 Stine A. Holmboe1,2*
Stine A. Holmboe1,2* Astrid L. Beck1,2
Astrid L. Beck1,2 Anna-Maria Andersson1,2
Anna-Maria Andersson1,2 Katharina M. Main1,2,3
Katharina M. Main1,2,3 Niels Jørgensen1,2
Niels Jørgensen1,2 Niels E. Skakkebæk1,2,3
Niels E. Skakkebæk1,2,3 Lærke Priskorn1,2
Lærke Priskorn1,2- 1Department of Growth and Reproduction, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark
- 2International Center for Research and Research Training in Endocrine Disruption of Male Reproduction and Child Health (EDMaRC), Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark
- 3Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark
Congenital cryptorchidism, also known as undescended testis, is the condition where one or both testes are not in place in the scrotum at birth and is one of the most common birth defects in boys. Temporal trends and geographic variation in the prevalence of cryptorchidism from 1% to 9% have been reported in prospective cohort studies. The testes develop in the abdominal cavity and descend to the scrotum in two phases, which should be completed by gestational week 35. Thus, the risk of cryptorchidism is higher in preterm boys. In many cases a spontaneous descent occurs during the first months of life during the surge of gonadotropins and testosterone. If not, the testis is usually brought down to the scrotum, typically by surgery, to increase future fertility chances and facilitate cancer surveillance. The increasing frequency of impaired semen quality and testicular cancer, with which cryptorchidism is associated, represents a concern for male reproductive health in general and a need to understand its risk factors. The risk of cryptorchidism is closely related to gestational factors (preterm birth, low birth weight and intrauterine growth restriction), and especially maternal smoking seems to be a risk factor. Evidence is accumulating that the increasing prevalence of cryptorchidism is also related to prenatal exposure to environmental chemicals, including endocrine disrupting compounds. This association has been corroborated in rodents and supported by ecological studies. Conducting human studies to assess the effect of endocrine disrupting chemicals and their interactions is, however, challenged by the widespread concomitant exposure of all humans to a wide range of chemicals, the combined effect of which and their interactions are highly complex.
Introduction
Congenital cryptorchidism, also known as undescended testis, is the condition where one or both testes are not in place in the scrotum at birth. This is one of the most common birth defects in newborn boys with a prevalence ranging from 1% to 9% in prospective cohort studies (1, 2), of which around 10% of cases are bilateral (3). Acquired cryptorchidism or ascending testes, where the testis ascends to a higher position after having been in the scrotum and retractile testes, when scrotal testes frequently retract to the groin, are not the focus of this review.
The testes develop in the abdominal cavity. Their descent to the scrotum is often described in two stages with different morphological and hormonal characteristics. The first, transabdominal stage, covering the descend to the internal inguinal ring between gestational week eight and fifteen, is highly dependent on insulin-like peptide 3 (INSL3) from the developing Leydig cells, which acts on the gubernaculum. The gubernaculum attaches the testis to the inner opening of the inguinal canal and creates a pathway for the testicular descent. The second, inguinoscrotal stage, where the testes move to their final position in the scrotum, begins around gestational week 25 and is in most cases completed by the 35th week of gestation. In this stage androgens play a key role (4). The testicular position is usually assessed at birth. In cases of cryptorchidism, the testis may be anywhere along the normal route of descent, in rare cases non-existent (vanishing testes) or ectopic. However, anomalies are most often related to the more complex second stage of testicular descent, while intra-abdominal testes, related to the first stage, are only seen in 5-10% of cases (4).
Around 80% of cases of cryptorchidism spontaneously descend within the first three months after birth to a low scrotal position during the postnatal surge of gonadotropins and testosterone. If this does not happen within the first six months, cryptorchid testes are usually brought down to the scrotum surgically (orchiopexy) (5, 6). This is done to prevent further deterioration of spermatogenic capacity and facilitate testicular cancer surveillance, as cryptorchidism is a risk factor for infertility and testicular cancer (7, 8). Approximately 10% of infertile men have a history of cryptorchidism (9), and based on men from the general population, unselected regarding fertility potential, a history of cryptorchidism was associated with reduced spermatogenic capacity, including reduced testis size, sperm count and inhibin B/FSH ratio (10). A recent meta-analysis estimated a fourfold increased risk of testicular cancer in boys with congenital cryptorchidism treated surgically compared to boys with no history of congenital cryptorchidism (11). However, while orchiopexy is associated with improved fertility chances, it remains unclear whether the risk for testicular cancer is also reduced. Notably, unilateral cryptorchidism should likely be considered a bilateral developmental disease as histopathological abnormalities and a higher testicular cancer risk is also observed in the contralateral non-cryptorchid testis (11).
The increasing frequency of impaired semen quality (12) and testicular cancer (13), with which cryptorchidism is associated, represents a concern for male reproductive health in general and a need to understand its risk factors (14). Here, we give a brief overview of the epidemiology of cryptorchidism, including national and temporal differences in its prevalence and risk factors, including environmental effects.
Prevalence of cryptorchidism
The reported prevalence of cryptorchidism ranges from 1% to 9% at birth in term, otherwise healthy, boys (1, 2) indicating some variation in this condition which may to some degree be explained by geographical differences. A comparative study of Danish and Finnish newborns using standardized examination protocols showed a four-fold higher risk of cryptorchidism in the Danish newborns compared to the Finnish (9.0% vs. 2.4%, respectively) after adjustment for confounders such as gestational age and birth weight (1). In general, few other European studies have reported the prevalence of cryptorchidism in full-term boys ranging from only 1.1% in Estonia (2), 3.4% in Italy (15), 3.8% in England (16) and 4.7% in Lithuania (17). Non-European studies have reported a prevalence of 2.1% in the United States (18) and 3.3% in Malaysia (19) in full-term boys (Figure 1A).
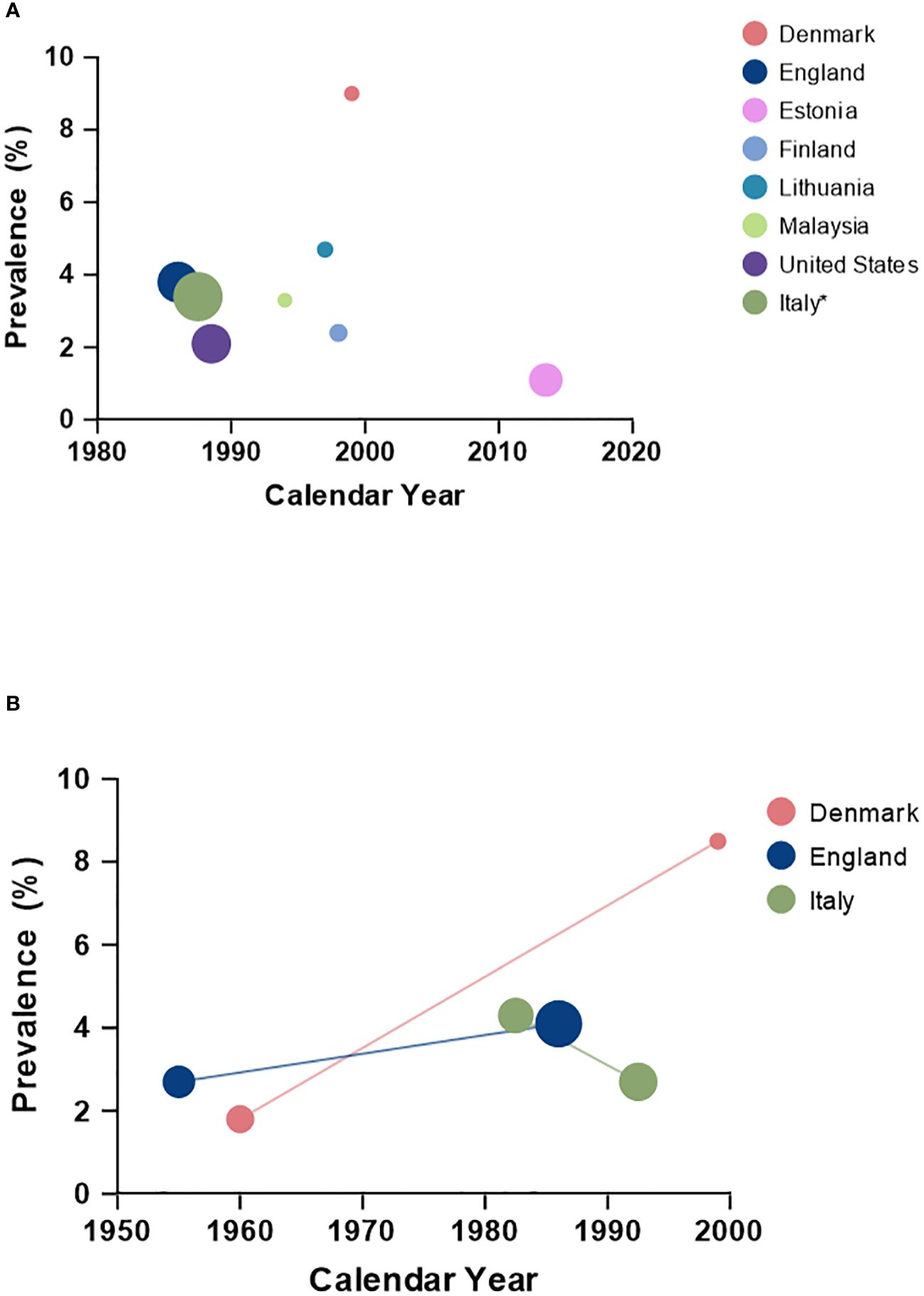
Figure 1 Prevalence (%) of cryptorchidism according to calendar year across countries; (A) including boys born term, and (B) including countries with comparative data using similar criteria for cryptorchidism within the given country. *The reported number reflects the period from 1978 to 1997.
Besides geographical differences, temporal changes in the prevalence of cryptorchidism have been suggested although the registration of cryptorchidism historically has been less reliable which has challenged comparisons over time (20). When applying the exact same clinical definition as previously an increase in the occurrence of cryptorchidism was seen in England from 2.7% in the 1950s to 4.1% in the 1980s in boys with a birthweight of at least 2500g (16, 21). Furthermore, an increase in incidence has been seen in Denmark among boys with normal birth weight when comparing with historical data (1.8% in 1959-61 vs. 8.5% in 1997-01) (1). Finally, data from Italy covering births from 1978-1997 suggest a modest decline in prevalence when stratifying across the time periods: 4.3% in 1978-1987 vs. 2.7% in 1988-1997 (15) (Figure 1B). In France the incidence rate of orchiopexy increased from 2.2 per 1000 in 2002 to 2.8 per 1000 in 2014 corresponding to a 36% increase within this period (22). Reasons for these temporal differences remain unclear, however, environmental factors, including differences in prenatal exposures to endocrine disruptors has been suggested as one contributing factor.
Also, ethnic differences in the prevalence of cryptorchidism have been described. A comparative study observed a slightly higher prevalence of cryptorchidism among white Americans compared to black Americans (1.90% vs. 1.55%, p=0.04) (23). In line with this, a comprehensive study from New Zealand observed significant differences in the incidence of cryptorchidism with Maoris having the highest risk followed by Europeans/others, and with Pacific and Asian ethnic groups having the lowest risk (24). Interestingly, the observed differences across ethnic groups mirrored that of testicular cancer in the same populations although the differences were less pronounced. This further supports a common testicular dysgenesis syndrome, i.e. cryptorchidism and testicular cancer are biologically related and both develop prenatally (25, 26).
Risk factors for cryptorchidism
Gestational risk factors
Since the last phase of testicular descent occurs in late pregnancy, the increased prevalence of cryptorchidism in preterm boys is to be anticipated and many such cases experience spontaneous descent after birth. Thus, the timing of assessment is an essential factor when comparing data across populations and time. In a recent prospective study of Estonian newborns, a total of 2.1% had cryptorchidism at birth, but the prevalence was 1.1% in full-term newborns, while it was 11.9% among preterm boys. Also low birthweight and intrauterine growth restriction are considered important factors with the prevalence of cryptorchidism being 16.7% among boys of low birthweight and 14% among boys born small for gestational age in the aforementioned study (2, 27). It is challenging to determine whether low birth weight and low weight for gestational age genuinely represent independent risk factors for cryptorchidism – or rather should be considered as proxy indicators linked with the risk of cryptorchidism due to shared underlying risk factors. Several risk factors outlined below also emerge as suggested risk factors for suboptimal in utero growth (28, 29). Overall, results from studies on the influence of maternal age on the risk of cryptorchidism are mixed (30). However, maternal age is often associated with other factors that could affect the risk of cryptorchidism, and the reported associations could thus be confounded.
Maternal health behavior
Maternal smoking behavior
Although several smaller studies have reported no association, epidemiological data from various populations have consistently demonstrated an association between maternal smoking and an increased risk of cryptorchidism. This is also the conclusion in four large meta-analyses reporting an overall pooled odds ratio for cryptorchidism between 1.13 and 1.18 in boys of mothers smoking during pregnancy compared to boys of non-smoking mothers (31–34). The magnitude of this risk appears to be dose-dependent, with a higher number of cigarettes smoked per day being associated with a higher risk of cryptorchidism in offspring (35, 36). Furthermore, Jensen et al. found that being preterm modified the association, and a higher risk of cryptorchidism was particularly observed in preterm boys of mothers smoking during pregnancy (37).
Maternal alcohol intake
As for maternal smoking, a number of population-based studies have investigated the association between maternal alcohol intake and the risk of cryptorchidism although with inconsistent findings (30). Findings from a meta-analysis including 15 studies and 5,601 cases of cryptorchidism showed no association between maternal alcohol drinking and the risk of cryptorchidism in sons (OR = 0.97, 95% CI: 0.87-1.07, p=0.08) (34). However, when pooling the estimates according to whether the alcohol intake was low (<1 drink/week), moderate (1-5 drinks/week) or high (≥ 5 drinks/week), high alcohol intake was associated with increased risk of cryptorchidism in sons, although insignificantly (OR = 2.74, 95% CI: 0.77-9.80, p=0.12), whereas moderate alcohol intake was associated with an apparent decreased risk of cryptorchidism (OR = 0.89, 95% CI: 0.82-0.96, p<0.01), indicating a non-linear association. The observation of no association between average maternal alcohol intake and risk of cryptorchidism in sons was confirmed in a recently conducted Danish study including more than 80,000 boys with prospectively collected information on maternal alcohol intake during pregnancy (38). However, one or two binge-drinking episodes during pregnancy were associated with a slightly lower risk of cryptorchidism in sons compared with no binge-drinking.
Maternal BMI
A Danish study observed a tendency of higher maternal pre-pregnancy BMI being significantly associated with higher cryptorchidism risk in Danish singleton boys (p-trend<0.01) (38). However, there is no consistent evidence suggesting that maternal pre-pregnancy BMI is associated with higher risk of cryptorchidism in sons, and a meta-analysis observed no difference in risk of cryptorchidism for women with BMI > 25 kg/m2 compared to women with BMI below this threshold (OR = 1.02, 95% CI: 0.95-1.09), p=0.67) (34). However, this meta-analysis showed that diabetes during pregnancy, for which higher BMI is a risk factor, was associated with increased risk of cryptorchidism (OR = 1.21, 95% CI: 1.00-1.46) (34).
In utero exposure to endocrine disrupting chemicals
The rising prevalence of male reproductive disorders, including cryptorchidism, appearing over a limited time frame, suggests that modern lifestyle plays a role. Specifically, in utero exposure to endocrine disrupting chemicals (EDCs) is a suspected contributor. These compounds can disrupt the hormone homeostasis in several ways, including acting on the normal production of hormones, mimicking or blocking their effects, affecting their transport or metabolism, or altering receptor expression. As described, testicular descent is a hormonally dependent event and thus sensitive to disruptions ensued by particularly estrogenic and anti-androgenic effects (39). Establishing associations between EDCs and cryptorchidism in humans is, however, challenging (40), whereas animal studies have clearly shown that in utero exposure to environmental chemicals can cause cryptorchidism (41–43). Carefully conducted rodent studies with controlled dose and timing of EDC exposure have demonstrated that anti-androgenic EDC exposure particularly during early fetal development, known as the masculinization programming window, can compromise sufficient androgen action and result in cryptorchidism and other signs of impaired male reproductive function (41, 44). Ex vivo studies of human fetal testis tissue manipulating androgen production during different time points of development, support the evidence from animal studies, indicating a critical window of androgen sensitivity observed during gestational week 7-14 in humans (45). During this period, experimentally induced reductions in androgen activity were shown to affect the function and density of several cell types in the human fetal testis with potential implications for the risk of cryptorchidism and future testicular function. Thus, the exact timing of prenatal exposure appears to determine the extent of adverse effects, both in the short term and long term, as the programming of later development and function of the male reproductive organs can be negatively affected (46).
In humans, ecological studies are used to indirectly relate exposures and outcome according to geographic area. Recently, a nationwide French study examined spatial clusters of cases of operated cryptorchidism and found that the incidence differed, with neighboring spatial units tending to show the same risks. Overall, the identified clusters with higher incidences of cryptorchidism were characterized by more dense industrial activities. Such differences could be related to socioeconomic status of the inhabitants but adjusting the spatial analyses for deprivation index did not change the results, suggesting a role of pollution related to former and prior industry (22). Similarly, incidences of cryptorchidism in Korea were shown to be higher in industrialized areas (47). A difference in the chemical burden has also been suggested to contribute to the prior difference in incidence of cryptorchidism observed between Denmark and Finland (48).
Besides ecological studies, an extensive number of epidemiological studies has been conducted assessing the effects of EDC exposure, and the conclusions from such studies are mixed when it comes to specific compounds. These studies aim to determine the level of fetal exposure to EDCs by measuring EDC concentrations in various biological matrices, such as maternal blood, cord blood, maternal urine, amniotic fluid, breast milk, or placenta, or indirectly through self-report of e.g., job exposures. However, such measures often represent an imprecise snapshot of fetal exposure. Furthermore, a major challenge in these studies is the rarity of non-exposed individuals and the fact that humans are continuously exposed to a wide range of chemicals, making it difficult to attribute effects to a single chemical. Most importantly, human exposure studies struggle to account for the common properties and likely interactions between these chemicals, the so-called mixture effects, that animal studies have clearly demonstrated (49). With these limitations in mind, in the following sections we summarize the literature on the epidemiological evidence for associations between the most studied EDCs and the risk of cryptorchidism.
Phthalates
Phthalates are used as plasticizers for their durability, transparency, and flexibility. Their appearance in plastics make phthalates ubiquitously present as they exist in a wide range of everyday products such as, but not restricted to, food packaging, pharmaceutical pills, adhesives, cosmetics, grouting, and children’s toys. Their means of entry into the human body are multiple: ingestion, inhalation, intravenous administration (via phthalates in medical devices), and skin absorption. Once taken up, phthalates are rapidly metabolized and are mostly excreted through urine but can also be found in other bodily fluids such as sweat and breast milk. A French study, in which phthalate exposure was indirectly determined through self-reporting of maternal occupational exposure found a tendency of higher prevalence of cryptorchidism among mothers with self-reported phthalate exposure compared to mothers with no self-reported phthalate exposure although the numbers were low (50). In addition, a study assessing maternal urine concentrations of phthalates collected during pregnancy (mean 28.6 gestational week) observed a significant association between higher concentrations of mono-2-ethylhexyl phthalate (MEHP) and cryptorchidism (51). However, the latest systematic review conducted in 2021 included nine studies assessing the impact of phthalates on male reproductive health, where all studies but one (51) found no significant association between phthalate exposure levels and cryptorchidism (52). This is moreover supported by a recent study published in 2022 utilizing maternal urine spot samples from each trimester of 1059 Dutch mothers, in which no association was found between prenatal phthalate exposure and cryptorchidism (53).
Bisphenols
Bisphenols are utilized in polycarbonate plastics, epoxy resins and thermal paper (54). Bisphenols are widely found in food packaging, but can also be detected in building materials, toys, cash register receipts, vinyl flooring and cosmetic products. Humans are orally and topically exposed to bisphenols, but also indirectly through the environment in the form of indoor dust (55) and soil pollution (56). Bisphenols have been measured in plasma, urine, cord blood and follicular fluid (57–59). A case-control study utilizing maternal serum concentrations of bisphenol A (BPA) of 330 mothers observed that the chemical was associated with a significant increase of cryptorchidism in sons. The same study furthermore observed that the significant association persisted when restricting their analysis to infants born full-term and not of low birth weight (60). A cohort study utilizing placentas to investigate the risk of urogenital malformations (defined as cryptorchidism and hypospadias) in 668 mother-son pairs observed that placentas within the highest tertile of BPA concentrations were associated with a higher risk of cryptorchidism/hypospadias (61). A Polish study observed that boys with cryptorchidism had significantly higher levels of conjugated BPA and total BPA in serum, however, notably, BPA levels were measured in samples taken prior to surgery rather than prenatally, which challenges any causal inferences as bisphenols are not considered to be persistent (62).
Parabens
Parabens are antifungal and antibacterial agents and are therefore widely applied in cosmetics, pharmaceuticals and in processed food. Due to their application in toiletry products, humans are commonly exposed to parabens through dermal application. Parabens permeate through the skin and have been detected in urine, breast milk, blood, and adipose tissues (63–65). In a cohort study utilizing placentas to ascertain paraben exposure and risk of urogenital malformations (defined as cryptorchidism and hypospadias) it was observed that placentas within the highest tertile of propyl-paraben were associated with higher odds of cryptorchidism/hypospadias. This association moreover persisted when including propyl-paraben as a continuous variable (61). In contrast, a study of 334 male infants found no association between cryptorchidism and propyl-paraben measured in maternal serum (60).
Pesticides
Pesticides are chemicals utilized to control pests to protect crop, preserve foods and eliminate illnesses spread by vectors. They have various functions such as herbicides, insecticides, avicides and fungicides, and are massively applied in agriculture and gardening. Humans are exposed to pesticides either directly, by using them on plants, or indirectly through consumption of crops and ground water. Pesticides are present in human serum (66), urine (67), adipose tissue (68) and amniotic fluid (69). In a Danish study assessing the self-reported prenatal pesticide exposure through occupation in four cohorts consisting of 1468 mother-son pairs, women occupationally exposed to pesticides had a higher risk of having sons with cryptorchidism than non-exposed women. Furthermore, an increased risk was observed for two out of the four cohorts compared to the background population, but this association was not seen in the combined cohort analysis (70). In a separate case-control study utilizing breast milk samples of Danish and Finnish mothers, 17 of 21 measured organochlorine pesticides were detected at slightly higher median concentrations in breast milk of mothers with cryptorchid sons than those with healthy sons. In addition, the combination of the eight most abundant pesticides were significantly higher in mothers of boys with cryptorchidism than those with healthy boys (71). In a study of 1326 Norwegian mother-son pairs in which exposure to organochlorine pesticides was ascertained in breast milk, only β-Hexachlorocyclohexane (β-HCH) was associated with cryptorchidism (72). A Spanish study that ascertained pesticide exposure in placenta tissues amongst cases of cryptorchidism and hypospadias together observed a higher detection rate of various pesticides in cases (72%) versus controls (54%), as well as an increased risk of the urogenital malformations if the mother’s occupation was in agriculture compared to other occupations. The study moreover observed increased risk of urogenital malformations associated with higher levels of some of the measured pesticides (73). In contrast, some studies have observed no associations between prenatal exposure to pesticides and cryptorchidism (74–77).
Poly- and perfluoroalkyl substances
Poly- and perfluoroalkyl substances (PFAS) are a group of chemicals used to make products resist heat, stains, oil, water, and grease. Due to their practicality, PFAS have been used in a wide range of everyday products, such as building materials, textiles, impregnation sprays, cookware, and fire-fighting foams. Their use in some products have since been restricted, yet due to their resistance to biodegradation through their carbon-fluorine bond, they can still be found accumulating in the environment (78, 79) and in the human body (80). Humans are mainly exposed to PFAS through drinking water, inhalation, and food (81). In a nested case-control study in 215 Danish and Finnish boys, perfluorooctanoic acid (PFOA) and perfluorooctanesulfonic acid (PFOS) was detected in all cord blood samples, however, no association was seen in relation to cryptorchidism (74). Similar findings of no association were also observed in a Danish study of 270 cryptorchidism cases and amniotic fluid levels of PFOS (82).
Polychlorinated biphenyls
Polychlorinated biphenyls (PCBs) have been widely applied in industrial applications due to their low flammability making them attractive to use as additives in the production of e.g., coolants, building materials and flame retardants. Humans are exposed to PCBs through inhalation and diet (83) with PCBs being detectable in serum and cord blood and showing accumulation in the brain (84–86). A Danish/Finnish case-control study of 130 breast milk samples observed that nine PCBs were higher in cryptorchid Danish cases than controls, whereas this was not seen in the Finnish cohort (48). A study utilizing postal addresses to identify PCB-contaminated apartments as a proxy of exposure reported that pregnant women had a 73% higher risk of giving birth to a son with cryptorchidism compared to unexposed women (87). Furthermore, a French study of 164 mother-son pairs utilizing colostrum samples observed that cases had higher individual scores of PCB than controls. Conversely, other studies have found no association between in utero exposure to PCBs and cryptorchidism (88–90).
Conclusion
To summarize, the incidence of cryptorchidism shows both regional and temporal differences. The risk in cryptorchidism is closely related to gestational factors (preterm birth, low birth weight and intrauterine growth restriction), and especially maternal smoking seems to be a risk factor. The increasing prevalence of cryptorchidism is likely also related to prenatal exposure to environmental chemicals, including endocrine disrupting compounds. This association has been corroborated in rodents and supported by ecological studies. Conducting human studies to assess the effect of endocrine disrupting chemicals and their interactions is challenged by the widespread concomitant exposure of all humans to a wide range of chemicals, the combined effect of which and their interactions are highly complex.
Author contributions
SH: Writing – original draft. AB: Writing – original draft. A-MA: Writing – review & editing. KM: Writing – review & editing. NJ: Writing – review & editing. NS: Writing – review & editing. LP: Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Authors received funding from Center on Endocrine Disrupters, Danish Environmental Protection Agency (MST-2022-23219) and Johan and Hanne Weimann, F. Seedforff’s grant (F-24230-01).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Boisen KA, Kaleva M, Main KM, Virtanen HE, Haavisto A-M, Schmidt IM, et al. Difference in prevalence of congenital cryptorchidism in infants between two Nordic countries. Lancet (London England). (2004) 363:1264–9. doi: 10.1016/S0140-6736(04)15998-9
2. Kübarsepp V, Varik K, Varendi H, Antson A, Veinla M, Nellis G, et al. Prevalence of congenital cryptorchidism in Estonia. Andrology. (2022) 10:303–9. doi: 10.1111/andr.13121
3. Leslie SW, Sajjiad H, Villaneuva CA. Cryptorchidism. In: StatPearls. Treasure Island (FL): StatPearls Publishing (2023).
4. Hutson JM. Cryptorchidism and hypospadias. Feingold KR, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, et al, editors. South Dartmouth (MA): MDText.com (2000).
5. Tekgül S, Stein R, Bogaert G, Nijman RJM, Quaedackers J, Hoen L, et al. European association of urology and european society for paediatric urology guidelines on paediatric urinary stone disease. Eur Urol Focus. (2022) 8:833–9. doi: 10.1016/j.euf.2021.05.006
6. Kolon TF, Herndon CDA, Baker LA, Baskin LS, Baxter CG, Cheng EY, et al. Evaluation and treatment of cryptorchidism: AUA guideline. J Urol. (2014) 192:337–45. doi: 10.1016/j.juro.2014.05.005
7. Ciongradi CI, Sârbu I, Iliescu Halițchi CO, Benchia D, Sârbu K. Fertility of cryptorchid testis-an unsolved mistery. Genes. (2021) 12(12):1–11. doi: 10.3390/genes12121894
8. Banks K, Tuazon E, Berhane K, Koh CJ, De Filippo RE, Chang A, et al. Cryptorchidism and testicular germ cell tumors: comprehensive meta-analysis reveals that association between these conditions diminished over time and is modified by clinical characteristics. Front Endocrinol (Lausanne). (2012) 3:182. doi: 10.3389/fendo.2012.00182
9. Mieusset R, Bujan L, Massat G, Mansat A, Pontonnier F. Clinical and biological characteristics of infertile men with a history of cryptorchidism. Hum Reprod. (1995) 10:613–9. doi: 10.1093/oxfordjournals.humrep.a135998
10. Koch T, Hansen AH, Priskorn L, Petersen JH, Carlsen E, Main KM, et al. A history of cryptorchidism is associated with impaired testicular function in early adulthood: a cross-sectional study of 6376 men from the general population. Hum Reprod. (2020) 35:1765–80. doi: 10.1093/humrep/deaa127
11. Florou M, Tsilidis KK, Siomou E, Koletsa T, Syrnioti A, Spyridakis I, et al. Orchidopexy for congenital cryptorchidism in childhood and adolescence and testicular cancer in adults: an updated systematic review and meta-analysis of observational studies. Eur J Pediatr. (2023) 182:2499–507. doi: 10.1007/s00431-023-04947-9
12. Levine H, Jørgensen N, Martino-Andrade A, Mendiola J, Weksler-Derri D, Jolles M, et al. Temporal trends in sperm count: a systematic review and meta-regression analysis of samples collected globally in the 20th and 21st centuries. Hum Reprod Update. (2023) 29:157–76. doi: 10.1093/humupd/dmac035
13. Huang J, Chan SC, Tin MS, Liu X, Lok VTT, Ngai CH, et al. Worldwide distribution, risk factors, and temporal trends of testicular cancer incidence and mortality: A global analysis. Eur Urol Oncol. (2022) 5:566–76. doi: 10.1016/j.euo.2022.06.009
14. De Jonge C, Barratt CLR. The present crisis in male reproductive health: an urgent need for a political, social, and research roadmap. Andrology. (2019) 7:762–8. doi: 10.1111/andr.12673
15. Ghirri P, Ciulli C, Vuerich M, Cuttano A, Faraoni M, Guerrini L, et al. Incidence at birth and natural history of cryptorchidism: a study of 10,730 consecutive male infants. J Endocrinol Invest. (2002) 25:709–15. doi: 10.1007/BF03345105
16. John Radcliffe Hospital Cryptorchidism Study Group. Cryptorchidism: a prospective study of 7500 consecutive male births, 1984-8. John Radcliffe Hospital Cryptorchidism Study Group. Arch Dis Child. (1992) 67:892–9. doi: 10.1136/adc.67.7.892
17. Preiksa RT, Zilaitiene B, Matulevicius V, Skakkebaek NE, Petersen JH, Jørgensen N, et al. Higher than expected prevalence of congenital cryptorchidism in Lithuania: a study of 1204 boys at birth and 1 year follow-up. Hum Reprod. (2005) 20:1928–32. doi: 10.1093/humrep/deh887
18. Berkowitz GS, Lapinski RH, Dolgin SE, Gazella JG, Bodian CA, Holzman IR. Prevalence and natural history of cryptorchidism. Pediatrics. (1993) 92:44–9. doi: 10.1542/peds.92.1.44
19. Thong M, Lim C, Fatimah H. Undescended testes: incidence in 1,002 consecutive male infants and outcome at 1 year of age. Pediatr Surg Int. (1998) 13:37–41. doi: 10.1007/s003830050239
20. Toppari J, Kaleva M, Virtanen HE. Trends in the incidence of cryptorchidism and hypospadias, and methodological limitations of registry-based data. Hum Reprod Update. (2001) 7:282–6. doi: 10.1093/humupd/7.3.282
21. Scorer CG. THE DESCENT OF THE TESTIS. Arch Dis Child. (1964) 39:605–9. doi: 10.1136/adc.39.208.605
22. Le Moal J, Goria S, Guillet A, Rigou A, Chesneau J. Time and spatial trends of operated cryptorchidism in France and environmental hypotheses: a nationwide study from 2002 to 2014. Hum Reprod. (2021) 36:1383–94. doi: 10.1093/humrep/deaa378
23. McGlynn KA, Graubard BI, Klebanoff MA, Longnecker MP. Risk factors for cryptorchism among populations at differing risks of testicular cancer. Int J Epidemiol. (2006) 35:787–95. doi: 10.1093/ije/dyl024
24. Gurney J, Sarfati D, Stanley J, Studd R. Do ethnic patterns in cryptorchidism reflect those found in testicular cancer? J Urol. (2013) 190:1852–7. doi: 10.1016/j.juro.2013.05.002
25. McGlynn KA, Devesa SS, Sigurdson AJ, Brown LM, Tsao L, Tarone RE. Trends in the incidence of testicular germ cell tumors in the United States. Cancer. (2003) 97:63–70. doi: 10.1002/cncr.11054
26. Sarfati D, Shaw C, Blakely T, Atkinson J, Stanley J. Ethnic and socioeconomic trends in testicular cancer incidence in New Zealand. Int J cancer. (2011) 128:1683–91. doi: 10.1002/ijc.25486
27. Sijstermans K, Hack WWM, Meijer RW, van der Voort-Doedens LM. The frequency of undescended testis from birth to adulthood: a review. Int J Androl. (2008) 31:1–11. doi: 10.1111/j.1365-2605.2007.00770.x
28. Cnattingius S. The epidemiology of smoking during pregnancy: smoking prevalence, maternal characteristics, and pregnancy outcomes. Nicotine Tob Res. (2004) 6 Suppl 2:S125–40. doi: 10.1080/14622200410001669187
29. Jensen MS, Wilcox AJ, Olsen J, Bonde JP, Thulstrup AM, Ramlau-Hansen CH, et al. Cryptorchidism and hypospadias in a cohort of 934,538 Danish boys: the role of birth weight, gestational age, body dimensions, and fetal growth. Am J Epidemiol. (2012) 175:917–25. doi: 10.1093/aje/kwr421
30. Gurney JK, McGlynn KA, Stanley J, Merriman T, Signal V, Shaw C, et al. Risk factors for cryptorchidism. Nat Rev Urol. (2017) 14:534–48. doi: 10.1038/nrurol.2017.90
31. Hackshaw A, Rodeck C, Boniface S. Maternal smoking in pregnancy and birth defects: a systematic review based on 173 687 malformed cases and 11.7 million controls. Hum Reprod Update. (2011) 17:589–604. doi: 10.1093/humupd/dmr022
32. Zhang Q, Zhang ZC, He XY, Liu ZM, Wei GH, Liu X. Maternal smoking during pregnancy and the risk of congenital urogenital malformations: A systematic review and meta-analysis. Front Pediatrics. Switzerland. (2022) 10:973016. doi: 10.3389/fped.2022.973016
33. Yu C, Wei Y, Tang X, Liu B, Shen L, Long C, et al. Maternal smoking during pregnancy and risk of cryptorchidism: a systematic review and meta-analysis. Eur J Pediatr. (2019) 178:287–97. doi: 10.1007/s00431-018-3293-9
34. Zhang L, Wang X-H, Zheng X-M, Liu T-Z, Zhang W-B, Zheng H, et al. Maternal gestational smoking, diabetes, alcohol drinking, pre-pregnancy obesity and the risk of cryptorchidism: a systematic review and meta-analysis of observational studies. PloS One. (2015) 10:e0119006. doi: 10.1371/journal.pone.0119006
35. Lindbo D, Arendt LH, Ernst A, Lunddorf LLH, Brix N, Ramlau-Hansen CH. Maternal cigarette smoking during pregnancy and genital anomalies in boys: A register-based cohort and sibling-matched design study. Clin Epidemiol. (2022) 14:901–10. doi: 10.2147/CLEP.S368826
36. Kjersgaard CL, Arendt LH, Ernst A, Søndergaard Lindhard M, Olsen J, Henriksen TB, et al. Lifestyle in pregnancy and hypospadias in sons: A study of 85,923 mother-son pairs from two danish pregnancy cohorts. Clin Epidemiol. (2022) 14:149–57. doi: 10.2147/CLEP.S335877
37. Jensen MS, Toft G, Thulstrup AM, Bonde JP, Olsen J. Cryptorchidism according to maternal gestational smoking. Epidemiology. (2007) 18:220–5. doi: 10.1097/01.ede.0000254061.90686.9f
38. Kjersgaard C, Arendt LH, Ernst A, Lindhard MS, Olsen J, Henriksen TB, et al. Lifestyle in pregnancy and cryptorchidism in sons: a study within two large Danish birth cohorts. Clin Epidemiol. (2018) 10:311–22. doi: 10.2147/CLEP
39. Fénichel P, Chevalier N, Lahlou N, Coquillard P, Wagner-Mahler K, Pugeat M, et al. Endocrine disrupting chemicals interfere with leydig cell hormone pathways during testicular descent in idiopathic cryptorchidism. Front Endocrinol (Lausanne). (2018) 9:786. doi: 10.3389/fendo.2018.00786
40. Skakkebæk NE, Rajpert-De Meyts E, Main KM. Testicular dysgenesis syndrome: An increasingly common developmental disorder with environmental aspects. Hum Reprod. (2001) 16:972–8. doi: 10.1093/humrep/16.5.972
41. van den Driesche S, Kilcoyne KR, Wagner I, Rebourcet D, Boyle A, Mitchell R, et al. Experimentally induced testicular dysgenesis syndrome originates in the masculinization programming window. JCI Insight. (2017) 2:e91204. doi: 10.1172/jci.insight.91204
42. Mylchreest E, Sar M, Cattley RC, Foster PM. Disruption of androgen-regulated male reproductive development by di(n-butyl) phthalate during late gestation in rats is different from flutamide. Toxicol Appl Pharmacol. (1999) 156:81–95. doi: 10.1006/taap.1999.8643
43. Foster PMD. Disruption of reproductive development in male rat offspring following in utero exposure to phthalate esters. Int J Androl. (2006) 29:140–5. doi: 10.1111/j.1365-2605.2005.00563.x
44. Welsh M, Saunders PTK, Fisken M, Scott HM, Hutchison GR, Smith LB, et al. Identification in rats of a programming window for reproductive tract masculinization, disruption of which leads to hypospadias and cryptorchidism. J Clin Invest. (2008) 118:1479–90. doi: 10.1172/JCI34241
45. Lundgaard Riis M, Matilionyte G, Nielsen JE, Melau C, Greenald D, Juul Hare K, et al. Identification of a window of androgen sensitivity for somatic cell function in human fetal testis cultured ex vivo. BMC Med. (2022) 20:399. doi: 10.1186/s12916-022-02602-y
46. World Health Organization. State of the science of endocrine disrupting chemicals 2012. In: Bergman Å, Heindel JJ, Jobling S, Kidd KA, Thomas Zoeller R, editors. Geneva, Switzerland: WHO (2013).
47. Chul Kim S, Kyoung Kwon S, Pyo Hong Y. Trends in the incidence of cryptorchidism and hypospadias of registry-based data in Korea: a comparison between industrialized areas of petrochemical estates and a non-industrialized area. Asian J Androl. (2011) 13:715–8. doi: 10.1038/aja.2010.53
48. Krysiak-Baltyn K, Toppari J, Skakkebaek NE, Jensen TS, Virtanen HE, Schramm K-W, et al. Association between chemical pattern in breast milk and congenital cryptorchidism: modelling of complex human exposures. Int J Androl. (2012) 35:294–302. doi: 10.1111/j.1365-2605.2012.01268.x
49. Hass U, Scholze M, Christiansen S, Dalgaard M, Vinggaard AM, Axelstad M, et al. Combined exposure to anti-androgens exacerbates disruption of sexual differentiation in the rat. Environ Health Perspect. (2007) 115 Suppl:122–8. doi: 10.1289/ehp.9360
50. Wagner-Mahler K, Kurzenne J-Y, Delattre I, Bérard E, Mas J-C, Bornebush L, et al. Prospective study on the prevalence and associated risk factors of cryptorchidism in 6246 newborn boys from Nice area, France. Int J Androl. (2011) 34:e499–510. doi: 10.1111/j.1365-2605.2011.01211.x
51. Swan SH. Environmental phthalate exposure in relation to reproductive outcomes and other health endpoints in humans. Environ Res. (2008) 108:177–84. doi: 10.1016/j.envres.2008.08.007
52. Rodprasert W, Toppari J, Virtanen HE. Endocrine disrupting chemicals and reproductive health in boys and men. Front Endocrinol (Lausanne). (2021) 12:706532. doi: 10.3389/fendo.2021.706532
53. Blaauwendraad SM, Jaddoe VWV, Santos S, Kannan K, Dohle GR, Trasande L, et al. Associations of maternal urinary bisphenol and phthalate concentrations with offspring reproductive development. Environ pollut. (2022) 309:119745. doi: 10.1016/j.envpol.2022.119745
54. Flint S, Markle T, Thompson S, Wallace E. Bisphenol A exposure, effects, and policy: A wildlife perspective. J Environ Manage. (2012) 104:19–34. doi: 10.1016/j.jenvman.2012.03.021
55. Geens T, Roosens L, Neels H, Covaci A. Assessment of human exposure to Bisphenol-A, Triclosan and Tetrabromobisphenol-A through indoor dust intake in Belgium. Chemosphere. (2009) 76:755–60. doi: 10.1016/j.chemosphere.2009.05.024
56. Zhang S, Yang X, Liu L, Zheng K, Ju M, Liu J. Bisphenol S adsorption behavior on ferralsol and biochar modified soil with dissolved organic matter. Int J Environ Res Public Health. (2019) 16(5):1–17. doi: 10.3390/ijerph16050764
57. Völkel W, Bittner N, Dekant W. Quantitation of bisphenol A and bisphenol A glucuronide in biological samples by high performance liquid chromatography-tandem mass spectrometry. Drug Metab Dispos. (2005) 33:1748–57. doi: 10.1124/dmd.105.005454
58. Dalkan C, Uncu M, Duran S, Bahçeciler NN. Association of cord blood bisphenol A (BPA) with cord blood adiponectin, leptin, fetal growth; adiposity and neoantal complications in a newborn cohort. J Matern neonatal Med Off J Eur Assoc Perinat Med Fed Asia Ocean Perinat Soc Int Soc Perinat Obstet. (2020) 33:2588–93. doi: 10.1080/14767058.2018.1555808
59. Ikezuki Y, Tsutsumi O, Takai Y, Kamei Y, Taketani Y. Determination of bisphenol A concentrations in human biological fluids reveals significant early prenatal exposure. Hum Reprod. (2002) 17:2839–41. doi: 10.1093/humrep/17.11.2839
60. Fisher BG, Thankamony A, Mendiola J, Petry CJ, Frederiksen H, Andersson AM, et al. Maternal serum concentrations of bisphenol A and propyl paraben in early pregnancy are associated with male infant genital development. Hum Reprod. (2020) 35:913–28. doi: 10.1093/humrep/deaa045
61. Fernández MF, Arrebola JP, Jiménez-Díaz I, Sáenz JM, Molina-Molina JM, Ballesteros O, et al. Bisphenol A and other phenols in human placenta from children with cryptorchidism or hypospadias. Reprod Toxicol. (2016) 59:89–95. doi: 10.1016/j.reprotox.2015.11.002
62. Komarowska MD, Hermanowicz A, Czyzewska U, Milewski R, Matuszczak E, Miltyk W, et al. Serum bisphenol A level in boys with cryptorchidism: A step to male infertility? Int J Endocrinol. (2015) 2015:973154. doi: 10.1155/2015/973154
63. Park N-Y, Cho YH, Choi K, Lee E-H, Kim YJ, Kim JH, et al. Parabens in breast milk and possible sources of exposure among lactating women in Korea. Environ pollut. (2019) 255:113142. doi: 10.1016/j.envpol.2019.113142
64. Zhang H, Quan Q, Li X, Sun W, Zhu K, Wang X, et al. Occurrence of parabens and their metabolites in the paired urine and blood samples from Chinese university students: Implications on human exposure. Environ Res. (2020) 183:109288. doi: 10.1016/j.envres.2020.109288
65. Artacho-Cordón F, Fernández MF, Frederiksen H, Iribarne-Durán LM, Jiménez-Díaz I, Vela-Soria F, et al. Environmental phenols and parabens in adipose tissue from hospitalized adults in Southern Spain. Environ Int. (2018) 119:203–11. doi: 10.1016/j.envint.2018.05.052
66. Li AJ, Banjabi AA, Takazawa M, Kumosani TA, Yousef JM, Kannan K. Serum concentrations of pesticides including organophosphates, pyrethroids and neonicotinoids in a population with osteoarthritis in Saudi Arabia. Sci Tot. Environ. (2020) 737:139706. doi: 10.1016/j.scitotenv.2020.139706
67. Li AJ, Kannan K. Urinary concentrations and profiles of organophosphate and pyrethroid pesticide metabolites and phenoxyacid herbicides in populations in eight countries. Environ Int. (2018) 121:1148–54. doi: 10.1016/j.envint.2018.10.033
68. Tawar N, Banerjee BD, Mishra BK, Sharma T, Tyagi S, Madhu SV, et al. Adipose tissue levels of DDT as risk factor for obesity and type 2 diabetes mellitus. Indian J Endocrinol Metab. (2021) 25:160–5. doi: 10.4103/ijem.ijem_198_21
69. Bradman A, Barr DB, Claus Henn BG, Drumheller T, Curry C, Eskenazi B. Measurement of pesticides and other toxicants in amniotic fluid as a potential biomarker of prenatal exposure: a validation study. Environ Health Perspect. (2003) 111:1779–82. doi: 10.1289/ehp.6259
70. Gabel P, Jensen MS, Andersen HR, Baelum J, Thulstrup AM, Bonde JP, et al. The risk of cryptorchidism among sons of women working in horticulture in Denmark: a cohort study. Environ Health. (2011) 10:100. doi: 10.1186/1476-069X-10-100
71. Damgaard IN, Skakkebaek NE, Toppari J, Virtanen HE, Shen H, Schramm K-W, et al. Persistent pesticides in human breast milk and cryptorchidism. Environ Health Perspect. (2006) 114:1133–8. doi: 10.1289/ehp.8741
72. Desalegn AA, Iszatt N, Stigum H, Jensen TK, Eggesbø M. A case-cohort study of perinatal exposure to potential endocrine disrupters and the risk of cryptorchidism in the Norwegian HUMIS study. Environ Int. (2021) 157:106815. doi: 10.1016/j.envint.2021.106815
73. Fernandez MF, Olmos B, Granada A, López-Espinosa MJ, Molina-Molina J-M, Fernandez JM, et al. Human exposure to endocrine-disrupting chemicals and prenatal risk factors for cryptorchidism and hypospadias: a nested case-control study. Environ Health Perspect. (2007) 115 Suppl:8–14. doi: 10.1289/ehp.9351
74. Carbone P, Giordano F, Nori F, Mantovani A, Taruscio D, Lauria L, et al. Cryptorchidism and hypospadias in the Sicilian district of Ragusa and the use of pesticides. Reprod Toxicol. (2006) 22:8–12. doi: 10.1016/j.reprotox.2006.01.006
75. Pierik FH, Klebanoff MA, Brock JW, Longnecker MP. Maternal pregnancy serum level of heptachlor epoxide, hexachlorobenzene, and beta-hexachlorocyclohexane and risk of cryptorchidism in offspring. Environ Res. (2007) 105:364–9. doi: 10.1016/j.envres.2007.04.005
76. Cognez N, Warembourg C, Zaros C, Metten M-A, Bouvier G, Garlantézec R, et al. Residential sources of pesticide exposure during pregnancy and the risks of hypospadias and cryptorchidism: the French ELFE birth cohort. Occup Environ Med. (2019) 76:672–9. doi: 10.1136/oemed-2019-105801
77. Axelsson J, Scott K, Dillner J, Lindh CH, Zhang H, Rylander L, et al. Exposure to polychlorinated compounds and cryptorchidism; A nested case-control study. PloS One. (2020) 15:e0236394. doi: 10.1371/journal.pone.0236394
78. Zhang X, Lohmann R, Sunderland EM. Poly- and perfluoroalkyl substances in seawater and plankton from the northwestern atlantic margin. Environ Sci Technol. (2019) 53:12348–56. doi: 10.1021/acs.est.9b03230
79. Jha G, Kankarla V, McLennon E, Pal S, Sihi D, Dari B, et al. Per- and polyfluoroalkyl substances (PFAS) in integrated crop-livestock systems: environmental exposure and human health risks. Int J Environ Res Public Health. (2021) 18(23):1–20. doi: 10.3390/ijerph182312550
80. Pérez F, Nadal M, Navarro-Ortega A, Fàbrega F, Domingo JL, Barceló D, et al. Accumulation of perfluoroalkyl substances in human tissues. Environ Int. (2013) 59:354–62. doi: 10.1016/j.envint.2013.06.004
81. Sunderland EM, Hu XC, Dassuncao C, Tokranov AK, Wagner CC, Allen JG. A review of the pathways of human exposure to poly- and perfluoroalkyl substances (PFASs) and present understanding of health effects. J Expo Sci Environ Epidemiol. (2019) 29:131–47. doi: 10.1038/s41370-018-0094-1
82. Toft G, Jönsson BAG, Bonde JP, Nørgaard-Pedersen B, Hougaard DM, Cohen A, et al. Perfluorooctane sulfonate concentrations in amniotic fluid, biomarkers of fetal leydig cell function, and cryptorchidism and hypospadias in danish boys (1980-1996). Environ Health Perspect. (2016) 124:151–6. doi: 10.1289/ehp.1409288
83. Norström K, Czub G, McLachlan MS, Hu D, Thorne PS, Hornbuckle KC. External exposure and bioaccumulation of PCBs in humans living in a contaminated urban environment. Environ Int. (2010) 36:855–61. doi: 10.1016/j.envint.2009.03.005
84. Li X, Hefti MM, Marek RF, Hornbuckle KC, Wang K, Lehmler H-J. Assessment of polychlorinated biphenyls and their hydroxylated metabolites in postmortem human brain samples: age and brain region differences. Environ Sci Technol. (2022) 56:9515–26. doi: 10.1021/acs.est.2c00581
85. Pavuk M, Olson JR, Sjödin A, Wolff P, Turner WE, Shelton C, et al. Serum concentrations of polychlorinated biphenyls (PCBs) in participants of the Anniston Community Health Survey. Sci Tot. Environ. (2014) 473–474:286–97. doi: 10.1016/j.scitotenv.2013.12.041
86. Park J-S, Bergman A, Linderholm L, Athanasiadou M, Kocan A, Petrik J, et al. Placental transfer of polychlorinated biphenyls, their hydroxylated metabolites and pentachlorophenol in pregnant women from eastern Slovakia. Chemosphere. (2008) 70:1676–84. doi: 10.1016/j.chemosphere.2007.07.049
87. Kofoed AB, Deen L, Hougaard KS, Petersen KU, Meyer HW, Pedersen EB, et al. Maternal exposure to airborne polychlorinated biphenyls (PCBs) and risk of adverse birth outcomes. Eur J Epidemiol. (2021) 36:861–72. doi: 10.1007/s10654-021-00793-x
88. McGlynn KA, Guo X, Graubard BI, Brock JW, Klebanoff MA, Longnecker MP. Maternal pregnancy levels of polychlorinated biphenyls and risk of hypospadias and cryptorchidism in male offspring. Environ Health Perspect. (2009) 117:1472–6. doi: 10.1289/ehp.0800389
89. Virtanen HE, Koskenniemi JJ, Sundqvist E, Main KM, Kiviranta H, Tuomisto JT, et al. Associations between congenital cryptorchidism in newborn boys and levels of dioxins and PCBs in placenta. Int J Androl. (2012) 35:283–93. doi: 10.1111/j.1365-2605.2011.01233.x
Keywords: cryptorchidism, testicular dysgenesis, prenatal exposure, endocrine disrupting compounds, epidemiology
Citation: Holmboe SA, Beck AL, Andersson A-M, Main KM, Jørgensen N, Skakkebæk NE and Priskorn L (2024) The epidemiology of cryptorchidism and potential risk factors, including endocrine disrupting chemicals. Front. Endocrinol. 15:1343887. doi: 10.3389/fendo.2024.1343887
Received: 24 November 2023; Accepted: 22 March 2024;
Published: 03 April 2024.
Edited by:
Martine Culty, University of Southern California, United StatesReviewed by:
Leandro Martin Velez, University of California, Irvine, United StatesHamid Ahmadi, University of Pécs, Hungary
Hamed Jafarpour, Mazandaran University of Medical Sciences, Iran
Copyright © 2024 Holmboe, Beck, Andersson, Main, Jørgensen, Skakkebæk and Priskorn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stine A. Holmboe, Stine.agergaard.holmboe@regionh.dk