 Masautso Joseph Chimombo
Masautso Joseph Chimombo- 1Graduate School of Global Environmental Studies, Sophia University, Tokyo, Japan
- 2Extension Department, Lilongwe University of Agriculture and Natural Resources (LUANAR), Lilongwe, Malawi
Introduction: Most studies on water justice and rural–urban divide in drinking water services coverage have been done at national scale. Such nationwide studies often mask injustices and differences happening at the sub-national and community levels.
Methods: Employing infrastructure violence as a theoretical framework and a mixed methods case study design, the study was carried out in Lilongwe to assess the extent of injustices in drinking water coverage and drinking water service levels in Lilongwe in Malawi. Service coverage was assessed on access, affordability, and reliability.
Results and discussion: The study reveals that disparities between Lilongwe urban and Lilongwe rural in drinking water coverage and service levels are wider than nationwide studies reveal. Lilongwe urban households have higher access to safe drinking water than rural households. Rural residents suffer the most from the pain of infrastructure violence caused by their exclusion from the centralised piped water infrastructure network. Therefore, deliberate interventions to improve drinking water services in rural areas of Malawi are critically needed. Investing in affordable and easy to manage sustainable water supply systems like solar powered water pumping systems and rainwater harvesting can go a long way in moving rural communities up the water service ladder. Further, empowering rural communities with finances and skills for repairing boreholes can reduce the proportion of boreholes which are nonfunctional which currently stands at 30%.
1 Introduction
Good health, quality of life, and human dignity are all crucially dependent on access to clean and potable drinking water (He et al., 2018). The risk of suffering life-threatening waterborne morbidities like cholera and diarrhea is significantly reduced if people have, at all times, access to safe drinking water (Adelodun et al., 2021). No wonder, recognizing the indispensability of water to human existence, the United Nations in 2010 declared that “The right to safe and clean drinking water is a human right that is essential for the full enjoyment of life and all human rights” (UN, 2010). The declaration of human right to water perhaps explains why the United Nations has included universal water access as one of the key goals under the global Sustainable Development Goals (SDGs). Specifically, SDG 6.1 aims to achieve equitable and sustainable universal access to safe and affordable drinking water (WHO and UNICEF, 2017). SDG 6.1 emphasizes “equitable” and “for all” in its framing. This framing is in line with the overarching philosophy behind the global agenda 2030 on which SDGs are anchored which is “Leaving no one behind.” This philosophy highlights the commitment of global leaders to achieve inclusive sustainable development (WHO and UNICEF, 2017). Malawi as a member of the UN is party to both SDG 6.1 and the right to water and is therefore under obligation to ensure that everyone in Malawi has continuous access to safe drinking water.
As desirable as it is that water must be enjoyed by all human beings without discrimination, injustices and inequities exist across the world in the provision of drinking water services. Studies show that the right to water is not being enjoyed equally. According to the joint monitoring program (JMP) by WHO and UNICEF, of the 771 million people in the world that had no access to basic drinking water in 2021, 50% were from sub-Saharan Africa alone (WHO and UNICEF, 2021). Without access to basic drinking water services, a larger proportion of the population in sub-Saharan Africa resorts to unsafe water sources like rivers, swamps, and unprotected wells (Matamanda et al., 2020). By accessing drinking water from unsafe sources, a lot of people in the region get exposed to life-threatening water-borne diseases like cholera and diarrhoea (Sultana, 2018; Chaudhuri and Roy, 2017). For example, it is reported that, in the developing countries, every year diarrhoeal alone claims lives of over 1.8 million people (Dattani et al., 2023; WHO, 2020). Even within Africa, intra-country injustices in drinking water services provision have been reported. Aydamo et al. (2023) provide such a case from Southern Ethiopia where their study found that high-income earners had more access to piped water compared to low-income earners. Similarly, in Kenya, a study by Othoo et al. (2020) showed that majority of residents living in informal and unplanned locations and urban slums walked longer distances to fetch water relative to their counterparts living in planned and rich neighborhoods. In West Africa, in a study that was conducted in Ghana, Akurugu et al. (2020) found that due to high levels of poverty, the country’s Northern region has the lowest drinking water service coverage. These findings demonstrate how uneven water services provisions are.
Despite, as a member of the UN, being party to both SDG 6.1 and the human right to water, nationwide studies (i.e., demographic and health surveys, multiple indicator cluster surveys, and integrated household surveys) conducted in Malawi reveal a persistence existence of inequalities and iniquities in access to safe drinking water. More pronounced of these water injustices is the wider disparities in access to drinking water between rural and urban areas. For instance, Akpabio et al. (2021) show that rural areas in Malawi lag far behind urban areas in coverage of improved drinking water at 63 and 87%, respectively. The integrated household survey results show that while 93.1% of urban population has access to improved water services, only 85.7% of the rural population has access to this level of water services (National Statistical Office, 2017b). Relatedly, the Malawi demographic and health survey results also showed that as of 2016, 15% of the rural population compared to only 2% of the urban population were accessing their drinking water from unimproved and unsafe sources which includes rivers and streams (National Statistical Office, 2017b). Such rural–urban disparities in access to safe drinking water have negative consequences on health and education outcomes among the rural population of Malawi. For instance, a study conducted in the rural areas of Balaka in Malawi showed that 50% of all disease burden were water borne diseases (Mkwate et al., 2017). Further, Kayser (2015) and Manda et al. (2016) report that, due to overreliance on unsafe drinking water, there are high incidences of waterborne diseases in the rural areas of Malawi. In the rural education sector in Malawi, lack of access to drinking water and longer walking distance have been singled out for contributing to high levels of absenteeism among learners in primary and secondary schools (UNICEF, 2020). Clearly, no meaningful development can take place in rural Malawi when most of its populace are made less economically productive due to frequent illnesses from waterborne diseases. With children being kept away from school due to limited access to drinking water, the future of rural development in Malawi is not only undermined but also threatened and compromised. This is because educated and skilled human capital is one of the prerequisites for sustained rural development.
Still in Malawi, previous studies have been conducted focusing on disparities in drinking water services provision. The 2016–2017 nation-wide integrated household survey revealed that while only 11% of the population that has zero years of schooling has access to safe drinking water compared to 38.5 and 30.6% of the population that completed secondary education and tertiary education, respectively (National Statistical Office, 2017b), indicating that drinking water provision services are favorably tilted towards the highly educated. Focusing on intra-urban inequalities, Rusca et al. (2017) applied urban political ecology approach to understand how social and political relations produce uneven waterscape in drinking water quality between low-income slum locations and high-income plush location in Lilongwe City. Similarly, Adams and Smiley (2018) investigated if access to improved water services in Malawi guarantees access to reliable safe drinking water for the urban poor in Malawi’s four cities of Blantyre, Zomba, Mzuzu, and Lilongwe. In the same vein, Tiwale et al. (2018) applied socio-ecological framework in examining how financial investments by the Malawi Government and the state-owned water utilities are biased towards funding the extension and expanding of piped water infrastructure to planned residential locations where the city’s government and business bureaucrats and political elites live. Further, Rusca et al. (2017) empirically assessed how the principle of full cost recovery in pricing of piped drinking water which international donors demand entrenches drinking water inequalities that disadvantage the urban poor. Cassivi et al. (2018) took a unique approach by focusing on trends analysis of progress towards eliminating drinking water inequalities between rural and urban areas in Malawi, making use of data from Demographic Health Survey (DHS) and Multiple Indicator Cluster Survey (MICS) covering a 25-year period from 1992 to 2017. In addition, in 2016, Adams and Smiley (2018) conducted a subnational study which revealed that the gap between rural and urban areas is wider than national level studies show. Their study compared access to water between rural areas in Lilongwe and peri-urban areas in Lilongwe City. The results exposed a wider gap of 36% as it found that 91% of peri-urban households had access to improved drinking water compared to only 54% of rural households. National level studies conducted around the same time by the National Statistics Office reported a rather narrow gap of 8.6% as it found that 93.1 and 85.7% of urban and rural households, respectively, had access to improved drinking water.
The review of previous studies presented above reveal that the theme of intra-urban inequalities in drinking water access has been extensively studied in Malawi. However, rural–urban inequalities in access to drinking water has not received adequate attention from scholars as evidenced by its being heavily underexplored. Further to that, with exception of Adams and Smiley (2018), to the best of my knowledge nearly all the previous studies on rural–urban divide in access to drinking water in Malawi have been national-level. These studies are undertaken periodically by the National Statistics office. They include the demographic and health survey (see for example National Statistics Office, 2017a), Malawi multiple cluster indicator surveys (MICS) (see for example National Statistical Office, 2021), and integrated household surveys (see for example National Statistical Office, 2017b). The strength of such national-wide studies is that their findings can easily be generalized to represent the whole country (Johnson et al., 2014). However, national-wide studies have several consequential limitations that necessitate local-level studies at subnational or community levels. According to Sung and Liaw (2020), such studies fail to capture detailed nuances and complexities happening at the local level. Further, Rodrigues-Silveira (2019) and points out that national level studies that evaluate policies and service delivery have often been found to be less reliable in unearthing and bringing to the attention of policymakers iniquities occurring at sub-national and community levels, a situation which results in no action being taken to solve inefficiencies and injustices peculiar and unique to specific community contexts. In sharp contrast, community-level or district-level studies have proven to be effective in providing comprehensive nuances and in explaining the complexities of factors and causes of issues under investigation at the local level (Sung and Liaw, 2020). Writing on environmental justice studies, Borderon et al. (2021) warns that studies conducted at national level, while necessary, have the greatest risk to “invisibilize” issues in drinking water service provision that affect small communities. Similarly, Karasaki et al. (2023) makes a strong case for more subnational and community level case studies to investigate issues of environmental justice in the drinking water spaces, pointing out that such studies collect data that “surface on-the-ground as well as perceived injustices closest to communities” (p. 4).
The aim of the study is to examine the rural–urban divide in drinking water service coverage and service levels in Lilongwe in Malawi. Specifically, the study interrogates the extent, nature, and impacts of inequalities and iniquities in drinking water service coverage and service levels between Lilongwe rural and Lilongwe urban. Drinking water service coverage has been examined on three main dimensions of access, reliability, and affordability. The quality dimension has only been partially assessed using qualitative proxy indicators of perceived color, taste, and odor. Informed by infrastructure violence as a theoretical framework, the study employed mixed-methods research design. Unlike previous studies cited above, this study makes explicit use of water justice framework and the concept of infrastructure violence in analysing rural–urban divide in drinking water access. This paper also departs from the use of national level data and makes use of primary data collected at subnational level.
1.1 Infrastructure violence
The term infrastructural violence was coined by Rodgers and O’Neill (2012). It refers to the deleterious effects, both direct and indirect, that infrastructures can have on human societies. The concept explores how infrastructures create and reproduce social inequalities, injustices, and marginalization in urban spaces (Rodgers and O’Neill, 2012). In other words, infrastructure violence refers to the processes through which planning, governance, and decision-making are designed and made in such a way that provision of infrastructures favor and prioritize the interests and needs of the rich and powerful in urban areas while at the same time ignoring the plight and suffering of the poor (Rodgers and O’Neill, 2012). Though mainly used in studying inequalities and injustices between social-economic groups within urban communities, the concept has now been extended to examining water justice issues in rural water provisioning systems (Stock, 2022). In theorizing and conceptualizing infrastructure violence, Rodgers and O’Neill (2012) identify two types of such violence: active infrastructure violence and passive infrastructure violence. By active infrastructure violence, they refer to situations in which infrastructure is intentionally designed to be violent to certain social groups of people. On the other hand, being excluded and omitted from infrastructure due to its technical limitations is what is referred to as passive infrastructure violence (Gandy, 2006; Ferguson, 1999). Passive infrastructure violence is the focus of this study, and its application is useful in providing a nuanced understanding of the sufferings and consequences that people experience due to their being excluded from piped water infrastructures.
Infrastructure violence has its roots in water justice. Put simply, water justice is about ensuring equity in access to drinking water. According to McLean (2007), water justice is a subset of broader environmental justice and has unfair distribution of and an uneven access to drinking water as its major concern. As Sultana (2018) unequivocally declares, there is water injustice if drinking water service provision is characterized by unfairness, inequalities, and inequities. However, other scholars led by Young (1994) believe that water justice and equity are nothing but mere utopia which can never be attained in real life. Young (1994) through his influential book Equity: In Theory and Practice, takes a very extreme stand by opining that equity does not exist and that it is effort in vain to try to achieve it. Young gives three main reasons that justify his stand which are the fact that equity and justice as concepts have no intrinsic meaning of their own and therefore fail to exist; that on the basis of the former reason, the two concepts are totally and hopelessly subjective because there are no scientific methods that can measure them; and finally, that equity and justice have no sensible theory that explains them. Other critics who believe in the proportionality of benefits perspective of water justice argue that communities should benefit from drinking water in proportion to their contribution to its infrastructure installation and supply (Neal et al., 2014). Such a view is somewhat antagonistic to goal of equalizing and universalizing access to drinking water. Regardless of the somewhat conflicting views on what constitutes water justice and equity, principle number 4 of human right to water which is equality and non-discrimination, places solemn duty on every member state of the United Nations to ensure that everyone has access to safe drinking water regardless of one’s contribution. Therefore, there is no water justice if there is no universal access to safe drinking water.
2 Data and methods
2.1 Study location
The study was conducted in Lilongwe in Malawi. Lilongwe City is the capital of Malawi. Lilongwe is divided into two: Lilongwe urban with a total area of 393km2 and Lilongwe rural which has a total area of 5,755 km2. It lies on flat plain with an elevation of between 1,000 and 1,200 meters above sea level. The city lies on a latitude of 13.59 South and longitude of 33.47 East. Lilongwe is the biggest city in Malawi in terms of size and population. Based on population census projections by the National Statistical Office (2021), at the end of 2024 Lilongwe urban had a population of 1,333,000 while Lilongwe rural had a population of 2,200,000. Though piped drinking water is the main source of drinking water in Lilongwe urban, handpump boreholes and unprotected wells serve a significant proportion of the urban poor living the city’s unplanned settlements (Rusca et al., 2017). For rural areas in Lilongwe, majority are served by handpump boreholes and unprotected wells (Adams and Smiley, 2018).
Informal housing, overreliance on informal precarious employment, and living in high-density locations characterize a typical urban household in Malawi (UN, 2010). For this reason, three high-density residential locations based in Lilongwe City were selected as the urban sample for the study. These three locations are Kawale 2, Area 36, and Chinsapo. Households living in these high-density locations are representative of a typical urban household in Malawi. Similarly, two locations in Lilongwe rural were also purposefully selected as study sites representing the rural communities. The two rural locations are villages surrounding two rural trading centers of Zamkutu and Nanjiri. Figure 1 below shows the study locations.
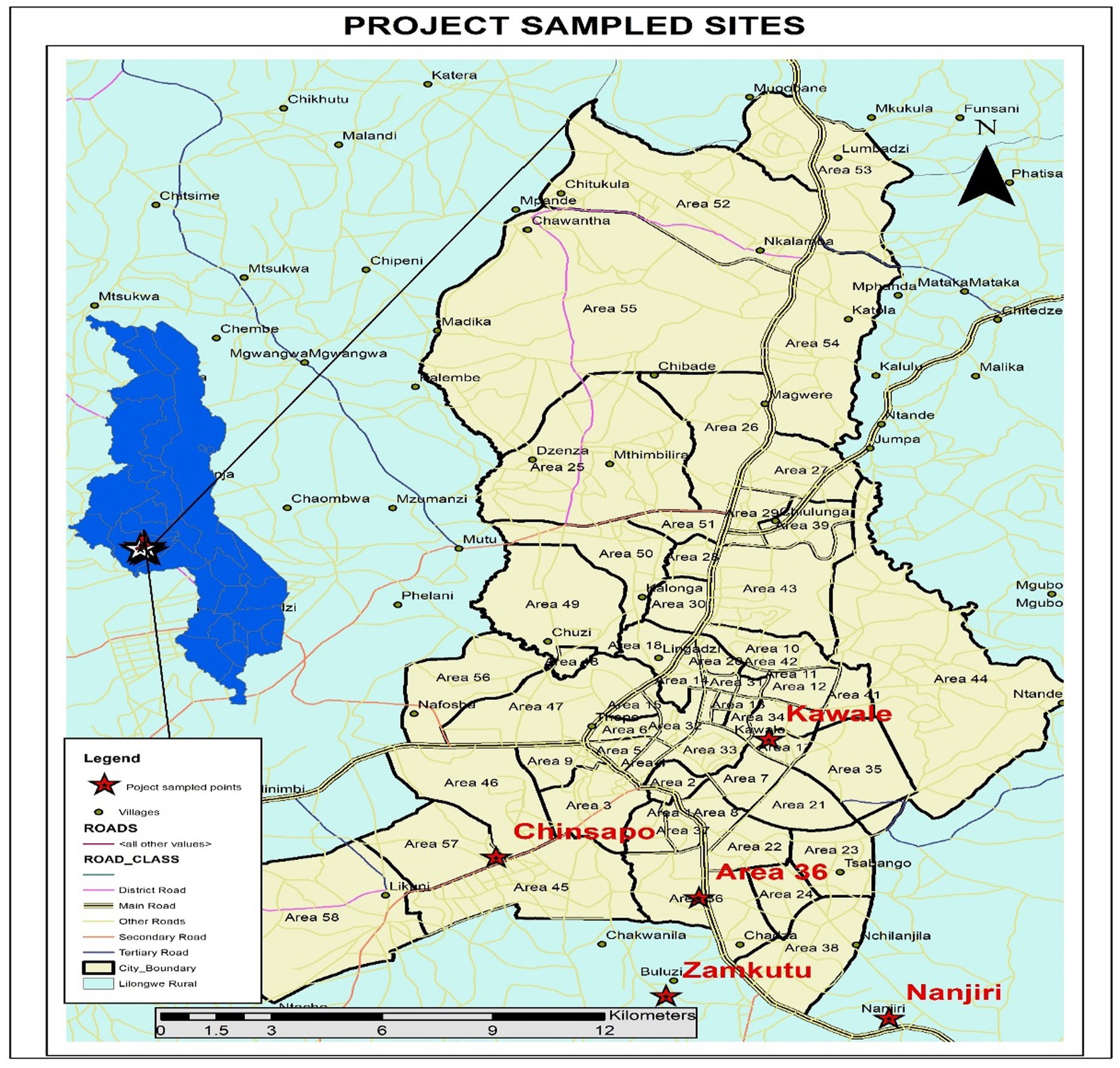
Figure 1. Study locations.
2.2 Research design and data collection and analysis
The study employed the case study mixed methods (CS-MM) research design. According to Guetterman and Fetters (2018), the “case study–mixed methods design as a research design that employs a ‘parent’ case study design and uses mixed methods by collecting, analysing, and integrating qualitative and quantitative data,” (p. 3). This was suitable for the study as the research questions required both qualitative and quantitative data to be answered (Guetterman and Fetters, 2018). Further, Morgan (2014) argues that mixed methods research is well suited to investigate social justice issues as it provides a flexible research framework that can address the concerns for critical realists about efficacy and the constructionist paradigm’s goal of eradicating social injustices in the world.
Fieldwork exercise took place between 3rd and 30th August 2024 in Lilongwe in Malawi. Quantitative data collection employed household survey using structured questionnaire, which was administered to either household head, spouse of household head or in their absence to any member of the household aged 18 and above (Bernard, 2017). Using systematic random sampling, the study collected quantitative data from 535 households comprising 262 households from Lilongwe urban and 273 households from Lilongwe rural. The sample size was determined following sample size calculation formula for cross sectional studies by Cochran (1977). The formula is as follows: where:
i. n is the desired sample size
ii. p is the proportion of the population that displays the attribute in question, in this case access to improved drinking water sources
iii. z is the z-value which is the level of confidence
iv. e is the margin of error which measures degree to which research results may differ with the real-world results.
Focus group discussions and key informant interviews were used in collecting qualitative data. Purposive sampling was used in the identification of FGD participants and key informants. Key informants included local chiefs, community leaders, government and NGO staff working in the water sector. Qualitative saturation point guided the number FGDs and KIIs that were conducted (Hennink et al., 2019; Morse, 1995). Further, by conducting 9 KIIs and 18 FGDs, the study exceeded the recommended minimum of 4–6 interviews for KIIs (Kostadinov et al., 2015) and 3–6 FGDs for FGDs (Krueger and Casey, 2015).
Qualitative data were analysed using qualitative content analysis (QCA). The QCA process followed the steps as recommended by Bengtsson (2016) and Wong (2008). Quantitative data was analysed using descriptive statistics and inferential statistics. To test if there were statistically significant disparities between or among subgroups in the sample, independent sample t-test and chi-square test of independence were conducted (p < 0.05). Furthermore, both binary and ordinal logistical regression analysis were run to test if household location (rural versus urban) predicted a household’s main water source, distance to main water source, affordability of drinking water, and position on the water service ladder based the WHO and UNICEF’s JMP metrics for SDG 6.1 (WHO and UNICEF, 2017). Figure 2 below shows the drinking water ladder which WHO and UNICEF use for their JMP.
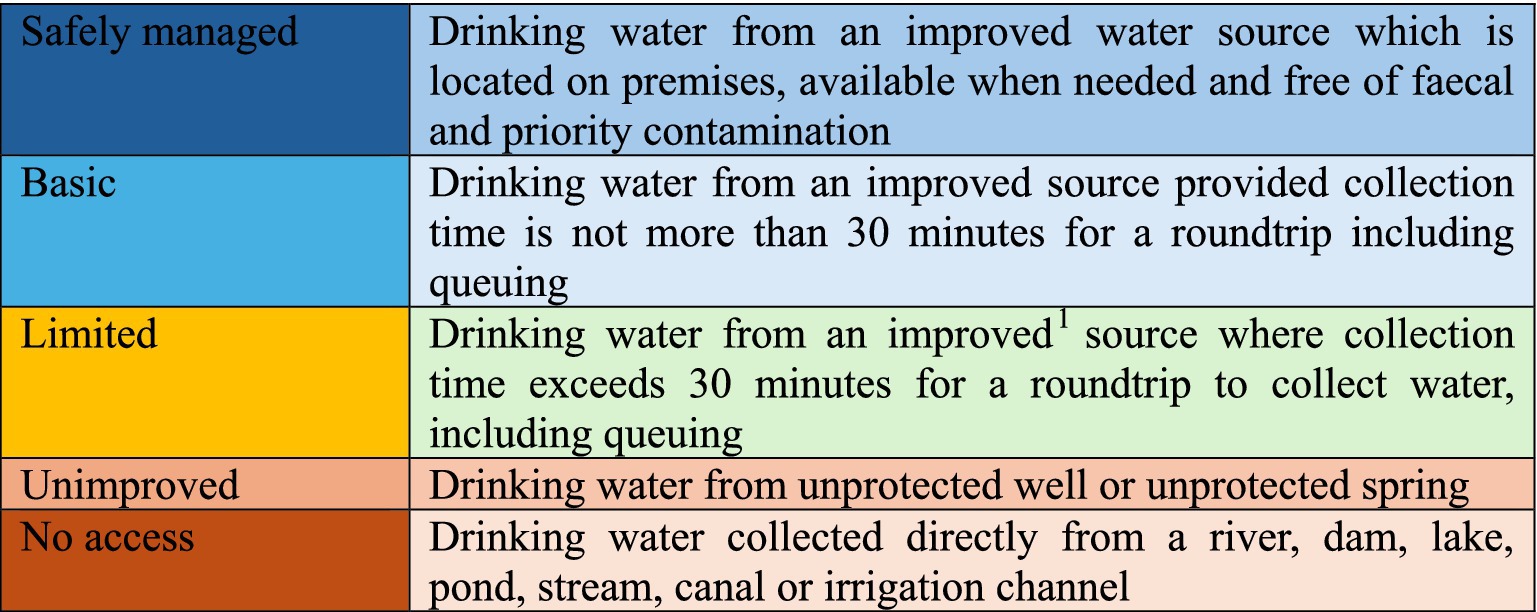
Figure 2. JMP drinking water service ladder under the SDG era (WHO and UNICEF, 2017).
3 Results
3.1 Social demographic characteristics of respondents
Table 1 provides a summary of socio-demographic characteristics of the respondents and sampled households. Out of the sample size of 535 households, 74.02% of the respondents were female while 25.98% were male. As expected of Malawi, which is largely a patriarchal society, most of the sampled households were male headed with 74.05 and 72.89% of households being male headed in Lilongwe urban and Lilongwe rural, respectively. The age distribution of the sample size is also reflective of Malawi’s demographic structure which is dominated by young people as at least 62% of the sample were composed of respondents in the age range of 18–35 years. As Table 1 also shows, there is a wide gap between rural and urban households in terms of average monthly income, which is K128,578 for the urban households and K36,260 for the rural households which are equivalent to US$74 and US$21, respectively, at the current (August 2024) exchange rate of US$1 to MK1,750. Household income is very important as it influences a household’s ability to meet the costs associated with accessing safe drinking water.
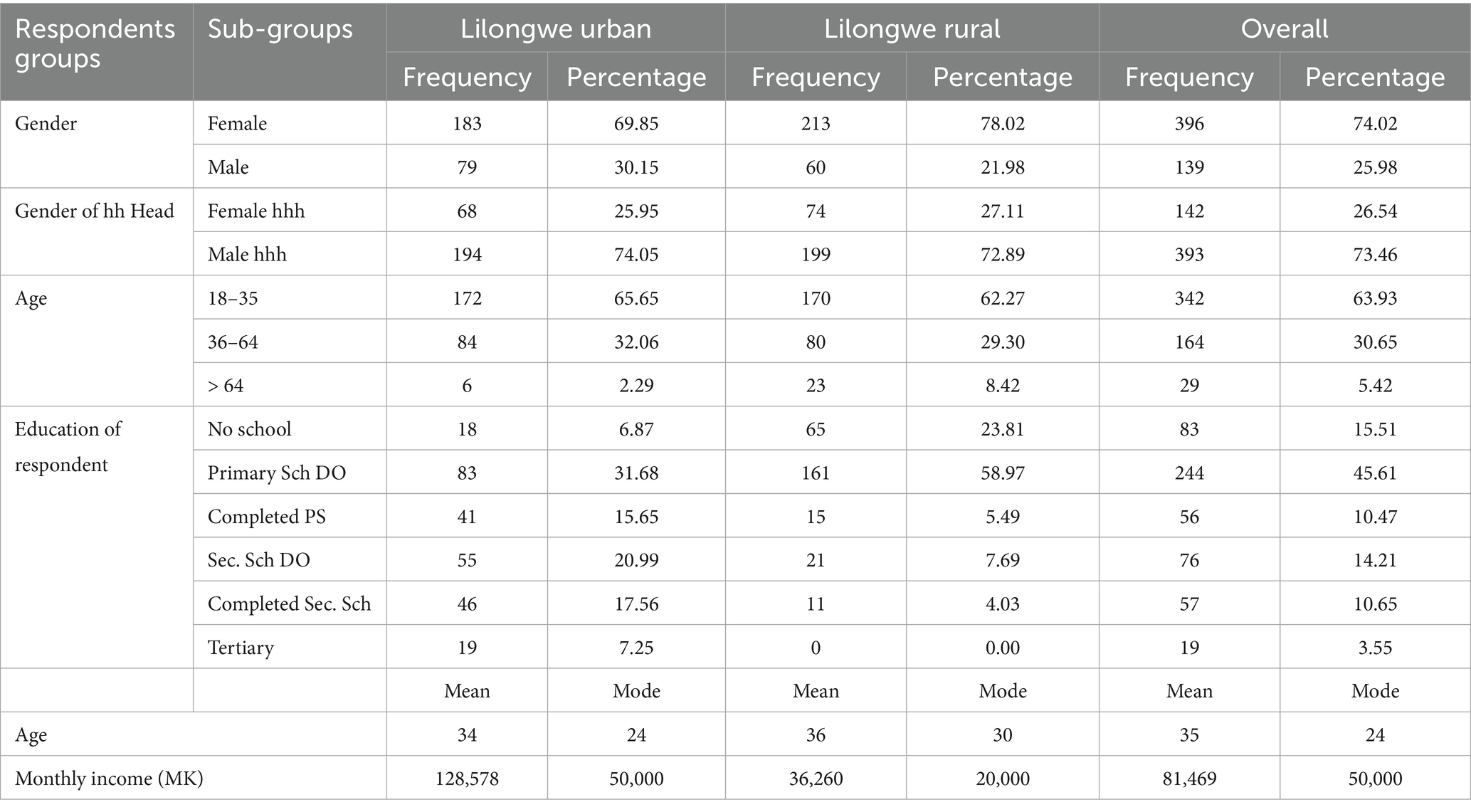
Table 1. Socio-demographic characteristics of the study participants.
3.2 Main sources of drinking water
Main source of drinking water is proxy indicator of water quality which people use. Results in Figure 2 below show clear disparities in main sources of drinking water for urban households and rural households in Lilongwe. While piped water (piped into dwelling + piped into yard/plot) is the main drinking water source for 3.66% of the households in Lilongwe rural, 90.08% of Lilongwe urban households reported piped water as their main source of drinking water. For the rural households, majority of them reported either borehole (54.58%) or open well (26.01%) as their main source of drinking water. While no urban household reported surface water as main source of drinking water, 2.56% of sampled households in Lilongwe rural depend on such source as their main water source. Accessing drinking water directly from rivers and dams poses serious health threats as such water is often unsafe. As shown by the chi-square test of independence in Table 2, the differences in household’s main source of drinking water between urban households and rural households in Lilongwe is statistically significant (p < 0.001). Results from FGDs and KIIs corroborate the quantitative results on the differential sources of drinking water between the two areas. Some key informants narrated:
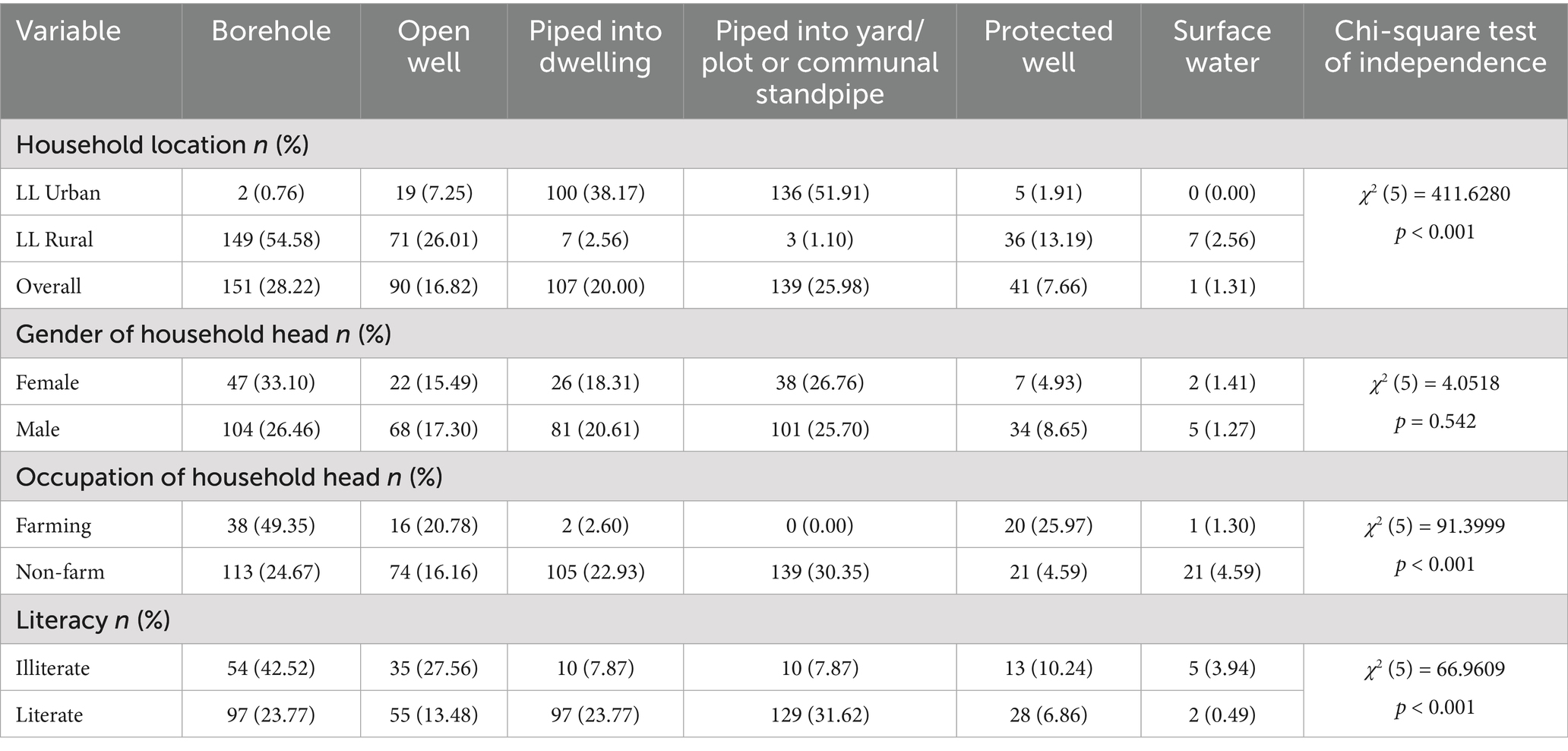
Table 2. Drinking water sources chi-square test of independence (n = 535).
Currently, urban areas have piped water, whereas rural areas mostly rely on boreholes. However, with Vision 2063 in place, we are working towards improving this situation. (KII with government official working in the water sector)
The truth is people in my area are really struggling. As for drinking water, most people use unprotected wells, and these wells are sparsely located. A few others use boreholes, but the boreholes are too few and can't cater to everyone. (KII with a traditional leader, Zamkutu area, Lilongwe rural)
Table 2 also reveals that there is an association between main occupation of head of household and the main source water for a household. Results show a wide gap between households whose household heads depend on farming as a main occupation and those who do not. For example, only 2.6% of farming households compared to 53.28% of non-farming households have piped water as their main source of drinking water. Moreover, while open/unprotected well is the main drinking water source for 20.78% of farming households, only 16.16% of non-farming households depends on this unprotected source. A chi-square test of independence confirms that the disparities in main drinking water sources between households whose head is mainly engaged in farming and those households whose head engage in non-farm activities as main source of livelihood is statistically significant (p < 0.001). The reliance on relatively inferior water sources by those households that depend on farming is not surprising given that in Malawi, farming occupation is strongly associated with low-income earnings (Benson and De-Weerdt, 2023). Low-income earnings prevent such farming households from accessing improved and better drinking water sources. Moreover, as has already been shown in Table 1, farming households are more likely to be based in the rural area (27.11%) where modern drinking water supply infrastructure is either limited or completely non-existent than urban areas (1.15%).
Previous studies show that literacy levels of people influence not only people’s behaviors, adoption of recommended health or agricultural technologies and practices but also access to resources and opportunities (Asadullah and Rahman, 2009; Fagerland and Hosmer, 2016). As Table 2 also shows, piped water is predominantly main source of drinking water for 42.52% of households whose head can read and write, yet it is a main source of drinking water for only 15.74% of those households whose head are neither able to read nor write. More households whose household heads are illiterate (27.56%) than literate (13.48%) rely on unprotected wells which pose high health risk to people (Figure 3).
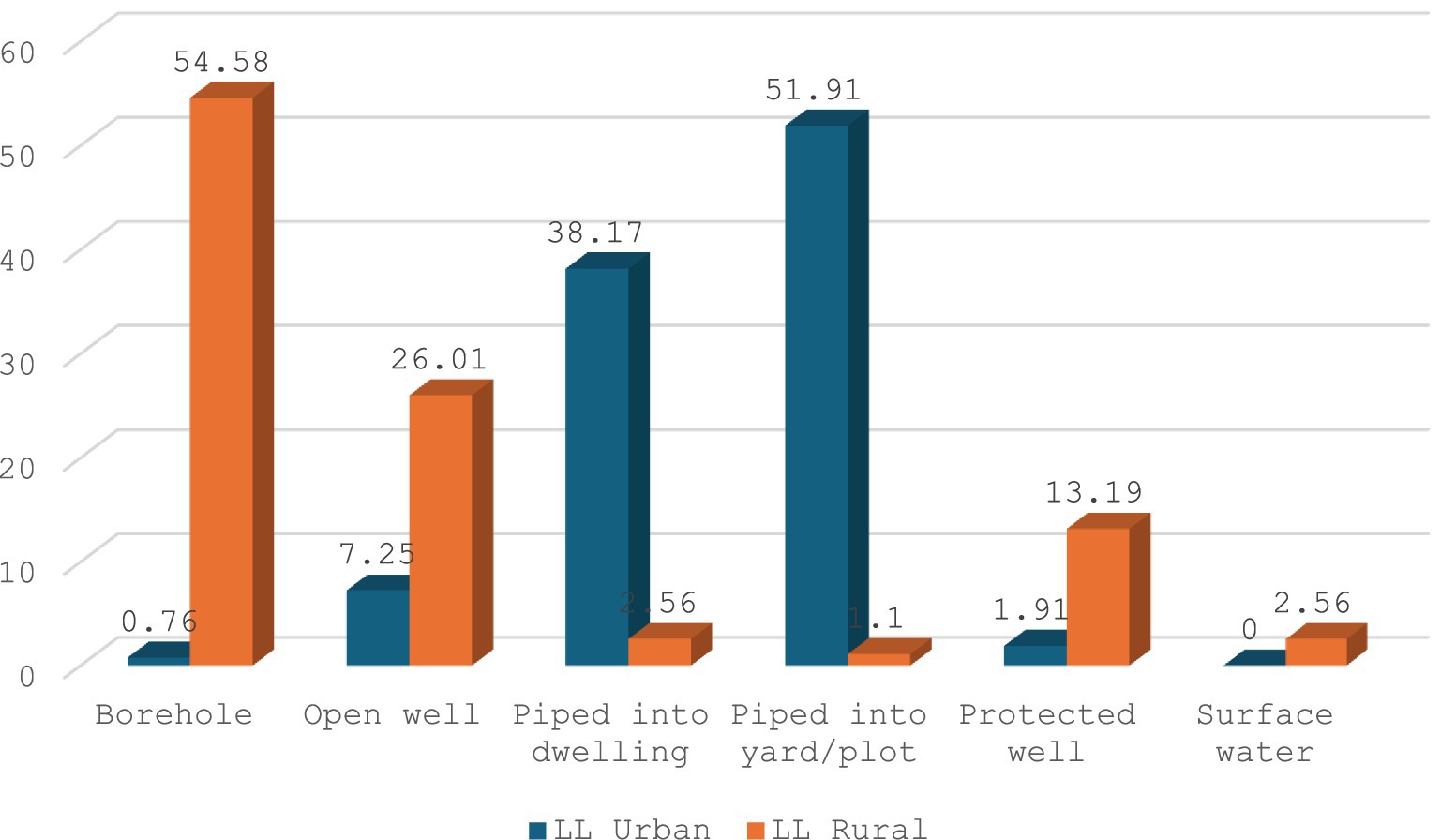
Figure 3. Main sources of drinking water.
3.3 Relative position on the water drinking ladder
According to WHO and UNICEF (2017), there are five drinking water service levels on the drinking water services ladder. These levels in ascending order are no access, unimproved access, limited access, basic services, and safely managed drinking water. The three levels of limited access, basic services, and safely managed access fall under the broad category of improved drinking water. Since it was not practically possible to conduct water tests on each sampled household, it was difficult to assess if drinking water from each household’s main drinking water source was free of faecal matter and other priority contamination. It is important to remember that no drinking water source can only be declared as safely managed after being tested and found to be free from faecal matter and priority contamination. Thus, which is also a limitation of this study, while the drinking water service ladder has five service levels, the study is only reporting on first four service levels.
Results in Figure 4 show that Lilongwe urban households occupy higher position on the drinking water services ladder. Nearly all Lilongwe urban households (90.08%) occupy highest position of basic services compared to only 53.11% of rural households. Table 3 shows disaggregated results by other social demographic factors. The results reveal that there are statistically significant differences between rural and urban areas in as far as their relative position on the drinking water service ladder is concerned [χ2 (3) = 90.8539; p < 0.001]. This implies that urban households are better off than rural households as majority of their households are at the top of the water service ladder. Further still, rural households’ disadvantaged position on the drinking water services ladder is laid bare by the fact the while no household from urban area was found to be on the no access level on the ladder, 2.2% of Lilongwe rural households occupy this position, implying that they access drinking water directly from rivers, lakes, streams and dams. No wonder, as will be seen in the subsequent sections, rural households in Lilongwe decried the high cholera and diarrhea incidences in their communities.
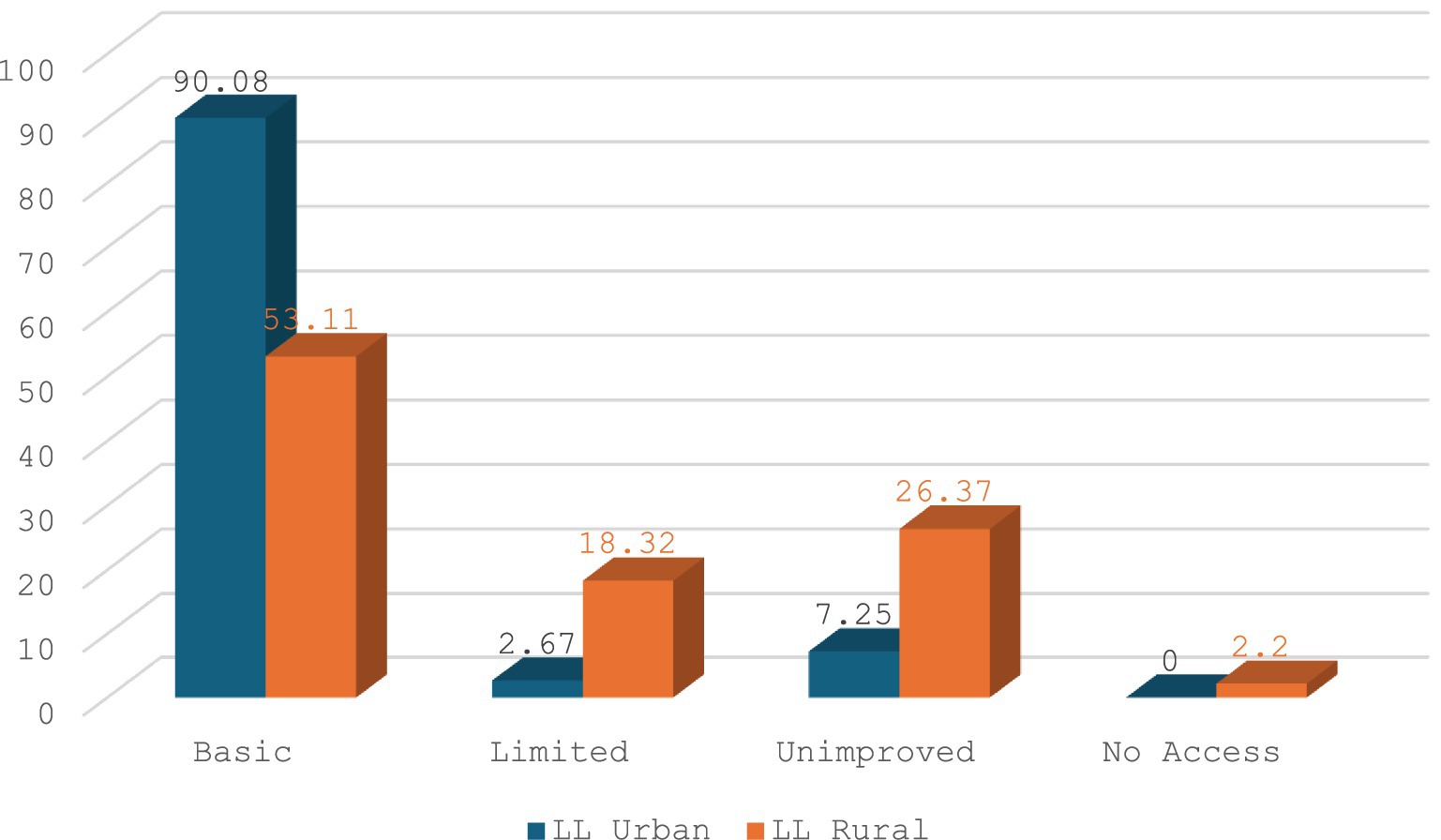
Figure 4. Position on drinking water service ladder.
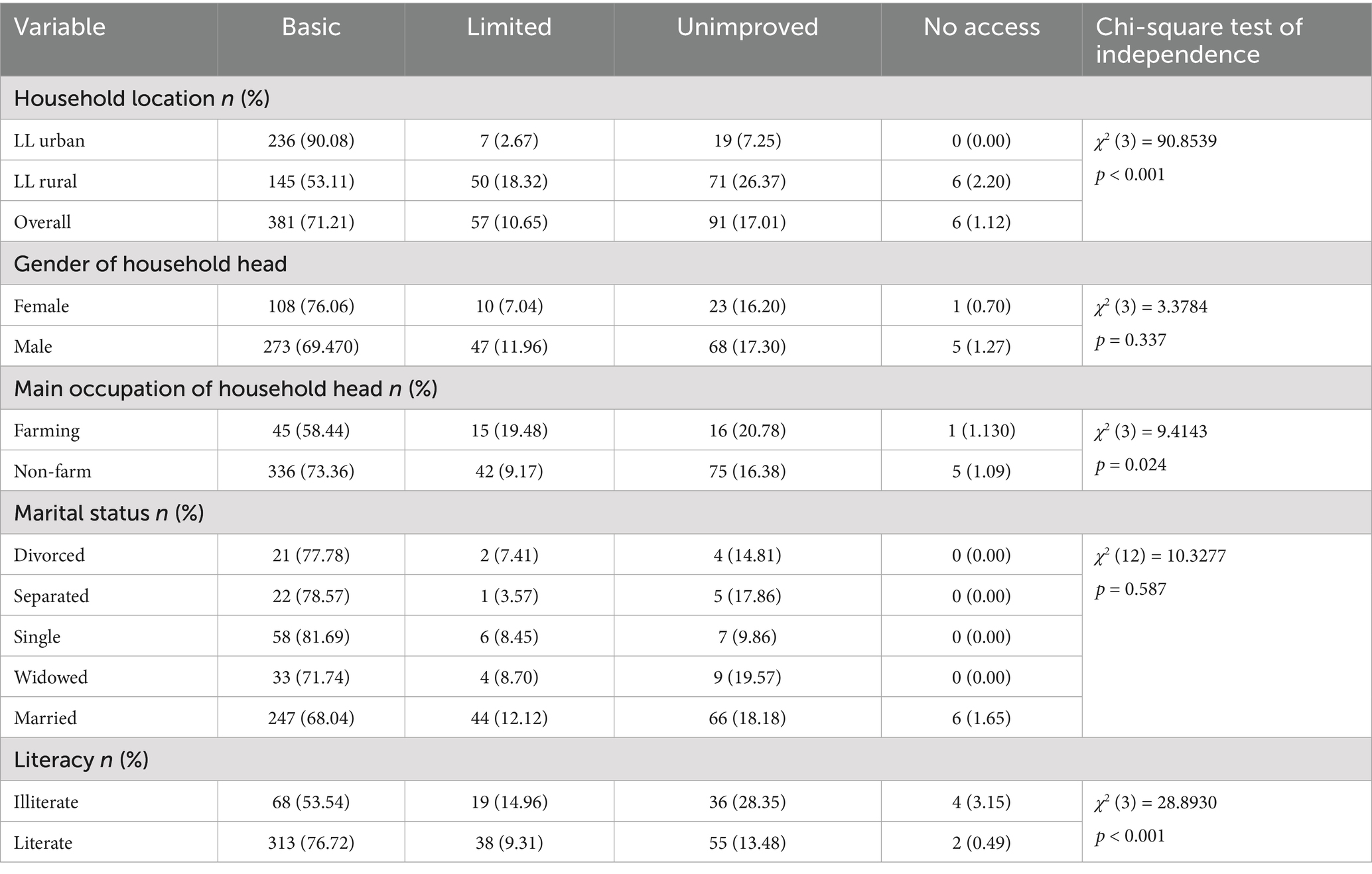
Table 3. Position on the drinking water ladder (n = 535).
Interestingly, though not statistically significant (p = 0.337), the results in Table 3 show that higher proportion of female-headed households (76.06%) than male-headed households (69.47) occupy the basic water services. Similarly, only 0.7% of female-headed households compared to 1.27% of male-headed households have no access to drinking water. This means that female-headed households are more likely to be on higher position of the drinking water service ladder, underscoring the priority that women give to safe drinking when they are leaders of their households. However, as discussed under differential impacts of water access challenges, women and girls bear the blunt of access challenges due to feminization of water fetching roles which translates into women and girls walking long distances in search for water, taking them away from education and economically productive activities.
Since the chi-square test of independence has weakness due to its inability to account for confounding variables, multivariate ordinal logistical regression was run to find predictor independent variables that predict a household’s position on the water service ladder. Based on literature review, an ordered logit model was estimated to investigate whether household location (rural versus urban), sex of household head, main occupation of household head, literacy of household head, marital status and household income predict the level of a household on the drinking water ladder (1 = No access; 2 = unimproved, 3 = limited, and 4 = Basic) where basic is the highest drinking water level on the ladder. Results of the ordered logit in Table 4 below show that only household location, OR = 5.00, p < 0.001, 95% CI (2.90, 8.62) significantly predicts a household’s position on the drinking water service ladder. That is, the odds of an urban household being on top level of basic services versus the combined levels of no access, unimproved, and limited are 5 times higher than that for a rural household. Goodness of fit test scores of ordinal Hosmer-Lemeshow = 0.2529, Pulkstenis-Robinson (Deviance) = 0.9950, and Lipsitz = 0.5851 prove that ordinal logistic model is a good fit (Fagerland and Hosmer, 2016).
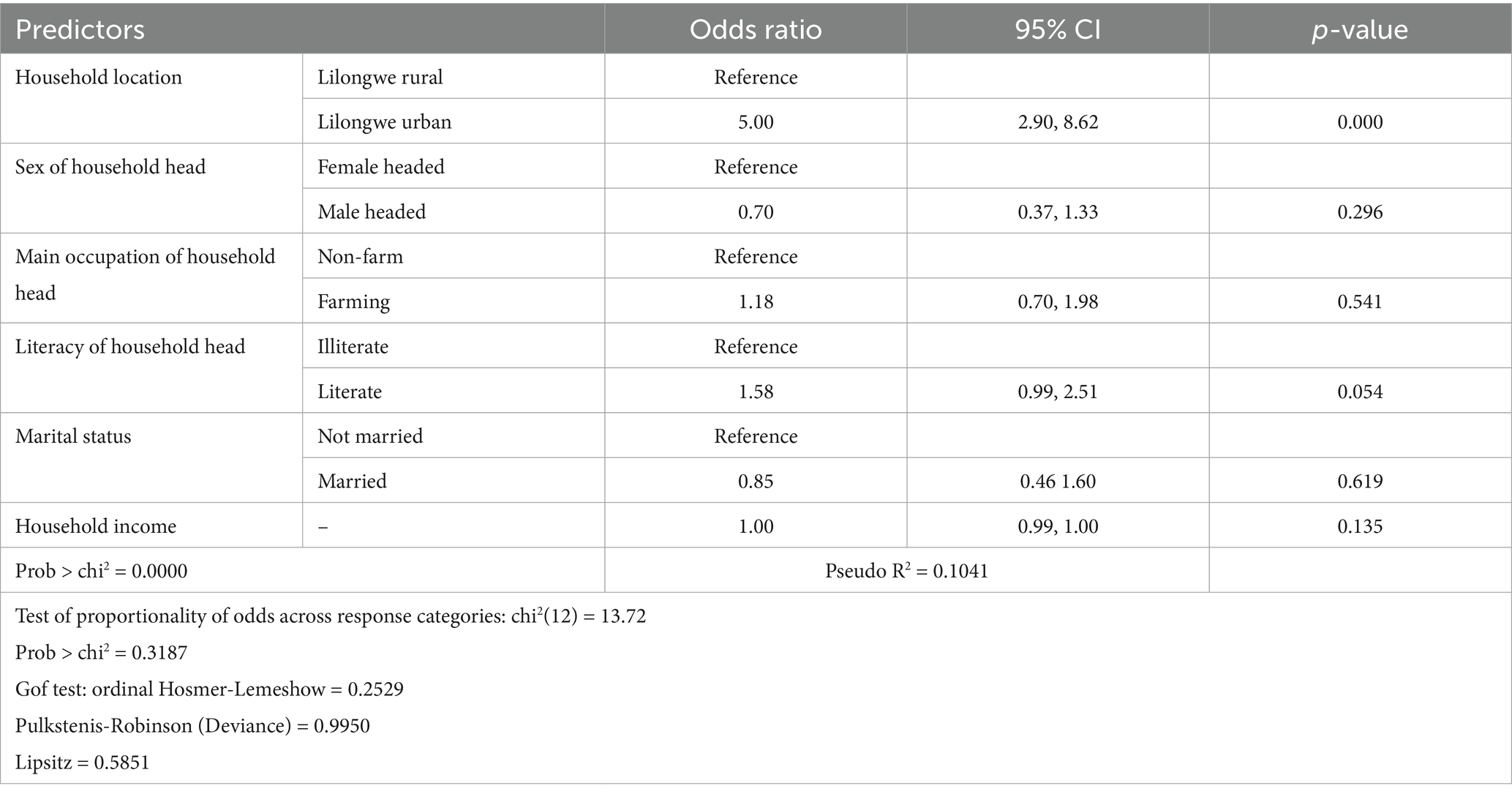
Table 4. Multivariate ordinal logistic regression for effect of predictor variables on household’s level on the drinking water ladder.
3.4 Distance to the main drinking water source
Based on the JMP framework, quality of water services delivery that households have access to be also measured by distance to the main water source (WHO and UNICEF, 2017). Distance to main drinking water source matters because studies show that when a main drinking water source is far from home premises, there are high risks of drinking water becoming contaminated during the water transportation process even if the water source itself had clean and safe drinking water (Levy et al., 2008). Further, long distance is associated with reduced daily per capita consumption of drinking water (Cassivi et al., 2018; Cairncross, 1990). The international standard is that a return walking trip to fetch water must not exceed 30 min (WHO and UNICEF, 2021). The results show that on average, a return walking trip to fetch water takes 8.74 min and 19.65 min in Lilongwe urban and Lilongwe rural, respectively (see Table 5). Though t-test of independence shows that the gap in collection time between rural and urban areas is significant (p < 0.001), the results indicate that both rural and urban areas do not suffer from time poverty related to water fetching as both spend <30 min threshold. Both KIIs and FGDs unearthed information that explains why relative to Lilongwe rural households, fetching water in Lilongwe urban takes significantly less time. Piped water connected to dwelling or standpipe in compound/yard are main source of drinking water for urban households. Lilongwe rural households are excluded from the drinking water pipeline. Piped water is more likely to be closer to people, including being directly connected to the dwelling house, allowing less travel time for the urban water users. One FGD participant in Lilongwe rural expressed frustration:

Table 5. Independent-means t-test on distance to main drinking water source.
We have a large population, over 3,000 households—that depend on these boreholes, which is unreasonable and results in long waiting time at the borehole. There are some households who are unable to fetch water from the boreholes because the distance is too far, so they just rely on the wells. (Anonymous, FGD with members of village development committee, Lilongwe rural)
3.5 Affordability of drinking water
Affordability is concerned with water users’ ability to pay for drinking water (Beecher and Shanaghan, 1998). When drinking water becomes unaffordable, the poor and other disadvantaged households who resort to alternative drinking water sources that in most cases are unsafe and unclean, thereby exposing their lives to water-borne diseases. The commonly adopted affordability threshold is the one set by the Organization for Economic Cooperation and Development (OECD) and the World Bank which states that monthly expenditures on drinking water should not exceed 3% of a household’s monthly income (Fan et al., 2013). The results in Table 6 show that households in Lilongwe rural and households in Lilongwe urban spend 1.75 and 12.36% of their monthly income on drinking water, respectively. Ordinarily, this would lead to a misleading conclusion that drinking water is more affordable in Lilongwe rural than in Lilongwe urban. This is not the case. While urban areas grapple with high and exclusion water user fees for their piped water, rural households are overburdened by high indirect costs such as the hospitalization costs due to high burden of waterborne diseases (Awuah et al., 2009). Rural areas also incur high opportunity cost by walking long distances to access drinking water, making them lose time which could be used in engaging in economically productive activities (WHO and UNICEF, 2022). Unfortunately, affordability metrics for drinking water fail to capture indirect costs that burden rural communities due to their overreliance on unimproved drinking water sources.

Table 6. Affordability of drinking water.
3.6 Reliability of drinking water source
Intermittence in drinking water supply matters because during periods of no water supply, water users are forced to access water from unsafe sources which expose their lives to health risks (Subbaraman et al., 2013). In assessing reliability of a drinking water services, the study adopted an indicator used by WHO and UNICEF (2017) which uses number of hours per day that water supply is available from main water source. The results in Table 7 show that there is very narrow difference in reliability of drinking water sources with households reporting daily water is availability of 17.8 h and 16.14 h for Lilongwe urban and Lilongwe rural, respectively. Results of binary logistic regression in Table 8 confirm that being a Lilongwe urban household or Lilongwe rural household is not a statistically significant predictor of a household having 24-h availability of drinking from the main source (OR = 1.49; p = 0.081). Similarly, marital status of household head, gender of household head (OR = 1.5477, p = 0.122), main occupation (OR = 1.0543, p = 0.850), household income (OR = 0.9999, p = 0.173), and literacy of household head (OR = 1.5395, p = 0.067) do not predict reliability of drinking water. Focus group discussions and KIIs reveal that while boreholes are the main source of water for the rural households, a significant proportion of the boreholes have in recent years become non-functional. Qualitative results reveal the seasonal nature of reliability performance of water sources in rural areas, with water being unavailable for long hours during the dry season due water table fluctuations. The reduced water table results in drying up of wells and failure of handpump boreholes to pump water.
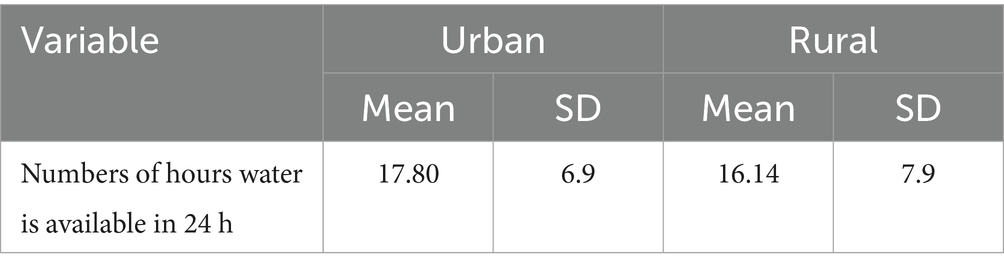
Table 7. Number of hours drinking water is available in a day.
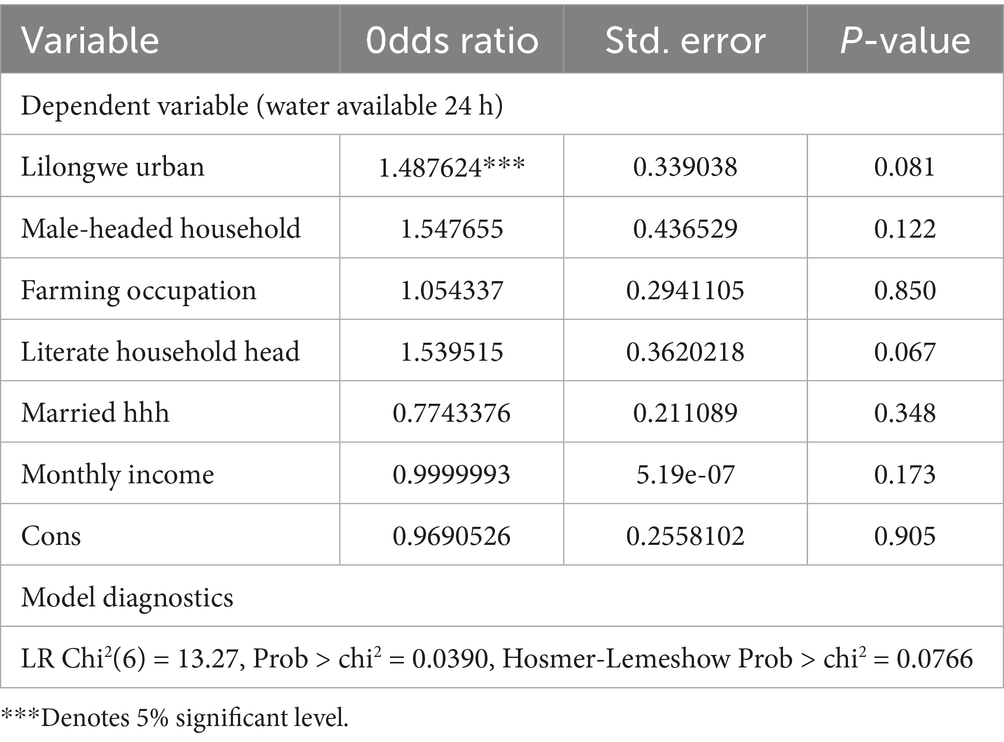
Table 8. Logistic regression results of factors influencing drinking water being available 24 h in a day.
3.7 Differential effects of the challenges in access to drinking water
To assess the negative effects of the challenges and examine if there are any differential magnitudes in terms of how Lilongwe rural and Lilongwe urban households are affected by such shortages, the study used an eight-item negatively worded Likert type statements. The statements were measured on 5-point Likert scale with 1 = strongly agree, 2 = agree, 3 = undecided, 4 = disagree, and 5 = strongly disagree. Since each statement indicated that there are negative effects that the households are facing due to their limited access to drinking water, the higher the score the less the burden of negative effects borne by households. Results in Table 9 show that based on the weighted average scores on the eight-item Likert scale, rural households disproportionately bear burden of the negative effects of low coverage of improved drinking water services. The weighted average score for the Lilongwe rural households is 2.57 which is relatively closer to 2 which indicates that the households agreed to the eight statements that their households experience negative effects due to the drinking water problems. For Lilongwe urban households, a weighted average score of 2.99 is almost equal to 3, indicating the urban households neither agree nor disagree that drinking water problems bring serious negative impacts on their lives and livelihoods.
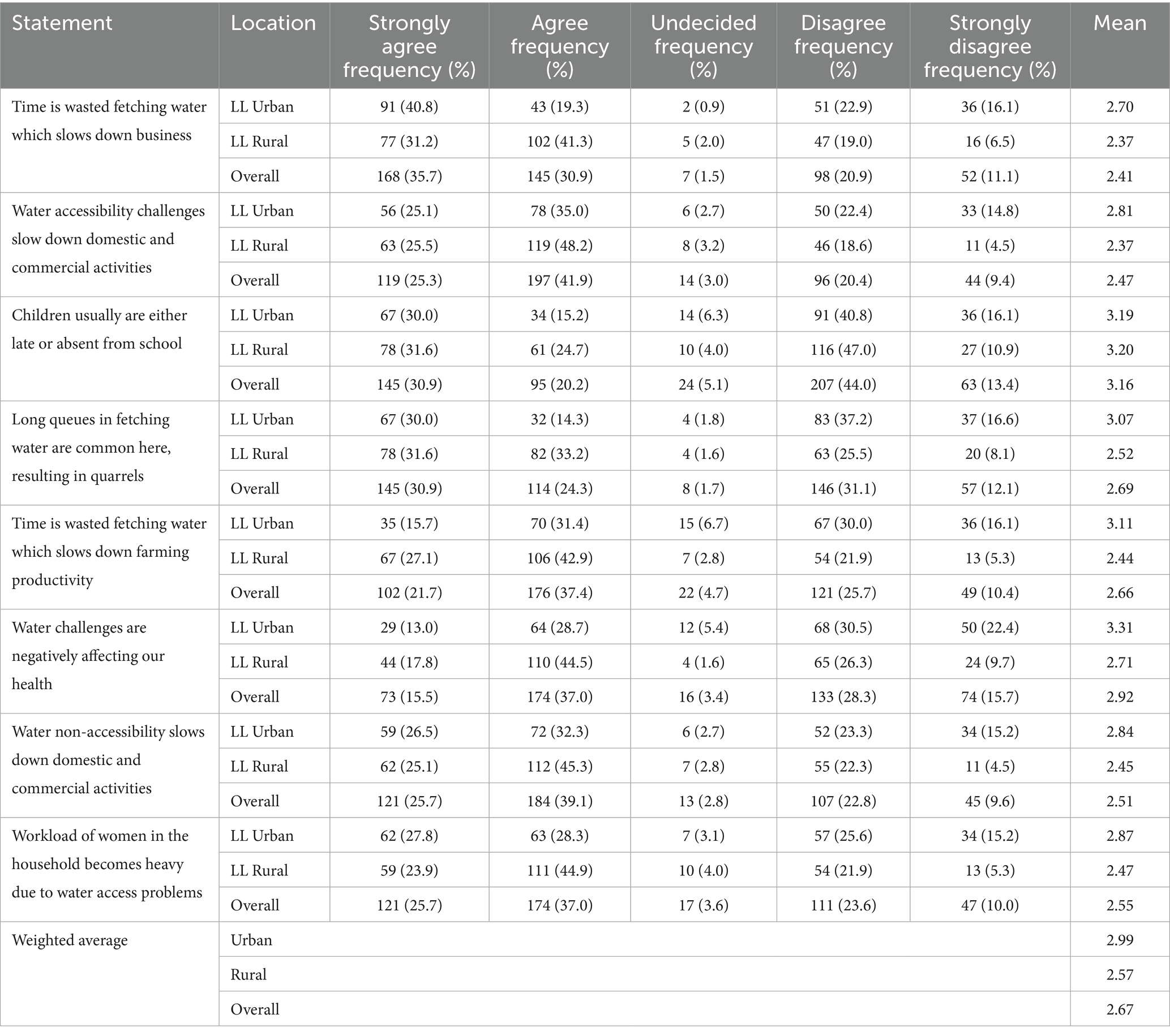
Table 9. How challenges in access to drinking water affects lives and livelihoods.
Concerning the specific negative effects that respondents responded to on the Likert score, 45.2% of Lilongwe urban households and 56.3% of Lilongwe rural households either strongly agreed or agreed that water challenges negatively affect the education of their children. The children either go to school late or completely absent themselves from school due to lack of bathing water or being ill from waterborne diseases. Further, agriculture is the backbone of the economy in Malawi, employing over two thirds of the rural population (Baulch et al., 2019). However, agriculture has not been spared by the negative consequences that come from drinking water problems as household labor is diverted from farming activities and invested in fetching water from distant sources that take up most of the productive hours of the day. In this regard, 47.5% of Lilongwe urban households versus 70% of Lilongwe rural households either strongly agreed or agreed that their farming activities are slowed down due to drinking water challenges faced in their communities and households. Similarly, crucial domestic and commercial activities for the households significantly get slowed down due to the longstanding and multifaceted drinking waters problems, with 60.1 and 73.7% of Lilongwe urban households and Lilongwe rural households, respectively, reporting the challenge. In an FGD, one male participant in Lilongwe rural shared her frustration with how women come to the farm very late.
It affects labour on our farms. Women sometimes come to the farms late, around 10AM instead of the normal 6AM as they spend a lot of time at the water point. (FGD with mixed gender group, Lilongwe rural)
Due to poor water quality, negative health outcomes were also reported. Specifically, more households in Lilongwe rural (62.3%) than in Lilongwe urban (41.7%) either strongly agreed or agreed that water challenges are afflicting their communities and households with a heavy burden of waterborne diseases. Even results from FGDs and KIIs collaborate the findings.
The water in this community is not safe. Sometimes we have to fetch stagnant water from the wells because we have no other option, and often, when we use this water, we end up with diarrhoea. But we have no choice; we still need to eat, even though we don’t have good water to use. (FGD with women, Mkulumimba village, Nanjiri area, Lilongwe rural)
In Malawi, which is one of the highly patriarchal societies, gender roles allocate the role of water fetching to women and girls. Water fetching therefore is a highly gendered issue which favors men at the expense of women and girls. The feminization of drinking water fetching roles entails that when water challenges arise, it is women and girls who bear the blunt of walking long distances to fetch drinking water and returning home with heavy buckets of drinking water weighing 20 liters for girls and 40 liters for women on their head. Water portage in Malawi is done using the woman as the porter who physically carries plastic buckets full of water on her head. The results show that, respectively, 56.1% of households from Lilongwe urban and 68.8% of households from Lilongwe rural either strongly agreed or agreed that women in their households suffer increased workload due to water challenges as they spend long hours and walk long distances fetching drinking water for their households. Qualitative results revealed that due to water shortages, women are forced to wake up as early as 2 AM in the morning to start their long day of hunting for drinking water.
4 Discussion
4.1 Main sources of drinking water and position on drinking water service ladder
Results show wide disparities between rural and urban households. Urban households have a disproportionately higher access to piped water (90.8%) than their rural counterparts (3.66%). For majority of rural households, borehole and unprotected wells remain their main source of drinking water. While these results agree with the nationwide studies conducted by the National Statistics Office that urban households have higher access to piped water, they reveal the unique situation of the extent of disparity between Lilongwe rural and Lilongwe urban. The 2017 integrated household survey results showed a narrow gap as national average showed that 67% of urban households had access to piped water compared to 6.7% of the rural households which is gap of 60%. This study finds a wider gap of 87%. Furthermore, while the national average for access to piped water for rural households is 6.7%, the wider gap in Lilongwe could be masked as only 3.66% of Lilongwe rural households have access to piped water.
The huge disparities between rural and urban areas in terms their main sources of drinking water are consequential. Firstly, a 2020 study that was conducted in five rural districts of Malawi revealed depressing results that show that only 43% of the boreholes in rural areas of Malawi meet the WHO standards on drinking water quality (Mkandawire et al., 2020). Further, MICS that was also conducted in 2020 in Malawi measured the quality of drinking water by source using number of E-coli detected in the water as an indicator. The results showed that piped water is relatively safer as 56.8% of water samples from piped water had low levels of faecal matter contamination (<1 per 100ML) compared to 43% from boreholes and a meagre 4.7% from unprotected wells (National Statistical Office, 2021). In fact, the MICS study found that as high as 81% of drinking water samples from unprotected wells had high (101–1,000 pe 100ML) or very high (> 1,000 per 100ML) concentration of E. coli, followed by boreholes at 27.9% and only 20.5% for piped water. Qualitative results from this study that water users in Lilongwe rural complained of strange color, unpalatable taste, and odor of drinking water which they draw from unprotected wells and surface sources like rivers and streams. The fact that nearly all households of Lilongwe rural have no access to piped water is therefore unjust and unfair for it exposes a disproportionately higher proportion of the rural households to waterborne diseases such as cholera and diarrhea as they are forced to rely on unsafe drinking water sources. A study that was conducted in the rural areas of Balaka in Malawi showed that 50% of all disease burden in the district were waterborne diseases (Mkwate et al., 2017). Further, the grave consequences of accessing drinking water from unsafe source is demonstrated by the fact that in 2019 alone, over 1.53 million people in the world died due to diarrheal which is water-borne disease (Dattani et al., 2023). By putting households of Lilongwe rural into perpetual conditions that force them to rely on unsafe drinking water sources, they are made victims of water injustices. This is because the rural residents’ right to safe drinking water as declared in 2010 by the United Nations Human Rights Council is violated (UN, 2010).
These findings on the water injustices faced by rural households as they lag urban households are consistent with findings of previous studies. In Asia, De Magny et al. (2011) found that rural households in Bangladesh have less access to piped drinking water than urban households. In Africa, drinking water disparities that favour urban areas at the expense of rural areas have been found to be historically persistent in South Africa (Mbana and Sinthumule, 2024; Mokoena, 2022), Kenya (Osiemo et al., 2019), Nigeria (Dan-Nwafor et al., 2019) and Uganda (Bwire et al., 2020).
In terms of position on the drinking water ladder, the study found that rural households lag urban households with 90.8% of urban households compared to only 53.11% of rural households being on the top position which is basic drinking water service level. The results show a larger proportion of Lilongwe urban households (92.75%) than Lilongwe rural households (71.43%) have access to improved drinking water. Nationwide demographic and health survey conducted in Malawi found similar results which showed that while only 85% of rural households had access to improved drinking water services, urban areas had 98% of its households having access to improved drinking water services (National Statistical Office, 2017b). At regional level, the findings of the study are in line with previous study which was conducted in Northern Ethiopia (Amsalu et al., 2022) and Eastern Province in South Africa (Mbana and Sinthumule, 2024).
Despite the study not finding statistically significant differences between female-headed and male-headed households in terms of their positions on the drinking water service ladder, the results show that female headed households are better off than male-headed counterparts. Previous studies in East Africa (Terefe et al., 2024), Ivory Coast (Angoua et al., 2018), and Vietnam (Tuyet-Hanh et al., 2016) found female-headed households have statistically significant higher access to basic water services than male-headed households. This is not attributed to female household heads being given preferential treatment and more opportunities to improved drinking water. Rather, it is because, being responsible for taking care of the sick children; cooking; and household cleanliness and hygiene, women place special importance and priority on guaranteeing access safe drinking water for their households and are willing to walk longer distances and spend their last penny to ensure this is achieved.
When it comes to distance to main water source, the study reveals that while both urban households (8.74 min) and rural households (19.65 min) fall within the internationally recommended 30 min or less for a return walking trip (WHO and UNICEF, 2017), Lilongwe urban households are 6.49 times more likely to spend 30 min or less on a water fetching trip than their rural counterparts. This can be explained by the fact that piped water is the main source of water for a significant proportion of the urban households. This is not the case with the Lilongwe rural households as the rural areas are excluded from drinking water supply from the infrastructure network that supply piped water. Based on Ghana’s nationwide demographic and household survey data, Amankwaa et al. (2024) found similar results that showed that rural households had 1.2 times higher odds of experiencing time poverty caused by longer hours spent on water fetching. It is concerning when households spend more than 30 min on water collection. There is scientific evidence that collection times of drinking water that exceeds 30 min have serious negative consequences on both the physical and the mental wellbeing of household members who are primarily responsible for water fetching (Abrefa-Busia, 2022; WHO, 2020) who, based on gender roles in Africa, are mostly women and children (Amankwaa et al., 2024; Gambe, 2019). For example, in Kenya (Nygren et al., 2016) and Burkina Faso (Dos Santos et al., 2015), drinking water collection times longer than 30 min were significantly associated with more incidences of diarrhea. In fact, a regional study conducted in Sub-Saharan Africa showed that a 15-min reduction in collection time of drinking water reduced incidences of diarrhea in children by 41% (Pickering and Davies, 2012). In addition, when a main drinking water source is distantly far away, drinking water is exposed to contamination during the carriage and transportation process (Levy et al., 2008; Trevett et al., 2005). This is especially the case in Malawi where water is carried on people’s heads in uncovered plastic buckets.
As already discussed above, the low coverage of improved drinking in rural areas and the associated low position on drinking water service ladder has very serious grave consequences on the healthy and socioeconomic status of rural communities. Overreliance on unsafe drinking water sources and exclusion from piped water infrastructure network inflict serious passive infrastructure violence on rural communities (Rodgers and O’Neill, 2012). While it may be financially not feasible to extend the central networks of piped water that serve the country’s cities and towns, there are less-costly small scale rural water supply systems which Malawi has not fully exploited. For instance, UNICEF and Water Mission have piloted solar powered water pumping systems (SPWPSs) in few selected rural areas in Malawi and the results of the pilot show that the SPWPSs are both effective and efficient in elevating the position of rural communities on the drinking water service ladder by allowing rural users access drinking water of improved quality while at the same time reducing walking distance to water sources (UNICEF, 2020; Longwe et al., 2019). The SPWPs have also proved to be both financially sustainable for rural communities and environmentally friendly (Longwe et al., 2019). Moreover, SPWPSs use photovoltaic energy to pump groundwater and studies show that Malawi has high levels of insolation of approximately 1,800 Wh per square meter per year (World Bank, 2017; Suri et al., 2015) which makes it conducive for using renewable energy technologies (RETs) for groundwater pumping. Rainwater harvesting, which involves the collection of rainwater from catchments and conveying it to a storage facility for drinking or farming purposes (Yannopoulos et al., 2017) has been successfully used to improve drinking water coverage in other countries like Cameroon (Qi et al., 2019) and South Africa (Matimolane et al., 2023). A recent study conducted in Mandara Mountains in Cameroon proved that rainwater harvesting an affordable system for supplying safe water to both rural and urban areas (Madomguia et al., 2025). To be effective and sustainable, it is important that storage facilities for harvested rainwater such as dams be constructed after conducting comprehensive technical and engineering research on project site (Gebreeyesus et al., 2025). However, scaling up of rainwater harvesting in rural areas is stifled by strong negative perception among rural water users that rainwater is both unclean and unsafe, only used by rural folks out of desperation (Anang and Asante, 2020; Matimolane et al., 2023). Addressing such negative perceptions can go a long way in improving the acceptability of harvested rainwater as an improved drinking water source. By investing in solar powered water pumping systems and rainwater harvesting systems, the Malawi Government and its development partners can significantly increase coverage of improved drinking water in rural communities.
4.2 Reliability of drinking water
Findings of the study reveal that there is no statistically significant difference between rural and urban households with regards to reliability of main drinking water source. On average, in 24 h, drinking water is available 17.8 h and 16.14 h for urban and rural households, respectively. A study that was conducted in China found that interruptions in water supply force households to reduce the amount of water used on household and personal hygiene (Fan et al., 2013). By reducing the amount of water available for household and personal hygiene, household members become more exposed to the risk of hygiene related morbidities (Fan et al., 2013). While this study finds no significance differences between urban households and rural households in terms of reliability of drinking water services, the results contradict findings of a similar study that was carried out in Lilongwe by Adams and Smiley (2018). In their study, Adams and Smiley (ibid) found that apart from temporary seasonal reduction in water table during the dry season, rural households, due to their reliance on groundwater sources like boreholes and wells which do not get affected by any system breakdown and interruptions, enjoy more reliable and uninterrupted services than urban households. However, frequent power cuts and low pressure negatively affect reliability of drinking water services in urban areas. However, this study finds that reliability of drinking water services in rural areas from their groundwater sources has also dramatically decreased in recent years. This can perhaps be explained by studies that show that significant proportions of boreholes which are the main source of drinking water for rural households have increasingly become nonfunctional due to lack of regular repairs and maintenance. This is not surprising given than recent studies show that 26% of the boreholes in Malawi were non-functional (Mkandawire et al., 2020). Rodgers and O’Neill (2012) argue that such nonfunctional boreholes are catalysts for perpetuating passive infrastructure violence. This is because, in the records of government they are more likely to indicate that the rural areas have access to good water simply because they installed boreholes there, yet in actual sense a significant number of such boreholes are not functional.
4.3 Affordability of drinking water
With regards to affordability of drinking water, results show that Lilongwe urban households spend 12.36% of their monthly income on drinking water which crosses the affordability cut off point of 3% set by World Bank and OECD (Goddard et al., 2021). A significant proportion of the urban residents in Lilongwe rely on low-income jobs and petty trading as their main primary occupation (Rusca et al., 2017). With low income for the average urban household, expenditure on water constitutes a significant portion of their household incomes. The results that drinking water is unaffordable in Lilongwe urban agree with a 2021 study by Beard and Mitlin (2021) which found that drinking water was unaffordable for urban households in the cities of Mzuzu in Malawi, Kampala in Uganda, and Cochabamba in Bolivia. The fact that water is unaffordable for most households in Lilongwe urban implies households who cannot afford piped water are forced to either rely on unsafe water sources or are forced to use less water which puts their physical wellbeing at greater risk of waterborne diseases (Foster and Hope, 2016). Spending a higher proportion of household income on drinking water alone also implies that households must forgo other essential basic needs like nutritious food.
In Lilongwe rural, the results show that households spend 1.75% of their monthly income on drinking water, which gives a misleading picture that drinking water is more affordable in Lilongwe rural than Lilongwe. This misleading affordability of rural drinking water is due to weaknesses in the metrics used in assessing drinking water affordability which do not capture high indirect costs that rural households grapple with due to their overdependence on unsafe drinking water sources. Literature shows that rural households spend a lot of money on hospitalization due to high burden of waterborne diseases (Awuah et al., 2009). Further, by walking long distances to access drinking water and losing more hours fetching water, high opportunity costs are incurred by rural households in terms of lost earnings (WHO and UNICEF, 2022). Indeed, FGD results in Lilongwe rural revealed that the women spend most of their awake time hunting for water instead of working in their subsistence farms or running their mostly informal businesses.
4.4 Effects of water injustices on rural people’s lives and livelihoods—passive infrastructure violence in action
Finally, in terms how lives and livelihoods are affected by drinking water access problems, more rural households either agree or strongly agree that their lives and livelihoods have been adversely affected than do Lilongwe urban households. Specifically, proportion wise, Lilongwe rural households were more likely to report that their children missed school, lost many productive hours to water fetching that slowed down their businesses and farming activities, and experienced higher incidences of waterborne morbidities than Lilongwe urban households. Previous studies have also reported similar findings that drinking water challenges significantly reduce the amount of time available to rural households to engage in economically productive activities (Adams and Smiley, 2018; Choudhuri and Desai, 2021). Further, lack of drinking water also has been reported by scholars to crowd children out of classrooms due to lack of water for bathing and laundry and the situation is worse for the girls who also spend long hours fetching water instead of being in the class (Dickin et al., 2021; Routray et al., 2017). In Malawi, Mkwate et al. (2017) found that drinking water challenges in the rural district of Balaka disrupt both education and economic activities of households as they spend more time dealing with waterborne illnesses. Rusca et al. (2017), however, argues that even urban households in Lilongwe urban, especially those in informal urban settlements, also bear the blunt of poor drinking water problems, warning that water justice interventions should not just focus on rural areas. Therefore, for Rusca et al. (2017), attention must also be given to the plight of the urban poor living in slums whose right to clean and safe drinking water are also in constant state of flux and marginality.
The results also show that that the consequences of low coverage of improved drinking water are gendered. Qualitative data with key informants, male FGD participants, and female FGD participants all point to women and girls being disproportionately burdened by poor and inferior drinking water services. It is women and girls, in fulfilling their patriarchy-influenced gender roles, that walk long distances to fetch water. They are also the same women and girls that stop everything that could economically or educationally benefit them just take to care of those hospitalized due to high waterborne disease burden. The findings on the gendered nature of impacts of limited access to drinking water are in sync with previous findings in Sub-Saharan Africa which revealed that women and girls are physically and sexually attacked as the walk long distances and sometimes in darkness at night in search for drinking water (Terefe et al., 2024; Bachwenkizi et al., 2023).
There is consensus among urban sociologists and anthropologists that infrastructures, including water supply infrastructure, can be oppressive to and violent against marginalized and vulnerable communities (Sharan, 2006; Kayser, 2015). The negative impacts which are disproportionately borne by Lilongwe rural households constitute passive infrastructure violence as they arise out of deliberate and planned exclusion of rural people from piped water supply infrastructure network. Such exclusions are a product of a systematic and often legitimized processes undertaken by powerful state bureaucrats that fundamentally reflect the social stratification and attendant inequalities prevalent in a particular society. The Waterworks Act of 1995 which establishes the Malawi’s five centralized water utility companies, called Water Boards, contributes to the marginalization of rural communities in as far as access to piped drinking water is concerned. The 1995 Act is very clear in limiting the jurisdiction of the five major water utility companies to only urban areas (Malawi Government, 1995). By limiting the water utility companies to only serve urban areas, the Act inadvertently not only facilitates but also legitimizes water injustice as it essentially excludes of rural communities from being connected to pipeline infrastructure. Further, funding for investments in drinking water infrastructure mirror the institutionalized urban bias at the expense of rural communities. Periodic comprehensive analyses conducted by UNICEF (2023) consistently find that funding in the water sectors is weaponized against rural communities, with more per capita investment for urban communities than rural communities. Moreover, institutions that are responsible for drinking water supply in rural communities in Malawi have the highest vacancy rate of 62.2% which translates into lack of capacity to optimally discharge their duties of moving rural communities up the drinking water service ladder (JICA, 2022). On the contrary, central water utilities which serve urban communities have zero vacancy rates and in some cases are even overstaffed (ibid). Thus, it can be conclusively stated that legislation, and budgetary allocations are tools of water injustices oppression in Malawi that perpetuate water-related oppression and suffering of rural communities. Drinking water supply infrastructure must be seen as merely a material expression and manifestation of disparities, hierarchies and iniquities existing within a society where power is not equally shared. According to Rodgers and O’Neill (2012), there is passive infrastructural violence if poor and marginalized communities suffer harmful health, social, and economic effects that arise out of the infrastructures’ deficiencies, omissions, and exclusions. Ferguson (1999) and Gandy (2006) provided a clear and persuasive demonstration of how violent infrastructure networks can be on those that are excluded from them, highlighting how vulnerable and poor communities experience sufferings due to their being disconnected from infrastructure networks. Ironically, the piped water supply infrastructure for Lilongwe draws its water from Malengunde Dam, which is based in Lilongwe rural, yet the households of Lilongwe rural are not connected to it. Decision makers and policy makers that decide which households and locations should be connected to the water supply infrastructure are middle class and senior officers who are elites living in the city. Their priority is to advance the interests of fellow urban elites. Mann (1984) refers to such powerful elites as state elites and goes further to point out that such elites are empowered to make decisions on how to allocate resources including which locations and people are to be served by infrastructure networks. The domination of the powerful state elites reflects the government’s strong grip on “infrastructural power” as first noted by Mann (1984). Infrastructure power happens when the state and elites develop and manipulate water infrastructures to protect and advance the interests of dominant social class (Rodgers and O’Neill, 2012). Moreover, the drive for profit and capital accumulation by government-owned water boards means that rural areas are seen as unattractive and lacking incentives for business. The primacy of the profit motive is explicitly clear for the Lilongwe Water which in its 2020–2025 strategic plan vows to implement “a reflective full cost recovery tariff, aggressive revenue collection mechanisms and diversified financing options based on sound financial management practices” (LWB, 2020, p. 7). Similar findings were reported in India by Kumar et al. (2021) who observe that through commodification and privatization which come with unaffordable water tariffs, poor residents in the city of Delhi suffer infrastructure violence.
5 Conclusion
The results show that relative to households in Lilongwe urban, households in Lilongwe rural walk longer distances, rely on drinking water from unsafe and more inferior sources, and occupy lower positions on the drinking water services ladder. While piped water is the main drinking water source for most of the households in Lilongwe urban, this is not the case for the Lilongwe rural households as they mostly rely on boreholes. Another highlight of the findings of the study is that while Lilongwe urban households have successfully graduated from depending on surface water sources like rivers, 2.56% of Lilongwe rural households continue to rely on such unsafe water sources. However, while previous studies found that rural areas enjoy higher levels of reliability of drinking water, this study finds that failure to repair boreholes have seen rural water services also become increasingly less reliable. Further, the results show that drinking water is unaffordable for Lilongwe urban households as they spend 12.36% of their monthly income on drinking water. Metrics for drinking water affordability fail to capture indirect costs borne by Lilongwe rural households as they lose more time fetching water and spend more money on healthcare due to high burden of drinking water related morbidities. Resultantly, affordability of drinking water rural areas is misleadingly overestimated.
The Lilongwe rural households are bearing the heaviest burden from consequences of drinking water access challenges. Losing more productive hours to water fetching which slows down farm and commercial activities, having children miss their classes due absenteeism caused by lack of drinking water, and high prevalence of waterborne diseases were reported by higher proportion of Lilongwe rural households than their Lilongwe urban counterparts. Therefore, to reduce such infrastructure violence which rural households suffer due to their exclusion from piped water networks, the study recommends that government and duty bearers should take deliberate action at policy and operational levels aimed at extending and expanding piped water to rural areas. This does not necessarily need to be connection to the central pipe network. Solar-powered water pumps which have been successfully implemented by UNICEF in selected rural areas of Malawi is an option for sustainably delivering piped water to the doorsteps of rural households (Longwe et al., 2019; UNICEF, 2020). Further, monitoring boreholes and ensuring their prompt and timely repairs would go a long way in ensuring reliable drinking water services from the already existing boreholes. Without these intended and deliberate actions, the right to safe and reliable drinking water will remain elusive to most rural residents. Given that the right to water entitles everyone to have access to potable and safe drinking water and that for a significant proportion of rural residents in Malawi their right to water is in constant and continuous violation, it entails that rural people are suffering water justice which is partly made worse by passive infrastructure violence. Future studies should explore legal remedies in both local and international legal instruments which can be taken against those whose statutory duty is to guarantee the enjoyment of the right to water by every human being.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study was cleared by my supervising professor as not requiring ethics approval at Sophia University for the studies involving humans. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MC: Conceptualization, Supervision, Writing – review & editing, Validation, Investigation, Writing – original draft, Formal analysis, Methodology, Software, Data curation, Visualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study is part of the MC PhD studies and Sophia University whose scholarship is provided by Japanese International Cooperation Agency (JICA). Funding for fieldwork for the study was drawn from the JICA scholarship.
Acknowledgments
The author would like to express heartfelt appreciation and gratitude to Guangwei Huang who is a professor at Sophia University in Japan for his analytical, enlightening and thoughtful guidance provided during the development of the manuscript. Further, the author acknowledges the indispensable contribution of water users, community leaders and water officials in Lilongwe in Malawi for accepting to participate in the study either as respondents or participants.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author declares that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abrefa-Busia, K. (2022). Married working women and work-family interface in urban Ghana: A holistic approach. Unpublished PhD thesis. Hong Kong: Lingnan University.
Adams, E. A., and Smiley, S. L. (2018). Urban-rural water access inequalities in Malawi: implications for monitoring the sustainable development goals. Nat. Res. Forum 42, 217–226. doi: 10.1111/1477-8947.12150
Adelodun, B., Ajibade, F. O., Ighalo, J. O., Odey, G., Ibrahim, R. G., Kareem, K. Y., et al. (2021). Assessment of socioeconomic inequality based on virus contaminated water usage in developing countries: a review. Environ. Res. 192:110309. doi: 10.1016/j.envres.2020.110309
Akpabio, E. M., Mwathunga, E., and Rowan, J. S. (2021). Understanding the challenges governing Malawi’s water, sanitation and hygiene sector. Int. J. Water Res. Dev. 38, 426–446. doi: 10.1080/07900627.2021.1897947
Akurugu, B. A., Chegbeleh, L. P., and Yidana, S. M. (2020). Characterisation of groundwater flow and recharge in crystalline basement rocks in the Talensi District, northern Ghana. J. Afr. Earth Sci. 161:103665. doi: 10.1016/j.jafrearsci.2019.103665
Amankwaa, G., Busia, K. A., Agbadi, P., Duah, H. O., and Arthur-Holmes, F. (2024). Access heterogeneities and collection time inequalities of drinking water sources in Ghana: implications for water and development policy. Local Environ. 29, 263–278. doi: 10.1080/13549839.2024.2306596
Amsalu, A., Atikilt, G., Taklual, W., and Tilahun, A. (2022). Progress of water, sanitation, and hygiene facilities in public primary schools of South Gondar zone, northern Ethiopia. PAMJ - One Health 7:30874. doi: 10.11604/pamj-oh.2022.7.19.30874
Anang, B. T., and Asante, B. O. (2020). Farm household access to agricultural services in northern Ghana. Heliyon, 6. doi: 10.1016/j.heliyon.2020.e05517
Angoua, E. L. E., Dongo, K., Templeton, M. R., Zinsstag, J., and Bonfoh, B. (2018). Barriers to access improved water and sanitation in poor peri-urban settlements of Abidjan, Côte d’Ivoire. PLoS One 13:0202928. doi: 10.1371/journal.pone.0202928
Asadullah, M. N., and Rahman, S. (2009). Farm productivity and efficiency in rural Bangladesh: the role of education revisited. Appl. Econ. 41, 17–33. doi: 10.1080/00036840601019125
Awuah, E., Nyarko, K. B., and Owusu, P. A. (2009). Water quality and infrastructure challenges in rural Ghana. J. Water Health 7, 581–592. doi: 10.2166/wh.2009.022
Aydamo, A. A., Gari, S. R., and Mereta, S. T. (2023). Access to drinking water, sanitation, and hand hygiene facilities in the peri-urban and informal settlements of hosanna town, southern Ethiopia. Environ. Health Insights 17:3604. doi: 10.1177/11786302231193604
Bachwenkizi, J., Mohamed, H., Funsan, P., Rweyemamu, D., Nelson, W., Shao, M., et al. (2023). Access to water sources and intimate partner violence against women in 26 sub-saharan African countries. Hyg. Environ. Health Adv. 7:100063. doi: 10.1016/j.heha.2023.100063
Baulch, B., Benson, T., Erman, A., Lifeyo, Y., and Mkweta, P. (2019). Malawi's challenging employment landscape. MaSSP working papers 27 international food policy research institute (IFPRI). Washington, DC: IFRI.
Beard, V. A., and Mitlin, D. (2021). Water access in global south cities: the challenges of intermittency and affordability. World Dev. 147:105625. doi: 10.1016/j.worlddev.2021.105625
Beecher, J. A., and Shanaghan, P. E. (1998). Water affordability and the DWSRF. J. Am. Water Works Assoc. 90, 68–75. doi: 10.1002/j.1551-8833.1998.tb08435.x
Bengtsson, M. (2016). How to plan and perform a qualitative study using content analysis. Nurs. Plus Open 2, 8–14. doi: 10.1016/j.npls.2016.01.001
Benson, T., and De-Weerdt, J. (2023). Employment options and challenges for rural households in Malawi: An agriculture and rural employment analysis of the fifth Malawi integrated household survey, 2019/10. MaSSP working paper 40. Washington, DC: International Food Policy Research Institute (IFPRI).
Bernard, H. R. (2017). Research methods in anthropology: Qualitative and quantitative approaches. Lanham: Rowman and Littlefield.
Borderon, M., Best, K. B., Bailey, K., Hopping, D. L., Dove, M., and Cervantes de Blois, C. L. (2021). The risks of invisibilization of populations and places in environment-migration research. Hum. Soc. Sci. Commun. 8:1. doi: 10.1057/s41599021-00999-0
Bwire, G., Sack, D. A., and Kagirita, A. (2020). The quality of drinking and domestic water from the surface water sources (lakes, rivers, irrigation canals and ponds) and springs in cholera prone communities of Uganda: an analysis of vital physicochemical parameters. BMC Public Health 20:1128. doi: 10.1186/s12889-020-09186-3
Cairncross, S. (1990). Health Impacts in Developing Countries: New Evidence and New Prospects. J Instit Water Environ Manag. 4, 571–77.
Cassivi, A., Johnston, R., Waygood, E. O. D., and Dorea, C. C. (2018). Access to drinking water: time matters. J. Water Health 16:wh2018009. doi: 10.2166/wh.2018.009
Chaudhuri, S., and Roy, M. (2017). Rural-urban spatial inequality in water and sanitation facilities in India: a cross-sectional study from household to national level. Appl. Geogr. 85, 27–38. doi: 10.1016/j.apgeog.2017.05.003
Choudhuri, P., and Desai, S. (2021). Lack of access to clean fuel and piped water and children’s educational outcomes in rural India. World Dev. 145:105535. doi: 10.1016/j.worlddev.2021.105535
Dan-Nwafor, C. C., Ogbonna, U., Onyiah, P., Gidado, S., Adebobola, B., and Nguku, P. (2019). A cholera outbreak in a rural north central Nigerian community: an unmatched case-control study. BMC Public Health 19, 1–7. doi: 10.1186/s12889-018-6299-3
Dattani, S., Spooner, F., Ritchie, H., and Roser, M. (2023). Diarrheal diseases. Oxford: OurWorldInData.
De Magny, G. C., Mozumder, P. K., Grim, C. J., Hasan, N. A., Naser, M. N., and Alam, M. (2011). Role of zooplankton diversity in Vibrio cholerae population dynamics and in the incidence of cholera in the Bangladesh Sundarbans. Appl. Environ. Microbiol. 77, 6125–6132. doi: 10.1128/AEM.01472-10
Dickin, S., Bisung, E., Nansi, J., and Charles, K. (2021). Empowerment in water, sanitation and hygiene index. World Dev. 137:105158. doi: 10.1016/j.worlddev.2020.105158
Dos Santos, S., de Charles, O. F., and Soura, A. B. (2015). Water-related factors and childhood diarrhoea in African informal settlements: a cross-sectional study in Ouagadougou (Burkina Faso). J. Water Health 13, 562–574. doi: 10.2166/wh.2014.115
Fagerland, M., and Hosmer, D. (2016). Tests for goodness of fit in ordinal logistic regression models. J. Stat. Comput. Simul. 86:1156682. doi: 10.1080/00949655.2016.1156682
Fan, L., Liu, B., Wang, F., Geissen, V., and Ritsema, C. (2013). Factors affecting domestic water consumption in rural households upon access to improved water supply: insights from the Wei River basin, China. PLoS One 8:e71977. doi: 10.1371/journal.pone.0071977
Ferguson, J. (1999). Expectations of modernity: Myths and meanings of urban life on the Zambian Copperbelt. Berkeley, CA: University of California Press.
Foster, T., and Hope, R. (2016). A multi-decadal and social-ecological systems analysis of community waterpoint payment behaviours in rural Kenya. J. Rural. Stud. 47, 85–96. doi: 10.1016/j.jrurstud.2016.07.026
Gambe, T. R. (2019). The gender dimensions of water poverty: exploring water shortages in Chitungwiza. J. Poverty 23, 105–122. doi: 10.1080/10875549.2018.1517399
Gandy, M. (2006). Planning, anti-planning and the infrastructure crisis facing metropolitan Lagos. Urban Stud. 43, 371–396. doi: 10.1080/00420980500406751
Gebreeyesus, M., Gwenzi, W., Mwamila, T. M., and Noubactep, C. (2025). Mitigating freshwater supply shortages in regions of high demand in Ethiopia: integrated water resources management approach. Environ. Earth Sci. 84:99. doi: 10.1007/s12665-025-12119-1
Goddard, J. J., Ray, I., and Balazs, C. (2021). Water affordability and human right to water implications in California. PLoS One 16:e0245237. doi: 10.1371/journal.pone.0245237
Guetterman, T. C., and Fetters, M. D. (2018). Two Methodological Approaches to the Integration of Mixed Methods and Case Study Designs: A Systematic Review. American Behavioral Scientist, 62, 900–918. doi: 10.1177/0002764218772641
He, W. J., Lai, Y. S., Karmacharya, B. M., Dai, B. F., Hao, Y. T., and Xu, D. R. (2018). Geographical heterogeneity and inequality of access to improved drinking water supply and sanitation in Nepal. Int. J. Equity Health 17:40. doi: 10.1186/s12939-018-0754-8
Hennink, M. M., Kaiser, B. N., and Weber, M. B. (2019). What influences saturation? Estimating sample sizes in focus group research. Qual. Health Res. 29, 1483–1496. doi: 10.1177/1049732318821692
JICA (2022). Sector Position Paper: Water Sector. Lilongwe, JICA. Available at: https://www.jica.go.jp/Resource/malawi/english/activities/c8h0vm00004bpzlh-att/water.pdf
Johnson, C. A., Berg, M., and Sabatini, D. (2014). Towards sustainable safe drinking water supply in low-income and middle-income countries: the challenges of geogenic contaminants and mitigation measures. Sci. Total Environ. 488, 475–489.
Karasaki, S., Goddard, J. J., Cohen, A., and Ray, I. (2023). Environmental justice and drinking water: a critical review of primary data studies. WIREs Water 10:e1653. doi: 10.1002/wat2.1653
Kayser, G. L. (2015). Drinking water quality governance: a comparative case study of Brazil, Ecuador, and Malawi. Environ. Sci. Pol. 48, 186–195. doi: 10.1016/j.envsci.2014.12.019
Kostadinov, I., Daniel, M., and Stanley, L. (2015). Assessing community readiness online: a concurrent validation study. BMC Public Health 15:598. doi: 10.1186/s12889-015-1953-5
Krueger, R., and Casey, M. (2015). Focus groups: A practical guide for applied research. Fifth Edn. Thousand Oaks, CA: Sage Publications.
Kumar, A., Singh, N., Cooper, S., Mdee, A., and Singhal, S. (2021). Infrastructural violence: five axes of inequities in water supply in Delhi, India. Front. Water 3:727368. doi: 10.3389/frwa.2021.727368
Levy, K., Nelson, K. L., Hubbard, A., Joseph, N. S., and Eisenberg, J. N. S. (2008). Following the water: a controlled study of drinking water storage in northern coastal Ecuador. Environ. Health Perspect. 116, 1533–1540. doi: 10.1289/ehp.11296
Longwe, B., Mganga, M., and Sinyiza, N. (2019). Review of sustainable solar powered water supply system design approach by water Mission Malawi. Water Pract. Technol. 14, 749–763. doi: 10.2166/wpt.2019.079
Madomguia, D., Nya, E. L., Njomou-Ngounou, E. L., Gatcha-Bandjun, N., Mwamila, T. B., Balna, J., et al. (2025). Revisiting water resources management in the Mandara Mountains. Heliyon 11:e41692. doi: 10.1016/j.heliyon.2025.e41692
Malawi Government. (1995). Waterworks Act (No. 17 of 1995). Malawi Legal Information Institute (MalawiLII). Available at: https://malawilii.org/akn/mw/1995/17/eng@2014-12-31
Manda, I. K., Manda, I. K. M., Chidya, R. C. G., Saka, J. D. K., and Biswick, T. T. (2016). Comparative assessment of water treatment using polymeric and inorganic coagulants. Phys. Chem. Earth. A, B, C. 93, 119–129. doi: 10.1016/j.pce.2015.09.008
Mann, M. (1984). The autonomous power of the state: its origins, mechanisms and results. Eur. J. Sociol. 25, 185–213. doi: 10.1017/S0003975600004239
Matamanda, A. R., Mphambukeli, T., and Chirisa, I. (2020). Applied systems analysis in water access for emerging human settlements: a case study of Hopley farm, Harare, Zimbabwe. Urban Water J. 17, 763–773. doi: 10.1080/1573062x.2020.1811882
Matimolane, S., Strydom, S., Mathivha, F. I., and Chikoore, H. (2023). Determinants of rainwater harvesting practices in rural communities of Limpopo Province, South Africa. Water Sci. 37, 276–289. doi: 10.1080/23570008.2023.2244784
Mbana, Z., and Sinthumule, N. I. (2024). What is there to drink? Water (in)justice in the democratic South Africa. Front. Water 6:1354477. doi: 10.3389/frwa.2024.1354477
McLean, J. (2007). Water injustices and potential remedies in indigenous rural contexts: a water justice analysis. Environmentalist 27, 25–38. doi: 10.1007/s10669-007-9012-0
Mkandawire, T., Mwathunga, E., MacDonald, A. M., Bonsor, H. C., Banda, S., and Mleta, P. (2020). An analysis of hand pump boreholes functionality in Malawi. Phys. Chem. Earth Parts A B C 119:102897. doi: 10.1016/j.pce.2020.102897
Mkwate, R., Chidya, R., and Wanda, E. (2017). Assessment of drinking water quality and rural household water treatment in Balaka District, Malawi. Phys. Chem. Earth Part A Solid Earth Geod. 100:6. doi: 10.1016/j.pce.2016.10.006
Mokoena, A. M. (2022). The geography of inequality in Cape Town: A case study of access to water in Khayelitsha (master's thesis). Cape Town: University of Cape Town.
Morse, J. (1995). The significance of saturation. Qual. Health Res. 5, 147–149. doi: 10.1177/104973239500500201
National Statistical Office (2017b). Malawi demographic and health survey 2015-16. Zomba: National Statistics Office.
National Statistical Office (2021). Malawi multiple indicator cluster survey 2019-20, survey findings report. Zomba: National Statistics Office.
National Statistics Office (2017a). Malawi integrated household survey 2015 – 2016. Zomba: National Statistics Office.
Neal, M. J., Lukasiewicz, A., and Syme, G. J. (2014). Why justice matters in water governance: some ideas for a water justice framework. Water Policy 16, 1–18. doi: 10.2166/wp.2014.109
Nygren, B. L., O’Reilly, C. E., Rajasingham, A., Omore, R., Ombok, M., and Awuor, A. O. (2016). The relationship between distance to water source and moderate-to-severe diarrhea in the global Enterics multi-center study in Kenya, 2008–2011. Am. J. Trop. Med. Hyg. 94, 1143–1149. doi: 10.4269/ajtmh.15-0393
Osiemo, M. M., Ogendi, G. M., and M'Erimba, C. (2019). Microbial quality of drinking water and prevalence of water-related diseases in Marigat Urban Centre, Kenya. Environ. Health Insights 13:1178630219836988. doi: 10.1177/1178630219836988
Othoo, C. O., Dulo, S., Olago, D., and Ayah, R. (2020). Proximity density assessment and characterization of water and sanitation facilities in the informal settlements of Kisumu City: implications for public health planning. J. UOEH 42, 237–249. doi: 10.7888/juoeh.42.237
Pickering, A. J., and Davies, J. (2012). Freshwater availability and water fetching distance affect child health in sub–Saharan Africa. Environ. Sci. Technol. 46, 2391–2397. doi: 10.1021/es203177v
Qi, Q., Marwa, J., Mwamila, T. B., Gwenzi, W., and Noubactep, C. (2019). Making rainwater harvesting a key solution for water supply: the universality of the Kilimanjaro concept. Sustain. For. 11:5606. doi: 10.3390/su11205606
Reimers, M., and Klasen, S. (2013). Revisiting the role of education for agricultural productivity. Am. J. Agric. Econ. 95, 131–152. doi: 10.1093/ajae/aas118
Rodgers, D., and O’Neill, B. (2012). Infrastructural violence: introduction to the special issue. Ethnography 13, 401–412. doi: 10.1177/1466138111435738
Rodrigues-Silveira, R. (2019). Public policy provision from a subnational perspective: context, institutions and spatial inequality. Reg. Fed. Stud. 29, 275–294. doi: 10.1080/13597566.2019.1566125
Routray, P., Torondel, B., Clasen, T., and Schmidt, W. P. (2017). Women’s role in sanitation decision making in rural coastal Odisha, India. PLoS One 12:e0178042. doi: 10.1371/journal.pone.0178042
Rusca, M., Alda-Vidal, C., Hordijk, M., and Kral, N. (2017). Bathing without water, and other stories of everyday hygiene practices and risk perception in urban low-income areas: the case of Lilongwe, Malawi. Environ. Urban. 29, 533–550. doi: 10.1177/0956247817700291
Sharan, A. (2006). In the city, out of place: environment and modernity, Delhi 1860s to 1960s. Econ. Polit. Wkly. 41, 4905–4911.
Stock, R. (2022). Triggering resistance: contesting the injustices of solar park development in India. Energy Res. Soc. Sci. 86:102464. doi: 10.1016/j.erss.2021.102464
Subbaraman, R., Shitole, S., Shitole, T., Sawant, K., O’Brien, J., Bloom, D. E., et al. (2013). The social ecology of water in a Mumbai slum: failures in water quality, quantity, and reliability. BMC Public Health 13:173. doi: 10.1186/1471-2458-13-173
Sultana, F. (2018). Water justice: why it matters and how to achieve it. Water Int. 43, 483–493. doi: 10.1080/02508060.2018.1458272
Sung, C. H., and Liaw, S. C. (2020). A GIS approach to analyzing the spatial pattern of baseline resilience indicators for community (BRIC). Water 12:1401. doi: 10.3390/w12051401
Suri, M., Cebecauer, T., Suriova, N., Schnierer, B., Betak, J., and Skoczek, A. (2015). Solar resource mapping in Malawi: Solar modeling report. Washington, DC: The Bank Group & ESMAP.
Terefe, B., Jembere, M. M., and Assimamaw, N. T. (2024). Access to drinking safe water and its associated factors among households in East Africa: a mixed effect analysis using 12 east African countries recent national health survey. J. Health Popul. Nutr. 43:72. doi: 10.1186/s41043-024-00562-y
Trevett, A. F., Carter, R. C., and Tyrrel, S. F. (2005). The importance of domestic water quality management in the context of fecal-oral disease transmission. J. Water Health 3, 259–270. doi: 10.2166/wh.2005.037
Tiwale, S., Rusca, M., and Zwarteveen, M. (2018). The power of pipes: mapping urban water inequities through the material properties of networked water infrastructures - the case of Lilongwe, Malawi. Water Alternatives 11, 314–335.
Tuyet-Hanh, T. T., Lee, J.-K., Oh, J., Van Minh, H., Ou Lee, C., Hoan, L. T., et al. (2016). Household trends in access to improved water sources and sanitation facilities in Vietnam and associated factors: findings from the multiple Indicator cluster surveys, 2000–2011. Glob. Health Action 9:29434. doi: 10.3402/gha.v9.29434
UN (2010). Human right to water and sanitation. UN document a/RES/64/292. New York, NY: United Nations.
UNICEF (2020). Scaling-Up Climate Resilient Sustainable Solar-Powered Systems for Institutions and Communities in Rural Malawi. Lilongwe, UNICEF. Available at: https://www.unicef.org/malawi/media/2741/file/Scaling-Up%20Climate%20Resilient%20Sustainable%20Solar-Powered%20Systems%20for%20Institutions%20and%20Communities%20in%20Rural%20Malawi%20.pdf
UNICEF (2023). Global Annual Results Report 2023: Goal Area 4 Every child lives in a safe and clean environment. New York: UNICEF. Available at: https://www.unicef.org/media/161361/file/UNICEF%202023%20GARR%20Goal%20Area%204%20Chapter.pdf.pdf
WHO and UNICEF (2017). Progress on drinking water, sanitation and hygiene: 2017 update and SDG baselines. Geneva: World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF).
WHO and UNICEF (2021). Progress on household drinking water, sanitation and hygiene 2000–2020: Five years into the SDGs. Geneva: WHO/UNICEF.
WHO and UNICEF (2022). Progress on household drinking water, sanitation, and hygiene in Africa: 2000 – 2022. Geneva: WHO and UNICEF.
Wong, L. (2008). Data analysis in qualitative research: a brief guide to using NVivo. Off. J. Acad. Family Phys Malaysia. 3, 14–20.
World Bank (2017). Solar resource mapping in Malawi: Annual solar resource report. Energy sector management assistance program. Washington, D.C: World Bank Group.
Yannopoulos, S., Antoniou, G., Kaiafa-Saropoulou, M., and Angelakis, A. N. (2017). Historical development of rainwater harvesting and use in Hellas: a preliminary review. Water Science and Technology: Water Supply 17, 1022–1034. doi: 10.2166/ws.2016.200
Keywords: drinking water services coverage, Malawi, rural–urban divide, sustainable development, access equity, water justice, infrastructure violence
Citation: Chimombo MJ (2025) Bridging the divide: analysing disparities in drinking water services between urban and rural areas in Lilongwe, Malawi—implications for water justice and infrastructure equity. Front. Water. 7:1615202. doi: 10.3389/frwa.2025.1615202
Edited by:
Yongping Wei, The University of Queensland, AustraliaReviewed by:
Chicgoua Noubactep, University of Göttingen, GermanyPriscila Neves Silva, Oswaldo Cruz Foundation, Brazil
Catarina Fonseca, IRC International Water and Sanitation Centre, Netherlands
Copyright © 2025 Chimombo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Masautso Joseph Chimombo, Y2hpbW9tYm9tYXNhQGdtYWlsLmNvbQ==