 Benjamin Assouline1,2,3
Benjamin Assouline1,2,3 Timothée Olivier4
Timothée Olivier4 Anne-Laure Rougemont2,5
Anne-Laure Rougemont2,5 Philippe Compagnon2,6
Philippe Compagnon2,6 Charles-Henri Wassmer6
Charles-Henri Wassmer6 Hervé Quintard1,2
Hervé Quintard1,2 Karim Bendjelid1,2,3Franz Immer7
Karim Bendjelid1,2,3Franz Immer7 Raphaël Giraud1,2,3*
Raphaël Giraud1,2,3*
- 1Intensive Care Division, Department of Acute Care Medicine, Geneva University Hospitals, Geneva, Switzerland
- 2Department of Anesthesiology, Pharmacology, Intensive Care and Emergency Medicine, Faculty of Medicine, University of Geneva, Geneva, Switzerland
- 3Geneva Hemodynamic Research Group, Faculty of Medicine, University of Geneva, Geneva, Switzerland
- 4Division of Oncology, Geneva University Hospitals, Geneva, Switzerland
- 5Division of Clinical Pathology, Geneva University Hospitals, Geneva, Switzerland
- 6Division of Transplantation, Geneva University Hospitals, Geneva, Switzerland
- 7Swisstransplant, Bern, Switzerland
Background: Donation after circulatory death (DCD) may be complicated by incidental findings, including tumor lesions that require urgent diagnosis. Here, we describe the case of a DCD donor with a large adnexal mass. Abdominal normothermic regional perfusion (A-NRP) enabled the safe resection of the mass, real-time pathological analysis, and subsequent kidney transplantation.
Case summary: A 60-year-old woman suffered a hypoxic cardiac arrest and subsequently remained in a deep coma with poor neurological prognostic indicators. In accordance with her presumed wishes, life support was withdrawn, and a controlled DCD procedure with A-NRP was initiated. Imaging revealed a 27-cm adnexal mass. Laboratory markers showed elevated cancer antigen 125 (CA 125) but low cancer antigen 19-9 (CA 19-9) and carcinoembryonic antigen (CEA), and cytology was negative. Bilateral oophorectomy was performed under A-NRP, and the frozen section excluded malignancy, with final pathology confirming an ovarian thecoma. Both kidneys were procured; only the left kidney was transplanted successfully. The recipient experienced immediate diuresis and regained stable renal function at 1 month.
Discussion: This case illustrates how A-NRP provides oxygenated perfusion while allowing time for surgical excision and a pathological diagnosis of incidental tumors. It prevented unnecessary donor exclusion and enabled transplantation.
Conclusion: In selected DCD donors with incidental lesions, A-NRP can safely bridge the diagnostic process, preserve organ viability, and expand the donor pool.
Introduction
Worldwide, organ donation is constrained by organ availability. In Switzerland, patients awaiting transplantation greatly outnumber donors (1), and nearly 100 individuals die annually while on the waiting list. Thus, high detection rates of potential donors and minimal exclusions are crucial. Organ evaluation is a comprehensive exercise involving blood tests, imaging, and screening for contraindications, notably malignancy. However, cancer is no longer an absolute contraindication unless it is metastatic. Incidental findings of unknown masses on CT scans are common and often delay organ donation, adding stress to families.
In 2023, donation after circulatory death (DCD) accounted for approximately half of organ donations in Switzerland (2). Two procurement methods are employed: super rapid recovery (SRR, or crush laparotomy) and abdominal normothermic regional perfusion (A-NRP). Compared with SRR, A-NRP enables in situ reperfusion and is associated with better outcomes in kidney and liver transplantation (3). In Switzerland, controlled DCD (Maastricht category III) is the standard practice. According to the 2023 national report, there were 200 deceased donors, with 104 donation after brain death (DBD), and 96 DCD, accounting for 48% of all donations.
Here, we report a DCD case involving a large abdominal mass. Following a multidisciplinary discussion (with the ICU team, the Swiss National Transplant Society, the donation team, and the oncology team), A-NRP was used to maintain organ perfusion during mass excision and histology, ultimately allowing kidney procurement.
Case description
A 60-year-old woman was admitted to our ICU after a cardiac arrest. Her history was largely unknown aside from active smoking. According to her husband, she had progressive dyspnea for several weeks but sought no medical advice. One night, she coughed up blood and collapsed. Her husband initiated CPR; paramedics arrived 15 min later and provided advanced life support. Return of spontaneous circulation (ROSC) was achieved after 10 min. The initial rhythm was asystole, with a no-flow time of 15 min and a low-flow time of 10 min. She was intubated, ventilated, and stabilized with epinephrine. An electrocardiogram showed sinus tachycardia without signs of acute coronary syndrome. A CT scan ruled out intracranial hemorrhage and pulmonary embolism, but it revealed a large necrotic mass near the adnexa with ascites (Figure 1), hypodense liver lesions, and bilateral pleural effusions with lower lobe atelectasis.
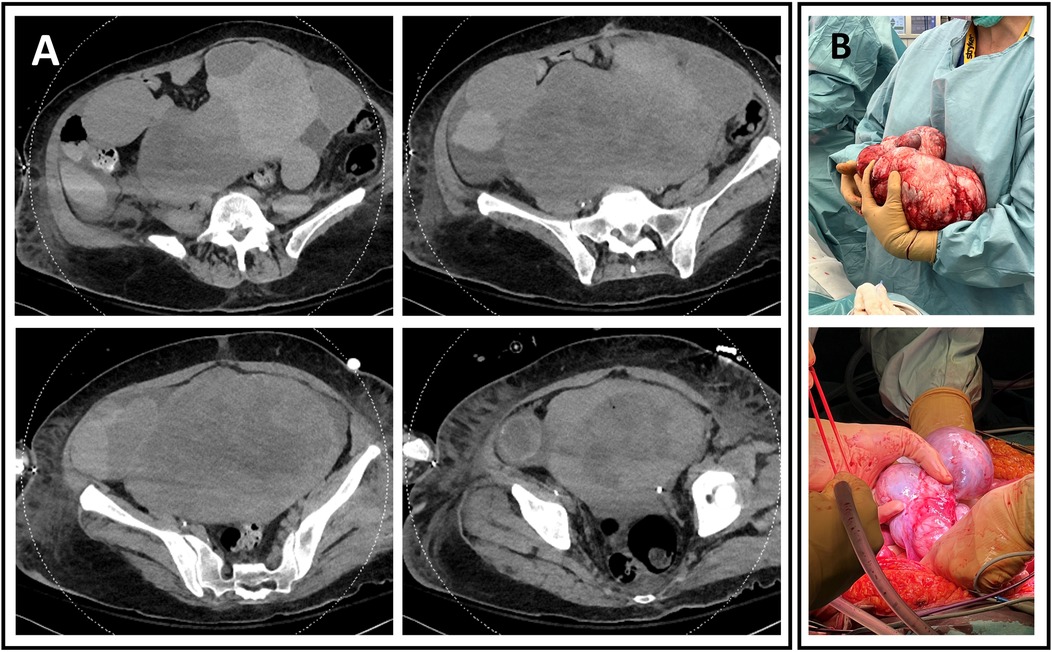
Figure 1. (A) Abdominal CT scan showing a large, heterogeneous, fleshy, and hypervascularized cystic mass measuring 27.2 cm wide, 14.1 cm deep, and 21.7 cm high. (B) Perioperative excision of two large multiloculated cystic masses. (Top) Left mass, weighing 2,932 g, measuring 27 cm × 20 cm × 20 cm. (Bottom) Right mass, weighing 436 g and measuring 15 cm × 8 cm × 5 cm.
Sedation was stopped early, but the patient remained comatose even after 72 h. Neurological prognostication revealed a poor prognosis: absent brainstem reflexes (corneal, oculocephalic, and cough), a highly malignant EEG, absent somatosensory evoked potentials, elevated neuron-specific enolase (162.8 µg/L), and diffuse anoxic lesions on brain MRI.
With family consent, therapeutic withdrawal was planned. Organ donation was considered, despite the adnexal mass. The levels of cancer antigen 19-9 (CA 19-9), cancer antigen 125 (CA 125), and carcinoembryonic antigen (CEA) were 10 kU/L, 537 kU/L, and 1.6 μg/L, respectively. The cytology of the pleural and ascitic fluids showed no malignancy. A percutaneous biopsy under ultrasound guidance revealed spindle cell proliferation in fibrocollagenous stroma without significant atypia (Figure 2). The liver was deemed unsuitable for transplantation due to hepatomegaly and heterogeneous hepatic lesions on imaging, raising concerns of an underlying pathology. A DCD heart was not offered, as DCD heart retrieval under A-NRP was not being performed in our center at that time. The lungs were not accepted for transplantation due to pneumonia, radiological infiltrates, and poor gas exchange on blood gases. Kidney function was preserved, and both kidneys were proposed for transplantation; however, acceptance was contingent upon prior resection and histological confirmation of the mass.
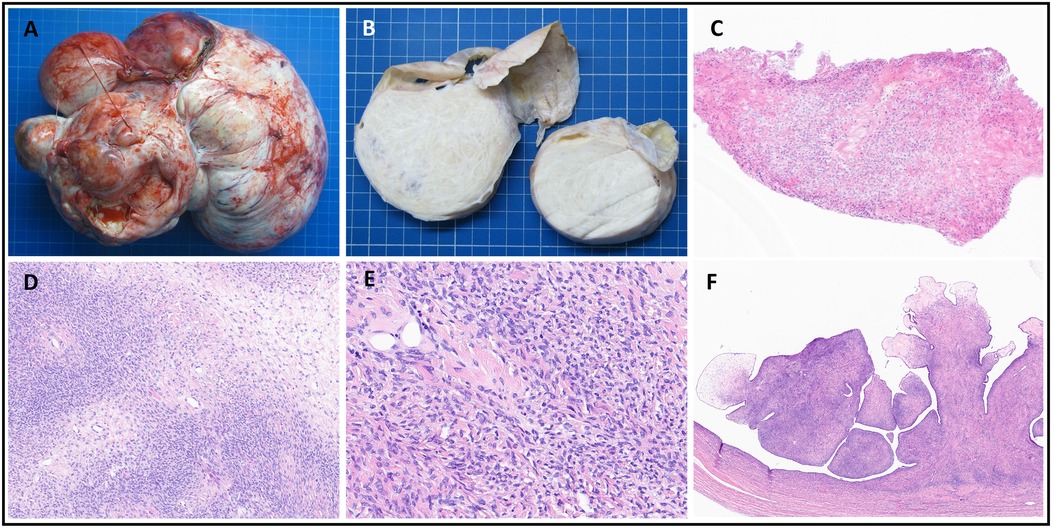
Figure 2. Pathology findings. (A,B) Gross findings of the left ovarian mass: a multiloculated cystic tumor (measuring 27 cm × 20 cm × 20 cm) with well-circumscribed, pale yellow fascicular areas. (C) Frozen section showing spindle cell proliferation without atypia (H&E, ×100). (D,E) Histology confirming ovarian thecoma with uniform spindle cells and collagen deposition (H&E, ×100–240). (F) Serous cystadenofibroma with fibromatous papillae lined by a Fallopian tube–like epithelium (H&E, ×240).
Following discussions with the Swiss transplant and surgical teams, a DCD-A-NRP procedure with mass excision and immediate analysis was agreed upon. A schematic pathway summarizing the clinical decision-making process from incidental mass discovery to final organ procurement, including the detailed chronological sequence of withdrawal, NRP, surgery, pathology, and kidney retrieval, is shown in Figure 3. Femoro-femoral cannulation for NRP and placement of the aortic occlusion balloon were feasible despite the pelvic mass and were performed under combined ultrasound and fluoroscopic guidance, without technical difficulty. During A-NRP, blood flow was maintained between 3.5 and 4 L/min at FiO2 50%. No transfusion was required. Donor management included the infusion of 3 L of 0.9% NaCl and 1 100 mL vial of 8.4% sodium bicarbonate to maintain hemodynamic and metabolic stability. Lactate levels decreased (9.3 → 3.6 mmol/L), Aspartate Aminotransferase (AST)/Alanine Aminotransferase (ALT) levels remained stable (48/31 → 43/25 UI/L), and pH normalized, supporting good organ quality. Bilateral oophorectomy was performed under A-NRP, and the frozen section excluded malignancy, with the final pathology confirming an ovarian thecoma. Only the left kidney was successfully transplanted, as the right kidney could not be used due to an acute infection in the intended recipient. The recipient of the left kidney experienced immediate graft function, with urine output of 1,600 mL/24 h, and regained stable renal function at 1 month.
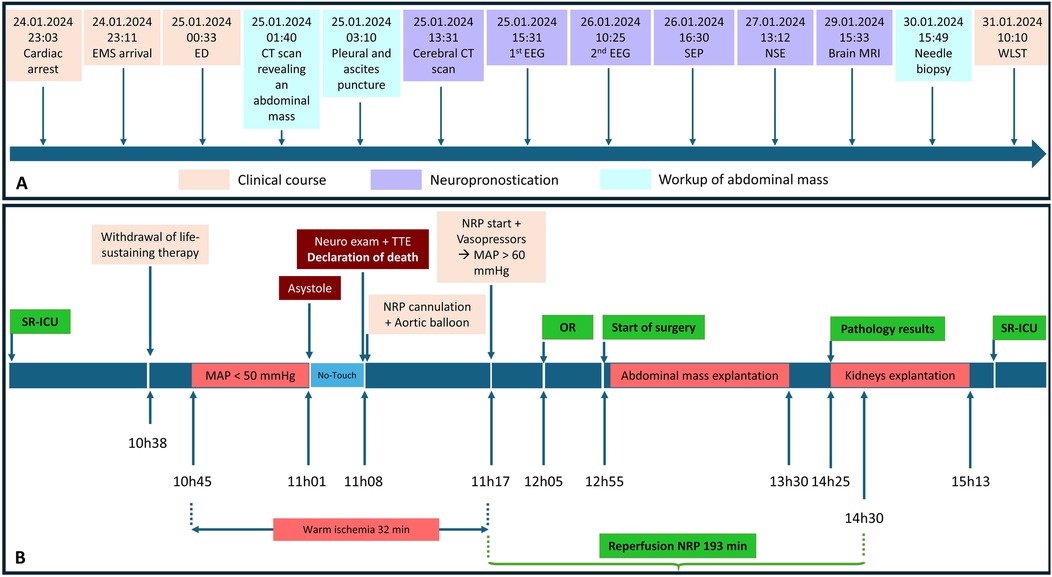
Figure 3. Chronological timeline of donor management, investigations, A-NRP, and surgical procedures. (A) Sequence from cardiac arrest, EMS arrival, emergency department admission, diagnostic workup of the abdominal mass (CT scan, pleural/ascites puncture, and needle biopsy), and neuroprognostication (EEG, SEP, NSE, and MRI) until WLST. (B) Controlled DCD process with abdominal NRP, showing withdrawal of therapy, decrease in arterial pressure (MAP <50 mmHg), circulatory arrest (asystole), declaration of death with neurological examination and TTE, cannulation and balloon placement, NRP initiation and hemodynamic stabilization, start of surgery (OR), excision of the adnexal mass, pathology results, and kidney procurement. ICU, intensive care unit; EMS, emergency medical service; ED, emergency department; CT, computed tomography; EEG, electroencephalogram; SEP, somatosensory evoked potentials; NSE, neuron-specific enolase; MRI, magnetic resonance imaging; WLST, withdrawal of life-sustaining therapy; MAP, mean arterial pressure; NRP, normothermic regional perfusion; OR, operating room; Neuro, neurological; TTE, transthoracic echocardiography; SR-ICU, single-occupancy ICU room.
Discussion
Cancer transmission from deceased donors is rare but potentially fatal (2). Donor cancer acceptance varies depending on recipient characteristics, the expected survival, and cancer type or stage. Despite its rarity, donor-transmitted cancer is difficult to quantify because of reporting bias and limited donor histories (3). Therefore, all donors undergo extensive screening through a review of medical and social history, a physical examination, imaging, and blood tests to exclude contraindications to donation.
Tumor markers CA19-9, CA 125, and CEA are associated with tumor burden and assist in differentiating benign from malignant ovarian masses 6. In our patient, CA 19-9 and CEA levels were low, while CA 125 was elevated. High CA 125 levels are most strongly linked with borderline or malignant tumors, followed by CA 19-9 and CEA 7-9. Moss et al. found that 80% of elevated CA 125 cases were not linked to cancer (4), prompting further investigation in our case. However, CA 125 can also be elevated in benign gynecological or inflammatory conditions, leading to false positives and potential unnecessary donor exclusion. In our donor, this marker profile alone was insufficient to rule out malignancy and was therefore combined with imaging, cytology, and biopsy results. Ultimately, definitive histology under A-NRP was required to safely exclude malignancy before proceeding with organ procurement.
Ovarian aspiration and biopsy can aid diagnosis, but sensitivity is low, and there is a risk of peritoneal tumor spread (5). In our patient, the frozen section showed a bland spindle cell pattern. Because of the size and bilaterality of the tumor, a bilateral oophorectomy was required to exclude malignancy. However, minimizing warm ischemia is vital to preserving graft function.
A-NRP permits oxygenated blood perfusion after death is declared (6). Compared with SRR, A-NRP is safe and improves early transplant outcomes by reducing delayed graft function in DCD kidneys (7, 8). In our patient, A-NRP enabled mass excision and real-time exclusion of malignancy while preserving perfusion, ultimately allowing organ procurement and transplantation. Beyond this patient case, A-NRP may also be valuable for donors presenting with other incidental findings, such as pulmonary or hepatic nodules, where biopsy and rapid pathological assessment could guide procurement decisions. In addition, A-NRP offers additional time for donors with complex surgical histories (e.g., multiple abdominal surgeries or adhesions), who require careful dissection or vascular reconstruction. Such applications could help avoid unnecessary donor exclusion and contribute to expanding the donor pool in centers equipped with A-NRP expertise. Recent experiences from Spain, the United Kingdom, and the United States further support the safety and effectiveness of A-NRP in expanding donor utilization and improving transplant outcomes (7–9).
Conclusion
In DCD donors with an abdominal mass of uncertain origin, A-NRP enables concurrent organ perfusion and malignancy exclusion, facilitating safe and timely organ procurement and transplantation.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent for publication of this case report was obtained from the patient's legal representative/healthcare proxy.
Author contributions
BA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. TO: Resources, Validation, Visualization, Writing – review & editing. A-LR: Formal analysis, Resources, Supervision, Validation, Visualization, Writing – review & editing. PC: Supervision, Validation, Visualization, Writing – review & editing. C-HW: Validation, Visualization, Writing – review & editing. HQ: Validation, Visualization, Writing – review & editing. KB: Conceptualization, Formal analysis, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. FI: Supervision, Validation, Visualization, Writing – review & editing. RG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence, and reasonable efforts have been made to ensure accuracy, including review by the authors, wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Immer FF. Organ donation after circulatory death in Switzerland: slow but constant progress. Swiss Med Wkly. (2015) 145:w14062. doi: 10.4414/smw.2015.14062
2. Lim WH, Au E, Teixeira-Pinto A, Ooi E, Opdam H, Chapman J, et al. Donors with a prior history of cancer: factors of non-utilization of kidneys for transplantation. Transpl Int. (2023) 36:11883. doi: 10.3389/ti.2023.11883
3. Xiao D, Craig JC, Chapman JR, Dominguez-Gil B, Tong A, Wong G. Donor cancer transmission in kidney transplantation: a systematic review. Am J Transplant. (2013) 13(10):2645–52. doi: 10.1111/ajt.12430
4. Moss EL, Hollingworth J, Reynolds TM. The role of CA125 in clinical practice. J Clin Pathol. (2005) 58(3):308–12. doi: 10.1136/jcp.2004.018077 PMCID: PMC177059015735166
5. Nagamine K, Kondo J, Kaneshiro R, Tauchi-Nishi P, Terada K. Ovarian needle aspiration in the diagnosis and management of ovarian masses. J Gynecol Oncol. (2017) 28(4):e40. doi: 10.3802/jgo.2017.28.e40
6. De Carlis R, Centonze L, Migliorini M, Pitoni L, Cerchione R, Lauterio A, et al. Abdominal normothermic regional perfusion in donation after circulatory death: organ viability or organ preservation? Eur J Transplant. (2023) 1(2):113–20. doi: 10.57603/EJT-013
7. Padilla M, Coll E, Fernández-Pérez C, Pont T, Ruiz Á, Pérez-Redondo M, et al. Improved short-term outcomes of kidney transplants in controlled donation after the circulatory determination of death with the use of normothermic regional perfusion. Am J Transplant. (2021) 21(11):3618–28. doi: 10.1111/ajt.16622
8. Pearson R, Geddes C, Mark P, Clancy M, Asher J. Transplantation of kidneys after normothermic perfusion: a single center experience. Clin Transplant. (2021) 35(10):e14431. doi: 10.1111/ctr.14431
9. Merani S, Urban M, Westphal SG, Dong J, Miles CD, Maskin A, et al. Improved early post-transplant outcomes and organ use in kidney transplant using normothermic regional perfusion for donation after circulatory death: national experience in the US. J Am Coll Surg. (2024) 238(1):107–18. doi: 10.1097/XCS.0000000000000880
Keywords: normothermic regional perfusion, pathological diagnosis, organ procurement, organ transplantation, ovarian serous cystadenofibroma, thecoma
Citation: Assouline B, Olivier T, Rougemont A-L, Compagnon P, Wassmer C-H, Quintard H, Bendjelid K, Immer F and Giraud R (2025) Case Report: Organ procurement in a DCD donor with ovarian thecoma: abdominal NRP enabled timely and safe resection, pathological confirmation, and successful kidney transplantation. Front. Transplant. 4:1680491. doi: 10.3389/frtra.2025.1680491
Received: 6 August 2025; Accepted: 9 September 2025;
Published: 2 October 2025.
Edited by:
Gennaro Selvaggi, University of Miami, United StatesReviewed by:
Paolo De Simone, University of Pisa, ItalyVighnesh Vetrivel Venkatasamy, University of Miami, United States
Copyright: © 2025 Assouline, Olivier, Rougemont, Compagnon, Wassmer, Quintard, Bendjelid, Immer and Giraud. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raphaël Giraud, cmFwaGFlbC5naXJhdWRAaHVnLmNo