 Pascale Nicaise-Roland1,2Vanessa Granger1,3
Pascale Nicaise-Roland1,2Vanessa Granger1,3 Angèle Soria4,5
Angèle Soria4,5 Annick Barbaud6
Annick Barbaud6 Marc Pallardy3
Marc Pallardy3 Sylvie Chollet-Martin1,3*†
Sylvie Chollet-Martin1,3*† Luc de Chaisemartin1,3,†
Luc de Chaisemartin1,3,†
- 1Service d’Immunologie Biologique, Hôpital Bichat, DMU BIOGÉM, APHP, Paris, France
- 2Université Paris Cité, Inserm PHERE, Paris, France
- 3Université Paris-Saclay, Inserm, Inflammation Microbiome Immunosurveillance, Orsay, France
- 4Département de Dermatologie et Allergologie, Sorbonne Université, Hôpital Tenon, Paris, France
- 5Centre D'immunologie et des Maladies Infectieuses - Paris (Cimi-Paris), INSERM, Paris, France
- 6Département de Dermatologie et Allergologie, Sorbonne Université, INSERM, Institut Pierre Louis D'Epidémiologie et de Santé Publique, AP-HP. Sorbonne Université, Hôpital Tenon, Paris, France
Soon after the release of the new anti-COVID mRNA vaccines, reports came in from the US and the UK of anaphylactic reactions. Fueled by the necessary caution toward these new vaccine platforms, these reports had a great impact and were largely commented upon in the scientific literature and global media. The current estimated frequency is of 5 cases per million doses. Very little biological data are presented in the literature to support the anaphylaxis diagnosis in these patients in addition to skin tests. Allergic reactions to vaccines are rare and mostly due to vaccine excipient. Therefore, the poly-ethylene-glycol (PEG) present in both mRNA formulation, and already known to be immunogenic, was soon suspected to be the potential culprit. Several hypersensitivity mechanisms to PEG or to other vaccine components can be suspected, even if the classical IgE-dependent anaphylaxis seems to be one of the most plausible candidates. In the early 2022, the international guidelines recommended to perform skin prick tests and basophil activation tests (BAT) in people experiencing allergic reaction to the first dose of COVID-19 vaccine or with a history of PEG allergy. The aim of this review is to discuss the main potential mechanisms of immediate allergy to COVID19 vaccines based on published data, together with the various techniques used to confirm or not sensitization to one component.
Introduction
In the context of COVID-19 pandemic, several vaccines have been developed in a few months, and the number of companies involved in vaccine development is increasing. These vaccines are presented in Table 1. Their effectiveness in reducing severe cases is remarkable. However, the existence of adverse events in particular potential allergic reactions has been rapidly reported. Indeed, severe immediate allergic reactions to the COVID-19 vaccines were described very early after the beginning of vaccination in the United States and the United Kingdom, and then all over the world. The more recent reports estimate that anaphylaxis cases for both Pfizer BNT162b2 and Moderna mRNA-1273 vaccines exhibit an estimated frequency of 11.1 to 12.4 and 2.5 to 20.4 cases per million doses administered, respectively (1, 2). Altogether, the number of doses given in the European Union as of June 2022 are the following : 649 million of Comirnaty, 155 millions of Spikevax, 69 millions of Vaxevria, 19 millions of Jcovden and 216,000 of Novavax. The existence of poorly understood severe reactions indirectly contributed to limiting vaccine access by fueling some reluctance to vaccination in the early 2021. To address this issue, a better knowledge of these reactions and of their mechanisms was urgently needed and led to several studies. Beside the identification of the mechanism(s) involved in allergic reactions, the identification of the culprit allergen(s) has also been evaluated.
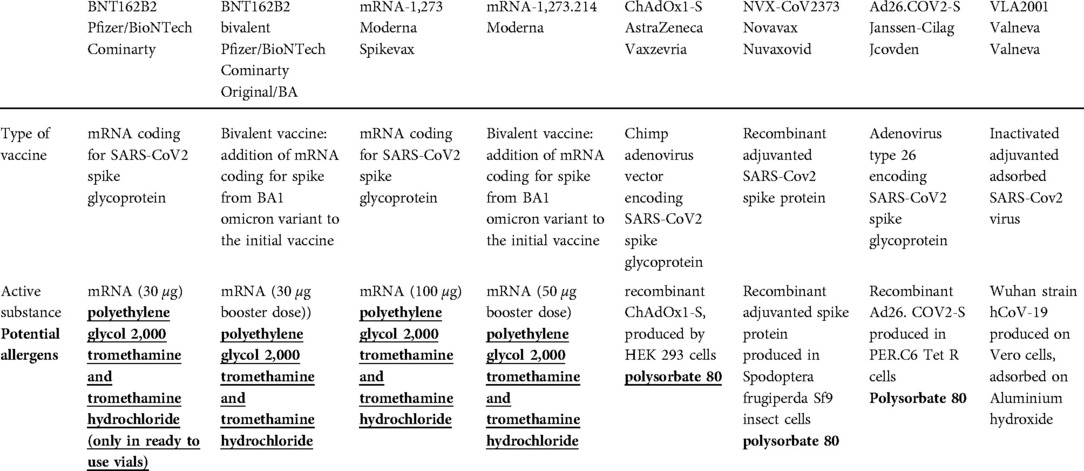
Table 1. Composition of the vaccines approved by the European medical agency (potential allergens in bold).
The mechanisms of drug-induced anaphylaxis can be immunological, involving IgE-mediated basophil and mast cell activation, or IgG-mediated with activation of neutrophils and possibly monocytes and platelets; in other cases, it mainly relies on pharmacological activation of mast cells via complement activation or engagement of MRGPRX2 (3). All these pathways have been investigated in COVID-19 vaccine-induced anaphylaxis by preliminary studies, sometimes controversial, that will be discussed in the present review. These recent information on the potential immediate hypersensitivity mechanisms led to the establishment of clinical (skin testing) and biological guidelines to (1) evaluate the risk of a second vaccine dose and propose a safe alternative for at-risk patients, and (2) identify at-risk patients with an history of a previous allergic reaction to one of the vaccine components.
Beside these immediate hypersensitivity reactions, some delayed reactions have been reported in less than 0.3% which were mostly mild and did not contraindicate subsequent vaccinations (4). These reactions will not be discussed in this review.
Potential mechanisms of COVID 19 vaccine-induced immediate hypersensitivity
The hypotheses regarding the mechanisms of anaphylactic reactions induced by mRNA vaccination against SARS-CoV-2 are multiple, and probably correspond, at least in part, to the classic mechanisms of drug anaphylaxis (5). Moreover, their rate is close the anaphylaxis rate to other vaccines (6). The first hypothesis is an IgE- or IgG-dependent mechanism linked to the presence of allergenic substance(s) in these vaccines which implies prior exposure and sensitization. However, the clinical reactions could also be linked to pseudo-allergic phenomena such as complement activation (complement activation-related pseudo-allergy or CARPA) without prior exposure, or the Mas-related G protein Receptor X2 receptor (MRGPRX2) engagement (7, 8) (Figure 1).
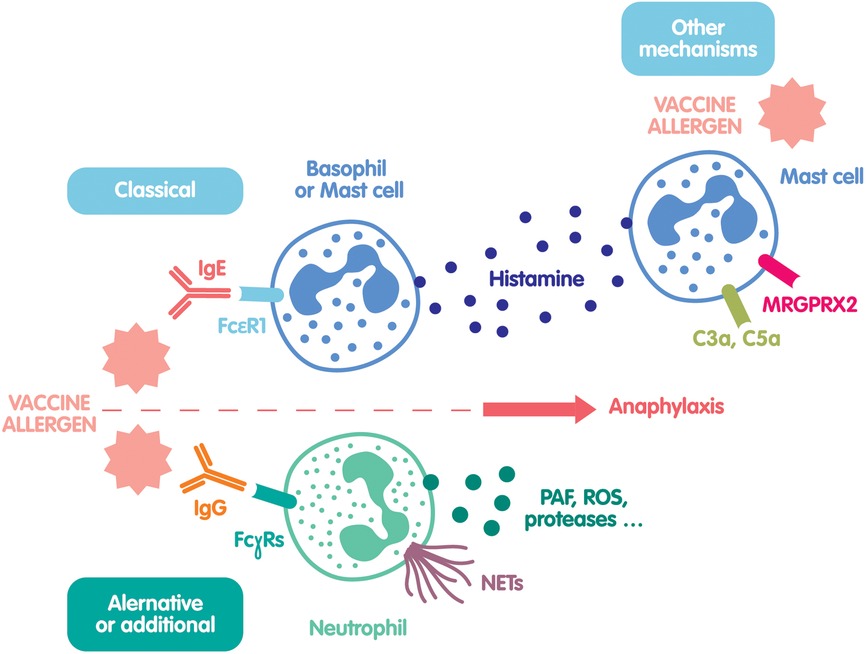
Figure 1. Legend. Main mechanisms of potential COVID-19 vaccine-induced hypersensitivity. The classical mechanism involves specific IgE-dependent mast cell and basophil activation leading to histamine/tryptase release. The alternative or additional mechanism involves specific IgG-dependent neutrophil activation leading to the release of reactive oxygen species (ROS), proteases such as elastase or neutrophil extracellular traps (NETs). Finally, several other mast cell activation mechanisms are suspected to play a role via C3a or C5a fixation to their receptors, or via the direct activation of MRGPRX2 by the vaccine.
IgE-mediated basophil and mast cell activation
IgE-mediated anaphylaxis implies a first exposure to an allergen leading to the production of specific IgE. These IgE bind to the high affinity receptors FcεRI on mast cells and basophils. Upon a new encounter, the allergen or a closely related substance activates mast cells and basophils by surface IgE cross-binding, which triggers degranulation of various mediators such as histamine or tryptase. This mechanism is the basis for routine anaphylaxis biological diagnosis, which encompass degranulated tryptase and histamine measurement, as well as specific IgE assessments. A true IgE-mediated allergic reaction to COVID-19 vaccines is possible, mainly based on documented PEG-mediated reactions in the literature, but seems very rare, as we'll see below.
IgG-mediated anaphylaxis
Up to 30% of patients with clinically proven drug anaphylaxis do not have any sign of an IgE-dependent mechanism (9). Our group has demonstrated in various mice models that anaphylaxis can be triggered by a pathway involving specific IgGs that activate neutrophils (10, 11). Activated neutrophils release platelet-activating factor (PAF), a potent vasoactive lipid with effect similar to histamine. In a multicentric clinical study, we were able to confirm this mechanism in human, and showed that signs of neutrophil activation (in particular degranulation of neutrophil elastase and production of neutrophil extracellular traps) were correlated with severity in perioperative anaphylaxis patients (9).
Complement activation and mast cell degranulation
Besides these two mechanisms, other pathways have been proposed to explain anaphylaxis that do not rely on the adaptive immune response. Since they do not require previous sensitization, these mechanisms may explain reactions observed to the first allergen exposure. Most of these mechanisms involve pharmacological activation of mast cells by the allergen. Some allergens have been described to activate the complement system, releasing C3a and C5a cleavage fragments that are able to trigger mast cell degranulation through specific receptors. These adverse effects known as CARPA have been documented with nanomedicines in experimental models but evidence in human are lacking (12). Moreover, Szebeni group also reported anti-PEG IgG-triggered complement terminal complex-mediated damage to PEGylated nanomedicines, that could decrease the efficacy of the nanomedicine and increase the toxicity via this complement activation (13).
Mas-related G protein-coupled receptor X2 (MRGPRX2) engagement on mast cells
Mast cell direct activation by positively charged substances like iodinated contrast media, quinolones, or some neuromuscular blocking agents has been described through the Mas-Related G Protein coupled Receptor X2 (MRGPRX2) (14). Interestingly, mRNA stabilization with PEG induces also a positive charge that could make this mechanism possible during COVID19 vaccine reaction. Whether basophils can also express MRGPRX2 at their surface upon activation remains controversial, but would be of great interest in assessing COVID19 vaccine-related hypersensitivity (15). However, it was recently shown that tryptase release by activated mast cells cannot discriminate between IgE- and MRGPRX2-related mechanisms, leaving yet unanswered questions concerning this interesting receptor (16).
Release of other active mediators
Finally, many mediators like prostaglandins, bradykinin, serotonin or nitric oxide could mimic anaphylaxis symptoms by inducing vasodilation or bronchoconstriction, and their potential contribution to anaphylaxis is only beginning to be investigated.
Potential allergens in COVID 19 vaccines
Allergic reactions to vaccines are mostly due to excipients or contaminants, and exceptionally to the antigens themselves (3). The potential allergens contained in the vaccines that are available in the European Union are listed in Table 1.
Both mRNA vaccines (Cominarty and Spikevax) have a similar structure: they contain no protein or adjuvant, but only the mRNA which is packed with stabilizing lipids inside a lipidic nanoparticle covered with polyethylene glycol (PEG) to increase water solubility. While PEG has been the first suspected candidate, other components must be evaluated (17).
PEG or macrogol is an ether polymer with a molecular weight ranging from 200 to 35,000 g/mol. It is used in many industrial products, either pure in preparation for colonoscopy and laxatives, or as an excipient in some food, cosmetics, topical drugs, or therapeutic proteins. Anaphylaxis to PEG-containing products remains rare but have been reported (18). These reactions were mostly with high molecular weight PEG (>2,000 g/mol), both with oral route (19) or injected drugs (20). Positive skin tests have been reported in PEG allergic patients, and specific IgG and IgE have been recently reported in some patients with severe reactions to injectable drugs and therapeutic protein (21, 22). This shows that PEG can be recognized by the immune system and can trigger the classical IgE pathway mechanism (23). The role of PEG IgG is less clear in this context. It has been suggested that specific IgG could activate the complement via the classical pathway, which in turn could activate mast cells via the anaphylatoxins. However, the prevalence of these IgG is high in patients exposed to PEG without any allergic reaction. Very recently, a time-course study of anti-PEG IgG did not evidence any increase in concentrations after each dose of mRNA vaccine, regardless of the vaccine used (24) A more detailed analysis of IgG subclasses involved, and the measurement of their affinity could help to distinguish harmful IgG susceptible of triggering a reaction. Moreover, it has been demonstrated that PEG itself can directly activate the complement system via the lectin and the alternative pathway (13, 25–27) and that lipid-conjugated PEG could be involved in the allergic reactions rather than PEG alone (28).
In addition to PEG, Moderna mRNA-1273 vaccine (Spikevax) also contains tromethamine (or trometamol), a widely used buffering agent. Some cases of anaphylaxis have been published to injectable drugs where tromethamine was identified as the culprit agent (29, 30). In the second version of Cominarty vaccine (ready to use vials), tromethamine has also been added. Very recently, bivalent mRNA vaccines from Pfizer (Cominarty Original/BA) and Moderna (mRNA-1273.214) have been approved by the EMA. mRNA coding for spike from BA1 omicron variant have been added to both original vaccines. However no other modification of the vaccine composition can be noticed, in particular concerning potential allergens.
A third vaccine, widely used in Europe, is a viral vector from a chimpanzee adenovirus coding for SARS-CoV2 spike protein (ChAdOx-1-S, AstraZeneca). It does not contain adjuvant either, but contains polysorbate 80 (or Tween 80), a non-ionic detergent with poly(ethylene oxide) side chains that are similar to the PEG structure. Anaphylaxis to polysorbate 80 has also been observed, with cross-reactivity to PEG components (25, 31).
Two vaccines consisting in recombinant spike proteins are also available in the European Union : Nuvaxovid (recombinant adjuvanted spike protein produced in Spodoptera frugiperda Sf9 insect cells) and JCovden (Recombinant Ad26. COV2-S produced in PER.C6 Tet R cells). They both contain polysorbate 80.
Finally the Valneva vaccine, composed of inactivated adjuvanted adsorbed SARS-Cov2 virus does not contain any component suspected to induce allergic reaction.
In summary, most of COVID-19 vaccines contain a few potential allergens able to trigger anaphylaxis via several mechanisms incompletely understood (32). In addition to the clinical evaluation by allergologists and the use of skin tests in a stepwise fashion (33, 34), a biological evaluation can be done to get more information and determine the risk for vaccination or re-vaccination.
Biological evaluation of COVID19 vaccine-induced allergy
Anti-PEG antibodies
The few studies carried out on the presence of anti-PEG of the IgE isotype but also IgG and IgM have been done using “in-house” techniques (21) A recent commercial ELISA was studied in 20 patients known to have experienced clinical reactions to drugs containing PEG; in this work, 4 out of these 20 patients had anti-PEG 2,000 IgE, and all had positive PEG skin tests (35). On a technical level, it is important to note the possible interference of bovine serum albumin and Tween 20, often used in ELISA; skimmed milk and an alternative detergent would probably be more appropriate reagents (35). Flow cytometric methods have also been described to assay anti-PEG IgE (36). Interestingly, Zhou et al. (21) found anti-PEG IgE and IgG in patients who had an anaphylactic reaction to products for colonoscopy preparation containing PEG 3350. It seems that some of these antibodies preexist in the general population, with a frequency of anti-PEG IgG of 5 to 9%, which could explain the manifestations observed at first administration (37).
The recent results on the frequency of anti-PEG antibodies during post-vaccination reactions are contradictory. This may be partly due to a lack of standardization of assay methods and of the gradation of the severity of allergy to PEG (38, 39). Some authors detected neither anti-PEG IgE nor IgG in post-vaccination reactions (34, 40), others found IgE and IgM but their control population was small. One of the questions is whether it would not be preferable to develop techniques to search for antibodies directed against PEG in the form of nanoparticles, or even against the vaccine itself (41). New robust tests are needed.
Proteins from complement activation
When hypothesizing CARPA-type mechanism, different complement activation parameters can be measured at the time of the reaction: anaphylatoxins C3a and C5a and the soluble fraction of the membrane attack complex C5b-9. In a pig experimental work, increased soluble C5b-9 levels correlated with the presence of anti-PEG IgM, after stimulation with PEGylated liposomes (32). Lim et al. (42) found increased C3a levels just after the clinical reaction in 3 patients, persisting from 48 h to one month. However, this increase was not confirmed by our group in 5 patients sampled at the time of the reaction (43). These preliminary results do not make it possible to conclude on the interest of these markers. Moreover, it is difficult to obtain a blood sample at the time of the clinical reaction, particularly in patients vaccinated outside a hospital.
Mast cell activation and -derived mediators
To assess a possible mast cell degranulation in favor of an anaphylactic reaction induced by mRNA vaccines, histamine and tryptase assays could be informative. Very few studies report the measurement of tryptase at the time of the reaction, and they do not show any increased levels (26, 38, 42, 44, 45). Warren et al. study is the only one reporting elevated tryptase levels (between 14 and 25 μg/l for a basal tryptase between 2 and 6 μg/L) in 8 patients at time of the reaction (34). Our group reported increased histamine levels in 1 patient out of 5, within 30 min of the post-vaccination reaction, while tryptase levels were not modified (43).
Basal tryptase levels could also be of interest, even if no increased risk for reaction has been described in patients with mastocytosis (3). A few studies have shown a subnormal concentration in some patients: median of 8.5 to 12.8 μg/l, i.e. above the 95th percentiles described in the general population (46, 47). This could be in favor of gene duplication-related hyper-alpha − tryptasemia that needs to be better documented in the future (48). Moreover, the KIT D816V mutation research in the blood can be done to document mastocytosis, even in the presence of normal baseline tryptase (49).
The basophil activation test
The basophil activation test (BAT) using CD63 and/or CD203 as activation markers by flow cytometry was developed as early as January 2021 to explore immediate hypersensitivity to mRNA vaccines. Various authors tried to determine its place in the management of patients who reported reactions to drugs containing PEG before the first dose (50), or experienced reactions just after the first dose. In both cases there was an urgent need to secure vaccine injections (46).
Most of the published studies have been done on small patient series. Troelnikov et al. (50) performed BAT with PEG 2,000 nanoparticles in 3 patients known for PEG allergy and evidenced basophil activation. Labella et al. (46) found a positive BAT to PEG 2,000 and to the vaccine in 5/16 patients. Warren et al. (34) reported a positive BAT in 10/11 patients tested in the presence of PEG 2,000 DMG in the form of nanoparticles and vaccine. The frequency of patients with positive BAT is therefore very variable and could depend on the patients (already known to react to PEG or not for example) and the stimuli used ex vivo, whole vaccine and PEG nanoparticles seeming to give the highest positivity. Different allergens can be used in BAT. PEG 2,000 and PEG 2,000 DMG have been recently marketed for this test. However, as PEG contained in the vaccines is in the form of nanoparticles conjugated with lipids, some authors carried out BAT in the presence of the vaccine and/or PEG in the form of lipid nanoparticles approaching the truly potential immunogenic form (34, 50). However, in the early 2022, some authors evidenced that BAT was positive in response to vaccine alone in 50% of the patients who had COVID, and did not react during the vaccine injection (46). This information, that remains to be confirmed, must encourage to interpret BAT results with caution, in particular in patients who experienced SARS-Cov 2 infection. However, most authors agree in concluding that in the event of an anaphylactic reaction after injection of an mRNA vaccine, BAT is more frequently positive than skin tests confirming an activation mechanism which would not necessarily be IgE dependent (34, 40, 50). In our group in Paris, preliminary data in 30 patients with anaphylaxis after the first injection of a mRNA vaccine confirm that BAT can be positive while skin tests are negative (Nicaise-Roland P, Soria A et al., unpublished results). A recent Review by Eberlein et al. concluded that BAT helps elucidate allergic reactions to COVID-19 vaccines, but defining exact threshold of positivity is still needed (51).
We can thus assume that BAT is a quite simple and well-known test that needs to be further evaluated in larger well-characterized patients, with appropriate and standardized stimuli.
The histamine release test
This test is only documented in two studies in this setting. The first one evidenced transient positive results in 3 patients who experienced a reaction (52), and the other one described positive results in 2/10 patients with positive skin tests to PEG (53).
Conclusion
Eighteen months after the first vaccinations against COVID-19, the present real-world cohort survey can suggest that serious adverse effects are extremely rare. For instance, an analysis of 20,000 participants revealed that the adverse effects observed in 0.3% of the subjects were associated with full vaccination dose, vaccine brand, young age and COVID-19 (54). Research improved our understanding of COVID-19 vaccine allergy mechanisms, and made available some biological tools to an adequate management of the suspected patients (55, 56). Some tests, such as BAT, are now available to help the diagnosis in addition to skin tests. We can assume that BAT is the best biological tool to evaluate the ex vivo reaction to both whole vaccine and each excipient. The identification of the culprit agent even led to a safe and successful desensitization in a recent series of 6 patients (57). Conversely, the quantification of anti-PEG IgE or IgE cannot be recommended so far. Finally, lessons learned from nanomedicines need to be applied (58). There is a need to safely immunize patients who are at risk or who experienced immediate vaccine reactions, using antihistamines for example. Several studies are still ongoing in order to increase our knowledge and make large-scale vaccination safe and successful.
Author contributions
All authors made substantial direct contributions to writing the manuscript, and approved it for publication. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors would like to thank Veronique Naizonard and Céline Champagnat for their excellent technical assistance.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Barbaud A, Garvey LH, Arcolaci A, Brockow K, Mori F, Mayorga C, et al. Allergies and COVID-19 vaccines: an ENDA/EAACI position paper. Allergy. (2022) 77(8):2292–312. doi: 10.1111/all.15241
2. Mahdiabadi S, Rezaei N. Anaphylaxis and allergic reactions to COVID-19 vaccines: a narrative review of characteristics and potential obstacles on achieving herd immunity. Health Sci Rep. (2022) 5(5):e787. doi: 10.1002/hsr2.787
3. Bruhns P, Chollet-Martin S. Mechanisms of human drug-induced anaphylaxis. J Allergy Clin Immunol. (2021) 147(4):1133–42. doi: 10.1016/j.jaci.2021.02.013
4. Kroumpouzos G, Paroikaki ME, Yumeen S, Bhargava S, Mylonakis E. Cutaneous complications of mRNA and AZD1222 COVID-19 vaccines: a worldwide review. Microorganisms. (2022) 10(3):624. doi: 10.3390/microorganisms10030624
5. McNeil MM, DeStefano F. Vaccine-associated hypersensitivity. J Allergy Clin Immunol. (2018) 141(2):463–72. doi: 10.1016/j.jaci.2017.12.971
6. Maltezou HC, Anastassopoulou C, Hatziantoniou S, Poland GA, Tsakris A. Anaphylaxis rates associated with COVID-19 vaccines are comparable to those of other vaccines. Vaccine. (2022) 40(2):183–6. doi: 10.1016/j.vaccine.2021.11.066
7. Risma KA, Edwards KM, Hummell DS, Little FF, Norton AE, Stallings A, et al. Potential mechanisms of anaphylaxis to COVID-19 mRNA vaccines. J Allergy Clin Immunol. (2021) 147(6):2075–2082.e2. doi: 10.1016/j.jaci.2021.04.002
8. Corey KB, Koo G, Phillips EJ. Adverse events and safety of SARS-CoV-2 vaccines: what's new and what's next. J Allergy Clin Immunol Pract. (2022) 10(9):2254–66. doi: 10.1016/j.jaip.2022.04.035
9. Jönsson F, de Chaisemartin L, Granger V, Gouel-Chéron A, Gillis CM, Zhu Q, et al. An IgG-induced neutrophil activation pathway contributes to human drug-induced anaphylaxis. Sci Transl Med. (2019) 11(500). doi: 10.1126/scitranslmed.aat1479
10. Jönsson F, Mancardi DA, Kita Y, Karasuyama H, Iannascoli B, Van Rooijen N, et al. Mouse and human neutrophils induce anaphylaxis. J Clin Invest. (2011) 121(4):1484–96. doi: 10.1172/JCI45232
11. Jönsson F, Mancardi DA, Zhao W, Kita Y, Iannascoli B, Khun H, et al. Human FcγRIIA induces anaphylactic and allergic reactions. Blood. (2012) 119(11):2533–44. doi: 10.1182/blood-2011-07-367334
12. Őrfi E, Mészáros T, Hennies M, Fülöp T, Dézsi L, Nardocci A, et al. Acute physiological changes caused by complement activators and amphotericin B-containing liposomes in mice. Int J Nanomedicine. (2019) 14:1563–73. doi: 10.2147/IJN.S187139
13. Gabizon A, Szebeni J. Complement activation: a potential threat on the safety of poly(ethylene glycol)-coated nanomedicines. ACS Nano. (2020) 14(7):7682–8. doi: 10.1021/acsnano.0c03648
14. Subramanian H, Gupta K, Ali H. Roles of Mas-related G protein–coupled receptor X2 on mast cell–mediated host defense, pseudoallergic drug reactions, and chronic inflammatory diseases. J Allergy Clin Immunol. (2016) 138(3):700–10. doi: 10.1016/j.jaci.2016.04.051
15. Sabato V, Elst J, Van Houdt M, Bridts C, Mertens C, Ebo DG. Surface expression of MRGPRX2 on resting basophils: an area of controversy. Allergy. (2020) 75(9):2421–2. doi: 10.1111/all.14252
16. Elst J, van der Poorten MLM, Van Gasse AL, Mertens C, Hagendorens MM, Ebo DG, et al. Tryptase release does not discriminate between IgE- and MRGPRX2-mediated activation in human mast cells. Clin Exp Allergy. (2022) 52(6):797–800. doi: 10.1111/cea.14110
17. Krantz MS, Liu Y, Phillips EJ, Stone CA. COVID-19 vaccine anaphylaxis: PEG or not? Allergy. (2021) 76(6):1934–7. doi: 10.1111/all.14722
18. Wenande E, Garvey LH. Immediate-type hypersensitivity to polyethylene glycols: a review. Clin Exp Allergy. (2016) 46(7):907–22. doi: 10.1111/cea.12760
19. Pizzimenti S, Heffler E, Gentilcore E, Raie A, Bussolino C, Nebiolo F, et al. Macrogol hypersensitivity reactions during cleansing preparation for colon endoscopy. J Allergy Clin Immunol Pract. (2014) 2(3):353–4. doi: 10.1016/j.jaip.2014.01.017
20. Rau RE, Dreyer Z, Choi MR, Liang W, Skowronski R, Allamneni KP, et al. Outcome of pediatric patients with acute lymphoblastic leukemia/lymphoblastic lymphoma with hypersensitivity to pegaspargase treated with PEGylated Erwinia asparaginase, pegcrisantaspase: a report from the Children's Oncology group. Pediatr Blood Cancer. Mars. (2018) 65(3). doi: 10.1002/pbc.26873
21. Zhou ZH, Stone CA, Jakubovic B, Phillips EJ, Sussman G, Park J, et al. Anti-PEG IgE in anaphylaxis associated with polyethylene glycol. J Allergy Clin Immunol Pract. (2021) 9(4):1731–1733.e3. doi: 10.1016/j.jaip.2020.11.011
22. Mortz CG, Kjaer HF, Rasmussen TH, Rasmussen HM, Garvey LH, Bindslev-Jensen C. Allergy to polyethylene glycol and polysorbates in a patient cohort: diagnostic work-up and decision points for vaccination during the COVID-19 pandemic. Clin Transl Allergy. (2022) 12(1):e12111. doi: 10.1002/clt2.12111
23. Kozma GT, Shimizu T, Ishida T, Szebeni J. Anti-PEG antibodies: properties, formation, testing and role in adverse immune reactions to PEGylated nano-biopharmaceuticals. Adv Drug Deliv Rev. (2020) 154–155:163–75. doi: 10.1016/j.addr.2020.07.024
24. Guerrini G, Gioria S, Sauer AV, Lucchesi S, Montagnani F, Pastore G, et al. Monitoring anti-PEG antibodies level upon repeated lipid nanoparticle-based COVID-19 vaccine administration. Int J Mol Sci. (2022) 23(16):8838. doi: 10.3390/ijms23168838
25. Stone CA, Liu Y, Relling MV, Krantz MS, Pratt AL, Abreo A, et al. Immediate hypersensitivity to polyethylene glycols and polysorbates: more common than we have recognized. J Allergy Clin Immunol Pract. Juin. (2019) 7(5):1533–1540.e8. doi: 10.1016/j.jaip.2018.12.003
26. Sellaturay P, Nasser S, Islam S, Gurugama P, Ewan PW. Polyethylene glycol (PEG) is a cause of anaphylaxis to the Pfizer/BioNTech mRNA COVID-19 vaccine. Clin Exp Allergy. (2021) 51(6):861–3. doi: 10.1111/cea.13874
27. Shi D, Beasock D, Fessler A, Szebeni J, Ljubimova JY, Afonin KA, et al. To PEGylate or not to PEGylate: immunological properties of nanomedicine's Most popular component, polyethylene glycol and its alternatives. Adv Drug Deliv Rev. (2022) 180:114079. doi: 10.1016/j.addr.2021.114079
28. Cabanillas B, Novak N, Akdis CA. The form of PEG matters: PEG conjugated with lipids and not PEG alone could be the specific form involved in allergic reactions to COVID-19 vaccines. Allergy. (2022) 77(6):1658–60. doi: 10.1111/all.15187
29. Lukawska J, Mandaliya D, Chan AWE, Foggitt A, Bidder T, Harvey J, et al. Anaphylaxis to trometamol excipient in gadolinium-based contrast agents for clinical imaging. J Allergy Clin Immunol Pract. (2019) 7(3):1086–7. doi: 10.1016/j.jaip.2018.08.035
30. Guler S, Ertok I, Sahin NY, Ramadan H, Katirci Y. Anaphylaxis after intravenous infusion of dexketoprofen trometamol. Turk J Emerg Med. (2016) 16(3):132–3. doi: 10.1016/j.tjem.2016.09.003
31. Calogiuri G, Foti C, Nettis E, Di Leo E, Macchia L, Vacca A. Polyethylene glycols and polysorbates: two still neglected ingredients causing true IgE-mediated reactions. J Allergy Clin Immunol Pract. (2019) 7(7):2509–10. doi: 10.1016/j.jaip.2019.05.058
32. Kozma GT, Mészáros T, Vashegyi I, Fülöp T, Örfi E, Dézsi L, et al. Pseudo-anaphylaxis to polyethylene glycol (PEG)-coated liposomes: roles of anti-PEG IgM and complement activation in a porcine model of human infusion reactions. ACS Nano. (2019) 13(8):9315–24. doi: 10.1021/acsnano.9b03942
33. Wolfson AR, Robinson LB, Li L, McMahon AE, Cogan AS, Fu X, et al. First-Dose mRNA COVID-19 vaccine allergic reactions: limited role for excipient skin testing. J Allergy Clin Immunol Pract. (2021) 9(9):3308–3320.e3. doi: 10.1016/j.jaip.2021.06.010
34. Warren CM, Snow TT, Lee AS, Shah MM, Heider A, Blomkalns A, et al. Assessment of allergic and anaphylactic reactions to mRNA COVID-19 vaccines with confirmatory testing in a US regional health system. JAMA Netw Open. (2021) 4(9):e2125524. doi: 10.1001/jamanetworkopen.2021.25524
35. Chen BM, Su YC, Chang CJ, Burnouf PA, Chuang KH, Chen CH, et al. Measurement of Pre-existing IgG and IgM antibodies against polyethylene glycol in healthy individuals. Anal Chem. (2016) 88(21):10661–6. doi: 10.1021/acs.analchem.6b03109
36. Fang JL, Beland FA, Tang Y, Roffler SR. Flow cytometry analysis of anti-polyethylene glycol antibodies in human plasma. Toxicol Rep. (2021) 8:148–54. doi: 10.1016/j.toxrep.2020.12.022
37. McSweeney MD, Mohan M, Commins SP, Lai SK. Anaphylaxis to pfizer/BioNTech mRNA COVID-19 vaccine in a patient with clinically confirmed PEG allergy. Front Allergy. (2021) 2:715844. doi: 10.3389/falgy.2021.715844
38. Schellekens H, Hennink WE, Brinks V. The immunogenicity of polyethylene glycol: facts and fiction. Pharm Res. (2013) 30(7):1729–34. doi: 10.1007/s11095-013-1067-7
39. Mathes S, Eberlein B, Darsow U, Faihs V, Vitus M, Bent R, et al. Variability of eliciting thresholds in PEG allergy limits prediction of tolerance to PEG-containing mRNA COVID vaccines. J Allergy Clin Immunol Pract. (2022) 10(7):1931–3. doi: 10.1016/j.jaip.2022.04.006
40. Jiang SY, Smith EM, Vo V, Akdis C, Nadeau KC. Non-immunoglobulin E-mediated allergy associated with Pfizer-BioNTech coronavirus disease 2019 vaccine excipient polyethylene glycol. Ann Allergy Asthma Immunol. (2021) 127(6):694–6. doi: 10.1016/j.anai.2021.09.012
41. Kelso JM. Anaphylactic reactions to novel mRNA SARS-CoV-2/COVID-19 vaccines. Vaccine. (2021) 39(6):865–7. doi: 10.1016/j.vaccine.2020.12.084
42. Lim XR, Leung BP, Ng CYL, Tan JWL, Chan GYL, Loh CM, et al. Pseudo-Anaphylactic reactions to pfizer BNT162b2 vaccine: report of 3 cases of anaphylaxis post pfizer BNT162b2 vaccination. Vaccines (Basel). (2021) 9(9):974. doi: 10.3390/vaccines9090974
43. de Chaisemartin L, Diep A, Gonnin C, Soria A, Barbaud A, Nicaise-Roland P. Immune parameters during anaphylaxis to messenger RNA coronavirus disease 2019 vaccines: not the usual suspects? Ann Allergy Asthma Immunol. (2022) 128(3):338–9. doi: 10.1016/j.anai.2021.11.012
44. Restivo V, Candore G, Barrale M, Caravello E, Graziano G, Onida R, et al. Allergy to polyethilenglicole of anti-SARS CoV2 vaccine recipient: a case report of young adult recipient and the management of future exposure to SARS-CoV2. Vaccines (Basel). (2021) 9(5):412. doi: 10.3390/vaccines9050412
45. Krantz MS, Bruusgaard-Mouritsen MA, Koo G, Phillips EJ, Stone CA, Garvey LH. Anaphylaxis to the first dose of mRNA SARS-CoV-2 vaccines: don’t give up on the second dose!. Allergy. (2021) 76(9):2916–2920. doi: 10.1111/all.14958
46. Labella M, Céspedes JA, Doña I, Shamji MH, Agache I, Mayorga C, et al. The value of the basophil activation test in the evaluation of patients reporting allergic reactions to the BNT162b2 mRNA COVID-19 vaccine. Allergy. (2022) 77(7):2067–79. doi: 10.1111/all.15148
47. Pitlick MM, Sitek AN, Kinate SA, Joshi AY, Park MA. Polyethylene glycol and polysorbate skin testing in the evaluation of coronavirus disease 2019 vaccine reactions: early report. Ann Allergy Asthma Immunol. (2021) 126(6):735–8. doi: 10.1016/j.anai.2021.03.012
48. Spoerl D, Docquier M, Coattrenec Y, Seebach JD. Patients with elevated basal tryptase serum levels should be tested for hereditary alpha-tryptasemia. Eur Ann Allergy Clin Immunol. (2022) 54(5):242–4. doi: 10.23822/EurAnnACI.1764-1489.220
49. Dölle-Bierke S, Siebenhaar F, Burmeister T, Worm M. Detection of KIT D816V mutation in patients with severe anaphylaxis and normal basal tryptase-first data from the anaphylaxis registry (NORA). J Allergy Clin Immunol. (2019) 144(5):1448–1450.e1. doi: 10.1016/j.jaci.2019.07.037
50. Troelnikov A, Perkins G, Yuson C, Ahamdie A, Balouch S, Hurtado PR, et al. Basophil reactivity to BNT162b2 is mediated by PEGylated lipid nanoparticles in PEG allergic patients. J Allergy Clin Immunol. (2021) 148(1):91–5. doi: 10.1016/j.jaci.2021.04.032
51. Eberlein B, Mathes S, Fischer J, Darsow U, Biedermann T, Brockow K. Do basophil activation tests help elucidate allergic reactions to the ingredients in COVID-19 vaccines? Allergy. (2022). doi: 10.1111/all.15278. [Epub ahead of print]
52. Rasmussen TH, Mortz CG, Georgsen TK, Rasmussen HM, Kjaer HF, Bindslev-Jensen C. Patients with suspected allergic reactions to COVID-19 vaccines can be safely revaccinated after diagnostic work-up. Clin Transl Allergy. (2021) 11(5):e12044. doi: 10.1002/clt2.12044
53. Bruusgaard-Mouritsen MA, Jensen BM, Poulsen LK, Johansen JD, Garvey LH. Optimizing investigation of suspected allergy to polyethylene glycols. J Allergy Clin Immunol. (2022) 149(1):168–75.e4. doi: 10.1016/j.jaci.2021.05.020
54. Beatty AL, Peyser ND, Butcher XE, Cocohoba JM, Lin F, Olgin JE, et al. Analysis of COVID-19 vaccine type and adverse effects following vaccination. JAMA Netw Open. (2021) 4(12):e2140364. doi: 10.1001/jamanetworkopen.2021.40364
55. Banerji A, Norton AE, Blumenthal KG, Stone CA, Phillips E. Rapid progress in our understanding of COVID-19 vaccine allergy: a cause for optimism, not hesitancy. J Allergy Clin Immunol. (2022) 150(1):12–6. doi: 10.1016/j.jaci.2022.03.023
56. Worm M, Alexiou A, Bauer A, Treudler R, Wurpts G, Dickel H, et al. Management of suspected and confirmed COVID-19 (SARS-CoV-2) vaccine hypersensitivity. Allergy. (2022). doi: 10.1111/all.15414. [Epub ahead of print]
57. AlMuhizi F, Ton-Leclerc S, Fein M, Tsoukas C, Garvey LH, Lee D, et al. Successful desensitization to mRNA COVID-19 vaccine in a case series of patients with a history of anaphylaxis to the first vaccine dose. Front Allergy. (2022) 3:825164. doi: 10.3389/falgy.2022.825164
Keywords: COVID-19 vaccine, anaphylaxis, basophil activation test, IgE, complement
Citation: Nicaise-Roland P, Granger V, Soria A, Barbaud A, Pallardy M, Chollet-Martin S and de Chaisemartin L (2022) Immediate hypersensitivity to COVID-19 vaccines: Focus on biological diagnosis. Front. Allergy 3:1007602. doi: 10.3389/falgy.2022.1007602
Received: 30 July 2022; Accepted: 15 September 2022;
Published: 30 September 2022.
Edited by:
Joana Vitte, INSERM UMRUA11 Institut Desbrest d'Épidémiologie et de Santé Publique (IDESP), FranceReviewed by:
Bettina Wedi, Hannover Medical School, Germany© 2022 Nicaise-Roland, Granger, Soria, Barbaud, Pallardy, Chollet-Martin and de Chaisemartin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sylvie Chollet-Martin c3lsdmllLmNob2xsZXQtbWFydGluQHVuaXZlcnNpdGUtcGFyaXMtc2FjbGF5LmZy
†These authors share senior authorship
Specialty Section: This article was submitted to Allergens, a section of the journal Frontiers in Allergy