 Laurence Pacot1
Laurence Pacot1 Jacques Pouchot2Nicolas De Prost3
Jacques Pouchot2Nicolas De Prost3 Marie Senant1,4
Marie Senant1,4 Eric Tartour1,4Françoise Le Pimpec-Barthes5Dominique Israel-Biet4,6
Eric Tartour1,4Françoise Le Pimpec-Barthes5Dominique Israel-Biet4,6 Marie-Agnes Dragon-Durey1,4*†
Marie-Agnes Dragon-Durey1,4*†- 1Service d'Immunologie Biologique, Hôpital Européen Georges Pompidou, Paris, France
- 2Service de Médecine Interne, Hôpital Européen Georges Pompidou, Paris, France
- 3Service de Réanimation Médicale, Hôpital Henri Mondor, Créteil, France
- 4Université Paris-Descartes, Paris, France
- 5Service de Chirurgie Thoracique, Hôpital Européen Georges Pompidou, Paris, France
- 6Service de Pneumologie, Hôpital Européen Georges Pompidou, Paris, France
Two patients presented simultaneously to our hospital with distinct clinical features associated with the presence of anti-MDA5 antibodies: the first one was admitted for a skin rash resembling to a toxic epidermal necrosis (Lyell syndrome) and the second one presented with pulmonary manifestations attributed to a diffuse fibrosing interstitial pneumonitis on chest CT-scan. In addition to the skin lesions involving 40% of the body surface area, the first patient developed a rapid diffuse interstitial pneumonitis with respiratory distress justifying the initiation of a systemic immunosuppressive treatment. However, she died 3 weeks after her admission from mesenteric thrombosis associated with septic shock. The second patient respiratory condition worsened despite an intensive immunosuppressive treatment with high doses of intravenous methylprednisolone and cyclophosphamide and plasmapheresis, and required lung transplantation. Anti-MDA5 antibody titer declined and disappeared on anti-rejection treatment. These two cases underline the diagnostic conundrum and the therapeutic difficulties in patients with anti-MDA5 antibodies and clinically amyopathic dermatomyositis (CADM) or interstitial lung disease (ILD), who may undergo rapidly-progressive and fatal outcome. Presence of anti-MDA5 antibodies should always be suspected when confronted to CADM patients with cutaneous ulcerations or ILD to allow a rapid and adapted treatment initiation.
Background
Polymyositis/dermatomyositis (PM/DM) are systemic inflammatory myopathies which involve skeletal muscles, skin and possibly other organs like joints and lung. Annual incidence of PM/DM is ~8.5 per million (1). In its clinically amyopathic form (CADM), which represents ~20% of all DM (2), the disease is mostly characterized by cutaneous lesions such as ulcerations, palm papules or Gottron's sign that persist for more than 6 months without sign of muscle weakness (Sontheimer criteria). Incidence of PM/DM-related interstitial lung diseases (ILD) ranges from 5 to 65%, depending on whether clinical, radiological, functional or histological criteria are used (3). Among these patients the presence of anti-synthetase antibodies seems to be of a relatively good prognosis (4, 5) whereas mortality rates can be high in other autoimmune-related ILD, with a poor response to immunosuppressive therapy, particularly in CADM-ILD. In 2005, Sato and collaborators described for the first time an antibody recognizing a 140 kDa protein (anti-CADM-140 antibodies) which was associated with CADM in Asian patients, who tended to develop rapidly-progressive ILD (RP-ILD) (6). They later on identified this 140 kDa protein as being melanoma differentiation–associated gene 5 (MDA5) (7), a protein implicated in long double-strand RNA recognition, notably picornaviruses RNAs, that activates the interferon signaling pathway through the adaptor molecule MAVS (8).
Since then, many studies have confirmed that anti-MDA5 antibodies are most frequently detected in CADM patients, representing up to 50–73% of CADM (2), and are often associated with ILD (9). Moreover, skin ulcerations are more frequent and severe in anti-MDA5 positive patients than in DM/CADM patients without anti-MDA5 antibodies (10).
We here report on two Caucasian patients, positive for anti-MDA5 antibodies, who were simultaneously admitted to the same hospital, with distinct clinical features.
Case Presentation
Case #1
A 59-year-old woman presenting with facial erythema and polyarthralgia was diagnosed with rheumatoid arthritis and treated by methotrexate (Figure 1). She rapidly developed hepatic cytolysis that persisted after a switch to hydroxychloroquine. Three months later, she developed vesicles and pustules on the shoulders, which firstly responded to a local corticosteroid treatment. The appearance of large cutaneous erosions on the back, chest, arms and the legs and necrotic skin lesions over the elbows and the ankles one month later led to suspect a Lyell syndrome, justifying her admission in the hospital. Cutaneous lesions of this patient have previously been described in a short letter (11). Her past medical history included a splenectomy for idiopathic thrombocytopenic purpura at the age of 37 years, an allergic asthma and a nasal polyposis.
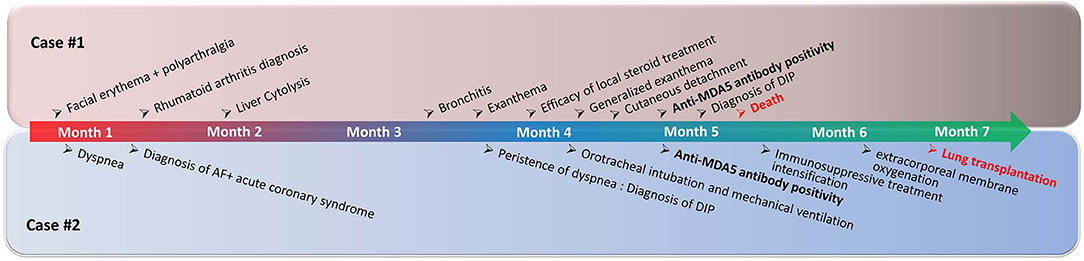
Figure 1. Chronological representation of the main clinical data of Case #1 (top) and Case #2 (bottom). AF, Atrial fibrillation; DIP, diffuse interstitial pneumonitis.
At the time of diagnosis, the patient showed anemia and moderate hepatic cytolysis (Table 1). Presence of antinuclear antibodies (ANA) was revealed by indirect immunofluorescence (IIF) on Hep-2 cells (Euroimmun©, Germany) with the association of a homogenous staining, multiple nuclear dots pattern, anti-Golgi apparatus pattern, and rare isolated cytoplasmic islets positivity (Figure 2). Antigenic specificity was studied by immunodots (Euroimmun©, Autoimmune Inflammatory Myopathies and Autoimmune Hepatopathies, Germany) using the systems EUROBlotMaster and EUROLineScan (Euroimmun©, Germany), and revealed high levels of anti-MDA5 (with an intensity of the antigen band superior to 10-fold the positive threshold), anti-SSA 52 (Trim 21) and anti-Sp-100 autoantibodies.
Table 1. Biological findings at diagnosis.
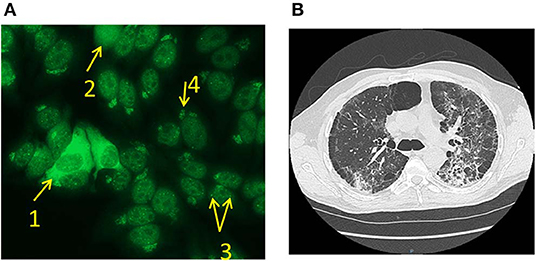
Figure 2. (A) ANA aspect of Case #1. IIF on Hep-2 (1/80) revealed presence of rare isolated cytoplasmic islets (1), homogenous staining (2), multiple nuclear dots pattern (3) and anti-Golgi apparatus pattern (4). (B) Radiographic imaging of Case #2. Thoracic computed tomography scan revealed bilateral interstitial lung disease with lower lung predominance, thickened alveolar septa, condensations, and traction bronchiectasis.
During the time of her hospitalization, the cutaneous erosions spread rapidly and reached 40% of the body surface. Because of a concomitant respiratory distress, a systemic immunosuppressive treatment with 500 mg/day of methylprednisolone for 3 days was initiated, followed by 1.5 mg/kg of prednisone per day and one pulse of 0.6 g/m2 of cyclophosphamide. Despite this treatment, a diffuse interstitial pneumonitis rapidly developed, followed by a mesenteric thrombosis with multiple organ failure and a septic shock. The patient ultimately died from a systemic infection, 3 weeks only after diagnosis.
Case #2
A 51-year-old man presented with dyspnea associated with atrial fibrillation and an acute coronary syndrome treated by angioplasty (Figure 1). His past medical history revealed a 45 pack-year smoking and dyslipidemia. As the dyspnea persisted, a lung CT-scan showed a diffuse fibrosing interstitial pneumonitis (Figure 2). Immunological analysis revealed only very rare cytoplasmic islets positivity in IIF and anti-MDA5 associated with anti-SSA 52 antibodies were detected.
After 5 days of bolus corticosteroids (500 mg) with only modest impact on respiratory distress, he received a first pulse of intravenous cyclophosphamide (600 mg/m2) associated with 1 mg/kg of oral corticosteroids then, 3 days afterwards, five sessions of plasmapheresis combined with 4 mg/kg/d of ciclosporin. A second pulse of cyclophosphamide was performed at D25 with a continued treatment with 400 mg/d of ciclosporin and 20 mg/d of corticosteroids. Respiratory failure required an extracorporeal membrane oxygenation (ECMO) as a bridge to lung transplantation which was performed 7 weeks after diagnosis. Post-transplantation treatment included 1,500 mg of mycophenolate and 11 mg of tacrolimus twice a day, together with 1,000 mg of intravenous methylprednisolone. Since transplantation, the immunological monitoring has showed no reappearance of anti-MDA5 antibodies after 20 weeks of antirejection treatment and a slow normalization of ferritinemia, measured on DxI800 (Beckman-Coulter©, France), was observed (Figure 3). Three years after lung transplantation, the patient is alive.
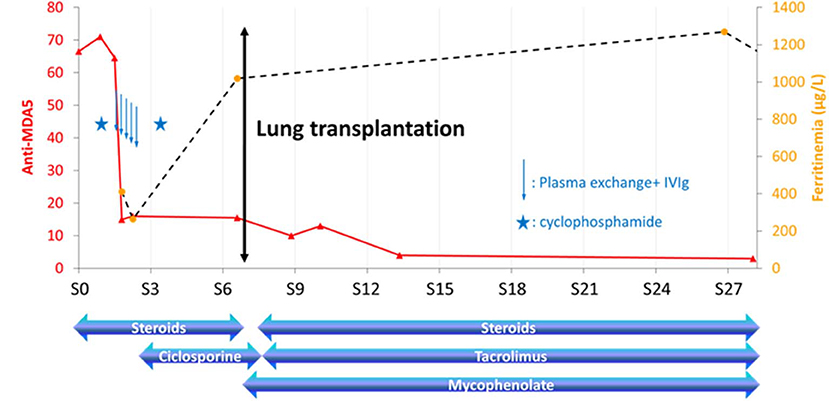
Figure 3. Biological follow-up and treatment of Case #2. The full curve represents the regression of anti-MDA5 antibodies titers (expressed as relative intensity) and the dotted curve the evolution of serum ferritin level. Five plasma exchanges were performed (arrows), preceded and followed by cyclophosphamide infusions (depicted with stars). MDA5, melanoma differentiation–associated gene 5.
Discussion
The cutaneous manifestations of dermatomyositis and clinically amyopathic dermatomyositis include Gottron papules, Gottron sign, which are almost pathognomonic of these pathologies, periorbital heliotrope erythema, periungual telangiectasias and photodistributed erythema or poikiloderma (12). The occurrence of skin ulcerations, which affect 3–19% of DM patients (13), is more frequently observed in CADM patients than in DM patients (12), especially when associated with anti-MDA5 antibodies (13, 14). In this latter form of CADM, cutaneous ulcerations may overlie Gottron papules over the digital pulp and periungual areas or Gottron sign over the elbows and knees, and may more generally develop on sun-exposed sites, such as chest, back, and arms. Vasculopathy may be a major actor in the development of such ulcerations (10). The other classical clinical features of anti-MDA5 positive patients include palmar papules, alopecia, painful oral ulcers, panniculitis, mechanic hands, arthritis, arthralgias, fever, and ILD (10, 13, 14). Biological findings may include lymphopenia and elevated levels of ferritin, erythrocyte sedimentation rate and interleukin 18 (12, 14) with no increase in serum creatinine kinase (CK). Our first patient indeed presented with fever and arthralgias and developed oropharyngeal ulcerations and ulcerative and necrotic lesions over the limbs with large skin erosions before the diagnosis of diffuse interstitial pneumonitis. Furthermore, she died of septic shock following mesenteric thrombosis, and polymyositis/dermatomyositis patients have an increased risk of venous thromboembolism (15). The mechanisms underlying this pro-thrombotic condition are still largely unknown but may be at least partially explained by a hypercoagulability state due to systemic inflammation in PM/DM patients (16). Concerning CK dosage, the first patient had a transient increase up to 4,100 U/L with an electromyogram compatible with a myogenic syndrome. Case #2 had normal CK levels.
ILD is frequently observed early in the disease course of PM/DM patients when using imaging even though respiratory symptoms may be absent (1). Its prognosis is particularly severe in CADM-ILD associated with anti-MDA5 antibodies (4, 5, 7) where it often progresses toward a rapidly progressive fibrosing ILD leading to respiratory failure despite intensive immunosuppression. Only few cases of lung transplantation have been reported in the context of dermatomyositis, often regarded as a contra-indication in these patients. Shoji et al. reported the case of a female patient with a rapidly progressive ILD associated with anti-MDA-5 antibodies that underwent successful lung transplantation after an intensive immunosuppressive therapy including cyclophosphamide and intravenous immunoglobulins (17). Other similar cases have been reported since then, with favorable outcomes (18, 19). Like our two patients, at least one of them had anti-SSA 52 antibodies (18), which are frequently associated with anti-MDA5 antibodies (10) and seem to be correlated with severe forms of ILD (2, 20). As illustrated by our patient #2, some cases may present with RP-ILD and poor or no cutaneous, articular or muscle involvement (2, 21), making diagnosis even more tricky and may delay proper support.
Some biological parameters have been evaluated as potential predictive markers of outcome in anti-MDA5 positive patients. Serum ferritin level has been proposed as a predictor of RP-ILD (when ≥217 ng/mL) and fatal outcome (when ≥828 ng/mL) in these patients (22). This study also revealed that anti-MDA5 antibody titers and IL-18 levels decreased significantly after treatment in the RP-ILD patients who survived, meaning that sustained high levels or reappearance of these parameters represent potential biomarkers of unfavorable outcome or relapse in RP-ILD patients with positive anti-MDA5 antibodies (23). Anti-MDA5 antibody levels are also correlated to the severity of skin ulcerations and ILD, as well as with acute/subacute vs. chronic form of the lung disease, with a cutoff at 500 units/mL (9). However, this threshold has to be calculated for each anti-MDA5 assay due to a lack of standardization. The detection of anti-MDA5 antibodies among DM-associated ILD might be a keystone to anticipate resistance to treatment and survival, as anti-MDA5-positive patients who exhibit initial response to treatment achieve long-term survival (4).
There is currently no consensus on the best treatment of anti-MDA5 positive patients with RP-ILD. Treatments targeting B-cell functions, like the chimeric monoclonal anti-CD20 antibody rituximab, have shown some efficiency by reducing the production of anti-MDA5 antibodies (24). However, such molecules considerably increase the infectious risk. On the other hand, plasma exchanges represent a reasonable alternative for refractory cases, though adverse events such as allergy cannot be predicted (25). Altogether, combined immunosuppressive therapies, possibly by adjunction of mycophenolate and/or tacrolimus, give promising results (26). Large prospective studies are still lacking to identify the optimal treatment in anti-MDA5 positive patients with RP-ILD, but the scarcity of such patients will most likely require the set-up of multicenter clinical trials.
In the two patients presented here, the diagnostic delay was about 4 months. Because of its unique clinical presentation and very discrete aspect in IIF, most often described as negative in ANA (10), anti-MDA5-associated-DM is still a diagnostic challenge and its prevalence is probably underestimated. Patients often exhibit mild to absent increase of muscle enzymes, concordant with the amyopathic form of the disease.
The two cases described here exemplify the difficulties of diagnosing and treating patients with anti-MDA5 positive DM or ILD, who may undergo rapidly-progressive and fatal outcome. Anti-MDA5 antibodies must be suspected in CADM patients with cutaneous ulcerations or ILD to allow rapid treatment initiation.
Ethics Statement
This study was performed in accordance with the Helsinki Declaration as revised in 2013 and Good Clinical Practice guidelines. It has been approved by the Institutional Review Board according to standards currently applied in France (Commission Nationale de l'Informatique et des Libertés, CNIL N°1922081 from 02/02/2016). Written informed consent was obtained from the participants or from their relatives for the use of their social and medical data for publication of this case report.
Author Contributions
LP, MS, ET, and M-AD-D performed the biological analysis and wrote the manuscript. JP, ND, FL, and DI-B took care of the patients and wrote the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Fathi M. Interstitial lung disease, a common manifestation of newly diagnosed polymyositis and dermatomyositis. Ann Rheum Dis. (2004) 63:297–301. doi: 10.1136/ard.2003.006122
2. Ortiz-Santamaria V, Babot A, Ferrer C. Anti-MDA5-positive dermatomyositis: an emerging entity with a variable clinical presentation. Scand J Rheumatol. (2017) 46:509–11. doi: 10.1080/03009742.2017.1340512
3. Arboleda R, Gonzalez O, Cortes M, Perez-Cerda F. Recurrent polymyositis-associated lung disease after lung transplantation. Interact Cardiovascular Thorac Surg. (2015) 20:560–2. doi: 10.1093/icvts/ivu423
4. Hozumi H, Fujisawa T, Nakashima R, Johkoh T, Sumikawa H, Murakami A, et al. Comprehensive assessment of myositis-specific autoantibodies in polymyositis/dermatomyositis-associated interstitial lung disease. Respir Med. (2016) 121:91–9. doi: 10.1016/j.rmed.2016.10.019
5. Chen F, Li S, Wang T, Shi J, Wang G. Clinical heterogeneity of interstitial lung disease in polymyositis and dermatomyositis patients with or without specific autoantibodies. Am J Med Sci. (2018) 355:48–53. doi: 10.1016/j.amjms.2017.07.013
6. Sato S, Hirakata M, Kuwana M, Suwa A, Inada S, Mimori T, et al. Autoantibodies to a 140-kd polypeptide, CADM-140, in Japanese patients with clinically amyopathic dermatomyositis. Arthritis Rheum. (2005) 52:1571–6. doi: 10.1002/art.21023
7. Sato S, Hoshino K, Satoh T, Fujita T, Kawakami Y, Fujita T, et al. RNA helicase encoded by melanoma differentiation-associated gene 5 is a major autoantigen in patients with clinically amyopathic dermatomyositis: association with rapidly progressive interstitial lung disease. Arthritis Rheum (2009) 60:2193–200. doi: 10.1002/art.24621
8. del Toro Duany Y, Wu B, Hur S. MDA5—filament, dynamics and disease. Curr Opin Virol. (2015) 12:20–5. doi: 10.1016/j.coviro.2015.01.011
9. Cao H, Pan M, Kang Y, Xia Q, Li X, Zhao X, et al. Clinical manifestations of dermatomyositis and clinically amyopathic dermatomyositis patients with positive expression of anti-melanoma differentiation-associated gene 5 antibody. Arthritis Care Res. (2012) 64:1602–10. doi: 10.1002/acr.21728
10. Fiorentino D, Chung L, Zwerner J, Rosen A, Casciola-Rosen L. The mucocutaneous and systemic phenotype of dermatomyositis patients with antibodies to MDA5 (CADM-140): a retrospective study. J Am Acad Dermatol. (2011) 65:25–34. doi: 10.1016/j.jaad.2010.09.016
11. Dumas M, Hua C, Hotz C, Velter C, Duong TA, Maraffi T, et al. Epidermal necrolysis and autoimmune diseases: two more observations supporting the concept that ‘toxic' epidermal necrolysis can be ‘non-toxic'. J Eur Acad Dermatol Venereol. (2018) 32:e360–1. doi: 10.1111/jdv.14935
12. Cao H, Xia Q, Pan M, Zhao X, Li X, Shi R, et al. Gottron papules and gottron sign with ulceration: a distinctive cutaneous feature in a subset of patients with classic dermatomyositis and clinically amyopathic dermatomyositis. J Rheumatol. (2016) 43:1735–42. doi: 10.3899/jrheum.160024
13. Narang NS, Casciola-Rosen L, Li S, Chung L, Fiorentino DF. Cutaneous ulceration in dermatomyositis: association with anti-melanoma differentiation-associated gene 5 antibodies and interstitial lung disease. Arthritis Care Res. (2015) 67:667–72. doi: 10.1002/acr.22498
14. Kurtzman DJB, Vleugels RA. Anti-melanoma differentiation-associated gene 5 (MDA5) dermatomyositis: a concise review with an emphasis on distinctive clinical features. J Am Acad Dermatol. (2018) 78:776–85. doi: 10.1016/j.jaad.2017.12.010
15. Lee YH, Song GG. Idiopathic inflammatory myopathy and the risk of venous thromboembolism: a meta-analysis. Rheumatol Int. (2017) 37:1165–73. doi: 10.1007/s00296-017-3735-0
16. Li Y, Wang P, Li L, Wang F, Liu Y. Increased risk of venous thromboembolism associated with polymyositis and dermatomyositis: a meta-analysis. Ther Clin Risk Manag. (2018) 14:157–65. doi: 10.2147/TCRM.S157085
17. Shoji T, Bando T, Fujinaga T, Chen F, Sasano H, Yukawa N, et al. Living-donor lobar lung transplantation for rapidly progressive interstitial pneumonia associated with clinically amyopathic dermatomyositis: report of a case. Gen Thor Cardiovasc Surg. (2013) 61:32–4. doi: 10.1007/s11748-012-0106-3
18. Leclair V, Labirua-Iturburu A, Lundberg IE. Successful lung transplantation in a case of rapidly progressive interstitial lung disease associated with antimelanoma differentiation-associated gene 5 antibodies. J Rheumatol. (2018) 45:581–3. doi: 10.3899/jrheum.171047
19. Deitchman AR, Kalchiem-Dekel O, Todd N, Reed RM. Rapidly progressive interstitial lung disease due to anti-melanoma differentiation associated protein-5 requiring a bilateral lung transplant, and complicated by kennel cough. Respir Med Case Rep. (2019) 28:100886. doi: 10.1016/j.rmcr.2019.100886
20. Huang K, Vinik O, Shojania K, Yeung J, Shupak R, Nimmo M, et al. Clinical spectrum and therapeutics in Canadian patients with anti-melanoma differentiation-associated gene 5 (MDA5)-positive dermatomyositis: a case-based review. Rheumatol Int. (2019) 39:1971–81. doi: 10.1007/s00296-019-04398-2
21. Sakamoto N, Ishimoto H, Nakashima S, Yura H, Miyamura T, Okuno D, et al. Clinical features of anti-MDA5 antibody-positive rapidly progressive interstitial lung disease without signs of dermatomyositis. Intern Med. (2019) 58:837–41. doi: 10.2169/internalmedicine.1516-18
22. Gono T, Sato S, Kawaguchi Y, Kuwana M, Hanaoka M, Katsumata Y, et al. Anti-MDA5 antibody, ferritin and IL-18 are useful for the evaluation of response to treatment in interstitial lung disease with anti-MDA5 antibody-positive dermatomyositis. Rheumatology. (2012) 51:1563–70. doi: 10.1093/rheumatology/kes102
23. Matsushita T, Mizumaki K, Kano M, Yagi N, Tennichi M, Takeuchi A, et al. Antimelanoma differentiation-associated protein 5 antibody level is a novel tool for monitoring disease activity in rapidly progressive interstitial lung disease with dermatomyositis. Br J Dermatol. (2017) 176:395–402. doi: 10.1111/bjd.14882
24. So H, Wong VTL, Lao VWN, Pang HT, Yip RML. Rituximab for refractory rapidly progressive interstitial lung disease related to anti-MDA5 antibody-positive amyopathic dermatomyositis. Clin Rheumatol. (2018) 37:1983–9. doi: 10.1007/s10067-018-4122-2
25. Abe Y, Kusaoi M, Tada K, Yamaji K, Tamura N. Successful treatment of anti-MDA5 antibody-positive refractory interstitial lung disease with plasma exchange therapy. Rheumatology. (2019) kez357. doi: 10.1093/rheumatology/kez357
26. Hoa S, Troyanov Y, Fritzler MJ, Targoff IN, Chartrand S, Mansour AM, et al. Describing and expanding the clinical phenotype of anti-MDA5-associated rapidly progressive interstitial lung disease: case series of nine Canadian patients and literature review. Scand J Rheumatol. (2018) 47:210–24. doi: 10.1080/03009742.2017.1334814
Keywords: autoantibodies, dermatomyositis, skin rash, interstitial lung disease, anti-rejection therapy, lung transplantation, anti-MDA5
Citation: Pacot L, Pouchot J, De Prost N, Senant M, Tartour E, Le Pimpec-Barthes F, Israel-Biet D and Dragon-Durey M-A (2020) Interstitial Lung Disease-Complicated Anti-MDA5 Antibody in Clinically Amyopathic Dermatomyositis Patients: Report of Two Cases With Distinct Clinical Features. Front. Med. 7:77. doi: 10.3389/fmed.2020.00077
Received: 02 December 2019; Accepted: 25 February 2020;
Published: 10 March 2020.
Edited by:
Hsiao-Chi Chuang, Taipei Medical University, TaiwanReviewed by:
Le Thuong Vu, Ho Chi Minh City Medicine and Pharmacy University, VietnamNaoki Iwamoto, Nagasaki University Hospital, Japan
Copyright © 2020 Pacot, Pouchot, De Prost, Senant, Tartour, Le Pimpec-Barthes, Israel-Biet and Dragon-Durey. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marie-Agnes Dragon-Durey, bWFyaWUtYWduZXMuZHVyZXlAYXBocC5mcg==
†ORCID: Marie-Agnes Dragon-Durey orcid.org/0000-0002-5809-8122