 R. Sáenz de Santa María1,2
R. Sáenz de Santa María1,2 G. Bogas1,2
G. Bogas1,2 M. Labella1,2
M. Labella1,2 A. Ariza2
A. Ariza2 M. Salas1,2
M. Salas1,2 I. Doña1,2,†
I. Doña1,2,† M. J. Torres1,2,3,4*†
M. J. Torres1,2,3,4*†
- 1Allergy Unit, Hospital Regional Universitario de Málaga, Hospital Civil, Málaga, Spain
- 2Allergy Research Group, Instituto de Investigación Biomédica de Málaga-IBIMA, Hospital Civil, Málaga, Spain
- 3Nanostructures for Diagnosing and Treatment of Allergic Diseases Laboratory, Andalusian Center for Nanomedicine and Biotechnology-BIONAND, Parque Tecnológico de Andalucía, Málaga, Spain
- 4Departamento de Medicina, Universidad de Málaga, Facultad de Medicina, Málaga, Spain
A considerable number of pediatric patients treated with beta-lactam (BL) antibiotics develop delayed onset of skin rashes during the course of treatment. Although the most frequent cause of these symptoms is infectious, many cases are labeled as allergic reactions to these drugs. BL allergy labels could have a negative impact, as they imply avoidance of this group of drugs and the use of second-line antibiotics, leading to a potential increase in adverse effects and the utilization of less effective therapies. This constitutes a major public health concern and economic burden, as the use of broad-spectrum antibiotics can result in multidrug-resistant organisms and prolonged hospital stays. Therefore, it is crucial to delabel patients during childhood to avoid false labeling in adult life. Although the label of BL allergy is among the most frequent causes of allergy referral, its management remains controversial, and new diagnostic perspectives are changing the paradigm of managing BL allergies in children. Traditionally, drug provocation testing (DPT) was exclusively performed in patients who had previously obtained negative results from skin tests (STs). However, the sensitivity of STs is low, and the role of in vitro testing in the pediatric population is not well defined. Recent studies have demonstrated the safety of direct DPT without prior ST or serum tests for pediatric patients who report a low-risk reaction to BLs, which is cost-effective. However, there is still a debate on the optimal allergic workup to be performed in children with a benign immediate reaction and the management of children with severe cutaneous adverse drug reactions. In this review, we will discuss the impact of the label of BL allergy and the role of the different tools currently available to efficiently address BL allergy delabeling in children.
1. Impact of beta-lactam allergy as a public health problem
Up to 10% of children treated with beta-lactams (BLs) develop delayed maculopapular exanthema or urticaria (1). Although the most frequent etiology for these symptoms is infectious, with approximately two-thirds of children presenting with a confirmed viral illness (2, 3), most of the cases are labeled as penicillin allergies.
A penicillin allergy label directly impacts the selection of antibiotics, potentially leading to negative consequences such as a higher risk of antimicrobial treatment failure, developing antimicrobial resistance, occurrence of adverse drug reactions due to the use of a broader spectrum or alternative antibiotic, and increased healthcare costs (4–15). In this regard, it has been observed that approximately 50% of children who have been diagnosed with an antibiotic allergy are prescribed antibiotics that are not suitable for the specific infection being treated (16–19), placing patients at risk for the use of less effective therapies and an increased likelihood of treatment failures (20, 21). Moreover, the use of broader spectrum antibiotics can lead to increased rates of infection with multidrug-resistant organisms such as Clostridium difficile infection, vancomycin-resistant Enterococcus, and methicillin-resistant Staphylococcus aureus (4–6, 9, 13, 15, 16, 22–25). All of this leads to increased length of hospital stays compared with the general population (5–9). It has also been reported that children labeled as allergic to penicillin have a higher comorbidity index and incur higher hospitalization costs (23). Globally, this constitutes a substantial public health threat and economic burden (4, 5, 15, 16, 22–25).
Penicillin allergy labels are usually acquired during childhood, with up to 75% of patients labeled as allergic before the age of 3 years (26). This labeling often persists throughout adulthood. Indeed, up to 20% of the general population denominate themselves “penicillin-allergic” (26–29). However, less than 10% of them are confirmed as truly allergic after a proper allergy assessment (30–34). Therefore, there is the potential for a large majority of these allergies to be effectively “delabeled” (35, 36). Consequently, the evaluation and delabeling of BL allergy in pediatric population constitute important public health goals in order to avoid dragging that label into adult life, with the above-mentioned consequences. Moreover, the evaluation study of suspected penicillin allergic reactions in children is a cost-effective measure, as delabeling plays a critical role in promoting antimicrobial stewardship (37). In this regard, it has been estimated that subjects labeled as penicillin-allergic prior to age 10 years have lifetime antibiotic costs that are $2,000 higher compared with those who were not allergic to penicillin (38). In addition, the evaluation and subsequent removal of the penicillin allergy label in hospitalized patients prevented 504 inpatient days and 648 outpatient days on alternative antibiotics (39). Moreover, the removal of penicillin allergy label from 145 charts in an antimicrobial stewardship program in a tertiary care hospital resulted in an annual savings of $82,000 (40).
Despite the importance of delabeling to reduce adverse healthcare outcomes and decrease healthcare costs, barriers in tackling incorrect penicillin allergy labels have been identified, being among the most relevant barriers is the lack of knowledge of local pathways for evaluating antibiotic allergy (41). Therefore, there is a great need to provide antibiotic allergy education to non-allergy specialists, as well as to determine the best strategies to safely delabel children (42).
In this manuscript, we review the role of the different tools currently available to efficiently tackle BL allergy labels, including both in vivo [skin tests (STs) and drug provocation test (DPT)] and in vitro tests. The data sources utilized in this study consisted of English language literature obtained from MEDLINE, specifically focused on beta-lactam drug hypersensitivity in children. The selection of the studies was based on relevance, date of publication, and originality.
2. Immunochemistry and mechanisms involved in BL allergy
BL antibiotics are classified into five families: penicillins, cephalosporins, carbapenems, monobactams, and beta-lactamase inhibitors. All BLs share a common four-carbon ring called BL ring, but differ in the adjacent ring (a thiazolidine ring in penicillins, dihydrothiazine in cephalosporins, dihydropyrrole in carbapenems, and oxazolidine in beta-lactamase inhibitors). All of them, with the exception of beta-lactamase inhibitors, have an R1 side chain, which determines their antibacterial and pharmacokinetic action and is shared by some penicillins and cephalosporins. Cephalosporins and carbapenems also have a second R2 side chain. Monobactams have a monocyclic core, the only representative of which is aztreonam, which distinguishes it from other BLs (43) (Figure 1).
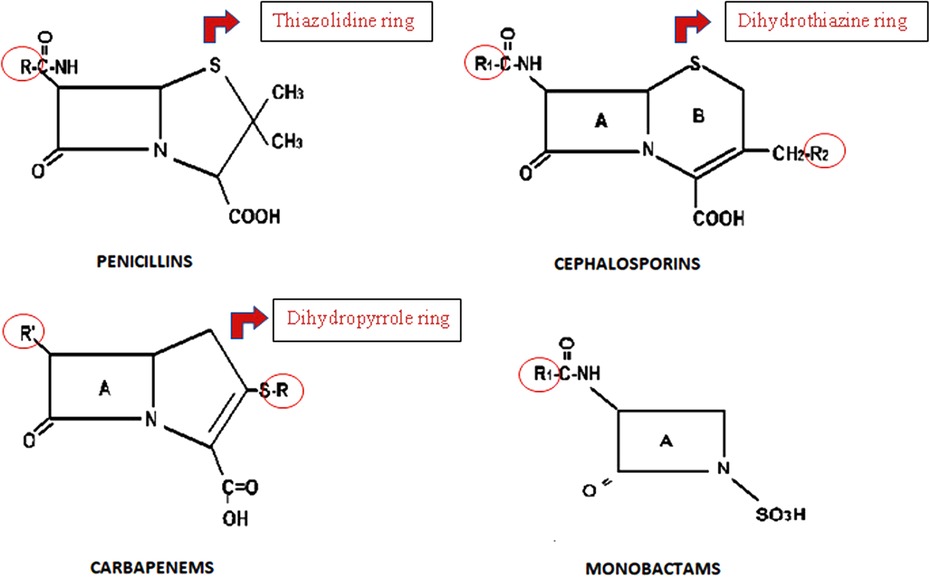
Figure 1. General chemical structure of BLs.
Hypersensitivity reactions can lead to any of the four immunologic effector mechanisms described by Coombs and Gell (44). Following penicillin administration, spontaneous opening of the beta-lactam ring occurs, giving rise to the different metabolites with the capacity to stimulate the immune system (43). They are low weight molecules that need to be conjugated to a carrier protein to induce an immune response (43, 45). Other immune activation mechanisms have also been described, wherein certain drugs are capable of binding to T cell or HLA receptors even in the absence of a hapten (46).
Clinically, the classification of hypersensitivity reactions to BL relies on the symptoms manifested in the reaction and their timing. In this sense, immediate reactions (IRs) occur within 1–6 h following administering the drug, while non-immediate reactions (NIRs) require a longer interval, usually after several hours or even days (47–49). IRs are usually IgE-mediated and manifest as urticaria, angioedema, rhinitis, bronchospasm, anaphylaxis, or acute gastrointestinal symptoms with abdominal pain, vomiting, and diarrhea. NIRs are related to a cellular mechanism and usually manifest as delayed urticaria, maculopapular rash, fixed drug rash, vasculitis, toxic epidermal necrolysis, Stevens–Johnson syndrome, drug reaction with eosinophilia and systemic symptoms, acute generalized rash pustulosis, symmetrical flexural intertriginous rash, or organ-specific involvement. Although this classification is not strict and overlaps exist, it proves to be valuable when considering the clinical evaluation and the diagnostic workup (43).
Allergic reactions may involve the BL ring, other rings, side chains, or allergenic determinants, which determines the cross-reactivity profile (50–53).
3. The value of clinical history
The first step in the approach of delabeling BL allergy in children involves a complete medical history, including questions regarding the patient, such as age or family history, as well as details regarding the reaction, symptoms, time of appearance, time of resolution, or drug implicated (54–57).
Concerning issues related to the patient, some studies have demonstrated that the age at the moment of the reaction is important. In this regard, confirmed allergic reactions to BLs is less frequent in children younger than 5 (58) or 7 (59). Moreover, reaction severity has also been associated with increasing age (32).
Previous studies have reported an association between atopic diseases and IRs to BLs (60, 61). However, other studies have not found evidences to support that allergologic background such as atopy, elevated specific IgE levels, or rhinitis increase the risk of developing an allergic reaction to BLs (2, 62–64).
A possible existence of some genetic factors involved in allergic reactions BLs has been proposed, as a higher proportion of confirmed allergic reactions has been reported in Europe compared with those in Asia and North America, without significant difference between Asia and North America (65).
In addition, familiar history of drug allergy has been associated in some studies with more prevalence of confirmed BL allergy (31, 59, 63). Indeed, a recent study has created a mathematical model to identify children with low-risk BL allergies where a backward multiple logistic regression showed that a family history of drug allergy was significantly associated with a confirmed BL allergy (66).
Considering issues related to the reaction, the first approach is usually classifying reactions according to the timing of symptom onset following the last dose in IRs and NIRs (2, 47). Several authors have observed a higher proportion of confirmed BL allergy in children reporting IRs compared with those experiencing NIRs (2, 62, 67, 68). However, others could not find any correlation between BL allergy and the timing of reactions (64). Indeed, it has been reported that up to 17% of children reporting NIRs were confirmed as allergic by experiencing an IR in DPT (2, 3, 54, 57, 59, 68–73). This observation suggests limitations in the reliability of reaction chronology registered in clinical history.
Cutaneous manifestations, such as urticaria or maculopapular exanthema, are the most frequently reported, but these symptoms can also be due to viral infections; therefore, differential diagnosis is difficult. However, if these symptoms persist less than 24 h, the child is considered at high risk for being allergic to BL (74, 75). Anaphylaxis is extremely rare in pediatric population, representing less than 0.05% of all cases (32). However, it has been recently identified as moderate to high risk for being allergic to BL, together with the immediate appearance of symptoms (76). Urticaria is the most controversial risk factor for BL allergy because it is included as a high or moderate risk factor in the majority of studies, but some reviews suggest that urticaria appearing more than 1 h after the last dose of BL can be considered as low risk (13, 37, 77). In most pediatric studies, mild cutaneous NIR to BLs is accepted as a low risk for BL allergy, as well as isolated generalized pruritus or gastrointestinal symptoms.
Regarding drugs involved in the reaction, some studies have demonstrated that a higher percentage of allergic patients are confirmed when cephalosporins are implicated (78). This can be explained by the fact that severe bacterial infections are treated with cephalosporins, whereas penicillin or amoxicillin are more frequently associated with viral infections. At this point, it is important to know that consumption patterns may vary between different regions, and that the drugs most commonly implicated are associated with those consumption patterns rather than with a particular drug (79, 80).
Finally, the approach differs between children and adults when the patient is unaware of any information regarding the reaction that resulted in the BL allergy label. While it is considered a moderate or high risk of allergy in the pediatric population, it is considered a low risk in the adult population (74, 81).
4. The role of skin testing in delabeling
After clinical history, conventional approach of BL allergy in patients of any age relies on skin testing (42). Sensitivity of STs has been reported to range from 2.6% to 37.8%, while specificity is overall high (96.8%), according to a recent meta-analysis that included 105 primary studies (82–84). However, it is important to take into account that these studies included mainly adults. Determining predictive values for ST with BLs in children is difficult, as only four studies performed DPT regardless of ST results (31, 54, 69, 85). It is of note that these studies assessed children who experienced various adverse reactions related to BLs intake, including not only allergic symptoms but also non-suggestive of allergy ones, such as gastrointestinal symptoms, which limits the generalizability of the results.
The prevalence of positive penicillin STs declines over time, from 27.7% to 0.4% in the period 1980–1993 to 1994–2003 (86). This may be due to changes in prescription patterns in favor of aminopenicillins (87). Therefore, it is important to take into account the determinants used for skin testing. It has been proposed that a standard panel reagents should include major (benzylpenicilloyl octa-L-lysine, BP-OL, DAP®, Diater, and benzylpenicilloyl poly-L-lysine, PPL, Pre-Pen®, AllerQuest LLC) and minor penicillin determinants (sodium benzylpenilloate, DAP®, Diater) (49, 88), amoxicillin, and the culprit BL (89). In this regard, testing clavulanic acid in adults has demonstrated to be beneficial due to its potential for inducing selective reactions (90, 91). Recently, this approach has been extrapolated to the diagnosis workup in pediatric patients (76). However, other authors argue for reducing the panel of STs in children, and propose that testing should only focus on the suspected drug in order to avoid the discomfort associated with STs (92).
The accuracy of STs has been more extensively evaluated in NIRs than in IRs (Table 1). It has been reported that only 3.4%–14% of children with a history of mild NIRs exhibited a positive DPT, experiencing only mild reactions in the DPT (3, 54, 99), which supports the avoidance of ST in non-severe cases (2, 3, 54, 57, 59, 68–73). In addition that STs could be time-consuming and painful, approximately 20% of children have been found to experience fear over their test performance (2). Accordingly, the latest recommendations of many academic societies propose avoiding STs in children particularly in NIRs following a favorable risk assessment (2, 42, 71, 97, 104–107). However, some authors consider that STs are safe and useful, and could avoid exposing children directly to the culprit BLs (58, 62, 92, 95, 99–102, 108) (Table 1). Regarding the utility of STs in NIRs with alarm signs within the spectrum of Severe Cutaneous Adverse Reactions (SCARs), a recent original article has presented findings suggesting that STs may serve as a safe and useful tool for determining the causative drug and assess cross-reactivity (109).
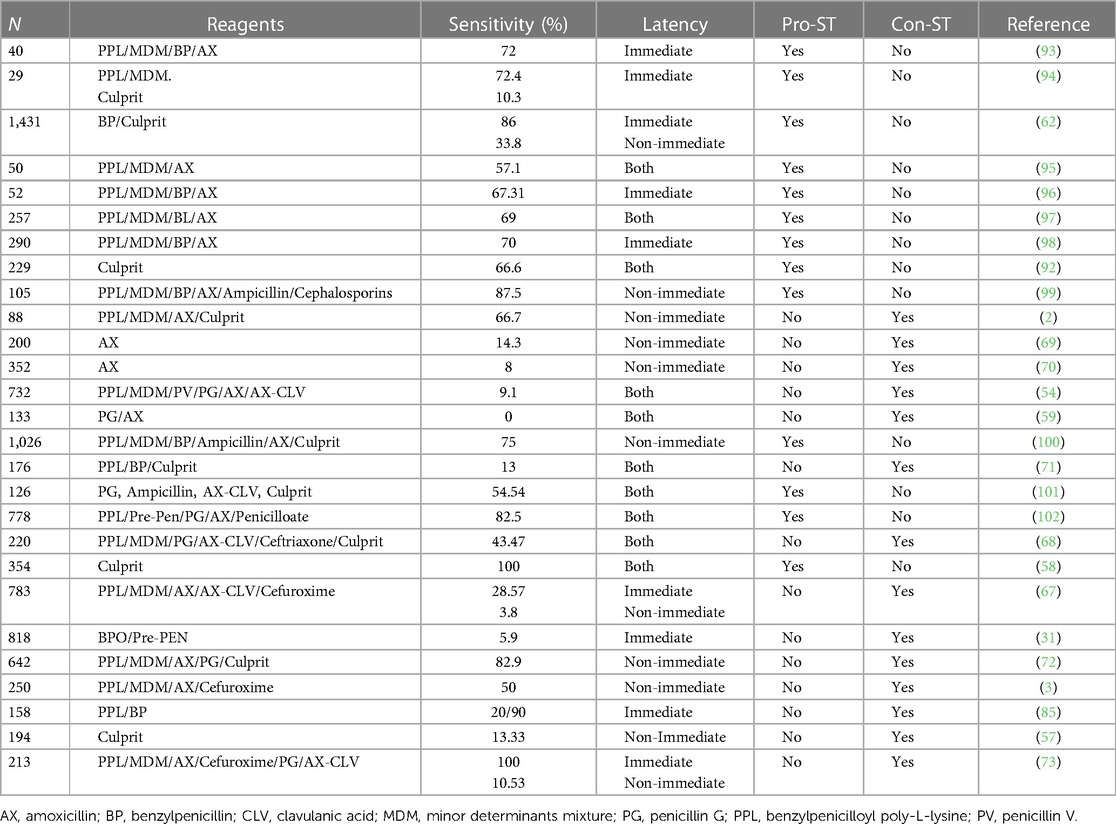
Table 1. Studies in which skin tests have been performed, showing the sensitivity of the test and whether the authors are in favor (Pro-ST) or against (Con-ST) performing the test.
5. Is there a place for in vitro testing?
In vitro tests are potential alternative methods that could help reduce the need for risky DPT; however, most of these tests are not clinically validated through well-controlled studies with large series of confirmed patients and controls. Moreover, controversies about their use still exist among American and European Scientific Societies (48). The National Institute of Allergy and Infectious Diseases (NAIAID) from the United States recommends in vitro tests for diagnosing IgE-mediated reactions when STs are neither available nor validated (110). By contrast, the European Academy of Allergy and Clinical Immunology (EAACI) has highlighted the major importance of correctly identifying these patients, to avoid severe reactions and also to decrease the percentage of children false-labeled as allergic (111). For that, a recent EAACI position paper (111) and EAACI task force (103) propose the utilization of in vitro tests for evaluating immediate severe reactions, as well as mild and severe NIRs.
In general, the decisions concerning in vitro testing are common for both adults and children, due to insufficient comparative data and significantly fewer experience and data in children (76). The position paper by the ENDA/EAACI Drug Allergy Interest Group reported good specificity but low sensitivity values in the adult population (112), which limits the diagnostic utility of these tests. The use and choice of in vitro tests is based on the mechanism involved, IgE- mediated (immediate) or T-cell-mediated (non-immediate) reactions.
5.1. IgE-mediated reactions
5.1.1. Determination of specific IgE
This method is based on the determination of serum drug-sIgE by immunoassay, and the commercial fluoro-enzyme-immunoassay (FEIA) (ImmunoCAP, ThermoFisher, Uppsala, Sweden) is the main in vitro procedure in the evaluation of IRs. However, the sensitivity values are limited (0%–50%), and evidences of not optimal specificity have been reported, related to false-positive to penicillin V and the influence of total IgE values (113–117). Moreover, its use is limited because it is only available for some BL structures (benzylpenicilloyl, amoxicilloyl, penicilloyl V, ampicilloyl, cefaclor) (118). Despite these limitations, their performance is recommended prior to in vivo tests in severe reactions, as reported by EAACI pediatric task force (106), or in complex cases with negative and/or confusing skin testing as proposed in a recent EAACI position paper (49), in order to reduce the need for DPT.
5.1.2. Basophil activation test
This a functional test based on the analysis of basophil activation in the presence of a stimulus (drug) using flow cytometry. The sensitivity value ranges from 22% to 55%, and the specificity value ranges from 79% to 96% (112, 119). Although it is a non-clinical standardized and validated test, BAT has been reported to be useful as a complementary tool (49), particularly when assessing reactions to BLs that lack a commercially available immunoassay, such as clavulanic acid (51, 120–122) and cefazolin (123, 124). In case of life-threating reactions or high-risk patients, it is recommended to perform BAT prior to in vivo tests, including skin testing (49, 112).
5.2. Non-IgE-mediated reactions
5.2.1. Lymphocyte transformation test
This is the most commonly used in vitro method for detecting T-cell-mediated reactions and is based on the identification of lymphocyte proliferation in the presence of a stimulus (drug). The sensitivity and specificity values range from 58% to 89% and from 85% to 100%, respectively (112). The differences in sensitivity values are related to clinical phenotypes, with higher values in mild and moderate reactions compared with that in severe reactions (112, 118). Although most of the studies refer to adult population, a recent study including 25 children with positive clinical histories of delayed skin reactions to amoxicillin or the amoxicillin–clavulanic acid combination confirmed by DPT showed a lymphocyte transformation test sensitivity of 52% and specificity of 92%, with a positive predictive value of 86% and a negative predictive value of 65% (125). Another study in 17 children with mild NIRs to BLs showed a sensitivity of 52.9% and a specificity of 100% (57). Despite it not being a standardized and validated test and not used routinely, it is recommended in high-risk patients prior to in vivo testing (49).
6. How to optimize DPT in children?
DPT continues to be widely regarded as the gold standard for confirming or excluding drug allergies (126). Although there is no consensus regarding DPT protocols, there is evidence on the safety and efficacy of DPT in children depending on risk stratification (42, 57, 76, 111, 127–133). One of the first questions that emerge is: when is it considered low, moderate, or high risk? Predictive models and artificial intelligence applications based on historical risk factors have been used to identify variables that can help (134) to elucidate the risk (59, 68, 135–141). In contrast to adults, risk assessment studies in children are scarce, and optimal risk definitions are controversial (76, 103). However, the last practical approaches and algorithms divide patients into low and moderate–high risk. Despite dissimilarities between some articles, there are characteristics that seem to be widely accepted. In some studies, moderate to high-risk patients are considered those who exhibit a reaction in less than 2 h following drug intake, the presence of symptoms compatible with SCARs (such us mucosal lesions, blisters, or desquamation), and/or the presence of one or more of these symptoms (facial swelling, difficulty breathing, lip swelling, wheezing, throat swelling, and drop in blood pressure) (68, 142, 143). On the other hand, low-risk patients are considered those affected with isolated pruritus, delayed urticaria that lasts more than 24 h, palmar exfoliation, or mild maculopapular exanthema.
6.1. When can direct DPT be performed?
Direct DPT implies skipping previous skin testing and proceeding to DPT as the unique assessment.
Mild NIRs such as maculopapular eruption and delayed urticaria/angioedema are the most investigated. In a prospective study published in 2021, a single-dose DPT without prior skin testing were performed in 194 children with NIRs, of which 12.4% reacted, but none was severe. Skin tests were conducted exclusively on patients who tested positive for DPT following the confirmation of allergies, showing a 13.33% positivity rate (57). Another study included 153 children who underwent direct DPT, revealing only 1.9% of reactions (128). Both studies concluded that direct DPT is a safe method for mild cutaneous NIRs.
However, little evidence is published for direct DPT for IRs in children. Although it appears to be safe for benign immediate urticaria/angioedema based on several articles, the number of participants included in these studies is limited (128, 130, 144). The largest study to date included a cohort of over 1,900 children with reported history of benign reactions to amoxicillin limited to the skin. The study involved the implementation of direct DPT without prior STs, and the results indicated that only 2.2% of participants experienced mild IRs, while 3.2% experienced NIRs. This study provides further evidence supporting the safe administration of a direct DPT in children with cutaneous symptoms surrounding a treatment with amoxicillin (97).
6.2. Using fractionated or single-dose DPT protocols?
The way of performing DPT in children is changing into a simple and less time-consuming manner going for direct and single-dose DPT in selected patients with a favorable risk stratification.
A recent article examined a cohort of 254 children who suffered a NIR to amoxicillin, either alone or in combination with clavulanic, using a graded incremental protocol and prolonged 5-day DPT at home. The study aimed to analyze the duration between the last dose intake and the onset of the observed reaction (129). Interestingly, only 6.5% of children had a positive DPT. Moreover, just one patient had a reaction during the first hour following the first 1/10 dose. The remaining patients experienced reactions more than 2 h after their last dose intake, with the majority of reactions occurring several days later. These results suggest that administering a single-dose DPT may be considered a safe approach for managing mild NIRs in pediatric patients.
In most of the studies where DPT was performed by fractionating the doses, the reactions tended to appear hours or days after the full dose was achieved, when the patient was already at home, which may suggest that a single-dose DPT could potentially offer a comparable level of safety to the multi-step approach, avoiding the need for prolonged hospital stays (69, 130, 131, 144, 145). Based on that, some articles have been published using a single-dose DPT for selected patients with mild NIRs (2, 57, 129, 146, 147). If we compare the percentage of positive DPT in NIRs between fractionated-dose protocols and single-dose protocols, they range from 1.8% to 78.9%, and from 3% to 12.5%, respectively (2, 57, 69, 129–131, 144–147).
7. Is a retest needed in children?
In IRs, it is recommended to perform a retest after an initial negative study if the reaction occurred more than 6 months ago due to the potential loss of sensitization over time, in order to avoid potentially severe reactions after subsequent prescriptions of these drugs (148). The rate of repositivization in adults has been reported to be 15%, with a potential increase to 45% in cases of immediate severe reactions (149). The rate of positive retest in children has been reported to be lower, occurring in approximately 2%–5.9% of cases after a positive oral DPT with the culprit (31, 150). The lower rate of resensitization observed in children could be explained by a long-lasting condition, in addition to the possibility that these reactions could be triggered by underlying viral infections, although they are clinically indistinguishable from allergic reactions (2, 151). However, it is important to take into account that in one of these studies, a retest was performed only with PPL and benzylpenicillin but not with amoxicillin, the involved drug in the reaction (31). Despite this, considering the low rate of resensitization, a retest is usually unnecessary in children. Although a retest seems to be unnecessary in mild reactions in children, considering the low rate of resensitization as reported in certain studies, it should be considered in cases of anaphylaxis.
8. Novel approaches for delabeling
Delabeling is routinely performed by allergists. However, the number of patients labeled as BL-allergic exceeds the capabilities of examination in many allergy clinics. Taking into account that most patients labeled as BL-allergic can safely receive this antibiotic group, delabeling could be performed by non-allergists in many cases, including pharmacists, nurses, and associate physicians (152). However, the main barrier for delabeling by non-allergists is the lack of training in this area. Therefore, various measures have been developed recently to enhance the management of antibiotic allergy labeling by non-allergists to facilitate their decisions, including educational programs (153), and implementation of visual algorithmic guidelines, digital decision support tools, and electronic health record-incorporated tools and alerts (140, 154–159). These measures have resulted in an increased confidence of non-allergists in managing antibiotic allergy labels and adherence to allergist recommendations, leading to a decrease in the use of broad-spectrum antibiotics for patients who previously reported penicillin allergies (140, 154–159).
Most of these approaches have been carried out in adults, with scarce information being available on the pediatric population. In this regard, delabeling strategies have been designed for implementation in the primary care outpatient setting, as this is the best way to reach the largest number of children with BL allergy label. It has been proposed to conduct an initial telemedicine consultation in order to screen children for a low probability of true penicillin allergy (replacing the outpatient visit), followed by a single-dose oral DPT in an outpatient setting (146). This approach was cost-saving during the COVID-19 pandemic (160), but more studies are required to consider whether this model, in primary care or as an entirely nurse-led procedure, will continue to be of value in the aftermath of Covid-19. The Standards of Care Committee of the British Society for Allergy and Clinical Immunology (BSACI) have developed a guideline to identify patients at low risk of penicillin true allergy and a framework for conducting DPT by non-allergists (161). Recently, a delabeling protocol has been developed by pediatricians to identify low-risk patients who may be allergic to BL, showing to be safe and viable for being implemented in a pediatric primary care clinic (162).
9. Conclusions
Most BL allergy labels are acquired during childhood, but only a small proportion of these patients have a true allergic response. However, this is rarely verified, and the label is carried out over adulthood, with a negative impact as they have been associated with less effective therapies, emergence of multidrug-resistant organisms, and prolonged hospital stays. Therefore, an allergological evaluation is crucial to address the delabeling of these patients, and to initiate this evaluation early in childhood to avoid false labeling in adult life. However, despite the important consequences and the high prevalence of the label of BL allergy, its management remains controversial. Due to the scarcity of studies conducted in children, the current recommendations are the same as those established for adults. The prevalence of positivity in STs among children is low, and the role of in vitro testing in this population is not well defined, being DPT considered the gold standard to confirm or discard the diagnosis of allergy and typically conducted only when preliminary tests are negative. However, novel strategies have been implemented in order to optimize a protocol for BL allergy diagnosis in the pediatric population. Several studies have demonstrated that it is possible to identify children who are at low risk of a true BL allergy and performing DPT without conducting prior skin testing in those showing non-severe reactions.
There have been significant efforts to expand BL allergy evaluations beyond allergists in order to reach the largest number of children with BL allergy label. However, more research is needed before delabeling by non-allergists can become a standard of care.
Author contributions
RS: Writing – original draft. GB: Writing – original draft. ML: Writing – original draft. AA: Writing – original draft. MS: Writing – original draft. ID: Conceptualization, Writing – original draft, Writing – review & editing. MT: Conceptualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
GB holds a contract from “Juan Rodes” program (JR18/00054) from the Institute of Health “Carlos III” of the Ministry of Economy and Competitiveness [grants co-funded by European Social Fund (ESF)]. AA holds a Senior Postdoctoral Contract (RH-0099-2020) from Andalusian Regional Ministry of Health [cofunded by European Social Fund (ESF): “Andalucía se mueve con Europa”]. The present study has been funded by Instituto de Salud Carlos III through the project “PI21/00329” and co-funded by the European Union.
Acknowledgments
The authors would like to thank Claudia Corazza for her help with the English version of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Coker TR, Chan LS, Newberry SJ, Limbos MA, Suttorp MJ, Shekelle PG, et al. Diagnosis, microbial epidemiology, and antibiotic treatment of acute otitis media in children: a systematic review. JAMA. (2010) 304(19):2161–9. doi: 10.1001/jama.2010.1651
2. Caubet JC, Kaiser L, Lemaitre B, Fellay B, Gervaix A, Eigenmann PA. The role of penicillin in benign skin rashes in childhood: a prospective study based on drug rechallenge. J Allergy Clin Immunol. (2011) 127(1):218–22. doi: 10.1016/j.jaci.2010.08.025
3. Caubet JC, Frossard C, Fellay B, Eigenmann PA. Skin tests and in vitro allergy tests have a poor diagnostic value for benign skin rashes due to beta-lactams in children. Pediatr Allergy Immunol. (2015) 26(1):80–2. doi: 10.1111/pai.12314
4. Blumenthal KG, Lu N, Zhang Y, Li Y, Walensky RP, Choi HK. Risk of meticillin resistant Staphylococcus aureus and Clostridium difficile in patients with a documented penicillin allergy: population based matched cohort study. Br Med J. (2018) 361:k2400. Available at: www.icmje.org/coi_disclosure.pdf and declare: no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. doi: 10.1136/bmj.k2400
5. Macy E, Contreras R. Health care use and serious infection prevalence associated with penicillin “allergy” in hospitalized patients: a cohort study. J Allergy Clin Immunol. (2014) 133(3):790–6. doi: 10.1016/j.jaci.2013.09.021
6. MacFadden DR, LaDelfa A, Leen J, Gold WL, Daneman N, Weber E, et al. Impact of reported beta-lactam allergy on inpatient outcomes: a multicenter prospective cohort study. Clin Infect Dis. (2016) 63(7):904–10. doi: 10.1093/cid/ciw462
7. Macy E, Contreras R. Adverse reactions associated with oral and parenteral use of cephalosporins: a retrospective population-based analysis. J Allergy Clin Immunol. (2015) 135(3):745–52. doi: 10.1016/j.jaci.2014.07.062
8. Lucas M, Arnold A, Sommerfield A, Trevenen M, Braconnier L, Schilling A, et al. Antibiotic allergy labels in children are associated with adverse clinical outcomes. J Allergy Clin Immunol Pract. (2019) 7(3):975–82. doi: 10.1016/j.jaip.2018.09.003
9. Huang KG, Cluzet V, Hamilton K, Fadugba O. The impact of reported Beta-lactam allergy in hospitalized patients with hematologic malignancies requiring antibiotics. Clin Infect Dis. (2018) 67(1):27–33. doi: 10.1093/cid/ciy037
10. Kim SH, Kim KH, Kim HB, Kim NJ, Kim EC, Oh MD, et al. Outcome of vancomycin treatment in patients with methicillin-susceptible staphylococcus aureus bacteremia. Antimicrob Agents Chemother. (2008) 52(1):192–7. doi: 10.1128/AAC.00700-07
11. McDanel DL, Azar AE, Dowden AM, Murray-Bainer S, Noiseux NO, Willenborg M, et al. Screening for beta-lactam allergy in joint arthroplasty patients to improve surgical prophylaxis practice. J Arthroplasty. (2017) 32(9S):S101–S8. doi: 10.1016/j.arth.2017.01.012
12. Park M, Markus P, Matesic D, Li JT. Safety and effectiveness of a preoperative allergy clinic in decreasing vancomycin use in patients with a history of penicillin allergy. Ann Allergy Asthma Immunol. (2006) 97(5):681–7. doi: 10.1016/S1081-1206(10)61100-3
13. Krishna MT, Huissoon AP, Li M, Richter A, Pillay DG, Sambanthan D, et al. Enhancing antibiotic stewardship by tackling “spurious” penicillin allergy. Clin Exp Allergy. (2017) 47(11):1362–73. doi: 10.1111/cea.13044
14. Li M, Krishna MT, Razaq S, Pillay D. A real-time prospective evaluation of clinical pharmaco-economic impact of diagnostic label of “penicillin allergy” in a UK teaching hospital. J Clin Pathol. (2014) 67(12):1088–92. doi: 10.1136/jclinpath-2014-202438
15. Picard M, Begin P, Bouchard H, Cloutier J, Lacombe-Barrios J, Paradis J, et al. Treatment of patients with a history of penicillin allergy in a large tertiary-care academic hospital. J Allergy Clin Immunol: in PractIn Practice. (2013) 1(3):252–7. doi: 10.1016/j.jaip.2013.01.006
16. Catalano AC, Pittet LF, Choo S, Segal A, Stephens D, Cranswick NE, et al. Impact of antibiotic allergy labels on patient outcomes in a tertiary paediatric hospital. Br J Clin Pharmacol. (2022) 88(3):1107–14. doi: 10.1111/bcp.15038
17. MacLaughlin EJ, Saseen JJ, Malone DC. Costs of beta-lactam allergies: selection and costs of antibiotics for patients with a reported beta-lactam allergy. Arch Fam Med. (2000) 9(8):722–6. doi: 10.1001/archfami.9.8.722
18. Moran R, Devchand M, Smibert O, Trubiano JA. Antibiotic allergy labels in hospitalized and critically ill adults: a review of current impacts of inaccurate labelling. Br J Clin Pharmacol. (2019) 85(3):492–500. doi: 10.1111/bcp.13830
19. Charneski L, Deshpande G, Smith SW. Impact of an antimicrobial allergy label in the medical record on clinical outcomes in hospitalized patients. Pharmacotherapy. (2011) 31(8):742–7. doi: 10.1592/phco.31.8.742
20. Jeffres MN, Narayanan PP, Shuster JE, Schramm GE. Consequences of avoiding beta-lactams in patients with beta-lactam allergies. J Allergy Clin Immunol. (2016) 137(4):1148–53. doi: 10.1016/j.jaci.2015.10.026
21. Blumenthal KG, Wickner PG, Hurwitz S, Pricco N, Nee AE, Laskowski K, et al. Tackling inpatient penicillin allergies: assessing tools for antimicrobial stewardship. J Allergy Clin Immunol. (2017) 140(1):154–61. doi: 10.1016/j.jaci.2017.02.005
22. Trubiano JA, Chen C, Cheng AC, Grayson ML, Slavin MA, Thursky KA, et al. Antimicrobial allergy “labels” drive inappropriate antimicrobial prescribing: lessons for stewardship. J Antimicrob Chemother. (2016) 71(6):1715–22. doi: 10.1093/jac/dkw008
23. Sousa-Pinto B, Araujo L, Freitas A, Delgado L. Hospitalizations in children with a penicillin allergy label: an assessment of healthcare impact. Int Arch Allergy Immunol. (2018) 176(3–4):234–8. doi: 10.1159/000488857
24. Sade K, Holtzer I, Levo Y, Kivity S. The economic burden of antibiotic treatment of penicillin-allergic patients in internal medicine wards of a general tertiary care hospital. Clin Exp Allergy. (2003) 33(4):501–6. doi: 10.1046/j.1365-2222.2003.01638.x
25. McDanel JS, Perencevich EN, Diekema DJ, Herwaldt LA, Smith TC, Chrischilles EA, et al. Comparative effectiveness of beta-lactams versus vancomycin for treatment of methicillin-susceptible Staphylococcus aureus bloodstream infections among 122 hospitals. Clin Infect Dis. (2015) 61(3):361–7. doi: 10.1093/cid/civ308
26. Vyles D, Chiu A, Simpson P, Nimmer M, Adams J, Brousseau DC. Parent-reported penicillin allergy symptoms in the pediatric emergency department. Acad Pediatr. (2017) 17(3):251–5. doi: 10.1016/j.acap.2016.11.004
27. Abrams EM, Atkinson AR, Wong T, Ben-Shoshan M. The importance of delabeling beta-lactam allergy in children. J Pediatr. (2019) 204:291–7. doi: 10.1016/j.jpeds.2018.09.035
28. Trubiano JA, Adkinson NF, Phillips EJ. Penicillin allergy is not necessarily forever. JAMA. (2017) 318(1):82–3. doi: 10.1001/jama.2017.6510
29. Romano A, Caubet JC. Antibiotic allergies in children and adults: from clinical symptoms to skin testing diagnosis. J Allergy Clin Immunol Pract. (2014) 2(1):3–12. doi: 10.1016/j.jaip.2013.11.006
30. Grinlington L, Cranswick N, Gwee A. QUESTION 1: what is the risk of a repeat reaction to amoxicillin or a cephalosporin in children with a history of a non-immediate reaction to amoxicillin? Arch Dis Child. (2017) 102(3):285–8. doi: 10.1136/archdischild-2016-312089
31. Mill C, Primeau MN, Medoff E, Lejtenyi C, O'Keefe A, Netchiporouk E, et al. Assessing the diagnostic properties of a graded oral provocation challenge for the diagnosis of immediate and nonimmediate reactions to amoxicillin in children. JAMA Pediatr. (2016) 170(6):e160033. doi: 10.1001/jamapediatrics.2016.0033
32. Bernaola M. Rodriguez Del Rio P. De-labelling of beta-lactam allergy in children. Clin Exp Allergy. (2022) 52(4):485–8. doi: 10.1111/cea.14125
33. Abrams EM, Wakeman A, Gerstner TV, Warrington RJ, Singer AG. Prevalence of beta-lactam allergy: a retrospective chart review of drug allergy assessment in a predominantly pediatric population. Allergy Asthma Clin Immunol. (2016) 12:59. doi: 10.1186/s13223-016-0165-6
34. Seitz CS, Brocker EB, Trautmann A. Diagnosis of drug hypersensitivity in children and adolescents: discrepancy between physician-based assessment and results of testing. Pediatr Allergy Immunol. (2011) 22(4):405–10. doi: 10.1111/j.1399-3038.2011.01134.x
35. Blumenthal KG, Peter JG, Trubiano JA, Phillips EJ. Antibiotic allergy. Lancet. (2019) 393(10167):183–98. doi: 10.1016/S0140-6736(18)32218-9
36. Sacco KA, Bates A, Brigham TJ, Imam JS, Burton MC. Clinical outcomes following inpatient penicillin allergy testing: a systematic review and meta-analysis. Allergy. (2017) 72(9):1288–96. doi: 10.1111/all.13168
37. Stone CA Jr., Trubiano J, Coleman DT, Rukasin CRF, Phillips EJ. The challenge of de-labeling penicillin allergy. Allergy. (2020) 75(2):273–88. doi: 10.1111/all.13848
38. Au LYC, Siu AM, Yamamoto LG. Cost and risk analysis of lifelong penicillin allergy. Clin Pediatr (Phila). (2019) 58(11–12):1309–14. doi: 10.1177/0009922819853014
39. Chen JR, Tarver SA, Alvarez KS, Tran T, Khan DA. A proactive approach to penicillin allergy testing in hospitalized patients. J Allergy Clin Immunol Pract. (2017) 5(3):686–93. doi: 10.1016/j.jaip.2016.09.045
40. Rimawi RH, Cook PP, Gooch M, Kabchi B, Ashraf MS, Rimawi BH, et al. The impact of penicillin skin testing on clinical practice and antimicrobial stewardship. J Hosp Med. (2013) 8(6):341–5. doi: 10.1002/jhm.2036
41. Maduemem K, Clark H, Sohal I, Dawson T, Makwana N. Paediatric research across the midlands N. Barriers to paediatric penicillin allergy de-labelling in UK secondary care: a regional survey. Arch Dis Child. (2023) 108(5):363–6. doi: 10.1136/archdischild-2022-324564
42. Khan DA, Banerji A, Blumenthal KG, Phillips EJ, Solensky R, White AA, et al. Drug allergy: a 2022 practice parameter update. J Allergy Clin Immunol. (2022) 150(6):1333–93. doi: 10.1016/j.jaci.2022.08.028
43. Torres MJ, Blanca M. The complex clinical picture of beta-lactam hypersensitivity: penicillins, cephalosporins, monobactams, carbapenems, and clavams. Med Clin North Am. (2010) 94(4):805–20., xii. doi: 10.1016/j.mcna.2010.04.006
44. Gell PGH, Coombs RRA. Clinical aspects of immunology. Oxford: Blackwell Scientific Publications (1963).
45. Blanca M, Mayorga C, Torres MJ, Warrington R, Romano A, Demoly P, et al. Side-chain-specific reactions to betalactams: 14 years later. Clin Exp Allergy. (2002) 32(2):192–7. doi: 10.1046/j.1365-2222.2002.01299.x
46. Pichler WJ. The p-i concept: pharmacological interaction of drugs with immune receptors. World Allergy Organ J. (2008) 1(6):96–102. doi: 10.1097/WOX.0b013e3181778282
47. Demoly P, Adkinson NF, Brockow K, Castells M, Chiriac AM, Greenberger PA, et al. International consensus on drug allergy. Allergy. (2014) 69(4):420–37. doi: 10.1111/all.12350
48. Torres MJ, Romano A, Celik G, Demoly P, Khan DA, Macy E, et al. Approach to the diagnosis of drug hypersensitivity reactions: similarities and differences between Europe and North America. Clin Transl Allergy. (2017) 7:7. doi: 10.1186/s13601-017-0144-0
49. Romano A, Atanaskovic-Markovic M, Barbaud A, Bircher AJ, Brockow K, Caubet JC, et al. Towards a more precise diagnosis of hypersensitivity to beta-lactams—an EAACI position paper. Allergy. (2019) 75(6):1300–15. doi: 10.1111/all.14122
50. Romano A, Gaeta F, Arribas Poves MF, Valluzzi RL. Cross-reactivity among beta-lactams. Curr Allergy Asthma Rep. (2016) 16(3):24. doi: 10.1007/s11882-016-0594-9
51. Torres MJ, Ariza A, Mayorga C, Dona I, Blanca-Lopez N, Rondon C, et al. Clavulanic acid can be the component in amoxicillin-clavulanic acid responsible for immediate hypersensitivity reactions. J Allergy Clin Immunol. (2010) 125(2):502–5. doi: 10.1016/j.jaci.2009.11.032
52. Freundt Serpa NP, Sanchez-Morillas L, Jaqueti Moreno P, Gonzalez-Gutierrez ML, Cimarra M, Cerecedo I, et al. Drug-Induced enterocolitis syndrome due to amoxicillin-clavulanic acid with good tolerance to penicillin. J Investig Allergol Clin Immunol. (2020) 30(4):301–2. doi: 10.18176/jiaci.0500
53. Sanchez-Morillas L, Perez-Ezquerra PR, Reano-Martos M, Laguna-Martinez JJ, Sanz ML, Martinez LM. Selective allergic reactions to clavulanic acid: a report of 9 cases. J Allergy Clin Immunol. (2010) 126(1):177–9. doi: 10.1016/j.jaci.2010.03.012
54. Ibanez MD, Rodriguez Del Rio P, Lasa EM, Joral A, Ruiz-Hornillos J, Munoz C, et al. Prospective assessment of diagnostic tests for pediatric penicillin allergy: from clinical history to challenge tests. Ann Allergy Asthma Immunol. (2018) 121(2):235–44. doi: 10.1016/j.anai.2018.05.013
55. Regateiro FS, Rezende I, Pinto N, Abreu C, Carreiro-Martins P, Gomes ER. Short and extended provocation tests have similar negative predictive value in non-immediate hypersensitivity to beta-lactams in children. Allergol Immunopathol (Madr). (2019) 47(5):477–83. doi: 10.1016/j.aller.2019.01.004
56. Moral L, Caubet JC. Oral challenge without skin tests in children with non-severe beta-lactam hypersensitivity: time to change the paradigm? Pediatr Allergy Immunol. (2017) 28(8):724–7. doi: 10.1111/pai.12800
57. Prieto A, Munoz C, Bogas G, Fernandez-Santamaria R, Palomares F, Mayorga C, et al. Single-dose prolonged drug provocation test, without previous skin testing, is safe for diagnosing children with mild non-immediate reactions to beta-lactams. Allergy. (2021) 76(8):2544–54. doi: 10.1111/all.14800
58. Ben Romdhane H, Ben Fredj N, Ben Fadhel N, Chadli Z, Abderrahmen A, Boughattas NA, et al. Beta-lactam hypersensitivity in children: frequency and risk factors. Br J Clin Pharmacol. (2023) 89(1):150–7. doi: 10.1111/bcp.14647
59. Faitelson Y, Boaz M, Asthma DI. Family history of drug allergy, and age predict amoxicillin allergy in children. J Allergy Clin Immunol Pract. (2018) 6(4):1363–7. doi: 10.1016/j.jaip.2017.11.015
60. Ariza A, Fernandez TD, Mayorga C, Blanca M, Torres MJ. Prediction of hypersensitivity to antibiotics: what factors need to be considered? Expert Rev Clin Immunol. (2013) 9(12):1279–88. doi: 10.1586/1744666X.2013.852957
61. Cornejo-Garcia JA, Gueant-Rodriguez RM, Torres MJ, Blanca-Lopez N, Tramoy D, Romano A, et al. Biological and genetic determinants of atopy are predictors of immediate-type allergy to betalactams, in Spain. Allergy. (2012) 67(9):1181–5. doi: 10.1111/j.1398-9995.2012.02867.x
62. Ponvert C, Perrin Y, Bados-Albiero A, Le Bourgeois M, Karila C, Delacourt C, et al. Allergy to betalactam antibiotics in children: results of a 20-year study based on clinical history, skin and challenge tests. Pediatr Allergy Immunol. (2011) 22(4):411–8. doi: 10.1111/j.1399-3038.2011.01169.x
63. Arikoglu T, Aslan G, Batmaz SB, Eskandari G, Helvaci I, Kuyucu S. Diagnostic evaluation and risk factors for drug allergies in children: from clinical history to skin and challenge tests. Int J Clin Pharm. (2015) 37(4):583–91. doi: 10.1007/s11096-015-0100-9
64. Sipahi Cimen S, Hizli Demirkale Z, Yucel E, Ozceker D, Suleyman A, Sayili U, et al. Risk factors of challenge-proven Beta-lactam allergy in children with immediate and non-immediate mild cutaneous reactions. Int Arch Allergy Immunol. (2023) 184(6):539–49. doi: 10.1159/000529084
65. Srisuwatchari W, Phinyo P, Chiriac AM, Saokaew S, Kulalert P. The safety of the direct drug provocation test in beta-lactam hypersensitivity in children: a systematic review and meta-analysis. J Allergy Clin Immunol Pract. (2023) 11(2):506–18. doi: 10.1016/j.jaip.2022.11.035
66. Demirhan A, Yildirim DD, Arikoglu T, Ozhan AK, Tokmeci N, Yuksek BC, et al. A combined risk modeling strategy for clinical prediction of beta-lactam allergies in children. Allergy Asthma Proc. (2021) 42(6):e159–e66. doi: 10.2500/aap.2021.42.210068
67. Zambonino MA, Corzo JL, Munoz C, Requena G, Ariza A, Mayorga C, et al. Diagnostic evaluation of hypersensitivity reactions to beta-lactam antibiotics in a large population of children. Pediatr Allergy Immunol. (2014) 25(1):80–7. doi: 10.1111/pai.12155
68. de Castro E D, Carolino F, Carneiro-Leao L, Barbosa J, Ribeiro L, Cernadas JR. Allergy to beta-lactam antibiotics in children: risk factors for a positive diagnostic work-up. Allergol Immunopathol (Madr). (2020) 48(5):417–23. doi: 10.1016/j.aller.2020.01.005
69. Mori F, Cianferoni A, Barni S, Pucci N, Rossi ME, Novembre E. Amoxicillin allergy in children: five-day drug provocation test in the diagnosis of nonimmediate reactions. J Allergy Clin Immunol Pract. (2015) 3(3):375–80. doi: 10.1016/j.jaip.2014.11.001
70. Barni S, Mori F, Sarti L, Pucci N, Rossi EM, de Martino M, et al. Utility of skin testing in children with a history of non-immediate reactions to amoxicillin. Clin Exp Allergy. (2015) 45(9):1472–4. doi: 10.1111/cea.12596
71. Arnold A, Sommerfield A, Ramgolam A, Rueter K, Muthusamy S, Noble V, et al. The role of skin testing and extended antibiotic courses in assessment of children with penicillin allergy: an Australian experience. J Paediatr Child Health. (2019) 55(4):428–32. doi: 10.1111/jpc.14220
72. Confino-Cohen R, Rosman Y, Meir-Shafrir K, Stauber T, Lachover-Roth I, Hershko A, et al. Oral challenge without skin testing safely excludes clinically significant delayed-onset penicillin hypersensitivity. J Allergy Clin Immunol Pract. (2017) 5(3):669–75. doi: 10.1016/j.jaip.2017.02.023
73. Vila L, Garcia V, Martinez Azcona O, Pineiro L, Meijide A, Balboa V. Mild to moderate hypersensitivity reactions to beta-lactams in children: a single-centre retrospective review. BMJ paediatrics Open. (2019) 3(1):e000435. doi: 10.1136/bmjpo-2019-000435
74. Bauer ME, MacBrayne C, Stein A, Searns J, Hicks A, Sarin T, et al. A multidisciplinary quality improvement initiative to facilitate penicillin allergy delabeling among hospitalized pediatric patients. Hosp Pediatr. (2021) 11(5):427–34. doi: 10.1542/hpeds.2020-001636
75. Vyles D, Antoon JW, Norton A, Stone CA Jr., Trubiano J, Radowicz A, et al. Children with reported penicillin allergy: public health impact and safety of delabeling. Ann Allergy Asthma Immunol. (2020) 124(6):558–65. doi: 10.1016/j.anai.2020.03.012
76. Arikoglu T, Kuyucu S, Caubet JC. New diagnostic perspectives in the management of pediatric beta-lactam allergy. Pediatr Allergy Immunol. (2022) 33(3):e13745. doi: 10.1111/pai.13745
77. Macy E, Ensina LF. Controversies in allergy: is skin testing required prior to drug challenges? J Allergy Clin Immunol Pract. (2019) 7(2):412–7. doi: 10.1016/j.jaip.2018.09.008
78. Eser Simsek I, Tuba Cogurlu M, Aydogan M. Suspected reaction with cephalosporin may be a predictive factor for beta-lactam allergy in children. Int Arch Allergy Immunol. (2019) 178(3):248–54. doi: 10.1159/000494506
79. Plager J, Judd A, Blumenthal K. Role of clinical history in beta-lactam hypersensitivity. Curr Opin Allergy Clin Immunol. (2021) 21(4):320–6. doi: 10.1097/ACI.0000000000000758
80. Chiriac AM, Banerji A, Gruchalla RS, Thong BYH, Wickner P, Mertes PM, et al. Controversies in drug allergy: drug allergy pathways. J Allergy Clin Immunol Pract. (2019) 7(1):46–60. doi: 10.1016/j.jaip.2018.07.037
81. Roberts H, Soller L, Ng K, Chan ES, Roberts A, Kang K, et al. First pediatric electronic algorithm to stratify risk of penicillin allergy. Allergy Asthma Clin Immunol. (2020) 16(1):103. doi: 10.1186/s13223-020-00501-6
82. Padial A, Antunez C, Blanca-Lopez N, Fernandez TD, Cornejo-Garcia JA, Mayorga C, et al. Non-immediate reactions to beta-lactams: diagnostic value of skin testing and drug provocation test. Clin Exp Allergy. (2008) 38(5):822–8. doi: 10.1111/j.1365-2222.2008.02961.x
83. Romano A, Gaeta F, Valluzzi RL, Caruso C, Rumi G, Bousquet PJ. The very limited usefulness of skin testing with penicilloyl-polylysine and the minor determinant mixture in evaluating nonimmediate reactions to penicillins. Allergy. (2010) 65(9):1104–7. doi: 10.1111/j.1398-9995.2009.02318.x
84. Sousa-Pinto B, Tarrio I, Blumenthal KG, Araujo L, Azevedo LF, Delgado L, et al. Accuracy of penicillin allergy diagnostic tests: a systematic review and meta-analysis. J Allergy Clin Immunol. (2021) 147(1):296–308. doi: 10.1016/j.jaci.2020.04.058
85. Labrosse R, Paradis L, Samaan K, Lacombe-Barrios J, Paradis J, Begin P, et al. Sensitivity and specificity of double-blinded penicillin skin testing in relation to oral provocation with amoxicillin in children. Allergy Asthma Clin Immunol. (2020) 16:57. doi: 10.1186/s13223-020-00449-7
86. Jost BC, Wedner HJ, Bloomberg GR. Elective penicillin skin testing in a pediatric outpatient setting. Ann Allergy Asthma Immunol. (2006) 97(6):807–12. doi: 10.1016/S1081-1206(10)60973-8
87. Solensky R, Khan DA. Evaluation of antibiotic allergy: the role of skin tests and drug challenges. Curr Allergy Asthma Rep. (2014) 14(9):459. doi: 10.1007/s11882-014-0459-z
88. Mayorga C, Montanez MI, Najera F, Bogas G, Fernandez TD, Gil DR, et al. The role of benzylpenicilloyl epimers in specific IgE recognition. Front Pharmacol. (2021) 12:585890. doi: 10.3389/fphar.2021.585890
89. Torres MJ, Blanca M, Fernandez J, Romano A, Weck A, Aberer W, et al. Diagnosis of immediate allergic reactions to beta-lactam antibiotics. Allergy. (2003) 58(10):961–72. doi: 10.1034/j.1398-9995.2003.00280.x
90. Salas M, Laguna JJ, Dona I, Barrionuevo E, Fernandez-Santamaria R, Ariza A, et al. Patients taking amoxicillin-clavulanic can become simultaneously sensitized to both drugs. J Allergy Clin Immunol Pract. (2017) 5(3):694–702. doi: 10.1016/j.jaip.2017.02.007
91. Dudgeon M, Carrillo-Martin I, Gonzalez-Estrada A. Anaphylaxis to amoxicillin-clavulanate: differentiating the components. Ann Allergy Asthma Immunol. (2019) 122(4):427–8. doi: 10.1016/j.anai.2019.01.005
92. Diaferio L, Chiriac AM, Leoni MC, Castagnoli R, Caimmi S, Miniello VL, et al. Skin tests are important in children with beta-lactam hypersensitivity, but may be reduced in number. Pediatr Allergy Immunol. (2019) 30(4):462–8. doi: 10.1111/pai.13041
93. Blanca-Lopez N, Perez-Alzate D, Ruano F, Garcimartin M, de la Torre V, Mayorga C, et al. Selective immediate responders to amoxicillin and clavulanic acid tolerate penicillin derivate administration after confirming the diagnosis. Allergy. (2015) 70(8):1013–9. doi: 10.1111/all.12636
94. Celik GE, Aydin O, Dogu F, Cipe F, Boyvat A, Ikinciogullari A, et al. Diagnosis of immediate hypersensitivity to β-lactam antibiotics can be made safely with current approaches. Int Arch Allergy Immunol. (2012) 157(3):311–7. doi: 10.1159/000328212
95. Richter AG, Wong G, Goddard S, Heslegrave J, Derbridge C, Srivastava S, et al. Retrospective case series analysis of penicillin allergy testing in a UK specialist regional allergy clinic. J Clin Pathol. (2011) 64(11):1014–8. doi: 10.1136/jcp.2010.088203
96. Antico A, Pagani M, Compalati E, Vescovi PP, Passalacqua G. Risk assessment of immediate systemic reactions from skin tests with β-lactam antibiotics. Int Arch Allergy Immunol. (2011) 156(4):427–33. doi: 10.1159/000324461
97. Exius R, Gabrielli S, Abrams EM, O'Keefe A, Protudjer JLP, Lavine E, et al. Establishing amoxicillin allergy in children through direct graded oral challenge (GOC): evaluating risk factors for positive challenges, safety, and risk of crossreactivity to cephalosporines. J Allergy Clin Immunol Pract. (2021) 9(11):4060–6. doi: 10.1016/j.jaip.2021.06.057
98. Torres MJ, Romano A, Mayorga C, Moya MC, Guzman AE, Reche M, et al. Diagnostic evaluation of a large group of patients with immediate allergy to penicillins: the role of skin testing. Allergy. (2001) 56(9):850–6. doi: 10.1034/j.1398-9995.2001.00089.x
99. Romano A, Gaeta F, Valluzzi RL, Caruso C, Alonzi C, Viola M, et al. Diagnosing nonimmediate reactions to cephalosporins. J Allergy Clin Immunol. (2012) 129(4):1166–9. doi: 10.1016/j.jaci.2011.12.995
100. Atanaskovic-Markovic M, Gaeta F, Medjo B, Gavrovic-Jankulovic M, Cirkovic Velickovic T, Tmusic V, et al. Non-immediate hypersensitivity reactions to beta-lactam antibiotics in children—our 10-year experience in allergy work-up. Pediatr Allergy Immunol. (2016) 27(5):533–8. doi: 10.1111/pai.12565
101. Manuyakorn W, Singvijarn P, Benjaponpitak S, Kamchaisatian W, Rerkpattanapipat T, Sasisakulporn C, et al. Skin testing with beta-lactam antibiotics for diagnosis of beta-lactam hypersensitivity in children. Asian Pac J Allergy Immunol. (2016) 34(3):242–7. doi: 10.12932/AP0750
102. Fox SJ, Park MA. Penicillin skin testing is a safe and effective tool for evaluating penicillin allergy in the pediatric population. J Allergy Clin Immunol Pract. (2014) 2(4):439–44. doi: 10.1016/j.jaip.2014.04.013
103. Blanca-Lopez N, Atanaskovic-Markovic M, Gomes ER, Kidon M, Kuyucu S, Mori F, et al. An EAACI task force report on allergy to beta-lactams in children: clinical entities and diagnostic procedures. Pediatr Allergy Immunol. (2021) 32(7):1426–36. doi: 10.1111/pai.13529
104. Wong T, Atkinson A, t'Jong G, Rieder MJ, Chan ES, Abrams EM. Beta-lactam allergy in the paediatric population. Paediatr Child Health. (2020) 25(1):62–3. doi: 10.1093/pch/pxz179
105. Iammatteo M, Lezmi G, Confino-Cohen R, Tucker M, Ben-Shoshan M, Caubet JC. Direct challenges for the evaluation of Beta-lactam allergy: evidence and conditions for not performing skin testing. J Allergy Clin Immunol Pract. (2021) 9(8):2947–56. doi: 10.1016/j.jaip.2021.04.073
106. Gomes ER, Brockow K, Kuyucu S, Saretta F, Mori F, Blanca-Lopez N, et al. Drug hypersensitivity in children: report from the pediatric task force of the EAACI drug allergy interest group. Allergy. (2016) 71(2):149–61. doi: 10.1111/all.12774
107. Torres MJ, Adkinson NF Jr., Caubet JC, Khan DA, Kidon MI, Mendelson L, et al. Controversies in drug allergy: beta-lactam hypersensitivity testing. J Allergy Clin Immunol Pract. (2019) 7(1):40–5. doi: 10.1016/j.jaip.2018.07.051
108. Bousquet PJ, Pipet A, Bousquet-Rouanet L, Demoly P. Oral challenges are needed in the diagnosis of beta-lactam hypersensitivity. Clin Exp Allergy. (2008) 38(1):185–90. doi: 10.1111/j.1365-2222.2007.02867.x
109. Ben Romdhane H, Fadhel NB, Chadli Z, Chaabane A, Benzarti W, Fredj NB, et al. Drug reaction with eosinophilia and systemic symptoms in a paediatric population: interest of skin tests. Contact Dermatitis. (2023). doi: 10.1111/cod.14416
110. Wheatley LM, Plaut M, Schwaninger JM, Banerji A, Castells M, Finkelman FD, et al. Report from the national institute of allergy and infectious diseases workshop on drug allergy. J Allergy Clin Immunol. (2015) 136(2):262–71. doi: 10.1016/j.jaci.2015.05.027
111. Atanaskovic-Markovic M, Gomes E, Cernadas JR, du Toit G, Kidon M, Kuyucu S, et al. Diagnosis and management of drug-induced anaphylaxis in children: an EAACI position paper. Pediatr Allergy Immunol. (2019) 30(3):269–76. doi: 10.1111/pai.13034
112. Mayorga C, Celik G, Rouzaire P, Whitaker P, Bonadonna P, Rodrigues-Cernadas J, et al. In vitro tests for drug hypersensitivity reactions: an ENDA/EAACI drug allergy interest group position paper. Allergy. (2016) 71(8):1103–34. doi: 10.1111/all.12886
113. Fontaine C, Mayorga C, Bousquet PJ, Arnoux B, Torres MJ, Blanca M, et al. Relevance of the determination of serum-specific IgE antibodies in the diagnosis of immediate beta-lactam allergy. Allergy. (2007) 62(1):47–52. doi: 10.1111/j.1398-9995.2006.01268.x
114. Ariza A, Mayorga C, Bogas G, Gaeta F, Salas M, Valluzzi RL, et al. Detection of Serum-specific IgE by fluoro-enzyme immunoassay for diagnosing type I hypersensitivity reactions to penicillins. Int J Mol Sci. (2022) 23(13):6992. doi: 10.3390/ijms23136992
115. Macy E, Goldberg B, Poon KY. Use of commercial anti-penicillin IgE fluorometric enzyme immunoassays to diagnose penicillin allergy. Ann Allergy Asthma Immunol. (2010) 105(2):136–41. doi: 10.1016/j.anai.2010.06.014
116. Vultaggio A, Matucci A, Virgili G, Rossi O, Fili L, Parronchi P, et al. Influence of total serum IgE levels on the in vitro detection of beta-lactams-specific IgE antibodies. Clin Exp Allergy. (2009) 39(6):838–44. doi: 10.1111/j.1365-2222.2009.03219.x
117. Johansson SG, Adedoyin J, van Hage M, Gronneberg R, Nopp A. False-positive penicillin immunoassay: an unnoticed common problem. J Allergy Clin Immunol. (2013) 132(1):235–7. doi: 10.1016/j.jaci.2012.11.017
118. Saretta F, Tomei L, Mori F, Mayorga C. In vitro diagnostic testing for drug allergy in children. Pediatr Allergy Immunol. (2023) 34(4):e13955. doi: 10.1111/pai.13955
119. Cespedes JA, Fernandez-Santamaria R, Ariza A, Bogas G, Dona I, Rondon C, et al. Diagnosis of immediate reactions to amoxicillin: comparison of basophil activation markers CD63 and CD203c in a prospective study. Allergy. (2023) 78(10):2745–55. doi: 10.1111/all.15610
120. Salas M, Fernandez-Santamaria R, Mayorga C, Barrionuevo E, Ariza A, Posadas T, et al. Use of the basophil activation test may reduce the need for drug provocation in amoxicillin-clavulanic allergy. J Allergy Clin Immunol Pract. (2018) 6(3):1010–8. doi: 10.1016/j.jaip.2017.08.009
121. Longo N, Gamboa PM, Gastaminza G, Audicana MT, Antepara I, Jauregui I, et al. Diagnosis of clavulanic acid allergy using basophil activation and leukotriene release by basophils. J Investig Allergol Clin Immunol. (2008) 18(6):473–5. PMID: 1912344119123441
122. Barbero N, Fernandez-Santamaria R, Mayorga C, Martin-Serrano A, Salas M, Bogas G, et al. Identification of an antigenic determinant of clavulanic acid responsible for IgE-mediated reactions. Allergy. (2019) 74(8):1490–501. doi: 10.1111/all.13761
123. Uyttebroek AP, Decuyper II, Bridts CH, Romano A, Hagendorens MM, Ebo DG, et al. Cefazolin hypersensitivity: toward optimized diagnosis. J Allergy Clin Immunol Pract. (2016) 4(6):1232–6. doi: 10.1016/j.jaip.2016.05.011
124. Bogas G, Dona I, Dionicio J, Fernandez TD, Mayorga C, Boteanu C, et al. Diagnostic approach of hypersensitivity reactions to cefazolin in a large prospective cohort. J Allergy Clin Immunol Pract. (2021) 9(12):4421–30. doi: 10.1016/j.jaip.2021.08.017
125. Mori F, Fili L, Sarti L, Capone M, Liccioli G, Giovannini M, et al. Sensitivity and specificity of lymphocyte transformation test in children with mild delayed hypersensitivity reactions to beta-lactams. Allergy. (2020) 75(10):2696–9. doi: 10.1111/all.14358
126. Moral L, Mori F. Drug provocation tests in children: all that glitters is not gold. Pediatr Allergy Immunol. (2023) 34(8):e14002. doi: 10.1111/pai.14002
127. Jaoui A, Delalande D, Siouti S, Benoist G, Seve E, Ponvert C, et al. Safety and cost effectiveness of supervised ambulatory drug provocation tests in children with mild non-immediate reactions to beta-lactams. Allergy. (2019) 74(12):2482–4. doi: 10.1111/all.13871
128. Pachasidchai C, Suksawat Y, Yooma P, Kiewngam P, Jotikasthira W, Sawatchai A, et al. Safety of direct oral provocation in children with mild beta-lactam hypersensitivity reactions. Pediatr Allergy Immunol. (2023) 34(2):e13927. doi: 10.1111/pai.13927
129. Liccioli G, Giovannini M, Caubet JC, Barni S, Sarti L, Parronchi P, et al. Simplifying the drug provocation test in non-immediate hypersensitivity reactions to amoxicillin in children: the experience of a tertiary care allergy unit. Pediatr Allergy Immunol. (2022) 33(6):e13809. doi: 10.1111/pai.13809
130. Chiriac AM, Rerkpattanapipat T, Bousquet PJ, Molinari N, Demoly P. Optimal step doses for drug provocation tests to prove beta-lactam hypersensitivity. Allergy. (2017) 72(4):552–61. doi: 10.1111/all.13037
131. Pouessel G, Winter N, Lejeune S, Thumerelle C, Deschildre A. Oral challenge without skin testing in children with suspected non-severe betalactam hypersensitivity. Pediatr Allergy Immunol. (2019) 30(4):488–90. doi: 10.1111/pai.13048
132. Dona I, Romano A, Torres MJ. Algorithm for betalactam allergy diagnosis. Allergy. (2019) 74(9):1817–9. doi: 10.1111/all.13844
133. Torres-Rojas I, Perez-Alzate D, Somoza ML, Haroun Diaz E, Ruano Perez FJ, Prieto-Moreno Pfeifer A, et al. Patterns of response and drugs involved in hypersensitivity reactions to beta-lactams in children. Pediatr Allergy Immunol. (2021) 32(8):1788–95. doi: 10.1111/pai.13608
134. Piotin A, Godet J, Trubiano JA, Grandbastien M, Guenard-Bilbault L, de Blay F, et al. Predictive factors of amoxicillin immediate hypersensitivity and validation of PEN-FAST clinical decision rule. Ann Allergy Asthma Immunol. (2022) 128(1):27–32. doi: 10.1016/j.anai.2021.07.005
135. Hierro Santurino B, Mateos Conde J, Cabero Moran MT, Miron Canelo JA, Armentia Medina A. A predictive model for the diagnosis of allergic drug reactions according to the medical history. J Allergy Clin Immunol Pract. (2016) 4(2):292–300. doi: 10.1016/j.jaip.2015.11.003
136. Chiriac AM, Wang Y, Schrijvers R, Bousquet PJ, Mura T, Molinari N, et al. Designing predictive models for beta-lactam allergy using the drug allergy and hypersensitivity database. J Allergy Clin Immunol Pract. (2018) 6(1):139–48. doi: 10.1016/j.jaip.2017.04.045
137. Siew LQC, Li PH, Watts TJ, Thomas I, Ue KL, Caballero MR, et al. Identifying low-risk beta-lactam allergy patients in a UK tertiary centre. J Allergy Clin Immunol Pract. (2019) 7(7):2173–81. doi: 10.1016/j.jaip.2019.03.015
138. Mohamed OE, Beck S, Huissoon A, Melchior C, Heslegrave J, Baretto R, et al. A retrospective critical analysis and risk stratification of penicillin allergy delabeling in a UK specialist regional allergy service. J Allergy Clin Immunol Pract. (2019) 7(1):251–8. doi: 10.1016/j.jaip.2018.05.025
139. Stevenson B, Trevenen M, Klinken E, Smith W, Yuson C, Katelaris C, et al. Multicenter Australian study to determine criteria for low- and high-risk penicillin testing in outpatients. J Allergy Clin Immunol Pract. (2020) 8(2):681–9. doi: 10.1016/j.jaip.2019.09.025
140. Trubiano JA, Vogrin S, Chua KYL, Bourke J, Yun J, Douglas A, et al. Development and validation of a penicillin allergy clinical decision rule. JAMA Intern Med. (2020) 180(5):745–52. doi: 10.1001/jamainternmed.2020.0403
141. Moreno E, Laffond E, Munoz-Bellido F, Gracia MT, Macias E, Moreno A, et al. Performance in real life of the European network on drug allergy algorithm in immediate reactions to beta-lactam antibiotics. Allergy. (2016) 71(12):1787–90. doi: 10.1111/all.13032
142. Ponvert C, Weilenmann C, Wassenberg J, Walecki P, Bourgeois ML, de Blic J, et al. Allergy to betalactam antibiotics in children: a prospective follow-up study in retreated children after negative responses in skin and challenge tests. Allergy. (2007) 62(1):42–6. doi: 10.1111/j.1398-9995.2006.01246.x
143. Blumenthal KG, Huebner EM, Fu X, Li Y, Bhattacharya G, Levin AS, et al. Risk-based pathway for outpatient penicillin allergy evaluations. J Allergy Clin Immunol Pract. (2019) 7(7):2411–4. doi: 10.1016/j.jaip.2019.04.006
144. Labrosse R, Paradis L, Lacombe-Barrios J, Samaan K, Graham F, Paradis J, et al. Efficacy and safety of 5-day challenge for the evaluation of nonsevere amoxicillin allergy in children. J Allergy Clin Immunol Pract. (2018) 6(5):1673–80. doi: 10.1016/j.jaip.2018.01.030
145. Kulhas Celik I, Guvenir H, Hurmuzlu S, Toyran M, Civelek E, Kocabas CN, et al. The negative predictive value of 5-day drug provocation test in nonimmediate beta-lactam allergy in children. Ann Allergy Asthma Immunol. (2020) 124(5):494–9. doi: 10.1016/j.anai.2019.12.029
146. Allen HI, Vazquez-Ortiz M, Murphy AW, Moylett EM. De-labeling penicillin-allergic children in outpatients using telemedicine: potential to replicate in primary care. J Allergy Clin Immunol Pract. (2020) 8(5):1750–2. doi: 10.1016/j.jaip.2019.12.034
147. Wang LA, Patel K, Kuruvilla ME, Shih J. Direct amoxicillin challenge without preliminary skin testing for pediatric patients with penicillin allergy labels. Ann Allergy Asthma Immunol. (2020) 125(2):226–8. doi: 10.1016/j.anai.2020.05.004
148. Dona I, Labella M, Bogas G, Saenz de Santa Maria R, Salas M, Ariza A, et al. Antibiotic allergy de-labeling: a pathway against antibiotic resistance. Antibiotics. (2022) 11(8):1055. doi: 10.3390/antibiotics11081055
149. Dona I, Guidolin L, Bogas G, Olivieri E, Labella M, Schiappoli M, et al. Resensitization in suspected penicillin allergy. Allergy. (2023) 78(1):214–24. doi: 10.1111/all.15508
150. Hershkovich J, Broides A, Kirjner L, Smith H, Gorodischer R. Beta lactam allergy and resensitization in children with suspected beta lactam allergy. Clin Exp Allergy. (2009) 39(5):726–30. doi: 10.1111/j.1365-2222.2008.03180.x
151. Romano A, Blanca M, Torres MJ, Bircher A, Aberer W, Brockow K, et al. Diagnosis of nonimmediate reactions to beta-lactam antibiotics. Allergy. (2004) 59(11):1153–60. doi: 10.1111/j.1398-9995.2004.00678.x
152. Staicu ML, Vyles D, Shenoy ES, Stone CA, Banks T, Alvarez KS, et al. Penicillin allergy delabeling: a multidisciplinary opportunity. J Allergy Clin Immunol Pract. (2020) 8(9):2858–68. doi: 10.1016/j.jaip.2020.04.059
153. Blumenthal KG, Shenoy ES, Hurwitz S, Varughese CA, Hooper DC, Banerji A. Effect of a drug allergy educational program and antibiotic prescribing guideline on inpatient clinical providers’ antibiotic prescribing knowledge. J Allergy Clin Immunol Pract. (2014) 2(4):407–13. doi: 10.1016/j.jaip.2014.02.003
154. Blumenthal KG, Shenoy ES, Wolfson AR, Berkowitz DN, Carballo VA, Balekian DS, et al. Addressing inpatient Beta-lactam allergies: a multihospital implementation. J Allergy Clin Immunol Pract. (2017) 5(3):616–25. doi: 10.1016/j.jaip.2017.02.019
155. Blumenthal KG, Shenoy ES, Varughese CA, Hurwitz S, Hooper DC, Banerji A. Impact of a clinical guideline for prescribing antibiotics to inpatients reporting penicillin or cephalosporin allergy. Ann Allergy Asthma Immunol. (2015) 115(4):294–300. doi: 10.1016/j.anai.2015.05.011
156. Ham Y, Sukerman ES, Lewis JS 2nd, Tucker KJ, Yu DL, Joshi SR. Safety and efficacy of direct two-step penicillin challenges with an inpatient pharmacist-driven allergy evaluation. Allergy Asthma Proc. (2021) 42(2):153–9. doi: 10.2500/aap.2021.42.200128
157. Stone CA Jr., Stollings JL, Lindsell CJ, Dear ML, Buie RB, Rice TW, et al. Risk-stratified management to remove low-risk penicillin allergy labels in the ICU. Am J Respir Crit Care Med. (2020) 201(12):1572–5. doi: 10.1164/rccm.202001-0089LE
158. Wright A, Rubins D, Shenoy ES, Wickner PG, McEvoy D, Wolfson AR, et al. Clinical decision support improved allergy documentation of antibiotic test dose results. J Allergy Clin Immunol Pract. (2019) 7(8):2919–21. doi: 10.1016/j.jaip.2019.04.052
159. Dunham TB, Gardner RM, Lippner EA, Fasani DE, Moir E, Halpern-Felsher B, et al. Digital antibiotic allergy decision support tool improves management of beta-lactam allergies. J Allergy Clin Immunol Pract. (2023) 11(4):1243–52. doi: 10.1016/j.jaip.2023.01.026
160. Allen HI, Gillespie P, Vazquez-Ortiz M, Murphy AW, Moylett EM. A cost-analysis of outpatient paediatric penicillin allergy de-labelling using telemedicine. Clin Exp Allergy. (2021) 51(3):495–8. doi: 10.1111/cea.13782
161. Savic L, Ardern-Jones M, Avery A, Cook T, Denman S, Farooque S, et al. BSACI Guideline for the set-up of penicillin allergy de-labelling services by non-allergists working in a hospital setting. Clin Exp Allergy. (2022) 52(10):1135–41. doi: 10.1111/cea.14217
Keywords: anaphylaxis, beta-lactam, children, drug provocation test, maculopapular exanthema, skin test, urticaria
Citation: Sáenz de Santa María R, Bogas G, Labella M, Ariza A, Salas M, Doña I and Torres MJ (2023) Approach for delabeling beta-lactam allergy in children. Front. Allergy 4:1298335. doi: 10.3389/falgy.2023.1298335
Received: 21 September 2023; Accepted: 24 October 2023;
Published: 15 November 2023.
Edited by:
Mariana C. Castells, Harvard Medical School, United StatesReviewed by:
Semanur Kuyucu, Mersin University, TürkiyeJay Lieberman, University of Tennessee Health Science Center (UTHSC), United States
© 2023 Sáenz de Santa María, Bogas, Labella, Ariza, Salas, Doña and Torres. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: M. J. Torres bWp0b3JyZXNqQHVtYS5lcw==
†These authors have contributed equally to this work