BA. Atrial arrhythmias after lung transplantation: epidemiology, mechanisms at electrophysiology study, and outcomes. Circ Arrhythm Electrophysiol. (2009) 2(5):504–10. doi: 10.1161/CIRCEP.109.867978
29. Oktay V, Baydar O, Sinan ÜY, Koçaş C, Abacı O, Yıldız A, et al. The effect of oxidative stress related with ischemia-reperfusion damage on the pathogenesis of atrial fibrillation developing after coronary artery bypass graft surgery. Turk Kardiyol Dernegi Arsivi Turk Kardiyol Derneginin Yayin Organidir. (2014) 42(5):419–25. doi: 10.5543/tkda.2014.84032
30. Wu Y, Kong XJ, Ji YY, Fan J, Ji CC, Chen XM, et al. Serum electrolyte concentrations and risk of atrial fibrillation: an observational and mendelian randomization study. BMC Genomics. (2024) 25(1):280. doi: 10.1186/s12864-024-10197-2
31. Aronow WS. Hypertension associated with atrial fibrillation. Ann Transl Med. (2017) 5(23):457. doi: 10.21037/atm.2017.10.33
32. Seyed Ahmadi S, Svensson AM, Pivodic A, Rosengren A, Lind M. Risk of atrial fibrillation in persons with type 2 diabetes and the excess risk in relation to glycaemic control and renal function: a Swedish cohort study. Cardiovasc Diabetol. (2020) 19(1):9. doi: 10.1186/s12933-019-0983-1
33. Goette A, Lendeckel U, Kuchenbecker A, Bukowska A, Peters B, Klein HU, et al. Cigarette smoking induces atrial fibrosis in humans via nicotine. Heart Br Card Soc. (2007) 93(9):1056–63. doi: 10.1136/hrt.2005.087171
34. Imtiaz Ahmad M, Mosley CD, O’Neal WT, Judd SE, McClure LA, Howard VJ, et al. Smoking and risk of atrial fibrillation in the REasons for geographic and racial differences in stroke (REGARDS) study. J Cardiol. (2018) 71(2):113–7. doi: 10.1016/j.jjcc.2017.07.014
35. Chamberlain AM, Agarwal SK, Folsom AR, Duval S, Soliman EZ, Ambrose M, et al. Smoking and incidence of atrial fibrillation: results from the atherosclerosis risk in communities (ARIC) study. Heart Rhythm. (2011) 8(8):1160–6. doi: 10.1016/j.hrthm.2011.03.038
36. D’Angelo AM, Chan EG, Hayanga JWA, Odell DD, Pilewski J, Crespo M, et al. Atrial arrhythmias after lung transplantation: incidence and risk factors in 652 lung transplant recipients. J Thorac Cardiovasc Surg. (2016) 152(3):901–9. doi: 10.1016/j.jtcvs.2016.04.070
37. Jesel L, Barraud J, Lim HS, Marzak H, Messas N, Hirschi S, et al. Early and late atrial arrhythmias after lung transplantation-incidence, predictive factors and impact on mortality. Circ J Off J Jpn Circ Soc. (2017) 81(5):660–7. doi: 10.1253/circj.CJ-16-0892
38. Barnes H, Gurry G, McGiffin D, Westall G, Levin K, Paraskeva M, et al. Atrial flutter and fibrillation following lung transplantation: incidence, associations and a suggested therapeutic algorithm. Heart Lung Circ. (2020) 29(10):1484–92. doi: 10.1016/j.hlc.2019.10.011
39. Lee G, Wu H, Kalman JM, Esmore D, Williams T, Snell G, et al. Atrial fibrillation following lung transplantation: double but not single lung transplant is associated with long-term freedom from paroxysmal atrial fibrillation. Eur Heart J. (2010) 31(22):2774–82. doi: 10.1093/eurheartj/ehq224
40. Hollings DD, Higgins RSD, Faber LP, Warren WH, Liptay MJ, Basu S, et al. Age is a strong risk factor for atrial fibrillation after pulmonary lobectomy. Am J Surg. (2010) 199(4):558–61. doi: 10.1016/j.amjsurg.2009.11.006
41. Vaporciyan AA, Correa AM, Rice DC, Roth JA, Smythe WR, Swisher SG, et al. Risk factors associated with atrial fibrillation after noncardiac thoracic surgery: analysis of 2588 patients. J Thorac Cardiovasc Surg. (2004) 127(3):779–86. doi: 10.1016/j.jtcvs.2003.07.011
42. Bessissow A, Khan J, Devereaux PJ, Alvarez-Garcia J, Alonso-Coello P. Postoperative atrial fibrillation in non-cardiac and cardiac surgery: an overview. J Thromb Haemost JTH. (2015) 13(1):S304–312. doi: 10.1111/jth.12974
43. Hadjizacharia P, O’Keeffe T, Brown CVR, Inaba K, Salim A, Chan LS, et al. Incidence, risk factors, and outcomes for atrial arrhythmias in trauma patients. Am Surg. (2011) 77(5):634–9. doi: 10.1177/000313481107700526
44. Shin J, Andrews M, DeJean L, Debski N, Exarchakis A, Fleming J, et al. Risk factors associated with atrial fibrillation in elderly patients. J Clin Med Res. (2023) 15(3):148–60. doi: 10.14740/jocmr4884
45. Hatch F, Lancaster MK, Jones SA. Aging is a primary risk factor for cardiac arrhythmias: disruption of intracellular Ca2+ regulation as a key suspect. Expert Rev Cardiovasc Ther. (2011) 9(8):1059–67. doi: 10.1586/erc.11.112
46. Wang N, Yu Y, Sun Y, Zhang H, Wang Y, Chen C, et al. Acquired risk factors and incident atrial fibrillation according to age and genetic predisposition. Eur Heart J. (2023) 44(47):4982–93. doi: 10.1093/eurheartj/ehad615
47. Kaakeh Y, Overholser BR, Lopshire JC, Tisdale JE. Drug-induced atrial fibrillation. Drugs. (2012) 72(12):1617–30. doi: 10.2165/11633140-000000000-00000
48. Kwon JH, Yoo SY, Kim S, Won H, Kim W, Her S, et al. Vasoactive inotropic score as a predictor of long-term mortality in patients after off-pump coronary artery bypass grafting. Sci Rep. (2022) 12(1):12863. doi: 10.1038/s41598-022-16900-1
49. Klompaa M, Branson R, Cawcutt K, Crist M, Eichenwald EC, Greene LR, et al. Strategies to prevent ventilator-associated pneumonia, ventilator-associated events, and nonventilator hospital-acquired pneumonia in acute-care hospitals: 2022 update. Infect Control Hosp Epidemiol. (2022) 43(6):687–713. doi: 10.1017/ice.2022.88
Keywords: arrhythmias, lung transplantation, extracorporeal membrane oxygenation, atrial fibillation, transplantation
Citation: Boscolo A, Sella N, Zarantonello F, Pittorru R, Mormando G, Bertoncello CA, Curmaci E, Ceccato R, Fincati V, Masetti Zannini P, Bianco A, Coniglio G, Pistollato E, Zambianchi A, Sindi M, Congedi S, Roca G, Peralta A, Muraro L, Pacchiarini G, Migliore F, De Lazzari M, Pettenuzzo T, Rea F and Perazzolo Marra M (2025) Postoperative atrial arrhythmias after bilateral lung transplantation with intraoperative V-A extracorporeal membrane oxygenation: a single-center experience. Front. Transplant. 4:1601228. doi: 10.3389/frtra.2025.1601228
Received: 27 March 2025; Accepted: 12 June 2025;
Published: 30 June 2025;
Corrected: 23 July 2025.
Edited by:
Varun Puri, Washington University in St. Louis, United StatesReviewed by:
Pietro Bertoglio, University of Bologna, ItalyThirugnanasambandan Sunder, Apollo Hospitals, India
Copyright: © 2025 Boscolo, Sella, Zarantonello, Pittorru, Mormando, Bertoncello, Curmaci, Ceccato, Fincati, Masetti Zannini, Bianco, Coniglio, Pistollato, Zambianchi, Sindi, Congedi, Roca, Peralta, Muraro, Pacchiarini, Migliore, De Lazzari, Pettenuzzo, Rea and Perazzolo Marra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tommaso Pettenuzzo, dG9tbWFzby5wZXR0ZW51enpvQGFvcGQudmVuZXRvLml0
†These authors have contributed equally to this work and share first authorship