 Orli Dahan
Orli Dahan Alon Goldberg
Alon Goldberg- 1Department of Multidisciplinary Studies, Tel-Hai College, Kiryat Shmona, Israel
- 2Department of Education, Tel-Hai College, Kiryat Shmona, Israel
Introduction: A flow experience typically occurs when the challenge of a demanding physical activity aligns with an individual's abilities, resulting in a sense of empowerment and fulfillment. Experiencing flow during physiological childbirth occurs in various birth environments, but quantitative studies comparing home birth and hospital birth in this respect are scarce. Childbirth is a psychological, social, and physiological event; thus, the birthing environment probably crucially affects the mental state of birthing women. We hypothesized that home birth will be positively correlated with a heightened flow state experienced by women during physiological labor, differing significantly from the experience of women birthing in a hospital.
Method: Israeli women with physiological childbirth experience were recruited through social media. Participants (n = 421) completed the Flow State Scale (FSS) and a demographic questionnaire.
Results: Comparing hospital births and home births, our research reveals a significant correlation between home birth environment and heightened birthing women's flow state. In physiological childbirth, women birthing at home report higher flow states compared to women in hospitals.
Discussion: The observed differences indicate a compelling connection between the birthing environment and the women's experience during labor. The heightened flow state during home births is explained in measured flow dimensions: challenge-skill balance, action-awareness merging, clear goals, unambiguous feedback, concentration, and joy. By comparing correlations of birthing environments and birthing women's flow state, this research contributes a novel perspective to the ongoing discourse on optimizing childbirth experience.
Introduction
Hospital birth is the cultural norm in Western industrialized countries, and the percentage of planned home births, for example, in the US, remains relatively low (1). This study took place in Israel, where maternity care operates within a general healthcare system, ensuring all residents have access to comprehensive prenatal, childbirth, and postnatal services (2). Most births in Israel occur in hospitals, accounting for approximately 99% of all births (3). These hospitals offer a spectrum of childbirth options, ranging from highly medicalized births with interventions like epidurals to low-intervention births supported by midwives (3, 4). Israeli midwives are registered nurses with specialized midwifery training (3). They provide autonomous care and emotional support, often managing multiple births simultaneously (4). Obstetricians, however, hold ultimate responsibility for birth outcomes and intervention decisions, sometimes influenced by liability issues. Thus, it is a medicalized maternity care system (3).
Planned home births are legal in Israel but remain relatively uncommon, constituting approximately 1% of all births (3, 5). These births are typically attended by certified midwives and are subject to strict regulations to ensure the safety of both mother and baby. Thus, women opting for home births must meet low-risk criteria (6). As for birth centers, in 2017, the Israeli Ministry of Health ordered the closure of all independent, midwife-led birth centers. This decision significantly reduced the options for out-of-hospital births (6, 7). However, in July 2021, the High Court ruled that these closures violated women's freedom of choice, ordering the reopening of these centers. Despite this ruling, free-standing birth centers have not yet resumed operations (7).
Qualitative studies reveal why women choose to plan home birth. Women's past traumatic encounters with hospital births, coupled with a desire for a more natural birthing process, appear to have driven their confident choice to opt for planned home births despite facing criticism and social stigma from both their social circles and certain maternity care providers (8, 9). In this context, an important example of a positive physiological outcome of home birth is reduction in perineum trauma. Perineum trauma severely affects postpartum women's ability to recover both physiologically and psychologically from birth, and planned home births are associated with fewer perineal tears and a reduced risk of third or fourth-degree tears during childbirth (10). Additionally, women who birth at home are less prone to experiencing postpartum depression compared to those who give birth at a hospital or birthing center (11). Women who opt for a planned home birth also report a high level of satisfaction, attributing it to the comfort of their home environment and the sense of increased control over the birthing experience. Qualitative studies consistently highlight feelings of empowerment during home births as a prevalent theme (12).
A positive birth experience is of paramount importance for both the mother and the newborn. It sets the stage for a healthy start to life, fostering immediate bonding and successful breastfeeding (13). A positive experience can also significantly impact the mother's emotional well-being, reducing the risk of postpartum depression and anxiety (14). It empowers women, making them feel confident and in control, which can have long-lasting effects on their self-esteem (15). Research shows that women view a positive birth experience as involving the safe birth of a healthy baby in a supportive environment, with both practical and emotional assistance from birth companions and understanding clinical staff. While many prefer physiological birth, most women recognize the uncertainty of childbirth and are willing to adapt. If intervention is required, women aim to retain a sense of control through active involvement in decision-making. In this sense, both safety and psychosocial wellbeing hold equal importance (14).
Conversely, negative birth experience usually correlates with a more medical birth, particularly instrumental births and unplanned cesarian sections (16), lack of support during childbirth (17), and obstetric violence (18). Negative birth experiences may have severe mental consequences during postpartum, such as childbirth-related PTSD or symptoms of somatization, obsessive compulsion, depression, and anxiety (16); thus, according to the World Health Organization, healthcare providers and support systems should strive to ensure that every birth is a positive, empowering experience (19). While there is a growing emphasis on promoting positive birth experiences, recent research by Kuipers et al. (20) explored women's firsthand accounts of their childbirth experiences across seven European countries – United Kingdom, Netherlands, Belgium, Germany, Austria, Spain, and the Czech Republic. The study specifically examined women's perceptions of their role and treatment within maternity care systems, revealing persistent issues of marginalization. Despite residing in countries often viewed as progressive and woman-centered, participants frequently reported not being treated as equal partners or primary decision-makers during their births (20).
Recent studies have demonstrated that during a physiological birth, women sometimes experience a positive altered state of consciousness (13). This state is referred to as “birthing consciousness,” and it resembles the mental flow state that is characterized by complete immersion and focus on an activity (4, 21). In a previous report, we discussed differences identified in an online survey of 766 women regarding the flow state experienced during childbirth. The findings showed that women who underwent physiological childbirth (i.e., without epidural anesthesia or instrumental interventions) had a higher flow state during birth (21). The flow state, often experienced during intense physical activity, involves focused engagement with a task that is both physiologically and psychologically challenging (22). During flow, individuals experience intense concentration, a sense of timelessness, effortless action, and deep enjoyment. Flow often occurs when the challenge of an activity matches the individual's abilities, leading to optimal performance and a feeling of accomplishment (23–27). This description fits fundamental aspects of physiological childbirth, thus labor and birth can induce a profound state of flow (28). It is crucial to note that flow experiences do not necessarily imply superficially cheerful sensations; rather, they involve a profound sense of intrinsic motivation, fulfillment, and positive engagement with the task at hand (29). Thus, experiencing flow during childbirth does not mean women feel explicitly cheerful or conventionally joyful throughout the entire labor, but rather that they experience labor as intrinsically meaningful, rewarding, and empowering.
According to Kirkham (28), while many women experience stressful births in medicalized birth environments, others seek autonomy in their birthing experience. These women often opt for home births with midwife care, valuing continuity, trust, and empowerment. A Flow state can occur in various birth settings, including traditional maternity wards, if women are treated with respect and actively involved. These experiences boost maternal confidence and strength (28). Thus, experiencing flow during physiological childbirth occurs not only in domestic birth environments – such as birth centers and homes – but also in typical hospital settings, but few studies compare the two. Because childbirth is a psychological, social, and physiological process, the birthing environment probably crucially affects the mental state of birthing women, especially during unmedicated birth (13, 30), we assumed the possibility of different subjective birthing experiences based on environment. The goal of our study was to investigate this potential link between birth environment and the physiological childbirth experience based on the occurrence of a heightened flow state during childbirth. For purposes of the study, we defined physiological birth simply as a vaginal birth with no epidural and no instrumental assistance in the second stage (see also (16).
Research hypothesis
Home birth will be positively correlated with a heightened flow state experienced by women during physiological labor, differing significantly from the experience of women birthing in a hospital environment.
Methods
Procedure
Israeli women were invited through social media to participate in an open online study presented as “Experience during physiological childbirth.” The physiological mode of birth was defined simply as vaginal birth without an epidural or instrumental assistance in the second stage of birth. In the current study, we intentionally chose to focus solely on the type of birth – specifically, physiological birth defined as birth without epidural analgesia or instrumental assistance during the second stage – as our primary criterion of interest. We deliberately refrained from collecting additional data regarding other birth interventions, such as the frequency of vaginal examinations or various forms of labor induction. This decision was made to maintain a concise, clear, and accessible online questionnaire, thereby maximizing participant responsiveness and reducing dropout rates.
After signing informed consent forms, each woman received a link and was asked to complete separately the online demographic questionnaire and a flow state questionnaire. Participants were informed that their anonymity would be preserved throughout the study and that they had the right to discontinue participation at any time. There was no financial incentive for participating; we did offer to share the results of the study with the participants. Respondents were able to review and change their answers through a Back button.
Instrument
Demographic questionnaire
We collected information about participants' age, marital status, number of children, education level, number of years since the birth being reported, number of births, birth order of the selected birth (first, second, etc.), and the environment in which their physiological birth took place: hospital or at home.
The Flow State Scale (FSS)
The FSS is a 36-item self-report questionnaire that assesses flow experiential awareness in sports and physical activity settings, which was developed based on Csikszentmihalyi (22) and is well-validated (25). The scale uses nine dimensions to evaluate flow awareness: challenge-skill balance (e.g., “I felt I was competent enough to meet the high demands of giving birth”), action-awareness merging (e.g., “I did things spontaneously and automatically”), clear goals (e.g., “I knew clearly what I wanted to do”), unambiguous feedback (e.g., “I could tell by the way I was performing how well I was doing”), concentration on the task (e.g., “I had total concentration”), sense of control (e.g., “ I felt in total control of my body”), loss of self-consciousness (e.g., “I was not worried about what others may have been thinking of me”), transformation of time (e.g., “Time seemed to alter – either slowed down or speeded up”), and autotelic experience (e.g., “I found the birthing experience extremely rewarding”). Each item was rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Mean internal consistency of the sub-scales in the current research was .87–.95.
While the Flow State Scale (FSS) was originally designed to measure flow experiences during demanding physical activities, it was adapted for this study to assess flow during childbirth. The instructions for completing the FFS questionnaire stipulated that the woman should answer the questions regarding the specific physiological childbirth experience she chose for the demographic questionnaire. Minor adjustments were made to certain items to align them more closely with the specific context of childbirth, such as replacing “high demand of the situation” with “high demands of giving birth.” This adaptation allowed for the application of the FSS to the unique physiological and psychological aspects of childbirth, providing a more nuanced exploration of flow within this context [see Supplementary Appendix A: Adapted Flow State Scale (FSS) for Childbirth Context].
Ethical considerations
Ethics approval was obtained from the Institutional Review Board (12/2021-7).
Results
Participants
Participants were 421 Israeli women who had experienced physiological childbirth. Of the women, 305 (72.4%) gave birth at the hospital and 116 (27.6%) gave birth at home. Their mean age was 36.42 years (SD = 7.34). The mean number of years after the reported birth event was 4.56 (SD = 3.11), with 42.5% of the women reporting on their first childbirth, 26.8% their second childbirth, and 30.6% other births. Demographically, 93.1% had a graduate/professional degree; and 64.4% were secular while 35.6% were traditionally religious.1
We have posted our invitation to participate in the survey on various women's Facebook groups, such as “Mothers on Maternal Leave” and “Natural Birth & Home Birth.” The latter group is a private group of nearly 40,000 women. This can explain the relatively high percentage of women who reported experiencing homebirths (27.6%), while in Israel, only 1% are giving birth at home.
Preliminary results
To test whether the demographic variables correlated with research variables, a series of Pearson correlation tests were conducted between the woman's age, number of years since reported childbirth, number of children and FSS scores. Furthermore, Spearman correlation tests were conducted between education level, number of births, birth order of the selected birth (first, second, etc.), religiosity and FSS. Finally, differences in demographic variables between women who birthed at home vs. women who birthed at hospital were tested. Results demonstrated no significant associations between demographic variables and research variables.
Research hypothesis analyses
To examine the hypothesis on the differences between physiological home childbirth and physiological hospital childbirth, a MANCOVA analysis was conducted with the place of childbirth as the independent variable, flow state level as the dependent variable, and mother's age, child's age, and birth number as covariates. Results demonstrated that the MANCOVA model was significant [F (9,399) = 4.18, p < .0001]. ANOVA tests revealed significant differences between the place of childbirth groups for most flow state dimensions, with women who experienced home childbirth reporting higher flow states than women who experienced physiological childbirth at the hospital (Table 1). The results confirmed our hypothesis.
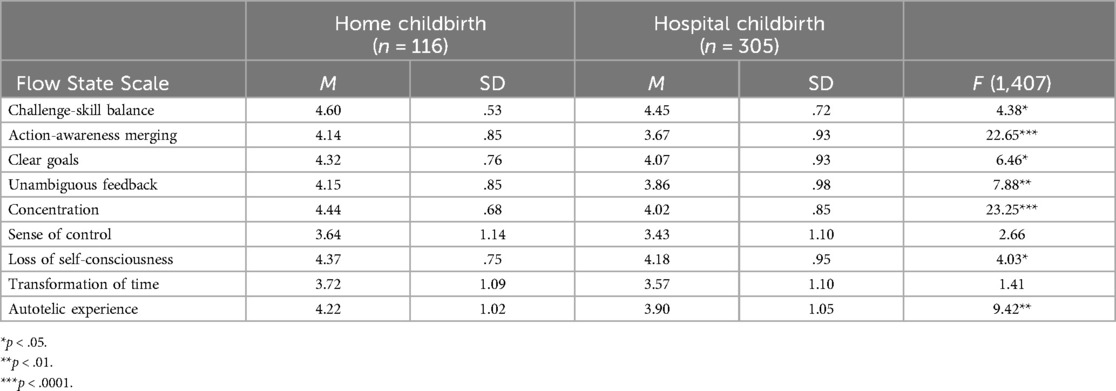
Table 1. MANOVA analysis: differences between the place of physiological childbirth on Flow State Scale (N = 421).
Discussion
We emphasize that childbirth is a complex and multifaceted event characterized by significant individual (31) and cultural (32) variability among birthing women. The findings of this study are limited in scope, focusing specifically on the reported experience of flow during physiological birth in home settings compared to physiological birth in hospital environments. Thus, the results should not be generalized broadly to all births or other birthing contexts.
Women who had physiological births at home reported elevated levels of mental flow state for 7 of the 9 dimensions of flow, indicating a correlation between birthing environment and the birthing woman's experience during labor. Several interconnected factors differentiating between the home and hospital environments explain the connection to each flow dimension. An in-depth explanation of each flow dimension can enrich our understanding of the subjective physiological birth experience – a perspective unexplored in the literature to date.
Moreover, recent theoretical advancements in flow research reinforce the significance of studying flow within natural, dynamic settings rather than controlled laboratory environments. Durcan et al. (33) expand the understanding of environmental and perceptual factors shaping flow experiences, emphasizing the role of autonomy, motivation, and personal connection to the activity. Their critique of traditional research approaches, which rely on sterile, short-term tasks in artificial settings, highlights the need for models that capture flow in real-world contexts. Similarly, the ecological dynamics perspective (34) underscores the dynamic interplay between individuals and their environment, proposing that perception, action, and environmental affordances are integral to the emergence of flow. While these studies do not address childbirth specifically, their insights align with our finding that the physical and social birth environment play a central role in shaping flow experiences during birth. The contrast between hospital and home birth provides a unique opportunity to explore how differences in autonomy, privacy, medical interventions, and environmental design influence flow states. Applying this approach to childbirth research strengthens the argument that factors such as physical design, emotional support, and birth setting are not peripheral but central to the flow experience. By investigating flow in birth environments rather than experimental settings, this study contributes to a growing body of literature advocating for a broader valid understanding of flow in high-intensity, real-world experiences.
Home settings offer a sense of comfort and familiarity that can positively impact a woman's experience during labor. Women feel they can have a customized birth experience at home but not in an institutionalized setting (35). Being in a familiar environment reduces stress and anxiety, which are known to hinder the progression of labor. The woman feels more relaxed, which contributes to the process of physiological birth (36). Reducing anxiety and pain during labor can also reduce the length of the first stage of labor (37). Indeed, in a qualitative study on the reasons of Canadian women for planning a home birth, the women outlined that laboring at home provided greater flexibility in pain management and coping strategies (35). Moreover, in a home birth setting, women typically have more autonomy regarding their birthing process (38). They have the freedom to move around, choose positions that feel most comfortable, and make decisions about their care in collaboration with their birth attendants. This sense of autonomy enhances feelings of agency, leading to a more positive childbirth experience (13).
These characteristics of home environment in contrast to the typical hospital environment can explain the flow dimensions of unambiguous feedback (“I had a good idea while I was birthing about how well I was doing”), action-awareness merging (“I made the correct movements without thinking about trying to do so”), and challenge-skill balance (“I felt I was competent enough to meet the high demands of giving birth”). The shared feature of these dimensions is the enhanced mind-body connection. Feeling autonomy to move at will and being free to use any strategies to ease the pain of contractions and feel comfortable in her surroundings allows for more profound connection to her body (13) and, in a way, letting her body to do its job without the mind interfering (36). After all, while childbirth is a demanding physiological process, it is very much affected by psychological factors such as comfort and confidence (15). Indeed, women who planned home birth voiced a preference for home birth not only for its comfort but also for the increased autonomy it offered (35).
The enhanced mind-body connection, expressed through automatic bodily movements and spontaneous actions during physiological birth, aligns with previous findings in the literature. Hrdy (39), xii–xiv) similarly emphasized that labor contractions may be perceived by women as intense yet captivating biological forces, evoking fascination rather than mere distress or pain (see also (40–42). These insights correspond closely to the current study's findings on the flow experience, reinforcing the idea that physiological birth uniquely facilitates embodied awareness and a relinquishment of conscious control, ultimately enriching the overall birth experience.
In this context, choosing a home birth reflects a deep trust in the body's ability to give birth naturally (43). Because having a home birth is not very common in industrialized societies, women who opt to plan for home birth must take ownership of their decision (35). Hence, it could be said that the sense of ownership – belief in the ability to give physiological birth – starts before birth itself. The sense of empowerment of women following physiological birth is a known phenomenon in midwifery literature (15). It is sometimes referred to as “the superwoman syndrome”: The euphoric sensation of accomplishment and joy that some women experience post-birth due to the surge of hormones and the sense of empowerment that comes with successfully giving birth (15, 42, 44). This feeling can lead to a heightened sense of confidence and capability, as if the woman can conquer anything, like a superhero. It reflects a deeply positive and empowering experience of childbirth that can leave a woman feeling invincible and capable of taking on any challenge (15). These profound sensations of euphoric pleasure can explain the flow dimension of autotelic experience (“I really enjoyed the experience of giving birth”). Thus, the emotional and practical meaning of the differences in the flow state scores can be translated into an enhanced positive peak experience at home.
Home birth settings provide a more intimate and private environment where birthing women can labor surrounded by loved ones and supportive birth attendants. This intimate setting positively impacts the woman's emotional state and overall experience of labor (45). For most people, home is a peaceful and restful place. A hospital setting is much different in environment and culture, and hospital staff have certain routines that can affect the birthing process. It is not uncommon to have different people walk in and out of a laboring woman's room. In one's own home, people who enter are invited guests and are usually individuals who will provide the woman with good support (12). This issue of privacy is highly crucial when it comes to physiological birth and is related to at least two dimensions of flow: loss of self-consciousness (“I was not concerned with how I was presenting myself”) and concentration on the task (“I was completely focused”).
During intense contractions, women report that it is helpful to handle the pain by focusing and retreating to a different zone, which also helps to relinquish some social constraints (36). The ability to be unconcerned about what others might think is crucial, especially during intimate and vulnerable events, such as sexual activity or giving birth (13). According to Cohen Shabot and Korem (18), the bodies of birthing women during physiological unmedicated childbirth are oxymoronic. When women give birth, from a functional point of view they complete one of the most fundamental missions of femininity – to bring new life into the world. However, at the same time, their bodies are the complete opposite of what society views as feminine: birth involves mess, blood, noisy sounds, and pain. A birthing body during physiological birth is a strong, expanding, loud, messy body; it challenges femininity's usual frame. The event of physiological birth is blatantly sexual in its “inappropriate” way. The norms of femininity are not to be overly sexual or exuberant – but to be beautiful and self-controlled, silent, delicate, obedient (18). Thus, when a woman is able to overcome the perceived “lost dignity” in physiological birth (46) she becomes uninhibited and can relax, which, in turn, can promote the birth process that feelings of embarrassment often hinder (13). Privacy and support from people who are not strangers – during one of life's most intimate episodes – can be crucial to focusing and surrendering self-consciousness (21, 44).
Home births involve fewer medical interventions than hospital births because the commonly used interventions in hospitals (oxytocin drips, epidurals, c-sections) cannot be implemented at home births. But as for other interventions, such as routine vaginal examinations, homebirth midwifes hold a philosophy of birth that is woman-centered. This philosophy is also a physiologic care model that emphasizes supporting and advocating for physiological childbirth, employing medical intervention only when necessary (47). As a result, birthing women are less likely to experience unnecessary interventions such as continuous fetal monitoring (48), or routine vaginal examinations (49, 50). Avoiding these interventions, or even the need to refuse to interventions, can contribute to the elevated sense of flow experienced by home birthing women by letting them focus on their goals – on what is important to them, to their specific situation, and not to general, strict hospital protocols. This feature can be related to the flow dimension of clear goals (“I knew what I wanted to achieve”), which reflects the strong feeling of confidence of the birthing woman.
In this context, Neerland et al. (45) suggest that midwives' trust in the natural childbirth process and their belief in its normalcy help instill similar confidence in birthing women. Conversely, many hospital settings have a different dynamic, where women report achieving physiological birth despite pressures from medical staff to accept unnecessary interventions (51). Although many midwives in hospitals aim to practice woman-centered care, rigid protocols, and a medicalized hospital philosophy can hinder such care, creating external pressures for interventions that may not always be medically necessary. As a result, women may feel compelled to advocate for their preferences and goals, sometimes facing provider-centered rather than woman-centered approaches. For example, birthing women often express the desire for empowerment, autonomy, and control over their birth experiences rather than being perceived or treated as weak or incapable (35).
As explained in the introduction, this study is about home births and not birth centers because all birth centers in Israel were closed in 2017 by the Israeli Ministry of Health see (52). However, birth centers are like home birth in many respects, such as being domestic birth environments with a women-centered philosophy and a tendency to promote a physiological birth. Thus, our findings here support prior studies of birth centers, which were found to increase feelings of confidence among birthing women (45). Birth centers, with intimate, homelike environments, are calming, fostering feelings of ease and empowerment during childbirth. The welcoming atmosphere of birth centers also contributed to birthing women's satisfaction. The design of birth rooms can affect the birthing experience. For instance, in birth centers, unlike in typical hospital birthing rooms, safety equipment is not prominently displayed. This contributes to the heightened confidence of birthing women (45), perhaps even allowing them to focus on their goals without interruption.
Two dimensions were not found to be elevated for home environments: the sense of control (“I felt in total control of what I was doing”) and the transformation of time (“Time seemed to alter”). A plausible explanation for the absence of differences in the sense of control dimension between home and natural hospital births may lie in the inherent complexity and ambiguity of the notion of control during physiological birth. As previous qualitative syntheses illustrate (53), women's psychological experiences during physiological childbirth are characterized by a paradoxical interplay between actively maintaining control and simultaneously surrendering or relinquishing it. Achieving a physiological birth requires women to feel empowered and in control of their decisions and environment, yet also demands the capacity to let go of conscious control to allow the physiological processes of birth to unfold naturally. This nuanced and ambivalent experience of control might explain why our study did not detect significant differences between home and hospital settings, given that the subjective meaning and control experience transcend straightforward categorizations by birth environment.
The sensation of time alteration is not unique to a positive peak experience; people can experience alterations in time perception (the feeling that time either slowed down or sped up) in relatively negative experiences such as simply being bored, or in the case of childbirth, during highly negative and traumatic experiences (54). Thus, it is reasonable that the event of birth would be experienced with a blurred sense of time, regardless of the mode of birth or the setting in which it took place (see also (21). Qualitative research will be more effective in measuring these more nuanced, specific sensations – i.e., the sense of control and the sensation of time alteration – during the experience of birthing.
Conclusion
In physiological childbirth, women birthing at home report higher flow states than those giving birth in hospitals. Given that the flow experience represents a highly positive and beneficial psychological state, it is important to further understand how it can be facilitated across different birth settings. Considering that the majority of women today give birth in hospital settings, future research should explore how conditions associated with increased flow experiences can be effectively integrated into hospital-based care, enhancing women's overall birth experiences.
Limitations and strengths
It is well established that the birthing environment significantly influences birth outcomes, including the mode of birth and the psycho-physical consequences that impact recovery and postpartum mental health. The current study employed a cross-sectional design; hence, there are limitations to any conclusions regarding causality realtionships between birthing at home and a hightened flow state during physiological childbirth. However, this study's significance lies in its novel perspective on measuring positive physiological birthing experiences. It also lies in being the first to identify a link between the strength of this experience and the domestic setting compared to the experience of the same birthing mode in a typical hospital environment. This is also one of the few studies applying the quantitative method to examine the physiological birth experience in terms of flow.
A potential limitation of this study could be recall bias, given the significant time elapsed (median = 4.56 years) between childbirth and data collection. However, childbirth represents a significant milestone with lasting psychological and emotional implications for women (55). It marks a profound transitional phase in life, carrying potential for both empowerment and trauma, influenced by factors such as personal perceptions of the birth experience, method of birth, and the availability of continuous support (56–58). Research dating back to Simkin (59) illustrates that women retain clear, detailed memories of their childbirth experiences even long after the event. Contemporary studies further validate these findings, demonstrating that due to childbirth's transformative nature, the experiences associated with it remain exceptionally vivid in women's long-term memory (60). Our current study focuses on physiological birth experiences, which are generally perceived as more positive than highly medicated births (13, 61). Therefore, despite the time elapsed since birth, the vividness and emotional intensity of these memories likely mitigate potential bias, reinforcing the reliability of women's retrospective accounts.
Our analysis did not control all labor interventions because we defined physiological birth as non-instrumental vaginal birth without epidural analgesia. This could include a range of interventions that may interrupt the physiological process and that would not occur if the labor and birth were happening spontaneously (“naturally”), including episiotomy (in both settings) or labor induction (via membrane sweep in both settings and by pharmacological means in hospital). This means that the differences found in the flow state could also be about the level of interventions. While this analysis could not be done for the current study, given that labor and birth procedures were not recorded, other explanations for the findings exist, and future studies that collect more information could test these alternatives. Numerous other factors not explored in our study – such as prior expectations, the extent of social and professional support, and previous birth experiences—may significantly influence reported flow experiences. Therefore, caution is warranted in interpreting these findings, acknowledging the phenomenon's complexity and highlighting the need for further research to investigate additional explanatory factors underlying differences in flow experience among birthing populations. Our survey was conducted in Hebrew; thus the sample was limited to Hebrew speaking women. A future study could conduct comparative research across countries with diverse healthcare systems and birth practices to examine the influence of cultural and contextual factors on the flow state experience during childbirth in various physiological birth settings, such as hospitals, birth centers, and homes.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics approval was obtained from the Institutional Review Board (12/2021-7). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
OD: Conceptualization, Methodology, Formal analysis, Investigation, Writing – original draft, Writing – review & editing, Project administration. AG: Conceptualization, Methodology, Formal analysis, Investigation, Writing – original draft, Writing – review & editing, Project administration.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgwh.2025.1573688/full#supplementary-material
Footnote
1. ^In the survey, religiosity was assessed by self-report, with participants categorizing themselves as either “secular” or “traditionally religious.” In the Israeli context, “traditionally religious” generally refers to women who identify with Jewish religious customs and traditions to varying degrees, ranging from moderate observance to more strictly religious lifestyles, but not explicitly adhering to the stricter Orthodox definitions.
References
1. MacDorman MF, Barnard-Mayers R, Declercq E. United states community births increased by 20% from 2019 to 2020. Birth. (2022) 49(3):559–68. doi: 10.1111/birt.12627
2. Stein-Zamir C, Shoob H, Katan S, Verbov G, Almashanu S. Non-uptake of newborn screening in planned homebirth is associated with preventive health practices for infants: a retrospective case-control study. Int J Neonatal Screen. (2025) 11(1):15. doi: 10.3390/ijns11010015
3. Benyamini Y, Tovim S, Preis H. Who plans to give birth with a doula? Demographic factors and perceptions of birth. Women Birth. (2025) 38(2):101880. doi: 10.1016/j.wombi.2025.101880
4. Dahan O, Goldberg A. Birthing with others: exploring the efficacy of one-on-one professional support on physiological birth and flow state. Birth. (2025). doi: 10.1111/birt.12908
5. Benyamini Y, Molcho ML, Dan U, Gozlan M, Preis H. Women’s attitudes towards the medicalization of childbirth and their associations with planned and actual modes of birth. Women Birth. (2017) 30(5):424–30. doi: 10.1016/j.wombi.2017.03.007
7. Cohen E. Public policy for regulating the congestion in delivery rooms in Israel: alternatives, consequences, and recommendations. Societies. (2025) 15(2):47. doi: 10.3390/soc15020047
8. Chauncy CC, Dawson K, Bayes S. What do safety and risk mean to women who choose to birth at home? A systematic review. Midwifery. (2025) 144:104340. doi: 10.1016/j.midw.2025.104340
9. Gillen P, Bamidele O, Healy M. Systematic review of women’s experiences of planning home birth in consultation with maternity care providers in middle to high-income countries. Midwifery. (2023) 124:103733. doi: 10.1016/j.midw.2023.103733
10. Edqvist M, Blix E, Hegaard HK, Ólafsdottir OÁ, Hildingsson I, Ingversen K, et al. Perineal injuries and birth positions among 2992 women with a low risk pregnancy who opted for a homebirth. BMC Pregnancy Childbirth. (2016) 16:1–8. doi: 10.1186/s12884-016-0990-0
11. Wolf AN, Ruiz C, Anderson TL. Perineal Tearing: Home vs. Hospital. NURS 200W: Principles of Nursing Research and Evidence-Based Practice. Mont Alto, PA: PennState College of Nursing (2021).
12. Zielinski R, Ackerson K, Kane Low L. Planned home birth: benefits, risks, and opportunities. Int J Womens Health. (2015) 7:361–77. doi: 10.2147/IJWH.S55561
13. Dahan O. Navigating intensive altered states of consciousness: how can the set and setting key parameters promote the science of human birth? Front Psychiatry. (2023) 14:1072047. doi: 10.3389/fpsyt.2023.1072047
14. Downe S, Finlayson K, Oladapo O, Bonet M, Gülmezoglu AM. What matters to women during childbirth: a systematic qualitative review. PLoS One. (2018) 13(4):e0194906. doi: 10.1371/journal.pone.0194906
15. Kurz E, Davis D, Browne J. ‘I felt like I could do anything!’ writing the phenomenon of ‘transcendent birth’ through autoethnography. Midwifery. (2019) 68:23–9. doi: 10.1016/j.midw.2018.10.003
16. Dekel S, Ein-Dor T, Berman Z, Barsoumian IS, Agarwal S, Pitman RK. Delivery mode is associated with maternal mental health following childbirth. Arch Womens Mental Health. (2019) 22:817–24. doi: 10.1007/s00737-019-00968-2
17. McKelvin G, Thomson G, Downe S. The childbirth experience: a systematic review of predictors and outcomes. Women Birth. (2021) 34(5):407–16. doi: 10.1016/j.wombi.2020.09.021
18. Cohen Shabot S, Korem K. Domesticating bodies: the role of shame in obstetric violence. Hypatia. (2018) 33(3):384–401. doi: 10.1111/hypa.12428
19. World Health Organization. WHO Recommendations on Intrapartum Care for a Positive Childbirth Experience. Geneva: World Health Organization (2018).
20. Kuipers YJ, Thomson G, Goberna-Tricas J, Zurera A, Hresanová E, Temesgenová N, et al. The social conception of space of birth narrated by women with negative and traumatic birth experiences. Women Birth. (2023) 36(1):e78–85. doi: 10.1016/j.wombi.2022.04.013
21. Dahan O, Zibenberg A, Goldberg A. Birthing consciousness and the flow experience during physiological childbirth. Midwifery. (2024) 138:104151. doi: 10.1016/j.midw.2024.104151
23. Goddard SG, Stevens CJ, Jackman PC, Swann C. A systematic review of flow interventions in sport and exercise. Int Rev Sport Exerc Psychol. (2023) 16(1):657–92. doi: 10.1080/1750984X.2021.1923055
24. Harris DJ, Allen KL, Vine SJ, Wilson MR. A systematic review and meta-analysis of the relationship between flow states and performance. Int Rev Sport Exerc Psychol. (2023) 16(1):693–721. doi: 10.1080/1750984X.2021.1929402
25. Jackson SA, Marsh HW. Development and validation of a scale to measure optimal experience: the flow state scale. J Sport Exerc Psychol. (1996) 18(1):17–35. doi: 10.1123/jsep.18.1.17
26. Stoll O. Peak performance, the runner’s high, and flow. In: Anshel MH, Petruzzello SJ, Labbé EE, editors. APA handbook of Sport and Exercise Psychology (Vol. 2): Exercise Psychology. Washington, DC: American Psychological Association (2019). p. 447–65.
27. Stoll O, Ufer M. Flow in sports and exercise: a historical overview. In: Peifer C, Engeser S, editors. Advances in Flow Research. Cham: Springer (2021). doi: 10.1007/978-3-030-53468-4_13
28. Kirkham M. Sustained by joy: the potential of flow experience for midwives and mothers and the blocking of that flow. In: Davies L, Daellenbach R, Kensington M, editors. Sustainability, Midwifery and Birth. London and New York: Routledge (2020). p. 99–115.
29. Abuhamdeh S. On the relationship between flow and enjoyment. In: Peifer C, Engeser S, editors. Advances in Flow Research. Cham: Springer (2021). p. 155–69. doi: 10.1007/978-3-030-53468-4_6
30. Balabanoff D, Foureur M. Disrupting the status quo to create the mindful birth space–spaces that ’sing’!. In: Davies L, Crowther S, editors. Mindfulness in the Birth Sphere. London: Routledge (2022). p. 114–29.
31. Preis H, Lobel M, Benyamini Y. Between expectancy and experience: testing a model of childbirth satisfaction. Psychol Women Q. (2019) 43(1):105–17. doi: 10.1177/0361684318779537
32. Navarro-Prado S, Sánchez-Ojeda MA, Marmolejo-Martín J, Kapravelou G, Fernández-Gómez E, Martín-Salvador A. Cultural influence on the expression of labour-associated pain. BMC Pregnancy Childbirth. (2022) 22(1):836. doi: 10.1186/s12884-022-05173-1
33. Durcan O, Holland P, Bhattacharya J. A framework for neurophysiological experiments on flow states. Commun Psychol. (2024) 2(1):66. doi: 10.1038/s44271-024-00115-3
34. Farrokh D, Davids K, Araújo D, Strafford BW, Rumbold JL, Stone JA. Towards an ecological dynamics theory of flow in sport. Acta Psychol (Amst). (2025) 253:104765. doi: 10.1016/j.actpsy.2025.104765
35. Murray-Davis B, McNiven P, McDonald H, Malott A, Elarar L, Hutton E. Why home birth? A qualitative study exploring women’s decision making about place of birth in two Canadian provinces. Midwifery. (2012) 28(5):576–81. doi: 10.1016/j.midw.2012.01.013
36. Dixon L, Skinner J, Foureur M. The emotional journey of labour—women’s perspectives of the experience of labour moving towards birth. Midwifery. (2014) 30(3):371–7. doi: 10.1016/j.midw.2013.03.009
37. Wu N, Huang R, Shan S, Li Y, Jiang H. Effect of the labour roadmap on anxiety, labour pain, sense of control, and gestational outcomes in primiparas. Complement Ther Clin Pract. (2022) 46:101545. doi: 10.1016/j.ctcp.2022.101545
38. Sperlich M, Gabriel C. “I got to catch my own baby”: a qualitative study of out of hospital birth. Reprod Health. (2022) 19(1):43. doi: 10.1186/s12978-022-01355-4
39. Hrdy SB. Mother Nature: Maternal Instincts and how They Shape the Human species. New York, NY: Ballantine Books (1999).
40. Henrique AJ, Rodney P, Joolaee S, Cox S, Shriver A, Moreira CB, et al. Understanding childbirth pain in Brazilian women: a qualitative descriptive study. Women Birth. (2021) 34(4):e368–75. doi: 10.1016/j.wombi.2020.08.003
41. Hosseini Tabaghdehi M, Keramat A, Kolahdozan S, Shahhosseini Z, Moosazadeh M, Motaghi Z. Positive childbirth experience: a qualitative study. Nurs Open. (2020) 7(4):1233–8. doi: 10.1002/nop2.499
42. Taghizdeh Z, Ebadi A, Dehghani M, Gharacheh M, Yadollahi P. A time for psycho-spiritual transcendence: the experiences of Iranian women of pain during childbirth. Women Birth. (2017) 30(6):491–6. doi: 10.1016/j.wombi.2017.04.010
43. Boucher D, Bennett C, McFarlin B, Freeze R. Staying home to give birth: why women in the United States choose home birth. J Midwifery Womens Health. (2009) 54(2):119–26. doi: 10.1016/j.jmwh.2008.09.006
44. Cheyney M, Davis-Floyd R. Birth and the big bad wolf: biocultural evolution and human childbirth. In: Davis-Floyd R, editor. Birthing Techno-Sapiens. London: Routledge (2021). p. 15–46.
45. Neerland CE, Delkoski SL, Skalisky AE, Avery MD. Prenatal care in US birth centers: midwives’ perceptions of contributors to birthing people’s confidence in physiologic birth. Birth. (2023) 50(3):535–45. doi: 10.1111/birt.12676
46. Malacrida C, Boulton T. Women’s perceptions of childbirth “choices” competing discourses of motherhood, sexuality, and selflessness. Gend Soc. (2012) 26(5):748–72. doi: 10.1177/0891243212452630
47. Mayberry LJ, Avery MD, Budin W, Perry S. Improving maternal and infant outcomes by promoting normal physiologic birth on hospital birthing units. Nurs Outlook. (2017) 65(2):240–1. doi: 10.1016/j.outlook.2017.02.007
48. MacLellan J, Ade M, Fitzsimons B, Kenyon S, Mulla S, Pope C, et al. Women’s experiences of intermittent auscultation fetal monitoring in labour: a qualitative study. Women Birth. (2024) 37(6):101805. doi: 10.1016/j.wombi.2024.101805
49. Dahlen HG, Downe S, Jackson M, Priddis H, de Jonge A, Schmied V. An ethnographic study of the interaction between philosophy of childbirth and place of birth. Women Birth. (2021) 34(6):e557–66. doi: 10.1016/j.wombi.2020.10.008
50. Moncrieff G, Gyte GM, Dahlen HG, Thomson G, Singata-Madliki M, Clegg A, et al. Routine vaginal examinations compared to other methods for assessing progress of labour to improve outcomes for women and babies at term. Cochrane Database Syst Rev. (2022) 3:CD010088. doi: 10.1002/14651858.CD010088.pub3
51. Cole L, LeCouteur A, Feo R, Dahlen H. “Trying to give birth naturally was out of the question”: accounting for intervention in childbirth. Women Birth. (2019) 32(1):e95–e101. doi: 10.1016/j.wombi.2018.04.010
52. Katvan E. Mining women’s bodies: the case of childbirth in Israel by Omi Leissner. Nashim J Jewish Womens Stud Gender Issues. (2019) 34(1):210–3. doi: 10.2979/nashim.34.1.15
53. Olza I, Leahy-Warren P, Benyamini Y, Kazmierczak M, Karlsdottir SI, Spyridou A, et al. Women’s psychological experiences of physiological childbirth: a meta-synthesis. BMJ Open. (2018) 8(10):e020347. doi: 10.1136/bmjopen-2017-020347
54. Kissler K, Jones J, McFarland AK, Luchsinger J. A qualitative meta-synthesis of women’s experiences of labor dystocia. Women Birth. (2020) 33(4):e332–8. doi: 10.1016/j.wombi.2019.08.001
55. Berman Z, Thiel F, Dishy GA, Chan SJ, Dekel S. Maternal psychological growth following childbirth. Arch Womens Mental Health. (2021) 24(2):313–20. doi: 10.1007/s00737-020-01053-9
56. Bell AF, Andersson E, Goding K, Vonderheid SC. The birth experience and maternal caregiving attitudes and behavior: a systematic review. Sex Reprod Healthc. (2018) 16:67–77. doi: 10.1016/j.srhc.2018.02.007
57. Dahan O. The riddle of the extreme ends of the birth experience: birthing consciousness and its fragility. Curr Psychol. (2021) 42:262–72. doi: 10.1007/s12144-021-01439-7
58. Karlström A, Nystedt A, Hildingsson I. The meaning of a very positive birth experience: focus groups discussions with women. BMC Pregnancy Childbirth. (2015) 15:1–8. doi: 10.1186/s12884-015-0683-0
59. Simkin P. Just another day in a woman’s life? Women’s long-term perceptions of their first birth experience. Part I. Birth. (1991) 18(4):203–10. doi: 10.1111/j.1523-536x.1991.tb00103.x
60. Takehara K, Noguchi M, Shimane T, Misago C. A longitudinal study of women’s memories of their childbirth experiences at five years postpartum. BMC Pregnancy Childbirth. (2014) 14:1–7. doi: 10.1186/1471-2393-14-221
Keywords: physiological birth, birthing consciousness, birth environment, flow state, home birth, hospital setting
Citation: Dahan O and Goldberg A (2025) Being in the zone during physiological birth: a comparative study of hospital and home birth environments. Front. Glob. Women's Health 6:1573688. doi: 10.3389/fgwh.2025.1573688
Received: 9 February 2025; Accepted: 2 April 2025;
Published: 15 April 2025.
Edited by:
Carmen Power, Swansea University, United KingdomReviewed by:
Emilie Elizabeth Egger, University of Pennsylvania, United StatesMaria Velo Higueras, Robert Gordon University, United Kingdom
Copyright: © 2025 Dahan and Goldberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Orli Dahan, b3JseWRhaEB0ZWxoYWkuYWMuaWw=